Embed Size (px)
Citation preview

Journal of The Association of Physicians of India ■ Vol. 66 ■ January 2018 59
Anticoagulation Management in Patients with Valve ReplacementDevendra Saksena1, S Muralidharan2, Yugal K Mishra3, Vivek Kanhere4, Bipin Bihari Mohanty5, CP Srivastava6, Jagdish Mange7, Manish Puranik8, Manoj P Nair9, Pankaj Goel10, Pankaj Srivastava11, RM Krishnan12, Sathyaki Nambala13, Vikrama Raja14
R e v i e w A R t i c l e
1Professor & Head, Dept. of Cardiac Surgery, Bombay Hospital, Mumbai, Maharashtra; 2Chief Cardiothoracic Surgeon, GKNM Hospital, Coimbatore, Tamil Nadu; 3Director, Department of Cardiovascular Surgery, Fortis Escorts Heart Centre, New Delhi; 4Consultant Cardiothoracic & Vascular Surgeon, Chirayu Health Centre, Bhopal, Madhya Pradesh; 5Chief Consultant Cardiothoracic Surgeon, CARE Hospitals, Bhubaneshwar, Orissa; 6Chief Consultant Cardiac Surgeon, Narayana Hrudayalaya, Jaipur, Rajasthan; 7Chief Cardiothoracic Surgeon, Shree Mahavir Health and Medical Relief Society, Surat, Gujarat; 8Consultant Minimally Invasive Cardiac Surgeon, Seth Nandlal Dhoot Hospital, Aurangabad, Maharashtra; 9Senior Consultant, Cardio Vascular Thoracic Surgery, Aster Medcity, Kochi, Kerala; 10Director, Cardiothoracic & Vascular Surgery, Ivy Healthcare, Amritsar, Punjab; 11Medical Director & Senior Consultant Cardiac Surgeon, Divine Heart & Multi-speciality Hospital, Lucknow, Uttar Pradesh; 12Chief Cardiothoracic Surgeon, Meenakshi Mission Hospital, Madurai, Tamil Nadu; 13Chief Heart Surgeon, Apollo Hospitals, Bangalore, Karnataka; 14Abbott Healthcare Pvt. Ltd.Received: 24.10.2017; Accepted: 25.11.2017
AbstractBackground: Prosthetic valve implantation requires postoperative prophylactic anticoagulation to preclude thrombotic events. The aim of this review is to assess the role of anticoagulation therapy in the management of valve replacement patients.
Methodology: Literature from PubMed, Embase, Medline and Google Scholar were searched using the terms “valvular heart disease”, “anticoagulant”, “mechanical heart valve”, “bioprosthesis”, “bridging”, “Vitamin K antagonist ( VKA)”, and “acenocoumarol”. A committee comprising leading cardiothoracic surgeons from India was convened to review the literature and suggest key practice points.
Results : Prosthetic valve implantation requires postoperative prophylactic anticoagulation to preclude thrombotic events. A paramount risk of thromboembolic events is observed during the first three months after surgery for both mechanical and bioprosthetic devices. The VKA therapy with individualized target international normalized ratio (INR) is recommended in patients after prosthetic valve replacement. Therapies for the management of prosthetic valve complications should be based on the type of complications. Special care is mandated in distinguished individuals and those with various co-morbidities.
Conclusion: In patients with prosthetic valve replacement, anticoagulant therapy with VKA seems to be an effective option. The role for non-VKA oral anticoagulants in the setting of prosthetic valve replacement has yet to be established. Furthermore, whether the novel oral anticoagulants are safe and efficacious in patients after placement of a bioprosthetic valve remains unanswered.
Introduction
Valvular heart disease (VHD) is one of the common causes of
cardiac morbidity and mortality.1 The burden of VHD is growing worldwide due to the high incidence of rheumatic heart disease (RHD), especially in developing countries and the increase in degenerative e t i o l o g i e s i n i n d u s t r i a l i z e d
n a t i o n s . 2 , 3 I n i n d u s t r i a l i z e d countries, the prevalence of VHD is est imated at 2 .5% (2) . Data on the burden of RHD in India comes from hospital data (20-50%), population based studies (2.2-1.6%) and school surveys (0.67-4.54%).4 The pattern of valve involvement is mitral (54.4%), aortic (11.1%), mitral and aortic (18.0%), tricuspid (10.7%) or pulmonary (0.04%). Overall, RHD contributed 63.4% to the prevalence of VHD.5 This pattern of VHD in India is in contrast to the developed countries, w h e r e t h e m o s t f r e q u e n t l y involved valve type is aortic with degenerative etiology.6,7 Surgical repair using either a mechanical or bioprosthetic valve is a common solution practiced globally. The worldwide annual rate of valve replacement is projected around 275,000 to 370,000; of which 55% are mechanical heart valves (MHVs) and 45% are bioprostheses heart valves. In India this number is estimated to be in excess of 10000.8 Global ly , the prosthet ic valve implantations are increasing at a rate of 5-7% per year.9-12 An ideal prosthetic valve with excellent

Journal of The Association of Physicians of India ■ Vol. 66 ■ January 201860
hemodynamic performance and long- term durab i l i ty wi thout enhanced thromboembolic risk or the requirement for long-term anticoagulation therapy does not exist. Choice of operation and the prosthesis used for those patients undergoing valve replacement is important for each individual pat ient and ideal ly should be made together by the patient , cardiologist, and surgeon.
Prosthetic valve implantation requires postoperative prophylactic a n t i c o a g u l a t i o n t o p r e c l u d e thrombotic events; which are the common cause of morbidity and mortality after surgery for VHD. A paramount risk of thromboembolic events is observed during the first three months after surgery for both mechanical and bioprosthetic devices. Nevertheless, mechanical valves exhibit life time thrombotic r i s k . At r i a l f i b r i l l a t i o n ( A F ) , which is a common arrhythmia in VHD, necess i ta tes l i fe long anticoagulation in the majority of patients; especially if it involves mitral valve. Therefore, patients on ant icoagulants are a t r i sk of thrombosis and bleeding, if the target INR leve ls are not m a i n t a i n e d . R e s t r i c t i o n s o n certain physical act ivi t ies are advised subsequently after surgery to reduce chances of bleeding accidents and these compromises the lifestyle of the young patients. These considerations emphasize the importance of addressing proper ant icoagulat ion techniques to minimize postoperative thrombotic
complications, while maintaining acceptable levels of risk related to bleeding.
Anticoagulation in ProsthesisAnticoagulants in mechanical prosthesis
Apart from the thrombogenicity of the intravascular prosthetic m a t e r i a l , m e c h a n i c a l va l v e s cause abnormal flow conditions wi th f low zones wi th in the i r components and areas of high shear stress. This could stimulate platelet activation leading to valve thrombosis and embolic events. A line of evidence shows marked benefits with vitamin K antagonist (VKA) therapy after mechanical valve placement. A meta-analysis inc luding 13 ,088 pat ients for 53,647 patient-years compared no antithrombotic therapy with VKA therapy. The study resulted in statistically significant reductions in the ra te of major systemic embol izat ion ( f rom 4 .0 to 1 .0 events per 100 pat ient-years) , total thromboembolism risk (from 8.6 to 1.8 events per 100 patient-years), and risk of valve thrombosis (from 1.8 to 0.2 events per 100 patient-years).13 Numerous studies have investigated the impact of lower and higher INR targets.14-
18 However, a meta-analysis by ACCP demonstrated an increased risk of major hemorrhage for those targeted for a higher international normalized ratio (INR) and vice
versa. However, the higher targets vary from 3.0 to 9.0 and also no evidence exists demonstrating that higher INR targets have additional benefits over harm.19 Moreover, a study has evaluated the pattern of oral anticoagulant use, achievement of target INR and the complications outside the therapeutic range in India. The study included 70.9% of mitral valve patients of which 58.2% patients were using warfarin and acenocoumarol by 44.8% patients. Thromboembolic complications were reported in 3.6% patients only when the mean INR is <1.6. Hence the study concluded to broaden the INR range from 1.6-4.20
Based on the current evidence, the American College of Chest P h y s i c i a n s ( A C C P ) a n d t h e American College of Cardiology ( A C C ) / A m e r i c a n H e a r t Associat ion (AHA) 19,21 provide recommendations regarding the use of anticoagulation and target INR in patients with mechanical prosthesis, which are comparable in both guidelines and summary of which is presented in Table 1.
Studies revealed, VKA therapy being superior to aspirin therapy alone for total thromboembolism risk and currently there is no evidence to support its replacement by antiplatelet agents (APA) as demonstrated in CAPTA trial.22
The pat ients with mechanical aortic valve were randomized to Coumadin vs aspirin/clopidogrel in this trial. The trial was stopped after valve thrombosis events reported in 22 patients in the APA group.22 Succeeding studies have shown that the addition of aspirin to VKA therapy in patients with mechanical valves leads to reduction in risk of thromboembolism and mortality when compared to VKA therapy alone (65% observed risk reduction in major systemic embolism or death in the aspirin plus VKA group) . 23,24 The addit ion of a t least 50 to 75 mg/day of aspirin is , therefore, recommended in the current ACC/AHA and ACCP guidelines in all patients with mechanical valves, though care must be taken to an individual patient’s bleeding risk.19,21
Anticoagulants in bioprosthesis
Thromboembolic events with
Table 1: The target INR values for prosthetic valve patients on VKA19, 21
Type of valve Target INRAortic position Mitral position
Uncomplicated/without risk
factors
With risk factors$
Uncomplicated/ without risk
factors
With riskfactors$
Mechanical Valve*Bileaflet 2.0-3.0 2.5-3.5 2.5-3.5 2.5-3.5Tilting disc 2.0-3.0 2.5-3.5 2.5-3.5 2.5-3.5Caged ball 2.5-3.5 2.5-3.5 2.5-3.5 2.5-3.5Caged disc valve 2.5-3.5 2.5-3.5 2.5-3.5 2.5-3.5
Bioprosthetic**Xenografts 2.0-3.0 2.0-3.0 2.0-3.0 2.0-3.0
$AF, previous thromboembolism, LV dysfunction, or hypercoagulable conditions; *VKA plus aspirin, class I indication by ACC (75-100 mg o.d.), ACCP (50-100mg o.d.) recommends aspirin only in high risk patients; **VKA for 3 months in all except uncomplicated aortic valve replacement where ACCP recommends aspirin over VKA and it should be continued if there is no other indication of anticoagulation. Postoperative aspirin (80-100mg o.d.) is recommended for all by ACC, while ACCP recommend aspirin 3 months after replacement.

Journal of The Association of Physicians of India ■ Vol. 66 ■ January 2018 61
bioprosthetic valves have been reported to range from 0.2% to 3.3% per year.19,25,26 The risk is higher in the mitral position compared to valves in the aortic position. Studies have demonstrated that bioprosthet ic devices have an increased risk for thromboembolic events during the first three months after the procedure but less than that associated with mechanical valves.27,28
Several large cohort studies h a v e a d d r e s s e d t h e n e e d o f VKA anticoagulation with and without APA after bioprosthetic valve replacement29-32 Numerous Indian studies have demonstrated the benefits of adding APA to anticoagulants.33-35 The optimal antithrombotic regimen and its durat ion af ter placement of a bioprosthetic device are less clear across these studies. The optimal antithrombotic regimen and its durat ion af ter placement of a bioprosthetic device are less clear across these studies.
The variat ion in an optimal
antithrombotic regimen and its duration after valve replacement in the literature have made the r e c o m m e n d a t i o n s g i v e n b y guidelines for bioprostheses to be d i s s imi la r compared wi th the mechanical prosthesis. The ACCP current ly recommends VKA therapy with target INR 2.5 (range 2.0 to 3.0) for the first three months after bioprosthetic mitral valve replacement . For aortic valve replacement with a bioprosthetic device, the ACCP recommends aspirin (50 to 100 mg/day) over VKA therapy for the first three months after surgery, for patients in whom there is no other indication for anticoagulation (i.e., atrial dysrhythmias, history of thromboembolism, etc.). If the patient remains without a definitive indication for anticoagulation, the ACCP recommends the continuation of aspirin therapy without VKA therapy beyond the initial three-month postoperative period in all patients with a bioprosthesis. In the 2014 ACC/AHA guidelines, class I recommendations supporting the
use of VKA therapy in patients wi th b ioprosthet ic va lves are not ava i lab le . The ACC/AHA does, however, offer a class IIa r e c o m m e n d a t i o n s u p p o r t i n g VKA therapy for the first three months after bioprosthetic valve replacement at the mitral position and a class IIb recommendation s u p p o r t i n g V K A t h e r a p y f o r t h e f i r s t t h r e e m o n t h s a f t e r bioprosthetic valve replacement at the aortic position. Aspirin therapy at a dose of 75 to 100 mg/day is recommended in patients regardless of whether ant icoagulat ion is employed in a l l b ioprosthet ic valve patients. Moreover, there are no specific recommendations offered in regards to duration of aspirin therapy in this population. Recommendations from the ACC/AHA largely leave the choice of the antithrombotic regimen in the setting of bioprosthetic valve replacement up to individual clinicians. Several factors that may influence a clinician’s decision include institutionally-specific o u t c o m e s , t h e l i k e l i h o o d f o r patient adherence to medication regimen, prior personal experience, regional convention, and personal preference . The durat ion and i n t e n s i t y o f t r e a t m e n t w i t h aspirin are also left up to the individual clinician’s discretion. These recommendations have been summarized in Table 1.Anticoagulants in TAVR
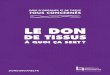
T r a n s c a t h e t e r a o r t i c va l ve replacement (TAVR) has become established as a treatment option for patients with symptomatic aortic stenosis. In comparison with surgical aortic valve replacement, TAVR offers superior quality of life with similar mortality rates among pat ients at very high surgical risk.36 However, thromboembolic complicat ions f rom TAVR are significant, and stroke, in particular is a concern.37 While the immediate procedural risk relates to valvular debris embolization, 50% of strokes develop after the first day and may re late to non-procedural e v e n t s . 3 6 - 3 8 T h e i n c i d e n c e o f cerebrovascular events after TAVR remains raised for ≤60 days. This implies that the prothrombotic environment of the bioprosthesis
Fig. 1: Post-procedural antithrombotic recommendations in patients undergoing transcatheter aortic valve implantation (TAVI)

Journal of The Association of Physicians of India ■ Vol. 66 ■ January 201862
itself may be implicated in distal thromboembolism, and therefore ant iplatelet or ant i thrombotic treatment should play an important role in stroke prevention.39
Va r i o u s c o m b i n a t i o n s o f antithrombotic regimens (single-antiplatelet , dual-antiplatelet , or VKAs) have been used, but evidence-based guidance remains lacking. A number of randomized a n d n o n - r a n d o m i z e d s t u d i e s evaluated the risk of embolization, optimal antithrombotic regimen and duration thereof after TAVI.36-
41 The evidence on anticoagulation after TAVI from India is limited t o o n l y f e w c a s e r e p o r t s . 4 2 - 4 3 Antithrombotic recommendations for TAVI from various guidelines are illustrated in Figure 1.
Key pointsAnticoagulants in mechanical prosthesis • VKA therapy with a target INR
range of 2.0 to 3.0 is recommended in patients with mechanical aortic valve replacement without risk factors.
• VKA therapy with a target INR range of 2.5 to 3.5 is recommended in patients with mechanical aortic valve replacement with risk factors- AF, previous thromboembolism,
LV dysfunction, or hypercoagulable conditions.
• In mechanical mitral valve replacement, VKA therapy with a target INR range of 2.5 to 3.5 is recommended in patients with and without additional thromboembolic risk factors.
• With mechanical valves in both the aortic and mitral position, a target INR range of 2.5 to 3.5 is recommended.
• VKA therapy in combination with antiplatelet therapy (aspirin 75- 100mg) is recommended for long-term management over no antiplatelet therapy with mechanical valve prosthesis.
Anticoagulants in bioprosthesis• VKA therapy is recommended in
bioprosthetic aortic valve and mitral valve replacement, with a target INR range of 2.0 to 3.0 over no VKA therapy for 3 months
• In patients with dual valve replacement (aortic, mitral) VKA therapy is recommended with a target INR range of 2.5 to 3.5
• After bioprosthetic aortic or mitral valve replacement, antiplatelet therapy at a dose of 75 to 100 mg/day is recommended
Anticoagulants in TAVR• Anticoagulants are recommended
pretreatment and during treatment.• Life-long aspirin 75-100 mg/day
along with clopidogrel 75 mg daily is recommended for 3- 6 months.
Bridging AnticoagulationThe perioperative management
of patients who are receiving VKAs or antiplatelet drugs and require a surgical or invasive procedure presents a dilemma for practicing clinicians. Several factors such as type, location and number of heart valve prosthesis and type of procedure and r isk factors should be taken into account while managing patients with mechanical heart valves in whom interruption of anticoagulation therapy is needed for diagnostic or surgical procedures. To minimize the delay in achieving therapeutic ant icoagulat ion, a “br idging” a n t i c o a g u l a n t i s p r e s c r i b e d . The “br idge” i s adminis tered p a r e n t e r a l l y ( s h o r t a c t i n g anticoagulant as UFH or LMWH), thereby providing an immediate anticoagulant effect. However, the use of low molecular weight heparin (LMWH) or unfractionated heparin (UFH) as perioperative bridging is an off-label use because their use is not approved by regulatory authorities or drug manufacturers in this clinical setting as a bridging agent. There is a relative paucity of well-designed clinical trials to enlighten best practices. There are a disproportionately large number of methodologically weak observational studies.
Large number of studies have e va l u a t e d , a n d p r o p o s e d a n interval of 1-3 days preoperatively and 7 days postoperatively for VKA interruption. 44 However , VKA interruption may not be required in minor procedures like dental procedures,45-50 minor dermatological procedures51-53 and cataract surgery.54 Furthermore, no wel l s tandardized s tudies were performed regarding the use of LMWH and UFH. However, a study showed no significant difference in thromboembolic and major bleeding between patients bridged with LMWH and those
bridged with UFH.55 Most studies assessing the use of LMWH as bridging anticoagulation have used therapeutic dose regimens; for detailed information refer Douketis et al.56 Two studies have used low dose LMWH (including patients with mitral valve prosthesis),57,58 however, whether the dose utilized is sufficient is not known clearly as it can be argued that higher doses of LMWH are needed for the prevention of arterial thrombosis. The latter, however, is also not established.
O n a c c o u n t o f t h e c u r r e n t e v i d e n c e , A C C a n d A C C P recommend uninterrupted VKA with local hemostasis optimizing agents in procedures with minimal bleeding, such as surgeries on the skin (excision of basal and squamous cell skin cancers, actinic keratosis, and premalignant or cancerous skin nevi), cataracts, glaucoma and dental c leaning or simple treatment for dental caries. For tooth extractions and endodontic procedures, ACCP recommend uninterrupted VKA with co-administration of an oral prohemostatic agent or stopping VKAs for 2 to 3 days (part ia l reversal). However, both guidelines recommend interruption of VKA with bridging anticoagulation in patients with any mitral valve prosthesis, caged-ball, tilting disc aortic valve prosthesis, bileaflet AVR with additional risk factors such as the recent (within 6 months) stroke or transient ischemic attack, prior thromboembolism during the temporary interruption of VKAs. In such cases when the interruption is required, ACC recommends s topping for 2 -4 days while ACCP recommends not less than 5 days before the p r o c e d u r e . B o t h r e c o m m e n d restarting approximately 12 to 24 h after surgery when there is adequate hemostasis instead of la ter resumption of VKAs. Moreover, the reversal of VKA required during emergency surgery or invasive procedures can be achieved by administration of fresh frozen plasma (FFP) or intravenous prothrombin complex concentrate (PCC).

Journal of The Association of Physicians of India ■ Vol. 66 ■ January 2018 63
Key points• It is not recommended to interrupt
VKA therapy during minor dental procedures (cleaning), dermatological procedures and cataract surgery due to minimal bleeding.
• In patients with low thrombotic risk (bileaflet AVR without any risk factors) it is recommended to interrupt VKA without bridging.
• Bridging anticoagulation is recommended in patients with any mitral valve prosthesis, any caged-ball or tilting disc aortic valve prosthesis, bileaflet AVR with additional risk factors, patients with recent (within 6 months) stroke or transient ischemic attack, patients with prior thromboembolism during temporary interruption of VKAs.
• When interruption of VKA therapy is required, it is recommended to stop 2-4 or not more than 5 days before the procedure. The VKA should be restarted after 12-24 hours after surgery.
• The reversal of VKA therapy during emergency surgeries can be achieved by administration of FFP or PCC. Low dose vitamin K may be administrated with caution to sustain effects with FFP as rebound is known with vitamin K.
• Interruption of VKA therapy with bridging anticoagulants is recommended for not more than 2 days in case of major surgeries.
Point of Care INR TestingT h e s u b t h e r a p e u t i c t a r g e t
I N R i n c r e a s e s t h e r i s k o f thromboembolic events, on the other side, above the therapeutic INR presents the patient to bleeding risk. Apart from the assistance i n d e c i d i n g t h e a p p r o p r i a t e dosage regimen, monitoring helps in avoiding over coagulat ion. Routine monitoring can help detect dangerous situations well in time, allowing dose adjustment, as well as actions can be taken to prevent recurrence of such situations. The prothrombin time (PT) test is the most common test used to monitor anticoagulation therapy that is expressed as the INR. Further, the time in therapeutic range (TTR) is a good overall measure of the quality of antithrombotic treatment with VKAs in patients with valvular heart disease.59-62
The gold standard for monitoring INR is the lab testing of blood obtained by venipuncture, in the
hospital. The point of care (POC) INR systems can be an alternative to older laboratory test ing of INR. POC testing involves putting a single drop of blood from a f inger st ick, onto a test s tr ip. POC is aimed at convenience for the patient , faster test results to a healthcare provider, faster decision making, improved clinical outcome and reduced healthcare resources. However, these devices are economical as they reduce the cost of visiting the healthcare facility. This is of great importance in India, as most of INR facilities are available far from the urban or semi urban area. These POC devices have shown to be cost-effective for patients on long term anticoagulants.63,64 Studies have found a statistically significant advantage of self-management methods for achieving better INR control in patients with mechanical valves. 65,66 Nevertheless , ACC/AHA recommends the practice of self-management of patients over outdoor INR monitoring for VKA anticoagulation, in patients who are motivated, and can demonstrate competency in self-management strategies.
Key points• Practice of self-management is
recommended in patients who are living in urban and semi-urban areas, who are competent of doing the same.
• Use of POC devices can be alternated with the conventional laboratory testing to reduce hospital visits and the cost of the treatment.
Management of Prosthetic Valve ComplicationsThromboembolic events
T h e a n n u a l r i s k o f thromboembolic events in patients with a mechanical heart valve is 1% to 2% versus 0.7% with a bioprosthetic valve, even with a p p r o p r i a t e a n t i t h r o m b o t i c t h e r a p y . 1 3 , 1 7 T r a n s t h o r a c i c echocardiogram (TTE) is the first step in the evaluation of suspected prosthetic valve thromboembolism to evaluate valve hemodynamics. H o w e v e r , t r a n s e s o p h a g e a l echocardiography (TEE) is needed o f ten , par t i cu lar ly for mi t ra l prosthetic valves.21,67 However, if
the echocardiography findings are unchanged the prosthetic valve should be considered the source of thromboembolism in suspected cases. 68
T h e p a t i e n t s w i t h t h e thromboembol ic event should be evaluated for the adequacy of anticoagulation and any issues related to compliance with medical therapy. Screening questions about symptoms that may be related to embolic events are especially important if anticoagulation has been suboptimal.69 Measures to improve patient compliance and more frequent monitoring should be instituted.70,71 Patients’ education about symptoms related to embolic events and instructing them to promptly report to a healthcare provider immediately after onset of an event should be in routine.72-75
Thrombosis of prosthetic valves
The prevalence of mechanical valve thrombosis is 0.3-1.3% per patient-year in developed countries and 6 .1% per pat ient -year in developing countries.76-78 Type of valve and location also affect the risk of thrombosis. Thrombosis is 20 times more likely to occur in the tricuspid position; mitral prosthetic valve thrombosis is 2-3 times more common than aortic prosthetic thrombosis.
It is suggested to perform TTE in suspected cases of thrombosis. This will allow evaluation of valve hemodynamics and detection of valve stenosis or regurgitation, measurement of left ventricular (LV) size and systolic function, left atrial size, right heart function, and an estimation of pulmonary pressures . 78,79 The TEE a l lows direc t imaging of mechanica l valve thrombosis particularly for thrombi on the left atrial side of the mitral valve.78,80 In addition to TTE and TEE, f luoroscopy can be used to assess annular or valvular calcification, as it enables calcification to be distinguished f r o m f i b r o s i s w i t h a h i g h e r specificity than echocardiography. I t i s a lso useful to assess the kinetics of the mobile part of a mechanical prosthesis. However, ACC recommends TTE in patients with suspected prosthetic valve

Journal of The Association of Physicians of India ■ Vol. 66 ■ January 201864
thrombosis to assess hemodynamic severity and resolution of valve dysfunction, and if the thrombus is detected, TEE to assess thrombus size and valve motion. The left s i d e d p r o s t h e t i c h e a r t va l ve thrombosis can be treated either wi th f ibr inolyt ics or surgica l intervention. When treating left-sided PVT, the risks associated with re-operative surgery must be weighed aga ins t the r i sks of embol ic complicat ions and bleeding associated with the use of fibrinolytic therapy. Factors that identify patients at risk for adverse outcomes of fibrinolytic therapy include active internal bleeding, history of hemorrhagic stroke, recent cranial trauma or neoplasm, diabetic hemorrhagic retinopathy, large thrombi, mobile thrombi, systemic hypertension (>200 mm Hg/120 mm Hg) , hypotension or shock, and New York Heart Association (NYHA) class III to IV symptoms. The degree of risk is directly related to thrombus size. Thrombus area (2D TEE) >0.8 cm2 and thrombus diameter 1.0 cm is associated with increased embolic risk. Rate of complications increases 2.4–fold, per 1.0 cm2 increase in s ize , which makes surgery better option.80 In patients with recent hemorrhagic stroke, surgery is a better choice because of the bleeding risks associated with fibrinolysis.80 Although RCTs have not been performed, the weight of the evidence favors surgical intervention for left-sided prosthetic valve thrombosis unless the patient is asymptomatic and the thrombus burden is small.81,
82 However, fibrinolysis of right-
sided valve thrombosis appears better option with the resulting small pulmonary emboli seem to be well tolerated and systemic emboli are uncommon.83,84
ACC and ACCP recommend fibrinolytics or surgical intervention for management of PVT; the clinical judgment should be based on the position of the valve (left or right) and thrombus burden as assessed by echocardiography.19,21
Bleeding complications
The incidence of major bleeding complications in patients with a mechanical valve and taking oral anticoagulants varies from 0.34% to 1.32% per patient-year.85 The prominent feature of anticoagulant overdose is bleeding, which may be manifested as nasal bleeds, h a e m a t e m e s i s , h a e m o p t y s i s , gastrointestinal bleeding, vaginal bleeding, haematuria, cutaneous haemorrhages, gingival bleeding, haematomata, and bleeding into joints or menorrhagia. Numerous risk scores have been developed to help predict bleeding events, considering the other comorbidities such as previous gastrointestinal bleeding, chronic kidney disease, previous stroke or myocardial infarct ion, and anemia (Table 2 ) . F u r t h e r m o r e , e x c e s s i v e anticoagulation (INR ≥ 5) greatly increases the risk of hemorrhage. Discontinuation of anticoagulation for 1-2 weeks had a low probability o f t hr omb oe mb ol i c even t s i n patients with high embolic risk.86
I n t h e p r e s e n c e o f m a j o r bleeding (active bleeding) with VKA, four factor prothrombin complex concentrate (FFPCC) or
FFP should be given for reversal of anticoagulation.21,56 However, ACCP recommends additional use of Vitamin K (5-10 mg IV inj.) along with coagulation factors and shows a preference for FFPCC over FFP. In the absence of active bleeding, but INR>10, withholding VKA and administrating oral Vitamin K (1-2.5mg) is recommended.21,56 In the cases of no active bleeding and INR between 4.5-10, withholding VKA with the serial determination of INR, and resuming the same, once the therapeutic INR is achieved is suggested.21,56
Key pointsThromboembolic events• TTE is recommended for diagnosis of
thromboembolic events.• Treatment with tPA and heparin is
recommended to patients with stroke; other vascular occlusions should be managed by surgery.
• Daily aspirin (75-80 mg) is recommended in anticoagulated patients with thromboembolic events with increase in the target INR range (mechanical AVR: 2.5-3, mechanical MVR: 3-4).
• In patients with bioprosthetic valve, who are already on aspirin, addition of VKA can be considered.
• Measures to increase patient compliance (patient education) are recommended in all patients with thromboembolic events.
Thrombosis of prosthetic valves• It is recommended to address adequacy
of anticoagulation (low INR), and exclusion of other causes of high gradients like anemia, tachycardia, fever.
• TTE is recommended in patients with suspected prosthetic valve thrombosis to assess hemodynamic severity and resolution of valve dysfunction.
Table 2: Bleeding risk prediction scores
Risk score Bleeding risk factors Risk classification points
Annual rate of major bleeding
Outpatient bleeding risk index169
Age ≥ 65 years, history of stroke, history of gastrointestinal bleeding, recent MI or, Hct<30% or SCr> 1.5 mg/dl or diabetes; 1 point each
Low: 0Intermediate: 1-2High: ≥3
Low: 3Intermediate: 12High: 30
Contemporary bleeding risk model170
(0.49 x age ≥70 years) + (0.32 x female sex) + (0.58 x remote bleed) + (0.62 x recent bleed) + ( 0.71 x alcohol/drug abuse) + (0.27 x diabetes) + (0.82 x anemia) + (0.32 x antiplatelet therapy)
Low: ≤1.07Intermediate: 1.07-2.18High: > 2.19
Low: 0.9Intermediate: 2.0High: 5.4
HAS-BLED171 Hypertension (SBP>160mmHg), abnormal renal/liver function, stroke, history of bleeding, labile INR, age >65 years), drugs (antiplatelet/NSAIDs/alcohol); 1 point each
Low: 0-1Intermediate: 2High: ≥3
Low: 1.1Intermediate: 1.9High: 4.9
HEMORR2HAGES172 Hepatic or renal disease, ethanol abuse, malignancy, older age (>75 years) reduced platelet function, re-bleeding, uncontrolled hypertension, anemia, genetic factors (CYP2C9 SNP), excessive fall risk, stroke; 1 point each
Low: 0-1Intermediate: 2-3High: ≥4
Low: 2.1Intermediate: 5High: 8.8
MI= myocardial infraction; SBP= systolic blood pressure; NSAIDs= non-steroidal anti-inflammatory drugs

Journal of The Association of Physicians of India ■ Vol. 66 ■ January 2018 65
• TEE is recommended to assess thrombus size and valve motion
• UFH is recommended in a very small thrombus burden of left sided PVT, if not treated fibrinolytics are recommended.
• In patients with left PVT, with thrombus burden ≤ 0.8 cm2, fibrinolytics are recommended over surgery.
• Emergency surgery is recommended in case of Left sided PVT with a mobile or large thrombus >0.8 cm2. Fibrinolytics can be considered in patients with contra-indications to surgery.
• The right sided thrombosis can be treated by fibrinolytics if no contraindications to fibrinolytics are present. If fibrinolytic therapy is successful, IV UFH is recommended until the patient achieves an INR of 3.0 to 4.0 for aortic prosthetic and 3.5 to 4.5 for mitral prosthetic valves.
• Patients with protein C and S deficiency are recommended for a change of mechanical to bioprosthetic valves as they are unsuited for Coumadin therapy
Bleeding complications• For patients with VKA associated active
bleeding, withhold VKA, administer FFP or PCC. Vitamin K may also be used with caution.
• In absence of active bleeding, and INR in range of 4.5-10, it is recommended withholding VKA with serial INR determination, and resuming when INR is therapeutic.
• In absence of active bleeding, and INR >10, it is recommended withholding VKA and administering FFP or PCC. Oral Vit.k1 (1-2.5 mg) can also be administered with caution.
Factors Affecting VKA TherapyPharmacogenetics
Growing evidence indicates that up to 60% of the individual p h a r m a c o l o g i c a l r e s p o n s e t o wa r f a r i n m i g h t b e d u e t o genetic variables and affected by polymorphisms in the genes mainly, v i tamin K epox ide reductase complex subunit 1 (VKORC1), the target enzyme of warfarin and cytochrome P450 2C9 (CYP2C9), the main enzyme involved in warfarin metabolism.87 Similarly, many Indian studies have earlier shown that around 75-80% of the Indian population carries VKORC1-1639GG (rs9923231) genotype, which is associated with the high dose requirement.88-92
Recently, FDA has recommended pharmacogenetics testing before in i t ia t ing warfar in . However , ACCP remains against the routine use of pharmacogenetics testing for guiding doses of VKA in patients initiating VKA therapy.93,94
Anticoagulant interactionsDrug-drug interaction
As VKAs are metabolized mainly by cytochrome P-450 (CYP) 2C9, the inhibition of CYP 2C9 results in a decreased catabolism of VKAs and a stronger anticoagulant effect, whereas its induction enhances their catabolism and leads to a lower anticoagulant effect. Drugs such as amiodarone, fluconazole, f l u v a s t a t i n , f l u v o x a m i n e , isoniazid, lovastatin, miconazole, metronidazole , t r imethoprim-sulfamethoxazole, phenylbutazone are known inhibitors of CYP 2C9, thus potentiating VKAs effect.95 Antibiotics, which cause decreased production of vitamin K by the intestinal microbiota result in an increased sensitivity to VKAs. Barb i tura tes ( carbamazepine , rifampicin) are inducers of CYP 2C9.95 Over the counter medications, i . e . p a r a c e t a m o l a n d o t h e r nonsteroidal anti-inflammatory drugs (NSAIDS) were shown to enhance the anticoagulant effect of warfarin, thus patients receiving warfarin must monitor their INR more f requent ly when taking these medicat ions espec ia l ly , paracetamol at doses exceeding 2g/day.96-98 However, acenocoumarol compared to warfarin may elicit lower drug interactions due to less sensitive to metabolic enzymes (CYP2C9) and easy clearance from the body.99 In line with this, ACCP suggests avoiding concomitant treatment with NSAIDs, including COX-2-se lect ive NSAIDs, and certain antibiotics for patients taking VKAs.93 For a more detailed list of drugs interacting with VKA, refer Bungard et al.95
Drug-Herbs interaction
The interaction of VKAs with herbs is well reported in literature. These includes the interaction with Panax ginseng, Hypericumper-foratum, Salvia milthiorizza, Gingko b i l oba , Serenoarepens , Ange l i ca sinensis, Vaccinium species, Allium
sativum, Zingiberofficinale, Tanac-etumparthenium, Luciumbarbarum, Matricariachamomilla, Boswelliaser-rata and Camellia sinensis have been estimated.100,101
Drug -food interaction
Indians with their different d i e t a r y h a b i t s c o m p a r e d t o their western counterparts are m o r e p r o n e f o r V K A s - f o o d interactions. An average Indian consumes more of dietary green leafy vegetables, which would prevent the achievement of target INR in patients with warfarin/a c e n o c o u m a r o l a n d c a u s e variabil i ty in INR values. The interaction between the dietary vitamin K and VKAs is well known. Evidence has demonstrated that anti-coagulated patients should maintain a steady intake of vitamin K once INR stabil i ty has been a c h i e ve d . Pa t i e n t s s h o u l d b e educated not to avoid Vitamin K rich foods; however, they should be advised to maintain the vitamin K content of diet constant. The best way to achieve this is by avoiding changes to normal eating pa t te rns . 102 ,103 ACCP sugges t s against routine use of vitamin K supplementation for patients on VKA.93
Key pointsDrug-drug interaction• It is recommended to avoid drugs
metabolized by cytochrome P450 enhancing or inhibiting VKAs effect during the therapy.
• It is recommended to educate patients on drug interaction with over the counter drugs and antibiotics; and need for frequent monitoring INR when they are used.
Drug-food interaction• Patients are advised to maintain
constant Vit K composition in the diet to avoid fluctuation of VKA therapy.
• Food inhibiting (Cabbage, spinach, brussels, sprouts) and potentiating (Mango, grapefruit, cranberry) the efficacy of VKAs should be taken in moderation while maintaining regularity
Anticoagulation in Special Patient PopulationsPregnancy
Pregnancy is a hypercoagulable state, due to increase in fibrinogen,

Journal of The Association of Physicians of India ■ Vol. 66 ■ January 201866
f a c t o r s V I I , V I I I a n d X , v o n Willebrand factor, and a relative decrease in protein S activity, stasis, and venous hypertension.104 T h e i n c r e a s e i n t o t a l b l o o d volume affects the distribution of anticoagulants during pregnancy contr ibut ing to unpredictable c h a n g e s i n t h e a m o u n t o f medication required. 105,106 This state of hypercoagulability extends into the postpartum period too, and requires a persistently higher maintenance dose of warfarin.105 Thus, optimal anticoagulat ion therapy is considered essential, but the appropriate choice of agent among the options available (VKAs, hepar in or LMWH) is highly debatable.107
T h e l o w m o l e c u l a r we i g h t of warfarin enables it to cross the placental barrier and cause embryopathy. The embryopathy actions are dose dependent; reduced adverse events are seen with dose <5mg.108-110 However, warfarin can be replaced with LMWH since they do not cross the placenta. The use of heparin is associated with reported incidence of 12-24% of the increased risk of maternal thromboembolic events.111 Henceforth, women of childbearing age should be warned about the teratogenic and harmful ef fects of VKAs, especial ly in early pregnancy. They should be advised to use secure methods of contraception while on VKAs. If pregnancy is suspected, early pregnancy test 5 weeks from last menstrual period must be offered. Hence, if patients are not prior educated about the teratogenic effects, the risk of embryopathy increases with continuous use of VKAs in the 1st trimester.112
T h e c u r r e n t A C C , A C C P guidelines recommend warfarin in first trimester if dose required for target INR is <5mg (or equivalent acenocoumarol dose). VKAs should be replaced with heparin at 36th week of gestation before delivery. T h e r e c o m m e n d a t i o n s f r o m ACC, ACCP and ESC have been summarized in Table 3.21,113,114
Elderly population
Management of anticoagulation in elderly patients represents a particularly challenging issue.
Indeed, this patient population is at high thromboembolic and hemorrhagic r isk . Assessment o f t h e b e n e f i t - r i s k b a l a n c e o f a n t i c o a g u l a t i o n i s t h e key point when decis ions are made about introducing and/or continuing such treatments in the individual elderly patient. In order to maximize the safety of anticoagulation in the elderly, factors like comorbidities and co-medication, pharmacokinetic and pharmacodynamics alteration due to the renal and hepatic function associated with aging, consequences due to insuff ic ient educat ion, need to be considered.115-117 The European society of cardiology- working group on thrombosis recommend considering all of the above factors for antithrombotic therapy in elderly.94,118
Renal impairment
As VKAs are metabolized in the liver, no dosage adjustments are required in patients with chronic renal impairment. Pharmacokinetic studies have shown that anti-Xa activity is prolonged in patients with severe renal impairment (creatinine clearance <30 mL/ min) and, to a lesser extent, in patients with moderate dysfunction (30-50 mL/minute) . 119 The prevalence of AF is reported to be higher in patients with renal impairment. Also, the risk of AF development increases with worsening of renal function.120 Heparin derivatives depend largely on renal excretion; dosage adjustment is necessary in order to avoid accumulation and hence over-anticoagulation.115 Dosage adjustment for factor Xa inhibitors in patients with renal insufficiency is recommended by ACCP.121
Key pointsPregnancy• Women of childbearing age who have
undergone valve replacement should be educated about the importance of early detection of pregnancy and informing the healthcare provider (cardiologist and gynecologist) immediately, which can help to avoid the potential teratogenic and harmful effects associated with higher dose VKAs
Before 36 weeks of gestation• Oral VKA therapy is recommended
throughout pregnancy in patients with daily warfarin dose requirement of ≤5mg (or equivalent acenocoumarol dose) with target INR of 3.
• It is recommended to replace VKAs by LMWH and UFH if warfarin dose>5mg (or equivalent acenocoumarol dose) is required for achieving therapeutic INR.
• Low dose (75-100 mg) aspirin is recommended in second and third trimester (only in high risk patients or all patients or in stable to reduce INR by 0.5 and reduce dose of VKAs).
At 36 weeks of gestation• At 36 weeks of gestation, VKA should
be discontinued and iv UFH or LMWH should be initiated and continued till 36 hours before delivery.
• If vaginal delivery is expected VKA should be discontinued at 34 weeks and LMWH should be administered with monitoring of factor X assays.
• If labor starts unexpectedly, 2-4 mg IV vitamin K and FFP should be administered to reduce risk of fetal injury.
• When hemostasis is adequate, VKA therapy should be restarted on day 1-2 as maintenance dose.
Elderly population• Frequent renal tests and observation
for adverse effects with concomitant medications, are recommended in elderly patients considering them as high risk patients for developing hemorrhagic complications.
Renal impairment• Monitoring of anticoagulation therapy
in renal insufficiency patients is recommended to avoid the risk of over anticoagulation
Concomitant Cardiac DiseaseHeart failure
Prosthetic valve patients are at high risk of congestive cardiac failure due to significant cardiac compromise. Cardiac medicines l i k e a n g i o t e n s i n c o n v e r t i n g enzyme inhibitors, diuretics, and digoxin should be given as per the standard heart failure management guidelines.122 CAD
The concurrent use of dual antiplatelet agents with VKAs has been a major issue in percutaneous c o r o n a r y i n t e r v e n t i o n ( P C I ) patients in an era of widespread use of drug-eluting stents (DES).

Journal of The Association of Physicians of India ■ Vol. 66 ■ January 2018 67
Table 3: Recommendations on management of anticoagulation in pregnancy
ACC/AHA21 ACCP113 ESC114
Before 36 gestational weeksOral (VKA) • Can be used throughout pregnancy (class IIa) with
substitution by UFH/LMWH during weeks 6-12 of gestation if
- preferred by the patient - dose of warfarin required to achieve target INR >5mg
(class IIa) - just before planned delivery has to be replaced by
UFH or LMWH (class I) - Strongly recommended in MPV in 2nd and 3rd
trimesters
• Can be used throughout pregnancy in high risk* patients with UFH or LMWH before delivery (grade 1A)
• If warfarin daily dose is <5mg, oral anticoagulation is the safest regimen with 3% embryopathy throughout the pregnancy
Heparin derivatives
• Recommendations on 1) s.c use of LMWH and UFH throughout pregnancy2) s.c UFH in the 1st trimester completely removed in current 2014 guidelines.
• The patients who prefer: **LMWH administered twice daily and the dose should be adjusted to attain peak anti-factor Xa levels: 0.8–1.2 U/mL approx. 4–6 hours after the injection.
• Alternatively, continuous IV UFH (with aPTT at least twice that of the control) during the 1st trimester is permissible if the dose of warfarin >is 5 mg/day
• IV UFH in the first trimester is difficult from a practical standpoint, as a three-month hospital admission is required.
• Monitored UFH or LMWH can be option throughout gestation Or during 6-12 weeks of gestation (grade 1A)
• In low risk patients LMWH should be given twice daily with anti-factor Xa levels of 0.35–0.70 U/mL 4 h after sc injection
• The starting dose should be 100 U/kg of dalteparin and 1 mg/kg of enoxaparin.
• LMWH and UFH considered if warfarin dose>5mg
• LMWH adjusted to achieve anti factor Xa activity of 0.8-1.2 U/ml 4-6 h after administration, monitored on a weekly basis
All of the above guidelines agree that LMWH should be given twice daily and that it is harmful to administer LMWH without regularly monitoring the patient’s anti-factor Xa levels
Aspirin • Low dose (75-100mg/day) given in second and third trimesters (Class I)
• Low dose given in addition to anticoagulation in high risk patients (grade 2C)
• Not recommended
Target INR • 3 for all prosthetic valve patients • 2-3 for patients with bileaflet aortic valves w/o high risk factors*
• No target recommendation
After 36 gestational weeks• The ACC/AHA guidelines suggest stopping warfarin
at 36 weeks and starting continuous IV UFH with aPTT monitoring, which should be continued until approximately 2–3 weeks before the planned delivery.
• Additionally, they recommend that UFH be discontinued 4–6 hours before the planned delivery and restarted 4–6 hours after delivery.
• In the absence of significant bleeding, oral warfarin should then be initiated 24 hours after the birth.
• ESC guidelines suggest stopping warfarin at 36 weeks and starting dose-adjusted IV UFH or LMWH.
• This treatment should continue until 36 hours before delivery, when LMWH should be replaced by IV UFH
• Continuing VKA until the patient is close to term$ (At this point, warfarin should be replaced by IV UFH or LMWH.
• If spontaneous labour occurs on oral anticoagulation, a caesarean section is indicated due to obstetric-related causes.
*First generation prosthesis, mitral valve prosthesis, history of thromboembolism, atrial fibrillation, left ventricular dysfunction; ACC/AHA: American college of cardiology/American heart institute; ACCP: American college of chest physician; ESC: European society of cardiology; INR: international normalized ratio; LMWH: low molecular weight heparin, UFH: unfractionated heparin; **ACC/AHA recommend to discuss the preferred option of anticoagulation in pregnant patients; $although the word term is not specified, it is generally accepted to signify 48 hours before delivery).
Approximately 5% of patients requiring PCI also present with an indication for oral anticoagulation therapy. In such cases, the type of stent selected; the use of oral anticoagulants, antiplatelet, or their combinations; the target INR; and the duration of treatment i s essent ia l cons iderat ions in relation to the risk of thrombosis/t h r o m b o e m b o l i c e v e n t s a n d bleeding risk. Whenever possible, shorter durations of triple therapy are favored in preference to longer durations of triple therapy.123 The
WOEST (What i s the Optimal Antiplatelet and Anticoagulant Therapy in Patients with Oral Anticoagulation and Coronary Stenting) trial is the first published study to address the question of optimal antiplatelet therapy in patients taking oral anticoagulant medication. Patients randomized to single antiplatelet treatment with clopidogrel had significantly fewer b leeding compl icat ions and no increase in thrombotic e ve n t s c o m p a r e d w i t h t h o s e randomized to DAPT with aspirin
and clopidogrel.124
The ACC/AHA recommends in patients with non ST segment elevation acute coronary syndrome (NSTE-ACS) who require oral anticoagulation for AF, mechanical h e a r t v a l v e , d e e p v e n o u s thrombosis, or other conditions, a bare-metal stent may offer the advantages of lower bleeding risk over a DES because of the potentially shorter duration of triple antithrombotic therapy.125 However, these recommendations do not specify the optimal treatment

Journal of The Association of Physicians of India ■ Vol. 66 ■ January 201868
according to the various indications for anticoagulation or the duration of treatment, nor do they take into account the estimated thrombosis and bleeding risks.Atrial Fibrillation
Overall , i t is estimated that the incidence of post-operative atrial fibrillation is approximately 30% after pure coronary artery bypass grafting (CABG) surgery, 40% following valve replacements o r r e p a i r , a n d i n c r e a s e s t o approximately 50% after combined CABG / valvular procedures.126,127 In a large prospective trial, the Prophylactic Oral Amiodarone for the Prevention of Arrhythmias that Begin Early After Revascularization, Valve Replacement , or Repair (PAPABEAR), amiodarone was compared wi th p lacebo . Ora l amiodarone prophylaxis of atrial tachyarrhythmia af ter cardiac surgery was effective and safe.128 Furthermore, a meta-analysis of 19 trials comparing amiodarone with placebo has demonstrated a significant reduction in AF (reduced by 50% in the amiodarone group), ve n t r i c u l a r t a c h ya r r h y t h m i a , s t r o k e s , a n d h o s p i t a l s t a y . Prophylactic amiodarone should be implemented as a routine therapy for high-risk patients undergoing cardiac surgery.129 The addition of beta-blockers can also help in reducing sympathetic triggers of AF post-operatively.130 The European Society of Cardiothoracic Surgery recommends the perioperative use of beta blockers as the first choice in all patients undergoing cardiac surgery, unless otherwise contraindicated.131
Cardiac catheterization in patients with prosthetic valves
B R U I S E C O N T R O L t r i a l , COMPARE trial and some similar t r i a l s e va l u a t e d wa r f a r i n i n patients undergoing implantation of a pacemaker or implantable c a r d i o v e r t e r – d e f i b r i l l a t o r . A s c o m p a r e d t o h e p a r i n o r d i s c o n t i n u a t i o n o f wa r f a r i n w i t h b r i d g i n g , a s t r a t e g y o f cont inued warfar in t reatment markedly reduced the incidence of clinically significant device-pocket hematoma, risk of the stroke and bleeding, and reduction of in-
hospital stay.132,133
The European Heart Rhythm A s s o c i a t i o n ( E H R A) p o s i t i o n d o c u m e n t o n a n t i t h r o m b o t i c management in patients undergoing electrophysiological procedures, recommends un-interrupted VKA in patients undergoing ablation procedures like pulmonary vein isolation ablation (PVI).134 Patients on VKS requiring implantation of cardiac implantable electronic devices should be operated on VKA unless they are a t very low risk for a thromboembolic event. In this particular case, it recommends interrupting VKA without bridging with heparin. The ACC recommends only slight modification in VKA dosing for procedures with a low bleeding risk, such as coronary angiography from the radial approach. With interventional procedures at higher risk, stopping VKA anticoagulation and using bridging therapy as is done for other surgical procedures has been recommended.21 Follow up cardiac evaluation
Doppler echocardiography at baseline (before discharge) serves as a reference for subsequent examinations. The measurements should include regional and global left and right ventricular systolic function and size, diastolic LV function (not assessable with mitral valve prosthesis) , atr ial s ize , funct ion of the nat ive valves , estimates of pulmonary artery pressure, pressure gradient across the newly implanted prosthesis, e f f e c t i ve va l va r o r i f i c e a r e a , presence of paravalvular leaks.135 The first postoperative workup should include echocardiography a long with a l l o ther physica l and blood tests.135,136 Ideally, all pat ients who have undergone valve surgery should continue to be followed-up at a cardiac center in order to detect deterioration in prosthetic function, recurrence of regurgitation following valve repair, or progression of disease at another valve site at an early stage.136 The frequency of future follow-up should be determined by the pat ient ’s progress and availability of local facilities. The frequency of echocardiography d u r i n g f o l l o w - u p s h o u l d b e
de termined by the resu l t s o f p r e v i o u s e c h o c a r d i o g r a p h y , symptomat ic s ta tus , the type of surgery , and the ex is tence of other pathology. However , ESC recommends the first post-operative visit to a hospital or a cardiac specialist within 6 weeks of discharge if there has been no period of inpatient rehabilitation or within 12 weeks if a rehabilitation program has been completed. The current 2014 ACC VHD guideline recommends annual follow up for cardiac history and physical examination in an asymptomatic uncomplicated patient . I t also recommends an echocardiographic examination at 6 weeks to 3 months after valve implantation, while AS-Echo guideline recommends a baseline TTE at discharge or 2-4 weeks after hospital discharge; as an essential component of the first post-operative visit . Both guidelines recommend further fol low up by TTE and/or TEE i f c l in ica l symptoms or s igns suggestive of prosthetic valve d y s f u n c t i o n o r o t h e r c a r d i a c pathology persist; with preference to TTE for initial examination. ACC and As-Echo recommend no further echocardiographic testing af ter the ini t ia l postoperat ive evaluation in stable mechanical valve patients and who have no symptoms or cl inical evidence of prosthetic valve or ventricular dysfunction or dysfunction of other heart valves. ACC recommend TTE after the first 10 years, while AS-Echo recommends annua l echocardiography after the first 5 years in bioprosthet ic valve patients; even in the absence of a change in clinical status.21,67
CT and MRI scan-Post valve implantation
Prosthetic cardiac valves are general ly made up of metals , polymers, and carbons. However, there is a hypothetical probability of e lectromagnetic interact ion with metal in valves that may cause interruption of opening and closing of valves (referred to as the Lenz effect). Nevertheless, no such cases have been reported in clinical practice.137 Consequently, these patients are unlikely to be at risk for valve dehiscence and the

Journal of The Association of Physicians of India ■ Vol. 66 ■ January 2018 69
heating due to MR was reported to be minor.138-141 Consequently, prosthetic heart valves, as well a s m e t a l s t e r n a l s u t u r e s a n d mediastinal clips, should not be considered as contraindications for an MRI at 3 T or less any time after implantation.142,143
According to AHA scientific s t a t e m e n t , t h e p r e s e n c e of a prosthet ic heart valve or annuloplasty ring that has been f o r m e r l y e v a l u a t e d f o r M R safety should not be considered a c o n t r a i n d i c a t i o n t o a n M R examination at 3 T or less (and possibly even 4.7 T in some cases) any time after implantation. MR examination of patients with sternal wires is generally considered to be safe and patients with endocarditis and risk of valve dehiscence cannot undergo MRI.144
Prosthetic Valve -Endocarditis
Prosthetic Valve Endocarditis (PVE) is a serious complication of cardiac valve replacement and is an important cause of morbidity and mortality. Echocardiography should be performed in all cases in which there is a medium or high clinical suspicion or when the patient is severely ill, after excluding other common causes of fever.145 The diagnostic strategy proposed by Durack and colleagues ( t he Duke c r i t e r ia ) comb ines echocardiographic findings with clinical and microbiological data. Three echocardiographic findings were considered to be major criteria for the diagnosis of endocarditis: (1) presence of vegetation defined as mobi le echo dense masses implanted in a valve or mural endocardium in the tra jectory of a regurgitant jet or implanted in prosthetic material with no alternative anatomical explanation; (2) presence of abscesses; or (3) presence of a new dehiscence of a valvular prosthesis.146
The reported sensitivity and specificity for the diagnosis of perivalvular abscesses with TTE are 28% and 98%, respectively, and wi th TEE, 87% and 95%, respectively.147-150 Bioprosthetic valve leaflets may become infected with secondary destruction of leaflet tissue. The distinction between
wear-and-tear degeneration of t issue valves and endocarditis is often difficult. TEE also led to an improved diagnostic accuracy in the diagnosis of endocarditis on bioprosthetic valves.151 TEE is therefore necessary in cases in which infective endocarditis is strongly suspected, even when no significant findings are seen on TTE.152 Further, multiple TEE planes combined with TTE views must be exploited to minimize the risk of missing a significant finding when images are technically difficult to obtain. When both TEE and TTE studies are negative, there is a 95% negative predictive value.153,154
Antimicrobial therapy remains the mainstay of therapy; however, most patients require surgical r e m o va l a n d r e p l a c e m e n t o f infected prosthesis . The delay in embol izat ion prevent ion is associated with stroke within 3 days of diagnosis.155 The risk of embolism is related to the size, and mobility of vegetation, the risk is increased in large (>10 mm) vegetation and particularly high with very mobile and large (>15 mm) vegetation. The risk of new embolism is highest during the first days following initiation of antibiotic therapy and decreases after 2 weeks.68
In a case-control study, Agarwal et al identified the risk factors for prosthetic valve endocarditis in Indian populat ion. 156 These r i s k f a c t o r s we r e f u n c t i o n a l class III or IV (New York Heart Association), alcohol consumption, pr ior h is tory of endocardi t is , fever in the intensive care unit, and gastrointest inal bleeding. Functional c lass I I I or IV and complications of the surgical wound we r e i n d e p e n d e n t p r e d i c t o r s of early infective endocarditis, whereas fever in the intensive care unit and gastrointestinal bleeding were predic tors of prosthet ic valve endocarditis late after the operation.156 However, there are no randomized studies assessing the impact of antithrombotic therapy on PVE. The results of observational s tudies sugges t tha t the r i sk of cont inuing ant icoagulat ion outweighs the benefits.155,157-160
I n p a t i e n t s o n V K A f o r a
prosthetic valve who develop IE, ACCP suggest VKA be discontinued at the time of initial presentation unt i l i t i s c lear that invas ive procedures will not be required and the patient has stabilized without signs of CNS involvement. When the patient is deemed stable without contraindications or neurologic complications, reinstitution of VKA therapy is recommended.19
Key points• Concomitant heart failure should be
managed as per standard heart failure management guidelines.
• In patients with non ST segment elevation acute coronary syndrome (NSTE-ACS) who are on anticoagulation, bare metal stent is preferred over drug eluting stent that offers the advantages of lower bleeding risk because of the potentially shorter duration of triple antithrombotic therapy.
• Beta blockers should be used for management of perioperative atrial fibrillation, unless otherwise contraindicated.
• Un-interrupted VKA can be offered in patients undergoing ablation procedures like PVI.
• Interruption of VKA should not be performed during implantation of cardiac implantable electronical devices unless patients are at very low risk of thromboembolic events. However, if required can be interrupted without bridging.
• Low bleeding risk procedures like coronary angiography by radial approach can be performed with slight modification in VKA dose. However, interventional procedures with high risk of bleeding should be performed with interruption of VKA and bridging as with other surgeries.
Follow up cardiac evaluation• The first postoperative workup should
include echocardiography along with all other physical and blood tests.
• The frequency of future follow-up should be determined by the patient’s progress and availability of local facilities.
CT and MRI scan-Post valve implantation • Patients with prosthetic valve which is
formerly evaluated for MR safety can undergo MR examination at 3T or less any time after implantation. However, patients at risk of valve dehiscence should not undergo MR examination
Prosthetic Valve -Endocarditis Diagnosis• TTE in recommended in suspected IE,
in case of negative TTE in suspected PVE, TEE is recommended. If initial examinations are negative, repetition of TTE/TEE is recommended within 7-10

Journal of The Association of Physicians of India ■ Vol. 66 ■ January 201870
days in patients with high suspicion of IE. Modified Duke Criteria should be used in evaluating a patient with suspected IE.
Prophylaxis• Antibiotic prophylaxis is recommended
in dental procedures (gingival tissue, perforation of oral mucosa), invasive respiratory tract procedures and skin tissue treatment procedures.
Antithrombotic• It is recommended to discontinue VKA,
in patients on VKA for a prosthetic valve who develop IE, until it is clear that invasive procedures will not be required and the patient has stabilized without signs of CNS involvement. When the patient is deemed stable without contraindications or neurologic complications, reinstitution of VKA therapy is recommended
Future AnticoagulantsIn the current era of expanding
strategies for anticoagulat ion, investigators have yet to establish t h e r o l e f o r n o n - V K A o r a l anticoagulants in the setting of prosthetic valve replacement. To date, there are no large randomized clinical trials enrolling to answer this question. New anticoagulants that are direct thrombin inhibitors or factor Xa inhibitors (dabigatran, apixaban, and rivaroxaban) have b e e n a p p r o ve d b y U . S . F o o d and Drug Adminis t ra t ion for an t i coag ulant prophylax i s in patients with AF not caused by VHD.161 There was no evidence of a differential effect of apixaban over VKAs in reducing stroke or systemic embolism, causing less bleeding, and reducing death in patients with and without valvular heart disease demonstrated in the ARISTOTLE tr ia l . 162 There a r e r e p o r t s o f t h r o m b o s i s o f valve despite dabigatran use.163-
166 Following this report, Food a n d D r u g A d m i n i s t r a t i o n (FDA) announced a s tatement to contraindicate dabigatran for mechanical heart valves.
A ques t ion i s unanswered , w h e t h e r t h e n o v e l o r a l a n t i c o a g u l a n t s a r e s a f e a n d e f f i c a c i o u s i n t h e p a t i e n t s early following placement of a bioprosthetic valve. Dedicated s t u d i e s i n t h i s s e t t i n g a r e unfortunately likely to be years away, thus leaving some degree of uncertainty regarding optimal
antithrombotic therapy for the near future.Disclaimer
This publication was funded by Abbott Healthcare Pvt Ltd. Dr. Vikrama Raja, Medical Affairs has authored this publication in the capacity of employee of Abbott Healthcare Pvt Ltd., Dr. Devendra Saksena, Dr. S. Muralidharan, Dr. Bipin Bihari Mohanty, Dr. C.P. Srivastava, Dr. Jagdish Mange, Dr. Manish Puranik, Dr. Manoj P Nair, Dr. Pankaj Goel, Dr. Pankaj Sr ivastava , Dr . RM Krishnan, Dr. Sathyaki Nambala, Dr. Vivek Kanhere, Dr.Yugal K Mishra have co-authorized this publication. The authors have declared and confirmed that there is no conflict of interest with respect to this authored publication.
References1. Baskett RJ, Exner DV, Hirsch GM, et al. Mitral
insufficiency and morbidity and mortality in left ventricular dysfunction. Can J Cardiol 2007; 23:797-800.
2. Iung B, Vahanian A. Epidemiology of acquired valvular heart disease. Can J Cardiol 2014; 30:962-70.
3. Howell EJ, Butcher JT. Valvular heart diseases in the developing world: Developmental biology takes center stage. J Heart Valve Dis 2012; 21:234.
4. Kumar RK, Tandon R. Rheumatic fever & rheumatic heart disease: The last 50 years. Indian J Med Res 2013; 137:643.
5. Manjunath C, Srinivas P, Ravindranath K, et al. Incidence and patterns of valvular heart disease in a tertiary care high-volume cardiac center: A single center experience. Indian Heart J 2014; 66:320-6.
6. Iung B, Baron G, Tornos P, et al. Valvular heart disease in the community : a European experience. Curr Probl Cardiol 2007; 32:609-61.
7. Singh JP, Evans JC, Levy D, et al. Prevalence and clinical determinants of mitral, tricuspid, and aortic regurgitation (the Framingham Heart Study). The Am J Cardiol 1999; 83:897-902.
8. Manji RA, Menkis AH, Ekser B, et al. The future of bioprosthetic heart valves. Indian J Med Res 2012; 135:150.
9. Isaacs AJ, Shuhaiber J, Salemi A, et al. National trends in utilization and in-hospital outcomes of mechanical versus bioprosthetic aortic valve replacements. J Thorac Cardiovasc Surg 2015; 149:1262-9.
10. Lee PH, Kilic A, Whitson B, et al. Racial and Income Disparities and Trends in the Use of Bioprosthetic Valves for Aortic Valve
Replacements. Circulation 2014; 130(Suppl 2):A15269-A.
11. Russell EA, Tran L, Baker RA, et al. A review of valve surgery for rheumatic heart disease in Australia. BMC Cardiovasc Disord 2014; 14:134.
12. Hammermeister K, Sethi GK, Henderson WG, et al. Outcomes 15 years after valve replacement with a mechanical versus a bioprosthetic valve: final report of the Veterans Affairs randomized trial. J Am Coll Cardiol 2000; 36:1152-8.
13. Cannegieter S, Rosendaal F, Briet E. T h r o m b o e m b o l i c a n d b l e e d i n g complications in patients with mechanical heart valve prostheses. Circulation 1994; 89:635-41.
14. Acar J, Iung B, Boissel JP, et al. AREVA: multicenter randomized comparison of low- dose versus standard- dose anticoagulation in patients with mechanical prosthetic heart valves. Circulation 1996; 94:2107-12.
15. Williams MA, van Riet S. The On-X heart valve: mid-term results in a poorly anticoagulated population. J Heart Valve Dis 2006; 15:80-6.
16. Puskas J, Gerdisch M, Nichols D, et al. Reduced anticoagulation after mechanical aortic valve replacement: interim results from the prospective randomized on-X valve anticoagulation clinical trial randomized Food and Drug Administration investigational device exemption trial. J Thorac Cardiovasc Surg 2014; 147:1202-11. e2.
17. Hering D, Piper C, Bergemann R, et al . Thromboembolic and bleeding complications following St. Jude Medical valve replacement: results of the German experience with low-intensity anticoagulation study. Chest J 2005; 127:53-9.
18. Torella M, Torella D, Chiodini P, et al. LO W E R i n g t h e I N t e n s i t y o f o r a l anticoaGulant Therapy in patients with bileaflet mechanical aortic valve replacement: results from the “LOWERING-IT” Trial. Am Heart J 2010; 160:171-8.
19. Whitlock RP, Sun JC, Fremes SE, et al. Antithrombotic and thrombolytic therapy for valvular disease: antithrombotic therapy and prevention of thrombosis: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest J 2012; 141(2_suppl):e576S-e600S.
20. Dhanya PS, Nidheesh C, Kuriakose KM, et al. Pattern of oral anticoagulant use following prosthetic heart valve replacement: a prospective observational study. Indian J Thorac Cardiovasc Surg 2011; 27:119-24.
21. Nishimura RA, Otto CM, Bonow RO, et al. 2014 AHA/ACC guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice

Journal of The Association of Physicians of India ■ Vol. 66 ■ January 2018 71
Guidelines. J Am Coll Cardiol 2014; 63:e57-e185.
22. Schlitt A, von Bardeleben RS, Ehrlich A, et al. Clopidogrel and aspirin in the prevention of thromboembolic complications after mechanical aortic valve replacement (CAPTA). Thromb Res 2003; 109:131-5.
23. Meschengieser SS, Fondevila CG, Frontroth J, et al. Low-intensity oral anticoagulation plus low-dose aspirin versus high-intensity oral anticoagulation alone: a randomized trial in patients with mechanical prosthetic heart valves. J Thorac Cardiovasc Surg 1997; 113:910-6.
24. Massel DR, Little SH. Antiplatelet and anticoagulation for patients with prosthetic heart valves. Cochrane Database Syst Rev 2013(7):Cd003464.
25. Cohn LH, Mudge GH, Pratter F, et al. Five to eight-year follow-up of patients u n d e r g o i n g p o r c i n e h e a r t - v a l v e replacement. N Engl J Med 1981; 304:258.
26. Heras M, Chesebro JH, Fuster V, et al. High risk of thromboemboli early after bioprosthetic cardiac valve replacement. J Am Coll Cardiol 1995; 25:1111-9.
27. Durães AR, Durães MA, Correia LC, et al. Antithrombotic strategy in the three first months following bioprosthetic heart valve implantation. Arq Bras Cardiol 2013; 101:466-72.
28. El-Husseiny M, Salhiyyah K, Raja SG, et al. Should warfarin be routinely prescribed for the first three months after a bioprosthetic valve replacement? Interact Cardiovasc Thorac Surg 2006; 5:616-23.
29. Sundt T, Zehr K, Dearani J, et al. Is early anticoagulation with warfarin necessary after bioprosthetic aortic valve replacement? J Thorac Cardiovasc Surg 2005; 129:1024-31.
30. Mérie C, Køber L, Olsen PS, et al. Association of war farin therapy duration after bioprosthetic aortic valve replacement with risk of mortality, thromboembolic complications, and bleeding. JAMA 2012; 308:2118-25.
31. Al-Atassi T, Lam K, Forgie M, et al. Cerebral Microembolization After Bioprosthetic Aortic Valve Replacement Comparison of Warfarin Plus Aspirin Versus Aspirin Only. Circulation 2012; 126(11 suppl 1):S239-S44.
32. Brennan JM, Edwards FH, Zhao Y, et al. Early anticoagulation of bioprosthetic aortic valves in older patients: results from the Society of Thoracic Surgeons Adult Cardiac Surgery National Database. J Am Coll Cardiol 2012; 60:971-7.
33. Mandiye SS, Agarwal S, Pratap H, et al. Comparison over short term of mortality and morbidity of mechanical and bioprosthetic heart valves in the Indian population. Indian J Thorac Cardiovasc Surg 2010; 26:139-43.
34. Agarwal S, Gupta S, Minhas HS, et al. Comparison of outcomes after mitral valve
replacement with a mechanical versus a bioprosthetic valve in patients between forty and sixty years of age. Indian J Thorac Cardiovasc Surg 2009; 25:12-7.
35. Talwar S, Sharma AK, Kumar AS. Tissue heart valve implantation in India; Indications, results and impact on quality of life. Indian J Thorac Cardiovasc Surg 2008; 24:10-4.
36. Smith CR, Leon MB, Mack MJ, et al. Transcatheter versus surgical aortic-valve replacement in high-risk patients. New England Journal of Medicine 2011; 364:2187-98.
37. Leon MB, Smith CR, Mack M, et al. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. New England Journal of Medicine 2010; 363:1597-607.
38. Kahlert P, Al-Rashid F, Döttger P, et a l . Cerebra l embol izat ion du r ing transcatheter aortic valve implantation: a transcranial Doppler study. Circulation. 2012:CIRCULATIONAHA. 112.092544.
39. Tay EL, Gurvitch R, Wijesinghe N, et al. A high-risk period for cerebrovascular events exists after transcatheter aortic valve implantation. JACC: Cardiovascular Interventions 2011; 4:1290-7.
40. Poliacikova P, Cockburn J, de Belder A, et al. Antiplatelet and antithrombotic treatment after transcatheter aortic valve implantation-comparison of regimes. The Journal of Invasive Cardiology 2013; 25:544-8.
41. Tamburino C, Capodanno D, Ramondo A, et al. Incidence and predictors of early and late mortality after transcatheter aortic valve implantation in 663 patients with severe aortic stenosis. Circulation 2011; 123:299-308.
42. Seth A, Rastogi V, Kumar V, et al . Transcatheter aortic valve implantation with Core Valve: First Indian experience of three high surgical risk patients with severe aortic stenosis. Indian Heart J 2013; 65:395-9.
43. Maqbool S, Kumar V, Rastogi V, et al. Transcatheter aortic valve implantation under conscious sedation - the first Indian experience. Indian Heart J 2014; 66:208-10.
44. Tinker JH, Tarhan S. Discontinuing anticoagulant therapy in surgical patients with cardiac valve prostheses. Observations in 180 operations. JAMA 1978; 239:738-9.
45. Bajkin BV, Popovic SL, Selakovic SD. Randomized, prospective trial comparing bridging therapy using low-molecular-weight heparin with maintenance of oral anticoagulation during extraction of teeth. J Oral Maxillofac Surg 2009; 67:990-5.
46. Evans IL, Sayers MS, Gibbons AJ, et al. Can warfarin be continued during dental extraction? Results of a randomized controlled trial. Br J Oral Maxillofac Surg 2002; 40:248-52.
47. Sacco R, Sacco M, Carpenedo M, et al. Oral
surgery in patients on oral anticoagulant therapy: a randomized comparison of different INR targets. J Thromb Haemost 2006; 4:688-9.
48. Al-Belasy FA, Amer MZ. Hemostatic effect of n-butyl-2-cyanoacrylate (histoacryl) glue in warfarin-treated patients undergoing oral surgery. J Oral Maxillofac Surg 2003; 61:1405-9.
49. Car ter G, Goss A. Tranexamic acid mouthwash--a prospective randomized study of a 2-day regimen vs 5-day regimen to prevent postoperative bleeding in anticoagulated patients requiring dental extractions. Int J Oral Maxillofac Surg 2003; 32:504-7.
50. Carter G, Goss A, Lloyd J, et al. Tranexamic acid mouthwash versus autologous fibrin glue in patients taking warfarin undergoing dental ex trac t ions : a randomized prospective clinical study. J Oral Maxillofac Surg 2003; 61:1432-5.
51. Alcalay J. Cutaneous surgery in patients receiving warfarin therapy. Dermatol Surg 2001; 27:756-8.
52. Kargi E, Babuccu O, Hosnuter M, et al. Complications of minor cutaneous surgery in patients under anticoagulant treatment. Aesthetic Plast Surg 2002; 26:483-5.
53. Syed S, Adams BB, Liao W, et al. A prospective assessment of bleeding and international normalized ratio in warfarin-anticoagulated patients having cutaneous surgery. J Am Acad Dermatol 2004; 51:955-7.
54. Jamula E, Anderson J, Douketis JD. Safety of continuing warfarin therapy during cataract surgery: a systematic review and meta-analysis. Thromb Res 2009; 124:292-9.
55. Spyropoulos AC1 TA, Dunn AS, Kaatz S, et al. Investigators. R. Perioperative bridging therapy with unfractionated heparin or low-molecular weight heparin in patients with mechanical prosthetic heart valves on long-term oral anticoagulants (from the REGIMEN Registry). Am J Cardiol 2008; 102:883-9.
56. Douketis JD, Spyropoulos AC, Spencer FA, et al. Perioperative management of antithrombotic therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 2012; 141(2 Suppl):e326S-50S.
57. Pengo V, Cucchini U, Denas G, et al. Standardized low-molecular-weight heparin bridging regimen in outpatients on oral anticoagulants undergoing invasive procedure or surgery: an inception cohort management study. Circulation 2009; 119:2920-7.
58. Malato A, Saccullo G, Lo Coco L, et al. Patients requiring interruption of long-term oral anticoagulant therapy: the use of fixed sub-therapeutic doses of low-molecular-weight heparin. J Thromb

Journal of The Association of Physicians of India ■ Vol. 66 ■ January 201872
Haemost 2010; 8:107-13.
59. Singer DE, Hellkamp AS, Piccini JP, et al. Impact of global geographic region on time in therapeutic range on warfarin anticoagulant therapy: data from the ROCKET AF clinical trial. J Am Heart Assoc 2013;2-e000067, Available online, doi: 10.1161/JAHA.112.000067.
60. Caldeira D, Cruz I, Morgado G, et al. Evaluation of time in therapeutic range in anticoagulated patients: a single-center, retrospective, observational study. BMC Res Notes 2014; 7-891, Available online,doi:10.1186/1756-0500-7-891.
61. KIM YK, Nieuwlaat R, Connolly S, et al. Effect of a simple two‐step warfarin dosing algorithm on anticoagulant control as measured by time in therapeutic range: a pilot study. J Thromb Haemost 2010; 8:101-6.
62. Phi l l ips K W, Ansel l J . O utpat ient management of oral vitamin K antagonist therapy: defining and measuring high-quality management. Expert Rev Cardiovasc Ther 2008; 6:57-70.
63. Connock M, Stevens C, Fry-Smith A, et al. Clinical effectiveness and cost-effectiveness of different models of managing long-term oral anticoagulation therapy: a systematic review and economic modelling. Health Technol Assess 2007; 11(38, Available online, http://dx.doi.org/10.3310/hta11380).
64. Kong MC, Lim TG, Ng HJ, et al. Feasibility, cost-effectiveness and patients’ acceptance of point-of-care INR testing in a hospital-based anticoagulation clinic. Ann Hematol 2008; 87:905-10.
65. Xu Z, Wang Z, Ou J, et al. Two monitoring methods of oral anticoagulant therapy in patients with mechanical heart valve prothesis: a meta-analysis. J Thromb Thrombolysis 2012; 33:38-47.
66. Nagler M, Bachmann LM, Schmid P, et al. Patient self-management of oral anticoagulation with vitamin K antagonists in everyday practice: efficacy and safety in a nationwide long-term prospective cohort study. PloS one 2014; 9: e95761, Available online.
67. Zoghbi WA, Chambers JB, Dumesnil JG, et al. Recommendations for evaluation of prosthetic valves with echocardiography and doppler ultrasound: a report From the American Society of Echocardiography’s Guidelines and Standards Committee and the Task Force on Prosthetic Valves, developed in conjunction with the American College of Cardiology Cardiovascular Imaging Committee, Cardiac Imaging Committee of the American Heart Association, the European Association of Echocardiography, a registered branch of the European Society of Cardiology, the Japanese Society of Echocardiography and the Canadian Society of Echocardiography, endorsed by the American College of Cardiology Foundation, American Heart
Association, European Association of Echocardiography, a registered branch of the European Society of Cardiology, the Japanese Society of Echocardiography, and Canadian Society of Echocardiography. J Am Soc Echocardiogr 2009; 22:975-1014.
68. Pepi M, Evangelista A, Nihoyannopoulos P, e t a l . R e c o m m e n d a t i o n s f o r echocardiography use in the diagnosis and management of cardiac sources of embolism. Eur Heart J Cardiovasc Imaging 2010; 11:461-76.
69. Huber KC, Gersh BJ, Bailey KR, et al. Variability in anticoagulation control p re d i c t s t h ro m b o e m b o l i s m a f te r mechanical cardiac valve replacement: a 23-year population-based study. Mayo Clin Proc 1997; 72:1103-10.
70. Lalonde L, Martineau J, Blais N, et al. Is long-term pharmacist-managed anticoagulation service efficient? A pragmatic randomized controlled trial. Am Heart J 2008; 156:148-54.
71. Locke C, Ravnan SL, Patel R, et al. Reduction in warfarin adverse events requiring patient hospitalization after implementation of a pharmacist-managed anticoagulation service. Pharmacotherapy 2005; 25:685-9.
72. Kagansky N, Knobler H, Rimon E, et al. Safety of anticoagulation therapy in well-informed older patients. Arch Intern Med 2004; 164:2044-50.
73. Tang EO, Lai CS, Lee KK, et al. Relationship between patients’ warfarin knowledge and anticoagulation control. Ann Pharmacother 2003; 37:34-9.
74. Zeolla MM, Brodeur MR, Dominelli A, et al. Development and validation of an instrument to determine patient knowledge: the oral anticoagulation knowledge test. Ann Pharmacother 2006; 40:633-8.
75. Kneeland PP, Fang MC. Current issues in patient adherence and persistence: focus on anticoagulants for the treatment and prevention of thromboembolism. Patient Prefer Adherence 2010; 4:51-60.
76. Karthikeyan G, Math RS, Mathew N, et al. Accelerated Infusion of Streptokinase for the Treatment of Left-Sided Prosthetic Valve Thrombosis: A Randomized Controlled Trial. Circulation 2009; 120:1108-14.
77. Talwar S, Kapoor CK, Velayoudam D, et al. Anticoagulation protocol and early prosthetic valve thrombosis. Indian Heart J 2003; 56:225-8.
78. Roudaut R, Serri K, Lafitte S. Thrombosis of prosthetic heart valves: diagnosis and therapeutic considerations. Heart 2007; 93:137-42.
79. Barbetseas J, Nagueh SF, Pitsavos C, et al. Differentiating thrombus from pannus formation in obstructed mechanical prosthetic valves: an evaluation of clinical, transthoracic and transesophageal echocardiographic parameters. J Am Coll
Cardiol 1998; 32:1410-7.
80. Tong AT, Roudaut R, Özkan M, et al. Transesophageal echocardiography improves risk assessment of thrombolysis of prosthetic valve thrombosis: results of the international PRO-TEE registry. J Am Coll Cardiol 2004; 43:77-84.
81. Deviri E, Sareli P, Wisenbaugh T, et al. Obstruction of mechanical heart valve prostheses: Clinical aspects and surgical management. J Am Coll Cardiol 1991; 17:646-50.
82. Roudaut R, Lafitte S, Roudaut M-F, et al. Management of prosthetic heart valve obstruction: Fibrinolysis versus surgery. Early results and long-term follow-up in a single-centre study of 263 cases. Arch Cardiovasc Dis 2009; 102:269-77.
83. Keuleers S, Herijgers P, Herregods M-C, et al. Comparison of thrombolysis versus surgery as a first line therapy for prosthetic heart valve thrombosis. J Am Coll Cardiol 2011; 107:275-9.
84. Cáceres-Lóriga FM, Pérez-López H, Morlans-Hernández K, et al. Thrombolysis as first choice therapy in prosthetic heart valve thrombosis. A study of 68 patients. J Thromb Thrombolysis 2006; 21:185-90.
85. Panduranga P, Al-Mukhaini M, Al-Muslahi M, et al. Management dilemmas in patients with mechanical heart valves and warfarin-induced major bleeding. World J Cardiol 2012; 4:54-9.
86. Phan TG, Koh M, Wijdicks EF. Safety of discontinuation of anticoagulation in patients with intracranial hemorrhage at high thromboembolic risk. Arch Neurol 2000; 57:1710-3.
87. L i m d i N A , Ve e n s t ra D L . Wa r f a r i n pharmacogenetics. Pharmacotherapy 2008; 28:1084-97.
88. Shalia KK, Doshi SM, Parikh S, et al. Prevalence of VKORC1 and CYP2C9 gene polymorphisms in Indian population and its effect on warfarin response. J Assoc Physicians India 2012; 60:34-8.
89. Rathore S, Agarwal S, Pande S, et al. The impact of VKORC1-1639 G> A polymorphism on the maintenance dose of oral anticoagulants for thromboembolic prophylaxis in North India: A pilot study. Indian J Hum Genet 2011; 17(Suppl 1):S54-S7.
90. Kumar DK, Shewade DG, Manjunath S, et al. Inter and intra ethnic variation of vitamin K epoxide reductase complex and cytochrome P450 4F2 genetic polymorphisms and their prevalence in South Indian population. Indian J Hum Genet 2013; 19:301.
91. Lee MTM, Chen C-H, Chuang H-P, et al. VKORC1 haplotypes in five East-A s i a n p o p u l a t i o n s a n d I n d i a n s . Pharmacogenomics 2009; 10:1609-16.
92. Gaikwad T, Ghosh K, Kulkarni B, et al. Influence of CYP2C9 and VKORC1 gene

Journal of The Association of Physicians of India ■ Vol. 66 ■ January 2018 73
polymorphisms on warfarin dosage, over anticoagulation and other adverse outcomes in Indian population. Eur J Pharmaco 2013; 710:80-4.
93. Holbrook A, Schulman S, Witt DM, et al. Evidence-based management of anticoagulant therapy: antithrombotic therapy and prevention of thrombosis: American College of Chest Physicians evidence-based clinical practice guidelines. Chest J 2012; 141(2_suppl):e152S-e84S.
94. Bajaj R, Karthikeyan G, Sinha N, et al. CSI consensus statement on prosthetic valve follow up. Indian Heart J 2012; 64(Suppl 2):S3-S11.
95. Bungard TJ, Yakiwchuk E, Foisy M, et al. Drug interactions involving warfarin: practice tool and practical management tips. Can Pharm J (Ott) 2011; 144:21-5.
96. Mahe I, Bertrand N, Drouet L, et al. Interaction between paracetamol and warfarin in patients: a double-blind, placebo-controlled, randomized study. Haematologica 2006; 91:1621-7.
97. Pinson GM, Beall JW, Kyle JA. A review of warfarin dosing with concurrent acetaminophen therapy. J Pharm Pract 2013; 26:518-21.
98. Zhang Q, Bal-dit-Sollier C, Drouet L, et al. Interaction between acetaminophen and warfarin in adults receiving long-term oral anticoagulants: a randomized controlled trial. Eur J Clin Pharmacol 2011; 67:309-14.
99. Penning-van Beest FJ, Koerselman J, Herings RM. Quantity and quality of potential drug interactions with coumarin anticoagulants in the Netherlands. Pharmacy World & Science 2007; 29:671-5.
100. Milić N, Milosević N, Golocorbin KS, et al. Warfarin interactions with medicinal herbs. Nat Prod Commun 2014; 9:1211-6.
101. Ge B, Zhang Z, Zuo Z, et al. Updates o n t h e C l i n i c a l Ev i d e n ce d H e r b -Warfarin Interactions. Evidence-Based Complementary and Alternative Medicine 2014; 20142014.
102. de Assis MC, Rabelo ER, Ávila CW, et al. Improved Oral Anticoagulation After a Dietary Vitamin K–Guided Strategy A Randomized Controlled Trial. Circulation 2009; 120:1115-22.
103. Franco V, Polanczyk CA, Clausell N, et al. Role of dietary vitamin K intake in chronic oral anticoagulation: prospective evidence from observational and randomized protocols. The Am J Med 2004; 116:651-6.
104. Davis GL. Hemostatic changes associated with normal and abnormal pregnancies. Clin Lab Sci 2000; 13:223-8.
105. Brooks C, Rutherford JM, Gould J, et al. Warfarin dosage in postpartum women: a case-control study. BJOG 2002; 109:187-90.
106. Lebaudy C, Hulot JS, Amoura Z, et al. Changes in enoxaparin pharmacokinetics during pregnancy and implications for antithrombotic therapeutic strategy. Clin
Pharmacol Ther 2008; 84:370-7.
107. Srivastava AR, Modi P, Sahi S, et al. Anticoagulation for pregnant patients with mechanical heart valves. Ann Card Anaesth 2007; 10:95-107.
108. Cotrufo M, De Feo M, De Santo LS, et al. Risk of warfarin during pregnancy with mechanical valve prostheses. Obstet Gynecol 2002; 99:35-40.
109. Hassouna A, Allam H. Limited dose warfarin throughout pregnancy in patients with mechanical heart valve prosthesis: a meta-analysis. Interact Cardiovasc Thorac Surg 2014; 18:797-806.
110. Vitale N, De Feo M, De Santo LS, et al. Dose-dependent fetal complications of warfarin in pregnant women with mechanical heart valves. J Am Coll Cardiol 1999; 33:1637-41.
111. C h a n W S , An a n d S , G i n s b e rg J S . Anticoagulation of pregnant women with mechanical heart valves: a systematic review of the literature. Archives of Internal Medicine 2000; 160:191-6.
112. Gopalakrishnan S, Narayanan S. Oral anticoagulants: Current Indian scenario. Med update: The Association of Physicians of India 2013; 410-3.
113. Bates SM, Greer IA, Middeldorp S, et al. VTE, thrombophilia, antithrombotic therapy, and pregnancy: antithrombotic therapy and prevention of thrombosis: American College of Chest Physicians evidence-based clinical practice guidelines. Chest J 2012; 141(2_suppl):e691S-e736S.
114. Vahanian A, Alfieri O, Andreotti F, et al. Guidelines on the management of valvular heart disease (version 2012). Eur Heart J 2012; 33:2451-96.
115. Grand’Maison A, Charest AF, Geerts WH. Anticoagulant use in patients with chronic renal impairment. Am J Cardiovasc Drugs 2005; 5:291-305.
116. Robert-Ebadi H, Le Gal G, Righini M. Use of anticoagulants in elderly patients: practical recommendations. Clin Interv Aging 2009; 4:165.
117. Dhond AJ, Michelena HI, Ezekowitz MD. Anticoagulation in the elderly. Am J Geriatr Cardiol 2003; 12:243-50.
118. Andreotti F, Rocca B, Husted S, et al. Antithrombotic therapy in the elderly: expert position paper of the European Society of Cardiology Working Group on Thrombosis. European Heart Journal 2015:ehv304.
119. Mahe I, Gouin-Thibault I, Drouet L, et al. Elderly medical patients treated with prophylactic dosages of enoxaparin. Drugs & Aging 2007; 24:63-71.
120. Kulkarni N, Gukathasan N, Sartori S, et al. Chronic Kidney Disease and Atrial Fibrillation: A Contemporary Overview. J Atr Fibrillation 2012; 2:62-70.
121. Wigle P, Hein B, Bloomfield HE, et al. Updated guidelines on outpatient
anticoagulation. Am Fam Physician 2013; 87:556-66.
122. Hunt SA, Abraham WT, Chin MH, et al. 2009 Focused update incorporated into the ACC/AHA 2005 Guidelines for the Diagnosis and Management of Heart Failure in Adults A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines Developed in Collaboration With the International Society for Heart and Lung Transplantation. J Am Coll Cardiol 2009; 53:e1-e90.
123. Sourgounis A, Lipiecki J, Lo TS, et al. Coronary Stents and Chronic Anticoagulation 2009.
124. Dewilde WJ, Oirbans T, Verheugt FW, et al. Use of clopidogrel with or without aspirin in patients taking oral anticoagulant therapy and undergoing percutaneous coronary intervention: an open-label, randomised, controlled trial. Lancet 2013; 381:1107-15.
125. Amsterdam EA, Wenger NK, Brindis RG, et al. 2014 AHA/ACC Guideline for the Management of Patients With Non–ST-Elevation Acute Coronary Syndromes. J Am Coll Cardiol 2014; 64:e139-e228.
126. Alqahtani AAR. Atr ia l Fibr i l lat ion Post Cardiac Surgery Trends Toward Management. Heart Views 2010; 11:57-63.
127. Filardo G, Hamilton C, Hamman B, et al. New-onset postoperative atrial fibrillation and long-term survival after aortic valve replacement surgery. Ann Thorac Surg 2010; 90:474-9.
128. Mitchell LB, Exner DV, Wyse DG, et al. Prophylactic Oral Amiodarone for the Prevention of Arrhythmias that Begin Early After Revascularization, Valve Replacement, or Repair: PAPABEAR: a randomized controlled trial. JAMA 2005; 294:3093-100.
129. Bagshaw SM, Galbraith PD, Mitchell LB, et al. Prophylactic amiodarone for prevention of atrial fibrillation after cardiac surgery: a meta-analysis. Ann Thorac Surg 2006; 82:1927-37.
130. Auer J, Weber T, Berent R, et al. A comparison between oral antiarrhythmic drugs in the prevention of atrial fibrillation after cardiac surgery: the pilot study of prevention of postoperative atrial fibrillation (SPPAF), a randomized, placebo-controlled trial. Am Heart J 2004; 147:636-43.
131. Dunning J, Treasure T, Versteegh M, et al. Guidelines on the prevention and management of de novo atrial fibrillation after cardiac and thoracic surgery. Eur J Cardiothorac Surg 2006; 30:852-72.
132. Birnie DH, Healey JS, Wells GA, et al. Pacemaker or Defibril lator Surgery without Interruption of Anticoagulation. New England Journal of Medicine 2013; 368:2084-93.
133. Tolosana JM, Berne P, Mont L, et al. Preparation for pacemaker or implantable

Journal of The Association of Physicians of India ■ Vol. 66 ■ January 201874
cardiac defibrillator implants in patients with high risk of thrombo-embolic events: oral anticoagulation or bridging with intravenous heparin? A prospective randomized trial. Eur Heart J 2009; 30:1880.
134. Sticherling C, Marin F, Birnie D, et al. Antithrombotic management in patients u n d e r g o i n g e l e c t r o p hy s i o l o g i c a l procedures: a European Heart Rhythm Association (EHRA) position document endorsed by the ESC Working Group Thrombosis, Heart Rhythm Society (HRS), and Asia Pacific Heart Rhythm Society (APHRS). Europace 2015; 17:1197-214.
135. Seiler C. Management and follow up of prosthetic heart valves. Heart 2004; 90:818-24.
136. Butchart EG, Gohlke-Bärwolf C, Antunes MJ, et al. Recommendations for the management of patients after heart valve surgery. European Heart Journal 2005; 26:2463-71.
137. Condon B, Hadley DM. Potential MR hazard to patients with metallic heart valves: the Lenz effect. J Magn Reson Imaging 2000; 12:171-6.
138. Shellock FG, Morisoli SM. Ex vivo evaluation of ferromagnetism, heating, and artifacts produced by heart valve prostheses exposed to a 1.5-T MR system. J Magn Reson Imaging 1994; 4:756-8.
139. Edwards MB, Taylor KM, Shellock FG. Prosthetic heart valves: evaluation of magnetic field interactions, heating, and artifacts at 1.5 T. J Magn Reson Imaging 2000; 12:363-9.
140. Shellock FG. Prosthetic heart valves and annuloplasty rings: assessment of magnetic field interactions, heating, and artifacts at 1.5 Tesla. J Cardiovasc Magn Reson 2001; 3:317-24.
141. Pruefer D, Kalden P, Schreiber W, et al. In vitro investigation of prosthetic heart valves in magnetic resonance imaging: evaluation of potential hazards. J Heart Valve Dis 2001; 10:410-4.
142. B a i k o u s s i s N G , A p o s t o l a k i s E , Papakonstantinou NA, et al. Safety of magnetic resonance imaging in patients with implanted cardiac prostheses and metallic cardiovascular electronic devices. Annals Thoracic Surg 2011; 91:2006-11.
143. Dill T. Contraindications to magnetic resonance imaging. Heart 2008; 94:943-8.
144. Levine GN, Gomes AS, Arai AE, et al. Safety of Magnetic Resonance Imaging in Patients With Cardiovascular Devices An American Heart Association Scientific Statement From the Committee on Diagnostic and Interventional Cardiac Catheterization, Council on Clinical Cardiology, and the Council on Cardiovascular Radiology and Intervention: Endorsed by the American College of Cardiology Foundation, the North American Society for Cardiac Imaging, and the Society for Cardiovascular Magnetic Resonance. Circulation 2007;
116:2878-91.
145. Evangelista A, Gonzalez-Alujas MT. Echocardiography in infective endocarditis. Heart 2004; 90:614-7.
146. Durack DT, Lukes AS, Bright DK. New criteria for diagnosis of infective endocarditis: utilization of specific echocardiographic findings. Duke Endocarditis Service. Am J Med 1994; 96:200-9.
147. Birmingham GD, Rahko PS, Ballantyne F, 3rd. Improved detection of infective endocarditis with transesophageal echocardiography. Am Heart J 1992; 123:774-81.
148. Daniel WG, Mugge A, Grote J, et al. Compar ison of t ransthoracic and transesophageal echocardiography for detection of abnormalities of prosthetic and bioprosthetic valves in the mitral and aortic positions. Am J Cardiol 1993; 71:210-5.
149. Karalis DG, Bansal RC, Hauck AJ, et al. Transesophageal echocardiographic recognition of subaortic complications in aortic valve endocarditis. Clinical and surgical implications. Circulation 1992; 86:353-62.
150. Rozich JD, Edwards WD, Hanna RD, et al. Mechanical prosthetic valve-associated st rands : Pathologic cor re lates to transesophageal echocardiography. J Am Soc Echocardiogr 2003; 16:97-100.
151. Lengyel M. The impact of transesophageal echocardiography on the management of prosthetic valve endocarditis: experience of 31 cases and review of the literature. J Heart Valve Dis 1997; 6:204-11.
152. Lowry RW, Zoghbi WA, Baker WB, et al. Clinical impact of transesophageal echocardiography in the diagnosis and management of infective endocarditis. Am J Cardiol 1994; 73:1089-91.
153. Ali AS, Trivedi V, Lesch M. Culture-negative endocarditis--a historical review and 1990s update. Prog Cardiovasc Dis 1994; 37:149-60.
154. Bayer AS. Infective endocarditis. Clin Infect Dis. 1993;17(3):313-20; quiz 21-2.
155. Davenport J, Hart RG. Prosthetic valve endocarditis 1976-1987. Antibiotics, anticoagulation, and stroke. Stroke 1990; 21:993-9.
156. Agarwal S, Rawtani S, Geelani MA, et al. Risk factors for prosthetic valve endocarditis—A case control study. Indian J Thorac Cardiovasc Surg 2009; 25:102-6.
157. Vilacosta I, Graupner C, San Roman JA, et al. Risk of embolization after institution of antibiotic therapy for infective endocarditis. J Am Coll Cardiol 2002; 39:1489-95.
158. Lieberman A, Hass WK, Pinto R, et al. Intracranial hemorrhage and infarction in anticoagulated patients with prosthetic heart valves. Stroke 1978; 9:18-24.
159. Masur H, Johnson WD, Jr. Prosthetic valve
endocarditis. J Thorac Cardiovasc Surg 1980; 80:31-7.
160. Wilson WR, Geraci JE, Danielson GK, et al. Anticoagulant therapy and central nervous system complications in patients with prosthetic valve endocarditis. Circulation 1978; 57:1004-7.
161. Ellis F. Unger UF. Atrial fibrillation and new oral anticoagulant drugs: U.S. Food and Drug Administartion; [updated July 7 2014. Available from: http://www.fda.gov/Drugs/NewsEvents/ucm405148.htm.
162. Avezum A, Lopes RD, Schulte PJ, et al. Apixaban Compared with Warfarin in Patients With Atrial Fibrillation and Valvular Heart Disease: Findings From the ARISTOTLE Trial. Circulation 2015:Published online before pr int. doi : 10.1161/CIRCULATIONAHA.114.014807.
163. Eikelboom JW, Connolly SJ, Brueckmann M, et al. Dabigatran versus warfarin in patients with mechanical heart valves. New England J Med 2013; 369:1206-14.
164. Chu JW, Chen VH, Bunton R. Thrombosis of a mechanical heart valve despite dabigatran. Annals Int Med 2012;157(4).
165. Price J, Hynes M, Labinaz M, et al. Mechanical valve thrombosis with dabigatran. J Am Coll Cardiol 2012; 60:1710-1.
166. Stewart RA, Astell H, Young L, et al. Thrombosis on a mechanical aortic valve whilst anti-coagulated with dabigatran. Heart Lung Circ 2012; 21:53-5.
167. Holmes DR, Mack MJ, Kaul S, et al. 2012 ACCF/AATS/SCAI/STS expert consensus document on transcatheter aortic valve replacement. J Am Coll Cardiol 2012; 59:1200-54.
168. Webb J, Rodés-Cabau J, Fremes S, et al. Transcatheter aortic valve implantation: a Canadian Cardiovascular Society position statement. Canadian J Cardiol 2012; 28:520-8.
169. Beyth RJ, Quinn LM, Landefeld CS. Prospective evaluation of an index for predicting the risk of major bleeding in outpatients treated with warfarin. Am J Med 1998; 105:91-9.
170. Shireman TI, Mahnken JD, Howard PA, et al. Development of a contemporary bleeding risk model for elderly warfarin recipients. Chest J 2006; 130:1390-6.
171. Lip GY, Frison L, Halperin JL, et al. Comparative validation of a novel risk score for predicting bleeding risk in anticoagulated patients with atrial fibrillation: the HAS-BLED (Hypertension, Abnormal Renal/Liver Function, Stroke, Bleeding History or Predisposition, Labile INR, Elderly, Drugs/Alcohol Concomitantly) score. J Am Coll Cardiol 2011; 57:173-80.
172. Gage BF, Yan Y, Milligan PE, et al. Clinical classification schemes for predicting hemorrhage: results from the National Registry of Atrial Fibrillation (NRAF). Am Heart J 2006; 151:713-9.