Embed Size (px)
Citation preview
UNIVERSITÉ DE MODÈNE ET REGGIO EMILIE - ITALIE
DÉPARTEMENT DE CHIRURGIE GÉNÉRALE ET SPÉCIALITÉS CHIRURGICALES
Directeur: Prof. Massimo Saviano
UNIVERSITÉ DE MODÈNE ET REGGIO EMILIA - ITALIE
Massimo SavianoIASI 2009
LA THYROÏDECTOMIE TOTALE DANS LE TRAITEMENT DE LA PATHOLOGIE BÉNIGNE
LA THYROLA THYROÏÏDECTOMIE TOTALE DANS LE DECTOMIE TOTALE DANS LE TRAITEMENT DE LA PATHOLOGIE BTRAITEMENT DE LA PATHOLOGIE BÉÉNIGNENIGNE
DÉPARTEMENT DE CHIRURGIE GÉNÉRALE ET SPÉCIALITÉS CHIRURGICALES
Directeur: Prof. Massimo Saviano
TOTAL THYROIDECTOMY IN THE TREATMENT OF BENIGN PATHOLOGY (ABSTRACT): Total thyroidectomy or subtotal thyroidectomy performed in benign pathology of thyroid? Methods: To answer this question we performed a retrospective study on 1103 cases with this pathology: 1082 cases first intervention and 51 cases for relapse pathology. Preoperative diagnosis included: evaluation of the functionality of the thyroid by lab tests, endocrinology exam, ORL exam, anhéstesiologique exam, chest radiograph, CT/MRI neck and thorax, ultrasound, scintigraphy, fine-needle aspiration cytologic diagnoses. Results: Preoperative diagnosis was multinodular goiter (1040 cs.) and Basedow (63 cs.) and surgical procedures performed were total thyroidectomy in 865 cs and subtotal thyroidectomy in 238 cs. In 92 cs were diving goiter and in 157 patients were diagnosed with large nodular goiter (>100 gr). The surgery made by 123 patients with thyroid carcinoma and 980 patients with benign pathology. Mean postoperative hospital stay was 2.5 days. In the group of 1032 patients without preoperative suspicion of neoplasia(cytology not performed preoperatively or negative) hidden carcinomas were 11.7% (121 patients) what requiring 11 surgical reinterventions for radicalization of subtotal thyroidectomy. In the group of 71 patients with preoperative suspicion of neoplasia by fine-needle aspiration papillary carcinoma were 2.8%, the rest being benign thyroid pathology. In the postoperative complications, recurrent nerve lesions were encountered in 78 cs (3.76% of 2206 nerves at risk). Bilateral paralysis immediate was encountered in 5 cs (0.4%): 2 cs after total thyroidectomy and 3 cs after subtotal thyroidectomy with permanent bilateral paralysis in all cases. The immediate unilateral paralysis was encountered in 73 patients, (6.6%/3.3% nerves): 40 cs (4.6%) after total thyroidectomy and 33 cs (13.8%) after subtotal thyroidectomy (p <0.0001). But permanent unilateral paralysis was recorded in 16 patients (1.4%/0.7% nerves): 9 cs (1.0%/0.5% nerves) after total thyroidectomy and 7 (2.9%/1.4% nerves) after subtotal thyroidectomy with insignificant p 0.030. Postoperative hypocalcemia secondary lesions of parathyroid glands was recorded in 222 patients. The permanent hypocalcemia was encountered in 52 cs (6%) after total thyroidectomy and 14 cs (5.8%) after subtotal thyroidectomy with insignificant p 0.8311. Conclusions: The incidence of recurrent nerve lesions, not higher even than in the total thyroidectomy versus subtotal thyroidectomy. The incidence of residual permanent hypoparathyroidism superimposable between the two techniques. The high incidence of carcinomas hidden above the 11% we can state that total thyroidectomy is considered the gold standard for benign bilateral thyroid guaranteeing radical surgery and the almost total disappearance of the risk of recurrence.
KEY WORDS: BENIGN PATHOLOGY OF THYROID, HIDDEN CARCINOMAS, MULTINODULAR GOITER, TOTAL THYROIDECTOMY, RECURRENT NERVE LESIONS, POSTOPERATIVE HYPOCALCEMIA
Correspondence to: Prof. Massimo Saviano MD PhD, Department of General Surgery and Other Surgical Specialties, University of Modena and Reggio Emilia Italy, Via Del Pozzo 71, 41100 Modena, Italy, e-mail: [email protected]
This presentation was exposed at the 15th Symposion Francophone d'Endocrinologie, Iasi, Romania, 6-8 May 2009
THYROÏDECTOMIE TOTALE OU THYROÏDECTOMIE SUBTOTALE DANS LA PATHOLOGIE BÉNIGNE BILATÉRALE ?
THYROTHYROÏÏDECTOMIE TOTALE OU THYRODECTOMIE TOTALE OU THYROÏÏDECTOMIE SUBTOTALE DECTOMIE SUBTOTALE DANS LA PATHOLOGIE BDANS LA PATHOLOGIE BÉÉNIGNE BILATNIGNE BILATÉÉRALE RALE ??
THYROÏDECTOMIE TOTALE OU THYROÏDECTOMIE SUBTOTALE DANS LA PATHOLOGIE BÉNIGNE BILATÉRALE ?
THYROTHYROÏÏDECTOMIE TOTALE OU THYRODECTOMIE TOTALE OU THYROÏÏDECTOMIE SUBTOTALE DECTOMIE SUBTOTALE DANS LA PATHOLOGIE BDANS LA PATHOLOGIE BÉÉNIGNE BILATNIGNE BILATÉÉRALE RALE ??
POURQUOIPOURQUOI LA LA THYROTHYROÏÏDECTOMIE TOTALE ?DECTOMIE TOTALE ?
Carcinomes cachCarcinomes cachééss
Risques de rRisques de réécidive du gocidive du goîîtretre
LLéésions des nerfs rsions des nerfs réécourrentscourrents
LLéésions des parathyrosions des parathyroïïdesdes
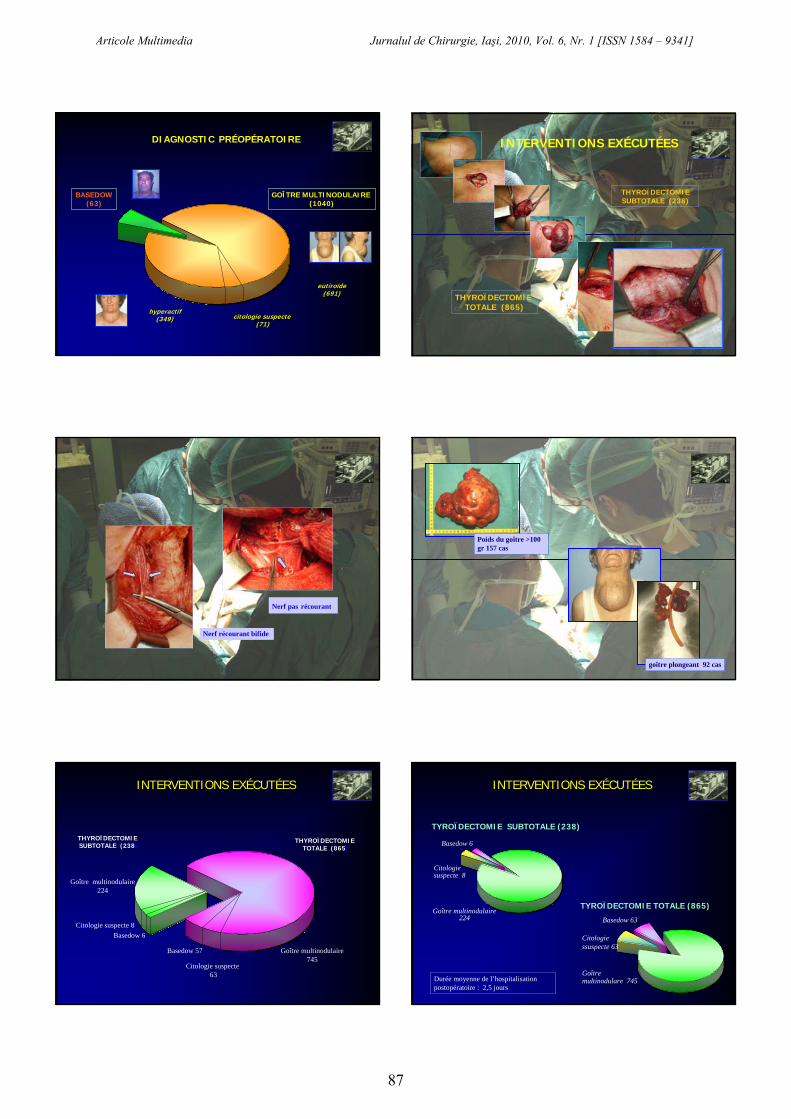
1ère intervention(1082 cas)
1ère intervention(1082 cas)Pathologie récidive
(51 cas)Pathologie récidive
(51 cas)
1103 INTERVENTION DE TYROÏDECTOMIE BILATÉRALE
1103 INTERVENTION DE 1103 INTERVENTION DE TYROTYROÏÏDECTOMIE BILATDECTOMIE BILATÉÉRALE RALE
Articole Multimedia Jurnalul de Chirurgie, Iaşi, 2010, Vol. 6, Nr. 1 [ISSN 1584 – 9341]
85
ÉVALUATION DE LA FONCTIONNALITÉ DE LA THYROÏDE
VISITE ENDOCRINOLOGIQUE
VISITE ANHÉSTESIOLOGIQUE
VISITE OTORINOLARINGOÏATRIQUE
DIAGNOSTIC PRÉOPÉRATOIRE
Compression trachéale
RADIOGRAPHIE DU THORAX - Goître cervico-médiastinique
DIAGNOSTIC PRÉOPÉRATOIRE
TRANSIT OESOPHAGIEN BARYTÉGoître cervico-médiastinique
Pièce opératoire
DIAGNOSTIC PRÉOPÉRATOIRE
TC / RMN DU COU ET DU THORAXGoître cervico-médiastinique avec compresssion trachéale et de l’oesophage
DIAGNOSTIC PRÉOPÉRATOIRE
ÉCOGRAPHIE SCINTIGRAPHIE ÉCOGRAPHIE + SCINTIGRAPHIE517 p.
(46,9%)32 p.
(2,9%)554 p.
(50,2%)
DIAGNOSTIC PRÉOPÉRATOIRE
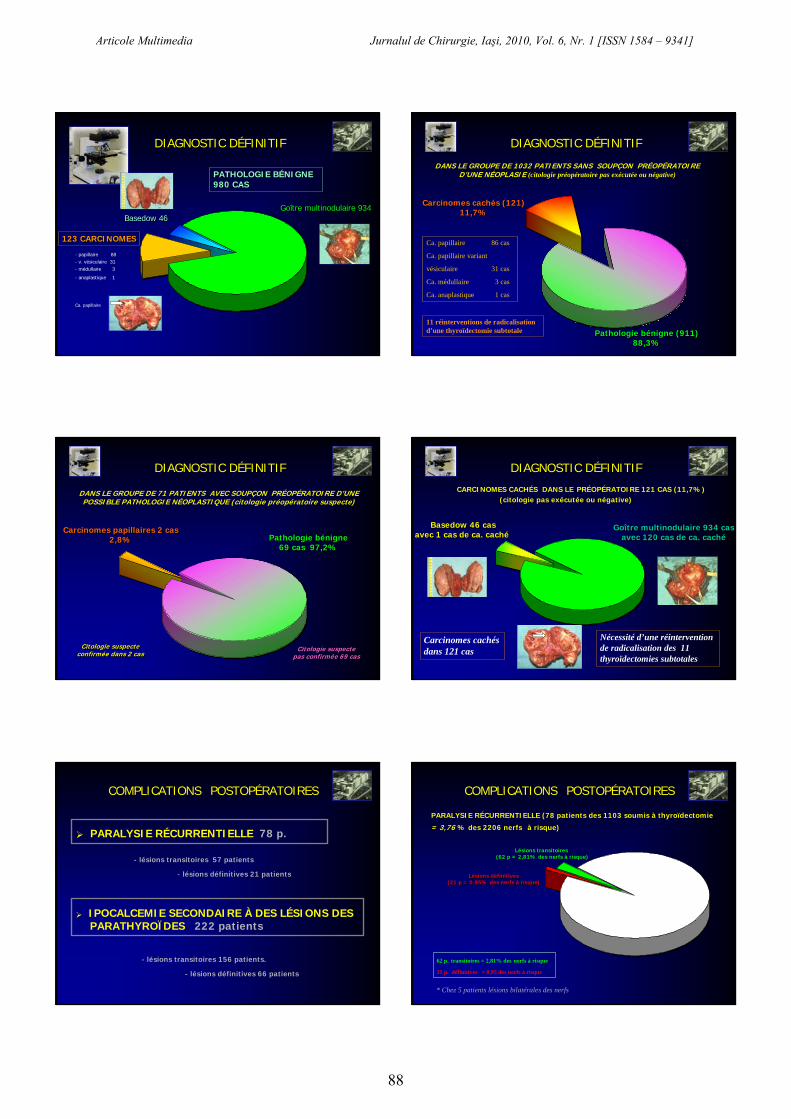
Pas d’indication (523)
Pas d’indication (523)
Citologie bénigne (509)
Citologie bénigne (509)
Citologie suspecte(71)
DIAGNOSTIC PRÉOPÉRATOIRE
EXAMEN CITOLOGIQUE
Articole Multimedia Jurnalul de Chirurgie, Iaşi, 2010, Vol. 6, Nr. 1 [ISSN 1584 – 9341]
86
citologie suspecte(71)
citologie suspecte(71)
BASEDOW(63)
hyperactif(349)
GOÎTRE MULTINODULAIRE (1040)
GOÎTRE MULTINODULAIRE (1040)
eutiroïde(691)
eutiroïde(691)
DIAGNOSTIC PRÉOPÉRATOIRE INTERVENTIONS EXÉCUTÉESINTERVENTIONS EXÉCUTÉES
THYROÏDECTOMIE SUBTOTALE (238)
THYROÏDECTOMIE TOTALE (865)
INTERVENTIONS EXÉCUTÉES
Nerf récourant bifide
Nerf pas récourant
INTERVENTIONS EXÉCUTÉES
Poids du goître >100 gr 157 cas
goître plongeant 92 cas
Basedow 6
Basedow 57
Citologie suspecte 8
Citologie suspecte63
Goître multinodulaire 224
Goître multinodulaire 745
INTERVENTIONS EXÉCUTÉES
THYROÏDECTOMIE SUBTOTALE (238)
THYROÏDECTOMIE TOTALE (865)
TYROÏDECTOMIE SUBTOTALE (238)
Basedow 6
Citologiesuspecte 8
Goître multinodulaire 224
TYROÏDECTOMIE TOTALE (865)
Basedow 63
Citologie ssuspecte 63
Goîtremultinodulare 745
INTERVENTIONS EXÉCUTÉES
Durée moyenne de l’hospitalisationpostopératoire : 2,5 jours
Articole Multimedia Jurnalul de Chirurgie, Iaşi, 2010, Vol. 6, Nr. 1 [ISSN 1584 – 9341]
87
Goître multinodulaire 934Goître multinodulaire 934Basedow 46Basedow 46
123 CARCINOMES123 CARCINOMES123 CARCINOMES
- papillaire 88- v. vésiculaire 31- médullaire 3
- anaplastique 1
DIAGNOSTIC DÉFINITIF
Ca. papillaire
PATHOLOGIE BPATHOLOGIE BÉÉNIGNE NIGNE 980 CAS980 CAS
Carcinomes cachés (121)11,7%
Carcinomes cachés (121)11,7%
Pathologie bénigne (911)88,3%
Pathologie bénigne (911)88,3%
DANS LE GROUPE DE 1032 PATIENTS SANS SOUPÇON PRÉOPÉRATOIRED’UNE NÉOPLASIE (citologie préopératoire pas exécutée ou négative)
Ca. papillaire 86 cas
Ca. papillaire variant
vésiculaire 31 cas
Ca. médullaire 3 cas
Ca. anaplastique 1 cas
11 réinterventions de radicalisation d’une thyroïdectomie subtotale
DIAGNOSTIC DÉFINITIF
Carcinomes papillaires 2 cas2,8%
Carcinomes papillaires 2 cas2,8% Pathologie bénigne
69 cas 97,2%Pathologie bénigne
69 cas 97,2%
DANS LE GROUPE DE 71 PATIENTS AVEC SOUPÇON PRÉOPÉRATOIRE D’UNE POSSIBLE PATHOLOGIE NÉOPLASTIQUE (citologie préopératoire suspecte)
Citologie suspecte pas confirmée 69 casCitologie suspecte
pas confirmée 69 casCitologie suspecte
confirmée dans 2 casCitologie suspecte
confirmée dans 2 cas
DIAGNOSTIC DÉFINITIF
Goître multinodulaire 934 casavec 120 cas de ca. caché
Goître multinodulaire 934 casavec 120 cas de ca. caché
Basedow 46 casavec 1 cas de ca. caché
Basedow 46 casavec 1 cas de ca. caché
Carcinomes cachés dans 121 cas
CARCINOMES CACHÉS DANS LE PRÉOPÉRATOIRE 121 CAS (11,7%)(citologie pas exécutée ou négative)
DIAGNOSTIC DÉFINITIF
Nécessité d’une réinterventionde radicalisation des 11 thyroïdectomies subtotales
PARALYSIE RÉCURRENTIELLE 78 p.
COMPLICATIONS POSTOPÉRATOIRES
IPOCALCEMIE SECONDAIRE À DES LÉSIONS DESPARATHYROÏDES 222 patients
- lésions transitoires 57 patients
- lésions définitives 21 patients
- lésions transitoires 156 patients.
- lésions définitives 66 patients
Lésions définitives(21 p = 0,95% des nerfs à risque)
Lésions définitives(21 p = 0,95% des nerfs à risque)
Lésions transitoires(62 p = 2,81% des nerfs à risque)
62 p. transitoires = 2,81% des nerfs à risque
21 p. définitives = 0,95 des nerfs à risque
PARALYSIE RÉCURRENTIELLE (78 patients des 1103 soumis à thyroïdectomie
= 3,76 % des 2206 nerfs à risque)
COMPLICATIONS POSTOPÉRATOIRES
* Chez 5 patients lésions bilatérales des nerfs
Articole Multimedia Jurnalul de Chirurgie, Iaşi, 2010, Vol. 6, Nr. 1 [ISSN 1584 – 9341]
88
1103 patients/ 2206 nerfs1103 patients/ 2206 nerfsThyroThyroïïdectomiedectomietotaletotale 865 p / 865 p /
1720 1720 nerfsnerfs
ThyroThyroïïdectomiedectomiesubtotalesubtotale
238 p / 476 238 p / 476 nerfsnerfs
p test
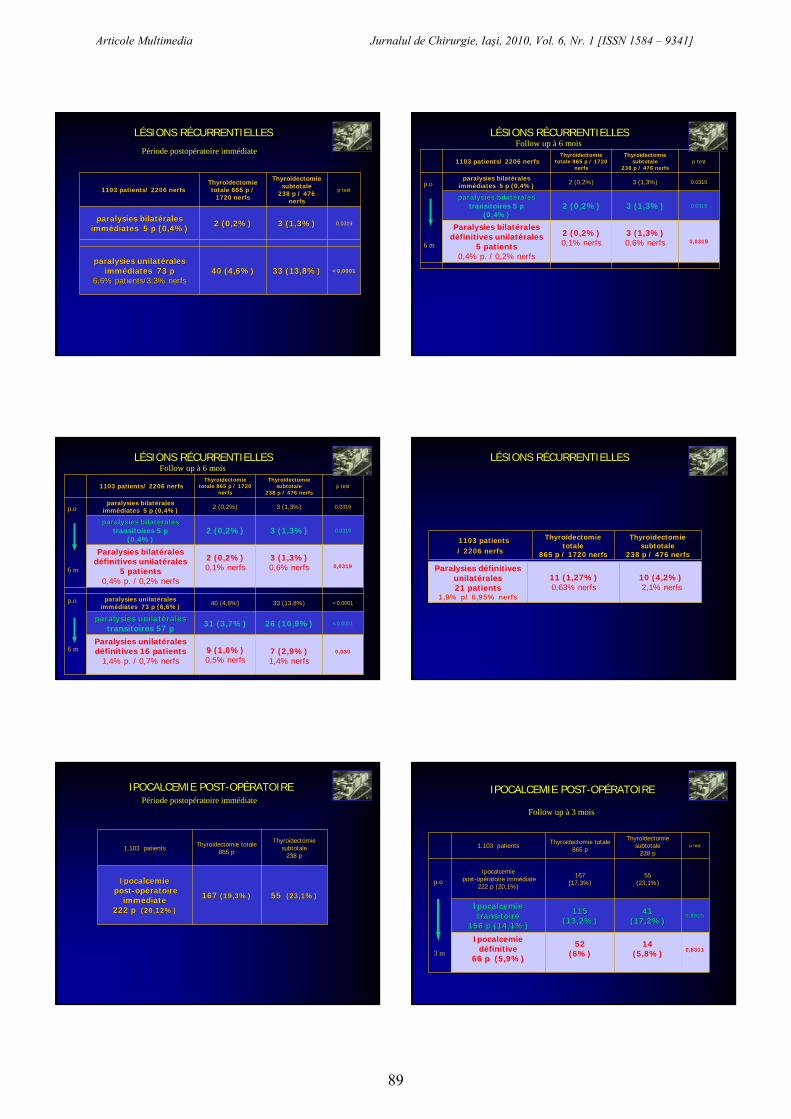
paralysiesparalysies bilatbilatééralesralesimmimméédiatesdiates 5 p (0,4%)5 p (0,4%) 2 (0,2%)2 (0,2%) 3 (1,3%)3 (1,3%) 0,0319
paralysiesparalysies unilatunilatééralesralesimmimméédiatesdiates 73 p 73 p
6,6% patients/3,3% 6,6% patients/3,3% nerfsnerfs40 (4,6%)40 (4,6%) 33 (13,8%)33 (13,8%) <0,0001
LÉSIONS RÉCURRENTIELLES
Période postopératoire immédiate1103 patients/ 2206 nerfs1103 patients/ 2206 nerfs
ThyroThyroïïdectomiedectomietotaletotale 865 p / 1720 865 p / 1720
nerfsnerfs
ThyroThyroïïdectomiedectomiesubtotalesubtotale
238 p / 476 nerfs238 p / 476 nerfsp test
paralysies bilatéralesimmédiates 5 p (0,4%) 2 (0,2%) 3 (1,3%) 0,0319
paralysiesparalysies bilatbilatééralesralestransitoires 5 p
(0,4%)2 (0,2%) 3 (1,3%) 0,0319
Paralysies bilatérales définitives unilatérales
5 patients0,4% p. / 0,2% nerfs
2 (0,2%)0,1% nerfs
3 (1,3%)0,6% nerfs 0,0319
p.o.
6 m
LÉSIONS RÉCURRENTIELLES Follow up à 6 mois
1103 patients/ 2206 nerfs1103 patients/ 2206 nerfsThyroThyroïïdectomiedectomie
totaletotale 865 p / 1720 865 p / 1720 nerfsnerfs
ThyroThyroïïdectomiedectomiesubtotalesubtotale
238 p / 476 nerfs238 p / 476 nerfsp test
paralysies bilatéralesimmédiates 5 p (0,4%) 2 (0,2%) 3 (1,3%) 0,0319
paralysiesparalysies bilatbilatééralesralestransitoires 5 p
(0,4%)2 (0,2%) 3 (1,3%) 0,0319
Paralysies bilatérales définitives unilatérales
5 patients0,4% p. / 0,2% nerfs
2 (0,2%)0,1% nerfs
3 (1,3%)0,6% nerfs 0,0319
paralysiesparalysies unilatunilatééralesralesimmimméédiatesdiates 73 p (6,6%)73 p (6,6%) 40 (4,6%) 33 (13,8%) <0,0001
paralysiesparalysies unilatunilatééralesralestransitoires 57 p 31 (3,7%) 26 (10,9%) <0,0001
Paralysies unilatérales définitives 16 patients
1,4% p. / 0,7% nerfs9 (1,0%)0,5% nerfs
7 (2,9%)1,4% nerfs
0,030
p.o.
6 m
6 m
LÉSIONS RÉCURRENTIELLES Follow up à 6 mois
p.o
1103 patients1103 patients/ 2206 nerfs/ 2206 nerfs
ThyroThyroïïdectomiedectomietotaletotale
865 p / 1720 865 p / 1720 nerfsnerfs
ThyroThyroïïdectomiedectomiesubtotalesubtotale
238 p / 476 nerfs238 p / 476 nerfs
LÉSIONS RÉCURRENTIELLES
Paralysies définitivesunilatérales21 patients
1,9% p/ 0,95% nerfs
11 (1,27%)0,63% nerfs
10 (4,2%)2,1% nerfs
1.103 patients Thyroïdectomie totale865 p
Thyroïdectomiesubtotale
238 p
IpocalcemieIpocalcemiepostpost--opopéératoire ratoire
immimméédiate diate 222 p 222 p (20,12%)(20,12%)
167 167 (19,3%)(19,3%) 55 55 (23,1%)(23,1%)
IPOCALCEMIE POST-OPÉRATOIREPériode postopératoire immédiate
1.103 patients Thyroïdectomie totale865 p
Thyroïdectomiesubtotale
238 pp test
Ipocalcemiepost-opératoire immédiate
222 p (20,1%)
167(17,3%)
55(23,1%)
IpocalcemieIpocalcemietransitoiretransitoire
156 p (14,1%)156 p (14,1%)
115 115 (13,2%)(13,2%)
41 41 (17,2%)(17,2%)
0,08150,0815
Ipocalcemiedéfinitive
66 p (5,9%)
52 (6%)
14 (5,8%) 0,8311
IPOCALCEMIE POST-OPÉRATOIRE
p.o.
3 m
Follow up à 3 mois
Articole Multimedia Jurnalul de Chirurgie, Iaşi, 2010, Vol. 6, Nr. 1 [ISSN 1584 – 9341]
89

transitoires 1,9%transitoires 1,9%définitives
0,6%définitives
0,6%
définitive 6%
transitoire 17,2%
THYROÏDECTOMIE TOTALE 209/865 p. = 24,1%
THYROÏDECTOMIE SUBTOTALE 91/238 p = 38,2%
Lésions des nerfs récurrentiels 36 p.Lésions des nerfs
récurrentiels 36 p.
Ipocalcemie 167 p.transitoires 6%transitoires 6%Definitives 2,1%Definitives 2,1%
Ipocalcemie 55 p.
transitoire 13,2%
définitive 5,8%
COMPLICATIONS POSTOPÉRATOIRES
Lésions des nerfs récurrentiels 42 p.Lésions des nerfs
récurrentiels 42 p.
l’incidence élevée de carcinomes cachés supérieure au 11% ...
l’incidence des lésions des nerfs récurrentielles non supérieuremême inférieure dans la thyroïdectomie totale par rapport à la thyroïdectomie subtotale …
……. . nousnous permettentpermettent dd’’affirmeraffirmer queque la la thyrothyroïïdectomiedectomie totaletotaleestest àà considconsidéérerrer le gold standard pour le gold standard pour la la pathologiepathologie bbéénignenignebilatbilatééralerale de la de la thyrothyroïïdede garantissantgarantissant la la radicalitradicalitéé de de ll’’interventionintervention et la et la presquepresque totaletotale disparitiondisparition dudu risquerisque de de rréécidivecidive. .
l’incidence d’ipoparathyroidisme définitif résiduel superposable entre le deux techniques …
CONCLUSION
Dans notre casistique
Articole Multimedia Jurnalul de Chirurgie, Iaşi, 2010, Vol. 6, Nr. 1 [ISSN 1584 – 9341]
90






















