Embed Size (px)
Citation preview
Bartter et Gitelman jouent aux
diurétiques
Rosa Vargas-Poussou Département de Génétique
Hôpital Européen Georges Pompidou
Paris
Syndromes de Bartter et Gitelman
Tubulopathies héréditaires rares
Transmission autosomique récessive
Prévalence
Syndrome de Gitelman: 1/40.000
Syndrome de Bartter: 1/1.000.000
Défaut de réabsorption de sodium dans le
néphron distal
Syndromes de Bartter et Gitelman
Caractéristiques cliniques communes
Activation secondaire du système rénine -
angiotensine - aldostérone
Alcalose métabolique
Hypokaliémie d’origine rénale
Pression artérielle normale ou basse
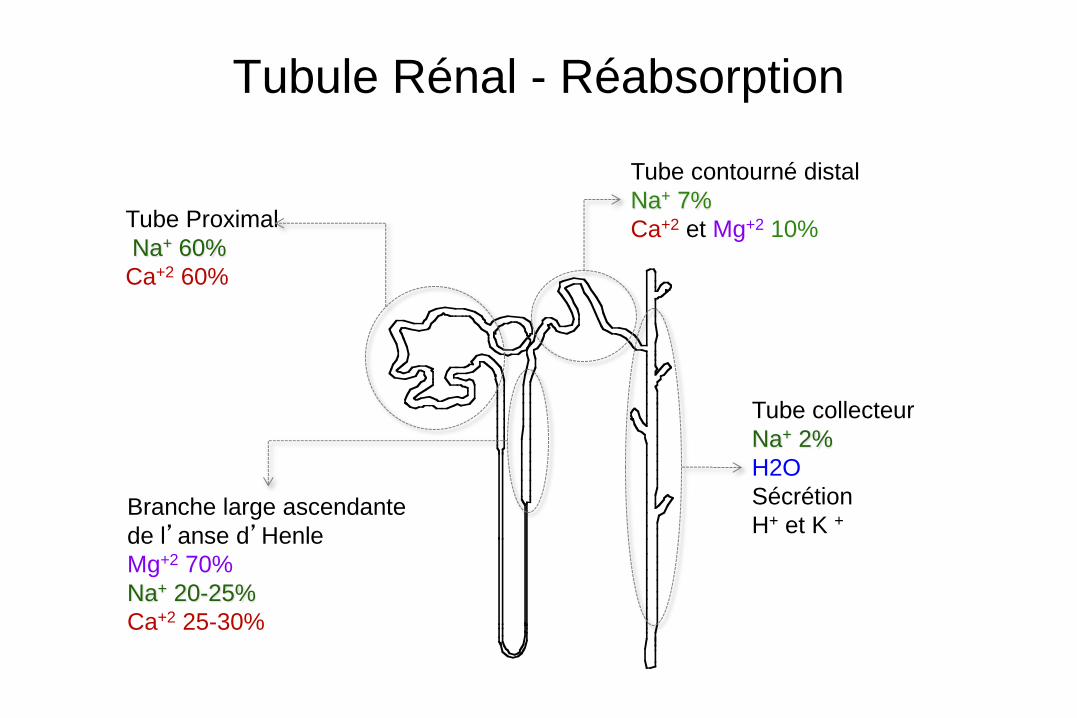
Tubule Rénal - Réabsorption
Tube Proximal
Na+ 60%
Ca+2 60%
Branche large ascendante
de l’anse d’Henle
Mg+2 70%
Na+ 20-25%
Ca+2 25-30%
Tube collecteur
Na+ 2%
H2O
Sécrétion
H+ et K +
Tube contourné distal
Na+ 7%
Ca+2 et Mg+2 10%
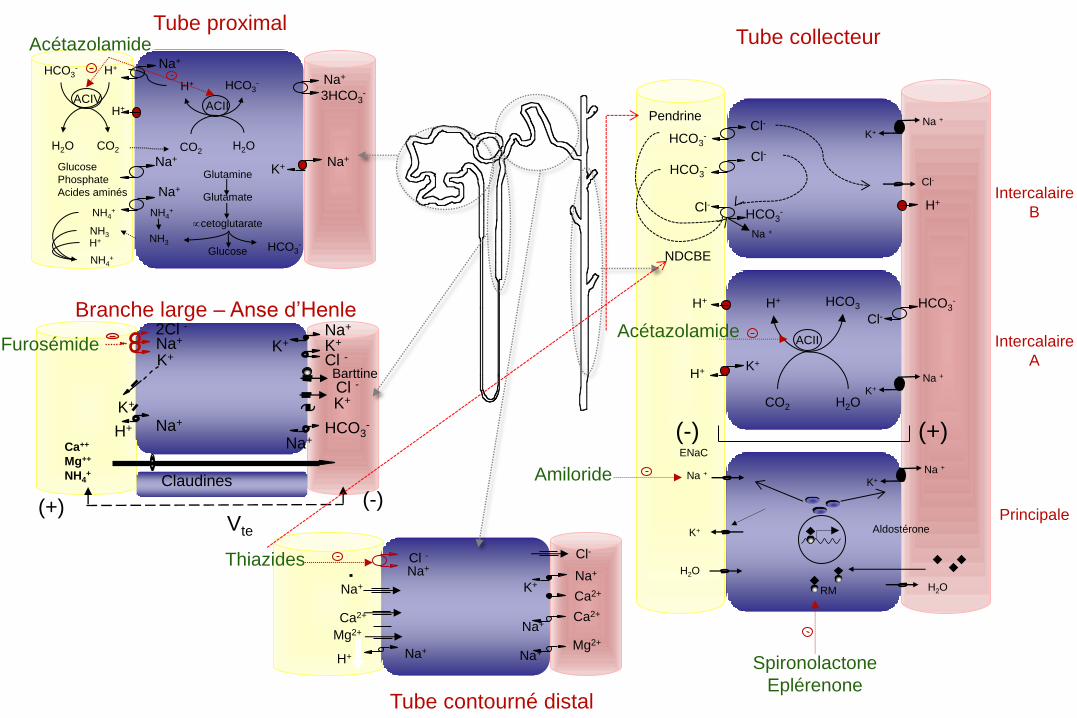
Na+
Na+
K+ Na+ Glucose
Phosphate
Acides aminés
Na+
3HCO3-
Tube proximal
H2O
H2O
Na +
K+ Aldostérone
K+
RM
ENaC
H+ HCO3-
H2O CO2
CO2 H2O
H+ HCO3-
Cl-
K+
H+
CO2 H2O
HCO3 H+ HCO3
-
Tube collecteur
Na +
ACII ACIV
ACII
H+
H+
Glutamine
Glutamate
cetoglutarate
Glucose
NH4+
NH3
Na+
NH4+
NH3
NH4+
HCO3- H+
(-) (+)
H+
K+
Na +
K+
Na + Cl-
HCO3-
Cl- HCO3
-
Cl-
Cl-
HCO3-
Na +
Intercalaire
B
Thiazides
Ca2+
Na+ Cl -
Na+
Ca2+
Na+
K+
Ca2+
Na+ H+
Mg2+ Na+
Na+ Mg2+
Cl-
Furosémide Na+
K+
2Cl - Na+
K+
K+
Na+ H+
K+
Cl -
Cl -
Na+ HCO3
-
Ca++
Mg++
NH4+
(-) (+) Vte
K+
Claudines
Barttine
Branche large – Anse d’Henle
Intercalaire
A
Principale
Tube contourné distal
Amiloride
Spironolactone
Eplérenone
Acétazolamide
Acétazolamide
Pendrine
NDCBE
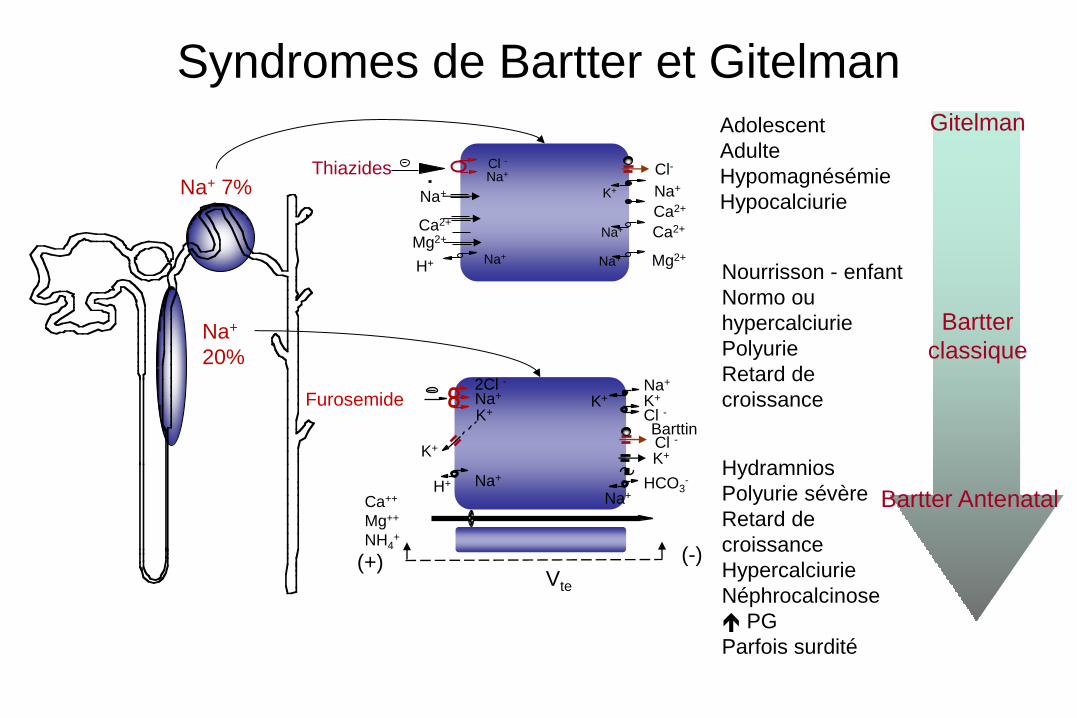
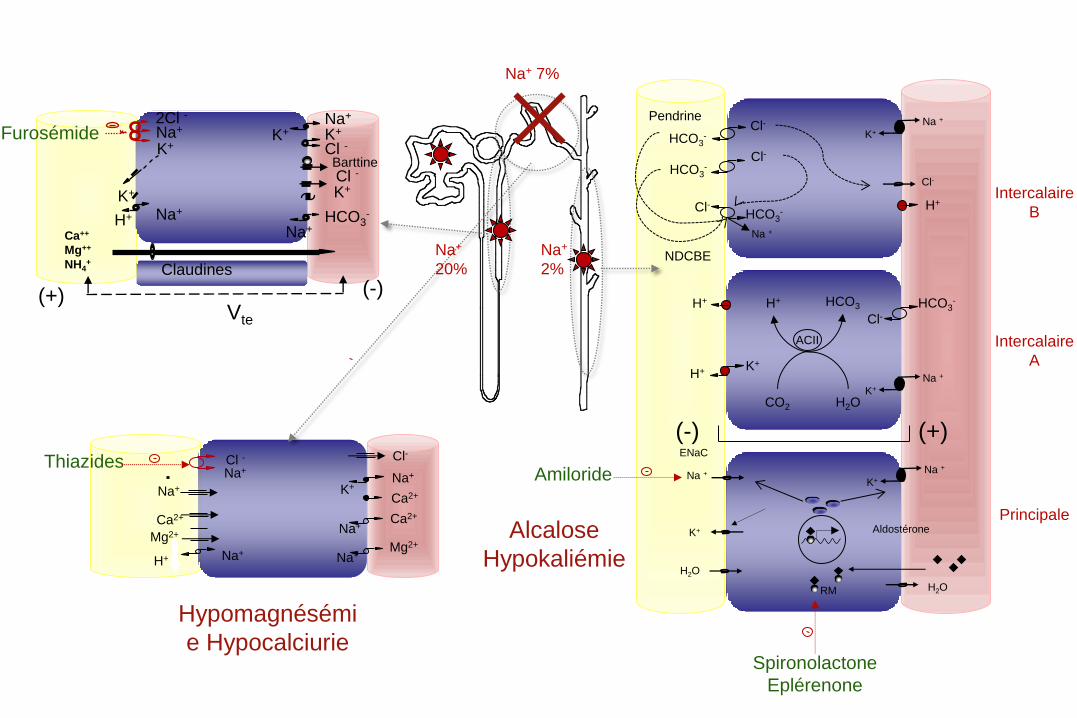
Syndromes de Bartter et Gitelman Gitelman Adolescent
Adulte
Hypomagnésémie
Hypocalciurie
Na+
20%
Na+ 7% Thiazides
Ca2+
Na+ Cl -
Na+
Ca2+
Na+ K+
Ca2+
Na+
H+
Mg2+ Na+
Na+ Mg2+
Cl-
Furosemide
(+)
Na+
K+
2Cl - Na+
K+
K+
Na+ H+
K+
Cl -
Cl -
Na+ HCO3
-
Ca++
Mg++
NH4+
(-) Vte
K+
Barttin
Bartter Antenatal
Hydramnios
Polyurie sévère
Retard de
croissance
Hypercalciurie
Néphrocalcinose
PG
Parfois surdité
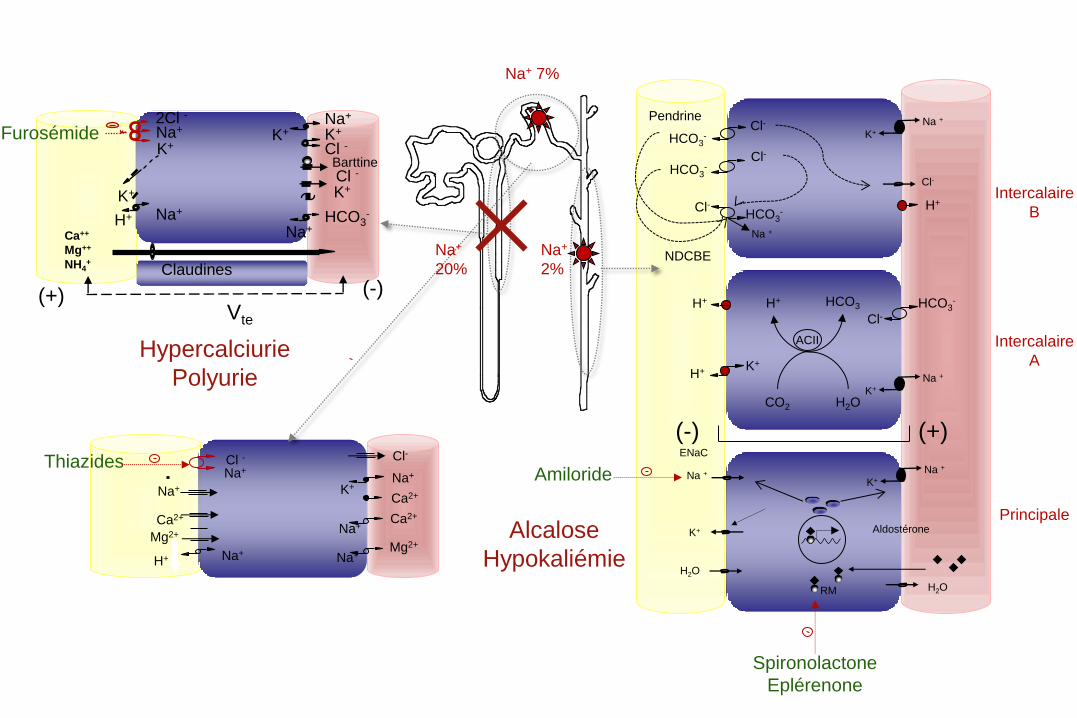
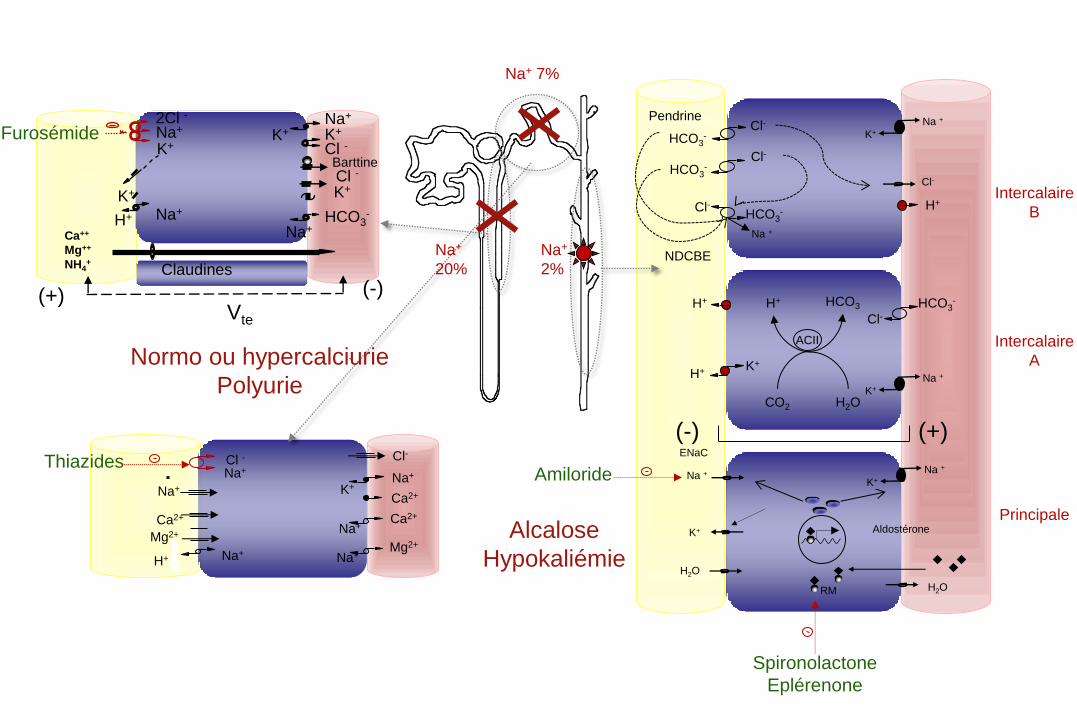
Bartter
classique
Nourrisson - enfant
Normo ou
hypercalciurie
Polyurie
Retard de
croissance
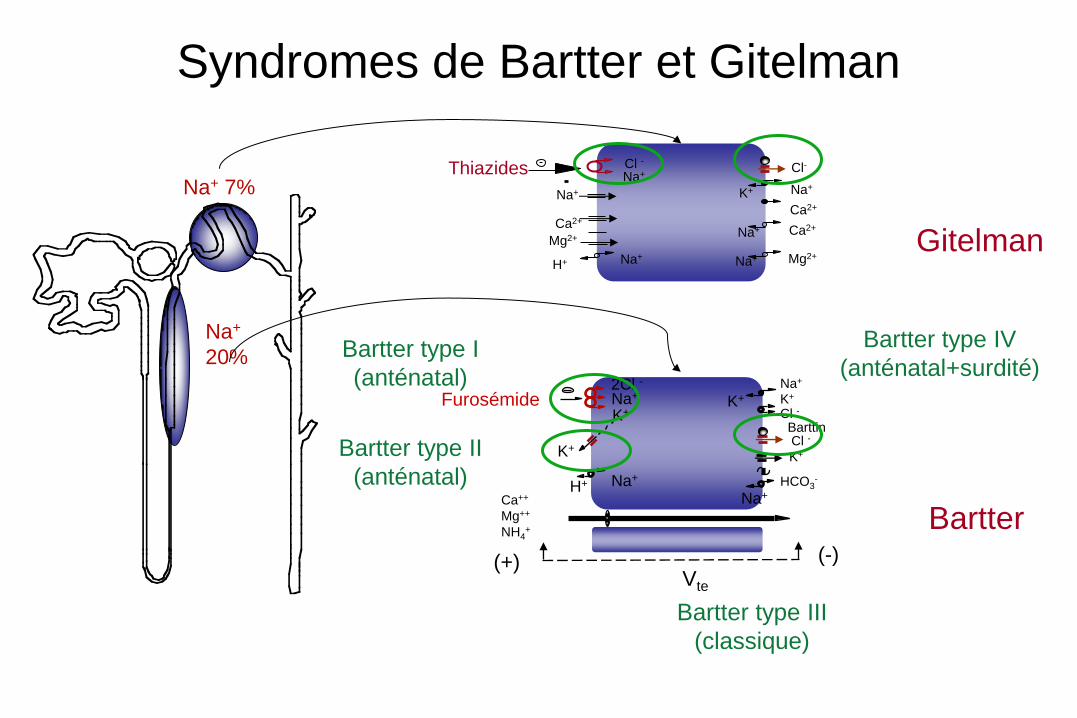
Na+
20%
Na+ 7% Thiazides
Ca2+
Na+ Cl -
Na+
Ca2+
Na+ K+
Ca2+
Na+
H+
Mg2+ Na+
Na+ Mg2+
Cl-
Furosémide
(+)
Na+
K+
2Cl - Na+
K+
K+
Na+ H+
K+
Cl -
Cl -
Na+
HCO3-
Ca++
Mg++
NH4+
(-) Vte
K+
Barttin
Bartter type I
(anténatal)
Bartter type II
(anténatal)
Bartter type III
(classique)
Syndromes de Bartter et Gitelman
Gitelman
Bartter
Bartter type IV
(anténatal+surdité)
H2O
H2O
Na +
K+ Aldostérone
K+
RM
ENaC
Cl-
K+
H+
CO2 H2O
HCO3 H+ HCO3
-
Na +
ACII
H+
(-) (+)
H+
K+
Na +
K+
Na + Cl-
HCO3-
Cl- HCO3
-
Cl-
Cl-
HCO3-
Na +
Intercalaire
B
Thiazides
Ca2+
Na+ Cl -
Na+
Ca2+
Na+
K+
Ca2+
Na+ H+
Mg2+ Na+
Na+ Mg2+
Cl-
Furosémide Na+
K+
2Cl - Na+
K+
K+
Na+ H+
K+
Cl -
Cl -
Na+ HCO3
-
Ca++
Mg++
NH4+
(-) (+) Vte
K+
Claudines
Barttine
Intercalaire
A
Principale
Amiloride
Spironolactone
Eplérenone
Pendrine
NDCBE
Alcalose
Hypokaliémie
Na+
20%
Na+ 7%
Na+
2%
Hypercalciurie
Polyurie
H2O
H2O
Na +
K+ Aldostérone
K+
RM
ENaC
Cl-
K+
H+
CO2 H2O
HCO3 H+ HCO3
-
Na +
ACII
H+
(-) (+)
H+
K+
Na +
K+
Na + Cl-
HCO3-
Cl- HCO3
-
Cl-
Cl-
HCO3-
Na +
Intercalaire
B
Thiazides
Ca2+
Na+ Cl -
Na+
Ca2+
Na+
K+
Ca2+
Na+ H+
Mg2+ Na+
Na+ Mg2+
Cl-
Furosémide Na+
K+
2Cl - Na+
K+
K+
Na+ H+
K+
Cl -
Cl -
Na+ HCO3
-
Ca++
Mg++
NH4+
(-) (+) Vte
K+
Claudines
Barttine
Intercalaire
A
Principale
Amiloride
Spironolactone
Eplérenone
Pendrine
NDCBE
Alcalose
Hypokaliémie
Na+
20%
Na+ 7%
Na+
2%
Normo ou hypercalciurie
Polyurie
H2O
H2O
Na +
K+ Aldostérone
K+
RM
ENaC
Cl-
K+
H+
CO2 H2O
HCO3 H+ HCO3
-
Na +
ACII
H+
(-) (+)
H+
K+
Na +
K+
Na + Cl-
HCO3-
Cl- HCO3
-
Cl-
Cl-
HCO3-
Na +
Intercalaire
B
Thiazides
Ca2+
Na+ Cl -
Na+
Ca2+
Na+
K+
Ca2+
Na+ H+
Mg2+ Na+
Na+ Mg2+
Cl-
Furosémide Na+
K+
2Cl - Na+
K+
K+
Na+ H+
K+
Cl -
Cl -
Na+ HCO3
-
Ca++
Mg++
NH4+
(-) (+) Vte
K+
Claudines
Barttine
Intercalaire
A
Principale
Amiloride
Spironolactone
Eplérenone
Pendrine
NDCBE
Alcalose
Hypokaliémie
Na+
20%
Na+ 7%
Na+
2%
Hypomagnésémi
e Hypocalciurie
Syndrome de Gitelman - Population
Janvier 2001 à août 2009
448 patients avec diagnostic clinique de SG (219 H et 229 F)
Réseau Français de Tubulopathies et Eunefron
Critères – Hypokaliémie d’origine rénale
– Alcalose métabolique
– Fuite sodée
– Activation secondaire du système RAA
– Hypomagnésémie
– Hypocalciurie
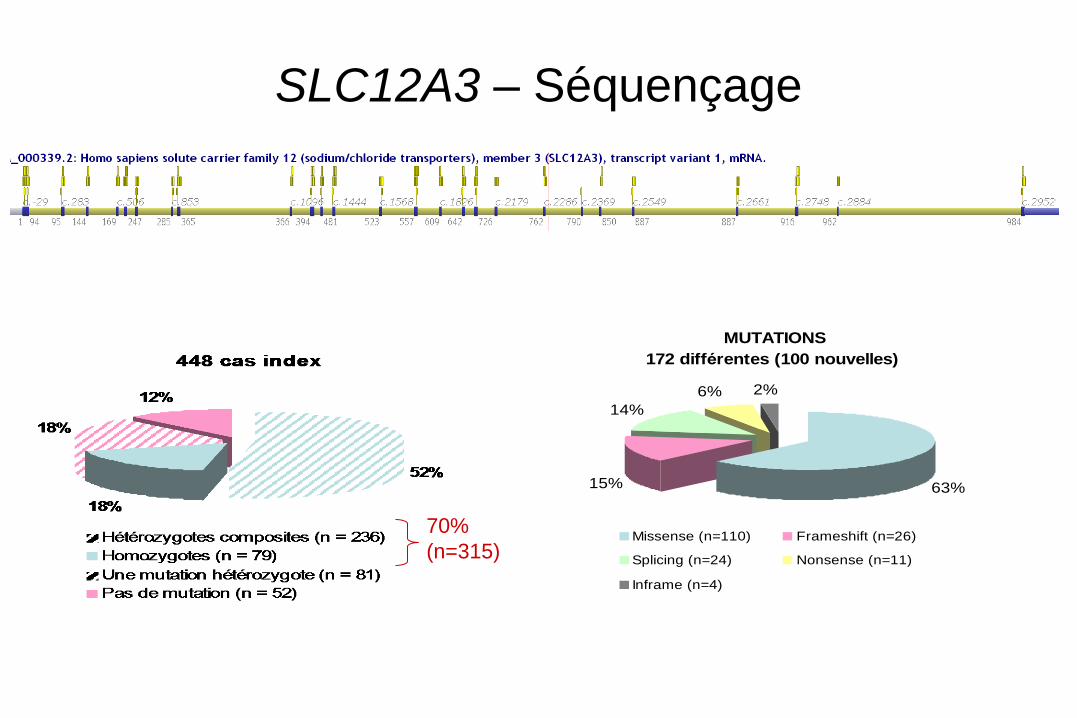
SLC12A3 – Séquençage
MUTATIONS
172 différentes (100 nouvelles)
63%15%
14%
6% 2%
Missense (n=110) Frameshift (n=26)
Splicing (n=24) Nonsense (n=11)
Inframe (n=4)
70%
(n=315)
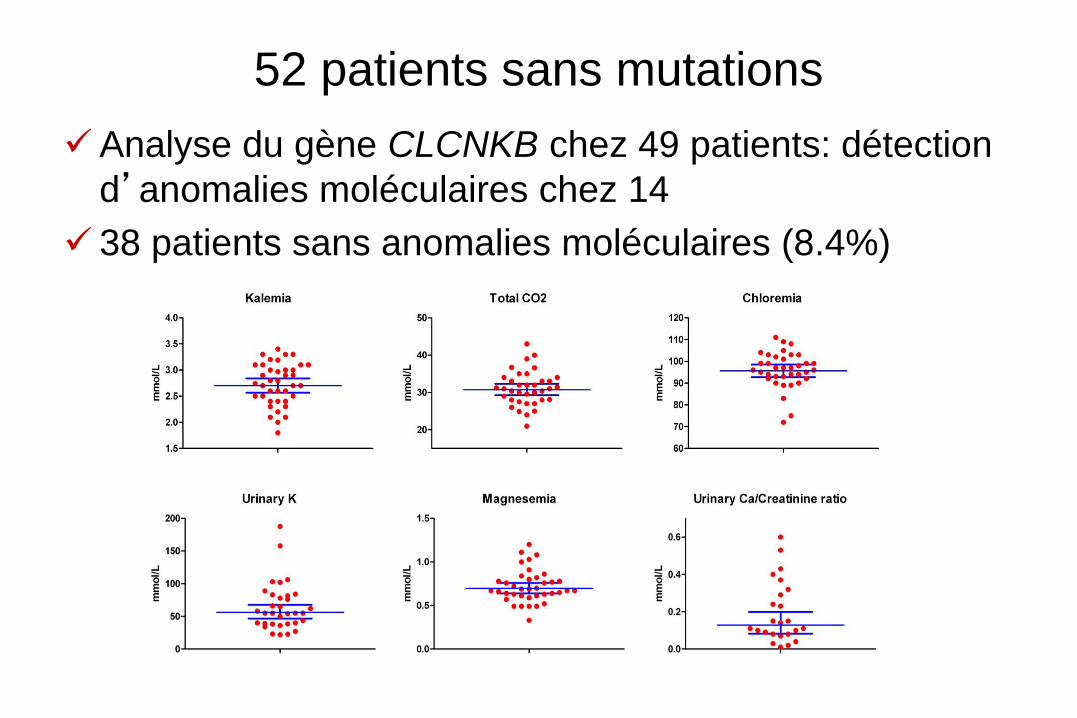
52 patients sans mutations
Analyse du gène CLCNKB chez 49 patients: détection
d’anomalies moléculaires chez 14
38 patients sans anomalies moléculaires (8.4%)
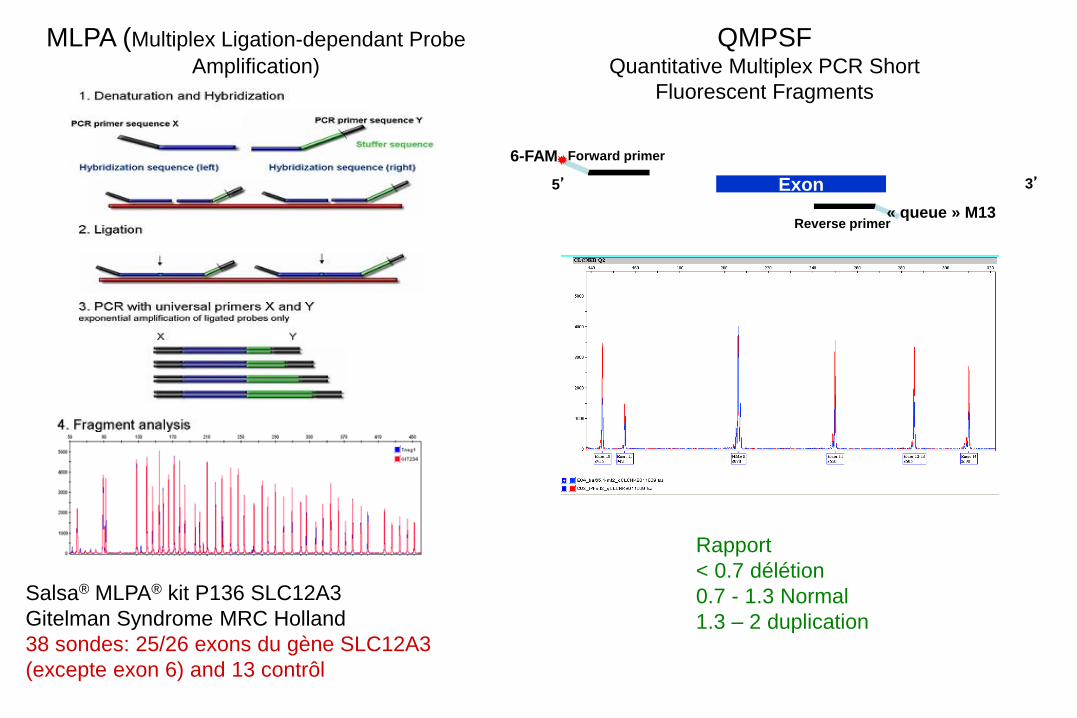
MLPA (Multiplex Ligation-dependant Probe
Amplification)
Rapport
< 0.7 délétion
0.7 - 1.3 Normal
1.3 – 2 duplication
Salsa® MLPA® kit P136 SLC12A3
Gitelman Syndrome MRC Holland
38 sondes: 25/26 exons du gène SLC12A3
(excepte exon 6) and 13 contrôl
QMPSF Quantitative Multiplex PCR Short
Fluorescent Fragments
Exon
6-FAM Forward primer
Reverse primer
5’ 3’
« queue » M13
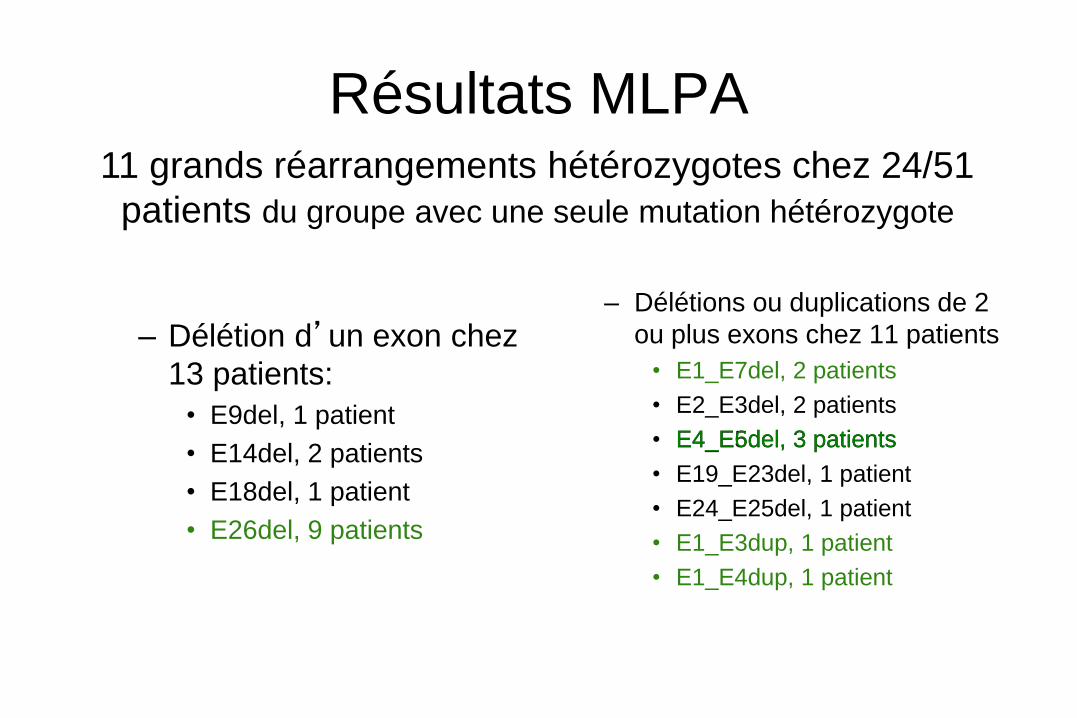
Résultats MLPA
– Délétion d’un exon chez
13 patients:
• E9del, 1 patient
• E14del, 2 patients
• E18del, 1 patient
• E26del, 9 patients
– Délétions ou duplications de 2
ou plus exons chez 11 patients
• E1_E7del, 2 patients
• E2_E3del, 2 patients
• E4_E5del, 3 patients
• E19_E23del, 1 patient
• E24_E25del, 1 patient
• E1_E3dup, 1 patient
• E1_E4dup, 1 patient
11 grands réarrangements hétérozygotes chez 24/51
patients du groupe avec une seule mutation hétérozygote
E4_E6del, 3 patients
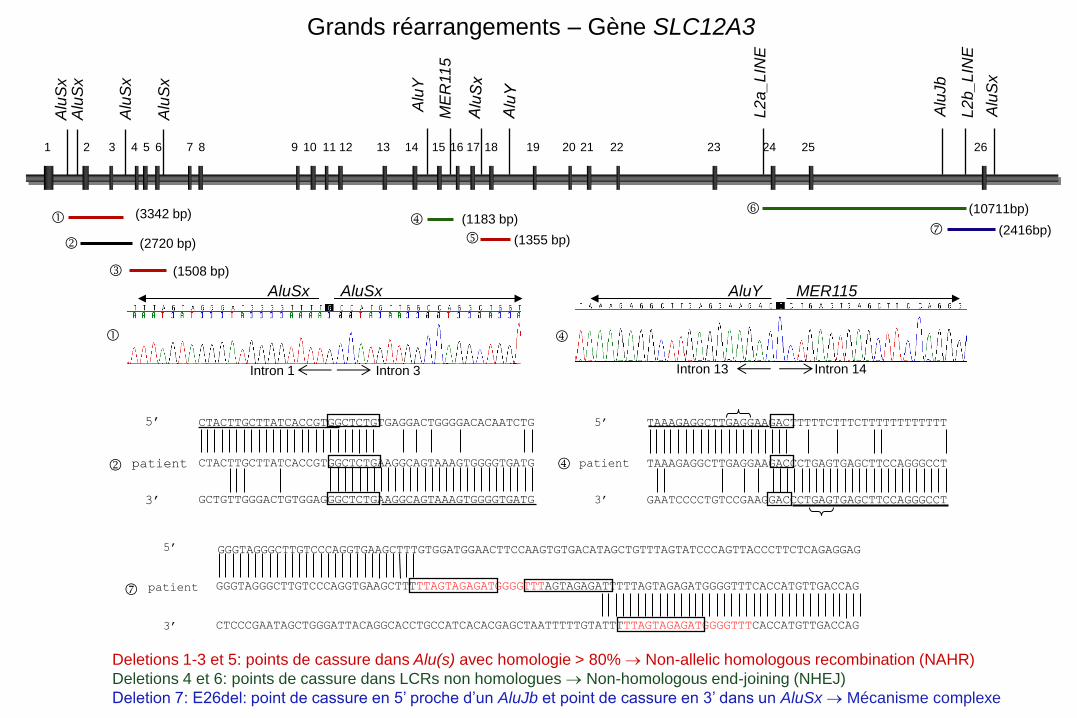
TAAAGAGGCTTGAGGAAGACTTTTTCTTTCTTTTTTTTTTTT
GAATCCCCTGTCCGAAGGACCCTGAGTGAGCTTCCAGGGCCT
TAAAGAGGCTTGAGGAAGACCCTGAGTGAGCTTCCAGGGCCT
5’
patient
3’
CTACTTGCTTATCACCGTGGCTCTGTGAGGACTGGGGACACAATCTG
CTACTTGCTTATCACCGTGGCTCTGAAGGCAGTAAAGTGGGGTGATG
GCTGTTGGGACTGTGGAGGGCTCTGAAGGCAGTAAAGTGGGGTGATG
5’
patient
3’
5’
patient
3’
GGGTAGGGCTTGTCCCAGGTGAAGCTTTGTGGATGGAACTTCCAAGTGTGACATAGCTGTTTAGTATCCCAGTTACCCTTCTCAGAGGAG
GGGTAGGGCTTGTCCCAGGTGAAGCTTTTTAGTAGAGATGGGGTTTAGTAGAGATTTTTAGTAGAGATGGGGTTTCACCATGTTGACCAG
CTCCCGAATAGCTGGGATTACAGGCACCTGCCATCACACGAGCTAATTTTTGTATTTTTAGTAGAGATGGGGTTTCACCATGTTGACCAG
Intron 1 Intron 3
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26
(1355 bp) (2720 bp)
Alu
Sx
Alu
Sx
Alu
Sx
Alu
Sx
(1508 bp)
(3342 bp)
ME
R11
5
Alu
Y
L2
a_
LIN
E
L2
b_
LIN
E
Alu
Sx
Alu
Jb
(1183 bp) (10711bp)
(2416bp)
Intron 13 Intron 14
AluSx AluSx AluY MER115
Deletions 1-3 et 5: points de cassure dans Alu(s) avec homologie > 80% Non-allelic homologous recombination (NAHR)
Deletions 4 et 6: points de cassure dans LCRs non homologues Non-homologous end-joining (NHEJ)
Deletion 7: E26del: point de cassure en 5’ proche d’un AluJb et point de cassure en 3’ dans un AluSx Mécanisme complexe
Grands réarrangements – Gène SLC12A3
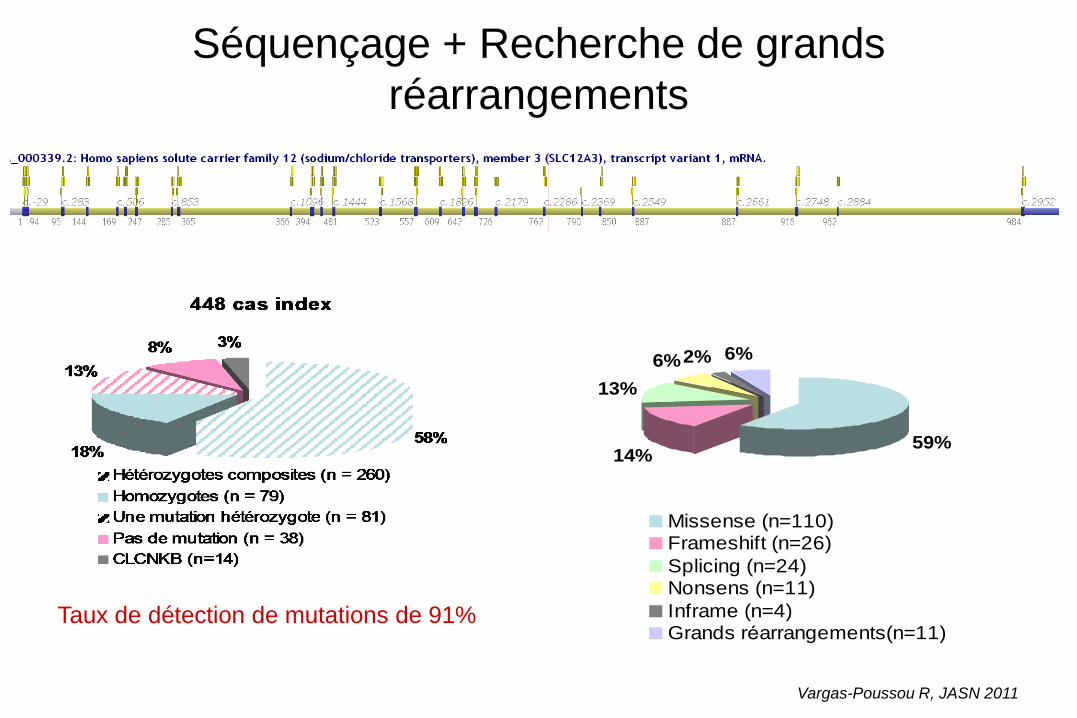
Séquençage + Recherche de grands
réarrangements
59%14%
13%
6%2% 6%
Missense (n=110)Frameshift (n=26)
Splicing (n=24)Nonsens (n=11)
Inframe (n=4)Grands réarrangements(n=11)
Taux de détection de mutations de 91%
Vargas-Poussou R, JASN 2011
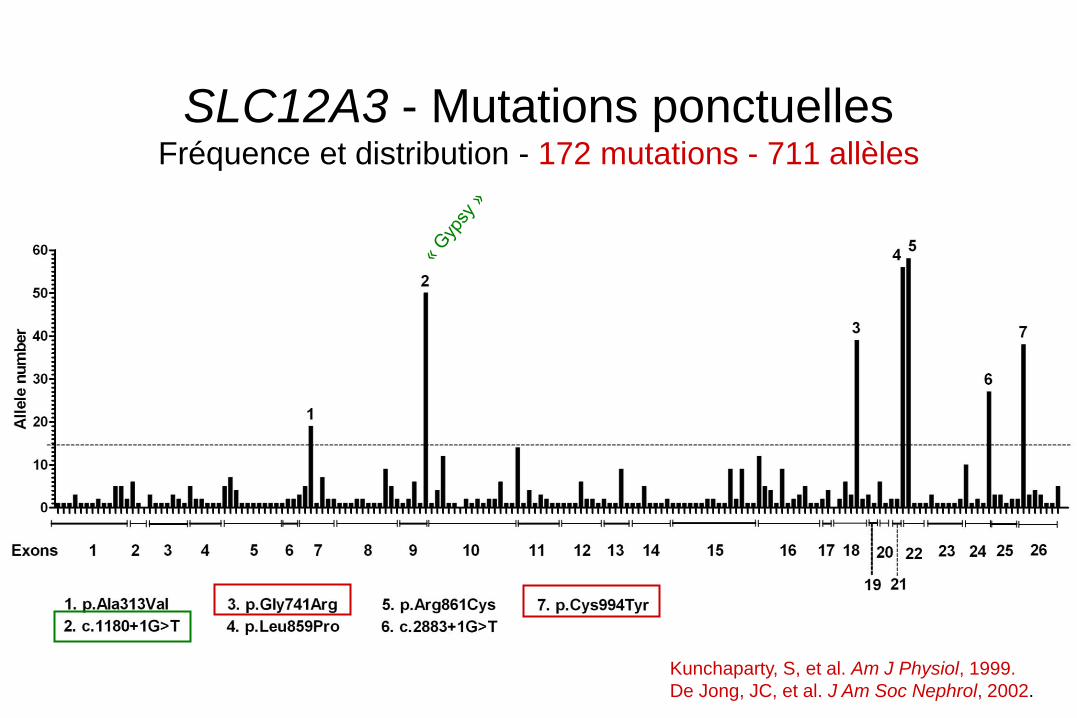
SLC12A3 - Mutations ponctuelles Fréquence et distribution - 172 mutations - 711 allèles
Kunchaparty, S, et al. Am J Physiol, 1999.
De Jong, JC, et al. J Am Soc Nephrol, 2002.
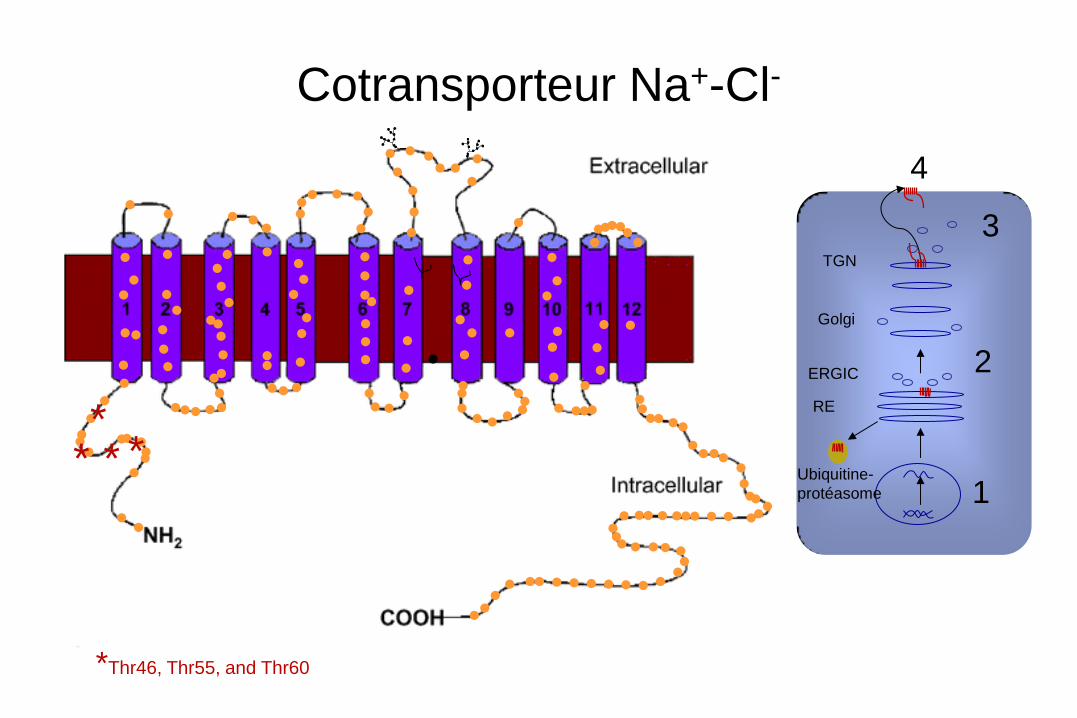
* * * *
Cotransporteur Na+-Cl-
RE
Ubiquitine-
protéasome
ERGIC
Golgi
TGN
1
2
3
4
*Thr46, Thr55, and Thr60
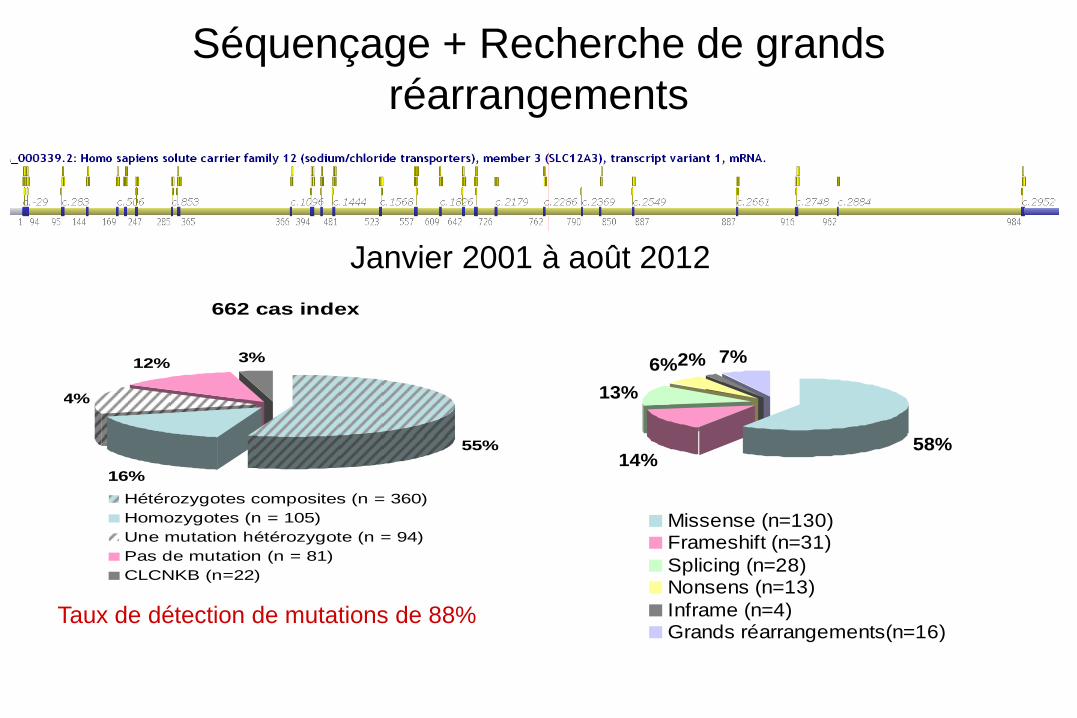
Séquençage + Recherche de grands
réarrangements
58%14%
13%
6%2% 7%
Missense (n=130)Frameshift (n=31)
Splicing (n=28)Nonsens (n=13)
Inframe (n=4)Grands réarrangements(n=16)
Taux de détection de mutations de 88%
Janvier 2001 à août 2012
662 cas index
55%
16%
14%
12% 3%
Hétérozygotes composites (n = 360)
Homozygotes (n = 105)
Une mutation hétérozygote (n = 94)
Pas de mutation (n = 81)
CLCNKB (n=22)
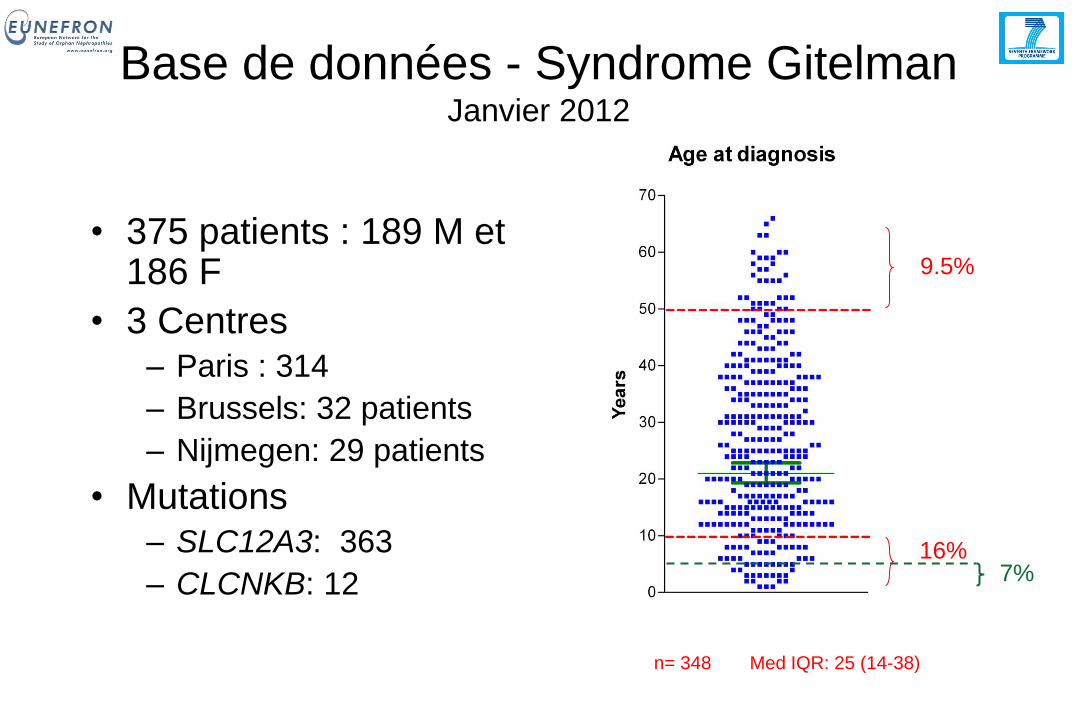
Base de données - Syndrome Gitelman Janvier 2012
• 375 patients : 189 M et 186 F
• 3 Centres – Paris : 314
– Brussels: 32 patients
– Nijmegen: 29 patients
• Mutations – SLC12A3: 363
– CLCNKB: 12
9.5%
16%
n= 348 Med IQR: 25 (14-38)
7%
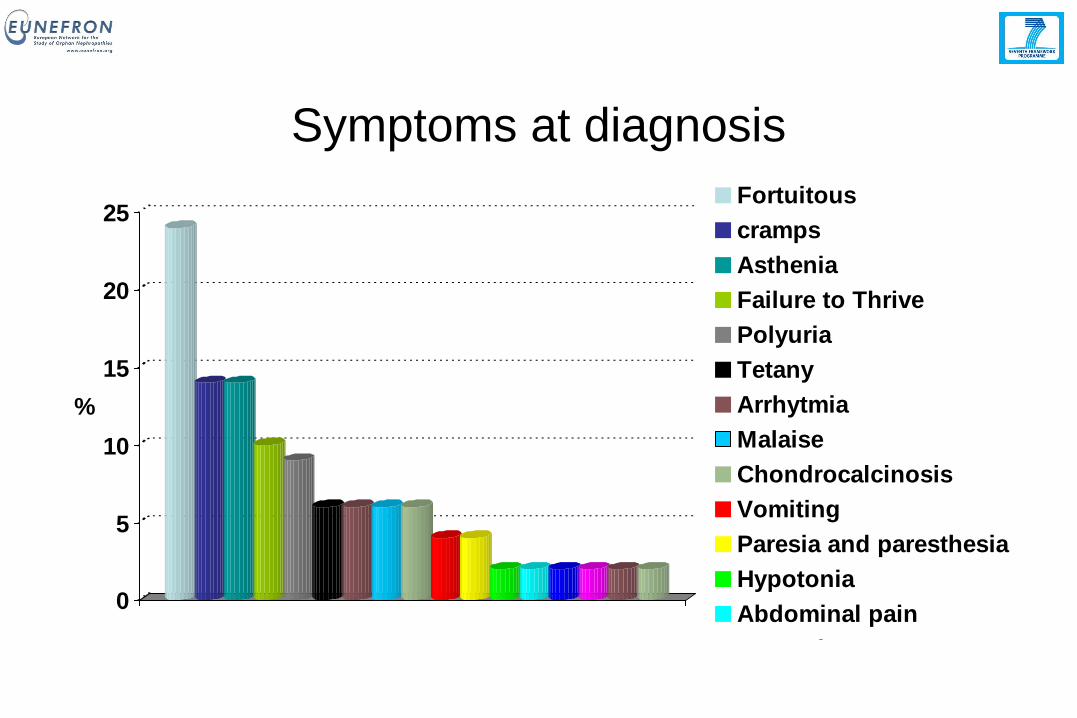
Symptoms at diagnosis
0
5
10
15
20
25
%
Fortuitous
cramps
Asthenia
Failure to Thrive
Polyuria
Tetany
Arrhytmia
Malaise
Chondrocalcinosis
Vomiting
Paresia and paresthesia
Hypotonia
Abdominal pain
Enuresis
constipation
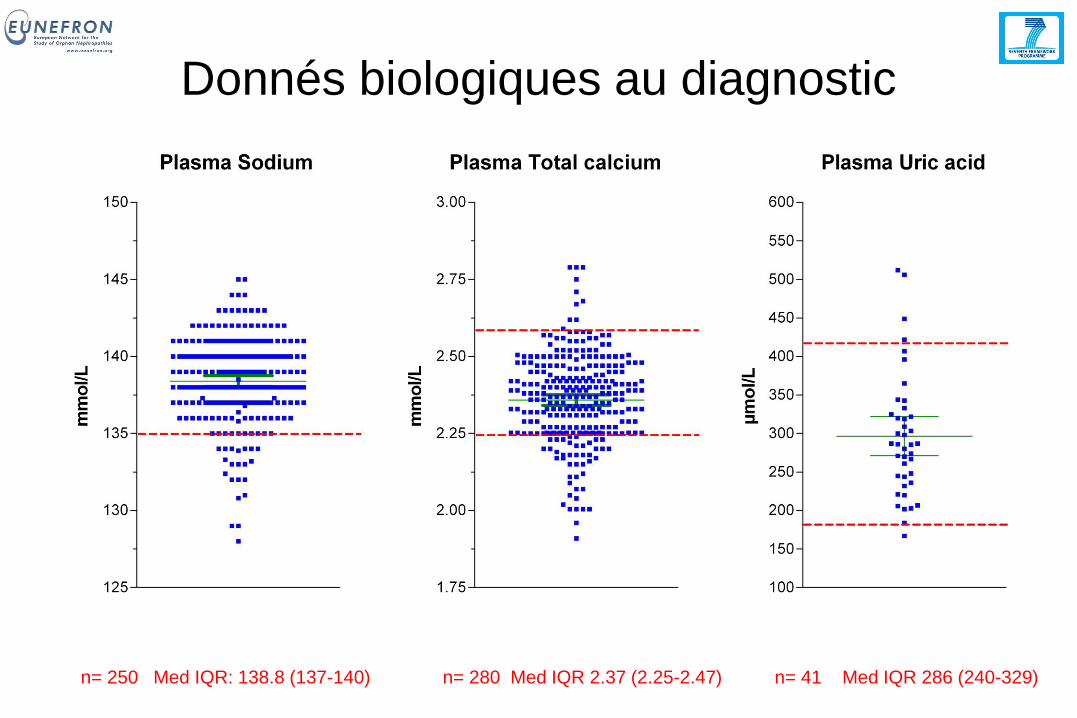
Donnés biologiques au diagnostic
n= 250 Med IQR: 138.8 (137-140) n= 280 Med IQR 2.37 (2.25-2.47) n= 41 Med IQR 286 (240-329)
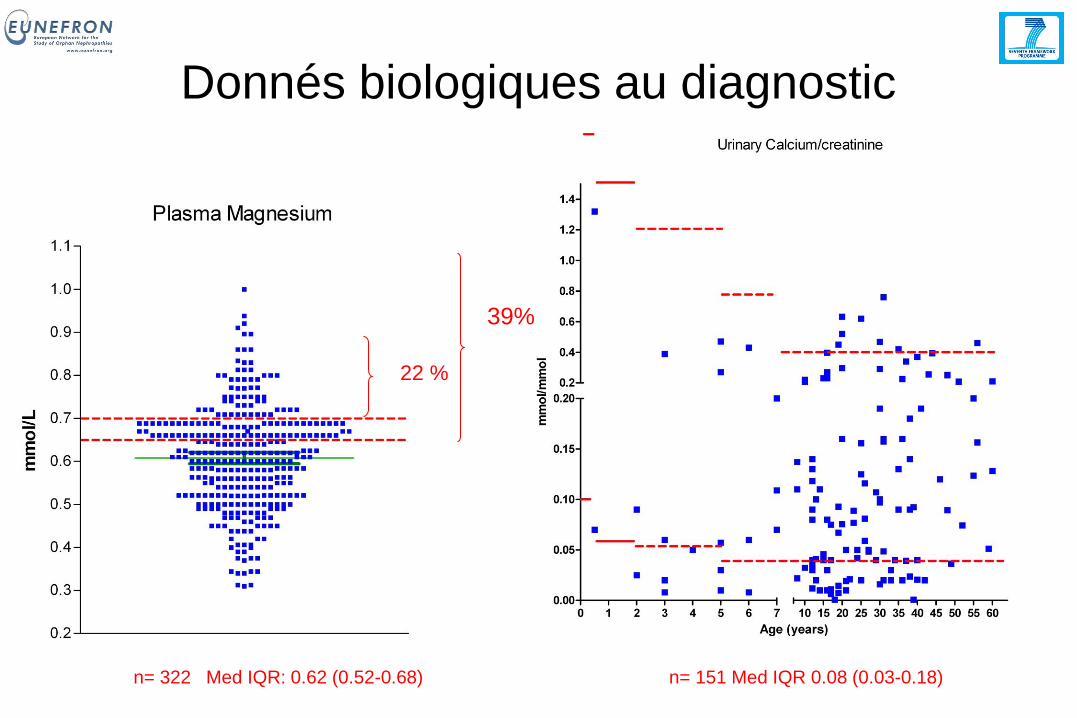
Donnés biologiques au diagnostic
n= 322 Med IQR: 0.62 (0.52-0.68) n= 151 Med IQR 0.08 (0.03-0.18)
22 %
39%
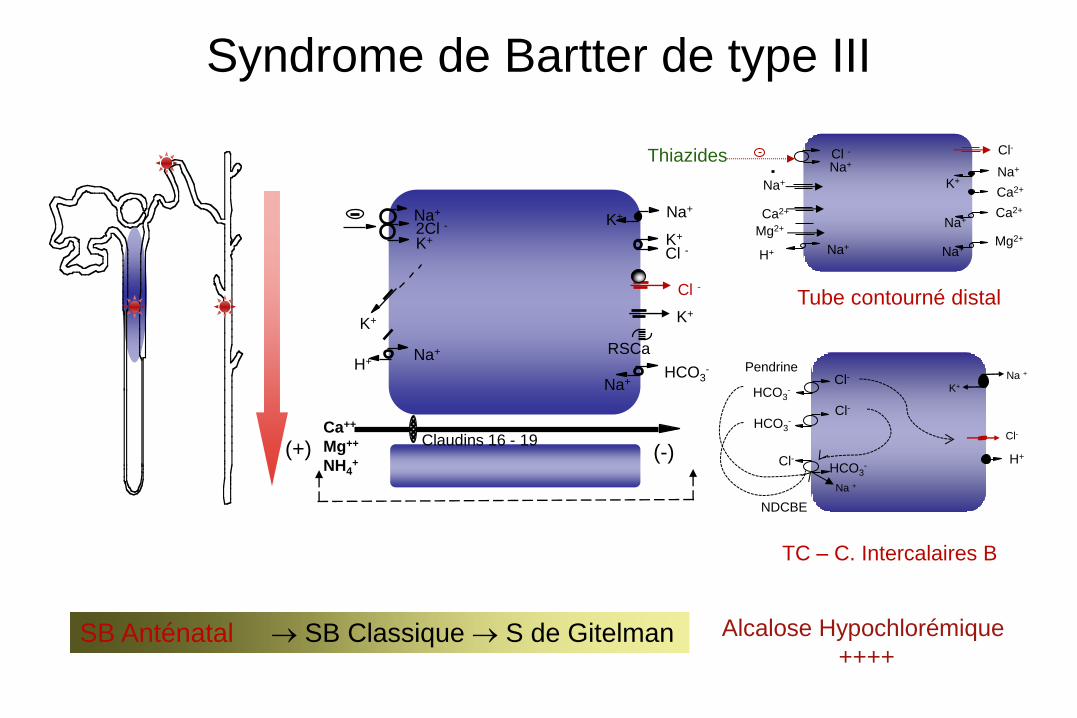
Syndrome de Bartter de type III
Na+
K+ 2Cl -
Na+
K+
K+
Na+
H+
K+
Cl -
Cl -
Na+ HCO3
-
Ca++
Mg++
NH4+
(-) (+)
K+
Claudins 16 - 19
RSCa
Alcalose Hypochlorémique
++++
Thiazides
Ca2+
Na+ Cl -
Na+
Ca2+
Na+
K+
Ca2+
Na+ H+
Mg2+ Na+
Na+ Mg2+
Cl-
Tube contourné distal
H+
K+
Na + Cl-
HCO3-
Cl- HCO3
-
Cl-
Cl-
HCO3-
Na +
TC – C. Intercalaires B
Pendrine
NDCBE
SB Anténatal SB Classique S de Gitelman
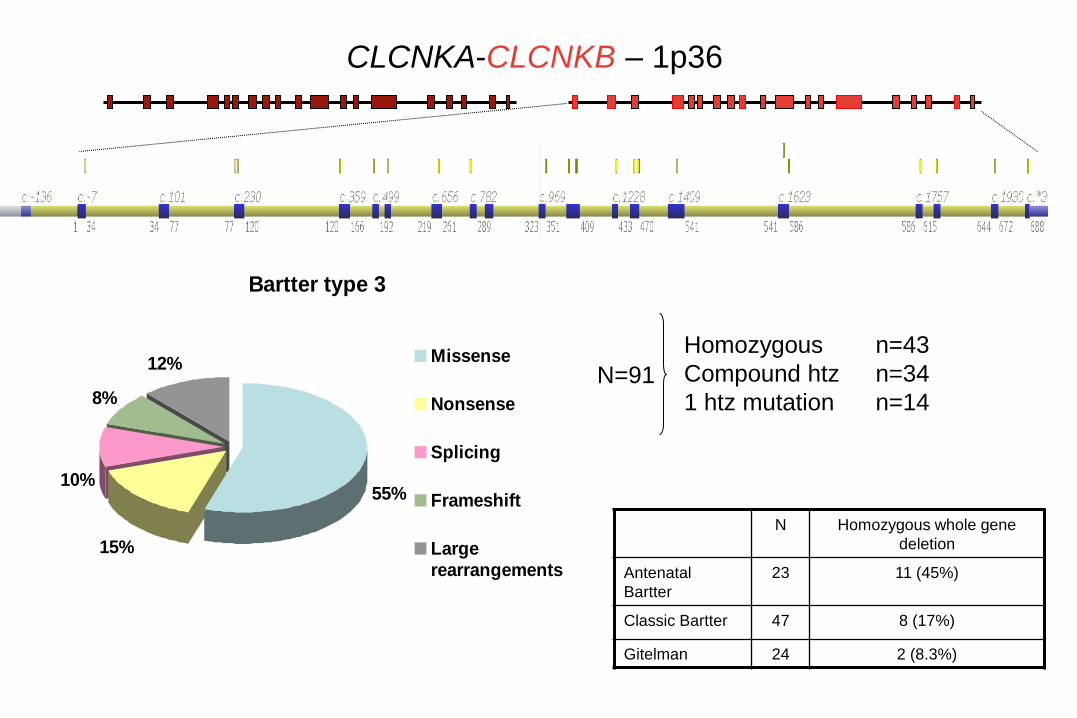
Bartter type 3
55%
15%
10%
8%
12% Missense
Nonsense
Splicing
Frameshift
Largerearrangements
CLCNKA-CLCNKB – 1p36
N Homozygous whole gene
deletion
Antenatal
Bartter
23 11 (45%)
Classic Bartter 47 8 (17%)
Gitelman 24 2 (8.3%)
N=91
Homozygous n=43
Compound htz n=34
1 htz mutation n=14
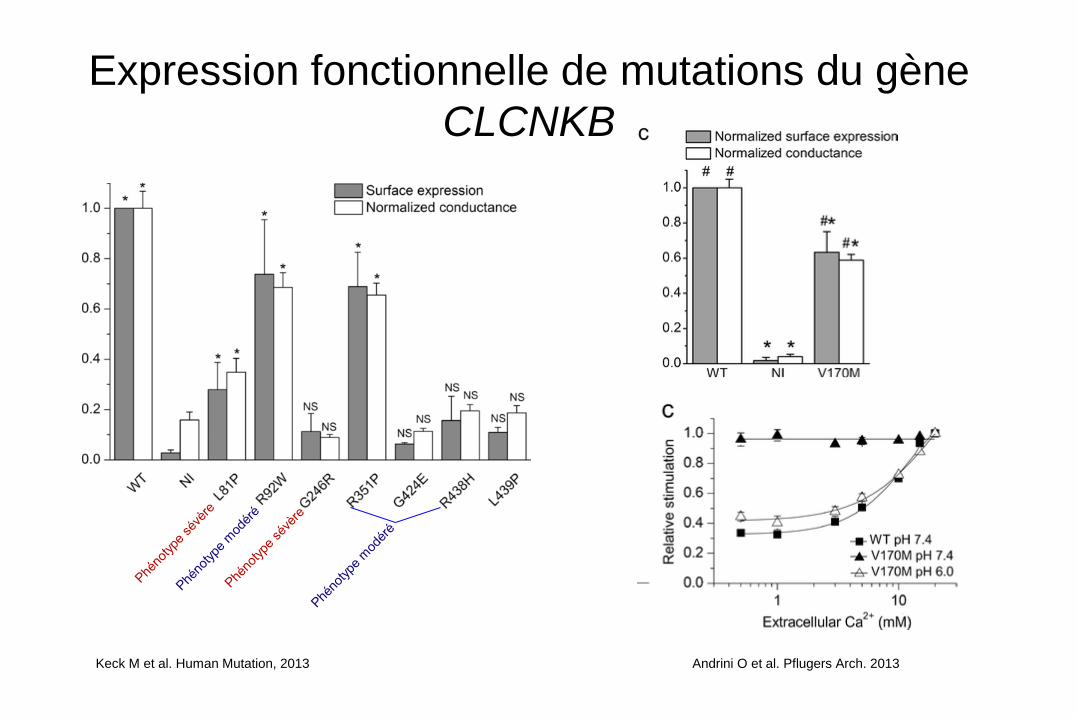
Expression fonctionnelle de mutations du gène
CLCNKB
Keck M et al. Human Mutation, 2013 Andrini O et al. Pflugers Arch. 2013
SLC12A3
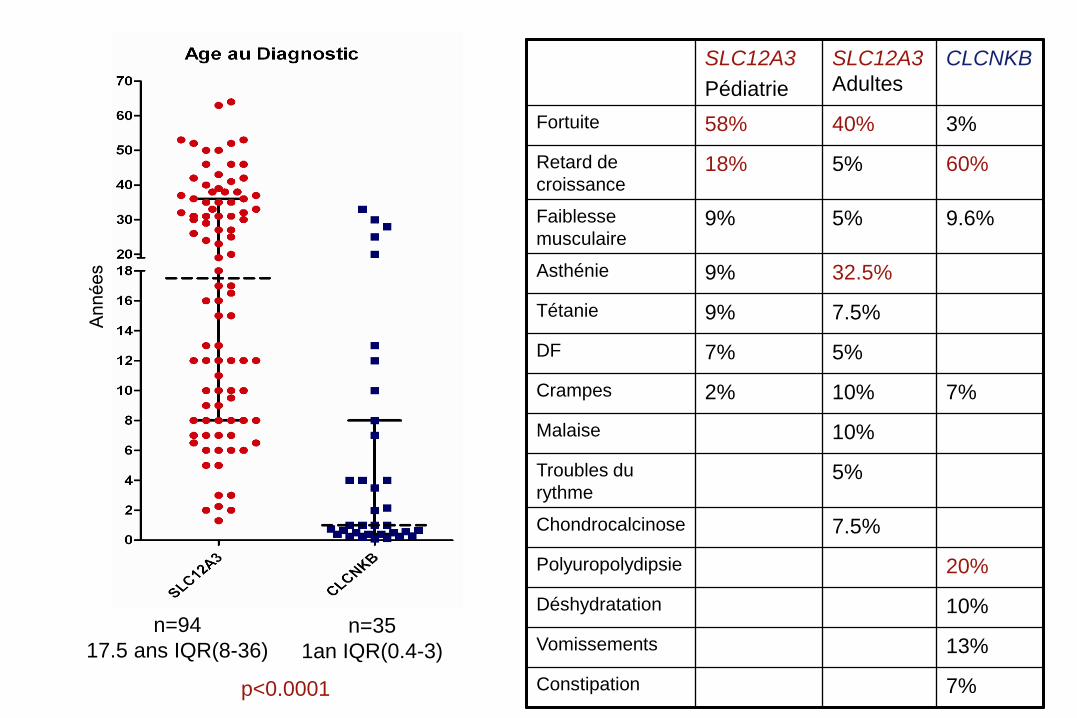
Pédiatrie
SLC12A3
Adultes
CLCNKB
Fortuite 58% 40% 3%
Retard de
croissance 18% 5% 60%
Faiblesse
musculaire 9% 5% 9.6%
Asthénie 9% 32.5%
Tétanie 9% 7.5%
DF 7% 5%
Crampes 2% 10% 7%
Malaise 10%
Troubles du
rythme 5%
Chondrocalcinose 7.5%
Polyuropolydipsie 20%
Déshydratation 10%
Vomissements 13%
Constipation 7%
n=94
17.5 ans IQR(8-36) n=35
1an IQR(0.4-3)
p<0.0001

n=85, Med. IQR
30 (28-32) n=25, Med. IQR
32.9 (28.5-36)
n=61, Med. IQR
97 (94.5-99)
n=25, Med. IQR
89 (80-96.5)
p=0.037 p<0.0001
n=89, Med. IQR
0.59 (0.51-0.68)
n=26, Med. IQR
0.87 (0.77-0.96) n=81, Med. IQR
0.05 (0.03-0.11) n=21, Med. IQR
0.62 (0.23-1.14)
p<0.0001
p<0.0001
Bartter anténatal

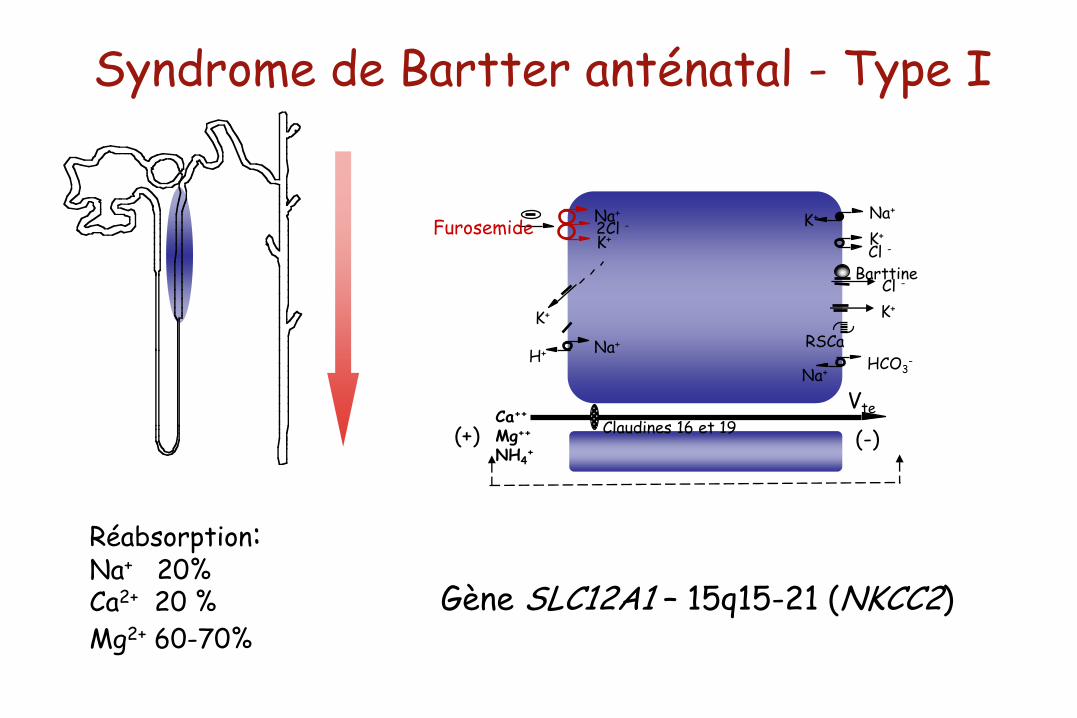
Syndrome de Bartter anténatal - Type I
Vte
Na+
K+ 2Cl -
Na+ K+
K+
Furosemide
Na+ H+
K+
Cl -
Cl -
Na+ HCO3
-
Ca++ Mg++ NH4
+ (-) (+)
K+
Claudines 16 et 19
RSCa
Barttine
Gène SLC12A1 – 15q15-21 (NKCC2)
Réabsorption: Na+ 20% Ca2+ 20 %
Mg2+ 60-70%
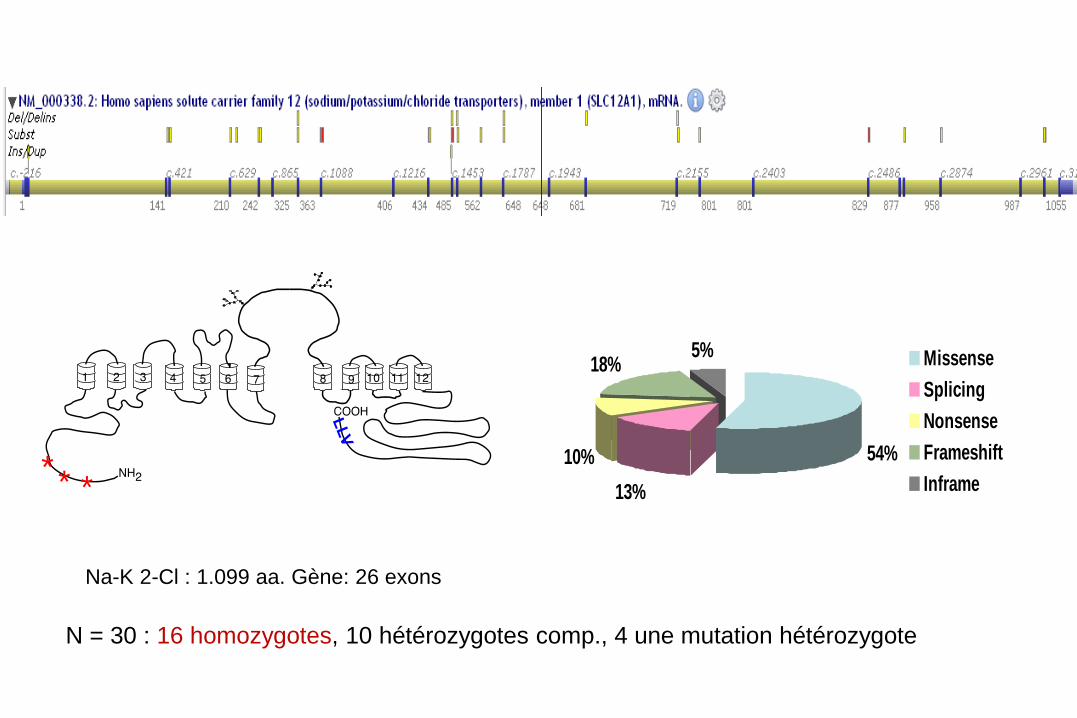
Na-K 2-Cl : 1.099 aa. Gène: 26 exons
54%
13%
10%
18%5% Missense
Splicing
Nonsense
Frameshift
Inframe
N = 30 : 16 homozygotes, 10 hétérozygotes comp., 4 une mutation hétérozygote
* * *
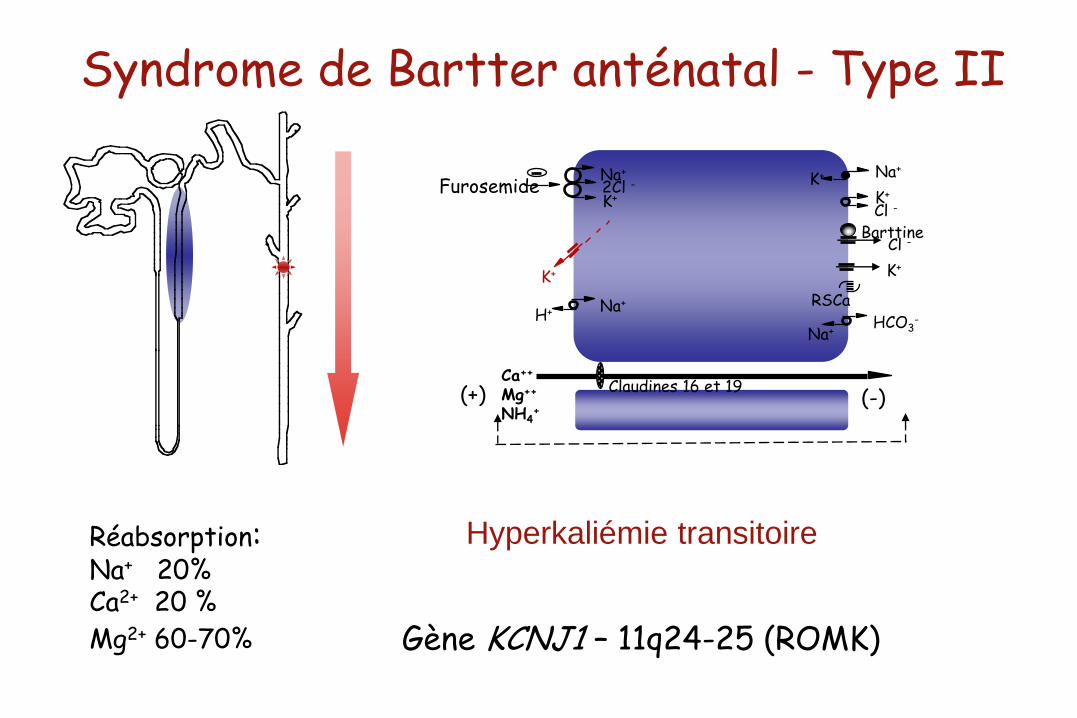
Syndrome de Bartter anténatal - Type II
Gène KCNJ1 – 11q24-25 (ROMK)
Na+
K+ 2Cl -
Na+ K+
K+
Furosemide
Na+ H+
K+
Cl -
Cl -
Na+ HCO3
-
Ca++ Mg++ NH4
+ (-) (+)
K+
Claudines 16 et 19
RSCa
Barttine
Réabsorption: Na+ 20% Ca2+ 20 %
Mg2+ 60-70%
Hyperkaliémie transitoire

Evolution Ionogramme – Bartter de type II
60
80
100
120
140
160
0 2 4 6 8 10 12 14 16 18 20 22 24
Na
Cl
0
2,5
5
7,5
10
12,5
15
17,5
20
22,5
25
27,5
30
0 2 4 6 8 10 12 14 16 18 20 22 24
Jours
K
RA
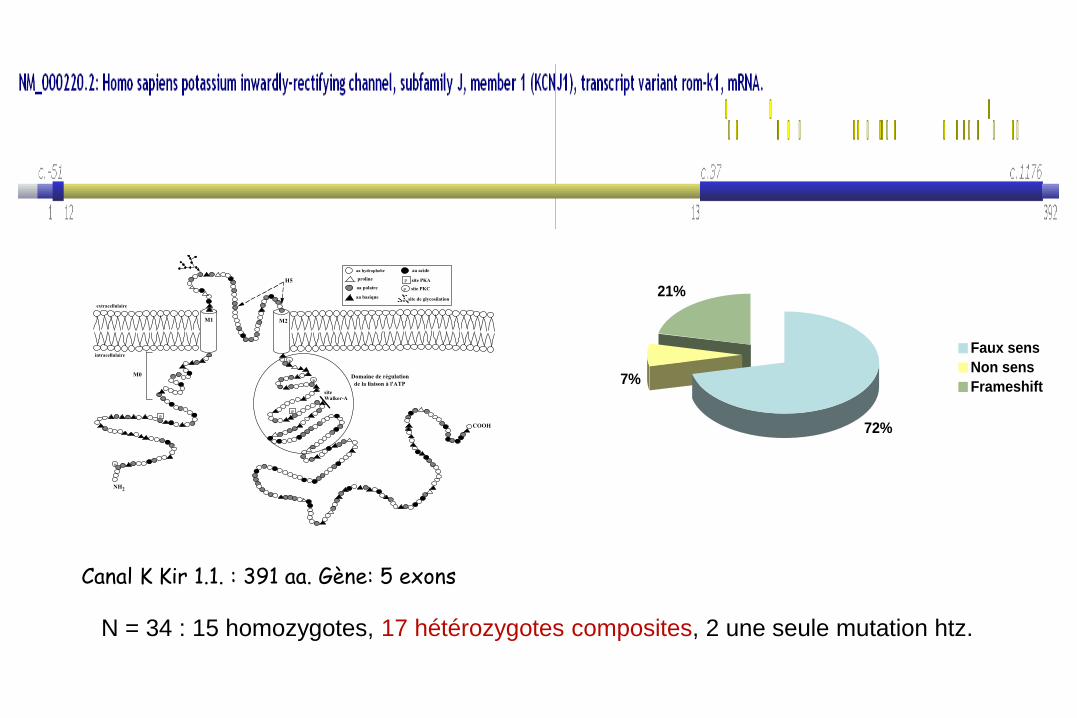
Canal K Kir 1.1. : 391 aa. Gène: 5 exons
72%
7%
21%
Faux sens
Non sens
Frameshift
N = 34 : 15 homozygotes, 17 hétérozygotes composites, 2 une seule mutation htz.
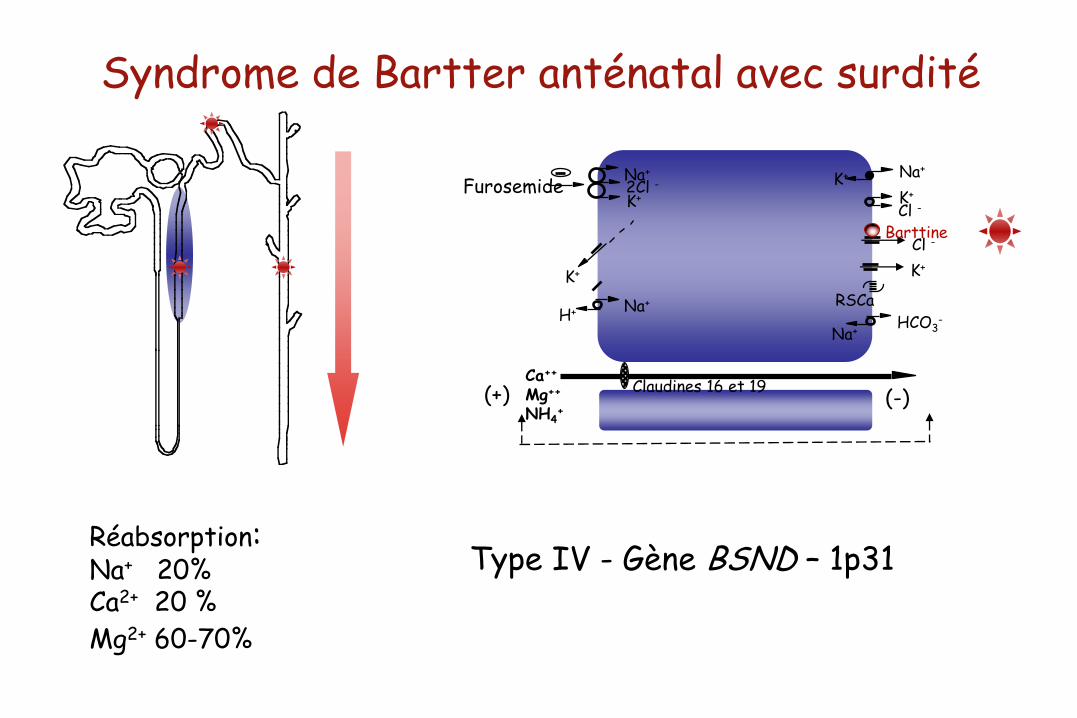
Syndrome de Bartter anténatal avec surdité
Type IV - Gène BSND – 1p31
Na+
K+ 2Cl -
Na+ K+
K+
Furosemide
Na+ H+
K+
Cl -
Cl -
Na+ HCO3
-
Ca++ Mg++ NH4
+ (-) (+)
K+
Claudines 16 et 19
RSCa
Barttine
Réabsorption: Na+ 20% Ca2+ 20 %
Mg2+ 60-70%
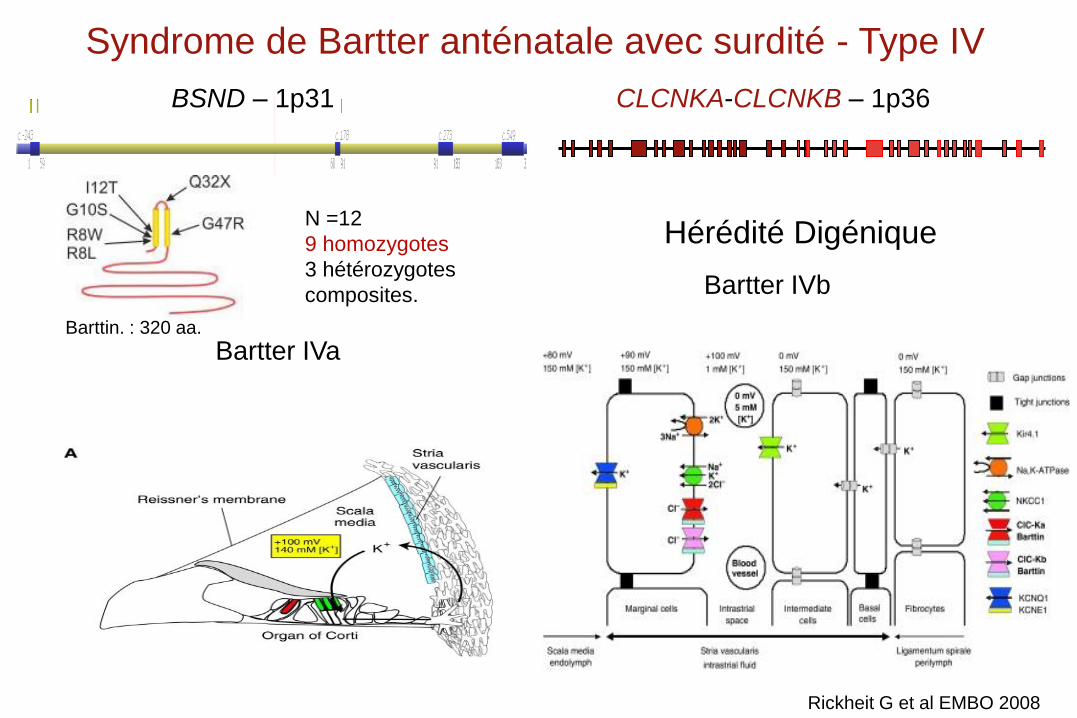
Barttin. : 320 aa.
N =12
9 homozygotes
3 hétérozygotes
composites.
Syndrome de Bartter anténatale avec surdité - Type IV
BSND – 1p31
Bartter IVa
CLCNKA-CLCNKB – 1p36
Hérédité Digénique
Bartter IVb
Rickheit G et al EMBO 2008
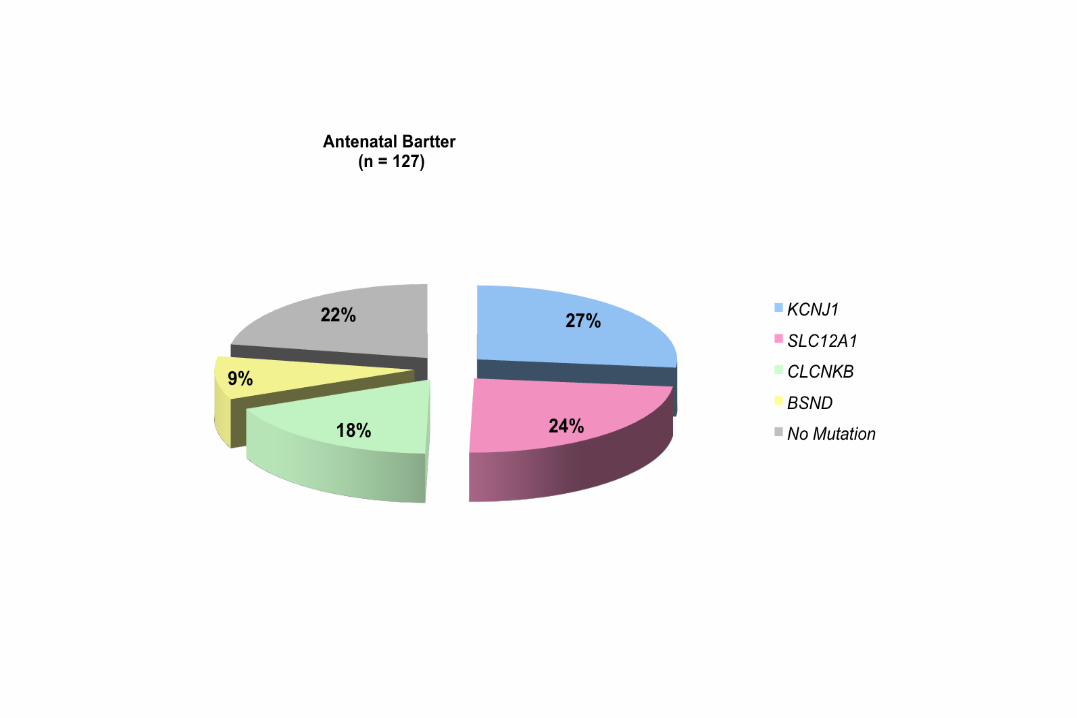
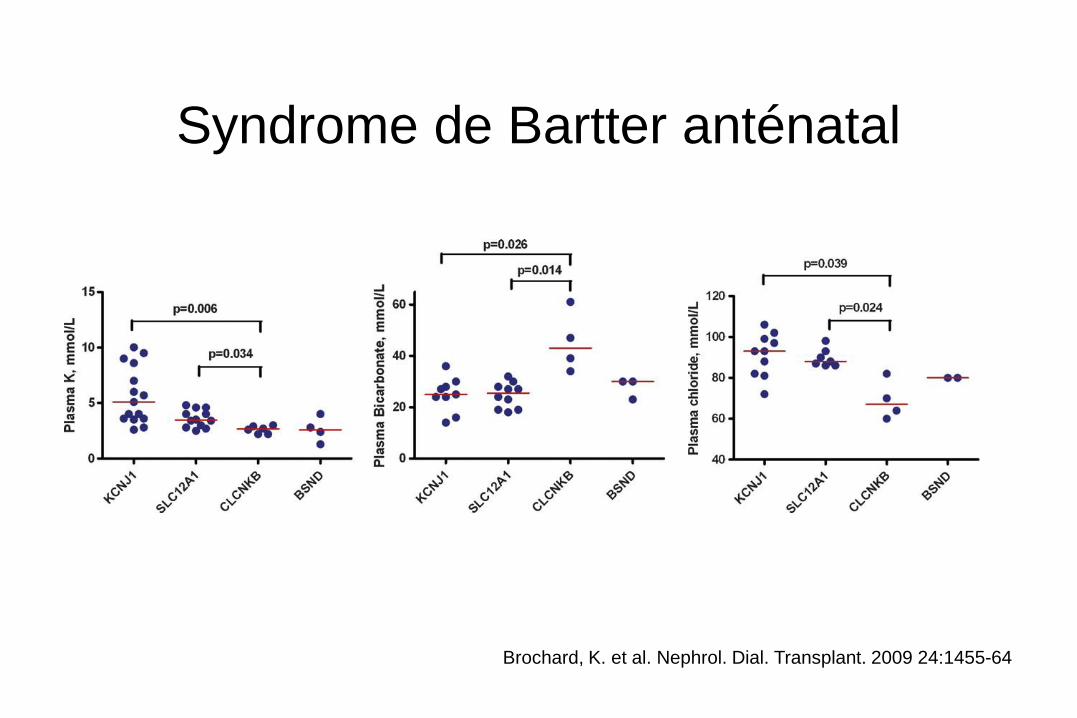
Syndrome de Bartter anténatal
Brochard, K. et al. Nephrol. Dial. Transplant. 2009 24:1455-64
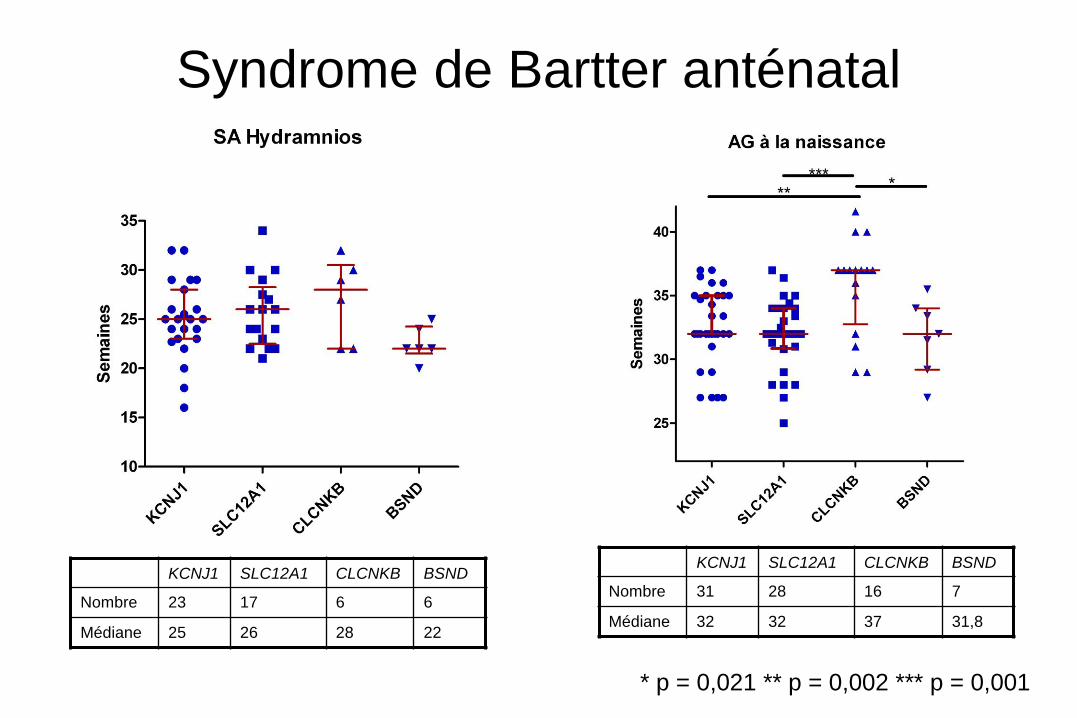
Syndrome de Bartter anténatal
KCNJ1 SLC12A1 CLCNKB BSND
Nombre 23 17 6 6
Médiane 25 26 28 22
KCNJ1 SLC12A1 CLCNKB BSND
Nombre 31 28 16 7
Médiane 32 32 37 31,8
* p = 0,021 ** p = 0,002 *** p = 0,001
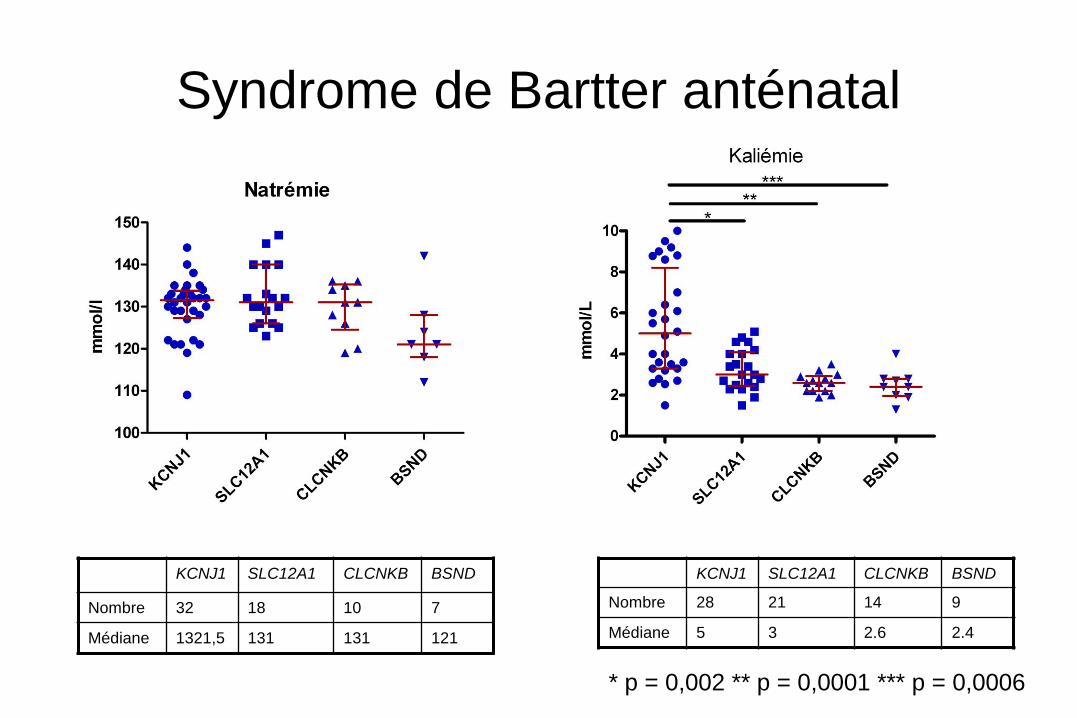
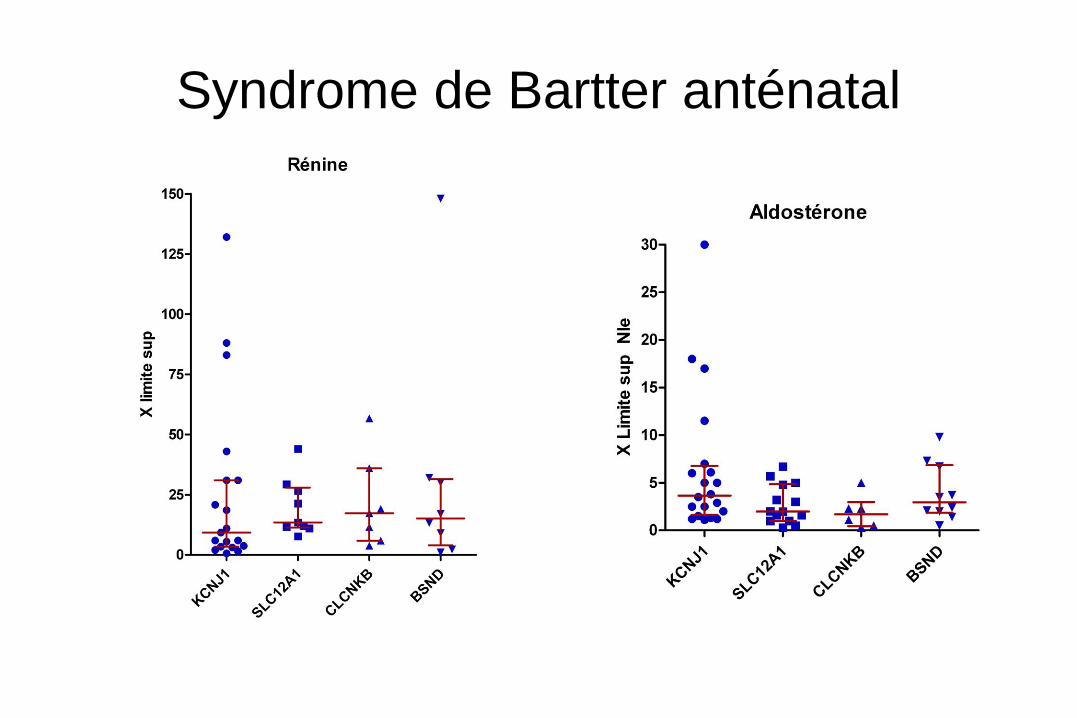
Syndrome de Bartter anténatal
KCNJ1 SLC12A1 CLCNKB BSND
Nombre 32 18 10 7
Médiane 1321,5 131 131 121
KCNJ1 SLC12A1 CLCNKB BSND
Nombre 28 21 14 9
Médiane 5 3 2.6 2.4
* p = 0,002 ** p = 0,0001 *** p = 0,0006
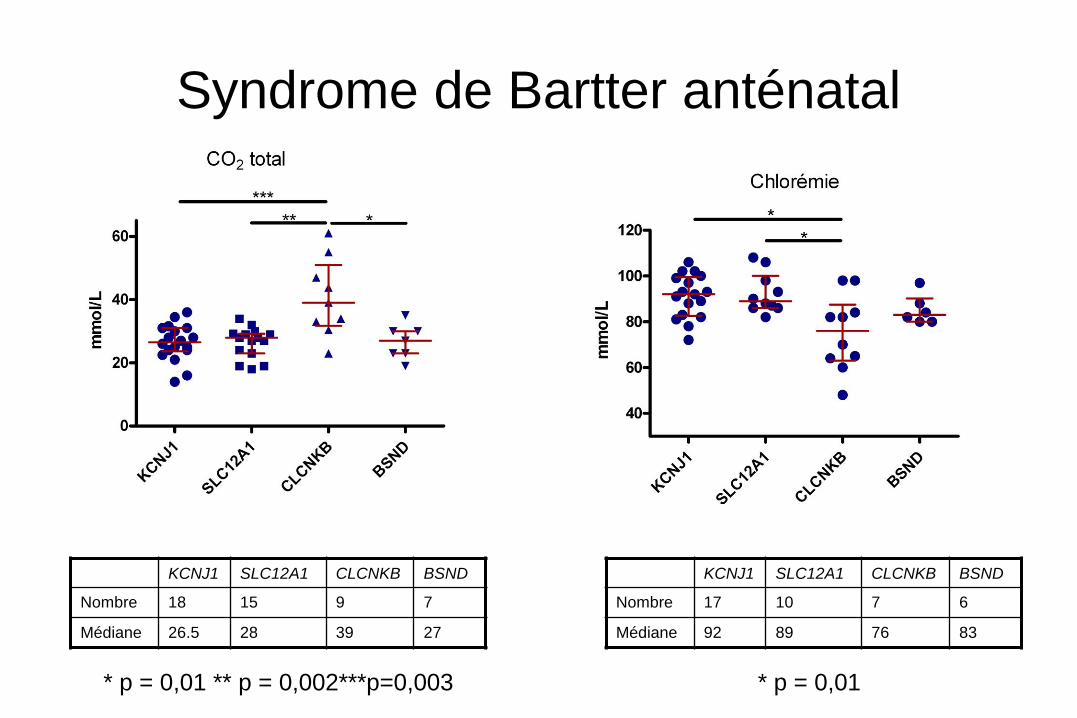
Syndrome de Bartter anténatal
KCNJ1 SLC12A1 CLCNKB BSND
Nombre 18 15 9 7
Médiane 26.5 28 39 27
KCNJ1 SLC12A1 CLCNKB BSND
Nombre 17 10 7 6
Médiane 92 89 76 83
* p = 0,01 * p = 0,01 ** p = 0,002***p=0,003
Syndrome de Bartter anténatal
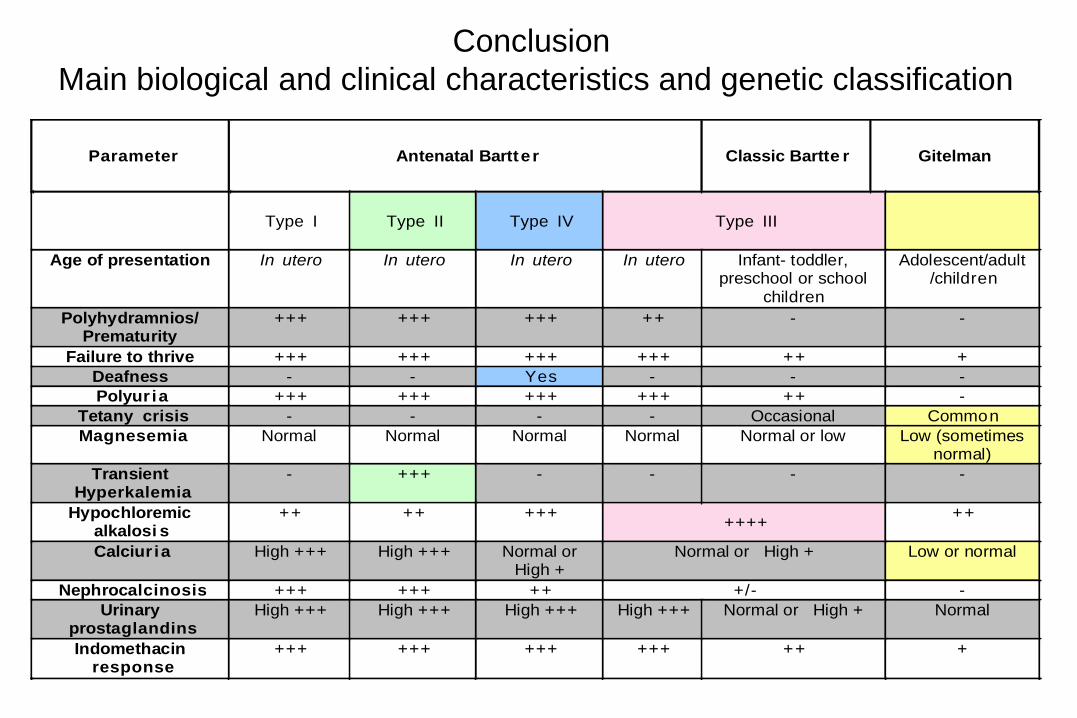
Parameter Antenatal Bartter Classic Bartte r Gitelman
Type I Type II Type IV Type III
Age of presentation In utero In utero In utero In utero Infant- toddler, preschool or school
children
Adolescent/adult /children
Polyhydramnios/ Prematurity
+++ +++ +++ ++ - -
Failure to thrive +++ +++ +++ +++ ++ + Deafness - - Yes - - - Polyur ia +++ +++ +++ +++ ++ -
Tetany crisis - - - - Occasional CommonMagnesemia Normal Normal Normal Normal Normal or low Low (sometimes
normal) Transient
Hyperkalemia - +++ - - - -
Hypochloremic alkalosi s
++ ++ +++++++
++
Calciur ia High +++ High +++ Normal or High +
Normal or High + Low or normal
Nephrocalcinosis +++ +++ ++ +/- - Urinary
prostaglandins High +++ High +++ High +++ High +++ Normal or High + Normal
Indomethacin response
+++ +++ +++ +++ ++ +
Conclusion
Main biological and clinical characteristics and genetic classification
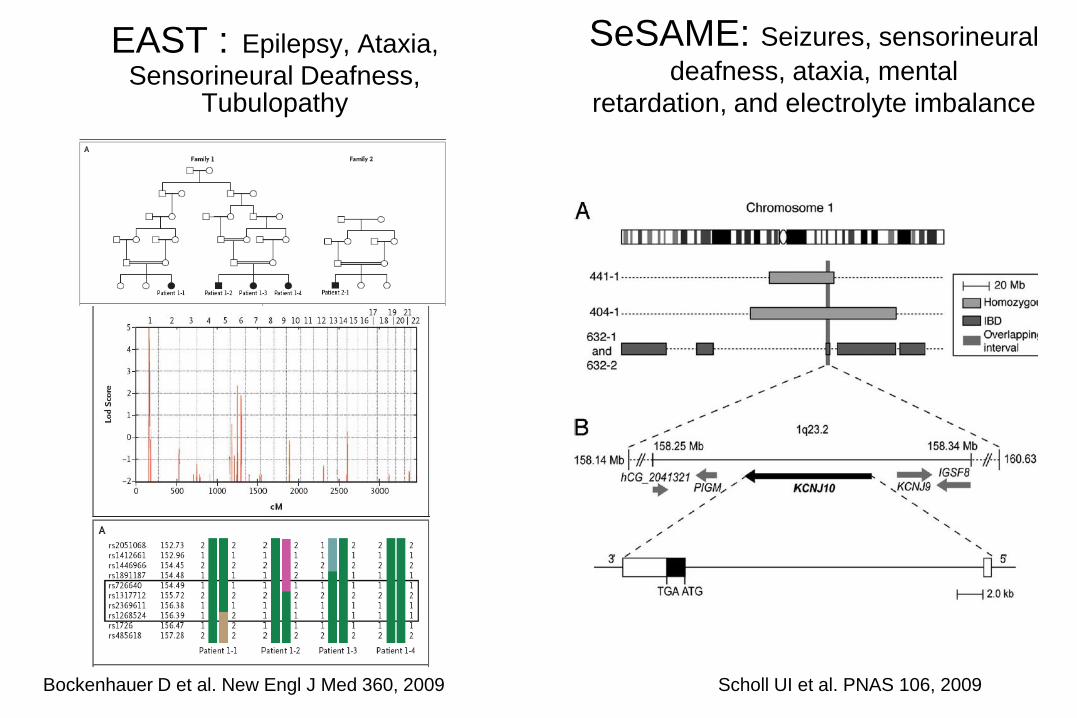
EAST : Epilepsy, Ataxia,
Sensorineural Deafness, Tubulopathy
Scholl UI et al. PNAS 106, 2009 Bockenhauer D et al. New Engl J Med 360, 2009
SeSAME: Seizures, sensorineural deafness, ataxia, mental
retardation, and electrolyte imbalance
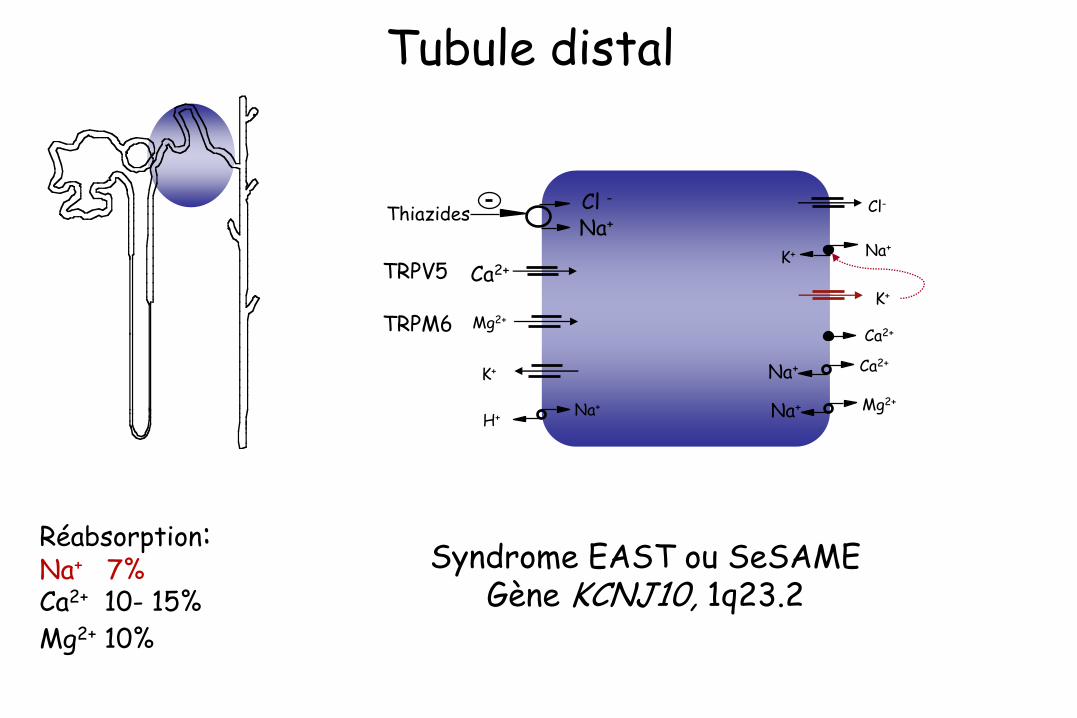
Tubule distal
Ca2+
Na+
Cl - Thiazides
Na+ K+
Na+
H+
Mg2+
Na+ Mg2+
Cl-
Réabsorption: Na+ 7% Ca2+ 10- 15%
Mg2+ 10%
TRPV5
TRPM6
K+
Ca2+
K+
Syndrome EAST ou SeSAME Gène KCNJ10, 1q23.2
Na+ Ca2+
H2O
H2O
Na +
K+ Aldostérone
K+
RM
ENaC
Cl-
K+
H+
CO2 H2O
HCO3 H+ HCO3
-
Na +
ACII
H+
(-) (+)
H+
K+
Na +
K+
Na + Cl-
HCO3-
Cl- HCO3
-
Cl-
Cl-
HCO3-
Na +
Intercalaire
B
Thiazides
Ca2+
Na+ Cl -
Na+
Ca2+
Na+
K+
Ca2+
Na+ H+
Mg2+ Na+
Na+ Mg2+
Cl-
Furosémide Na+
K+
2Cl - Na+
K+
K+
Na+ H+
K+
Cl -
Cl -
Na+ HCO3
-
Ca++
Mg++
NH4+
(-) (+) Vte
K+
Claudines
Barttine
Intercalaire
A
Principale
Amiloride
Spironolactone
Eplérenone
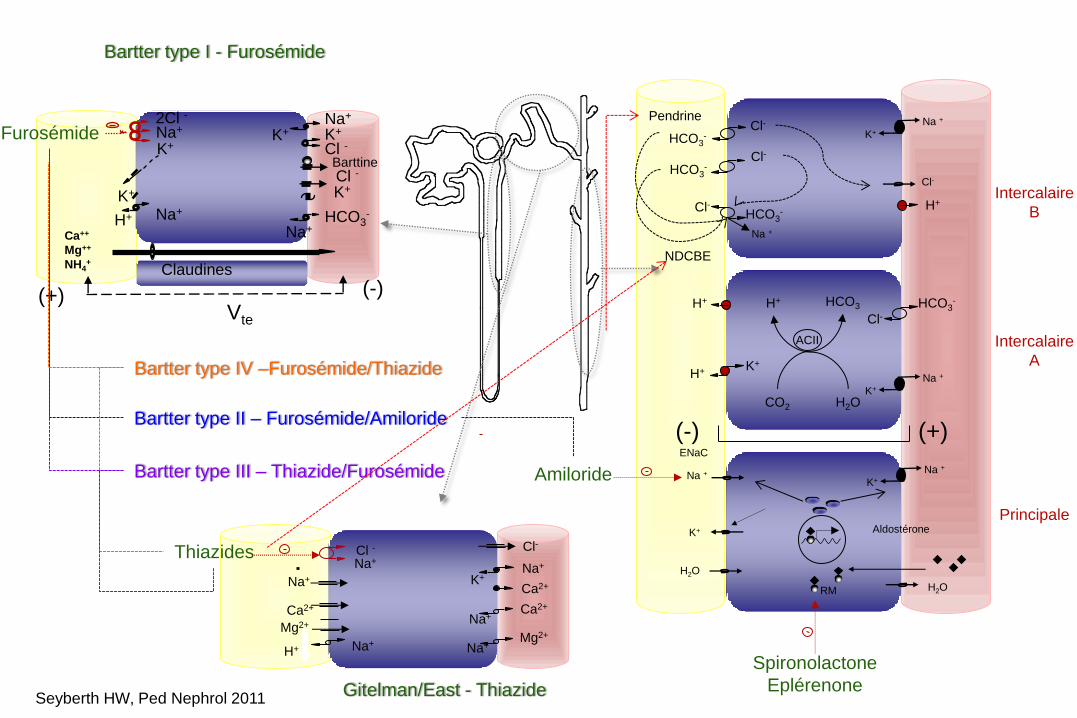
Bartter type I - Furosémide
Gitelman/East - Thiazide
Bartter type II – Furosémide/Amiloride
Bartter type III – Thiazide/Furosémide
Bartter type IV –Furosémide/Thiazide
Pendrine
NDCBE
Seyberth HW, Ped Nephrol 2011
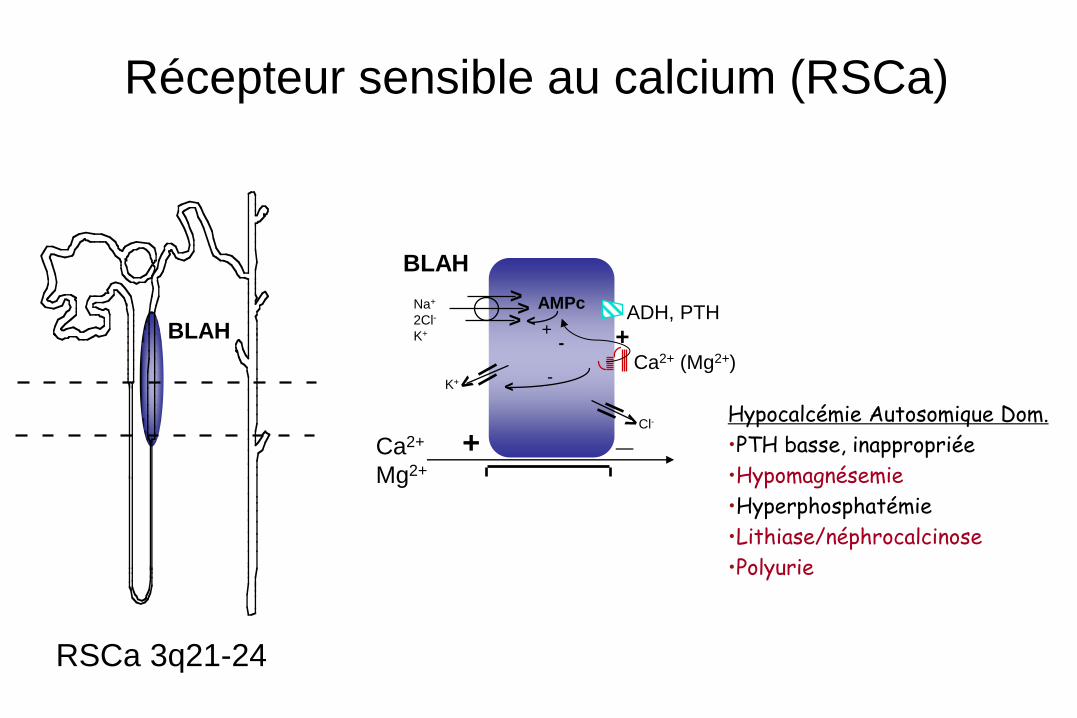
Récepteur sensible au calcium (RSCa)
BLAH
Ca2+
Mg2+
BLAH
ADH, PTH
Ca2+ (Mg2+)
AMPc
+ -
Na+
2Cl-
K+
- K+
Cl-
+ _
+
> >
>
RSCa 3q21-24
Hypocalcémie Autosomique Dom.
•PTH basse, inappropriée
•Hypomagnésemie
•Hyperphosphatémie
•Lithiase/néphrocalcinose
•Polyurie
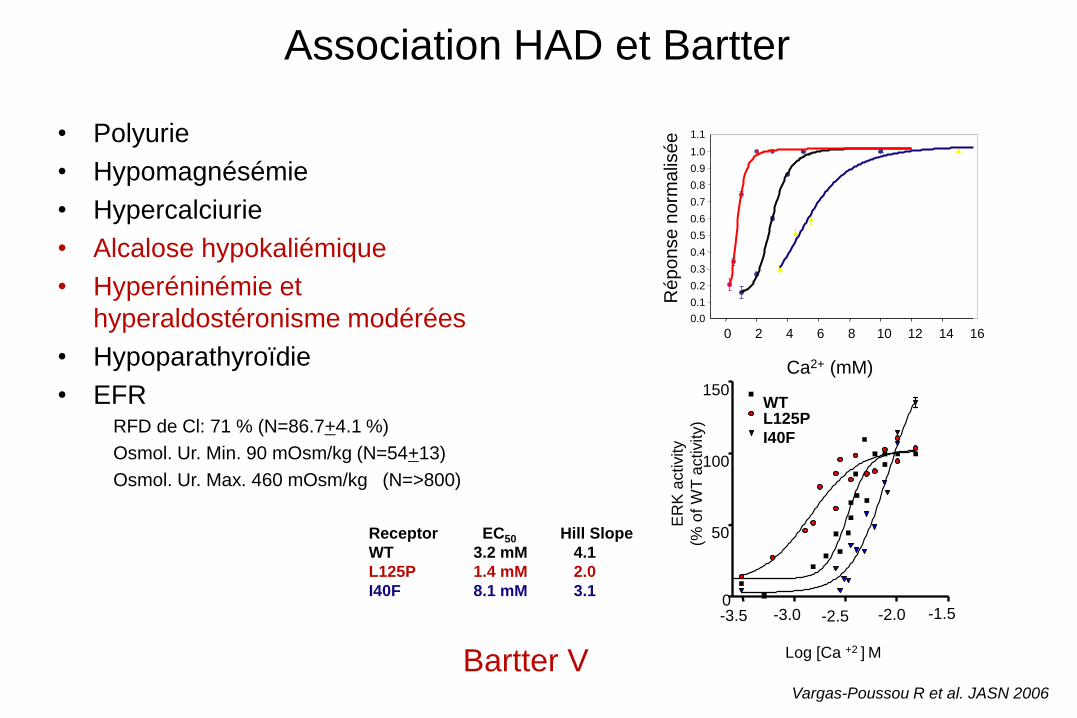
Association HAD et Bartter
• Polyurie
• Hypomagnésémie
• Hypercalciurie
• Alcalose hypokaliémique
• Hyperéninémie et
hyperaldostéronisme modérées
• Hypoparathyroïdie
• EFR RFD de Cl: 71 % (N=86.7+4.1 %)
Osmol. Ur. Min. 90 mOsm/kg (N=54+13)
Osmol. Ur. Max. 460 mOsm/kg (N=>800)
0 2 4 6 8 10 12 14 16
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
1.1
Ré
po
nse
no
rma
lisé
e
Ca2+ (mM)
ER
K a
ctivity
(% o
f W
T a
ctivity)
150
100
50
0 -3.5 -3.0 -2.5 -2.0 -1.5
Log [Ca +2 ] M
WT L125P
I40F
Receptor EC50 Hill Slope WT 3.2 mM 4.1 L125P 1.4 mM 2.0 I40F 8.1 mM 3.1
Bartter V Vargas-Poussou R et al. JASN 2006
Diagnostic différentiel – Dossier 1
• Dossier et prélèvement adressés pour diagnostique
génétique d’un pseudohypoaldostéronisme de type 1
• Fille née le 22/03/2008, prématurée - 35 SA. Grossesse
compliqué par hydramnios. PN:1.92kg TN: 44.5 cm
• A J6 Tableau de déshydratation avec hyponatrémie,
hyperkaliémie et polyurie
• Prélèvements pour bilan hormonal et début d’un traitement
par fludrocortisone
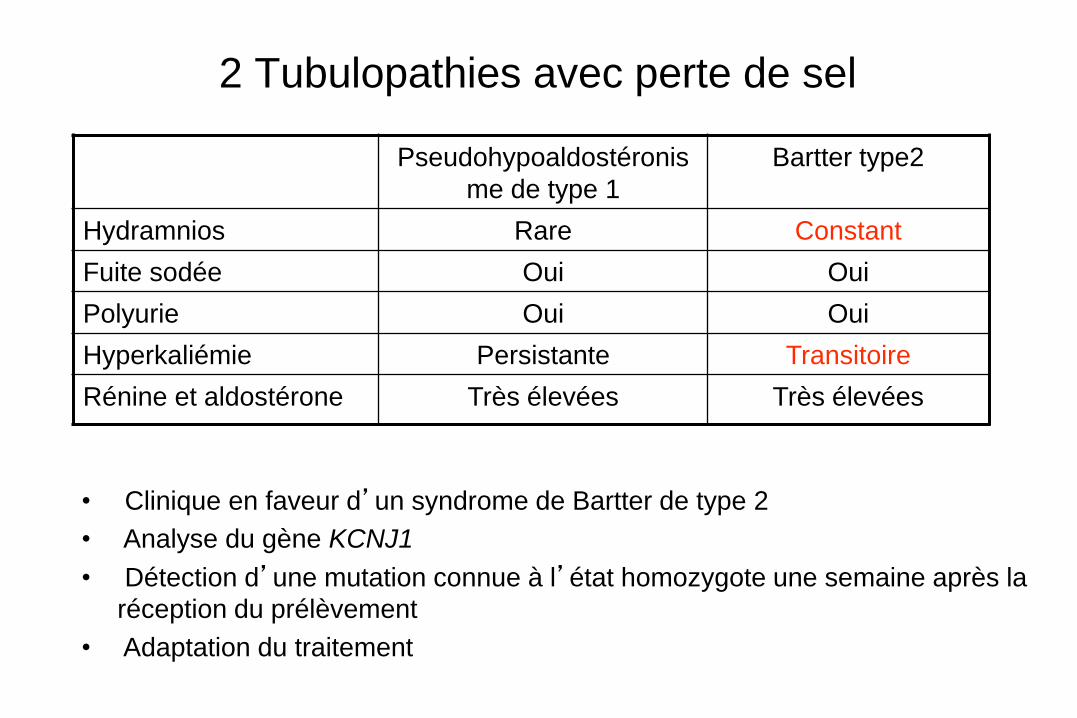
2 Tubulopathies avec perte de sel
Pseudohypoaldostéronis
me de type 1
Bartter type2
Hydramnios Rare Constant
Fuite sodée Oui Oui
Polyurie Oui Oui
Hyperkaliémie Persistante Transitoire
Rénine et aldostérone Très élevées Très élevées
• Clinique en faveur d’un syndrome de Bartter de type 2
• Analyse du gène KCNJ1
• Détection d’une mutation connue à l’état homozygote une semaine après la
réception du prélèvement
• Adaptation du traitement
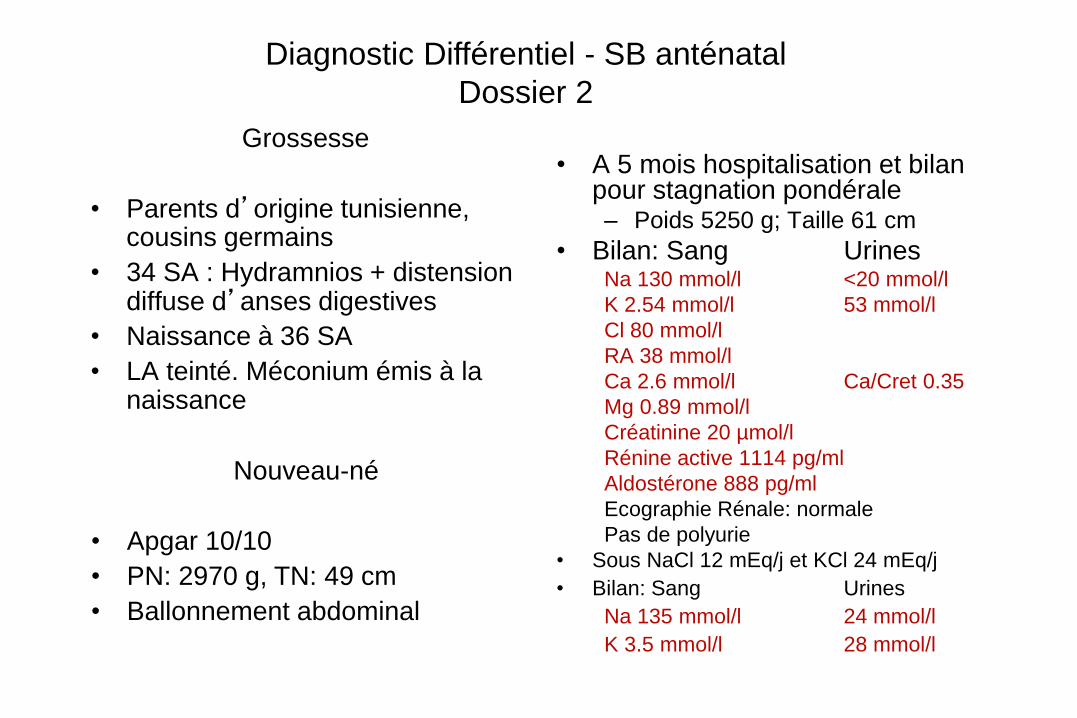
Grossesse
• Parents d’origine tunisienne, cousins germains
• 34 SA : Hydramnios + distension diffuse d’anses digestives
• Naissance à 36 SA
• LA teinté. Méconium émis à la naissance
• A 5 mois hospitalisation et bilan pour stagnation pondérale – Poids 5250 g; Taille 61 cm
• Bilan: Sang Urines Na 130 mmol/l <20 mmol/l
K 2.54 mmol/l 53 mmol/l
Cl 80 mmol/l
RA 38 mmol/l
Ca 2.6 mmol/l Ca/Cret 0.35
Mg 0.89 mmol/l
Créatinine 20 µmol/l
Rénine active 1114 pg/ml
Aldostérone 888 pg/ml
Ecographie Rénale: normale
Pas de polyurie
• Sous NaCl 12 mEq/j et KCl 24 mEq/j
• Bilan: Sang Urines
Na 135 mmol/l 24 mmol/l
K 3.5 mmol/l 28 mmol/l
Nouveau-né
• Apgar 10/10
• PN: 2970 g, TN: 49 cm
• Ballonnement abdominal
Diagnostic Différentiel - SB anténatal
Dossier 2
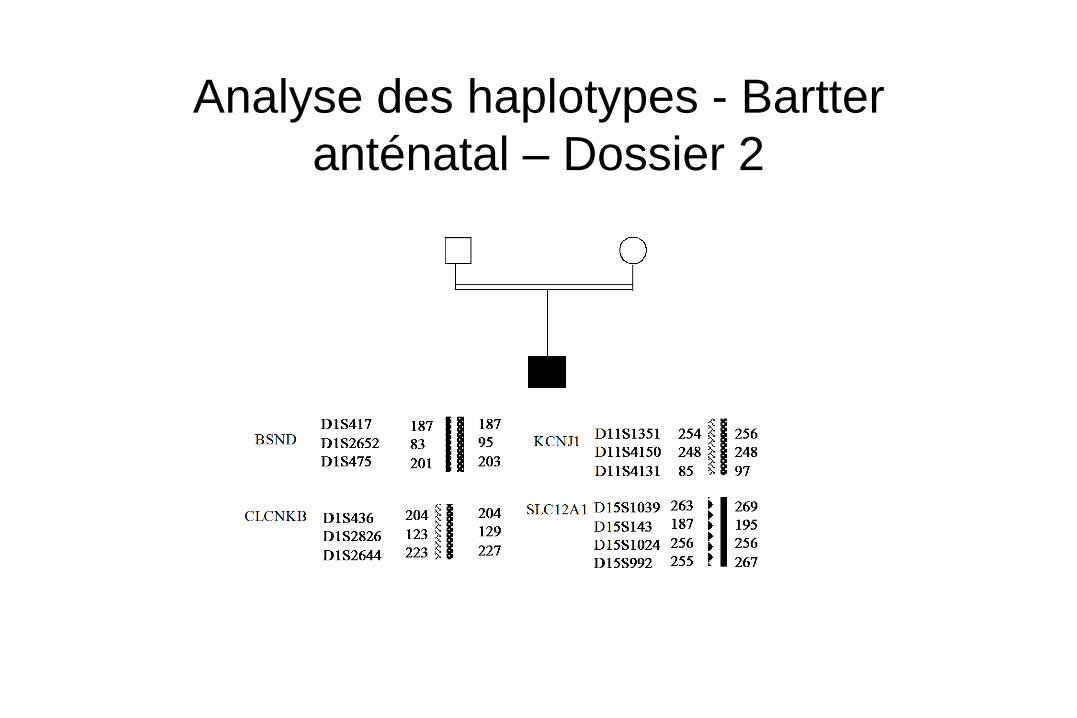
Analyse des haplotypes - Bartter
anténatal – Dossier 2
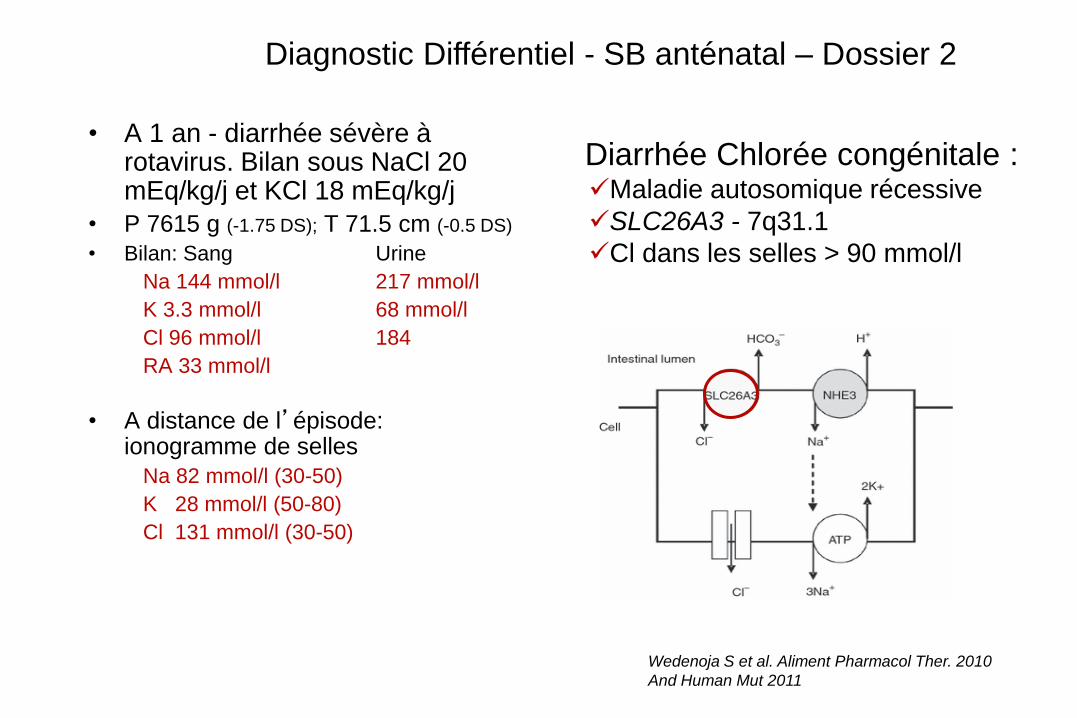
• A 1 an - diarrhée sévère à rotavirus. Bilan sous NaCl 20 mEq/kg/j et KCl 18 mEq/kg/j
• P 7615 g (-1.75 DS); T 71.5 cm (-0.5 DS)
• Bilan: Sang Urine
Na 144 mmol/l 217 mmol/l
K 3.3 mmol/l 68 mmol/l
Cl 96 mmol/l 184
RA 33 mmol/l
• A distance de l’épisode: ionogramme de selles
Na 82 mmol/l (30-50)
K 28 mmol/l (50-80)
Cl 131 mmol/l (30-50)
Diarrhée Chlorée congénitale : Maladie autosomique récessive
SLC26A3 - 7q31.1
Cl dans les selles > 90 mmol/l
Diagnostic Différentiel - SB anténatal – Dossier 2
Wedenoja S et al. Aliment Pharmacol Ther. 2010
And Human Mut 2011
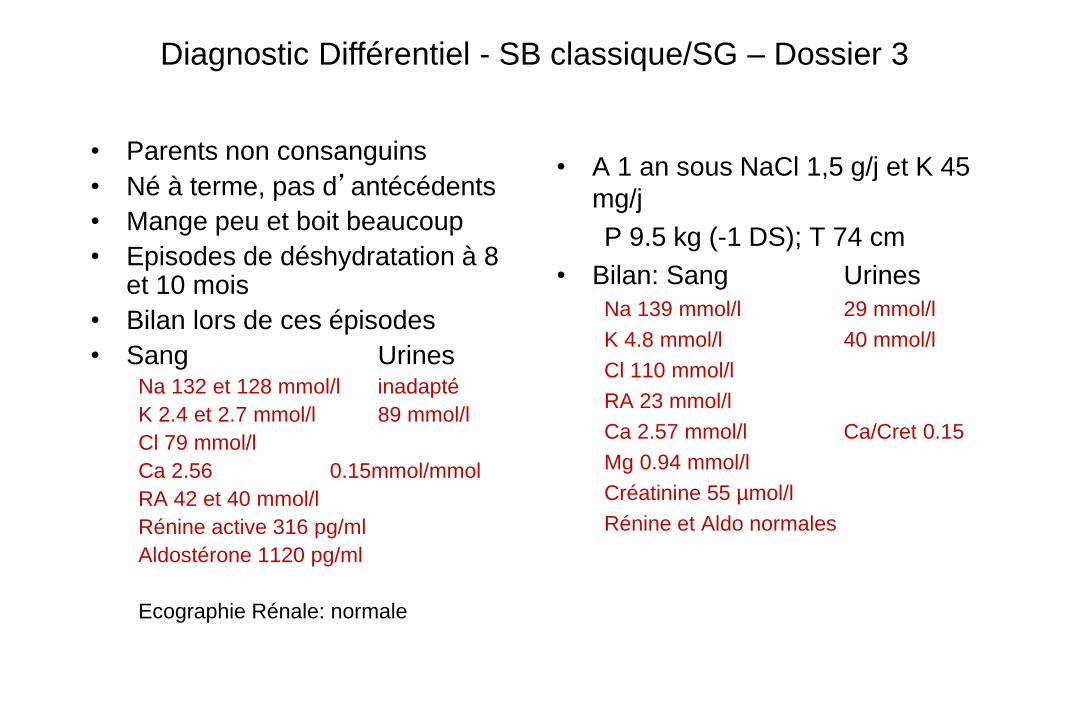
• Parents non consanguins
• Né à terme, pas d’antécédents
• Mange peu et boit beaucoup
• Episodes de déshydratation à 8 et 10 mois
• Bilan lors de ces épisodes
• Sang Urines Na 132 et 128 mmol/l inadapté
K 2.4 et 2.7 mmol/l 89 mmol/l
Cl 79 mmol/l
Ca 2.56 0.15mmol/mmol
RA 42 et 40 mmol/l
Rénine active 316 pg/ml
Aldostérone 1120 pg/ml
Ecographie Rénale: normale
• A 1 an sous NaCl 1,5 g/j et K 45
mg/j
P 9.5 kg (-1 DS); T 74 cm
• Bilan: Sang Urines
Na 139 mmol/l 29 mmol/l
K 4.8 mmol/l 40 mmol/l
Cl 110 mmol/l
RA 23 mmol/l
Ca 2.57 mmol/l Ca/Cret 0.15
Mg 0.94 mmol/l
Créatinine 55 µmol/l
Rénine et Aldo normales
Diagnostic Différentiel - SB classique/SG – Dossier 3
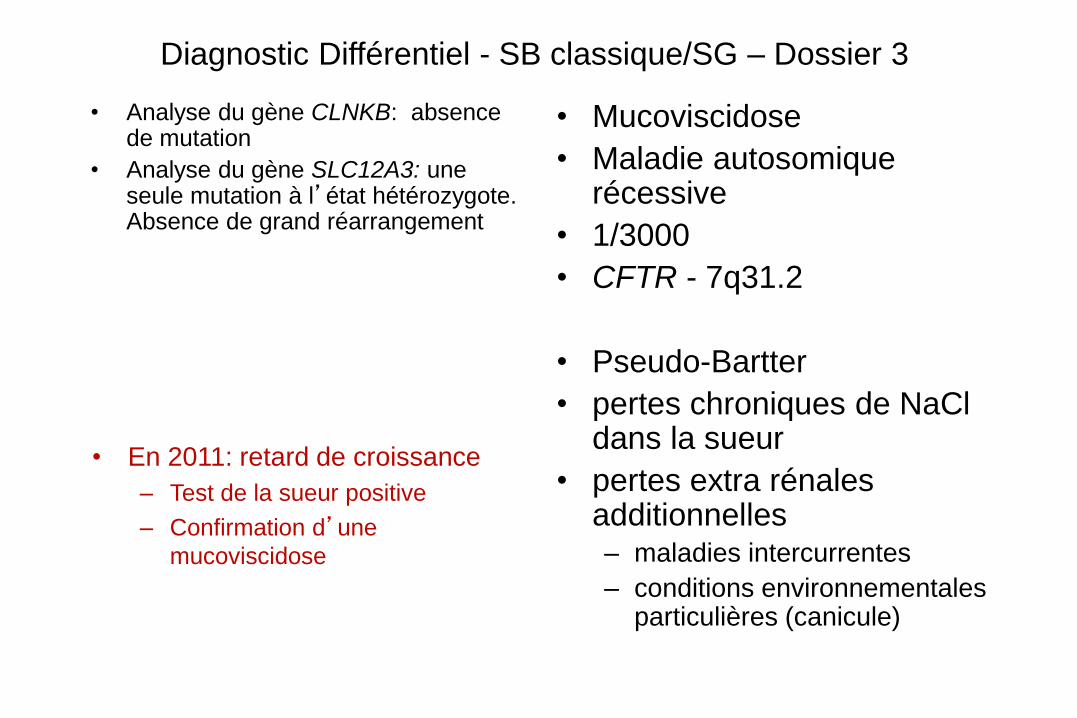
• Analyse du gène CLNKB: absence de mutation
• Analyse du gène SLC12A3: une seule mutation à l’état hétérozygote. Absence de grand réarrangement
• Mucoviscidose
• Maladie autosomique récessive
• 1/3000
• CFTR - 7q31.2
• Pseudo-Bartter
• pertes chroniques de NaCl dans la sueur
• pertes extra rénales additionnelles – maladies intercurrentes
– conditions environnementales particulières (canicule)
• En 2011: retard de croissance
– Test de la sueur positive
– Confirmation d’une
mucoviscidose
Diagnostic Différentiel - SB classique/SG – Dossier 3
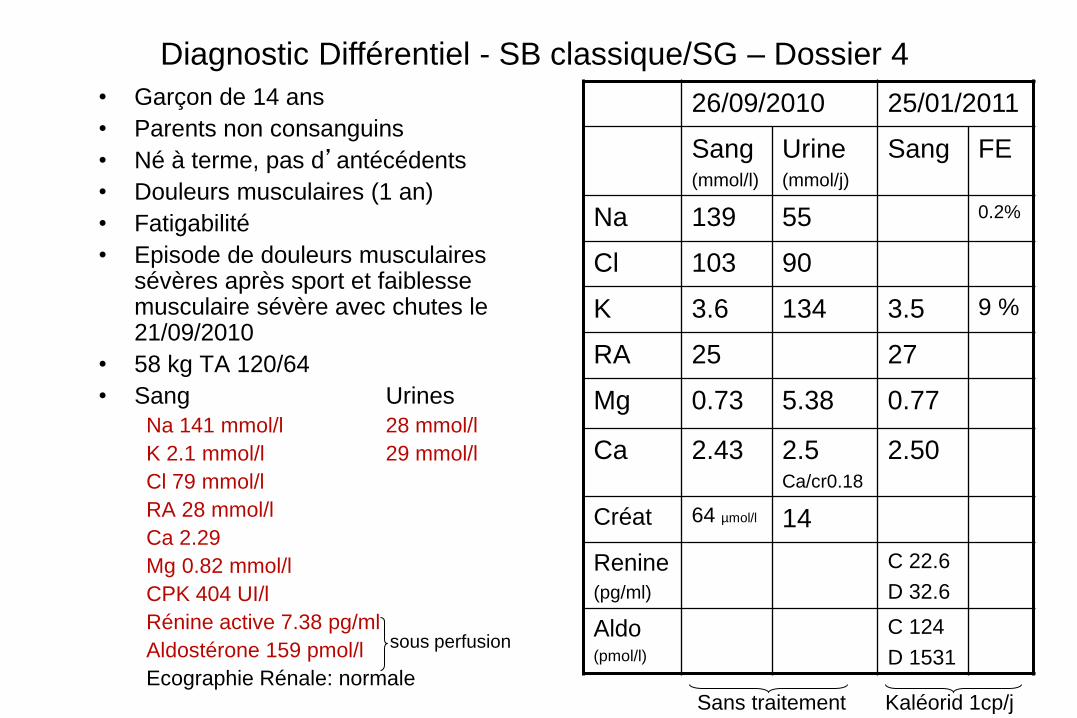
• Garçon de 14 ans
• Parents non consanguins
• Né à terme, pas d’antécédents
• Douleurs musculaires (1 an)
• Fatigabilité
• Episode de douleurs musculaires sévères après sport et faiblesse musculaire sévère avec chutes le 21/09/2010
• 58 kg TA 120/64
• Sang Urines
Na 141 mmol/l 28 mmol/l
K 2.1 mmol/l 29 mmol/l
Cl 79 mmol/l
RA 28 mmol/l
Ca 2.29
Mg 0.82 mmol/l
CPK 404 UI/l
Rénine active 7.38 pg/ml
Aldostérone 159 pmol/l
Ecographie Rénale: normale
sous perfusion
26/09/2010 25/01/2011
Sang (mmol/l)
Urine (mmol/j)
Sang FE
Na 139 55 0.2%
Cl 103 90
K 3.6 134 3.5 9 %
RA 25 27
Mg 0.73 5.38 0.77
Ca 2.43 2.5 Ca/cr0.18
2.50
Créat 64 µmol/l 14
Renine (pg/ml)
C 22.6
D 32.6
Aldo (pmol/l)
C 124
D 1531
Sans traitement Kaléorid 1cp/j
Diagnostic Différentiel - SB classique/SG – Dossier 4
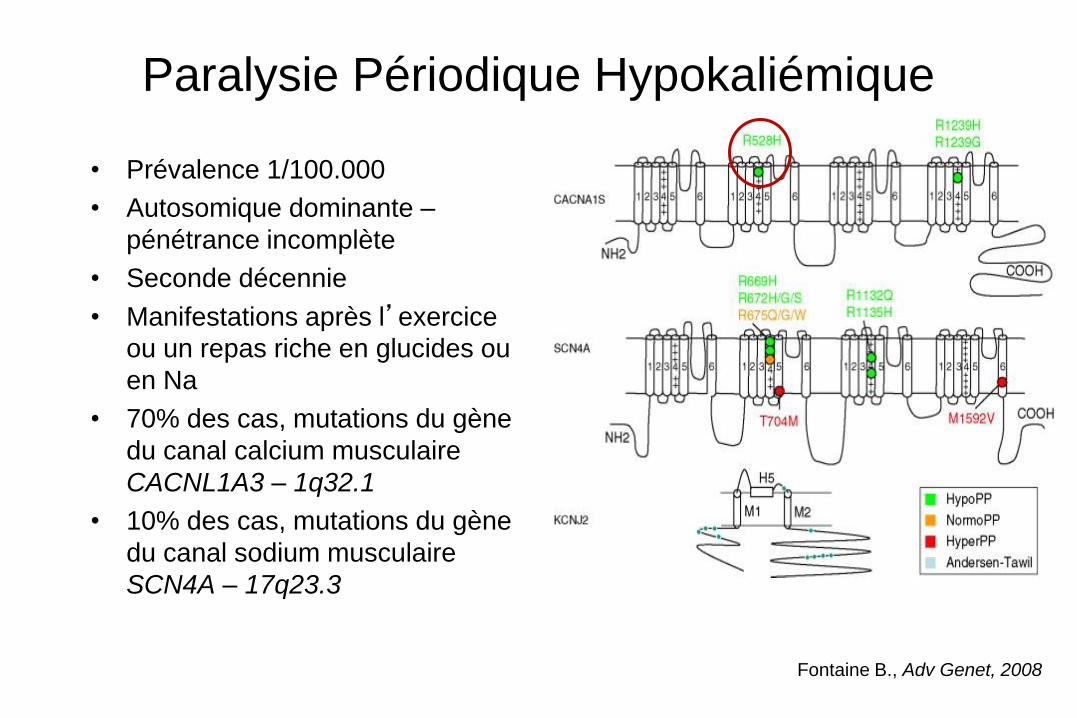
Paralysie Périodique Hypokaliémique
• Prévalence 1/100.000
• Autosomique dominante –
pénétrance incomplète
• Seconde décennie
• Manifestations après l’exercice
ou un repas riche en glucides ou
en Na
• 70% des cas, mutations du gène
du canal calcium musculaire
CACNL1A3 – 1q32.1
• 10% des cas, mutations du gène
du canal sodium musculaire
SCN4A – 17q23.3
Fontaine B., Adv Genet, 2008
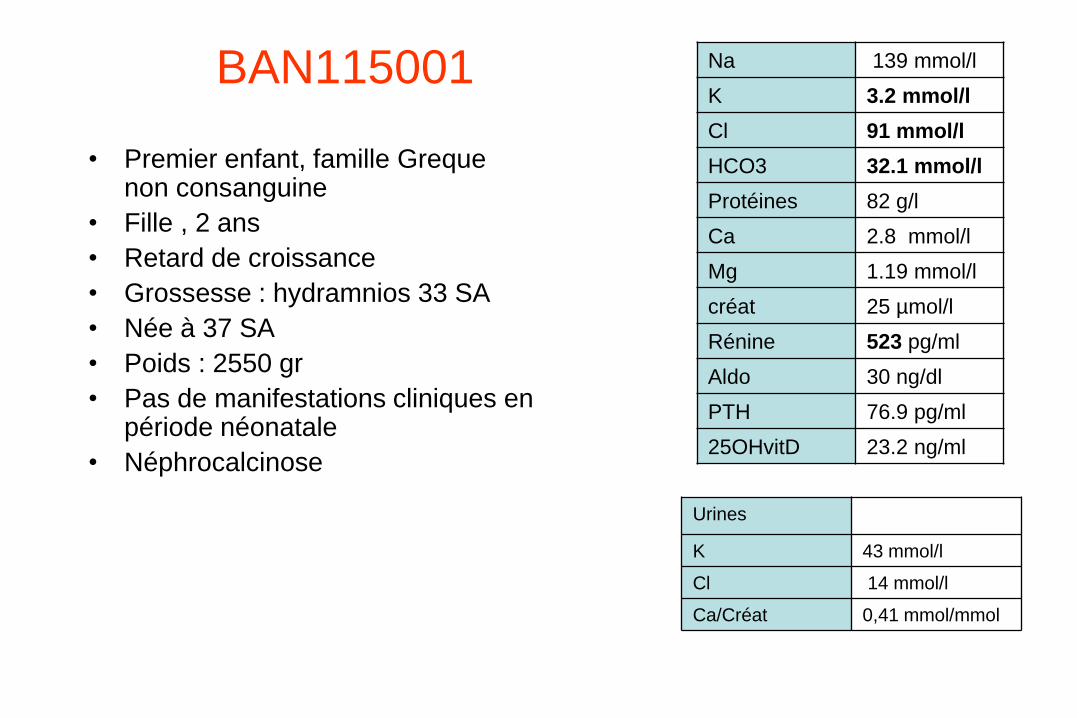
BAN115001
• Premier enfant, famille Greque non consanguine
• Fille , 2 ans
• Retard de croissance
• Grossesse : hydramnios 33 SA
• Née à 37 SA
• Poids : 2550 gr
• Pas de manifestations cliniques en période néonatale
• Néphrocalcinose
Na 139 mmol/l
K 3.2 mmol/l
Cl 91 mmol/l
HCO3 32.1 mmol/l
Protéines 82 g/l
Ca 2.8 mmol/l
Mg 1.19 mmol/l
créat 25 µmol/l
Rénine 523 pg/ml
Aldo 30 ng/dl
PTH 76.9 pg/ml
25OHvitD 23.2 ng/ml
Urines
K 43 mmol/l
Cl 14 mmol/l
Ca/Créat 0,41 mmol/mmol
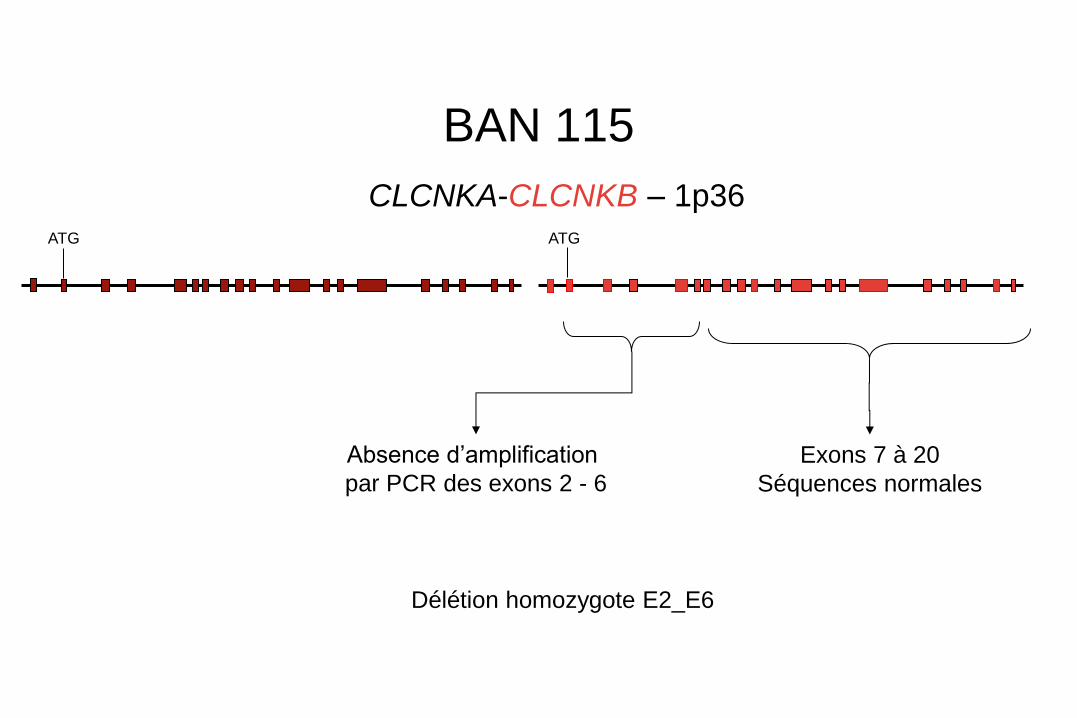
BAN 115
CLCNKA-CLCNKB – 1p36 ATG ATG
Absence d’amplification
par PCR des exons 2 - 6
Exons 7 à 20
Séquences normales
Délétion homozygote E2_E6
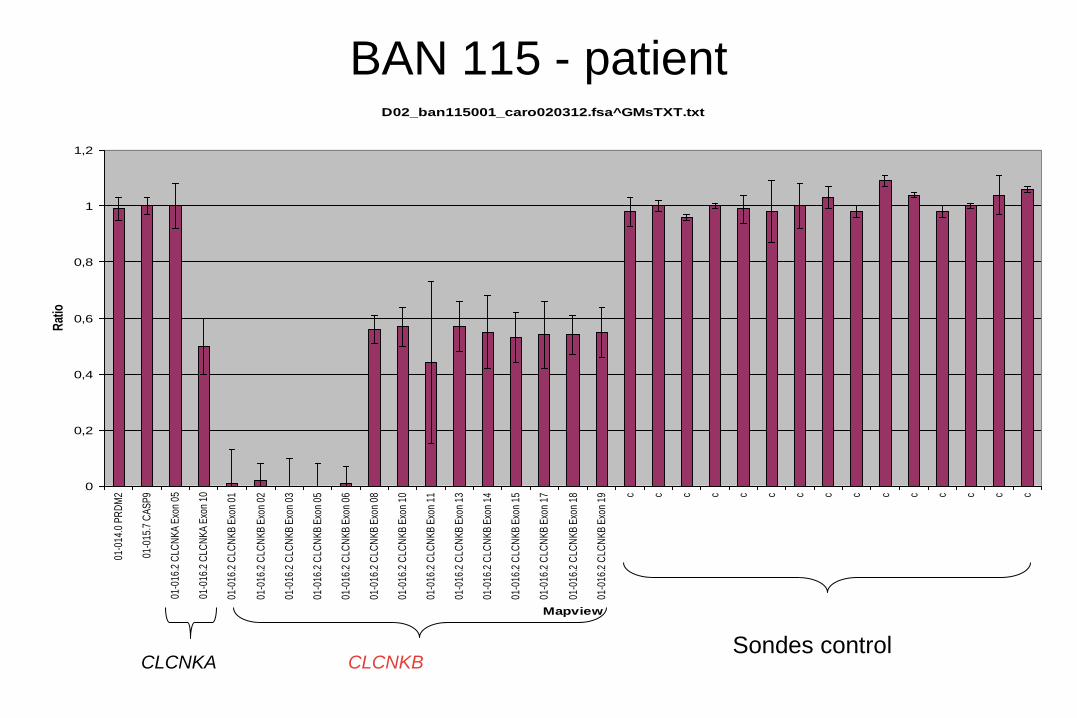
BAN 115 - patient D02_ban115001_caro020312.fsa^GMsTXT.txt
0
0,2
0,4
0,6
0,8
1
1,2
01-0
14.0
PR
DM
2
01-0
15.7
CA
SP
9
01-0
16.2
CLC
NK
A E
xon
05
01-0
16.2
CLC
NK
A E
xon
10
01-0
16.2
CLC
NK
B E
xon
01
01-0
16.2
CLC
NK
B E
xon
02
01-0
16.2
CLC
NK
B E
xon
03
01-0
16.2
CLC
NK
B E
xon
05
01-0
16.2
CLC
NK
B E
xon
06
01-0
16.2
CLC
NK
B E
xon
08
01-0
16.2
CLC
NK
B E
xon
10
01-0
16.2
CLC
NK
B E
xon
11
01-0
16.2
CLC
NK
B E
xon
13
01-0
16.2
CLC
NK
B E
xon
14
01-0
16.2
CLC
NK
B E
xon
15
01-0
16.2
CLC
NK
B E
xon
17
01-0
16.2
CLC
NK
B E
xon
18
01-0
16.2
CLC
NK
B E
xon
19 c c c c c c c c c c c c c c c
Mapview
Rat
io
Sondes control CLCNKA CLCNKB
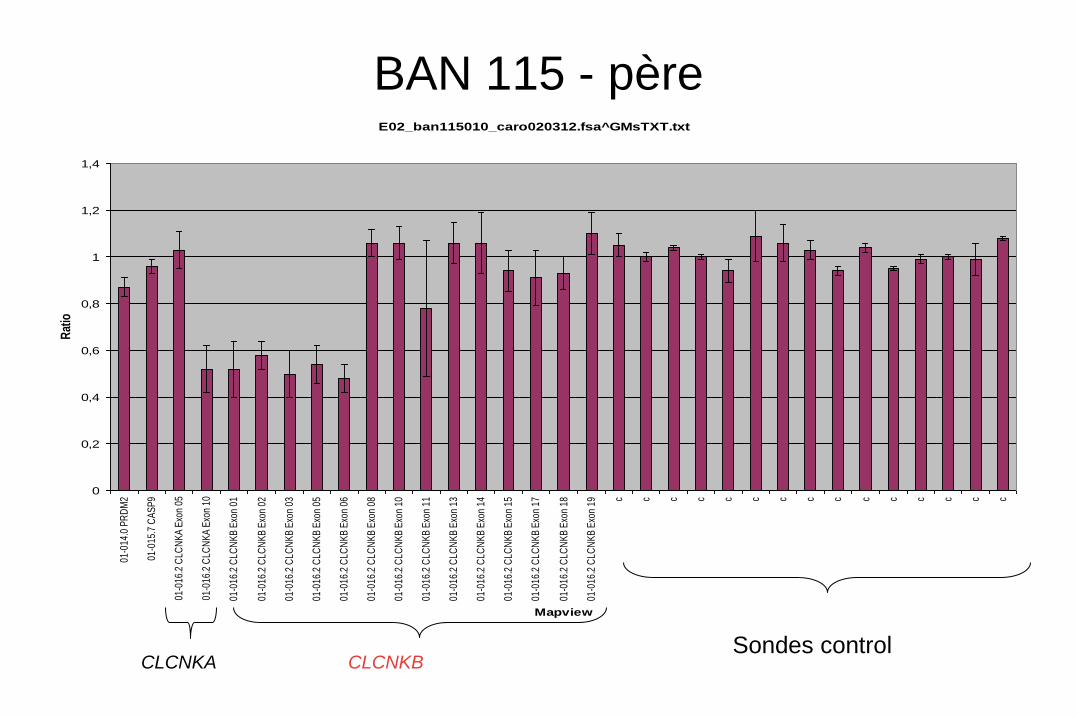
BAN 115 - père
Sondes control CLCNKA CLCNKB
E02_ban115010_caro020312.fsa^GMsTXT.txt
0
0,2
0,4
0,6
0,8
1
1,2
1,4
01-0
14.0
PR
DM
2
01-0
15.7
CA
SP
9
01-0
16.2
CLC
NK
A E
xon
05
01-0
16.2
CLC
NK
A E
xon
10
01-0
16.2
CLC
NK
B E
xon
01
01-0
16.2
CLC
NK
B E
xon
02
01-0
16.2
CLC
NK
B E
xon
03
01-0
16.2
CLC
NK
B E
xon
05
01-0
16.2
CLC
NK
B E
xon
06
01-0
16.2
CLC
NK
B E
xon
08
01-0
16.2
CLC
NK
B E
xon
10
01-0
16.2
CLC
NK
B E
xon
11
01-0
16.2
CLC
NK
B E
xon
13
01-0
16.2
CLC
NK
B E
xon
14
01-0
16.2
CLC
NK
B E
xon
15
01-0
16.2
CLC
NK
B E
xon
17
01-0
16.2
CLC
NK
B E
xon
18
01-0
16.2
CLC
NK
B E
xon
19 c c c c c c c c c c c c c c c
Mapview
Rat
io
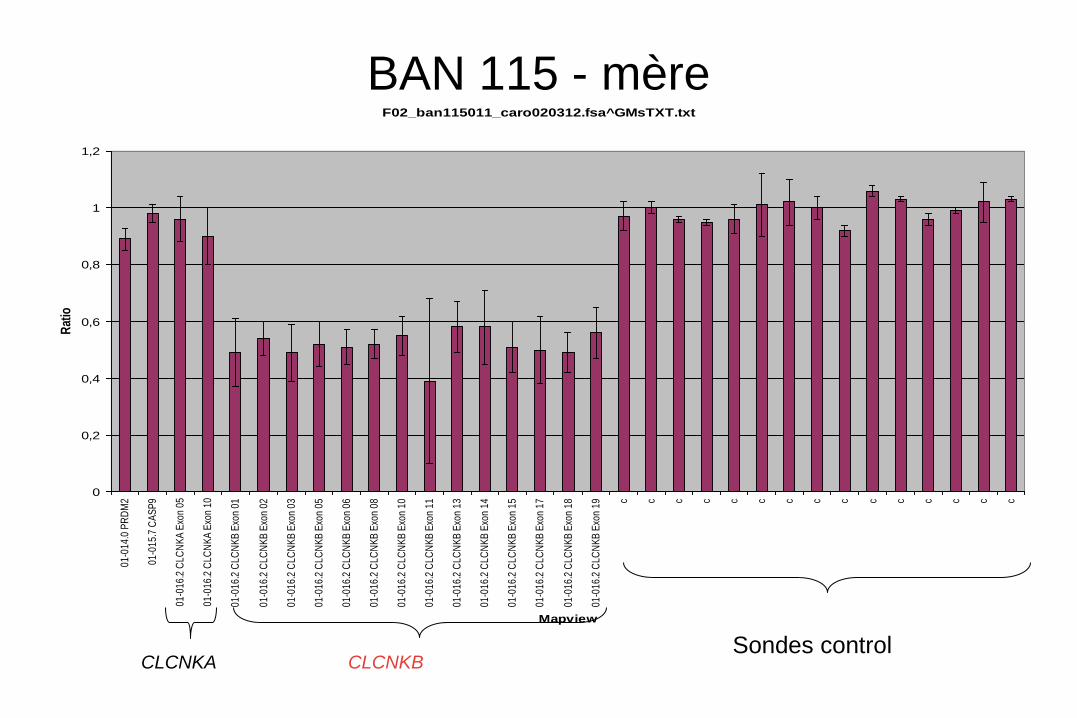
BAN 115 - mère
Sondes control CLCNKA CLCNKB
F02_ban115011_caro020312.fsa^GMsTXT.txt
0
0,2
0,4
0,6
0,8
1
1,2
01-0
14.0
PR
DM
2
01-0
15.7
CA
SP
9
01-0
16.2
CLC
NK
A E
xon
05
01-0
16.2
CLC
NK
A E
xon
10
01-0
16.2
CLC
NK
B E
xon
01
01-0
16.2
CLC
NK
B E
xon
02
01-0
16.2
CLC
NK
B E
xon
03
01-0
16.2
CLC
NK
B E
xon
05
01-0
16.2
CLC
NK
B E
xon
06
01-0
16.2
CLC
NK
B E
xon
08
01-0
16.2
CLC
NK
B E
xon
10
01-0
16.2
CLC
NK
B E
xon
11
01-0
16.2
CLC
NK
B E
xon
13
01-0
16.2
CLC
NK
B E
xon
14
01-0
16.2
CLC
NK
B E
xon
15
01-0
16.2
CLC
NK
B E
xon
17
01-0
16.2
CLC
NK
B E
xon
18
01-0
16.2
CLC
NK
B E
xon
19
c c c c c c c c c c c c c c c
Mapview
Rat
io
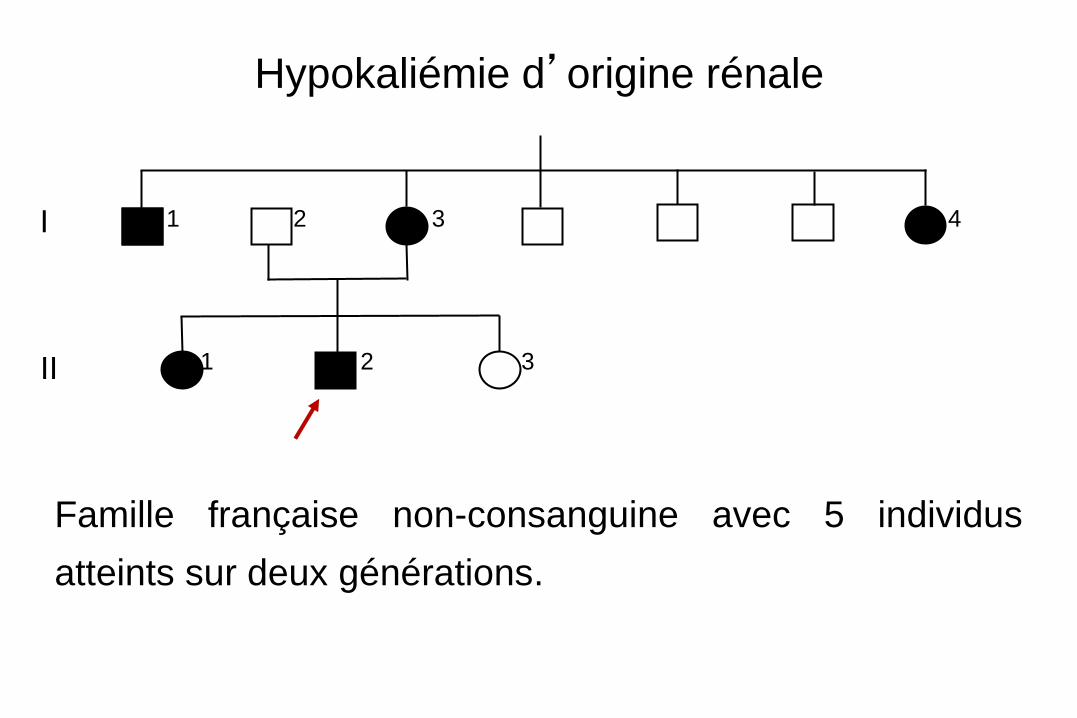
Hypokaliémie d’origine rénale
3 2
4 1 3
1
2
Famille française non-consanguine avec 5 individus
atteints sur deux générations.
I
II
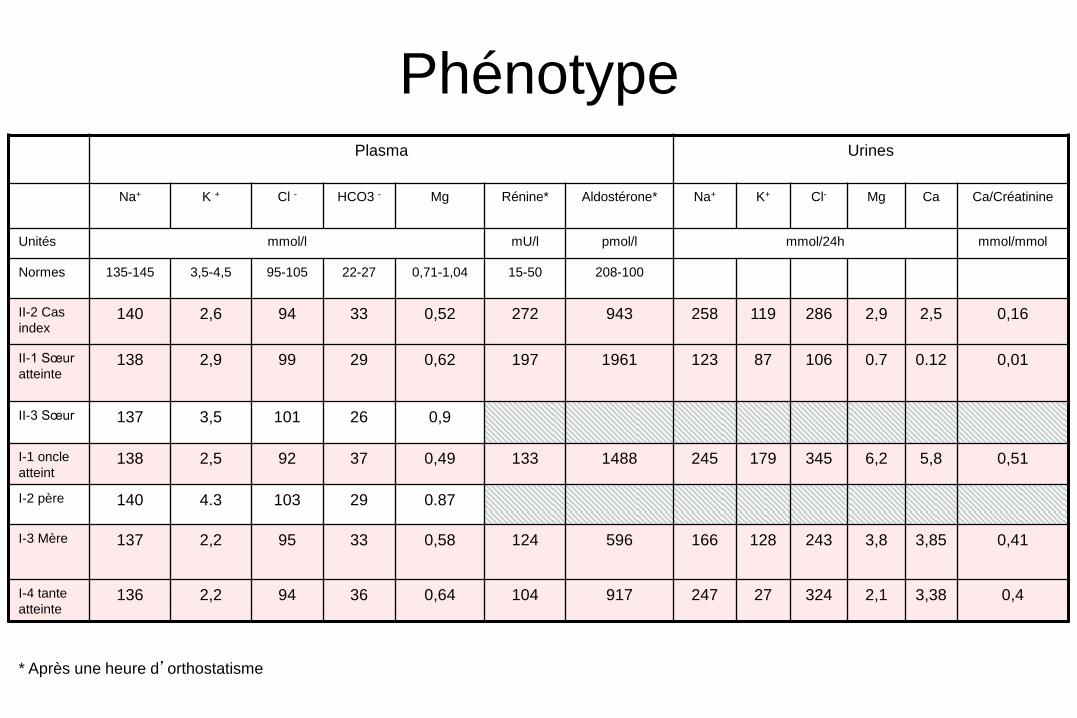
Plasma Urines
Na+ K + Cl - HCO3 - Mg Rénine* Aldostérone* Na+
K+
Cl-
Mg
Ca
Ca/Créatinine
Unités mmol/l mU/l pmol/l mmol/24h mmol/mmol
Normes 135-145 3,5-4,5 95-105 22-27 0,71-1,04 15-50 208-100
II-2 Cas
index 140 2,6 94 33 0,52 272 943 258 119 286 2,9 2,5 0,16
II-1 Sœur
atteinte 138 2,9 99 29 0,62 197 1961 123 87 106 0.7 0.12 0,01
II-3 Sœur 137 3,5 101 26 0,9
I-1 oncle
atteint 138 2,5 92 37 0,49 133 1488 245 179 345 6,2 5,8 0,51
I-2 père 140 4.3 103 29 0.87
I-3 Mère 137 2,2 95 33 0,58 124 596 166 128 243 3,8 3,85 0,41
I-4 tante
atteinte 136 2,2 94 36 0,64 104 917 247 27 324 2,1 3,38 0,4
Phénotype
* Après une heure d’orthostatisme
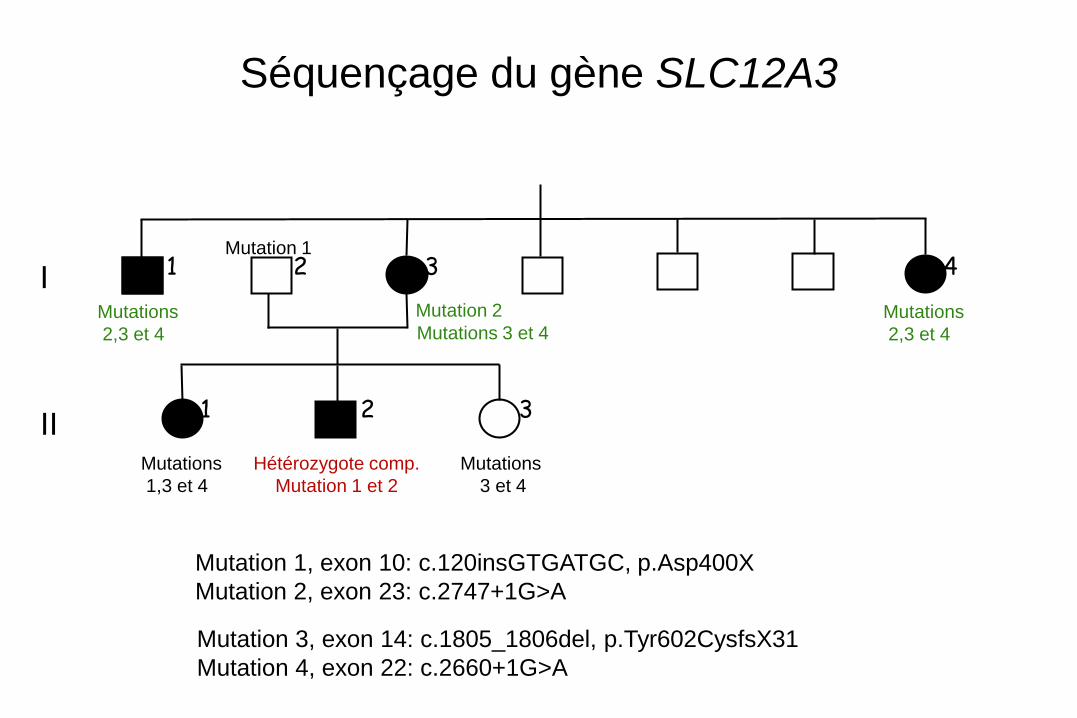
Séquençage du gène SLC12A3
Mutation 1, exon 10: c.120insGTGATGC, p.Asp400X
Mutation 2, exon 23: c.2747+1G>A
3 2
4 1 3
1
2 I
II
Mutation 3, exon 14: c.1805_1806del, p.Tyr602CysfsX31
Mutation 4, exon 22: c.2660+1G>A
Hétérozygote comp.
Mutation 1 et 2
Mutation 2 Mutations
2,3 et 4
Mutations
2,3 et 4
Mutations
1,3 et 4
Mutations
3 et 4
Mutation 1
Mutations 3 et 4
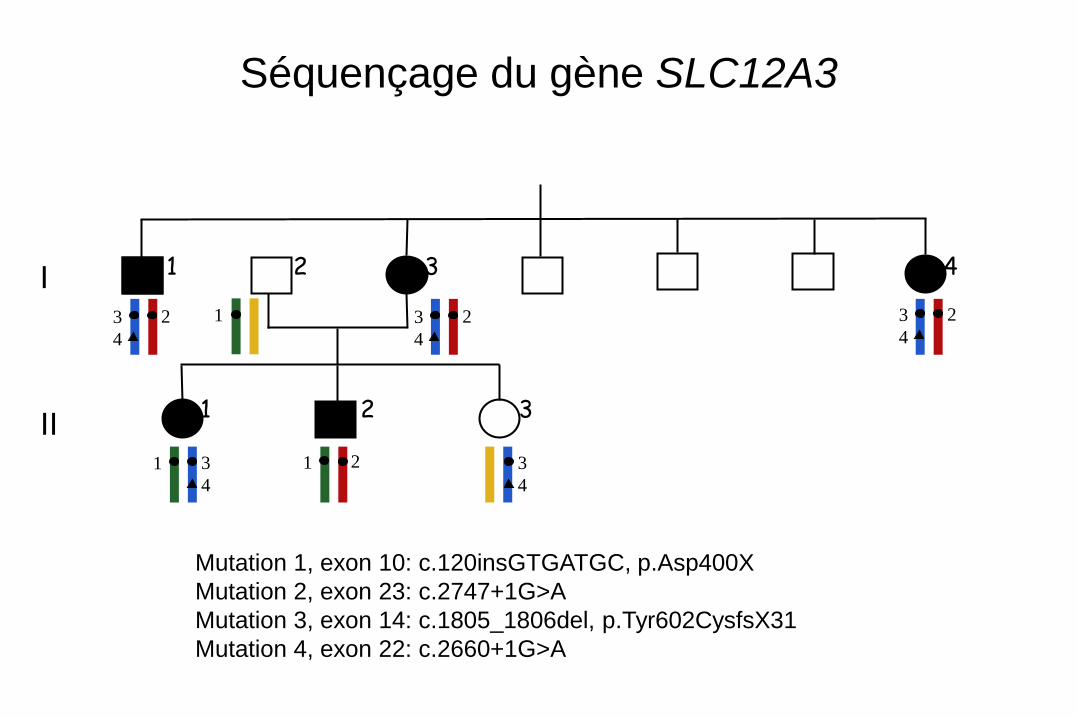
Séquençage du gène SLC12A3
Mutation 1, exon 10: c.120insGTGATGC, p.Asp400X
Mutation 2, exon 23: c.2747+1G>A
Mutation 3, exon 14: c.1805_1806del, p.Tyr602CysfsX31
Mutation 4, exon 22: c.2660+1G>A
2
1 2 3
4
2 3
4 2 3
4
3
4
1 3
4
3 2
4 1 3
1
2
1
I
II
Na+
20%
Na+ 7% Thiazides
Ca2+
Na+ Cl -
Na+
Ca2+
Na+ K+
Ca2+
Na+
H+
Mg2+ Na+
Na+ Mg2+
Cl-
Furosémide
(+)
Na+
K+
2Cl - Na+
K+
K+
Na+ H+
K+
Cl -
Cl -
Na+
HCO3-
Ca++
Mg++
NH4+
(-) Vte
K+
Barttin
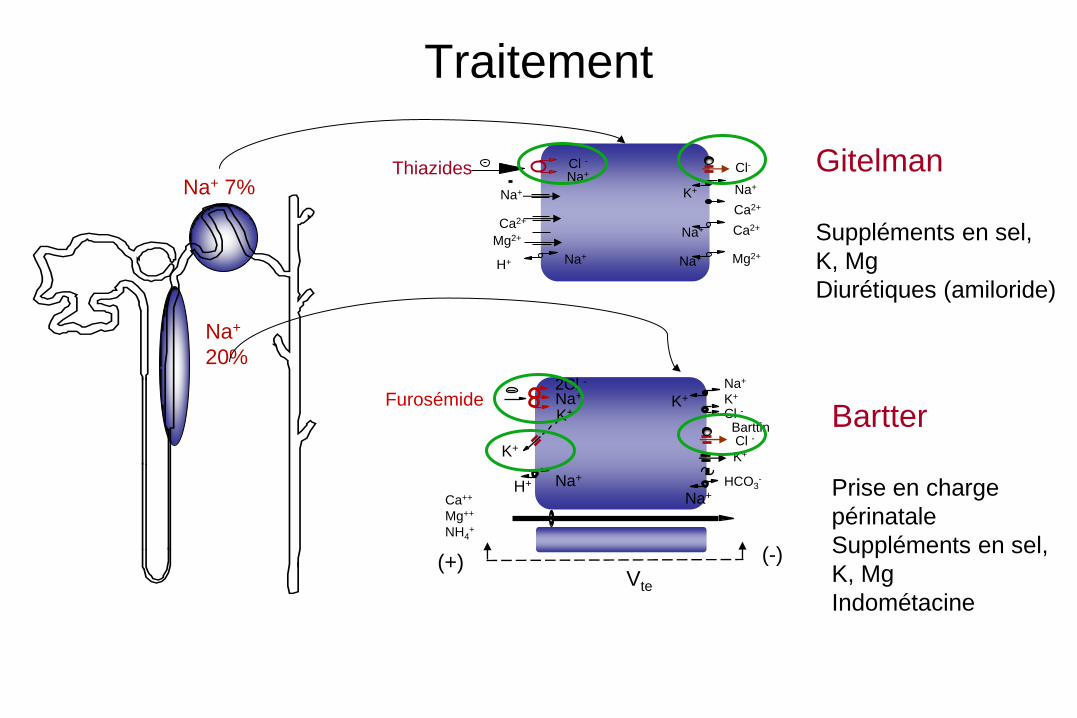
Traitement
Gitelman
Suppléments en sel,
K, Mg
Diurétiques (amiloride)
Bartter
Prise en charge
périnatale
Suppléments en sel,
K, Mg
Indométacine
- Hommes ou femmes âgés de 18-60 ans,
- atteints de syndrome de Gitelman génétiquement confirmé.
- Contraception efficace chez les femmes en âge de procréer. S’il s’agit d’une contraception œstro-progestative maintenue inchangée pendant toute l’étude.
- Consentement éclairé signé
PHRC- GITAB- Dr Anne BLANCHARD
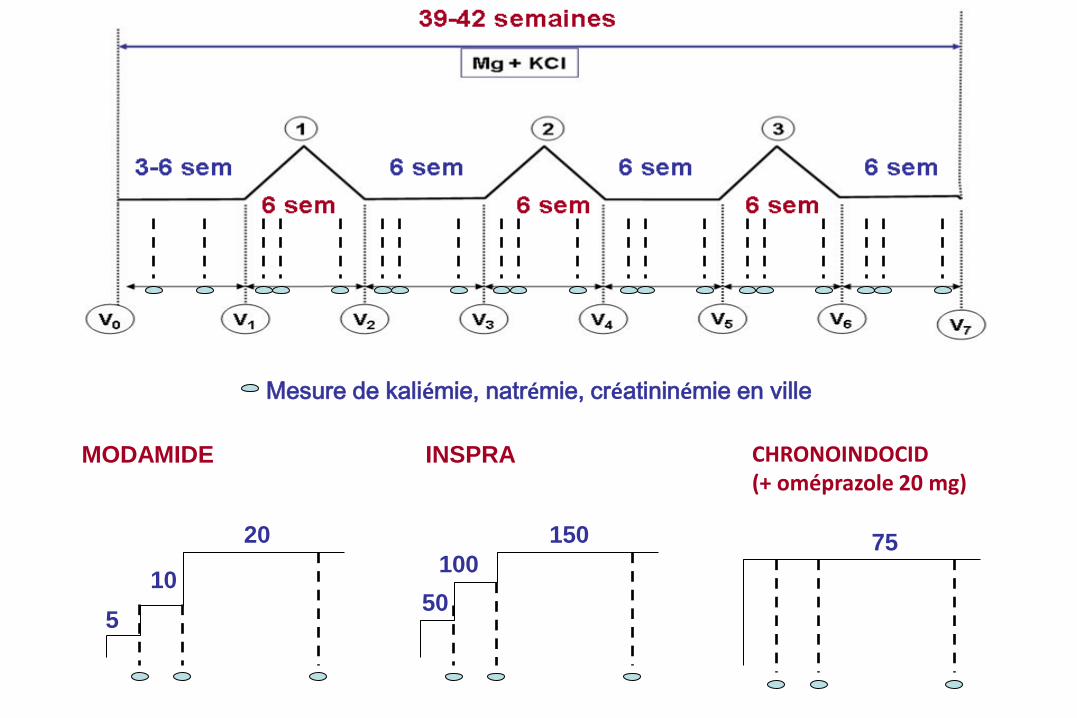
Mesure de kaliémie, natrémie, créatininémie en ville
MODAMIDE
5
10
20
50
100
150
INSPRA
75
CHRONOINDOCID (+ oméprazole 20 mg)
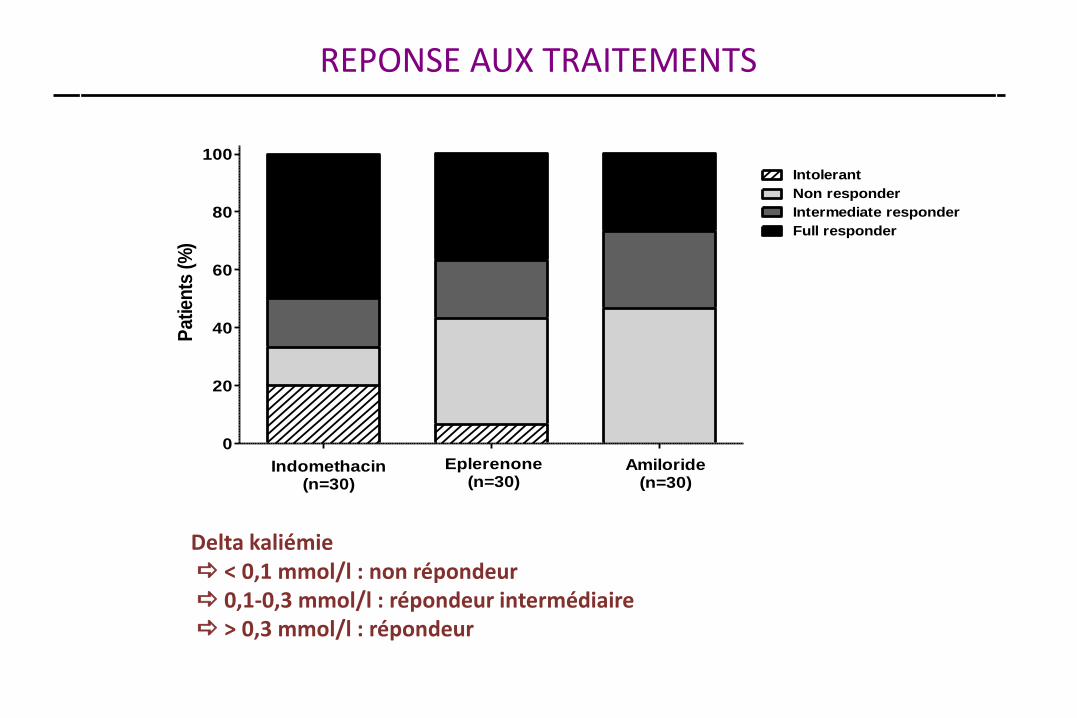
REPONSE AUX TRAITEMENTS
Delta kaliémie < 0,1 mmol/l : non répondeur 0,1-0,3 mmol/l : répondeur intermédiaire > 0,3 mmol/l : répondeur
0
20
40
60
80
100
Indomethacin(n=30)
Amiloride(n=30)
Eplerenone(n=30)
Non responder
Intermediate responder
Full responder
IntolerantP
atien
ts (
%)
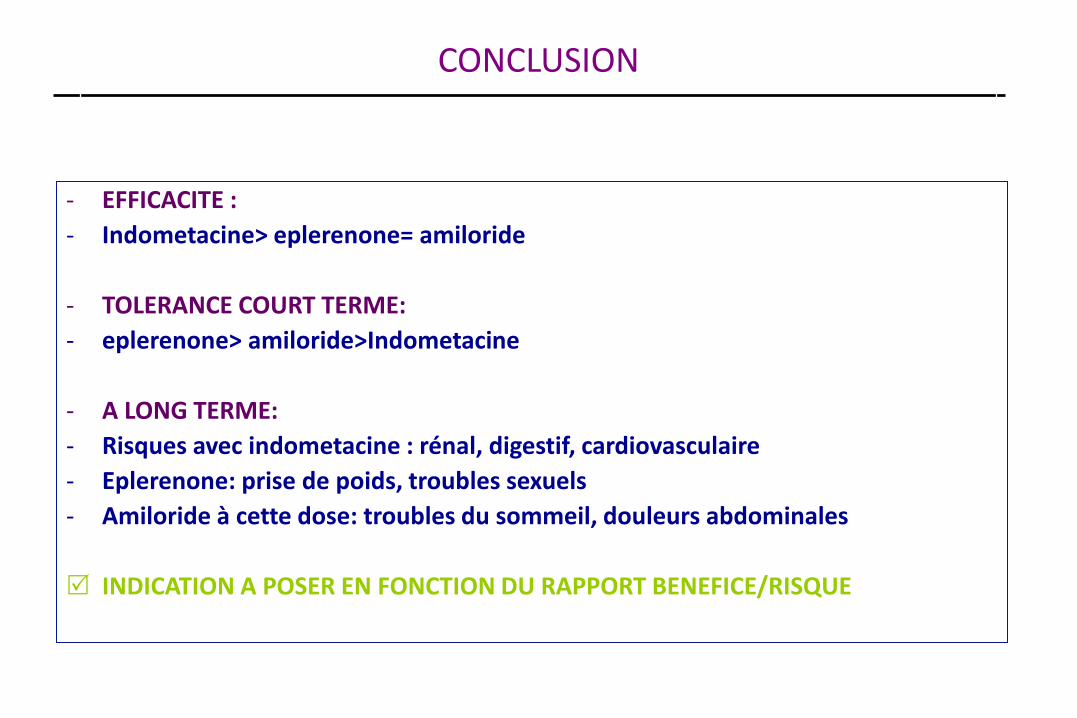
CONCLUSION
- EFFICACITE :
- Indometacine> eplerenone= amiloride
- TOLERANCE COURT TERME:
- eplerenone> amiloride>Indometacine
- A LONG TERME:
- Risques avec indometacine : rénal, digestif, cardiovasculaire
- Eplerenone: prise de poids, troubles sexuels
- Amiloride à cette dose: troubles du sommeil, douleurs abdominales
INDICATION A POSER EN FONCTION DU RAPPORT BENEFICE/RISQUE
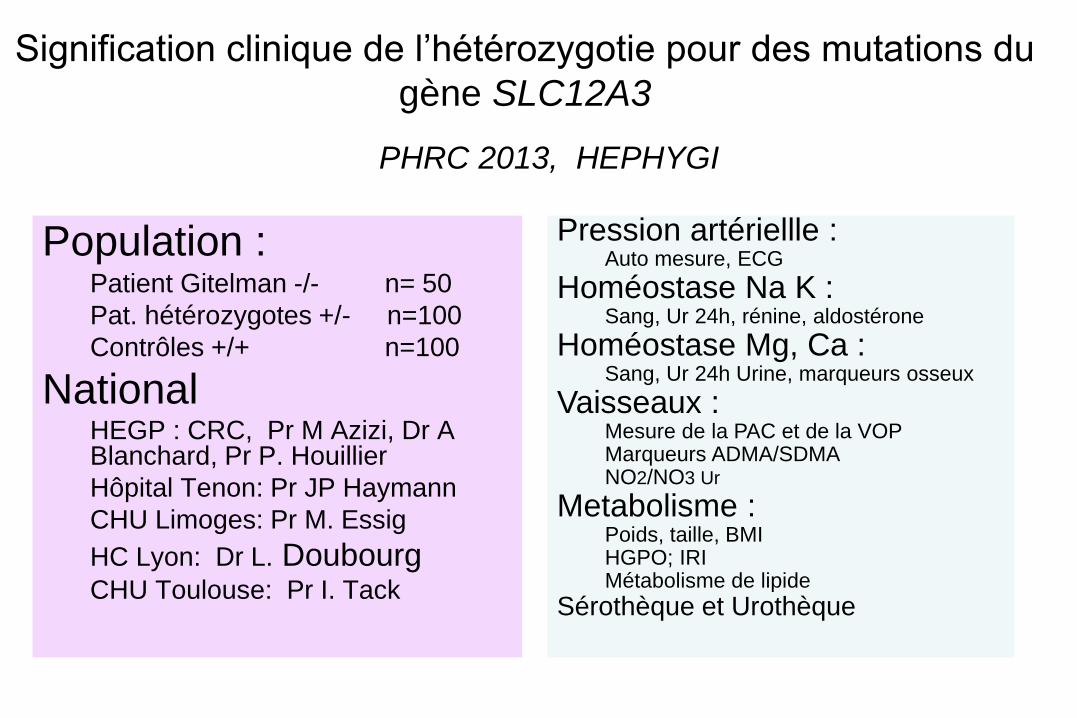
Population : Patient Gitelman -/- n= 50
Pat. hétérozygotes +/- n=100
Contrôles +/+ n=100
National HEGP : CRC, Pr M Azizi, Dr A Blanchard, Pr P. Houillier
Hôpital Tenon: Pr JP Haymann
CHU Limoges: Pr M. Essig
HC Lyon: Dr L. Doubourg CHU Toulouse: Pr I. Tack
Signification clinique de l’hétérozygotie pour des mutations du
gène SLC12A3
Pression artériellle : Auto mesure, ECG
Homéostase Na K : Sang, Ur 24h, rénine, aldostérone
Homéostase Mg, Ca : Sang, Ur 24h Urine, marqueurs osseux
Vaisseaux : Mesure de la PAC et de la VOP Marqueurs ADMA/SDMA NO2/NO3 Ur
Metabolisme : Poids, taille, BMI HGPO; IRI Métabolisme de lipide
Sérothèque et Urothèque
PHRC 2013, HEPHYGI
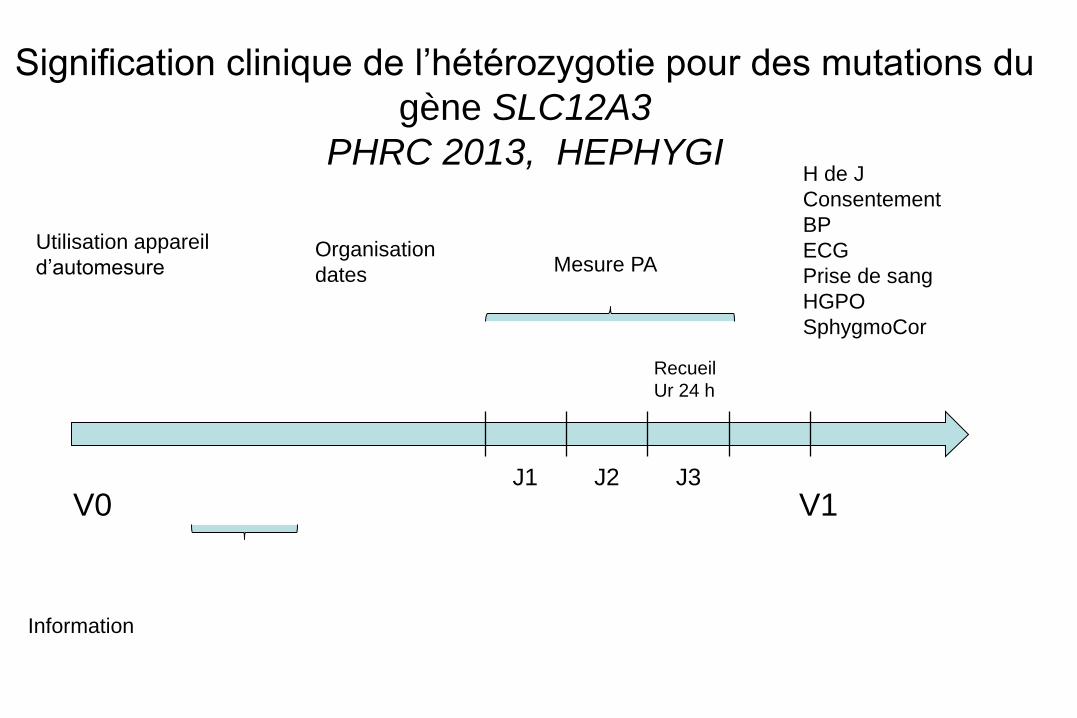
V0
Utilisation appareil
d’automesure Mesure PA
Recueil
Ur 24 h
V1
H de J
Consentement
BP
ECG
Prise de sang
HGPO
SphygmoCor
Organisation
dates
J1 J2 J3
Information
Signification clinique de l’hétérozygotie pour des mutations du
gène SLC12A3
PHRC 2013, HEPHYGI

MERCI Centres de Référence
Centres de Compétences
La Réunion