Embed Size (px)
Citation preview
AAD • "6 1938 O
III I I I II III
JOURNAL Of t h e
A m e m c a N A c a D e m Y OF
D e r M a T O L O G Y V O L U M E 16 N U M B E R 5 PART 1 MAY 1987
II III
Continuing medical educat ion
Bullous pemphigoid
Nell Korman, Ph.D., M.D. Cleveland, OH
Bullous pemphigoid is an autoimmune blistering dermatologic disease characterized clinically by tense bullae that may develop on normal or erythematous skin. The major histologic feature is a subepiderrnal blister with variable degrees of dermal inflammation. Other immunologically mediated blistering skin diseases may mimic bullous pemphigoid, including herpes gestationis, cicatricial pemphigoid, dermatitis herpetiformis, and epidermolysis bullosa acquisita. These diseases will be discussed, Most patients with bullous pemphigoid demonstrate circulating autoantibodies reactive with an antigen located in the lamina lucida region of the basement membrane zone. Complement activation by these autoantibodies initiates influx and activation of mast cells along with other inflammatory cells. Tissue injury with damage and eventual destruction of the basement membrane occurs as a result of the release of inflammatory mediators. The final result is subepidermal blister formation. The course of bullous pemphigoid tends to be self-limited, and successful treatment is usually effected with systemic glucocorticosteroids. (J AM ACAD DERMATOL 1987; 16:907-24.)
Bullous pemphigoid is an autoimmune subepi- dermal blistering disease. Until Lever's classic description ~ in 1953, bullous pemphigoid was grouped with pemphigus vulgaris and had various names, including pemphigus vulgaris chronicus, pemphigus vulgaris benignus, and bullous der- matitis herpetiformis. In 1967, Jordon et al 2 de- fined the immunopathologic features of bullous pemphigoid by demonstrating the existence of
The CME articles are made possible through an educa- tional grant from Syntex Laboratories, Inc.
From the Department of Dermatology, University Hospitals of Cleveland,
Reprint requests to: Dr. Neil Korman, Department of Dermatology, University Hospitals of Cleveland, 2074 Abington Rd., Cleveland, OH 44106.
bound IgG at the epidermal basement membrane with the use of direct immunofluorescence and found circulating IgG antibodies directed against the epidermal basement membrane zone. These observations confirmed Lever's original hypothe- sis that bullous pemphigoid was an entity distinct from pemphigus vulgaris.
CLINICAL MANIFESTATIONS
The definitive description of the clinical char- acteristics of bullous pemphigoid was published by Lever 3 in his 1965 monograph. Bullous pem- phigoid is generally a disease of elderly persons. The median age of onset ranges from 60 to 75 years, although childhood onset of bullous pem- phigoid has also been reported. 4 There is no in- creased prevalence of bullous pemphigoid in any
907
908 Korman Journal of the
American Academy of Dermatology
racial group, and men and women are equally af- fected. Unlike patients with pemphigus vulgaris, in which there are reported associations with cer- tain human lymphocyte antigen (HLA) haplo- types, patients with bullous pemphigoid have no known HLA associations. 5
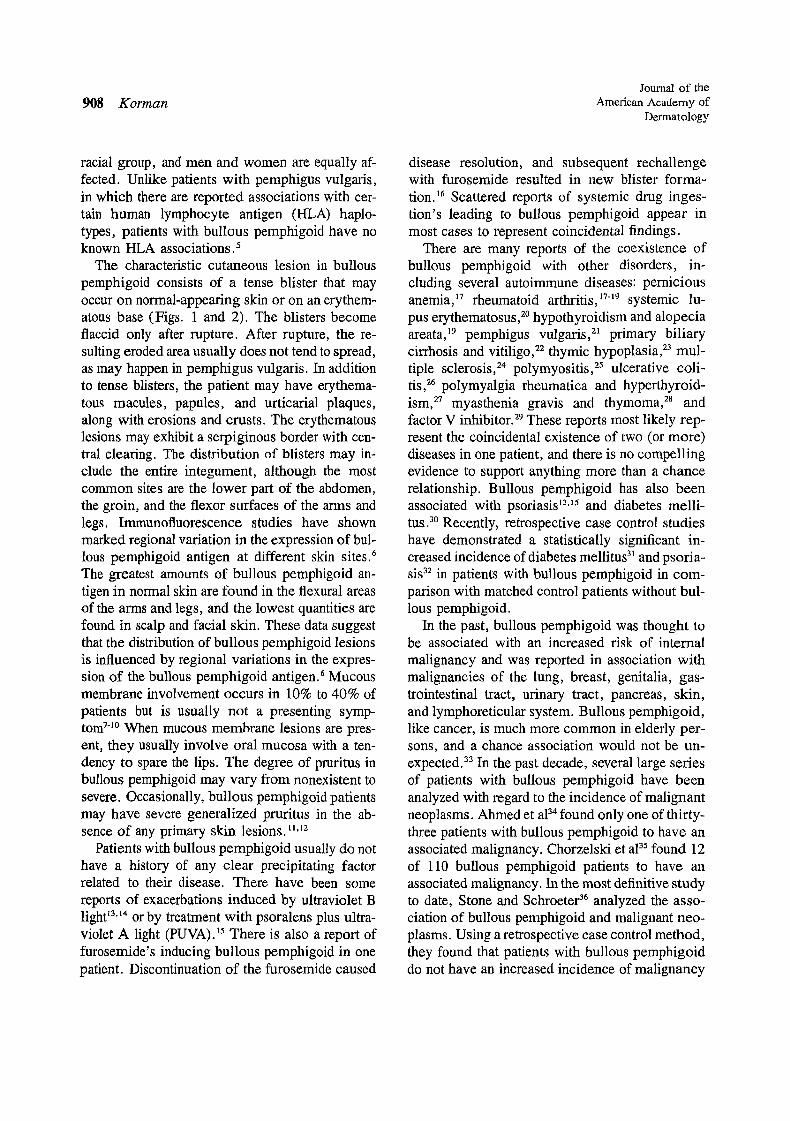
The characteristic cutaneous lesion in butlous pemphigoid consists of a tense blister that may occur on normal-appearing skin or on an erythem- atous base (Figs. 1 and 2). The blisters become flaccid only after rupture. After rupture, the re- suiting eroded area usually does not tend to spread, as may happen in pemphigus vulgaris. In addition to tense blisters, the patient may have erythema- tous macules, papules, and urticarial plaques, along with erosions and crusts. The erythematous lesions may exhibit a serpiginous border with cen- tral clearing. The distribution of blisters may in- clude the entire integument, although the most common sites are the lower part of the abdomen, the groin, and the flexor surfaces of the arms and legs. Immunofluorescence studies have shown marked regional variation in the expression of bul- lous pemphigoid antigen at different skin sites. 6 The greatest amounts of bullous pemphigoid an- tigen in normal skin are found in the flexural areas of the arms and legs, and the lowest quantities are found in scalp and facial skin. These data suggest that the distribution of bullous pemphigoid lesions is influenced by regional variations in the expres- sion of the bullous pemphigoid antigen.6 Mucous membrane involvement occurs in 10% to 40% of patients but is usually not a presenting symp- tom 7"1° When mucous membrane lesions are pres- ent, they usually involve oral mucosa with a ten- dency to spare the lips. The degree of pruritus in bullous pemphigoid may vary from nonexistent to severe. Occasionally, bullous pemphigoid patients may have severe generalized pruritus in the ab- sence o f any primary skin lesions. ,.~2
Patients with bullous pemphigoid usually do not have a history of any clear precipitating factor related to their disease. There have been some reports of exacerbations induced by ultraviolet B light ~3'14 or by treatment with psoralens plus ultra- violet A light (PUVA).t5 There is also a report of furosemide's inducing bullous pemphigoid in one patient. Discontinuation of the furosemide caused
disease resolution, and subsequent rechallenge with furosemide resulted in new blister forma- tion. 16 Scattered reports of systemic drug inges- tion's leading to bullous pemphigoid appear in most cases to represent coincidental findings.
There are many reports of the coexistence of bullous pemphigoid with other disorders, in- cluding several autoimmune diseases: pernicious anemia, 17 rheumatoid arthritis, 17-~9 systemic lu- pus erythematosus,2° hypothyroidism and alopecia areata, ~9 pemphigus vulgaris, 2~ primary biliary cirrhosis and vitiligo, 22 thymic hypoplasia, 23 mul- tiple sclerosis, 24 polymyositis, 25 ulcerative coli- tis, 26 polymyalgia rheumatica and hyperthyroid- ism, 27 myasthenia gravis and thymoma, 28 and factor V inhibitor. 29 These reports most likely rep- resent the coincidental existence of two (or more) diseases in one patient, and there is no compelling evidence to support anything more than a chance relationship. Bullous pemphigoid has also been associated with psoriasis ~3,~5 and diabetes melli- tus. 3° Recently, retrospective case control studies have demonstrated a statistically significant in- creased incidence of diabetes mellitus 3~ and psoria- sis 32 in patients with bullous pemphigoid in com- parison with matched control patients without bul- lous pemphigoid.
In the past, bullous pemphigoid was thought to be associated with an increased risk of internal malignancy and was reported in association with malignancies of the lung, breast, genitalia, gas- trointestinal tract, urinary tract, pancreas, skin, and lymphoreticular system. Bullous pemphigoid, like cancer, is much more common in elderly per- sons, and a chance association would not be un- expected. 33 In the past decade, several large series of patients with bullous pemphigoid have been analyzed with regard to the incidence of malignant neoplasms. Ahmed et a134 found only one of thirty- three patients with bullous pemphigoid to have an associated malignancy. Chorzelski et a135 found 12 of 110 bullous pemphigoid patients to have an associated malignancy. In the most definitive study to date, Stone and Schroeter 36 analyzed the asso- ciation of bullous pemphigoid and malignant neo- plasms. Using a retrospective case control method, they found that patients with bullous pemphigoid do not have an increased incidence of malignancy

Volume 16 Number 5, Part 1 May 1987 BuUous pemphigoid 909
in comparison with appropriately age- and sex- matched control subjects. 36 However, when bul- lous pemphigoid patients are subdivided according to indirect immunofluorescence findings, seroneg- ative patients tend to have an increased risk of internal malignancy in comparison with seroposi- tive patients. 8'9"37 Studies comparing bullous pem- phigoid patients with negative indirect immuno- fluorescence with age- and sex-matched subjects without bullous pemphigoid are needed in order to establish a more definite association between seronegative bullous pemphigoid patients and in- ternal malignancy.
Laboratory abnormalities in patients with bul- lous pemphigoid include peripheral blood eosin- ophilia, noted to occur in 50% of patients, 3s and elevated serum IgE, found in 70% of patients. 39
The natural history of bullous pemphigoid tends to be much more benign than that of pemphigus vulgaris. If untreated, bullous pemphigoid may persist from months to years and is characterized by spontaneous remissions and exacerbations. I Re- current disease may be less severe than the initial episode, and some patients may achieve prolonged clinical remission after initial glucocorticosteroid treatment. The mortality rate is relatively low even in the absence of systemic glucocorticosteroid treatment, 4° but the disease can be fatal during the active stage, especially in elderly or debilitated patients, l
CLINICAL VARIANTS OF BULLOUS PEMPI-IIGOID
Bullous pemphigoid may start as a localized eruption in 15% to 30% of patients. Generally, bullous pemphigoid in these patients is more re- sponsive to therapy and can often be controlled with topical corticosteroids alone. 41 The majority of patients with localized pemphigoid have a pre- dilection for lesions on the lower extremities. 7.30.42
Bullous pemphigoid may occur in childhood, and the clinical features of the few reported cases are similar to bullous pemphigoid occurring in adulthood: Other blistering diseases of childhood that may be difficult to distinguish clinically from bullous pemphigoid include dermatitis herpetifor- mis and benign chronic bullous dermatosis of childhood. Immunofluorescence studies are nec-
essary to distinguish these three entities. Patients with childhood bullous pemphigoid have linear de- position of IgG at the basement membrane zone, those with dermatitis herpetiformis have granular deposition of IgA at the basement membrane zone, and those with benign chronic bullous dermatosis of childhood have linear deposition of IgA at the basement membrane zone. 43 Bullous pemphigoid of childhood is managed similarly to the disease in adults. Because of the limited number of re- ported cases, the course and prognosis of bullous pemphigoid in childhood are difficult to evaluate:
Vesicular pemphigoid is a variant of bullous pemphigoid in which the blisters tend to be tense, small, and grouped. 44 Direct immunofluorescence reveals the deposition of IgG at the basement mem- brane zone. Polymorphic pemphigoid is another bullous pemphigoid variant that has some clinical features of dermatitis herpetiformis. The blisters in polymorphic pemphigoid are intermediate in size between those seen in bullous pemphigoid and those occurring in dermatitis herpetiformis. 4~ Di- rect immunofluorescence reveals linear deposition of IgG or IgA at the basement membrane zone. These patients do not have any specific HLA as- sociation or jejunal atrophy, both of which are classically seen in dermatitis herpetiformis.4S Poly- morphic pemphigoid in association with linear IgG deposits at the basement membrane zone may rep- resent a variant of bullous pemphigoid, whereas polymorphic pemphigoid in association with linear IgA deposits may represent what is now referred to as linear IgA disease. 4~
Vegetating pemphigoid is a rare variant of the disease and is characterized by purulent and ver- rucous vegetating intertriginous lesions. 47 Clini- cally the lesions resemble those seen in pemphigus vegetans, but biopsy and direct immunofluores- cence reveal findings most compatible with bullous pemphigoid. To date, three cases of vegetating pemphigoid have been described. 48,49
Another unusual variant of bullous pemphigoid is hyperkeratotic scarring pemphigoid. Histologic study of these lesions reveals a subepidermal blis- ter with hyperkeratosis, papillomatosis, and acan- thosis. Direct immunofluorescence shows linear basement membrane zone deposition of C3 and IgG. 4~ Pemphigoid nodularis, which has recently
910 Kor tnan
Journal of the American Academy of
Dermatology
Fig. 1. The feet of a patient with bullous pemphigoid show tense blisters and erosions on normal-appearing skin. Fig. 2. Close-up view of truncal lesions of a patient with bullous pemphigoid, revealing several confluent blisters and erosions. Fig. 3. Photomicrograph of a specimen from a bullous pemphigoid blister. There is subepidermal blister formation with an inflammatory infiltrate consisting of eosinophils, lymphocytes, and neutrophils. Fig. 4. Direct immunofluorescence of perilesional skin of a patient with bullous pem- phigoid, showing linear IgG deposits at the dermoepidermal junction.
been described as bullous pemphigoid mimicking prurigo nodularis, s° appears to be identical to hy- perkeratotic scarring pemphigoid. Four patients with either hyperkeratotic scarring pemphigoid or pemphigoid nodularis have been described to date. All these patients have had chronic persistent le- sions even when treated aggressively with gluco- corticosteroids and immunosuppressive agents.
Bullous pemphigoid presenting as an erythro- derma has also been described? ~ In one patient the disease began with tense blisters on the ab- domen. Within 3 weeks the blisters spread to in- volve the abdomen, arms, and thighs, and the pa- tient had a generalized erythroderma. Direct im- munofluorescence revealed linear C3 deposition, and indirect immunofluorescence was positive for

Volume 16 Number 5, Part 1 May 1987
Bullous pemphigoid 911
a high titer of circulating IgG antibodies. The di- agnosis of bullous pemphigoid was further sup- ported by the immunoelectron microscopic dem- onstration of bound antibodies in the lamina lucida? I
The relationship of these uncommon variants of bullous pemphigoid to classic bullous pemphigoid is not presently known. Ultrastructural localization of the immunoreactants or immunochemical char- acterization of the involved antigen will be nec- essary in order to determine the relationship of these unusual variants of bullous pemphigoid to classic bullous pemphigoid.
DIFFERENTIAL DIAGNOSIS Cicatricial pemphigoid
Cicatricial pemphigoid is a chronic subepider- real blistering disease involving primarily mucosal surfaces (Table 2). Involved mucosal surfaces, in decreasing order of frequency, are the oral mu- cosa, the conjunctiva, the larynx, the genitalia, and the esophagus. 9 There is a tendency toward scarring as the lesions heal, and conjunctival in- volvement can lead to entropion, trichiasis, and symblepharon formation with corneal ulceration and eventual blindness. The esophageal lesions may infrequently result in stricture formation, and the laryngeal lesions can rarely be life-threatening, necessitating emergency tracheostomy. 33 Only one fourth of cicatricial pemphigoid patients have cu- taneous lesions. These lesions may occur in two forms: tense, scattered blisters over the legs and genitalia that heal without scarring or flaccid blis- ters over the face and scalp that heal with scarring. 9 Biopsy specimens of cicatricial pemphigoid le- sions show a subepidermal blister. Direct immu- nofluorescence reveals C3 and IgG at the lamina lucida in 80% to 97% of patients, 9'52 and indirect immunofluorescence reveals circulating lgG in 20% to 30% of patients. 53 There is an increased incidence of the HLA-B 12 phenotype in patients with ocular cicatricial pemphigoid in comparison with control subjects, s4 Cicatricial pemphigoid is a chronic disease, and treatment generally includes systemic glucocorticosteroids, often supplemented with immunosuppressive agents. 9 The use of dap- sone in the treatment of cicatricial pemphigoid has recently been reported to be of some value? 5 Cic- atricial pemphigoid is a distinct entity from bullous
pemphigoid, as shown by suction blister studies, which reveal that the cicatricial pemphigoid anti- gen localizes at a level below that o f the bullous pemphigoid antigen in the lamina lucida. 53.56 The Brunsting-Perry variant of cicatricial pemphigoid is characterized by the absence of mucosal lesions and by the presence of intermittent crops of grouped blisters limited to the head and neck that heal with atrophic scars? 7
Herpes gestationis
Herpes gestationis is a subepidermal vesiculo- bullous disease of pregnancy. It may occur at any time between the second month of gestation and the first week post partum, but the most common time of onset is in the second trimester.* The ear- liest lesions are urticarial papules and polycyclic wheals, which subsequently evolve into vesicles and bullae. In 80% to 90% of patients the eruption begins at the umbilicus and spreads peripherally. Intense pruritus is generally associated with these lesions. Although herpes gestationis is typically associated with pregnancy, it has also been re- ported in association with hydatidiform mole and choriocarcinoma.* Histologie study of herpes ges- tationis reveals a subepidermal blister with eosin- ophils, and electron microscopy reveals isolated necrotic basal keratinocytes. Direct immunofluo- rescence reveals linear deposition of C3 at the lamina lucida in all patients and linear deposition of IgG at the lamina lucida in 30% to 40% of patients? 8 Indirect immunofluorescence demon- strates the presence of the "herpes gestationis fac- tor" in 85% to 100% of patients? 9,6° This factor is a circulating IgG that avidly fixes complement. 6t Patients with herpes gestationis usually go into remission within 2 weeks of delivery and fre- quently have recurrence in subsequent pregnan- cies. Exacerbations of their disease may occur be- tween pregnancies after ingestion o f oral contra- ceptives and as a result of changes in the menstrual cycle. 6z There is a significantly increased incidence of the HLA-A1, -B8, and -DR3 phenotype in pa- tients with herpes gestationis. 62 Systemic gluco- corticosteroids are the treatment o f choice for herpes gestationis. The relative safety of these
*Holmes RL, Black MM, Herpes gestationis. Dermatol Clin 1983;1:195-203.
912 Korman Journal of the
American Academy of Dermatology
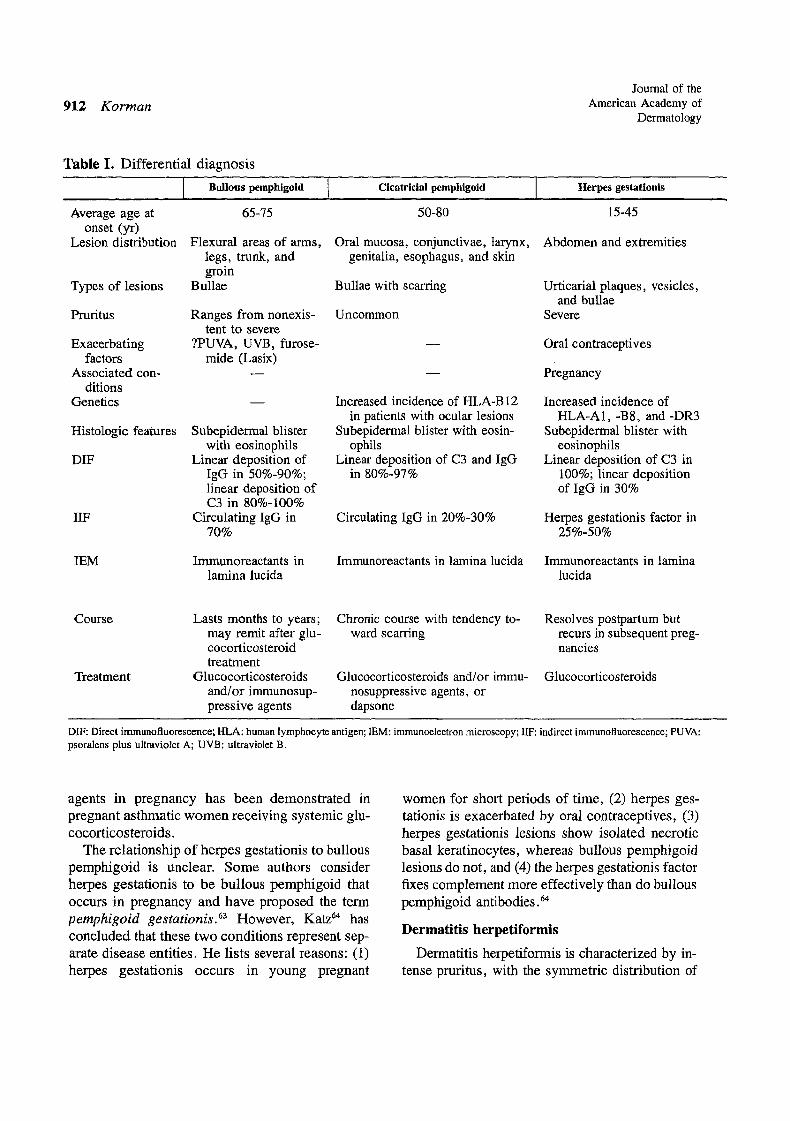
Table I. Differential diagnosis
Bullous pemphigoid Cicatricial pemphigoid
Average age at onset (yr)
Lesion distribution
Types of lesions
65 -75
Flexural areas of arms, legs, trunk, and groin
Bullae
5O-8O
Oral mucosa, conjunctivae, larynx, genitalia, esophagus, and skin
Bullae with scarring
Pruritus
Exacerbating factors
Associated con- ditions
Genetics
Ranges from nonexis- tent to severe
?PUVA, UVB, furose- mide (Lasix)
Histologic features Subepidermal blister with eosinophils
DIF Linear deposition of IgG in 50%-90%; linear deposition of C3 in 80%-100%
IIF Circulating lgG in 70%
Uncommon
Increased incidence of HLA-B 12 in patients with ocular lesions
Subepidermal blister with eosin- ophils
Linear deposition of C3 and IgG in 80%-97%
Circulating IgG in 20%-30%
IEM Immunoreactants in lamina lucida
Immunoreactants in lamina lucida
Herpes gestationis
15-45
Abdomen and extremities
Urticarial plaques, vesicles, and bullae
Severe
Oral contraceptives
Pregnancy
Increased incidence of HLA-A1,-BS, and-DR3
Subepidermal blister with eosinophils
Linear deposition of C3 in 100%; linear deposition of IgG in 30%
Herpes gestationis factor in 25%-50%
Immunoreactants in lamina lucida
Course Lasts months to years; may remit after glu- cocorticosteroid treatment
Treatment Glucocorticosteroids and/or immunosup- pressive agents
Chronic course with tendency to- ward scarring
Glucocorticosteroids and/or immu- nosuppressive agents, or dapsone
Resolves postpartum but recurs in subsequent preg- nancies
Glucocorticosteroids
DIF: Direct irnmunofluorescence; HLA: human lymphocyte antigen; IEM: immunoelectron microscopy; IIF: indirect immunofluorescence; PUVA: psoralens plus ultraviolet A; UVB: ultraviolet B.
agents in pregnancy has been demonstrated in pregnant asthmatic women receiving systemic glu- cocorticosteroids.
The relationship of herpes gestafionis to bullous pemphigoid is unclear. Some authors consider herpes gestationis to be bullous pemphigoid that occurs in pregnancy and have proposed the term pemphigoid gestationis. 63 However, Katz 64 has concluded that these two conditions represent sep- arate disease entities. He lists several reasons: (1) herpes gestationis occurs in young pregnant
women for short periods of time, (2) herpes ges- tationis is exacerbated by oral contraceptives, (3) herpes gestationis lesions show isolated necrotic basal keratinocytes, whereas bullous pemphigoid lesions do not, and (4) the herpes gestationis factor fixes complement more effectively than do bullous pemphigoid antibodies. 64
Dermati t i s herpet l formis
Dermatitis herpetiformis is characterized by in- tense pruritus, with the symmetric distribution of
Volume 16 Number 5, Part 1 May 1987
Bullous pemphigoid 913
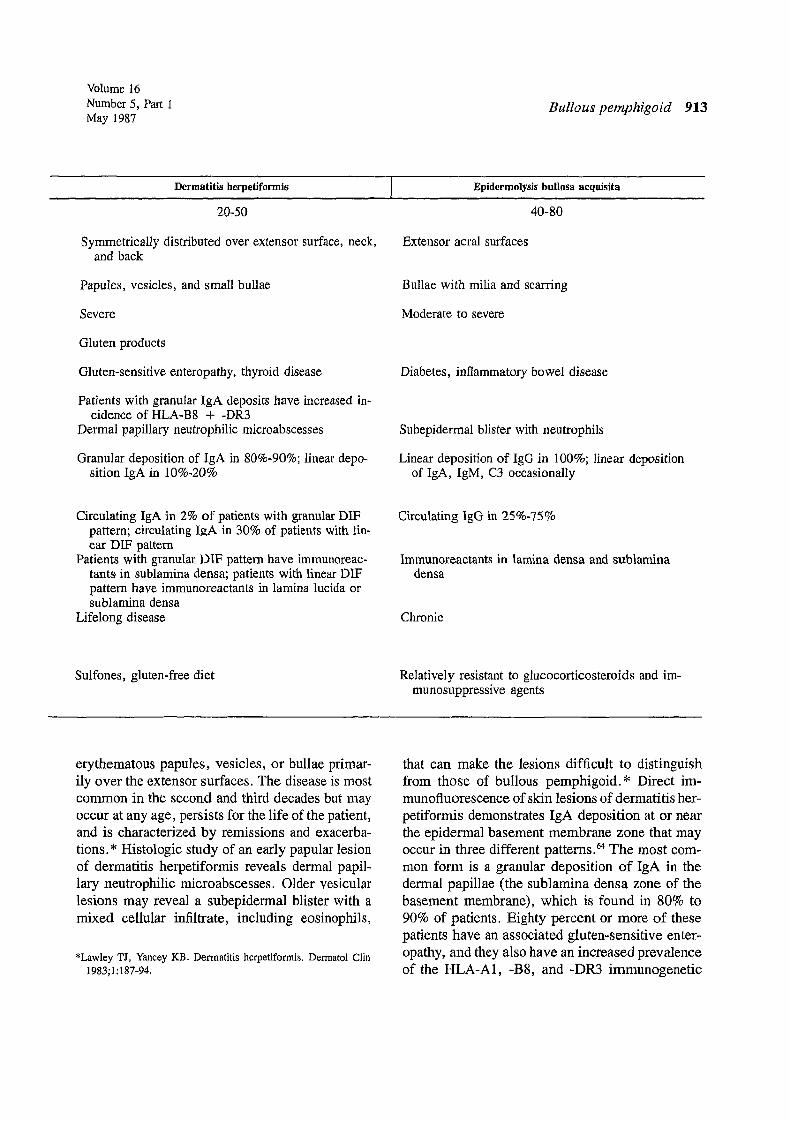
Dermatitis herpetiformis
20-50
Symmetrically distributed over extensor surface, neck, and back
Papules, vesicles, and small bullae
Severe
Gluten products
Gluten-sensitive enteropathy, thyroid disease
Patients with granular IgA deposits have increased in- cidence of HLA-B8 + -DR3
Dermal papillary neutrophilic microabscesses
Granular deposition of IgA in 80%-90%; linear depo- sition IgA in 10%-20%
Epidermolysis bullosa aequisita
40-80
Extensor acral surfaces
Bullae with milia and scarring
Moderate to severe
Diabetes, inflammatory bowel disease
Subepidermal blister with neutrophils
Linear deposition of IgG in 100%; linear deposition of IgA, IgM, C3 occasionally
Circulating IgA in 2% of patients with granular DIF pattern; circulating IRA in 30% of patients with lin- ear DIF pattern
Patients with granular DIF pattern have imrnunoreac- tants in sublamina densa; patients with linear DIF pattern have immunoreactants in lamina lucida or sublamina densa
Lifelong disease
Circulating IgG in 25%-75%
Immunoreactants in lamina densa and sublamina densa
Chronic
Sulfones, gluten-free diet Relatively resistant to glucocorticosteroids and im- munosuppressive agents
erythematous papules, vesicles, or bullae primar- ily over the extensor surfaces. The disease is most common in the second and third decades but may occur at any age, persists for the life of the patient, and is characterized by remissions and exacerba- tions. * Histologic study of an early papular lesion of dermatitis herpetiformis reveals dermal papil- lary neutrophilic microabscesses. Older vesicular lesions may reveal a subepidermal blister with a mixed cellular infiltrate, including eosinophils,
*Lawley TJ, Yancey KB. Dermatitis herpetiformis. Dermatol Clin 1983;1:187-94.
that can make the lesions difficult to distinguish from those of bullous pemphigoid.* Direct im- munofluorescence of skin lesions of dermatitis her- petiformis demonstrates IgA deposition at or near the epidermal basement membrane zone that may occur in three different patterns. 64 The most com- mon form is a granular deposition of IgA in the dermal papillae (the sublamina densa zone of the basement membrane), which is found in 80% to 90% of patients. Eighty percent or more of these patients have an associated gluten-sensitive enter- opathy, and they also have an increased prevalence of the HLA-A1, -B8, and -DR3 immunogenetic
914 Korman Journal of the
American Academy of Dermatology
type: s The DR3 association is the most closely linked of these associations. This is perhaps not surprising, since an increased prevalence of this haplotype has also been observed in many other autoimmune diseases, including systemic lupus er- ythematosus, Sj6gren's syndrome, myasthenia gravis, Addison's disease and Graves' disease: 6 Indirect immunofluorescence in patients with gran- ular IgA deposition is positive for circulating IgA antibodies in approximately 2% of patients. 67
Another immunofluorescence pattern seen in dermatitis herpetiformis is linear IgA deposition. By immunoelectron microscopy the deposits may be localized either within the lamina lucida or in the sublamina densa zone. Patients with linear de- position of IgA have no evidence of small bowel disease and a normal prevalence of HLA-B8 and -DR3 antigens, 65 but they do have a 30% incidence of circulating IgA antibodies: 7 These significant differences between dermatitis herpetiformis pa- tients with granular and those with linear IgA de- position suggest that these disorders are distinct disease processes, and some authors do refer to linear IgA deposition as a marker for a separate entity known as linear IgA disease.47 The treatment of dermatitis herpetiformis is either dapsone or sulfapyridine. Adherence to a strict gluten-free diet may, in some patients, lead to significant amelio- ration of the skin disease and/or reduction in the need for sulfone therapy: 4
Epidermolysis bullosa aequisita
Epidermolysis bullosa acquisita is characterized by trauma-induced blisters, increased skin fragil- ity, and erosions often localized to extensor skin surfaces that heal with scars and milium formation. The term epidermolysis bullosa acquisita was first used to describe a group of patients with features of epidermolysis bullosa arising in adulthood who had no family history of epidermolysis bullosa. 68 Since epidermolysis bullosa acquisita may mimic many primary blistering disorders, the exclusion of bullous pemphigoid, cicatricial pemphigoid, dermatitis herpefiformis, and porphyria cutanea tarda is an important criterion for making this di- agnosis. Histopathologic study of epidermolysis bullosa acquisita reveals a subepidermal blister with a moderately dense cellular infiltrate coin-
posed primarily of neutrophils. Direct immunoflu- orescence reveals linear deposition of IgG at the basement membrane zone in all patients and oc- casional linear deposition of IgA, IgM, and C3. Circulating IgG antibasement membrane zone an- tibodies may be found in 25% to 75% of patients with epidermolysis bullosa acquisita patients. 69 Immunoelectron microscopic and immunochemi- cal studies have revealed that, unlike bullous pem- phigoid, the IgG deposits are in the lamina densa and sublamina densa region. 7° Recently the epi- dermolysis bullosa acquisita antigen has been iden- tified and partially purified. 7~
Generally patients with epidermolysis bullosa acquisita tend to be elderly and are resistant to therapy with systemic glucocorticosteroids: 9 The existence of an inflammatory, as well as a noninflammatory, phase of disease in patients with epidermolysis bullosa acquisita was re- ported recently. 72 The inflammatory phase may clinically mimic bullous pemphigoid or, less com- monly, cicatricial pemphigoid or dermatitis herpet- iformis, whereas the noninflammatory phase rep- resents classic epidermolysis bullosa acquisita with trauma-induced blisters, erosions, and in- creased skin fragility, resulting in scarring and mil- ium formation. Because of the difficulty in distin- guishing inflammatory-phase epidermolysis bul- losa acquisita from bullous pemphigoid by means of clinical, histologic, and immunofluorescence criteria, Gammon et a173 examined the serum of eighty-five patients with a diagnosis of bullous pemphigoid for the presence of epidermolysis bul- losa acquisita antibodies. They found that 10% of these sera contained epidermolysis bullosa ac- quisita and not bullous pemphigoid antibodies, demonstrating that there are patients with a diag- nosis of bullous pemphigoid who actually have epidermolysis bullosa acquisita. 73 Recently it has been proposed that the name epidermolysis bullosa acquisita be changed to dermolytic pemphigoid to emphasize its close resemblance to bullous pem- phigoid. Criteria for the diagnosis of dermolytic pemphigoid would include (1) a chronic bullous disease, (2) subepidermal blisters, (3) linear de- posits of IgG at the basement membrane zone, and (4) IgG deposits in the papillary dermis beneath the lamina densa. 69
Volume 16 Number 5, Part 1 May 1987 Butlous pemphigoid 915
PATHOLOGIC STUDY Light microscopy
The major histologic feature in bullous pem- phigoid is a subepidermal blister with a normal epidermis (Fig. 3). Since blisters may arise on either normal or erythematous skin, microscopic findings will vary depending on the biopsy site. Blisters arising on a nonerythematous base show a mild perivascular infiltrate admixed with some eosinophils and are often referred to as "infiltrate poor." When biopsy specimens are taken from blisters arising on an erythematous base, marked cellularity is noted in the papillary dermis, both perivascularly and in the blister cavity. The pre- dominant cell type is the eosinophil, but lympho- eytes, histiocytes, and neutrophils are present, and these cells are referred to as "infiltrate rich" le- sions. Early blisters are subepidermal.
After approximately 2 days, regeneration of the epidermis in the floor of the blister begins at the periphery and gradually extends over the entire floor, resulting in an apparent intraepidermal blis- ter. Necrosis of the overlying epidermis is not a feature of early lesions but may be seen in more advanced lesions. 74
Electron microscopy Ultrastructural studies of blisters arising on clin-
ically normal skin show focal thinning of the base- ment membrane, disruption of anchoring fila- ments, and dermoepidermal separation within the lamina lucida, v5 The ultrastructural features of bul- lae arising on erythematous skin show much more extensive basement membrane zone damage, in- cluding (1) disintegration of the basement mem- brane, (2) fragmentation and/or disappearance of anchoring fibrils, anchoring filaments, and hemi- desmosomes, and (3) basal cell degeneration. 76
IMMUNOPATHOLOGIC STUDY Immunofluorescence microscopy
The immunofluorescence studies of Beutner et a177 and Jordon et al 2 defined the immunopa- thology of bullous pemphigoid and further ex- tended Lever's observations a that it was an entity distinct from pemphigus vulgaris. These investi- gators demonstrated that almost all bullous pem- phigoid patients had IgG bound to the epidermal
basement membrane zone and that most patients had circulating IgG antibodies that reacted with the basement membrane zone of normal epider- mis.2 Since that time, these observations have been amply confirmed.
The linear deposition of both IgG and C3 at the epidermal basement me~brane zone is found in the majority of patients with buUous pemphigoid (Fig. 4). In most published studies, 45% to 90% of patients have been shown to have linear IgG deposition and 80% to 100% linear C3 deposi- tion. 7.9.78 Subtyping of the IgG deposits reveals that IgG4 is found in almost all patients, followed by IgG1 and IgG3. 78 IgA and IgM deposition are each found in approximately 25% of patients. 7 IgD and IgE deposition has also been rarely reported. 7,79 Biopsy specimens obtained from perilesional skin will provide the best results for direct immuno- fluorescence. Since biopsy specimens from lower extremities generally yield many false negative results, this area should be avoided whenever possible, s°
Approximately 70% of patients with bullous pemphigoid have circulating antibasement mem- brane zone IgG antibodies detectable by standard indirect immunofluorescence technics. 2,7 IgE and IgA antibasement membrane zone antibodies also occur rarely. 41,81-83 With the use of technical mod- ifications such as overnight incubation of bullous pemphigoid serum with skin 84 and pretreatment of bullous pemphigoid serum to dissociate antibody from blocking factors, s5 so-called "occul t" anti- basement membrane zone antibodies may become detectable. Approximately 10% of patients with bullous pemphigoid have neither circulating nor tissue-bound antibodies, but these patients consis- tently show complement at the basement mem- brane zone, suggesting that complement-fixing an- tibodies are or were present. 7 Although early re- ports suggested that circulating antibody titer correlated with disease activity, subsequent studies of patients with bullous pemphigoid revealed no correlation between the indirect immunofluores- cence antibody titer and disease activity. T M These circulating autoantibodies are highly specific for bullous pemphigoid and have been found in less than one of a thousand patients examined who did not have bullous pemphigoid or other diseases

916 Korman
Joumal of the American Academy of
Dermatology
known to be associated with circulating antibase- ment membrane zone antibodies: 1
Immtmoelec t ron microscopy
Immunoelectron microscopy performed on le- sions reveals deposition of immune reactants within the upper portion of the lamina lucida in patients with bullous pemphigoid. Patients with cicatricial pemphigoid have immune reactants de- posited at a lower level of the lamina lucida, sug- gesting that a different antigen may be i nvo lved :
PATHOPHYSIOLOGIC STUDY
Bullous pemphigoid antigen
Patients with bullous pemphigoid have a cir- culating antibody that binds specifically to a nor- mal basement membrane zone component--the bullous pemphigoid antigen, s7 The bullous pem- phigoid antigen is a component of the basement membrane of stratified squamous epithelia of all vertebrates 88 and is also found in the basement membrane of urethra, bladder, bronchi, and gall- bladder, s9 The bullous pemphigoid antigen is also expressed by cultured keratinocytes, 9° is synthe- sized by epidermal basal cells, 91 and has recently been partially characterized as a 220,000-dalton protein. 92 The bullous pemphigoid antigen is found both extracellularly in the lamina lucida 9a and intracellularly in association with hemides- mosomes 94-96
Various roles for the bullous pemphigoid antigen in normal skin have been proposed,* including (1) direction of normal keratinocyte differentiation, since the basement membrane zone of basal cell carcinoma patients is selectively deficient in the bullous pemphigoid antigen, 97 and (2) substrate attachment of basal cells during epidermal cell mi- gration in wound healing. 98
Circulating bullous pemphigoid antibodies
Circulating antibodies are found in the serum of most patients with bullous pemphigoid and are directed against the bullous pemphigoid antigen. Although it has been hypothesized that immune tolerance to the bullous pemphigoid antigen could
*Stanley JR. Bullous pemphigoid. Derrnatol Clin 1983;1:205-216.
play a role in the formation of these antibodies, this hypothesis is not supported by the finding that patients with bullous pemphigoid have normal sup- pressor cell function. 99,1°° Bullous pemphigoid an- tibodies are functionally heterogeneous, consisting of complement-activating and non-complement- activating antibodies, l°J Complement-activating antibodies, which are primarily of the IgG3 sub- class in bullous pemphigoid, ~o~ are thought to play the major pathogenic role in bullous pemphi- gold. t°2 However, it has been demonstrated that IgG4, which is generally not capable of activating complement, is the predominant subclass of IgG found in the serum of patients with bullous pem- phigoid. 7s It is important to emphasize that anti- body alone, in the absence of other inflammatory mediators, does not result in bullous pemphigoid blister formation. ~°3 This contrasts sharply with pemphigus vulgaris, in which antibody alone, in the absence of complement and inflammatory me- diators, can cause acantholysis and blister for- mation. ,04
Complement
In vitro studies have demonstrated that most circulating antibasement membrane zone antibod- ies can lead to complement deposition at the base- ment membrane zone. ~°2 C3 is most frequently observed at the basement membrane zone by direct immunofluorescence, and immunoelectron micro- scopic studies demonstrate C3 in the lamina lu- cida, which is at the same site where the blister is formed. 105 Other complement components, includ- ing Clq, C4, C5, properdin, factor B, and B1H globulin, have also been found at the basement membrane zone, indicating classic complement pathway activation with alternate pathway ampli- fication, x°6q°9 More recently, deposition of the membrane attack complex (C5-C9) has been found in bullous pemphigoid lesions, demonstrating that complement activation has proceeded to comple- tion.l~° Functional evidence for the activation of complement in bullous pemphigoid lesions comes from the observation of reduced total hemolytic complement, as well as reduced levels of individ- ual complement components in bullous pemphi- goid blister fluids, nl
Volume 16 Number 5, Part 1 May 1987 Bullous pemphigoid 917
Immune complexes
Circulating immune complexes have been iden- tified in 20% to 45% of patients with bullous pem- phigoid, m-.4 These immune complexes generally correlate with the presence of active disease. ~3,114 An inverse relationship between the presence of circulating antibasement membrane zone antibody and circulating immune complexes was noted in one study. 114 These findings suggest that bullous pemphigoid antigen may be produced in excess and may even circulate, thus providing a nidus for immune complex formation, 114 Although it is not known whether circulating immune complexes play a primary role in the pathogenesis of bullous pemphigoid or are formed as a reactive phenom- enon secondary to tissue injury, current opinion supports the latter hypothesis. 115
The important role of tissue-deposited immune complexes has recently been studied with the use of an in vitro model system, H6 Peripheral blood leukocytes were suspended in serum with and without complement and then incubated with sec- tions of lesional and adjacent normal-appearing skin from patients with bullous pemphigoid, The results demonstrated significantly greater leuko- cyte attachment to the basement membrane zone of lesional bullous pemphigoid skin in comparison with clinically normal bullous pemphigoid skin and control skin. Additionally, there was a sig- nificant decrease in leukocyte attachment in the absence of complement. 116 These studies provide functional evidence for the presence of comple- ment-activating immune complexes in lesional skin of bullous pemphigoid patients.It6
Cellular interactions and soluble mediators
The importance of inflammatory cells in the pro- duction of bullous pemphigoid lesions has been demonstrated by several investigators. Morpho- logic studies have shown that mast cells are closely adjacent to the basement membrane zone in bul- lous pemphigoid lesions and that they subse- quently degranulate, releasing their cellular con- tents. 117-119 Elevated levels of histamine have been reported in blister fluid obtained from patients with bullous pemphigoid, further supporting the role of mast cell activation. 12° Following mast cell de-
granulation, an influx of lymphocytes and eosin- ophils is seen. 1~7,119 Eosinophil chemotactic factor of anaphylaxis, which may aid in eosinophil re- cruitment, has been found in the blister fluid 82 and serum TM of patients with bullous pemphi- gold. Eosinophils accumulate at the lamina lucida and subsequently degranulate, releasing their gran- ular contents, including several proteolytic en- zymes. 118,n9 With the use of human skin explants cultured with bullous pemphigoid blister fluid in vitro, it has been found that dermoepidermal junction separation can be blocked by the addition of a2-macroglobulin, a universal proteinase inhib- itor. 122 The importance of proteinases in the patho- genesis of bullous pemphigoid lesions is under- scored by these observations. The continued stim- ulation and activation of eosinophils may be affected by an eosinophil-stimulating material found in bullous pemphigoid blister fluids.123 An interesting report of elevated bullous pemphigoid blister fluid levels of eosinophil major basic pro- tein, a cytotoxic protein found in eosinophil gran- ules, has appeared in abstract form. 124
Lymphocytes are also found near the basement membrane zone of bullous pemphigoid lesions and are among the first cells to migrate there . 117,n9
The role of lymphocytes in lesion production is poorly understood; however, lymphokines with chemoattractant activity ~25 and lymphotoxin-like activity 1'-~ have been identified in bullous pem- phigoid blister fluid. Lymphocytes can also elab- orate histamine-releasing factor . 127 Diminished levels of interleukin-2 have been found in lym- phocytes obtained from patients with bullous pem- phigoid, although the significance of this obser- vation is not known. 128 The role of other soluble mediators in bullous pemphigoid lesion production has not been extensively studied; however, ele- vated blister fluid levels of prostaglandin E2 have been demonstrated. ~29
MODELS FOR BULLOUS PEMPHIGOID
An in vitro model for bullous pemphigoid, using normal human skin sections incubated with bullous pemphigoid sera, complement, and peripheral blood leukocytes, was described in Gammon's lab- oratory. 13o The authors demonstrated leukocyte mi-
918 Korman
Journal of the American Academy of
Dermatology
gration toward, and attachment to, the basement membrane zone. Migration and attachment were dependent on the presence of complement-fixing bullous pemphigoid antibodies and human serum as a complement source. Leukocytes that attached to the basement membrane zone were activated and produced focal areas of basement membrane zone separation similar to that seen in early bullous pemphigoid lesions. No leukocyte attachment or basement membrane zone separation occurred when heat-inactivated serum, C2-deficient serum, or decomplemented serum was used or when bul- lous pemphigoid antibodies were omitted. These experiments support the important role of anti- body, complement, and activated leukocytes in buUous pemphigoid lesion production.13°
An in vivo model of bullous pemphigoid was recently developed with the use of partially puri- fied bullous pemphigoid IgG injected into normal rat corneas. ~3~ Linear deposition of IgG and C3 at the corneal basement membrane was seen 24 hours afterward. Within 48 hours, 90% of the injected corneas had eosinophil and neutrophil infiltration, with 30% revealing subepidermal blister forma- tion. The intensity of inflammation correlated with the in vitro complement fixation titers of the bul- lous pemphigoid IgG fractions in most cases. TM
Attempts to induce bullous pemphigoid lesions in skin by intradermal injection of partially purified bullous pemphigoid IgG into rabbit ear skin have been unsuccessful. 131
Another in vivo model of bullous pemphigoid has been developed that successfully reproduces the skin lesions of bullous pemphigoid. 132 The au- thors utilized high-titer, concentrated, partially pu- rified bullous pemphigoid IgG antibodies injected intradermally into the skin of guinea pigs. They noted the development of in vivo dermoepidermal junction separation within 6 hours of intradermal injection of partially purified bullous pemphigoid IgG or concentrated high-titer bullous pemphigoid serum. Within 24 hours after injection, approxi- mately 75% of injected guinea pigs developed sep- aration at the dermoepidermal junction. Histologic examination revealed infiltration of eosinophils and lymphocytes at the dermoepidermal junction, and direct immunofluorescence revealed linear de- position of C3 and IgG. t32 The injection of known
inhibitors of leukocyte function and migration, in- cluding colchicine, ethylenediamine tetraacetic acid, and betamethasone, prior to injection of bul- lous pemphigoid IgG inhibited leukocyte migra- tion and subsequent dermoepidermal junction separation. When bullous pemphigoid IgG was in- jected into C3-depleted guinea pigs, dermoepi- dermal junction separation was inhibited in all an- imals, whereas most, but not all, C4-deficient an- imals demonstrated dermoepidermal separation after injection with bullous pemphigoid IgG. These results demonstrate the crucial role that leu- kocyte migration plays in bullous pemphigoid blis- ter formation and also highlight the important role of the alternate complement pathway. 132 The im- portance of an elevated local concentration of high- titer bullous pemphigoid antibodies in producing blisters in vivo is supported by this study 132 and may explain why other investigators have been unable to induce bullous pemphigoid lesions in animal skin.
HYPOTHESIS FOR THE PATHOGENESIS OF LESION FORMATION
Based on the experimental evidence presently available, the following mechanism to explain the pathophysiology of blister formation in bullous pemphigoid has recently been proposed by Jordon et al. 133
The first step, which is the result of an unknown stimulus, is to convert the bullous pemphigoid an- tigen into an immunogenic signal. B cell clones are produced and then activated to become plasma cells, and IgG antibodies are synthesized. These IgG antibodies bind to the bullous pemphigoid antigen within the lamina lucida and initiate com- plement activation. Several inflammatory media- tors are produced, including the anaphylatoxins-- C3a and C5a. Lymphocytes, eosinophils, and neu- trophils migrate to the site of injury, and mast cell activation and degranulation also occur. Although the cause of mast cell activation is unknown, com- plement anaphylatoxins and bullous pemphigoid antigen-antibody complexes are thought to play the major role. to2 In light of recent evidence demon- strating the predominance of non-complement- fixing IgG4 antibody at the basement membrane zone and circulating in the serum of bullous pem-

Volume 16 Number 5, Part 1 May 1987 BuUous pemphigoid 919
phigoid patients, vs along with the reported homo- cytotropic properties of IgG4 for mast cells, TM it is likely that in addition to complement activation, other mechanisms may lead to mast cell activa- tion. TM Once activated, the mast cell releases sev- eral proinflammatory mediators, including eosin- ophil chemotactic factor of anaphylaxis, high-mo- lecular-weight neutrophil chemotactic factor, and possibly histamine, proteolytic enzymes, and eo- sinophil-stimulating material. As a consequence, neutrophils and eosinophils are activated, resulting in further release of inflammatory mediators in- cluding lysosomal proteolytic enzymes. Dermo- epidermal junction separation occurs either as a result of direct cytotoxic action or because of the effect of lysosomal proteolytic enzymes. The end result is a subepidermal blister. Lymphocyte elab- oration of histamine-releasing factor with subse- quent histamine release could lead to further mast cell degranulation and continued blister for- mation. 133
TREATMENT
Bullous pemphigoid is generally a benign dis- ease and usually has a self-limiting course. The mortality rate is low even in the absence of treat- ment, although death may occur in some elderly or debilitated patients. ~ Since the factors that ini- tiate bullous pemphigoid antibody production are not understood, current treatment of bullous pem- phigoid is, of necessity, directed at the pathologic process rather than at the primary cause.
The major form of therapy for bullous pemphi- goid is the administration of systemic glucocorti- costeroids. Numerous pharmacologic effects of corticosteroids have been elucidated, but most in- vestigators believe that it is their anti-inflammatory properties that are of primary importance in ex- plaining their beneficial effects in bullous pem- phigoid patients. These properties include inhibi- tion of lysosomal enzyme release, inhibition of leukocyte chemotaxis, and inhibition of B lym- phocyte function with subsequent diminution in immunoglobulin production.
Most therapeutic regimens are based on clinical experience, and no controlled studies comparing patients treated by means of systemic glucocorti- costeroids with nontreated control patients have
been published. However, a vast body of clinical experience supports the efficacy of glucocortico- steroids in the treatment of patients with bullous pemphigoid. Patients with localized bullous pem- phigoid often respond well to topical glucocorti- costeroids. 7'4~ Patients with more extensive disease require oral glucocorticosteroids in moderate to high doses (equivalent to 1 mg/kg/day or more of prednisone) to control the eruption. Many authors have suggested the use of cytotoxic agents, either azathioprine or cyclophosphamide, in addition to systemic glucocorticosteroids: '9'33 The rationale for the use of these agents is their purported im- munosuppressive and steroid-sparing effects. To date, no controlled studies have verified this con- cept. Nonetheless, extensive clinical experience supports the utility of the immunosuppressive agents, particularly azathioprine, in patients whose condition cannot be controlled with glucocorti- eosteroids alone or in whom high-dose systemic glucocorticosteroid therapy cannot be tolerated or is contraindicated.
Recently high-dose pulse therapy (1 gm/day of intravenous methylprednisolone for 3 consecutive days) has been reported to be successful in the management of eight patients with severe gener- alized bullous pemphigoid.~a5 Maintenance treat- ment after pulse therapy was with 0.4 mg/kg/day of orally administered prednisone. The authors ob- served a marked decrease in blistering within 1 day of the first treatment, and the number of new blisters decreased by 97% after the third dose. Recrudescent blistering was always less severe than before treatment. One severely ill patient died of presumed septicemia 5 days after treatment, t35 Pulse therapy has been used to treat many other autoimmune diseases, and reported side effects in- clude hypertension, infection, anaphylaxis, and myocardial infarction; in addition, death may en- sue. 136 Although this form of therapy may have some benefit in the treatment of bullous pemphi- goid, its efficacy needs to be evaluated in an ap- propriately designed and controlled study. At this time it seems prudent to reserve pulse therapy only for those bullous pemphigoid patients with the most severe generalized disease who are un- responsive to other standard therapeutic inter- ventions.
920 Korman Journal of the
American Academy of Dermatology
A small percentage of patients with bullous pemphigoid respond to treatment with either sul- fapyridine or dapsone. ~7 Most of these patients tend to be younger, and many have associated di- abetes mellitus. Histologic examination of skin bi- opsy specimens from these sulfone-responsive pa- tients reportedly shows greater numbers of neu- trophils and fewer eosinophils than are generally seen in bullous pemphigoid lesions. ~37
The use of plasma exchange as an adjunct to systemic glucocorticosteroid therapy in bullous pemphigoid patients was recently investigated. 138 A series of thirty-seven patients was treated with oral prednisolone, 0.3 mg/kg/day, and twenty-two of these patients were also treated with plasma exchange. Patients treated with both glucocorti- costeroids and plasma exchange required signifi- cantly lower doses of glucocorticosteroids to con- trol their disease than did patients treated with glucocorticosteroids alone. The authors ~3~ were unable to demonstrate any greater benefit of plasma exchange in patients with circulating bul- lous pemphigoid antibodies in comparison with patients without circulating antibody. Morbidity associated with this therapy includes fever, chills, hypotension, and difficulties with venous access. Proposed mechanisms to explain the observed beneficial effects include immune complex clear- ance and depletion of circulating complement components. 138
Cyelosporine, an immunosuppressive agent originally used to prevent graft rejection in organ transplant patients, has recently been reported to be of benefit in the treatment of two patients with bullous pemphigoid. 139 Further trials are needed to determine what role this agent may play in the management of patients with bullous pemphigoid.
REFERENCES
1. Lever WF. Pemphigus. Medicine 1953;32:1-123. 2. Jordon RE, Beutner EH, Witebsky E, Blumenthal G,
Hale WL, Lever WF. Basement membrane zone anti- bodies in bullous pemphigoid. JAMA 1967;200:751-6.
3. Lever WF. Pemphigus and pemphigoid. Springfield, IL: Charles C Thomas, Publisher, 1965.
4. Robison JW, Odom RB. Bullous pemphigoid in chil- dren. Arch Dermatol 1978;114:899-902.
5. Ahmed AR, Konqui A, Park MS, Tiwari JL, Terasaki PI. DR antigens in bullous pemphigoid. Arch Dermatol 1984;120:795,
6. Goldberg DJ, Sabolinski M, Bystryn JC. Regional vari- ation in the expression of bullous pemphigoid antigen and location of lesions in bullous pemphigoid. J Invest Dermatol I984;82:326-8.
7. Ahmed AR, Maize JC, Provost TT. Bullous pemphi- goid: Clinical and immunologic follow-up after suc- cessful therapy. Arch Dermatol 1977;113:1043-6.
8. Hodge L, Marsden RA, Black MM, Bhogal B, Corbett MF. Bullous pemphigoid: the frequency of mucosal in- volvement and concurrent malignancy related to indirect immunofluorescence findings. Br J Dermatol 1981; 105:65-9.
9. Person JR, Rogers RS. Bullous and eicatricial pem- phigoid. Mayo Clinic Proc 1977;52:54-66,
10. Laskaris G, Sklavounou A, Stratigos J. Bullous pem- phigoid, cicatricial pemphigoid and pemphigus vul- garis. Oral Surg 1982;54:656-62.
11. Barker DJ. Generalized pruritus as the presenting fea- ture of bullous pemphigoid. Br J Dermatol 1983; 109:237-8.
12. Bingham EA, Burrows D, Sandford JC. Prolonged pru- ritus and bullous pemphigoid. Clin Exp Dermatol 1984;9:564-70.
13. Koerber WA, Price NM, Watson W. Coexistent pso- riasis and bullous pemphigoid. Arch Dermatol 1978; 114:1643-6.
14. Cram DL, Fukayama K. Immunohistochemistry of ul- traviolet-induced pemphigus and pemphigoid lesions. Arch Dermatol 1972; 106:819-24,
15. Thomsen K, Sehmidt H. PUVA-induced bullous pem- phigoid. Br J Dermatol 1976;95:568-9.
16. Fellner M J, Katz JM. Occurrence of bullous pemphi- goid after furosemide therapy. Arch Dermatol 1976; 112:75-7.
17. Savin JA. The events leading to the death of patients with pemphigus and pemphigoid. Br J Dermatol 1979; 101:521-34.
18. Callen JP. Internal disorders associated with bullous disease of the skin. J AM ACAD DERMATOL 1980;3: 107-19.
19. Lynfield YL, Green K, Gopal R. Bullous pemphigoid and multiple autoimmune disease. J AM AChD DER- MATOL 1983;9:257-61.
20. StollDM, KingLE. Association ofbullous pemphigoid with systemic lupus erythematosus. Arch Dermatol 1984;120:362-6.
21. Chorzelski JP, Maciejowski E, Jablonska S, et al. Co- existence of pemphigus and bullous pemphigoid. Arch Dermatol 1974;109:849-53.
22. Hamilton DV, McKenzie AW. Bullous pemphigoid and primary biliary cirrhosis. Br J Dermatol 1978;99: 447-50.
23. Bloomfield S, Stockdill G, Barnetson RSC. Thymic hypoplasia, autoimmune hemolytic anemia and juvenile pemphigoid ifi an infant. Br J Dermatol 1982;106: 353-5.
24. Simjee S, Konqui A, Ahmed AR. Multiple sclerosis and bullous pemphigoid, Dermatologica 1985;170: 86-9.
25. Peck SM, Lefkovits AM. Bullous pemphigoid with polymyositis and coexisting contact dermatitis. Arch Dermatol 1966;94:672-4.
Volume 16 Number 5, Part 1 May 1987
Bullous pemphigoid 921
26. Bean SF, Good RA, Windhorst DB. Bullous pemphi- gold in an l 1-year-old boy. Arch Dermatol 1970; 102:205-8.
27. How J, Bewsher PD, Stankler L. Bullous pemphigoid, polymyalgia rheumatica and thyroid disease. Br J Der- matol 1980;103:201-4.
28. James WD. Bullous pemphigoid, myasthenia gravis and thymoma. Arch Dermatol 1984;120:397.
29. Bryning K, Leslie J. Factor V inhibitor and bullous pemphigoid. Br Med J 1977;1:677-8.
30. Downham JF, Chapel TA. Bullous pemphigoid: therapy in patients with and without diabetes mellitus. Arch Dermatol 1978;114:1639-42.
31. Chuang TY, Korkij W, Soltani K, Clayman J, Cook J. Increased frequency of diabetes mellitus in patients with bullous pemphigoid: a case-control study. J AM ACAO DERMATOL 1984;6:1099-102.
32. Grattan CEH. Evidence of an association between bul- lous pemphigoid and psoriasis. Br J Dermatol 1985; 113:281-3.
33. Lever WF. Pemphigus and pemphigoid. J AM ACAD Dr~r~MATOL 1979;1:2-31.
34. Ahmed AR, Chu TM, Provost TT. Bullous pemphigoid: clinical and serologic evaluation for associated malig- nant neoplasms. Arch Dermatol 1977;113:969.
35. Chorzelski TP, Jabonskla S, Maciejowska E, Beutner EH, Wronkowski L. Coexistence of malignancies with bullous pemphigoid. Arch Dermatol 1978;114:964.
36. Stone SP, Schroeter AL. Bullous pemphigoid and as- sociated malignant neoplasms, Arch Dermatol 1975; 111:991-4.
37. Venecie PY, Rogers RS, Schaeter AL. Bullous pemphi- gold and malignancy: relationship to indirect immu- nofluoreseence findings. Acta Derm Venereol (Stoekh) 1984;64:316-9.
38. Bushkell LL, Jordon RE. Bullous pemphigoid: a cause of peripheral blood eosinophilia. J AM ACAO DERMATOL 1983;8:648-51.
39. Arbesman CE, Wypych JI, Reisman RE, Beutner EH. IgE levels in sera of patients with pemphigus or bullous pemphigoid. Arch Dermatol 1974;110:378-81.
40. Stevenson CJ. Treatment in bullous disease with eor- ticosteroid drugs and corticotrophin. Br J Dermatol 1960;72:11-21.
41. Provost TT, Maize JC, Ahmed AR, Strauss JS, Dobson RL. Unusual subepidermal bullous diseases with im- munologic features of bullous pemphigoid. Arch Der- matol 1979; 115:156-60.
42. Person JR, Rogers RS, PeiTy HO. Localized pemphi- gold. Br J Derrnatol 1976;95:531-4.
43, Marsden RA, McKee PH, Bhogal B, Black MM, Ken- nedy LA. A study of benign chronic bullous dermatosis of childhood and comparison with dermatitis herpeti- formis and bullous pemphigoid occurring in childhood. Clin Exp Dermatol 1980;5:159-72.
44. Bean SF, Michel B, Furey N. Vesicular pemphigoid. Arch Derrnatol 1976;112:1402-4.
45. Honeyman JF, Honeyman AR, De la Parra MA, Pinto A, Eguiguren G. Polymorphic pemphigoid. Arch Dermatol 1979; 115:423-7.
46. Leonard JN, Haffenden GP, Ring NP, et al. Linear IgA disease in adults. Br J Dermatol 1982;107:301-16.
47. Winldeman RK, Su WPD. Pemphigoid vegetans. Arch Dermatol 1979;115:446-8.
48. A1-Najjar A, ReiIly GD, BIeehen SS. Pemphigoid veg- etans: a case report. Acta Derm Venereol (Stockh) 1984;64:450-2.
49. Kuokkanen K, Helin H. Pemphigoid vegetans: report of a case. Arch Dermatol 1981;117:56-7.
50. Yung CW, Soltani K, Lorinez AL, Pemphigoid nodu- laris. J AM Ac,~a3 DERMATOL 1981 ;5:54-60.
51. Tappeiner G, Konrad K, Holubar K. Erythrodermic bul- lous pemphigoid: Report of a case. J A~ ACAD DER- MATOL 1982;6:489-92.
52. Bean SF, Waisman M, Michel B, Thomas CI, Knox JM, Levine M. Cicatricial pemphigoid: immunoflu- orescent studies. Arch Dermatol 1972;106:195-9.
53, Fine JD, Neises GR, Katz SI. Immunofluorescence and immunoeleetron microscopic studies in cicatricial pem- phigoid. J Invest Dermatol 1984;82:39-43.
54. Mondino B J, Brown SI, Rabin BS. HLA antigens in ocular cicatricial pemphigoid. Arch Ophthalmol 1979; 97:479.
55. Rogers RS, Seehafer JR, Perry HO. Treatment of cic- atricial pemphigoid with dapsone. J AM ACAD D~R- MATOL 1982;6:215-23.
56. Fine JD. Epidermolysis bullosa: variability of expres- sion of cicatricial pemphigoid, bullous pemphigoid, and epidermolysis bullosa acquisita antigens in clini- cally uninvolved skin, J Invest Dermatol 1985;85: 47 -9.
57. Brunsting LA, Perry HO. Benign pempbigoid? A report of seven cases with chronic, scarring, herpetiform plaques about the head and neck, Arch Dermatol 1957;75:489-501,
58. Shomick JK, Bangert JL, Freeman RG, Gilliam JN. Herpes gestationis: clinical and histologic features of twenty-eight cases. J AM ACAO DEmaATOL 1983;8: 214-24.
59. Jordon RE, Heine KG, Tappeiner G, BushkeI1LL, Pro- vost TT. The immunopathology of herpes gestationis: immunofluorescence studies and characterization of "FIG factor." J Clin Invest 1976;57:1426-33.
60. Carruthers JA, Ewins R. Herpes gestationis: studies on the binding characteristics, activity and pathogenetic significance of the complement-fixing factor. Clin Exp Immunol 1978;3l:38-44.
61. Katz SI, Hertz KC, Yaoita H: Herpes gestationis: im- munopathology and characterization of the HG factor. J Clin Invest 1976;57:1434-41.
62. Holmes RC, Black MM, Jurecka W, et al. Clues to the etiology and pathogenesis of herpes gestationis. Br J Dermatol 1983; 109:131-9.
63. Holmes RC, Black MM. The specific dermatoses of pregnancy. J AM ACAD DERMATOL 1983;8:405-12.
64. Katz SI. The epidermal basement membrane zone-- structure, ontogeny and role in disease. J AM ACAD DERMATOL 1984;11 : 1025-37,
65. Lawley TJ, Strober W, Yaoita H, Katz SI. Small in- testinal biopsies and HLA types in dermatitis herpeti- formis patients with granular and linear IgA skin de- posits. J Invest Dermatol 1980;74:9-12.
66. Sasazuki T, McDevitt I-IO, Grumet FC. The association between genes in the major histocompatibility complex
922 Korman
Journal of the American Academy of
Dermatology
and disease susceptibility. Ann Rev Med 1977;28: 425-52.
67, Yaoita H, Katz SI. Circulating IgA antibasement mem- brane zone antibodies in dermatitis herpetiformis. J In- vest Dermatol 1977;69:558-60.
68. Roenigk HH, Ryan JG, Bergfeld WF. Epidermolysis bullosa acquisita: report of three cases and review of all published eases. Arch Derraatol 1971;103:1-10.
69. Briggaman RA, Gammon WR, Woodley DT. Epider- molysis bullosa acquisita of the immunopathological type (dermolytic pemphigoid). J Invest Dermatol 1985; 85(suppl):79-84.
70. Yaoita H, Briggaman RA, Lawley TJ, Provost TT, Katz SI. Epidermolysis bullosa acquisita: ultrastructural and immunological studies. J Invest Dermatol 1981;76: 288-92,
71, Woodley DT, Bfiggaman RA, O'Keefe EJ, Inman AD, Queen LL, Gammon WR. Identification of the skin basement membrane autoantigen in epidermolysis bul- losa acquisita. N Engl J Med 1984;310:1007-13.
72. Gammon WR, Briggaman RA, Wheeler CE Jr, Epi- dermolysis bullosa acquisita presenting as an inflam- matory builous disease. J AM ACAD DERMATOL 1982; 7:382-7.
73. Gammon WR, Briggaman RA, Woodley DT, Heald PW, Wheeler CE. Epidermolysis bullosa acquisita--a pemphigoid-like disease. J AM ACAD DERMhTOL 1984; 11:820-32.
74. Lever WF, Schaumburg-Lever G. Histopathology of the skin. 6th ed. Philadelphia: JB Lippincott, 1983: 113-7.
75. Kobayashi T. The dermo-epidermal junction in bullous pemphigoid: an electron microscopic study. Dermato- logica 1967;134:157-65.
76. Schaumburg-Lever G, Orfanos CE, Lever WF: Electron microscopic study of bullous pemphigoid. Arch Der- matol 1972;106:662-7.
77. Beutner EH, Lever WF, Witebsky E, et al. Autoanti- bodies in pemphigus vulgaris: response to an intercel- lular substance of epidermis. IAMA 1965;192:682-8.
78. Bird P, Friedmann PS, Ling N, Bird AG, Thompson RA. Subclass distribution of IgG autoantibodies in bul- lous pemphigoid, J Invest Dermatol 1986;86:21-5.
79. Provost TT, Tomasi TB. Immunopathology of bullous pemphigoid: basement membrane deposition of IgE, alternate pathway components and fibrin. Clin Exp Im- munol 1974;18:193-200.
80. Weigand DA. Effect of anatomic region on immunoflu- orescence diagnosis of bullous pemphigoid. J AM ACAD DERMATOL 1985;12;274-8.
81. Nieboer C, van Leeuwen HIE. IgE in the serum and on mast cells in bullous pemphigoid. Arch Dermatol 1980;116:555-6.
82. Baba J, Sonozaki H, Seki K, Uchiyama M, Ikesawa Y, Toriso M. An eosinophil chemotaetic factor present in blister fluids ofbullous pemphigoid patients. J Immunol 1976;116:112-6.
83. Ullman S, Halberg P, Nielsen R. Anti-basement mem- brane antibodies in sera from patients without bullous pemphigoid. Acta Derm Venereol (Stockh) 1975;55: 305-8.
84, Kumar V, Binder WL, Schotland E, Beutner EH, Chor-
zelski TP. Coexistence of bullous pemphigoid and sys- temic lupus erythematosus. Arch Dermatol 1978;114: 1187-90.
85. Hermann K, Lohrisch I, Bohme HI, Haustein UF. De- tection of antibodies after immune complex splitting in serum of patients with bullous pemphigoid and systemic lupus erythematosus. Br J Dermatol 1978;99:635-40.
86. Sams WM, Jordon RE. Correlation of pemphigoid and pemphigus antibody titers with activity of disease. Br J Dermatol 1971;84:7-13.
87. Stanley JR. A specific antigen-antibody interaction trig- gers the cellular pathophysiology of bullous pemphi- gold. Br J Dermatol 1985;l13(suppl 28):67-73.
88. Diaz LA, Weiss HI, Calvanlco NJ. Phylogenetic studies with pemphigus and pemphigoid antibodies, Aeta Derm Venereol (Stockh) 1978;58:537-40.
89. Beutner EH, Jordon RE, Chorzelski TP. The immu- nopathology of pemphigus and bullous pemphigoid. J Invest Dermatol 1968;51:63-80.
90. Stanley JR, Hawley-Nelson P, Yuspa SH, Shevach EM, Katz SI. Characterization of bullous pemphigoid anti- gen: a unique basement membrane protein of stratified squamous epithelia. Cell 1981;24:897-903.
91. Woodley DT, Didierjean L, Regnier M, Saurat J, Pru- nieras M, Bullous pemphigoid antigen synthesized in vitro by human epidermal cells. J Invest Dermatol 1980;75:148-51.
92. Stanley JR, Woodley DT, Katz SI. Identification and partial characterization of pemphigoid antigen extracted from normal human skin. J Invest Dermatol 1984; 82:108-11.
93. Stanley JR, Woodley DT, Katz SI, Martin GR. Structure and function of basement membrane. J Invest Dermatol 1982;79(suppl):69-72.
94. Regnier M, Vaigot P, Michel S, Prunieras M. Location of bullous pemphigoid antigen in isolated human kera- tinocytes. J Invest Dermatol 1985;85:187-90.
95. Westgate GE, Weaver AC, Couchman JR. Bullous pem- phigoid antigen localization suggests an intracellular association with hemidesmosomes. J Invest Dermatol 1985;84:218-24.
96. Mutasim DR, Takahashi Y, Labib RS, Anhalt GJ, Patel HP, Diaz LA. A pool of bullous pemphigoid antigen is intracellular and associated with the basal cell cyto- skeleton-hemidesmosome complex. J Invest Dermatol 1985 ;84:47-53.
97. Stanley JR, Beckwith JB, Fuller RP, Katz SI. A specific antigenic defect of the basement membrane is found in basal cell carcinoma but not in other epidermal tumors. Cancer 1982;50:1486-90.
98. Stanley JR, Alvarez OM, Bere EW, Eaglstein WH, Katz SI. Detection of basement membrane zone antigens dur- ing epidermal wound healing in pigs. J Invest Dermatol 1981 ;77:240-3.
99. King AJ, Schwartz SA, Lopatin D, Voorhees JJ, Diaz LA. Suppressor cell function is preserved in pemphigus and pemphigoid. 1 Invest Dermatol 1982;79:183-5.
100. Ahmed AR. Suppressor cell functions in bullous pem- phigoid. Arch Dermatol Res 1985;277:307-12.
101. Sams WM, Schur PH: Studies of the antibodies in pem- phigoid and pemphigus. J Lab Clin Med 1973;82: 249-54.
Volume 16 Number 5, Part 1 May 1987
Bullous pemphigoid 923
102. Sams WM Jr, Gammon WR. Mechanism of lesion pro- duction in pemphigus and pemphigoid. J AM ACAD DER- MA'tOg 1982;6:431-52.
103. Pehamberger H, Gschnait F, Konrad K, Holubar K: Bullous pemphigoid, herpes gestationis and linear der- matitis herpetiformis: circulating anti-basement mem- brane zone antibodies; in vitro studies. J Invest Der- matol 1980;74:105-8.
104. Schiltz JR, Michel B. Production of epidermal acan- tholysis in normal human skin in vitro by the IgG frac- tion from pemphigus serum. J Invest Dermatol 1976; 67:254-60.
105. Schmidt-Ullrich B, Rule A, Schaumburg-Lever G, Leblanc C. Ultrastructural localization of in vivo bound complement in bullous pemphigoid. J Invest Dermatol 1975;65:217-9.
106. Carlo JR, Gammon WR, Sams WM, Ruddy S. Dem- onstration of the complement regulating protein, BIH, in skin biopsies from patients with bullous pemphigoid. J Invest Dermatol 1979;73:551-3.
107. Jordon RE, Nordby JM, Milstein H. The complement system in bullous pemphigoid: fixation of Clq and C4 by pemphigoid antibody. J Lab Clin Med 1975;86: 733-40.
108. Provost TT, Tomasi TB. Evidence for complement ac- tivation via the alternate pathway in skin disease: herpes gestationis, systemic lupus erythematosus and bullous pemphigoid. J Clin Invest 1973;52:1779-87.
109. Gammon WR, Merritt CC, Lewis DM, Sams WM, Wheeler CE, Carlo J. Leukocyte chemotaxis to dermal- epidermal junction of human skin mediated by pem- phigoid antibody and complement: mechanism of cell attachment in the in vitro leukocyte attachment method. J Invest Dermatol 1981;76:514-22.
110. Dahl MV, Falk RJ, Carpenter R, Micheal AF. Depo- sition of the membrane attack complex of complement in bullous pemphigoid. J Invest Dermatol 1984;82: 132-5.
111. Jordon RE, Day NK, Sams WM, Good RA. The com- plement system in bullous pemphigoid: complement and component levels in sera and blister fluids. J Clin Invest 1973;52:1207-13.
112. Jordon RE, McDuffie FC. Serum and blister fluid an- ticomplementary activity in pemphigus and bullous pemphigoid: sucrose density gradient studies. Proc Soc Exp Biol Med 1976;151:594-8.
113. Tappeiner G, Heine KG, Kahl JC, Jordan RE. Clq bind- ing substances in pemphigus and bullous pemphigoid. Clin Exp Immunol 1977;28:40-8.
114. Gomes MA, Dambuyant C, Thivolet J, Bussy R. Bul- lous pemphigoid: a correlative study of autoantibodies, circulating immune complexes and dermo-epidennal deposits. Br J Dermatol 1982;107:43-52.
115. Yancey KB, Lawley TJ. Circulating immune com- plexes: their immunochemistry, biology and detection in selected dermatologic and systemic diseases. J Ar~ ACAD DERMATOL 1984; 10:711-31.
116. Gammon WR, Merritt CC, Lewis DM, Sams WM, Wheeler CE, Carlo JR. Functional evidence for com- plement-activating immune complexes in the skin of patients with bullous pemphigoid. J Invest Dermatol 1982;78:52-7.
117. Wintroub BU, Mihrn MC, Goetzl EJ, Soter NA, Austen KF. Morphologic and functional evidence for release of mast cell products in bullous pemphigoid. N Engl J Med 1978;298:417-21.
118. Dubertret L, Bertaux ]3, Fosse M, Touraine R. Cellular events leading to blister formation in bullous pemphi- gold. Br J Dermatol 1980;104:615-24.
119. Dvorak AM, Mihm MC, Osage JE, Kwan TH, Austen KF, Wintroub BU. Bullous pemphigoid, an ultrastruc- rural study of the inflammatory response: eosinophil, basophil and mast cell granule changes in multiple biop- sies from one patient. J Invest Dermatol 1982;78:91- 101.
120. Katayama I, Doi T, Nishioka K. High histamine level in the blister fluid of bullous pemphigoid. Arch Der- matol Res 1984;276:126-7.
121. Czarnetzki BM, Kalveram KJ, Dierksmeier U, Serum eosinophil chemotactie factor levels in patients with bul- lous pemphigoid, drug reactions and atopic eczema. J Invest Dermatol 1979;163-5.
122. Naito K, Morioka S, Ogawa H. The pathogenic mech- anisms of blister formation in bullous pemphigoid. J Invest Dermatol 1982;79:303-6.
123. Varigos GA, Morstyn G, Vadas MA. Bullous pemphi- gold blister fluid stimulates eosinophil colony formation and activates eosinophils. Clin Exp Immunol 1982; 50:555-62.
124. Wintroub BU, Dvorak AM, Mihm MC, Gleich GJ, Bullous pemphigoid: cytotoxic eosinophil degranulation and release of eosinophil major basic protein [abstract]. J Invest Dermatol 1981 ;76:310.
125. Center DM, Wintroub BU, Austen KF. Identification of chemoattractant activity for lymphocytes in blister fluid of patients with bullous pemphigoid: evidence for the presence of a lymphokine. J Invest Dermatol 1983;81:204-8.
126. Jeffes EWB, Yamamoto RS, Ahmed AR, Granger GA. Lymphotoxin detected in the blister fluid of bullous pemphigoid patients. J Clin Immunol 1984;4:31-5.
127. Thueson DO, Speck LS, Lett-Brown MA, Grant JA. Histamine-releasing activity: production by mitogen or antigen stimulated human mononuclear cells. J Im- munol 1979;123:626-32.
128. Ahmed AR, Hijri K, Arab-Kermani V. Interleukin-2 production in bullous pemphigoid. Arch Derm Res 1984;276:330-2.
129. Strandberg K, Hagermark O. Prostaglandin F_~ in blister fluid of bullous diseases and experimental suction blis- ters. Acta Derrn Venereol (Stockh) 1977;57:487-92.
130. Gammon WR, Merritt CC, Lewis DIM, Sams WM, Carlo JR, Wheeler CE. An in vitro model of immune complex-mediated basement membrane zone separa- tion caused by pemphigoid antibodies, leukocytes, and complement. $ Invest Dermatol 1982;78:285-90.
131. Anhalt GJ, Bahn CF, Labib RS, Voorhees JJ, Sugar A, Diaz LA. Pathogenic effects of bullous pemphigoid au- toantibodies on rabbit corneal epithelium. J Clin Invest 1981;68:1097-101.
132. Naito K, Morioka S, Ikeda S, Ogawa H. Experimental bullous pemphigoid in guinea pigs: the role of pem- phigoid antibodies, complement and migrating cells. J Invest Dermatol 1984;82;227-30.
9 2 4 K o r m a n
Journal of the American Academy of
Dermatology
133. Jordon RE, Kawana S, Fritz KA. Irnmunopathologie mechanisms in pemphigus and bullous pemphigoid. J Invest Dermatol 1985;85(suppl):72-8.
134. Nakagawa T, deWeck AL. Membrane receptors for the IgG4 subclass on human basophils and mast cells. Clin Rev Allergy 1983;1:197-206.
135. Siegel J, Eaglstein WH. High-dose methylprednisolone in the treatment of bullous pemphigoid. Arch Dermatol 1984; 120:1157-65.
136. Johnson RB, Lazarus GS. Pulse therapy: therapeutic
efficacy in the treatment of pyoderma gangrenosum. Arch Derrnatol 1982;118:76-84.
137. Person JR, Rogers RS. Bullous pemphigoid responding to sulfapyridine and the sulfones, Arch Dermatol 1977;113:610-5.
138. Roujeau JC, Morel P, Dalle E, et al. Plasma exchange in bullous pemphigoid. Lancet 1984;2:486-8.
139. Thivolet J, Barthelemy H, Rigot-Muller G, et al. Effects of cyelosporin on bullous pemphigoid and pemphigus. Lancet 1985;1:334-5.
A B S T R A C T S
Acquired ichthyosiform dermatosis following a carcinoma of the vulva
Remy W, Mayerhausen W. A.kt Derrnatol 1986; 12:119-20 (German)
Acquired ichthyosis has been reported to be associated with ma- lignancy, mostly with Hodgkin's disease, Present in other patients were cancers of the breast, lung, cervix, and other areas. The authors report a patient with acquired ichthyosiform dermatosis following a cancer of the vulva. They discuss whether the skin lesiens were related to occult metastases of this tumor. Furthermore, there were histologic and immunologic findings indicating a developing cuta- neous malignant lymphoma elsewhere on the skin,
Yehudi M. Felman, M,D.
Treatment of malignant melanoma with alpha interferons
Mayerhausen W, Remy W. Akt Dermatol 1986;12:133-6 (German)
A summarized analysis of the therapeutic results in the literature (including the authors' own patients) in treatment of malignant mel- anoma with alpha interferons (or combined with cimetidine) is given. If the criteria complete response, partial response, minor response, and stable disease are summed up, 23% of the patients show remis- sion; however, if we consider only the complete and partial responses, merely 11% of the patients show remission. It is of no advantage to combine alpha intefferons with eimetidine.
Yehudi M. Felman, M.D.
Cyclosporin A in the treatment of pemphigus foliaceus and pemphigus erythematosus
Balda BR, Rosenzweig R, Hautarzt 1986;37:454-7 (German)
The authors present the cases of two female patients with pem- phigus erythematosus who did not respond to long-term azathioprine and prednisone treatment in high dosages. In both patients the skin condition improved nearly completely after therapy with cyclosporine (cyelosporin A) (3.5-6.5 mgtkglday) in combination with prednisone (7.5-10 mg every 2 days). We did not observe any side effects during 1 year of this therapy,
Yehudi M. Felman, M.D.
Treatment with factor XIII and long term follow-up of 86 patients with progressive systemic sclerosis
Guillevin L, Euller-Ziegler L, Chouvet B, et al. Presse Med 1985;14:2327-9 (French)
Eighty-six patients with progressive systemic sclerosis were given coagulation factor XIII intravenously in different dosage regimens. The mean duration of treatment was 19 -+ 18 months, and patients were followed up for 22.9 _+ 18.8 months. Improvement or stabi- lization of the lesions was obtained in forty-four of eighty-six patients and exclusively concerned skin lesions; there was no improvement in visceral lesions. The drug was well tolerated in short- and long- term treatment. It is concluded that factor XIII demonstrated lasting effectiveness in one half of the patients treated.
Yehudi M. Felman, M.D.
Reactive perforating collagenosis
Battan VJ, Plausis-Giron G. Med Cutan Iber Lat Am 1986;14:120-4 (Spanish)
This first patient with reactive perforating collagenosis reported from Venezuela presented with a papular eruption over an erythem- atous base on the right forearm and the dersum of the right hand. After histopathologic confirmation of the diagnosis, the patient was successfully treated with topical retinoic acid, 0.05% nightly for 1 week.
Yehudi M. Felman, M.D.
Skeletal alterations from etretinate
Crespi HG, Massimo JA, Gentile F, Cordero AA. Med Cutan Iber Lat Am 1986;14:77-81 (Spanish)
A 4-year-eld boy with generalized pustular psoriasis failed to respond to prednisone and was then treated with etretinate, 1 mg/kg/ day for 6 months, to obtain a remission. Two years later he developed periostic separation in the inferior part of the femur, modeling alter- ation of the metaphysis, diffuse demineralization of bone, slenderi- zation of bone, and growth retardatlon. The authors advise that chil- dren receiving etretinate be examined radiologically periodically.
Yehudi M. Felman, M.D,