Embed Size (px)
Citation preview

Bullous pemphigoid and glomerulonephritisReport offour cases
Claude A. Simon, M.D., and R. K. Winkelmann, M.D., Ph.D. Rochester, MN
We report on four patients with bullous pemphigoid and other autoimmunediseases who had or developed glomerulonephritis. The relationship betweenthese two immunologic disorders involving the basement membrane isdiscussed. Our data suggest a coincidental phenomenon in patients whosuccessively or concurrently have multiple diseases of autoimmunity.(J AM ACAD DERMATOL 14:456-463, 1986.)
Multiple associations
Table I. Other autoimmune diseasesassociated with bullolls pemphigoid
Alopecia universalis, Hashimoto's thyroiditis, rheumatoid arthritis, autoimmune neutropenia20
Polymyositis, myasthenia gravis, Hashimoto'sthyroiditis21
Rheumatoid arthritis, pernicious anemia22Vitiligo, primary biliary cirrhosis23
copy revealed linear deposition of IgG, C3, and fibrin.Direct immunofluorescence microscopy of a perilesional area showed deposition of IgG, IgA, and C3along the basement membrane zone. The indirect immunofluorescence titer was 1: 160 for bullous pemphigoid antibodies. Bullous pemphigoid was diagnosed,and therapy with nicotinic acid, 100 mg three times a
NonclltaneollS
Factor V inhibitor~
Hashimoto's thyroiditis6
Multiple sclerosis7
Myasthenia gravisH
Pernicious anemia9
Polymyalgiarheumatica 10
Polymyositis II
Rheumatoid arthritis 12-15Systemic lupus
erythematosus l6-
1H
Ulcerative colitis 19
Single association
Cutaneous
Dermatitis herpetiformis I
Lichen planus2•3
Pemphigus4
Whereas bullous pemphigoid has been observedin association with several cutaneous and systemic autoimmune diseases during the last 20years (Table I), its association with glomerulonephritis has been reported in only a few isolatedcases, 19.24-26 and the relationship between these twodiseases in which basement membrane antibodieshave a major role27.28 has been the source of challenging discussions.
We have observed the association of bullouspemphigoid and glomerulonephritis in four additional cases that demonstrated various microscopicrenal changes, together with the bullous pemphigoid and several other immunologic disorders.
CASE REPORTSCase 1
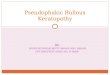
A 25-year-old woman had had idiopathic thrombocytopenic purpura in 1970. She was referred to theMayo Clinic in 1976 because of a burning and itchingskin rash with macular, papular-edematous, and vesicular-bullous lesions over her trunk and extremities thatwere unresponsive to prednisone (Fig. I). A skin biopsy specimen showed a subepidermal bulla with aperivascular infiltrate in the papillary dermis containingeosinophils, and direct immunofluorescence micros-
From the Department of Dermatology, Mayo Clinic and Mayo Foundation.
Accepted for publication Oct. 3.1. 1985.
Reprint requests to: Dr. R. K. Winkelmann, Mayo Clinic, 200 FirstSt. SW, Rochester, MN 55905.
456

Volume 14Number 3March, 1986
Bullous pemphigoid and glomerulonephritis 457
Fig. 1. A, Macular and vesicular bullous lesions on the trunk. B, Macular, papularedematous, and vesicular-bullous lesions on the extremities.
day, was begun while the dose of oral prednisone wasreduced gradually. The patient's skin condition improved dramatically. Because of the patient's sleepyappearance, thyroid tests were performed, revealing alow thyroxine level, a greatly elevated thyroid-stimulating hormone level, and a positive titer to thyroglobulin antibodies (l: 1,600). The patient was consideredto have Hashimoto's thyroiditis, and replacement therapy with 0.15 mg of levothyroxine sodium daily wasstarted. Farther into the course of therapy, several attempts at reducing the prednisone dose were accompanied by the recurrence of the skin lesions. The useof sulfapyridine, as much as 2 gm daily, did not help.
In March 1977 the patient developed a Coombs' testpositive hemolytic anemia and was treated with increased daily intake of prednisone for 6 months. InDecember 1977 the patient complained of headache,nausea, and dark urine. The erythrocyte sedimentationrate was 136 mm in 1hour, and results of the antinuclearantibody test and the lupus erythematosus clot test werenegative. The values for C3, C4, and native DNA werenormal. Results of the Raji test for circulating immunecomplexes were negative. Urinalysis revealed proteinuria and leukocyturia, but a urine culture was negative.
A kidney biopsy specimen showed a membranousglomerulonephropathy. Direct immunofluorescence microscopy revealed granular deposits of IgG, IgM, andcomplement (Clg, C3, and C4). Findings on electronmicroscopy also were consistent with a membranousglomerulonephropathy because of chronic immunecomplex production. The dose of prednisone was increased to 40 mg daily, and a long-term tapering program was begun.
In February 1978, although the patient's skin did notshow any abnormality except cushingoid changes resulting from prolonged prednisone therapy, protein,erythrocytes, leukocytes, and occasional hyaline andgranular cysts were still present in her urine. In N0
vember 1978 the patient was hospitalized because of arapidly spreading varicella, complicated by severepneumonitis with respiratory failure and deep-veinthrombosis in the left lower extremity. In June 1981the cessation of prednisone therapy was followed bythe development of uveitis in the left eye. This requiredprednisone treatment (40 mg daily) again. Despite oralsteroid therapy, a bulla appeared on the left knee, rapidly followed by a severe clinical flare of bullous pemphigoid. Biopsy was not performed. Indirect immu-

458 Simon and Winkelmann
nofluorescence was negative. Urinalysis showed protein, erythrocytes, leukocytes, and waxy and granularcasts-findings suggestive of an increase in nephritisactivity. The serum creatinine level was normal. A second renal biopsy revealed morphologic and immunologic changes that were no different from those on thefirst biopsy in 1977. Hospital treatment consisted of 40mg of prednisone daily, and her skin and kidney condition improved. In September 1982 an acquired factorVIII inhibitor was discovered-the latest manifestationof this patient's complex series ofautoimmune diseases.
Case 2
A 29-year-old man was hospitalized in April 1976because of a 3-month history of a generalized itchyrash. He had had bullous impetigo, condylomata acuminata, herpetic stomatitis, localized neurodermatitis,and alopecia areata involving the eyebrows and genitalregion. Physical examination revealed diffuse maculopapular, urticarial, and vesicular lesions on the trunkand extremities. The oral mucosa was eroded in severalareas. A skin biopsy specimen showed a subepidermalbulla with scattered eosinophils, and direct immunofluorescence microscopy showed a linear deposition of C3along the basement membrane zone. Results of indirectimmunofluorescence testing were positive (1: 640) forantibodies to the basement membrane zone. Laboratorytests were relevant for a marked blood eosinophilia(20,000 leukocytes/mm:1 with 15% eosinophils), andabnormal results on urinalysis (1.5 gm of protein excreted per 24 hours, erythrocytes, and occasional hyaline and granular casts). A urine culture was negative.Intravenous urography did not show any abnormalityexcept duplication of the collecting system in the rightkidney. Iothalamate clearance was normal. The levelsof C3 and C4 were normal. Results of the antinuclearantibody test were negative. Local therapy and 2 gmof sulfapyridine a day improved the patient's skin condition. The renal disease also improved, the amount ofurine protein decreasing to 0.86 gm/24 hr. A monthlater the patient had a flare of bullous pemphigoid onthe extremities. Direct immunofluorescence microscopy showed linear deposition ofC3 along the basementmembrane zone. Sulfapyridine was replaced by 50 mgof dapsone daily, and the skin improved. In addition,the eyebrows began to regrow.
In December 1976 the urine protein was 3.6 gm124hr. A renal biopsy specimen demonstrated a chronicmembranous glomerulonephropathy, with diffuse fineand coarse granular deposits of IgG, IgA, and C3 alongwith segmental and diffuse granular deposits of Clq.Electron microscopy showed a generalized mild to mod-
Joumal of theAmerican Academy of
Dermatology
erate thickening of all capillary walls. Subepithelialelectron-dense deposits with numerous "spike" formations were found. During 1977 the patient's renalcondition and bullous pemphigoid improved on a regimen of dapsone, 50 to ISO mg daily. In January 1978a severe bullous pemphigoid flare was treated with prednisone. Biopsy and direct immunofluorescence microscopy again showed bullous pemphigoid. The patient'scondition improved with local therapy, dapsone' (l00mg), nicotinic acid (300 mg daily), and cyproheptadinehydrochloride.
Recurrent flares required the use of prednisone andazathioprine, which produced good control. Urinalysisshowed erythrocytes, and the total urine protein wasreduced to 0.66 gm124 hr. During 1980 and 1981, several attempts to stop the prednisone therapy failed, withflares of bullous pemphigoid. The patient required 30mg of prednisone a day for his bullous pemphigoid.The addition of methotrexate did not help. By 1982 thepatient responded to lower doses of prednisone, and hiscondition was in relative remission in January 1983 witha regimen of 10 mg of prednisone daily.
Case 3An 83-year-old man was seen in October 1979, com
plaining of a 4-month history of a widespread, pruritic,burning, and painful eruption. He had suffered frombilateral painful ankle swelling with morning stiffnessand redness for 26 years. Symptoms were partially relieved by acetylsalicylic acid. Physical examination revealed generalized erythematous maculopapuies withlarge, tense bullae. A skin biopsy specimen showed asubepidermal bulla, and a dermal perivascular inflammatory reaction containing eosinophils and direct immunofluorescence microscopy showed a linear deposition of C3 on the basement membrane. The indirectimmunofluorescence titer was I :2,560 for bullous pemphigoid antibodies. Results of an antinuclear antibodytest were negative, and thyroid test results were normal.Urinalysis showed microhematuria. The serum creatinine level was normal. Stool analysis revealed occultblood, and rectosigmoidoscopy showed a thickened,friable mucosa with abscesses in the crypts. A rectalbiopsy specimen demonstrated ulcerative colitis. Thepatient was treated with prednisone, 40 mg daily, andsulfapyridine, 500 mg four times a day, and his condition improved. In February 1980, new blisters formedon the upper portion of the right arm. The patient hadstopped taking the prednisone a month earlier. Halcinonide cream was given, and by March 1980 the blistershad disappeared.
In September 1982 the patient experienced a new

Volume 14Number 3March, 1986
blistering eruption on the upper extremities. The blistering became rapidly generalized, and the patient washospitalized and treated with oral prednisone (60 mgdaily). Laboratory findings revealed severe proteinuria(protein excretion, 7.4 gm124 hr) with hyaline, granular, leukocytic, and waxy casts in the urine. Iothalamate clearance was decreased to 28 ml/min. A urineculture, antinuclear antibody test results, and rheumatoid factor were all negative. Renal lithiasis was ruledout by radiologic study. The patient refused a renalbiopsy. The diagnosis of membranous or membranoproliferative glomerulonephritis was clinically assumed, and the patient was given a low protein diet forhis renal condition.
In June 1984 the prednisone therapy was stopped,and in December 1984 a new flare of erythematous,infiltrated, vesicular lesions developed on the trunk andback. A skin biopsy specimen demonstrated dennaledema and eosinophilia, and direct immunofluorescence microscopy showed linear deposition of IgO andC3 along the basement membrane. The indirect immunofluorescence basement-membrane-zone antibodytiter was I: 640. The antinuclear antibody titer was1:40, and the complement level was normal. Mild proteinuria, leukocyturia, and hematuria were present,along with occasional hyaline and granular casts. Thepatient was treated with prednisone, 40 mg daily. Whenseen in January 1985, he was taking 40 mg of prednisone daily and denied having any new skin lesionduring this treatment.
Case 4
A 63-year-old man had suffered from microscopichematuria and hypertension since 1970. In December1972 a renal biopsy specimen demonstrated mesangialthickening, increased cellularity of the glomeruli, andperiglomerular fibrosis with complete hyalinization ofmost glomeruli. The tubules contained scattered eosinophilic casts with some flattening of epithelial cells andminimal atrophy. Minimal patchy interstitial chronicinflammation and fibrosis were also present, along witha slight thickening of the walls of the arterioles-findings consistent with chronic glomerulonephritis. Renalinsufficiency rapidly developed, and hemodialysis wasstarted a few months later.
In January 1973, transient intravascular hemolysiswith positive Donath-Landsteiner test results developed-findings suggestive of paroxysmal cold hemoglobinuria. In February and July 1977, transplantationof a cadaver donor kidney was carried out; both transplants were rejected. The patient was redialyzed andthen put on long-term ambulatory peritoneal dialysis
Bullous pemphigoid and glomerulonephritis 459
from 1979 onward. At the end of 1981 a severely pruritic, generalized rash with blisters developed on theextremities. A skin biopsy specimen showed a subepidennal bulla containing eosinophils and a papillary dermal perivascular infiltrate of eosinophils, with positivedirect immunofluorescence microscopy (linear C3 deposition along the basement membrane). The indirectimmunofluorescence titer was 1: 80 for bullous pemphigoid antibodies. Oral prednisone therapy was started(30 mg daily), and the bullous pemphigoid was fairlywell controlled by this treatment. In November 1984the patient was still taking 10 mg of prednisone a dayand had not had a recurrence of the bullous pemphigoidduring this period.
DISCUSSION
In 1953, Lever7 established bullous pemphigoidas an individual entity. A decade later, Jordonet aF9 demonstrated its autoimmune nature by discovering antibodies bound along the skin basementmembrane and circulating antibodies in patientswith bullous pemphigoid. The antigen responsiblefor this blistering disease was later purified by Diazet apo and called bullous pemphigoid antigen.
Our four patients had their clinical diagnosis ofbullous pemphigoid confirmed by a typical histologic picture-the presence of linear depositionof IgO or C3 (or both) along the basement membrane zone (positive direct immunofluorescence)and the presence of circulating bullous pemphigoid antibodies (positive indirect immunofluorescence).
In two patients, glomerulonephritis developedshortly after the onset of the bullous disease, 3years later in one patient and 11 years before inthe other (Table II). Prior to the first renal symptoms, neither had been receiving nephrotoxicagents or drugs reported to induce glomerulonephritis. 31 Urine cultures were negative, and radiologic study did not show any significant urinarytract abnormality. Systemic lupus erythematosus,known as one of the major causes of glomerulonephritis, was excluded by the absence of fulfillment of the American Rheumatism Associationcriteria, by the absence of circulating antinuclearantibodies, and by negative results of a lupus-bandtest on direct immunofluorescence.
In our cases the chronologie relationship between glomerulonephritis and bullous pemphigoid

460 Simon and Winkelmann
Table II. Data on four patients with bullous pemphigoid and glomerulonephritis
Journal of theAmerican Academy of
Dermatology
Bullous pemphigoid Glomerulonephritis
Year, Year,Case Sex, age (yr) Duration age (yr) DurationNo. age (yr) at onset (yr) at onset (yr) Associated immunologic disorders
F,25 1976,25 6 1977,26 5 Idiopathic thrombocytopenic purpura; Coombs'test-positive hemolytic anemia; Hashimoto'sthyrOiditis; uveitis; acquired factor VIIIinhibitor
2 M,29 1976,29 7 1976, 29 4 Alopecia areata3 M,83 1979, 83 6 1982, 86 6 Rheumatoid arthritis; ulcerative colitis4 M,63 1981,63 1 1970, 52 2 Paroxysmal cold hemoglobinuria; two consecu-
tive renal transplant rejections
and the kidney biopsy findings varied considerablyfrom one patient to another. In Case 1 the firstclinical and microscopic renal changes were notedwhen the blistering disease was under fair control,and although the kidney biopsy findings were consistent with chronic deposition of circulating immune complexes on the glomerular basementmembrane, we failed to detect these complexes inthe serum. It is of interest that the increase innephritis activity in 1981 was concomitant not onlywith a flare of bullous pemphigoid but also withthe development of uveitis. In Case 2, proteinuriaincreased while the skin was healing, and althoughnumerous spikes were found on the glomerularbasement membrane, consistent with immunecomplex deposition, a fine, diffuse deposition of19G, IgA, and C3 was also noted. The strikingfeature in Case 3 was the development of proteinuria and renal insufficiency during the severe flareof bullous pemphigoid in 1982, 3 years after itsbeginning. The patient was 86 years old and refused to have a renal biopsy specimen taken. Glomerulonephritis in Case 4 preceded the bullousdisease by 11 years, and the renal biopsy disclosednot only glomerular mesangial thickening and increased cellularity but also flattening of the tubularepithelial cells with atrophy and patchy interstitialchronic inflammation and fibrosis.
Kida et aP5 described a 39-year-old woman inwhom edema and proteinuria abruptly developed6 months after the onset of bullous pemphigoid.A renal biopsy specimen, taken 5 months later,showed deposition of IgG and C3 along the glo-
merular basement membrane, together with aslight thickening of the basement membrane anddense deposits on electron microscopy. The lightmicroscopic findings were normal. During thecourse of the bullous disease, proteinuria fluctuated in proportion to the level of circulating bullous pemphigoid antibodies. Despite these findings, the authors failed to obtain direct evidencefor an immune complex-mediated glomerulonephritis because deposition in vitro of fluoresceinisothiocyanate-stained serum gamma globulinsand kidney immunoglobulins onto normal skin,normal kidney tissue, and kidney tissue from thepatient was negative. In addition, there was noanticomplementary activity in the serum of thispatient, and results of the Clq binding test werenegative.
More recently, Merot et aF6 described two elderly patients (one described earlier by Glassonet aP2) in whom hematuria, proteinuria, and amoderate renal insufficiency developed shortly after the onset of bullous pemphigoid. Renal biopsy revealed diffuse proliferative and exudativechanges with humplike deposits along the glomerular basement membrane and granular depositsof C3. Systemic steroids were given, leading to arapid resolution of the skin and kidney problems.All these findings suggested to the authors evidence for deposition of bullous pemphigoid immune complexes on the glomerular basementmembrane.
Deposition of circulating immune complexesalong the glomerular basement membrane is a pos-

Volume 14Number 3March, 1986
sible mechanism responsible for glomerulone_phritis in patients with bullous pemphigoid, because the presence of circulating immune complexes has been recognized in several studies. 33·35Jordon et aP6 developed a method with which theyfound these complexes in as many as 68% of theirserum samples and discovered that they were largeenough (l9S or greater) to deposit in the kidneys.
In some respects, our data suggest the deposition of immune complexes on the glomerular basement membrane (proteinuria after a severe bullousflare in Case 3, granular deposits and/or spikes inCases 1 and 2), whereas in other respects, they donot (absence of detectable circulating immunecomplexes in Case 1; fine deposition of IgG, IgA,and C3 in Case 2; chronology and tubulointerstitialinvolvement in Case 4).
The case reported by Esterly et aJ24 is of specialinterest because the renal symptoms preceded (by9 months) bullous pemphigoid, as in our fourthpatient. Moreover, in spite of this time discrepancy, occasional spikes were found on the glomerular basement membrane, along with a slightdiffuse thickening of the capillary walls and deposition of IgG, and beta1c globulins were foundin discontinuous and continuous linear pattern, asin our second patient. The patient died shortlyafterward, and at autopsy a thrombus was notedto be occluding the right renal vein. The authorsbelieved that the thrombus was an epiphenomenonand could not have been the cause of the renalimpairment. Recently, Kaplan et aP7 reviewed thissubject and concluded that renal vein thrombosiswas the result, rather than the cause, of the nephrotic syndrome. The data on our four patients,in addition to those obtained by Esterly et al,24raise the question of another mechanism that leadsto glomerulonephritis in patients with bullous pemphigoid.
An antigenic cross-reactivity between the basement membrane of the skin and the glomeruli ishighly unlikely because the bullous pemphigoidantigen is known to be synthesized in the epidermal basal cells. 38 Further, although the antigen ispresent in the skin basement membrane of almostall vertebrates,39 it has not been found in the basement membrane of other tissues.40
The association of bullous pemphigoid and glo-
Bullous pemphigoid and glomerulonephritis 461
merulonephritis could occur through coincidence;however, the presence of three or more immunologic disorders in our patients is a clinical andimmunologic fact currently designated as "multiple autoimmune disease." Our first patient illustrates a unique state of "self-intolerance" througha never previously reported sequence of autoimmune diseases: idiopathic thrombocytopenic purpura, Coombs' test-positive hemolytic anemia,Hashimoto's thyroiditis, uveitis, acquired factorVIII inhibitor, bullous pemphigoid, and glomerulonephritis. The second patient had alopeciaareata, as well as bullous pemphigoid and glomerulonephritis. Patient 3 suffered from rheumatoid arthritis and ulcerative colitis when he wasseen for bullous pemphigoid and, later, for glomerulonephritis. Patient 4 not only presented withparoxysmal cold hemoglobinuria, bullous pemphigoid, and glomerulonephritis but also experienced two consecutive renal transplant rejections.This immunologic host response to the "nonself"is not entirely foreign to the rejection of the' 'self"because both conditions are known to require similar immunologic pathways.4t Bullous pemphigoidhas been recently reported in a 12-year-old girlduring chronic rejection of her second kidneytransplant. It is of interest that graft nephrectomywas rapidly followed by the disappearance of theskin lesions. 42
Many observations support the concept that autoimmune diseases are closely related host responses whether or not they involve different tissues. 43 Although the link they share is still poorlyunderstood,44 these autoimmune diseases are believed to occur under the influence of the sameetiologic agent-that is, genetic,45 viral,46 ortoxic. 47
Glomerulonephritis is an inflammatory renaldisease in which the glomerular basement membrane is immunologically injured, mainly throughthree major mechanisms: antibodies directed against the glomerular basement membrane, deposition of circulating immune complexes, andformation of immune complexes in situ.48 However, these immunologic mechanisms are not mutually exclusive and can occur simultaneouslyin vivo, being artificially separated for didacticreasons. 31 This may explain why bullous pemphi-

462 Simon and Winkelmann
gold and glomerulonephritis were not always concurrent in our cases and why the renal changeswere not uniform. Some conditions, such as lupuserythematosus, thymoma,4'1 and penicillamine-induced reactions;t1 can lead to expression of multiple autoimmune reactions. We believe that ourpatients-as well as the young patient describedin 1970 by Bean et al,19 who had ulcerative colitisfollowed by acute hemolysis of unclear origin andproteinuria with minimal mesangial changes on thekidney biopsy-fulfill such a description and thatthe occurrence of bullous pemphigoid and glomerulonephritis, although partially causal, is a coincidental phenomenon in patients who successively or concurrently demonstrate multiple diseases of autoimmunity.
REFERENCES
1. Honeyman JF, Honeyman A, Lobitz WC Jr, Storrs FJ:The enigma of bullous pemphigoid and dermatitis herpetifonnis. Arch Dennatol 106:22-25. 1972.
2. Stingl G. Holubar K: Coexistence of lichen planus andbullous pemphigoid: An immunopathological study. BrJ Dennatol 93:313-320, 1lJ75.
3. Saurat J-H. Guinepain M-T, Didierjean L. et al: Coexistence d'un lichen plan et d'une pemphigoide bulleuse: Etude en immunofluorescence d'un lichen pemphigoidc. Ann Dermatol Venereol 104:368-374. 1971.
4. Chorzefski TP, Maciejowski E. lablonska S, et al: Coexistence of pemphigus and bullous pemphigoid. ArchDennatol 109:849-853, 1974.
5. Bryning K. Leslie J: Factor Y inhibitor and bullous pemphigoid. Br Med J 2:677-678. 1977.
6. Callen JP, McCall MW: Bullous pemphigoid and Hashimoto's thyroiditis. J AM ACAP DERMATOL 5:558-560.1981.
7. Simjee S. Konqui A. Ahmed AR: Multiple sclerosis andlJulious pemphigoid. Dennatologica 170:86-89. 1985.
8. James WD: Bullous pemphigoid. myasthenia gravis. andthymoma. Arch Dennatol 120:397. 1984.
9. Obasi DE. Savin JA: Pemphigoid and pernicious anaemill. HI Med J 2:1458-1459. 1977.
10. How J. Sewsher PD. Stankler L: Bullous pemphigoid,polymyalgia rheumatica and thyroid disease. Br J Dermatoll03:201-204. 1980.
II. Peck SM. Lefkovits AM: Bullous pemphigoid with polymyooitis and co-existing contact dennatitis. Arch Dermatol94:672. 1966.
12. Lillicrap DA: Rheumatoid arthritis and pemphigoid. ProcR S<x: Med 56:921-922, 1963.
13. Salo OP. Rlisanen JA: Pemphigoid and rheumatoid arthritis: A clinical and immunological study. Ann Clin Res4:173-177. 1972.
14. Spigel GT. Winkelmann RK: Cicatricial pemphigoid andrheumatoid arthritis. Arch DennatoI1l4:415-417. 1978.
15. Giannini JM. Callen JP. GruberGG: Bullous pemphigoid
Journal of theAmerican Academy of
Dermatology
and rheumatoid arthritis. J AM ACAD DERMATOL 4:695697, 1981.
16. Jordon RE, Muller SA, Hale WL, Beutner EH: Bullouspemphigoid associated with systemic lupus erythematosus. Arch Dennatol 99: 17-25, 1969.
17. Kumar V, Binder WL, Schotland E, et al: Coexistenceof bullous pemphigoid and systemic lupus erythematosus. Arch DermatoI1I4:1187-1190, 1978.
18. Stoll DM, King LE Jr: Association of bullous pemphigoidwith systemic lupus erythematosus. Arch Dennatol120:362-366, 1984.
19. Bean SF, Good RA, Windhorst DB: Bullous pemphigoidin an II-year-old boy. Arch Dermatol 102:205-208,1970.
20. Lynfield YL, Green K, Gopal R: Bullous pemphigoidand multiple autoimmune diseases: Alopecia universalis,bullous pemphigoid. hypothyroidism, rheumatoid arthritis, and neutropenia in one patient. J AM ACAD DERMATOL 9:257-261. 1983.
21. Behan WMH, Behan PO. Doyle D: Association of myasthenia gravis and polymyositis with neoplasia, infection and autoimmune disorders. Acta Neuropathol (Ber!)57:221-229, 1982.
22. Callen JP. Anderson TF, Chanda 11, Taylor WB: Bullouspemphigoid and other disorders associated with autoimmune phenomena. Arch Dermatol 1I4:245-246, 1978.
23. Hamilton DV, McKenzie AW: Bullous pemphigoid andprimary biliary cirrhosis. Br J Dermatol 99:447-450,1978.
24. Esterly NB, Gotoff SP, Lolekha S, et al: Bullous pemphigoid and membranous glomerulonephropathy in achild. J Pediatr 83:466-470, 1973.
25. Kida K. Takaya Y, Makino H. et a1: Membranous glomerulonephritis associated with bullous pemphigoid.Nippon Jinzo Gakkai Shi 23:799-805, 1981.
26. Merot Y, Poffet D, Glasson P, Chatelanat F. SauratJ-H: Glomerulonephrite et pemphigoYde bulleuse: Deuxobservations. Ann Derm VenereolllO:739-740. 1983.
27. Lever WF: Pemphigus. Medicine (Baltimore) 32:1-123,1953.
28. Andres GA, Bren~ens JR: Autoimmune diseases of thekidney. Proc Soc Exp BioI Med 176:226-237, 1984.
29. Jordon RE, Beutner EH. Witebsky E. et al: Basementzone antibodies in bullous pemphigoid. lAMA 200:751756, 1967.
30. Diaz LA. Calvanico NJ, Tomasi TB Jr, Jordon RE: Bullous pemphigoid antigen: Isolation from normal humanskin. J Immunol 118:455-460, 1977.
31. Brenner BM, Rector FC Jr. editors: The kidney, ed. 2.vol. I. Philadelphia, 1981, W. B. Saunders Co.
32. Glasson P. Pfister G. Poffet D. et al: Glomerular lesionsin a patient with bullous pemphigoid (BP). Kidney Int21:123.1982. (Abst.)
33. Tappeiner G, Heine KG, Kahl IC, Jordon RE: Clq binding substances in pemphigus and bullous pemphigoid.Clin Exp Immunol 28:40-48, 1977.
34. Gomes MA, Dambuyant C, Thivolet]. Bussy R: Bullouspemphigoid: A correlative study of autoantibodies, circulating immune complexes and derrno-epidennal deposits. Br J Dermatol 107:43-51, 1982.
35. Haustein U-F, Lohrisch I, Herrmann K: Pathogeneticstudies in bullous pemphigoid: Review of the literature

Volume 14Number 3March, 1986
and our own results. J Dermatol (Tokyo) 11:508-518,1984.
36. Jordon RE, Struve MF, Bushkell LL: Serum and blisterfluid immune complexes in bullous pemphigoid: Detection with Clq and monoclonal rheumatoid factor. ClioExp Immunol 45:29-36, 1981.
37. Kaplan BS, Chesney RW, Drummond KN: The nephroticsyndrome and renal vein thrombosis. Am J Dis Child132:367-370, 1978.
38. Woodley D, Didierjean L, Regnier M, et al: Bullouspemphigoid antigen synthesized in vitro by human epidermal cells. J Invest Dermatol 75:148-151, 1980.
39. Diaz LA, Weiss HJ, Calvanico NJ: Phylogenetic studieswith pemphigus and pemphigoid antibodies. Acta DermVenereol (Stockh) 58:537-540, 1978.
40. Seutner EH, Chorzelski TP, Jordon RE: Autosensitization in pemphigus and bullous pemphigoid. Springfield,IL, 1970, Charles C Thomas, Publisher.
41. Stites DP, Stobo 10, Fudenberg HH, Wells JV, editors:Basic and clinical immunology, ed. 4. Los Altos. CA,1982, Lange Medical Publications.
42. Feehally J, Reilly DT, Walls J, Wood RPM: An antibody-
Bullous pemphigoid and glomerulonephritis 463
mediated bullous skin eruption caused by chronic renalallograft rejection. Transplantation 34:295-296, 1982.
43. Sell S: Immunopathology. Am J PathoI 90:215-279,1978.
44. Cohen IR: Autoimmunity: Physiologic and pernicious.Adv Intern Med 29:147-165, 1984.
45. Adams DD: The genetic predisposition to autoimmunedisease. NZ Med J 97:638-640, 1984.
46. Christian CL, MelJors RC, Lightfoot RW Jr, Block SR:Aspects of systemic lupus erythematosus: Considerationof viral and genetic factors, and remarks on therapy. AmJ Med Sci 270:515-522, 1975.
47. Bucknall RC, Dixon ASJ, Glick EN, et al: Myastheniagravis associated with penicillamine treatment for rheumatoid arthritis. Br Med J 1:600-602, 1975.
48. Samter M, editor: Immunological diseases, ed. 2, vol.2. Boston, 1978, Little, Brown & Co.
49. Souadjian JV, Enriqucz P, Silverstein MN, Pepin J-M:The spectrum of diseases associated with thymoma: Coincidence or syndrome? Arch Intern Med 134:374-379,1974.
ABSTRACTS
Toxoplasma antibodies in morbus Beh~et (Germantext)
Breustedt W, Audring H, Brenke A, Jacobza D:Dermatol Monatsschr 171:324-328, 1985
Changing titers of Toxoplasma-specificantibodies, frompositive at the onset of the disease to negative 12 weeks later,point to the possibility of a causal connection between toxoplasmosis and Behs;et's disease. Treatment with colchicine,fifteen to twenty drops three to four times daily, seems to besuccessful, particularly for the acute disease stage.
Alfred Hal/ander, M.D.
Lupus vulgaris; clinical findings and therapy,past and present (German text)
Simon N: Z Hautkr 60:1295-1306, 1985
The number of lupus vulgaris patients has greatly decreased in both West and East Germany during the last decade.Regardless of the type of sldn tuberculosis, all patients undergo monotherapy with isonicotinic acid hydrazide (INH),5-7 mg/kg daily. After clinical cure therapy is continued forone-half year. Clinical resistance was found in only one of100 patients. In clinically resistant patients a combined treatment of INH, rifampin, and ethambutol is recommended.
Alfred Hollander, M.D.
Antenatal therapy with corticosteroids andpostpartum complications
Curet LB, Morrison lC, Rao AV: Am J ObstetGynecol 152:83-84, 1985
In another comparative study, using placebo and steroid,careful evaluations show that moderate doses of corticosteroidcan be used safely in pregnancy, in this situation for manyweeks, to control fetal distress.
P. C. Anderson, M.D.
Cutaneous blisters and carbon monoxidepoisoning
Myers RA, Snyder SK, Majerus TC: Ann EmergMed 14:603-606, 1985
A reminder to emergency room staffers that skin findingscan be crucial in making a correct diagnosis and doing sorapidly enough to give therapy to the patient while he needsit.
P. C. Anderson, M.D.