Embed Size (px)
Citation preview

G a s t r i t e a s s o c i 6 e au Campylobacter pylori : Essai t h 6 r a p e u t i q u e en d o u b l e - i n s u a m o x y c i l l i n e v e r s u s p l a c e b o
A . B U R E T T E * , Y . G L U P C Z Y N S K I * * , M . L A B B E * * , C . D E P R E Z * * * , M . D E R E U C K * , M . D E L T E N R E *
* Dep t . o f G a s t r o e n t e r o l o g y ** D e p t . o f Cl in ica l M i c r o b i o l o g y
*** Dept . o f P a t h o l o g y B r u g m a n n Univers i t y Hosp i ta l , 1020 B r u s s e l s ( B e l g i u m )
Campylobacter pylori-associated gastritis: A double-blind placebo controlled trial with amoxycillin
RI~SUMI~
Une ~tude contr616e en double aveugle (amoxycilline vs placebo) a ~t6 r6alis6e chez des adultes porteurs d'une gastrite antrale associ~e ~ une infection ~ C. pylori. Dans la premiere partie de eette ~tude, les patients ont ~t~ trait~s par sirop d'amoxycilline (2 • 1 gr) ou de placebo en deux prises quotidiennes pendant une semaine. Vingt deux patients ont re~u de I'amoxycilline et vingt trois du placebo. Apr~s traitement, l 'infection ~ C. pylori avait disparu chez 9 1 % (20/22) des patients trait~s par amoxycilline eontre 16 % (4/23) chez les patients trait6s par placebo (p < 0.001).
La gastrite active de l 'antre a disparu chez 15/22 (68 %) patients dans le groupe amoxycilline mais chez seulement 2/23 (16 %) patients dans le groupe placebo (p < 0.001). Aucune amelioration significative n 'a 6t~ observ6e en ce qui concerne la symptomatolo- gie et l'aspect endoscopique.
Dans la deuxi~me partie de cette ~tude (simple aveagle), 19 patients devenus C. pylori n~gatifs apr~s une semaine de traitement ont ensuite re~u du sirop placebo pendant 2 semaines : une r~apparition de l'infection ~ C. pylori associ~e ~ une aggravation tr~s significative de score histologique de la gastrite a 6t6 observ~e chez tous ies patients.
A rinverse, 18 patients rest6s positifs apr~s une semaine ont ensuite ~t~ trait~s en simple aveugle par sirop d'amoxycilline pendant 14 jours : la disparition du C. pylori, objectiv~e ~ la fin de cette p6riode chez 13 d'entre-eux (72 %), 6tait eorr~l~e ~ une nette am61ioration du score histologique de la gastrite. Parmi ces 13 patients, 8 ont ~t~ recontr616s apr~s un mois et tous pr&entaient
nouveau une infection ~ C. pylori et une aggravation significative des 16sions de gastrite ~ l'histologie.
Ces r6sultats montrent que le sirop d'amoxycilline fi la dose de 2g/jour est efficace dans le traitement de la gastrite active associ6e fi l 'infection ~ C. pylori mais ne permet pas de pr6venir les rechutes qui surviennent chez tous les patients dans le mois qui suit l 'arr~t du traitement.
S U M M A R Y
A double-blind, placebo-controlled treatment study was performed in adults with antral gastritis associated with C. pylori. Patients received 20 ml o f a placebo or an amoxycillin suspension (lg) two times daily for 8 days. Twenty-two patients received amoxycillin and twenty-three received a placebo. At the end of therapy 9 1 % (20/22) of patients treated with amoxycillin demonstrated clearance of the organism from the antrum compared to 16 % (4/23) in the placebo group (p < 0.001), Active antral gastritis resolved in 68 % (15/22) of patients in the amoxycillin group versus only 9 % (2/23) in the placebo group (p < 0.001). No significant improvement was observed in the assessment o f clinical symptoms and endoscopic appearance. Reappearance of C. pylori and significant aggravation of the histological score was observed after 2 weeks in 100 % (19/19) of patients who demonstrated bacterial clearance after 8 days and had then received placebo for 14 days. Conversely, eighteen patients (not cleared from their bacteria after 8 days) received amoxycillin in single blind for 14 days. CLearance of bacteria associated with improvement or resolution of active gastritis was observed in 72 % (13/ 18) o f patients. In this subgroup, 100 % (8/8) of patients observed at follow-up 1 month after stopping therapy were recolonized with C. pylori and again had histological active gastritis.
These results indicate that amoxycillin suspension 2 g daily for 1 or 2 weeks is effective in treating active antral gastritis associated with C. pylori, but not in preventing relapses, which occur in all patients within one month after therapy.
Tir6s ~ pa r t : Dr. A. BURETTE, Dept. Gastroenterology, Brugmann University Hospital, Pl. A. Van Gehuchten 4, B- 1020 Brussels (Belgium)
Mots-cl~s : amoxyciiline, Campylobacter pylori, gastrite, traite- ment.
Key-words : amoxycillin, Campylobacter pylori, gastritis, treat- ment.
Acta Endoscopica Volume 17 N ~ 5 - 1987 25 !

INTROD UCTION
Plusieurs 6tudes r6centes ont montr6 une corr6- lation 6troite entre la pr6sence de germes de type Campylobacter, actuellement d6sign6s officielle- ment Campylobacter pylori, et la pr6sence de 16sions histologiques de gastrite ou d'ulc6res pepti- ques [2, 3, 10, 22, 24, 32]. Le lien 6tiologique entre ces micro-organismes et les 16sions inflamma- toires de la muqueuse gastrique n'est pas encore 6tabli, mais deux 6tudes s6par6es sur volontaires satisfont les crit6res de Koch et appuient cette hypoth6se pathog6nique [23, 29]. Par ailleurs, le r61e du C. pylori dans la pathog6nie de la maladie uic6reuse reste h 61ucider [2, 14]. La pr6valence du C. pylori dans la population des patients exa- min6s dans notre unit6 endoscopique est de 54 % dans la dyspepsie non ulc6reuse (n = 308), 64 % des ulc6res gastriques tout-venants (n = 61) et 80 % de l'ensemble des ulc6res duod6naux (n = 123).
Des 6tudes in vitro montrent que ce germe est sensible ~ de nombreux agents antibact6riens (p6nicillines, c6phalosporines, 6rythromycine, t6- tracyclines, nitrofuranes et d6riv6s nitro-imidazole) ainsi qu'aux sels de bismuth [1, 8, 11, 15, 18, 25].
Jusqu'~ pr6sent, peu d'6tudes contr616es ont 6valu6 le b6n6fice 6ventuel d'une antibioth6rapie dans une infection ~ C. pylori [6, 12, 19, 26].
Dans le but de d6terminer si ces micro-orga- nismes ont un r61e 6tiologique dans la gastrite laquelle ils sont associ6s, nous avons entrepris une 6tude prospective, randomis6e, en double aveugle, en vue de d6terminer les effets compar6s de l'amoxycilline et du placebo, du point de vue 6radication du germe et effet th6rapeutique sur la gastrite.
MATER1EL ET METHODES
Le groupe de patients soumis h l'6tude est cons- titu6 de sujets soumis ~ une endoscopie pour sympt6mes du tractus digestif sup6rieur, et chez iesquels les biopsies antrales ont r6v616 la pr6sence de Campylobacter pylori. Ont 6t6 exclus de l'6tude : les malades porteurs d'un ulc6re pepti- que, d'une 16sion maligne, d'cesophagite, ant6c6- dents de chirurgie pour ulc6re (except6 la vagoto- mie), ceux d6jh trait6s par agents antimicrobiens ou m6dicaments anti-ulc6reux (sauf les antacides), ou enfin les malades dont l'anamn6se r6v61e une allergie aux p6nicillines. Le projet d'6tude a 6t6 approuv6 par le Comit6 d'Ethique M6dicale de l'H6pital Universitaire Brugmann, et tous les patients 6tudi6s, inform6s de leur participation l'essai, ont donn6 leur consentement.
Schema th~rapeutique
I! a 6t6 appliqu6 en deux phases:
Phase I : les malades C. pylori positifs ont 6t6 r6partis en double-insu, de fagon randomis6e, recevant soit un sirop d'amoxycilline (deux lois 1 f par jour) ou de placebo en deux prises quoti- diennes pendant une semaine.
Phase II : les patients ont 6t6 trait6s en simple- aveugle pendant 14 jours, soit par l'amoxycilline (m6me dose qu'au cours de la phase I) ou par placebo selon qu'ils 6taient rest6s C. pylori positifs ou devenus C. pylori n6gatifs au cours de la phase I. L'antibiotique et le placebo ont 6t6 fournis gracieusement par Beecham Pharma Benelux dans des r6cipients d'aspect identique (80 ml) contenant un sirop de couleur blanche aromatis6 ~ la fraise.
Endoscopie
Une gastroscopie a 6t6 r6alis6e dans tous les cas en d6but d'essai, au 106me jour (apr6s traitement de la phase I), au 21~me jour apr6s la fin de la phase II (d'habitude darts un d61ai de 3 jours). Un examen de contr61e a 6t6 r6alis6 un mois apr6s la phase th6rapeutique chez la majorit6 des patients. Afin d'6viter une concentration r6siduelle d'anti- biotique susceptible d'inhiber la culture de C. pylori, les malades n'ont jamais 6t6 examin6s au cours des 24 premi6res heures apr~s la fin du traitement. Chez la plupart des patients, la gas- troscopie avant et apr6s traitement a 6t6 effectu6e par le m6me endoscopiste. Les donn6es macroscopiques suivantes ont 6t6 relev6es : hyper- h6mie, 6rosions, exulc6rations, atrophie ou hyper- trophie de la muqueuse. Un score endoscopique class6 en trois degr6s a 6t6 6tabli de la fa~on suivante : aspect normal = 0 ; hyperh6mie = 1 ; quelques exulc6rations gastriques (<~ 3) = 2 ; 6ro- sions gastriques diffuses = 3. Quatre biopsies ont pr61ev6es syst6matiquement au niveau de la muqueuse antrale. Deux biopsies ont 6t6 fix6es dans une solution de formol h 10 % pour examen histologique, et deux autres plong6es avec un 6couvillon st6rile, dans un milieu de transport agar semi-solide (Portagerm, Bio-M6rieux, France) en vue de l'examen bact6riologique.
Histologie
Des sections sur paraffine apr6s fixation au for- mol ont 6t6 color6es par l'h6matoxyline-6osine. La pr6sence d'une gastrite a 6t6 6valu6e par un ana- tomo-pathologiste consultant (C.D.) qui ignorait l'histoire clinique, les r6sultats de I'endoscopie et de la bact6riologie. La classification des degr6s de gastrite (absente, chronique ou active) a 6t6 rdali- s6e sur base des crit6res de Whitehead, Rotterdam et Sommer [30, 35].
Cette classification classe les 16sions en 6 degr6s en fonction du type de l'infiitrat cellulaire (cellules
252 V o l u m e 1 7 - N ~ 5 - 1 9 8 7 A c t a E n d o s c o p i c u

mononucl6aires et polynucl6aires) et 6galement en fonction de l ' intensit6 de l'infiltrat inflammatoire. La muqueuse normale correspond au degr6 0. Les degr6s 1 h 3 concernent l 'infiltration par les cel- lules mononucl6es (16g~re, mod6r6e, s6v~re) alors que les grades 4 h 6 concernent l'infiltrat polynu- cl6aire (16ger, mod6r6, s6v6re). La pr6sence ou l 'absence de C. pylori a 6t6 not6e (coloration h6matoxyline-6osine) mais sans 6valuation quanti- tative de la positivit6.
Bactdriologie
T o u s l e s 6chantillons ont 6t6 transport6s au laboratoire dans un intervaile de temps infgrieur deux heures apr~s pr61~vement. Une partie de la biopsie a 6t6 6tal6e sur lames de verre et pr6par6e pour une colorat ion de Gram. Les 6chantillons ont 6t6 incub6s dans un milieu s61ectif "agar chocolat" (modifi6 selon Thayer -Mar t in) contenant : vanco- mycine (4 mg/1 ) , colistine (7.5 mg/1) , amphoteri- cine B ( 2 m g / 1 ) et t r imethoprim ( 5 m g / 1 ) . Le reste de la biopsie a 6t6 enfin d6pos6 dans 0.5 ml d 'un bouillon fi 2 % d 'ur6e. Les plaques ont 6t6 incub6es ~ 37 ~ dans une atmosphere micro-a6ro- phile (6 % 02, 10 % CO2, Anaerocul t C ; Merck ; Darmstadt , R F A ) et examin6es apr~s 3, 5 et 7 jours. Les biopsies ont 6t6 consid6r6es positives pour le C. pylori si la pr6paration pour le Gram montrai t des bact6ries spiral6es, e t / ou la culture r6v61ait un aspect de pullulation caract6ristique (gris, translucide, convexe) . La positivit6 des culture a 6t6 grossi~rement 6valu6e en trois cat6- gories : abondante , mod6r6e et peu abondante en fonction du nombre de quadrants de plaques mon- trant la croissance de colonies.
Le diagnostic des cultures a 6t6 confirm6 par la coloration au gram, une activit6 ur6ase rapide et des r6actions enzymat iques oxydase et catalase po- sitives.
Une biopsie positive pour le test ~ l 'ur6ase en l 'absence d 'autres crit&res de positivit6 bact6riolo- gique, n'a pas 6t6 consid6r6e comme suffisante pour 6tablir la pr6sence du C. pylori. Dans tous les cas, les 6tudes bact6riologiques ont 6t6 r6ali- s6es dans l ' ignorance des donn6es cliniques, endoscopiques et histologiques.
Evaluation des symptomes
Avant t ra i tement , les patients ont 6t6 interrog6s au sujet de la pr6sence et de la s6v6rit6 de six sympt6mes bien d6finis : naus6es, vomissements, brfilures 6pigastriques, dyspepsie, douleurs ulc6- reuses ou 6pigastriques. Les sympt6mes ont 6t6 class6s en degr6s de 0 ~ 3 (absents, 16gets, mod6r6s ou s6v~res). Apr~s t rai tement , les malades ont 6t6 interrog6s h propos de l '6volution des symt6mes : inchang6s, aggrav6s ou am61ior6s.
Un score symptomat ique individuel a rendu pos- sible une 6valuation de degr6s de s6v6rit6 variant de 0 h 18.
Analyse statistique
Les r6sultats ont 6t6 analys6s selon le t e s t X 2 et le test de Wilcoxon. Le degr6 de signification a 6t6 atteint pour une valeur de p < 0.05.
R E S U L T A T S
Rdsultats cliniques
Quarante-hui t patients ont 6t6 inclus dans le groupe d '6tude entre Juin et Octobre 1986. Deux malades ont 6t6 propos6s comme candidats l '6tude, mais n 'ont pas commenc6 leur t ra i tement . Un patient a 6t6 exclu apr~s huit jours en raison d 'une d6couverte d 'un ulc~re duod6nal actif qui n'avait p robab lement pas 6t6 reconnu lors de la premiere endoscopie. Le groupe de 45 patients restants compor te 38 hommes et 7 femmes, dont les figes varient de 22 h 82 ans (moyenne d'fige : 54.1 ans). 32 malades ont 6t6 soumis ~ une endoscopie pour plaintes gastro-intestinales, 11 en raison d 'ant6c6dents d 'ulc~re gastroduod6nal, sou- mis pour contr61e de cicatrisation ou pris en sur- veillance de routine pour recherche de r6cidive ulc6reuse. Deux patients avec ant6c6dent d 'ulc~re r6cidivant avaient subi pr6c6demment une vagoto- mie s61ective. Lors de l ' examen endoscopique ini- tial, l 'hyperh6mie de l 'antre e t / o u du fundus a 6t6 observ6e dans 32 cas, des 6rosions antrales dans 5, l 'ulc~re duod6nal dans 3 ; aucun patient ne pr6- sentait une gastrite a t rophique antrale.
Aucune difference n'existe, parmi les groupes trait6s, en ce qui concerne le sexe, l'fige, l 'origine ethnique, le tabagisme, l 'alcoolisme, les ant6c6- dents d'ulc~re ou les t ra i tements anti-ulc6reux. Sur les 45 patients investigu6s, 22 ont re~u de l 'amoxy- cilline et 23 du placebo au cours de la phase I.
La compliance totale des patients inclus dans l '6tude est de 100 % ~ la premiere semaine (pha- s e I ) (45 patients sur 45) et de 8 2 % lots de la phase II (37/45 patients).
Bactdriologie
Sur les 45 6chantillons requs avant t ra i tement , 40 (89 %) 6taient positifs ~ la culture, et 34 ( 7 6 % ) apr6s colorat ion au Gram. Vingt-neuf cultures pr6sentaient une croissance bact6rienne mod6r6e ou forte, tous ces 6chantillons 6taient 6galement positifs ~ l ' examen direct avec colora- tion au Gram. Inversement , les germes de type Campylobacter apr6s colorat ion au Gram ont 6t6 observ6s seulement dans 5 sur 11 6chantillons dont la culture 6tait peu abondante . Le test h l 'ur6ase 6tait positif sur 40 6chantillons (89 %) (Tableau 1). Si l 'on tient compte du temps n6cessaire h ia positivit6 du test, 29 6chantillons (72 %) 6taient positifs apr6s deux heures. Vingt-quatre patients ont 6t6 d6barrass6s du C. pylori en fin de traite-
Acta Endoscopica Volume 17 N ~ 5 - 1987 253

ment : 20 malades sur les 22 trait6s par amoxycil- line (91%) et 4 sur les 23 trait6s par placebo (17 %) (Tableau 2).
TABLEAU I
C O M P A R A I S O N E N T R E LES D E U X G R O U P E S A V A N T T R A I T E M E N T A V E C RI~FI~RENCE
A U X MI~THODES D E DI~TECTION DU C. P Y L O R 1
M6thode de d6tection
Nombre Test Groupe trait6 de Colora- l'ur6ase
patients tion au Gram sur
biopsies
Amoxycilline (n = 22) 13 + +
4 - + 2 - - 2 + + 1 + -
1 4 + + 4 - + 1 - - - -
2 + + 1 + -
Placebo (n = 23)
Culture
+ + + _ (a)
+
+ + + _ (a)
+
(a) Cultures contamin6es par d 'autres esp6ces bact6riennes.
T A B L E A U I I
C O M P A R A I S O N E N T R E LES D E U X G R O U P E S APRILS 8 J O U R S DE T R A I T E M E N T (PHASE I) "
A V E C RI~FI~RENCE A U X MI~THODES DE Di~TECTION D U C. P Y L O R I
M6thode de d6tection
Nombre Test Groupe trait6 de Colora- l'ur6ase
patients tion au Gram sur
biopsies
Amoxycilline (n = 22)
Culture
Placebo (n = 23)
2 0 - - m
2 - + +
12 + + + 2 - + + 3 + + - (") ] + - +
1 - -t- - 4 _ (b) _ _
(a) Cultures contamin6es par d 'autres esp6ces bact6riennes. (b) Pr6sence du C. p y l o r i ~ l 'examen histologique chez un malade.
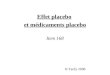
L'effet de l'amoxycilline sur l'61imination de la bact6rie 6tait significativement sup6rieur h celui du placebo (• 8 .9 ; p < 0.004) (Fig. 1). Au cours de la seconde phase, l'amoxycilline a permis l'61i- ruination du C. pylori de la muqueuse gastrique chez 13 patients sur 18 (72 %). Aucune diff6rence entre les taux d'61imination des bact6ries n'a 6t6 observ6e en comparant les groupes trait6s apr~s la
premiere et la deuxi6me semaine. Tous les patients n6gativ6s apr~s huit jours (19/19), et ensuite trait6s par placebo pendant 14 jours, 6taient ~t nouveau positifs lors du contr61e ~ 3 semaines.
Nombre de patients
25
20
15
10
5.
o I Amoxyciiline
(N=22)
[--1 Elimination du CP
[ ] Pas d'elimination du CP
Placebo
(N=23)
Figure 1
Elimination du C. pylori apres une semaine d'amoxyci l l ine (20/22) ou de placebo (4/23)
Rgsultats histologiques
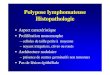
L'ensemble des malades pr6sentaient des signes histologiques de gastrite avant traitement. Treize (67 %) avaient une gastrite chronique active (infil- trat ~ polynucl6aires). Quinze (33 %) pr6sentaient une gastrite chronique non 6volutive (infiltrat lym- phocytaire ou lympho-plasmocytaire). Aucune dif- f6rence entre les scores histologiques avant traite- ment n'existait entre les groupes amoxycilline et placebo (score moyen : 3.6 vs 3.8). L'61imination du C. pylori apr6s 8 jours 6tait associ6e ~ une am61ioration significative du score de gastrite (score moyen : 2.1 vs 4 .2 ; p < 0.0002) (fig. 2).
Nombre de patients
20
15
10
0 m Normal
/ -U
Gastrite Gastrite chronique active
Figure 2
Elimination �9 du C. pylori [ ] Pas d'elimination
du C. pylori
Donnees histologiques apres une semaine de traitement en fonction d'elimination du micro-organisme.
De plus, le score histologique 6tait significative- ment am61ior6 apr6s traitement ~t l'amoxycilline (score moyen : 3.6 vs 2 .2 ; p < 0.05), mais non apr~s placebo (score moyen : 4.1 vs 2.8 ; p < 0.03). N6anmoins, la r6cidive de C. pylori
254 V o l u m e 17 - N ~ 5 - 1987 A c t a E n d o s c o p i c a

Score histologique
Avant traitement Apres traitement
6
5
4
3
2
1
Placebo
Score histologique
Avant traitement Apres traitement
6
5
Amoxycilline
Figure 3
Evolution du score histologique apr~s une semaine de traitement par amoxycilline ou placebo.
6tait associ6e h une aggravation histologique signl- ficative chez les 19 patients C. pylori n6gatifs trait6s par placebo pendant 2 semaines (score moyen : 2.1 vs 4.2 ; p < 0.001).
Endoscopie et 6valuation des symptomes
L'endoscopie a montr6 une am61ioration de l'aspect macroscopique respectivement dans 4 et 3 cas des groupes amoxycilline et placebo. En ce qui concerne les sympt6mes cliniques, aucune diff6- rence significative n'a 6t6 observ6e entre les deux groupes de patients.
DISCUSSION
La pr6sente 6tude en double-aveugle confirme l'6troite corr61ation entre la pr6sence du C. pylori au niveau de la muqueuse antrale et une gastrite active d6montr6e par l 'examen histologique [2, 10, 22, 31, 34, 36]. L'Elimination du C. pylori est associ6e ~ une r6gression de l'activit6 de la gastrite
et la r6cidive de l'infection ~ une r6apparition des 16sions histologiques. Nous n'avons observ6 aucune r6gression des signes de gastrite chez les patients dont l'infection a persist6.
Les concentrations minimales d'amoxycilline sus- ceptibles d'inhiber la croissance de C. pylori varient de 0.015 ~ 0.125 ug/ml [8, 11, 18, 25]. Ces concentrations sont tr~s inf6rieures ~ celles obte- nues (limites : 14.6 - 180 ; moyenne 117 Ixg/g) sur les biospies gastriques pr61ev6es apr6s administra- tion de capsules de 500 mg d'amoxycilline [28]. Nous avons pr6f6r6 l'administration de l'amoxycil- line en suspension plut6t qu'en capsules en postu- lant le b6n6fice d'un traitement mixte h la lois local et syst6mique. En r6alit6, le taux d'61imina- tion (91%) obtenu apr~s une semaine est sup6- rieur ~ ceux de la litt6rature, se r6f6rant h l'admi- nistration d'amoxycilline en monoth6rapie. Le sch6ma th6rapeutique nous permet 6galement de souligner la r6cidive pr6coce de l'infection par C. pylori (100 % deux semaines apr6s le traitement par amoxycilline).
Dans une 6tude ouverte non contr616e, Langen- berg et al [21] montrent Qae l'administration d'amoxycilline - - capsules 375 mg deux lois par jour pendant 4 semaines - - entraine l'61imination du germe en fin de traitement dans 70 % des cas. N6anmoins, ces auteurs ont observ6 6galement un taux de r6cidives de 60 % fa 4 semaines. L'associa- tion amoxycilline-subcitrate de bismuth fournit des r6sultats sup6rieurs (90 % d'61imination apr6s 4 semaines), mais est n6anmoins associ6e ~ un taux de r6cidives 61ev6 (47 % apr~s 4 semaines). Dans une 6tude en double-insu avec placebo, Goodwin et al [12] ont observ6 l'61imination de C. pylori chez 33 % des sujets trait6s par subcitrate de bismuth seul et rapportent un taux d'elimination de 75 % en combinant subcitrate de bismuth (8 semaines) et tinidazole (10 jours). Ces auteurs observent 6galement, par comparaison avec la cim6tidine, une r6duction significative du taux de r6cidives ulc6reuses apr~s traitement par bismuth- tinidazole. Dans une autre 6tude en double-insu comparant salicylate de bismuth, 6thylsuccinate d'6rythromycine et placebo, Mc Nulty et al [26] observent un taux d'61imination de 78 % apr~s trois semaines sous bismuth vs 7 % sous 6rythro- mycine et 0 % sous placebo.
D'autres auteurs ont 6galement rapport6 des r6sultats pr61iminaires favorables par monoth6rapie au bismuth (taux d'61imination variant de 50 75 %) [4, 5, 16, 17, 33].
Parmi les autres agents antimicrobiens, la fura- zolidone et nitrofurantoine ont 6t6 6valu6es et se sont av6r6es efficaces (taux d'61imination respecti- vement 93 et 79 % apr6s 2 semaines) [6]. II est int6ressant de noter que des auteurs chinois ont signal6 l'efficacit6 de la furazolidone dans le traite- ment de l'ulc/~re. Par contre, 1'6rythromycine [26], la spiramycine [33], la josamycine (19), la doxycy- dine [29] et l'ofloxacyne [7] et ciprofloxacine [13] se sont r6v616es inefficaces au cours des essais cliniques.
A c t a E n d o s c o p i c a V o l u m e 17 N ~ 5 - 1987 255

Ces r6sultats contrastent avec ceux des 6tudes in vitro, qui montrent qu 'une grande vari6t6 d 'agents anti-microbiens sont actifs et en th6rorie pour- raient servir h l '6valuation du r61e 6tiologique du C. pylori dans la gastrite et l 'ulc6re [1, 8, 11, 13, 15, 18, 24, 25]. D'autres facteurs, tels que Faction locale ou syst6mique de la drogue, la stabilit6 pH acide, les concentrat ions obtenues au niveau des cryptes de la muqueuse gastrique, la diffusion
travers le mucus, interf6rent p robab lement dans l'efficacit6 de ces diff6rents m6dicaments [9, 27]. Ces variables devraient 6tre 6valu6es avant le choix des m6dicaments en vue d'essais th6rapeuti- ques.
Derni~rement , une r6sistance du C. pylori aux antibiotiques a 6t6 rapport6e [7, 12]. Si ce ph6no- m~ne devait 6tre confirm6, il importerai t dans le futur d 'associer les antibiotiques. De toutes fa~ons, ces observations incitent h l '6valuation syst6mati- que de la r6sistance des souches r6sistantes. Dans la pr6sente 6tude, aucune r6sistance h l 'amoxycil- line n 'a 6t6 observ6e chez les patients qui ont r6cidiv6 apr6s trai tement.
CONCL USIONS
Les r6sultats de cette 6tude plaident en faveur du caract6re pathog6nique du C. pylori plut6t que de son r61e de micro-organisme commensai . Ils appuient l 'hypoth6se selon laquelle ce germe joue un r61e dans la pathog6nie de la gastrite. Son r61e exact dans la maladie ulc6reuse, l'influence favora- ble de son 61imination sur le cours naturel de la maladie, restent des questions en suspens.
Le probl6me fondamental pos6 par la r6appari- tion du C. pylori est le suivant : s'agit-il d'une r6- infection ou d'une recrudescence due h une 61imi- nation insuffisante ? Les r6sultats des analyses par restriction endonucl6ase D N A plaident, en cas de r6cidive apr~s traitement, en faveur d'une r6activa- tion plut6t que d'une r6infection [20]. Si cette hypoth6se est confirm6e, l'61imination complete et prolong6e du CP pose un probl~me. D'autres sch6mas d'application de l'amoxycilline, ou d'au- tres antibiotiques, ou la combinaison de diff6rents m6dicaments devraient permettre d'atteindre ce but.
R E F E R E N C E S
1. A N D R E A S E N J . J . , A N D E R S E N L . P . - - In vitro sus- ceptiblility of Campylobacter pyloridis to c imet idine , sucral- fate, b i smuth and sixteen antibiotics. Acta Path. Microbiol. Immunol. Scand., 1987, Sect. B ; 95, 147-149.
2. A X O N A T R . - - Campylobacter pyloridis : what role in gastritis and peptic ulcer ? Br. Med. J., 1986 (sept. 27), 293-772.
3. B U R E T I ' E A . , G L U P C Z Y N S K I Y. , J O N A S C., D E R E U C K M., V A N G O S S U M M., D E P R E Z C. , TIE- L E M A N S C., D E L T E N R E M. - - Signification de la pr6- sence de Campylobacter pyloridis dans l 'antre gastr ique : R6sui ta t d ' une 6tude prospective chez 212 pat ients . Acta. Gastroenterol. Belgica, 1986, 49, 70-84.
4. E B E R H A R D T R. , K A S P E R G. , D E T T ' M E R A. , H O C H - T E R W. , H A G E N A D. - - Effect of oral b i smuth subsaly- cilate on Campylobac te r pyloridis and on duodena l ulcer. Gastroenterol., 1987, 92, 1379.
5. G I L L I G A N D. , C O G H L A N G. , H U M P H R I E S H. , MC K E N N A D. , D O O L E Y C., S W E E N E Y E., KEA- NE C. , O ' M O R A I N C. - - Campylobacter pyloridis and recurrence of duodena l ulcers - - An e ighteen m o n t h fol- low-up study. Abstr . No 235, IV th Internat ional Wor- kshop on Campylobac te r Infections, G6 tebo rg , June 16-18, 1987.
6. G I L M A N R. , L E O N - B A R U A R. , R A M I R E Z - R A M O S A. , M O R G A N D. , R E C A V A R R O N S., SPI- R A W . , W A T A N A B E P., K R A F T W. , P E A R S O N A. - - Efficacy of n i t rofurans in the antral gastritis associated with Campylobaeter pyloridis. Abstr. Gastroenterology, 1987, 92 (5, par t 2), 1528.
7. G L U P C Z Y N S K I Y. , L A B B E M., B U R E T T E A. , DEL- MI~E M. , A V E S A N I V., B R O C K C. - - T r e a t m e n t failure of ofloxacin in Campylobacter pyloridis infection. Lancet, 1987 (May 9), i, 1096.
8. G L U P C Z Y N S K I Y. , B R I J C K C., B U R E T T E A . , LAB- BE M. , DELMI~E M., A V E S A N I V. - - Compara t ive in- vitro activity of 21 antimicrobial and anti-ulcer agents against clinical isolates of Campylobacter pyloridis. Abstr. No 58, IV th Internat ional W o r k s h o p on Campylobac te r Infect ions, G6teborg , June 16-18, 1987.
9. G O O D W l N C. S., A R M S T R O N G J. A. - - Will ant ibacte- rial c h e m o t h e r a p y be efficacious for gastritis and peptic ulcer ? J. Antimicrob. Chemother, 1986, 17, 1-4.
10. G O O D W l N C . S . , A R M S T R O N G J . A . , M A R S - H A L L B. J. - - Campylobacter pyloridis gastritis, and pep- tic ulcerat ion. J. Clin. Pathol., 1986, 39, 353-365.
11. G O O D W l N C . S . , B L A K E P., B L I N C O W E. - - The m i n i m u m inhibi tory and bactericidal concent ra t ions of anti- biotics and ant i -ulcer agents against Campylobacter pylori- dis. J. antimicrob Chemoter, 1986, 17, 309-314.
12. G O O D W l N C . S . , M A R S H A L L B . J . , W A R R E N J. R. , B L A C K B O U R N S., B L I N C O W E. D. - - Clearance of C. pyloridis, hnd reduced duodena l relapse with b i smuth and tinidazole c o m p a r e d to cimetidine. Abst r . No 60, IV th In ternat ional W o r k s h o p on Campylobac te r Infect ions, G6- teborg, June 16-18, 1987.
13. H I R S C H L A . M . , S T A N E K G. , R O T F E R M. L., H E N T S C H E L E. , S C H U T Z E K. , P O T Z I R. , G A N G L A. - - C. pyloridis : f requency of occurrence, serology, and susceptibil i ty to antibiotics and ulcer-drugs. Abs t r . No 64, IV th In te rna t iona l W o r k s h o p on Campylobac te r Infec- t ions, G6 tebo rg , June 16-18, 1987.
14. H O R N I C K R. B. - - Peptic ulcer d i s e a s e : A bacterial infection ? N Engl. J. Med., 1987, 316, 1598-1600.
15. K A S P E R G . , D I C K G I E S S E R N . - - Antibiot ic sensit ivity of "Campylobacter pyloridis". Eur. J. Clin. Microbiol., 1984, 5, 444.
16. L A M B E R T J . R . , B O R R O M E O M., P I N K A R D K., T U R N E R H. - - Role of C. pyloridis in essential non ulcer dyspepsia. A r andomized control led trial. Abst r . No 92, IV th In te rna t iona l W o r k s h o p on Campylobac te r Infect ions, G6teborg , June 16-18, 1987.
17. L A M B E R T J. R . , B O R R O M E O M., K O R M A N M. G. , H A N S K Y J . , E A V E S E . R . - - Effect of colloidal b i smuth (De-Nol) on heal ing and relapse of duodena l ulcers - - Role of Campylobacter pyloridis. Abstr . No 91, IV th In ternat ional W o r k s h o p on Campylobac te r Infect ions , G6- teborg, June 16-18, 1987.
256 Volume 17 - N ~ 5 - 1987 Acta Endoscopica

18. LAMBERT T., MI~GRAUD F., G E R B A U D G., COUR- VALIN P. - - Susceptibility of Campylobacter pyloridis to 20 antimicrobial agents. Antimicrob. Agents Chemother, 1986, 30, 510-511.
19. LAMOULIAq ' I 'E H., M E G R A U D F., DE MASCA- REL A . , Q U I N T O N A . - - Placebo-controlled trial of josa- mycin in C. pyloridis associated-gastritis. Abstr. No 190, IV th International Workshop on Campylobacter Infec- tions, Gt3teborg, June 16-18, 1987.
20. L A N G E N B E R G W., RAUWS E. A. J., WIDJOJOKUSU- MO A., T Y T G A T G. N. J . , ZANEN H. C. - - Identifica- tion of Campylobacter pyloridis isolates by restriction endo- nuclease DNA analysis. J. Clinical Microbiol, 1986, 24, 414-417.
21. L A N G E N B E R G W., RAUWS E. A . J . , HOU- THOFF H . J . , O U D B I E R J., TYTGAT G. N. J . , ZA- NEN H . C . - - Follow-up of C. pyloridis-associated gastritis after t reatment with amoxycillin and/or colloidal bismuth subcitrate. Abstr. No 94, IV th International Workshop on Campylobacter Infections, G6teborg, June 16-18, 1987.
22. MARSHALL B . J . , W A R R E N J. R . - - Unidentified cur- ved bacilli in the stomach of patients with gastritis and peptic ulcerations. Lancet, 1984 (June 16), i, 1311-1314.
23. MARSHALL B . J . , ARMSTRONG J . A . , Mc GE- CHIE D. B., GLANCY R. J. - - Attempt to fulfil Koch's postulates for pyloric campylobacter. Med. J. Aust, 1985 (April 15), 142, 436-439.
24. MARSHALL B. J., Mc GECHIE D. B., ROGERS P. A., GLANCY R. J. - - Pyloric Campylobacter infection and gastroduodenal disease. Med. J. Aust., 1985 (April 15), 142, 439-444.
25. Mc NULTY C. A. M., DENT J., WISE R. - - Susceptibi- lity of clinical isolates of Campylobacter pyloridis to 11 antimicrobial agents. Antimicrob. Agents Chemother, 1985, 28, 837-838.
26. Mc NULTY C. A . M . , GEARTY J . C . , CRUMP B., DAVIS M., D O N O V A N I . A . , MELIKIAN V., LIS- TER D. M., WISE R. - - Campylobacter pyloridis and as- sociated gastrit is: investigator blind, placebo controlled
trial of bismuth salicylate and erythromycin ethylsuccinate. Br. Med. J., 1986 (September 13), 293, 645-649.
27. Mc NULTY C. A. M. - - Campylobacter-associated gastri- tis. Am. J. Gastroenterol., 1987, 82, 245-247.
28. Mc NULTY C. A. M., DENT J., FORD G. A., WILKIN- SON S . P. - - Antimicrobial concentrations in the gastric mucosa. Abstr. No 113, IV th International Workshop on Campylobacter Infections, G6teborg, June 16-18, 1987.
29. MORRIS A., NICHOLSON G. - - Ingestion of Campylo- bacter pyloridis causes gastritis and raised fasting gastric pH. Am. J. Gastroenterol., 1987, 82, 192-199.
30. RO ' Iq 'ERDAM H., SOMMERS S. C. - - Biopsy diagnosis of the digestive t rac t : Biopsies interpretation series. Ed. Raven Press, New York, 1981, Chapter 3 ("Stomach"), 63- 79.
31. STEER H. W. - - The gastro-duodenal epithelium in peptic ulceration. J. Pathol., 1985, 146, 355-362.
32. TYTGAT G. N. J . , RAUWS E. A . J . , LANGEN- BERG W . - - The role of colloidal bismuth subcitrate in gastric ulcer and gastritis. Scand. J. Gastroenterol., 1986, 21 (suppl. 122), 22-29.
33. TYTGAT G. N. J . , RAUWS E. A . J . , LANGEN- BERG M. L., H O U T H O F F H. J. - - Campylobacter pylori- d/s : The Amsterdam study. Dig. Dis. Sci., 1986, 10 (Suppl.), 1495.
34. WARREN J. R . , M A R S H A L L B . J . - - Unidentified cur- ved bacilli on gastric epithelium in active chronic gastritis. Lancet, 1983 (June 4), i, 1273-1275.
35. W H I T E H E A D R. - - Mucosal biopsy of the gastrointesti- nal tract. (Volume 3 in the series: Major problems in pathology). 2nd Edition, Saunders Company, Philadelphia, 1979, Chapter 2, pages 11-30.
36. WYATT J. I., R A T H B O N E B . J . , HEATLEY R. V. - - Local immune response to gastric campylobacter in non- ulcer dyspepsia. J. Clin. Pathol., 1986, 39, 863-870.
37. ZHI-THIAN Z, ZHENG-YING W., YA-XIAN C., CHU Y. X., LI Y. N., LI Q. F., LIN S. R., XU Z. M. - - Double-blind short-term trial of furazolidone in peptic ul- cer. Lancet, 1985, i, 1048-1049.
I N T R O D U C T I O N
Several recent studies have shown correlation bet- ween the presence o f Campylobacter-like orga- nisms, now officially recognized as C a m p y l o b a c t e r p y l o r i , and the presence o f histological evidence o f gastritis ans peptic ulcers [2, 3 , 10, 22 , 24 , 32] . Whether this organism is aetiologically linked to the inflammatory alterations o f the gastric mucosa is not yet established, though at least two independent studies in healthy volunteers fulfilling the Koch's postulates strongly support a role in pathogenesis [23, 29] . Furthermore, the role of C. p y l o r i in the pathogenesis o f peptic ulcer disease remains to be clarified [2, 14]. Prevalence o f C. p y l o r i in our group of patients attending the endoscopy clinic is 54 % in non ulcer dyspepsia (n = 308), 64 % in non selected gastric ulcer (n = 61) and 80 % in non selected duodenal ulcer (n = 123).
In vitro susceptibility testings indicate that many antimicrobial agents (penicillins, cephalosporins, erythromycin, tetracyclines, nitrofuranes, nitro-imi- dazole derivatives) and also bismuth salts are active against this bacterium [1, 8, 11, 15, 18, 25].
To date, only f ew controlled studies have been conducted to evaluate the potential benefit o f anti- microbial therapy in C . p y l o r i infection [6, 12, 19, 26].
In order to determine whether these organisms are aetiologically related to the associated gastritis, we undertook a prospective, randomized, double- blind study comparing amoxycillin and placebo in their ability to eradicate these organisms and to study the effect o f therapy on gastritis.
P A T I E N T S A N D M E T H O D S
The study group consisted o f patients attending endoscopy for upper gastrointestinal symptoms in which antral biopsy specimens revealed the presence o f C a m p y l o b a c t e r p y l o r i . Patients were excluded i f they had peptic ulcer, malignancy, cesophagitis, his- tory o f surgery for peptic ulcer (except vagotomy), i f they were already receiving antimicrobial agents or anti-ulcer treatment (except antacids), or i f they gave a history o f allergy to penicillins. The study
Acta Endoscopica Volume 17 N~ 5 - 1987 257

was approved by the medical ethics committee of the Brugmann University Hospital, and all patients enrolled gave informed consent.
Drug administration
The study schedule consisted in two phases :
In phase I, C. pylori positive patients were dou- ble-blind randomized to receive either amoxycillin suspension 20 ml (1 g) twice daily for 8 days or placebo matched to amoxycillin 20 ml twice daily for 8 days.
In phase II, patients were treated on a single blind basis for 14 days with either amoxycillin (at the same dose than phase I) or placebo according to whether they remained C. pylori positive or became C. pylori negative at the end of phase I. Active drug and placebo were kindly provided by Beecham pharma, Benelux, and were offered in identical containers (80 ml) as white suspensions. Both products were strawberry flavoured.
Endoscopy
Gastroscopy was performed in all cases before the beginning of the trial, at day 10 (after treatment phase I) and after 21 days at the end of treatment phase H (usually within 3 days). Follow-up exami- nation was repeated one month after the end of therapy in most patients. In order to avoid that residual inhibitory concentration of the test drug could interfere with the culture of C. pylori, patients were never assessed within the first 24 hours after end of therapy. In most cases gas- troscopy before and after treatment was performed by the same endoscopist. The presence of hyperce- mia, erosions, exulcerations, atrophy or hypertro- phy of the mucosa were recorded. An endoscopic score ranging from 0 to 3 was established as follo- wing : normal appearance = 0 ; hyperaemia = 1 ; some (<~ 3) gastric exulcerations = 2 ; diffuse gas- tric erosions = 3. Four biopsy specimens were systematically taken from the gastric antrum. Two specimens were placed in 10 % formalin solution for histological examination and the two others dipped with a sterile cotton swab within a semi- solid agar transport medium (Portagerm, Bio- Merieux, France) for microbiology.
Histology
Paraffin sections of the tissues fixed in formalin were stained with hematoxylin and eosin. The pre- sence of gastritis was assessed by the same consul- tant histopathologist (C.D.) who was unaware of the patient's history, the endoscopy or the bacterio- logical results. The classification of gastritis (absent, chronic or active) was made on the basis of White- head's and Rotterdam and Sommer's criteria [30, 35]. Grading 1 to 6 was based on the type (mono- nuclear or polymorphonuclear leukocytes) and the
extent of inflammatory cell infiltration. Normal mucosa was considered as grade O. Grade 1 to 3 was attributed to mononuclear infiltration (mild, moderate, severe) whereas grade 4 to 6 referred to polymorphonuclear infiltration (mild, moderate, severe). The presence or absence of C. pyiori was noted (Hematoxylin-eosin stain) but no attempts" were made to score the degree of positivity.
Microbiology
All specimens were transported to the laboratory and processed within two hours of collection. A portion of a biopsy was minced on glass slide and prepared for Gram stain. The specimens were then inoculated onto chocolate agar and a selective medium (modified Thayer-Martin) containing van- comycin (4 mg/1), colistin (7.5 mg/1), amphoteri- cin B (2 mg/1) and trimethoprim (5 mg/ l ) as sup- plements. The rest of the biopsy was finally dipped in 0.5 ml of a 2 % urea broth. The plates were incubated at 37~ in a microaerophilic atmosphere (6 % 02, 10 % C02, Anaerocult C ; Merck, Dar- mstadt, Germany) and examined after 3, 5 and 7 days. Biopsies were considered to be positive for C. pylori if a direct Gram stain preparation showed spiral-shaped bacteria and~or if culture revealed characteristic colonial appearance (grey, translucent, convex). The positive culture results were grossly classified as heavy, moderate and scanty according to the number of quadrants of the plates showing growth of colonies.
The cultural diagnosis was confirmed by a gram- stain on the colonies, a rapid urease activity, and by positive oxidase and catalase reactions. A posi- tive biopsy urease test results in the absence of other positive findings was not considered enough to establish the presence of the organism. In all cases the bacteriological investigations were carried on without knowledge of the clinical, endoscopic or histological data.
Assessments of symptoms
Before treatment, the patients were questioned about the presence and severity of 6 defined symp- toms : nausea, vomiting, heartburn, dyspepsia, ulcer or epigastric pain. The symptoms were graded 0 to 3 (absent, mild, moderate or severe). After treatment, the patients were asked if the symptoms were the same, worse or better. The symptom scores were added for each patient giving a possible score ranging from 0 to 18.
Statistical analysis
Statistical analysis was carried out with the X2 test and the Wilcoxon test. Results were considered significant when the p value was < 0.05.
258 Volume 17 - N ~ 5 - 1987 Acta Endoscopica

R E S U L T S
C h a r a c t e r i s t i c s o f t h e p a t i e n t s
Forty-eight patients were included in the study group from June 1986 through October 1986. Two patients were allocated study numbers but did not start their treatment. One patient was excluded from the study after 8 days, because o f an active duode- nal ulceration which had probably been overlooked at the first endoscopy. O f the remaining 45 patients, there were 38 men and 7 women, and their age ranged from 22 to 82 years (mean, 54.1 years). 32 patients attended endoscopy for upper gastrointestinal symptoms, 11 were attending because of a past history of gastroduodenal ulcer to check for ulcer healing or as part o f a routine follow-up to check for ulcer recurrence. Two patients with an history of recurrent duodenal ulcer had had selective gastric vagotomy. At initial endoscopy, hyperaemia of the antrum or of the fundus was seen in 32 patients, a n t r a l e r o s i o n s i n 5 a n d d u o d e n a l e x u l c e r a t i o n s i n 3 ; n o p a t i e n t had atrophic antral mucosa.
There were no significant differences among the treatment groups with regard to sex, age, ethnic origin, smoking, alcohol intake, past history of ulcer or anti-ulcer treatment. O f the 45 evaluated patients, 22 received amoxycillin and 23 placebo in phase L Overall, the patient's compliance to the study protocol was 100 % (45/45 patients) after one week (phase I) and 82 % (37/45 patients) for phase H.
B a c t e r i o l o g i c a l r e s u l t s
Among the 45 specimens received before treat- ment, 40 (89 %) were positive by culture and 34 (76 %) by the Gram-stain. Twenty-nine cultures yielded moderate or heavy growth and all these specimens were also positive by direct Gram-stain smear. Conversely, Campylobacter-like organisms were seen by gram stain only 5 out o f 11 samples which yielded scanty growth at culture, The biopsy urease test was positive in 40 (89 %) specimens (Table 1). When the time at which the test became positive was recorded, it was seen that 29 (72 %) of the specimens turned to be positive within 2 hours. Twenty-four patients were cleared o f C. pylori after one week treatment : these were 20 of the 22 patients given amoxycillin ( 9 1 % ) and 4 of the 23 given placebo (17 %) (Table 2). Amoxycillin was significantly better than placebo (~=8 .9 ; p < 0.004) in clearing organisms (Fig. 1). In the second phase of the study, amoxycillin proved effective in clearing C . p y l o r i f rom the gastric mucosa in 13/18 (72 %) patients. No significant difference o f bacterial clearance was observed when comparing the group of patients treated for 1 week and the one treated for 2 weeks. All the patients (19/19) who were CP negative after 8 days and subsequently received placebo for 14 days relapsed from their infection when reevaluated after 3 weeks.
T A B L E I
D E T E C T I O N O F C. PYLOR1 B E F O R E T R E A T M E N T BY D I F F E R E N T M E T H O D S
IN T H E T W O T R E A T M E N T G R O U P S
Method of detect ion
No of Urease T r e a t m e n t g roup patients Gram-
stain B i o p s y t e s t
Culture
Amoxyci l l in (n = 22)
Placebo (n = 23)
13 + + + 4 - + + 2 - - + 2 + + _ (a )
1 + - +
14 + + + 4 - + + 1 - - +
2 + + _ ( a )
1 + - +
(a) Cultural con tamina ted by overgrowth of o the r bacterial species.
TABLE II
D E T E C T I O N O F C. PYLOR1 A F T E R 8 D A Y S T R E A T M E N T ( P H A S E I) BY D I F F E R E N T M E T H O D S
IN T H E T W O T R E A T M E N T G R O U P S
Method of detect ion
No of Urease T r e a t m e n t group pat ients Gram-
stain B i o p s y t e s t
Cul ture
Amoxyci l l ine (n = 22)
Placebo (n = 23)
2 0 - m _
2 - + +
12 + + + 2 - + + 3 + + - ( " )
1 + - +
1 - + - 4 _ (b ) - - - -
(a) Cultural con tamina t ed by overgrowth of o the r bacterial species. (b) Presence of C. pylori at histology in one pat ient .
No of patients
25-
20
15
10
5
m Amoxycillin
( N = 2 2 )
[ ] Clearance of CP
lib No clearance of CP
Placebo
(N=23)
Fig. 1
Clearance of C. pylori after one week amoxycillin (20/22) or placebo (4/23)
Acta Endoscopica Volume 17 N ~ 5 - 1987 2 5 9

Histological results
All the patients had histological evidence of gas- tritis before therapy. Thirty (67 %) had chronic active gastritis (polymorphonuclear infiltration). Fif- teen (33 %) had chronic non evolutive gastritis (lymphocytar or lympho-plasmatocytar infiltration). There was no difference in the histological score between the amoxycillin and placebo groups before therapy (mean score : 3.6 vs 3.8). Clearance of C. pylori after 8 days was associated with a significant improvement of the gastritis score (mean score : 2.1 vs 4.2 ; p < 0.0002) (Fig. 2). Moreover, histologi- cal score significantly improved after amoxycillin treatment (mean score : 3.6 vs 2.2 ; p < 0.05), but did not after placebo (mean score : 3.8 vs 4.0 ; ns) (Fig. 3).
Histological score
Histological score
Before After treatment treatment
6
4
3
2
0 ~ - - _ Amoxyclllin
6
5
4
3
2
1
Before After treatment treatment
Fig. 2
Histological features after one week treatment according to the clea- rance of organisms
0 Placebo
Fig. 3
Evolution of histological score after one week amoxycillin or placebo.
Similar improvement of the histological score was observed after 14 days amoxycillin therapy (mean score : 4.1 vs 2.8 ; p < 0.03). However, recurrence of C. pylori was associated with a significant aggra- vation in all 19 C. pylori negative patients who received placebo for 2 weeks (mean score : 2.1 vs 4.2, p < 0.001).
Endoscopy and assessment of symptoms
Endoscopy results showed an improvement in 4 and 3 cases in the amoxycillin and placebo groups, respectively. Concerning the clinical symptoms, no significant difference was noted between the two groups of patients.s
DISCUSSION
This double blind placebo controlled study confirms the strong correlation between the pre- sence of C. pylori in the gastric antrum and histo- logical active gastritis [2, 10, 22, 31, 34, 36]. Clea- rance of C. pylori was associated with resolution of active gastritis and recurrence of infection with reapparance of active gastritis. We observed no resolution of active gastritis in patients with persis- tent infection.
Minimum inhibitory concentration of amoxycillin for C. pylori are in the range of 0.015 to 0.125 txg/ ml [8, 11, 18, 25]. These concentrations lie far below those achieved (range 14.6 - 180 ; mean 117 ug/g) in gastric biopsy specimens after administra- tion of 500 mg amoxycillin capsule [28]. Our aim in using amoxycillin suspension instead of capsules was based on the assumption that simultaneous local and systemic effect would be more beneficial in clearing the organisms. In fact, the clearance rate (91%) obtained after one week is the highest reported to date with amoxycillin administered in monotherapy. The study schedule allowed also to stress upon the early relapse rate of C. pylori infection (100 % two weeks after amoxycillin the- rapy).
In an open non controlled study, Langenberg et al. [21] found that amoxycillin given as 375 mg tablets t.i.d for 4 weeks eradicated organisms in 70 % at completion of therapy. However, these authors also observed a 60 % relapse rate 4 weeks later. Combination of amoxycillin and bismuth sub- citrate achieved better results (90 % eradication after 4 weeks) but was also associated with a high relapse rate (47 % after 4 weeks). In a double- blind placebo-controlled study, Goodwin et al. [12] found that C. pylori was eradicated in 33 % with bismuth suscitrate alone and reported a 75 % clea- rance rate with combination of bismuth subcitrate (8 weeks) and tinidazole (10 days). These authors also found a significantly reduced duodenal ulcer relapse rate after treatment with bismuth and tinida- zole compared to cimetidine. In an other investiga- tory blind trial comparing bismuth salicylate, ery-
260 V o l u m e 1 7 - N ~ 5 - 1 9 8 7 A c t a E n d o s c o p i c a

thromycin ethylsuccinate and placebo, Mc Nulty et al. [26] observed a 78 % elimination rate after 3 weeks of bismuth salicylate versus 7 % with ery- thromycin and 0 % with placebo. Other workers have also reported preliminary favourable results with bismuth salts alone (clearance rate ranging from 50 to 75 %) [4, 5, 16, 17, 33].
Among other antimicrobial agents, furazolidone and nitrofurantoin have been evaluated and found effective (93 % and 79 % clearance after 2 weeks, respectively) [6]. It is worth mentionning that fura- zolidone had already been used with success by Chinese investigators for the treatment o f peptic ulcer [37]. On the other hand, erythromycin [26], spiramycin [33], ]osamycin [19], doxycycline [29] and ofloxacin [7] as well as ciprofloxacin [13] are not efficacious in the clinical experience.
The results o f these latter studies contrast with in- vitro reports showing that a wide variety of antimi- crobial agents are active and could theoretically be used in clinical controlled trials to study the ~etiolo- gical role o f C. pylori in gastritis and peptic ulcer [1, 8, 11, 13, 15, 18, 24, 25]. Other factors such as local and systemic activity o f the drug, the stability at low pH, the concentrations obtained in the gas- tric crypts and diffusion through the mucus are probably of uttermost importance for predicting the clinical efficacy of different drug regimen [9, 27]. These variables should be further investigated prior to selecting drugs for therapeutic trials.
Emergence of resistance to antimicrobials during treatment has lately been reported [7, 12]. Should
this phenomenon occur more frequently in the future, it would strongly support the use of antimi- crobial drugs in combination. Anyway, these obser- vations underscore the need of systematically scree- ning the organisms for resistance in order to detect possible emergence of resistance to amoxycillin was detected in the patients relapsing after treatment.
CONCLUSIONS
These results clearly support the evidence that C. pylori is a pathogenic rather than a commensal organism and are consistent with the hypothesis that C. pylori is important in the pathogenesis o f gastri- tis. The exact role of this organism in peptic ulcer disease and whether its eradication will have a beneficial influence on the natural history of peptic ulcer disease are questions that will probably take some time to answer. One of the most important question concerning the reappearance of C. pyiori is : does it mean reinfection or recrudescence due to incomplete eradication ? Result of identification of isolates by restriction endonuclease DNA analy- sis seems to support that relapses after apparently successful antimicrobial treatment could be attribu- ted to recrudescence rather than reinfection [20]. With regards of the second hypothesis complete and long lasting eradication of CP remains a problem. Either other scheme of amoxycillin treatment or other antibiotics or combination of different drugs must be seeked in order to achieve this goal.
Acta Endoscopica Volume 17 N" 5 - 1987 261

















![Gastrites-chroniques [Mode de compatibilité]univ.ency-education.com/uploads/.../gastro4an_gastrites-chroniques.pdf · Gastrite chronique liée a l’environnement Définit par la](https://img.pdfslide.fr/doc/110x75/5c99bf2709d3f272758b4dc7/gastrites-chroniques-mode-de-compatibiliteunivency-gastrite-chronique-liee.jpg)