Embed Size (px)
Citation preview

HealthNet TPO
Strategy Paper
2011-2015
12/1/2010

Strategy HealthNet TPO 2011-2015 2
Contents
1. Summary ....................................................................................................... 3 2. Introduction .................................................................................................... 4
1.1 Mission, vision & strategy ............................................................................ 4 1.2 General approach ....................................................................................... 5 1.3 Results 2005-2010 as compared with previous strategic plan .......................... 6
2 The position of HealthNet TPO: context analysis .................................................. 8 2.1 Health challenges in the coming years .......................................................... 8 2.2 The working environment: fragile states and excluded populations ................. 10 2.3 Trends in the donor world ......................................................................... 11
2.3.1 National governments ........................................................................ 11 2.3.2 International agencies ........................................................................ 11 2.3.3 The public ......................................................................................... 12 2.3.4 Corporate support .............................................................................. 12
3 HealthNet TPO towards 2015 .......................................................................... 13 3.1 Operations & Support ............................................................................... 16
3.1.1 Contract Management ........................................................................ 17 3.1.2 Public Health and Community Mobilization/Reflection ............................. 18 3.1.3 Human Resource Management ............................................................ 22 3.1.4 Finance ............................................................................................. 23
3.2 Research, strategy and fund development ................................................... 23 3.2.1 Strategy and risk ............................................................................... 23 3.2.2 Knowledge management & network ..................................................... 23 3.2.3 Branding and fund development: from Charity to Social Entrepreneur ...... 24
3.2.3.1 Branding strategy ........................................................................ 24 3.2.3.2 The financial need of HealthNet TPO ............................................... 25 3.2.3.3 Project funds ............................................................................... 25 3.2.3.4 Coverage of indirect costs ............................................................. 25 3.2.3.5 The business-model ..................................................................... 26
3.2.4 Research and development ................................................................. 28 3.2.5 Development ..................................................................................... 30
4 Budget ......................................................................................................... 31

Strategy HealthNet TPO 2011-2015 3
1. Summary
In 2015 HealthNet TPO is a medium sized aid agency, with an annual turnover of € 20-30
million, some 30 ongoing projects in at least 10 different countries at any given time, and a
headquarter support staff of about 45 Fte’s. Funds will be drawn from institutional donors, and
indirect costs will be covered through a combination of corporate funding and income generated
through a for-profit foundation that is linked with HealthNet TPO.
in 2015, HealthNet TPO has strengthened its organizational and financial organisation, and
strengthened its capacity to produce evidence based intervention models. Key issues in the
coming five years will be:
1. A robust financial and administrative organization;
2. A functional knowledge network;
3. A HRM system that responds to organizational needs and is able to contribute to capacity
building in project sites;
4. Development of a research portfolio according to a new research agenda where
‘collective trauma’ is a central concept;
5. Relation building with institutional donors following a documented donor strategy;
6. A proper balance in coverage of indirect costs.
At the heart of this Strategy Paper 2011-2015 is the identity of HealthNet TPO which consists of
improving access to quality health care for excluded populations in fragile states, through the
development of evidence based interventions.
Four important pointers are:
1. The expertise of HealthNet TPO in specific areas (disease control, mental health, health
finance models, and psychosocial community work) will be continued and extended – but
also needs to be embedded in a coherent approach that contributes to the development
of systems of care.
2. HealthNet TPO aims to improve access to health through integrating public and private
sector health care delivery, based on a contracting approach.
3. HealthNet TPO accepts the ‘basic health care package’ approach as a necessary step
towards building functional systems of service delivery, but also continues to address
broader issues such as women’s health, the role of violence, the position of mental
health and issues of psychosocial suffering.
4. HealthNet TPO will develop a partner-policy that is specifically responding to instable
situations in fragile states where basic capacity is lacking. This includes a
remuneration package for local staff that leads to sustainable development of a
functional civil society agents.

Strategy HealthNet TPO 2011-2015 4
2. Introduction
HealthNet TPO develops a new 5 year strategy in the midst of discussion about the future of
international development cooperation, a global economic crisis and the formation of a new
government in the Netherlands; An interesting time to think about the future. In this era of
change it is important to be very clear about the added value of HealthNet TPO. What role do
we want to play, and what do we need to do in the coming years to be able to play it?
HealthNet TPO is not a classical development agency that works primarily with partners in low
income countries to alleviate poverty. Nor is it a neutral, impartial and independent
humanitarian agency that aims to deliver services paid by funds generated from the general
public. HealthNet TPO’s overall aim is to produce evidence based interventions that help
populations who are excluded from access to quality health care to manage their own health. In
order to achieve that, HealthNet TPO implements projects with these populations, very often in
fragile states, but sometimes for excluded groups in more stable states. These projects
contribute to development of sustainable health services. When possible HealthNet TPO works
closely with governments and always with representatives of local populations, in order to build
local capacity and self-reliance.
This agenda brings HealthNet TPO in the midst of discussions about equity in access to health:
about private and public health care providers; about cultural values and action to reduce
domestic violence; about clarifying the difference between respected traditions and war-bred
habits. In order to do this HealthNet TPO tenders for project funds from institutional donors,
while lobbying actively and sometimes successfully to influence their agenda’s. HealthNet TPO’s
idea of independence is in the successful participation in these debates. The agency has no
funds to call itself independent from institutional donors in a financial way. HealthNet TPO is not
a faith-based organization, and does not shy away from political and ethical questions about
motivation and justification of our work.
In short, HealthNet TPO needs to define it position vis-à-vis a range of strategies most common
in the world of international cooperation such as emergency relief, rehabilitation, structural
poverty reduction, economic sustainable economic growth or civil society contributions to
(global) production of public goods. In this strategy document, this position is defined, the
necessary actions to reach and maintain that position are described, and a sketch of the
outcomes we aim for is given.
1.1 Mission, vision & strategy
Mission
HealthNet TPO develops evidence-based interventions to reach better health for all. The mission
is to enhance the ability of communities in fragile states to better manage their own health and
to build health systems with communities that are excluded from functioning health care by
combining international public health expertise with local tradition.
Vision
HealthNet TPO enters fragile communities using ‘health’ as a universal goal to unite people.
HealthNet TPO aims to rebuild community structures and trust after warfare by building
functional health services, thus uses ‘health’ as a means.
HealthNet TPO starts from local resources and local strengths, and mobilizes communities to
become active stakeholders in health and development.
Throughout the programs HealthNet TPO is sensitive to gender inequity and violence in
relations on all levels.

Strategy HealthNet TPO 2011-2015 5
Strategy
HealthNet TPO gains in-depth understanding of local resources, capacities, beliefs and needs
through action research.
It develops and implements new interventions to support health and sustainable health care
in close collaboration with relevant stakeholders.
Among these stakeholders HealthNet TPO selects effective and sustainable implementers
and/or partners in the field of health care and relevant cross-sectoral interventions to
strengthen health.
By monitoring the effect and applying academic research, HealthNet TPO builds the evidence
base to disseminate successful models.
1.2 General approach
HealthNet TPO develops evidence-based interventions to strengthen the health of populations in
distress. HealthNet TPO aims to contribute to the overall health situation, by developing
systems for the provision of health care and by contributing to community reflection as a
conditional necessity in populations recovering from long-time warfare. The overall health of a
population is more than the sum of its parts, while concurrently it is evident that individuals
cannot heal in a sick society. ‘Health’ is defined by different factors and interventions are
undertaken from various sides. The HealthNet TPO approach can be summarized as follows:
HealthNet TPO works on the structural rehabilitation of health care systems in conflict
affected areas worldwide. It aims at improving the health condition of populations at risk by
understanding, supporting and strengthening coping mechanisms that help communities
recover from decades of warfare, conflict, disaster.
In collaboration with the local population and stakeholders HealthNet TPO focuses on the
implementation, development, reconstruction and improvement of sustainable and
accessible health care systems. It trains and encourages the local population to carry out
initiatives that combat disease, provide psychosocial care, restore infrastructure and
strengthen organizational systems. The aim is to rebuild both individual and family lives as
well as society, and to contribute to the design and installation of functional health care
delivery systems.
A scientific knowledge base is essential to back up the programme interventions, resulting in
higher and sustained impact. HealthNet TPO offers innovative and unconventional solutions
that foster self-reliance and promote sustainable health care accessible to all.
The identity of HealthNet TPO is thus rooted in three ways: 1) building public health systems, 2)
working with excluded populations and in fragile states, and 3) academic work and attitude.
We consider the following to be our core values: to be outspoken, scientific, professional,
improvement oriented, and passionate. The objectives, mission and vision of HealthNet TPO
have been redefined in 2010.
In the five-year period covered in this strategy paper (2011-2015), HealthNet TPO aims:
in general: to consolidate its portfolio volume, strengthen its organizational set-up and financial
basis, and strengthen its capacity to produce evidence based intervention models that enable
people in distress to cope better with their health situation. The strategy to achieve this is a
combination of fund development, knowledge management and applied intervention logic.
more specific: HealthNet TPO will develop a comprehensive approach based on the experience
gained in the last 18 years. The work done on health systems strengthening, disease control,
integration of mental health care, and the development of interventions to address psychosocial
suffering will continue to be developed within a framework that responds to overall challenges
in global health developments. The outcomes of the different interventions will be focused

Strategy HealthNet TPO 2011-2015 6
towards the development of community owned mechanisms that allow communities to take an
active role in the design and management and of health services. The core of this approach is
summarized below. The approach has been leading in the proposals for funding as they have
been forwarded to the Netherlands government (MFS II), the World Bank (in collaboration with
PharmAccess), and the Nationale Postcode Loterij.
In order to achieve this, HealthNet TPO will:
install and manage a knowledge network;
update its human resource management systems;
finalize the review of financial and administrative systems;
implement research, directly and in partnerships, according to a new research agenda;
build sustainable relations with institutional donors following a documented donor strategy;
Create a basis for coverage of indirect costs in balancing income from project activities, free
funds from third parties, and participation in fund-raising actions.
Below we will look at the last five years in order to check our course over time. Then we will
briefly explain the integrated HealthNet TPO approach, and finally we will translate this into
strategic planning.
1.3 Results 2005-2010 as compared with previous strategic plan
In the 5 year strategy plan adopted in 2005, HealthNet TPO aimed to become a an innovative
international health organization, well known among donors, peers, and health policy
developers for specific areas of expertise such as mental health, psychosocial care, disease
control and financially sustainable post-conflict health systems development by 2010. The idea
was that HealthNet TPO should be implementing intervention models as developed in its
projects.
Organization-wise, HealthNet TPO would have a functioning variety of implementation models to
contribute to building sustainable health for people in crisis. The volume of the organisation
would ensure that managerial bureaucracy would not hinder innovative work, while a well-
managed portfolio volume should secure continuity. There should be a decentralized
management structure that allows local specification in implementation, based on universally
applicable management tools; and we would have furthered our contribution to building an
‘evidence based approach’.
In terms of volume, HealthNet TPO was expected to manage a portfolio of € 10-12 million
annually by 2010, of which some 15-20% would be applied research-related; the headquarters
(‘overhead’) occupation should be a maximum of 15 Fte’s, and the indirect cost percentage
maximum 12%.
We have achieved al of these goals – with one exception. The goal not reached is to manage an
annual turnover of 10-12 m annually with only 15 Fte’s. In 2009, turnover was some 14 million,
and Fte’s amounted to around 20.
New interventions have been developed, tested and published. Research has been done to
support this, and publications are listed in each annual report. Examples of new interventions
include the CTP programme, the community based health insurance scheme, and experience
with results based financing.
Overall strategy as developed over last five years
Over the last five years HealthNet TPO has formulated the overall strategy for its project work
in a more coherent way. In its projects, HealthNet TPO aims to come to an integrated, self-
supported continuity of care. Enabling people to take responsibility for their own health and
health care requires people that are able to function at a minimal level. Given the distortion of

Strategy HealthNet TPO 2011-2015 7
warfare on individual and societal levels, the functionality and capability of people is at stake.
For many individuals, rehabilitation through psychosocial care is a necessary first step. For
communities, community reflection is often a first necessary step to create a situation that
allows for effective change. Access to proper primary health care is another condition for
rehabilitation. It takes healthy people to (re)build a society.
The first step is to help those people that need it overcome their fear and trauma. That is done
by drawing on the strength and resilience of others in the community. The community approach
is essential, not only because individual psychological work is not feasible and may not be
culturally relevant, but because of the numbers of people and lack of resources, and the
positive extra effects of working with the whole community. The psychosocial programme (A)
thus helps to bring people together. Not only are those that need help most sought out and
helped, others in the community that can act as resources but often lack the courage in the
light of recent violence are helped to overcome this fear and take on their former, or new, role.
Thus communities are re-created, and also find new roles. Beginnings are made with ‘bottom-
up dialogues’ towards confidence building. Women are involved in conflict-preventive initiatives
and peace building. Initiatives are thought out to help supporting formal peace processes by
planning informal dialogues, building the necessary capacity and influencing the participants in
the official peace process. Exclusion of specific members of society is addressed, and links are
created with peace building activities that promote reconciliation, truth-seeking and transitional
justice. HealthNet TPO has learned that a too strong focus on health in this phase can lead to a
‘tunnel-view’ in which every problematic aspect of daily life is translated as a psychosocial
problems that would need a psychosocial care or health care response. By starting out with the
more neutral term ‘community reflection’ it is possible to bridge to other sectors more easily to
connect resources to needs – which in itself is the most important aspect of psychosocial work.
The second step is to actually ensure access to quality health care: access especially for those
that have (to) overcome fear and trauma, and for the poorest and most vulnerable part of the
population. The most severe health problems are killer diseases such as malaria, tuberculosis
and HIV/AIDS. Overall, mother and child and reproductive health are essential elements of
health care for populations recovering from warfare or natural disaster. Building a basic,
general, primary health care structure is a necessary condition for creating access to any
specific care.
As stated above, the creation of a system that is – at least partly – owned, managed and used
by people is part of a process of building mutual trust and a return to normalcy. Governments
are not expected to contribute much in terms of public services in the process of recovery and
rehabilitation. Making use of all resources available, including user fees, helps to extend the
coverage of services as well as the sense of ownership in the population. The contracting
approach, where performance-based incentives are key to generate both necessary additional
income for health staff and higher quality care for clients, has proven its validity in DR Congo,
Rwanda, Cambodia and Afghanistan. The approach is applies whenever possible.
The third step is in supporting the actual process of restoring local government and the fabric of
society. This may require conflict resolution, mediation processes and anthropologically
informed processes of recovery at community level. Often these processes are conditional to
reaching effects with local government.
Local government is always partner in the installation of primary care services. Even when
material input, trained staff, and political goodwill to establish basic services is lacking, the
additional value of the local government is the potential to embed services into a sustainable
system, as much as provide various levels of government with practical, evidence based ideas
for health reform.
The social fabric of society is addressed in community reflection efforts. The specific focus for
HealthNet TPO is on health services. The effect of working towards a shared goal cannot be

Strategy HealthNet TPO 2011-2015 8
overestimated in the process of bringing people back together again. As a complementary
process to the often top-down defined ‘peace and reconciliation’ process, villagers begin to think
out local strategies. The goals they set are often more modest (not reconciliation, but being
able to live together) and are close to interventions in the psychosocial domain. E.g. self help
groups of veterans, specific, culturally appropriate interventions to work with child soldiers,
raped women, perpetrators in the wider sense of the word, produce very valuable information
and intervention ideas for active prevention of conflict and peace-building). The relations
between conflict resolution and prevention, human rights monitoring, psychosocial and public
healthcare services, and peace-building activities require further underpinning and elaboration
of clear relationships. This will constitute part of the ongoing research agenda and increase the
organisations’ understanding.
Capacity building and training are always central. Training is based on the participatory
development of culturally informed and locally sustainable interventions, in all fields from
human resource development, organisational development and institutional growth.
2 The position of HealthNet TPO: context analysis
2.1 Health challenges in the coming years
In a globalizing world health cannot be seen as a local issue. Health risks are closely related to
issues of poverty and exclusion, to political developments related to the agenda of state
security and the complementary concept of human security, and to new insights in health risks
that have to do with ecological developments as well as a new balance between the traditional
communicable ‘killer diseases’ to non-communicable disease. The challenges ahead should not
take away attention from the problems that are still enormous and that have defined the
agenda of HealthNet TPO: disease control in fragile states, mental health problems and
psychosocial suffering in (the aftermath of) war. But new insights lead to more emphasis on the
interrelated elements of a health system.1
There is growing consensus on the importance of health systems, such as the need for equity in
access, the need to contribute to rebuilding and/or strengthening health systems taking into
account the importance of all health system’s building blocks, the need to find ways to include
both public and private stakeholders, and the challenges of the introduction of results-based
financing.
The expertise of HealthNet TPO in specific areas needs to be continued and extended –
but also needs to be embedded in a coherent approach that contributes to the
development of systems of care.
More emphasis on health systems also has to do with the growing criticism on Official
Development Assistance (ODA). Enormous investments in health have not led to sustainable
development of functional health systems. The focus on the public sector is an important factor
in this failure. Most low income countries that have a functional public sector at all, find it
overburdened and insufficiently equipped to deliver the required quality health services. As a
result the rich benefit more from (donor-) funded public health care than the poor.2 3 This
causes inequalities and inequity, translated in a high proportion of out-of-pocket health
expenditure (>50%). The health providers that operate outside of the public sector remain
invisible, because they do not fit in the pattern that believes that the government should
provide health care.
1 http://www.globalhealth.org/health_systems/ 2 Preker AS, Langenbrunner JC et al, Spending wisely, buying health services for the poor, World Bank, Washington,
D.C.: 2005. 3 Castro-Leal F, Dayton J, Demery L and Mehra K, Public spending on health care in Africa: do the poor benefit? Bulletin of the World
Health Organization, 78(1): 66-74, 2000.

Strategy HealthNet TPO 2011-2015 9
Governments need to take responsibility, but when necessary preconditions to install a public
health system are not met - the availability of the budget to pay for health care for all -
alternatives need to be found. These funds should be brought in through the collection of taxes,
as a means to enforce income solidarity and in the end deliver the services. An increase in
public healthcare spending through donor financing does not fundamentally alleviate the
problem, as it draws private finance (and as a consequence consumers) away from the private
healthcare providers to the public ones, potentially even leaving the sector worse off – the so-
called crowding out effect. The health sector in low income countries is thus stuck in a vicious
circle of low supply and low demand for health care.
HealthNet TPO wants to respond to this problem by integrating public and private sector health
care delivery, through a contracting approach. Proposals have been prepared in 2010 in
partnership with PharmAccess, and submitted to the Netherlands Government and the World
Bank.
Technical expertise that is partly in-house already and needs to be further extended includes:
Relevant skills and know-how on establishing and implementing smaller and larger private
and public health insurance schemes: the design of risk pools, insurance packages, systems
for premium collection, design of risk equalization mechanisms and raising funding for
implementation, administrative systems for risk pooling such as identification of patients and
related administrative processes, design of a clearing house, selection and contracting of
health administrators and insurance agents;
Design and implementation of equity and debt funds for investments in the health care
delivery system, in assuring quality in health care provision (development of an international
system for accreditation/certification) and involving the private (for profit and not for profit)
sector in the delivery of basic health services and primary health care, including sub-
contracting:
Design and implementation of Health Equity Funds that provide a solid base for inclusion of
the poorest groups until they can be included in an equitable RBF health care delivery
system;
Design and management of large scale disease control programs (Malaria, TB, Aids, Kala
Azar, etc.) that replace disease control models used by governments prior to the conflict,
adapt and modernize an approach that holds in an instable environment and introduce these
adapted models in new health governance structures;
Design of a variety of organizational models for health care provision, e.g. the design of
appropriate approaches to health service delivery for remote and difficult-to-reach target
groups including for HIV/AIDS control interventions such as hill tribes in Southeast Asia,
nomads in Sudan;
Integration of basic psychiatry in national health systems, including psychosocial care that
supports health service delivery;
Socio-economic analysis of determinants of health that lead to ‘bottom-up’ involvement of
civil society in health systems strengthening, community participation, and (community
based) programs providing tailor-made psychosocial support to specific target groups and
broader assistance to strengthen community engagement and community ownership in
fragile states;

Strategy HealthNet TPO 2011-2015 10
Conducting of impact analyses through operational research, measuring medical and financial
effects of programs at various levels (from individual through household and community to
national levels).
This expertise is to be developed in a more systematic way than was done up to now. A
knowledge management system will be operational as from 2011 to organise development of
expertise. Below is a brief description of this knowledge management network.
2.2 The working environment: fragile states and excluded populations
‘Fragile states’ are those complex emergencies that include a risk as potential safe havens for
terrorists. The state security approach that has largely taken over de agenda of international
collaboration since ‘9/11’ focuses on these fragile states, and this focus has shifted attention
away from the traditional agenda on erasing poverty. On the one hand, this has put the work of
HealthNet TPO much more central stage – there is more attention now for the gap between
relief and development than ever before. HealthNet TPO has always sought attention and
support for this ‘gap’, and now seems to be the time to be active in responding to this growing
attention.
On the other hand there is a keen interest from governments in an international agenda where
aid and military pressure are much more linked. NATO and governments put pressure on the
re-development of old counterinsurgency skills, and countries like the Netherlands want to
move ahead in improving the ‘3D’ approach. Close collaboration between military and civil input
in fragile states is a political choice that still needs to prove to be effective in its outcomes in
peace-enforcing operations, but definitely changes the ‘humanitarian space’. This comes with
EU ideas to set up groups of civilian volunteers on a European scale who should provide the
‘civil’ element in international interventions. All this creates a new environment, in which NGOs
need to be more competitive in showing what their added value is.
In terms of health policy and health systems development, fragile states offer opportunities for
leaps forward in design and implementation of health systems that can often not be made in
countries where hampering aspects of legislation, tradition and elites are still functional. This is
a harsh truth, but the only advantage to be found in an instable situation that leads to
insecurity, lack of governmental protection or civil rights such as fragile states are, is in the
relative absence of rules and regulations that limit innovative interventions. There are often
little or no restrictions on methods or ideas applied in projects in a lawless environment. One
has the opportunity to convince law- and policymakers of specific approaches once national
health policies are developed and implemented on a national level. The experience gained in
pilot projects is invaluable here.
The ethical questions are obvious: does a lack of law- and policymakers not also imply a void in
control of basic principles, ranging from general ‘do-no-harm’ principles in project design to
peer review of the quality of services? HealthNet TPO has chosen to address this problem
through the combination of implementing projects on institutional donor funds and academic
input. The institutional donors require high standards of planning, transparency and reporting.
This is offers a first line of accountability: HealthNet TPO is always fully accountable, not only
for the funds it spends, but also for the way in which these funds are spend – up to the
technical-medical details. The second extra line of accountability is in the academic perspective
in base-line assessments, epidemiological surveys and effect-studies. Outcomes, reports and
publications are shared and submitted for peer review.
Whereas HealthNet TPO accepts the ‘basic health care package’ approach as a necessary
step towards building functional systems of service delivery, HealthNet TPO will continue
to address broader issues such as women’s health, the role of violence, the position of
mental health and issues of psychosocial suffering.

Strategy HealthNet TPO 2011-2015 11
The development of evidence-based interventions that contribute to health systems in fragile
states is thus the core business of HealthNet TPO. HealthNet TPO has contributed to an advice
to the Netherlands government, “Strategy for Dutch engagement in health recovery processes
in fragile states: Building on contemporary policies, practice and science”.4 It was – of course –
recommended that health should be given more attention in policy design for fragile states, and
the approach to ‘basic health care packages’ was seen as helpful for increased access and
equity. It was also noted that maternal health and sexual and gender based violence, as well as
mental health services are not included in the packages as developed in some countries where
the needs are greatest in these field.
2.3 Trends in the donor world
2.3.1 National governments
The present day climate is hostile towards ODA. The new Netherlands government reduced –
for the first time in decades – the 0.8% of GNI for ODA to 0.7%. It has also installed the MSF II
methodology that forces civil society organisation to organise themselves in consortia.
HealthNet TPO is part of the ‘Dutch Consortium for Rehabilitation’, and will work closely with
Care NL, Save the Children NL, and ZOA in the coming five years – provided that the submitted
proposal is accepted. This basically means that funds diminish, while obligations in terms of
accountability and inter-agency coordination grow substantially. This trend in the Netherlands is
not isolated. ODA is criticized worldwide. It seems thus clear that ODA will become a scarcer
commodity than it already is.
The Netherlands government is expected to make choices for ODA for the coming years. The
idea is that there should be a focus on a limited number of themes and countries. The report of
the WRR (Less Pretension, More Ambition) is leading. Health and education sections in the
report have not been well received, but the important issue for HealthNet TPO is that the idea of
working in an innovative way with different players in the field, including the private sector, and
using the added value of specific expertise in the Netherlands (mother and child health, micro-
finance products such as health insurance) offer productive avenues for collaboration with the
Ministry of Foreign Affairs.
2.3.2 International agencies
UN agencies and especially the World Bank, public-private partnerships such as the Global
Fund, the GAVI alliance, and private funds such as the Gates Foundation are important funders
for international health. In line with what is mentioned above, the governmental contributions
to these institutes are expected to diminish with the reduced ODA.
There is a trend starting in the US where very wealthy civilians press their peers to donate more
(the “Giving Pledge”: Gates and Buffet proposed to 40 of their peers to give away half of their
fortunes. which would amount to some 125 billion USD), and in general private funds are
becoming more important in setting agenda’s. Most of these donors fund the international
agencies such as Global Fund or Gavi, and it does not look like a new type of money is
becoming available.
It is important to note that there is maneuvering space in working with the World Bank, and
especially with Global Fund and GAVI funds. The agencies are under pressure to deliver and are
interested in unorthodox options. This maneuvering space can be used to negotiate better
coverage of indirect costs and more efficient ways of managing (clusters of) projects.
4 Netherlands Platform for Global Health Policy and Health Systems Research, June 2009

Strategy HealthNet TPO 2011-2015 12
2.3.3 The public
Since the Netherlands government changed the subsidy regulations some 4 years ago there has
been, as predicted, fierce competition in the Development branch over the public’s attention.
Initiatives range from sponsoring individuals who participate in sports events to radio-shows
and links with companies. There is no visible change in real interest in the underlying issues,
however. Fundraising attempts towards the general public remain costly, and are difficult to
combine with awareness campaigns about the actual situation people live in. The emotional
factor is still predominant, and as such HealthNet TPO still finds it difficult to see how the
continuity that we strive for in a respectful and realistic approach that avoids victimization can
be combined with successful development of fundraising towards the general public.
The market for public fundraising is not only extremely competitive, but also conservative if not
to say extremely old-fashioned in its replication of asymmetric relations between the ‘emotion
of charity’ and a rights-based approach towards development. Some agencies manage to raise
enough funds from the general public to work without institutional donor funds. This position is
tempting in terms of freedom of action (‘anything’ can be done with free funds) and simple
accounting methods (requirements as given by institutional donors are not present). There is
however danger in lack of accountability as well as lack of discipline in achieving and showing
results.
A selected group of the public consists of entrepreneurs or retired businessmen who are
interested in the problems of poverty and exclusion. These are often people with a sincere and
active interest. A clear trend here is personal involvement. This involvement is concrete and
direct: people want to be involved in planning and execution of projects; they want to visit
project sites, organize different support lines, sometimes to the point where the agency is seen
as a facilitator of personal contact between the donor and the people he or she wants to work
with. These initiatives of individuals or groups of individuals is often based on specific capacities
people have, and their perception on how thee can be made of use in poverty alleviation or
other acts of solidarity.5 This assumption is that international cooperation is in essence nothing
more than the application of a specific set of technical skills in other surroundings: the same
assumption that has limited the effect of ODA investment in health for decades. The lack of a
systematic approach and the emphasis on personal relations weakens the effect of this
involvement, whereas relationships of this kind can easily strain the organization that is seen as
the interlocutor.
2.3.4 Corporate support
Sometimes a similar assumption governs the involvement of business, companies that want to
shape their effort in Corporate Social Responsibility (CSR) through active involvement in
international collaboration. The technical skills that a corporation can offer open possibilities
that can go beyond individual project contributions. HealthNet TPO has a long term relation
(since 2004) with the cooperative insurance company Achmea/Eureko, and is beginning to
develop a similar partnership with the cooperative Rabobank. Both companies were
instrumental in the development of a community based micro health insurance scheme, which is
now starting up. There is interesting dynamics in the development of different views on CSR,
but at the same time it is not difficult to see where the problem is. No company can be
expected to become a structural donor; most companies lack the necessary international
expertise in low-income countries, especially those ‘under stress’ now labeled fragile states; as
long as the interest is limited to CSR agenda’s there is no real commitment. More interesting,
not only for companies but for potential beneficiaries, is an attitude that emphasizes ‘return on
investment’. HealthNet TPO is stimulating potential partners to broaden the view on exchange
of knowledge and experience. The challenge for HealthNet TPO is to help partners think about
what that return should be, and how that can be materialized.
5 See description of ‘particulier initiatief’ in De anatomie van het PI: Resultaten van vijf jaar onderzoek naar Particuliere Initiatieven op
het terrein van ontwikkelingssamenwerking. Lau Schulpen, CIDIN, 2010.

Strategy HealthNet TPO 2011-2015 13
Given this brief tour on trends in the donor world, there are conclusions to be drawn and
choices to be made for HealthNet TPO. They are listed under heading ‘branding and fund
development’ below (3.2.2).
3 HealthNet TPO towards 2015
Amidst growing competition over scarce funds for international collaboration, scepticism about
the use of international collaboration, and more and more politicized international agenda,
HealthNet TPO has set a number of aims for the coming five years.
Points of departure are
that HealthNet TPO is not
about service delivery in
itself, but about developing
new, evidence based
intervention models. We
therefore need to be
keenly aware of the role of
civil society in international
change in health policies,
define the added value of
HealthNet TPO in this
perspective, and organize
HealthNet TPO to deliver
this value.
The role of civil society is
changing, as described
above: governments in low income countries have failed to take on the responsibility for health
service delivery, and governments in the high income countries are shying away from real
investment in global health. The ‘market’ is expected to play an increasing role in service
delivery in high income countries, but the private sector is ignored in development of health
systems. In other words, there are openings on all sides for an active civil society, and within
that, agencies that do not automatically expect their activities to be subsidized. This is not to
say that government has become less relevant for finding lasting solutions for lack of services,
but a realistic assessment of the shift in initiative and leadership.
The challenge is in funding the activities of an agency that accepts the diminishing role of state
subsidies. The mix of activities in this respect is under heading ‘fund development’ in this paper.
The potential success of that mix depends first of all on a clear vision, a clear message, a clear
added value.
There is no doubt about what should constitute the added value of HealthNet TPO. The
combination of direct implementation of projects in combination with research to develop new
interventions in health in fragile states is a unique agenda. HealthNet TPO’s added value is
accepted and respected in this field, recognized as it is by WHO, World Bank and national
governments.
Special targets for the coming 5 years are the following:
The establishment of a functional knowledge management network;
A clear research agenda that covers the activities of HNTPO and links with the academic
world;
New tools for new type of field operations (performance based contracts for field staff,
contracted relations within HNTPO);
A fund development and communication system that is ahead of charity models and
manages to link interests between companies, government and CSOs.
HealthNet TPO at a glance:
What: The goal is always related to improved health for populations
excluded from health care How: The means to reach this goal vary from straightforward public
health programming to social rehabilitation of specific target groups or communities (community reflection)
Modus operandi: HealthNet TPO works though a mix of self-managed projects funded through grants in instable settings,
advisory tasks for partners paid by consultancy fees, subcontracted technical support, tendered health system strengthening projects, research grants
Research: These means are applied as much as possible in a research context that leads to evidence based interventions
Communication: These interventions are disseminated through
peer reviewed journals but also in ‘grey literature’, and through
other media that prove to be effective. Communication is continuous in relating to target populations as beneficiaries and benefactors alike.

Strategy HealthNet TPO 2011-2015 14
There is continuity in the following strategic choices:
Working towards complementary modes of interventions in every region/country. The
integrated approach where health systems are built with special attention for mental
health and psychosocial care, health financing, and disease control – as argued for
above.
Strive towards a more balanced geographical spread, where the strength of experience
can be used in clusters of projects and programmes.
Activities of HealthNet TPO include a range of themes…
community reflection activities to prepare for change
disease control = HIV/Aids, malaria, TB, onchocerciasis, kala azar etc
mental health and psychosocial care = integrated psychiatry in primary health care,
psychosocial care, psycho-trauma work
health systems development = district health development, health financing, public-
private mix
…and a range of contexts
Programmes that aim at strengthening local capacity to deal with public health needs of
populations excluded from (or limited) access to primary care in:
Complex emergencies;
Countries that have come out of complex emergencies;
Situations where people are excluded from health care.
Thematic choices are based on the most immediate needs of people challenged by the need to
rebuild their lives and society. We have come to see how important psychosocial care, health
systems development, and peace building are as themes. Within these, HealthNet TPO has
chosen to build special expertise in mental health, disease control and health finance in
rehabilitation. A special focus on mother and child health and HIV/AIDS are natural outcomes of
this choice. But there are other indicators:
Social development, human rights, self-determination and capacity building: these issues
are essential for health – and essential for project funding.
Is there conflict, post conflict, chronic conflict, or exclusion?
Is there sufficient manoeuvring space for developmental activities?
Are potential local partners present, and if not, is there some capacity to relate to in the
local population? And vice-versa, if sufficient local capacity is present, how do we translate
that in our role (partners instead of independent implementers), and are we necessary at
all?
For whom do we work: local government, national government, ‘the population’, a local
organisation?
What is our position vis-à-vis the powers that be – cooperative, avoiding, negotiating, etc?
Do we distinguish between local, regional and national government/authorities, and how
does that effect planning?
Other themes that are close to what we do and sometimes overlap with, include peace building,
human rights work, child protection and gender programmes. Programme activities should be
linked to other sectors when relevant. HealthNet TPO will seek partnership and alliances with
agencies that excel in these fields, rather than ‘do it alone’. There is clear task here that is
related to the knowledge management as relevant in the public health & research department.
Where
HealthNet TPO is currently active in Asia, Africa and Europe. The number of countries where we
work has slowly diminished over the past years. HealthNet TPO has left Eritrea, Ethiopia,
Georgia, Uganda, Bosnia, Rumania, East Timor and Indonesia over the past years. We have a
very modest beginning in Sierra Leone, but overall it proves very difficult to get started in new
countries. At the same time, the project portfolio has grown in financial volume. This

Strategy HealthNet TPO 2011-2015 15
concentration has to do with the growing budgets for programmes where the basic health care
package is to be delivered, rather than the one-issue projects in the past.
It is important to follow a double strategy. The core of
the HealthNet TPO approach is to develop new models.
One needs time to develop these, and the required
project volume depends fully on the type of intervention
at hand. The implementation of the basic health care
package in combination with a health financing model
that requires financial input from the population or
another agent is not something that can be developed in
isolation – a certain minimal coverage is needed.
Coverage is less important when it comes to
interventions that depend more in depth understanding
of specific issues – a community reflection strategy can
be developed in a relatively small area, as long as it
remains possible to test the approach in a wider area –
which can also be done by offering the intervention
technique to partners. The best working situation is one
where a certain volume allows for an input in national
policy debates, while offering a protective environment
for more specialist interventions.The work field is given in
the present clusters of programmes and projects: the
African Great Lakes area (Burundi, DRC, Rwanda,
Uganda, Sudan) in Africa, and Afghanistan, Pakistan,
Nepal, Cambodia and Sri Lanka in Asia. Extension to
areas where there is an obvious need will be sought in
the coming years: North Sudan, Central Africa, Somalia,
West Africa, but also the countries surrounding
Afghanistan, as well as Birma, Indonesia and Laos in East
Asia.
We are interested in consolidation and extension of our
activities in these areas – but we are by no means limited
to these. We can work anywhere where there is a group
of people excluded form access to minimal quality health.
Modes of working
There is a variety of implementation strategies:
The continuation of a set of activities that started in an emergency (projects handed over
to us by other agencies;
Programmes started by HealthNet TPO in areas where there is a clear need for external
assistance in organising access to health, whereas no other presence can fulfil this need
(projects formulated after an initial assessment on or own initiative, or on request from
others;
Programmes developed in response to a call for proposals (be it grants, tenders or
other);
Collaborative work with any other type of agency (as subcontractor, partner, researcher,
in joint venture, partner in a consortium);
As provider of technical assistance to an existing organisation.
Linking skills is a matter of ‘knowledge management’. In HealthNet TPO projects,
‘international knowledge’ is applied locally. We channel the information that is available
in academic institutions or other centres of excellence to the field, where there is a dire
need for this knowledge. Applying this knowledge locally yields new knowledge that
should be channelled back to the international level. Linking local needs with
internationally available expertise is something we will keep doing until the link can be
organised in other ways.
Guidelines for proposal
development
Protocols for the formulation of new proposals as well as for the extension of existing projects need guidelines: Decisions concerning extension will
be taken 6 months for donor-money expires. Decisions are taken in management team.
Donor mapping is done in Amsterdam and the field, in accordance with available capacity.
A final proposal is ready one month
before donor deadline. Proposal writing is seen as a team
effort, with the input of relevant staff. One person will be assigned to take the lead and is responsible for timely production.
Budgets are initially developed
according to standard HealthNet TPO format, later to be adapted to requirements of the foreseen donor (adaptation of the present
HealthNet TPO standard to meet new requirements is done as soon
as possible). Project proposals will circulate
among the relevant staff for comments and final check.
The final version of the project proposal will be submitted to donors only after endorsement by management team.

Strategy HealthNet TPO 2011-2015 16
Bridging in time means that the task of HealthNet TPO comes to an end when there is
local capacity available to do the work. The exit strategy is always closely connected to
the installation of local capacity. This capacity may be supported by newly created links
with the (inter)national world. This local capacity should be able to take on the task of
organising health HealthNet TPO for the target population. It can be organised in a
variety of ways: in a governmental institution, in the private sector, as a local
organisation of any shape.
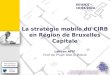
Organisation of the agency headquarters
The organisation of HealthNet TPO is constantly reviewed and updated. Structure follows
strategy, and in 2008-2009 the organisation transformed from an agency with 16 staff in
Amsterdam to an agency with 34 staff and a double portfolio volume. The project ‘Ready for the
Future’ was started in 2009 and continues until at least end of 2011, with the aim to update the
agency in terms of organisation to the demands of a new size as well as a new environment. At
the moment of writing, the outline of the structure at the Amsterdam office is best summarized
in a scheme like this:
(Project Implementation)
Field
HNTPO organisation
Liaison
Officer
Operational Support Team
Implementation &
OrganizationMT
Knowledge Management
Strategy & Risk
Communication & Funds
Development
Research &
Acquisition
Finance
Officer
Research &
Development
P&O
Officer
Technical
Officer
Two parallel ‘streams’ support and guide the projects, from complementary perspectives:
‘Operations & Support’ organises management support to deliver quality work in contracted
projects, and ‘Strategy and Research’ provides development support in translating outcomes
into better input in strategies, projects and dissemination of end results.
3.1 Operations & Support
The Operations & Support department combines all tasks related to ongoing projects. Finance,
contract management, public health support and human resource management is organized in
country teams. ‘Country teams’ are in fact the central platform where relations between
projects and HQ are managed. A country team meets regularly to check on ongoing issues and
decide what type of support is needed. Portfolio managers function as secretaries and
coordinators to the country teams, which are made up of representatives of all relevant
departments.

Strategy HealthNet TPO 2011-2015 17
3.1.1 Contract Management
Contract management relates to all contracted activities both in the field and in the
Netherlands. The portfolio of HealthNet TPO will be much bigger in 2010 as compared to 2009 –
but will most probably shrink back to a more structural volume of around 18-20 million euro’s
on an annual basis for the longer term.
HealthNet TPO works through contracted projects, and submits proposals for funding to
institutional donors. The tendency towards tender procedures is growing. In the context of
HealthNet TPO work there is discussion about this approach: the competitive element is not
always easy to combine with a needs based approach. The challenge is in negotiating
acceptable terms with the donors. So far HealthNet TPO has had moderate success in this.
Contract management is the core of the Operations & Support department. Projects are
supervised and supported, while relations with donors are maintained, all in order to provide
quality project implementation.
In the period 2011-2015 the liaison between HQ and the projects needs to be developed
further. It has been noticed that capacity building poses extra challenges in the environment of
fragile states. Not only in the fragile states, but also in the Amsterdam HQ! The relation
between the Amsterdam HQ and the projects depends on capacity on both ends. This has
implications for notions of partnership.
An important question that needs to be answered in the coming years is whether
partners are available and how they qualify; and if not, how HealthNet TPO strikes a
balance between implementing projects to assist the population and building
partnership capacity?
Independence in the field, the way to offer guidance and supervision, the danger of dependence
through salaried positions rather than performance-based positions, the location of ownership
and policy development, and the very notion of partnership itself are important concepts that
need to be updated in a new environment.
Independence Afghanistan projects
A strong, Afghan and independent public health agency is needed in Afghan civil society for the
future, and HealthNet TPO should prepare its exit as an international NGO in favour of a
national agency. The process will take some years, and the current situation in Afghanistan is of
course not one in which long term predictions can be made.
The Afghanistan the portfolio and the general position of the Afghan national program
management team is ready for an exit strategy of HealthNet TPO. There is no rush to get out of
Afghanistan, but the situation requires a well-planned road towards an independent agency in
Afghanistan that can function as a partner organization. This is a complex process, and needs to
be managed very carefully.
In 2009, a meeting was held in Dubai (November) to mark the first steps in the process. The
O&S department is in charge of guiding this process. The first step is to improve the
management capacity of the Afghanistan Management Board (AMB) of HealthNet TPO
Afghanistan towards the management of an Afghan independent Non-Governmental
Organization (NGO).
A committee is formed at the beginning of 2010, and this committee will organize the process –
both the planning and monitoring of the process itself, as the organization, funding and
implementation of the necessary HRM steps to be taken. It is foreseen that this process will
take several years.
MFS II and challenges to work in a consortium

Strategy HealthNet TPO 2011-2015 18
In November 2010 the Netherlands Ministry of International Cooperation decided that the Dutch
Consortium for Rehabilitation (CARE NL, Save the Children NL, ZOA refugee care and HealthNet
TPO) will be funded with 71 million euro’s for the period 2011-2015. This consortium aims to
improve rehabilitation programming by creating synergy between the different sectors that are
represented: community development, good governance, education and livelihood. Next to the
projects in South Sudan, DR Congo and Burundi, HealthNet TPO is to manage the knowledge
network for this consortium. Developing the above mentioned synergy is an interesting
challenge that will force HealthNet TPO to think beyond the public health spectrum. The
management of this package of activities has proven to be difficult under MFS I and the
previous TMF program. The challenge is more complex now since the consortium approach so
far has produced complex compromises but no clear set management standards. Nevertheless,
the opportunity to learn lessons in collaborating with others is useful.
South Sudan and DR Congo
Growth is aimed for in South Sudan and DR Congo. After the referendum in South Sudan
HealthNet TPO should move forward and start using the opportunities of the different funding
mechanism, as has been done in the set up of HIV/Aids programmes with the World Bank in
2010. The most important lessons to be learnt from the experience in Afghanistan is to avoid
setting up an overhead structure in Sudan and DR Congo itself that hinders rather than enables
strong local organizational capacity building. As said above in the section on HRM, building a
strong organisation without creating a non-sustainable salary structure is important. In
Afghanistan, HealthNet TPO has created a very heavy structure, with an enormous staff. This is
a burden on project development that is hardly realized as long as the budgets remain available
with donors, but even while it lasts it puts too much pressure on the organisation. Management
is more focused on internal problems than on project development. This must be avoided in
South Sudan.
Countries like Afghanistan, Sudan and DR Congo are at the receiving end of different funding
mechanisms (see study on the funding gap in post-conflict situations as commissioned by the
Fragile States Network). The strategy in Sudan and DR Congo must be to make use of the
available funds in a sensible way. The strategy department should provide guidance in finding
the right match between donors that provide complementary funds.
3.1.2 Public Health and Community Mobilization/Reflection
Developments in public health in fragile states point towards a growing focus on health systems
development. HealthNet TPO has already worked towards a more comprehensive approach
since the MSF I projects started. This will be continued and intensified. The point of departure is
to build upon the present evidence base in health care development in fragile states –
acknowledging that more evidence is needed, but also acknowledging that clear choices need to
be made to reach effect.
HealthNet TPO has proven that the introduction of performance based incentives in combination
with smart use of user fees contributes to tangible poverty reduction6. The development and
enhancement of pre-payment systems for health care is expected to bring more beneficial
effects on poverty reduction strategies. Prepayment systems may directly support the poor, by
avoiding catastrophic unpredictable and high out-of-pocket expenditure. A strong program focus
on improving geographical and financial access to quality basic health care, including essential
emergency (obstetric and other) care is expected to lead to improved utilization of essential
health services. HealthNet TPO has been developing Community Based Health Insurance (CBHI)
Schemes on a cooperative basis in fragile states. This is done in collaboration with Achmea and
Rabobank, on the basis of extensive experience in building health systems in the aftermath of
war.
6 Benjamin Loevinsohn, April Harding, “Buying results: Contracting for health services in developing countries” Lancet 2005; 366: 676-81
and “Achieving the twin objectives of efficiency and equity: contracting health services in Cambodia” ERD Policy Brief Series no 6. Asian
Development Bank, March 2002.

Strategy HealthNet TPO 2011-2015 19
The results of this approach extend beyond the function of an insurance scheme as such.
Extra’s are:
Access to health is created for the poor;
Poverty reduction is reached through economizing on out-of-pocket health expenditure;
Applying the association philosophy helps repair the fabric of social life that is often
destroyed by decades of warfare;
And governments are presented with role models that help them take their responsibility
in enabling cost-effective public health care.
Building civil society
Building civil society is an explicit strategy in this approach. In the fragile post-conflict states
the program works on community reflection aimed at supporting vulnerable groups to
reintegrate in society and to strengthen - in a bottom-up manner - specific and diverse
community groups. Community reflection aims to contribute to building sustainable health care
systems. One of the strengths of the program is the combination of a) concrete economic,
organizational and public health experience in rebuilding functional health systems, with b)
experience in the field of activating and ‘mobilizing’ traumatized communities through
psychosocial interventions. In stable countries, the program works with and builds capacity of
existing institutions (public and private health care providers; patient organizations;
performance-based finance (PBF) committees; private health insurers; other national partners).
Partnerships and the promotion of ‘ownership’, amongst others by effectively transferring
knowledge and skills, is an essential feature of the program.
Influencing policy
Developing innovative and responsive models of health care implies supporting and empowering
clients and community organizations to express their needs and to facilitate their participation
in health care planning and management. At the local level, this impacts on power relations
between local health providers, health financers, clients and local government. Therefore, the
program is instrumental in health policy development at the local level. Further, the program is
strongly involved in policy development at national and global levels; field experiences on
innovative models for health care are analyzed in an in-depth manner, discussed in relevant
forums and published in international peer-reviewed journals7. Policy issues around the
following themes are directly addressed: sustainable economic development; HIV/AIDS; health
system development; human rights; good governance. Overall, the program is in line with
broader development objectives and strategies. The Millennium Development Goals 1, 4, 5 and
6 are directly addressed and the focus of the Health Access Consortium program on influencing
development of national health policies is most relevant for the Paris Agenda which promotes
results based management as a guiding principle of engagement.
The public health group in the Operation & Support department provides technical support to
projects in the field based on this approach.
Community Mobilization/Reflection
Communities in post-conflict areas have specific characteristics. The social fabric is often
destroyed by man-made, sometimes natural disasters; families are scattered, community
members mistrust each other, institutions, political and legal systems designed to protect and
support people malfunction or disappear. Frequently, conflict causes an increase in social
tension as well as damage to the (health) infrastructure and destruction of economic capital,
resulting in an increase in poverty. Cultural notions and practices are under pressure and
families lose their function as a safety net and support system.
For example, sexual and gender based violence in East Congo has dramatically changed ideas
and practice of sexuality with ever-younger girls there. Child soldiers in Uganda and Sudan have
lost the knowledge of a community’s cultural rules; they only know the army rules and
practices. Uprooting of large groups of people in Sudan or Cambodia has destroyed traditional
7 For example: http://content.healthaffairs.org/cgi/content/abstract/28/6/1799

Strategy HealthNet TPO 2011-2015 20
family support systems. These specific aspects of post-conflict situations frequently create a
shift in power relations at all levels of a society; power relations are always gendered and often
related to ethnicity and/or class. Shifts in gender relations provoke a continuation of violence,
often narrowing down within families and communities (e.g. domestic violence). Because the
communal destruction of cultural identity manifests in physical, psychological and social
aspects, these situations can be considered as collective trauma. If we want to properly analyse
and use an effective approach to these problems we need to adopt a holistic view.
The omnipresence of social problems justifies the introduction of community
mobilization/reflection (CMR) —an essential prerequisite for establishing and strengthening
social fabric, networks and services. CMR is an essential component of the HealthNet TPO
intervention strategy, which emphasizes demand-based, sustainable well-being/health. But it
goes beyond; CMR creates a condition in which poor health of individuals does not become an
extra burden on the community. The final outcome is that people of communities in fragile
states are able to better manage their own well-being and health and participate in the
management of their own health care.
Community Mobilization and ‘reflection’: action research in order to develop evidence-
based programmes
CMR is an essential action in post-conflict settings to achieve a level where one can contribute
to the sustainable development of services. HealthNet TPO considers CMR as an integral
component of health programmes and critical in the (re-) establishment of functional health
systems. However, HNTPO also considers CMR as a concept / an approach that goes beyond / is
more than a ‘health programme’. CMR can have an effect on health without the interference of
formal health care; its focus is to improve well-being in the broadest sense. It is about
empowering people to restore social cohesion and build their capacity to take charge of their
own health and well-being; this refers to people’s ability to ‘bounce back’ and to manage the
difficulties they face. Without ignoring or underestimating the importance of professional
(mental) health care and health-related psychosocial support for populations at risk, a much
more socially oriented action should and can be undertaken by local people within the
communities where they live or are forced to live.
CMR describes and analyses the individual and collective mechanisms (which can differ from
community to community) that ensure or hinder the sustainable development of services that
might contribute to a better health and well-being. CMR not only emphasises social
determinants of health, but also food security and livelihoods, education, income, social justice,
shelter and peace which are essential preconditions that need to be addressed to ensure the
development of sustainable health care delivery.
At the very moment of this description and analysis, a crucial intervention occurs. Discovering,
together with the population in crisis or stressful situations, what is most needed and how this
might be obtained not only provides invaluable information about further intervention strategies
but also revitalises skills and (helping) attitudes that as a result of the event or disaster are no
longer utilised. By obtaining an in-depth understanding of local resources, capacities, beliefs
and needs through immediate action and by monitoring the effects, followed by academic and /
or operational research as a next stage, HealthNet TPO aims to build the evidence base to
disseminate successful models.
The entrance is the community; CMR is socially oriented and focuses on enhancing genuine
community engagement in all aspects from planning to on-the-ground actions. Mobilizing people
to undertake action will only be possible by involving community members, institutions and
organisations in decision-making processes, establishing a common ground (values), and
describing and agreeing on everyone's rights and responsibilities in the process. This is import
because people who draw up ideas, norms, rules and resources of social structures (re)produce
society.

Strategy HealthNet TPO 2011-2015 21
CMR is a means to a goal. It is an approach aimed at repairing or strengthening community life,
which is a necessary condition to rebuild life in the aftermath of man-made or natural disasters.
CMR is an umbrella for other interventions; it is underlying our health programmes and
interventions, but it is also underlying the programmes of other organisations, e.g. our partners
in the Dutch Consortium for Rehabilitation (DCR). CMR is thus an intervention strategy that
works at different levels.
In itself, CMR contributes to reconstruct the social fabric of society, to enhancing empowerment
and to help communities define their own agenda. The actual mobilisation takes place through a
wide range of activities that have their own dynamics: from projects that aim at reducing
gender violence, to the creation of health associations and health insurance systems, to socio-
therapy, livelihood and educational programmes and models to improve community
governance.
Putting community reflection into practice
CMR requires community-based approaches that acknowledge and build on existing structures,
practices, traditions and protection mechanisms within the cultural context. As mentioned, CMR
actively promotes community member participation, as well as participation by local
organisations, government and other relevant stakeholders.
Considering CMR as an essential part of HealthNet TPO’s intervention strategies has practical
consequences. First, it requires that in the starting up of a project or programme more time
should be reserved to conduct a proper context analysis and to perform more specific needs
assessments. CMR requires specific staff qualities: people who conduct such assessments need
to be well perceived by other community members, should have the required skills and be
sensitive toward the concerns, feelings and needs of these members. Assessments should
include relevant questions about specific intervention areas; the data to be collected can vary
depending of what is already known, done or on the specific characteristics of an area (related
to tribes, customs, environmental issues, such as land pressure etc.). Since not all problems
can be solved within a limited timeframe, needs must be prioritized and organisations, groups
and/or key persons to work with should be identified.
This ‘community mapping’ will provide invaluable information about the right ‘entry point’ within
specific communities and is needed to create a structure where (local) organisations and
governmental institutions can work together and take responsibility. Only when there is
cohesion among community structures and organisations and government institutions, can
genuine and meaningful capacity building occur; it is a process of direct empowerment through
cooperative participation by which people are invited to take responsibilities from the very start.
Only after analysis of the obtained data, can specific interventions be designed in close
cooperation with all stakeholders. Interventions are not pre-designed, but depend on the needs,
gaps, existing or lacking resources and contextual factors that have been identified during
community mapping.
The relationship between community reflection and ‘standard’ HealthNet TPO’s
activities
The overall purpose of HealthNet TPO is to improve the health status and well being of the
target population by:
1. Understanding, supporting and strengthening coping mechanisms that help communities
to recover from decades of conflict and rebuild their lives and society;
2. To the design and (re-)establishment and / or strengthening of functional health systems
that guarantee access to basic health services.
Ad1) CMR is a strategy aimed at understanding local problems and identifying and
understanding available local resources to address needs. The action research approach used to
collect information at the start of a programme provides the basis to determine the focus of the
interventions. The range of interventions is limited to the definition of the programme: a
malaria control programme will look at context factors such as local health beliefs and

Strategy HealthNet TPO 2011-2015 22
explanatory models, ecological contexts, socio-economic indicators for vulnerability,
acceptability of specific preventive measures and drug resistance. A general health systems
strengthening programme will also consider the socio-cultural, economic and historical context
in which determinants of health are embedded.
Action research will in itself provide the first steps of community mobilisation: in organising the
response from the community, information is gathered about the community itself and
mobilisation starts with the first group discussions. CMR in its ‘underlying function’ can be used
to ‘connect’ the different thematic or specific projects of HealthNet TPO and will help to bring
the so-called ‘multi sectoral approach’ into practice. Given that the mandate and expertise of
HealthNet TPO is focused on specific aspects, interventions will not address all perceived needs
and gaps directly. However, CMR can contribute to connecting the service delivery requirements
with intervention strategies implemented in other projects by other organisations (for example,
for the DCR – see below).
Ad 2) Frequently used concepts within HealthNet TPO are Health System Strengthening with a
specific focus on Mental Health and Psychosocial Support.
Health System Strengthening refers to the design and (re-)establishment of a functional
health system and includes all aspects that accompany the various functions of a health
system (see building blocks annex 3).
Delivery of Mental Health services is an essential and integral component of basic and
essential hospital service delivery, reflected in developed policies and strategies as well
as in health sector plans. HealthNet TPO has an extensive track record in the
development and implementation of psychosocial programmes. CMR should facilitate
expanding the potentially narrow focus on specific mental health concepts (e.g.
psychological trauma) to include a focus on the social context which is vital to well-being
and ensuring that family and community are fully integrated in assessing needs and
interventions.
Providing psychosocial support can vary from the follow-up of patients with mental disorders, to
individual counselling and group work with adults or children in order to prevent more serious
problems (CTP, support groups etc) or psycho-education and awareness-raising to inform the
population at large.
3.1.3 Human Resource Management
The most important challenges for the coming years cover two areas: a clear and competitive
HRD policy for people that work with HealthNet TPO, and a clear and realistic vision on how to
install HRM skills in the field. This division is important and is present in each of the separate fields where action will be taken:
3.1.6.1. New ways to work with regional expatriates and local staff.
As we see in most of the operations there is a very fast increase in salaries for local staff in
management positions overall. HealthNet TPO has so far seen no other option than to follow the
trend or lose the best field staff available. The implications of this trend are bleak: when large
donor commitments will fade away, the new elite that has been groomed by NGOs in countries
such as Afghanistan, Burundi and DR Congo, will have to make a choice to continue their work
on a much lower remuneration base or to seek other options. Many will leave, and the outcome of years of work can be severely damaged.
By 2015, HealthNet TPO will have developed and installed a system where remuneration of local
staff is based on performance, commitment and ownership. We will no longer simply offer
salary contracts. In contributing to the development of an accountable and sustainable civil
society we need to work towards the establishment of local organisations that offer a future for

Strategy HealthNet TPO 2011-2015 23
their staff that goes beyond donor contracts as they exist in the emergency or recovery phase. The solution is in applying insights from the private sector, be it for-profit or not-for-profit.
3.1.6.2. Human Resource Development: for whom?
There are at present no clear ideas about the idea behind human resource development – there
is an ad hoc policy that depends on requests from the field. By 2015 HealthNet TPO has a
strategy that clearly separates the HRD for its own staff from the HRD that should be part of
projects. Building the capacity of staff that is foreseen to play key roles in the long-term should
be part of project implementation. Human resource development will be closely linked to an
overall approach on capacity development, but in the implementation we shall be more clear on
the division between the needs of HealthNet TPO as an international agency and the needs of
he projects. These may of course overlap, and this should also be explicit in formulating an
integrated approach to capacity development (using opportunities such as the LWT with PSO) throughout the organisation.
3.1.4 Finance
The financial department is a new entity. The roles, staff and responsibilities need to be decided
upon at the time of writing. There are some essential tasks that shall be included:
It will provide high quality and timely management information to the MT;
It will make up budgets for program proposals, and ensure that minimal requirements
are met in terms of project implementation and organizational needs;
It will check the quality of financial reports from the field, and prepare these to be send
to the donors;
Upon this basis, it will notice lack of financial-administrative skills in the field, and then
be responsible to build capacity in the field in terms of financial administration and
reporting;
It should therefore be able to either provide or organize admin-finance training in the
field - so there is need for didactic skills.
The very first and absolutely most urgent task for the financial department is in providing
correct and smart management information.
3.2 Research, strategy and fund development
3.2.1 Strategy and risk
The strategy unit will work on overall strategies:
• Country strategies, cross sectoral relations, linking health policies, fragile states,
military-civil relations, links with business and private sector;
• Donor policies, new opportunities in donor country policies and institutional funds;
linking the variety of policies and different types of donors;
• A controllers role vis-à-vis the financial department and financial strategies.
3.2.2 Knowledge management & network
HealthNet TPO is a knowledge-intensive8 organisation. Knowledge is generated for and
disseminated internally to improve project implementation and externally to a market of
multiple stakeholders: academic institutes, INGOs, funding agencies, donors (bi-lateral and
multi-lateral), media, governments, forums and panels. Building upon field experience in
programme and project implementation as well as scientific and applied research, HealthNet
TPO is now developing a uniform system to measure effects, record outcomes and create
“added value” in terms of knowledge quantified as data and documented as information in
reports, documents and publications in external journals, other publications and media.
8 Knowledge intensity is the increasing importance of knowledge for socio-economic activity and for the workforce, resulting in
“knowledge workers” taking on greater prominence within organisations.

Strategy HealthNet TPO 2011-2015 24
HealthNet TPO is responsible for the organisation and maintenance of the knowledge network in
the MFS II consortium for the five years of its implementing work starting January 2011.9
HealthNet TPOs role as a knowledge organisation needs to be reassessed or audited regularly to
stay ahead in a global market where in provision of cutting-edge development services NGOs
need to add to, and at times compete with, academic, commercial and military sectors.
Increasingly, activities are undertaken under a corporate social responsibility mandate or a civil-
military ‘3-D’agenda. These activities at times combine a high level of professional skills with
limited contextual sensitivity in terms of development theory.
HealthNet TPO has a track record of scientific publications, but is weak in documenting concrete
experience in project implementation. The production of ‘grey literature’ needs to be improved,
given that this is the first and most effective line of dissemination of knowledge and experience
towards counterparts in civil society.
HealthNet TPO is developing a phased knowledge management development plan. The initial
development plan starts in the fall of 2010 as a project within the organisation, and will be
tested towards its quality assurance prior to it being made structural to the organisation. Thus
in the coming years development of knowledge management strategies, indicators and specific
time bound actions will be undertaken.
The knowledge network is financed by contributions from project grants. At the outset, as form
2011, thee are funds available from PSO and MFS II. Over time, knowledge network activities
will be budgeted for in all projects eligible.
3.2.3 Branding and fund development: from Charity to Social Entrepreneur
3.2.3.1 Branding strategy
Every day, communications strategies unfold all around us. In this age of unparalleled choice,
communications is committed above all to the principle of broadcasting differences: formulating
the added value and competitive advantages. Here is what separates our findings from all the
others. Here is what makes our approach and our organisation unique.
While it may be easier to think about communications in terms of products or services, it is
more constructive to think in terms of an ongoing and iterative process. A communications
strategy is not the glue between different communications products: it is a means of elaborating
how we network, participate, and interact with relevant target groups. Good communications
reflect a two-way dialogue, where we listen to what our stakeholders expect, design and deliver
audience-informed strategies, and then gather feedback to assess higher impact. But before
proceeding with any form of communication planning, it is necessary to develop the guidelines
for a ‘brand’. Brand marketing is the art of making the right impression on relevant
stakeholders. It is the active process of discovering, developing and bringing the right image or
identity of HealthNet TPO towards different target groups and stakeholders, although consistent
at all times.
Two opposing forces work when it comes to formulating the principles for such an ambitious
plan. First, the knowledge that attention should be paid to the careful choice of strategies,
making choices about focus and setting priorities in imaging, the shape of a professional device
that is sufficiently equipped to perform tasks properly. In short, investing time, resources and
people is a primary step. Secondly, the urgency to gain (fundraising) results in the short term is
evident. The coherence of the various components is described in the matrix below. Although
four different fields (marketing, communications, partnership marketing and fundraising)
basically have their own objectives, there is a question of priorities between the various parts.
9 See appendix “Knowledge Network of the Dutch Consortium Rehabilitation”.

Strategy HealthNet TPO 2011-2015 25
MARKETING
COMMUNICATIONS
PARTNERSHIPS
FUNDRAISING
INTERNAL EXTERNAL
STRATEGIC LEVEL (3 to 5 years)
MARKETING PLAN o 4 P’s o SWOT analysis o Product definition o Product – market
combination o Target Groups o IDENTITY / IMAGE
BRAND STRATEGY o Triangle Website, Intranet, Newsletters o Media and target groups o News and press strategy o HOUSE STYLE
IMAGO TRANSFER o Strategy on
partners o Rights o Develop HNTPO
package o Differentiation of
partners
RISC SPREADING o Strategy recourses
Legal entities Individuals
o Brand association o Instrumental choices
TACTICAL LEVEL (annual plan)
Improving formal/ informal comm. flows, aiming cohesive structures at HQ; HQ-Field; Field-Field
Media training Speakers group Communication materials
Plan for Achmea Proposal for Dutch Lottery
o Prepare active
fundraising 2011. o Elaborate
cooperation: PifWOrld Civil Society Lottery
OPERATIONAL LEVEL (monthly)
Intranet
Newsletters
Website
PR
Newsletters
Achmea
Plexus
Online platform PifWorld
Development /submission Lottery proposal 2011-2015
FUNDAMENT: o CRM – database and information management system o G-drive (joint network HQ) o New location (presentation)
3.2.3.2 The financial need of HealthNet TPO
Based on current trends, the volume of ODA for health will not increase – it will probably
decrease. Is that bad? Not necessarily. Funding may not be the biggest challenge to improve
coverage of quality health care. Given the approach developed over the last years, increased
access to health care requires a new paradigm rather than new funding.
What is important for HealthNet TPO is not growth in turnover, but consistency. HealthNet TPO
needs to be able to keep functioning on the current turn-over level of about € 20-25 million on
an annual basis. The turn-over is necessary for sufficient coverage of indirect funds, and for the
implementation of programmes that have sufficient volume to be able to work on health
systems models. Projects that have the ambition to make a difference in creating local,
functional health systems need a minimal volume to be able to cover the necessary elements of
the system – although it is not always necessary to cover all six ‘building blocks’ covered.
3.2.3.3 Project Funds
In order to implement projects in an environment of accountability, of the necessary volume,
and with the opportunity to disseminate the results through effective channels, HealthNet TPO
needs excellent contacts with institutional donors. Relations with EU, national governments,
PPP’s and large private funds need to be strengthened. A new donor strategy will be developed
for these institutional donors in 2011.
3.2.3.4 Coverage of indirect costs
The weakest point in the organisation HealthNet TPO is the acquisition of free funds. These are
needed to cover the indirect costs that are not covered by institutional donors. This amounts to
the difference between the average contribution to these costs (at about 6%) and a realistic
indirect cost percentage (which is some 14%). There are several sources that are explored: a

Strategy HealthNet TPO 2011-2015 26
possible contribution from the Nationale Postcode Loterij, income through projects that are
implemented for market-conform prices, corporate fund development and public fund raising.
The model that HealthNet TPO aims to realize is as follows:
An annual turnover in the range of €20m;
Composed of e.g. 90% regular, institutional donor funded projects, 10% ‘for-profit’ (or
otherwise regular consultancies);
14% admin and development costs should allow for quality management;
Free funds in range of €1m are needed to cover indirect costs (fundraising is not done
for projects).
HealthNet TPO aims at developing a long-term cooperation with some 20 foundations in Europe
and the United States for co-financing large grants and extra activities. HealthNet TPO aims to
secure 14% of its gross turn-over to maintain an operational level. Therefore, we will seek long-
term funding from corporations, ‘professional philanthropists, participation in ‘electronic
fundraising’, and legacies.
In order to realize this, the department of communication and fund development develops a
marketing strategy that positions HealthNet TPO as a modern, business minded NGO vis-à-vis
corporations with an interest in participation in international health development.
A focus on corporate fund development should be seen as a strategy to reach a number of
goals. Participation of companies that have overlapping interests in developing health systems
will be based on sharing knowledge. Direct funding can be an outcome, as we have known
before in the first years of the relationship with Achmea/Eureko. The value of participation in
project development can also be ‘costed’ and counted as contribution in line with funds from
institutional donors.
Another goal is the introduction of HealthNet TPO to the constituency of partnering companies.
This constituency consists of other stakeholders in the trajectory for project development, such
as clients, employees and other partners. HealthNet TPO has started working with PifWorld as
one option to be further developed in this line.
3.2.3.5 The business-model
HealthNet TPO shall develop a ‘BV’ structure to allow us to make more efficient use of the
resources we have. Some of the work done through tenders is better administrated through a
business-model approach. HealthNet TPO therefore aims to establish a specific branch that is
also able to work ‘for profit’, in order to:
1. Be better able to work on the mandate;
2. Bridge the gap between the public and private sectors in health and fund development;
3. Improve its financial independence;
4. Enhance its position in the chari-market.

Strategy HealthNet TPO 2011-2015 27
Ad 1: The mandate and vision of HealthNet TPO imply that improved access to quality health
care is central for the organisation. People living in ‘low-income countries under stress’ are the
traditional target – but as time goes by, new indicators become more important. Inclusion and
sustainability are indicators that bring groups of people forward for whom we increasingly work.
This includes specifics groups of people who lack good governance (or any governance), access
to work and income, political representation and are deprived of public services. They are found
in urban and rural areas in countries where rcisis continues in a variety of forms, ranging from
warfare to everyday-poverty. Most of these settings are non-responsive to a traditional NGO-
funding request. Moreover, effective interventions require a business-like approach to local
contributions and sustainability. “Profitability is the price for sustainability”.
Ad 2:
In order to reach these people boundaries between so-called public and private sectors of
health need to be crossed. The ADB and World Bank supported ‘contract-approach’, a system of
performance based incentives, has helped achieving just that (Cambodia, Rwanda and other
experience). The logical next step is to initiate quality service delivery through partnerships with
suppliers, clients, and local regulators (ref). This means establishing regulatory bodies that
relate to local and national governments (such as insurance companies); service providers with
adequate clinical and managerial skills; and installation of supervisory skills in governmental
levels. Some of these roles can be played through the NGO set-up, but in other roles a
corporate set-up enables for more effective achievements.
Ad 3:
An example may be the setting where HealthWorks BV bids for the EC tenders that are
exclusively open for for-profit companies, and where one is to organise the spending of EC
funds in a given setting/country. Such contracts are expected to deliver profit, which can be
used to cover indirect costs for the NGO projects of Stichting HealthNet TPO. Furthermore,
other activities may also yield results that add to the free reserve of HealthNet TPO.
HealthWorks BV is legally committed to this goal, as is shown in its constituency, bylaws and
ownership regulations.
Ad 4:
Not only a more stable financial position, but also the entrepreneur-spirit that private sponsors
and ‘professional philanthropists’ are looking for, HealthNet TPO will strengthen its position the
chari-market. Full transparency and accountability in the balance between for-profit activities of
the BV and NGO-programmes of the Stichting HealthNet TPO constitutes a modern framework
for action.
HealthNet TPO wants to establish a subsidiary LLC (BV) under the name of HealthWorks BV. to
execute its market services. Over the years HealthNet TPO has established best practices and a
wealth of experience and knowledge. In ‘HealthWorks BV’ this experience is taken to the
market. The mission of HealthWorks BV is to transform best practices into functional, effective
and sustainable health care systems in low income countries under stress.
Services
The market services of HealthWorks BV are foreseen to consist of:
Project Consultancy: providing knowledge both on specialist topics related to health
system development;
Project Implementation: executing third party projects
Project Development: executing projects initiated by ourselves.
Currently we are developing several business cases. The most detailed are:
Initiating a health care insurance system in Cambodia
Initiating a storage centre and distribution system for medical supplies in Afghanistan
Achmea and Rabobank are already partners, and at the time of writing HealthNet TPO is in
touch with Philips.

Strategy HealthNet TPO 2011-2015 28
HealthWorks BV will be a subsidiary of Stichting HealthNet TPO. As major shareholder of the BV,
Stichting HealthNet TPO is responsible for policy development and the distribution of profits.
The aim is to register the BV at the Chamber of Commerce in Amsterdam by 30 September
2011. The registration of the BV in formation at the Chamber of Commerce is a formality with
no strings attached for Stichting HealthNet TPO. For the legalization of the BV a legal document
is required with Articles of Association in which the relation between the Stichting and the BV is
defined and a business plan with a clear definition of the products, markets and prospects. A
deposit of €18.000 is required to finalize the legalization of HealthWorks BV. The board of
HealthNet TPO will be provided with the required documents before 1st July 2011.
3.2.4 Research and development
Background
Research is necessary to create a better understanding of the underlying mechanisms that
cause the needs and, (health) problems of individuals and communities living in complex
circumstances as fragile states and low income countries. Research in this context needs to be
participative, action and solution oriented to produce the options for action and the evidence for
specific interventions. The production of evidence is only the first step towards the application
and implementation of sound health policies. Research within HealthNet TPO is also used to
develop procedures to translate knowledge in activities that change health policies.
Research
HealthNet TPO defines the development and implementation of evidence-based interventions for
public health in the realm of post-conflict and complex emergency situations as its core
business. Implementing programmes and conducting research are therefore narrowly linked.
The process is best described as a ‘cybernetic loop’ that integrates research outcomes as
feedback into the programmes. Research is part and parcel of basically all HealthNet TPO
activities, as research is implemented to prepare, support and evaluate interventions. Some
research activities are a fully funded integral part of programme implementation. Other
research is funded separately, and is done on the basis of monitoring and evaluation data by us
or in collaboration with academic partners. Research is also undertaken as an individually
funded activity or conducted by partners under the umbrella/aegis of HealthNet TPO or as a
partner in a consortium of research groups and other organizations.
The main objective of research within HealthNet TPO is the focus on development of and
increase effective interventions, knowledge and expertise.
A second objective of research within HealthNet TPO is related to monitoring and evaluation of
the field activities. A consolidated monitoring and evaluation design is part of any proposal for a
field activity and allows implementing the data collection that is required to serve the ongoing
project, enrich future project cycles, and add to a wider set of research questions, like
improvement, quality control and efficiency of the intervention techniques. Last but not least,
HealthNet TPO uses (publications of) research to promote its expertise and position in the field
among other experts and professionals.
HealthNet TPO stresses the importance of both operational and academic research in order to
address the above-mentioned objectives. HealthNet TPO uses methodologies from several
relevant disciplines (eg social sciences, medical sciences/epidemiology and economic sciences).
In doing so we employ a variety of qualitative and quantitative research methods, including (but
not limited to), case studies, process evaluations, treatment efficacy studies, treatment
mechanisms and processes research. The choice of the methodology will be dictated by the
overall goal: the development of effective, evidence based interventions. Some of the
traditional types of research that apply strict scientific procedures have long term or indirect
effects on projects. Other types of research, eg action research can yield effect in a short time
span. Depending on the research subject and the preferred methodology, the ‘loop’ of applying
results in implementation design may take anything between days, weeks, months and years.

Strategy HealthNet TPO 2011-2015 29
We aim to gain in-depth understanding of local resources, capacities, beliefs and needs, as well
as by monitoring the effect and applying academic research, we build the evidence base to
disseminate successful models. Accordingly, HealthNet TPO has lead and participated in
multidisciplinary academic research projects and has performed research within service-oriented
projects and programs.
Research Themes
HealthNet TPO’s present research program covers a range of research activities within the
different operational themes (eg health system development, disease control, health financing,
public health and mental health and psychosocial distress)
The general main objective of the current research program is to link the burden of
disease with biological and social determinants in relation to (development of) interventions,
(cost-) effectiveness and (possibilities of) financing. (see scheme)
Specific objectives are:
Identification of individual and community indicators to describe and define the
relationships between health and context.
Identification of individual and community mechanisms to describe and define health
(status), functioning and wellbeing
Exploring Individual and communities’ perspectives: from health beliefs, help seeking
behavior, to perceptions of what health care should deliver
Implementation of state-of-the-art knowledge in local, culturally informed research
designs and applications
Integration of relevant sectors that promote or sustain health – eg livelihood
empowerment, education, advocacy, health system development and health economics
Exploring and defining interactions of themes from the major domains: health financing,
disease control, mental health and psycho-social well-being, mother and child health
Understanding of mechanisms in the context that explain individual and
community health/functioning/well-being
Health System development
Core Objectives
i. Theory formation
ii. Development/ improvement of care
iii. Development of tools and procedures
iv. Quality control
Health financing PH/Disease
control MHPSD
Existing coping
strategies and resources
Bio –Medical
determinants Socio-Cultural
determinants

Strategy HealthNet TPO 2011-2015 30
In addition, the overall perspective of the research program anticipates on ongoing and future
issues:
Need for quality improvement of current project activities,
Development and implementation of activities within the framework of MFS II
Collaboration with other organizations
Community Mobilization
- Understanding of community mechanisms that contribute to strengthening resilience and
healing
- Exploring existing resources and coping strategies that help communities recover from
warfare and rebuild their lives and society.
- Development of research tools and methods for collection and analyzing of data.
Socio-cultural mechanisms and determinants of health
- Exploring contextual factors of (mental) health and social functioning, including the
erosion of (social) support structures, poverty, violence and structural (gender-based)
injustice
- Exploring connections between and integration of (mental) health and non-health
sectors, including human rights and poverty alleviation.
- Exploring effects of community-based services, resources and processes on individual
and community health.
- Development of research tools and methods for collection and analyzing of data.
Public health and disease control
- Epidemiological research into the occurrence of diseases and risk factors for diseases
- Effectiveness of existing and new health practices and health programs
- Community perceptions related to health problems and health services
Mental health and psychosocial support
- Development and (process) evaluation of implementation, organization and financing of
context-appropriate care packages/ systems for vulnerable populations in fragile states.
- Exploration and evaluation of treatment and support mechanisms and processes for
mental health and psychosocial problems.
- The integration and up-scaling of mental health in primary health care in fragile states
- Exploring mental health status and subsequent risk and protective factors of populations
in post disasters and complex emergencies.
- Long-term preventive effect of resilience-promoting and community-mobilization
interventions
- Evidence building of specific interventions or treatments; i.e. substance abuse
treatment; mother and child care (psychosocial aspects).
Health financing
- Exploring local perceptions and beliefs of health, helpseeking behaviour and explanatory
models of health in public services and health financing models
- Exploring user perspectives in public services and health financing models
- Exploring community/contextual perspectives in public services and health financing
models
- Development of subjective indicators for assessment of impact and effectiveness of
health financing models
3.2.5 Development
Development in HealthNet TPO refers to the implementation, eg dissemination of all types of
knowledge and expertise and research findings, both within and outside the organisation.
The management of knowledge is therefore a key activity for and throughout the whole
organisation. Strengthening knowledge management by the implementation of knowledge
management systems/procedures and knowledge networks are crucial..

Strategy HealthNet TPO 2011-2015 31
Knowledge management takes into account that the dissemination of “knowledge” should fit in
the perspectives of the different stakeholders:
Country-specific:
- clients of health services and individuals and communities in need for health services,
- local program management
- health professionals (HealthNet TPO), donors and others
- governmental agencies
Non-country specific:
- general program management
- (other) organizations/institutes, universities
- (peer reviewed) journals.
4 Budget
The estimated budget development 2011-2015 follows separately.