Embed Size (px)
Citation preview
1
Intoxication aux cardiotoxiques de l’enfant :
prise en charge en réseau C. Bragança - M. Thicoïpe - SAMU 33 J. Naud - SMUR pédiatriqueP.Chanseau - Centre Antipoison et de Toxicovigilance
2
GGéénnééralitralitééss• Substance cardiotoxique ≠ cardiotrope
– Substance pouvant être dépourvue d’indication cardiologique
– Ayant un tropisme cardiaque– Effet stabilisant de membrane ou toxicité cardiaque directe
• Mortalité élevée– 20 % vs < 2 % pour l’ensemble des intoxications
• Rare• Intoxication accidentelle du jeune enfant (10 %)• Intoxication volontaire de l’adolescent (90%)
Kremlin-Bicêtre 1997-2003: motif hospitalisation en réanimation pour intox = 2% des enfants du service10% >> jeunes enfants intox accidentelles (2/3 d’origine médicamenteuse)90% >> adolescents, intox volontaires 90% toxiques médicamenteux dans 50% cas poly-intoxications
3
PharmacologiePharmacologie
• Propriétés :– Toxicité dose dépendante– Délai d’apparition : 1 à 3 heures
(max 6h sauf LP et digitaliques)
• Médicaments :– Stabilisants de membrane– Inhibiteurs calciques– Digitaliques– Carbamates
4
Médicaments à effet stabilisant de membrane
(ESM) et inhibiteurs calciques
5
MMéédicaments dicaments àà ESMESM
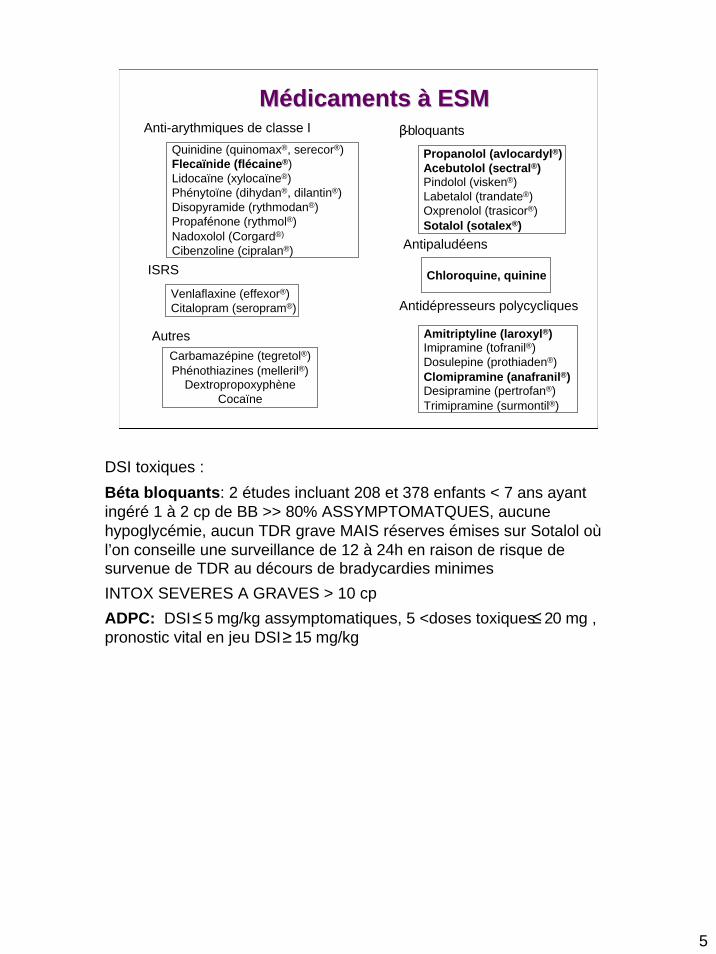
Quinidine (quinomax®, serecor®)Flecaïnide (flécaine®)Lidocaïne (xylocaïne®)Phénytoïne (dihydan®, dilantin®)Disopyramide (rythmodan®)Propafénone (rythmol®)Nadoxolol (Corgard®)
Cibenzoline (cipralan®)
Anti-arythmiques de classe I
Propanolol (avlocardyl®)Acebutolol (sectral®)Pindolol (visken®)Labetalol (trandate®)Oxprenolol (trasicor®)Sotalol (sotalex®)
β-bloquants
Carbamazépine (tegretol®)Phénothiazines (melleril®)
DextropropoxyphèneCocaïne
Autres
Chloroquine, quinine
Antipaludéens
Amitriptyline (laroxyl®)Imipramine (tofranil®)Dosulepine (prothiaden®)Clomipramine (anafranil®)Desipramine (pertrofan®)Trimipramine (surmontil®)
Venlaflaxine (effexor®)Citalopram (seropram®)
ISRS
Antidépresseurs polycycliques
DSI toxiques :Béta bloquants: 2 études incluant 208 et 378 enfants < 7 ans ayant ingéré 1 à 2 cp de BB >> 80% ASSYMPTOMATQUES, aucune hypoglycémie, aucun TDR grave MAIS réserves émises sur Sotalol oùl’on conseille une surveillance de 12 à 24h en raison de risque de survenue de TDR au décours de bradycardies minimesINTOX SEVERES A GRAVES > 10 cpADPC: DSI ≤5 mg/kg assymptomatiques, 5 <doses toxiques≤20 mg , pronostic vital en jeu DSI ≥15 mg/kg
6
ESM : physiopathologieESM : physiopathologie
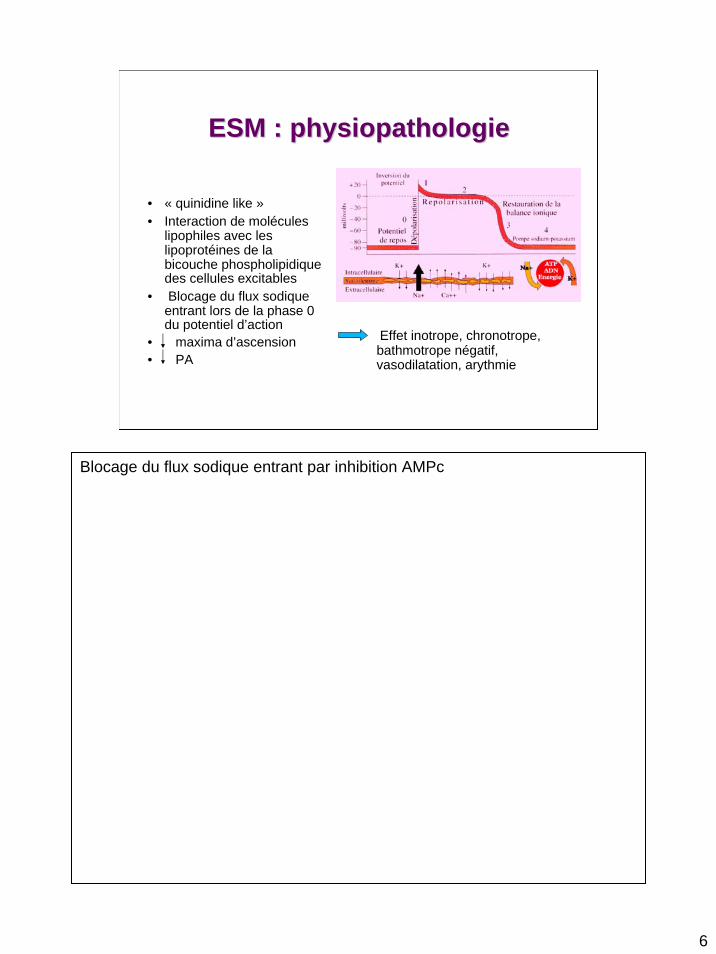
• « quinidine like »• Interaction de molécules
lipophiles avec les lipoprotéines de la bicouche phospholipidique des cellules excitables
• Blocage du flux sodique entrant lors de la phase 0 du potentiel d’action
• maxima d’ascension• PA
Effet inotrope, chronotrope, bathmotrope négatif, vasodilatation, arythmie
Blocage du flux sodique entrant par inhibition AMPc
ESM : clinique
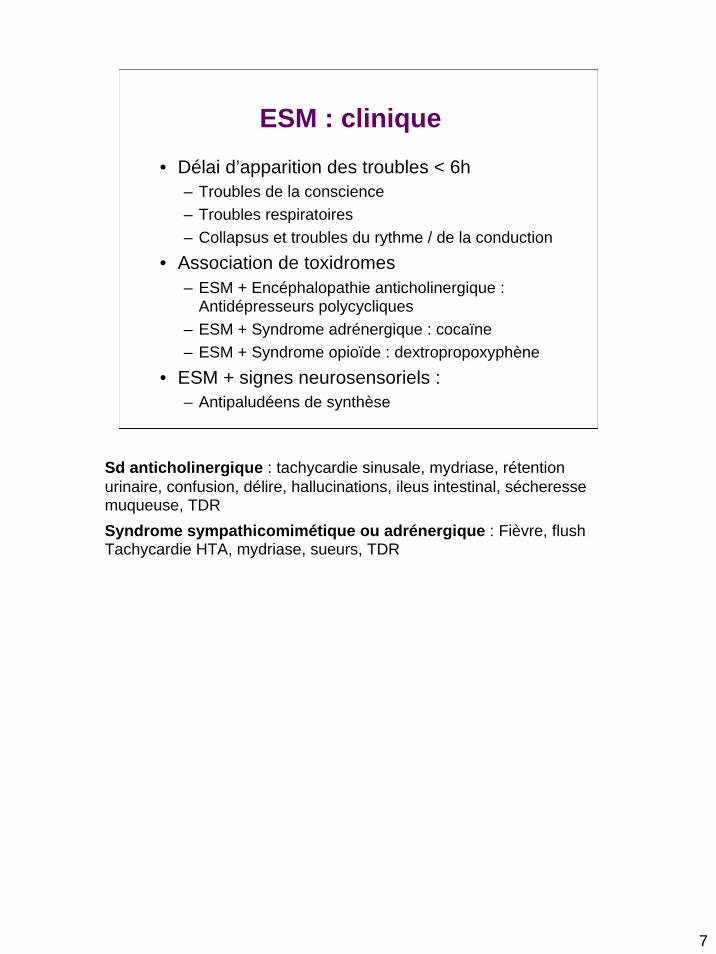
• Délai d’apparition des troubles < 6h– Troubles de la conscience– Troubles respiratoires– Collapsus et troubles du rythme / de la conduction
• Association de toxidromes– ESM + Encéphalopathie anticholinergique :
Antidépresseurs polycycliques– ESM + Syndrome adrénergique : cocaïne– ESM + Syndrome opioïde : dextropropoxyphène
• ESM + signes neurosensoriels :– Antipaludéens de synthèse
Sd anticholinergique : tachycardie sinusale, mydriase, rétention urinaire, confusion, délire, hallucinations, ileus intestinal, sécheresse muqueuse, TDRSyndrome sympathicomimétique ou adrénergique : Fièvre, flush Tachycardie HTA, mydriase, sueurs, TDR
7
8
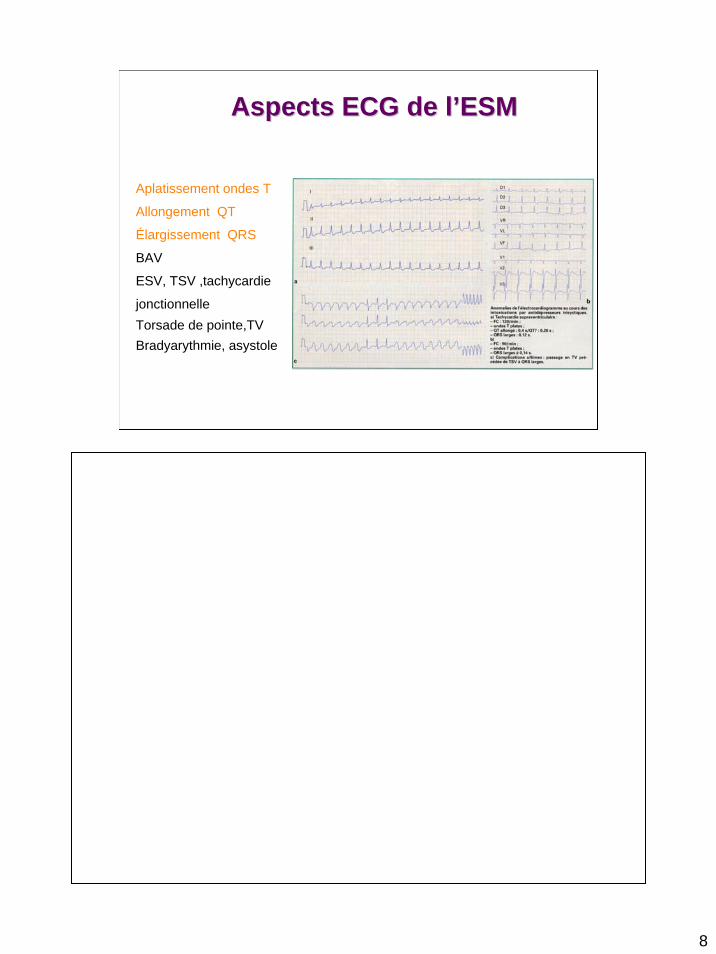
Aspects ECG de lAspects ECG de l’’ESMESM
Aplatissement ondes T
Allongement QT
Élargissement QRS
BAV
ESV, TSV ,tachycardie
jonctionnelleTorsade de pointe,TVBradyarythmie, asystole
9
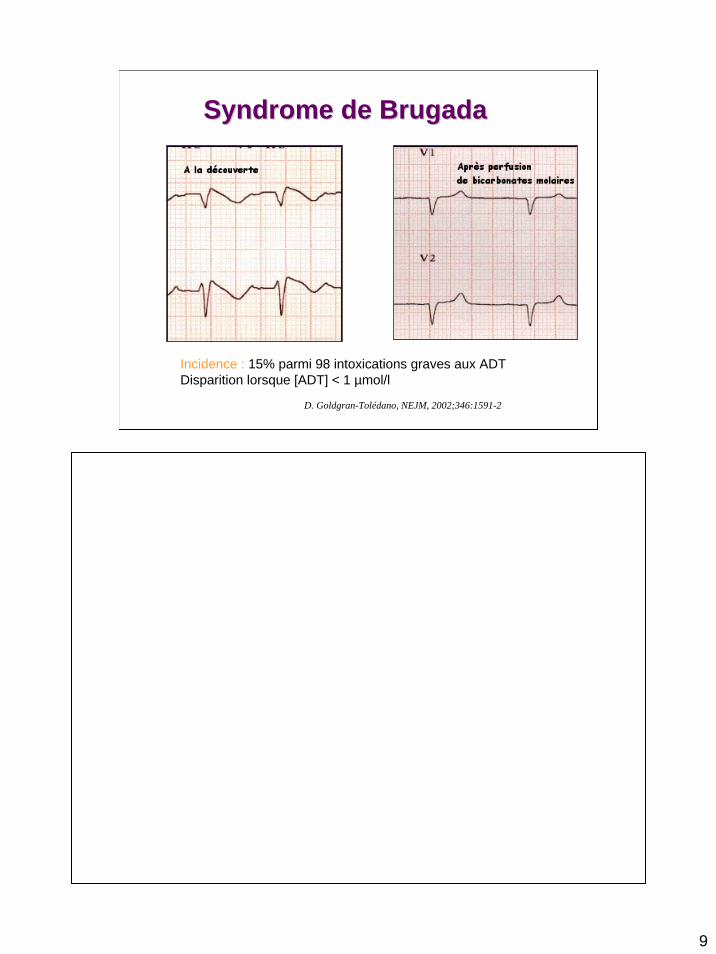
Syndrome de Syndrome de BrugadaBrugada
D. Goldgran-Tolédano, NEJM, 2002;346:1591-2
A la découverte: Après perfusion de bicarbonates molaires:
Incidence : 15% parmi 98 intoxications graves aux ADTDisparition lorsque [ADT] < 1 µmol/l
10
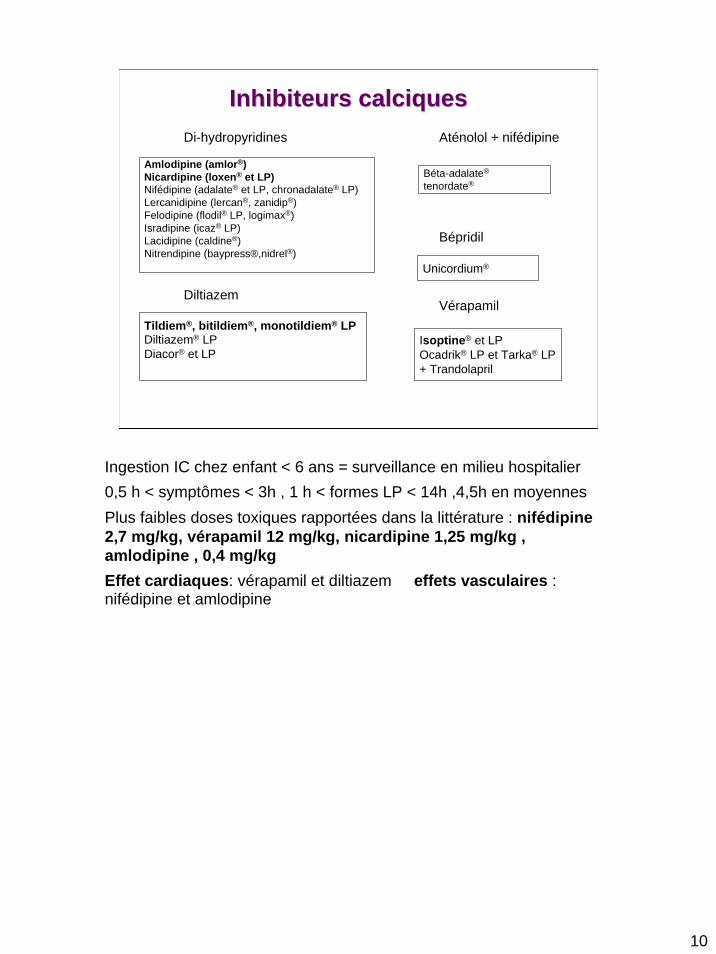
Inhibiteurs calciquesInhibiteurs calciques
Amlodipine (amlor®)Nicardipine (loxen® et LP)Nifédipine (adalate® et LP, chronadalate® LP)Lercanidipine (lercan®, zanidip®)Felodipine (flodil® LP, logimax®)Isradipine (icaz® LP)Lacidipine (caldine®)Nitrendipine (baypress®,nidrel®)
Di-hydropyridines
Béta-adalate®
tenordate®
Aténolol + nifédipine
Tildiem®, bitildiem®, monotildiem® LPDiltiazem® LPDiacor® et LP
Diltiazem
Unicordium®
Bépridil
Isoptine® et LPOcadrik® LP et Tarka® LP+ Trandolapril
Vérapamil
Ingestion IC chez enfant < 6 ans = surveillance en milieu hospitalier0,5 h < symptômes < 3h , 1 h < formes LP < 14h ,4,5h en moyennesPlus faibles doses toxiques rapportées dans la littérature : nifédipine2,7 mg/kg, vérapamil 12 mg/kg, nicardipine 1,25 mg/kg , amlodipine , 0,4 mg/kg Effet cardiaques: vérapamil et diltiazem effets vasculaires : nifédipine et amlodipine
Inhibiteurs calciques : physiopathologie
• Mécanisme– Blocage entrée Ca2+
• phase 0 du PA dans les cellules cardiaques pace maker• Phase 2 pour les cellules contractiles
– Choc cardiogénique par effet inotrope, chronotrope, dromotrope négatif
– Vasoplégiant• Mortalité :
– précoce : 10%– Retardée par SDRA vers J3 (toxicité pulmonaire
des IC?)Sauder, Kopferschmitt, Kempf et Jaeger. Intoxications par les inhibiteurs calciques. Réanimation des intoxications aïgues. Paris, Masson 1995:140-9
11
12
MMéédicaments dicaments CadiotoxiquesCadiotoxiquesThThéérapeutique :rapeutique :
traitements conventionnels traitements conventionnels ththéérapeutiques drapeutiques d’’exceptionexception
13
Traitements conventionnelsTraitements conventionnels• Monitorage, O2, VVP
• Intubation et ventilation d’indications larges– Coma, convulsions– Collapsus même si sujet conscient, détresse respiratoire
• Remplissage vasculaire
• Alcalinisation : bicarbonate ou lactate de Na molaire– 1-2 ml/kg, max 350 ml– Systématique en cas de choc et/ou bloc de conduction
• Catécholamines– Adrénaline ++ si choc d’emblée sévère– Dobutrex, noradrénaline, Isuprel en fonction de la clinique
• Entrainement Electro Systolique– Bradycardie prédominante sans hypoTA
Epuration, dEpuration, déécontamination, contamination, antidotesantidotes
• Lavage gastrique :– Peu d’intérêt si toxiques carbo adsorbables
• Charbon :– Ingestion < 1 h sauf cas particuliers– Doses répétés si formes LP
• Antidotes :– Béta bloquants :
• Isuprel, dobutamine, glucagon– APS :
• Valium– Inhibiteurs calciques :
• Glucagon, sels de calcium• Insuline euglycémique
Insuline euglycémiqueQq cas d’utilisation en pédiatrie concomittente aux amines sels de ca et glucagon (Boyer, Duic,Evans. Hyperinsulinemia euglycemia therapy for IC; Pediatric emergency Care 2002 Feb; 18 (1), 36-7)
14
15
BBééta Bloquantsta Bloquants• Bradycardie sans chute TA :
– Atropine 20 μg/kg, Isuprel 0,1 μg/kg/min , EES
• Hypo TA + bradycardie :– Atropine 20 μg/kg– Remplissage– Echec :
• Dobutamine 10 μg/kg/min– Résistance à la dobutamine :
• Intubation et ventilation assistée• Glucagon 100 μg/kg IVL (2 à 3 min) en bolus renouvelable
puis entretien 70 μg/kg/h IVSE• Alcalinisation• Adrénaline (0,5 μg/kg/min) ou d’emblée si état de choc
majeur
16
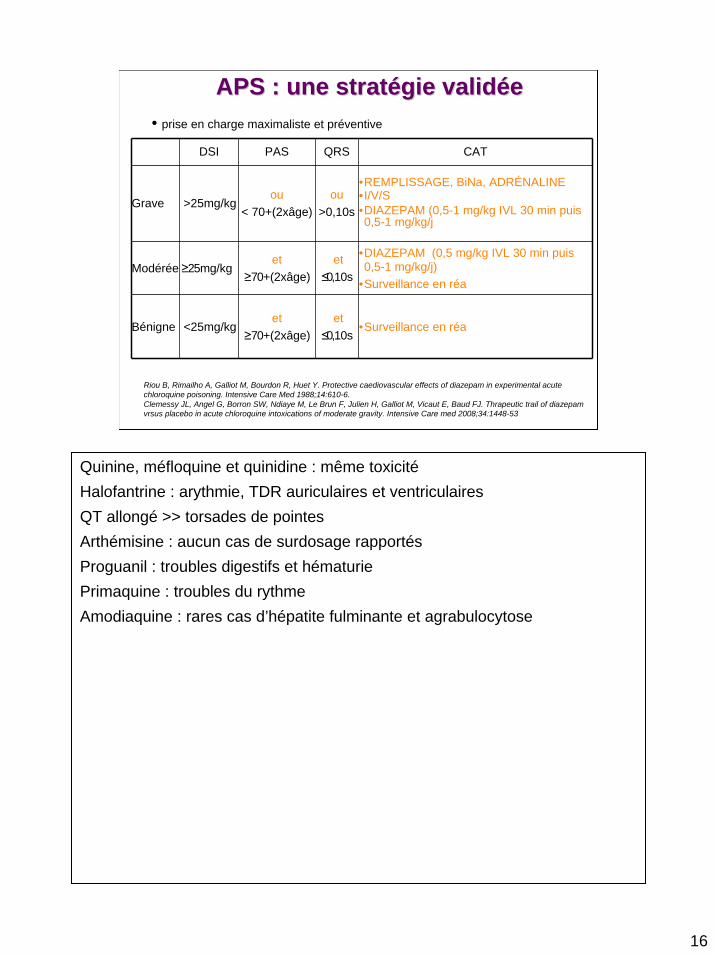
APS : une stratAPS : une stratéégie validgie validééee
DSI PAS QRS CAT
Grave >25mg/kgou
< 70+(2xâge)ou
>0,10s
•REMPLISSAGE, BiNa, ADRÉNALINE•I/V/S•DIAZEPAM (0,5-1 mg/kg IVL 30 min puis 0,5-1 mg/kg/j
Modérée≥25mg/kget
≥70+(2xâge)et
≤0,10s
•DIAZEPAM (0,5 mg/kg IVL 30 min puis 0,5-1 mg/kg/j)
•Surveillance en réa
Bénigne <25mg/kget
≥70+(2xâge)et
≤0,10s•Surveillance en réa
• prise en charge maximaliste et préventive
Riou B, Rimailho A, Galliot M, Bourdon R, Huet Y. Protective caediovascular effects of diazepam in experimental acute chloroquine poisoning. Intensive Care Med 1988;14:610-6.Clemessy JL, Angel G, Borron SW, Ndiaye M, Le Brun F, Julien H, Galliot M, Vicaut E, Baud FJ. Thrapeutic trail of diazepam vrsus placebo in acute chloroquine intoxications of moderate gravity. Intensive Care med 2008;34:1448-53
Quinine, méfloquine et quinidine : même toxicitéHalofantrine : arythmie, TDR auriculaires et ventriculairesQT allongé >> torsades de pointesArthémisine : aucun cas de surdosage rapportésProguanil : troubles digestifs et hématuriePrimaquine : troubles du rythmeAmodiaquine : rares cas d’hépatite fulminante et agrabulocytose
Inhibiteurs calciques
• Bradycardie sans chute TA – Atropine,Isuprel, EES
• HypoTA + bradycardie– Intubation précoce – Remplissage– Amines
• Noradrénaline si vasoplégie prédominante• Dobutamine si choc cardiogénique prédominant• Adrénaline si incertitudes ou explorations impossibles
– Sels de calcium• CaCl2 10% (0,2 ml/kg IVL sur 10 min puis 0,2 ml/kg/h)
– Glucagon,Insuline euglycémique
Insuline euglycémique :1 UI/kg en bolus + 25 g de glucose IV bolus, en entretien : 0,5 à 1 UI/kg/h et 15 à 30 g/h de glucose en fonction des dextro
17
18
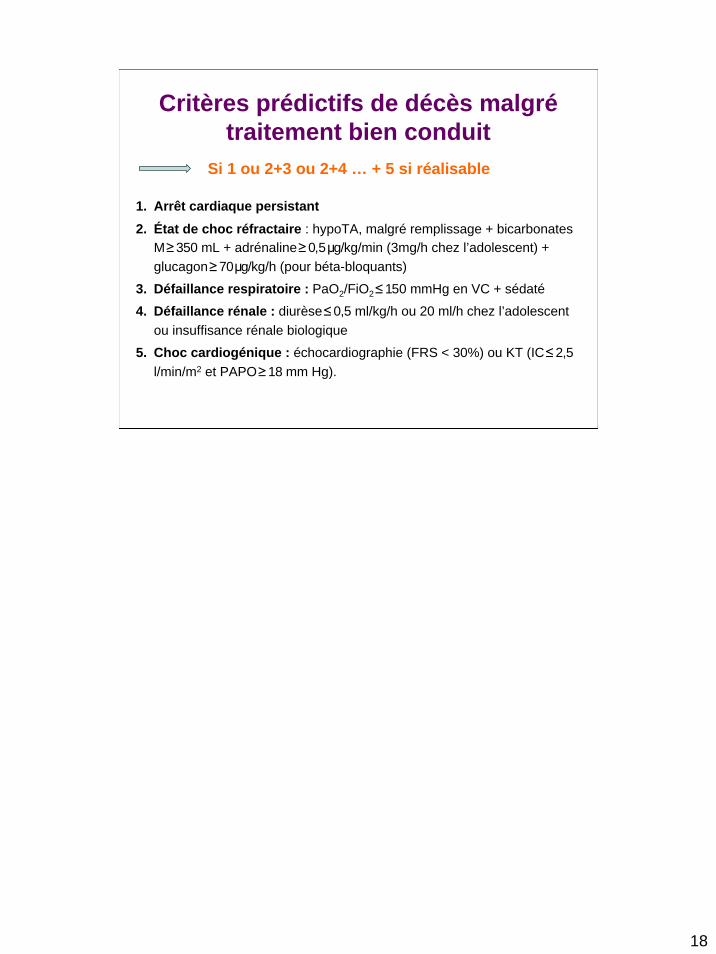
1. Arrêt cardiaque persistant2. État de choc réfractaire : hypoTA, malgré remplissage + bicarbonates
M ≥350 mL + adrénaline ≥0,5 μg/kg/min (3mg/h chez l’adolescent) + glucagon ≥70 μg/kg/h (pour béta-bloquants)
3. Défaillance respiratoire : PaO2/FiO2≤150 mmHg en VC + sédaté
4. Défaillance rénale : diurèse ≤0,5 ml/kg/h ou 20 ml/h chez l’adolescent ou insuffisance rénale biologique
5. Choc cardiogénique : échocardiographie (FRS < 30%) ou KT (IC ≤2,5 l/min/m2 et PAPO ≥18 mm Hg).
Critères prédictifs de décès malgrétraitement bien conduit
Si 1 ou 2+3 ou 2+4 … + 5 si réalisable

ACR et toxique à ESM-IC
• Cas particulier de l’ACR devant une équipe médicale
– Réanimation cardio pulmonaire– Alcalinisation précoce– Dispositif de massage cardiaque automatique– Transport médicalisé en ACR– Assistance circulatoire périphérique
• Limites:– Géographiques– Dispositif MCE
19
Assistance circulatoire
• Pour qui ?– Choc cardiogénique réfractaire– ACR survenant devant une équipe médicale débutant
immédiatement une réanimation cardio pulmonaire
• Où ?– Service rompu à la technique de l’assistance circulatoire
(chirurgie cardiaque)
• Comment ?– Mise en place de procédures– Coopération inter-services
20

Massage cardiaque externe automatisé
• Autopulse® Zoll– Massage cardiaque externe par striction
• Limitations d’utilisation chez l ’enfant : poids > 35 kg• 2 études françaises• Faible population des échantillons
21
22
MCE par striction
Compressions
mécaniques
circonférentielles
Compressions
manuelles
uni-directionnelles
What is the optimal manual compression rate?A quote from the AHA Guidelines:“There is insufficient evidence from human studies to identify a single optimal chest compression rate. Animal and
human studies support a chest compression rate of >80 compressions per minute to achieve optimal forwardblood flow during CPR.” (IV-25)
• The AHA and ERC set the compression rate for manual chest compressions to 100 cpm in order to compensate for the need to achieve a 50% duty cycle (the percent of time the heart is under active compression versus relaxation).
Why does the AutoPulse® run at 80 compressions/minute? Cardiac Pump Thoracic Pump Compresses mainly the heart Compresses the entire chest
It is all based on optimizing blood flow and being within guidelines. The important overview is that the AutoPulse delivers circumferential chest compressions as opposed to a single point of compression.
• The AutoPulse technique of compressions has shown to improve blood flow with a key element being enough chest relaxation time to enhance venous return.
• Here are the important points on why AutoPulse improves blood flow. The references are listed below. • The AutoPulse compression rate is within the guidelines of 80 – 100 per minute.• The AutoPulse will automatically size the chest and deliver 20% circumferential chest compressions.• Instead of the heart being compressed between the sternum and the spine, the entire chest is compressed.
During thoracic compression the intrathoracic volume is reduced, increasing intrathoracic pressure therefore, compressing the heart, collapsing the thoracic arteries, veins and atria driving blood forward.
• With a duty cycle of 50% and 80 compressions per minute, it allows time for good venous return resulting in improved blood flow.
Important studies that show improved blood flow with AutoPulse are:Halperin HR et al. JACC. 2004;44(11):2214-20 Ikeno F et al. Resuscitation. 2006;68:109-118 Timerman S et al. Resuscitation. 2004;61:273-280
23
Compressions
mécaniques
circonférentielles
Compressions
manuelles
uni-directionnelles
MCE par striction
What is the optimal manual compression rate?A quote from the AHA Guidelines:“There is insufficient evidence from human studies to identify a single optimal chest compression rate. Animal and
human studies support a chest compression rate of >80 compressions per minute to achieve optimal forwardblood flow during CPR.” (IV-25)
• The AHA and ERC set the compression rate for manual chest compressions to 100 cpm in order to compensate for the need to achieve a 50% duty cycle (the percent of time the heart is under active compression versus relaxation).
Why does the AutoPulse® run at 80 compressions/minute? Cardiac Pump Thoracic Pump Compresses mainly the heart Compresses the entire chest
It is all based on optimizing blood flow and being within guidelines. The important overview is that the AutoPulse delivers circumferential chest compressions as opposed to a single point of compression.
• The AutoPulse technique of compressions has shown to improve blood flow with a key element being enough chest relaxation time to enhance venous return.
• Here are the important points on why AutoPulse improves blood flow. The references are listed below. • The AutoPulse compression rate is within the guidelines of 80 – 100 per minute.• The AutoPulse will automatically size the chest and deliver 20% circumferential chest compressions.• Instead of the heart being compressed between the sternum and the spine, the entire chest is compressed.
During thoracic compression the intrathoracic volume is reduced, increasing intrathoracic pressure therefore, compressing the heart, collapsing the thoracic arteries, veins and atria driving blood forward.
• With a duty cycle of 50% and 80 compressions per minute, it allows time for good venous return resulting in improved blood flow.
Important studies that show improved blood flow with AutoPulse are:Halperin HR et al. JACC. 2004;44(11):2214-20 Ikeno F et al. Resuscitation. 2006;68:109-118 Timerman S et al. Resuscitation. 2004;61:273-280
24
Compressions
mécaniques
circonférentielles
Compressions
manuelles
uni-directionnelles
MCE par striction
What is the optimal manual compression rate?A quote from the AHA Guidelines:“There is insufficient evidence from human studies to identify a single optimal chest compression rate. Animal and
human studies support a chest compression rate of >80 compressions per minute to achieve optimal forwardblood flow during CPR.” (IV-25)
• The AHA and ERC set the compression rate for manual chest compressions to 100 cpm in order to compensate for the need to achieve a 50% duty cycle (the percent of time the heart is under active compression versus relaxation).
Why does the AutoPulse® run at 80 compressions/minute? Cardiac Pump Thoracic Pump Compresses mainly the heart Compresses the entire chest
It is all based on optimizing blood flow and being within guidelines. The important overview is that the AutoPulse delivers circumferential chest compressions as opposed to a single point of compression.
• The AutoPulse technique of compressions has shown to improve blood flow with a key element being enough chest relaxation time to enhance venous return.
• Here are the important points on why AutoPulse improves blood flow. The references are listed below. • The AutoPulse compression rate is within the guidelines of 80 – 100 per minute.• The AutoPulse will automatically size the chest and deliver 20% circumferential chest compressions.• Instead of the heart being compressed between the sternum and the spine, the entire chest is compressed.
During thoracic compression the intrathoracic volume is reduced, increasing intrathoracic pressure therefore, compressing the heart, collapsing the thoracic arteries, veins and atria driving blood forward.
• With a duty cycle of 50% and 80 compressions per minute, it allows time for good venous return resulting in improved blood flow.
Important studies that show improved blood flow with AutoPulse are:Halperin HR et al. JACC. 2004;44(11):2214-20 Ikeno F et al. Resuscitation. 2006;68:109-118 Timerman S et al. Resuscitation. 2004;61:273-280
25
Compressions
mécaniques
circonférentielles
Compressions
manuelles
uni-directionnelles
MCE par striction
What is the optimal manual compression rate?A quote from the AHA Guidelines:“There is insufficient evidence from human studies to identify a single optimal chest compression rate. Animal and
human studies support a chest compression rate of >80 compressions per minute to achieve optimal forwardblood flow during CPR.” (IV-25)
• The AHA and ERC set the compression rate for manual chest compressions to 100 cpm in order to compensate for the need to achieve a 50% duty cycle (the percent of time the heart is under active compression versus relaxation).
Why does the AutoPulse® run at 80 compressions/minute? Cardiac Pump Thoracic Pump Compresses mainly the heart Compresses the entire chest
It is all based on optimizing blood flow and being within guidelines. The important overview is that the AutoPulse delivers circumferential chest compressions as opposed to a single point of compression.
• The AutoPulse technique of compressions has shown to improve blood flow with a key element being enough chest relaxation time to enhance venous return.
• Here are the important points on why AutoPulse improves blood flow. The references are listed below. • The AutoPulse compression rate is within the guidelines of 80 – 100 per minute.• The AutoPulse will automatically size the chest and deliver 20% circumferential chest compressions.• Instead of the heart being compressed between the sternum and the spine, the entire chest is compressed.
During thoracic compression the intrathoracic volume is reduced, increasing intrathoracic pressure therefore, compressing the heart, collapsing the thoracic arteries, veins and atria driving blood forward.
• With a duty cycle of 50% and 80 compressions per minute, it allows time for good venous return resulting in improved blood flow.
Important studies that show improved blood flow with AutoPulse are:Halperin HR et al. JACC. 2004;44(11):2214-20 Ikeno F et al. Resuscitation. 2006;68:109-118 Timerman S et al. Resuscitation. 2004;61:273-280
26
Compressions
mécaniques
circonférentielles
Compressions
manuelles
uni-directionnelles
MCE par striction
What is the optimal manual compression rate?A quote from the AHA Guidelines:“There is insufficient evidence from human studies to identify a single optimal chest compression rate. Animal and
human studies support a chest compression rate of >80 compressions per minute to achieve optimal forwardblood flow during CPR.” (IV-25)
• The AHA and ERC set the compression rate for manual chest compressions to 100 cpm in order to compensate for the need to achieve a 50% duty cycle (the percent of time the heart is under active compression versus relaxation).
Why does the AutoPulse® run at 80 compressions/minute? Cardiac Pump Thoracic Pump Compresses mainly the heart Compresses the entire chest
It is all based on optimizing blood flow and being within guidelines. The important overview is that the AutoPulse delivers circumferential chest compressions as opposed to a single point of compression.
• The AutoPulse technique of compressions has shown to improve blood flow with a key element being enough chest relaxation time to enhance venous return.
• Here are the important points on why AutoPulse improves blood flow. The references are listed below. • The AutoPulse compression rate is within the guidelines of 80 – 100 per minute.• The AutoPulse will automatically size the chest and deliver 20% circumferential chest compressions.• Instead of the heart being compressed between the sternum and the spine, the entire chest is compressed.
During thoracic compression the intrathoracic volume is reduced, increasing intrathoracic pressure therefore, compressing the heart, collapsing the thoracic arteries, veins and atria driving blood forward.
• With a duty cycle of 50% and 80 compressions per minute, it allows time for good venous return resulting in improved blood flow.
Important studies that show improved blood flow with AutoPulse are:Halperin HR et al. JACC. 2004;44(11):2214-20 Ikeno F et al. Resuscitation. 2006;68:109-118 Timerman S et al. Resuscitation. 2004;61:273-280
27
Compressions
mécaniques
circonférentielles
Compressions
manuelles
uni-directionnelles
MCE par striction
What is the optimal manual compression rate?A quote from the AHA Guidelines:“There is insufficient evidence from human studies to identify a single optimal chest compression rate. Animal and
human studies support a chest compression rate of >80 compressions per minute to achieve optimal forwardblood flow during CPR.” (IV-25)
• The AHA and ERC set the compression rate for manual chest compressions to 100 cpm in order to compensate for the need to achieve a 50% duty cycle (the percent of time the heart is under active compression versus relaxation).
Why does the AutoPulse® run at 80 compressions/minute? Cardiac Pump Thoracic Pump Compresses mainly the heart Compresses the entire chest
It is all based on optimizing blood flow and being within guidelines. The important overview is that the AutoPulse delivers circumferential chest compressions as opposed to a single point of compression.
• The AutoPulse technique of compressions has shown to improve blood flow with a key element being enough chest relaxation time to enhance venous return.
• Here are the important points on why AutoPulse improves blood flow. The references are listed below. • The AutoPulse compression rate is within the guidelines of 80 – 100 per minute.• The AutoPulse will automatically size the chest and deliver 20% circumferential chest compressions.• Instead of the heart being compressed between the sternum and the spine, the entire chest is compressed.
During thoracic compression the intrathoracic volume is reduced, increasing intrathoracic pressure therefore, compressing the heart, collapsing the thoracic arteries, veins and atria driving blood forward.
• With a duty cycle of 50% and 80 compressions per minute, it allows time for good venous return resulting in improved blood flow.
Important studies that show improved blood flow with AutoPulse are:Halperin HR et al. JACC. 2004;44(11):2214-20 Ikeno F et al. Resuscitation. 2006;68:109-118 Timerman S et al. Resuscitation. 2004;61:273-280
28
Compressions
mécaniques
circonférentielles
Compressions
manuelles
uni-directionnelles
MCE par striction
What is the optimal manual compression rate?A quote from the AHA Guidelines:“There is insufficient evidence from human studies to identify a single optimal chest compression rate. Animal and
human studies support a chest compression rate of >80 compressions per minute to achieve optimal forwardblood flow during CPR.” (IV-25)
• The AHA and ERC set the compression rate for manual chest compressions to 100 cpm in order to compensate for the need to achieve a 50% duty cycle (the percent of time the heart is under active compression versus relaxation).
Why does the AutoPulse® run at 80 compressions/minute? Cardiac Pump Thoracic Pump Compresses mainly the heart Compresses the entire chest
It is all based on optimizing blood flow and being within guidelines. The important overview is that the AutoPulse delivers circumferential chest compressions as opposed to a single point of compression.
• The AutoPulse technique of compressions has shown to improve blood flow with a key element being enough chest relaxation time to enhance venous return.
• Here are the important points on why AutoPulse improves blood flow. The references are listed below. • The AutoPulse compression rate is within the guidelines of 80 – 100 per minute.• The AutoPulse will automatically size the chest and deliver 20% circumferential chest compressions.• Instead of the heart being compressed between the sternum and the spine, the entire chest is compressed.
During thoracic compression the intrathoracic volume is reduced, increasing intrathoracic pressure therefore, compressing the heart, collapsing the thoracic arteries, veins and atria driving blood forward.
• With a duty cycle of 50% and 80 compressions per minute, it allows time for good venous return resulting in improved blood flow.
Important studies that show improved blood flow with AutoPulse are:Halperin HR et al. JACC. 2004;44(11):2214-20 Ikeno F et al. Resuscitation. 2006;68:109-118 Timerman S et al. Resuscitation. 2004;61:273-280
29
Compressions
mécaniques
circonférentielles
Compressions
manuelles
uni-directionnelles
MCE par striction
What is the optimal manual compression rate?A quote from the AHA Guidelines:“There is insufficient evidence from human studies to identify a single optimal chest compression rate. Animal and
human studies support a chest compression rate of >80 compressions per minute to achieve optimal forwardblood flow during CPR.” (IV-25)
• The AHA and ERC set the compression rate for manual chest compressions to 100 cpm in order to compensate for the need to achieve a 50% duty cycle (the percent of time the heart is under active compression versus relaxation).
Why does the AutoPulse® run at 80 compressions/minute? Cardiac Pump Thoracic Pump Compresses mainly the heart Compresses the entire chest
It is all based on optimizing blood flow and being within guidelines. The important overview is that the AutoPulse delivers circumferential chest compressions as opposed to a single point of compression.
• The AutoPulse technique of compressions has shown to improve blood flow with a key element being enough chest relaxation time to enhance venous return.
• Here are the important points on why AutoPulse improves blood flow. The references are listed below. • The AutoPulse compression rate is within the guidelines of 80 – 100 per minute.• The AutoPulse will automatically size the chest and deliver 20% circumferential chest compressions.• Instead of the heart being compressed between the sternum and the spine, the entire chest is compressed.
During thoracic compression the intrathoracic volume is reduced, increasing intrathoracic pressure therefore, compressing the heart, collapsing the thoracic arteries, veins and atria driving blood forward.
• With a duty cycle of 50% and 80 compressions per minute, it allows time for good venous return resulting in improved blood flow.
Important studies that show improved blood flow with AutoPulse are:Halperin HR et al. JACC. 2004;44(11):2214-20 Ikeno F et al. Resuscitation. 2006;68:109-118 Timerman S et al. Resuscitation. 2004;61:273-280
30
Compressions
mécaniques
circonférentielles
Compressions
manuelles
uni-directionnelles
MCE par striction
What is the optimal manual compression rate?A quote from the AHA Guidelines:“There is insufficient evidence from human studies to identify a single optimal chest compression rate. Animal and
human studies support a chest compression rate of >80 compressions per minute to achieve optimal forwardblood flow during CPR.” (IV-25)
• The AHA and ERC set the compression rate for manual chest compressions to 100 cpm in order to compensate for the need to achieve a 50% duty cycle (the percent of time the heart is under active compression versus relaxation).
Why does the AutoPulse® run at 80 compressions/minute? Cardiac Pump Thoracic Pump Compresses mainly the heart Compresses the entire chest
It is all based on optimizing blood flow and being within guidelines. The important overview is that the AutoPulse delivers circumferential chest compressions as opposed to a single point of compression.
• The AutoPulse technique of compressions has shown to improve blood flow with a key element being enough chest relaxation time to enhance venous return.
• Here are the important points on why AutoPulse improves blood flow. The references are listed below. • The AutoPulse compression rate is within the guidelines of 80 – 100 per minute.• The AutoPulse will automatically size the chest and deliver 20% circumferential chest compressions.• Instead of the heart being compressed between the sternum and the spine, the entire chest is compressed.
During thoracic compression the intrathoracic volume is reduced, increasing intrathoracic pressure therefore, compressing the heart, collapsing the thoracic arteries, veins and atria driving blood forward.
• With a duty cycle of 50% and 80 compressions per minute, it allows time for good venous return resulting in improved blood flow.
Important studies that show improved blood flow with AutoPulse are:Halperin HR et al. JACC. 2004;44(11):2214-20 Ikeno F et al. Resuscitation. 2006;68:109-118 Timerman S et al. Resuscitation. 2004;61:273-280
31
Compressions
mécaniques
circonférentielles
Compressions
manuelles
uni-directionnelles
MCE par striction
What is the optimal manual compression rate?A quote from the AHA Guidelines:“There is insufficient evidence from human studies to identify a single optimal chest compression rate. Animal and
human studies support a chest compression rate of >80 compressions per minute to achieve optimal forwardblood flow during CPR.” (IV-25)
• The AHA and ERC set the compression rate for manual chest compressions to 100 cpm in order to compensate for the need to achieve a 50% duty cycle (the percent of time the heart is under active compression versus relaxation).
Why does the AutoPulse® run at 80 compressions/minute? Cardiac Pump Thoracic Pump Compresses mainly the heart Compresses the entire chest
It is all based on optimizing blood flow and being within guidelines. The important overview is that the AutoPulse delivers circumferential chest compressions as opposed to a single point of compression.
• The AutoPulse technique of compressions has shown to improve blood flow with a key element being enough chest relaxation time to enhance venous return.
• Here are the important points on why AutoPulse improves blood flow. The references are listed below. • The AutoPulse compression rate is within the guidelines of 80 – 100 per minute.• The AutoPulse will automatically size the chest and deliver 20% circumferential chest compressions.• Instead of the heart being compressed between the sternum and the spine, the entire chest is compressed.
During thoracic compression the intrathoracic volume is reduced, increasing intrathoracic pressure therefore, compressing the heart, collapsing the thoracic arteries, veins and atria driving blood forward.
• With a duty cycle of 50% and 80 compressions per minute, it allows time for good venous return resulting in improved blood flow.
Important studies that show improved blood flow with AutoPulse are:Halperin HR et al. JACC. 2004;44(11):2214-20 Ikeno F et al. Resuscitation. 2006;68:109-118 Timerman S et al. Resuscitation. 2004;61:273-280
32
Compressions
mécaniques
circonférentielles
Compressions
manuelles
uni-directionnelles
MCE par striction
What is the optimal manual compression rate?A quote from the AHA Guidelines:“There is insufficient evidence from human studies to identify a single optimal chest compression rate. Animal and
human studies support a chest compression rate of >80 compressions per minute to achieve optimal forwardblood flow during CPR.” (IV-25)
• The AHA and ERC set the compression rate for manual chest compressions to 100 cpm in order to compensate for the need to achieve a 50% duty cycle (the percent of time the heart is under active compression versus relaxation).
Why does the AutoPulse® run at 80 compressions/minute? Cardiac Pump Thoracic Pump Compresses mainly the heart Compresses the entire chest
It is all based on optimizing blood flow and being within guidelines. The important overview is that the AutoPulse delivers circumferential chest compressions as opposed to a single point of compression.
• The AutoPulse technique of compressions has shown to improve blood flow with a key element being enough chest relaxation time to enhance venous return.
• Here are the important points on why AutoPulse improves blood flow. The references are listed below. • The AutoPulse compression rate is within the guidelines of 80 – 100 per minute.• The AutoPulse will automatically size the chest and deliver 20% circumferential chest compressions.• Instead of the heart being compressed between the sternum and the spine, the entire chest is compressed.
During thoracic compression the intrathoracic volume is reduced, increasing intrathoracic pressure therefore, compressing the heart, collapsing the thoracic arteries, veins and atria driving blood forward.
• With a duty cycle of 50% and 80 compressions per minute, it allows time for good venous return resulting in improved blood flow.
Important studies that show improved blood flow with AutoPulse are:Halperin HR et al. JACC. 2004;44(11):2214-20 Ikeno F et al. Resuscitation. 2006;68:109-118 Timerman S et al. Resuscitation. 2004;61:273-280
33
Compressions
mécaniques
circonférentielles
Compressions
manuelles
uni-directionnelles
MCE par striction
What is the optimal manual compression rate?A quote from the AHA Guidelines:“There is insufficient evidence from human studies to identify a single optimal chest compression rate. Animal and
human studies support a chest compression rate of >80 compressions per minute to achieve optimal forwardblood flow during CPR.” (IV-25)
• The AHA and ERC set the compression rate for manual chest compressions to 100 cpm in order to compensate for the need to achieve a 50% duty cycle (the percent of time the heart is under active compression versus relaxation).
Why does the AutoPulse® run at 80 compressions/minute? Cardiac Pump Thoracic Pump Compresses mainly the heart Compresses the entire chest
It is all based on optimizing blood flow and being within guidelines. The important overview is that the AutoPulse delivers circumferential chest compressions as opposed to a single point of compression.
• The AutoPulse technique of compressions has shown to improve blood flow with a key element being enough chest relaxation time to enhance venous return.
• Here are the important points on why AutoPulse improves blood flow. The references are listed below. • The AutoPulse compression rate is within the guidelines of 80 – 100 per minute.• The AutoPulse will automatically size the chest and deliver 20% circumferential chest compressions.• Instead of the heart being compressed between the sternum and the spine, the entire chest is compressed.
During thoracic compression the intrathoracic volume is reduced, increasing intrathoracic pressure therefore, compressing the heart, collapsing the thoracic arteries, veins and atria driving blood forward.
• With a duty cycle of 50% and 80 compressions per minute, it allows time for good venous return resulting in improved blood flow.
Important studies that show improved blood flow with AutoPulse are:Halperin HR et al. JACC. 2004;44(11):2214-20 Ikeno F et al. Resuscitation. 2006;68:109-118 Timerman S et al. Resuscitation. 2004;61:273-280
34
Compressions
mécaniques
circonférentielles
Compressions
manuelles
uni-directionnelles
MCE par striction
What is the optimal manual compression rate?A quote from the AHA Guidelines:“There is insufficient evidence from human studies to identify a single optimal chest compression rate. Animal and
human studies support a chest compression rate of >80 compressions per minute to achieve optimal forwardblood flow during CPR.” (IV-25)
• The AHA and ERC set the compression rate for manual chest compressions to 100 cpm in order to compensate for the need to achieve a 50% duty cycle (the percent of time the heart is under active compression versus relaxation).
Why does the AutoPulse® run at 80 compressions/minute? Cardiac Pump Thoracic Pump Compresses mainly the heart Compresses the entire chest
It is all based on optimizing blood flow and being within guidelines. The important overview is that the AutoPulse delivers circumferential chest compressions as opposed to a single point of compression.
• The AutoPulse technique of compressions has shown to improve blood flow with a key element being enough chest relaxation time to enhance venous return.
• Here are the important points on why AutoPulse improves blood flow. The references are listed below. • The AutoPulse compression rate is within the guidelines of 80 – 100 per minute.• The AutoPulse will automatically size the chest and deliver 20% circumferential chest compressions.• Instead of the heart being compressed between the sternum and the spine, the entire chest is compressed.
During thoracic compression the intrathoracic volume is reduced, increasing intrathoracic pressure therefore, compressing the heart, collapsing the thoracic arteries, veins and atria driving blood forward.
• With a duty cycle of 50% and 80 compressions per minute, it allows time for good venous return resulting in improved blood flow.
Important studies that show improved blood flow with AutoPulse are:Halperin HR et al. JACC. 2004;44(11):2214-20 Ikeno F et al. Resuscitation. 2006;68:109-118 Timerman S et al. Resuscitation. 2004;61:273-280
35
Compressions
mécaniques
circonférentielles
Compressions
manuelles
uni-directionnelles
MCE par striction
What is the optimal manual compression rate?A quote from the AHA Guidelines:“There is insufficient evidence from human studies to identify a single optimal chest compression rate. Animal and
human studies support a chest compression rate of >80 compressions per minute to achieve optimal forwardblood flow during CPR.” (IV-25)
• The AHA and ERC set the compression rate for manual chest compressions to 100 cpm in order to compensate for the need to achieve a 50% duty cycle (the percent of time the heart is under active compression versus relaxation).
Why does the AutoPulse® run at 80 compressions/minute? Cardiac Pump Thoracic Pump Compresses mainly the heart Compresses the entire chest
It is all based on optimizing blood flow and being within guidelines. The important overview is that the AutoPulse delivers circumferential chest compressions as opposed to a single point of compression.
• The AutoPulse technique of compressions has shown to improve blood flow with a key element being enough chest relaxation time to enhance venous return.
• Here are the important points on why AutoPulse improves blood flow. The references are listed below. • The AutoPulse compression rate is within the guidelines of 80 – 100 per minute.• The AutoPulse will automatically size the chest and deliver 20% circumferential chest compressions.• Instead of the heart being compressed between the sternum and the spine, the entire chest is compressed.
During thoracic compression the intrathoracic volume is reduced, increasing intrathoracic pressure therefore, compressing the heart, collapsing the thoracic arteries, veins and atria driving blood forward.
• With a duty cycle of 50% and 80 compressions per minute, it allows time for good venous return resulting in improved blood flow.
Important studies that show improved blood flow with AutoPulse are:Halperin HR et al. JACC. 2004;44(11):2214-20 Ikeno F et al. Resuscitation. 2006;68:109-118 Timerman S et al. Resuscitation. 2004;61:273-280
36
Compressions
mécaniques
circonférentielles
Compressions
manuelles
uni-directionnelles
MCE par striction
What is the optimal manual compression rate?A quote from the AHA Guidelines:“There is insufficient evidence from human studies to identify a single optimal chest compression rate. Animal and
human studies support a chest compression rate of >80 compressions per minute to achieve optimal forwardblood flow during CPR.” (IV-25)
• The AHA and ERC set the compression rate for manual chest compressions to 100 cpm in order to compensate for the need to achieve a 50% duty cycle (the percent of time the heart is under active compression versus relaxation).
Why does the AutoPulse® run at 80 compressions/minute? Cardiac Pump Thoracic Pump Compresses mainly the heart Compresses the entire chest
It is all based on optimizing blood flow and being within guidelines. The important overview is that the AutoPulse delivers circumferential chest compressions as opposed to a single point of compression.
• The AutoPulse technique of compressions has shown to improve blood flow with a key element being enough chest relaxation time to enhance venous return.
• Here are the important points on why AutoPulse improves blood flow. The references are listed below. • The AutoPulse compression rate is within the guidelines of 80 – 100 per minute.• The AutoPulse will automatically size the chest and deliver 20% circumferential chest compressions.• Instead of the heart being compressed between the sternum and the spine, the entire chest is compressed.
During thoracic compression the intrathoracic volume is reduced, increasing intrathoracic pressure therefore, compressing the heart, collapsing the thoracic arteries, veins and atria driving blood forward.
• With a duty cycle of 50% and 80 compressions per minute, it allows time for good venous return resulting in improved blood flow.
Important studies that show improved blood flow with AutoPulse are:Halperin HR et al. JACC. 2004;44(11):2214-20 Ikeno F et al. Resuscitation. 2006;68:109-118 Timerman S et al. Resuscitation. 2004;61:273-280
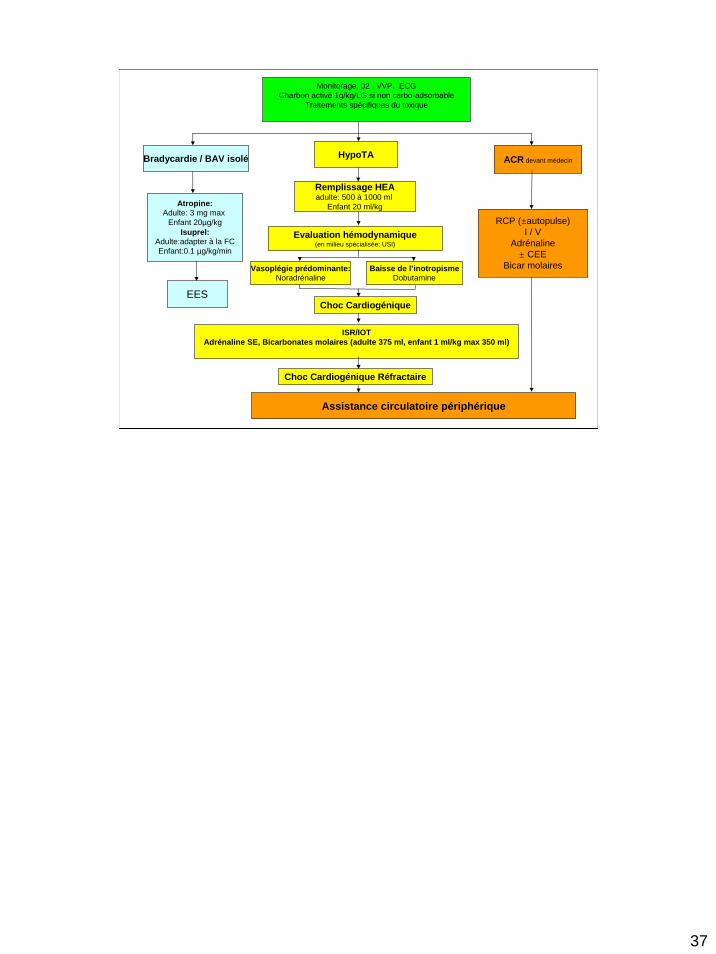
Monitorage, 02 , VVP, ECGCharbon activé 1g/kg/LG si non carbo-adsorbable
Traitements spécifiques du toxique
Bradycardie / BAV isolé HypoTA ACR devant médecin
Atropine:Adulte: 3 mg max
Enfant 20µg/kgIsuprel:
Adulte:adapter à la FCEnfant:0.1 µg/kg/min
EES
Vasoplégie prédominante:Noradrénaline
Baisse de l’inotropismeDobutamine
Remplissage HEAadulte: 500 à 1000 ml
Enfant 20 ml/kg
Assistance circulatoire périphérique
RCP (±autopulse)I / V
Adrénaline± CEE
Bicar molaires
Choc Cardiogénique
Choc Cardiogénique Réfractaire
Evaluation hémodynamique(en milieu spécialisée: USI)
ISR/IOTAdrénaline SE, Bicarbonates molaires (adulte 375 ml, enfant 1 ml/kg max 350 ml)
37

Digitaliques
• Physiopathologie– Inhibition pompe Na+/K+- ATPase membranaire
• Augmentation de l’automaticité des fibres de Purkinje• Baisse de la conduction et de la periode réfractaire des cellules
atriales et ventriculaires• Déplétion potassique intracellulaire
• Délai apparition anomalies cardiovasculaires > 6è
heure après l’ingestion– Anomalies ondes T– Cupule digitalique, raccourcissement QT– Bradycardie sinusale– Troubles de conduction sino auriculaire et auriculo
ventriculaire– Troubles du rythme ventriculaire
38
39
Antidotes
Quantité de digitalique à neutraliser = quantité supposée ingérée en mg x 0,6
1 flacon de Digidot® neutralise 1 mg de digoxine1 flacon de Digibind® neutralise 0,5 mg de digoxine
• neutralisation prophylactique ou semi molaire
•Devant 3 facteurs :• Sexe masculin• Antécédents cardio vasculaires• BAV >1 er degré ou bradycardie < 50 résistante àl’atropine• K+ > 4,5 mmol/l
• neutralisation curative ou équimolaire• devant un seul facteur
• Arythmies ventriculaires (TV, FV)
• Bradycardie résistante àl’atropine:
• K+ > 5 mmol/l• Infarctus mésentérique• Choc cardiogénique
Bradycardie résistante à l’atropine: < 75 bpm avant 1 an; < 60 bpm avant 6 ans; < 40 bpm après 6 ans
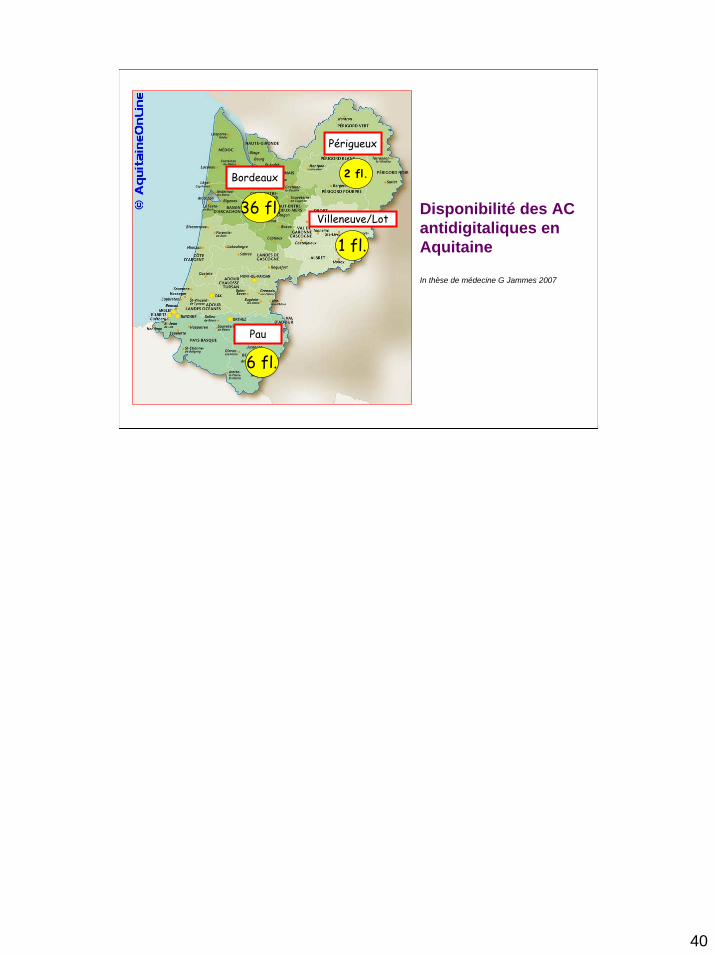
Pau
Bordeaux
Périgueux
Villeneuve/Lot
2 fl.
36 fl.
1 fl.
6 fl.
Disponibilité des AC antidigitaliques en Aquitaine
In thèse de médecine G Jammes 2007
40
41
• Coma calme hypotonique :Parfois: coma hypertonique (10%), mydriase, syndrome pyramidal
• Collapsus dose-dépendant à QRS fins :- hypovolémique- vasoplégique- cardiogénique
•Traitement :- Décontamination digestive par charbon activé- Remplissage modéré- Catécholamines: dobutamine voire adrénaline - Hémodialyse - Assistance circulatoire (exceptionnelle)
Intoxication aux carbamates
Conclusion
• Intoxications rares mais graves• Augmentation incidence prévisible• Procédures de prise en charge et d’orientation
- Information- Concertation- Travail en réseau
Série Bordelaise: 7 patients, 6 ECLS, 4 récupération ad integretum, 2 décès (une patiente en mort cérébrale, avait fait ACR avant arrivée des secours, l’autre en défaillance multiviscérale MCE automatisé > 1h)
42