Embed Size (px)
Citation preview
1
C H R O N I C S T R E S S A M O N G A D O L E S C E N T S C O N T R I B U T I N G F A C T O R S A N D C O N S E Q U E N C E S O N A C A D E M I C A C H I E V E M E N T .
Karin Schraml
2
Chronic stress among adolescents Contributing factors and consequences on academic achievement
Karin Schraml

3
Abstract
Recent nationwide surveys indicate that there have been dramatic increases in reports of stress and serious stress-related health problems among Swedish adolescents. By means of three empirical studies, the general aim of the present thesis was to investigate the prevalence of perceived chronic stress among sixteen year old high school students, to examine if factors that have been found to be relevant in the development of chronic stress among adults my as well contribute to chronic stress among adolescents and to investigate the impact of chronic stress and sleep-related variables on adolescents’ academic achievement. Data on severe stress symptoms and stress-related factors were collected among sixteen year old high school students from three different high schools in the Stockholm area. The main findings indicated that serious stress symptoms were reported by more than 30% of the investigated high school students. Moreover, 15% reported severe stress symptoms throughout high school and were thus considered to suffer from chronic stress. More girls then boys reported to suffer from stress symptoms. Perceived high demands, low global self-esteem, sleep disturbances, low social support and negligent eating habits explained 56,3% of the variance in stress symptoms. Another main finding showed that perceived chronic stress can have more immediate consequences on adolescents in addition to potential negative long-term health implications, in terms of a negative impact on adolescents’ academic achievement. Moreover, a closer look was taken on the potential contribution of sleep–related variables on academic achievement and found that beside chronic stress and other variables, also a fairly new concept, namely social jetlag was involved in predicting variation in academic achievement. Taken together, the current thesis summarized these results and discussed their impact on future research. Taken together, this thesis has put forward data that indicate a high prevalence of chronic stress among adolescents. The results should be taken seriously, as young people’s sense of wellbeing during this period impacts not only their successful transition into adulthood but also their life course and adult options. Therefore, to provide adolescents with the optimal preconditions for their future life and to maintain their health and wellbeing in the long run, by preventing them from chronic stress is and, in fact, must be of great public concern. Based on the present findings future research options and practical implications in terms of chronic stress prevention measures were suggested and discussed.

4
Acknowledgements
àWorkinprogress
5
List of Studies
This thesis is based on the following studies:
I. Schraml, K., Perski, A., Grossi, G., & Simonsson-Sarnecki, M. (2011). Stress symptoms among adolescents: The role of subjective psychosocial conditions, lifestyle, and self-esteem. Journal of Adolescence, 34, 987-996.
II. Schraml, K., Perski, A., Grossi, G., & Makower, I. (2012). Chronic stress and its
consequences on subsequent academic achievement among adolescents. Journal of Educational and Developmental Psychology, 2 (1), 69-79.
III. Schraml, K., Schwarz, J., & Perski, A. (submitted). The impact of social jetlag and stress
on academic achievement among adolescents.
6
Contents
Introduction .............................................................................................................................................................. 7 Stress theory ..................................................................................................................................................................................... 12
Stress – a physiological reaction ................................................................................................................................................ 12 Psychological stress ................................................................................................................................................................... 12 Chronic stress and burnout ......................................................................................................................................................... 13
Chronic stress among adolescents .................................................................................................................................................... 14 Factors that may contribute to chronic stress among adolescents .............................................................................................. 15 Chronic stress, sleep, and academic achievement ...................................................................................................................... 20
Methods .................................................................................................................................................................. 23 Participants and procedure ............................................................................................................................................................... 23 Measures ........................................................................................................................................................................................... 23 Statistical analyses ............................................................................................................................................................................ 25
Summary of Studies ............................................................................................................................................... 27 Study I - Stress symptoms among adolescents: The role of subjective psychosocial conditions, lifestyle, and self-esteem .......... 27
Background and aim ................................................................................................................................................................... 27 Method ....................................................................................................................................................................................... 27 Main findings and conclusions ................................................................................................................................................... 27
Study II - Chronic stress and its consequences on subsequent academic achievement among adolescents .................................... 30 Background and aim ................................................................................................................................................................... 30 Method ....................................................................................................................................................................................... 30 Main findings and conclusions ................................................................................................................................................... 30
Study III – The impact of stress and social jetlag on academic achievement among adolescents ................................................... 32 Background and aim ................................................................................................................................................................... 32 Method ....................................................................................................................................................................................... 32 Main findings and conclusions ................................................................................................................................................... 33
Discussion .............................................................................................................................................................. 35 Summary of the findings .................................................................................................................................................................. 35 Adolescence - a period of “storm and chronic stress”? ................................................................................................................... 36
Factors that play a crucial role in chronic stress among adolescents ......................................................................................... 36 Impact of chronic stress and sleep on academic achievement ................................................................................................... 40 Gender differences ..................................................................................................................................................................... 42
Limitations and methodological considerations ............................................................................................................................... 42
Concluding remarks ............................................................................................................................................... 49
References .............................................................................................................................................................. 50
7
Abbreviations
ACT Acceptance and commitment therapy ANOVA Analysis of variance CBT Cognitive behavioral therapy GAS General adaptation syndrome HPA Hypothalamic–pituitary–adrenocortical KSQ Karolinska sleep questionnaire PBS Performance-based self-esteem scale RSE Rosenberg self-esteem scale SAM Sympathetic adrenal medullary SMBQ Shirom-Melamed Burnout Questionnaire SPSS Statistical Package for Social Sciences
8
Introduction
“While all life requires stresses and strains in the everyday give-and-take of demands, chronic stress is a state of persistent excess of demands over resources. To struggle, to achieve and to strive are admirable and essential characteristics. Yet, without moderation the struggling goes awry, rendering the body and mind susceptible to health and disease problems.” (Thoreson & Eagleston, 1983, p. 54).
In modern Western society, chronic stress is a major public health problem (Levi, 2005; Perski, 2006; Shirom, 2003) because it increases the risk for stress-related health implications and diseases. In Sweden, stress-related health problems, such as clinical burnout, are among the most common diagnoses for long-term sick leave among the adult working population, leading to high costs for society as well as individual suffering (Lidwall, 2010; Socialstyrelsen, 2003). It is not only adults who suffer from prolonged stress, as stress-related and mental health problems are becoming more common among younger people. Recent nationwide surveys indicate that there have been dramatic increases in reports of stress and serious stress-related health problems among Swedish adolescents (Ahrén, 2010; Bremberg, 2006; Hagquist, 2010; Socialstyrelsen, 2009). Over the past 20 years, the number of 16-year-olds reporting stress, fatigue, and psychosomatic complaints as well as psychological and physical tension has been steadily rising (Bremberg, 2006; Hjern, Alfven, & Östberg, 2007; Östberg, 2001; Socialstyrelsen, 2009), indicating an increasing prevalence of chronic stress among younger age groups. Adolescence is a stressful period in life, involving a high number of physiological, social, and psychological changes. During these years the choices that are made and the behaviors that emerge have the potential to influence the rest of one’s life (Eccles, Brown, & Templeton, 2008; Mortimer, Zimmer-Gembeck, Holmes, & Shanahan, 2002). Young people’s sense of wellbeing during this period impacts not only their successful transition into adulthood but also their life course and adult options. Therefore, to provide adolescents with the optimal preconditions for their future life and to maintain their health and wellbeing in the long run, by preventing them from chronic stress is and, in fact, must be of great public concern (KVH, 2010; SBU, 2010). In order to do this an increased understanding of chronic stress among adolescents is called for. Adolescent wellbeing and health is dependent on a variety of factors, including individual (physiological, psychological, and social factors), contextual (e.g., socioeconomic status, school context, and family structure), and societal factors (e.g., labor market conditions and societal values). However, since many of these factors were beyond the scope of what is feasible for an exhaustive investigation of a broad and complex research topic such as chronic stress in a heterogeneous and complex population, like adolescents, the present thesis was limited to the following aims.
9
Aims of the thesis The general aims of the present thesis were to investigate the prevalence of chronic stress among adolescents, to examine if factors that have been found to be relevant in the development of chronic stress among adults also contribute to chronic stress among adolescents, and to investigate the consequences of chronic stress and sleep-related variables on adolescents’ academic achievement.
The specific aims of the present thesis, which were covered by three empirical studies, were
I. to investigate the prevalence of severe stress symptoms among adolescents, to better understand the factors that may contribute to or exacerbate stress symptoms in adolescents and to examine possible gender differences.
II. to examine the impact of chronic stress on adolescents’ academic achievement. III. to investigate whether variability in academic achievement among high school students can
be explained by chronic stress as well as whether a number of sleep-related variables also influence adolescents’ academic performance.

10
Theoretical framework
The subsequent section provides a theoretical background to the empirical studies, which this thesis is based upon. To begin with adolescents, who are the target group of this thesis, and the challenges they face are described. Thereafter, a short introduction to the concept of stress and chronic stress is made, followed by a description of burnout, which is one possible health consequence of chronic stress. Next, the literature on different factors that have previously been related to stress are introduced. Finally, a discourse on the research on chronic stress, sleep, and academic achievement is provided.
The “storm and stress” of adolescence The study of adolescence from a scientific point of view started in the 20th century. Adolescence (Latin: adolescere: to grow up, to nourish) refers to a transitional stage of physical and psychological development, the individual’s transition from childhood to adulthood (Arnett, 1999, 2000). Adolescence has been described as a period of “storm and stress” (Hall, 1904) when various types of problems are more common to arise than in other life periods. At the root of the disturbance is an enormous number of major changes and challenges that normally occur as one emerges into adulthood (Eccles et al. 2008; Frydenberg, 2002; Nounopoulos, Ashby, & Gilman, 2006; Seiffge-Krenke, 2000). The changes include physiological changes that are connected with the onset of puberty and physical growth, affecting sex organs, bodily dimensions in terms of height and weight, and brain structure. Psychological changes also take place, which concern cognitive advances in abstract thinking and reasoning capabilities. Personality and identity development is another key aspect of adolescence, as existential thoughts and questions of personal values, commitments and expectations begin to receive more attention and the desire for autonomy and independence becomes more central. Also, social and contextual changes are happening which affect, for example, the parent–child relationship, the importance of the peer group, intimate relationships, and school transitions. All of these inevitable changes and challenges imply a varying amount of stress in every young person’s life (Eccles, et al., 2008; Frydenberg, 2002). Other potential stress sources concern the school context, where adolescents usually spend most of their time (Modin & Östberg, 2009; Modin, Östberg, Toivanen, & Sundell, 2011; Salmela-Aro, Kiuru, Pietikäinen, & Jokela, 2008). Additionally, adolescents may have to deal with accumulated stress from increased academic pressure, economic constraints, interpersonal conflicts with peers or parents or from unforeseen major life events that could affect anyone at any time, such as divorcing parents, severe illness, or the death of a significant other. Moreover, there are a number of more general potential stressors which are characteristic of modern Western societies, such as high degree of individualization, which provides personal freedom but also increased uncertainty. Also high youth unemployment and job insecurity are prevalent stressors in today’s society. Moreover, technological advances such as global communication and
11
instantaneous access to information and social media provide both advantages but may also be sources for stress (Bremberg, 2006; Eccles et al., 2008; Wiklund, Bengs, Malmgren-Olsson, & Öhman, 2010). Although the transition from childhood to adulthood basically demands the same from young people today as it did twenty years ago, in Sweden, several investigations and surveys have pointed to an increase in stress and mental health problems among adolescents over these years (Ahrén, 2010; Bremberg, 2006; Socialstyrelsen, 2009). Mental health problems refer to depressive symptoms, sleeping difficulties, worries, and psychosomatic symptoms. Based on a review of several studies, Bremberg (2006) found that worry and anxiety, sleep disturbances, tiredness, and tension and pain were increasing among 16 to 24 year olds. It has also been found that the increase in psychological problems and stress-related disorders is more common among girls than boys (Ahrén, 2010; Bremberg, 2006; Haquist, 2009). In an investigation among 10 and 18 year olds, 42% reported that they felt stressed at least once a week and 21 % reported that they felt stressed several times per week; in addition, every third adolescent reported suffering from psychosomatic problems such as headaches, stomach aches, and problems falling asleep (Östberg, 2001). A more recent internet-based investigation on adolescent psychosomatic health revealed that a high percentage of participants felt stressed very often or often (47% among girls and 29% among boys) (Friberg, Hagquist, & Osika, 2012). It also showed that psychosomatic health was deteriorating among the participants (between 2007 and 2010) and that older adolescent girls reported psychosomatic symptoms to a high degree. Skolverket’s (2010), the Swedish National Agency for Education, longitudinal survey on school children’s attitudes towards school showed that, in 1997, 25% of high school students reported that they often or constantly felt stressed, reaching a peak of 41% in 2000 and finally leveling out at 36% in 2009. In 2009, every other girl and every fifth boy reported feeling stressed in school. In an investigation among 15 year olds, it was observed that the number of adolescent girls to report perceiving at least two disturbing psychosomatic or psychological symptoms per week had increased from 30% to 50% between 1985 and 2001, where it remained since then. The measurement among boys went from 15% to 30% over this period. When asked about their self-rated health, in 2009, only 28% of the girls reported perceiving that their health was good as compared to 49% of the boys (SFI, 2011). Furthermore, the number of young people to complain of daytime fatigue and sleep disturbances has increased dramatically in the past decade, with the prevalence of sleeping problems reaching the same level as for adults in 2009, between 20% and 25% (Socialstyrelsen, 2009). According to the “Survey of living conditions among children,” a national longitudinal survey conducted among Swedish children and adolescents every other year, the percentage of girls with sleeping problems rose from 9% to 13% between 1980 and 1997, and suddenly increased to 27% in 2003. For boys a similar development took place, going from 6% in 1980 to 12% in 1997, and finally to 19% in 2003 (Bremberg, 2006 in reference to SCB). As a consequence of these developments, there has been an increase in the number of young people who are hospitalized for mental health problems (Ahrén, 2010; Socialstyrelsen, 2009). In fact, in 2006 adolescents and young adults constituted the largest group of psychiatric patients in Stockholm (Dalman, & Wicks, 2006). The high proportion of young individuals suffering from stress and stress-

12
related health problems has to be taken seriously, as it is likely to be indicative of something far more serious than could be attributed to the “normal” storm-and-stress period during adolescence.
Stress theory Beginning in the early 1920’s, stress research has a short history. It is and may always be a complex and difficult concept to define. Depending on the research approach, stress can refer to the direct influence of harmful stimuli, physical strain, subjectively perceived threats, physiological reactions or psychological states. Common to all definitions of stress, however, is that it represents an imbalance that is rooted in the need of the individual to adapt to environmental changes and demands (Butler, 1993).
Stress – a physiological reaction Hans Selye was the first to speak of stress as a non-specific physical response to any demand for change (Selye, 1936). Selye had observed that certain physical and emotional stimuli (stressors) resulted in physiological responses that were intended to restore a physical balance, known as homeostasis. Based on this observation, he formulated a model of the general adaptation syndrome (GAS), which consists of three phases. In a first immediate reaction (the alarm stage), when confronted with a stressor, the body mobilizes energy and resources to respond to the stressor. The second stage is the resistance stage, where the increased arousal is maintained and followed by adaptation to the stressor. However, if the stress does not abate, the body’s resources and energy deplete, leading to the exhaustion stage in which the risk for negative health outcomes increases. (Selye, 1936, 1978). The body’s constant striving to maintain homeostasis is a process called allostasis (McEwen, 2006; Sterling & Eyer, 1988). If stressors challenge homeostasis, the organism reacts with a so-called allostatic response. The allostatic, or physical stress response, is characterized by the activation of two bodily systems. Acute stress activates the sympathetic adrenal medullary (SAM) system, which aims to prepare the body for dealing with a threat through what Cannon (1922) coined as the “fight-or-flight” response. Hereby, cardiovascular activity and the secretion of epinephrine and norepinephrine are stimulated (Folkow, 1997; Lundberg 2005). The reaction is immediate, short lived, and adaptive in order to re-establish homeostasis. Parallel to this, the hypothalamic–pituitary–adrenocortical (HPA) system also becomes activated, which stimulates the release of cortisol from the adrenal cortex. Cortisol increases gradually after stimulation of the HPA-axis, indicating that the reaction is less immediate. Moreover, the activation of the HPA-axis is associated with more affective stress and the long-term adaption of an organism to stress (Sapolsky, Romero, & Munck, 2000). The physiological reaction described above is similar for all mammals when they are facing an immediate physiological threat that could cost them their life if they do not react by either fighting or fleeing (Sapolsky, 2004).
Psychological stress In humans, psychological states also have a role in activating the physiological stress reaction. An individual’s evaluation of a situation as stressful or not affects whether a situation is evoking stress or not.

13
According to the transactional model, stress is a dynamic process involving an interaction between the individual and the environment (Lazarus, 1993, 1999; Lazarus & Folkman, 1984). The process whereby individuals appraise their situation is therefore central. It begins with a primary appraisal where the relevance of the situation for one’s wellbeing is evaluated in terms of the potential threat or challenge that is posed. It is not only negative events but also positive events that can set this process in motion, as both may involve the need to adapt to changing or new circumstances and therefore evoke stress. This is followed by secondary appraisal, another cognitive process, where the internal and external resources for handling the situation are evaluated (Lazarus, 1993; Lazarus & Folkman, 1984). Thus, stress is occurring when there is an imbalance in terms of the actual and/or perceived resources not being adequate to counter actual and/or perceived demands (Butler, 1993; Lazarus & Folkman, 1984). Coping is defined as an individual’s behavioral or cognitive efforts to handle stress-evoking internal and external demands (Lazarus & Folkman, 1984). Usually a distinction is made between active, problem-focused coping, which aims at addressing the sources of stress, and passive, avoidant or emotion-focused coping, which aims at regulating distressing emotions. The effectiveness and adaptability of each type depends on the nature of the stressor (Butler, 1993; Lazarus & Folkman, 1984). Taken together, the research and theory suggests that there is a constant interplay between physiological, psychological, and environmental factors that influences whether stress is elicited or not, which (if any) stress symptoms are evoked, and how the individual reacts to stress. It is this complex interplay of multiple factors, along with the variation between individuals that makes it difficult to definitively explain the causes and effects of stress processes. It is, however, well understood that prolonged stress and strain, also called chronic stress, eventually has a negative impact on health and may cause serious mental and physical diseases (Perski, 2006; Theorell, 2004).
Chronic stress and burnout The allostatic response is an important physical reaction that protects the body from external and internal stress. It usually decreases together with decreasing stress, but if the imbalance between spending and regaining energy persists over a long period of time, allostatic load may result (McEwen, 2006; McEwen & Stellar, 1993). More specifically, it results from a lack of energy regeneration which occurs when too few essential anabolic processes are taking place. Allostatic load is often described as the wear and tear on the body that results from chronic overactivity of the allostatic system. This kind of prolonged stress is then referred to as chronic stress, which is associated with severe stress symptoms such as somatic symptoms, emotional and physical exhaustion, and sleep and cognitive difficulties. Chronic stress and its associated symptoms eventually lead to a depletion of the body’s energy. The degree to which this occurs has been associated with a stage of exhaustion that carries with it an increased susceptibility to negative health outcomes, such as a heightened risk for cardiovascular morbidity, diabetes, immunosuppression, and affective disorders (Sapolsky, 2004). Not least of all, one of these possible negative health outcomes is burnout. The term burnout has been used in different ways in different contexts. Freudenberger (1974) was the first to describe burnout from a clinical perspective, describing it in terms of physical and emotional symptoms. Burnout has also been defined as a work-related multidimensional syndrome, most notably

14
by Maslach and her colleagues (Maslach 2001; Maslach & Jackson, 1981; Maslach & Leiter, 1997). From this perspective, burnout refers to a psychological condition in which a sequential progression of emotional exhaustion, depersonalization, and reduced personal accomplishment is experienced in relation to an occupational setting (Maslach, Schaufeli & Leiter, 2001). Coming from another perspective, Pines and her research associates have extended the definition of burnout to potentially apply to situations beyond the occupational setting that are emotionally demanding, where an individual’s sense of importance and influence are strained, and decreases in self-esteem can eventually result (Pines & Aronson, 1988; Pines & Keinan, 2005). According to Hallsten, Josephson, and Torgén’s (2005) burnout theory, performance-based self-esteem contributes to the process of burning out. Cherniss (1980), who conceives of burnout as entailing further consequences, describes it as a process that starts with a perceived imbalance between demands and resources, followed by a lack of adequate coping strategies, and then an experiencing of disturbing symptoms such as tension, anxiety, and exhaustion, which finally leads to negative changes in attitude and behavior. In the context of this thesis, the term burnout refers to the definition of Melamed, Kushnir, and Shirom (1992). They conceptualize burnout as an individual’s negative affective response to chronic stress, a response that comprises experiencing severe stress symptoms in three areas: emotional exhaustion, physical exhaustion, and cognitive difficulties (Melamed et al. 1992; Melamed, Shirom, Toker, Berliner & Shapira 2006; Shirom, 2003). Emotional exhaustion refers to experiencing a lack of energy in relation to social interaction, while physical exhaustion manifests itself in tension and an inability to accomplish everyday tasks. Cognitive difficulties are characterized by decelerated cognitive processes, impaired memory and concentration problems. In this definition of burnout, the individual’s initial unsuccessful attempts to cope with stress, and successive increasing efforts to protect resources, gradually lead to more and more stress symptoms, including physical exhaustion, concentration problems, listlessness, and tension. According to Shirom (2003), the core feature of burnout is “the gradual depletion over time of individuals’ intrinsic energetic resources” (p. 245), due to long-term stress exposure. The prevalence of severe stress symptoms can be measured by means of the Shirom-Melamed Burnout Questionnaire (Lundgren-Nilsson, Jonsdottir, Pallant, & Ahlborg, 2012; Melamed et al., 1992).
This last definition of burnout fits with the diagnostic criteria of exhaustion syndrome, also called clinical burnout, which, in Sweden was described as a stress related disease in 2003, and in 2005 was added to the ICD-10 (code F43.8) as an established medical diagnosis (ICD-10, code F43.8) (Schaufeli, Leiter & Maslach, 2009; Socialstyrelsen 2003). The criteria include difficulties concentrating, reduced ability to cope with stress, emotional distress, and sleep disturbance as well as somatic symptoms, such as muscle pain, palpitations or dizziness, which cause significant clinical suffering for the individual (Armon, Shirom, Shapira, & Melamed, 2008; Jonsdottir et al., 2012; Schaufeli et al., 2009; Socialstyrelsen, 2003). As exhaustion syndrome is considered to be the result of complete energy erosion, recovery only comes slowly even after the energy draining stress source has disappeared. It is among the most common diagnoses for long-term sick leave among the Swedish adult working population (Lidwall, 2010; Socialstyrelsen, 2003). It is a serious disease that carries with it individual suffering and societal costs.
Chronic stress among adolescents As mentioned above, besides causing individual suffering, chronic stress increases the risk for stress-related ill-health in the long run (Theorell, 2004). There may be a substantial risk that today’s

15
adolescents who experience serious stress-related symptoms over a prolonged time will become tomorrow’s adult patients at stress clinics (Perski, 2006). In order to prevent adolescents from ill-health due to chronic stress, it is important to increase our understanding of chronic stress and the factors that may elicit chronic stress among adolescents. In the present thesis, the contribution of factors that have been found to be relevant in the experiencing of chronic stress among adults are examined in more detail, namely, subjective psychosocial conditions, self-esteem, lifestyle routines, and sleep (Perski, 2006). Since stress-related health problems emerge over an extended period of time, a fully developed exhaustion syndrome might not be expected to be prevalent among younger populations (Thoreson & Eagelston, 1983). Therefore, an investigation of the more immediate impact of chronic stress on another relevant life domain, academic achievement, was of interest in the present thesis.
Factors that may contribute to chronic stress among adolescents
Psychosocial conditions – demands, control, and social support The job demand-control-support model, which is derived from research among the adult working population, can and has been applied to adolescents, who “work” in schools (Gillander-Gådin & Hammarström, 2000; Modin et al., 2011). According to the model, perceived high work demands and low influence (control; decision latitude) over one’s work situation are positively associated with elevated levels of stress (Karasek & Theorell, 1990; Theorell, 1996) and chronic stress (Lindblom, Linton, Fedeli & Bryngelsson, 2006). It also poses that a higher risk of psychological strain and physical illness is to be expected among individuals who face high demands but who perceive having little control or social support for handling these demands (Karasek & Theorell, 1990; Kivimäki & Kalimo, 1996; Theorell, 1996). The demands that school places on students are comparable to those faced by working adults (e.g., with regard to high workload, deadlines, and performance) (Gillander-Gådin & Hammarström, 2000; Modin et al., 2011). According to the latest results of the “Survey of living conditions among children,” the perceived demands of adolescents were most often connected to school-related work, such as tests and homework (SCB, 2007; 2012). In fact, 60% of high school students reported feeling stressed over school-related tasks and academic demands (50% among boys and 71% among girls). Furthermore, 55% reported that they felt stressed over the high demands they placed on themselves (68% among girls and 42% among boys). 15% felt stress over their parents’ demands and 32% felt stress over their teacher’s demands and expectations (SCB, 2012), which is in line with the findings of Huan, Lay-See, Ang and Wan-Har (2008), who showed that high school students’ academic stress is not only related to the demands they put on themselves, but also to external demands from their parents. It has also been found that students who rated school-related demands as one of their main sources of stress were more likely to worry about their studies and felt overwhelmed by their workload (Huan et al., 2008). Ollfors and Andersson’s (2007) study among Swedish youths showed that the combination of greater commitment to school work and perceiving that demands on school performance were high was associated with greater stress. Worries over school achievement and feeling that schoolwork is too demanding as well as the pressure to achieve good grades were shown to be particularly associated with psychosomatic symptoms (Murberg & Bru, 2004).

16
Concerning perceived control, Modin et al. (2011) found that high levels of control could mitigate the negative impact of high levels of perceived school-related demands on subjective health among fifteen-year-old adolescents. Based on the results of interview studies, Bremberg (2006) concluded that adolescents associated stress mainly with high academic demands and lack of control over school-related work, in the form of, for example, unclear instructions and multiple tasks. The interviewed students mentioned that high workloads forced them to frequently skip regenerative or social activities. While some studies indicate that there are no differences between girls and boys when it comes to the degree of stress they perceive over school-related demands (deAnda et al., 2000; Seiffge-Krenke, Aunola, & Nurmi, 2009), others point out that females report experiencing significantly more stress symptoms due to school-related worry than males (Murberg & Bru, 2004). According to Dedovic, Wadiwalla, Engert and Pruessner (2009), females were found to perceive less control than males, which they pose are due to differences in socialization processes. According to these researchers, compared to boys, girls are more closely supervised and are not granted as much autonomy from adults and thus have fewer opportunities of exerting influence. As the experiencing of high demands increases during adolescence, social support and interpersonal relationships tend to deteriorate. Murberg and Bru (2004) emphasize the fact that school is the primary social meeting place for adolescents and where the number and quality of interactions with peers having a crucial impact on their wellbeing. Supportive relationships are considered to be a buffer against stress (Haraldsson, 2010; Langstedt, Asplund, & Gillander-Gådin, 2009; Rudolph, 2002). Moreover, since social relationships in general can be a cause of conflicts, they constitute a potential source of increased stress symptoms, especially among adolescent girls (Byrne, Davenport, & Mazanov 2007; Rudolph, 2002). Brolin-Låftman and Östberg (2006) found that strained relationships with both parents and peers had a stronger impact on health among adolescents than did supportive relationships. Also, perceived lack of social support and perceived social isolation have been associated with an increased risk for stress and affective problems (Brolin-Låftman & Östberg, 2006; Hankin, Mermelstein, & Roesch 2007). With increasing age, adolescents tend to more often turn to their friends rather than to their parents for social support (Aldwin, 2007). Especially for girls, supportive peer relationships have been shown to be important (Langstedt et al., 2009; SCB, 2011). Females have been found to be exposed to higher levels of interpersonal stress than the males and to react more negatively when experiencing social stressors (Murberg & Bru, 2004; Rudolph, 2002; Stroud, Salovey, & Epel, 2002). Girls rather than boys tend to blame themselves for problems in relationships. Moreover, girls are usually more occupied with worries and concerns about others. In sum, recent research indicates that perceived demands as well as resources such as perceived control and social support play an important role in the experiencing of stress. However, it is not only the perception of the psychosocial conditions that is associated with stress but also the perception of one’s self.
Self-esteem Disturbances in self-esteem are believed to essentially contribute to the high prevalence of stress and stress-related health complaints (Birndorf, Ryan, Auinger, & Aten, 2005; Rhee, Holditch-Davis, & Miles, 2005; Stinson et al., 2008). Even though there are several different theories about self-esteem, all of them are based on the concept that self-esteem corresponds with an individual’s perception of her own value. The conception of self-
17
esteem that is used in the present thesis is referred to as global self-esteem, which is defined as one’s overall positive or negative attitude towards the self (Pyszczynski, Greenberg, Solomon, Arndt, & Schimel, 2004; Rosenberg, 1972; Tarafodi & Swann, 1995). High global self-esteem has been found to be related to positive self-evaluations, characterized by having an accepting attitude towards one’s self. In contrast, low global self-esteem has been found to be associated with negative self-evaluations, characterized by self-doubts and self-rejection (Baumeister, Campbell, Krueger, & Vohs, 2003). It has been proposed that every person acts according to a universal human need to protect their feelings of being valuable and increase their sense of worth (Pyszczynski et al. 2004; Rosenberg, Schooler & Schoenbach, 1989; Schütz, 2003). Self-esteem is a central aspect of humans’ self-understanding and it is essential for their psychological wellbeing and functioning. During adolescence, however, it dips (Moksnes, Moljord, Espnes, & Byrne, 2010; Robins & Trzesniewski, 2005). Adolescent decline in self-esteem is thought to be due to an increase in self-consciousness and in the ability to think abstractly about one’s self (Moksnes et al., 2010). Leaving behind the childlike, unrealistically positive self-view, external feedback and social comparison are brought into the equation when adolescents evaluate their self-worth. Many of the changes that come along with adolescence (related to puberty, body image, academically more challenging environments, and more complex social and intimate relationships) pose further challenges to self-esteem (Robins & Trzesniewski, 2005). High global self-esteem has been identified as a crucial factor in preventing stress and mental health problems such as depression (Avison & McAlpine, 1992; Major, Barr, Zubek, & Babey, 1999; Rector & Roger, 1997), while low global self-esteem has been shown to predict stress symptoms and ill-health (Birndorf et al., 2005; Kernis, 2006; Kivimäki & Kalimo, 1996). In a prospective study among young adults, high self-esteem was shown to be a buffer against emotional exhaustion and was positively associated with personal accomplishments ten years later (Salmela-Aro & Nurmi, 2007). The cognitive and affective reactions of individuals with high and low self-esteem have been found to differ from each other, even when they face the same situation (Campbell & Lavallee, 1993). Studies suggest that high self-esteem may foster the individual’s self-efficacy, which is the belief in one’s abilities and competence to handle stressful situations (Bandura, 1997, 2000; Dumont & Provost, 1998). Other characteristics of those with high self-esteem, according to Locke, McClear, and Knight, (1996), is that they tend to appraise stressful events as challenges rather than threats and experience less fear of failure. It is therefore perhaps not surprising that individuals with high self-esteem have also been found to use more adequate coping strategies (Moksnes et al., 2010). In contrast, Chapman and Mullis (1999) observed that adolescents with low self-esteem tended to ventilate their feelings and avoid problems rather than directly dealing with difficult, stressful situations, thus they tended to utilize emotional, avoidant coping strategies rather than active problem-solving strategies. Individuals low on self-esteem are more insecure about themselves and thus their self-beliefs fluctuate over time and depend on the circumstances, which tends to make them more sensitive and reactive to their social environment. Their self-view and their mood are highly dependent on external feedback. Both the negative and the positive feedback they encounter are crucial to shaping how they feel about themselves (Campbell & Lavallee, 1993). High self-esteem individuals, on the other hand, are less disturbed when facing a particular stressful situation because they hold a consistent self-view which does not get disrupted so easily by changing circumstances (Spencer, Josephs & Steele, 1993).
18
In their meta-analysis on self-esteem among adolescent girls and boys, Kling, Shibley-Hyde, Showers, and Buswell (1999) revealed that, even though the overall differences were small, boys scored higher on global self-esteem than girls, with the largest effect emerging in late adolescence. In a study by Harter (1993), it was found that girls’ global self-esteem in general was lower than that of the boys. Global self-esteem has to be distinguished from lower order factors that represent contingent aspects of self-evaluation, also called domain-specific self-esteem (Crocker, 2002; Crocker & Wolfe, 2001; Kling et al., 1999; Major et al., 1999), where the target of the evaluation is not the self as a whole but a specific domain of the self. Harter’s (1993) research among adolescents also highlights a contingent component of self-esteem, indicating that perceived competence in domains which the individual perceives as important as well as the approval by significant others are essential determinants of adolescents’ self-esteem. According to Harter (1993), low self-esteem individuals usually get insufficient or only contingent social approval, which depends on the fulfillment of external expectations. One example of contingent self-esteem, which has been shown to play a crucial role in the development of chronic stress by increasing the risk of psychological and physiological exhaustion, is performance-based self-esteem (Blom, 2012; Hallsten, Bellaagh & Gustafsson, 2002; Hallsten et al., 2005; Hallsten, Voss, Stark, Josephson, & Vingård, 2011; Perski, 2006). According to Hallsten et al. (2005), performance-based self-esteem relies on the belief that one’s self-worth equals one’s performance and is a prerequisite for burnout. Typically, individuals with high performance-based self-esteem have a strong need to prove their competence and to exert maximum effort in order to feel worthy. Since failures and setbacks are particularly detrimental to the self-esteem of these individuals, they put a great amount of effort into performing well and succeeding (Hallsten et al., 2005). Stress then develops as a result of one’s self-worth being threatened by the risk of not succeeding since failure would be tantamount to not being good enough. Consequently, deriving one’s self-esteem from external sources, such as performance outcomes and recognized success, means not only that it is vulnerable, but also that the individual is exposed to a higher risk for negative health outcomes (Blom, 2011; Johnson, 1997; Johnson & Forsman, 1995). Performance-based self-esteem has been found to be more prevalent among women (Blom, 2012; Hallsten, et al., 2005). Also, in an interview study among adolescent girls, it was observed that they perceived their value as a person to be highly related to their accomplishments (Wiklund et al., 2010). Ruble, Greulich, Pomerantz, and Gochberg (1993) showed that women tend to be more concerned about future success and that they show more maladaptive attributions for success and failure, which prevents them from feeling content with themselves and their performance. It is therefore plausible that their greater concern with success may increase the impact of performance-based self-esteem. In conclusion, self-esteem, the overall attitude that individuals have towards their selves, influences their appraisals of situations, the actions they take, and, consequently, their experiencing of stress. The next section focuses on the things people actually do on a daily basis, because, according to research on lifestyle habits, also behavioral routines have been shown to be associated with stress, wellbeing and health.
19
Lifestyle factors Lifestyle factors, such as eating habits and physical exercise, often take root in adolescence and are difficult to change later in life. While a healthy lifestyle can help prevent physical stress reactions, an unhealthy lifestyle has been associated with greater susceptibility to stress and other negative health outcomes (Lien, 2006; Sundblad, Jansson, Saartok, Renström, & Engström, 2008; Wiles et al., 2008). Breakfast skipping, for example, has been associated with other health compromising behaviors (Keski-Rahkonen, Kaprio, Rissanen, Virkkunen, & Rose, 2003). Several studies have found positive associations between physical exercise and physical and psychological wellbeing (Nabkasorn et al., 2005; Wiles et al., 2008). At least one hour of moderate physical activity per day seems to be necessary in order to maintain health (Wiles et al., 2008). Physical exercise has also been found to work against depressive symptoms among adolescent females (Nabkasorn et al., 2005). In a study by Sagatun, Sogaard, Bjertness, Selmer, and Heyerdahl (2007), the physically active 16 year olds reported better wellbeing in terms of mental health than their physically inactive counterparts. However, these results were not found to be consistent at follow-up three years later. Earlier research has shown that adolescent girls skip breakfast more often, smoke more frequently, and engage in physical exercise less often than boys (Östberg, 2001). Moreover, this study found that unhealthy lifestyle habits become more common with increasing age. Besides the investigated associations between lifestyle, stress, and health, an essential factor that has come to play a crucial role in research on stress and burnout is disturbed sleep.
Sleep and recovery Sleep is an antagonist to stress; it accounts for the anabolic, energy providing processes that prevent the wear and tear of the body (Ekstedt, 2005). It is essential for brain functioning, health, and overall wellbeing. Disturbed sleep and impaired recovery are among the most important and early symptoms of clinical burnout, as they contribute essentially to the depletion of energy (Ekstedt, et al 2006; Shirom, Melamed, Toker, Berliner, & Shapira, 2005; Söderström, 2012; Söderström, Ekstedt, Åkerstedt, Nilsson, & Axelsson, 2004; Sonnenschein, Sorbi, VanDoornen, Schaufeli, & Maas, 2007). Armon et al. (2008) found a bidirectional relationship between burnout and insomnia, in that they contributed to each other’s development and intensification over time. Since poor sleep quality, sleep deprivation, and sleep disturbances have been associated with chronic stress among adults (Armon et al., 2008; Ekstedt, 2005; Lund, Reider, Whiting, & Prichard, 2010) it is essential to take sleep and recovery into account as relevant factors when studying chronic stress among adolescents. Recent investigations show that many adolescents do not obtain an adequate amount of sleep (Dagys, et al. 2012; Fuligni & Hardway, 2006; Roberts, Roberts, & Doung, 2009; Saxvig, Pallesen, Wilhelmsen-Langeland, Molde, & Bjorvatn, 2012). In fact, the number of young people who complain of daytime fatigue and sleep disturbances has increased dramatically in the past ten years and is now at the same level as for adults (Socialstyrelsen, 2009). In research on adolescent sleep and its associations to stress and wellbeing, sleep disturbances and insufficient sleep have been found to affect daily functioning by negatively impacting academic performance and social interaction, an effect that can in turn give rise to stressful experiences (Bernert, Merrill, Braithwaite, VanOrden, & Joiner, 2007). Looking at it from another direction, stress has been found to interfere with individuals’ ability to obtain adequate sleep, according to Fuligni and Hardway (2006). Their findings showed that stressful demands during the day were associated with less sleep during the night and higher levels of anxiety, depressive feelings, and daytime fatigue during the subsequent day. In another study, adolescent sleeping problems have been shown to be associated with stress, decreases in social functioning, and reduced quality of life (Lund et al., 2010), while yet another found poor sleep quality
20
and insufficient sleep quantity to be associated with health complaints (Pilcher, Ginter, & Sadowsky, 1997). Moreover, occasional and persistent sleeping problems have been associated with concentration problems (Ipsiroglu, Fatemi, Werner, Paditz, & Schwarz, 2002). From a behavioral perspective, sleep is equivalent to “going to sleep,” which implies a reversible perceptual disengagement from the environment (Ekstedt, 2005). However, the individual cannot force herself deliberately to sleep; there are several physiological factors involved, as described by several studies (Ekstedt, 2005; Söderström, 2012). When it comes to adolescents, it is essential to keep in mind that their sleep is opposed by biologically based phase changes in their circadian rhythm during puberty, which makes it physically harder to maintain earlier bedtimes (Auger, Burgess, Dierkhising, Sharma, & Slocumb, 2001; Brandalize, Felden-Pereira, Leite, Lorenzi-Filho, & Mazzilli-Louzada, 2011; Randler, 2011; Wolfson & Carskadon, 2003). This is compounded by the fact that adolescents tend to wish to stay up later to engage in social and other stimulating activities and therefore choose to go to bed later (Dahl & Lewin, 2002). In more conceptual terms, a reorientation, or phase shift, towards more evening activity, or eveningness, commonly occurs during puberty, which is presumably caused by both biological and social factors (Besoluk, Önder & Deveci, 2011; Roenneberg, Wirz-Justice, & Merrow, 2003; Wittmann, Dinich, Merrow, & Roenneberg, 2006). In general, male adolescents have been found to be more evening oriented than female (Randler, 2011). Evening chronotypes are more active later in the day than intermediate or morning chronotypes. With school days starting early, a problem arises for evening chronotypes when their typically late bed times and required early wake-ups combine to lead to less sleep and create an increasing sleep debt over the course of the school week (Auger et al., 2011; Mecacci & Rocchetti, 1998; Taylor, Clay, Bramoweth, Sethi, & Roane, 2011). Consequently, on average, evening chronotypes usually get less sleep per school night compared to morning chronotypes (Roenneberg et al., 2003). Moreover, evening chronotypes are at higher risk for experiencing a phenomenon known as social jetlag (Roenneberg et al., 2003; Zimmermann, 2011). Social jetlag refers to a pattern that implies a drastic variability between a person’s weekday (school day) and weekend sleeping schedules. It refers to the individual’s tendency to increase the weekend sleeping time in order to compensate for a sleep debt accumulated during the weekdays, often in combination with staying up even later and sleeping in. This shift in sleeping times over the weekend results in a disturbance in circadian rhythms, which then makes it difficult to get up at the regular times during the school week (Dahl & Lewin, 2002; Roenneberg et al., 2003; Wittmann et al., 2006). For students returning to school after the weekend or days off, the symptoms of this can be similar to jetlag, as they may experience severe tiredness, irritability, lack of energy, lack of appetite, and problems concentrating. Taken together, sleep and recovery have previously been found to be of particular relevance to adolescent stress and wellbeing. Previous research has focused on sleep-related factors and their impact on academic achievement among adolescents, which is further referred to in the next section. Since the rather new concept of social jetlag has not been exhaustively investigated, another purpose of the present thesis was to take a closer look at its associations with adolescent stress and academic achievement.
Chronic stress, sleep, and academic achievement In Sweden, school is compulsory for children between the ages of seven and sixteen. Following this, a minority of adolescents choose to enter directly into the labor market, while about 90% choose to
21
either pursue vocational training or enroll in an academic track in high school (usually a three-year education) (Skolverket, 2010). While continuing on to high school is optional, its successful completion is necessary in order to get accepted to tertiary education, which usually also involves having completed an academic track. If the goal is to enter a high-ranking tertiary educational program, good final grades, which are based on students’ total academic performance throughout high school, are crucial for selection. About 30% of high school students in Sweden and almost 40% of high school students in Stockholm in particular do not finish their high school educations (Ahrén, 2010; KIF, 2009). Academic achievement can be considered to be an important domain in the life of high school students, as it profoundly affects young people’s transition into adulthood in terms of access to higher education and vocational careers. Academic achievement is also considered to be a reliable indicator for future health and wellbeing (Brolin-Låftman & Modin, 2011; Schmidt & Padilla, 2003). Chronic stress symptoms, such as emotional and physical exhaustion as well as cognitive difficulties, might complicate the accomplishment of academic tasks, such as exams, participation in school lessons, project work, and homework, which typically are the basis for grades and academic achievement. It would therefore not be surprising if chronic stress had a negative impact on academic achievement. However, little attention has been paid thus far to the effects that the experiencing of chronic stress has on adolescents’ academic achievement. There are, however, several neuropsychological investigations which suggest that chronic stress has a considerable negative impact on brain functioning throughout a person’s lifespan (Marin et al., 2011). This functioning should be important in the school environment as a number of factors are crucial to performing school-related tasks, including cognitive processes regarding learning, attention, and concentration, as well as one’s capacity for complex thinking, working memory, problem solving, and creativity. During adolescence, the prefrontal cortex, the most evolved brain region that serves higher order cognitive abilities, such as executive functioning, is still developing (Arnstein, 2009; Lupien, McEwen, Gunnar, & Heim, 2009). It is also the brain region that is most sensitive to the detrimental effects of stress exposure. In fact, in otherwise healthy individuals, chronic stress has been found to disrupt working memory, problem solving, creativity and other prefrontal cortex-related processes (Liston, McEwen, & Casey, 2008). Liston et al. (2009) compared the performance of twenty university students, who were experiencing prolonged psychosocial stress for four weeks as they prepared for a major academic examination, with twenty control students who did not perceive stress. Experiencing psychosocial stress selectively impaired attentional control and disrupted attention shifting. Moreover, prolonged stress implies an accumulation of neurocognitive deficits over time (Arnstein, 2009). The effects of chronic stress on the brain may also explain the cognitive impairments of clinical burnout patients. In fact, cognitive difficulties are not only included in the definition of burnout (Melamed et al., 1992; Socialstyrelsen, 2005), but have been found to be among the most pronounced and handicapping symptoms among clinical burnout patients (Jonsdottir, et al. 2012). As indicated by the studies described above, chronic stress seems to have an impact on cognitive functioning and thus on cognitive performance. However, psychological studies on this matter are rare. Kaplan, Liu, and Kaplan (2005) showed that stress had an impact not only on emotional

22
adjustment but also on academic performance among adolescents. A bidirectional negative relationship between stress and academic achievement has also been observed (Gustafsson et al., 2010). In this study, internalized problems, such as stress, anxiety, and depressive mood, were associated with negative effects on academic achievement; poor academic achievement, in turn, was shown to affect mental health. While the impact of self-reported chronic stress symptoms on academic achievement is rarely investigated, a growing number of studies have discovered the importance of sleep and recovery for processes of learning, memory, and academic achievement (Dahl & Lewin, 2002; Walker, 2008; Wolfson & Carskadon, 2003). Insufficient sleep duration has been linked to decreases in academic performance (Beebe, Rose, & Amin 2010; Kelly, Kelly, & Clanton, 2001; Lund et al., 2010; Roberts et al., 2009; Wolfson & Carskadon, 2003). In their longitudinal study among 4175 adolescents, Roberts et al. (2009) found that amount of sleep was related to alertness during the day and, consequently, the ability to concentrate and perform school-related tasks. Despite finding an association between sleep quality and school performance, Meijer, Habekothe, and Wittenboer (2000) also found that objective sleep duration had no impact on school performance. Also, the experience of sleeping difficulties has been associated with academic achievement (Buboltz, Brown, & Soper, 2001; Saxvig et al. 2012), as well as sleep quality (Curcio, Ferrara, & DeGennaro, 2006; Fuligni & Hardway, 2006; Lund et al.; 2010). Moreover, academic achievement among evening chronotypes was found to be worse compared to morning chronotypes (Besoluk et al., 2011; Gomes, Tavares, & deAzevedo, 2011; Howell, Jahrig, & Powell, 2004; Wolfson & Carskadon, 2003; Yeung, Chung, & Cy Chan, 2008). However, research on the association between the consequences of not going to bed at a regular time throughout the entire week (i.e., social jetlag) and academic achievement are lacking.

23
Methods
The present thesis is based on three empirical studies which make use of questionnaire data that have been collected among Swedish high schools within the project “Stress prevention in high school” (Perski, Schraml, Grossi, Makower, & Ivarsson, 2010). Collaboration was established with three academically high-ranking high schools from suburban areas of Stockholm, namely Hersby, Gångsätra, and Blackeberg high schools. The samples are described below, followed by a description of the measures and statistical analyses.
Participants and procedure In all of the studies, questionnaire data were collected among sixteen-year-old (+/− one year) high school students during their first year in high school (in February), after approval by the local ethics review board. All participants were students in an academic high school track. Prior to the data collection, students and parents were informed in writing about the study’s aims and procedures and their consent was requested. Participation was voluntary. The data collection was organized in collaboration with the school staff. During a designated school lesson, all of the participating students answered the questionnaires individually and in silence in the presence of a school staff member. The average completion time for the questionnaires was approximately thirty minutes. In all three studies, missing and incomplete data were deleted. In study II and study III, participants were asked to answer the same questionnaire twice, at the age of sixteen in their first year of high school and again two years later at the end of high school.
Measures The data used in all three studies is based on a set of established scales and questions that were collectively distributed to the participants as a “stress screening questionnaire.” First, the Shirom-Melamed Burnout Questionnaire (SMBQ) is described, which was used to assess severe stress symptoms throughout all three studies and therefore is considered to be of most importance. Thereafter, the other applied scales are presented in alphabetical order. Finally, single items are mentioned, followed by a description of the applied indicators for academic achievement, namely final grades.
To measure the prevalence of severe stress symptoms and chronic stress among adolescents, the Shirom-Melamed Burnout Questionnaire was used, which contains 22 items (graded 1–7) that measure different facets of chronic stress by focusing on the depletion of an individual’s energy resources (Melamed et al., 1992). Respondents were asked to rate the degrees of physical, emotional, and psychological stress symptoms that they were experiencing (e.g., I feel physically exhausted; I have difficulties concentrating; I feel restless; I feel like I have had enough) (Shirom & Melamed, 2006). High scores indicate an intense degree of perceived stress symptoms. An overall chronic stress
24
or burnout index can be calculated according to the four dimensions of burnout, tension, listlessness, and cognitive difficulties. Throughout this thesis, as in previous studies, a rating of 4 or above is considered to be indicative of serious stress symptoms (Grossi, Perski, Evengård, Blomkvist, & Orth-Gomér, 2003). The indications of chronic stress differed among the studies. In study I, the term chronic stress was used to describe the prevalence of extremely pronounced stress symptoms (indicated by a rating of 5 or above), which have otherwise only been observed in clinical burnout patients (Perski, 2006). In study II, chronic stress was indicated by the prevalence of severe stress symptoms at more than one time point. In study III, the mean value of perceived stress symptoms from two time points was used to indicate the prevalence of severe stress symptoms. The Cronbach’s α coefficient for this scale was determined to be between 0.90 and 0.94 for the different studies.
Perceived demands, control, and social support, which are important stress-related variables according to Karasek and Theorell (1990), were measured by 17 items (graded 1–4) in an adapted version of the questionnaire (instead of referring to the workplace, the questions referred to high school students’ life situation). Demands were measured using an index of five items concerning qualitative and quantitative demands, such as time pressure and conflicting demands (e.g., Do you feel life is too demanding?; Are there many conflicting demands in your life?). High scores indicated that the perceived demands were high. The Cronbach’s α coefficient was between 0.80 and 0.84 for the different studies. The control index included six items to capture such areas as skill discretion and authority over decisions (e.g., Can you make decisions about your life on your own?; I constantly need to learn new things in order to deal with my life). Low scores indicated a lack of perceived control. The Cronbach’s α coefficient was between 0.30 and 0.54. Social support was measured by an index of 6 items and focuses on the social climate in school (e.g., I get along well with my schoolmates; There is a good sense of togetherness in my class) (Theorell, 1996). High scores indicated that social support was high. The Cronbach’s α coefficient was between 0.70 and 0.76 for the different studies.
Sleep disturbances/difficulties were examined by a nine questionnaire index (study I) and an eight question index (study II and study III) (graded 1-5) taken from the Karolinska sleep questionnaire (KSQ) (e.g., I have difficulties falling asleep; I do not feel well-rested when I wake up in the morning; I experience disturbed sleep) with lower scores indicating more pronounced sleeping difficulties (Kecklund & Åkerstedt, 1992). The Cronbach’s α coefficients were 0.67 (study III), 0.71 (study II), and 0.73 (study I). The Performance-Based Self-esteem scale (PBS scale) (Hallsten et al., 2005) consists of four items (graded 1–4) and was used in study I and study II to assess to what degree the respondents’ self-esteem was based on performance and success (I think I sometimes try to prove my worth by being competent; My self-esteem is far too dependent on my daily achievements; At times, I have to be better than others to be good enough myself; Occasionally I feel obsessed to accomplish something of value). High scores indicate high performance-based self-esteem. In study I, a cut-off point of 4 or above indicated a high level of performance-based self-esteem. This cut-off point was set to one standard deviation above the groups’ mean. The Cronbach’s α coefficient was 0.80 in study I and 0.81 in study II.
The Rosenberg self-esteem scale (RSE scale), the most extensively applied instrument for the assessment of global self-esteem among adolescents, was utilized (Baumeister et al., 2003; Butler & Gasson, 2005; Rosenberg, 1972; Vispoel, Boo, & Bleiler, 2001). It consists of 10 generally formulated items (graded 1–4) which enable a global self-assessment (e.g., Sometimes I feel rather worthless; There is nothing I could be proud of; In general, I am quite content with myself). High scores in this assessment indicate high global self-esteem, which reflects a respondent’s overall feeling of being

25
good enough. In study I, the cut-off point for high global self-esteem was fixed in the middle of the scale at 2.5. The Cronbach’s α coefficient was 0.90 in both study I and study II.
Some single items were used as indicators for lifestyle variables, such as breakfast and lunch routine (How often do you skip breakfast?; How often do you skip lunch?; graded from 1=every day to 5=never) (study I), degree of physical exercise (To what extent do you exercise physically?; graded from 1=no physical exercise to 5=intense physical exercise) (study I), and alcohol use and tobacco use (How often do you drink alcohol?; How often do you consume nicotine?; graded from 1=every day to 5= never) (study III). Study II included a question about life satisfaction (In general, how satisfied are you with your current life situation?; graded from 1=very unsatisfied to 5=very satisfied) and one item on self-rated health (How would you say your general health has been during the past year?; graded from 1=bad to 5=very good). Moreover, one question about subjectively perceived sleep duration/sleep quantity was asked in both study II and study III (Do you believe that you get enough sleep?; graded from 1=no, not nearly enough to 5= yes, definitely enough). More conclusive information on participants’ sleep-related variables was collected in study III, where, in addition to subjective sleep quantity, sleep quality was measured (How would you estimate the quality of your sleep?) on a scale from 1 to 5, with higher scores indicating better sleep quality. Also, information about the participants’ average bed and rise times during the week and during the weekend was collected. They were also asked to estimate their average sleep onset latency (that is the length of time that it takes to fall asleep). The answers were used to calculate sleep duration, in terms of the average number of hours spent in bed daily on weekdays and on weekends. Also, the data was used to determine the participants’ degree of social jetlag, which was determined according to the absolute difference between the time of mid-sleep (midpoint between sleep onset and rise time) on school days and on weekends (Roenneberg et al., 2003; Wittmann et al., 2006). Higher values indicate a higher degree of social jetlag. Finally, academic achievement, which was the outcome variable of most interest in study II and study III, was indicated by the students’ final grades. The final grades are based on the students’ total academic performance throughout high school and access to these public data was provided by the participating schools. In these studies, the final grades varied from 6.20 to 20 points, with a mean of 16.80 (SD=2.36) in study II and a mean of 16.92 (SD= 2.36) in study III with higher values indicating better grades.
Statistical analyses In study I, the first aim of the study was to survey the incidence of severe stress symptoms and chronic stress among adolescents. In our analysis of the SMBQ questionnaire data, minimum cut-off scores were set to demarcate at what point both stress and chronic stress were perceived, which were based on earlier studies and clinical settings (Grossi et al., 2003; Perski, 2006). A simple frequency analysis for both males and females was then carried out. By conducting a one-way ANOVA, three stress groups (representing non-stressed, stressed, and chronically stressed adolescents) could be compared, and post hoc tests (Scheffé) of the least significant differences were performed on all pairwise comparisons. Also, to investigate possible gender differences, a one-way ANOVA was conducted. The second aim of the study was to determine which factors may contribute to or exacerbate stress symptoms in adolescents. To do this, a linear stepwise regression analysis was conducted. The independent variables were added one by one into the model to test whether they were statistically significant. The purpose of this statistical analysis was to examine the order of entry of the predictors

26
into the model, as well as the relative strength of the relations between the predictors and the outcome. The statistical analyses in study I and study II were carried out using the Statistical Package for Social Sciences (SPSS) version 16.0 for Windows.
In study II, according to their responses on the SMBQ items at time 1 and time 2, and using the cut-off point of 4 or more, the students were categorized into three different stress groups: a no-stress group, a transitory stress group, and a chronic stress group. In the first step, the data was explored by means of descriptive statistics, and a multivariate analysis (gender x stress groups) of variance was conducted. In addition, the differences between the final grades in the three stress groups were investigated by means of an analysis of variance. Finally, a logistic regression analysis was conducted to determine the relative importance of the various risk factors that may contribute to chronic stress.
In study III, descriptive analyses were conducted for a number of sleep-related variables among the overall sample (bed and rise times, sleep latency, sleep duration on school days and weekends, chronotype, and social jetlag). Among the subsample of those whose final grades were available and who had also filled in the questionnaire at both time 1 and time 2, the contribution of stress symptoms, gender, sleep duration, sleep difficulties, sleep quality, sleep quantity, and social jetlag in predicting academic achievement was investigated. The analyses were based on average values over the two test points. Multilevel mixed effects regression models were utilized with a random intercept for school, using the analytical method “xtmixed” within the statistical package STATA 12.1. Academic achievement was treated as the dependent variable and stress symptoms, gender, sleep duration, sleep difficulties, sleep quality, sleep quantity, and social jetlag were subsequently added to the model. Each model was then tested against the hitherto best-fitting model using likelihood ratio testing (Rabe-Hesketh & Skrondal, 2008). Finally, the best-fitting model was estimated using restricted maximum likelihood.
27
Summary of Studies
Study I - Stress symptoms among adolescents: The role of subjective psychosocial conditions, lifestyle, and self-esteem
Background and aim Over the past 20 years, the number of 16-year olds reporting stress, fatigue, psychosomatic complaints as well as psychological and physical tension has been steadily rising, especially among adolescent females (Bremberg, 2006). Adolescence is considered a stressful period in life. However, the fact that an increasing number of Swedish adolescents and young adults seek psychiatric health care (Dalman & Wicks, 2006; Socialstyrelsen, 2009) is likely to be indicative of something far more serious than what could be attributed to the expected storm and stress of adolescence (Hall, 1904). This alarming trend has stimulated great public concern, especially since it may lead to the development of chronic stress. Chronic stress is associated with deteriorating energy resources (Shirom, 2003). If an imbalance between spending and regaining energy persists over a long period of time, severe stress symptoms may occur which eventually lead to negative health outcomes, such as exhaustion syndrome. The aim of study I was to survey the incidence of severe stress symptoms among adolescents in order to better understand the factors that may contribute to or exacerbate these symptoms and to examine possible gender differences.
Method The data collection took place at two high schools over the course of one week in February 2006. The sample included 304 first-year high school students, of whom 159 were males (52%) and 145 were females (48%). They participated by responding to a stress screening questionnaire that included questions regarding stress symptoms, perceived demands and control, and social support as well as self-esteem and lifestyle variables, such as sleep, eating habits, and physical exercise. At both schools the response rate was very high (98%) even though participation was voluntary.
Main findings and conclusions About one-third (32.9%) of the participants reported a high degree of stress symptoms. This group consisted of 68 girls (45.9% of all girls) and 32 boys (20.5% of all boys). Twenty-five of the participants (8.2% of all participants) reported a very high degree of stress symptoms – levels which are similar to those reported by patients who suffer from exhaustion syndrome – and which were therefore considered to be indicative of chronic stress in this study. More than five times as many girls
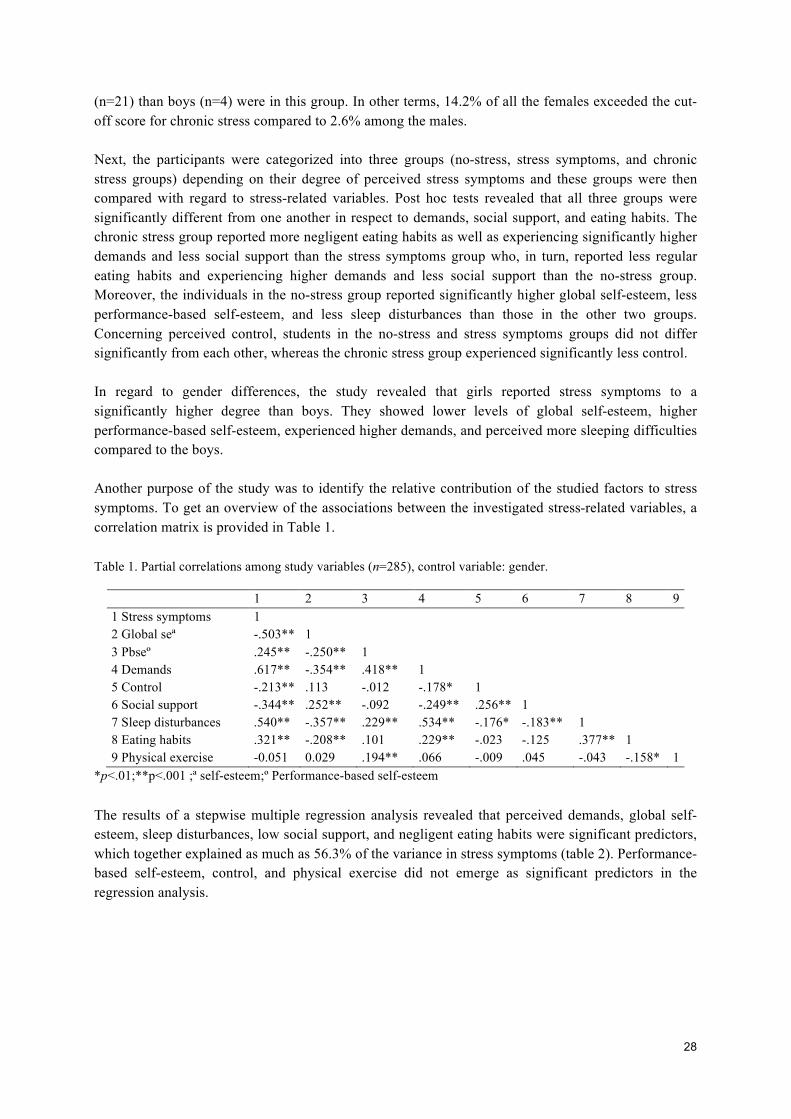
28
(n=21) than boys (n=4) were in this group. In other terms, 14.2% of all the females exceeded the cut-off score for chronic stress compared to 2.6% among the males. Next, the participants were categorized into three groups (no-stress, stress symptoms, and chronic stress groups) depending on their degree of perceived stress symptoms and these groups were then compared with regard to stress-related variables. Post hoc tests revealed that all three groups were significantly different from one another in respect to demands, social support, and eating habits. The chronic stress group reported more negligent eating habits as well as experiencing significantly higher demands and less social support than the stress symptoms group who, in turn, reported less regular eating habits and experiencing higher demands and less social support than the no-stress group. Moreover, the individuals in the no-stress group reported significantly higher global self-esteem, less performance-based self-esteem, and less sleep disturbances than those in the other two groups. Concerning perceived control, students in the no-stress and stress symptoms groups did not differ significantly from each other, whereas the chronic stress group experienced significantly less control. In regard to gender differences, the study revealed that girls reported stress symptoms to a significantly higher degree than boys. They showed lower levels of global self-esteem, higher performance-based self-esteem, experienced higher demands, and perceived more sleeping difficulties compared to the boys. Another purpose of the study was to identify the relative contribution of the studied factors to stress symptoms. To get an overview of the associations between the investigated stress-related variables, a correlation matrix is provided in Table 1. Table 1. Partial correlations among study variables (n=285), control variable: gender.
1 2 3 4 5 6 7 8 9 1 Stress symptoms 1 2 Global seª -.503** 1 3 Pbseº .245** -.250** 1 4 Demands .617** -.354** .418** 1 5 Control -.213** .113 -.012 -.178* 1 6 Social support -.344** .252** -.092 -.249** .256** 1 7 Sleep disturbances .540** -.357** .229** .534** -.176* -.183** 1 8 Eating habits .321** -.208** .101 .229** -.023 -.125 .377** 1 9 Physical exercise -0.051 0.029 .194** .066 -.009 .045 -.043 -.158* 1
*p<.01;**p<.001 ;ª self-esteem;º Performance-based self-esteem The results of a stepwise multiple regression analysis revealed that perceived demands, global self-esteem, sleep disturbances, low social support, and negligent eating habits were significant predictors, which together explained as much as 56.3% of the variance in stress symptoms (table 2). Performance-based self-esteem, control, and physical exercise did not emerge as significant predictors in the regression analysis.

29
Table 2. Significant predictors in the linear stepwise regression analysis with stress symptoms as the dependent variable.
Predictors B SE Beta t p Demands 0.583 0.078 0.369 7.481 <0.001 Global self-esteem -0.391 0.068 -0.260 -5.782 <0.001 Sleep disturbances 0.312 0.082 0.195 3.820 <0.001 Social support -0.301 0.091 -0.137 -3.302 0.001 Eating habits 0.077 0.036 0.091 2.134 0.034
The fact that serious stress symptoms were reported by more than 30% of the investigated high school students indicates that this phenomenon should not be simply regarded as a passing occurrence within the normal storm-and-stress period but should, rather, be seen as the first phase of a potentially prolonged state involving future health implications, such as exhaustion syndrome. If stress-related problems in adolescence are dismissed as normal there is a risk that young people will not receive the help they actually need.
30
Study II - Chronic stress and its consequences on subsequent academic achievement among adolescents
Background and aim Chronic stress has been associated with stress-related symptoms among adults and may lead to negative health outcomes, such as exhaustion syndrome. However, it is not only adults who suffer from prolonged stress, as research has shown that every third adolescent reports severe stress-related symptoms (study I). Since the chronic depletion of energy emerges over an extended period of time, finding a fully developed exhaustion syndrome among young populations is difficult to expect. However, chronic stress may have more immediate consequences on adolescents (Thoreson & Eagelston, 1983). While the pernicious consequences of chronic stress on health are recognized, research has not focused on the effects that chronic stress may have on other important life domains, such as academic achievement among adolescents. The aim of study II was to investigate how academic achievement, in terms of final high school grades, is affected by perceived chronic stress symptoms, and to investigate which factors may constitute a heightened risk for chronic stress.
Method The initial sample consisted of 456 sixteen-year-old high school students from two different high-ranking high schools who answered the stress screening questionnaire at the beginning of their time in high school. In this first round of data collection which took place in February 2006 for the first school and February 2008 for the second, 171 and 285 high school students participated, respectively. Two years after the first round, at the end of high school, a second round of data collection took place at each school where 119 students from the first school and 176 from the second voluntarily participated again in the study, yielding longitudinal response rates of 70% and 62%, respectively, and 65% combined. After excluding incomplete and missing data, the data from 273 participants remained for the analyses. Academic achievement, the outcome variable of most interest, was indicated by the students’ final grades at the end of high school.
Main findings and conclusions Based on the prevalence of perceived stress symptoms at both time points, three stress groups were defined, a no-stress group, a transitory stress group, and a chronic stress group. Among all of the investigated high school students, 41 students (15%) (31 girls and 10 boys) were found to be chronically stressed, as they reported experiencing serious stress symptoms both at the beginning and in the end of high school. Fifty-nine students (22%), 39 girls and 20 boys, perceived severe stress on just one of the measurement occasions. Taken together, 100 high school students (37%) perceived stress symptoms at least once during their time in high school. The remaining 63% of the study’s participants (67 girls and 106 boys) did not feel stressed at all. When it comes to gender differences,
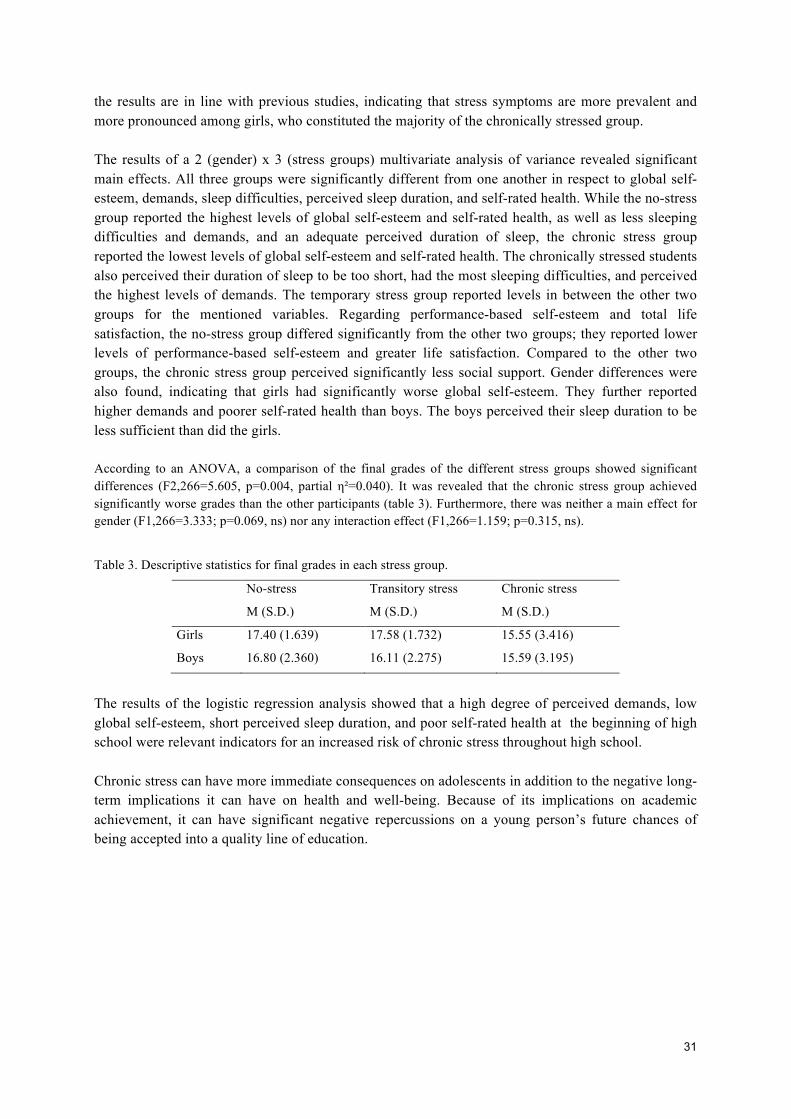
31
the results are in line with previous studies, indicating that stress symptoms are more prevalent and more pronounced among girls, who constituted the majority of the chronically stressed group. The results of a 2 (gender) x 3 (stress groups) multivariate analysis of variance revealed significant main effects. All three groups were significantly different from one another in respect to global self-esteem, demands, sleep difficulties, perceived sleep duration, and self-rated health. While the no-stress group reported the highest levels of global self-esteem and self-rated health, as well as less sleeping difficulties and demands, and an adequate perceived duration of sleep, the chronic stress group reported the lowest levels of global self-esteem and self-rated health. The chronically stressed students also perceived their duration of sleep to be too short, had the most sleeping difficulties, and perceived the highest levels of demands. The temporary stress group reported levels in between the other two groups for the mentioned variables. Regarding performance-based self-esteem and total life satisfaction, the no-stress group differed significantly from the other two groups; they reported lower levels of performance-based self-esteem and greater life satisfaction. Compared to the other two groups, the chronic stress group perceived significantly less social support. Gender differences were also found, indicating that girls had significantly worse global self-esteem. They further reported higher demands and poorer self-rated health than boys. The boys perceived their sleep duration to be less sufficient than did the girls. According to an ANOVA, a comparison of the final grades of the different stress groups showed significant differences (F2,266=5.605, p=0.004, partial η²=0.040). It was revealed that the chronic stress group achieved significantly worse grades than the other participants (table 3). Furthermore, there was neither a main effect for gender (F1,266=3.333; p=0.069, ns) nor any interaction effect (F1,266=1.159; p=0.315, ns).
Table 3. Descriptive statistics for final grades in each stress group.
No-stress Transitory stress Chronic stress
M (S.D.) M (S.D.) M (S.D.)
Girls 17.40 (1.639) 17.58 (1.732) 15.55 (3.416)
Boys 16.80 (2.360) 16.11 (2.275) 15.59 (3.195)
The results of the logistic regression analysis showed that a high degree of perceived demands, low global self-esteem, short perceived sleep duration, and poor self-rated health at the beginning of high school were relevant indicators for an increased risk of chronic stress throughout high school. Chronic stress can have more immediate consequences on adolescents in addition to the negative long-term implications it can have on health and well-being. Because of its implications on academic achievement, it can have significant negative repercussions on a young person’s future chances of being accepted into a quality line of education.

32
Study III – The impact of stress and social jetlag on academic achievement among adolescents
Background and aim Stress symptoms have not only been found to be highly prevalent among high school students (study I), but it has also been shown that chronic stress has negative implications on their academic achievement (study II).
Along with the high prevalence of stress-related symptoms, sleep-related problems have also been rapidly increasing among adolescents over the last decade. Moreover, sleep and recovery have been shown to be associated with academic achievement (Dahl & Lewin, 2002; Walker, 2008; Wolfson & Carskadon, 2003). In light of this, a further investigation of the role of sleep and sleep-related variables, as well as the impact of chronic stress, in explaining adolescents’ academic achievement was undertaken in study III.
For adolescents, the need to sleep is opposed by biologically based phase changes in their circadian rhythm during puberty, which makes it physically harder to maintain earlier bedtimes (Auger et al., 2001; Brandalize et al., 2011; Wolfson & Carskadon, 2003). Furthermore, social and other arousing activities may impede earlier bedtimes at this age (Dahl & Lewin, 2002). Although adolescence brings with it a tendency towards more evening orientation, there are differences in how evening or morning orientated one is, which is also referred to as the individuals’ chronotype.
The main aims of study III were to investigate whether variability in academic achievement among high school students is due to stress symptoms, as shown in study II, and to examine whether a number of sleep-related variables contribute to the prediction of adolescents’ academic achievement. The investigated sleep variables were objective sleep duration (time in bed), sleep difficulties (such as having trouble falling asleep or waking up during the night), subjectively perceived quality and quantity of sleep as well as degree of social jetlag. High social jetlag refers to a pattern that implies a drastic variability between a person’s weekday (school day) and weekend sleeping schedules.
Since social jetlag is a relatively new construct, a closer look was taken at its associations with unhealthy lifestyle habits, stress symptoms, and the other investigated sleep-related variables.
Method The overall sample consisted of 1035 sixteen-year-old high school students from three different high schools, who answered questions about stress and sleep-related variables. After the deletion of missing and incomplete data, the data of 958 high school students remained for the subsequent analyses. Furthermore, the data from a subsample of 244 high school students, who had answered our questionnaire on stress and sleep at two time points, at the beginning of high school and two years later at the end of high school, was analyzed. For this subsample, the final grades were available. Degree of social jetlag was determined by calculating the absolute difference between the time of mid-sleep (midpoint between sleep onset and rise time) on school days and on weekends (Roenneberg et al., 2003; Wittmann et al., 2006). Academic achievement, the outcome variable of most interest, was indicated by the final grades at the end of high school.
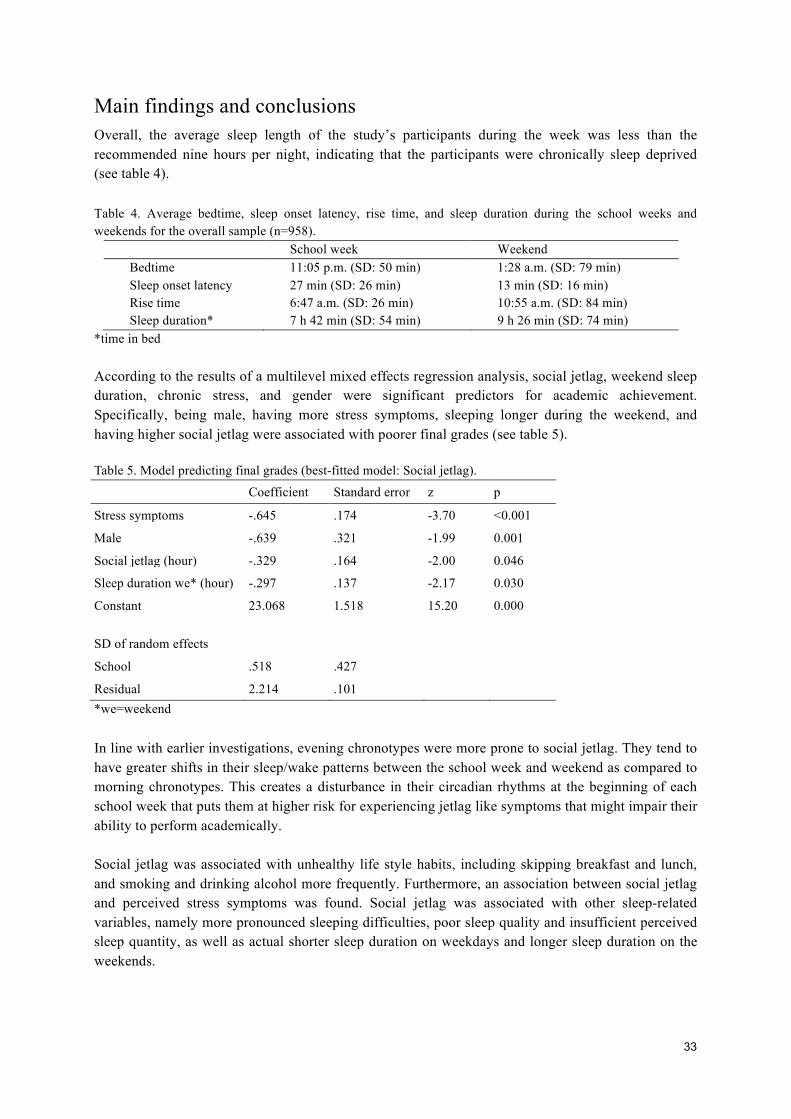
33
Main findings and conclusions Overall, the average sleep length of the study’s participants during the week was less than the recommended nine hours per night, indicating that the participants were chronically sleep deprived (see table 4).
Table 4. Average bedtime, sleep onset latency, rise time, and sleep duration during the school weeks and weekends for the overall sample (n=958).
School week Weekend Bedtime 11:05 p.m. (SD: 50 min) 1:28 a.m. (SD: 79 min) Sleep onset latency 27 min (SD: 26 min) 13 min (SD: 16 min) Rise time 6:47 a.m. (SD: 26 min) 10:55 a.m. (SD: 84 min) Sleep duration* 7 h 42 min (SD: 54 min) 9 h 26 min (SD: 74 min)
*time in bed According to the results of a multilevel mixed effects regression analysis, social jetlag, weekend sleep duration, chronic stress, and gender were significant predictors for academic achievement. Specifically, being male, having more stress symptoms, sleeping longer during the weekend, and having higher social jetlag were associated with poorer final grades (see table 5). Table 5. Model predicting final grades (best-fitted model: Social jetlag).
Coefficient Standard error z p
Stress symptoms -.645 .174 -3.70 <0.001
Male -.639 .321 -1.99 0.001
Social jetlag (hour) -.329 .164 -2.00 0.046
Sleep duration we* (hour) -.297 .137 -2.17 0.030
Constant
23.068 1.518 15.20 0.000
SD of random effects
School .518 .427
Residual 2.214 .101 *we=weekend In line with earlier investigations, evening chronotypes were more prone to social jetlag. They tend to have greater shifts in their sleep/wake patterns between the school week and weekend as compared to morning chronotypes. This creates a disturbance in their circadian rhythms at the beginning of each school week that puts them at higher risk for experiencing jetlag like symptoms that might impair their ability to perform academically. Social jetlag was associated with unhealthy life style habits, including skipping breakfast and lunch, and smoking and drinking alcohol more frequently. Furthermore, an association between social jetlag and perceived stress symptoms was found. Social jetlag was associated with other sleep-related variables, namely more pronounced sleeping difficulties, poor sleep quality and insufficient perceived sleep quantity, as well as actual shorter sleep duration on weekdays and longer sleep duration on the weekends.
34
Undoubtedly, adequate and regular sleep timing is an important factor when it comes to preventing adolescent stress and improving academic performance. Evening chronotypes, in particular, would benefit from having regular sleep/wake schedules throughout the entire week and later school start times in order to counteract the risk for social jetlag.

35
Discussion
The main aims of the present thesis were to investigate the prevalence of severe stress symptoms among adolescents, to examine factors that may contribute to chronic stress among adolescents, and to examine the impact of chronic stress and sleep-related variables on subsequent academic achievement. After a short summary of the empirical studies’ results, the main findings and their implications are discussed in more detail. Next, limitations and methodological consideration are provided. Finally, possible implications on both future research and clinical practice are considered.
Summary of the findings Concerning the prevalence of severe stress symptoms, the results of study I indicated that almost exactly one-third of the total group reported that they experienced a high degree of stress symptoms, whereas 60% of the adolescents did not perceive severe stress symptoms. The highest degree was perceived by the remaining 8% who perceived especially pronounced stress symptoms. In fact, they suffered from symptoms to an extent which otherwise only has been reported by adult clinical burnout patients (Grossi et al., 2003; Perski, 2006). In study II, the prevalence of chronic stress among adolescents was investigated using a longitudinal approach. While 63% of the participants did not perceive stress symptoms during high school, 22% experienced severe stress symptoms once, and 15% reported severe stress symptoms throughout high school and were thus considered to suffer from chronic stress. Potential differences between boys and girls with regard to chronic stress were also looked at. It was shown that almost every other girl and every fifth boy struggled with stress-related symptoms (study I). Not only were girls more prevalent among the students who perceived stress symptoms, they also perceived more pronounced symptoms compared to the boys. Similar gender differences were noticed in study II, where the majority of those chronically stressed were girls. Furthermore, an attempt was made to investigate if the factors that have been found to be relevant in the development of chronic stress among adults also contribute to severe stress symptoms among adolescents. The results of study I found that perceived demands, global self-esteem, sleep disturbances, low social support, and negligent eating habits were significant predictors of severe stress symptoms, which together explained a considerable amount of variation in stress symptoms (56%). Moreover, perceived high demands, low global self-esteem, perceived short sleep duration, and poor self-rated health in the beginning of high school were found to be relevant indicators for an increased risk of chronic stress throughout high school (study II). The impact of chronic stress on academic achievement was also investigated (in study II and study III), motivated by previous neuropsychological findings on the negative impact of chronic stress on brain functioning. In study II, the investigation of the impact of chronic stress on subsequent academic
36
achievement revealed that the group which was chronically stressed throughout high school had significantly worse final grades compared to both students who did not perceive stress symptoms and those who perceived stress symptoms occasionally. In addition, since regenerative processes are especially crucial for cognitive functioning, the relative importance of sleep and sufficient recovery for subsequent academic achievement was investigated in study III. The results indicated that, besides chronic stress, social jetlag, a factor that had not been discussed before in this context in literature, and longer sleep duration during the weekend impaired subsequent academic success.
Adolescence - a period of “storm and chronic stress”? Considering the extensiveness and impact of the major developmental changes which take place during adolescence, it is not surprising that adolescence has been considered a “stormy and stressful” period in life (Hall, 1904). While the majority of adolescents, namely two out of three, seem to pass through this period without excessively high levels of stress symptoms, a substantial number of individuals (30%) reported experiencing severe stress symptoms at least once during their time in high school. Moreover, 15% reported chronic stress. This represents a substantial number of affected individuals who feel extremely stressed and psychologically burdened, especially when considering the age of the respondents (16 years of age). The high prevalence of severe stress symptoms among adolescents indicates that the stress-related problems probably represent something far more serious than what would be associated with the normal transition into adulthood and thus might have negative long-term consequences on adolescent’s future options and health status. If experienced over a prolonged period of time, severe stress symptoms, such as emotional exhaustion, physical exhaustion, and cognitive difficulties, may eventually lead to the depletion of energy and thus result in stress-related diseases, such as clinical burnout (Melamed, et al., 1992; Melamed et al., 2006; Shirom, 2003). Clinical burnout causes severe individual suffering, impacts the ability to work, and is among the most common diagnoses for long-term sick leave in Sweden (Socialstyrelsen, 2003). The results of the present thesis indicate that the roots of the problem might start earlier in life and therefore should not be regarded as a passing occurrence within the normal storm-and-stress period of adolescence.
Factors that play a crucial role in chronic stress among adolescents By increasing our knowledge about the factors that may contribute to chronic stress, the results of the present thesis could facilitate in the early identification of adolescents at risk for chronic stress. High perceived demands and low self-esteem are factors that have been found to be highly associated with the perception of severe stress symptoms and an increased risk for chronic stress among adolescents. Moreover, sleep and recovery-related variables along with perceived social support proved to be relevant for severe stress symptoms among adolescents. Hence, these factors merit a more detailed description. Additionally, some relevant associations among the identified relevant factors are pointed out.
37
High perceived demands In the present thesis, adolescents who perceived high demands were more likely to suffer from chronic stress. Even though the present findings cannot provide distinctive conclusions about the relative importance of different domains within which adolescents may perceive high demands, a number of possible demand-creating sources in the life of adolescents are worth discussing. A higher risk for psychological strain is prevalent among individuals who perceive high demands from and low control over their work situation (Karasek & Theorell, 1990; Kivimäki & Kalimo, 1996; Theorell, 1996). This is also true for adolescents who ”work” in schools (Gillander-Gådin & Hammarström, 2000; Modin et al., 2011). In fact, besides worries about their future, adolescents most often report that school-related demands are the most stressful (deAnda et al., 2000; Murberg & Bru, 2004). To study, gain new insights, and learn new skills are the main purposes of attending school, which naturally puts demands on the individual in terms of time and effort. Thus, being a high school student is inescapably demanding to some degree. This is evidenced by the results of a recent national Swedish survey, which indicate that many high school students, namely 60% (50% boys and 71% girls), feel stressed by demands related to school issues and academic tasks (SCB, 2012). One explanation for this high degree could be that the fact that final grades are based on the students’ total academic achievement throughout high school is perceived as extremely demanding and thus contributes to an increased risk for chronic stress. Final high school grades are crucial in determining an adolescent’s academic future by facilitating admission to high-ranking tertiary educations. This is especially relevant for high school students in an academic track, who usually aspire to entering tertiary education. Consequently, adolescents are asked to excel academically throughout the entire school period, which may lead some to feel pressured constantly. To perceive constant pressure to succeed academically may then imply a prolonged imbalance between spending and regaining energy, which may result in chronic stress symptoms. It could, however, also be true that some students lack adequate strategies for coping with the demands they perceive. Instead of using active strategies, such as solving tasks or asking others for help, they may struggle with aversive feelings related to the source of stress, associated with avoidant behaviors like procrastination or distraction. According to Modin et al. (2011), it is the students who lack strategies for dealing with high demands who are especially at higher risk for negative health outcomes. It could, however, also be the case that the demands placed upon and perceived by today’s adolescents are different from the demands faced by earlier generations. For example, changes in the school system and school environment may play a crucial role in shaping adolescents’ demands and stress perceptions (Ahrén, 2010). Moreover, cultural and societal changes may force young people today to develop and apply other coping strategies in order to maintain wellbeing. According to Eccles et al. (2008), today’s adolescents grow up in a climate of uncertainty about their options and the impact their choices have on their future life, and this is because of the more transient and less rigid social norms which are typical for modern Western, heterogeneous societies. One’s life course is in fact less predictable in a post-industrial modern society, like Sweden, which is among the most individualized countries in the world (Welzel, & Inglehart, 2010; World Values Survey, 2005/08). A high degree of individualization implies a culture that places a high value on individual freedom and self-expression, which is an advantage in many respects (Bremberg, 2006). However, to live according to the saying “Man forges his own destiny” places high demands on oneself for taking responsibility that the “right” decisions are made. In the face of today’s innumerable possibilities, it may also overstrain the

38
decision-making capabilities of some adolescents. In fact, to pick one alternative always implies abandoning other ones. In particular, adolescents are often concerned with the decisions and plans that could affect their occupational futures (Eccles et al., 2008; Mortimer et al., 2002) and worries over their future career prospects are both common and entitled due to an increase in youth unemployment rates (Bremberg, 2006). Moreover, social comparisons based on unrealistically high standards might be a source of perceived high demands and prolonged stress (Wiklund et al., 2010). Even though “nobody is perfect” is an established expression, societal standards and discourse in the media point more often than not to the opposite, reinforcing that striving for perfection is a necessary precondition for a happy and fulfilled life. Consequently, individuals may struggle and strive to become somebody who they think they are supposed to be. It is not only impossible to have “everything under control,” vulnerability and imperfection are inescapable parts of being human. Based on interviews conducted among adolescent girls, Wiklund et al. (2010) found that young girls feel a considerably high degree of pressure to achieve individual success and perfection as well as a high degree of pressure to manage challenges and overcome barriers on their own. Girls have also tended to equate their self-worth with achievement outcomes Wiklund et al. (2010), an observation, which is in accordance to what Hallsten et al. (2005) described as high performance-based self-esteem and which in previous research has been associated with a heighted risk for burnout (Blom, 2012; Hallsten et al. 2011). In fact, in the present thesis (study I) high performance-based self-esteem was significantly correlated with high perceived demands, indicating that individuals who perceived high demands also tended to base their self-worth on performance and success, or vice versa. According to earlier investigations, extremely high commitment to school work in combination with high perceived demands was found to be related to stress, worries about stress, and the feeling of being overwhelmed by school work (Huan et al., 2000; Ollfors & Andersson, 2007). It is possible that underlying the high levels of commitment are deeper-seated fears of failure and inadequacy and of being evaluated as ”not being good enough”, implying that their strong performance drive is fueled by low self-esteem. Obviously, adolescents who perceive their own value as being partly dependent on their performance also perceive higher demands put on them.
Low self-esteem Global self-esteem was found to be associated with stress symptoms and chronic stress in the present thesis, confirming the results of earlier investigations that high self-esteem is a buffer against stress (Rector & Roger, 1997). An individual’s self-esteem might not only influence if a situation is perceived as threatening and stressful but also influence in which ways the individual deals with the demands she faces. Thus, an individual with high global self-esteem might also perceive herself to be more capable of dealing with a stressful situation. In other words, according to the transactional stress model, individuals with high self-esteem seem to have advantages in regard to the processes of primary and secondary appraisal, and consequently experience less stress. According to Locke et al. (1996), individuals with high self-esteem tend to appraise stressful situations as challenges rather than threats. Thus, they perceive the same situation as less demanding than do individuals with low self-esteem, who not only feel threatened by experiences of and thoughts about failure but also tend to perceive their coping resources as insufficient.

39
Inadequate coping increases the feeling of being incapable of solving problems and successfully dealing with stressors and of having access to resources for eliminating sources of stressors. Thus, it impairs self-efficacy and, consequently, decreases self-esteem (Liu & Kaplan, 1999). High global self-esteem, on the other hand, implies a higher self-efficacy in stressful situations and the ability to use more adequate coping strategies (Bandura, 2000; Moksnes et al., 2010), which is a protector against chronic stress. This is also in line with Salmela-Aro & Nurmi (2007), who concluded, based on the association between self-esteem among university students and their vocational careers ten years later, that self-esteem improves the individual’s beliefs in her competencies, which supports the use of more active coping strategies in demanding situations.
Lack of social support The degree of social support perceived by the adolescents influenced their perception of severe stress symptoms. The chronically stressed students perceived the least social support. This result is in line with earlier studies, which point to the stress preventive impact of supportive relationships (Brolin-Låftman & Östberg, 2006; Haraldsson, 2010; Langstedt et al., 2009), especially for girls. The relations adolescents have with their peers in school have an impact on their health and wellbeing. Moreover, especially strained relationships have previously been shown to have a negative impact on health (Brolin-Låftman & Östberg, 2006). In order to prevent adolescents from health complaints and chronic stress, it is therefore important to provide a school context that counteracts social rejection and social isolation. In this respect, accessibility to significant others as well as being able to view oneself as being significant to others might be of importance. Perhaps, individualistic, competitive values impede the possibility and perception of connectedness to others. This, however, remains a question for future research.
Insufficient sleep and recovery Not surprisingly, sleep and sufficient recovery also played a crucial role in predicting severe stress symptoms among adolescents. Sleep is essential for the anabolic (energy providing) processes in the body. Lack of sleep or bad sleep quality prevents adequate recovery after effort and has been found to be a risk factor in the development of clinical burnout (Ekstedt et al., 2006; Shirom et al., 2005; Söderström, 2012; Sonnenschein, et al., 2007). In the present thesis, it was shown that perceived sleeping difficulties and the perception of not getting sufficient sleep duration were associated with severe stress symptoms among adolescents. It was further shown that sleeping difficulties were highly associated with the perception of high demands (study I), which indicates that the perception and cognitive preoccupation with stressful demands may impair sleep. According to Söderström (2012), sustained cognitive activation in the form of, for example, worries and rumination makes it more difficult to initiate and maintain sleep and sufficient recovery, which, according to the finding in the present thesis, also seems to be the case for adolescents. Of particular interest was also the novel finding that, besides sleeping difficulties and perceived lack of sleep duration, social jetlag was also associated with the perception of severe stress symptoms, indicating that having disturbances in the circadian rhythm and related jetlag-like symptoms on a weekly basis stresses the organism and, in the long run, may also be responsible for an increased susceptibility to chronic stress among adolescents. Taken together, the investigated factors were not only associated with the perception of severe stress symptoms but were also partly associated with each other, indicating that there are multiple influences which together account for a heightened risk of chronic stress among adolescents.
40
Impact of chronic stress and sleep on academic achievement At the end of high school, the academic achievement of chronically stressed high school students was shown to be significantly worse compared to that of non-stressed or occasionally stressed students (study III). This is an interesting finding because academic achievement has a crucial impact on young people in terms of their future occupational and educational options. This is especially relevant for high school students who are in academic high school tracks, since their successful completion of high school is a requirement for access to tertiary education. In accordance with theories about stress physiology, increased effort and strain over a limited period of time, which is the case during short-term stress, permits the organism to recover and regain energy after decreasing stress (Lundberg, 2005; Sapolsky, 2004) and thus does not imply allostatic load (McEwen, 2006). If an imbalance between spending and regaining energy persists over a prolonged time, as with chronic stress, anabolic and regenerative processes are prohibited. Prolonged stress is accompanied by severe symptoms, such as emotional exhaustion, physical exhaustion, and cognitive weariness (Melamed et al. 1992), which have a negative impact on academic achievement. This is in line with results from neuropsychological findings, indicating that chronic stress impedes optimal brain functioning, which then can lead to cognitive difficulties and impairments (Arnstein, 2009; Liston et al., 2008). Based on the present findings, the conclusion is therefore made that chronic stress leads to worse academic achievement, because the symptoms associated with chronic stress make it harder for the individual to accomplish school-related tasks and maintain academically high standards. It should be mentioned that the effect of chronic stress on subsequent academic achievement was small, indicated by a small effect size (η²=0.040). However, chronic stress had an effect in the investigated group of elite high school students which may suggest there would be even stronger effects in other, more diverse adolescent populations. It could, however, also be the case that adolescents from the academic high school track in particular are more concerned about school-related issues and academic achievement and thus experience more stress related to those concerns as compared to students from other educational programs. A recent study conducted by Samela-Aro and Tynkkynen (2012) indicated that it was adolescents from an academic educational track rather than those from a vocational track who tended to develop school burnout symptoms. Determining more specifically what the prevalence and impact of chronic stress is on achievement in adolescent populations from other educational programs is a task for future research. Otherwise, the big-fish-little-pond effect (Marsh & Hau, 2003) might be useful in providing an explanation for the associations found between chronic stress and poor academic achievement. According to this theory, it is better to be a big fish in a little pond than a little fish in big pond, referring to the fact that the academic self-concept of high-achieving students is lower in a high-achieving, competitive educational context, compared to the academic self-concept of equally able students who are educated in an average-ability school. With respect to the present findings, this would mean that, after entering the high-ranking elite high schools, some of the initially equally able adolescents may feel especially challenged and stressed in a more selective and high-achieving school context. When among other high-achieving students, it is probably tougher to sustain one’s position as an excellent student. Consequently, based on the perception of facing higher demands in combination with insufficient resources, perhaps also in
41
combination with perceiving oneself as “not being good enough” any longer, prolonged stress may result, which then impairs performance. Of course, the perception of not being able to live up to one’s own or others expectations in terms of academic performance can feed into a vicious circle that leads to even more stress and performance-disturbing symptoms. In fact, Gustafsson et al. (2010) found a bidirectional relationship between stress and academic achievement, where academic achievement decreased due to stress and affective symptoms and poor performance evoked stress and affected mental health. Moreover, in previous research, sleep and sufficient recovery have not only been described as resources against the negative impact of chronic stress on health (Ekstedt, 2005; Söderström, 2012) but are also considered necessary for cognitive processes, such as learning and memory (Dahl & Lewin, 2002; Walker, 2008; Wolfson & Carskadon, 2003). Therefore, the relative contribution of different sleep-related variables were also taken into account when studying adolescents’ academic achievement. It was found that, besides chronic stress, degree of social jetlag contributed to the prediction of adolescents’ academic achievement at the end of high school. Longer sleep duration during the weekend was associated with poorer grades, which may have been the consequence of an accumulated sleep debt during the week. The finding that social jetlag contributed to worse academic achievement should be highlighted in particular because it is a novel and interesting finding. Social jetlag results from the individual’s tendency to drastically shift sleeping times between weekdays and weekends. This implies a disturbance in circadian rhythms and difficulties getting up at regular times during the school week in combination with symptoms of tiredness, irritability, lack of energy, lack of appetite, and concentration problems, i.e. social jetlag (Dahl & Lewin, 2002; Roenneberg et al. 2003; Wittmann et al., 2006; Zimmermann, 2011). Thus, students with social jetlag most likely start their school days off feeling tired and exhausted while at the same time being in a constant hurry to make it to their morning school lessons in time. It stands to reason that this might inhibit one’s chances of performing well in school. Social jetlag was more pronounced in evening chronotypes, which is in line with previous studies (Roenneberg et al., 2003; Zimmermann, 2011). Specifically, evening chronotypes tended to have greater shifts in their sleep/wake patterns between the school week and weekends compared to morning chronotypes. The disturbance in their circadian rhythms may not only make it more difficult to get up at the regular time at the beginning of each school week (Dahl & Lewin, 2002; Roenneberg et al., 2003; Wittmann et al., 2006) but may also account for a lack of alertness and difficulties concentrating, which makes school work more demanding and the perception of stress more likely. Consequently, it is harder for them to academically perform properly in school. In conclusion, evening chronotypes and especially those with high social jetlag are disadvantaged by the timing of school activities, which are concentrated in the morning, since they are forced to both perform under conditions where circadian factors promote sleep (Mecacci & Rochetti, 1998; Saxvig et al., 2012) and to struggle with social jetlag symptoms.
42
Gender differences The results of the present thesis indicated that girls not only constituted the majority of chronically stressed individuals but also showed more pronounced stress symptoms. This is in line with previous research and national investigations (Ahrén, 2010; Basow & Rubin, 1999; Bremberg, 2006; Friberg, et al., 2012; Hagquist, 2009; Skolverket, 2010). Unfortunately, the present thesis only provides descriptive data concerning gender differences without being able to conclusively explain the reasons for their occurrence; however, a number of possible causes are shortly mentioned. Previous research provides several possible explanations for stress-related gender differences. One possible explanation is that gender differences could be caused by differences in stress exposure, which implies that adolescent girls experience more or other stressors than boys and thus perceive more stress symptoms (Rudolph, 2002). Another explanation, which suggests biological differences, is based upon the assumption that the gender differences found could be due to differences in stress reactivity. In other words, there are differences in physiological predispositions, in which case women would have a higher vulnerability, which is a lower threshold for releasing the stress reaction when confronted with certain stressors, compared to men (Rudolph, 2002; Stroud et al., 2002). Research indicates that this might occur in connection with events which have negative interpersonal consequences (Stroud et al., 2002; Trosisi, 2001). A third explanation emphasizes differences in socialization processes which may also account for differences not only when it comes to the cognitive appraisal of the situation as stressful but also in the way of dealing with stressors (Renstig & Sandmark, 2005). In fact, girls have been shown to be more exposed to interpersonal stress (Murberg & Bru, 2004; Rudolph, 2002; Stroud, et al., 2002) and to be more sensitive to others reactions over their successes and failures (Liu & Kaplan, 1999; Thomson, 1998). Furthermore, Wiklund et al. (2010) found that girls tend to adapt to and live up to the needs and expectations of others. In another study, the girls tended to use more passive, avoidant coping strategies compared to boys, based on the misconception that active coping implies a heightened risk for failure and that therefore the avoidance of dealing with the stressor spares them from disappointment (Liu & Kaplan, 1999).Yet another explanation is that they are more mature at this period of life than boys and thus experience life as more serious and demanding (Murberg & Bru, 2004). Gender differences in stress perception could also be due to differences in affiliate relationship patterns, as indicated by Feingold (1994). While women put more emphasis on interpersonal relationships, men tend to focus more on personal autonomy. The “Cost of caring hypothesis” suggests that women and men are equally vulnerable to self-focused events, but women react stronger to events affecting others (Troisi, 2001). However, based on the results of the present thesis, reliable explanations of the gender differences found cannot be provided. Future research will hopefully be able to produce more conclusive findings on gender differences in regard to chronic stress perceptions and responses among adolescents and whether they are related to physiological dispositions, socialization or both. Future research might focus on giving a more conclusive picture about gender differences in chronic stress perception and responses and whether they represent the influence of physiological dispositions, socialization or both.
Limitations and methodological considerations Several limitations may have influenced the results of the included studies and therefore ought to be considered in the following section.

43
The first limitation relates to the samples used and the generalizability of the findings. Although the distribution of the sexes was relatively balanced in all samples, one should be cautious in generalizing the results to all high school students. The samples were drawn from only one geographic area, Stockholm, and thus represent a limited range of community and school environments. Moreover, since the investigations only involved students from high-ranked high schools, further investigations would be needed among adolescents from less elite high schools or with other socioeconomic backgrounds in order to draw conclusions for all adolescents. However, the proportion of the students reporting stress symptoms as well as the proportion of females who did so is similar to the results of nation-wide surveys (Ahrén, 2010; Bremberg, 2006; Socialstyrelsen, 2009). Furthermore, it is worth mentioning that, in the present thesis, only students who had chosen an academic educational high school track were investigated. Typically, adolescents who choose an academic high school track are confronted with higher academic demands and expectations, and due to the greater competition it can be more difficult for them to maintain their position as excellent students, compared to high school students from less demanding educational programs. Thus, the prevalence and consequences of chronic stress may very well differ between high school students who attend an academic educational track and those who attend a vocational educational track, as indicated by Samela-Aro and Tynkkynen’s (2012) findings on school burnout. Another limitation concerns the fact that all of the instruments for measuring stress and stress-related factors were based on self-report questionnaires. Self-reports may be affected by perceptual and cognitive biases (e.g., mood and social desirability). Moreover, studies among adolescents that are only based on self-report instruments can be especially problematic, because the respondents’ personality and identity development are still not complete, which may contribute to more fluctuating self-perceptions (Kroger, 2006; Marcia 2006). In future investigations, the use of more objective measures such as physiological indicators of stress (e.g., saliva cortisol and heart rate variability) and sleep parameters would be preferable. Yet, to develop sufficiently sensitive methods of capturing reliable associations between physiological indicators of stress and self-reported wellbeing and stress is still a challenge and thus a topic for future research. Study I had a cross-sectional design, which does not permit drawing any conclusions on causal relationships among the investigated variables or on the direction of the relation regarding chronic stress development. More longitudinal studies on this topic are therefore warranted in order to disentangle the potential causal relationships between variables. In study II and study III, access to baseline measures of academic achievement among the investigated participants would have been desirable. However, it seems safe to assume that all of the participating students had at least sufficiently good grades from primary school since they had met the requirements needed for entering elite high schools. Moreover, in study II access to some of the participant’s entrance grades permitted analyses that revealed no significant initial differences between the stress groups. Based on the findings in the present thesis, 15% of the adolescents suffered from chronic stress (study II). It cannot be shown for certain, of course, that these students will end up developing stress-related diseases, such as clinical burnout, in the long run. Conducting follow-up measurements at some point or otherwise gathering a more objective confirmation of the impact of their chronic stress after high

44
school could have provided useful information on the risks for subsequent stress-related health problems and diminished career prospects. The fact that some of the scales, such as the PBS scale and the SMBQ, have not been previously applied to such young respondents may also be limiting in that there does not exist any previous information on the basic measurement properties with which to draw comparisons. Moreover, recent research on the internal construct validity of the SMBQ among healthy and burnout adults came to the conclusion that a revised 18-item version of the SMBQ would correspond better with modern measurement standards (Lundgren-Nilsson et al., 2012). Nonetheless, in the present studies the reliabilities of the SMBQ measurements were tested and found to be satisfactory (Cronbachs α ≥ 0.80). However, for some scales the reliability was low. For example, in study II the Cronbach’s α for the control index was .30. Therefore, it was decided to refrain from applying the construct in the subsequent statistical analyses of the study. A possible reason for the low reliability of the applied scale could be that questions about perceived control were very general and abstractly formulated and thus did not match with the situation of adolescent high school students (e.g., I constantly need to learn new things in order to deal with my life.). However, in previous studies, perceived control has been successfully measured among adolescents by using more appropriately formulated items (Gillander-Gådin & Hammarström, 2000; Modin et al. 2011), and this should be continued in future research. Finally, the number of study variables was rather limited. Unfortunately, a number of potentially relevant variables fell outside the scope of the present investigation, such as stressful life events, extra work, school context, physical illness, peer rejection, cognitive deficits, and family-related issues, which could have had some influence on the present results. The attempt of the present thesis was to investigate stress in an otherwise healthy population of adolescent high school students. Thus, more severe psychiatric diagnoses, such as anxiety disorders or major depression, were not taken into account as potential explanatory or confounding factors when analyzing the data, which can be considered a limitation. However, the data analysis in study II and III was limited to participants with available final high school grades. Maybe it is therefore legitimate to make the conclusion that the fact that they had completed high school suggested that they did not suffer from any severe psychiatric conditions. Despite the limitations, the studies also have strengths, such as the relatively large sample sizes, high response rates, and use of objective measures of academic achievement based on final grades. Also, the prospective design of study II and study III contributed to the strength of the conclusions.
Implications for future research As stated in the beginning of the present thesis, an exhaustive investigation of a broad and complex research topic like chronic stress in a heterogeneous and complex population like adolescents would be impossible to accomplish within the scope of the present thesis. However, an attempt was made to provide some novel and exciting insights which may inspire other researchers to dig into and further this very important research area.
45
Experiencing the symptoms of social jetlag on a weekly basis, as occurred among the adolescents of this thesis, will eventually drain a person of the energy that is needed for overall functioning, health, and wellbeing. While social jetlag may be a fairly new concept, its prevalence and potential negative impact provide reason to dedicate more attention to it in the future within the research area of chronic stress among adolescents. The fact that sufficient recovery has been shown to be essential for preventing adults from clinical burnout, as shown by Söderström (2012), also highlights the importance of further research on regenerative processes, such as sleep and recovery among adolescents. Not only sleep but also other regenerative activities, such as contemplation, relaxation, and participation in cultural or physical activities, may be helpful in restoring the body’s energy and thus deserve consideration in future research attempts within this area. It was shown that chronic stress was associated with academic achievement at the end of high school (study II, III). For future research, it would be interesting to separately investigate the relative contribution of each of the three chronic stress/burnout dimensions, namely emotional exhaustion, physical exhaustion, and cognitive difficulties, to adolescents’ academic achievement. One might expect that cognitive difficulties and/or physical exhaustion might contribute most to the impairment of school performance. Hypotheses on this could be formulated and tested. The findings in the present thesis may also be useful for developing, estimating, and testing theories and hypotheses about the causes and effects of chronic stress. The results of the present thesis indicate that high perceived demands are associated with an increased risk for chronic stress (study I and study II). Providing a more exhaustive picture of both the origins of these demands, in terms of inner versus external demands, as well as of the domains within which these demands are perceived and their relative importance (like academic demands, physical appearance, social demands, economic demands etc.) would be an interesting task for future research. Moreover, the definition of social support was limited to supportive relationships in school only. Therefore, more thorough measurements of the impact of different aspects of social support on chronic stress perceptions would be of interest in future research. The question of whether chronic stress may not only have an impact on academic achievement but also increase the risk for negative health problems, such as clinical burnout later in life, remains. In order to provide an answer to this important question, longitudinal research is needed. Following the same individuals over the course of several years, for example, through high school and into adulthood, may provide an answer to that question. Future research could further build upon the findings of this thesis through a qualitative research approach. An investigation of the factors that serve to protect individuals from experiencing chronic stress in high school would be interesting. Interviews of stress-resilient adolescents could provide useful information for chronic stress prevention. The question of whether chronically stressed adolescents differ in their appraisal and/or coping attempts when facing a demanding situation compared to non-stressed adolescents could be tested by means of an experimental design. Moreover, it would be interesting to see if self-esteem might moderate stress reactivity or coping strategies. To investigate the importance of other personality aspects, such as perfectionism or obsessive–compulsive personality disorder, would also be of interest when examining chronic stress among adolescents. The focus in the present thesis was exclusively on individual characteristics. Yet, the context within which individuals behave, study, and live certainly also influences their wellbeing. For example,
46
previous studies have taken the school setting into account when studying adolescent stress and psychosomatic health (Modin et al., 2011; Modin & Östberg, 2009; Salmela-Aro et al., 2008) and found that having a positive school climate promoted health and decreased the risk for stress-related health problems. Other contextual factors which probably play a crucial role for adolescents’ stress perception include the family context and the socioeconomic context. It remains for future research to take such factors into consideration when investigating chronic stress among adolescents. In short, hopefully, research on chronic stress among adolescents is “to be continued.” When it comes to chronic stress prevention among adolescents, more scientifically satisfactory research attempts are called for, as indicated below.
Practical implications – preventing chronic stress among adolescents If stress-related problems during adolescence are dismissed as a normal part of maturation, there is a risk that young people will not receive the help they actually need. The results of the present thesis indicate that there is a critical need to develop effective practical measures for minimizing chronic stress among adolescents. Several attempts to decrease stress among adolescents have been made (Harraldsson et al., 2008; Hampel, Meier & Kuemmel, 2008; deAnda, 1998; Yahav & Cohen, 2008). A natural setting for attempting to promote the health of as many adolescents as possible is school (Haraldsson, et al., 2008; Kimber, Sandell, & Bremberg, 2008). It not only provides good accessibility to adolescents but it is also appropriate because the stressors and demands perceived by students most often concern school-related issues (deAnda et al., 2000). In their meta-analysis on nineteen stress interventions in classroom settings, Kraag, Zeegers, Kok, Hosman, and Huijer-Abu-Saad (2006) came to the conclusion that school programs targeting stress management or coping skills were effective. In spite of the attempts, it has been pointed out that it is particularly difficult to develop interventions for adolescents (Frydenberg et al., 2004; SBU, 2010). SBU’s (2010) review on programs that aim at preventing young people from experiencing stress and mental ill-health found that the effectiveness of the programs either could not be backed by more than limited scientific evidence or was supported by only minor effects. The systematic development, implementation, and evaluation of stress treatment programs by means of randomized controlled trials with systematic follow-up measurements are rare. Such an attempt to include implementation has been made by my research group at the Stress Research Institute where a chronic stress prevention program was developed within the project “Stress prevention in high school” in 2009–10 (Perski et al., 2010). Within the project, my colleague Giorgio Grossi and I developed and pilot-tested a stress-prevention program among high school students who suffered from severe stress symptoms as indicated by the SMBQ. The program was designed as a group intervention. The components of the program were based on the then available findings from the present thesis in combination with insights from clinical psychological work with adult burnout patients and current relevant treatment findings and manuals (Grossi, 2008; Hayes, Strohsal, & Wilson, 1999; Livheim, 2004; Makower, 2008; Söderström, 2007). Due to the fairly high dropout rates among the participating high school students, it has been problematic to scientifically evaluate the program’s treatment effects. The program is still in development and more research is needed in
47
order to confirm its effectiveness. In the following section, some reflections on chronic stress prevention based on the findings of the present thesis and the experiences from the intervention pilot-project are provided. The program was developed based on the theory and several treatment elements from Cognitive Behavioral Therapy (CBT) and Acceptance and Commitment Therapy (ACT). It consisted of elements such as psychoeducation about stress and sleep, values work and committed action, mindfulness, assertiveness training, and positive diary to enhance self-esteem, just to name a view. The inclusion of psychoeducation aimed to provide the participants with knowledge about stress in general and training in recognizing individual stress-evoking situations, stress-evoking thoughts, physiological stress reactions, stress behaviors (i.e., adequate vs. inadequate coping strategies), and stress symptoms (Grossi, 2008). ACT provides a promising approach for equipping individuals with a broader and more flexible behavior repertoire even when facing challenging unforeseen events and high perceived demands, which was a main purpose of the prevention program (Hayes et al., 1999; Livheim, 2004). Thus, participants were asked to define their personal values, commit to them, and try to live up to them despite any perceived barriers they may have. Because of the stress buffering effect of social support, the participants were also provided with assertiveness training. Through this, the participants learned how to adequately deal on their own with the aversive feelings and thoughts that arise from perceived demands, as they also became more skilled in how to mobilize social support by communicating their needs, worries, and feelings of vulnerability to their social network. They were taught that it is not only okay to show vulnerability and ask for help, it is also necessary and appropriate to do so in the face of insuperable barriers and challenges. Of course, in order to do so, a secure social network that consists of accessible adults and supportive relationships is needed. Moreover, it can also be helpful to focus on the present moment and envision situations more objectively in order to see future events and challenging situations, such as academic exams, in a more neutral light rather than as unmanageable threats and potential catastrophes. Therefore, mindfulness training, which in fact has been found to have a positive impact on performance (Shao & Skarlicki, 2009), also was incorporated in the intervention. In addition, the students were also given the opportunity to learn some body-consciousness and breathing techniques, which have been found to be useful in the treatment of adult burnout patients (Ristiniemi). To increase adolescents’ global self-esteem and to help them maintain their sense of self-worth even when difficulties arise in life (Baumeister et al., 2003; Rosenberg, 1972) was also identified as an important aspect in chronic stress prevention. Self-esteem is indicative of a person’s self-efficacy, which, according to Bandura (1997, 2000), provides the person with awareness about her own capability of mastering certain situations. Therefore, focusing on increasing adolescents’ self-efficacy, by giving them the tools to help them realize that they are capable of successfully and autonomously solving problems or difficulties, may not only boost their self-esteem, but also help young people to appraise demands as less threatening or more manageable. In other words, adolescents have to be given the opportunity to experience that they can master challenges, which increases their self-efficacy and self-esteem. Within the program, the participants were invited to use a CBT-based method, called positive diary, developed by Makower (2008).
48
Finally, my colleague and I were especially surprised by the participants’ astonishment when they learned about the importance of sleep and sufficient recovery in order to prevent stress, stay healthy, and perform well in school. Within the program, the participants learned about sleep in general, the importance of adequate sleeping routines, and how to promote their sleep (Grossi, 2008; Söderström, 2007). Undoubtedly, adequate and regular sleep timing is an important factor when it comes to chronic stress prevention among adolescents. However, to simply increase adolescents’ awareness of the importance of regular and sufficient sleep and recovery is probably not enough. In previous research, late chronotypes in particular found it difficult to implement earlier and regular bed and rise times (Digdon, 2010; Zimmermann, 2011). Also, the present findings that social jetlag was associated with severe stress symptoms and worse academic achievement emphasize the importance of finding effective methods to promote behavior changes that support sufficient recovery and regular sleep. Other alternatives for accommodating adolescents’ circadian rhythms and thereby counteracting the risk for social jetlag and associated chronic stress may be to delay school start times or to add more flexibility to the organization of the school curriculum (Hsu, Gau, Shang, Chiu, & Lee, 2012; Mecacci & Rocchetti, 1998; Owens, Belon, & Modd, 2010; Wolfson & Carskadon, 2003). Of course, it is not possible to develop a group intervention program which fits the individual needs and circumstances of all participants, but, hopefully, it will turn out to have provided the participants with useful insights and practical skills for coping better with stress. To prove this is a mission for future research.

49
Concluding remarks
The fact that serious stress symptoms were reported by more than 30% of the investigated sixteen-year old high school students indicates that this phenomenon should not be simply regarded as a passing occurrence within the normal storm-and-stress period but should, rather, be seen as the first phase of a potentially prolonged state. Besides the negative consequences it might have on health in the long run, chronic stress among adolescents has more immediate consequences, for example, on academic achievement, which has a direct impact on a young person’s future chances of being accepted into a quality line of education. Moreover, academic achievement is not only impaired by chronic stress but also by social jetlag, which refers to the effects of major shifts in bedtimes between school days and weekends. Global self-esteem, perceived demands, sleep/recovery, and social support are considered to be the most relevant factors in understanding adolescents’ chronic stress, and, thus, their improvement should be seen as an essential aim in chronic stress prevention programs for adolescents.
50
References
Ahrén, J.C. (2010). Skolan och ungdomars psychosociala hälsa [School and adolescents’ psychosocial health]. Stockholm: Socialdepartementet, SOU 2010:80. Aldwin, C.M. (2007). Stress, coping and development. An integrative perspective. (2nd ed.) Guilford Press. deAnda, D. (1998). The evaluation of a stress management program for middle school adolescents. Child and
Adolescent Social Work Journal, 15 (1), 73-84. deAnda, D., Baroni, S., Boskin, L., Buchwald, L., Morgan, J., Ow, J., Siegel Gold, J., & Weiss, R. (2000).
Stress, stressors and coping among high school students. Children and Youth Services Review, 22 (6), 441-463.
Arnett, J.J. (1999). Adolescent storm and stress, reconsidered. American Psychologist, 54 (5), 317-326. Arnett, J.J. (2000). Emerging adulthood: A theory of development from the late teens through the twenties.
American Psychologist, 55(5), 469–480. Arnsten, A.F. (2009). Stress signaling pathways that impair prefrontal structure and function. Nature Reviews
Neuroscience, 10 (6), 410-422. Armon, G., Shirom, A., Shapira, I., & Melamed, S. (2008). On the nature of burnout-insomnia relationships: A
prospective study of employed adults. Journal of Psychosomatic Research, 65 (1), 5-12. Auger, R.R., Burgess, H.J., Dierkhising, R.A., Sharma, R.G., & Slocumb, N.L. (2011). Light exposure among
adolescents with delayed sleep phase disorder: a prospective cohort study. Chronobiology International, 28 (10), 911-920.
Avison, R., & McAlpine, D.D. (1992). Gender differences in symptoms of depression among adolescents. Journal of Health and Social Behavior, 33 (2), 77-96.
Bandura, A. (1997). Self-efficacy. The exercise of control. New York: Freeman and Company, Inc. Bandura, A. (2000). Self-efficacy. In A.E. Kazdin (Ed.), Encyclopedia of psychology 7 (pp. 212-213).
Washington, DC, US: American Psychological Association. Basow, S.A., & Rubin, L.R. (1999). Gender influences on adolescent development. In N.G. Johnson, M.C.
Roberts & J. Worell (Eds.), Beyond appearance: A new look at adolescent girls (p25-52). Washington DC: APA.
Baumeister, R.F., Campbell, J.D., Krueger, J.I., & Vohs, K.D. (2003). Does high self-esteem cause better performance, interpersonal success, happiness, or healthier lifestyles? Psychological science in the public interest, 4 (1), 1-44.
Beebe, D.W., Rose, D., & Amin, R. (2010). Attention, learning, and arousal of experimentally sleep-restricted adolescents in a simulated Classroom. Journal of Adolescent Health, 47, 523-525.
Besoluk, S., Önder, I., & Deveci, I. (2011). Morning-evening preferences and academic achievement of university students. Chronobiology International, 28 (2), 118-125.
Bernert, R., Merrill, K., Braithwaite, S., VanOrden, K., & Joiner, T. (2007). Family life stress and insomnia symptoms in a prospective evaluation of young adults. Journal of Family Psychology, 21(1), 58-66.
Birndorf, S., Ryan, S., Auinger, P., & Aten, M. (2005). High self-esteem among adolescents: Longitudinal trends, sex differences, and protective factors. Journal of Adolescent Health, 37, 194-201.
Blom, V. (2011). Striving for self-esteem: Conceptualization and role in burnout. Doctoral thesis, Department of Psychology, Stockholm university.
Blom, V. (2012). Contingent self-esteem, stressors and burnout in working women and men. Work: A Journal of Prevention, Assessment and Rehabilitation, 43 (2), 123-131.
Brandalize, M., Felden Pereira, R., Leite, N., Lorenzi Filho, G., & Mazzilli Louzada, F. (2011). Effect of morning school schedule on sleep and anthropometric variables in adolescents: a follow-up study. Chronobiology International, 28 (9), 779-785.

51
Bremberg, S. (2006). Ungdomar, stress och psykisk ohälsa - Analyser och förslag till åtgärder. [Adolescents, stress and mental health – Analysis and proposals for action] Stockholm: Socialdepartementet, SOU 2006:77. Available: http://www.regeringen.se/sb/d/108/a/67472
Brolin-Låftman, S., & Modin, B. (2012). School-performance indicators and subjective health complaints: are there gender differences?. Sociology of Health and Illness, 34 (4), 608-625.
Brolin-Låftman, S., & Östberg, V. (2006) The pros and cons of social relations: an analysis of adolescents’ health complaints. Social Science & Medicine, 63 (3), 611-623.
Buboltz, W.C., Brown, F., & Soper, B. (2001). Sleep habits and patterns of college students: a preliminary study. Journal of American college health, 50 (3),131-135.
Butler, G. (1993). Definitions of stress. Occasional Paper Series RCGP, 61, 1-5. Butler, R.J., & Gasson, S.L. (2005). Self esteem/Self concept scales for children and adolescents: A review.
Child and Adolescent Mental Health, 10 (4), 190-201. Byrne, D.G., Davenport, S.C., & Mazanov, J. (2007). Profiles of adolescent stress: The development of the
adolescent stress questionnaire (ASQ). Journal of Adolescence, 30, 393-416. Campbell, J. D., & Lavallee, L. F. (1993). Who am I? The role of self-concept confusion in understanding the
behavior of people with low self-esteem. In R. F. Baumeister (Ed.), Self-esteem: The puzzle of low self-regard (pp. 1 – 20). NY: Plenum.
Cannon, W.B. (1922). Bodily changes in pain, hunger, fear and rage. An account of recent researches into the function of emotional excitement. New York and London D. Appleton and Company.
Chapman, P.L., & Mullis, R.L. (1999). Adolescent coping and self-esteem. Child study journal 29 (1), 69-78. Cherniss, C. (1980). Staff Burnout. Job stress in the human services. Sage Publications, Beverly Hills, London. Crocker, J., & Wolfe, C.T. (2001). Contingencies of self-worth. Psychological Review, 108 (3), 593-623. Crocker, J. (2002). The costs of seeking self-esteem. Journal of Social Issues, 58(3), 597-615. Curcio, G., Ferrara, M., & DeGennaro, L. (2006). Sleep loss, learning capacity and academic performance. Sleep
Medicine Reviews, 10, 323-337. Dagys, N., McGlinchey, E.L., Talbot, L.S., Kaplan, K.A., Dahl, R.E., & Harvey, A.G. (2012). Double trouble?
The effects of sleep deprivation and chronotype on adolescent affect. Journal of Child Psychology and Psychiatry, 53 (6), 660-667.
Dahl, R.E., & Lewin, D.S. (2002). Pathways to adolescent health: sleep regulation and behavior. Journal of Adolescent Health, 31, 175-184.
Dalman, C., & Wicks, S. (2006).Vilka grupper söker vård inom psykiatrin? En uppföljningsstudie av psykiatrisk vård och beroende vård i Stockholms län 1998-2005 [Who is seeking psychiatric care? A follow-up study on psychiatric care and care of addicts in Stocholm between 1998 and 2005]. Rapport nr. 6. Epidemiologiska Enheten, Avdelningen för socialmedicin och epidemilogi, Centrum för folkhälsa, Stockholms läns landsting.
Dedovic, K., Wadiwalla, M., Engert, V., & Pruessner, J.C. (2009). The role of sex and gender socialisation in stress reactivity. Developmental Psychology, 45 (1), 45-55.
Digdon, N. (2010). Circadian preference and college students’ beliefs about sleep education. Chronobiology International, 27 (2), 297-317.
Dumont, M., & Provost, M.A. (1998). Resilience in adolescents: Protective role of social support, coping strategies, self-esteem, and social activities on experience of stress and depression. Journal of Youth and Adolescence, 28 (3), 343-363.
Eccles, J., Brown, B.V., & Templeton, J. (2008). A development framework for selecting indicators of well-being during the adolescent and young adult years. In Brown B.V. (eds), Key indicators of child and youth well-being (pp.197-236). Lawrence Erlbaum Associates, New York.
Ekstedt, M. (2005). Burnout and Sleep. Doctoral thesis, Department of Public Health Sciences. Karolinska Institute, Stockholm.
Ekstedt, M., Söderström, M., Åkerstedt, T., Nilsson, J., & Sondergaard, H.P., & Perski, A. (2006). Disturbed sleep and fatigue in occupational burnout. Scandinavian Journal of Work Environment and Health, 32 (2), 121-131.
Feingold, A. (1994). Gender differences in personality: a meta-analysis. Psychological Bulletin, 116, 429-456. Folkow, B. (1997). Physiological aspects of the “defence” and “defeat” reactions. Acta Physiologica
Scandinavica Supplementum, 640, 34-37. Freudenberger, H.J. (1974). Staff burn-out. Journal of Social Issues, 30, 159-165.
52
Friberg, P., Hagquist, C., & Osika, W. (2012). Self-perceived psychosomatic health in Swedish children, adolescents and young adults: an internet-based survey over time. BMJ Open; 2:e000681.
Frydenberg, E. (2002). Adolescent coping. Advances in Theory, Research and Practice. Taylor & Francis. Frydenberg, E., Lewis, R., Bugalski, K., Cotta, A., McCarthy, C., & Luscombe-Smith, N., et al. (2004).
Prevention is better than cure: Coping skills training for adolescents at school. Educational Psychology in Practice, 20, 117-134.
Fuligni, A., & Hardway, C. (2006). Daily variation in adolescents’ sleep, activities, and psychological well-being. Journal of Research on Adolescence, 16 (3), 353-378.
Gillander-Gådin, K., & Hammarström, A. (2000). School-related health - a cross-sectional study among young boys and girls. International Journal of Health Services, 30 (4), 797-820.
Gomes, A.A., Tavares, J., & de Azevedo, M.H. (2011). Sleep and academic performance in undergradutates: a multi-measure, multi-predictor approach. Chronobiology International, 28 (9), 786-801.
Grossi, G. (2008). Hantera din stress med kognitiv beteendeterapi. [Cope with your stress with CBT]. Viva Grossi, G., Perski, A., Evengård, B., Blomkvist, V., & Orth-Gomér, K. (2003). Physiological correlates of
burnout among women. Journal of Psychosomatic Research, 55, 309-316. Gustafsson, J.-E., Allodi, M., Alin.-Åkerman, B., Eriksson, C., Eriksson, L., & Fischbein, S., et al. (2010),
School, Learning and Mental Health. A systematic review. Health committee, The Royal Swedish Academy of Sciences. Available: http://www.kva.se
Hagquist, C. (2009). Psychosomatic health problems among adolescents in Sweden – are the time trends gender related? European Journal of Public Health, 19 (3), 331-336.
Hagquist, C. (2010). Discrepant trends in mental health complaints among younger and older adolescents in Sweden: An analysis of WHO data 1985-2005. Journal of Adolescent Health, 46, 258-264.
Hall, G.S. (1904). Adolescence: Its psychology and its relation to physiology, anthropology, sociology, sex, crime, religion, and education. Englewood Cliffs, NJ: Prentice-Hall.
Hallsten, L., Bellaagh, K., & Gustafsson, K. (2002). Utbränning i Sverige – en populationsstudie. [Burnout in Sweden – a population study]. Arbete och Hälsa, Arbetslivsinstitutet (Nr. 2002:6).
Hallsten, L., Josephson, M., & Torgén, M. (2005). Performance-based self-esteem: A driving force in burnout processes and its assessment. Arbete och Hälsa. Arbetslivsinstitutet [National Institute of Working Life], Nr.2005:4.
Hallsten, L., Voss, M., Stark, S., Josephson, M., & Vingård, E. (2011). Job burnout and job wornout as risk factors for long-term sickness absence. Work, 38, 181-192.
Hampel, P., Meier, M., & Kuemmel, U. (2008). School-based stress management training for adolescents: longitudinal results from experimental study. Journal of Youth and Adolescence, 37, 1009-1024.
Hankin, B.L., Mermelstein, R., & Roesch, L. (2007). Sex differences in adolescent depression: Stress exposure and reactivity models. Child Development, 78 (1), 279-295.
Haraldsson, K. (2010). Buffra stress i riktning mot välbefinnande. Interventionsstudier och utforskande studier med fokus på unga flickor. [Buffering stress towards well-being. Interventive and explorative studies with focus on adolescent girls.] Doctoral thesis, University of Gothenburg, Sahlgrenska Academy.
Haraldsson, K.S., Lindgren, E-C.M., Fridlund, B.G., Baigi, A.M., Lydell, M.C., & Marklud, B.R. (2008). Evaluation of a school-based health promotion program for adolescents aged 12-15 years with focus on well-being related to stress. Public Health, 122, 25-33.
Harter, S. (1993). Causes and consequences of low self-esteem in children and adolescents. In RF. Baumeister (Ed.), Self-esteem. The puzzle of low self-regard (pp. 87-116). NY: Plenum.
Hayes, S.C., Strohsal, K.D., & Wilson, K.G. (1999). Acceptance and Commitment Therapy. An experiential approach to behavior change. The Guliford Press. New York London.
Hjern, A., Alfven, G., & Östberg, V. (2007). School stressors, psychological complaints and psychosomatic pain. Acta Paediatrica, 97, 112-117.
Howell, A.J., Jahrig, J.C., & Powell, R.A. (2004). Sleep quality, sleep propensity and academic performance. Perceptual and Motor Skills, 99 (2), 525-535.
Hsu, C-Y., Gau, S.S-F., Shang, C-Y., Chiu, Y-N., & Lee, M-B. (2012). Associations between chronotypes, psychopathology, and personality among college students. Chronobiology International, 29 (4), 491-501.
Huan, V.S., Lay See, Y., Ang, R.P., & Wan Har, C. (2008). The impact of adolescent concerns on their academic stress. Educational Review, 60 (2), 169-178.

53
Ipsiroglu, O.S., Fatemi, A., Werner, I., Paditz, E., & Schwarz, B. (2002). Self-reported organic and nonorganic sleep problems in schoolchildren aged 11 to 15 years in Vienna. Journal of Adolescent Health, 31, 436-422.
Johnson, M. (1997). On the dynamics of Self-Esteem. Empirical validation of Basic self-esteem and Earning self-esteem. Doctoral thesis, Department of Psychology, Stockholm university.
Johnson, M., & Forsman, L. (1995). Competence strivings and self-esteem: an experimental study. Personality and. Individual Differences, 19 (4), 417-430.
Jonsdottir, I.H., Nordlund, A., Ellbin, S., Ljung, T., Gilse, K., Währborg, P., & Wallin, A. (2012). Cognitive impairment in patients with stress-related exhaustion. Stress, 1-10.
KFA, Karolinska Folkhälsoakademi (2009). Barnen i folkhälsorapporterna. Hur mår barn och unga vuxna i Stockholms län? [About children in public health reports. How are children and adolescents in Stockholm?] Research Report, 2009:02. Karolinska Institutet
Kaplan, D.S., Liu, R.X., & Kaplan, H.B. (2005). School related stress in early adolescence and academic performance three years later: the conditional influence of self-expectations. Social Psychology of Education, 8, 3-17.
Karasek, R., & Theorell, T. (1990). Healthy work: stress, productivity, and the reconstruction of working life. New York, NY: Basic Books.
Kecklund & Åkerstedt, (1992). The psychometric properties of the Karolinska Sleep Questionnaire. Journal of Sleep Research, 1 (suppl 1) 113.
Kelly, W.E., Kelly, K.E., & Clanton, R.C. (2001). The relationship between sleep length and grade-point average among college students. College Student Journal, 35 (1), 84-87.
Kernis, M. H. (2006). Self-esteem, issues and answers. A sourcebook of current perspectives. New York: Psychology Press.
Keski-Rahkonen, A., Kaprio, J., Rissanen, A., Virkkunen, M., & Rose, R.J. (2003). Breakfast skipping and health-compromising behavios in adolescents and adults. European Journal of Clinical Nutrition, 57, 842-853.
Kimber B., Sandell R., & Bremberg S. (2008). Social and emotional training in Swedish classrooms for the promotion of mental health: results from an effectiveness study in Sweden. Health Promotion International, 23, 134-143.
Kivimäki, M., & Kalimo, R. (1996). Self-esteem and the occupational stress process: testing two alternative models in a sample of blue-collar workers. Journal of Occupational Health Psychology, 1 (2), 187-196.
Kling, K.C., Shibley Hyde, J., Showers, C.J., & Buswell, B.N. (1999). Gender Differences in Self-Esteem: A Meta-Analysis. Psychological Bulletin, 125 (4), 470-500.
Kraag, G., Zeegers, M.P., Kok, G., Hosman, C., & Huijer Abu-Saad, H. (2006). School programs targeting stress management in children and adolescents: A meta-analysis. Journal of School Psychology, 44, 339-472.
Kroger, J. (2006). Identitetsutvecklingen i de tidiga vuxenåren [Identity development in young adults]. In A. Frisén & P. Hwang (Eds.), Ungdomar och Identitet. [Adolescents and Identity]. Blåvita Serien. Natur och Kultur.
KVH Kungliga Vetenskapsakademiens Hälsoutskott [The Royal Swedish Academy of Science] (2010). Barns och ungdomars psykiska hälsa i Sverige. En systematisk litteraturöversikt med tonvikt på förändring över tid [children’s and adolescents’ mental health in Sweden. A systematic review of the literature with focus on change over time]. Research report. Available: http://kva.episerverhotell.net/sv/
Langstedt, E., Asplund, K., & Gillander-Gådin, K. (2009). Understanding adolescent mental health: The influence of social processes, doing gender and gendered power relations. Sociology of Health and Illness, 31(7), 962-978.
Lazarus, R.S. (1993). From psychological stress to the emotions: A history of changing outlooks. Annual Review of Psychology, 44, 1-21.
Lazarus, R.S. (1999). Stress and emotion. A new synthesis. Springer Publishing Company Inc. Lazarus, R.S., & Folkman, S. (1984). Stress, appraisal, and coping. New York: Springer. Levi, L. (2005). Stress – en översikt. Internationella och folkhälsoperspektiv [Stress - an overview. An
international and public health perspective]. In R. Ekman & B. Arnetz (Eds), Stress. Molekylerna-individen-Organisationen– Samhället [Stress. Molecules – the individual – the organisation – society] (pp. 56-71). Liber: Stockholm.
54
Lidwall, U. (2010). Långtidssjukskrivna. Beskrivande statistik 1999-2009: kön, ålder, arbetsmarknadsstatus, sjukskrivningslängd, och diagnospanorama [Individuals on long-term sickleave. Descriptive statistics 1999-2009: sex, age, working status, duration of sickness absence and medical diagnoses] Socialförsäkringsrapport [Social insurance report] 2010:11. Stockholm, Försäkringskassan.
Lien, L. (2006). Is breakfast consumption related to mental distress and academic performance in adolescents? Public health Nutrition, 10 (4), 422-428.
Lindblom, K.M., Linton, S.J., Fedeli, C., & Bryngelsson, I-L. (2006). Burnout in the working population: Relations to psychosocial work factors. International Journal of Behavioral Medicine, 13(1),51-59.
Liston, C., McEwen, B.S., & Casey, B.J. (2008). Psychosocial stress reversibly disrupts prefrontal processing and attentional control. PNAS, Proceedings of the National Academy of Sciences 103( 3), 912-917.
Liu, X., & Kaplan, H.B. (1999). Explaining gender differences in symptoms of subjective distress in young adolescents. Stress Medicine, 15, 41-51.
Livheim, F. (2004). Acceptance and Commitment Therapy i skolan - att hantera stress. En randomiserad, kontrollerad studie. [Acceptance and Commitment Therapy in school – coping with stress. A RCT study] Psykologexamensuppsats, Uppsala University.
Locke, E.A., McClear, K., & Knight D. (1996). Self-esteem and work. International Review of Industrial/Organizational Psychology, 11, 1-32.
Lund, H.G., Reider, B.D., Whiting, A.B., & Prichard, J.R. (2010). Sleep patterns and predictors of disturbed sleep in a large population of college students. Journal of Adolescent Health, 46, 124-132.
Lundberg, U. (2005). Stress hormones in health and illness: The roles of work and gender. Psychoneuroendocrinology, 30 (10), 1017-1021.
Lundgren-Nilsson, Å., Jonsdottir, I.H., Pallant, J., & Ahlborg, G. (2012). Internal construct validity of the Shirom-Melamed Burnout Questionnaire (SMBQ). Public Health, 12, 1-8.
Lupien, S.J., MeEwan, B.S., Gunnar, M.R., & Heim, C. (2009). Effects of stress throughout the lifespan on the brain, behavior and cognition. Nature Reviews Neuroscience, 10, 434-445.
Major, B., Barr, L., Zubek, J., & Babey, S. H. (1999). Gender and self-esteem: A meta-analysis. In W. B. Swann, J. H. Langlois, & L. A. Gilbert (Eds.) Sexism and stereotypes in modern society: The gender science of Janet Taylor Spence (pp. 223–253). Washington, DC: American Psychological Association.
Makower, I. (2008). Att bygga upp självkänslan med hjälp av KBT [How to increase self-esteem with CBT]. Psykisk Hälsa [Mental health], 2 (28), 22-34. Available: http://www.makowerpsykologi.se/forskning/kbt-vid-sviktande-sjalvkansla
Marcia, J. (2006). Jagidentitet och objektrelationer [Identity and object relations]. In A. Frisén & P. Hwang, (Eds..), Ungdomar och Identitet [Adolescents and Identity]. Blåvita Serien. Natur och Kultur.
Marin, M-F., Lord, C., Andrews, J., Juster, R-P., Sindi, S., Arsenault-Lapierre, G., et al. (2011). Chronic stress, cognitive functioning and mental health. . Neurobiology of Learning and Memory, 96, 583-595.
Marsh, H.W., & Hau, K-T., (2003). Big-Fish-Little-Pond Effect on academic self-concept. A cross- cultural (26-country) test of the negative effects of academically selective schools. American Psychologist, 58 (5), 364-376.
Maslach, C. (2001). What have we learned about burnout and health? Psychology and Health, 16 (5), 607-611. Maslach, C., & Jackson, S.E. (1981). The measurement of experienced burnout. Journal of Occupational
Behaviour, 2, 99-113. Maslach, C., & Leiter, M.P. (1997). The truth about burnout. San Fransico: Jossey-Bass. Maslach, C., Schaufeli, W.B., & Leiter, M.P. (2001). Job burnout. Annual Review of Psychology, 52, 397-422. McEwen, B.S., & Stellar, E. (1993). Stress and the Individual: Mechanisms leading to disease. Archives of
Internal Medicine, 153 (18), 2093-2101. McEwen, B.S. (2006). Protective and damaging effects of stress mediators: central role of the brain. Dialogues
Clinical Neuroscience, 8 (4), 367-381. Mecacci, L., & Rocchetti, G. (1998). Morning and evening types: stress-related personality aspects. Personality
and Individual Differences, 25, 537-542. Meijer, A.M., Habekothe, H.T., & Van Den Wittenboer, G.L. (2000). Time in bed, quality of sleep and school
functioning of children. Journal of Sleep Research, 9, 145–153. Melamed, S., Kushnir, T., & Shirom, A. (1992). Burnout and Risk Factors for Cardiovascular Diseases.
Behavioral medicine. An interdisciplinary journal of research and practice, 18, 53-60.
55
Melamed, S., Shirom, A., Toker, S., Berliner, S., & Shapira, I. (2006). Burnout and Risk of Cardiovascular Disease: Evidence, Possible Causal Paths, and Promising Research Directions. Psychological Bulletin, 132 (3), 327-353.
Modin, B., & Östberg, V. (2009). School climate and psychosomatic health: a multilevel analysis. School Effectiveness and School Imporovement: An International Journal of Research, Policy and Practice, 20 (4), 433-455.
Modin, B., Östberg, V., Toivanen, S., & Sundell, K. (2011). Psychosocial working conditions, school sense of coherence and subjective health complaints. A multilevel analysis of ninth grade pupils in the Stockholm area. Journal of Adolescence, 34 (1), 129-139.
Moksnes, U.K., Moljord, I.E., Espnes, G.A., & Byrne, D.G. (2010). The association between stress and emotional states in adolescents: The role of gender and self-esteem. Personality and Individual Differences, 49, 430-435.
Mortimer, J.T., Zimmer-Gembeck M.J., Holmes M., & Shanahan, M.J. (2002). The process of occupational decision making: Patterns during the transition to adulthood. Journal of Vocational Behavior, 61, 439-65.
Murberg, T.A., & Bru, E. (2004). School-related stress and psychosomatic symptoms among Norwegian adolescents. School Psychology International, 25 (3), 317-332.
Nabkasorn, C., Miyai, N., Sootmongkol, A., Junprasert, S., Yamamoto, H., Arita, M., & Miyashita, K. (2005). Effects of physical exercise on depression, neuroendocrine stress hormones and physiological fitness in adolescent females with depressive symptoms. European Journal of Public Health, 16 (2), 179-184.
Nounopoulos, A., Ashby, J.S., & Gilman, R. (2006). Coping resources, perfectionism and academic performance among adolescents. Psychology in the Schools, 4 (5), 613-622.
Ollfors, M., & Andersson, S.I. (2007). Ability of stress, sense of control, and self-theories to predict Swedish high school students’ final grades. Educational Research and Evaluation, 13 (2), 143-169.
Östberg, V. (2001). Hälsa och välbefinnande [Health and wellbeing]. In: Barns och ungdomars välfärd [children’s and adolescents’ welfare]. Stockholm: Socialdepartementet, SOU 2001:55.
Owens, J.A., Belon, K., & Moss, P. (2010). Impact of delaying school start time on adolescent sleep, mood, and behavior. Archives of Pediatrics and Adolescent Medicine, 164 (7), 608-614.
Perski, A. (2006). Ur balans. Bonnier Fakta. Perski, A., Schraml, K., Grossi, G., Makower, I., & Ivarsson, M., (2010). Intervention mot stress i gymnasiet.
En slutrapport avseende projektet FP308 för Länsförsäkringars Forskningsfond. Research Report, Stressforskningsinstitutet, Stockholms universitet.
Pilcher, J.J., Ginter, D.R., & Sadowsky, B. (1997). Sleep quality versus sleep quantity: relationships between sleep and measures of health, well-being and sleepiness in college students. Journal of Psychosomatic Research, 42 (6), 583-596.
Pines, A.M., & Aronson, E. (1988). Career burnout: causes and cures. New York. Free Press. Pines, A.M., & Keinan, G. (2005). Stress and burnout: The significant difference. Personality and Individual
Differences, 39, 625-635. Pyszczynski, T., Greenberg, J., Solomon, S., Arndt, J., & Schimel, J. (2004). Why do people need self-esteem?
A theoretical and empirical review. Psychological Bulletin, 130 (3), 435-468. Rabe-Hesketh, S., & Skrondal, A. (2008). Multilevel and longitudinal modeling using Stata. Stata Press. Randler, C. (2011). Age and gender differences in morningness-eveningness during adolescence. Journal of
Genetic Psychology, 172 (3), 302-308. Rector, N.A., & Roger, D. (1997). The stress buffering effects of self-esteem. Personality and Individual
Differences, 23(5), 799-808. Renstig, M., & Sandmark, H. (2005), Kvinnors sjukskrivning – riskfaktorer för långtidssjukskrivning bland
kvinnliga högre tjänstemän [Women’s sickness absence – risk factors for long term sickness absence among female white-collar workers in high positions]. Research Report, Karolinska Institutet, Institutionen för folkhälsovetenskap.
Rhee, H., Holditch-Davis, D., & Miles, M.S. (2005). Patterns of physical symptoms and relationships with psychosocial factors in adolescents. Psychosomatic Medicine, 67, 1006-1012.
Ristiniemi, H. Grounding and breathing exercises. For information: www.stressmottagning.nu Roberts, R.E., Roberts, C.R., & Duong, H.T. (2009). Sleepless in adolescence: Prospective data on sleep
deprivation, health and functioning. Journal of Adolescence, 32, 1045-1057.
56
Robins R.W., & Trzesniewski, K.H. (2005). Self-esteem development across the lifespan. Current Directions in
Psychological Science, 14 (3), 158-162. Roenneberg, T., Wirz-Justice, A., & Merrow, M. (2003). Life between clocks: Daily temporal patterns of human
chronotypes. Journal of Biological Rhythms, 18 (1), 80-90. Rosenberg, M. (1972). Society and the adolescent self image. Princeton, NJ University Press. Rosenberg, M., Schooler, C., & Schoenbach, C. (1989). Self-esteem and adolescent problems: Modeling
reciprocal effects. American Sociological Review, 54(6), 1004-1018. Ruble, D.N., Greulich, F., Pomerantz, E., & Gochberg, B. (1993). The role of gender-related processes in the
development of sex differences in self-evaluation and depression. Journal of Affective Disorders, 29, 97-128.
Rudolph, K.D. (2002). Gender Differences in Emotional Responses to Interpersonal Stress during Adolescence. Journal of Adolescent Health, 30, 3-13.
Sagatun, A., Sogaard, A.J., Bjertness, E., Selmer, R., & Heyerdahl, S. (2007). The association between weekly hours of physical activity and mental health: A three-year follow-up study of 15-16-year-old students in the city of Oslo, Norway. BMC Public Health, 7, 155-164.
Salmela-Aro, K., Kiuru, N., Pietikäinen, M., & Jokela, J. (2008). Does school matter? The role of school context in adolescents’ school related burnout. European Psychologist, 13 (1), 12-23.
Salmela-Aro, K., & Nurmi, J.E., (2007). Self-esteem during university studies predicts career characteristics 10 years later. Journal of Vocational Behavior, 70, 463-477.
Salmela-Aro, K., & Tynkkynen, L. (2012). Gendered pathways in school burnout among adolescents. Journal of Adolescence, 35, 929-939.
Sapolsky, R.M. (2004). Why zebras don’t get ulcer: the acclaimed guide to stress, stress-related diseases and coping. (3rd edition). Henry Holt and Company.
Sapolsky, R.M., Romero, L.M., & Munck, A.U., (2000). How do Glucocorticoids influence stress responses? Integrating permissive, suppressive, stimulatory, and preparative actions. Endocrine Reviews, 21 (1), 55-89.
Saxvig, I.W., Pallesen, S., Wilhelmsen-Langeland, A., Molde, H., & Bjorvatn, B. (2012). Prevalence and correlates of delayed sleep phase in high school students. Sleep medicine, 13, 193-199.
SBU Statens beredning för medicinsk utvärdering [Swedish Council on Health Technology Assessment] (2010). Methods to prevent mental ill-health in children. A systematic review. Research Report 202. Available: http://www.sbu.se/upload/Publikationer/Content0/1/Program_forebygga_psykisk_ohalsa_hos_barn.pdf
SCB, Statistiska centralbyrån [Statistics Sweden] (2007). Barns hälsa [Children’s health]. Living Conditions Report, 115.
SCB, Statistiska centralbyrån [Statistics Sweden] (2011). Barns sociala relationer [Children’s social relationships]. Living Conditions Report, 119.
SCB, Statistiska centralbyrån [Statistics Sweden] (2012). Barns upplevelser i skolan[Children’s experiences from school]. Living Conditions Report, 125.
Schaufeli, W. B., Leiter, M. P. & Maslach, C. (2009). Burnout: 35 years of research and practice. Career Development International, 14 (3), 204-220.
Schmidt, J.A., & Padilla, B. (2003).Self-esteem and family-challenge: An intervention of their effects on achievement. Journal of Youth and Adolescence, 32 (1), 37-46.
Schütz, A. (2003). Psychologie des Selbstwertgefühls. Von Selbstakzeptanz bis Arroganz. [Psychology on self-esteem. From self-acceptance to arrogance] (2nd ed). Kohlhammer.
Seiffge-Krenke, I. (2000). Causal links between stressful events, coping style, and adolescent symptomatology. Journal of Adolescence, 23, 675-691.
Seiffge-Krenke, I., Aunola, K., & Nurmi, J-E., (2009). Changes in stress perception and coping during adolescence: the role of situational and personal factors. Child Development, 80 (1), 259-279.
Selye, H. (1936). A syndrome produced by nocuous agents. Nature, 138, 32. Selye, H. (1978). The stress of life. (2nd ed). New York: McGraw Hill. SFI, Statens folkhälsoinstitut [Swedish National Institute of Public Health] (2011), Svenska skolbarns
hälsovanor 2009/10 [Swedish school children’s health realted habits 2009/10] Grundrapport, 2011:27. Shao, R., & Skarlicki, D.P. (2009). The Role of Mindfulness in Predicting Individual Performance. Canadian
Journal of Behavioral Science, 41 (4), 195-201.
57
Shirom, A. (2003). Job-related burn out. In J.C. Quick & L.E. Tetrick (Eds.), Handbook of occupational health psychology (pp. 245-265).Washington, DC: American Psychological Association.
Shirom, A., & Melamed, S. (2006). A comparison of the Construct Validity of Two Burnout Measures in Two Groups of Professionals. International Journal of Stress Management, 13 (2), 176-200.
Shirom, A., Melamed, S., Toker, S., Berliner, S., & Shapira, I. (2005). Burnout and health review: Current knowledge and future research directions. In G.P. Hodgkinson, & J.K. Ford (Eds), International review of industrial and organizational psychology (Vol. 20, pp. 269–309). Chichester, UK: Wiley.
Skolverket [The Swedish National Agency for Education] (2010). Attityder till skolan 2009. Elevernas och lärarnas attityder till skolan [Attitudes towards school 2009. Pupils and teachers attitudes towards school]. Research Rapport 334.
Socialstyrelsen [The National Board of Health and Welfare] (2003). Utmattningssyndrom. Stressrelaterad psykisk ohälsa. [Exhaustion syndrome. Stress-related mental illness.] Research report. Available: http://www.socialstyrelsen.se/publikationer2003/2003-123-18.
Socialstyrelsen [The National Board of Health and Welfare] (2009). Folkhälsorapport [Public Health report]. Available: http://www.socialstyrelsen.se/publikationer2009/2009-126-71
Söderström, M. (2007). Sov bättre med kognitiv beteendeterapi [Enhance your sleep with CBT]. Viva Söderström, M. (2012). Burnout – a matter of impaired recovery. Doctoral thesis, Karolinska Institute. Söderström, M., Ekstedt, M., Åkerstedt, T., Nilsson, J., & Axelsson, J. (2004). Sleep and Sleepiness in Young
Individuals with High Burnout Scores. Sleep: Journal of Sleep and Sleep Disorders Research, 27 (7), 1369-1377.
Sonnenschein, M., Sorbi, M.J., Van Doornen, L.J.P., Schaufeli, W.B., & Maas, C.J.M. (2007). Evidence that impaired sleep recovery may complicate burnout improvement independently of depressive mood. Journal of Psychosomatic Research, 62, 487-494.
Spencer, S.J., Josephs, RA, & Steele, C.M. (1993). Low self-esteem. The uphill struggle for self-integrity. In R. F. Baumeister (Ed.), Self-esteem: The puzzle of low self-regard (pp. 21-36). NY: Plenum.
Sterling, P., & Eyer, J. (1988). Allostasis: A new paradigm to explain arousal pathology. In S. Fisher & J. Reason (Eds), Handbook of life stress, cognition and health (pp.631-651). John Wiley and Sons Ldt.
Stinson, D.A., Logel, C., Zanna, M.P., Holmes, J.G., Cameron, J., Wood, J.V., & Spencer, S.J. (2008). The cost of lower self-esteem: Testing a self- and social-bonds model of health. Journal of Personality and Social Psychology, 94 (3), 412-428.
Stroud, L.R., Salovey, P., & Epel, E.S. (2002). Sex differences instress responses: social rejection versus achievement stress. Society of Biological Psychiatry, 52, 318-327.
Sundblad, G.B., Jansson, A., Saartok, T., Renström, P., & Engström, L.M. (2008). Self-rated pain and perceived health in relation to stress and physical activity among school-students: A 3-year follow-up. Pain, 136 (3), 239-249.
Tarafodi, R.W., & Swann, W.B. (1995). Self-Liking and Self-Comptence as Dimensions of Global Self-Esteem: Initial Validation of a Measure. Journal of Personality Assessment, 65 (2), 322-342.
Taylor, D.J., Clay, K.C., Bramoweth, A.D., Sethi, K., & Roane, B.M. (2011). Circadian Phase Preference in College Students: Relationships with psychological functioning and academics. Chronobiology International, 28 (6), 541-547.
Theorell, T. (1996). The demand-control-support model for studying health in relation to work environment – an interactive model. In: K. Orth-Gomer & N. Schneiderman (Eds.), Behavioral medicine approaches to cardiovascular disease prevention (pp. 69-85). New Jersey: Lawrence Erlbaum Associates.
Theorell, T. (2004). Stressmekanismer och sjukskrivning [Stress mechanisms and sickness absence]. In C. Hogstedt, M. Bjurvald, S. Marklund, E. Palmer and T.Theorell (Eds.). Den höga sjukfrånvaron – sanning och konsekvens [The high sickness absence rates – thruth and consequence]. Research report, R 2004:15. SFI Statens folkhälsoinstitut [Swedish National Institute of Public Health].
Thomson, H. (1998). Anpassningens pris. Kvinnors liv i vård och vardag [The cost of adaptation. The life of women who work in health care and their every day life].Förlagshuset Gothia AB, Stockholm.
Thoreson, C.E., & Eagleston, J.R. (1983). Chronic stress in children adolescents. Theory into Practice, 22 (1), 48-56.
Troisi, A. (2001). Gender differences in vulnerability to social stress. A Darwinian perspective. Physiology & Behavior, 73, 443-449.

58
Vispoel, W.P., Boo, J., & Bleiler, T. (2001). Computerized and paper-and-pencil versions of the Rosenberg self-esteem scale: a comparison of psychometric features and respondent preferences. Educational and Psychological Measurement, 61 (3), 461-474.
Walker, M.P. (2008). Cognitive consequences of sleep and sleep loss. Sleep Medicine, 9 (1), 29-34. Welzel, C., & Inglehart, R. (2010). Agency, Values and Well-Being: A Human Development Model. Social
Indicators Research, 97, 43-63. Wiklund, M., Bengs, C., Malmgren-Olsson, E-B., & Öhman, A. (2010). Young women facing multiple and
intersecting stressors of modernity, gender orders and youth. Social Science & Medicine, 71, 1567-1575. Wiles, N.J., Jones, G.T., Haase, A.M., Lawlor, D.A., Macfarlane, G., & Lewis, G. (2008). Physical activity and
emotional problems amongst adolescents: a longitudinal study. Social Psychiatry and Psychiatric Epidemiology, 43, 765–772.
Wittmann, M., Dinich, J., Merrow, M., & Roenneberg, T. (2006). Social jetlag: Misalignment of biological and social time. Chronobiology International, 23 (1&2), 497-509.
Wolfson, A.R., & Carskadon, M.A. (2003). Understanding adolescents’ sleep patterns and school performance: a critical appraisal. Sleep Medicine Review, 7 (6), 491-506.
World Values Survey (2005/08). Available: www.worldvaluessurvey.org Yahav, R., & Cohen, M. (2008). Evaluation of a Cognitive-Behavioral Intervention for Adolescents.
International Journal of Stress Management, 15 (2), 173-188. Yeung, W-F., Chung, K-F., & Cy Chan, T. (2008). Sleep-wake habits, excessive daytime sleepiness and
academic performance among medical students in Hong Kong. Biological Rhythm Research, 39 (4), 369-377.
Zimmermann, L.K. (2011). Chronotype and the transition to college life. Chronobiology International, 28 (10), 904-910.
















![ENTRE POLCAS E ESTUDOS...8 ABSTRACT The collection of sixteen pieces for piano titled Etudes and Polkas [H.308], by Czech composer Bohuslav Martinů (1890-1959) were composed in 1945,](https://img.pdfslide.fr/doc/110x75/6113ebda208ef66cca4c7863/entre-polcas-e-estudos-8-abstract-the-collection-of-sixteen-pieces-for-piano.jpg)