Embed Size (px)
Citation preview
with Perio Reports by Trisha E. O’Hehir, RDH, BS
March 2011 – Volume 7, Issue 3
Discussion from Hygienetown.com
Burned Out
Bone Fill on “Hopeless”
Anterior Tooth

Education Entertainment Camaraderie
Dr. UdellWEBB
Dr. ScottLEUNE
Ms. SandyPARDUE
Dr. RhondaSAVAGE
TEAM DEVELOPMENT
Dr. RichardROSENBLATT
Dr. ArmenMIRZAYAN
Dr. MichaelSKRAMSTAD
Dr. SameerPURI
Dr. DavidJULIANI
CEREC
Dr. TarunAGARWAL
Ms. SandyPARDUE
Dr. LouisMALCMACHER
Dr. BruceBAIRD
Dr. SameerPURI
Dr. RaymondYUKNA
Dr. HowardFARRAN
Register online at towniemeeting.com
or call 866.336.8696.
Dr. LouisMALCMACHER
Dr. RonaldJACKSON
Dr. BarryGLASSMAN
Dr. TommyMURPH
Dr. MichaelMELKERS
Dr. JohnNOSTI
Dr. RodKURTHY
Dr. TarunAGARWAL
Dr. ChipPAYET
CLINICAL
Dr. JohnKWAN
ChristineHOVLIARAS, RDH
Dr. AlbertFRYDMAN
SarahCOTTINGHAM, RDH
TrishaO’HEHIR, RDH
JennROBERTSON
HYGIENE
TimLOTT
RalphUJANO
JasonWOOD
PERSONAL DEVELOPMENT
Dr. NealPATEL
Dr. JasonLUCHTEFELD
Dr. JayREZNICK
Dr. MikeSCOLES
Dr. UdayREEBYE
IMPLANT
HeidiCHRISTOPHER,RDH
PeggyBLACKBURN,RDH
Dr. GlennVAN AS
Dr. JamesJESSE
AMD
MarkDILATUSH
Dr. JimBOYD
Dr. RyanSWAIN
HowieHORROCKS
WORKSHOPS
Dentist RDH Staff/Spouse Social Student Poker Golf
DentalMarketing
Six MonthSmiles
NTI-TSSCourse
towniemeeting.comFor more event & speaker information, visit us online at
Get Townie Meeting updates on Facebook & Twitter. 24
Earn up to
CE Credits
BRING ALL YOU HAVEat the Townie Golf Extravaganza
SIX MONTH SMILESCERTIFICATION
MARKETING SUMMIT by New Patients Inc.
NTI: NOT TOTALLY INDICATEDwith Dr. Jim Boyd
ALL BETS ARE OFFTownie Poker Tournament
CAESARS PALACE
$189Call 866-227-5944 &
mention code SCTOW1.
PERNIGHT
OPTIONAL WORKSHOPS
REGISTER NOW!
CCERE
Dr. Tarunr. TarunALALWWWAWAGARGARAA
Dr. BruceDr. BruceAIRDAIRDBB
Dr LouDr. LouisCHERCHERCMACMAMALMAL
ee Dr. HowardDr. HowardARRANARRANFF
MENTPOEVEL DTEAM
Ms. SandyMs. SandyUEUEARDARDPPPAPA
Dr. SameerDr. SameerURIURIPP
DrYY
MENT
r. Raymondr. RaymondAAYUKNYUKN
all 866.3all 866.3r cr cooeeeeememwniwnioott
er oer ottssgigieeRR
ONTHOMMSIXSIXCE TCERT
336.8696.336.8696.omom.c.cggtintinee
tte ae aatatonlinonlin
SMILESSMILESNTHNTHNNOOTITICAAATATTIFI
Dr. Armen. ArmenANANYYYAYAMIRZAMIRZAAYAY
Dr. Davidr. DavidJULIANIJULIANI
Dr. BarryDr. BarrySMANSMANSSGLAGL
Dr. TarunDr. TarunALALWWGARARAA
CALCLINI
Dr. RichardDr. RichardTTTTLALASENBSENBORR
Dr. MichaelDr. MichaelADADTTSSSKRAMSKRAM
Dr. SameerDr. SameerURIURIPP
Dr. LouisDr. LouisCHECHECMACMAMALMAL
Dr. RonaldDr. RonaldNNOOSSKKACAJJ
Dr. RodDr. RodTHYTHYKURKUR
Dr. ScottDr. ScottEUNELEUNE
Ms. SandyMs. SandyUEUERDARDPPPA
Dr. RhoDr. RhoGGAAVAVSSDD
RRDr. TommyDr. Tommy
HHMURPMURPDr. MichaelDr. Michael
SSMELKERMELKERDr JDr. Jo
TTNOSNO
Dr. UdellDr. UdellBBEBWEB
ndandaEEGG
nhnIITT
Dr. ChipDr. ChipETYETAAAYPPPAPA
TTCERT
ARKETMARKETby Newby New
TTOOTTTTOONN::TINTI
NT OTICACAATATIFIIFI
UMMITUMMITSSGGTINTINw Patients Inc.w Patients Inc.
TEDTEDCACAATATII IND INDYYALLALLTT
HHDr. AlbertDr. Albert
MANMANYDYDFRFSaraharah
HH RDRD,GHAMGHAMTTININOOCC
GIENEHY
LANTIMP
Dr. JohnDr. JohnANANWKW
ChristineChristineHHRDRD,,SSVLIARAVLIARAOOHHOO
TrishaTrishaRD RD,,HEHIRHEHIR’’OO
HHJennJenn
ONONSSTTRROBEOBRRTTim
TTTOTLLRalphRalph
NANUJUJ
EVEL DALNOSERP
PSOSHRKOW
hhOONN
JJasonDDOOWOWO
MENTPOEVEL
G ALLGRINRINBBat the Townieat the Townie
EEB BALALL
ARARCAESCAES
Townie PoTownie Po
VEVEHAHAAVAVUUOOYYALLALLe Golf Extravaganzae Golf Extravaganza
FFFFOO AREARETSTS
CECEALAALAPPPAPASSRR
ker Tournamentker Tournament
Dr. NealDr. NealTELTELAAATATPPPAPA
Dr. JasonDr. JasonCHTEFELDCHTEFELDLUL
AMD
Dr. JayDr. JayCKCKREZNIREZNI
Dr. MikeDr. MikeLESLESOOSCS
Dr. UdayDr. UdayYEYEEEBREEB
MarMarkDYDBOBO
Dr JDr. JimSHSHTUTUILAILAATATDD
HowiHowiRROCKRROOHH
WO NTERSGIRE
Dr. RyanDr. RyanAINAINWWSS
iieSSCKOCK mention cmention c
Call 866-Call 866-1818$$
ARCAESCAES
!W
GHTGHTNINIRRPEPE
..SCTOW1SCTOW1odeode&&-227-5944-227-5944
99ECEALALAPPPAPASSAR
HeidiHeidiHHRDRD,,HERHERPPPPOSTSCHRICHRI
PeggyPeggyHHRDRD,,URNURNCKBCKBLALABB
eboeboccaaon Fon FFaFawniwnioot Tt TToToGeGe
Dr. GlennDr. GlennSSAANNVAVA
Dr. JamesDr. JamesSESEJESJES
.ererr.tttetettwiwiook & Took & Tsseettteteaapdpdg ug uupuptintineeeee Me MMeMeii 24
Earn up to
CE Credits
24Earn up to
CE Credits
hygienetown.com « March 2011
from trisha’s desk hygienetown
2
Has this ever happened to you? A regular patient is scheduledand it’s been a year since his last visit. Mr. Hal E. Tosis presents forhis “cleaning” and you begin with a review of medical history,extraoral and intraoral oral cancer screening exam and then youtake a look at his teeth and gums.Not much supragingival calculusand the probing looks within nor-mal limits, with only slight bleed-ing. You tell him he’s doing fine andhe’s happy to hear that, reportingthat he only brushes and neverflosses. You begin instrumentationand suddenly, you drop into 4-6mminterproximal pockets and find sub-gingival calculus. What happened?
How could the probing meas-urements have been so wrong?Now, after just telling the patientthat everything looks fine, you find he actually has early to mod-erate periodontal disease in all posterior interproximal areas.
The reason is simple and we can blame it on researchers andeducators who listen to the researchers. Remember back inschool when you were taught to probe with the tip of the probein constant contact with the root surface, holding the probe par-allel to the long axis of the tooth and making sure to probe theline angles of all the teeth? Researchers wanted their probing tobe reproducible, so rather than angling the probe to reach themid-interproximal surface and find any crater development,they kept the probe parallel to the long axis of the tooth andguided the probe around the tooth, from line angle to line angle.This method, while being easily reproducible, will not detectany mid-interproximal pockets. This significantly underesti-mates the prevalence of periodontal disease. According to theAmerican Academy of Periodontology, periodontal diseasemight be underestimated by as much as 50 percent.
Good educators followed the direction of researchers andinstructed years of students to hold the probe parallel to the longaxis of the tooth and measure around the tooth from line angleto line angle. This explains why interproximal defects can bemissed so easily.
Next time you see a patient who hasn’t been in for a whileand who doesn’t practice daily interproximal oral hygiene, tryprobing according to Dr. Howard Farran. Wish I could takecredit for this idea, but it was Howard who came up with it and
it’s a great idea! No more probingaround the teeth as instructed inschool and as so many computerprograms require. Instead, separatefacial and lingual surfaces frominterproxiaml surfaces, making twopasses with the probe. First, probeall the brushing surfaces. Tell thepatient you are doing a new test forgum disease and you will say themeasurements out loud so he canhear them. The numbers should be1 to 3, anything 4 or higher is dis-ease and any bleeding points are a
sign of infection. After probing the brushing surfaces, tell thepatient you are now going to check for infection on his flossingsurfaces. Same rules about numbers – 1 to 3 are healthy, any-thing 4 or higher is disease. After you finish this probing systemon patients, they will know their periodontal status before yousay another word.
Make these two simple changes and you will never overlookinterproximal disease again. First, be sure to angle your probeinto the mid-interproximal, despite what you were taught inschool. Second, probe brushing surfaces first, and then probeflossing surfaces. You might be surprised to find that you toohave underestimated the prevalence of periodontal disease inyour practice. n
In This Issue
3 Perio Reports7 Profile in Oral Health: Your Fresh Breath Program11 Drug-free Oral Wound Dressing Makes for Happier Patients
(and a More Pleasant Office)15 Message Board: Burned Out17 Message Board: Bone Fill on “Hopeless” Anterior Tooth
by Trisha E. O’Hehir, RDH, MS, Hygienetown Editorial Director
Underestimation ofPeriodontal Disease
Here’s where you can catch Trisha live! To schedule Trishato speak at your next national, state or local dental hygienemeeting, e-mail [email protected].
March 24-26, 2011Thomas P. Hinman Dental Meeting n Atlanta, Georgia
April 9, 2011Make Yourself Indispensable n Salt Lake City, Utah
April 14, 2011New Orleans Dental Conference n New Orleans, Louisiana
Trisha Live

March 2011 » hygienetown.com
hygienetown perio reports
3
Perio Reports Vol. 23 No. 3Perio Reports provides easy-to-read research summaries on topics of specific interest to clinicians.
Perio Reports research summaries will be included in each issue to keep you on the cutting edge of dental hygiene science.
Timing of SystemicAntibiotic Important
Generalized aggressive periodontitis (GAgP) exhibitssevere destruction of supporting alveolar bone, oftenleading to edentulism early in life. The initial phase oftreatment is reducing or eliminating the pathogenicmicroorganisms. Researchers suggest adding systemicantibiotics when treating GAgP.
Researchers at the Eastman Dental Institute inLondon, UK wanted to know if the timing of when asystemic antibiotic was given changed the outcome oftreatment. In a two-phase study they first treated a groupof 41 GAgP subjects with full-mouth SRP within twodays, giving half the subjects placebo pills and the otherhalf amoxicillin and metronidazole to be taken for sevendays. Subjects were all given chlorhexidine mouth rinseto be used twice daily for two weeks. Clinical indiceswere monitored at baseline, two and six months.
At six months, all subjects again received full-mouthSRP. Those that had received the placebo before werenow given the antibiotics.
The greatest healing took place in the first twomonths following treatment for both the test andplacebo groups. At eight months, more healing had beenrealized in both groups, confirming other research thatreported healing up to nine months after initial treat-ment. Those who received antibiotics at baseline showedgreater overall healing than those who received anti-biotics later at re-treatment. This might be due toincreased vascularity in the beginning, delivering moreantibiotic to the area.
Clinical Implications: If you are treating a patientwith GAgP, consider using systemic antibiotics at theinitial phase of treatment rather than waiting.
Griffiths, G., Ayob, R., Guerrero, A., Nibali, L., Suvan, J.,Moles, D., Tonetti, M.: Amoxicillin and Metronidazole as anAdjunctive Treatment in Generalized Aggressive Periodontitisat Initial Therapy or Re-treatment: A RandomizedControlled Clinical Trial. J Clin Perio 38: 43-49, 2011. n
Generalized aggressive periodontitis (GAgP) is often rapidlyadvancing and is associated with Aa (Aggregatibacter [Actino-bacillus] actinomycetemcomitans) bacteria. Two decades agoProfessor Arie Jan van Winkelhoff introduced the idea of givingGAgP patients two antibiotics at the same time, metronidazoleand amoxicillin, in conjunction with SRP. It has since becomeknown as the van Winkelhoff Cocktail. This approach wasdesigned specifically to treat Aa infections.
Researchers at the University of Basel in Switzerland per-formed bacterial susceptibility tests specifically for metronidazoleand amoxicillin using plaque samples from four smokers withuntreated GAgP. They collected the plaque from the two deepestpockets in each subject and immediately plated them on severaldishes of blood agar infused with varying concentrations of theindividual antibiotics and a combination of the two.
The bacterial counts of the plaque samples on standard agarwere very high. Low concentrations of amoxicillin reduced thenumber of colony-forming units for all four samples. Higherconcentrations prevented growth for two samples and reducedgrowth for the others. The low and high concentrations ofmetronidazole lowered the counts, but never eliminated growth.Both the low and high concentrations of the combination of thetwo antibiotics prevented all bacterial growth in all four samples.
It seems there is either an additive or synergistic effect whenthe two antibiotics are combined, which stops all growth for allthe plaque samples.
Clinical Implications: Systemic antibiotics are not recom-mended for routine periodontal treatment, but for cases ofGAgP, especially in smokers, the van Winkelhoff Cocktailmight provide significant benefits.
Walter, C., Kulik, E., Weiger, R., Zitzmann, N., Waltimo, T.:Additive or Synergistic Antimicrobial Effects of Amoxicillin andMetronidazole on Whole Plaque Samples: A Preliminary Report. Jof Inter Academy of Perio 13: 11-16, 2011. n
Metronidazole and Amoxicillin – The “van Winkelhoff Cocktail”
continued on page 5

March 2011 » hygienetown.com
hygienetown perio reports
5
Removing subgingival bacterial biofilm and any deposits onthe root surfaces is the primary goal of both surgical and non-surgical therapy for moderate to severe periodontitis. The timeframe for accomplishing the scaling and root planing (SRP) canbe one quadrant per week or full-mouth (FM) instrumentationwithin two days. Comparisons show both approaches achievesimilar clinical outcomes, so the choice is up to the patient andthe clinician.
Researchers at Pontificia University in Bogota, Colombiacompared quadrant SRP to FM instrumentation with andwithout systemic antibiotics, to see if the antibiotics wouldenhance healing. A total of 29 patients with moderate tosevere periodontitis participated in the study. The threegroups were seen at baseline for data collection, for theirassigned treatment appointment and re-evaluation four to sixweeks after treatment. Those in the FM plus antibiotic groupunderwent bacterial susceptibility testing to determine whichantibiotic should be used. Amoxicillin, 875mg, was taken
twice daily by four subjects and doxycycline, 100mg, once aday was taken by the other six subjects.
No significant differences were found in clinical healingbetween the three groups. All groups showed significant reduc-tions in bleeding and probing depths. No additional clinicalbenefits were obtained by those taking antibiotics. Both FMgroups showed significant reductions in anaerobic bacterialcounts compared to the quadrant control group.
Clinical Implications: Similar clinical outcomes are achievedwith both traditional quadrant SRP and FM SRP, with andwithout systemic antibiotics. It is still up to the clinician andpatient to decide which approach they prefer.
Serrano, C., Torres, N., Bejarano, A., Caviedes, M., Castellanos,M.: Clinical and Microbiological Comparisons of Three Non-Surgical Protocols for the Initial Treatment of ChronicPeriodontitis. J Inter Academy of Perio 13: 17-26, 2011. n
In an earlier report, short-term calcium and vitamin Dsupplementation seemed to enhance periodontal health. Thesame research group evaluated the periodontal maintenancepatients after one year to determine if the positive benefits ofnutritional supplementation persisted.
A total of 51 periodontal maintenance patients were evaluated at Saint Louis University and Southern IllinoisUniversity. Mandibular posterior teeth were evaluated at base-line, six and 12 months. Clinical indices included plaque,bleeding, probing, attachment levels, calculus and furcations.All patients had at least two interproximal sites with 3mm ormore of clinical attachment loss. Digital radiographs wereused to measure alveolar bone levels.
Nutritional supplements were taken by 23 of the sub-jects and nutritional analysis was used to determine totaldaily intake of vitamin D and calcium for both test andcontrol groups.
Total daily calcium and vitamin D intakes varied signifi-cantly between the groups. Those with supplementation aver-aged 1,769mg of calcium and 1,049IU of vitamin D. Those
not taking supplementation were estimated from diet analysisto be receiving an average of 642mg of calcium and 156IU ofvitamin D each day.
Both groups showed significantly improved periodontalhealth over the one-year period. Those taking calcium andvitamin D supplementation showed a modest positiveeffect on periodontal health. It’s difficult to separate out all the factors that influence periodontal health, includingoral hygiene and subgingival instrumentation. Randomizedclinical trials are needed to confirm a positive effect forsupplementation.
Clinical Implications: Although calcium and vitamin Dsupplementation showed a slight benefit, at this time wecannot suggest these two nutrients will significantlyenhance periodontal health.
Garcia, M., Hildebolt, C., Miley, D., Dixon, et al: One-YearEffects of Vitamin D and Calcium Supplementation on ChronicPeriodontitis. J Perio 82: 25-32, 2011. n
Calcium and Vitamin D Supplementation
Quadrant and Full-mouth SRP Equivalent
continued from page 3

hygienetown.com « March 2011
perio reports hygienetown
6
Periodontal disease begins between the teeth, yet oral hygiene instructions begin withtooth brushing and eventually add dental flossing. Cleaning between the teeth with floss ismore difficult than brushing, and consequently, the majority of people rarely use dental floss.Other effective, easy-to-use devices needto be recommended.
Researchers at the University ofAmsterdam in the Netherlands comparedthree interdental devices in a group of 104university students (no dental students).To participate in the study, students had tohave bleeding scores of at least 50 percent,with at least five teeth per quadrant andno advanced periodontal disease. Subjectswere randomly assigned to one of threegroups: Johnson and Johnson waxed dental floss, Water Pik WaterFlosser withthe standard jet tip and the Water PikWaterFlosser with a new irrigator tip withthree tufts of bristles around the opening.
Bleeding was evaluated at baseline,two weeks and four weeks. All threegroups showed reduced bleeding scores attwo weeks, with relative reductions of 13percent in the flossing group, and 20 and26 percent in the two irrigation groups. Byweek four, the flossing group had returnedto baseline bleeding levels. The oral irriga-tion groups also showed some backsliding,but still maintained significant bleedingreductions of 15 and 17 percent. Therewas no significant difference between thetwo irrigation tips for reducing bleeding.
Plaque scores showed no differences atany point in time for any of the groups.
Clinical Implications: Based on thesefindings, the Water Pik WaterFlosser isbetter than waxed floss for reducinggingival bleeding.
Rosema, N., Hennequin-Hoenderdos, N.,Berchier, C., Slot, D., Lyle, D., Van derWeijden, G.: The Effect of DifferentInterdental Cleaning Devices on GingivalBleeding. J Inter Academy of Perio 13: 2-10, 2011. n
Water Floss Better Than String Floss
Many studies have been published over the past two decades comparingpower and manual toothbrushes. The evidence reported in these research stud-ies shows power toothbrushes to be at least as effective as manual toothbrushesand in some cases better. Concerns have been raised that power toothbrushesmight potentially cause trauma to both hard and soft tissues, raising questionsof safety. Many studies do include an evaluation of power toothbrush safety,but few studies are focused specifically on safety.
No review articles covering the published literature on the safety of specificpower toothbrushes were available. Therefore, a team of researchers from uni-versities in Amsterdam, Germany, Missouri and Michigan evaluated publishedresearch comparing oscillating-rotating power toothbrushes to manual tooth-brushes for safety.
They evaluated several hundred papers and found 35 studies that met theirstated research and reporting criteria. In most studies, toothbrush safety wasmeasured by gingival recession and/or abrasion. Only two of these studieslooked primarily at safety outcomes and there was no significant difference inrecession reported when comparing the oscillating-rotating brush to a manualbrush. A descriptive analysis was reported in 24 of the studies which showedvery few brushing related adverse events. These studies also showed no differ-ence in recession between the power and manual brushes tested.
Based on these findings, the researchuntil now shows that oscillating-rotatingpower toothbrushes do not pose a risk forgingival recession.
Clinical Implications: According to theresearch, oscillating-rotating powertoothbrushes are as safe as manualtoothbrushes.
Van der Weijden, F., Campbell, S., Dörfer,C., Gonzalez-Cabezas, C., Slot, D.: Safety ofOscillating-Rotating Powered BrushesCompared to Manual Toothbrushes: ASystematic Review. J Perio 82: 5-24, 2011. n
Oscillating-rotating Power Brushes Safe

March 2011 » hygienetown.com
hygienetown profile in oral health
7
by Trisha E. O’Hehir, RDH, MS
Although many topics once considered taboo are openly dis-cussed today, bad breath is still not easily discussed, even amongfriends and colleagues. Not discussing it doesn’t mean peopledon’t spend money on it. Fresh breath is big business! Many ofthe several billion dollars spent on oral health care products eachyear are spent on mints, candies and rinses that mask but do noteliminate the volatile sulfur gases of bad breath.
Agree or not, you are in the fresh breath business, so why notturn it to your advantage? Start offering a new service for yourpatients in the form of a fresh breath program. This is how youcan take the time for oral hygiene instructions/patient educationand actually charge for your time and expertise, instead of giv-ing away such valuable information. Offering a fresh breath pro-gram is also a good way to attract new patients to your practice.
What is Bad Breath?According to the research, 90 percent of oral malodor comes
from the oral cavity. This odor originates with periodontal dis-ease, caries, overhangs, open margins and deposits on the veryback of the tongue. Ten percent of oral malodor comes fromextraoral factors. These would be infections in other parts of thebody. The volatile sulfur compounds (VSCs) are released in theblood and taken to the lungs where they are expelled. This is rec-ognized in the late stages of disease, not usually in the beginningstages. When all oral factors have been ruled out, referral to aphysician might be necessary, but only in a few cases.
Fifty percent of people have bad breath sometimes – usuallyin the morning – with 25 percent of people suffering withchronic bad breath. Bad breath is the third most common den-tal complaint after caries and periodontal disease. People whobelieve they have bad breath, when no bad breath can be con-firmed by organoleptic testing, suffer from halitophobia orimaginary bad breath. Patients need reassurance that they do nothave bad breath and if they still don’t accept your diagnosis,might need a psychological referral.
The actual smell of bad breath is due to gases in the mouth –volatile sulfur compounds. The smells associated with these VSCsare quite distinctive. Methyl mercaptan smells like feces, hydro-
gen sulphide smells like rotten eggs and dimethyl sulphide smellslike cabbage, sulphur and gasoline. Periodontal disease is associ-ated with methyl mercaptan and dimethyl sulfide, or the smells offeces, cabbage, sulphur and gasoline. Add to that a breath mintand you have perio breath with an overlay of sickly sweet mint.Add in cigarettes and you recognize the smell immediately.Linking the treatment of periodontal disease to fresh breath mightincrease your case acceptance for periodontal treatment.
Besides periodontal disease, bad breath is linked to stress,dry mouth, dehydration, certain foods, alcohol, tobacco, med-ications, hormonal changes, metabolic disorders, chronic nasalproblems, tonsil stones or tonsilith and hunger.
History of Fresh Breath Clinics The first official U.S. fresh breath clinic was opened in 1992
by Dr. Jon Richter, in Philadelphia, Pennsylvania. This was thefirst clinic devoted entirely to treating oral malodor. In additionto dental hygiene and periodontal therapy, Dr. Richter used amodified ultrasonic scaler tip with a throat shield to detoxify thetongue using a chlorine dioxide solution. ProFresh is the line ofchlorine dioxide fresh breath products developed and sold byDr. Richter.
The first West Coast fresh breath clinic was opened by Dr.Harold Katz in 1994 after being faced with helping his daugh-ter overcome bad breath. He now has several California breathclinics and a product line called TheraBreath.
Our neighbors to the north had a halitosis assessment clinicat the University of Toronto. When it closed in 1993, Canadianhygienist Anne Bosy and pediatric dentist Dr. Julian Gelleropened a new fresh breath clinic by renting space in a Torontodental office one half-day each week. In 1995 the fresh breathclinic moved to its own facility and today the name of these clin-ics across Canada is OraFresh.
In 1995, Drs. Phil Stemmer and Mel Rosenberg opened theFresh Breath Centre in London, UK. Hygienist Mhari Coxon pro-vided tongue manicures as part of the fresh breath treatment there.
In 1997, Dr. Geoffrey Speiser opened the Australian BreathClinic (formerly called BreezeCare) in Sydney, Australia. Dr.
Speiser uses Halicheck gas chromotography to evaluate breath odors andrecommends the oral probiotic K-Force to introduce missing bacteriathat combat bad breath.
All of these clinics around the world offer their own line of oralhealth care products. Undoubtedly there are more fresh breath clinicsacross this country and the world, as well as many dental practicesoffering a fresh breath program as part of their full array of dental anddental hygiene services.
Starting Your Fresh Breath ProgramFirst, let’s cover what your fresh breath program isn’t. It is not simply a
mouth rinse and toothpaste. It’s much more than that. It includes data col-lection about the person’s experience with bad breath, diagnosis of the actualbad breath problem, a treatment plan including any professional treatmentsneeded, what the patient will do at home on a daily basis, what products areprovided or recommended and the follow-up visits to measure success of thefresh breath program. And of course, there is a fee for this program.
Fresh Breath Data CollectionThe periodontal examination including bleeding points will provide a
basis for discussing bad breath. Bleeding and periodontal pockets are pri-mary sources of VSCs between the teeth. Your patient questionnaire shouldcover several topic areas including oral hygiene habits, eating habits, med-ical issues and a description of the problem in their own words. Questionsabout oral hygiene habits will cover products they currently use includingboth interdental and tongue cleaning, and their use of mints, sprays andrinses for fresh breath. Diet questions will determine if the diet is high inproteins, dairy products, spices, alcohol or coffee that all impact oral mal-odor. Diet questions should also cover frequency of eating during the day,special diets and hydration.
The impact of medications that cause xerostomia should be consideredwith medical history questions. Mouth breathing questions should includequestions about snoring, talking a lot for work, running or working outand the stress level they experience.
Diagnosis of Bad BreathThe three primary ways to diagnose bad breath, ways that are used
in research as well as clinical practice, are organoleptic testing, sulfidemonitoring and gas chromatography. The gold standard is organoleptic
hygienetown.com « March 2011
profile in oral health hygienetown
continued on page 9
8

March 2011 » hygienetown.com
hygienetown profile in oral health
testing, or one person sniffing another’s breath. People whoare organoleptic breath testers are trained to distinguishbetween different levels of odor and types of odors. This canbe done simply by placing your nose close to the mouth andsmelling the breath. It can also be done by extracting mouthair with a disposable syringe and then in the same room withthe patient or in another room, smell the air as it is expelledfrom the syringe. Organoleptic reports from the patient’sfriends and loved ones can also be used, by asking for thatfeedback from the patient. Has someone complained to themabout their bad breath?
The Halimeter is a portable sulphide monitor that calculatesthe level of volatile gasses produced by oral bacteria. Thepatient is instructed to close the mouth,breathe through the nose for one minute,allowing VSCs to accumulate in the mouth.After one minute, the patient is instructed totake a deep breath through the nose and holdtheir breath while a straw is inserted one to twoinches into the mouth, careful not to touch teethor tissues and resting on the back of the tongue.The lips are gently not yet completely closedaround the straw, leaving a slight gap. The strawis attached to a hose going to the machine.While the patient holds their breath, the Halimeter reads themouth air to determine the total level of VSCs. The peak VSCvalue for the air sample is visible on the digital display.
The OralChroma, also called Halicheck, is a digital gas chro-matograph that measures VSCs in the mouth and provides acomputer readout of the findings. A syringe is placed in themouth for 30 seconds and 5cc of mouth air is extracted bypulling back the plunger. This air sample is injected into theOralChroma unit and within eight minutes the breath analysisis visible on a monitor. The same three VSCs that are measuredwith the Halimeter are measured with the OralChroma, but thismachine will distinguish between the three, providing a score foreach individual VSC. This provides more information aboutwhat might be the cause of the malodor.
Treatment PlanPeriodontal treatment, as well as any necessary restorative
work, is essential to eliminating sources of bad breath. Oralhygiene will include tongue cleaning, especially the back of thetongue and cleaning between the teeth with floss, interdentaltools or water. Dry brushing the inside first and brushing untilthe teeth feel clean and taste clean before brushing with tooth-paste will assure more effective plaque biofilm removal.
Several products should be consid-ered for your fresh breath programincluding xylitol, chlorine dioxide, zincand oral probiotics. One hundred per-cent xylitol-sweetened products used
five times daily will reduce bacterial biofilm levels by 50 percent,a significant reduction leading to lower levels of VSCs. Chlorinedioxide will neutralize VSCs and kill bacteria. It is used exten-sively to purify the public water supply. Zinc will also kill thebacteria associated with oral malodor. Oral probiotics provide anadditional tool to change the balance of bacteria in the mouth,leading to fresher breath. Research in this area has identifiedmissing bacteria in the mouths of those with bad breath andperiodontal disease. By providing a daily oral probiotic, a natu-ral balance of oral bacteria can be achieved, thus eliminating anovergrowth of malodor-producing bacteria.
Diet modifications are made based on the information col-lected in the written questionnaire completed by the patient.
Reducing intake of dairy products, garlic,onions and spices will reduce oral malodor ifthese foods have been identified as culprits inbad breath.
A fee for this service should be decided, basedon your current fee structure. Scheduling 30 min-utes of the hygienist’s time for the analysis anddiscussion should be a fee comparable with yourcurrent prophylaxis fee. This fee will also coverthe cost of products you provide the patient.Having the products you want them to use avail-
able at the appointment will insure better compliance than send-ing them out to buy the products. The necessary restorative andperiodontal treatment will also need to be scheduled.
To introduce your new fresh breath program, consider plac-ing a table-top display in your reception area with a photo, twolines of text and the fee if you want. The line above the photo:“Worried About Bad Breath?” and the line below the photo:“Ask about our Fresh Breath Program.” This lets the patientsknow you offer this service and provides an opportunity forthem to ask about it.
Measuring SuccessFollow-up visits are needed to see if the treatment is work-
ing. Re-evaluation is done with the same diagnostic tool youused at baseline. Discussion with patients will reveal how thetreatment has impacted their social interactions with friends andloved ones. In only a few cases, bad breath remains despite treat-ing all oral aspects. In these cases, referral to a physician is indi-cated to rule out a systemic cause.
You now have a fresh breath program in your practice! Jointhe message board on Hygienetown to see the wide range ofproducts available for fresh breath and to compare notes withothers implementing a program in their practices. n
continued from page 8
Find It Online
Discuss this topic online. Visit Hygienetown.com and search for “How do you treat bad breath?”
9
Simple ingredients. Powerful protection.
100% XYLITOL
Xylitol is a natural-occurring sugar that research has shown can dramatically
improve the health of your teeth and mouth. Spry gives you a full line of great-
tasting oral care products, each rich in Xylitol and at levels proven to be effective.
To learn more, visit www.sprydental.com or call toll-free 1.877.901.6672
Available at:
And other fi ne stores.
March 2011 » hygienetown.com11
hygienetown article
For decades science has recognized that wound dressingsare extremely important components of wound care andare necessary for optimal wound healing. Wound dress-
ings perform three basic functions: they protect wounds, theyhelp prevent infection and they maintain optimal moisture.Maintenance of optimal moisture is not typically a major prob-lem in the mouth, although, ironically, many products used totreat oral wounds cause the same cell damage or death that a dryenvironment would cause. For example, many products cur-rently in use might contain alcohols, iodine, chlorhexidine, top-ical anesthetics or other harsh chemicals known to be toxic tocells such as fibroblasts and endothelial cells.1-3 Damage to thesecells can impair the wound healing process. Protection ofwounds and prevention of microbial colonization is extremelyimportant in wounds of the mouth, where a vibrant and variedmicrobiota flourish. Unfortunately, standard wound dressingsare not practical in dentistry.
Unlike medicine, where the thought of sending a patienthome with an open wound would be considered malpractice, indentistry, we typically send patients home with gaping wounds(e.g. tooth sockets) with nothing more than a prescription forpain medication, a pat on the back and a cursory “Good Luck”– not ideal for compromised tissues in such a hostile environ-ment as the mouth. So, dentists resort to the use of variousantimicrobial rinses (cytotoxicity and all), coverage with sys-temic antibiotics or, just as often, no treatment at all.
Dentistry needs a practical, predictably effective means tomanage intraoral wounds. An ideal product for oral wounds:
• would adhere to injured tissues for a sustained period of time.
• would protect wounds from irritation and contamination.• would provide significant, continuous pain relief. • would not damage the cells involved in wound healing.• would have no contraindications.• could be used as often as needed to continuously provide
protection and pain relief.Standard products that contain drugs or harsh chemicals
cannot meet all of these requirements. Drugs with contraindica-tions and harsh chemicals such as chlorhexidine are toxic to cellsnecessary for wound healing. A great need exists for a drug-freeproduct free of toxic chemicals.
Turns out, a product like this already exists. It’s a topical gelcalled SockIt. Our oral surgery practice has used it for the lastthree years. This product is drug-free, is comprised entirely ofall-natural, food-grade ingredients and provides all the benefitslisted. Pain relief is without numbness, because the product con-tains no anesthetics. Most patients prefer an analgesic effect toan anesthetic effect, so this is another plus for this product.
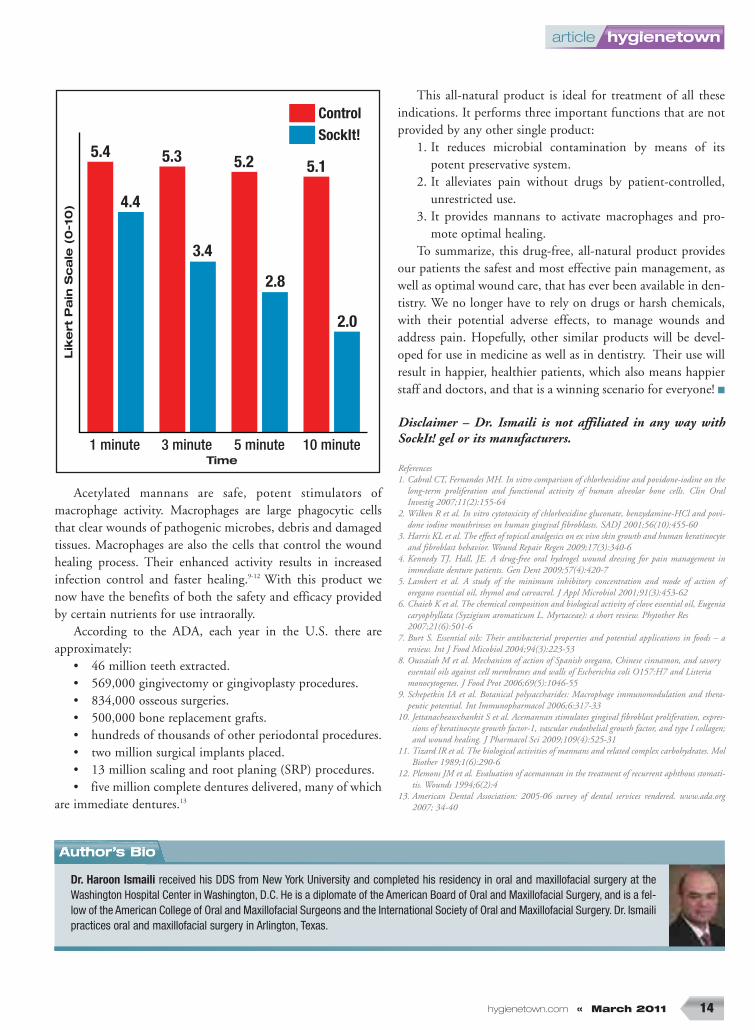
We use this product in all our surgery patients (almost5,000 to date) because they obtain more pain relief than thatprovided with prescription medication only. This observationmirrors the results seen in immediate denture patients whoexperienced significant pain relief within one minute with thisproduct, with increasing relief over time, above that providedby narcotic alone (see chart on p. 126).4 We have also seen adramatic decrease in the incidence of alveolar osteitis (dry
by Dr. Haroon Ismaili
continued on page 13

March 2011 » hygienetown.com13
hygienetown article
socket) and other post-operative complaints. This obvious ben-efit to our patients translates to a more enjoyable office envi-ronment. Our staff enjoys the reduced number of phone callsregarding post-operative complaints, and I enjoy the reducedstress of treating happy patients.
In addition to improved patient care, the product providesanother income center for our office. We include it in all ourtreatment plans, apply it at the time of surgery, then send ithome with patients with instructions to use it as often asneeded to maintain comfort and to use for wound manage-ment. Most patients obtain about three to four hours of painrelief before the gel washes away, so they need to use it four tosix times each day to stay comfortable and to keep the woundprotected. Many patients return to the office and ask for moreof the product. They like the ability to stay comfortable with-out numbness, and without the effects of narcotics. In addi-tion, the office benefits from fewer phone calls handled by ourstaff, and less chairtime addressing post-operative complaints atno charge to the patient.
Many well-known products claim to be all-natural; how-ever, almost all of them contain one or more man-made com-pound. Generally, these agents should not be swallowedbecause of potential adverse effects. Natural food ingredients,on the other hand, are by nature, very safe, and the bodyalready knows how to metabolize and dispose of foods. Thisproduct is comprised of nutrients in concentrations equal to orless than those found in the food sources, which assures evengreater safety.
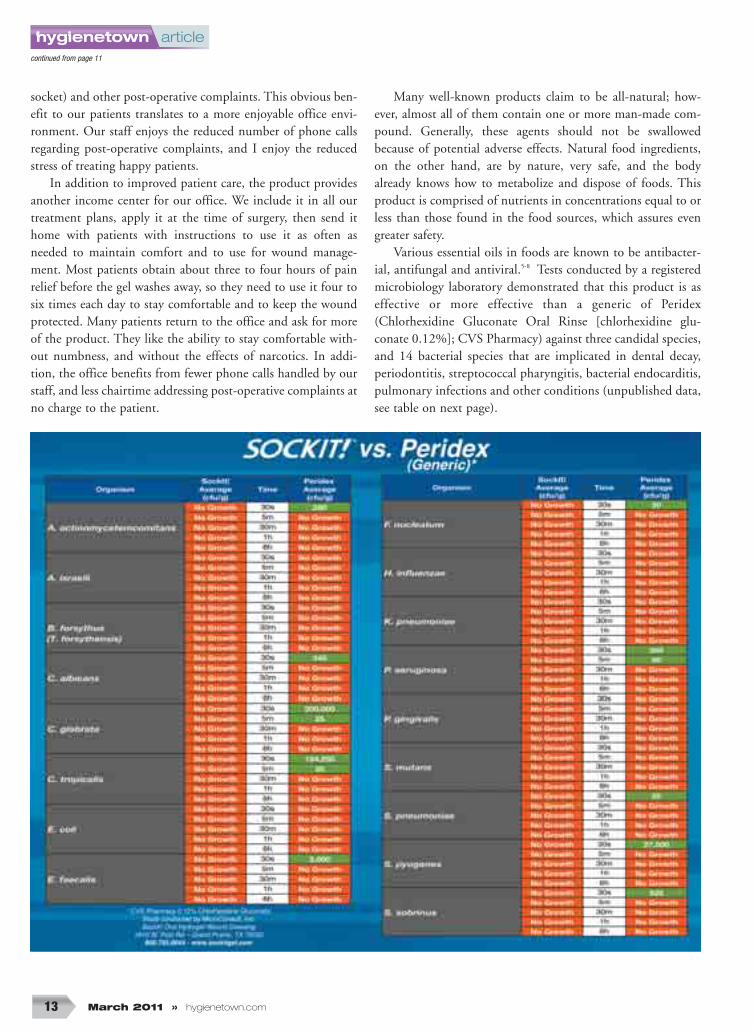
Various essential oils in foods are known to be antibacter-ial, antifungal and antiviral.5-8 Tests conducted by a registeredmicrobiology laboratory demonstrated that this product is aseffective or more effective than a generic of Peridex(Chlorhexidine Gluconate Oral Rinse [chlorhexidine glu-conate 0.12%]; CVS Pharmacy) against three candidal species,and 14 bacterial species that are implicated in dental decay,periodontitis, streptococcal pharyngitis, bacterial endocarditis,pulmonary infections and other conditions (unpublished data,see table on next page).
continued from page 11
article hygienetown
hygienetown.com « March 2011 14
Dr. Haroon Ismaili received his DDS from New York University and completed his residency in oral and maxillofacial surgery at theWashington Hospital Center in Washington, D.C. He is a diplomate of the American Board of Oral and Maxillofacial Surgery, and is a fel-low of the American College of Oral and Maxillofacial Surgeons and the International Society of Oral and Maxillofacial Surgery. Dr. Ismailipractices oral and maxillofacial surgery in Arlington, Texas.
Acetylated mannans are safe, potent stimulators ofmacrophage activity. Macrophages are large phagocytic cellsthat clear wounds of pathogenic microbes, debris and damagedtissues. Macrophages are also the cells that control the woundhealing process. Their enhanced activity results in increasedinfection control and faster healing.9-12 With this product wenow have the benefits of both the safety and efficacy providedby certain nutrients for use intraorally.
According to the ADA, each year in the U.S. there areapproximately:
• 46 million teeth extracted.• 569,000 gingivectomy or gingivoplasty procedures.• 834,000 osseous surgeries.• 500,000 bone replacement grafts.• hundreds of thousands of other periodontal procedures.• two million surgical implants placed.• 13 million scaling and root planing (SRP) procedures.• five million complete dentures delivered, many of which
are immediate dentures.13
This all-natural product is ideal for treatment of all theseindications. It performs three important functions that are notprovided by any other single product:
1. It reduces microbial contamination by means of itspotent preservative system.
2. It alleviates pain without drugs by patient-controlled,unrestricted use.
3. It provides mannans to activate macrophages and pro-mote optimal healing.
To summarize, this drug-free, all-natural product providesour patients the safest and most effective pain management, aswell as optimal wound care, that has ever been available in den-tistry. We no longer have to rely on drugs or harsh chemicals,with their potential adverse effects, to manage wounds andaddress pain. Hopefully, other similar products will be devel-oped for use in medicine as well as in dentistry. Their use willresult in happier, healthier patients, which also means happierstaff and doctors, and that is a winning scenario for everyone! ■
Disclaimer – Dr. Ismaili is not affiliated in any way withSockIt! gel or its manufacturers.
References1. Cabral CT, Fernandes MH. In vitro comparison of chlorhexidine and povidone-iodine on the
long-term proliferation and functional activity of human alveolar bone cells. Clin OralInvestig 2007;11(2):155-64
2. Wilken R et al. In vitro cytotoxicity of chlorhexidine gluconate, benzydamine-HCl and povi-done iodine mouthrinses on human gingival fibroblasts. SADJ 2001;56(10):455-60
3. Harris KL et al. The effect of topical analgesics on ex vivo skin growth and human keratinocyteand fibroblast behavior. Wound Repair Regen 2009;17(3):340-6
4. Kennedy TJ, Hall, JE. A drug-free oral hydrogel wound dressing for pain management inimmediate denture patients. Gen Dent 2009;57(4):420-7
5. Lambert et al. A study of the minimum inhibitory concentration and mode of action oforegano essential oil, thymol and carvacrol. J Appl Microbiol 2001;91(3):453-62
6. Chaieb K et al. The chemical composition and biological activity of clove essential oil, Eugeniacaryophyllata (Syzigium aromaticum L. Myrtaceae): a short review. Phytother Res 2007;21(6):501-6
7. Burt S. Essential oils: Their antibacterial properties and potential applications in foods – areview. Int J Food Micobiol 2004;94(3):223-53
8. Oussaiah M et al. Mechanism of action of Spanish oregano, Chinese cinnamon, and savory essentail oils against cell membranes and walls of Escherichia coli O157:H7 and Listeria monocytogenes. J Food Prot 2006;69(5):1046-55
9. Schepetkin IA et al. Botanical polysaccharides: Macrophage immunomodulation and thera-peutic potential. Int Immunopharmacol 2006;6:317-33
10. Jettanacheawchankit S et al. Acemannan stimulates gingival fibroblast proliferation, expres-sions of keratinocyte growth factor-1, vascular endothelial growth factor, and type I collagen;and wound healing. J Pharmacol Sci 2009;109(4):525-31
11. Tizard IR et al. The biological activities of mannans and related complex carbohydrates. MolBiother 1989;1(6):290-6
12. Plemons JM et al. Evaluation of acemannan in the treatment of recurrent aphthous stomati-tis. Wounds 1994;6(2):4
13. American Dental Association: 2005-06 survey of dental services rendered. www.ada.org2007; 34-40
Author’s Bio
5.4
1 minute
Lik
ert
Pa
in S
ca
le (
0-1
0)
Time
ControlSockIt!
3 minute 5 minute 10 minute
4.4
3.4
5.3 5.2
2.8
2.0
5.1

March 2011 » hygienetown.com15
hygienetown message board
melly420 Posted: 9/14/2010
Post: 1 of 23
Burned OutBurn out happens for many reasons, from the interactions of the staff, to the economy, to the philosophy of the practice. Townies share ways
to avoid or overcome burn out.
I have been a hygienist for six years. I really enjoyed it until the last year. Itseems with the economy being down patients are difficult to deal with as well asemployers. Anyone else having these issues? How do you deal with being burnedout? I am trying to look into other careers but have no idea what to go into. ■
Sorry to hear you are burned out. I might not be the best person toanswer your questions as I’ve been a hygienist for 43 years and can’tremember ever being burned out. My goal has always been to getpatients to optimum health levels – a task that seems never ending. I’malways looking for new ways to achieve that goal. More recently, I want
to let people know that dental disease is completely preventable and if they knowwhat causes it, how easy it is to prevent it. It’s really very simple and so much morefun than always treating disease. ■
Many of the dedicated professionals I knew and worked for haveretired and their practices have been bought out by younger, less dedi-cated doctors who do not respect the knowledge an older, more experi-enced person might have to offer. The other doctors are selling theirsouls to the corporate offices, where the amount of micro-managing
makes it unbearable to go to work every day. ■
Well, this is my first post in a long time, and I came to the site because I am feel-ing “burnt out” as well (13 years). I will try the exercise of writing down my goals,because it seems to be the environment I am in, not the profession.
I have been working part-time at three different offices and I would really like tobe at one, and develop a rapport with my patients. There is a dental placementagency in my state that interviews dental staff, and puts them together according topersonality, so I might go there. ■
Welcome back, Nancy. Posting here is a great step toward curingyour burn out. I find that sharing ideas and practice philosophies witheveryone on Hygientown really increases my knowledge and sparks creativity. You will definitely start to think of ways to improve yourworking environment.
Before you leave your present employment, weigh the pros and cons of workingevery day in one office, and working in three, as you do now. For example, workingevery day in one office might facilitate more continuity regarding the patients you see;however, working out of more than one office has never hindered me in forming a
trishaohehirPosted: 9/16/2010
Post: 2 of 23
jersey devil Posted: 9/16/2010
Post: 4 of 23
Nancy1997 Posted: 10/16/2010
Post: 6 of 23
lindadouglasPosted: 10/16/2010
Post: 7 of 23
Find it online at www.hygienetown.com
message board hygienetown
hygienetown.com « March 2011 16
~hygienetown~7786Posted: 10/22/2010
Post: 9 of 23
MarionRDH Posted: 10/22/2010
Post: 11 of 23
nkboecker Posted: 10/22/2010
Post: 8 of 23
rapport with patients. I have a “following” at each location, even at the office whereI work one day per week, and it has four other hygienists. I guess you are more likelyto get benefits, but how secure is it, really? If you lose that job, you end up with noth-ing. Also, if you hate it there, it will be really tough to go in every day. Working inone office can also make one quite insular, as it is more difficult to keep up-to-date.
Working out of multiple offices can have advantages in this economic climate. Itcan be more secure because you are unlikely to lose all of those jobs at once (unless itis through disability). You have more of a safety net. Also, more exposure to differentdoctors (and potential new job openings). You also learn more about different tech-niques, equipment and materials and philosophies of practice.
Have you had meetings with your bosses? They might be amenable to change. Forexample, if you can suggest ways to increase appointment times without losing pro-ductivity, and facilitate optimal oral health for your patients: i.e. most adult patientsneed more than a six-month prophy, as perio is often underdiagnosed, etc. Bossesoften like it if you approach them with a concern, if only you came up with a sug-gested solution too. ■
Yes, we all have issues. Try to remain positive. Do not take someone else’s prob-lems on as your own. Work on self-development. Think about your “Plan B.” Dosome temp work, if you have time; see what else is out there. The atmosphere is different in each office. ■
Are you burned out with hygiene or what is going on with the economy? Thoseare two different issues. I have been in dentistry for 22 years (15 years of being aRDH). I have never ever had a problem with finding hygiene jobs until now. In fact,recently I was on unemployment. Having two to three months off was nice, but a real“eye opening” experience. I finally found a job... what a humbling experience. Goingthrough not having a job, and wanting one very badly was a rough road. Thankfully,I now have a two day per week job. I regained that “love” for hygiene that I had yearsago! I encourage you to take this “crazy” time in your career and really sit and thinkof anything else you would rather be doing. It might just be a “bump” in the road. Itmight be just a “wake up call” for your love for dentistry. Good luck to you! ■
I have been a hygienist for 50 years, and have worked in offices that were totallywrong for me, and for offices that were right. Please do not take your present situa-tion as a sign that all dentists and all dental offices do not care for their patients, norcare for the work you do.
I recently went back to work for a dentist I believe is the most ethical, caring den-tist I have ever worked for. The extra time I put in with patients that need it isencouraged by even the doctor taking X-rays on my next patient, if that is what isneeded to stay on schedule. I love her, and love the office. ■
Burned Out
March 2011 » hygienetown.com17
hygienetown message board
periopeak Posted: 1/22/2011
Post: 1 of 31
Bone Fill on “Hopeless” Anterior ToothRegenerative periodontal endoscopy, including enzyme inhibitors, power scaling, soft tissue laser and Emdogain saved a hopeless tooth
scheduled for extraction.
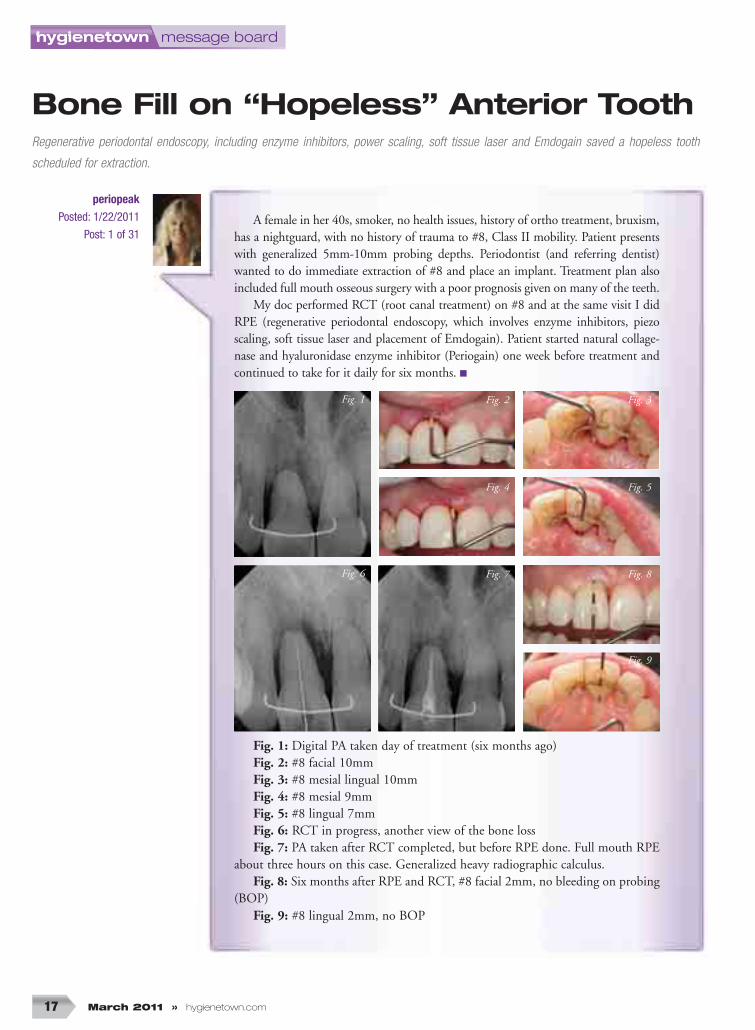
A female in her 40s, smoker, no health issues, history of ortho treatment, bruxism,has a nightguard, with no history of trauma to #8, Class II mobility. Patient presentswith generalized 5mm-10mm probing depths. Periodontist (and referring dentist)wanted to do immediate extraction of #8 and place an implant. Treatment plan alsoincluded full mouth osseous surgery with a poor prognosis given on many of the teeth.
My doc performed RCT (root canal treatment) on #8 and at the same visit I didRPE (regenerative periodontal endoscopy, which involves enzyme inhibitors, piezoscaling, soft tissue laser and placement of Emdogain). Patient started natural collage-nase and hyaluronidase enzyme inhibitor (Periogain) one week before treatment andcontinued to take for it daily for six months. ■
Fig. 1: Digital PA taken day of treatment (six months ago)Fig. 2: #8 facial 10mmFig. 3: #8 mesial lingual 10mmFig. 4: #8 mesial 9mmFig. 5: #8 lingual 7mmFig. 6: RCT in progress, another view of the bone lossFig. 7: PA taken after RCT completed, but before RPE done. Full mouth RPE
about three hours on this case. Generalized heavy radiographic calculus.Fig. 8: Six months after RPE and RCT, #8 facial 2mm, no bleeding on probing
(BOP)Fig. 9: #8 lingual 2mm, no BOP
Fig. 1 Fig. 2 Fig. 3
Fig. 4 Fig. 5
Fig. 6 Fig. 7 Fig. 8
Fig. 9
message board hygienetown
hygienetown.com « March 2011 18
Find it online at www.hygienetown.com
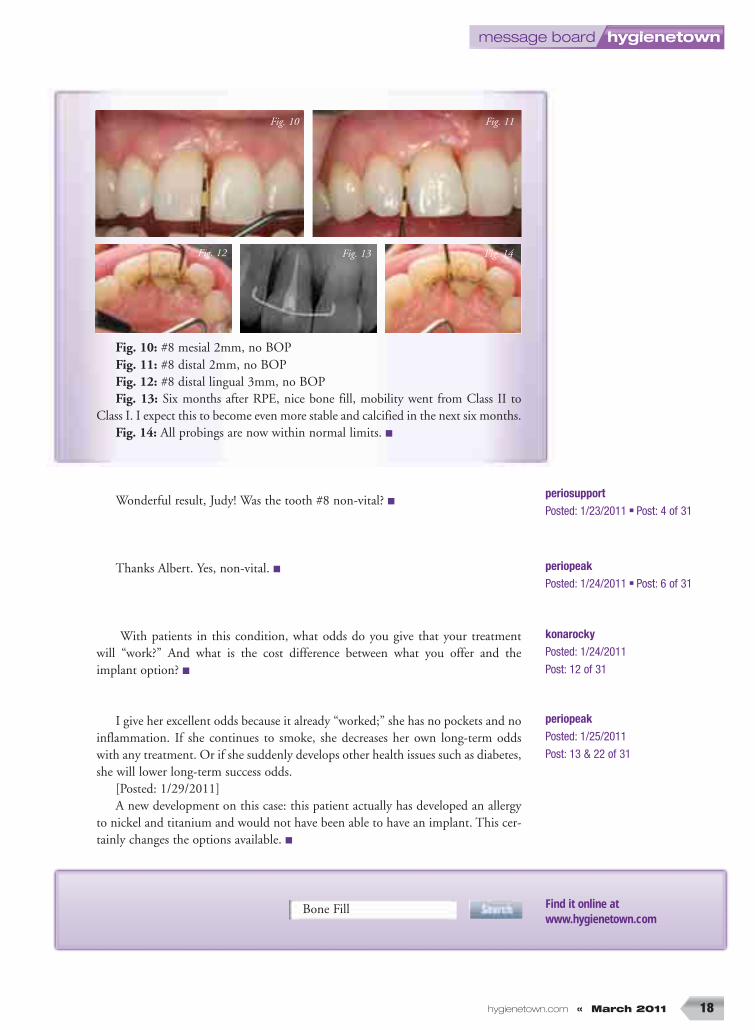
Fig. 10: #8 mesial 2mm, no BOPFig. 11: #8 distal 2mm, no BOPFig. 12: #8 distal lingual 3mm, no BOPFig. 13: Six months after RPE, nice bone fill, mobility went from Class II to
Class I. I expect this to become even more stable and calcified in the next six months.Fig. 14: All probings are now within normal limits. ■
Wonderful result, Judy! Was the tooth #8 non-vital? ■
Thanks Albert. Yes, non-vital. ■
With patients in this condition, what odds do you give that your treatment will “work?” And what is the cost difference between what you offer and theimplant option? ■
I give her excellent odds because it already “worked;” she has no pockets and noinflammation. If she continues to smoke, she decreases her own long-term oddswith any treatment. Or if she suddenly develops other health issues such as diabetes,she will lower long-term success odds.
[Posted: 1/29/2011] A new development on this case: this patient actually has developed an allergy
to nickel and titanium and would not have been able to have an implant. This cer-tainly changes the options available. ■
Bone Fill
periopeak Posted: 1/24/2011 ■ Post: 6 of 31
periosupport Posted: 1/23/2011 ■ Post: 4 of 31
periopeakPosted: 1/25/2011
Post: 13 & 22 of 31
Fig. 10 Fig. 11
Fig. 13 Fig. 14Fig. 12
konarockyPosted: 1/24/2011
Post: 12 of 31