Embed Size (px)
Citation preview

Pr Milou-Daniel Drici
CHU de Nice
Fibrillation atriale: avis d’expert sur les antithrombotiques

Effet préventif des AVK sur la survenue des AVC
2/3 des AVC dus à une FA sont évités par AVK (INR 2-3)1
L’anticoagulation par AVK est recommandée chez les patients en FA à risque modéré 2 avec un score CHADS 2 d’au moins 2.
Cependant l’usage des AVK est difficile:• Augmentation significative du risque hémorragique (intracérébral)• Difficile à manipuler : interactions• Respect de la fenêtre thérapeutique (INR:2-3)
1. Hart RG et al. Ann Intern Med. 2007;146:857-867 2. Fuster V, et al. JACC. 2006; 48: 854-906
…
Les anticoagulants = 1ère cause de morbi-mortalité
Le risque hémorragique = 1ère cause d’hospitalisation pour iatrogénie

RELY :Randomized Evaluation of
Long-term anticoagulant therapY
Dabigatran vs Warfarine chez 18,113 Patients avec une FA et un risque modéré ou élevé d'AVC ou d'embolie systémique

Objectif de l’étude
Comparer l'efficacité et la tolérance • de 2 doses de dabigatran (110 mg x 2/J et 150 mg x 2/J) en aveugle• vs la warfarine (INR cible : 2,0-3,0) en ouvert• chez des patients ayant une FA non valvulaire et à risque d'AVC
Critère principal de jugement : AVC, Embolies systémiques • Critères secondaires analysés en supériorité
Critère Principal de tolérance = Saignements majeurs

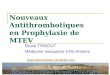
RE-LY dessin de l’étude
Ezekowitz MD, et al. Am Heart J 2009;157:805-10.
R
Warfarineajustée
(INR 2.0-3.0)N = 6000
Dabigatran Etexilate 110 mg 2x/J
N = 6000
Dabigatran Etexilate 150 mg 2x/J
N = 6000
Ouvert Aveugle
PROBE = Prospective Randomized Open Trial with Blinded Adjudication of Events.
FA +
≥ 1 Facteur de RisqueAbsence de contre-indications

Caractéristiques des patients
Caractéristiques Dabigatran 110 mg Dabigatran 150 mg WarfarineAge (ans) 71,4 71,5 71,6
CHADS2 (moyenne) 2,1 2,2 2,1
0-1 (%) 32,6 32,2 30,9
2 (%) 34,7 35,2 37,0
3+ (%) 32,7 32,6 32,1
Antécédent d’AVC/AIT (%) 19,9 20,3 19,8
Antécédent d’IDM (%) 16,8 16,9 16,1
Insuffisance cardiaque (%) 32,2 31,8 31,9
Aspirine à l’état basal (%) 4,0 38,7 40,6
Naif d’AVK (%) 49,9 49,8 51,4

Caractéristiques de l’étude
Caractéristique % patients/Temps
Suivi complet(18 093 patients)20 patients perdus de vue
99.9 %
Durée de l’étude Déc 2005 - Mars 2009
Moyenne de suivi :min :1 an, max : 3 ans 2 ans
Fenêtre thérapeutique sous warfarine – INR [2-3] 64 %
Connolly SJ., et al. N Engl J Med. 2009 ; 361: 1139-51

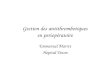
Pourcentage de patients dans l’INR cible selon les pays participants
Connolly SJ. Communication orale AHA 2009

RE-LY dessin de l’étude
Ezekowitz MD, et al. Am Heart J 2009;157:805-10.
R
Warfarineajustée
(INR 2.0-3.0)N = 6000
Dabigatran Etexilate 110 mg 2x/J
N = 6000
Dabigatran Etexilate 150 mg 2x/J
N = 6000
Ouvert Aveugle
PROBE = Prospective Randomized Open Trial with Blinded Adjudication of Events.
FA +
≥ 1 Facteur de RisqueAbsence de contre-indications

Critère primaire: AVC ou embolie systémique
D 110 mg D 150 mg warfarine D 110 mg vs Warfarin
D 150 mg vs Warfarin
%/an%/an %/an%/an %/an%/anRRRR
IC 95% IC 95% PP**
RRRRIC 95% IC 95%
P*P*
AVC ou embolie systémique
1,5 %/an 1,1 %/an 1,7 %/an0,91
0,74-1,110,34
0,660,53-0,82
< 0,001
AVC 1,4 %/an 1,0 %/an 1,6 %/an0,92
0,74-1,130,41
0,640,51-0,81
< 0,001
Embolie systémique
0,1 %/an 0,1 %/an 0,2 %/an0,73
0,37-1,460,38
0,670,33-1,36
0,27
* P de supériorité

Réduction des saignements :Dabigatran vs warfarine a démontré une réduction significative des saignements
Saignements majeurs (D110 mg bid vs W)• 20% D 110 mg bid vs W (p = 0,003) ; ns pour D150 mg bid vs W
Saignements engageant le pronostic vital• 32% D 110 mg bid vs W (p < 0,001)• 19% D 150 mg bid vs W (p = 0,037)
Hemorragies intracranniennes• 69% D 110 mg bid vs W (p < 0,001)• 60% D 150 mg bid vs W (p < 0,001)
AVC Hémorragiques • 69% D 110 mg bid vs W (p < 0,001)• 74% D 150 mg bid vs W (p < 0,001)

Effets indésirables
Taux comparables d'événements indésirables dans les 3 bras• Taux faibles d'événements indésirables
Seul événement plus fréquent sous dabigatran : la dyspepsie
Connolly SJ., et al. N Engl J Med. 2009 ; 361: 1139-51

Critère primaire AVC ou embolie systémique
* Interaction p évaluée par approche multivariable avec TTR basés par centres comme une valeur continue
D 110 mg D 150 mg warfarinD 110 mg vs
warfarinD 150 mg vs
warfarin
TTR par centreTaux
annuelTaux
annuelTaux
annuelRR
IC 95% P *RR
IC 95% P
Tous patients 1,5 % 1,1 % 1,7 % 0,910,74-1,11 0,34 0,66
0,53-0,82 < 0,001
< 56,9 % 1,9 % 1,1 % 1,7 % 1,10,73-1,6
0,610,39-0,96
56,9 - 65,4 % 1,6 % 1,1 % 2,2 % 0,740,51-1,1
0,480,32-0,74
65,4 % - 72,4 % 1,4 % 1,1 % 1,4 % 1,00,65-1,5
0,760,48-1,21
> 72,4 % 1,3 % 1,3 % 1,4 % 0,880,57-1,4
0,880,57-1,37
Int P 0,27 * 0,41 *

Effets indésirables
Taux comparables d'événements indésirables dans les 3 bras• Taux faibles d'événements indésirables
Seul événement plus fréquent sous dabigatran : la dyspepsie
Connolly SJ., et al. N Engl J Med. 2009 ; 361: 1139-51
Événement survenu plus fréquemment sous dabigatran (p < 0,001)
Dabigatran 110 mg
Dabigatran 150 mg Warfarine
Dyspepsie 11.8% 11.3% 5.8%688 patients 707 patients 348 patients

Conclusions :
• Le dabigatran 150 mg réduit significativement la survenue d’AVC comparativement à la warfarine sans majorer le risque de saignements majeurs et réduit la mortalité vasculaire.
• Le dabigatran 110 mg démontre une non infériorité à la warfarine sur la survenue d’AVC avec réduction significative du risque de saignements majeurs.
• Le dabigatran 110 et 150 mg réduisent la survenue d’hémorragies intra-craniennes et les saignements totaux : (majeurs, mineurs).
• Le dabigatran n’induit pas de toxicité hépatique vs warfarine, augmente la survenue de dyspepsie et de saignements gastro-intestinaux.