Embed Size (px)
Citation preview

1
ppnmdsct
rpqfitLdcgurc(
pndls
C
A
R
[
[
d
Pc
L
rotmi
C
Ahsbatsaaitlprotctt
016
eut compliquer une pneumatose pariétale. L’absence deerforation explique vraisemblablement ce mécanisme dansotre observation, même s’il n’a pas été constaté de pneu-atose sur les planches de scanner abdominopelvien. Lesiagnostics différentiels à évoquer sont le volvulus du côlonigmoïde ou du grêle, la dilatation gastrique, une occlusionolique avec une valvule de Bauhin très continente ou uneumeur du cæcum.
Les bases du traitement reposent sur trois éléments :éduire la torsion, traiter les complications évolutives etrévenir les récidives. La chirurgie en constitue le pilier,u’elle soit conservatrice (détorsion simple, cæcopexie parxation du cæcum au péritoine postérieur) ou non (cæco-omie, hémicolectomie droite et résection iléocæcale).es réductions de volvulus du cæcum par coloscopie ou pares lavements aux hydrosolubles sont plutôt considéréesomme « accidentelles » [8]. Des résultats peu encoura-eants ont été rapportés dans des séries anciennes avecn taux d’échec dépassant plus de 75 % des cas [9,10]. Uneéduction perendoscopique pourrait être tentée en cas deontre-indication à la chirurgie ou de chirurgie à risquegrossesse) pour retarder le recours à cette dernière [11].
La survenue d’une douleur abdominale avec un pneumo-éritoine après une polypectomie colique perendoscopiquee signe pas toujours une perforation colique et mérite’évoquer exceptionnellement un volvulus du cæcum, donta torsion ou la bascule est précipitée par l’exploration endo-copique.
onflits d’intérêts
ucun.
éférences
[1] Lapalus MG, Saurin JC. Complications de l’endoscopie diges-tive : gastroscopie et coloscopie. Gastroenterol Clin Biol2003;27:909—21.
[2] Pelletier AL, Vallot T. Complications de l’endoscopie digestive.In: Gastro-entérologie. Paris: EMC (Elsevier Masson SAS); 2008,9-013-V-05.
[3] Petersen CR, Adamsen S, Gocht-Jensen P, Arnesen RB,Hart-Hansen O. Splenic injury after colonoscopy. Endoscopy2008;40:76—81.
[4] Viney R, Fordan SV, William E, Gulchin E, Mickael E. Cecalvolvulus after colonoscopy. Am J Gastroenterol 2002;9:3211—2.
[5] Pirro N, Le Corroler, Solari C, Merad A, Sielezzneff I, Sastre B,et al. Volvulus du cæcum : base anatomique et physiopatholo-gique. Morphologie 2006;90:197—202.
[6] Habre J, Sautot-Vial N, Marcotte C, Benchimol D. Cæcal volvu-lus. Am J Surg 2008;192:48—9.
[7] Delabrousse E, Sarliève P, Michalakis D, Louis G, RodiereE, Kastler B. Tomodensitométrie de l’occlusion colique chezl’adulte. Feuill Radiol 2004;44:90—103.
[8] Abita T, Lachachi F, Durand-Fontanier S, Maisonnette F, Rou-daut PY, Valleix D, et al. Les volvulus du cæcum. J Chir2005;142:220—4.
[9] Anderson JR, Welch GH. Acute volvulus of the right colon: an
analysis of 69 patients. World J Surg 1986;10:336—42.10] Friedman JD, Odland MD, Bubrick MP. Experience with colonicvolvulus. Dis Colon Rectum 1989;32:409—16.
11] Montes H, Wolf J. Cecal volvulus in pregnancy. Am J Gastroen-terol 1999;94:2554—6.
cgvtg
Lettres à la rédaction
M. Pernina,∗
M. Legnameb
P. Nauletc
C. Bertinotti b
R. Delpya
P. Reya
a Service des maladies digestives, hôpital d’instruction desarmées Legouest, 27, avenue de Plantières, BP 90001,
57000 Metz cedex 3, Franceb Service de chirurgie viscérale, hôpital d’instruction des
armées Legouest, 27, avenue de Plantières, BP 90001,57077 Metz cedex 3, France
c Service d’imagerie médicale, hôpital d’instruction desarmées Legouest, 27, avenue de Plantières, BP 90001,
57077 Metz cedex 3, France
∗ Auteur correspondant.Adresse e-mail : [email protected] (M. Pernin).
Disponible sur Internet le 25 fevrier 2009
oi:10.1016/j.gcb.2009.01.008
rimary dedifferentiated liposarcoma of theolon: A case report
iposarcome dédifférencié primaire du côlon
Liposarcoma, the most common soft tissue sarcoma,epresents 20% of mesenchymal malignancies, and tends toccur in the retroperitoneum and deep soft tissues of therunk and extremities. Colonic liposarcoma (LS) are extre-ely rare. To our knowledge, this is the fifth case reported
n the literature.
ase report
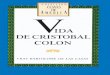
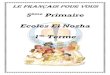
69-year-old male patient presented with a three-monthistory of abdominal pain, a ten pound weight loss andlow transit. Physical examination revealed a large, firmut non-tender, upper abdominal mass. Colonoscopy showedn obstructive polypoid mass in the left colon. Histopa-hological examination of the biopsy specimen suggested atromal origin. Serum concentrations of carcino-embryonicntigen (CAE), CA 19-9 was within normal limits. CT of thebdomen revealed an 8 cm × 8 cm low-density mass withrregular enhancement in the upper left quadrant close tohe spleen flexure of the colon and the spleen (Fig. 1). Aeft hemiocolectomy with radical lymph node resection waserformed. Gross examination revealed a 7 cm × 6 cm greyose mass involving the colonic submucosa. There were twother yellow fatty masses that were 7 and 6 cm, respec-ively and nearly adjacent to the serosa of the resectedolon (Fig. 2). Histological finding showed that the threeumors were characteristic of LS including multivacuola-ed lipoblasts with hyperchromatic nuclei. These areas were
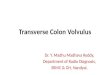
ontiguous with pleomorphic zones, spindle cells mixed withiant cell tumors and abundant necrosis (Fig. 3). Mitotic acti-ity in this pleomorphic dedifferentiated LS ranged from 10o 12 mitoses per 10 high power fields. The resected mar-ins were free from lesions. Immunolabelling for S-100 was
1017
Fa
tumors of the omentum [1]. Genetically, myxoid/round cellLS and well-/dedifferentiated LS are different diseases.Myxoid/round cell LS are characterized by translocationcausing FUS-CHOP or EWSR1-CHOP fusion, whereas well-/dedifferentiated LS are characterized by an amplification
Lettres à la rédaction
positive, but CD 117 and CD34 were negative excluding gas-trointestinal stromal tumors (GIST). The tumor was positivefor CDK4 and MDM2. Based on histopathology and the immu-noprofile, a diagnosis of dedifferentiated LS was made. Thepostoperative course was uneventful. The patient did notundergo adjuvant radiotherapy and there were no signs ofrelapse 10 months after surgery.
Discussion
LS is the most common soft tissue sarcoma and accountsfor at least 20% of all adult sarcomas [1,2]. These tumorscan grow slowly by direct invasion and may metastasize inthe lungs, liver and other viscera. Classification of LS intofour subtypes based on morphologic features and cytoge-nic aberrations is now widely accepted. These four typesare:
• well-differentiated;• dedifferentiated;• myxoid/round cell;• pleomorphic [2].
Singer et al. have shown by multivariate analysis thathistologic subtype and margin of resection are independentprognostic factors for survival in primary retroperitoneal LS[3]. Dedifferentiated subtypes are associated with an increa-sed risk of local and distant recurrences. Primary colonic LSare extremely rare, and to our knowledge this is the fifthreported case and the first case of dedifferentiated primarycolonic LS in the literature (there are two reported casesof myxoid LS, one well-differentiated and one pleomorphic[1—4].
As with other sarcomas, there are no characteristics cli-nical findings and no specific symptoms. Most tumors occurbetween 40—60 years of age [1,3]. Colonoscopy may helpconfirm the diagnosis by showing endoluminal lesions orsubmucosal filling defects. For diagnosis, CT and magneticresonance images (MRI) can provide important informationabout the size and involvement of adjacent structures aswell as tissue characteristics of the tumors. The reportedcharacteristics of LS on CT images are:
• lack of homogeneity;• infiltration or poor margination;• CT numbers greater than the patient’s normal fat;• irregular contrast enhancement [1,2].
There are high intensity MRI images on T2-weightedimages and low intensity on fat-suppressed T1-weighedimages. These suggest the presence of fat and malignancy[1].
The location of the lesion in the colon suggests GIST.Theses tumors typically stain with CD117 and CD34. Immu-nohistochemially, dedifferentiated LS are usually negativefor these markers and positive for S100. The diagnosis
can be confirmed with CDK4 and MDM2 (LS markers) andto distinguish dedifferentiated LS (positive) from poorlydifferentiated sarcomas (negative) [1—4]. Other diagnosesinclude adenocarcinoma, lipoma, leiomyosarcoma, lym-phoma, peritoneal LS, peritoneal carcinomatosis, primary Figure 1 Axial CT showing a huge lesion with low attenuationnd slight and irregular enhancement.
igure 2 Macroscopic appearance of the operative specimen.

1018
Ffi(
oAst
calsdactdawr
R
[
[
[
[
[
[
d
V
C
daegdga
étgpour des antécédents multiples de thrombophlébites des
igure 3 Microscopic view showing numerous lipoblasts andbrous septa with pleopmorphic nuclei and tumor giant cells HE× 400).
f the 12q13-15 region, including MDM2 and CDK4 genes.s myxoid/round cell LS are highly radio- and chemosen-itive, differentiation of subtypes is important to optimizereatment [4].
The treatment of choice is surgical resection with suffi-ient surgical margins; often followed by radiation and/ordjuvant chemotherapy with a high risk of relapse such as forarge tumors or low-grade tumors [3]. Despite an aggressiveurgical approach, the tumors in over 80% of patients withedifferentiated histology recur locally and 30% metastasizet distant sites within 3 years of diagnosis [1—3]. Doxorubi-in is the chemotherapy drug of choice. Patel el al. reportedhe efficacy of systemic chemotherapy using doxorubicin andacarbazine for 21 patients with myxoid LS [5]. Ishiguro etl. reported a case of resected ileocolonic mesenteric LShich responded to preoperative chemotherapy with doxo-
ubicin, cisplatin and ifosfamide [6].
eferences
1] Hirakoba M, Kume K, Yamasaki M, Kanda K, Yoshikawa I, OtsukiM. Primary mesenteric liposarcoma successfully diagnosed by
preoperative imaging studies. Intern Med 2007;46:373—5.2] Dodo IM, Adamthwaite JA, Jain P, Roy A, Guillou PJ, MenonKV. Successful outcome following resection of a pancreaticliposarcoma with solitary metastasis. World J Gastroenterol2005;11:7684—5.
m
dt
Lettres à la rédaction
3] Singer S, Antonescu CR, Riedel E, Brennan MF. Histologic subtypeand margin of resection predict pattern of recurrence and survi-val for retroperitoneal liposarcoma. Ann Surg 2003;238:358—70.
4] Binh MB, Sastre-Garau X, Guillou L, de Pinieux G, Terrier P,Lagace R, et al. MDM2 and CDK4 immunostainings are usefuladjuncts in diagnosing well-differentiated and dedifferentiatedliposarcoma subtypes: a comparative analysis of 559 soft tis-sue neoplasms with genetic data. Am J Surg Pathol 2005;29:1340—7.
5] Patel SR, Burgess MA, Plager C, Papadopoulos NE, Linke KA, Ben-jamin RS. Myxoid liposarcoma. Experience with chemotherapy.Cancer 1994;74:1265—9.
6] Ishiguro S, Yamamoto S, Chuman H, Moriya Y. A case of resec-ted huge ileocolonic mesenteric liposarcoma which respondedto pre-operative chemotherapy using doxorubicin, cisplatin andifosfamide. Jpn J Clin Oncol 2006;36:735—8.
S. Jarbouia,∗
A. Moussi a
H. Jarrayaa
K. Ben Mnaa
M.M. Abdesselema
A. Kourdab
S. Ben Jilanib
C. Guettierc
A. Zaouchea
a Department A of general surgery, Charles-Nicole’sHospital, boulevard 9-Avril, 1006, Tunis, Tunisia
b Department of histopathology, Charles-Nicole’s Hospital,Tunis, Tunisia
c Département d’histopathologie, centre hospitalierKremlin-Bicêtre, Paris, France
∗ Corresponding author.E-mail address: [email protected] (S. Jarboui).
Available online 9 March 2009
oi:10.1016/j.gcb.2008.11.014
arices coliques traitées par hémicolectomie
olonic varices treated by right colectomy
Les varices coliques sont une cause rare d’hémorragieigestive basse, potentiellement grave. Elles appartiennentu groupe des varices ectopiques, c’est-à-dire des varicesxtra-œsophagiennes [1]. De même que les varices œsopha-iennes, leur principale étiologie est l’hypertension portale’origine cirrhotique. Nous rapportons un cas de rectorra-ies à répétition dues à des varices coliques secondairesyant nécessité un traitement chirurgical radical.
Mme B., âgée de 77 ans, était prise en charge pour troispisodes de rectorragies isolées survenus en l’espace derois mois, ayant nécessité la transfusion de cinq culotslobulaires. Elle était sous anticoagulants au long cours
embres inférieurs et d’embolie pulmonaire.Lors du bilan étiologique, la coloscopie mettait en évi-
ence de nombreuses varices coliques droites de grandeaille (Fig. 1 et 2). La fibroscopie œsogastroduodénale ne











![Cancer de Colon[1]](https://img.pdfslide.fr/doc/110x75/577cc60e1a28aba7119d99ae/cancer-de-colon1-578eff9aaa14a.jpg)