-
7/29/2019 surgery Lec # 5
1/14
1
-
7/29/2019 surgery Lec # 5
2/14
2
Bone and Joint Infections
Theres a well-known overlap between orthopedics and dentistry in
the field of bone. What
affects the bones in the skeleton might as well affect the
maxillofacial area and the mandible; an
infection in the tibia or femur could also affect the mandible,
or a cystic arthritis in the knee jointcould occur in the
temporomandibular joint.
The bone is composed of two layers; Cortex and Medulla. The
cortex as the outer layer, and the
medulla as the inner layer containing the bone marrow.
The medical terms used to describe bone infections are
Osteomyelitis and Osteitis. The word
Osteomyelitis is divided into two parts, Osteo: bone and
Myelitis: Bone marrow. So
Osteomyelitis implies that the infection involves not only the
cortex but also the bone marrow
spaces in the medulla, however if the infection is present only
in the cortex of the bone it is
referred to as Osteitis.
Classifications of Osteomyelitis
Osteomyelitis is classified according to the:
I. Routes of Infection1)
Exogenous: A source of microorganism introduced from the
external environmentdirectly to the bone, for example a stab
wound.
2) Hematogeneous: Microorganisms disseminated through the blood
stream from a site ofinfection in the body to settle in the bone.
The source of infection will travel through the
blood to reach the proximal or the metaphyseal part of the bone.
Examples of way the
infection could get through:
- In the infantile stage, Osteomyelitis might be transmitted
through an infectedumbilical chord at birth.
- Through skin infection.- If an adult had history of Urinary
Tract Infection.- Through arterial catheterization or
administration of an IV line for antibiotics
or fluid intake.
-
7/29/2019 surgery Lec # 5
3/14
3
3) Contiguous spread: A direct spread from a nearby focal
infection, most commonlyaffecting the superficial bones (Ex: Tibia
and Ulna) where an infection could easily
extend from the infected overlying soft tissues.
II. Types of Microorganisms: they are organized according to age
groups whereStaphylococcus Aureus is the most common.
1) Neonates ( 5 years (Osteomyelitis is commonly knownas being a
pediatric disease).
Rare in adults unless they are immunocompromised. Boys >
Girls. 1/3 of cases have reported history of trauma. 80% of
Osteomyelitis cases are located in the metaphysis of the bone.
-
7/29/2019 surgery Lec # 5
4/14
4
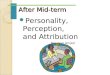
Anatomy of the bone:
Epiphysis: Ends of the bone, either upper or lowerends.
Diaphysis: Site of entry of blood vessels.Growth
platesMetaphysis: Unique anatomical structure and rich
in blood vessels. These blood vessels enter
through the diaphysis as large caliber (largediameter), they
start to narrow down extending
through the bone reaching the metaphysis and
the growth plate (which is active in young age).
The vessels cannot penetrate the growth plate
and they will form a loop (harping loop or reverse
loop) at the metaphysis. So blood flow through
these vessels will slow down gradually, and this
slow blood flow is a good media for bacterial
growth. This is why Osteomyelitis most commonly
occurs at the metaphysis.
** So Osteomyelitis is more common in the
metaphysis area of the bone. But out of all bones in
the body, the Femur Bone (27% of cases), the Tibia,
or long bones in general are the most commonly
affected.
-
7/29/2019 surgery Lec # 5
5/14
5
Stages of Osteomyelitis:
1) Primary Focus Infection2) Stage of Inflammation: Where
chemotaxis of macrophages and other inflammatory
mediators occurs.
3) Formation of sub-periosteal abscess: Abscess may migrate
within the bone through theHaversian canals or could travel by a
duct outside the bone creating what is called a sinus
discharging pus.
*All these changes in the inflammatory habits will increase the
intra-osseous pressure, so
the pus will try to drain at any escape.
4) Sequestrum formation: after the drainage of pus, the bone
will be left with empty spaces
called bony infarction (dead bone).
5) Resolution of infection: New bone formation, and this is very
important for healing
because otherwise the infection will alternate into its chronic
form.
Acute Osteomyelitis
Clinical Picture (Diagnosis):
Three sequels should be taken into consideration when a
physician is trying to reach a
diagnosis to manage a certain case:
1) History:- In most of the cases, Osteomyelitis will be
associated with preceding infections. For
example, if a 5 year old child presents pointing to pain in
his/her femur and this pain was
persisting for that last 48 hours. The mother should be asked
about any history of
previous infections (Ex. Respiratory tract infections,
Tonsillitis, trauma, or even skin
lesions that occurred somewhere else in the body) to identify
the source of infection
transmitted from the blood to the bone.
- The older the child gets, the easier it is to take history,
but the challenge arises when aneonate for example is reported from
the department of prematurity by pediatricians
suspecting an infection in a certain bone. The physician in this
case will relypredominantly on his/her sense and intuition.
Symptoms associated with neonates could
be:
Failure to thrive: the baby refuses to breastfeed and is not
gaining weight. Drowsiness Baby is irritable most of the time
-
7/29/2019 surgery Lec # 5
6/14
6
Most of the cases occur around the knee, distal or proximal
femur, or on the shaftof the femur.
2) Examination:Pain will be very localized rather than diffused;
the area of tenderness will be at its
maximum in a single point, just like a bell ring. So this
presentation is called The Ring
Bell Sign and its an indication for a focus of infection and
will rule out many other
diseases (Ex. Tumors, Trauma, or any metabolic bone
disease).
Affected limb will be reluctant to move.Fever: Patients usually
present with intermediate fever rather than high grade fever,
the reason behind that is that the patients would have already
started taking
medications Ex. Paracetamol or NSAIDs.
MalaiseLoss of appetiteSepticemia (only in severe/toxic
cases)
3) Investigations: How to approach the case?a) Laboratory
Investigations: They are to some extent invasive, Ex. needles
to
withdraw blood.
- Complete blood count (CBC): Standard test for any work up
especially forpatients with suspected Osteomyelitis. This test is
not accurate and does not
give a direct indication to the disease. In infected patients,
levels of WBCs
should be elevated however this occurs only in one third of the
cases, this is
why more sensitive tests should be done; ESR and CRP which are
called
Inflammatory Phase Reactants (both are elevated during
inflammation).
- ESR: Erythrocyte Sedimentation rate. Used more in the follow
up of patientsrather than diagnosis.
- CRP: C-reactive protein test, measures general level of
inflammation in thebody. Elevated in 98% of infected patients,
peaking on day 2 of
inflammation. More specific than ESR since it fluctuates easily
with thebodys inflammatory changes; it rises on infection more
quickly and will
respond to antibiotics faster. So it is the most diagnostic lab
investigation.
- Blood Culture: 50% of cultures from CBC are positive.
-
7/29/2019 surgery Lec # 5
7/14
7
- Direct/Needle aspiration: Using a sterile needle (18gauge) or
a spinal needleafter sterilization with a bit of anesthesia Ex.
Lidocane, a sample is taken
from the suspected location of infection, or if there were any
pus
production it could also be aspired. The aspiration is sent to
blood culturing
(positive in 2/3 of cases).
b) Radiological Investigations: The imaging study for a child
with Osteomyelitis. Plain X-ray:- Initial X-ray: Pathological
changes in the body need time to manifest
themselves, so initial x-rays could appear to be negative/normal
most of
the time, especially in the early few days (72 hours) where the
only sign is
soft tissue elevation. So initially, x-rays are not to depend on
but they are
done to rule out fracture.
- After 1-2 weeks: X-rays are most informative in that period of
time. Theywill start to show rarefaction (reduced density) of bone
and periosteal
reactions.
- More than two weeks: Changes will be more prominent and
infection willspread over the entire bone (Epiphysis, Diaphysis and
Metaphysis).
*Patients cannot wait for a couple of weeks with infection to
have a clear diagnosis, so for
more precise methods of investigation, other non-invasive tests
could be made:
Ultra-Sound: it will be further explained later. (Page 12 ^)
Bone Scan: Its an injection with a nuclear labeled material
(technetium-
99m) where it is up-taken in areas with higher metabolic
rates.
Gallium scan: More sensitive (sensitivity>91%) than bone scan
because inthis test the polymorphonucleus of the white blood cells
themselves are
the marker for the investigation.
Other tests include: CT-scan and MRI. They are not frequently
used if thediagnosis was established from the previous tests,
however if the physician
is having problems with the differential diagnosis especially in
cases of
tumors and Ewings sarcomas they could be done.
-
7/29/2019 surgery Lec # 5
8/14
8
Osteomyelitis in adults:
Osteomyelitis in adults is very rare but if it happened the most
affected locations would be the
vertebrae, specially the thoracolumbar vertebrae.
Symptoms and signs of adults with Vertebral Osteomyelitis:
- Localized pain in the vertebrae.- Back ache- Fever- History of
Urinary tract or Neurological infection or any procedure done in
the near past
(1-2 weeks).
Risk factors:
- Immunocompromisation- Diabetes- Old age
*If the adult is healthy is it very unlikely to develop this
sort of infection.
Differential Diagnosis:
Septic Arthritis: Septic Arthritis is the infection of the joint
itself. In some cases, especiallyin young patients, the infection
might attack the metaphysis as Osteomyelitis and then
easily spread into the joint causing secondary Septic Arthritis.
This occurs particularly in
younger age groups because of two reasons:
1. The growth barrier did not yet make a border between the
metaphysis and theepiphysis.
2. The metaphysis is still a part of the joint. Rheumatologic
Disorders Sickle Cell Crisis Thalassemic Crisis Ewing's Sarcoma: It
is a malignant tumor of the bone. The lamellated or "onion
peel"
appearance of the bone seen on a radiograph with this disease is
similar to what is seen
with Osteomyelitis.
-
7/29/2019 surgery Lec # 5
9/14
9
Management of Osteomyelitis:
Once the diagnosis of Osteomyelitis is confirmed, the patient
must be hospitalized. Unlike any
other type of infection (ex: tonsillitis), bone infections are
difficult to treat because the infection
is hidden within a barrier (bone), so a strong antibiotic at
high concentration is needed to
penetrate through the bone and reach the site of infection in an
adequate amount.
Unfortunately, oral antibiotics cannot achieve this penetration,
and thus IV antibiotics are
needed in early stages. Other reasons for hospitalization are
that the patient has high fever and
requires IV fluids for hydration and correction of the
electrolyte imbalance. In addition, the
patient must be immobilized and analgesics might be needed for
the pain.
The specific treatment of Osteomyelitis is the administration of
antibiotics at an early stage as
they become less potent when administered at a late stage. One
knows that it is impractical to
start a course of antibiotic before knowing for sure the exact
type of microorganism causing theinfection (ex: Staph, Strep,
Pseudomonas, or E.coli) and a clinician should normally wait
for
laboratory results and blood cultures to decide what type of
antibiotic is most suitable. However,
a patient with Osteomyelitis should not be left without
treatment waiting for laboratory results
(which take 72 hours ~ 3 days) so empirical therapy must be
used.
Empirical therapy means that an antibiotic is chosen by common
sense according to the
microorganism that is most likely present. Examples of empirical
antibiotics are: Gentamycin,
Cephotaxime, Ceforuxime, Clindamycin, Vancomycin. These
empirical antibiotics should be given
in the first 72 hours until the laboratory results are out.
Once the specific microorganism causing the infection is known,
the patient should be treated
with a more specific antibiotic. For example, if the infection
is caused by Staph aurous, the
patient is treated by Penicillins (Amoxicillin and Ampicillin)
or by Cephalosporins (Cephozulin). If
the cause of infection is a gram negative bacteria like
Salmonella, the patient may be give
Ampicillin, etc.
IV antibiotics should be given for about 3 weeks followed by
oral antibiotics, the patient starts
taking oral antibiotics once his/her symptoms alleviate (no
pain, no fever, CRP level normal,
ESR
-
7/29/2019 surgery Lec # 5
10/14
10
Indications for Surgery:
1. Abscess formation: surgery is required in any case where soft
tissue or subperiostealabscess is present (when pus is discharged).
Antibiotics should not be used in the
presence of an abscess since it will exacerbate the situation
because the abscess will
enclose itself to prevent the entry of the antibiotic. So as a
general rule in medicine,
abscess formation requires incision and drainage.
2. When a Fine Needle Aspiration reveals a purulent fluid,
suggesting the presence of pus.3. Failure of antimicrobial
treatment in the first 3 days. In this case, the bone should be
drilled and the Sequestrum (the dead bone cavity depriving the
bone from blood
supply) should be removed by a process called Sequestrectomy.
Sequestrectomy
should be handled by an expert especially if the Sequestrum is
near the growth plate.
Complications of Osteomyelitis:
- Focal infection (ex: in the head of the femur) might spread
throughout the body, causingsepticemia.
- Progression into a Septic Arthritis.- If the infection spreads
and involved a nearby growth plate, this will cause growth
disturbances.
- Pathological fractures, since Osteomyelitis weakens the bone.-
Progression into chronic Osteomyelitis (very dangerous
complication, should be avoided)
Sub-Acute Osteomyelitis
This type of Osteomyelitis is challenging because of its unclear
presentations and because it
usually mimics other Oncological disorders such as Osteoid
Osteoma.
Unlike Acute Osteomyelitis, a patient with Sub-Acute
Osteomyelitis is presented with a longer
history of pain (1-2 months); the pain is usually mild,
intermittent, irritating and the onset of pain
is not acute. Other constitutional symptoms like fever and
toxemia are not present. Also, themicroorganism involved is less
virulent and not powerful enough to cause the usual
pathological
changes.
Initial radiographs may be abnormal, and laboratory data are not
always conclusive as in acute
Osteomyelitis. For instance, WBC count may be normal, and CRP
might as well be normal. So in a
case where a patient has a long history of pain in his distal
tibia, but his/her test results show a
-
7/29/2019 surgery Lec # 5
11/14
11
normal WBC count and CRP level, then Sub-Acute Osteomyelitis
should be suspected as well as
other malignancies. In this case, a biopsy is usually taken, and
this biopsy is cultured. The culture
will usually show Staphylococcus or Gramve anaerobic
Pseudomonas, but in more than half of
the cases the cause is polymicrobial. Polymicrobial infections
can be treated by Gentamycin,
Tinam, Imipenem
What is most concerning about Sub-Acute Osteomyelitis is that it
has a high recurrence rate of
about 40%.
Treatment of Sub-Acute Osteomyelitis:
After results of the tissue culture are obtained, IV antibiotics
should be administered followed by
oral antibiotics for at least one month.
Chronic Osteomyelitis
Chronic Osteomyelitis is usually a progression of an untreated
Acute Osteomyelitis, and here the
patient entered whats called an On-Off phenomenon. In On-Off
phenomena, the patient will
experience times free of symptoms (4-5moths or even more), and
other times where the
symptoms relapse (may last for 2-3 weeks).
The pain may be continues or intermitted, and pus may be
discharged from a sinus, which opens
at times and closes at others.
Patients with higher risk of progression of acute Osteomyelitis
into Chronic Osteomyelitis usually
suffer from:
Nutritional deficiencies Vascular Diseases Low immunity Diabetes
Acute Osteomyelitis caused by a high virulent organism not
responding to antimicrobial
agents.
As mentioned above, Chronic Osteomyelitis is most commonly a
complication of an
unsuccessfully treated Osteomyelitis. However, it might be due
to a post-traumatic injury
especially in war victims where a microorganism has entered the
bone through a stab or a
contaminated injury. Chronic Osteomyelitis might also occur as a
post-operative complication.
-
7/29/2019 surgery Lec # 5
12/14
12
Investigations:
- Lab test- Cultures (maybe pus culture)- Plain X-ray- Sinogram:
Dye injected into the sinus to trace and follow the amount of bone
involved,
sometimes the whole bone is found to be complicated.
Complications of Chronic Osteomyelitis:
- High recurrence rate- Pathological fractures- Metabolic bone
disease- Carcinogenic transformation
Treatment of Chronic Osteomyelitis is unfortunately very
depressing for the patient due to its
long period. The treatment includes: antibiotic administration,
local antibiotic inside the bone
defect (ex: Gentamycin beads), and maintenance of bone stability
to avoid pathological
fractures.
Septic Arthritis
Septic Arthritis is an infection in the joint, and the word
'Septic' implies that this type of Arthritis
is caused by a microbial agent, mainly bacterial (Staph aurous,
Strept, Pnemococcus). It might
also be due to a viral infection, which tends to be transient
and does not usually cause the
destructive changes inside the joint.
A good way to distinguish between Septic Arthritis and other
forms of Arthritis (ex: Rheumatoid)
is that Septic Arthritis is monoarticular, meaning that it
affects only one joint of the body, unless
if it's caused by Neisseria Gonorrhea were the infection will
occur in multiple joints (ex: both
knee joints).
Septic Arthritis occurs most commonly in the hip joint, with
more than 50% of cases seen in
pediatric age groups of less than 3 years of age. So, a common
presentation of this disease in the
ER is a child (usually
-
7/29/2019 surgery Lec # 5
13/14
13
In most of the cases, Septic Arthritis is seen in association
with Osteomyelitis. However, it is not
important to find out whether Osteomyelitis occurred first and
caused a secondary Septic
Arthritis or vice versa
Pathogeneses:
Changes in the Synovium (synovial fluid) lining the joint
capsule. Vascular Changes (because of inflammation) Attraction of
WBC, macrophages, and inflammatory mediators (Interleukins)
causing
further exaggeration of the condition.
Clinical picture of Acute Septic Arthritis:
Huge swelling around the infected joint Pain, Calor (hotness),
redness Immobilization Fever Malaise
Lab investigations:
CBC CRP, ESR
Blood Culture (40-50% positive) Plain X-ray Bone Scan/ Gallium
Scan Ultrasound
^Ultrasound is an easy, noninvasive, and informative test that
is necessary for the
diagnosis of Septic Arthritis. It enables the clinician to
examine hidden joints (for example
hip joint), and check for the presence of accumulated fluids
within it. A needle aspiration
is performed on the accumulated fluid, in case of its presence,
under the guidance of the
ultrasound. As a role, if WBC count in this fluid showed up to
be greater than 50,000 withmore than 90% being polymorphonuclear,
then a diagnosis of Septic Arthritis is confirmed
even if the blood cultures were negative.
In the absence of an ultrasound (limited facilities), an X-ray
might be sufficiently
informative. The diagnostic mark in an X-ray is the teardrop
sign, which is the space
between the acetabulum (concavity in the pelvis where the head
of the femur meets,
-
7/29/2019 surgery Lec # 5
14/14
14
forming the hip joint) and the head of the femur compared to the
other healthy hip joints.
If the space is widened, this is an indication of fluid
accumulation in the joint pushing the
head of the femur laterally.
Differential Diagnosis:
1. Acute Osteomyelitis (same management and treatment)2.
Transient Sinovitis of the hip: viral reactive Arthritis, patients
usually have history
of Upper Respiratory Tract Infection, Hemarthrosis (bleeding
into joint spaces)
etc
Treatment of Septic Arthritis:
1. A patient with Septic Arthritis requires admission to
hospital.2. The infected joint should be splinted to ensure
fixation and immobilization, because it'svery painful to the
patient.3. Empirical antibiotics are given followed by definitive
antibiotics.4. Surgical drainage: it is of high importance to drain
all the pus accumulated inside the joint
to avoid lysis and destruction of the cartilage by inflammatory
mediators.
Complications of Septic Arthritis:
- Secondary Osteoarthritis: Occurs when the patient is not
treated from the joint infectionresulting in growth disturbances in
that joint, leg shorter than the other, and the need for
an early artificial joint.- Cartilage damage- Slow dislocation
of the joint- Arrest of bone growth
Done By: Lama Ashour & Raya Dawood