Embed Size (px)
Citation preview
Cas clinique
DOI of or1Vascular
Hospital, Turi2Departme
Turin, Italie.
CorrespondSurgery Unit,Turin, Italie, E
Ann Vasc Surhttp://dx.doi.or� Annals of V�Edit�e par ELS
Traitement en urgence d’une fistuleaorto-esophagienne et d’une fistuletrach�eo-esophagienne par endoproth�eseaortique thoracique et endoproth�eseoesophagienne : Un cas mal diagnostiqu�een tant que cancer oesophagien
Emanuele Ferrero,1 Andrea Viazzo,1 Michelangelo Ferri,1 Rodolfo Rocca,2 A. Pecchio,1
Salvatore Piazza,1 Pia Cumbo,1 Giuseppe Berardi,1 Franco Nessi,1 Turin, Italie
Les fistules aorto-esophagiennes sont rares mais mortelles si non trait�ees. La chirurgie thora-cique ouverte est associ�e �a une mortalit�e et �a une morbidit�e op�eratoires �elev�ees. Nous rap-portons le cas d’un homme de 77 ans qui, trait�e par r�eparation aortique endovasculairethoracique (TEVAR) pour an�evrysme thoracique descendant dans un autre centre, apr�es un�episode aigu d’h�emat�em�ese et de moelena avait �et�e transfer�e dans notre centre. Le scannercorps entier montrait la re-perfusion du sac an�evrysmal thoracique descendant (8,8 cm dediam�etre) au niveau de la zone proximale et distale d’ancrage de TEVAR (endofuite de type I)sans signes clairs de fistule avec la lumi�ere oesophagienne. Le malade a eu un nouveau TEVAR�a travers l’implantation pr�ec�edente avec ancrage proximal tr�es proche de l’art�ere sous-clavi�eregauche et ancrage distal juste au-dessus du tronc coeliaque. En raison de la pr�esence d’unefistule trach�eo-esophagienne, une endoproth�ese oesophagienne a �et�e implant�ee peu apr�es, etune j�ejunostomie a �et�e faite. �A 30 jours, le malade �etait en bonne �etat g�en�eral, mais il est mort �a3 mois. Les fistules aorto-oesophagiennes sont rares et habituellement mortelles ; l’identificationpr�ecoce et le traitement par TEVAR empechent l’exsanguination imm�ediate des malades, maisapr�es d�eploiement de l’endoproth�ese, la plupart des malades sont �a risque de complicationsinfectieuses. L’arret du saignement et la restauration de la circulation sont l’urgence primordiale,mais les complications infectieuses et la r�eparation oesophagienne demeurent des probl�emesnon r�esolus.
iginal article: 10.1016/j.avsg.2011.06.009.
and Endovascular Surgery Unit, Mauriziano Umberto In, Italie.
nt of Gastroenterology, Mauriziano Umberto I Hospital,
ance : Emanuele Ferrero, Vascular and EndovascularMauriziano Umberto I Hospital, Largo Turati 62, 10128-mail: [email protected]
g 2011; 25: 1142.e1-1142.e5g/10.1016/j.acvfr.2013.02.011ascular Surgery Inc.EVIER MASSON SAS
Aortoesophageal fistula (AEF) is rare but fatal
if untreated; it results from an abnormal communi-
cation between the aorta and the esophagus
and constitutes less than 10% of all aortoenteric
communications; the clinical manifestation is gas-
trointestinal hemorrhage, melena, and hemateme-
sis. Generally, it is caused by thoracic aortic
aneurysms, foreign body ingestion, esophageal mali-
gnancy and traumatic aorticwounds, ruptured pene-
trating aortic ulcers, esophageal or bronchogenic
malignancies, and thoracic surgery.1,2 The thoracic
endovascular aortic repair (TEVAR) has become a
therapeutic alternative for high-risk patients with
1216.e1
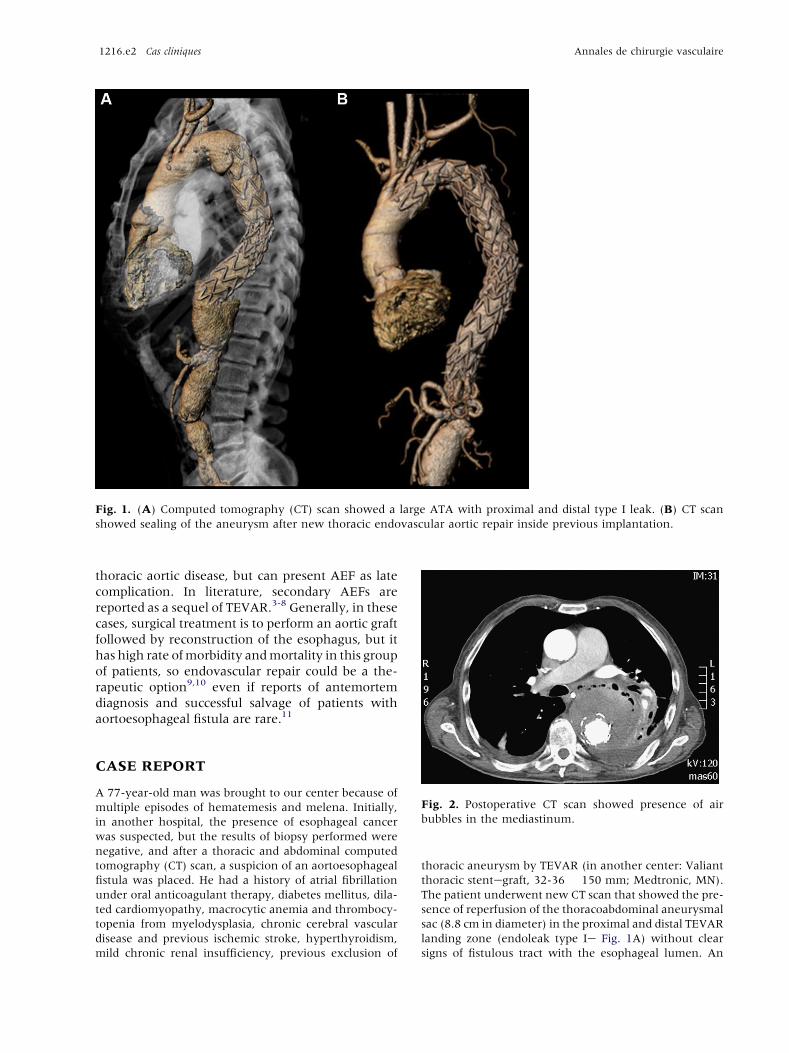
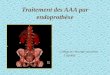
Fig. 1. (A) Computed tomography (CT) scan showed a large ATA with proximal and distal type I leak. (B) CT scan
showed sealing of the aneurysm after new thoracic endovascular aortic repair inside previous implantation.
1216.e2 Cas cliniques Annales de chirurgie vasculaire
thoracic aortic disease, but can present AEF as late
complication. In literature, secondary AEFs are
reported as a sequel of TEVAR.3-8 Generally, in these
cases, surgical treatment is to perform an aortic graft
followed by reconstruction of the esophagus, but it
has high rate ofmorbidity andmortality in this group
of patients, so endovascular repair could be a the-
rapeutic option9,10 even if reports of antemortem
diagnosis and successful salvage of patients with
aortoesophageal fistula are rare.11
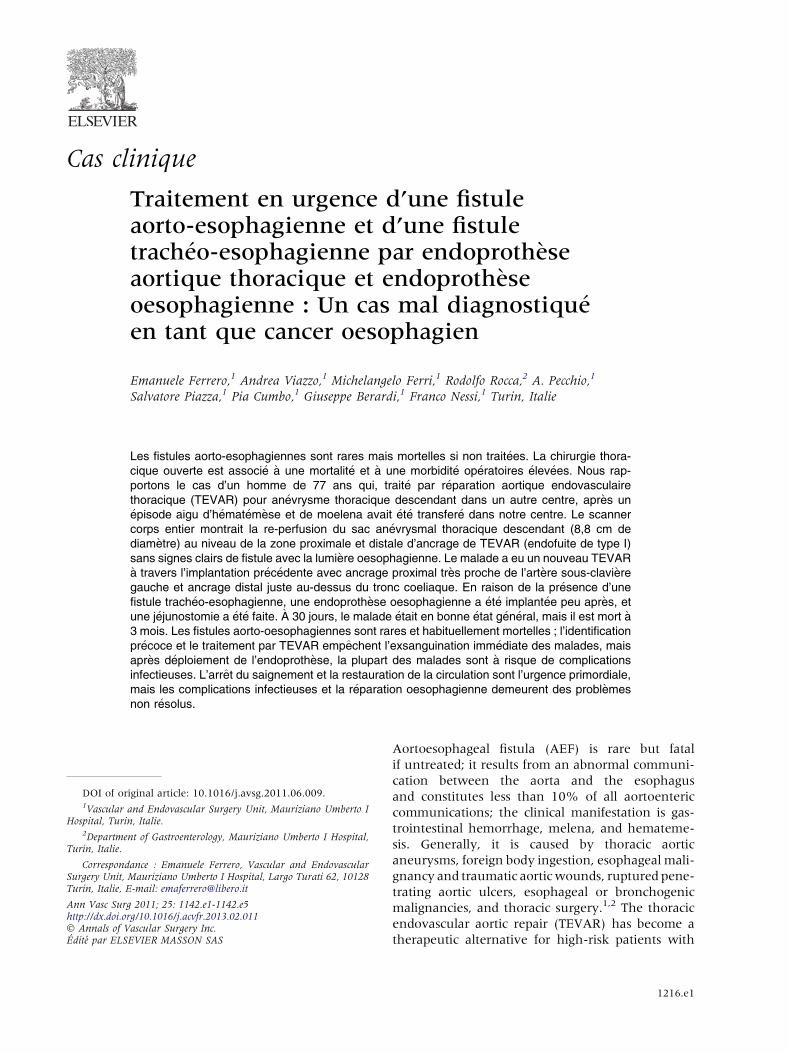
Fig. 2. Postoperative CT scan showed presence of air
bubbles in the mediastinum.
CASE REPORT
A 77-year-old man was brought to our center because of
multiple episodes of hematemesis and melena. Initially,
in another hospital, the presence of esophageal cancer
was suspected, but the results of biopsy performed were
negative, and after a thoracic and abdominal computed
tomography (CT) scan, a suspicion of an aortoesophageal
fistula was placed. He had a history of atrial fibrillation
under oral anticoagulant therapy, diabetes mellitus, dila-
ted cardiomyopathy, macrocytic anemia and thrombocy-
topenia from myelodysplasia, chronic cerebral vascular
disease and previous ischemic stroke, hyperthyroidism,
mild chronic renal insufficiency, previous exclusion of
thoracic aneurysm by TEVAR (in another center: Valiant
thoracic stentegraft, 32-36 � 150 mm; Medtronic, MN).
The patient underwent new CT scan that showed the pre-
sence of reperfusion of the thoracoabdominal aneurysmal
sac (8.8 cm in diameter) in the proximal and distal TEVAR
landing zone (endoleak type Ie Fig. 1A) without clear
signs of fistulous tract with the esophageal lumen. An
Fig. 3. (A) Barium radiography reported a bronchial-esophageal fistula. (B) Bronchial-esophageal fistula excluded by
esophageal endoprosthesis.
Vol. 25, No. 8, 2011 Cas cliniques 1216.e3
esophagogastroduodenoscopy was performed, and it
showed, at 30 cm from dental arch, a foramen (15 mm in
diameter) with regular margins; the bottom of the lesion
was covered by granulation tissue and blood clots; no
bleedingwas observed, and the lesion appeared suggestive
not of malignancy but of esophageal fistula. Because of
persistent intermittent hematemesis and the need for
blood transfusion, patient underwent new TEVAR treat-
ment (proximally two Relay 28-200 and 28-150 mm:
Bolton Medical, FL; distally Endurant 32-49 mm: Med-
tronic, MN), inside previous implantation, with proximal
landing very close to left subclavian artery and distal
landing just above celiac trunk. The CT scan performed on
fourth postoperative day showed perfect sealing of the
aneurysm (Fig. 1B), but presence of air bubbles in the
mediastinum (Fig. 2), and a bronchial-esophageal fistula
was detected. A barium X-ray examination of the eso-
phagus was performed; it confirmed the presence of the
bronchial-esophageal fistula (Fig. 3A). Due to the poor
general condition of the patient and high operative risk in
executing an esophageal reconstruction, we decided to
exclude the bronchial-esophageal fistula and position
an esophageal endoprosthesis (Fig. 3B) associated with
jejunostomy. The patient underwent enteral nutrition via
a needle catheter jejunostomy; even though the patient
did not present fever or leukocytosis due to air collection,
detected onCT, we started an aggressive antibiotic therapy
(tigecycline, ertapenem, teicoplanin). At 30 days’ follow-
up, the patient was alive in fairly general condition; no
spinal cord and visceral ischemia was present. After 3
months, the patient died suddenly without a specific
cause, probably due to infection.
DISCUSSION AND CONCLUSION
AEF is a rare cause of massive gastrointestinal bleed-
ing and is usually a fatal condition. In the English
literature, a relatively small number of TEVARs for
AEF/ABF are published to date, consisting primarily
of single case reports or small case series with less
than 12 patients,12 and this may account for a
considerable underestimation of the problem. The
most common cause of fistulization is the erosion of
a thoracic aortic aneurysm,13 probably due to the
compression of the esophagus or the airways by the
aneurysm that may result in a local inflammatory
response with formation of stable adhesions and

1216.e4 Cas cliniques Annales de chirurgie vasculaire
tissue necrosis leading to erosion and final fistuli-
zation. While, in ruptured aortic aneurysm, the
extravasation of blood and periaortic hematoma,
with increased local inflammatory response and
compression of surrounding organs, may play a role
in late fistulization.14 Chiesa15 in his report consi-
dered the excessive TEVAR stent-graft oversizing
as possible additional mechanism of AEF fistuliza-
tion: He found that 42% of patients presenting late
AEF/aortobronchial fistulae had a proximal over-
sizing of 20% or more; this probably caused a
deterioration of the arterial wall, the stent-graft
migration, and the aortic aneurysm enlargement.
Generally, common presenting symptoms of AEF
are characteristic Chiari triad features, including
chest pain and sentinel hematemesis of red blood
followed at a variable interval of time by rapidly fatal
massive exsanguinating hematemesis.11 In a few
cases, AEF can be suspected on the basis of isolated
sepsis or septic embolism in a lower extremity16;
other suggestive findings include dysphagia and/or
chest pain and history of surgical treatment
involving the thoracic aorta. The CT scan is the first
imaging study performed in most of the cases, but
rarely detects fistulous tracts. Endoscopy is the most
sensitive and specific method for the diagnosis of
AEF, but it often requires sedation and entails the
risk of dislodging clots during the progress of the
endoscope, which can cause fatal bleeding. Early
recognition, a high index of suspicion, and impro-
ved critical care and emergency services have lead to
an increasing number of cases being recognized
before fatal hemorrhage. Mortality after surgery for
thoracic aortic fistulae reaches 61% in cases of pri-
mary etiology and 78% in cases of secondary fistu-
lae.17,18 Endoluminal repair of thoracic aortic
disease requiring emergent or urgent treatment has
yielded encouraging early results with low morbi-
dity and mortality rates compared with open sur-
gery.19 TEVAR prevents immediate exsanguination
in patients with AEF, but after deployment of the
endograft, most patients are at risk for infectious
complications and death. Cessation of bleeding and
restoration of circulation are of paramount urgency,
whereas esophageal reconstruction could be carried
out later, even if this did not guarantee the survival
of the patient. In the overtly moribund patient,
TEVAR has been proposed as the most appropriate
definitive strategy, as a palliative procedure, whe-
reas in good surgical candidates, coverage of the
aortic lesion, along with an aggressive antibiotic
therapy, may be used to achieve an improvement in
the patient’s general conditions, serving as a
‘‘bridge’’ to open surgical treatment of the aortic
and/or esophageal/ bronchial defect. Following
successful TEVAR, in absence of clear signs of rein-
fection or bleeding, there is no general consensus
concerning the need of staged surgical intervention.
Although clear limitations of the TEVAR strategy
alone include the risk of reinfection and septic
complication, due to the inability to debride or drain
the mediastinum, some success with this approach
has been reported in the literature.20,21 We think
that TEVAR alone does not provide complete and
durable cure for AEF, that these patients need to be
followed closely to evaluate the opportunity and the
appropriate timing for a secondary surgical pro-
cedure according to patient conditions and the grade
of sepsis, but in patients at high risk for complica-
tions with open surgical repair, we consider TEVAR
as a potential definitive treatment. In conclusion,
AEF, although rare and probably underestimated, is
considered a fatal condition. AEF sometimes is a late
sequelae of TEVAR. Surgical and endovascular
treatments are associated with high mortality, but
conservative treatment is not a viable option
because AEF is inevitably fatal if untreated; in these
cases, TEVAR has a predominant role in controlling
the massive hemorrhage associated with AEF, but
infectious diseases and esophageal repair remains an
open problem.
REFERENCES
1. Hance KA, Hsu J, Eskew T, Hermreck AS. Secondary aor-
toesophageal fistula after endoluminal exclusion because of
thoracic aortic transaction. J Vasc Surg 2003;37:886-888.
2. Hollander JE, Quick G. Aortoesophageal fistula: a compre-
hensive review of the literature. Am JMed 1991;91:279-287.
3. Riesenman PJ, Farber MA, Mauro MA, Selzman CH,
Feins RH. Aortoesophageal fistula after thoracic endo-
vascular aortic repair and transthoracic embolization. J Vasc
Surg 2007;46:789-791.
4. Isasti G, G�omez-Doblas JJ, Olalla E. Aortoesophageal fistula:
an uncommon complication after stent-graft repair of an
aortic thoracic aneurysm. Interact Cardiovasc Thorac Surg
2009;9:683-684.
5. Neuhauser B, Czermak BV, Fish J, et coll. Type A dissection
following endovascular thoracic aortic stent-graft repair. J
Endovasc Ther 2005;12:74-81.
6. Bockler D, Schumacher H, Ganten M, et coll. Complications
after endovascular repair of acute symptomatic and chronic
expanding Stanford type B aortic dissections. J Thorac Car-
diovasc Surg 2006;132:361-368.
7. Eggebrecht H, Mehta RH, Dechene A, et coll. Aortoeso-
phageal fistula after thoracic aortic stent-graft placement: a
rare but catastrophic complication of a novel emerging
technique. JACC Cardiovasc Interv 2009;2:570-576.
8. Porcu P, Chavanon O, Sessa C, Thony F, Aubert A, Blin D.
Esophageal fistula after endovascular treatment in a type B
aortic dissection of the descending thoracic aorta. J Vasc
Surg 2005;41:708-711.
9. Martens K, De Mey J, Everaert H, Delvaux G, Van Den
Brade P. Aortoesophageal fistula following endovascular
exclusion of a thoracic aneurysm. Int Angiol 2007;26:
292-296.

Vol. 25, No. 8, 2011 Cas cliniques 1216.e5
10. Flores J, Shiiya N, Kunihara T, Yoshimoto K, Yasuda K.
Aortoesophageal fistula: alternatives of treatment. Case
report and literature review. Ann Thorac Cardiovasc Surg
2004;10:241-246.
11. Kieffer E, Chiche L, Gomes D. Aortoesophageal fistula.
Value of in situ aortic allograft replacement. Ann Surg
2003;238:283-290.
12. Jonker FH, Heijmen R, Trimarchi S, Verhagen HJ, Moll FL,
Muhs BE. Acute management of aortobronchial and aor-
toesophageal fistulas using thoracic endovascular aortic
repair. J Vasc Surg 2009;50:999-1004.
13. Coselli JS, Crawford ES. Primary aortoesophageal fistula
from aortic aneurysm: successful surgical treatment by use
of omental pedicle graft. J Vasc Surg 1990;12:269-277.
14. Piciche‘ M, De Paulis R, Fabbri A, Chiariello L. Postoperative
aortic fistulas into the airways: etiology, pathogenesis, pre-
sentation, diagnosis, and management. Ann Thorac Surg
2003;75:1998-2006.
15. Chiesa R, Melissano G, Marone EM, Marrocco-
Trischitta MM, Kahlberg A. Aorto-oesophageal and
aortobronchial fistulae following thoracic endovascular
aortic repair: a national survey. Eur J Vasc Endovasc Surg
2010;39:273-279.
16. Seymour EQ. Aortoesophageal fistula as a complication of
aortic prosthetic graft. Am J Roentgenol 1978;131:160-161.
17. Pipinos II, Reddy DJ. Secondary aortoesophageal fistulae.
Ann Vasc Surg 1999;13:649-652.
18. Dossa CD, Pipinos II, Shepard AD, Ernst CB. Primary aor-
toenteric fistula: part II. Primary aortoesophageal fistula.
Ann Vasc Surg 1994;8:207-211.
19. Bell RE, Taylor PR, Aukett M, Sabharwal T, Reidy JF.
Results of urgent and emergency thoracic procedures trea-
ted by endoluminal repair. Eur J Vasc Endovasc Surg
2003;25:527-531.
20. Bond SE, McGuinness CL, Reidy JF, Taylor PR. Repair of
secondary aortoesophageal fistula by endoluminal stent-
grafting. J Endovasc Ther 2001;8:597-601.
21. Rodriguez JA, Olsen DM, Shtutman A, et coll. Application of
endograft to treat thoracic aortic pathologies: a single center
experience. J Vasc Surg 2007;46:413-420.















![· Web viewRadiographie d'une fistule [Fistulographie] 17.01.03 Scanographie, sans précision topographique ZZQH001 Scanographie d'une fistule ZZQK024 Scanographie de 3 territoires](https://img.pdfslide.fr/doc/110x75/6082029a8abcec493b1ef04b/web-view-radiographie-dune-fistule-fistulographie-170103-scanographie-sans.jpg)