Canad. Med. Ass. J.Sept. 19, 1964, vol. 91 PECKHAM .i.rn OTHERS: CONGENITAL AORTIC STENOSIS 639
Congenital Aortic Stenosis: Some Observations on theNatural History and Clinical AssessmentGERALD B. PECKHAM, M.D.,* JOHN D. KEITH, M.D. and
JOHN R. EVANS, M.D., Toronto
SOMMAIRE
Les auteurs ont pass6 en revue trois centsmalades dont l'&ge maximum ne d6pas-sait pas 30 ans et chez lesquels avait 6t6port6 le diagnostic de st.nose de l'aorte.Cette 6tude avait pour but de recuejilir desrenseignements sur 1'exactitude du bilanclinique et sur l'.volution clinique naturellede la maladie laiss6e sans traitement. Lamort subite s'est produite rarement et uni-quement chez des malades pr6sentant lessignes dliniques d'une occlusion grave.Chez les nourrissons, l'apparition pr6coceet la nature mortelle de la pathologie6taient la cons6quence d'autres l6sionscardiaques. Chez 83 malades, la corr6lationdes signes cliniques avec les donn6es deI'hrmodynamique indiquait qu'une st6nosegrave existait si le bruit systolique s'ac-compagnait d'un fr6missement et d'uneaugmentation de la pulsation du ventriculegauche, d'une diminution du pouls del'art.re brachiale ou d'une hypertrophie duventricule gauche sur l'6lectrocardiogram-me. L'examen clinique n'a pas permisd'.tablir avec certitude le siege de 1'oc-clusion, mais un bruit pr6cose d'6jectionsystolique constituait une forte preuvequ'il ne s'agissait pas d'une st6nose sous-valvulaire.
640 PECKHAM AND OTHERS: CONGENITAL AORTIC STENOSIS Canad. Med. Ass. J.Sept. 19, 1964, vol. 91
30 mm. Hg or greater, in agreement with resultsreported by Hancock, Fleming and Abelmann.'5' 16A standard 12-lead electrocardiogram was per-formed on all patients, and criteria for the diagnosisof atrial and ventricular hypertrophy were thoseof Keith, Rowe and Vlad7 for children, and ofGrant8 for adults. The cardiothoracic ratio andevidence of poststenotic dilatation of the ascendingaorta were obtained from chest roentgenograms.
TABLE 1.-INCIDENCE OF ASSOCIATED ABNORMALITIES IN25 PATIENTS WITH CONGENITAL AORTIC STENOSIS*
Number ofType of lesion patients
Patent ductus arteriosus.Endocardial fibroelastosis.Coarctation of the aorta.Ventricular septal defect.Pulmonary stenosis.Atrial septal defect (secundum).Mitral stenosis.
*19 patients under 18 months of age.
141154422
TABLE 11.-CLINICAL FINDINGS IN 300 PATIENTS WITH CONGENITALAGETIC STENOSIS AT VARIOUS AGE GROUPS
iSmo.-Age in years 0-1 4 yr. 5-9 10-14 15-20 21-30 Total
No. of patients 24 38 84 101 39 14 300
SymptomS and Signs:Dyspnea 18Syncope 0Angina 0Heart failure 18SyStolic thrill 1Ejection click 6LV impulse 1Pulse pressure
25 mm.Hgor less 2
ElectrocardiogramLVH 10RVH 10
X-RayCTR>50%Postst'notic
dilatation
16
0
1102
34236
6420715335
141240905754
191172
321524
13653114
14
71341825
239158134
17 31 43 17 4 114
16 48 67 26 12 1793 0 0 0 0 13
23
1
30
14
38
22
9
12
4
4
120
53
abnormal. The presence of a systolic thrill, in-creased left ventricular impulse or reduced pulsepressure was exceedingly rare in patients underone year of age.The electrocardiogram (EGG) showed evidence
of left ventricular hypertrophy by voltage in 179patients, and 63 of these showed the "strain" patternof T-wave inversion in the left precordial leads. In13 patients under 18 months of age with multiplecardiac lesions, right ventricular hypertrophy alonewas present in 10 and was associated with leftventricular hypertrophy in three more. No electro-cardiographic abnormality was detected in 108patients.The cardiothoracic ratio was greater than 50%
in 120 cases. Poststenotic dilatation of the ascend-ing aorta was noted in 53 cases on chest roentgeno-gram or fluoroscopy and was recognized chiefly inpatients over five years of age.Sudden death occurred in four patients in this
series at 6, 8, 12 and 16 years of age. In each pa-tient there was a thrill associated with the murmurand an increased left ventricular impulse. TheEGG showed left ventricular hypertrophy with astrain pattern in three patients and complete leftbundle branch block in the fourth.The incidence of associated lesions was higher
than that reported by others," but this might beexplained by the large number of patients under18 months of age. All patients with associatedlesions had valvular rather than subvalvularstenosis. Endocardial fibroelastosis of the leftatrium or ventricle was present in 11 patients. Onepatient had aortic stenosis, patent ductus arteriosusand coarctation of the aorta; others have notedthis triad with both valvular and subvalvular aorticstenosis.'82' Combined aortic and pulmonary valvestenosis"' 24,28 occurred in four of our patients,two of whom had the rubella syndrome.
RELATIONSHIP OF THE CLINICAL DATA TOSrrE AND SEVERITY OF GEsmucrIoN
Retrograde aortic and/or trans-septal left-heartcatheterization was carried out in 83 patients in-
Canad. Med. Ass. J.Sept. 19, 1964, vol. 91 PEcIUAM . OTHERS: CONGENITAL AORTIC Sn.iosis .641
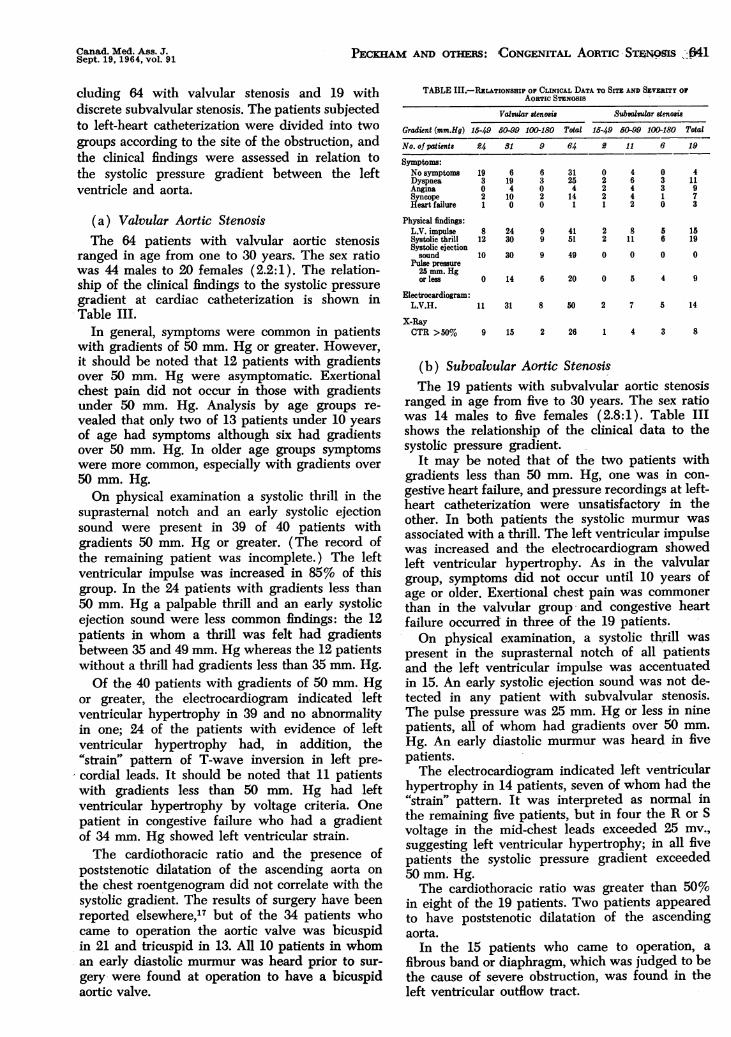
cluding 64 with valvular stenosis and 19 withdiscrete subvalvular stenosis. The patients subjectedto left-heart catheterization were divided into twogroups according to the site of the obstruction, andthe clinical findings were assessed in relation tothe systolic pressure gradient between the leftventricle and aorta.
(a) Valvular Aortic StenosisThe 64 patients with valvular aortic stenosis
ranged in age from one to 30 years. The sex ratiowas 44 males to 20 females (2.2:1). The relation-ship of the clinical findings to the systolic pressuregradient at cardiac catheterization is shown inTable III.
In general, symptoms were common m patientswith gradients of 50 mm. Hg or greater. However,it should be noted that 12 patients with gradientsover 50 mm. Hg were asymptomatic. Exertionalchest pain did not occur in those with gradientsunder 50 mm. Hg. Analysis by age groups re-vealed that only two of 13 patients under 10 yearsof age had symptoms although six had gradientsover 50 mm. Hg. In older age groups symptomswere more common, especially with gradients over50 mm. Hg.On physical examination a systolic thrill in the
suprasternal notch and an early systolic ejectionsound were present in 39 of 40 patients withgradients 50 mm. Hg or greater. (The record ofthe remaining patient was incomplete.) The leftventricular impulse was increased in 85% of thisgroup. In the 24 patients with gradients less than50 mm. Hg a palpable thrill and an early systolicejection sound were less common findings: the 12patients in whom a thrill was felt had gradientsbetween 35 and 49 mm. Hg whereas the 12 patientswithout a thrill had gradients less than 35 mm. Hg.Of the 40 patients with gradients of 50 mm. Hg
or greater, the electrocardiogram indicated leftventricular hypertrophy in 39 and no abnormalityin one; 24 of the patients with evidence of leftventricular hypertrophy had, in addition, the"strain.. pattern of T-wave inversion in left pre-cordial leads. It should be noted that 11 patientswith gradients less than 50 mm. Hg had leftventricular hypertrophy by voltage criteria. Onepatient in congestive failure who had a gradientof 34 mm. Hg showed left ventricular strain.The cardiothoracic ratio and the presence of
poststenotic dilatation of the ascending aorta onthe chest roentgenogram did not correlate with thesystolic gradient. The results of surgery have beenreported elsewhere,'7 but of the 34 patients whocame to operation the aortic valve was bicuspidin 21 and tricuspid in 13. All 10 patients in whoman early diastolic murmur was heard prior to sur-gery were found at operation to have a bicuspidaortic valve.
AoaTIc S.ssosss
Valvular stenosie Subsainslar atenosie
Gradient (mm.Hg) 15-49 50-99 1(K)-iSO Total 15-49 50-99 1(K)-iSO Total
No. of patients 54 81 9 64 £ 11 6 19
Symptoms:No symptoms 19Dyspnea 3Angina ()Syncope 2Heart failure 1
Physical findings:L.V. impulse 8Systolic thrill 12Systolic ejection
sound 10Pulse pressure
25 mm. Hgorlese 0
Electrocardiogram:L.V.H. 11
X-RayOTR >50% 9
6194
100
2430
30
14
31
15
63020
9
9
9
31254
14
41
51
49
0222
2
2
0
46442
8
11
0
033
0
5
6
0
411973
15
19
0
6 20 0 5 4 9
8 50 2 7 5 14
2 26 4 3 8
(b) Subvalvukzr Aortic StenosisThe 19 patients with subvalvular aortic stenosis
ranged in age from five to 30 years. The sex ratiowas 14 males to five females (2.8:1). Table IIIshows the relationship of the clinical data to thesystolic pressure gradient.
It may be noted that of the two patients withgradients less than 50 mm. Hg, one was in con-gestive heart failure, and pressure recordings at left-heart catheterization were unsatisfactory in theother. In both patients the systolic murmur wasassociated with a thrill. The left ventricular impulsewas increased and the electrocardiogram showedleft ventricular hypertrophy. As in the valvulargroup, symptoms did not occur until 10 years ofage or older. Exertional chest pain was commonerthan in the valvular group and congestive heartfailure occurred in three of the 19 patients.On physical examination, a systolic thrill was
present in the suprasternal notch of all patientsand the left ventricular impulse was accentuatedin 15. An early systolic ejection sound was not de-tected in any patient with subvalvular stenosis.The pulse pressure was 25 mm. Hg or less in ninepatients, all of whom had gradients over 50 mm.Hg. An early diastolic murmur was heard in fivepatients.The electrocardiogram indicated left ventricular
hypertrophy in 14 patients, seven of whom had the"strain.. pattern. It was interpreted as normal inthe remaining five patients, but in four the R or Svoltage in the mid-chest leads exceeded 25 my.,suggesting left ventricular hypertrophy; in all fivepatients the systolic pressure gradient exceeded50 mm. Hg.The cardiothoracic ratio was greater than 50%
in eight of the 19 patients. Two patients appearedto have poststenotic dilatation of the ascendingaorta.
In the 15 patients who came to operation, afibrous band or diaphragm, which was judged to bethe cause of severe obstruction, was found in theleft ventricular outflow tract.
642 PECKHAM AND OTHERS: CONGENITAL AORTIC SmNosIs Canad. Med. Ass. J.Sept. 19, 1964, vol. 91
Poststenotic dilatation of the aorta was a lessreliable sign since it was not detected in manycases of significant valvular aortic stenosis andoccasionally appeared to be present in patientswith subvalvular stenosis. An early diastolicmurmur was heard with obstruction at either site.As noted by Spencer et al.,23 subvalvular obstruc-tion rarely caused symptoms in infancy and in thepresent series no patient with subvalvular stenosiswas detected under five years of age. In contrast,valvular stenosis frequently presented in the firstyear of life, often with heart failure, and was in-variably fatal unless surgically relieved. In thepresent series, exertional chest pain was muchcommoner with subvalvular obstruction than withvalvular stenosis; this may simply reflect differ-ences in severity of the stenosis in the two groups.The incidence of sudden death in aortic stenosis
as reported by various authors ranges from four to18% 7,27-32 In our group of 300 patients there wereonly four deaths (1%). In all four patients theclinical criteria for severe aortic stenosis werepresent. In 160 patients with aortic stenosis studiedby VIad et al.,33' . sudden death occurred in twopatients both of whom had physical and electro-cardiographic findings suggesting severe aorticstenosis. From the combined experience of Vladand the present study, the incidence of suddendeath in aortic stenosis may be estimated at 1-2%and it would appear that in most instances theseverity of obstruction might be predicted fromclinical assessment.
SUMMARY
This study of 300 patients with a clinical diagnosisof aortic ste.nosis helps to illustrate the natural historyof the condition, when it is left untreated.The early presentation and lethal nature of aortic
stenosis in infancy may be attributed in part to thepresence of associated cardiac lesions.
Clinical assessment of the patient provides a usefulestimate of the severity of obstruction, as judged by thesystolic pressure gradient, and should assist in theselection of patients with moderate and severe aorticstenosis who warrant further investigation. Thepresence of a thrill, together with an increased leftventricular impulse on palpation, a decreased brachialartery pulse pressure or electrocardiographic changesof left ventricular hypertrophy by voltage criteria,indicated significant obstruction. Left ventricular hyper-trophy with the "strain. pa.em on the electrocardio-gram invariably meant severe stenosis.
Differentiation of valvular from subvalvular stenosiswas not always possible on clinical grounds but thepresence of an early systolic ejection sound was strongevidence against subvalvular stenosis.From the present study the incidence of sudden
death in persons with aortic stenosis may be estimatedat 1-2%. Clinical assessment should indicate the severityof obstruction in such cases.
Canad. Med. Ass. J.Sept. 19, 1964, vol.91 GIBsON: DE LANGE SYNDROME 643
RUFERENCES
1. TUFFIER, T.: Etat actuel do la chirurgie intrathoracique.Tr. Internat. Cong. Med. 1913, Lond. 1914, Sect.VII, Surg. pt. 2, 249-326 (Discussion), 326-338.
2. BAILEY, C. P., Rsiunuz, H. P. R. AND LAREELERE, H. B.:J. A. M. A., 150: 1647, 1952
3. SWANK, W K. BRADSHER 3 T., Jn. AND RODRIGUEZ-AEROYA, 3.: ,k. Therac. dard.ov. Burg., 28: 266, 1954.
4. JUL1AM, 0. C. et el: A.M.A. Arch. Burg., 73: 493, 1956.5. BsocK, IL: Br4t. Med. J., 1: 1019, 1957.6. LILLEHEI, C. W. et ai: Di.. Cheat, 30: 123, 1956.7. KEITH, J. D., Rowu, R. D. AND VLAD, P.: Heart disease
in infancy and childhood, The Macmillan Company,New York, 1958.
8. GRANT, H. P.: ClInical electrocardiography; the spatialvector approach, Blakiston Company, New York, 1957.
9. WioLs, E. D., HUIMIECKUR, H. 0. AND GUNTON, H. W.:Csrcukstson, 26: 325, 1962.
10. Moas, C. A. F., PUCKHAM, G. B. AND KEITH, 3. D.:Idiopathic hypertrophy of the intervontricular septumcausing subaortlc stenosis In children, Radsolog.i. Inpress.
11. BRAUNWALD, E. et al.: Circulation, 27: 426, 1963.12. ONGLEY, P. A. et ol.: Pediatrics, 21: 207, 1958.13. SPENCER, F. C. et al.: Amer. Burg., 26: 204, 1960.14. TAUSSIG H. B. Congenital malformations of the heart,
voL j 2nd ed., University Press. Cambridge, Mass.,1960, p. 835.
15. HANCOCK E W AND FLEMING, P. R.: Quart. ,f. Med.,29: 206, 1960.
16. HANCOCK E W. AND ABELMANN, W. H.: (Jtrculatson, 16:572, 1i57.
17. MUSTARD, W. T., TRUSLUR G A. AND YAO, 3.: Canod.Med. Ass. J., 89: 1068, 1963.
18. Stockholm. Karolinska SJukhuset. Barnkliniken: Diag-nosis of Co.enital heart disease; a clinical andtechnical study by the eardiologic team of thepediatric clinic, by S. R. Kjellberg et al, 2nd ed.,Year Book Publishers, InC., Chicago, 1959.
19. PAPPAS, E. G., LAZARIDUS, D. P. AND DOWNING, D. F.:Dia. C1&est, 33: 323, 1958.
29. DOWNING, D. F.: Circulation 14: 188. 1956.21. AWAD, J. A. AND MANNIX, E. j)., JL: J. Thorac. Cardsov.
Burg., 43: 203, 1962.22. HANCOCK, E. W.: G'aij Hoap. Rep., 110: 1. 1961.23. SPENCER, F. C. et aL: Amer. Burg., 26: 204, 1960.24. SIS5MAN, N. J. et aL: Csrcuiat4oa, 19: 458, 1958.25. NADAs, A. S. et al: Ibid., 25: 346, 1962.26. JONEs, R. C. et aL: Ann. Intern. Med., 58: 486, 1963.27. MARQUIS, H. M. AND LOGAN, A.: Br&t. Heart .7., 17: 373,
1955.28. WooD, P. H.: Diseases of the heart and circulation, 2nd
ed., Eyre and Spottiswoode Ltd., London, 1956.29. NADAS, A. S.: Pediatric cardiology, W. B. Saunders
Company, Philadelphia, 1957.30. BRAVURMAN, I. B. AND GIBSON, S.: Amer. Heart .T., 53:
487, 1957.31. MORROw, A. G., SHARP, E. H. AND BRAUNWALD, E.:
Circulation, 18: 1091, 1958.32. REYNOLDS, 3. L. et aL: New Eng. .7. Med., 262: 276, 1960.33. VL.w, P. et aL: Circulation, 24: 1062, 1961.34. VLAD, P.: Personal communication.
The de Lange Syndrome: Report of Three CasesROBERT GIBSON, M.D., Gh.B., D.P.M.,*
Portage la Prairie, Man.
ABSTRACT
Three cases of de Lange's syndrome aredescribed. This condition is characterizedby generally severe mental retardation, re-duced stature, mild microcephaly, hyper-trichosis, various anomalies of hands andfeet, and a peculiar facies. The most out-standing features of the latter are the lowforehead, profuse, generally confluent eye-brows, abundant long eyelashes, eyes thatfrequently slant downwards and outwardsin antimongoloid fashion, pug nose withprominent anteverted nostrils, increaseddistance between nose and vermilion borderof upper lip, slight reduction in size of chin,and often abnormally low-placed ears. Theetiology of de Lange's syndrome is atpresent unknown.
SOMMAIRE
L'auteur rapporte trois cas de maladie dede Lange. Ce syndrome est caract6ris6 parune d6ficience mentale grave, une tailler6duite, une l6g.re microc6phalie, del'hypertrichose, diverses anomalies desmains et des pieds et un faci.s particulier.Parmi les traits les plus remarquables dufaci.s figurent un front bas, des sourcilsabondants et g.n6ralement confluents, descils longs et fournis, des yeux qui sontsouvent inclin6s vers le bas et l'ext6rieur, .il'inverse de ce qui se passe chez les mongo-bides, un nez camus dont les narinespro6minentes sont en ant.version, une plusgrande distance entre le nez et le bord ex-terne de la l.vre supfrieure, une I6g.rediminution de la dimension du menton, etdes oreilles iniplant6es anormalement bas.On ignore encore actuellement l'6tiologiedu syndrome de de Lange.
THE de Langel syndrome was originally de.gave her name to this condition. Until 1963 onlyabout 15 cases had been described, all in the Euro-pean literature. In the course of the past year, how-ever, the American literature has included adescription of five new cases by Jervis and Stim-son,2 while Ptacek et al.3 have discussed in detailsix cases and mentioned three further cases in anappendix to their paper.
ClinIcal Director, The Manitoba School, Portage la Prairie,Man.
Patients with the de Lange syndrome arecharacterized by mental defect, reduced stature,mild microcephaly, distinctive facies, and a numberof additional peculiarities including hirsutism andwebbing of toes.
Mental defect is invariably present and is gener-ally severe. Of the five cases reported by Jervisand Stimson, one had an intelligence quotient of52, while the others were below 25. All patientsdescribed by Ptacek et al. were severely retarded,
Recommended
![VALVED STENT FOR OFF-PUMP MITRAL V AL VE REPLACEMENTBIB_42715.P001/... · 2016-11-16 · vitro[12]. In 2000, Sochman J. et al designed a catheter-based aortic valve consisting of](https://img.pdfslide.fr/doc/110x75/5f98352a23f55226e71a51b3/valved-stent-for-off-pump-mitral-v-al-ve-replacement-bib42715p001-2016-11-16.jpg)