TRAITEMENT MEDICAMENTEUX DES TROUBLES COGNITIFS DANS LES
«DEMENCES»
Olivier SAINT JEAN HEGP
Université Paris Descartes Conflit d’intérêt : aucun
La prise en charge des malades est multidimensionnelle
1. Annoncer le diagnostic 2. Mettre en place des aides financières et matérielles 3. Etablir le plan de soins et coordonner les professionnels 4. Accompagner et éduquer les aidants familiaux 5. Sauvegarder les droits et anticiper les questions éthiques 6. Organiser le domicile et l’environnement 7. Traiter des troubles du comportement 8. Gérer l’incontinence 9. Pratiquer une rééducation motrice 10. Veiller à l’équilibre nutritionnel 11. Evaluer et optimiser les autres pathologies 12. Traiter les troubles cognitifs
– Action symptomatique • Par de la réadaptation neuro-cognitive • Par des médicaments à visée symptomatiques
– Action étiologique • Equilibre cardio-vasculaire (?) • Modulateur amyloïde, inhibiteurs kinases
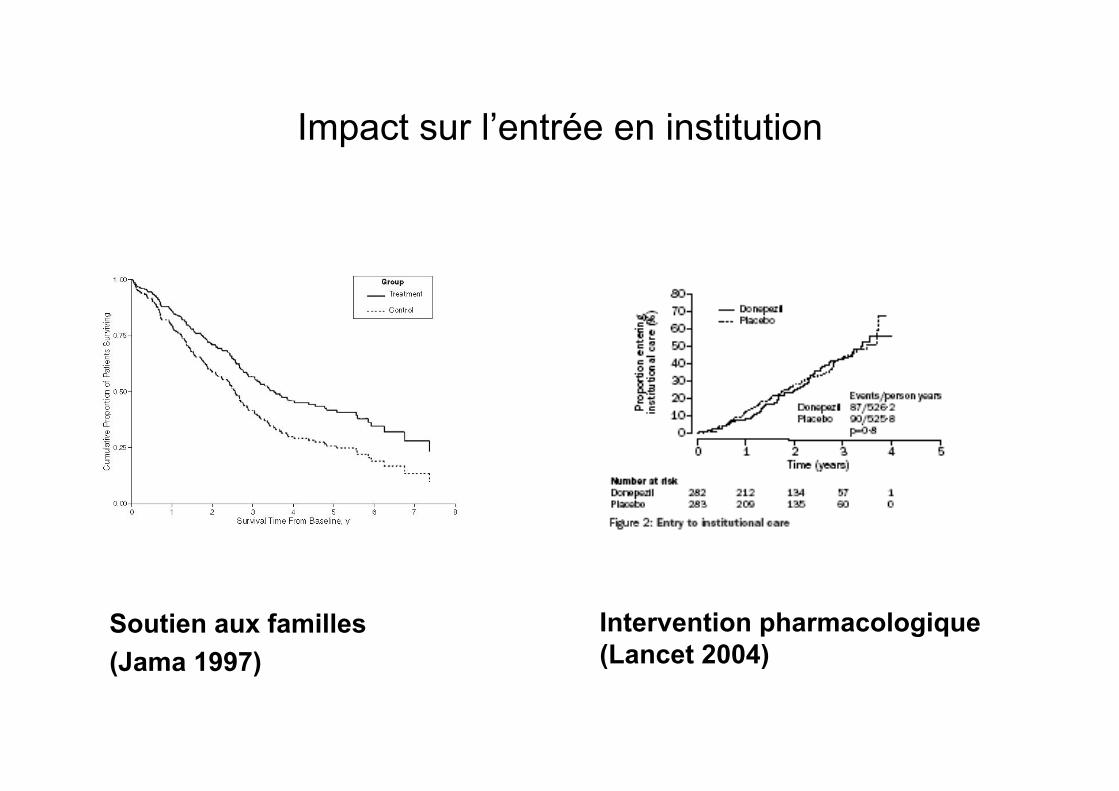
Impact sur l’entrée en institution
Soutien aux familles (Jama 1997)
Intervention pharmacologique (Lancet 2004)
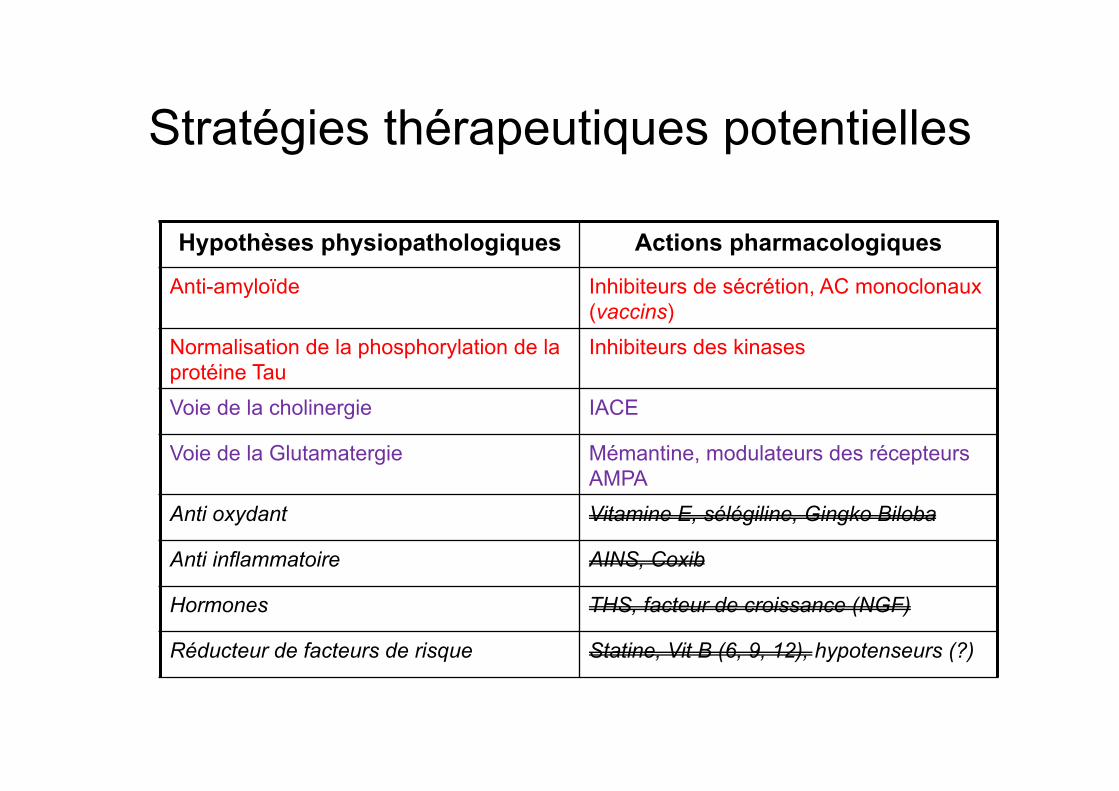
Stratégies thérapeutiques potentielles
Hypothèses physiopathologiques Actions pharmacologiques
Anti-amyloïde Inhibiteurs de sécrétion, AC monoclonaux (vaccins)
Normalisation de la phosphorylation de la protéine Tau
Inhibiteurs des kinases
Voie de la cholinergie IACE
Voie de la Glutamatergie Mémantine, modulateurs des récepteurs AMPA
Anti oxydant Vitamine E, sélégiline, Gingko Biloba
Anti inflammatoire AINS, Coxib
Hormones THS, facteur de croissance (NGF)
Réducteur de facteurs de risque Statine, Vit B (6, 9, 12), hypotenseurs (?)
Rappels méthodologiques sur la preuve d’action
pharmacologique et l’EBM
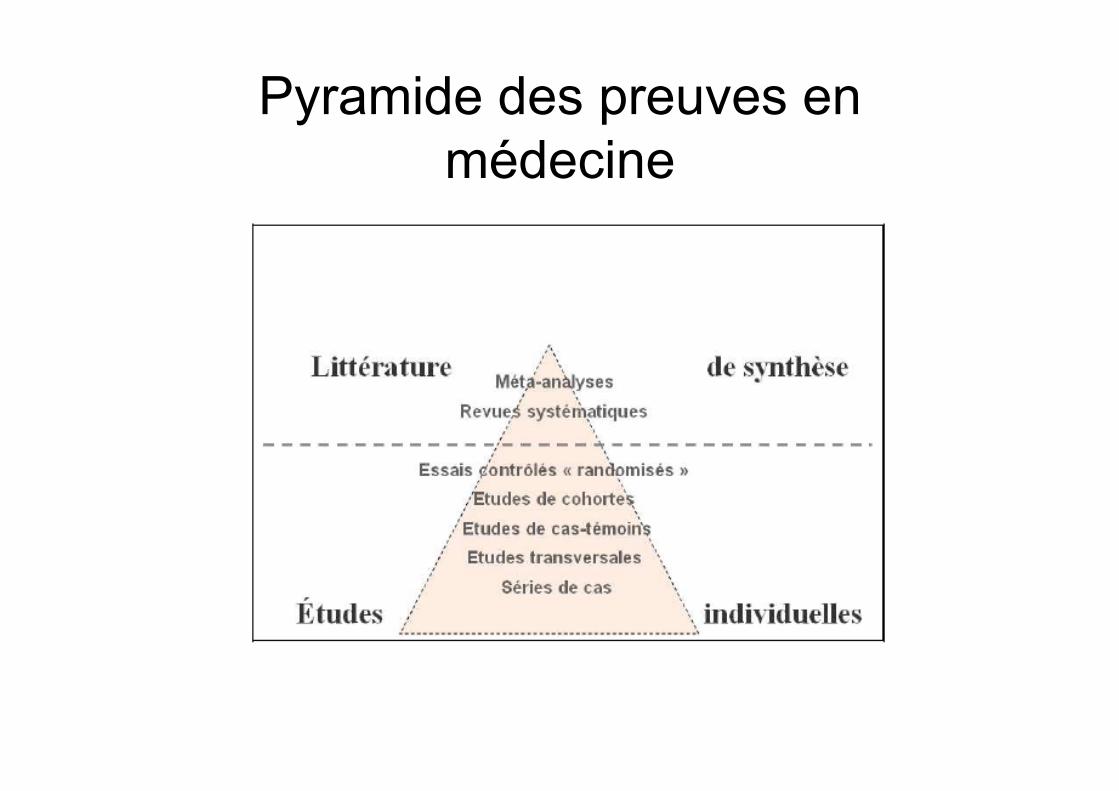
Pyramide des preuves en médecine
Des rappels méthodologiques sur les essais
1. Différenciation de – Puissance statistique – Variation d’une échelle de mesure et pertinence clinique
2. S’interroger sur les qualités métrologiques des échelles de mesure du résultat
3. Vérifier la satisfaction des critères de qualité du RCT et de sa publication
4. S’interroger sur la validité de la population incluse dans l’essai 5. Accéder au répertoire de tous les essais, y compris les essais
négatifs
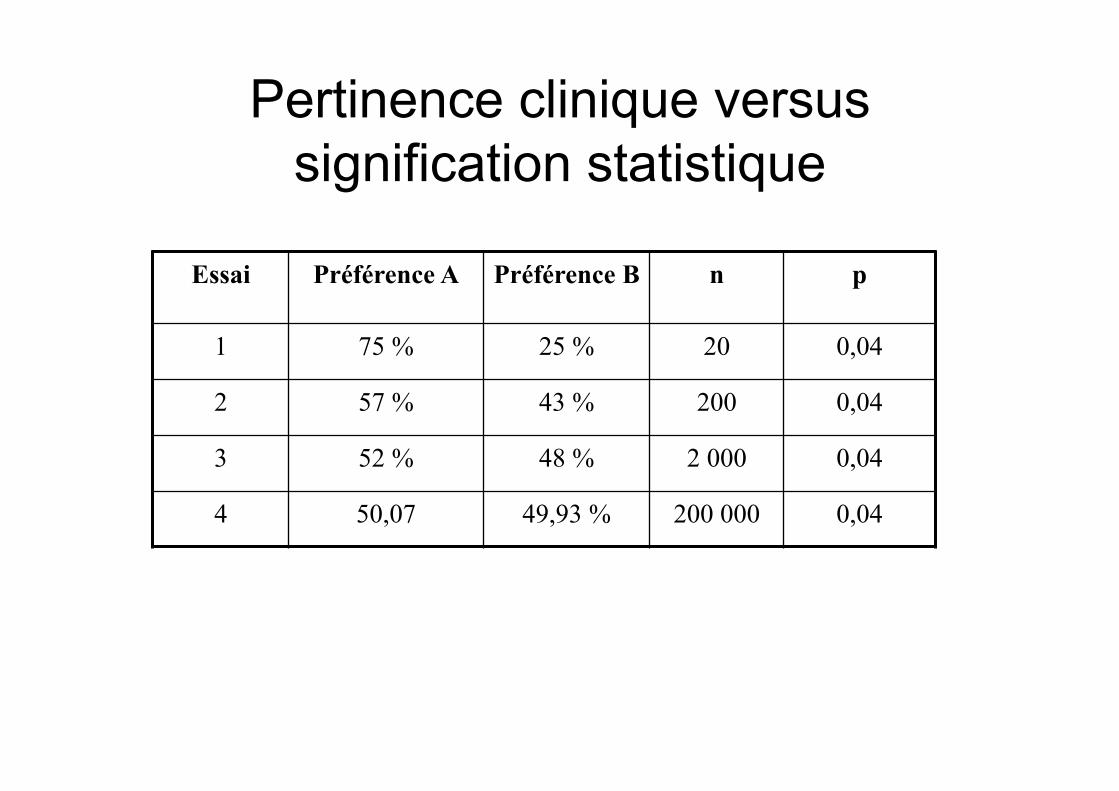
Pertinence clinique versus signification statistique
Essai Préférence A Préférence B n p
1 75 % 25 % 20 0,04
2 57 % 43 % 200 0,04
3 52 % 48 % 2 000 0,04
4 50,07 49,93 % 200 000 0,04
Echelles utilisées dans les essais cliniques
• Trois critères majeurs de jugement pour les formes non sévères – La cognition par l’ADAS-Cog (0-70), parfois le MMS – La CIBIC (variable discrète à 7 classes) – L’autonomie fonctionnelle par l’ADCS-ADL (0-78) ou la DAD (0-100)
• La mesure de la dimension comportementale – Le NPI-10 (0-120) ou NPI-12 (0-144)
• Une échelle cognitive pour les formes sévères – La SIB (0-100)
• Des éléments disparates (Zarit, institutionnalisation, coût/bénéfice, qualité de vie, …)
ADAS-cog (score 0-70) • Mémoire et apprentissage (35 pts)
– Rappel des mots (10 pts) – Orientation (8 pts) – Reconnaissance des mots (12 pts) – Rappel de consignes (5 pts)
• Langage (25 pts) – Dénomination (objet, doigt) (5 pts) – Exécution d’ordre (5 pts) – Intelligibilité de langage parlé (5 pts) – Manque du mot (5 pts) – Compréhension (5 pts)
• Praxies – Praxie constructive (5 pts) – Praxie idéatoire (5 pts)
Rosen WG et al Am J Psychiatry 1984;141:1356-64
Evolution du score ADAS cog selon le stade de démence
• Effet plafond ou plancher de certains sous-items à différents stades de la maladie, notamment pour le – Déclin de l’orientation – Déclin de la dénomination et des praxies constructives ou
idéatoires
• Evolution du score plus lente aux extrêmes • Pertinence des critères d’inclusion classiques (MMS
entre 10 et 24) ?
Zec RF et al, Alzheimer Dis Assoc Disord 1992;6:164-81
Définition du seuil de pertinence clinique
• Une variation de 10% – De la pression diastolique a du sens clinique pour un
cardiologue – Des index spirométriques est à la limite pour le pneumologue – Du taux des plaquettes n’a pas de pertinence pour
l’hématologue
• Comment définir la pertinence clinique ? – Par consensus d’expert (identité des experts) – Par une approche statistique de la différence perceptible en
clinique (multiple x SD)
Quel seuil de pertinence clinique ? • Selon un consensus d’experts de la FDA *
– - 4 points pour l’ADAS-Cog – Une CIBIC stable ou sans déclin
• Définition de la différence minimale importante en clinique – Selon une interrogation de 161 gériatres et neurologues
• Pour le MMS : > 3,72 (3,5-3,95) **
– Selon une définition statistique : • 127 participants*** validant 0,4xSD, soit
– Pour le MMS : 1,4 – Pour le NPI : 8,0 – Pour la Bristol ADL : 3,5
• Aucune réflexion publiée pour les autres variables : SIB ou échelles d’autonomie (avant 2011)
* PCNS Drugs Advisory Committee Meeting, July 7, 1989. Rockville, FDA 1989 : 227 ** Dement geriatr Cogn Disord 1999;10:534-40
*** Int J Ger Psychiatry 2011; 26: 812-817 & NEJM 2012;366:893-903
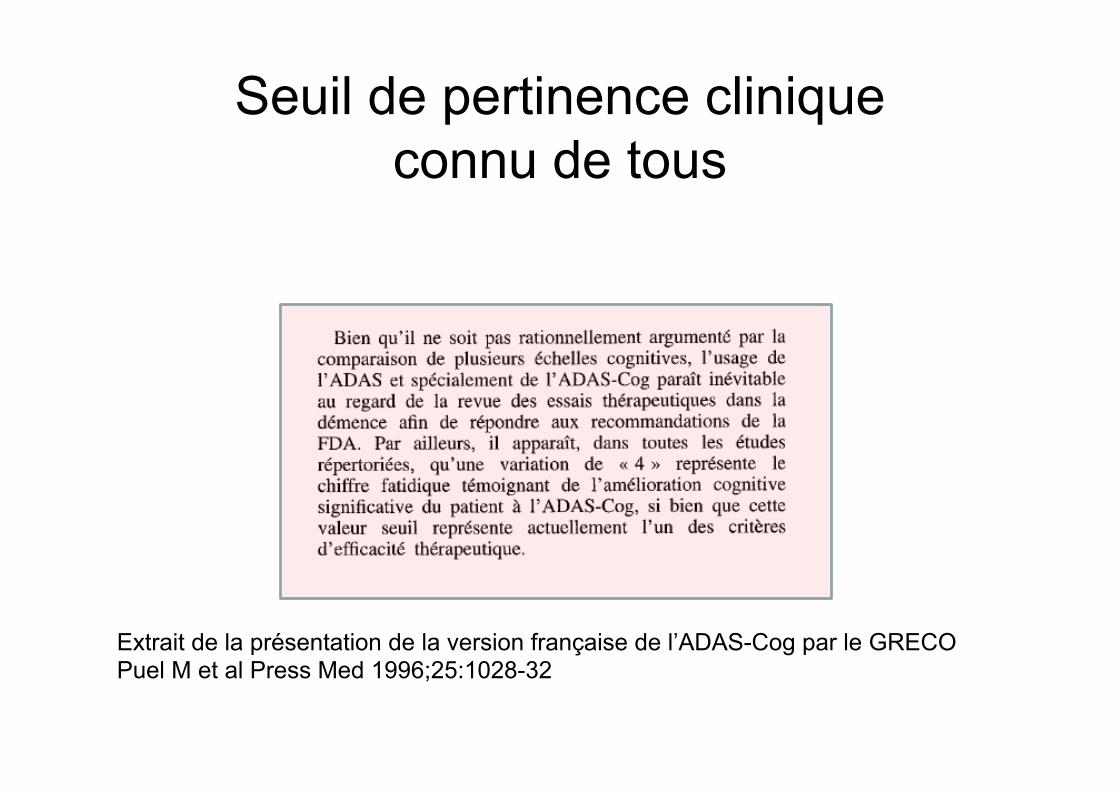
Seuil de pertinence clinique connu de tous
Extrait de la présentation de la version française de l’ADAS-Cog par le GRECO Puel M et al Press Med 1996;25:1028-32
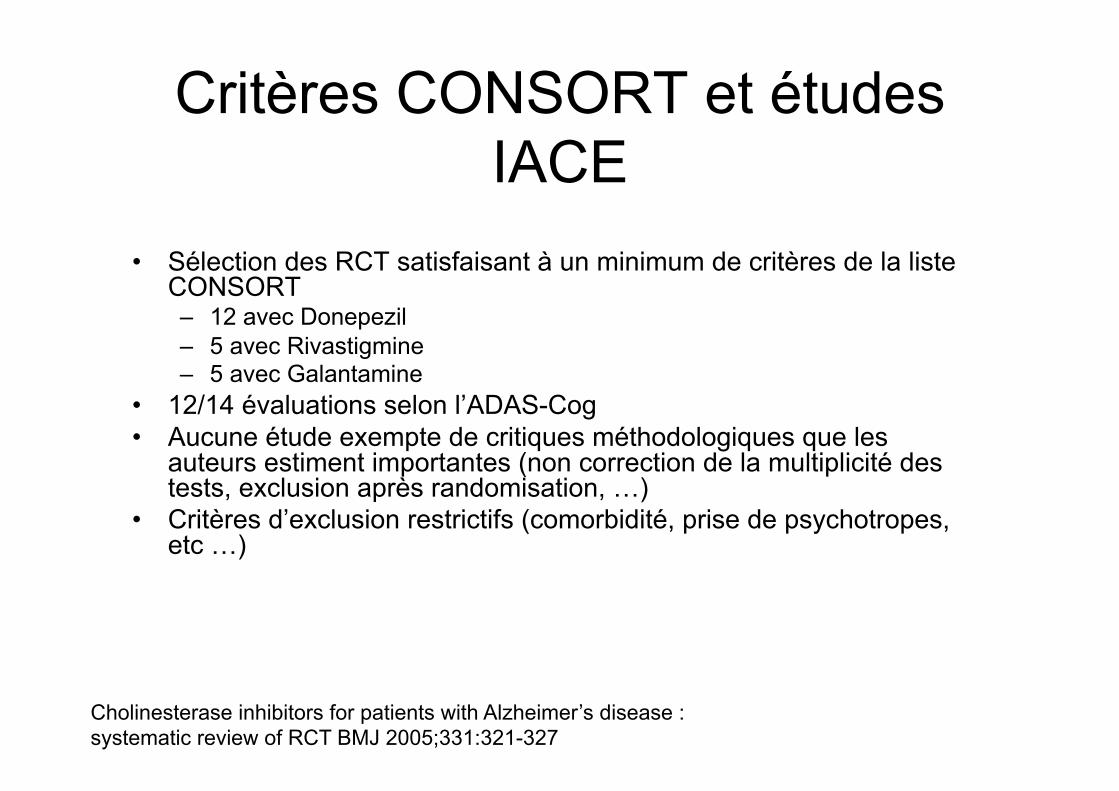
Critères CONSORT et études IACE
• Sélection des RCT satisfaisant à un minimum de critères de la liste CONSORT – 12 avec Donepezil – 5 avec Rivastigmine – 5 avec Galantamine
• 12/14 évaluations selon l’ADAS-Cog • Aucune étude exempte de critiques méthodologiques que les
auteurs estiment importantes (non correction de la multiplicité des tests, exclusion après randomisation, …)
• Critères d’exclusion restrictifs (comorbidité, prise de psychotropes, etc …)
Cholinesterase inhibitors for patients with Alzheimer’s disease : systematic review of RCT BMJ 2005;331:321-327
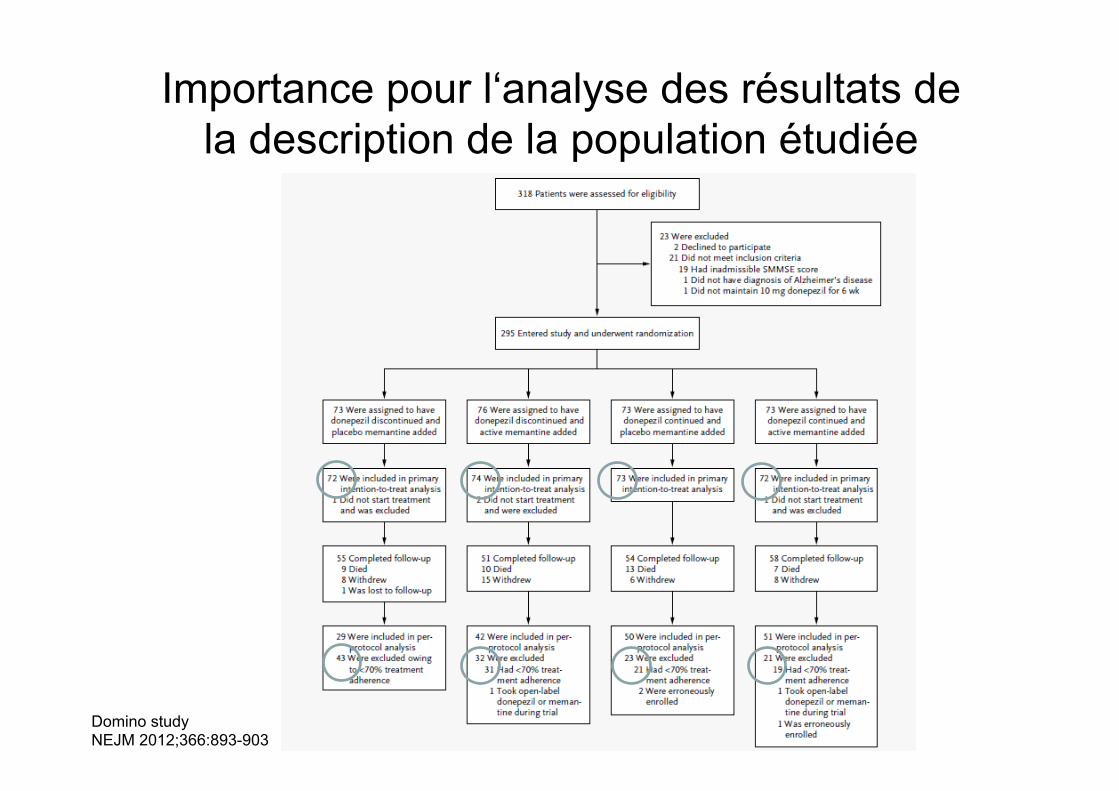
Importance pour l‘analyse des résultats de la description de la population étudiée
Domino study NEJM 2012;366:893-903
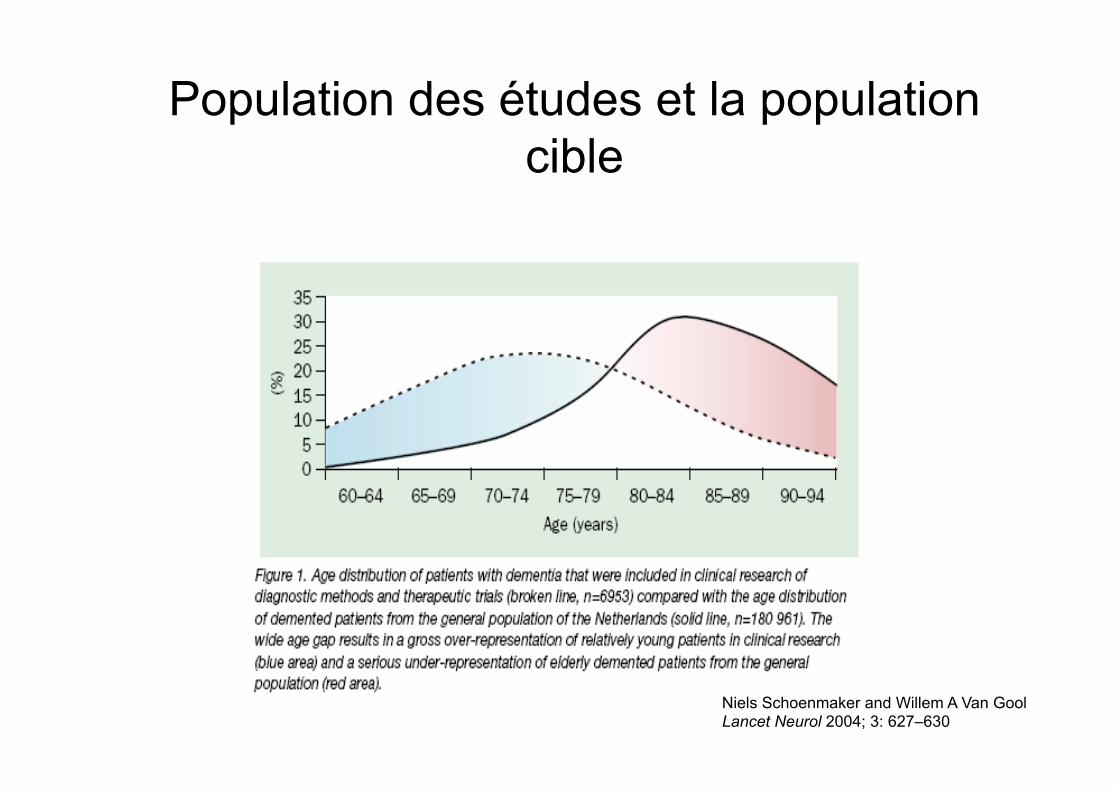
Population des études et la population cible
Niels Schoenmaker and Willem A Van Gool Lancet Neurol 2004; 3: 627–630
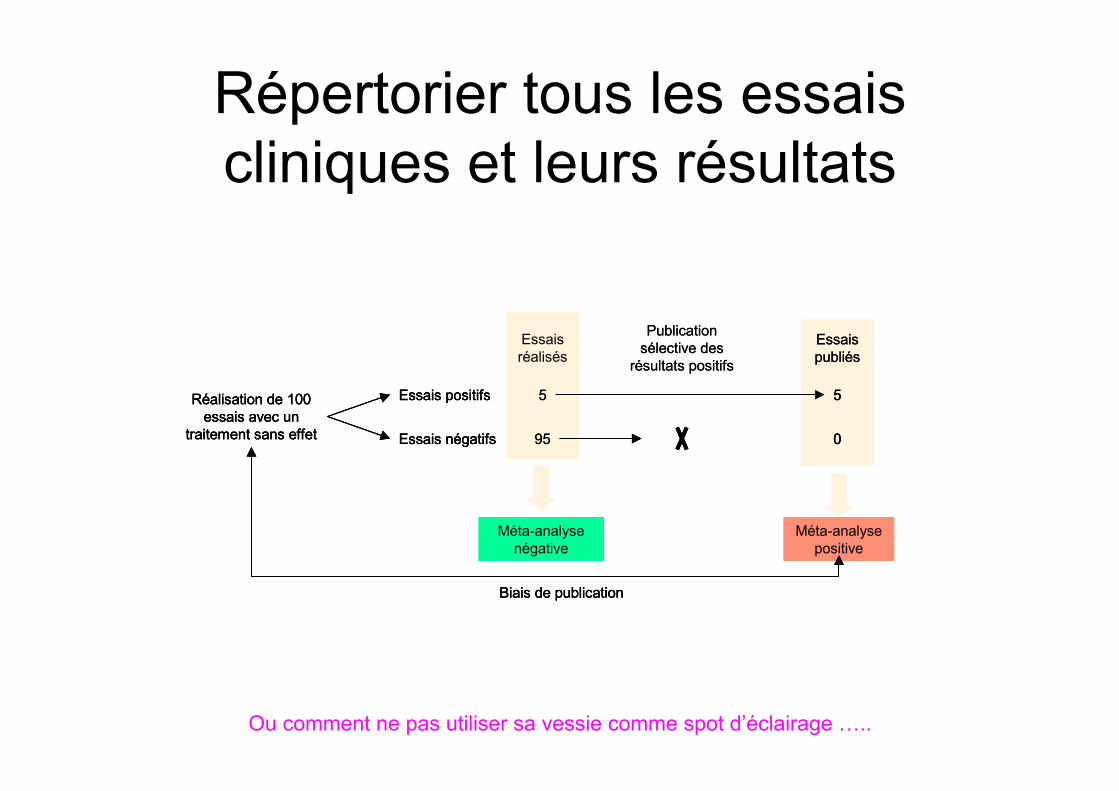
Répertorier tous les essais cliniques et leurs résultats
Essais réalisés
Méta-analyse négative
Méta-analyse positive
Essais publiés
5
0
Publication sélective des
résultats positifs
Essais positifs
Essais négatifs
5
95
Réalisation de 100 essais avec un
traitement sans effet
Biais de publication
Essais réalisés
Méta-analyse négative
Essais réalisés
Méta-analyse négative
Méta-analyse positive
Méta-analyse positive
Essais publiés
5
0
Essais publiés
5
0
5
0
Publication sélective des
résultats positifs
Essais positifs
Essais négatifs
5
95
Réalisation de 100 essais avec un
traitement sans effet
Essais positifs
Essais négatifs
5
95
Réalisation de 100 essais avec un
traitement sans effet
Biais de publicationBiais de publication
Ou comment ne pas utiliser sa vessie comme spot d’éclairage …..
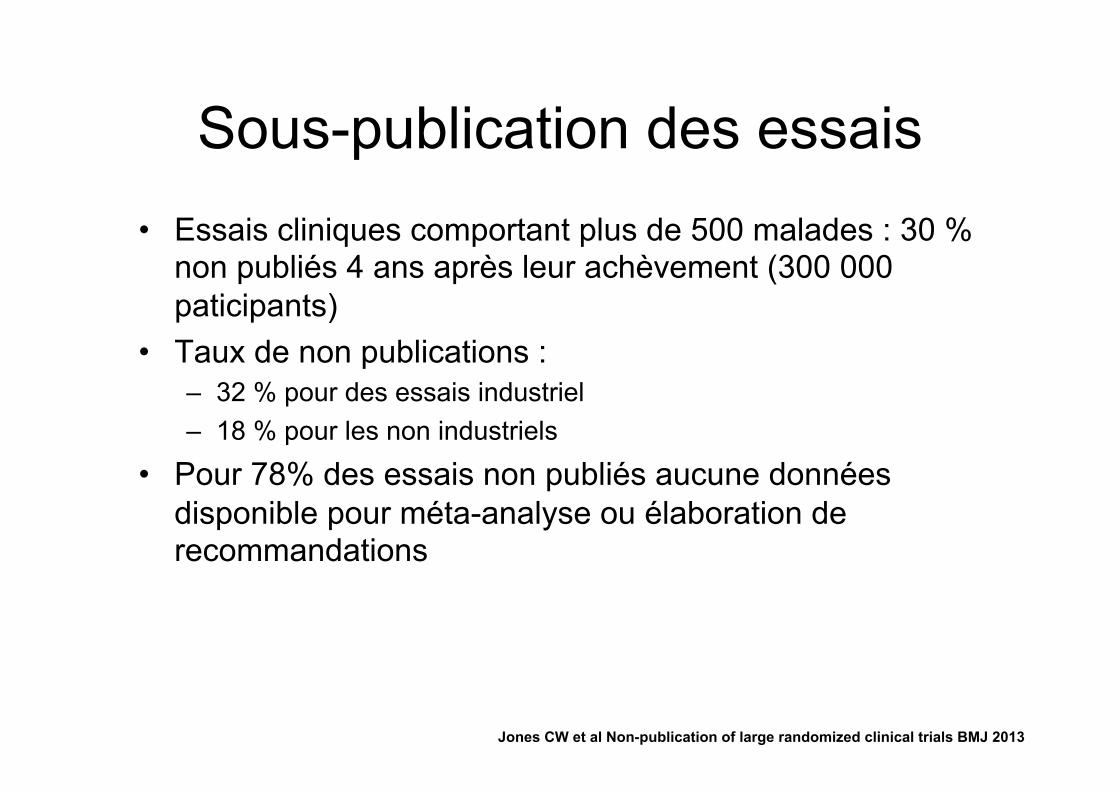
Sous-publication des essais • Essais cliniques comportant plus de 500 malades : 30 %
non publiés 4 ans après leur achèvement (300 000 paticipants)
• Taux de non publications : – 32 % pour des essais industriel – 18 % pour les non industriels
• Pour 78% des essais non publiés aucune données disponible pour méta-analyse ou élaboration de recommandations
Jones CW et al Non-publication of large randomized clinical trials BMJ 2013
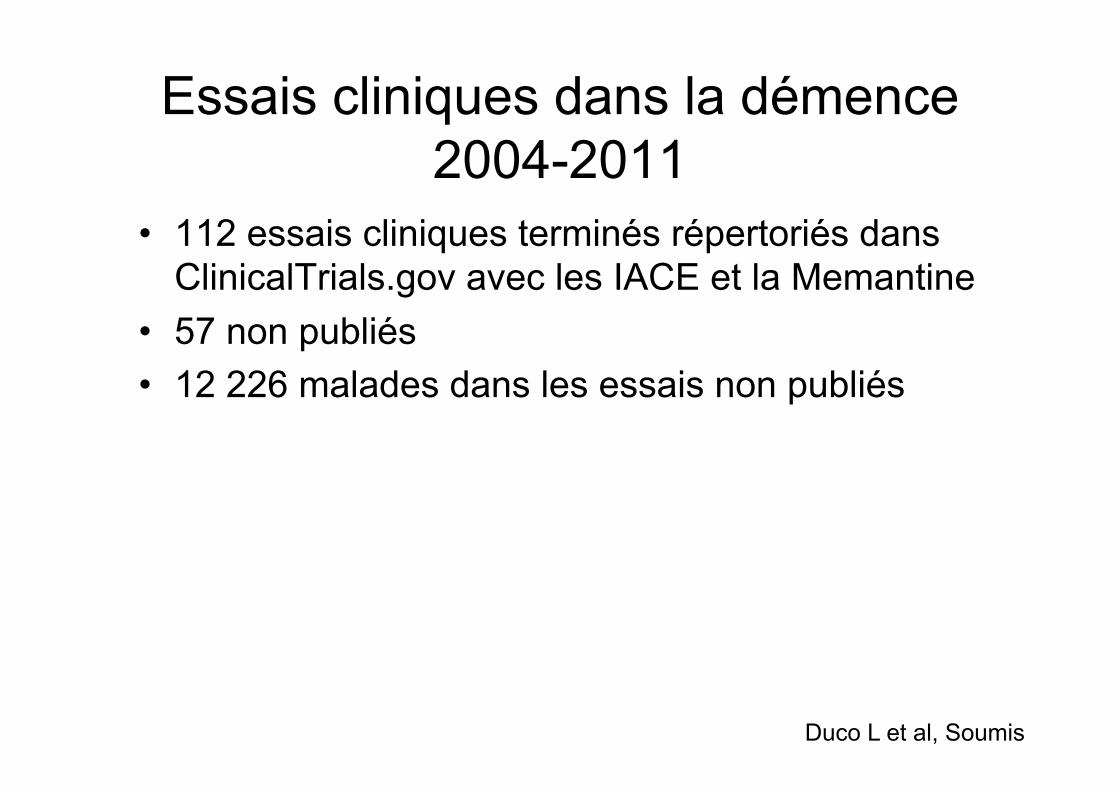
Essais cliniques dans la démence 2004-2011
• 112 essais cliniques terminés répertoriés dans ClinicalTrials.gov avec les IACE et la Memantine
• 57 non publiés • 12 226 malades dans les essais non publiés
Duco L et al, Soumis
Impact de la non publication sur l’analyse de l’effet : exemple des antidépresseurs ISRS
• 74 essais déclarés à la FDA – 23 non publiés (3449 patients) – 40 essais publiés avec accord entre opinion de la FDA et
conclusion de l’article – 11 essais publiés avec désaccord entre opinion de la FDA et
conclusion de l’articles
• Les essais publiés sont positifs à 94% pour les auteurs contre 51% pour la FDA
• Effet thérapeutique mesuré par l’effect-size (ampleur d’effet)
NEJM 2008;358:252-60
29/10/2014 12:05Template
Page 4 sur 5http://www.spc.univ-lyon1.fr/polycop/indices%20continu.htm
traitement, une valeur du critère de jugement supérieure. Si, par exemple, le critère de jugement est le périmètre demarche chez des patients artéritiques, le patient moyen aura une amélioration de ces performances qui l’amènera à unniveau où seulement 16% des sujets ont spontanément un périmètre de marche supérieur.
Figure 4 – Interprétation d’un effet standardisé de 1.
Cet indice ne donne cependant pas une vision directe de la pertinence clinique de l’effet. En effet, si le score initial est peudiscriminant (faible variabilité), un effet traitement, ne modifiant que peu cliniquement l’état des patients, peut se traduirepar un effet standardisé important.
Exemple
Par exemple, avec les données de l’essai MAST concernant le score de handicap, l’écart type des observations est de 5,4dans le groupe streptokinase (n=81) et de 6,8 dans le groupe placebo (n=94). L’écart type global est de(80×5,4+93×6,8)/(80+93)=6,15. L’effect size correspondant à la différence de 1,8 points entre les deux groupes est :
1,8 / 6,15 = 0,29. Cet effect size correspond à une avancée du patient moyen au niveau du 61ème percentile. Cela veutdire que sous traitement 50% des patients ont un niveau de performance supérieur à celui que seulement 39% despatients avaient spontanément.
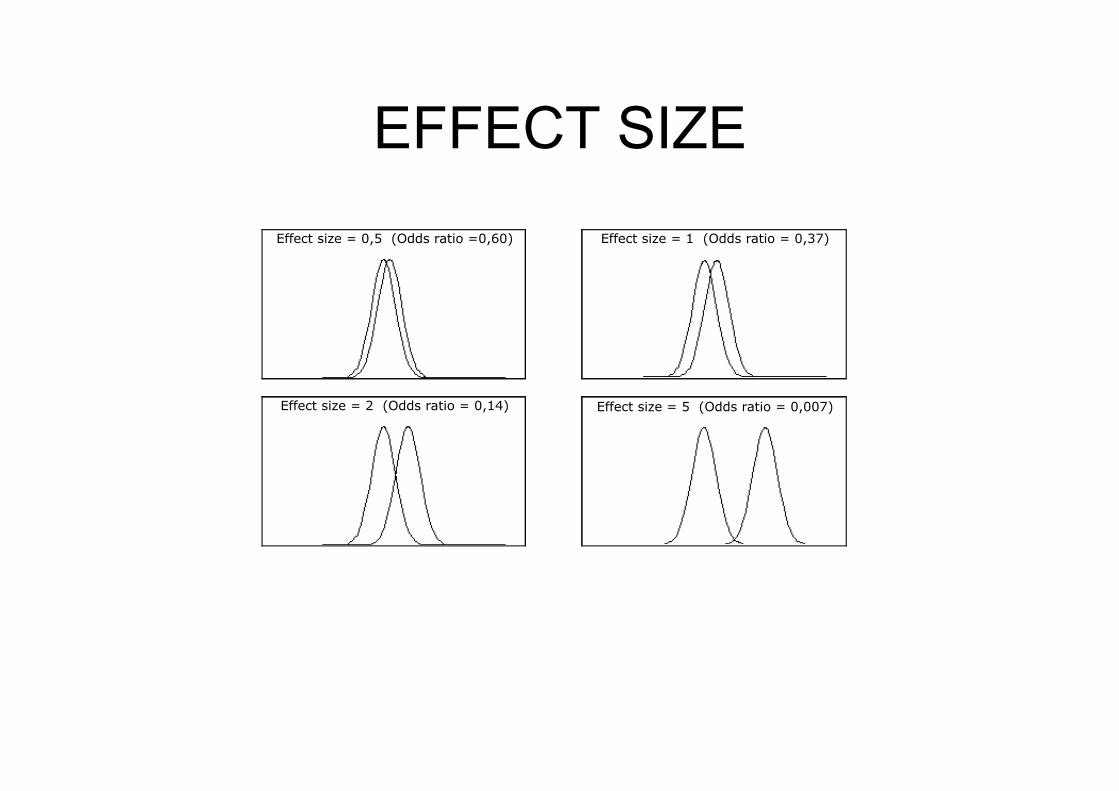
1.3 Appréciation de la taille de l’effet
La représentation graphique du décalage des distributions d’une variable continue entre le groupe contrôle et traitévisualise la taille de l’effet traitement. La figure 5 représente ce décalage pour différentes tailles d’effet exprimées enterme d’effect size et d’odds ratio. Les effets traitement de tailles courantes (effects size de l’ordre de 0,5 ou odds-ratioproche de 0,60) correspondent à des décalages de faible ampleur. Pour que sous traitement, la moitié des patients soit« mieux » que la totalité des patients sans traitement, l’effet traitement doit correspondre à un effect size de 2 ou à unodds ratio de 0,14. Des effets traitements aussi important sont rarement rencontrés.
Effect size = 0,5 (Odds ratio =0,60) Effect size = 1 (Odds ratio = 0,37)
Effect size = 2 (Odds ratio = 0,14) Effect size = 5 (Odds ratio = 0,007)
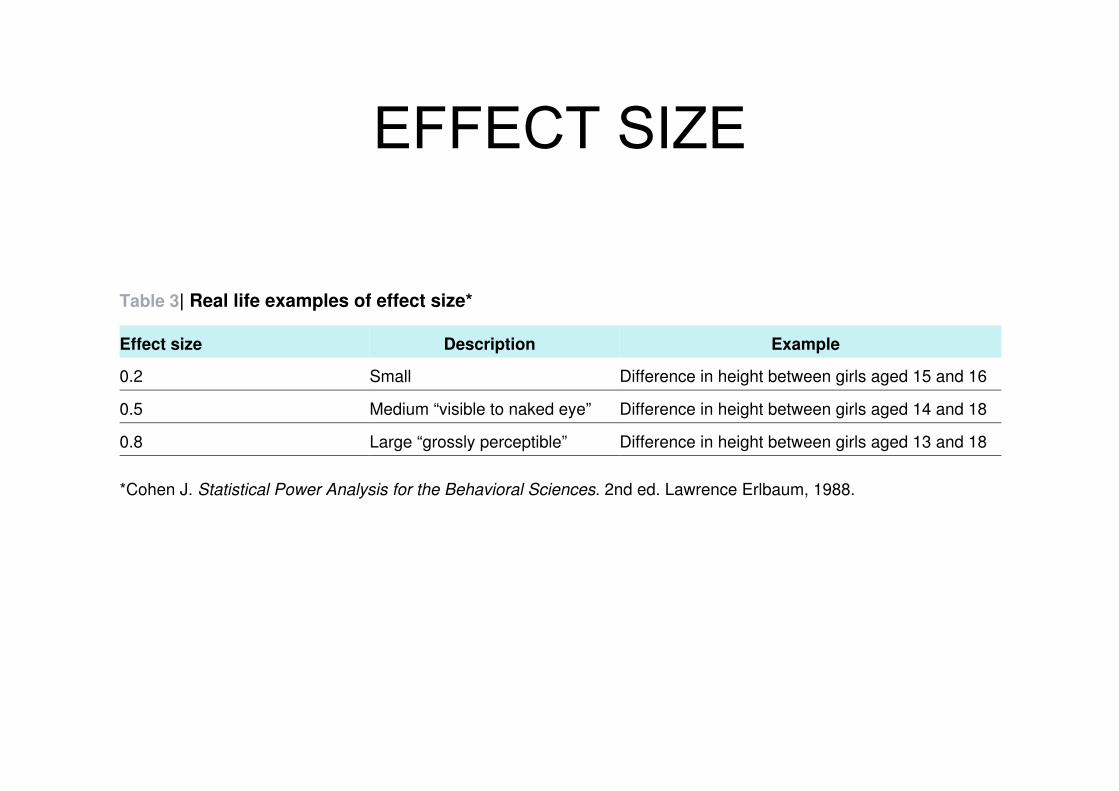
EFFECT SIZE
EFFECT SIZE
Table 3| Real life examples of effect size*
ExampleDescriptionEffect size
Difference in height between girls aged 15 and 16Small0.2
Difference in height between girls aged 14 and 18Medium “visible to naked eye”0.5
Difference in height between girls aged 13 and 18Large “grossly perceptible”0.8
*Cohen J. Statistical Power Analysis for the Behavioral Sciences. 2nd ed. Lawrence Erlbaum, 1988.
No commercial reuse: See rights and reprints http://www.bmj.com/permissions Subscribe: http://www.bmj.com/subscribe
BMJ 2014;348:g1888 doi: 10.1136/bmj.g1888 (Published 19 March 2014) Page 10 of 19
RESEARCH
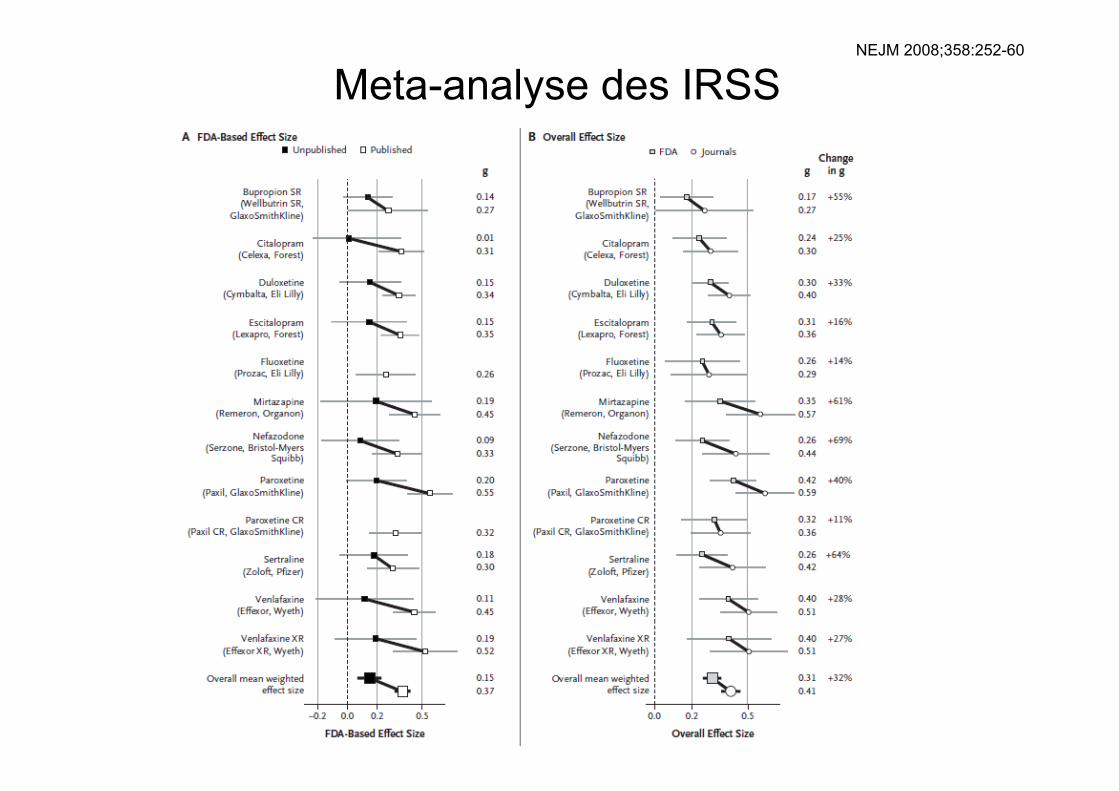
Meta-analyse des IRSS NEJM 2008;358:252-60
Les traitements avec AMM
IACE Mémantine
Coup de tonnerre 1986
Parallèlement à un travail de fond
• Sur les critères de sélection des malades • Sur les variables de résultats et leur mesure
– Alzheimer’s Disease Assessment Scale ADAS – Clinician’s Interview-Based Impression of Change
CIBIC – Severe Impairment Battery SIB
• Sur la méthodologie des essais : RCT de 6 mois maximum
Les inhibiteurs de l’acétylcholinestérase dans la
maladie d’Alzheimer • Une hypothèse physiopathologique crédible • La première classe thérapeutique évaluée par des RCT et
ayant obtenu une AMM uniquement dans les formes MMS 10-24
1. Tacrine
2. Donépezil
3. Rivastigmine
4. Galantamine
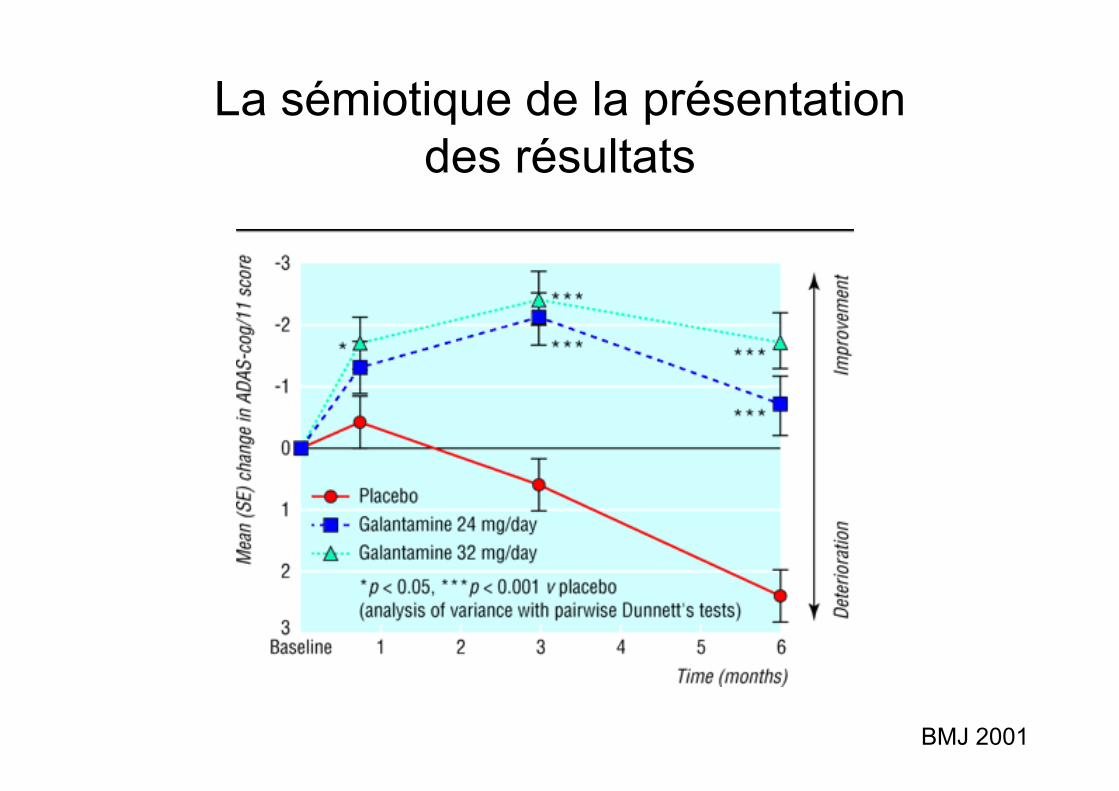
La sémiotique de la présentation des résultats
BMJ 2001
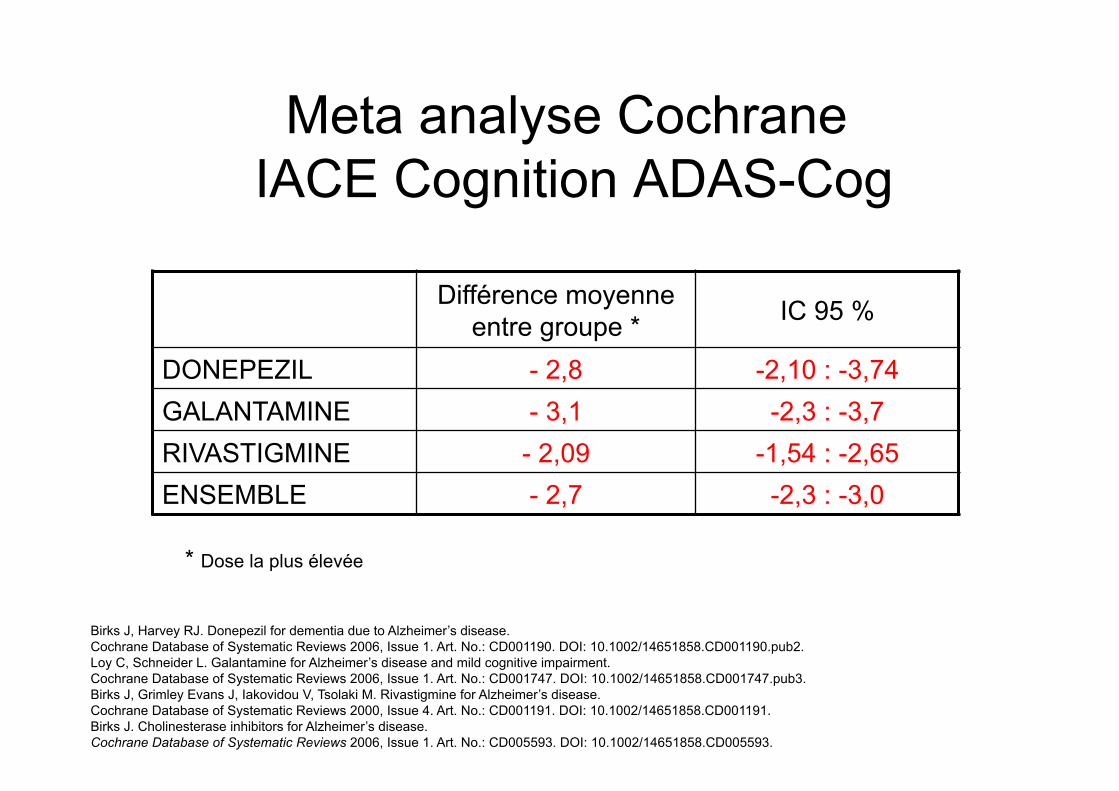
Meta analyse Cochrane IACE Cognition ADAS-Cog
Différence moyenne entre groupe * IC 95 %
DONEPEZIL - 2,8 -2,10 : -3,74 GALANTAMINE - 3,1 -2,3 : -3,7 RIVASTIGMINE - 2,09 -1,54 : -2,65 ENSEMBLE - 2,7 -2,3 : -3,0
* Dose la plus élevée
Birks J, Harvey RJ. Donepezil for dementia due to Alzheimer’s disease. Cochrane Database of Systematic Reviews 2006, Issue 1. Art. No.: CD001190. DOI: 10.1002/14651858.CD001190.pub2. Loy C, Schneider L. Galantamine for Alzheimer’s disease and mild cognitive impairment. Cochrane Database of Systematic Reviews 2006, Issue 1. Art. No.: CD001747. DOI: 10.1002/14651858.CD001747.pub3. Birks J, Grimley Evans J, Iakovidou V, Tsolaki M. Rivastigmine for Alzheimer’s disease. Cochrane Database of Systematic Reviews 2000, Issue 4. Art. No.: CD001191. DOI: 10.1002/14651858.CD001191. Birks J. Cholinesterase inhibitors for Alzheimer’s disease. Cochrane Database of Systematic Reviews 2006, Issue 1. Art. No.: CD005593. DOI: 10.1002/14651858.CD005593.
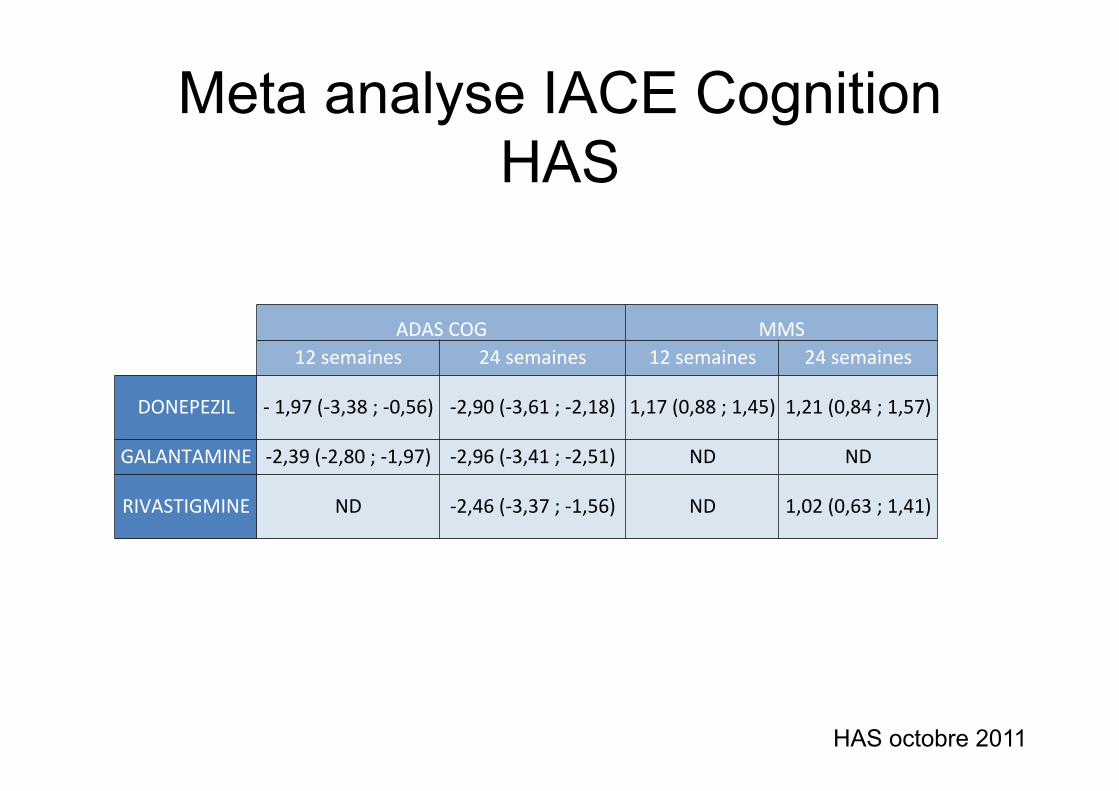
ADASCOG MMS12semaines 24semaines 12semaines 24semaines
DONEPEZIL -1,97(-3,38;-0,56) -2,90(-3,61;-2,18) 1,17(0,88;1,45) 1,21(0,84;1,57)
GALANTAMINE -2,39(-2,80;-1,97) -2,96(-3,41;-2,51) ND ND
RIVASTIGMINE ND -2,46(-3,37;-1,56) ND 1,02(0,63;1,41)
Meta analyse IACE Cognition HAS
HAS octobre 2011
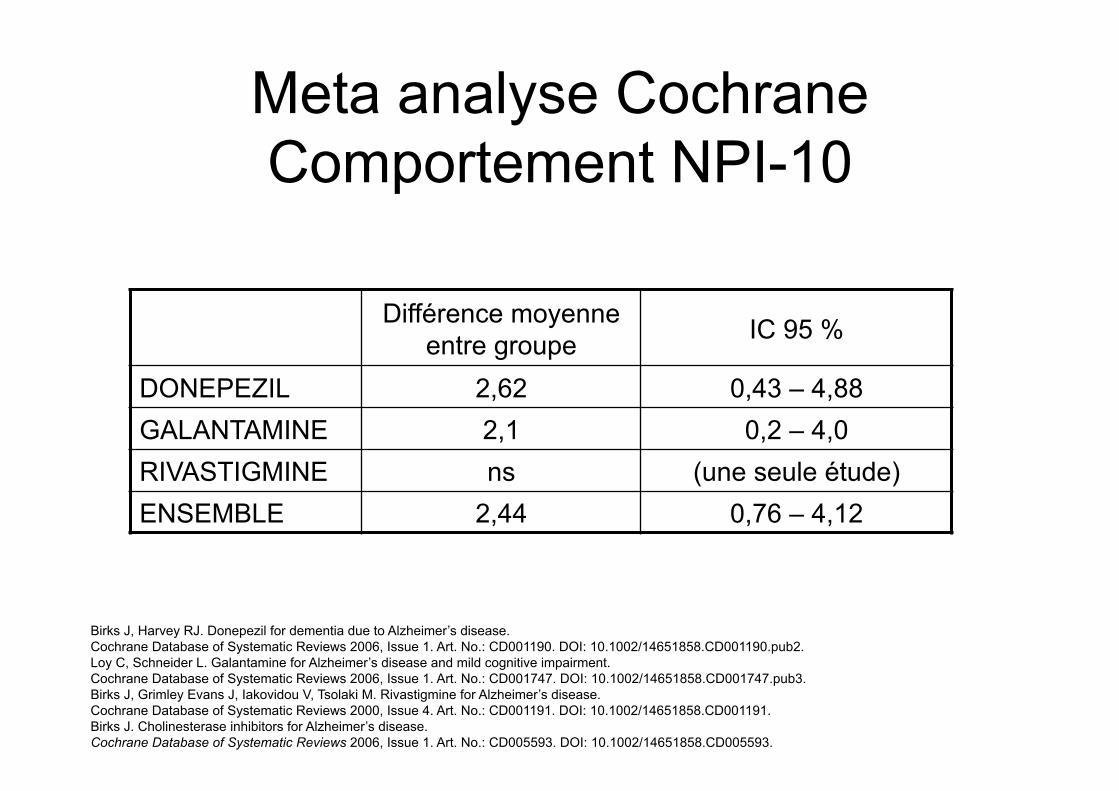
Meta analyse Cochrane Comportement NPI-10
Différence moyenne entre groupe IC 95 %
DONEPEZIL 2,62 0,43 – 4,88 GALANTAMINE 2,1 0,2 – 4,0 RIVASTIGMINE ns (une seule étude) ENSEMBLE 2,44 0,76 – 4,12
Birks J, Harvey RJ. Donepezil for dementia due to Alzheimer’s disease. Cochrane Database of Systematic Reviews 2006, Issue 1. Art. No.: CD001190. DOI: 10.1002/14651858.CD001190.pub2. Loy C, Schneider L. Galantamine for Alzheimer’s disease and mild cognitive impairment. Cochrane Database of Systematic Reviews 2006, Issue 1. Art. No.: CD001747. DOI: 10.1002/14651858.CD001747.pub3. Birks J, Grimley Evans J, Iakovidou V, Tsolaki M. Rivastigmine for Alzheimer’s disease. Cochrane Database of Systematic Reviews 2000, Issue 4. Art. No.: CD001191. DOI: 10.1002/14651858.CD001191. Birks J. Cholinesterase inhibitors for Alzheimer’s disease. Cochrane Database of Systematic Reviews 2006, Issue 1. Art. No.: CD005593. DOI: 10.1002/14651858.CD005593.
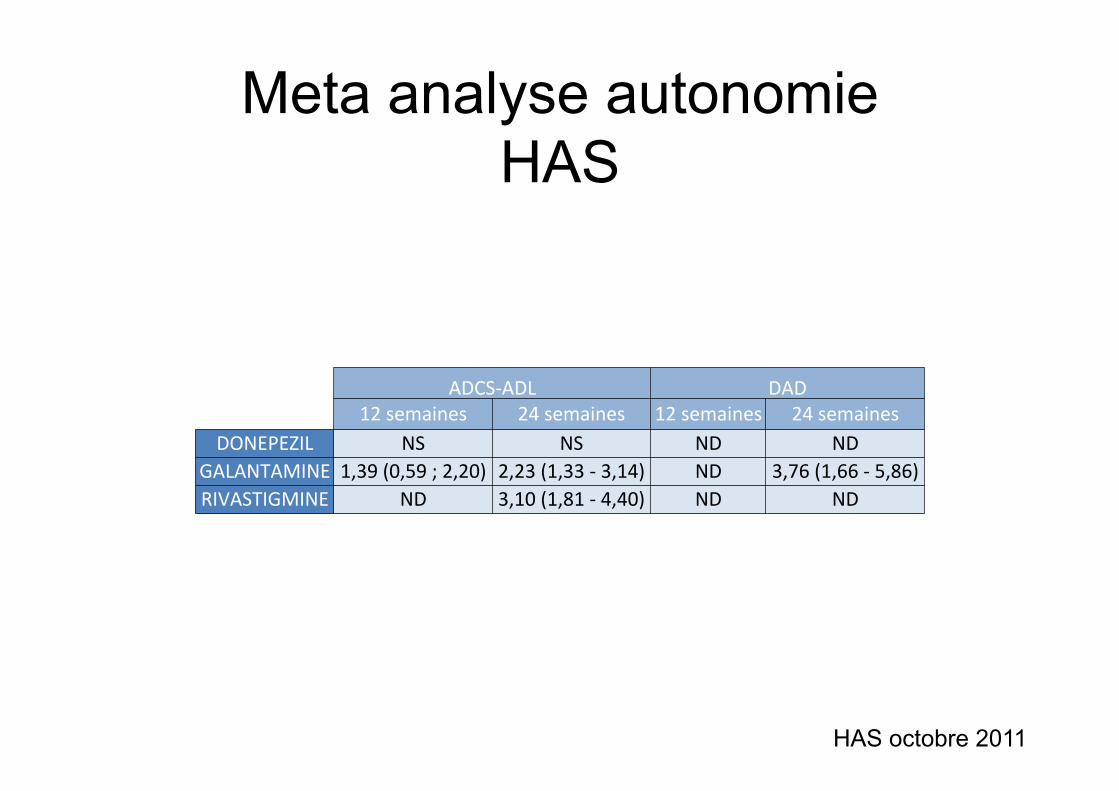
Meta analyse autonomie HAS
HAS octobre 2011
ADCS-ADL DAD 12semaines 24semaines 12semaines 24semaines
DONEPEZIL NS NS ND NDGALANTAMINE 1,39(0,59;2,20) 2,23(1,33-3,14) ND 3,76(1,66-5,86)RIVASTIGMINE ND 3,10(1,81-4,40) ND ND
D’autres variables • Réduction du fardeau ressenti
– Effet très modeste sur le fardeau ressenti (effect size 0,18 IC 95 % : 0,04-0,32) et le temps consacré (0,15 IC 95 % : 0,07-0,32) *
• Retard à l’entrée en institution – Aucun effet constaté ** (tendance p = 0.15 à 1 an dans AD2000
non retrouvé à 3 ans) – Voire un effet négatif à 5 ans (Cohorte 3C) ***
• Coût de prise en charge – Non significatif (débat méthodologique vif)
• Qualité de vie – Effet rarement mesuré, résultats non significatifs
* Linger JH et al JAGS 53:983–990, 2005. ** Birks J. Cholinesterase inhibitors for Alzheimer’s disease. Cochrane Database of Systematic Reviews 2006. *** Pimouget et al Alz & Dem 2015
Etude DOMINO 2012 T h e n e w e ngl a nd j o u r na l o f m e dic i n e
n engl j med 366;10 nejm.org march 8, 2012 893
original article
Donepezil and Memantine for Moderate-to-Severe Alzheimer’s Disease
Robert Howard, M.D., Rupert McShane, F.R.C.Psych., James Lindesay, D.M., Craig Ritchie, M.D., Ph.D., Ashley Baldwin, M.R.C.Psych., Robert Barber, M.D.,
Alistair Burns, F.R.C.Psych., Tom Dening, F.R.C.Psych., David Findlay, M.B., Ch.B., Clive Holmes, Ph.D., Alan Hughes, M.B., Ch.B., Robin Jacoby, D.M.,
Rob Jones, M.B., Ch.B., Roy Jones, M.B., Ian McKeith, F.Med.Sc., Ajay Macharouthu, M.R.C.Psych., John O’Brien, D.M., Peter Passmore, M.D.,
Bart Sheehan, M.D., Edmund Juszczak, M.Sc., Cornelius Katona, M.D., Robert Hills, D.Phil., Martin Knapp, Ph.D., Clive Ballard, M.D., Richard Brown, Ph.D.,
Sube Banerjee, M.D., Caroline Onions, P.G.Dip., Mary Griffin, R.G.N., Jessica Adams, B.Sc., Richard Gray, M.Sc., Tony Johnson, Ph.D.,
Peter Bentham, M.B., Ch.B., and Patrick Phillips, Ph.D.
From the Institute of Psychiatry (R. How-ard, M.K., R. Brown, S.B., J.A.) and the Wolfson Centre for Age Related Disease (C.B.), King’s College London, the Centre for Mental Health, Imperial College Lon-don (C.R.), the Department of Mental Health Sciences, University College Lon-don (C.K.), and the Medical Research Council (MRC) Clinical Trials Unit (T.J., P. Phillips) — all in London; the Fulbrook Centre, Churchill Hospital (R.M.), and the Department of Psychiatry (R. Jacoby), the Centre for Statistics in Medicine (E.J.), and the Clinical Trial Service Unit (R.G.), University of Oxford — all in Oxford; Health Sciences, University of Leicester, Leicester ( J.L.); Knowlsey Resource & Re-covery Centre, Whiston Hospital, Prescot (A. Baldwin); Institute for Ageing and Health, Newcastle University, Newcastle upon Tyne (R. Barber, I.M., J.O.); the School of Psychiatry and Behavioural Sciences, Wythenshawe Hospital, Manchester (A. Burns); Older People’s Mental Health Service, Fulbourn Hospital (T.D.), and the MRC Biostatistics Unit, Cambridge University (T.J.) — both in Cambridge; Royal Dundee Liff Hospital, Dundee Com-munity Health Partnership, Dundee (D.F.); Memory Assessment and Research Centre, University of Southampton, Southamp-ton (C.H.); the Department of Geriatric Psychiatry, Inverclyde Royal Hospital, Inverclyde (A.H.); Section of Old Age Psychiatry (Rob Jones) and Faculty of Medicine & Health Sciences (C.O.), Uni-versity of Nottingham, Nottingham; the Research Institute for the Care of Older People, Bath (Roy Jones); Mental Health Directorate, Crichton Royal Hospital, Dumfries (A.M.); Centre for Public Health, Queens University Belfast, Bel-fast (P. Passmore); Health Sciences Re-search Institute, University of Warwick, Coventry (B.S.); the Department of Hae-matology, University of Wales, Cardiff (R. Hills); South West Dementias and Neurodegenerative Diseases Research Network, Avon and Wiltshire Mental Health Partnership, Chippenham (M.G.); and Queen Elizabeth Psychiatric Hospi-tal, Birmingham (P.B.) — all in the United Kingdom. Address reprint requests to Dr. Howard at King’s College London, Insti-tute of Psychiatry, Department of Old Age Psychiatry, Box PO70, 16 DeCrespigny Park, London SE5 8AF, United Kingdom, or at [email protected].
N Engl J Med 2012;366:893-903.Copyright © 2012 Massachusetts Medical Society.
A bs tr ac t
BackgroundClinical trials have shown the benefits of cholinesterase inhibitors for the treatment of mild-to-moderate Alzheimer’s disease. It is not known whether treatment benefits continue after the progression to moderate-to-severe disease.MethodsWe assigned 295 community-dwelling patients who had been treated with donepezil for at least 3 months and who had moderate or severe Alzheimer’s disease (a score of 5 to 13 on the Standardized Mini–Mental State Examination [SMMSE, on which scores range from 0 to 30, with higher scores indicating better cognitive function]) to continue donepezil, discontinue donepezil, discontinue donepezil and start me-mantine, or continue donepezil and start memantine. Patients received the study treatment for 52 weeks. The coprimary outcomes were scores on the SMMSE and on the Bristol Activities of Daily Living Scale (BADLS, on which scores range from 0 to 60, with higher scores indicating greater impairment). The minimum clinically important differences were 1.4 points on the SMMSE and 3.5 points on the BADLS.ResultsPatients assigned to continue donepezil, as compared with those assigned to discon-tinue donepezil, had a score on the SMMSE that was higher by an average of 1.9 points (95% confidence interval [CI], 1.3 to 2.5) and a score on the BADLS that was lower (indicating less impairment) by 3.0 points (95% CI, 1.8 to 4.3) (P<0.001 for both com-parisons). Patients assigned to receive memantine, as compared with those assigned to receive memantine placebo, had a score on the SMMSE that was an average of 1.2 points higher (95% CI, 0.6 to 1.8; P<0.001) and a score on the BADLS that was 1.5 points lower (95% CI, 0.3 to 2.8; P = 0.02). The efficacy of donepezil and of memantine did not differ significantly in the presence or absence of the other. There were no significant benefits of the combination of donepezil and memantine over donepezil alone.ConclusionsIn patients with moderate or severe Alzheimer’s disease, continued treatment with donepezil was associated with cognitive benefits that exceeded the minimum clini-cally important difference and with significant functional benefits over the course of 12 months. (Funded by the U.K. Medical Research Council and the U.K. Alzheimer’s Society; Current Controlled Trials number, ISRCTN49545035.)
The New England Journal of Medicine Downloaded from nejm.org at ASSISTANCE PUBLIQUE HOPITAUX PARIS on March 9, 2012. For personal use only. No other uses without permission.
Copyright © 2012 Massachusetts Medical Society. All rights reserved.
Question : que se passe-t-il quand on arrête le donepezil lors de l’introduction de la mémantine ?
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
n engl j med 366;10 nejm.org march 8, 2012898
tion). There was no significant benefit of adding memantine to donepezil, with respect to scores on the SMMSE (0.8 points higher with memantine than with placebo; 95% CI, −0.1 to 1.6; P = 0.07) or with respect to scores on the BADLS (0.5 points lower with memantine than with placebo; 95% CI, −2.2 to 1.2; P = 0.57).
The severity of dementia at entry significantly influenced the effect of donepezil on SMMSE scores, with larger benefits observed in patients with moderate disease (SMMSE score, 10 to 13) than in those with severe disease (SMMSE score, 5 to 9). The average difference in scores between
the groups assigned to continue donepezil and the groups assigned to discontinue donepezil was 2.6 points (95% CI, 1.5 to 3.7) among patients with moderate disease (P<0.001) and 1.3 points (95% CI, 0.2 to 2.4) among patients with severe disease (P = 0.02). Because we undertook several tests for interaction, this difference according to the severity of dementia, which was only moder-ately significant, may have arisen by chance and needs to be confirmed, particularly since the se-verity of dementia did not have a significant effect on the difference in the BADLS score that was observed with continued, as compared with dis-
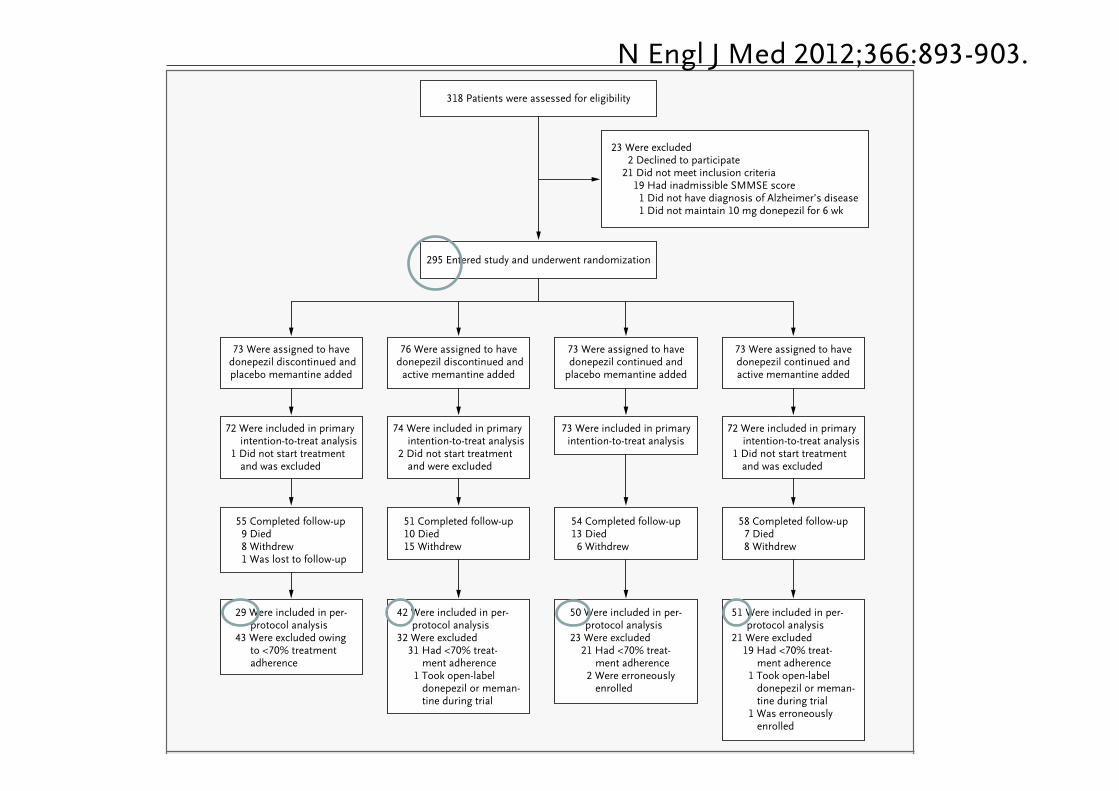
295 Entered study and underwent randomization
318 Patients were assessed for eligibility
23 Were excluded2 Declined to participate
21 Did not meet inclusion criteria19 Had inadmissible SMMSE score1 Did not have diagnosis of Alzheimer’s disease1 Did not maintain 10 mg donepezil for 6 wk
73 Were assigned to havedonepezil continued andactive memantine added
73 Were assigned to havedonepezil continued and
placebo memantine added
76 Were assigned to have donepezil discontinued and
active memantine added
73 Were assigned to have donepezil discontinued andplacebo memantine added
72 Were included in primaryintention-to-treat analysis
1 Did not start treatmentand was excluded
74 Were included in primaryintention-to-treat analysis
2 Did not start treatmentand were excluded
73 Were included in primaryintention-to-treat analysis
72 Were included in primaryintention-to-treat analysis
1 Did not start treatmentand was excluded
55 Completed follow-up9 Died8 Withdrew1 Was lost to follow-up
51 Completed follow-up10 Died15 Withdrew
54 Completed follow-up13 Died6 Withdrew
58 Completed follow-up7 Died8 Withdrew
29 Were included in per-protocol analysis
43 Were excluded owingto <70% treatmentadherence
42 Were included in per-protocol analysis
32 Were excluded31 Had <70% treat-
ment adherence1 Took open-label
donepezil or meman-tine during trial
50 Were included in per-protocol analysis
23 Were excluded21 Had <70% treat-
ment adherence2 Were erroneously
enrolled
51 Were included in per-protocol analysis
21 Were excluded19 Had <70% treat-
ment adherence1 Took open-label
donepezil or meman-tine during trial
1 Was erroneouslyenrolled
Figure 1. Enrollment, Randomization, and Follow-up.
SMMSE denotes Standardized Mini–Mental State Examination.
The New England Journal of Medicine Downloaded from nejm.org at ASSISTANCE PUBLIQUE HOPITAUX PARIS on March 9, 2012. For personal use only. No other uses without permission.
Copyright © 2012 Massachusetts Medical Society. All rights reserved.
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
n engl j med 366;10 nejm.org march 8, 2012 893
original article
Donepezil and Memantine for Moderate-to-Severe Alzheimer’s Disease
Robert Howard, M.D., Rupert McShane, F.R.C.Psych., James Lindesay, D.M., Craig Ritchie, M.D., Ph.D., Ashley Baldwin, M.R.C.Psych., Robert Barber, M.D.,
Alistair Burns, F.R.C.Psych., Tom Dening, F.R.C.Psych., David Findlay, M.B., Ch.B., Clive Holmes, Ph.D., Alan Hughes, M.B., Ch.B., Robin Jacoby, D.M.,
Rob Jones, M.B., Ch.B., Roy Jones, M.B., Ian McKeith, F.Med.Sc., Ajay Macharouthu, M.R.C.Psych., John O’Brien, D.M., Peter Passmore, M.D.,
Bart Sheehan, M.D., Edmund Juszczak, M.Sc., Cornelius Katona, M.D., Robert Hills, D.Phil., Martin Knapp, Ph.D., Clive Ballard, M.D., Richard Brown, Ph.D.,
Sube Banerjee, M.D., Caroline Onions, P.G.Dip., Mary Griffin, R.G.N., Jessica Adams, B.Sc., Richard Gray, M.Sc., Tony Johnson, Ph.D.,
Peter Bentham, M.B., Ch.B., and Patrick Phillips, Ph.D.
From the Institute of Psychiatry (R. How-ard, M.K., R. Brown, S.B., J.A.) and the Wolfson Centre for Age Related Disease (C.B.), King’s College London, the Centre for Mental Health, Imperial College Lon-don (C.R.), the Department of Mental Health Sciences, University College Lon-don (C.K.), and the Medical Research Council (MRC) Clinical Trials Unit (T.J., P. Phillips) — all in London; the Fulbrook Centre, Churchill Hospital (R.M.), and the Department of Psychiatry (R. Jacoby), the Centre for Statistics in Medicine (E.J.), and the Clinical Trial Service Unit (R.G.), University of Oxford — all in Oxford; Health Sciences, University of Leicester, Leicester ( J.L.); Knowlsey Resource & Re-covery Centre, Whiston Hospital, Prescot (A. Baldwin); Institute for Ageing and Health, Newcastle University, Newcastle upon Tyne (R. Barber, I.M., J.O.); the School of Psychiatry and Behavioural Sciences, Wythenshawe Hospital, Manchester (A. Burns); Older People’s Mental Health Service, Fulbourn Hospital (T.D.), and the MRC Biostatistics Unit, Cambridge University (T.J.) — both in Cambridge; Royal Dundee Liff Hospital, Dundee Com-munity Health Partnership, Dundee (D.F.); Memory Assessment and Research Centre, University of Southampton, Southamp-ton (C.H.); the Department of Geriatric Psychiatry, Inverclyde Royal Hospital, Inverclyde (A.H.); Section of Old Age Psychiatry (Rob Jones) and Faculty of Medicine & Health Sciences (C.O.), Uni-versity of Nottingham, Nottingham; the Research Institute for the Care of Older People, Bath (Roy Jones); Mental Health Directorate, Crichton Royal Hospital, Dumfries (A.M.); Centre for Public Health, Queens University Belfast, Bel-fast (P. Passmore); Health Sciences Re-search Institute, University of Warwick, Coventry (B.S.); the Department of Hae-matology, University of Wales, Cardiff (R. Hills); South West Dementias and Neurodegenerative Diseases Research Network, Avon and Wiltshire Mental Health Partnership, Chippenham (M.G.); and Queen Elizabeth Psychiatric Hospi-tal, Birmingham (P.B.) — all in the United Kingdom. Address reprint requests to Dr. Howard at King’s College London, Insti-tute of Psychiatry, Department of Old Age Psychiatry, Box PO70, 16 DeCrespigny Park, London SE5 8AF, United Kingdom, or at [email protected].
N Engl J Med 2012;366:893-903.Copyright © 2012 Massachusetts Medical Society.
A bs tr ac t
BackgroundClinical trials have shown the benefits of cholinesterase inhibitors for the treatment of mild-to-moderate Alzheimer’s disease. It is not known whether treatment benefits continue after the progression to moderate-to-severe disease.MethodsWe assigned 295 community-dwelling patients who had been treated with donepezil for at least 3 months and who had moderate or severe Alzheimer’s disease (a score of 5 to 13 on the Standardized Mini–Mental State Examination [SMMSE, on which scores range from 0 to 30, with higher scores indicating better cognitive function]) to continue donepezil, discontinue donepezil, discontinue donepezil and start me-mantine, or continue donepezil and start memantine. Patients received the study treatment for 52 weeks. The coprimary outcomes were scores on the SMMSE and on the Bristol Activities of Daily Living Scale (BADLS, on which scores range from 0 to 60, with higher scores indicating greater impairment). The minimum clinically important differences were 1.4 points on the SMMSE and 3.5 points on the BADLS.ResultsPatients assigned to continue donepezil, as compared with those assigned to discon-tinue donepezil, had a score on the SMMSE that was higher by an average of 1.9 points (95% confidence interval [CI], 1.3 to 2.5) and a score on the BADLS that was lower (indicating less impairment) by 3.0 points (95% CI, 1.8 to 4.3) (P<0.001 for both com-parisons). Patients assigned to receive memantine, as compared with those assigned to receive memantine placebo, had a score on the SMMSE that was an average of 1.2 points higher (95% CI, 0.6 to 1.8; P<0.001) and a score on the BADLS that was 1.5 points lower (95% CI, 0.3 to 2.8; P = 0.02). The efficacy of donepezil and of memantine did not differ significantly in the presence or absence of the other. There were no significant benefits of the combination of donepezil and memantine over donepezil alone.ConclusionsIn patients with moderate or severe Alzheimer’s disease, continued treatment with donepezil was associated with cognitive benefits that exceeded the minimum clini-cally important difference and with significant functional benefits over the course of 12 months. (Funded by the U.K. Medical Research Council and the U.K. Alzheimer’s Society; Current Controlled Trials number, ISRCTN49545035.)
The New England Journal of Medicine Downloaded from nejm.org at ASSISTANCE PUBLIQUE HOPITAUX PARIS on March 9, 2012. For personal use only. No other uses without permission.
Copyright © 2012 Massachusetts Medical Society. All rights reserved.
Bristol ADL : mélange ADL et IADL n/60
• Préparer les repas • Manger • Préparer les boissons • Boire • S’habiller • Hygiène • Dents • Bain/douche • Toilette/Continence
• Mobilité • Orientation temps/espace • Communication • Téléphone • Ménage • Courses • Finances • Jeux/hobby • Transports
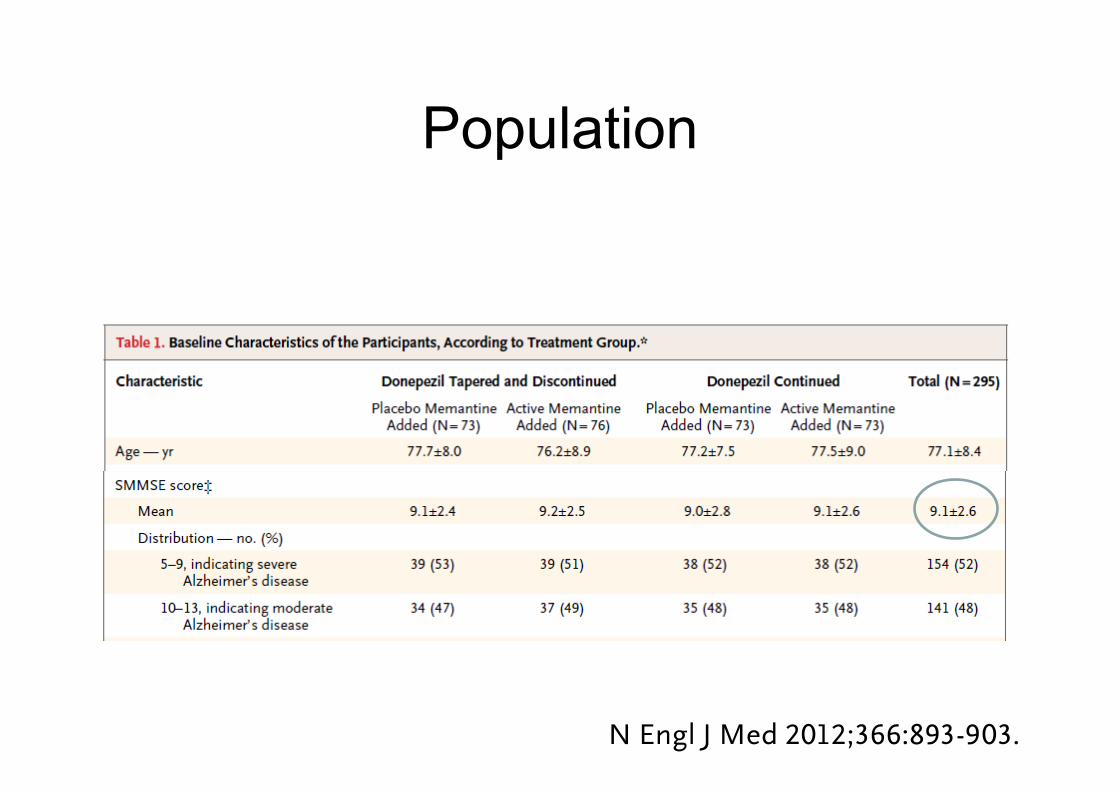
Population
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
n engl j med 366;10 nejm.org march 8, 2012 893
original article
Donepezil and Memantine for Moderate-to-Severe Alzheimer’s Disease
Robert Howard, M.D., Rupert McShane, F.R.C.Psych., James Lindesay, D.M., Craig Ritchie, M.D., Ph.D., Ashley Baldwin, M.R.C.Psych., Robert Barber, M.D.,
Alistair Burns, F.R.C.Psych., Tom Dening, F.R.C.Psych., David Findlay, M.B., Ch.B., Clive Holmes, Ph.D., Alan Hughes, M.B., Ch.B., Robin Jacoby, D.M.,
Rob Jones, M.B., Ch.B., Roy Jones, M.B., Ian McKeith, F.Med.Sc., Ajay Macharouthu, M.R.C.Psych., John O’Brien, D.M., Peter Passmore, M.D.,
Bart Sheehan, M.D., Edmund Juszczak, M.Sc., Cornelius Katona, M.D., Robert Hills, D.Phil., Martin Knapp, Ph.D., Clive Ballard, M.D., Richard Brown, Ph.D.,
Sube Banerjee, M.D., Caroline Onions, P.G.Dip., Mary Griffin, R.G.N., Jessica Adams, B.Sc., Richard Gray, M.Sc., Tony Johnson, Ph.D.,
Peter Bentham, M.B., Ch.B., and Patrick Phillips, Ph.D.
From the Institute of Psychiatry (R. How-ard, M.K., R. Brown, S.B., J.A.) and the Wolfson Centre for Age Related Disease (C.B.), King’s College London, the Centre for Mental Health, Imperial College Lon-don (C.R.), the Department of Mental Health Sciences, University College Lon-don (C.K.), and the Medical Research Council (MRC) Clinical Trials Unit (T.J., P. Phillips) — all in London; the Fulbrook Centre, Churchill Hospital (R.M.), and the Department of Psychiatry (R. Jacoby), the Centre for Statistics in Medicine (E.J.), and the Clinical Trial Service Unit (R.G.), University of Oxford — all in Oxford; Health Sciences, University of Leicester, Leicester ( J.L.); Knowlsey Resource & Re-covery Centre, Whiston Hospital, Prescot (A. Baldwin); Institute for Ageing and Health, Newcastle University, Newcastle upon Tyne (R. Barber, I.M., J.O.); the School of Psychiatry and Behavioural Sciences, Wythenshawe Hospital, Manchester (A. Burns); Older People’s Mental Health Service, Fulbourn Hospital (T.D.), and the MRC Biostatistics Unit, Cambridge University (T.J.) — both in Cambridge; Royal Dundee Liff Hospital, Dundee Com-munity Health Partnership, Dundee (D.F.); Memory Assessment and Research Centre, University of Southampton, Southamp-ton (C.H.); the Department of Geriatric Psychiatry, Inverclyde Royal Hospital, Inverclyde (A.H.); Section of Old Age Psychiatry (Rob Jones) and Faculty of Medicine & Health Sciences (C.O.), Uni-versity of Nottingham, Nottingham; the Research Institute for the Care of Older People, Bath (Roy Jones); Mental Health Directorate, Crichton Royal Hospital, Dumfries (A.M.); Centre for Public Health, Queens University Belfast, Bel-fast (P. Passmore); Health Sciences Re-search Institute, University of Warwick, Coventry (B.S.); the Department of Hae-matology, University of Wales, Cardiff (R. Hills); South West Dementias and Neurodegenerative Diseases Research Network, Avon and Wiltshire Mental Health Partnership, Chippenham (M.G.); and Queen Elizabeth Psychiatric Hospi-tal, Birmingham (P.B.) — all in the United Kingdom. Address reprint requests to Dr. Howard at King’s College London, Insti-tute of Psychiatry, Department of Old Age Psychiatry, Box PO70, 16 DeCrespigny Park, London SE5 8AF, United Kingdom, or at [email protected].
N Engl J Med 2012;366:893-903.Copyright © 2012 Massachusetts Medical Society.
A bs tr ac t
BackgroundClinical trials have shown the benefits of cholinesterase inhibitors for the treatment of mild-to-moderate Alzheimer’s disease. It is not known whether treatment benefits continue after the progression to moderate-to-severe disease.MethodsWe assigned 295 community-dwelling patients who had been treated with donepezil for at least 3 months and who had moderate or severe Alzheimer’s disease (a score of 5 to 13 on the Standardized Mini–Mental State Examination [SMMSE, on which scores range from 0 to 30, with higher scores indicating better cognitive function]) to continue donepezil, discontinue donepezil, discontinue donepezil and start me-mantine, or continue donepezil and start memantine. Patients received the study treatment for 52 weeks. The coprimary outcomes were scores on the SMMSE and on the Bristol Activities of Daily Living Scale (BADLS, on which scores range from 0 to 60, with higher scores indicating greater impairment). The minimum clinically important differences were 1.4 points on the SMMSE and 3.5 points on the BADLS.ResultsPatients assigned to continue donepezil, as compared with those assigned to discon-tinue donepezil, had a score on the SMMSE that was higher by an average of 1.9 points (95% confidence interval [CI], 1.3 to 2.5) and a score on the BADLS that was lower (indicating less impairment) by 3.0 points (95% CI, 1.8 to 4.3) (P<0.001 for both com-parisons). Patients assigned to receive memantine, as compared with those assigned to receive memantine placebo, had a score on the SMMSE that was an average of 1.2 points higher (95% CI, 0.6 to 1.8; P<0.001) and a score on the BADLS that was 1.5 points lower (95% CI, 0.3 to 2.8; P = 0.02). The efficacy of donepezil and of memantine did not differ significantly in the presence or absence of the other. There were no significant benefits of the combination of donepezil and memantine over donepezil alone.ConclusionsIn patients with moderate or severe Alzheimer’s disease, continued treatment with donepezil was associated with cognitive benefits that exceeded the minimum clini-cally important difference and with significant functional benefits over the course of 12 months. (Funded by the U.K. Medical Research Council and the U.K. Alzheimer’s Society; Current Controlled Trials number, ISRCTN49545035.)
The New England Journal of Medicine Downloaded from nejm.org at ASSISTANCE PUBLIQUE HOPITAUX PARIS on March 9, 2012. For personal use only. No other uses without permission.
Copyright © 2012 Massachusetts Medical Society. All rights reserved.
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
n engl j med 366;10 nejm.org march 8, 2012900
analyses were conducted to assess the effect of treatment withdrawal and missing outcome as-sessments on the results. The results of the sen-sitivity analyses were broadly similar to those of the primary analysis (see Table S3 in the Supple-mentary Appendix).
SafetyA total of 188 serious adverse events were reported, of which 6 (2 in the group receiving placebo done-pezil and placebo memantine, 2 in the group re-ceiving memantine and placebo donepezil, and 2 in the group receiving donepezil and memantine) were considered to be possibly related to the study drugs. None were considered to be unexpected se-rious adverse reactions. There was no evidence that the incidence of serious adverse events or death differed according to treatment group (P = 0.77). Details of the serious adverse events and deaths in
all treatment groups are provided in Table S5 in the Supplementary Appendix.
Discussion
This double-blind, placebo-controlled trial involv-ing community-living patients with moderate or severe Alzheimer’s disease who were already re-ceiving treatment with a cholinesterase inhibitor showed that there were modest cognitive and func-tional benefits of continuing donepezil over the course of 12 months. The difference in scores on the SMMSE between those who continued donep-ezil and those who discontinued it exceeded the prespecified minimum clinically important differ-ence of 1.4 points, but the difference in scores on the BADLS was less than the minimum clinically important difference of 3.5 points. The initiation of memantine therapy was also associated with sig-
SMM
SE
10
8
9
7
6
4
3
1
5
2
00 6 18 30 52
Visit WeekBA
DLS
42
38
40
36
34
30
28
32
260
0 6 18 30 52
Visit Week
Direction of improvement
Direction of improvement
Placebo donepezil and placebo memantine
Placebo donepezil and active memantine
Active donepezil and placebo memantine
Active donepezil and active memantine
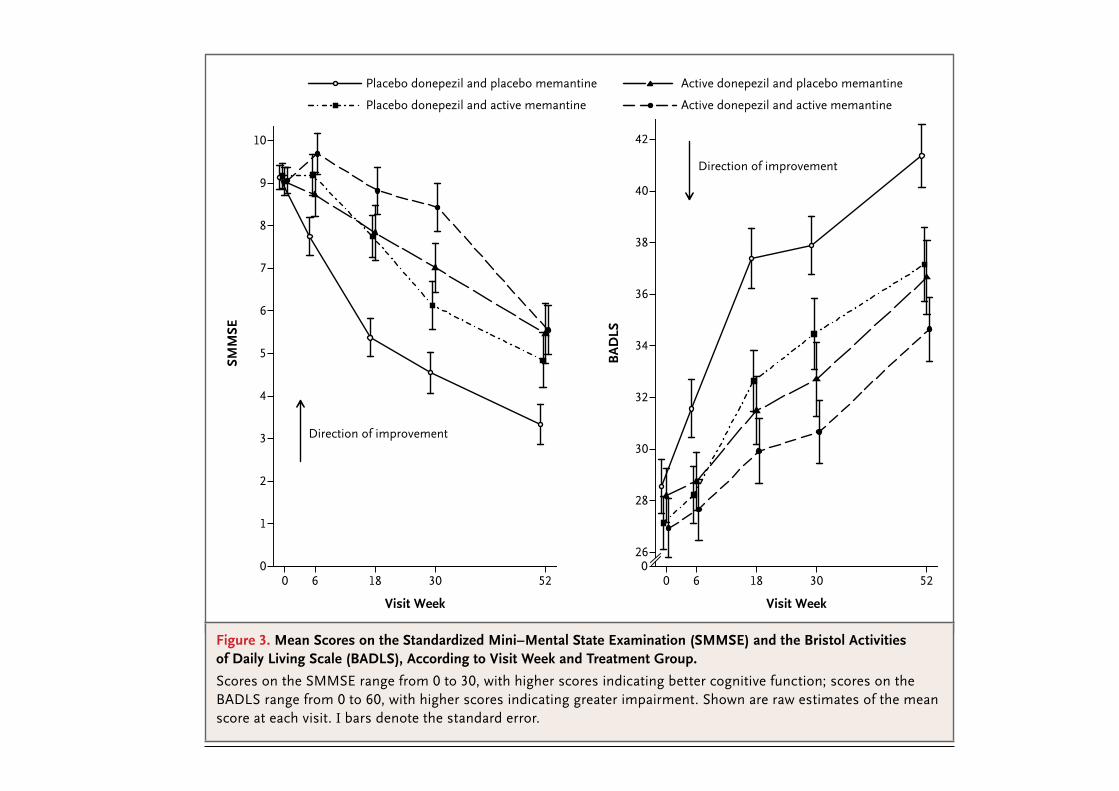
Figure 3. Mean Scores on the Standardized Mini–Mental State Examination (SMMSE) and the Bristol Activities of Daily Living Scale (BADLS), According to Visit Week and Treatment Group.
Scores on the SMMSE range from 0 to 30, with higher scores indicating better cognitive function; scores on the BADLS range from 0 to 60, with higher scores indicating greater impairment. Shown are raw estimates of the mean score at each visit. I bars denote the standard error.
The New England Journal of Medicine Downloaded from nejm.org at ASSISTANCE PUBLIQUE HOPITAUX PARIS on March 9, 2012. For personal use only. No other uses without permission.
Copyright © 2012 Massachusetts Medical Society. All rights reserved.
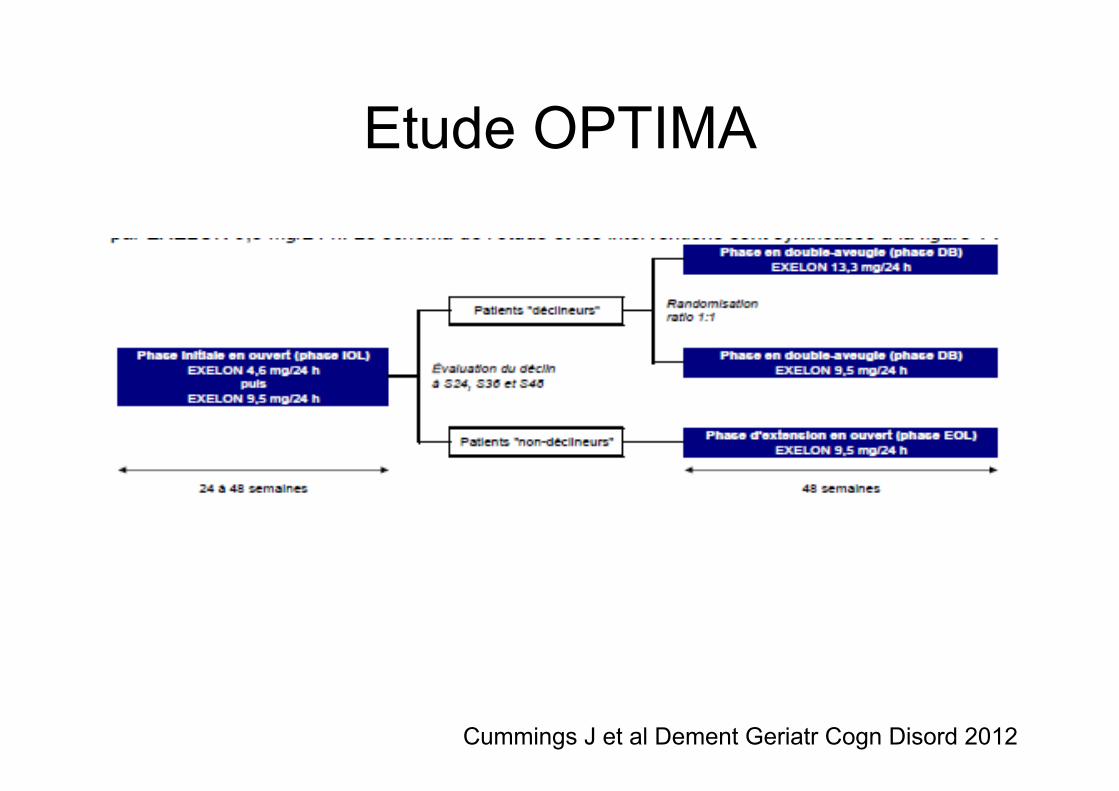
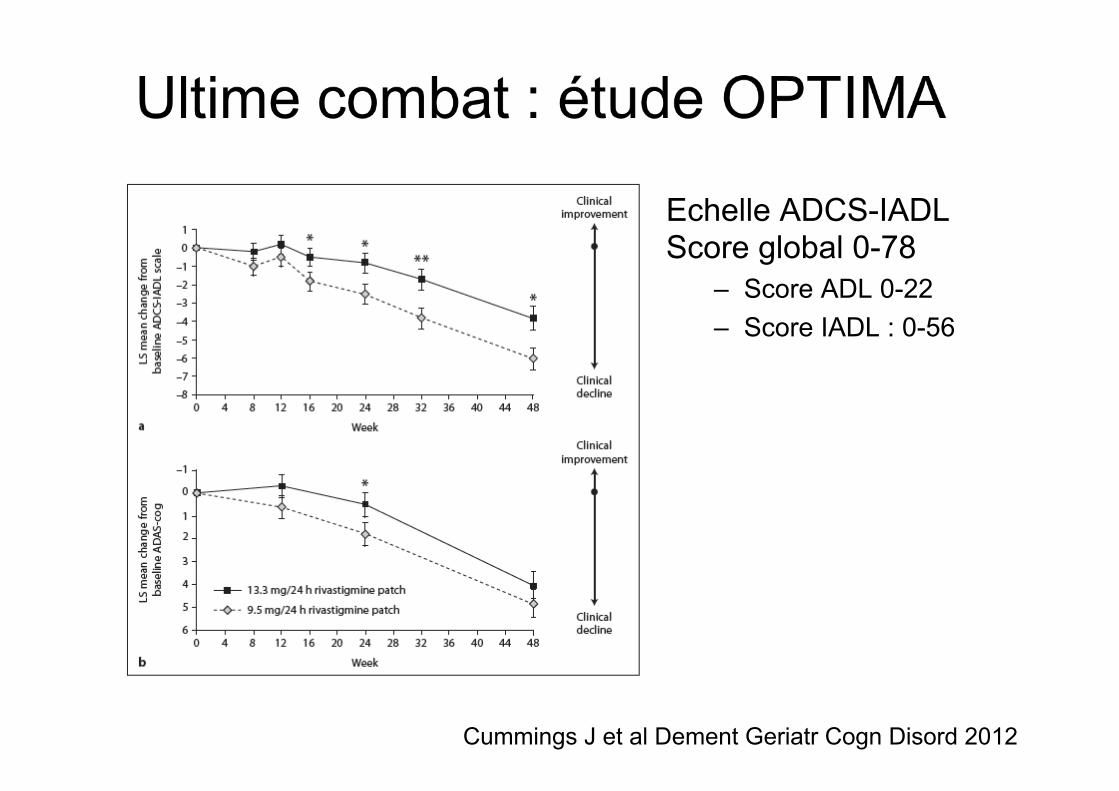
Etude OPTIMA
Cummings J et al Dement Geriatr Cogn Disord 2012
Cummings J et al Dement Geriatr Cogn Disord 2012
Echelle ADCS-IADL Score global 0-78
– Score ADL 0-22 – Score IADL : 0-56
Les études dans les pathologies hors AMM
• Alzheimer à un stade sévère • Mild Cognitive Impairment • Autres déclins cognitifs
• Maladie des corps de Lewy diffus • Démence parkinsonnienne (AMM
Réminyl) • Démences vasculaires
Autres questions sur les IACE
Existence de bons répondeurs ? L’un meilleur que l’autre ?
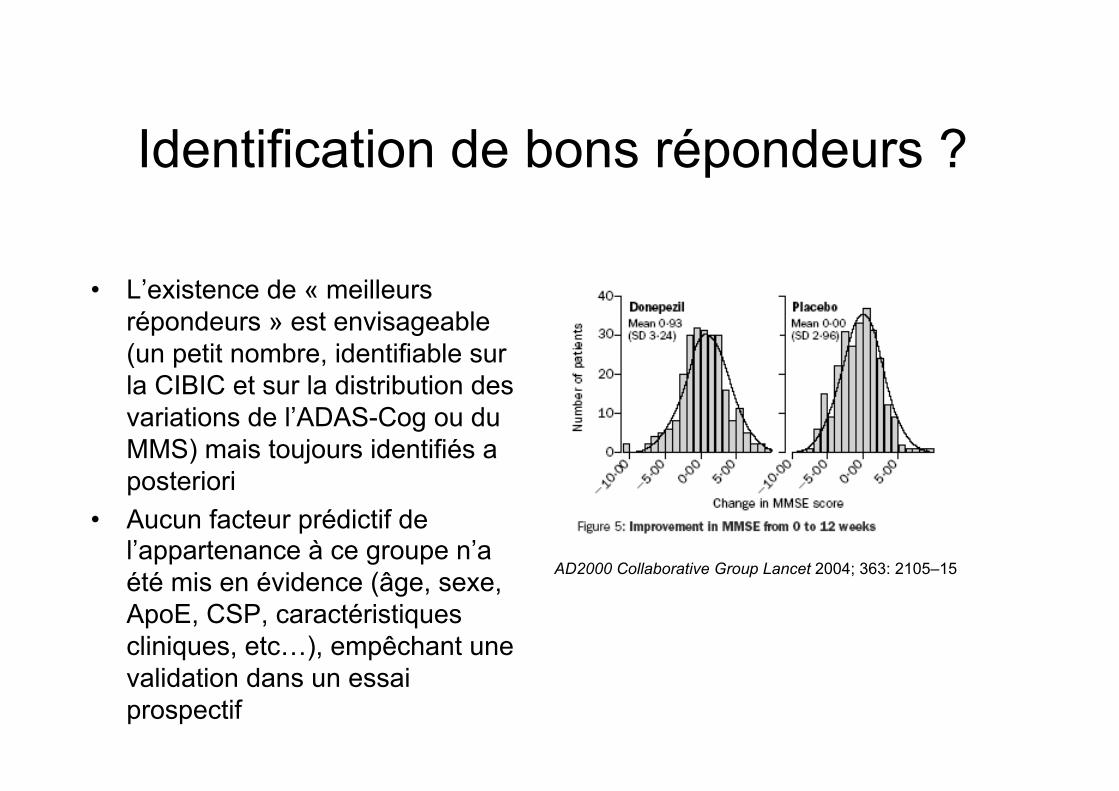
Identification de bons répondeurs ?
• L’existence de « meilleurs répondeurs » est envisageable (un petit nombre, identifiable sur la CIBIC et sur la distribution des variations de l’ADAS-Cog ou du MMS) mais toujours identifiés a posteriori
• Aucun facteur prédictif de l’appartenance à ce groupe n’a été mis en évidence (âge, sexe, ApoE, CSP, caractéristiques cliniques, etc…), empêchant une validation dans un essai prospectif
AD2000 Collaborative Group Lancet 2004; 363: 2105–15
Un IACE meilleur que l’autre ?
• Une littérature contradictoire, probablement biaisée *, voire avec de grosses lacunes méthodologiques **
• Pas de différences dans les variables de résultats ou de tolérance ***
• Aucune donnée solide sur le « switch »
* David B Hogan, Barry Goldlist, Gary Naglie, and Christopher Patterson Lancet Neurol 2004; 3: 622–26 ** G Wilkock et al Drugs Aging 2003; 20 (10): 777-789) *** Birks J. Cholinesterase inhibitors for Alzheimer’s disease. Cochrane Database of Systematic Reviews 2006, Issue 1. Art. No.: CD005593. DOI: 10.1002/14651858.CD005593.
Un exemple de méthodologie plus que douteuse
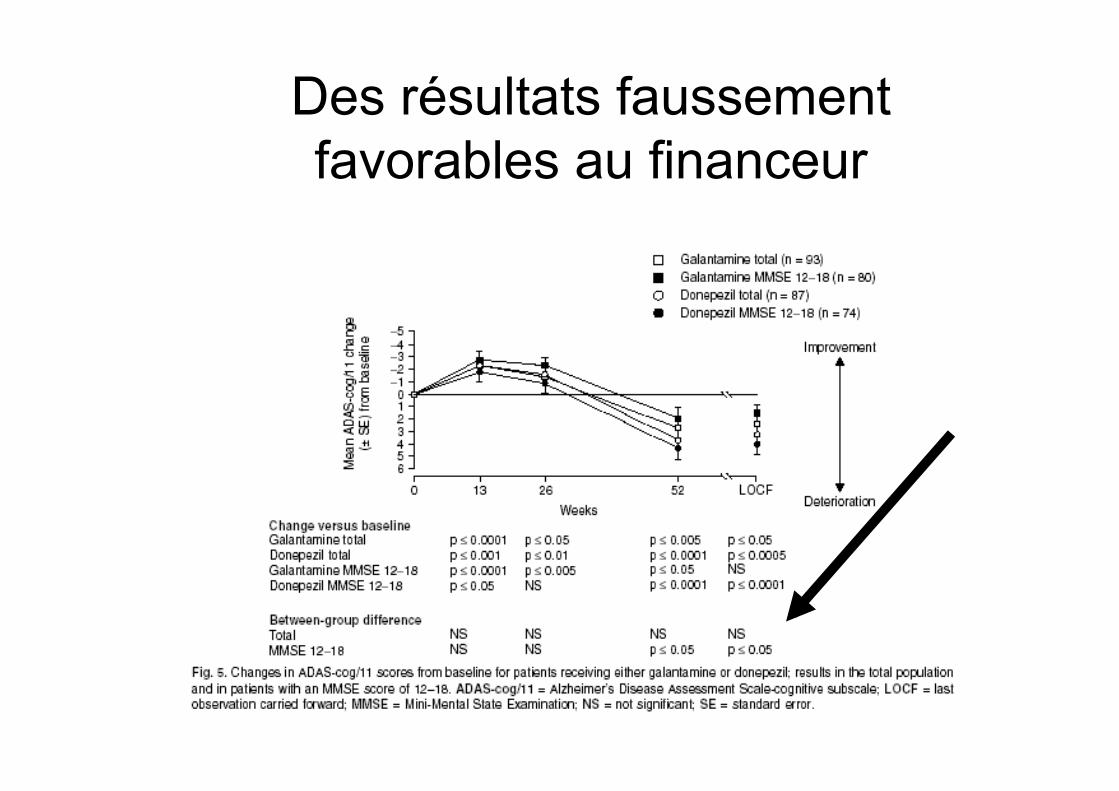
Des résultats faussement favorables au financeur
MEMANTINE
• Un dossier mince • Une hypothèse physiopathologie fragile
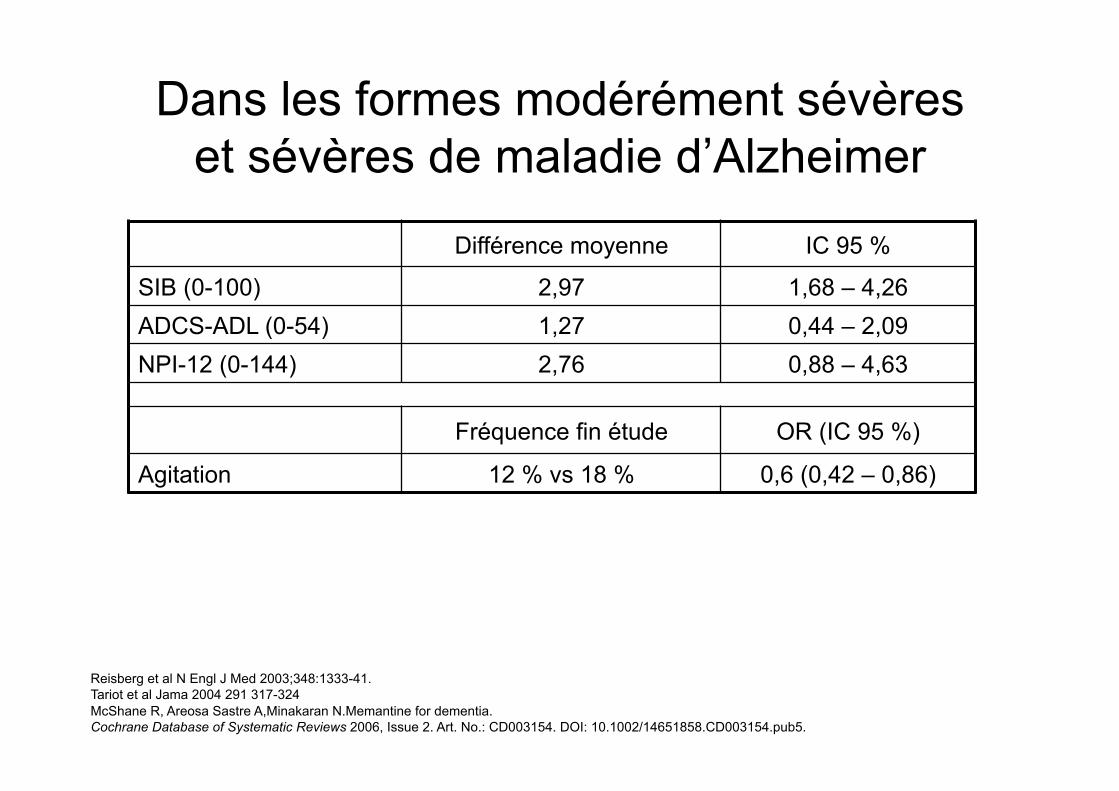
Dans les formes modérément sévères et sévères de maladie d’Alzheimer
Différence moyenne IC 95 %
SIB (0-100) 2,97 1,68 – 4,26 ADCS-ADL (0-54) 1,27 0,44 – 2,09 NPI-12 (0-144) 2,76 0,88 – 4,63
Fréquence fin étude OR (IC 95 %)
Agitation 12 % vs 18 % 0,6 (0,42 – 0,86)
Reisberg et al N Engl J Med 2003;348:1333-41. Tariot et al Jama 2004 291 317-324 McShane R, Areosa Sastre A,Minakaran N.Memantine for dementia. Cochrane Database of Systematic Reviews 2006, Issue 2. Art. No.: CD003154. DOI: 10.1002/14651858.CD003154.pub5.
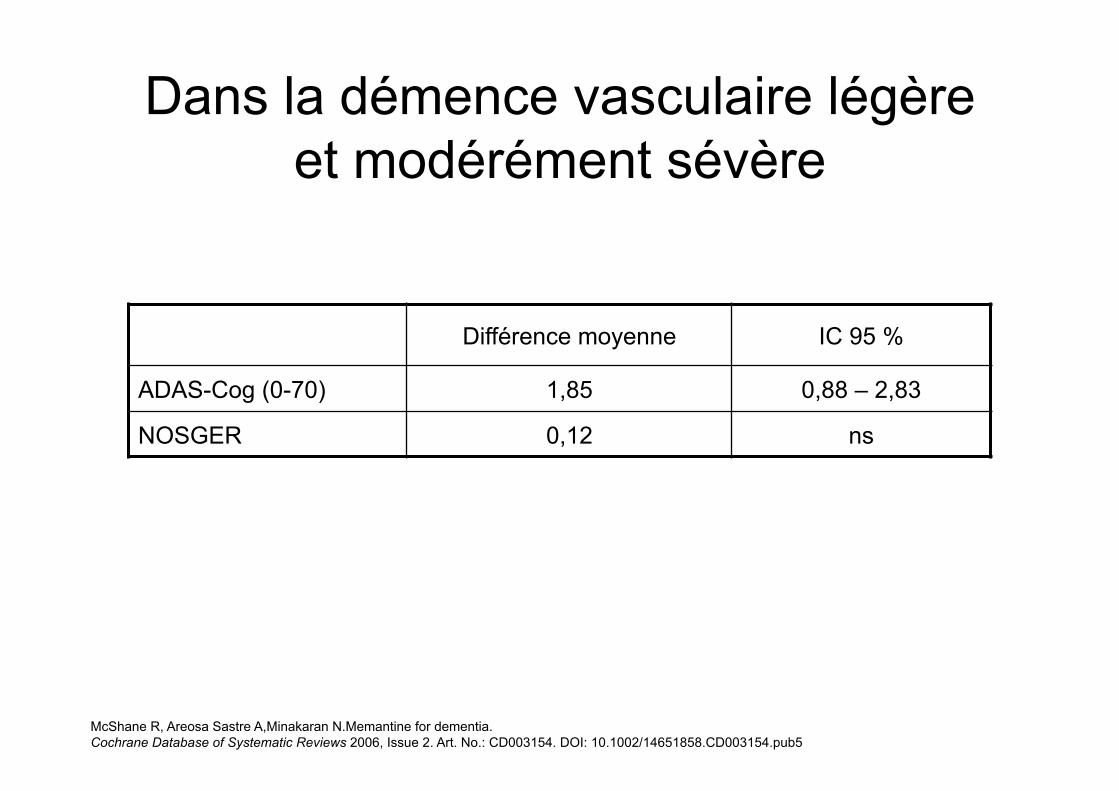
Dans la démence vasculaire légère et modérément sévère
Différence moyenne IC 95 %
ADAS-Cog (0-70) 1,85 0,88 – 2,83
NOSGER 0,12 ns
McShane R, Areosa Sastre A,Minakaran N.Memantine for dementia. Cochrane Database of Systematic Reviews 2006, Issue 2. Art. No.: CD003154. DOI: 10.1002/14651858.CD003154.pub5
NEJM 2003; 348: 1333-41
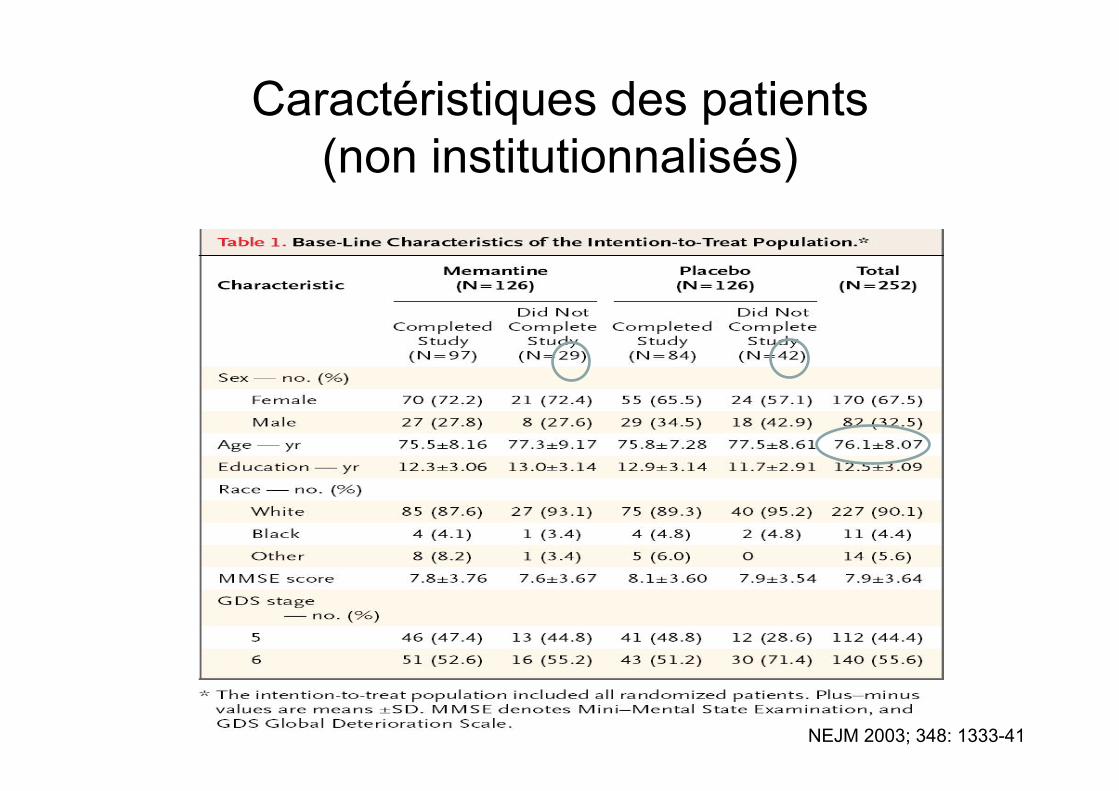
Caractéristiques des patients (non institutionnalisés)
NEJM 2003; 348: 1333-41
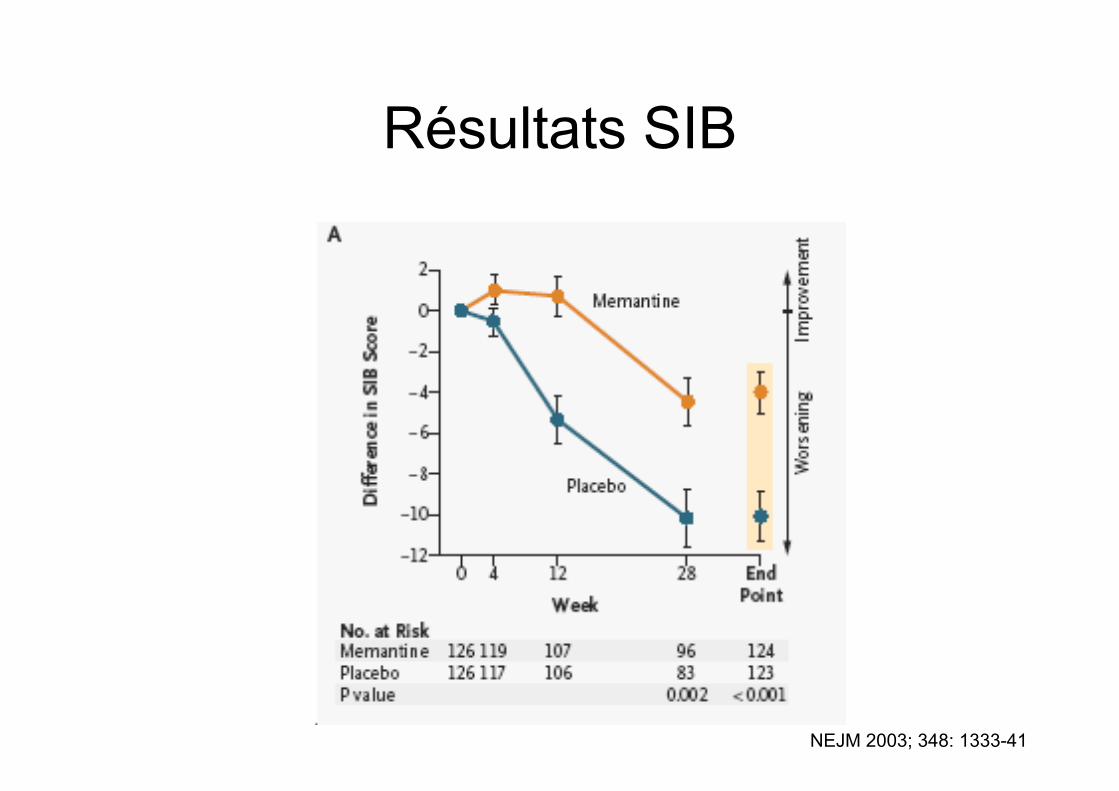
Résultats SIB
NEJM 2003; 348: 1333-41
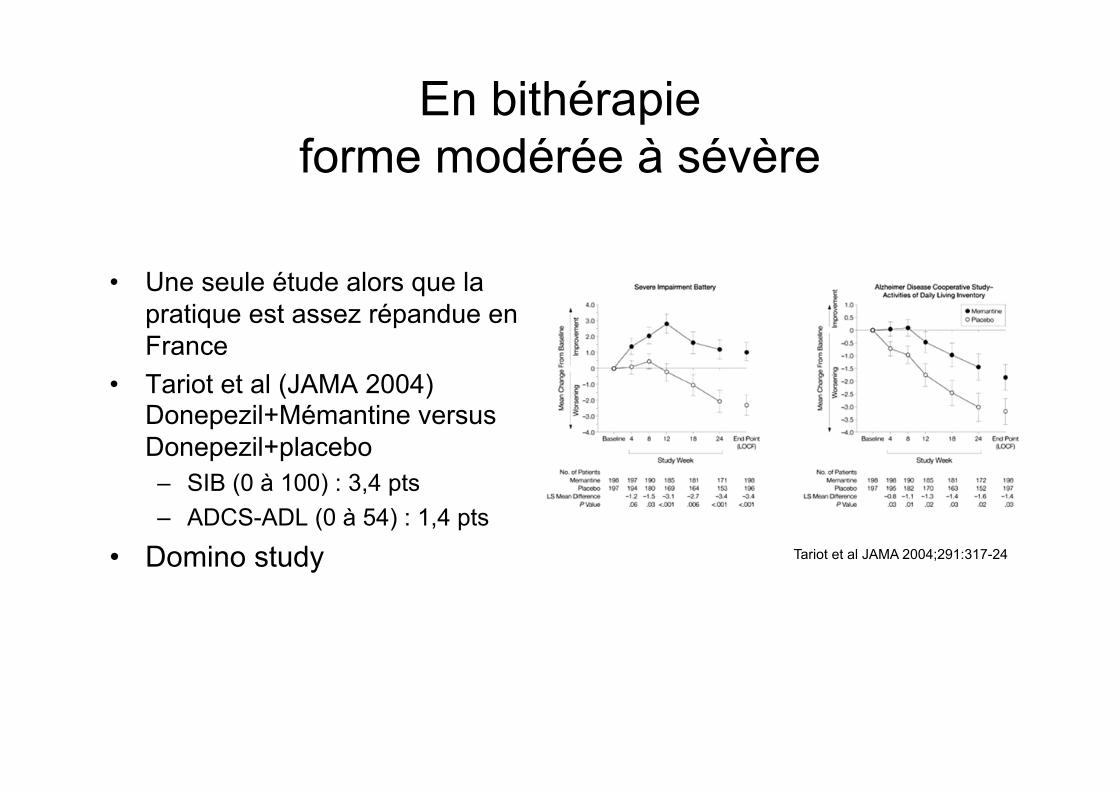
En bithérapie forme modérée à sévère
• Une seule étude alors que la pratique est assez répandue en France
• Tariot et al (JAMA 2004) Donepezil+Mémantine versus Donepezil+placebo – SIB (0 à 100) : 3,4 pts – ADCS-ADL (0 à 54) : 1,4 pts
• Domino study Tariot et al JAMA 2004;291:317-24
IACE et MCI
• Objectif : réduire le taux de conversion en maladie avérée
• Toutes les études sont négatives – Donepezil* : 3 études – Galantamine** : 2 études (dont une avec surmortalité
dans le groupe traité)
* Russ Tc et al Cochrane 2012 ** Loy C et al Cochrane 2006
Démences avec Parkinsonnisme 1. Quelques études éparses ne permettant pas
d’aboutir à un niveau de preuve suffisant
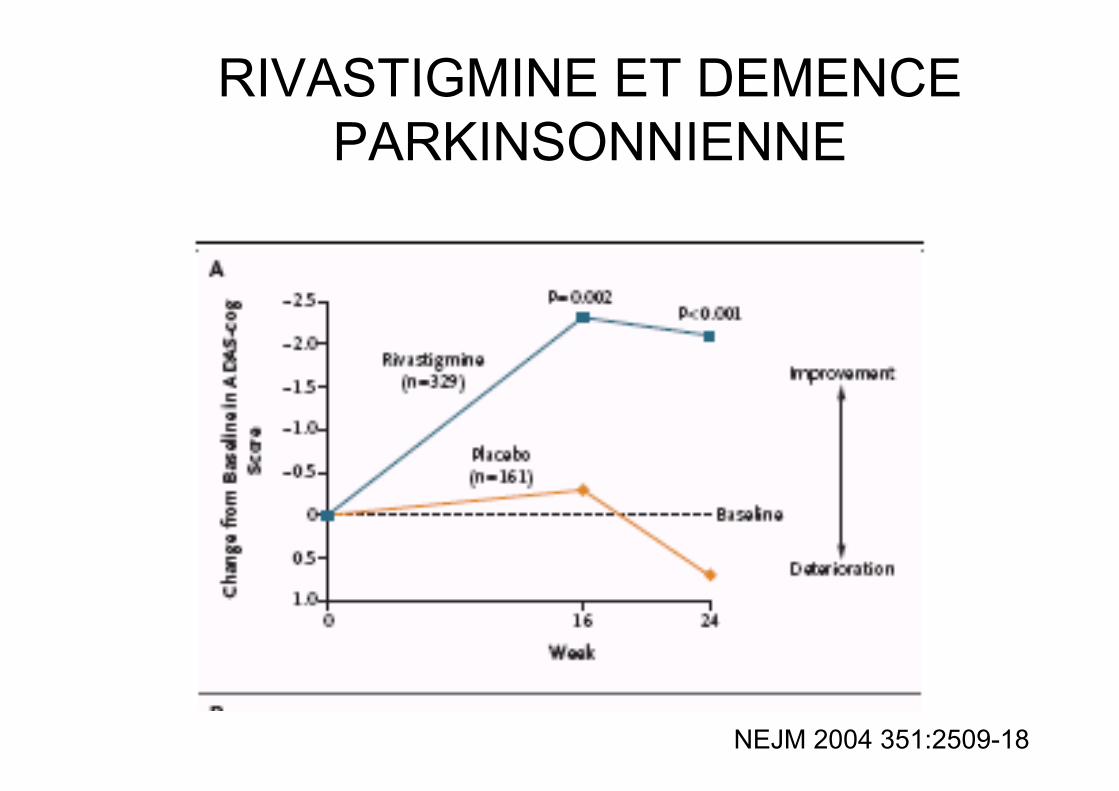
RIVASTIGMINE ET DEMENCE PARKINSONNIENNE
NEJM 2004 351:2509-18
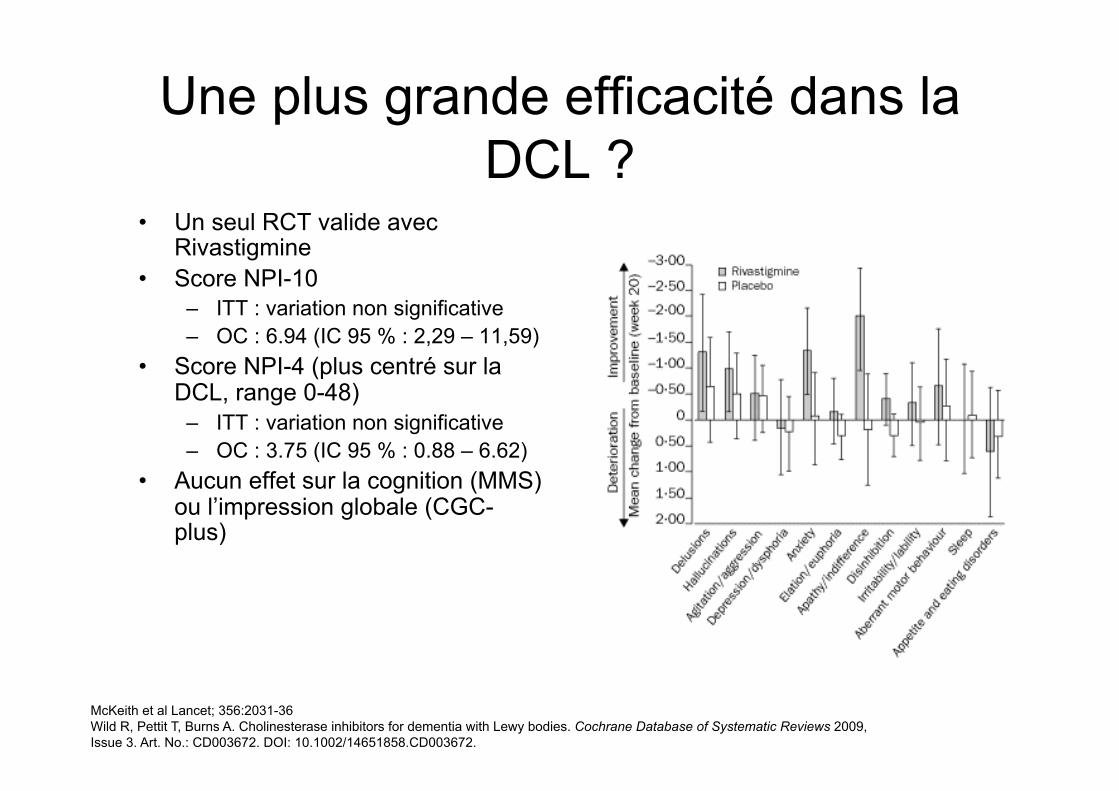
Une plus grande efficacité dans la DCL ?
• Un seul RCT valide avec Rivastigmine
• Score NPI-10 – ITT : variation non significative – OC : 6.94 (IC 95 % : 2,29 – 11,59)
• Score NPI-4 (plus centré sur la DCL, range 0-48)
– ITT : variation non significative – OC : 3.75 (IC 95 % : 0.88 – 6.62)
• Aucun effet sur la cognition (MMS) ou l’impression globale (CGC-plus)
McKeith et al Lancet; 356:2031-36 Wild R, Pettit T, Burns A. Cholinesterase inhibitors for dementia with Lewy bodies. Cochrane Database of Systematic Reviews 2009, Issue 3. Art. No.: CD003672. DOI: 10.1002/14651858.CD003672.
DEMENCES FRONTO-TEMPORALES
• Une inconnue totale
Quelle prescription dans la vraie vie ?
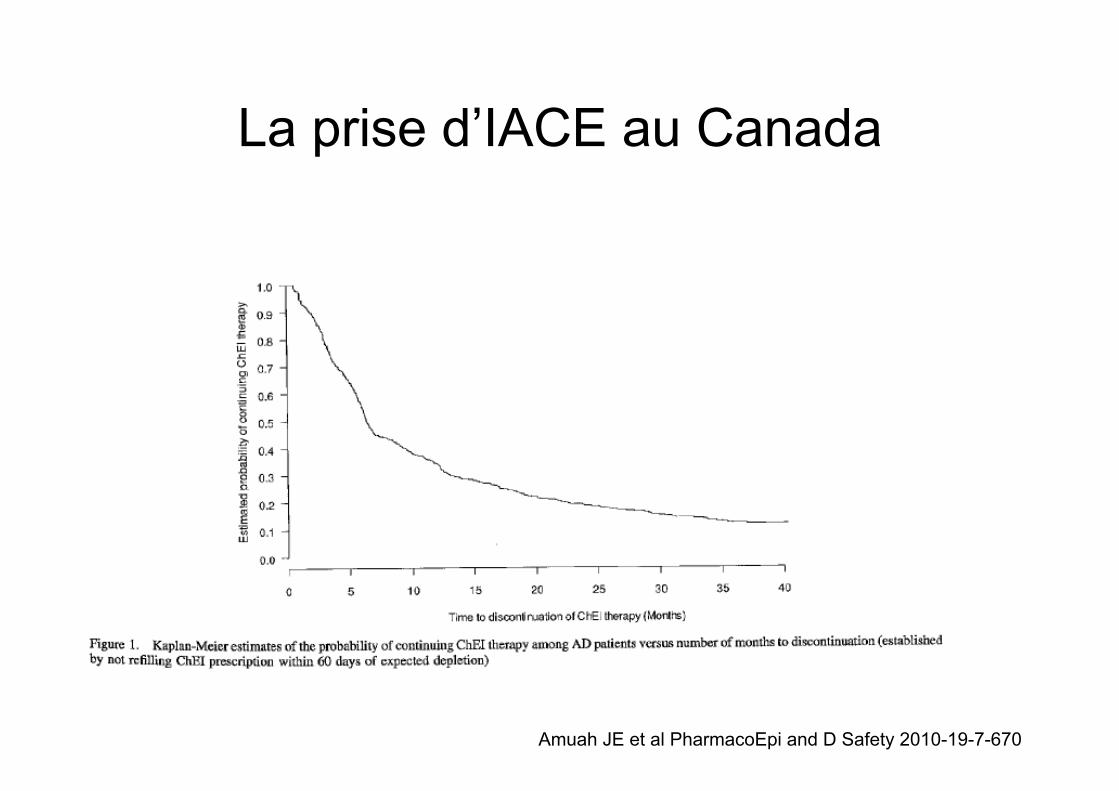
La prise d’IACE au Canada
Amuah JE et al PharmacoEpi and D Safety 2010-19-7-670
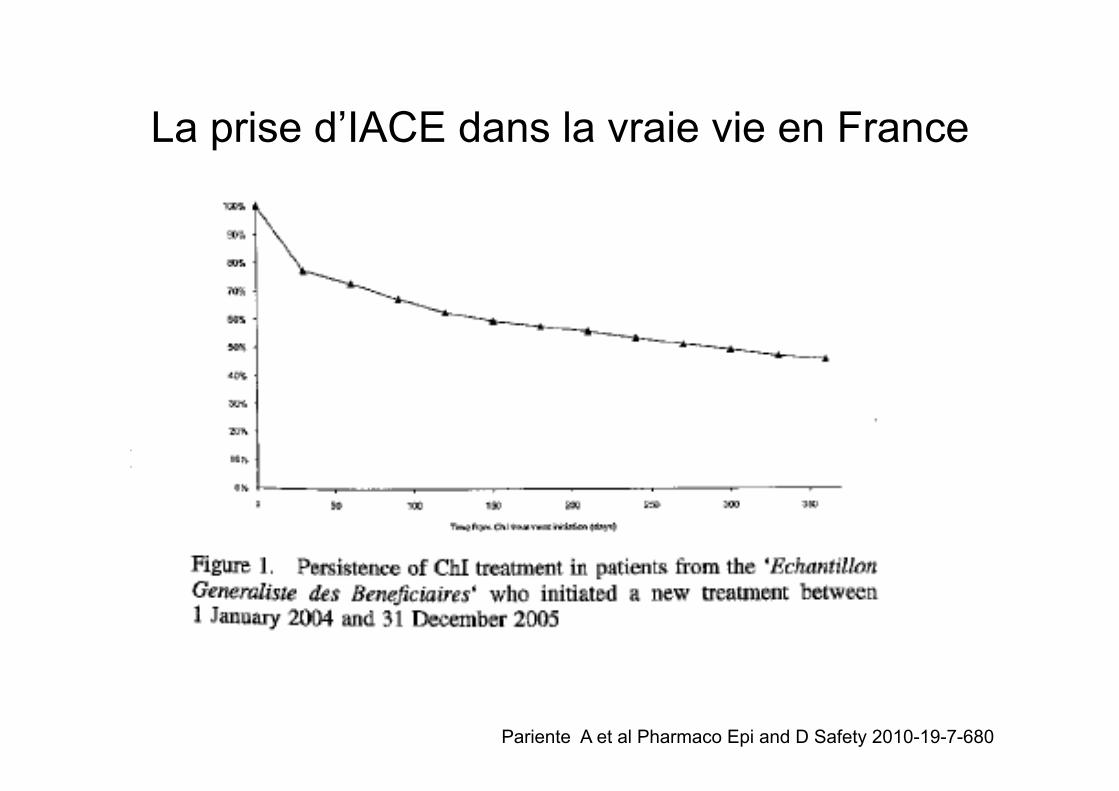
La prise d’IACE dans la vraie vie en France
Pariente A et al Pharmaco Epi and D Safety 2010-19-7-680
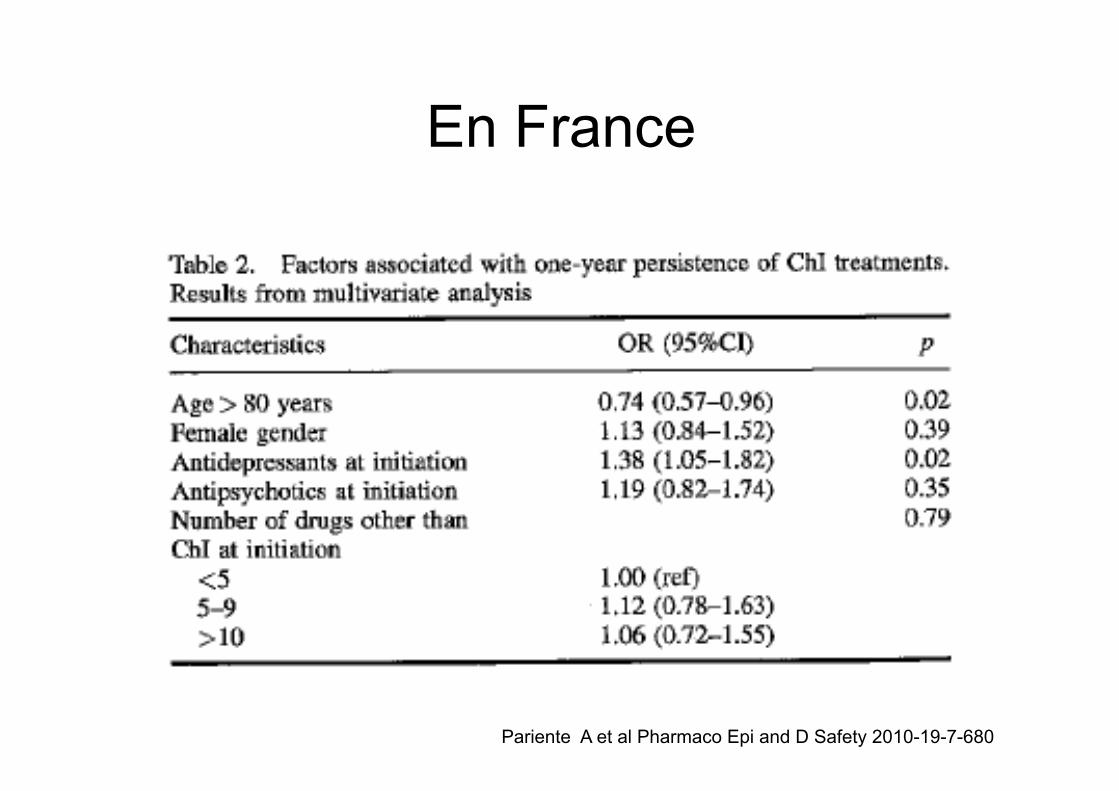
En France
Pariente A et al Pharmaco Epi and D Safety 2010-19-7-680
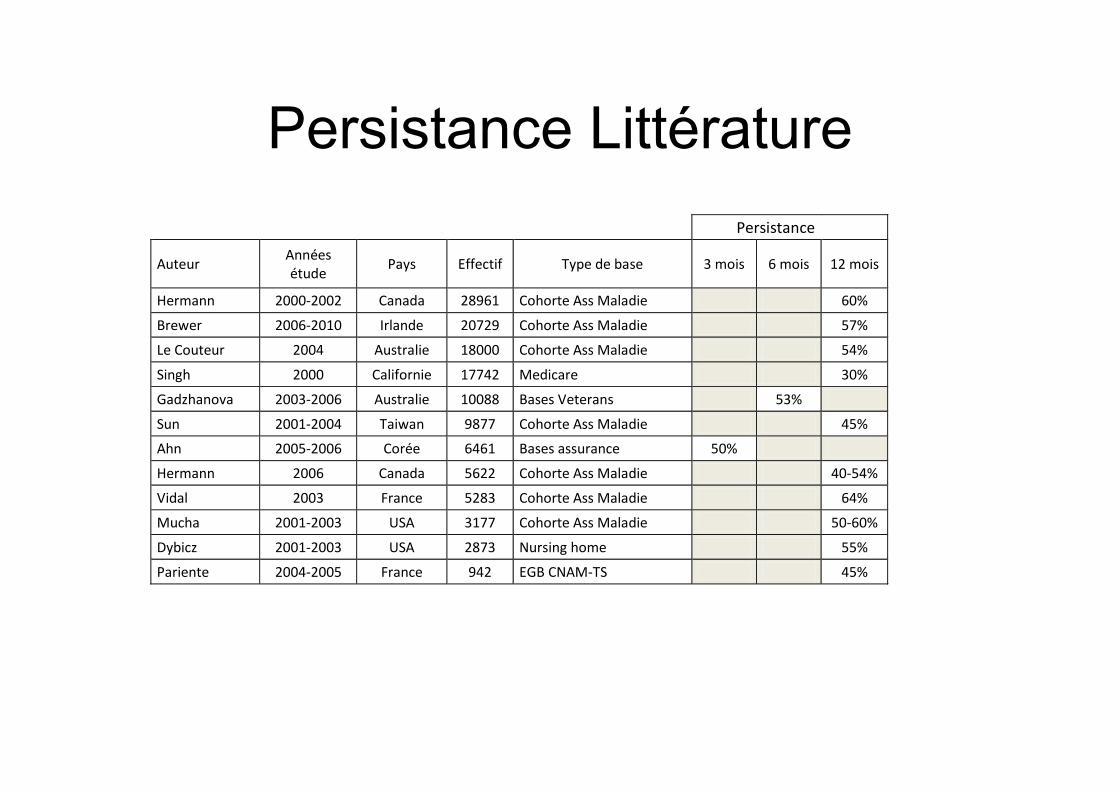
Persistance Littérature Persistance
Auteur Annéesétude Pays Effectif Typedebase 3mois 6mois 12mois
Hermann 2000-2002 Canada 28961 CohorteAssMaladie 60%
Brewer 2006-2010 Irlande 20729 CohorteAssMaladie 57%
LeCouteur 2004 Australie 18000 CohorteAssMaladie 54%
Singh 2000 Californie 17742 Medicare 30%
Gadzhanova 2003-2006 Australie 10088 BasesVeterans 53%
Sun 2001-2004 Taiwan 9877 CohorteAssMaladie 45%
Ahn 2005-2006 Corée 6461 Basesassurance 50%
Hermann 2006 Canada 5622 CohorteAssMaladie 40-54%
Vidal 2003 France 5283 CohorteAssMaladie 64%
Mucha 2001-2003 USA 3177 CohorteAssMaladie 50-60%
Dybicz 2001-2003 USA 2873 Nursinghome 55%
Pariente 2004-2005 France 942 EGBCNAM-TS 45%
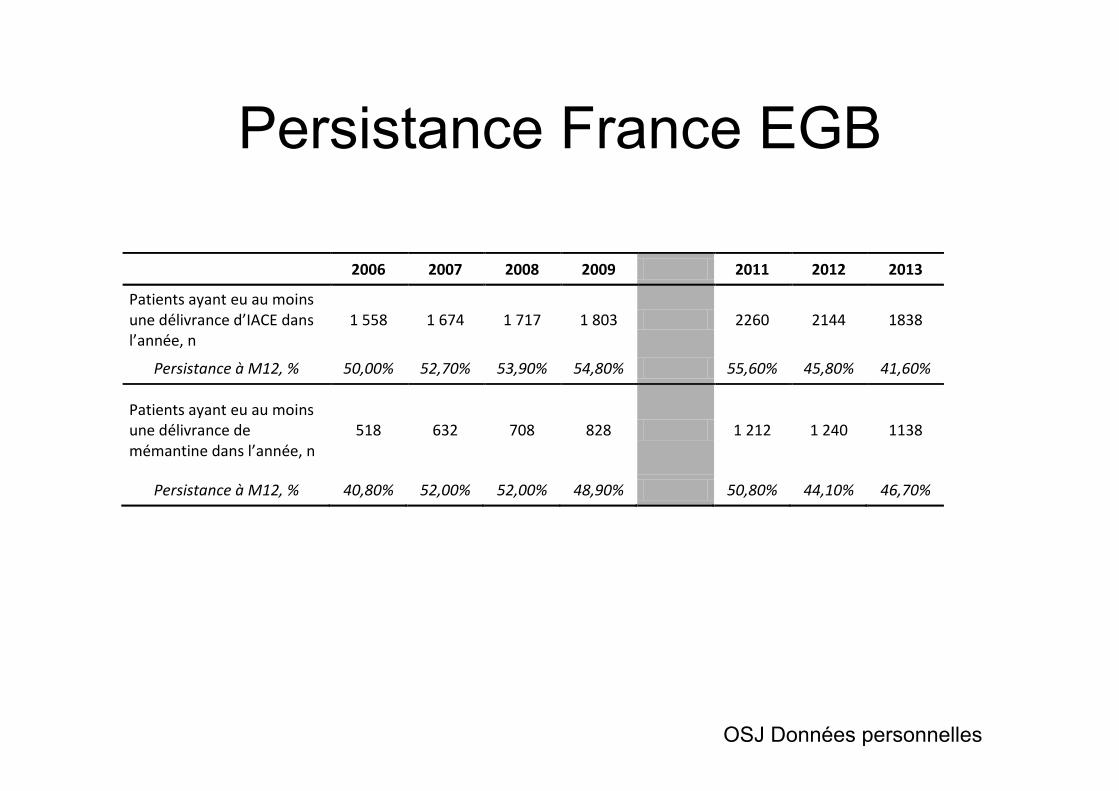
Persistance France EGB
2006 2007 2008 2009 2011 2012 2013
Patientsayanteuaumoinsunedélivranced’IACEdansl’année,n
1558 1674 1717 1803 2260 2144 1838
PersistanceàM12,% 50,00% 52,70% 53,90% 54,80% 55,60% 45,80% 41,60%
Patientsayanteuaumoinsunedélivrancedemémantinedansl’année,n
518 632 708 828 1212 1240 1138
PersistanceàM12,% 40,80% 52,00% 52,00% 48,90% 50,80% 44,10% 46,70%
OSJ Données personnelles
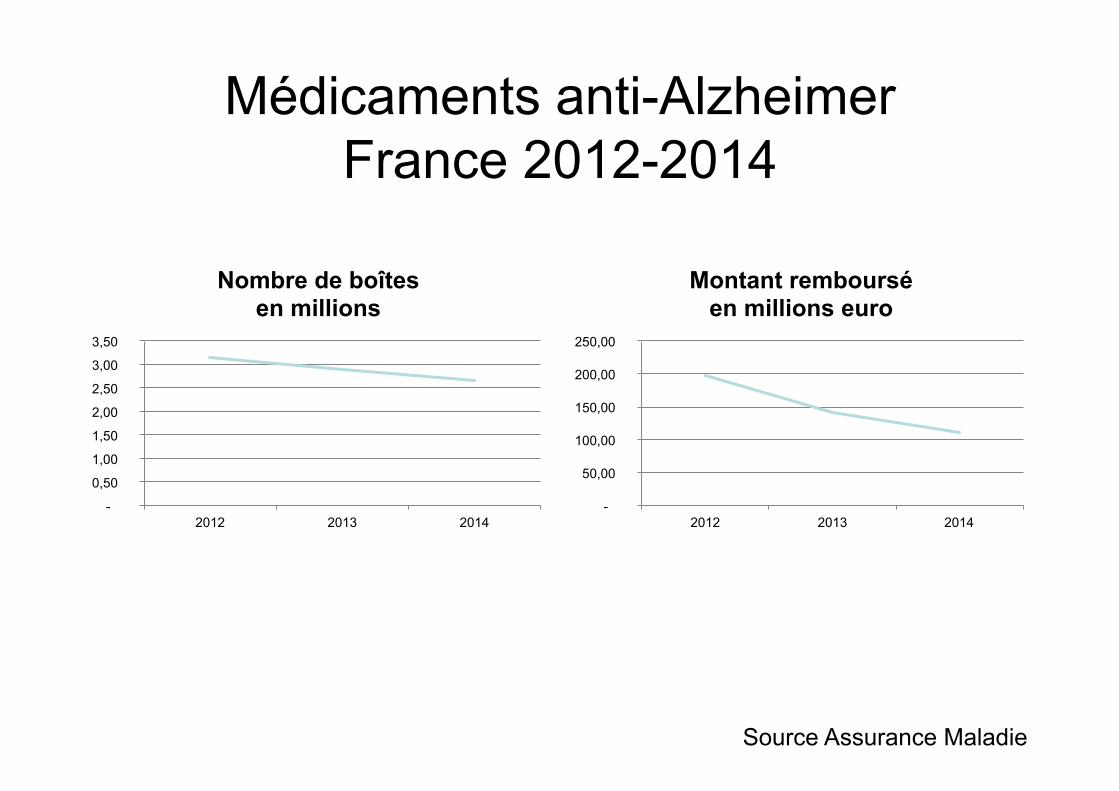
Médicaments anti-Alzheimer France 2012-2014
Source Assurance Maladie
-
0,50
1,00
1,50
2,00
2,50
3,00
3,50
2012 2013 2014
Nombre de boîtes en millions
-
50,00
100,00
150,00
200,00
250,00
2012 2013 2014
Montant remboursé en millions euro
La question de la tolérance
Quelle tolérance à court terme dans les essais publiés ?
• Effets « mineurs », dose- dépendants dans les essais à 6 mois * – Troubles digestifs – Cauchemars, céphalées, rhinorrhée, crampes musculaires
• Mortalité dans la maladie d’Alzheimer – ns à 6 mois – ns à plus long terme (12 mois et plus)
• Nordic, Donepezil 10 mg/j • AD 2000, Donepezil 5 et 10 mg/j
* Birks J. Cholinesterase inhibitors for Alzheimer’s disease. Cochrane Database of Systematic Reviews 2006, Issue 1. Art. No.: CD005593. DOI: 10.1002/14651858.CD005593.
Galantamine et mortalité (AFSSAPS 2004)
• Pour évaluer l’impact de la galantamine sur le délai d’apparition de la démence, deux essais cliniques versus placebo ont été réalisés chez 2048 patients souffrant d’altération modérée de la fonction cognitive.
• La galantamine n’a pas allongé le délai de survenue de la démence, par rapport au placebo mais l’analyse préliminaire montre une fréquence plus élevée de décès dans le groupe traité par galantamine (15 décès) par rapport au groupe placebo (5 décès). La cause des décès est variable mais souvent de nature cardiovasculaire. L’AFSSAPS et les autres états membres européens procèdent à une réévaluation du médicament.
• L’AFSSAPS : – rappelle que Réminyl* n’est pas indiqué chez les patients atteints d’altération
modérée de leurs fonctions cognitives (en particulier de la mémoire) – recommande le respect strict de l’indication autorisée, à savoir le « traitement
symptomatique de la maladie d’Alzheimer dans ses formes légères à modérément sévères ».
Syncope et IACE dans une population de sujets atteints de déclin cognitif
• Etude de cohorte en population en Ontario (Canada) • 19 803 patients déments sous IACE vs 61 499 sujets
contrôles • Validation de la comparabilité des deux groupes
(comorbidité, tt cardiovasculaire, port de PM, score de Charlson, etc…)
• Etude des incidents cardiovasculaires et fractures du col fémoral
Gill S et al Arch Int Med 2009;169:867-873
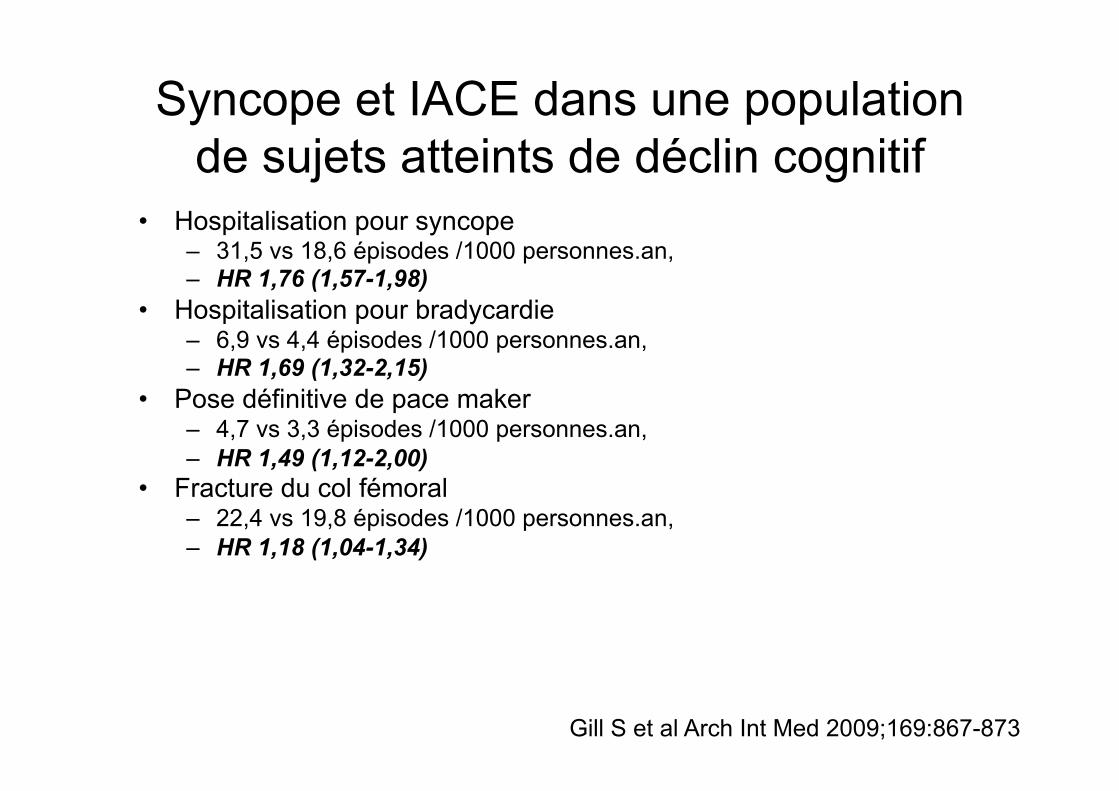
Syncope et IACE dans une population de sujets atteints de déclin cognitif
• Hospitalisation pour syncope – 31,5 vs 18,6 épisodes /1000 personnes.an, – HR 1,76 (1,57-1,98)
• Hospitalisation pour bradycardie – 6,9 vs 4,4 épisodes /1000 personnes.an, – HR 1,69 (1,32-2,15)
• Pose définitive de pace maker – 4,7 vs 3,3 épisodes /1000 personnes.an, – HR 1,49 (1,12-2,00)
• Fracture du col fémoral – 22,4 vs 19,8 épisodes /1000 personnes.an, – HR 1,18 (1,04-1,34)
Gill S et al Arch Int Med 2009;169:867-873
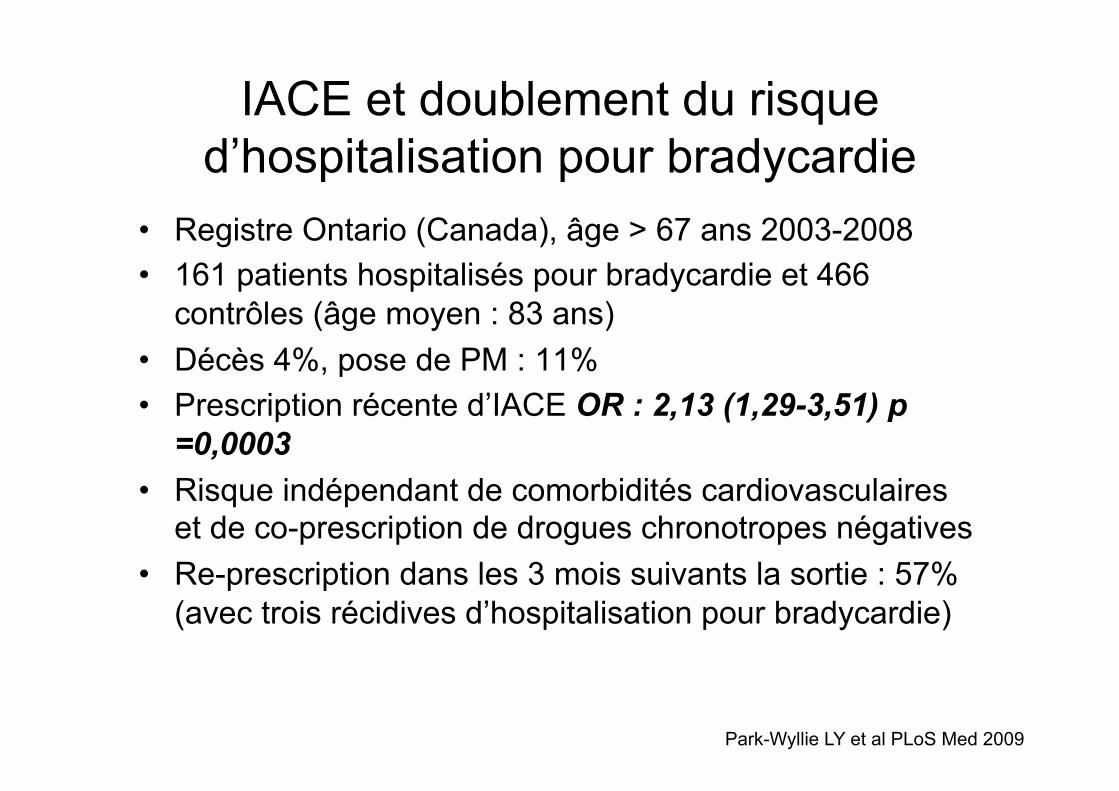
IACE et doublement du risque d’hospitalisation pour bradycardie
• Registre Ontario (Canada), âge > 67 ans 2003-2008 • 161 patients hospitalisés pour bradycardie et 466
contrôles (âge moyen : 83 ans) • Décès 4%, pose de PM : 11% • Prescription récente d’IACE OR : 2,13 (1,29-3,51) p
=0,0003 • Risque indépendant de comorbidités cardiovasculaires
et de co-prescription de drogues chronotropes négatives • Re-prescription dans les 3 mois suivants la sortie : 57%
(avec trois récidives d’hospitalisation pour bradycardie)
Park-Wyllie LY et al PLoS Med 2009
L’effet structurant
Existe-t-il des prestations liées à la prescription ? La prescription change-t-elle le parcours ?
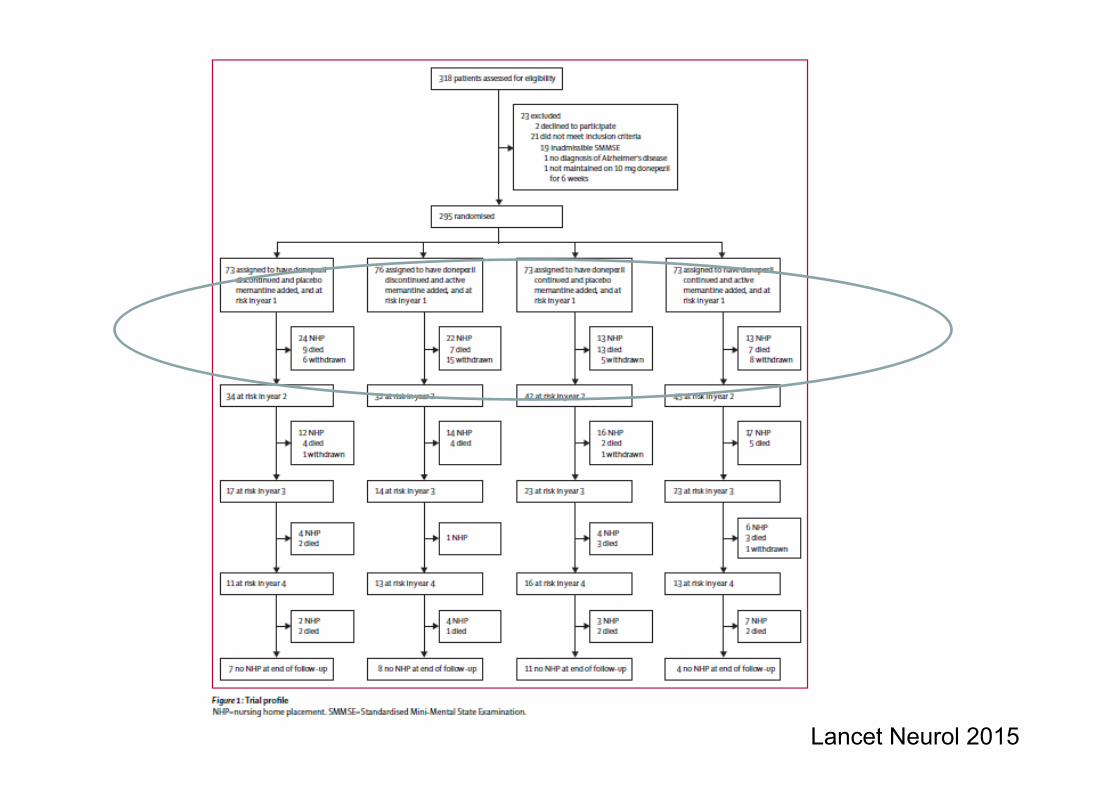
Lancet Neurol 2015
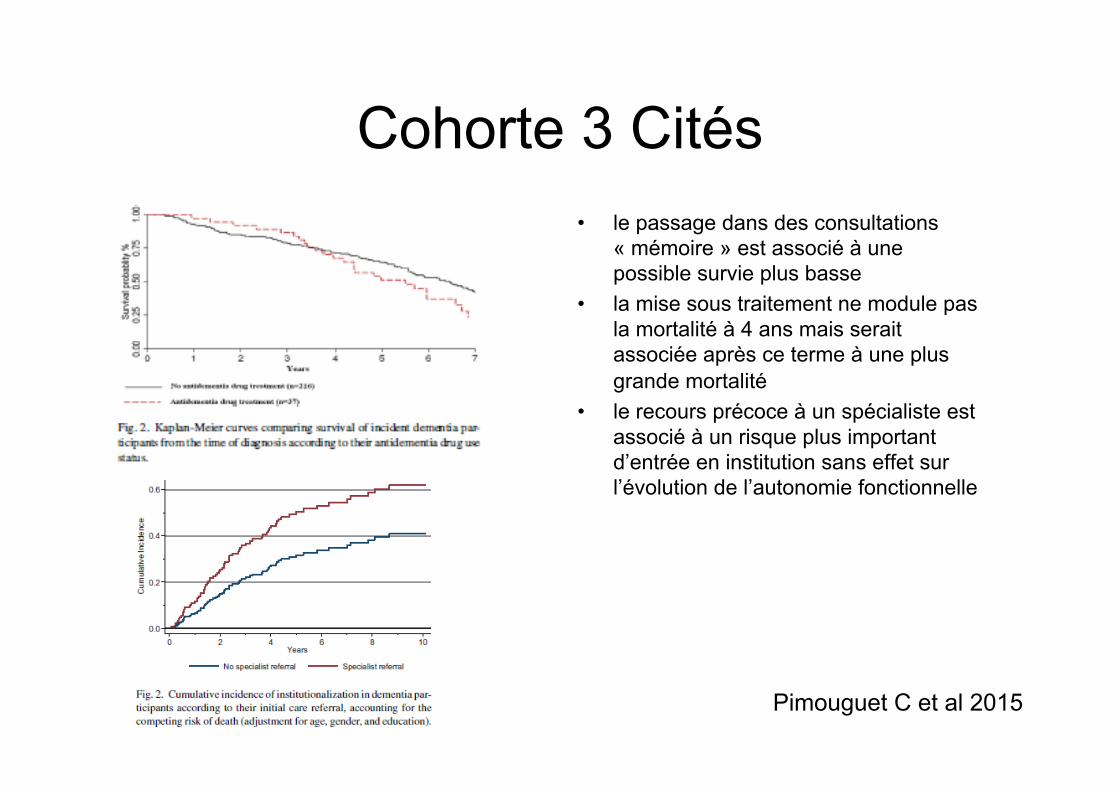
Cohorte 3 Cités • le passage dans des consultations
« mémoire » est associé à une possible survie plus basse
• la mise sous traitement ne module pas la mortalité à 4 ans mais serait associée après ce terme à une plus grande mortalité
• le recours précoce à un spécialiste est associé à un risque plus important d’entrée en institution sans effet sur l’évolution de l’autonomie fonctionnelle
Pimouguet C et al 2015
L’avenir est sombre
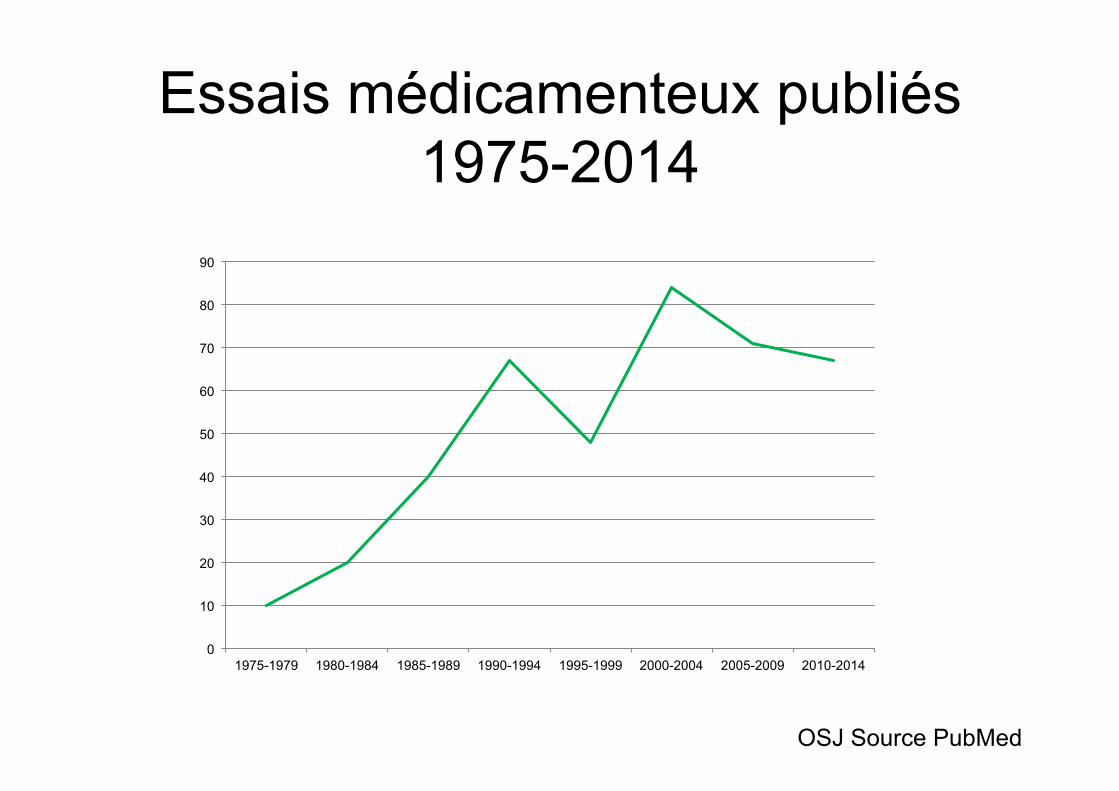
Essais médicamenteux publiés 1975-2014
0
10
20
30
40
50
60
70
80
90
1975-1979 1980-1984 1985-1989 1990-1994 1995-1999 2000-2004 2005-2009 2010-2014
OSJ Source PubMed
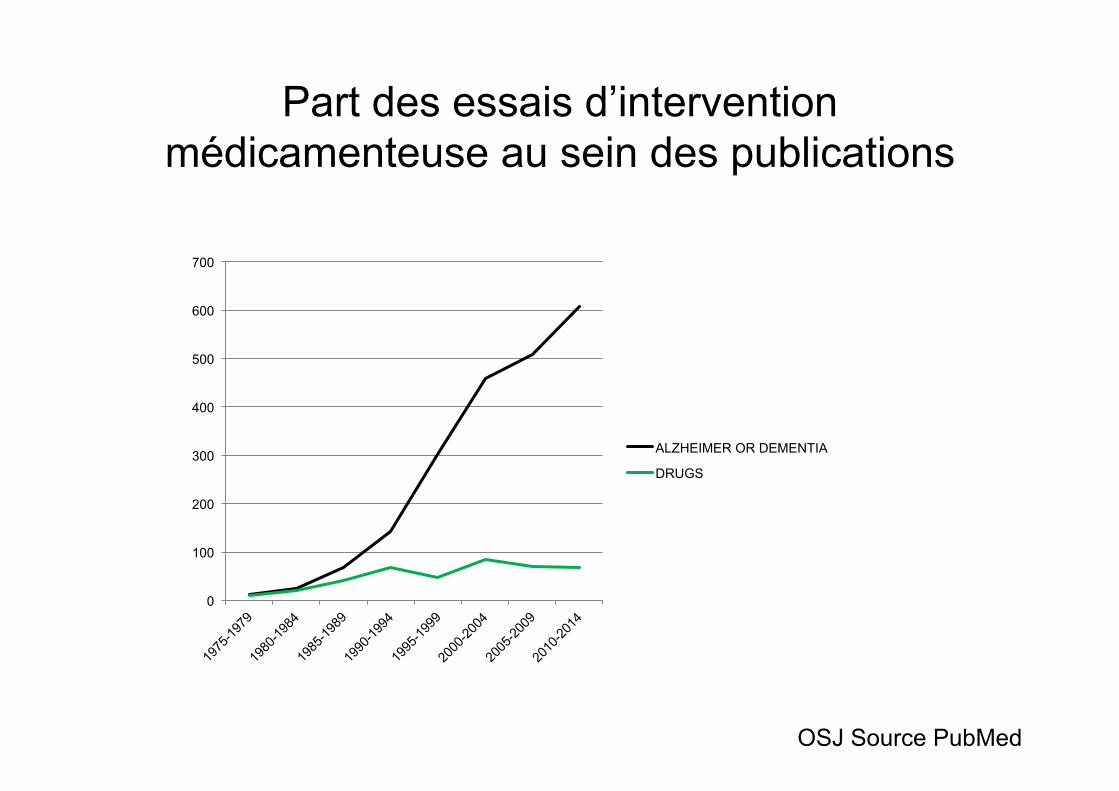
Part des essais d’intervention médicamenteuse au sein des publications
0
100
200
300
400
500
600
700
ALZHEIMER OR DEMENTIA
DRUGS
OSJ Source PubMed
Les anti-corps monoclonaux • Dirigés contre les composants de la plaque amyloïde • Deux publications récentes négatives (NEJM en
02/2014) – Bapineuzumab
• Reconnaît la partie intact N-terminale du peptide Abêta – Solanezumab
• Reconnaît Abêta soluble
• Débat sur le rôle de variations des marqueurs biologiques
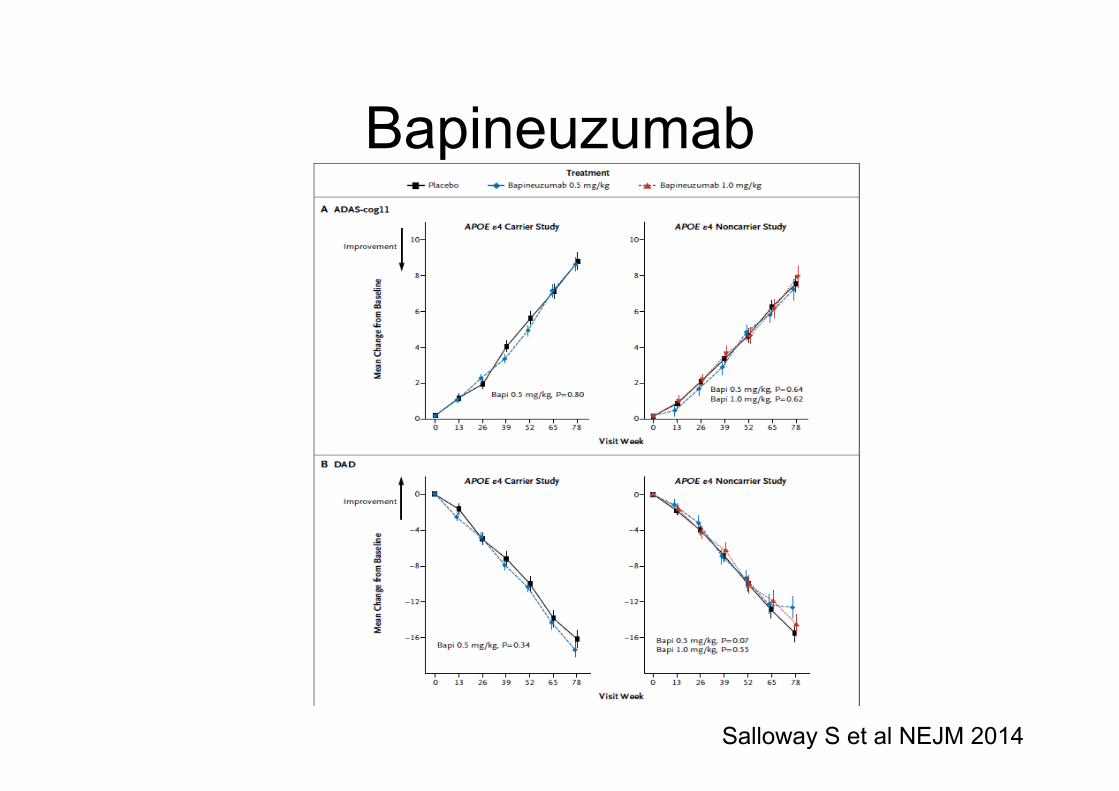
Bapineuzumab
Salloway S et al NEJM 2014
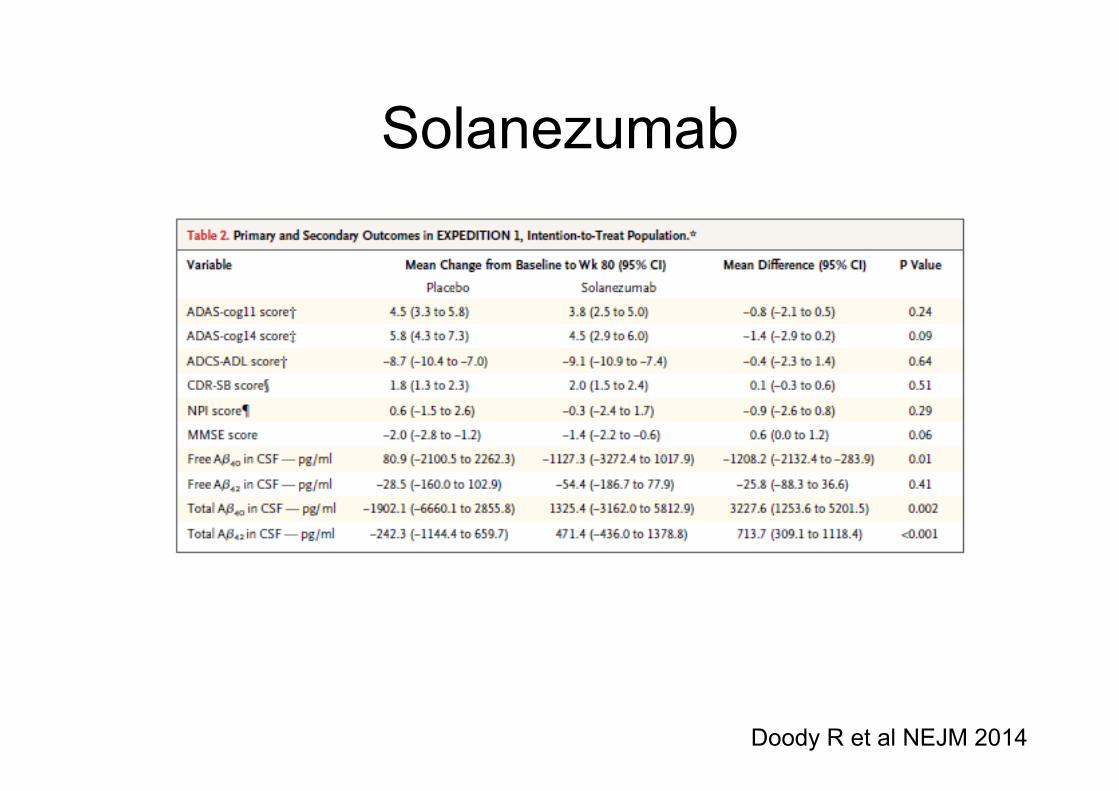
Solanezumab
Doody R et al NEJM 2014
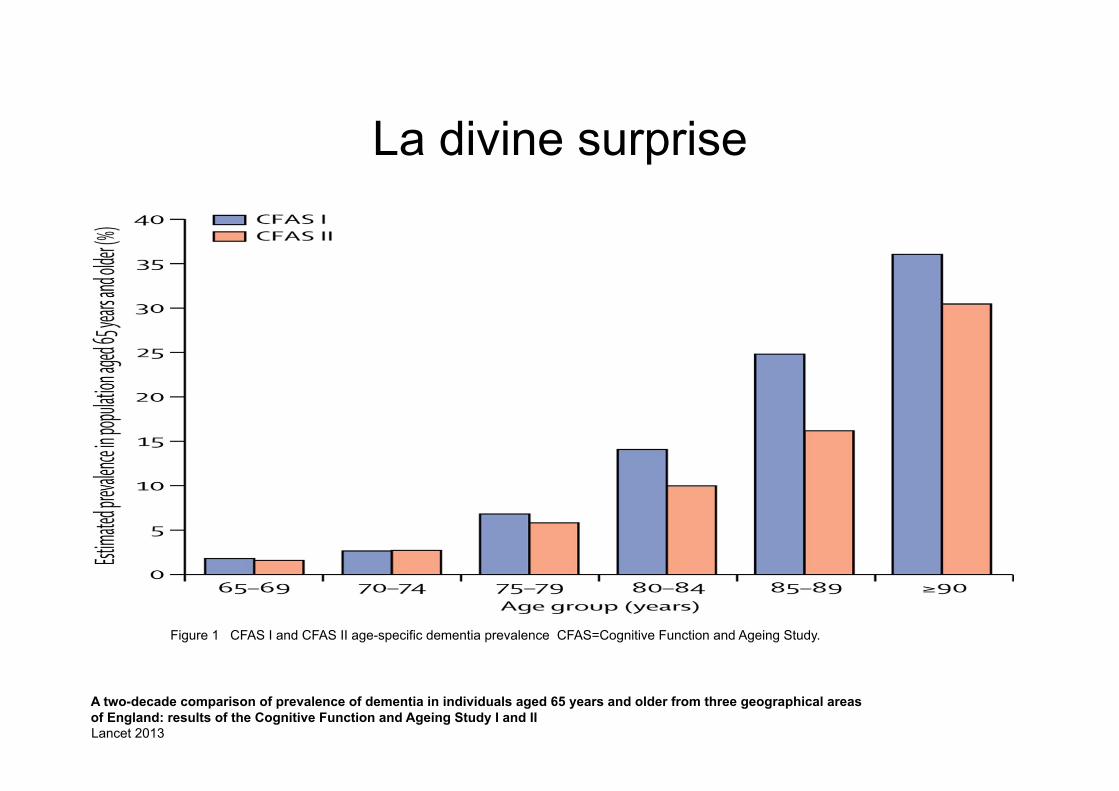
Figure 1 CFAS I and CFAS II age-specific dementia prevalence CFAS=Cognitive Function and Ageing Study.
A two-decade comparison of prevalence of dementia in individuals aged 65 years and older from three geographical areas of England: results of the Cognitive Function and Ageing Study I and II
La divine surprise
Lancet 2013
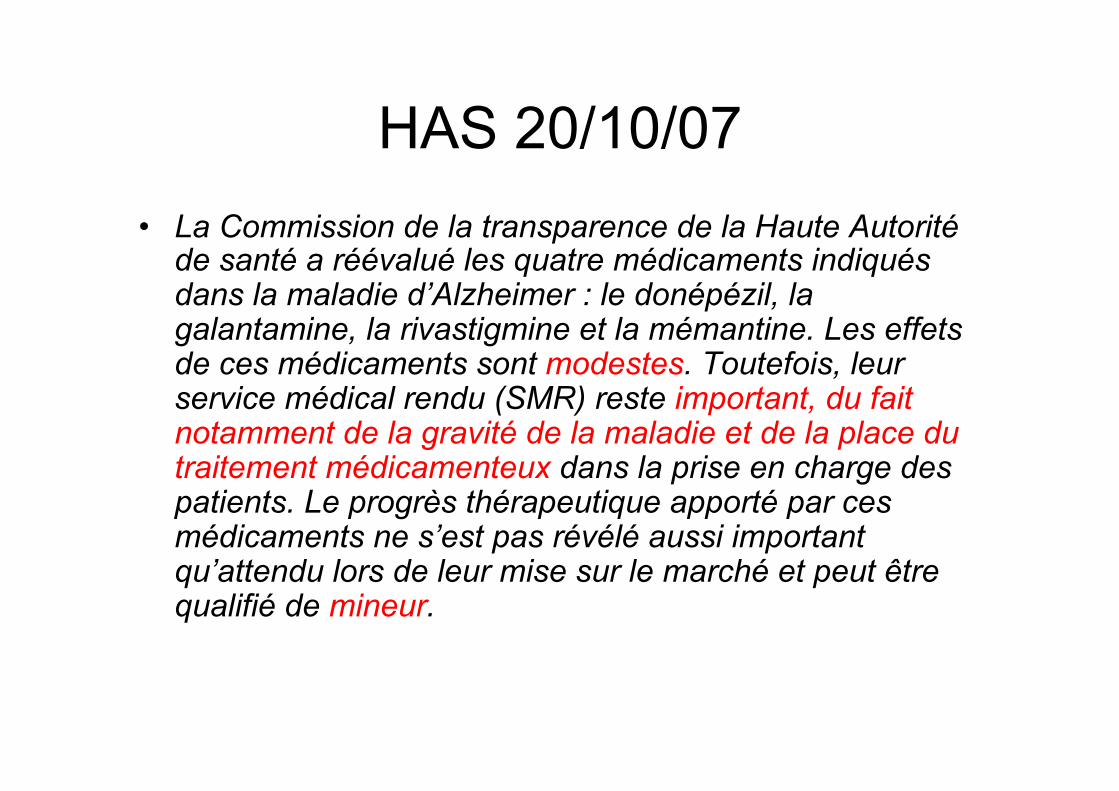
HAS 20/10/07 • La Commission de la transparence de la Haute Autorité
de santé a réévalué les quatre médicaments indiqués dans la maladie d’Alzheimer : le donépézil, la galantamine, la rivastigmine et la mémantine. Les effets de ces médicaments sont modestes. Toutefois, leur service médical rendu (SMR) reste important, du fait notamment de la gravité de la maladie et de la place du traitement médicamenteux dans la prise en charge des patients. Le progrès thérapeutique apporté par ces médicaments ne s’est pas révélé aussi important qu’attendu lors de leur mise sur le marché et peut être qualifié de mineur.
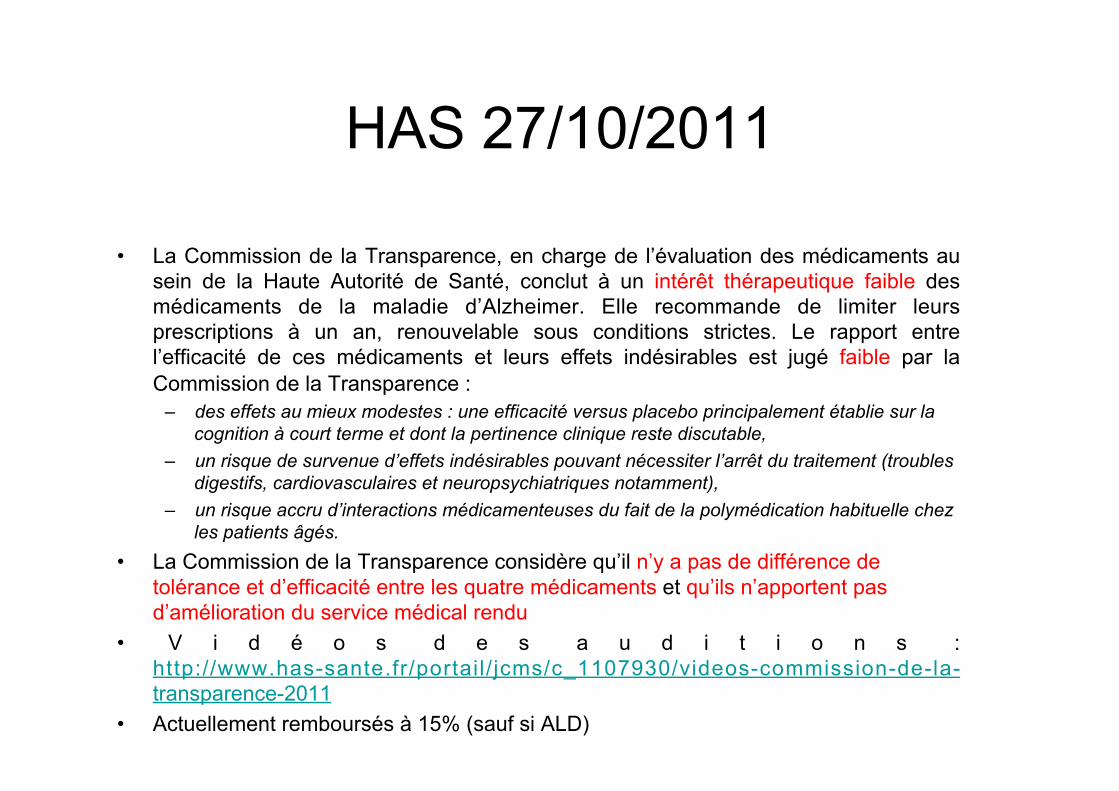
HAS 27/10/2011
• La Commission de la Transparence, en charge de l’évaluation des médicaments au sein de la Haute Autorité de Santé, conclut à un intérêt thérapeutique faible des médicaments de la maladie d’Alzheimer. Elle recommande de limiter leurs prescriptions à un an, renouvelable sous conditions strictes. Le rapport entre l’efficacité de ces médicaments et leurs effets indésirables est jugé faible par la Commission de la Transparence :
– des effets au mieux modestes : une efficacité versus placebo principalement établie sur la cognition à court terme et dont la pertinence clinique reste discutable,
– un risque de survenue d’effets indésirables pouvant nécessiter l’arrêt du traitement (troubles digestifs, cardiovasculaires et neuropsychiatriques notamment),
– un risque accru d’interactions médicamenteuses du fait de la polymédication habituelle chez les patients âgés.
• La Commission de la Transparence considère qu’il n’y a pas de différence de tolérance et d’efficacité entre les quatre médicaments et qu’ils n’apportent pas d’amélioration du service médical rendu
• V i d é o s d e s a u d i t i o n s : http://www.has-sante.fr/portail/ jcms/c_1107930/videos-commission-de-la-transparence-2011
• Actuellement remboursés à 15% (sauf si ALD)
HAS 19/10/2016 • La Commission de la Transparence conclut à un service médical rendu insuffisant
pour justifier leur remboursement. • Une efficacité au mieux modeste, un risque de survenue d’effets indésirables
– Les données nouvelles confirment que l’efficacité des médicaments du traitement symptomatique de la maladie d’Alzheimer est, au mieux, modeste. Elle est établie uniquement à court terme, essentiellement sur les troubles cognitifs, dans des études cliniques versus placebo dont la pertinence clinique et la transposabilité en vie réelle ne sont pas assurées. Les patients de ces études sont en effet plus jeunes que ceux qui sont pris en charge en pratique réelle, et contrairement à ceux-ci ne présentent ni comorbidités, ni risques d’interactions médicamenteuses. De surcroit, les effets sur les troubles du comportement, la qualité de vie, le délai d’entrée en institution, la mortalité, la charge de la maladie pour les aidants ne sont toujours pas établis.
– Il n’est pas possible de vérifier si les conditions d’utilisation des médicaments, telles que définies par la Commission de la Transparence en 2011 (réévaluation attentive de la prescription à six mois, décision en réunion de concertation pluridisciplinaire au-delà d’un an) ont été mises en œuvre. Or, les données accumulées depuis la commercialisation des médicaments confirment le risque de survenue d’effets indésirables (troubles digestifs, cardiovasculaires ou neuropsychiatriques pour les plus notables) potentiellement graves, pouvant altérer la qualité de vie. En outre, dans une population âgée, souvent polypathologique et polymédiquée, il existe un risque supplémentaire d’effets indésirables graves du fait d’interactions médicamenteuses.
• Au regard de l’absence de pertinence clinique de l’efficacité de ces médicaments et des risques de survenue d’effets indésirables, la HAS considère donc que ces médicaments n’ont plus de place dans la stratégie thérapeutique
Recommended

















