Embed Size (px)
Citation preview

Hum. Genet. 53, 111-112 (1979)
© by Springer-Verlag 1979
A New Translocation in Burkitt's Tumor Cells
R. Berger ~*, A. Bernheim ~, H.-J. Weh I, G. F l andr in 2, Marie-Th6r~se Daniel 2, J.-C. Brouet 3, and N. Colbert 4
Laboratoire de Cytog6n6tique, Institut de Recherche sur les Leuc6mies et les Maladies du Sang, U.E.R. d'H6matologie, H6pital Saint-Louis, 2 place du Dr. Fournier, 75475 Paris Cedex 10, France
2 Laboratoire d'H6matologie, U. E. R. d'H6matologie, H6pital Saint-Louis, Paris 3 Unit6 d'Immunochimie et d'Immunopathologie, U 108 INSERM, U.E.R. d'H6matologie, H6pital Saint-Louis, Paris 4 Clinique des Maladies du Sang, U. E.R. d'H6matologie, H6pital Saint-Louis, Paris
Summary. A t(8;22)(q24;q11) t ranslocat ion was found in blood, bone marrow, and ascites cells from a European Burkit t ' s lymphoma. Cell surface markers were identified as monoc lona l IgG. The relationship between these two unusua l findings is quest ionable in this cytologically typical Burki t t ' s lymphoma.
A t(8;14) t ranslocat ion was consistently found in Burkit t ' s l ymphoma cells by Zech et al. (1976). The same t ranslocat ion has been observed in Burkit t ' s type
of acute lymphocytic leukemia (ALL) (Berger et al,, 1979). Here we report a new translocat ion in a European Burki t t ' s lymphoma.
C a s e R e p o r t
The patient, a 65-year-old man, was admitted to the hospital on the February 25, 1979 with an ascitis which had appeared the previous week and edema in both legs.
Born in Turkey, he arrived in France in 1951 and had lived here ever since. Clinical examination showed only mild rector- raghia and no tumor was clinically detectable. No satisfactory X-rays of the abdomen could be obtained. The ascites fluid contained 25,000 red cells/ram 3 and 60,000 white cells/mm 3, most of them being blast cells. In the peripheral blood, the white cell count was 23,000 including 30% hemoblasts, 7% myelo- cytes, and 2% metamyelocytes. The bone marrow contained 90% blast cells and meningeal fluid red cells, and 16 white cells/ mm 3 including blast cells.
Table 1. Chromosome studies. No. of metaphases
No, of chromosomes Without structural abnormalities
44 45 46
With structural abnormalities
t(8;22) t(8;22), t(ll;19) 6q+
44 45 46 46 46
No. total mitoses
Ascites (direct)
Ascites (24h culture)
Bone marrow 24 h culture
48 h culture
Blood
72h - PHA
72h + PHA
2" 2 a 16
18
3 a 35
1 37"
1 27 1 37
2 a 7 1 11
2 a 5 a 15 3 45
10 28
7 ~ 29 76
8 1 47
Random loss
* To whom offprint requests should be sent
0340-6717/79/0053/0111/$ 01.00

112 R. Berger et al.: New Translocation in Burkitt's Lymphoma
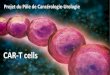
Fig. 1. Translocation t(8;22)(q24;q11). (R-bands)
All the blast cells were identical: their cytoplasm was uni- formely and intensively deeply basophilic and lacking in granules. Empty cytoplasmic vacuoles were present in most of them. The nuclei were round and large with a finely clumped chromatin. These cytological characteristics are typical of Burkitt's tumor cells.
Tumor cell surface markers were studied on the ascites cells. Cells from the ascitic fluid were washed three times and analyzed by means of direct immunofluorescence with antisera to /z, 7, a, c~, 1¢, and 2 chains as described previously (Preud'homme and Seligmann, 1972). Binding of immune com- plexes (goat antibodies to rabbit IgG-rabbit IgG) was used to detect the presence of an IgG Fc receptor.
In direct immunofluorescence, only ~ and 2 chains were detected. There was no binding of immune complexes to the cell surface and Fc receptors were therefore concluded to be absent.
A diagnosis of Burkitt's tumor with ALL was made and treatment (rubidazone and vincaleucoblastine) was started. However, the patient died suddenly on March 3, 1979. An autopsy could not be performed.
Cytogenetic studies were performed on ascites, blood (unstimulated and PHA-stimulated cultures), and bone marrow cells. RHG-, CBG-, and GTG-banding was used. The con- stitutional karyotype was normal male with a variant chromo- some 22 (22p+). Three kinds of karyotype were found (Table 1): normal; 46,XY, t(8q22)(q24;qll) (Fig. 1) and 46,XY, t(1;6)(q21; qter),t(8;22)(q24;ql 1).
Discussion
The case reported here was classified as a Burkit t ' s lymphoma with ALL, based on the morphological appearance and the monoclona l B-cell origin of the
blast cells (F landr in et al., 1975).
Two unusua l features whose relationships is un- clear were observed. In our experience, Burkit t ' s tumor cells only rarely synthesize IgG molecules (2 out
of 24 cases, unpubl i shed data). The other pat ient with IgG-producing cells was a young male with an abdomina l lymphoma. In African Burkit t ' s disease, almost all cases have surface IgM-positive cells.
The t(8;14) t ranslocat ion identical to that of Bur- kitt 's t umor cells was present in six personal cases of Burkit t 's type of ALL. In this case t(8;22), t ranslocat ion was present with a Ph l-like chromosome. However, the rearrangement involved the same band region on the chromosome 8q as the other cases. The question thus arises of whether the rearrangement of 8q is equally as impor tan t as that of 14q in this disease. If so, other
variant t ranslocat ions involving 8q may be found either in Burkit t ' s t umor cells or in blasts cells. An analogy can be made with the Phi chromosomal variants in chronic granulocytic leukemia. The 22q is often partially translocated onto a chromosome other than 9 in these cases.
Acknowledgments. We sincerely acknowledge the excellent tech- nical assistance of Mrs. M. Le Coniat and Miss D. Vecchione.
References
Berger, R., Bernheim, A., Flandrin, G., Daniel, M. T., Schaison, G., Brouet, J. C., Bernard, J.: Translocation t(8;14) dans la leuc6mie lymphoblastique de type Burkitt. Nouv. Presse M~d. 8, 181--183 (1979)
Flandrin, G., Brouet, J. C., Daniel, M. T., Preud'homme, J. L.: Acute leukemia with Burkitt's tumor ceils: A study of six cases with special reference to lymphocyte surface markers. Blood 45, 89--188 (1975)
Preud'homme, J. L., Seligmann, M.: Immunoglobulins on the surface of lymphoid cells in Waldenstr6m's macroglobulin- emia. J. Clin. Invest. 51, 701--705 (1972)
Zech, L., Haglund, U., Nilsson, K., Klein, G.: Characteristic chromosomal abnormalities in biopsies and lymphoid cell lines from patients with Burkitt and non-Burkitt lymphomas. Int. J. Cancer 17, 45--56 (1976)
Received June 15, 1979









![novembre 2013 [Mode de compatibilité] Weinstein D.C. and Aaronson S.A. β-Catenin-Independent Activation of TCF1/LEF1 in Human Hematopoietic Tumor Cells through Interaction with ATF2](https://img.pdfslide.fr/doc/110x75/5f097d827e708231d42712f9/novembre-2013-mode-de-compatibilit-weinstein-dc-and-aaronson-sa-catenin-independent.jpg)