Embed Size (px)
Citation preview

Accepted Manuscript
Assessment of two contact activation reagents for the diagnosis ofcongenital factor XI deficiency
Salam Salloum-Asfar, María E. de la Morena-Barrio, JulioEsteban, Antonia Miñano, Cristina Aroca, Vicente Vicente,Vanessa Roldán, Javier Corral
PII: S0049-3848(17)30627-8DOI: https://doi.org/10.1016/j.thromres.2017.12.023Reference: TR 6877
To appear in: Thrombosis Research
Received date: 5 October 2017Revised date: 14 December 2017Accepted date: 29 December 2017
Please cite this article as: Salam Salloum-Asfar, María E. de la Morena-Barrio, JulioEsteban, Antonia Miñano, Cristina Aroca, Vicente Vicente, Vanessa Roldán, Javier Corral, Assessment of two contact activation reagents for the diagnosis of congenital factorXI deficiency. The address for the corresponding author was captured as affiliation forall authors. Please check if appropriate. Tr(2017), https://doi.org/10.1016/j.thromres.2017.12.023
This is a PDF file of an unedited manuscript that has been accepted for publication. Asa service to our customers we are providing this early version of the manuscript. Themanuscript will undergo copyediting, typesetting, and review of the resulting proof beforeit is published in its final form. Please note that during the production process errors maybe discovered which could affect the content, and all legal disclaimers that apply to thejournal pertain.

ACC
EPTE
D M
ANU
SCR
IPT
Assessment of two contact activation reagents for the diagnosis of congenital Factor XI
deficiency
Salam Salloum-Asfar1, María E. de la Morena-Barrio1, Julio Esteban2, Antonia Miñano1, Cristina
Aroca1, Vicente Vicente1, Vanessa Roldán1 and Javier Corral1*.
1Servicio de Hematología y Oncología Médica, Hospital Universitario Morales Meseguer,
Centro Regional de Hemodonación, Universidad de Murcia, IMIB-Arrixaca, CIBERER, Murcia.
Spain.
2Servicio de Hematología. Hospital Virgen del Castillo de Yecla, Murcia, Spain.
*Contact information for correspondence
Dr. Javier Corral University of Murcia Centro Regional de Hemodonación Calle Ronda de Garay s/n Murcia 30003, Spain Tel: +34968341990/ Fax: +34968261914 E-mail: [email protected]
Keywords: FXI deficiency, APTT, silica, ellagic acid, FXI:C, rs1801020.
Highlights
Moderate FXI deficiency might be underestimated by current diagnostic methods.
The sensitivity of two contact activators is evaluatedin140 FXI deficiencycases.
APTT is a low sensitive method for the screening of FXI deficiency.
APTT is strongly dependent on the type of activator and both FXI and FXII levels.
The best screening method forFXI deficiency is FXI:C using silica.
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
Abstract
Introduction. Congenital FXI deficiency, a coagulopathy associated with low bleeding risk but
thrombotic protection, is usually diagnosed by prolonged APTT and confirmed by coagulation
assays. Recent evidences suggest that FXI deficiency might be underestimated. Sensitive and
reliable methods to detect FXI deficiency are required. Aim. To examine the sensitivity of two
methods and two contact activators on FXI deficiency screening. Methods. 140 cases with FXI
deficiency, 9 severe and 131 moderate, caused by 11different mutations were recruited. APTT
and FXI:C were assessed in ACL-TOP 500coagulometer with silica-based (SynthASil) and ellagic
acid-based (SynthAFax) reagents. F12 rs1801020 SNP was genotyped with Taqman probes.
Results. Severe FXI deficiency significantly prolonged APTT with both reagents. However, a
high proportion of moderate deficiencies would not be detected using APTT, with false
negatives of 22% for SynthASil and 12% for SynthAFax. False negatives results mainly
corresponded to cases with qualitative deficiency (CRM+: p.Pro538Leu), which also had higher
FXI coagulant activity. Using SynthASil, the common F12 rs1801020 variant, associated to low
FXII levels, significantly prolonged APTT in moderate FXI deficiency subjects. FXI:C values were
significantly higher with SynthAFax than with SynthASil (47.7±12.7 vs. 40.4±14.9), so SynthAFax
rendered higher rate of false negatives than SynthASil (7% vs.2%). Conclusions. Moderate FXI
deficiency, particularly CRM+, might be underestimated using current diagnostic methods. The
activator, FXI and FXII levels may contribute to a higher rate of false negatives using APTT. Our
results suggests that the best screening method for FXI deficiency is FXI:C using silica.
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
Introduction
Activated partial thromboplastin time (APTT) is a global coagulation test that has been used
during the last 50 years as a standard screening test in clinical laboratories throughout the
world [1]. APTT levels are considered to reflect global coagulation activity. This test
cumulatively explores factors belonging to the classic intrinsic (FXII, FXI, FIX, and FVIII) or
common (FII, FV and fibrinogen) coagulation cascade. Factor XII is a known determinant of
APTT. Polymorphism rs1801020, which has been associated with FXII levels, showed a highly
significant association with APTT in normal population and case-control cohort of thrombosis
[2, 3]. Besides its sensitivity toward variation levels of these coagulation factors, APTT is also
associated with age, gender, estrogen therapy, and obesity [4].
Generally, coagulopathies involving deficiencies in the intrinsic pathway are evaluated widely
by APTT. Prolonged APTT is an indicator of deficiencies of factors involved the intrinsic
pathway [5, 6]. Numerous reagent systems for performing the APTT assay are commercially
available. However, when the deficiency is mild, these assays vary in their sensitivity to clotting
factor deficiencies.
FXI is a plasma serine protease zymogen of hepatic synthesis with a key role in bridging the
initiation phase and the amplification phase of blood coagulation in vivo [7, 8]. FXI deficiency
originally called haemophilia C, however yields mild bleeding tendency and, in turn, has
significant protective effects from thrombotic diseases [9-11]. FXI deficiency has been
considered a rare disorder and is usually diagnosed by prolonged APTT and confirmed by
coagulation assays (FXI:C<70%). Nevertheless, current reports suggest that this disorder is
present worldwide in many populations and may be underestimated [12-14].
Sensitive and reliable methods to detect FXI deficiency and quantify FXI levels are required. In
this study, using a large cohort of subjects with congenital FXI deficiency caused by 11 different
mutations, we evaluated two assays for their ability to detect deficiencies of FXI, particularly
mild deficiencies. Moreover, two commercially available contact activator reagents were
compared, one based on ellagic acid and one based on silica.
Materials and methods
Study subjects
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
The study included 140 subjects (77 male and 63 female donors varying in age from 5 to 88
years) from the Spanish Yecla-study [15], with congenital FXI deficiency characterized
biochemically, functionally and molecularly. Briefly, during 20 years, 324,764 APTT tests from
51,366 hospital in- patients/out-patients were screened, selecting 1,700 patients with an APTT
ratio>1.3 using SynthASil for further studies. Determination of FXI coagulation activity (FXI:C) in
173 patients with replicated and unexplained prolonged APTT (lupus, hepatopathy, and
anticoagulants were excluded) revealed 46 unrelated Caucasian cases with severe to moderate
FXI deficiency (<70% of the value obtained in the reference plasma). Family studies of 265
available relatives from index cases revealed 170 additional subjects with FXI:C deficiency
and/or F11 mutation. The 140 subjects selected for this study belonged to 42 families and
included 9 homozygous or compound heterozygous with severe FXI deficiency and 131
heterozygous with mild-moderate FXI deficiency. FXI deficiency was caused by 11 different
mutations (Table 1).
Table 1. Demographic, analytical and genetic characteristics of the 140 subjects with FXI
deficiency included in this study.
Mutation Ref Mut Type
N (fam)
Genetic Status (N) Age Sex M/F
c.1613C>T; p.Pro538Leu (CM051916)
[13] CRM+ 32 (1)
Homozygous (3) 71.6±5.1 3/0
Heterozygous (29) 34.4±13.7 13/16
c.166T>C; p.Cys56Arg (CM020681)
[16] CRM- 55 (23)
Homozygous &CH (4)
57±10.6 2/2
Heterozygous (51) 41.9±22.1 33/18
c.1247G>A; p.Cys416Tyr (CM053240)
[13] CRM- 18 (7) Heterozygous (18) 50.5±25 9/9
c.1693G>A (CM051917) [17] CRM- 19 (6) Heterozygous (19) 45.5±15.1 8/11
c.1796G>A; p.(Cys599Tyr). New
[15] CRM+ 3 (1) CH (2) 46±2.8 1/1
Heterozygous (1) 81 1/0
c.325G>A (CS081910) [13] CRM- 1 (1) Heterozygous (1) 61 1/0
c.1277T>C; p.(Ile426Thr). New [15] CRM- 4 (1) Heterozygous (4) 47.5±29.9 2/2
c.1608G>C; p.Lys536Asn (CM002953)
[18] CRM- 1 (1) Heterozygous (1) 74 0/1
c.965C>T; p.Thr322Ile (CM950373)
[17] CRM- 1 (1) Heterozygous (1) 44 1/0
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
c.802C>T; p.Arg268Cys (CM035499)
[13] CRM- 1 (1) Heterozygous (1) 71 0/1
Exon 8&9 duplication. New [15] CRM- 5(1) Heterozygous (5) 29.4±15.9 3/2
Ref: Reference. Mut Type: Mutation type. CRM-: cross-reacting material-negative. CRM+:
cross-reacting material-positive. M: male; F: female. CH: compound heterozygous
Blood Collection and Plasma Preparation
Blood was collected from the antecubital vein into non siliconized Vacutainer® tubes
containing 3.8% buffered sodium citrate (Becton-Dickinson, Rutherford, NJ). Plasma was
obtained within less than 2 hours after extraction was collected using by centrifugation at
2,500 g for 20 minutes. All plasma samples were aliquoted and stored at -80ºC.
All included subjects gave their informed consent to enter the study performed according to
the declaration of Helsinki, as amended in Edinburgh in 2000. The study was approved by the
Ethical Committee on human research of the Hospital Universitario Reina Sofia in Murcia,
Spain.
Clotting tests
The citrated plasma of all samples was thawed and analyzed the same day. The clotting tests
were performed immediately after thawed, under identical conditions and using the same
batch of reagents for all samples. APTT and FXI:C values were measured using automated ACL
TOP 500 coagulometer (Instrumentation Laboratory) by activating the contact phase with two
different reagents(both from HemosIL): 1) SynthASilTM (colloidal silica-based reagent) and 2)
SynthAFaxTM (ellagic acid-based reagent) using the manufacturer’s standards and calibrators
and following the manufacturer’s instructions. Both reagents used the same CaCl2
concentration (Table 2). For FXI:C clotting assays, FXI deficient plasma (also from HemosIL) was
used following the procedure indicated by the manufacturer.
For APTT, results were expressed either as the raw clotting time in seconds or as a normalized
ratio between the clotting time of the sample and the clotting time of a laboratory reference
standard. A prolonged APTT was considered when the ratio is > 1.3, the cut-off established in
our Hemostasis Unit. For FXI:C clotting activity, results were expressed as % of a laboratory
reference standard.
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
Table 2: Features of APTT reagents evaluated in this study
APTT Reagent SynthASil SynthAFax
Part Number and Size 0020006800 APTT reagent 5 x 10 mL 0.020M CaCl2 5 x 10 mL
0020007400 APTT reagent 5 x 10 mL 0.020M CaCl2 5 x 10 mL
Liquid or Lyophilized Liquid Liquid Activator Colloidal Silica Ellagic Acid Phospholipids Synthetic Synthetic Reconstituted Stability at 2-8°C APTT reagent 30 days
in original vial CaCl2 30 days in original vial
APTT reagent 30 days in original vial CaCl2 30 days in original vial
Normal Range * 25.4 - 38.4 seconds 19.7 - 27.6 seconds Heparin Sensitivity +++ ++ Factor Sensitivity +++ ++ Lupus Sensitivity ++ +
*Obtained on the ACL Family of instruments. Source: From HemosIL® - Instrumentation Laboratory- Providing the Right Solutions for Your APTT Testing.
Genetic studies
The polymorphism rs1801020 (c.-4C>T; g.5046C>T) that affects the Kozak sequence of F12 and
has significant functional effects on FXII levels[19] was genotyped by Taqman® probes.
Statistical analysis
Statistical analysis was performed using IBM Statistical Package for Social Sciences (SPSS 21.0;
New York, USA) software. In terms of the management of continuous variables, it was first
verified the normality of its distribution using the Kolmogorov-Smirnov. If the distribution of
data is normal, the majority in our study, is presented as mean ± standard deviation; and are
expressed as median (P25-P75), for non-normal continuous variables. To compare differences
of means among groups, analysis of variance (ANOVA) is used for parametric values, while for
non-parametric values; the U-Mann Whitney tests were applied. Differences resulting from
comparative tests are considered statistically significant when the value of the bilateral "p" is
less than 0.05.
Results
Overall results
Table 3 shows a summary of all the results of APTT and FXI:C obtained in FXI deficiency
patients analyzed by using two activators of the contact phase.
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
The silica-based reagent rendered significantly prolonged APTT times but lower APTT ratio
than the ellagic acid-based reagent (Table 3). FXI:C values were significantly lower when
determined with silica than when using ellagic acid.
Severe FXI deficiency (homozygous or compound heterozygous) largely prolonged APTT times
and increased APTT ratios with both silica- and ellagic acid-based reagents (Table 3). This was
also evident for the three homozygous for the CRM+ mutation p.Pro538Leu (Table 3).
The adjustment of the equipment did not allow quantification of FXI:C values in cases with
very severe FXI deficiency (p.Cys56Arg homozygous and compound heterozygous) when
activated by the ellagic acid-based reagent (Table 3).
Table 3.APTT and FXI:C results obtained in 140 patients with FXI deficiency after activation
with two different contact activators: SynthASil and SynthAFax.
FXI Deficiency (N)
APTT seconds (range) SynthASil SynthAFax
APTT ratio (range) SynthASil SynthAFax
FXI:C % (range) SynthASil SynthAFax
All (N= 140)
44.3±13.3 (29.4-115.9)
36.4±16.2 (26.7-132.6)
1.48±0.42 (0.98-3.86)
1.60±0.70 (1.18-5.84)
40.4±14.9 (0.4-73.1)
47.7±12.7 (12.0-83.3)
p < 0.01 < 0.01 < 0.01 Severe deficiency (N= 9)
84.0±25.1 (47.1-115.9)
87.8±34.3 (43.3-132.6)
2.80±0.83 (1.57-3.86)
3.86±1.50 (1.91-5.84)
4.5±5.7 (0.4-12.9)
17.9±1.8 (16.0-19.6)
p 0.86 0.08 0.11 p.Pro538Leu homozygous (N= 3)
52.1±5.3 (47.1-57.6)
46.7±5.2 (43.3-57.2)
1.73±0.17 (1.57-1.92)
2.05±0.22 (1.91-2.32)
12.0±1.3 (10.5-12.9)
17.9±1.8 (16-16.9)
p 0.11 0.11 0.10 Very severe deficiency* (N= 6)
99.9±8.9 (90.4-115.9)
108.3±18.6 (82.2-132.6)
3.33±0.29 (3.01-3.86)
4.77±0.82 (3.62-5.84)
0.7±0.4 (0.4-1.4)
ERROR
p 0.35 0.03 - All heterozygous (N= 131)
41.9±4.4 (29.4-55.1)
32.9±3.5 (26.7-44.7)
1.39±0.14 (0.98-1.84)
1.44±0.15 (1.18-1.97)
42.8±11.8 (11.4-73.1)
48.4±12.0 (12.0-83.3)
p < 0.01 < 0.01 < 0.01 p.Cys56Arg heterozygous (N= 51)
41.7±3.3 (35.2-51.1)
33.2±3.1 (27.1-42.9)
1.38±0.11 (1.17-1.70)
1.46±0.13 (1.19-1.89)
37.9±8.3 (19.7-65.5)
44.1±8.9 (18.3-71.0)
p < 0.01 0.03 0.04 p.Pro538Leu heterozygous (N= 29)
39.8±4.2 (29.4-52.4)
31.1±2.4 (27.6-37.1)
1.32±0.14 (0.98-1.75)
1.36±0.10 (1.22-1.63)
53.7±10.3 (31.7-73.1)
61.2±10.0 (44.0-83.3)
p < 0.01 0.01 < 0.01 c.1693G>A heterozygous (N= 19)
42.8±5.4 (36.9-55.1)
33.4±4.3 (26.7-42.3)
1.42±0.18 (1.23-1.84)
1.45±0.18 (1.18-1.86)
40.5±11.1 (22.0-70.9)
40.9±11.3 (12.0-70.2)
p < 0.01 0.15 0.04
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
p.Cys416Tyr heterozygous (N= 18)
43.6±5.2 (35.4-54.3)
34.5±4.6 (29.6-44.7)
1.45±0.17 (1.18-1.81)
1.52±0.20 (1.30-1.97)
42.6±12.0 (23.9-68.8)
46.7±9.8 (27.5-66.7)
p < 0.01 0.02 0.01
* p.Cys56Arg homozygous and compound heterozygous.
Heterozygous subjects with moderate FXI deficiency.
The results of carriers of F11 mutations in heterozygosis has been analyzed globally in the
whole cohort and on the other hand they have been split into four groups of the recurrent
mutations (p.Cys56Arg, p.Pro538Leu, c.1693G>A, and p.Cys416Tyr), which have been analyzed
separately (Table 3). The APTT, expressed both in seconds or as a ratio, was significantly
greater with SynthASil than with SynthAFax for all mutations, except for the APTT ratio for the
mutation affecting the splicing (c.1693G>A). In contrast, for FXI:C, the ellagic acid-based
reagent generated results significantly higher than those generated by silica for all mutations
(Table 3).
Evaluation of sensitivity of SynthASil and SynthAFax reagents for diagnosis of FXI deficiency.
This study was only done for cases with moderate FXI deficiency (heterozygous), as both
methods clearly identify homozygous or compound heterozygous subjects.
Sensitivity refers to a test ability to designate an individual with disease as positive. A highly
sensitive test means that there are few false negative results, and thus fewer cases of disease
are missed. SynthAFax had higher sensitivity (88%) compared to SynthASil (78%) for the
screening of FXI deficiency in subjects with genetic FXI deficiency when using APTT. Thus, the
percentage of false negatives (APTT ratio <1.3) was significantly higher with SynthASil (22.1%)
than with SynthAFax (12.1%) (p<0.01) (Figure 1). When the analysis was done attending to the
mutations, we observed that most (40-46%) of false negatives for both activators
corresponded to cases with qualitative deficiency (CRM+: p.Pro538Leu) (Figure 1).
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
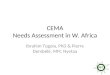
Figure 1: Comparison between true positives and false negatives for the APTT ratio depending on whether SynthASil or SynthAFax was used as activator. The percentage of false negatives for heterozygous mutations (p.Cys416Tyr, c.1693G>A, p.Pro538Leu, p.Cys56Arg, p.Ile426Thr, and p.Thr322Ile) is also shown.
Actually, the silica-based reagent rendered higher rates of false negatives (around two times)
than the ellagic acid-based reagent when using APTT ratio for all mutations, except for
c.1693G>A (Table 4).
Table 4: False negatives for the APTT ratio using both different contact activators in
heterozygous carriers of recurrent mutations.
Mutation (N) SynthASil; N (%) SynthAFax; N (%)
p.Cys416Tyr (N= 18) 3 (16.6%) 0 c.1693G>A (N= 19) 4 (21.1%) 4 (21.1%) p.Pro538Leu (N= 32) 13 (40.6%) 8 (25.0%) p.Cys56Arg (N= 51) 9 (17.6%) 4 (7.8%)
Sensitivity was higher for both activators when using FXI:C in heterozygous subjects with FXI
deficiency. However, and in contrast to the results obtained with APTT; the silica-based
activator had higher sensitivity (98%) than the ellagic acid-based activator (93%) (Figure 2).
Thus, the percentage of false negatives observed with SynthAFax was almost three times
higher than with SynthASil (7% vs. 2%, respectively). Again, CRM+ deficiencies are mainly
represented among false negative cases using this assay with both activators (Figure 2).
Figure 2: Comparison between true positives and false negatives for the FXI:C assay
depending on whether SynthASil or SynthAFax was used as activator. The percentage of
false negatives for heterozygous mutations (c.1693G>A, p.Pro538Leu, Exon 8&9 duplication
(dup), and p.Cys56Arg) is also shown.
Indeed, analysis by mutations revealed that only CRM+ mutations have increased rate of false
negatives when evaluating FXI:C levels by using SynthAFax (Table 5).
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
Table 5: False negatives for the FXI:C using both different contact activators in heterozygous
carriers of recurrent mutations.
Mutation (N) SynthASil; N (%) SynthAFax; N (%)
p.Cys416Tyr (N= 18) 0 0 c.1693G>A (N= 19) 1 (5.2%) 1 (5.2%) p.Pro538Leu (N= 32) 2 (6.3%) 6 (18.8%) p.Cys56Arg (N= 51) 0 1 (1.9%)
Role of functional F12 polymorphism in the APTT and FXI:C results of subjects with FXI
deficiency.
Since the reagents evaluated in this study activate FXII, variations on the levels of FXII might
significantly affect the results of these assays, particularly APTT. A common F12 polymorphism,
rs1801020 (Minor Allele Frequency –MAF-: 0.472), by disturbing the Kozak sequence of this
gene reduced plasma FXII levels and prolonged APTT results in healthy subjects [19]. We aimed
to evaluate the influence of this polymorphism on APTT and FXI:C assays of subjects with FXI
deficiency. This study was exclusively done in heterozygous carriers since the very low FXI
levels of homozygous or compound heterozygous carriers is the element with biggest weight
on both APTT and FXI:C results.
The rs1801020 polymorphism results in a significantly prolonged APTT in subjects with
heterozygous FXI deficiency only when activated with SynthASil, but it has minor effect when
SynthAFax was used (Table 6). The same effect was observed when we analyzed each mutation
separately, although not significant differences were obtained, probably due to small the
number of patients in each subgroup. As expected, this polymorphism had no effect on FXI: C
values independently of the activator employed (Table 6).
Table 6: Effect of the F12 polymorphism rs1801020 on the APTT and FXI:C values obtained
with SynthASil and SynthAfax from subjects with heterozygous FXI deficiency
SynthASil SynthAFax
Mutation
(N) Genotype rs1801020
N APTT (sec) APTT (ratio)
FXI:C (%) APTT (sec) APTT (ratio)
FXI:C (%)
All cases (N= 131)
CC CT/TT
88 43
41.2±4.3 42.4±7.8
1.37±0.14 1.44±0.14
43.0±12.7 42.4±9.5
32.7±3.4 32.4±6.3
1.44±0.15 1.46±0.16
48.7±13.1 47.9±9.4
p 0.69 0.04 0.77 0.88 0.59 0.95
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
p.Cys56Arg (N= 51)
CC CT/TT
36 15
40.9±3.2 41.5±11.9
1.36±0.11 1.47±0.15
40.5±10.6 39.9±9.9
32.8±2.8 32.1±9.5
1.44±0.12 1.51±0.19
47.0±11.2 44.9±9.9
p 0.22 0.13 0.95 0.44 0.36 0.46
p.Pro538Leu (N= 29)
CC CT/TT
23 6
38.8±3.3 41.9±2.5
1.29±0.11 1.39±0.09
49.5±11.8 48.2±6.4
30.9±2.3 30.5±0.9
1.36±0.10 1.34±0.04
55.6±13.0 55.9±9.8
p 0.33 0.33 0.93 0.95 0.76 1.00
c.1693G>A (N= 19)
CC CT/TT
11 8
41.4±5.1 43.2±5.5
1.38±0.17 1.44±0.18
44.7±15.2 42.2±11.1
32.2±4.6 33.2±4.2
1.42±0.20 1.46±0.18
44.6±20.0 46.3±9.7
p 0.93 0.61 0.61 0.74 0.51 0.51
p.Cys416Tyr (N= 18)
CC CT/TT
8 10
45.4±5.2 43.3±3.5
1.51±0.18 1.44±0.12
38.5±13.5 44.4±8.7
36.4±3.8 33.0±3.1
1.60±0.17 1.46±0.14
43.7±9.5 51.1±6.9
p 0.82 0.94 0.17 0.14 0.55 0.04
Role of age and gender on the APTT results of subjects with FXI deficiency.
In our cohort, gender has not a significant effect on APTT of all carriers of any heterozygous
mutation, however when we analyzed each recurrent mutation separately, we found that
women have significant lower values of APTT in carriers of c.1693G>A mutation (Table 7).
Table 7: Effect of gender on the APTT obtained with SynthASil and SynthAfax from subjects with heterozygous FXI deficiency and in each recurrent mutation. SynthASil SynthAFax
Mutation (N) Male (71) Female (60) Male (71) Female (60) All heterozygous (N= 131)
APTT (sec) p APTT ratio p
41.7±6.5 0.38
1.41±0.14 0.31
41.4±4.6 1.38±0.15
32.4±5.2 0.73
1.45±0.16 0.36
32.7±3.4 1.44±0.15
Male (33) Female (18) Male (33) Female (18) p.Cys56Arg heterozygous (N= 51)
APTT (sec) p APTT ratio p
40.5±7.9 0.73
1.39±0.11 0.60
42.3±4.8 1.41±0.16
31.8±6.4 0.50
1.44±0.13 0.52
34.0±3.9 1.49±0.17
Male (13) Female (16) Male (13) Female (16) p.Pro538Leu heterozygous (N= 29)
APTT (sec) p APTT ratio p
40.1±2.6 0.48
1.34±0.08 0.48
38.4±3.7 1.28±0.12
31.2±2.4 0.78
1.37±0.11 0.78
30.6±2.0 1.35±0.09
Male (11) Female (8) Male (11) Female (8) c.1693G>A heterozygous (N= 19)
APTT (sec) p APTT ratio p
44.0±7.1 0.01
1.47±0.24 0.01
41.3±3.2 1.37±0.11
34.1±5.8 0.02
1.50±0.25 0.01
31.8±0.26 1.40±0.11
Male (9) Female (9) Male (9) Female (9) p.Cys416Tyr heterozygous (N= 18)
APTT (sec) p APTT ratio p
46.3±4.9 0.09
1.54±0.16 0.09
42.2±2.7 1.41±0.09
35.4±4.4 0.44
1.56±0.19 0.46
33.6±2.9 1.48±0.13
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
Regarding age, no significant effect observed on the APTT, independently of the activator
(Table 8). No subjects below 15 years old carry c.1693G>A or p.Cys416Tyr mutations.
Table 8: Effect of age on the APTT obtained with SynthASil and SynthAFax from subjects with heterozygous FXI deficiency and in each recurrent mutation.
SynthASil SynthAFax
Mutation (N) Age <15 (10) Age >15 (121) Age <15 (10) Age >15 (121) All heterozygous (N= 131)
APTT (sec) P APTT ratio P
40.7±3.2 0.67
1.36±0.11 0.81
41.7±5.9 1.40±0.15
31.9±2.48 0.58
1.41±0.11 0.57
32.6±2.6 1.45±0.16
Age <15 (5) Age >15 (47) Age <15 (4) Age >15 (47) p.Cys56Arg heterozygous (N= 51)
APTT (sec) P APTT ratio P
40.4±4.6 0.50
1.34±0.16 0.52
41.2±7.2 1.40±0.13
32.3±3.4 0.83
1.42±0.15 0.85
32.6±5.9 1.46±0.15
Age <15 (5) Age >15 (25) Age <15 (5) Age >15 (25) p.Pro538Leu heterozygous (N= 29)
APTT (sec) P APTT ratio P
39.7±1.8 0.26
10.32±0.06 0.26
39.1±3.5 1.30±0.11
30.9±1.6 0.25
1.36±0.07 0.25
30.9±2.3 1.36±0.10
Discussion
FXI deficiency has been considered a rare disease except for some specific populations. Thus
among Ashkenazy Jews, FXI deficiency may be present in up to 8% of the population [8, 20].
However, a recent study evaluating available whole exome sequencing from different
populations found a frequency higher than expected of pathogenic mutations leading to FXI
deficiency [21]. This apparent contradiction may be explained by two reasons: 1) current
diagnostic methods for FXI screening fail to identify subjects with FXI deficiency, particularly
with mild FXI deficiency; 2) the clinical consequences of FXI deficiency (particularly bleeding)
are very mild or absent. Our data shows new evidences on the strong limitation of APTT as a
screening method for the diagnosis of FXI deficiency. Although all severe FXI deficiencies
significantly prolonged APTT using any activator, a high proportion of cases with mild-
moderate FXI deficiencies had APTT values within the normal range and may be missed. The
rate of false negatives is particularly high when using the silica-based reagent. This method
particularly fails to detect a CRM+ deficiency, p.Pro538Leu, as almost half of heterozygous
carriers of this mutation (40.6%) had APTT ratios within the normal range (< 1.3). This
observation may be explained by the strong dependence of APTT on FXI coagulant activity
(Figure 3) and the higher coagulant activity of FXI among heterozygous carriers of the
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
p.Pro538Leu(53.7±10.3withSynthASil and 61.2±10.0withSynthAFax)compared with carriers or
all other mutations (40.25±12.46 with SynthASil and 45.90±10.85 with SynthAFax).
Figure 3: Percentage of false negatives of APTT ratio with FXI:C levels.
Thus, moderate levels of FXI:C (>50%) are correlated with high rate of false negatives,
especially with SynthASil reaching 41% (Figure 3).
Our study shows some other clues that contribute to explain the low specificity of this method.
The activator of the contact phase is really important. Thus, the rate of false-negatives
increases two-fold (although it is still quite high) when using a stronger activator (the ellagic
acid reagent in our study). Moreover, the common and functional rs1801020SNP affecting the
plasma levels of FXII also contributes to reduce the sensitivity of APTT to detect moderate FXI
deficiency. Subjects with moderate FXI deficiency that also have high levels of FXII in plasma
(carriers of the C/C genotype of rs1801020 SNP, which represent up to 65% of the general
Spanish population[19]) had more possibilities to have normal APTT values. On the other hand,
it has been previously described that APTT were significantly lower in women than in men in
random population[4].In our cohort, gender has not a significant effect in all carriers of any
heterozygous mutation, however when we analyze each recurrent mutation separately, we
found that women have significant lower APTT ratios in carriers of c.1693G>A mutation. These
data support that APTT is neither a specific nor sensitive method to diagnose mild FXI
deficiency[22] and interference of other factors such type of activator, F12 polymorphism,
FXI:C levels and gender may lead to false interpretation of APTT values.
Our study shows that FXI:C assays have much better sensitivity to diagnose FXI deficiency.
Moreover, this method is not influenced by any of the studied factors (age, gender, or F12
0%
19%
41%
0% 4%
27%
0%
50%
100%
<20 20-50 >50
% o
f fa
lse
ne
gati
ves
of
AP
TT r
atio
% of FXI:C
SynthASil SynthFAx
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
SNP), and the activator has a mild effect, as although the rate of false negatives is almost three
times lower with SynthASil, than with SynthAFax, the rates are small (2% vs. 7%, respectively).
Our study has some strengths: 1) it has been done with one of the largest series of patients
with FXI deficiency collected worldwide, particularly of Caucasian origin (N= 140); 2) the study
has not been restricted to carriers of a single molecular defect, although there is a noticeably
molecular homogeneity as the majority of cases are heterozygous carriers of 4 recurrent
mutations identified in our population; 3) the study had been performed on the same day,
using the same reagents, same controls and the same coagulometer, reducing then
experimental variations; 4) we have evaluated two commercial contact activator reagents used
for the two routinely tests used for the diagnosis of FXI deficiency: APTT and FXI:C. However,
our study also has some limitations. It has been done with selected cases with FXI deficiency,
some of them selected by having a prolonged APTT using SynthASil. Moreover, our study has
been restricted to available carriers of described mutations. Finally, we have only evaluated
two contact activators reagents from a single company. Although further studies are required
to validate these results and to study other contact activators, our data suggests that the best
way to diagnose a case with FXI deficiency is by FXI:C using a weak activator (SynthASil in our
case).
Conclusions
Moderate FXI deficiency, particularly CRM+, might be underestimated by the limitations of
current diagnostic methods. APTT has particularly low sensitivity for FXI diagnosis as it is
influenced by FXII levels (determined by a common F12 SNP), by FXI:C levels and by the
activator of the contact phase. Our results suggests that the best screening method for FXI
deficiency is FXI:C using silica.
Funding
This work was supported by PI15/00079; CB15/00055 (ISCIII and FEDER); and 19873/GERM/15
(Fundación Séneca). SS-A is the recipient of the Research Fellowship from the Spanish Society
of Hematology and Hemotherapy (SEHH).MEM holds a fellowship from Fundación Española de
Trombosis y Hemostasia (FETH).
Acknowledgments
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
This research was supported by Izasa Scientific/A WerfenLife Company. The authors are
thankful to Alberto Lopez and Josep Garcia for assistance and the provided expertise that
greatly assisted the research.
Authorship
S.S-A., J.E., M.E.M-B., J.C., V.R. and V.V. collected patients and clinical data, designed research,
analyzed the data and wrote the paper. A.M. and C.A. performed genetic and biochemical
experiments.
Conflict of interest
Authors have no conflict of interest.
References
[1] White G. The partial thromboplastin time: defining an era in coagulation. Journal of Thrombosis and Haemostasis 2003;1:2267-70. [2] Calafell F, Almasy L, Sabater-Lleal M, Buil A, Mordillo C, Ramírez-Soriano A, et al. Sequence variation and genetic evolution at the human F12 locus: mapping quantitative trait nucleotides that influence FXII plasma levels. Human molecular genetics 2009;19:517-25. [3] Houlihan LM, Davies G, Tenesa A, Harris SE, Luciano M, Gow AJ, et al. Common variants of large effect in F12, KNG1, and HRG are associated with activated partial thromboplastin time. The American Journal of Human Genetics 2010;86:626-31. [4] Lowe GD, Haverkate F, Thompson SG, Turner RM, Bertina RM, Turpie AG, et al. Prediction of deep vein thrombosis after elective hip replacement surgery by preoperative clinical and haemostatic variables: the ECAT DVT Study. Thrombosis and haemostasis 1999;81:879-86. [5] Marlar RA, Bauer PJ, Endres-Brooks JL, Montgomery RR, Miller CM, Schanen MM. Comparison of the sensitivity of commercial APTT reagents in the detection of mild coagulopathies. American journal of clinical pathology 1984;82:436-9. [6] Turi DC, Peerschke EI. Sensitivity of three activated partial thromboplastin time reagents to coagulation factor deficiencies. American journal of clinical pathology 1986;85:43-9. [7] Gailani D, Broze Jr GJ. Factor XI activation in a revised model of blood coagulation. Science 1991;253:909-13. [8] Gomez K, Bolton‐Maggs P. Factor XI deficiency. Haemophilia 2008;14:1183-9. [9] Morrissey JH. Targeting factor XI to prevent thrombosis. Am Heart Assoc; 2013. [10] Colakoglu S, Bayhan T, Tavil B, Keskin E, Cakir V, Gümrük F, et al. Molecular genetic analysis of the F11 gene in 14 Turkish patients with factor XI deficiency: identification of novel and recurrent mutations and their inheritance within families. Blood transfusion= Trasfusione del sangue 2016:1. [11] Kawankar N, Rathi J, Ghosh K, Shetty S. Clinical and molecular epidemiology of factor XI deficiency in India. Thrombosis Research 2016;147:85-7.
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
[12] Keskin EY, Gürsel T, Kaya Z, Dai L, Koçak Ü, Yenicesu I, et al. Molecular basis and bleeding manifestations of factor XI deficiency in 11 Turkish families. Blood Coagulation & Fibrinolysis 2015;26:63-8. [13] Mitchell M, Mountford R, Butler R, Alhaq A, Dai L, Savidge G, et al. Spectrum of factor XI (F11) mutations in the UK population–116 index cases and 140 mutations. Human mutation 2006;27:829-. [14] Shao Y, Cao Y, Lu Y, Dai J, Ding Q, Wang X, et al. Clinical manifestations and mutation spectrum of 57 subjects with congenital factor XI deficiency in China. Blood Cells, Molecules, and Diseases 2016;58:29-34. [15] Esteban J, de la Morena-Barrio M, Salloum-Asfar S, Padilla J, Miñano A, Roldán V, Soria J, Vidal F, Corral J, Vicente V. High incidence of FXI deficiency in a Spanish town caused by 11 different mutations and the first duplication of F11. Results from the Yecla study. Haemophilia 2017. https://doi.org/10.1111/hae.13356. [16] Zivelin A, Bauduer F, Ducout L, Peretz H, Rosenberg N, Yatuv R, et al. Factor XI deficiency in French Basques is caused predominantly by an ancestral Cys38Arg mutation in the factor XI gene. Blood 2002;99:2448-54. [17] Quélin F, Francois D, d'Oiron R, Guillet B, de Raucourt E, de Mazancourt P. Factor XI deficiency: identification of six novel missense mutations (P23L, P69T, C92G, E243D, W497C and E547K). Haematologica 2005;90:1149-50. [18] Ventura C, Santos AI, Tavares A, Gago T, Lavinha J, McVey JH, et al. Molecular genetic analysis of factor XI deficiency: identification of five novel gene alterations and the origin of type II mutation in Portuguese families. Thrombosis and haemostasis 2000;84:833-40. [19] Corral J, Antón AI, Quiroga T, Gonzalez-Conejero R, Pereira J, Roldán V, et al. Influence of the F12-4 C> T polymorphism on hemostatic tests. Blood Coagulation & Fibrinolysis 2010;21:632-9. [20] Asakai R, Chung DW, Ratnoff OD, Davie EW. Factor XI (plasma thromboplastin antecedent) deficiency in Ashkenazi Jews is a bleeding disorder that can result from three types of point mutations. Proceedings of the National Academy of Sciences 1989;86:7667-71. [21] Asselta R, Paraboschi EM, Rimoldi V, Menegatti M, Peyvandi F, Salomon O, et al. Exploring the global landscape of genetic variation in coagulation factor XI deficiency. Blood 2017:blood-2017-04-780148. [22] Bolton-Maggs PH. Factor XI deficiency—resolving the enigma? ASH Education Program Book 2009;2009:97-105.
ACCEPTED MANUSCRIPT

本文献由“学霸图书馆-文献云下载”收集自网络,仅供学习交流使用。
学霸图书馆(www.xuebalib.com)是一个“整合众多图书馆数据库资源,
提供一站式文献检索和下载服务”的24 小时在线不限IP
图书馆。
图书馆致力于便利、促进学习与科研,提供最强文献下载服务。
图书馆导航:
图书馆首页 文献云下载 图书馆入口 外文数据库大全 疑难文献辅助工具