Embed Size (px)
Citation preview
Authors: G. Guagliumi1, G. Musumeci1, V. Sirbu1, N. Suzuki3, G. Biondi Zoccai2, L. Mihalcsik1, A. Matiashvili1, A. Trivisonno1, N. Lortkipanidze1, L. Fiocca1, J. Coletta3, H. Bezerra3,
O.Valsecchi1, M. Costa3
2 Division of Cardiology, University of Turin, Italy1 Division of Cardiology, Ospedali Riuniti di Bergamo, Italy3 Case Western Reserve University, Cleveland, OH, US
TaxusN=22
CypherN=22
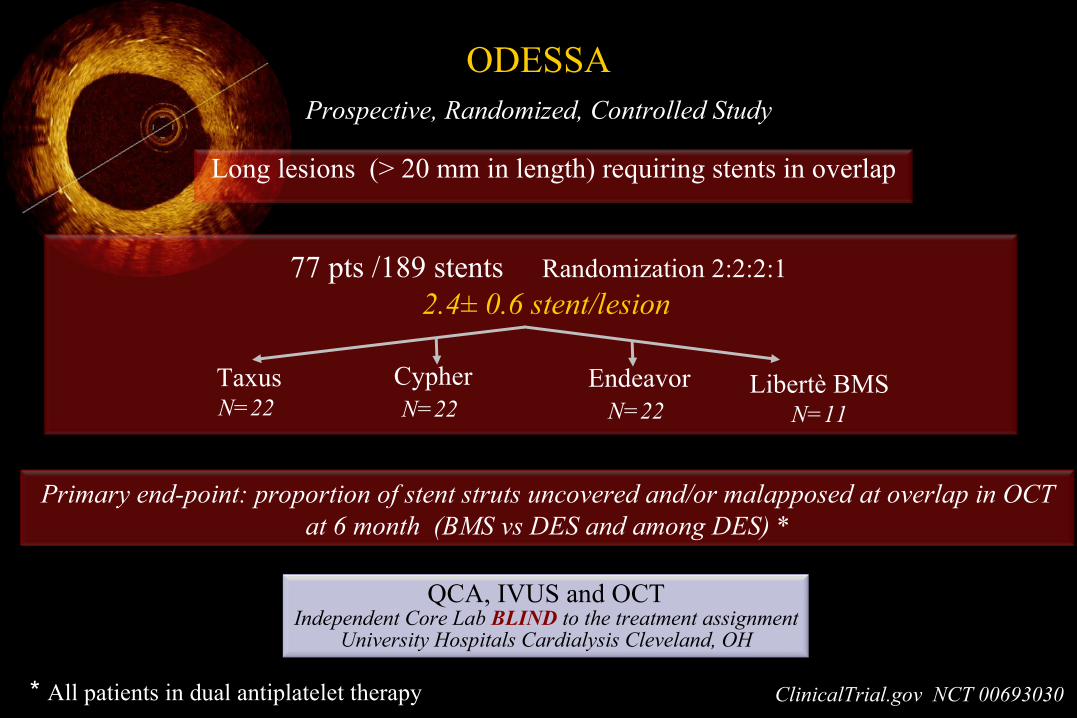
Long lesions (> 20 mm in length) requiring stents in overlap
77 pts /189 stents Randomization 2:2:2:1 2.4± 0.6 stent/lesion
ODESSAProspective, Randomized, Controlled Study
EndeavorN=22
Libertè BMSN=11
Primary end-point: proportion of stent struts uncovered and/or malapposed at overlap in OCT at 6 month (BMS vs DES and among DES) *
QCA, IVUS and OCTIndependent Core Lab BLIND to the treatment assignment
University Hospitals Cardialysis Cleveland, OH
ClinicalTrial.gov NCT 00693030* All patients in dual antiplatelet therapy
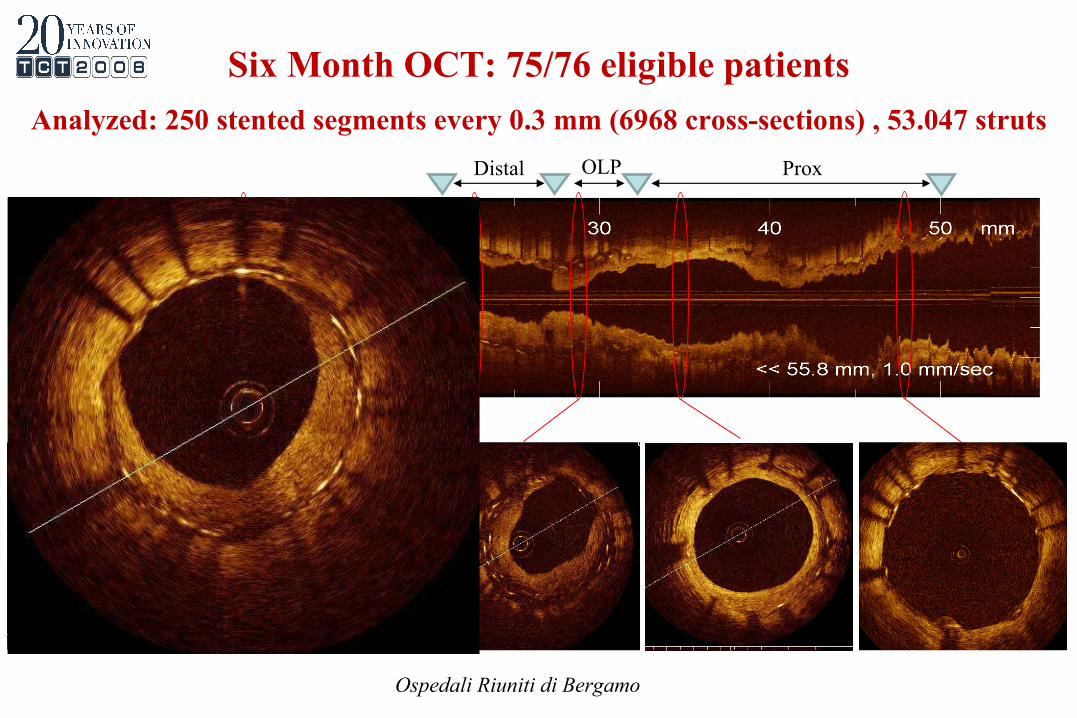
Distal OLP Prox
Ospedali Riuniti di Bergamo
Six Month OCT: 75/76 eligible patients
Analyzed: 250 stented segments every 0.3 mm (6968 cross-sections) , 53.047 struts
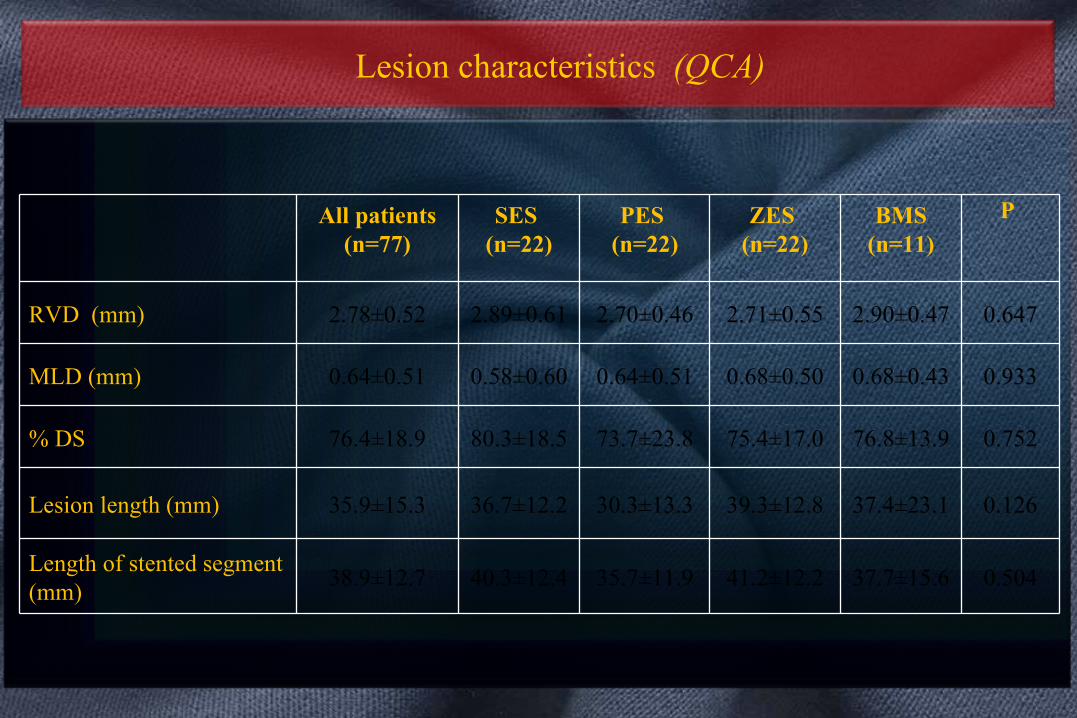
Lesion characteristics (QCA)
All patients (n=77)
SES (n=22)
PES (n=22)
ZES (n=22)
BMS (n=11)
P
RVD (mm) 2.78±0.52 2.89±0.61 2.70±0.46 2.71±0.55 2.90±0.47 0.647
MLD (mm) 0.64±0.51 0.58±0.60 0.64±0.51 0.68±0.50 0.68±0.43 0.933
% DS 76.4±18.9 80.3±18.5 73.7±23.8 75.4±17.0 76.8±13.9 0.752
Lesion length (mm) 35.9±15.3 36.7±12.2 30.3±13.3 39.3±12.8 37.4±23.1 0.126
Length of stented segment (mm)
38.9±12.7 40.3±12.4 35.7±11.9 41.2±12.2 37.7±15.6 0.504
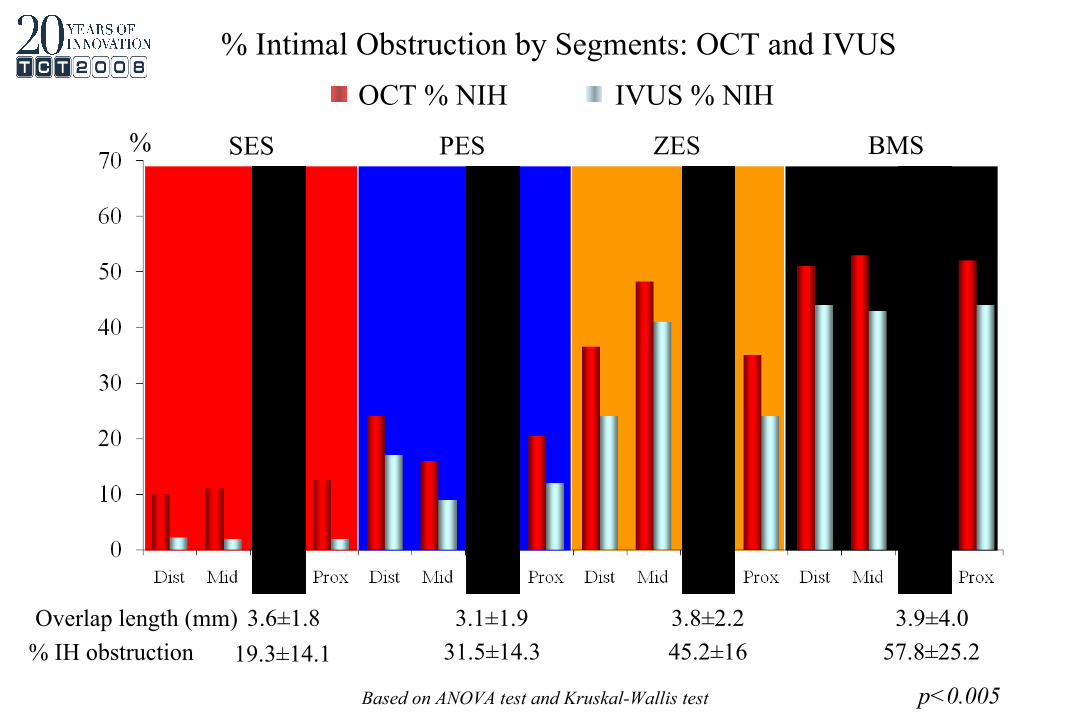
SES PES ZES BMS%
OCT % NIH IVUS % NIH
% Intimal Obstruction by Segments: OCT and IVUS
Based on ANOVA test and Kruskal-Wallis test p<0.005
3.6±1.8 3.1±1.9 3.8±2.2 3.9±4.0Overlap length (mm)
% IH obstruction 19.3±14.1 31.5±14.3 45.2±16 57.8±25.2
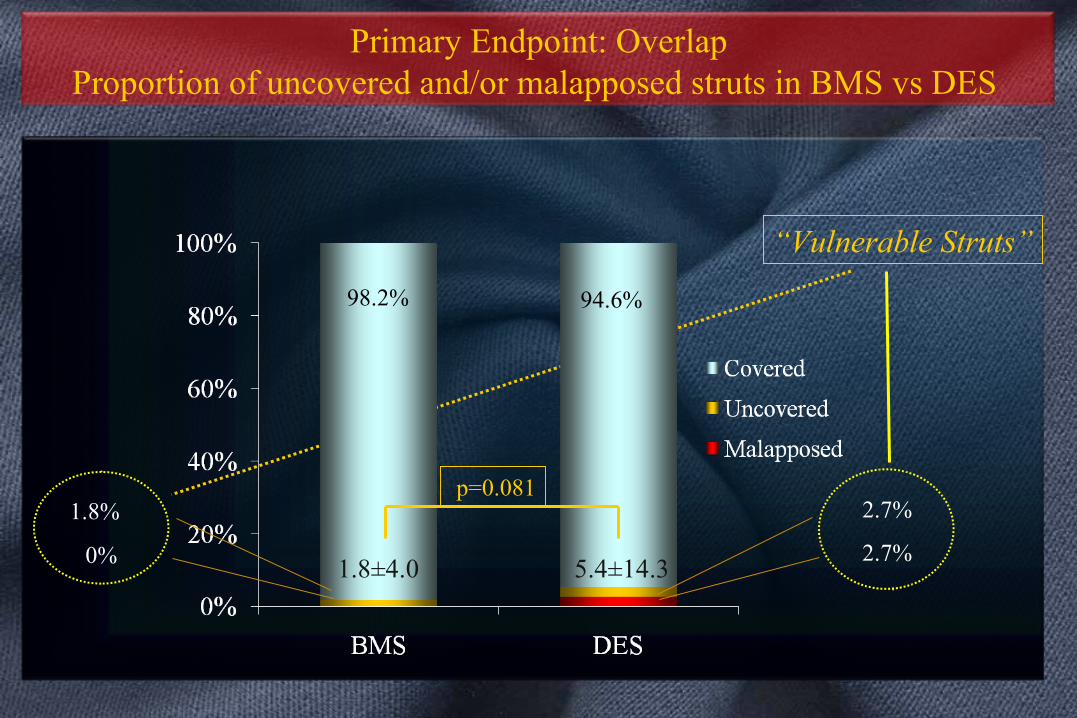
0%
1.8%
98.2% 94.6%
2.7%
2.7%
“Vulnerable Struts”
p=0.081
Primary Endpoint: OverlapProportion of uncovered and/or malapposed struts in BMS vs DES
1.8±4.0 5.4±14.3
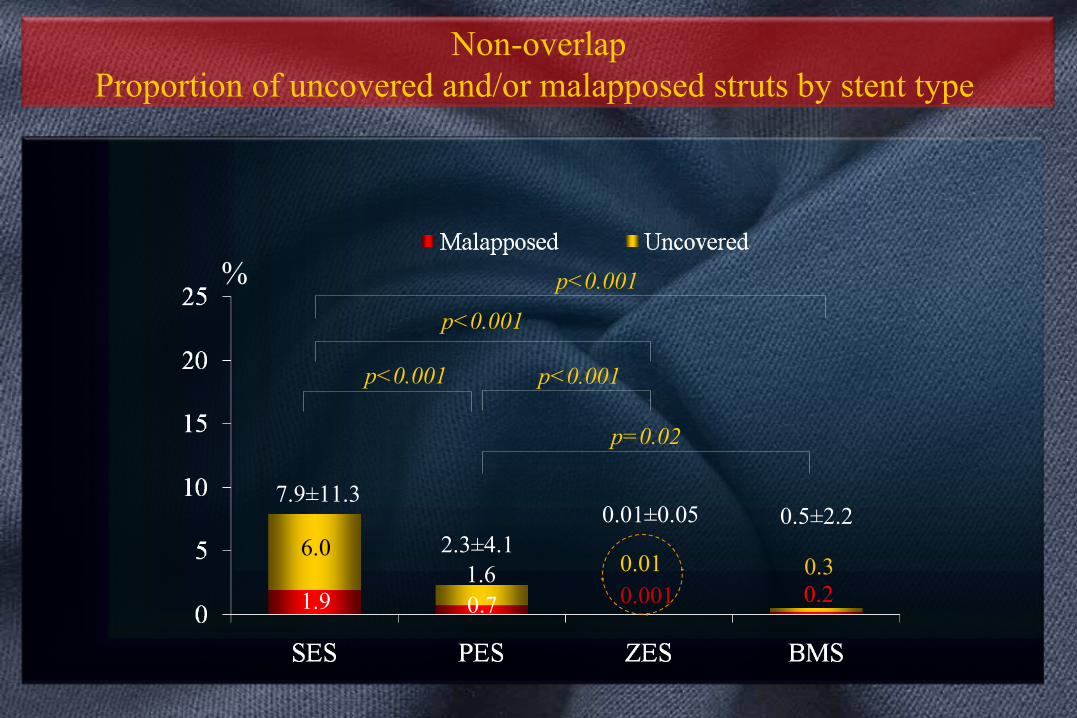
1.9
6.0
0.7 0.0010.01
0.2
7.9±11.3
2.3±4.10.01±0.05 0.5±2.2
p<0.001
p=0.02
p<0.001
p<0.001 p<0.001
Non-overlapProportion of uncovered and/or malapposed struts by stent type
1.6 0.3
%
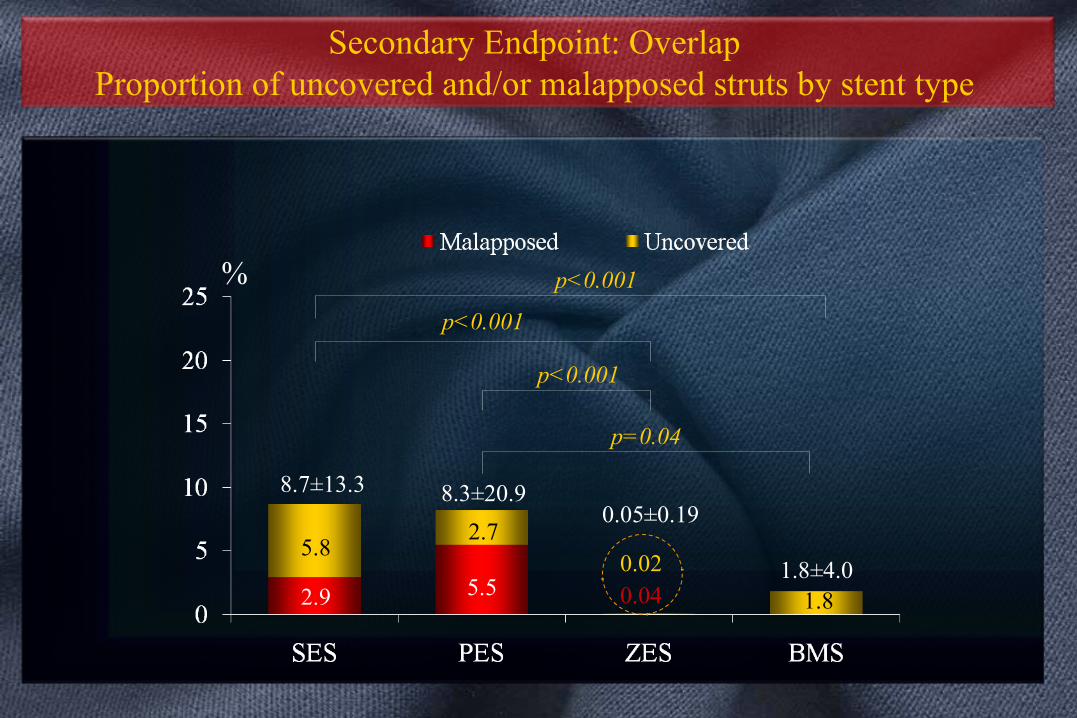
2.9
5.8
5.5
2.7
0.040.02
1.8
%
8.7±13.3 8.3±20.90.05±0.19
1.8±4.0
p<0.001
p=0.04
p<0.001
p<0.001
Secondary Endpoint: Overlap Proportion of uncovered and/or malapposed struts by stent type
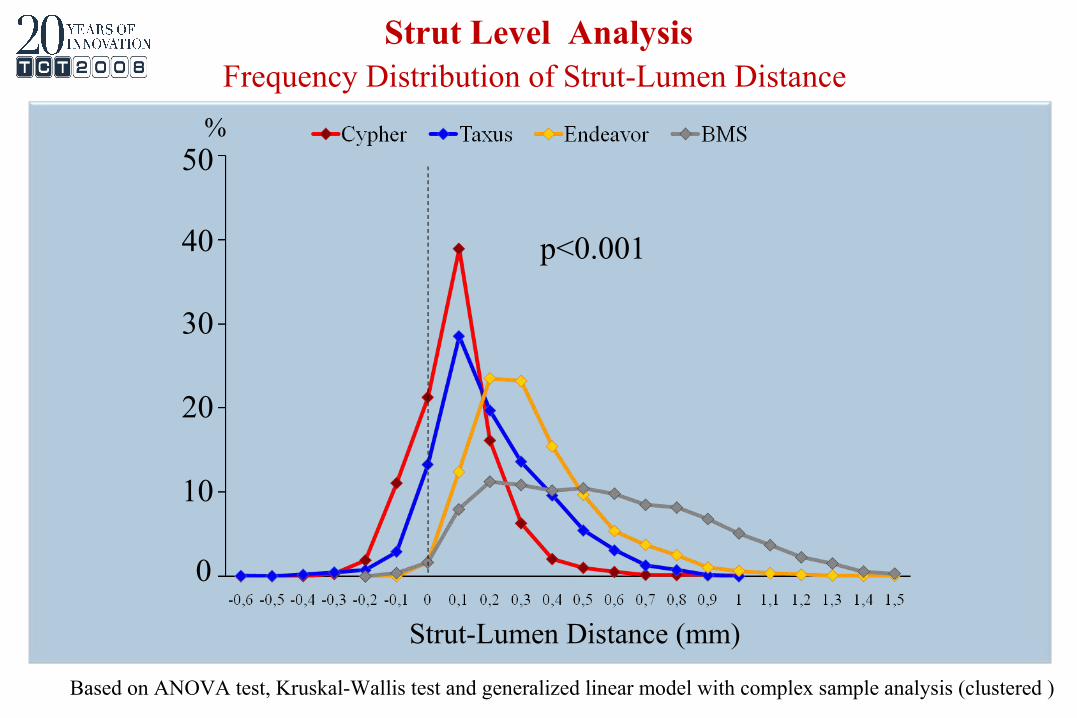
Strut-Lumen Distance (mm)
0
10
20
30
40
50%
Strut Level AnalysisFrequency Distribution of Strut-Lumen Distance
p<0.001
Based on ANOVA test, Kruskal-Wallis test and generalized linear model with complex sample analysis (clustered )
Conclusions
The ODESSA trial demonstrated:
• Feasibility of using intravascular OCT in prospective clinical trials
• >90% strut coverage at 6-month follow-up
•Trend towards higher incidence of uncovered and malapposed struts at the OL site of DES than in BMS
• Different degrees of strut coverage and NIH among DES platforms:
SES : Highest rate of uncovered and malapposed struts (OL = non-OL) Lowest degree of NIH (OL> non-OL)
ZES: Lowest rate (≈ 0%) of uncovered and malapposed struts (OL = non-OL) Highest degree of NIH (OL> non-OL)
PES: Higher incidence of uncovered and malapposed struts (OL> non-OL) Intermediate degree of NIH (OL> non-OL)