Embed Size (px)
Citation preview

2012
KCE REPORT 1
DÉPIS
76B
STAGE DDU CANNCER DDU SEINN ENTRE 70 ETT 74 AN
www.kce.fgo
S
ov.be

Le Centre
Conseil d’a
fédéral d’ex
administratio
xpertise desLe CedécemIl est de l’a
on
PrésidFonctPrésidPrésidAdminRepré
Repré
Repré
Agenc
Organdes m
Organdes inFédér
Parte
Cham
s soins de saentre fédéral d’embre 2002 (articchargé de réalis
assurance malad
dent tionnaire dirigeantdent du SPF Santdent du SPF Sécunistrateur généralésentants du minis
ésentants du minis
ésentants du Cons
ce intermutualiste
nisations professiomédecins
nisations professionfirmiers rations hospitalièr
naires sociaux
mbre des Représe
anté expertise des soles 259 à 281), sser des études é
die.
t de l'INAMI (vice té publique (vice purité sociale (vice de l'AFMPS stre de la Santé p
stre des Affaires s
seil des ministres
e
onnelles représen
onnelles représen
res
ntants
oins de santé essous tutelle du Méclairant la décis
MePie
président) Jo président) Dirprésident) Fra
Xapublique Be
Masociales Oli
Ri Jea
DaMicPaXa
ntatives MaJea
ntatives MicMyJohJeaRitPaLie
st un parastatal, Ministre de la Sansion politique da
embres effectifserre Gillet De Cock
rk Cuypers ank Van Massenh
avier De Cuyper ernard Lange arco Schetgen vier de Stexhe De Ridder an-Noël Godin
aniel Devos chiel Callens
atrick Verertbruggeavier Brenez arc Moens an-Pierre Baeyenchel Foulon yriam Hubinon han Pauwels an-Claude Praetta Thys
aul Palsterman eve Wierinck
créé par la loi-pnté publique et dans le domaine d
Memb
Benoît Chris D
hove Jan BeGreet MFrançoAnnickKarel VLambeFrédérBart OoFrank D
en YolandGeert M
s RolandRita Cu
Ludo MOlivier KatrienPierre Leo NeCelien
programme (1) ddes Affaires socdes soins de san
res suppléants
Collin Decoster ertels Musch ois Perl k Poncé Vermeyen ert Stamatakis ric Lernoux oghe De Smet de Husden Messiaen d Lemye uypers Meyers
Thonon n Kesteloot Smiets
eels Van Moerkerke
du 24 iales. nté et

Contrôle
Direction
Contact
Comm
DirecDirecDirec
CentrDoorbBouleB-100Belgi T +32F +32info@http://
missaire du Gouv
cteur Général cteur Général Adjocteurs du program
re Fédéral d’Expebuilding (10e étagevard du Jardin B00 Bruxelles que
2 [0]2 287 33 88 2 [0]2 287 33 85
@kce.fgov.be /www.kce.fgov.be
vernement
oint mme d'études
ertise des Soins dee) otanique, 55
e
Yv
RaJeChKr
e Santé (KCE)
ves Roger
af Mertens ean-Pierre Closonhristian Léonard ristel De Gauquierr


2012
KCE REPORT 1GOOD CLINICA
DEPIS FRANÇOISE M
76B AL PRACTICE
STAGE D
MAMBOURG, JO R
DU CAN
ROBAYS, SOPHI
NCER D
IE GERKENS
DU SEINN ENTRE 70 ETT 74 AN
www.kce.fgo
S
ov.be

COLOPHOTitre:
Auteurs:
Relecture:
Experts externe
Validateurs exte
Conflits d’intérê
Layout:
Disclaimer:
Date de publica
Domaine:
MeSH:
Classification N
Langue:
ON
es:
ernes:
êt:
ation:
NLM:
Dépi
Fran
Fran
Marc(ASBNeveVand
Philip
Aucu
Ine V
• Lereet
• Ucora
• F• Le
re
26 ap
Good
Brea
WP 8
franç
stage du cancer d
çoise Mambourg
k Hulstaert (KCE)
c Arbijn (WIV - ISBL Brummammo)en (UZ Leuven), Mdenbroucke (UCL
ppe Autier (IPRI-L
un conflit déclaré
Verhulst
es experts exteremarques ont étét n’étaient pas néne version (finaonsensus ou d’uapport scientifiquinalement, ce rape KCE reste seuecommandations
pril 2012
d Clinical Practice
st Neoplasms ; M
870 - Breast - Neo
çais, anglais
du sein entre 70 e
(KCE), Jo Robays
), Pascale Jonckh
SP), Martine Berli), Joëlle DesreuxMyriam Provost (SSaint-Luc), Geert
Lyon), Geert Page
rnes ont été coné discutées au cécessairement dale) a ensuite étun vote majoritaue et ils n’étaienpport a été appro
ul responsable ds faites aux auto
e (GCP)
Mammography ; M
oplasms
et 74 ans
s (KCE), Sophie G
heer (KCE), Nancy
ière (UCL Saint-Lx (CHU Liège), ASSMG), Hubert Tht Villeirs (UZ Gent
e (Jan Yperman Z
nsultés sur une vours des réunion
d’accord avec soté soumise aux
aire entre les valt pas nécessaireouvé à l'unanimies erreurs ou omrités publiques.
ass Screening
Gerkens (KCE)
y Thiry (KCE)
Luc), Hilde BosmAndré-Robert Grivhierens (UGent), Rt).
Ziekenhuis), Chant
version (préliminns. Ils ne sont pan contenu.
x validateurs. Laidateurs. Les va
ement tous les trté par le Conseilmissions qui po
ans (UZ Leuven)vegnée (Institut JReinhilde Van Ee
tal Van Ongeval (
naire) du rapporas co-auteurs du
a validation du ralidateurs ne sonrois d’accord avel d’administratiourraient subsiste
), Jean-Benoit BuJules Bordet), Pa
eckhoudt (WVG), A
(KU Leuven)
rt scientifique. Lu rapport scientif
rapport résulte nt pas co-auteurec son contenu. n. er de même que
urrion atrick Anne
Leurs fique
d’un rs du
e des

Format:
Dépot légal:
Copyright:
Comment citer
ce rapport?
Adob
D/20
Les rhttp:/
Mam(GCPD/20
Ce d
be® PDF™ (A4)
12/10.273/19
rapports KCE son//kce.fgov.be/fr/co
mbourg F, RobaysP). Bruxelles: C12/10.273/19.
ocument est disp
nt publiés sous Licontent/a-propos-du
s J, Gerkens S. Dentre Fédérale
onible en téléchar
cence Creative Cou-copyright-des-ra
Dépistage du cand’Expertise des
rgement sur le sit
ommons «by/nc/napports-kce
ncer du sein entreSoins de Sant
e Web du Centre
d»
e 70 et 74 ans. Gté (KCE). 2012.
fédéral d’expertis
Good Clinical PraKCE Report 1
se des soins de sa
actice 76B.
anté.


KCE Report 176
PRÉF
6B
FACE Faire des csur l’âge. Cpersonne, uraisonnemeparfois diamLa présenteâgées de 7particulièrene présenteL’adage priEn matière logique utilscreening. clairement explique polaisser l’opipolitiquemeMême si onpour autanpeut attend
Jean-PierreDirecteur G
Dé
choix en matière dComment par exeuniquement sur uents conduisent symétralement oppoe étude qui pose 70 à 74 ans, noument vigilants surent a priori pas deimum non nocered’argumentation isée pour poser Dans le premierconsidéré comm
ourquoi les inconvinion publique ind
ent. n mobilise toutes t espérer arrêter
dre d’un organe d’
e CLOSON Général Adjoint
épistage du cancer
de soins ressembemple justifier le rn critère d’âge, mystématiquement
osés. la question de sa
us place donc à r un tel sujet. Come plainte de santéest donc ici d’autà développer, il yun diagnostic cher cas, le risque de moins importanvénients d’un dépdifférente, un lobb
les preuves scienla controverse. Navis scientifique d
r du sein
ble vite à de la disrefus de rembour
même si pour le reà des discussion
avoir s’il faut offrirnouveau sur un mme dans tout déé et qui n’étaient dtant plus importany a aussi un défi pez une personned’un résultat fauxnt qu’un résultat fpistage sont systébying intense est
ntifiques disponibNous osons néandans un tel débat.
scrimination, en prsement d’une inteste cette personnns enflammées, no
r un dépistage orsol glissant. Maisépistage organisédonc pas nécessant. particulier à relevee qui a une plaintx positif est nonfaux négatif, qui matiquement sout organisé à son
bles pour fonder unmoins espérer q
particulier lorsque tervention coûteusne est encore en ourries à partir de
rganisé du cancers il y a encore dé, on s’adresse enairement demand
er. Le clinicien este que de celle u seulement plus équivaut à loupe
us évalués. De plupropos, et il est
un avis sur la queue ce rapport ap
ces choix sont base sur le cœur à bonne forme? De
e systèmes de val
r du sein aux fem’autres raisons dn effet à des genseurs d’un tel exam
t plus coutumier dutilisée en matière
petit mais est aer un diagnostic. us, le sujet est loi(donc) aussi sen
estion, on ne peutpportera tout ce q
Raf MERTENDirecteur Gén
i
asés une
e tels leurs
mmes d’être s qui men.
de la e de aussi Cela n de sible
t pas qu’on
S néral

ii
RÉSUUMÉ
Déépistage du cancer
ICdnasLddmasLedecLfeaLqspdstrEqdle
r du sein
NTRODUCCe travail fait partdu rapport: «Dépisn°11). Il concerneaux femmes âgésymptôme évocateLe dépistage du cdes bénéfices etdépistage du canmorbidité liées à allègement des tstades métastatiquLes risques princieffet, un résultatdiagnostic) suivi dest la durée par laclinique) ont des cLes résultats fauemmes en bonanxiogènes voire iLe sur-diagnosticqui n’auraient jams’accroit au fur et population dépistdiagnostic. Vu qu’se développer, laraités. Enfin, le dépistageque ne le ferait udevient «malade de décours de sa v
CTION tie d’un projet plustage du cancer
e plus particulièremes de 70 à 74eur, ni facteur de cancer du sein est des risques. Lcer du sein sontla maladie. La di
traitements, soit ues de la maladiepaux liés au dépfaussement pos
’un traitement et laquelle le diagnosconséquences surssement positifs ne santé dans invasifs (biopsies)peut être défini cais été perçus clin à mesure de la ée. Le sur-traiteil est actuellemen
a très grande ma
e met les cancersun diagnostic clindu cancer» et reçovie.
us large ayant podu sein», publié ment l’extension ans qui ne présrisque particulier.
st un processus cLes principaux bt la diminution deiminution de morune diminution d
e. pistage concernensitif, un diagnost’avance au diagnstic par dépistager la qualité de vie.
ont pour conséun circuit d’ex
). comme la détectiniquement en l’abdiminution de l’e
ement est une cnt impossible de pajorité des cance
s en évidence deunique. Ceci imploit des traitements
KCE Report 1
ur objet la mise àen 2005 (rapportdu dépistage org
sentent par ailleu
complexe qui combénéfices attendue la mortalité et rbidité implique sodes récidives ou
nt la qualité de vitic excédentaire ostic (ou lead tim
e précède le diagn
équence d’inclurexamens diagnost
on de cas de cabsence de dépistaespérance de vie conséquence duprédire si un cancers diagnostiqués
ux ou trois ans plique que la perss invasifs plus tôt
176B
à jour KCE anisé
urs ni
mporte us du de la oit un u des
e. En (sur-
e, qui nostic
e des tiques
ncers age. Il de la sur-
cer va sont
us tôt sonne
dans

KCE Report 176
QUESTIOCe rapport invorganisé du canSi la réponse àpose: que répodépistage?
MÉTHODL’étude des bélittérature effectrevue a inclus Français de janL’évaluation durevue des étudNHS EED et EAllemand, NéerAfin de quantifimodèle a été nécessité de r(1950-10/2011)dépistage et lemaximum de doEnfin, des recobase des élérecommandatiod’intérêts n’a ét
6B
ONS POSÉvestigue la questncer du sein aux fà cette question
ondre à la personn
DOLOGIE énéfices cliniquestuée dans OVID Mles articles publ
nvier 2004 à avril 2 rapport bénéficedes de modélisat
Econlit. Cette revurlandais et Françaier le rapport bénconstruit dans cechercher dans ) les études relative traitement du onnées belges utiommandations deéments de pre
ons a été effectuété signalé.
ES ion suivante: faufemmes âgées deest négative, unene de cette tranch
s du dépistage seMedline, EMBASEiés en Anglais, A2011. s-risques de ce dtion recherchées ue a inclus les arais de janvier 2000néfices-risques dace but. La constMedline, Embaseves à la qualité dcancer du sein.
ilisables. e bonne pratiqueeuve obtenus.ée par les expert
Dé
ut-il étendre le dée 70 à 74 ans? e question subsidhe d’âge qui dem
e base sur une rE, CDSR et DARAllemand, Néerla
épistage se basedans Medline, E
rticles publiés en 0 à septembre 20ans le contexte btruction de ce me, HTA EED et Pe vie pendant et . Le modèle con
e ont été rédigéeUne révision d
ts externes. Aucu
épistage du cancer
épistage
diaire se ande un
evue de RE. Cette
ndais et
sur une Embase, Anglais,
011. elge, un
modèle a Psycinfo après le ntient le
es sur la desdites
un conflit
RMLm•
•
Dnla
MOepbvfotodtrcDrédma
r du sein
RÉSULTATMortalité Les résultats desmettre en évidenc Le dépistage
période de subénéficié d’un
Cette diminutdépistage. Il l’espérance d70 ans et de 1
Dans l’interprétationombre de participa mortalité n’a pu
Morbidité Outre le gain en aest de permettre pour objectif de mbelges dont nousvalider cette asseont état de 58% dotales dans les stdes bénéficiaires raitement par radchimiothérapie néoD’autre part, les eécidives ni l’évolu
donc impossible dmorbidité sur cetteaux métastases es
TS ISSUS D
s différents essaise les faits suivantentraîne une dim
uivi de 13 ans chen dépistage tous letion de mortalité s
convient donc e vie moyenne d13 ans à 74 ans (don des études intepantes âgées de 7être statistiqueme
années de vie, le pdes traitements mmettre en évidens disposons acturtion. Les donnéede chirurgie constades les moins ade la chirurgie
diothérapie, 38% do-adjuvante et 41essais contrôlés rution vers les stad’infirmer ou de coe base. Par contrst inclue dans le m
DE LA LITT
s contrôlés randots: minution de mortez les femmes dees deux ans. se manifeste entr
de la mettre e ce groupe d’âgdonnées belges dernationales, il fau70 à 74 ans; consent démontré pou
principal avantagemoins agressifs, vnce des petites tuellement ne noues les plus récenservatrice versus avancés (Stades conservatrice reçd’entre elles reço% un traitement h
randomisés n’ont des métastatiqueonfirmer l’hypothère, la perte de qumodèle (voir ci-de
TÉRATURE
omisés permette
talité de 23% sue plus de 50 ans
re 4 et 7 ans apren perspective
ge qui est de 16 ade 2009). ut tenir compte duséquemment, l’effeur celles-ci.
e attendu du dépivu que le dépistaumeurs. Les donus permettent pates (rapport KCE38% de mastectoI and II). Près deçoivent égalemen
oivent un traitemehormonal. quantifié ni le tau
es de la maladie. èse d’une réductioualité de vie impuessous).
iii
E
nt de
r une ayant
rès le avec
ans à
u petit et sur
stage age a nnées as de 150)
omies e 90% nt un
ent de
ux de Il est
on de utable

iv
ÉTUDESLes principalesCISNET (Cancmodèles avaiedépistage par mla mortalité due2000, et ils utConsortium. Les résultats de9 à 22 ans parla méthodologscientifique. Ces modèles ncar il est imposspécifique a do
UN MODÈBELGIQUMéthodologieLe modèle conpar cycles annplus de 70 ansl’autre où les feparticipation et les cancers d’inla tranche d’âgeLe dépistage a précoce (I et métastatique) qles cancers dépmême temps qD’autre part, nqualité de vie dElle ne tient pa
DE MODÉ études de modé
cer Intervention aent pour objectimammographie ete au cancer du tilisent les donné
e ces modèles indr 1.000 femmes dgie CISNET son
ne sont pas adaptssible d’y inclure nc été construit.
ÈLE DE COUE e struit pour ce rapuels. Il compare s, l’une sans inviemmes continuenla répartition des
ntervalle sont conse 50-69 ans. pour objectif de m
II) afin d’évitequi est incurable. pistés, la proportioque la proportionous avons émis
dépendent de l’âgas compte du fait
ÉLISATIONélisation ont été réand Surveillance if d’évaluer la t du traitement adsein observée auées issues du B
diquent un gain edépistées. D’autrent également d
tables en tant queles données belg
OHORTE P
pport est un modèdeux cohortes th
itation au dépistant à être invitées s cancers détectéssidérés comme é
mettre en évidencer l’évolution veCe «stage-shift»
on des stades prén des stades aval’hypothèse selon
ge de la patiente eque le pronostic d
Dé
éalisées au sein dModeling Netwocontribution relajuvant sur la réduux Etats-Unis de
Breast Cancer Sc
n années de vie aes modèles n’utilisdécrits dans le
e tels à la situatioges. Un nouveau
POUR LA
èle de cohorte quhéoriques de femage (situation actau dépistage. Le s par le dépistagetant les mêmes q
ce les tumeurs à uers le stade IV implique que pa
écoces (I, II) augmancés (II et IV) dn laquelle la survet du stade de la des cancers déte
épistage du cancer
du projet rk). Ces
ative du uction de
1975 à creening
allant de sant pas
rapport
on belge modèle
ui évolue mmes de uelle) et taux de
e versus que dans
un stade V (stade
rmi tous mente en diminue. vie et la tumeur.
ectés par
le(cp
PCl’disnIndooLé
MLpsdtabLd•
•
Pc
r du sein
e dépistage estcancers d’interva
participantes).
Paramètres Ce modèle explespérance de v
données du regisssues du progranécessaire pour ntermutualiste, AIdu stade (Registreont été privilégiéesopportuniste aprèsLa durée de l’avanété estimées au dé
Mesure de la qLes données sur proviennent de la santé est l’EQ-5descriptions ont éariffs»). Nous nebelge. Les variations de dans le modèles s La perte de
faussement p Pour les patie
le diagnostic (estimée à 16Pendant les a6% pour les pour les stade
Plusieurs limitatiochiffres avec préca
meilleur que celalle et cancers
loite au maximuie moyenne des
stre du cancer (Camme de dépis
infirmer un diaIM/IMA) et les doe du Cancer). Less car elles sont pls 70 ans y est monce au diagnostic épart de l’analyse
ualité de vie la qualité de vielittérature. L’instr
5D (European été valorisées pare disposons pas
la qualité de vie dsont les suivantesqualité de vie coositif est estimée
entes cancéreuse(quel que soit le t% pour les stade
années suivantes,stades I, II, III. Ces IV. ons de cette appaution
lui des cancers survenant che
um les données femmes selon Communauté Flastage actuel (50agnostic faussem
onnées de survie données de la Clus complètes et poins fréquent que
et le pourcentagee de la littérature.
e pendant le déprument utilisé pouQuality of Life-r la population géde données rela
des femmes de p: onsécutive à un à 16% pendant 4s et pendant la ptraitement) la pertes I, II, III et à 18 la perte de qualit
Cette perte demeu
proche nous oblig
KCE Report 1
détectés cliniqueez les femmes
s belges, à saleur âge (2009)
amande), les don0-69 ans), le tment positif (Agà cinq ans en fonommunauté Flamparce que le dépidans le reste du e de sur-diagnost
istage et le traiteur décrire les éta-5 Dimensions); énérale anglaise atives à la popu
lus de 70 ans util
résultat de dépi45 jours. remière année qute de qualité de v8% pour les stadeté de vie est estimure stationnaire (
gent à interpréte
176B
ement non-
avoir : ), les nnées emps
gence nction
mande stage pays.
tic ont
ement ats de
ces («UK lation
lisées
stage
ui suit ie est es IV. mée à (18%)
r ces

KCE Report 176
Résultats Le scénario dpermettrait d’évreprésente uned’années de vieEtant donné qules discussionsune analyse dcomprend un scLe scenario pe20%, d’un taux vie de 0,19 perdrésultats). La actuellement daa été appliquéd’estimer un ga1000 femmes circonstances, aboutir à une peLe scenario opd’un taux de fa0,13 perdurant la distribution dépistage orgapermet d’estimepour 1000 femnécessaire d’invpour gagner un
6B
de base montre viter 1,3 décès poe réduction de 2e sauvées est estiu’il existe une incs dans le rapport de sensibilité ducénario pessimistessimiste fait l’hyde faux positifs d
durant pendant 54distribution des
ans le cadre du dée au groupe dain de 8,7 annéeparticipant au déau demeurant t
erte en terme de qtimiste fait l’hypotux positifs de 2%pendant 36 jourspar stades obs
anisé aux Pays-Ber un gain de 17mmes participant viter 67 femmes à QALY.
que le dépistagour 1000 femmes
21% des décès. imé à 13,1 et le gcertitude importanscientifique) au s
u modèle a été te et un scénario oypothèse d’un exde 10%, entrainan4 jours (temps nécancers dépisté
dépistage organisdépisté. Ce scénes de vie et une épistage. Ceci sigtout à fait réalistqualité de vie. thèse d’un excéd
%, entrainant une ps. Ce scénario apservée actuellemBas (70-74 ans),0 années de vie
au dépistage. à participer au dé
Dé
ge entre 70 et s qui y participentGlobalement, le ain en QALY à 3,nte (pour les détasujet des ces estim
réalisée. Cette optimiste. xcédent de diagnnt une perte de quécessaire pour infiés par stades oé en Flandre (50-nario pessimiste perte de 3,1 QA
gnifie que dans ctes, le dépistage
ent de diagnosticperte de qualité dpplique au groupement dans le ca). Ce scénario oet un gain de 16,Ceci signifie qu’
épistage pendant c
épistage du cancer
74 ans t, ce qui nombre
9. ails, voir mations, analyse
ostic de ualité de irmer les
observée -69 ans)
permet ALY pour certaines e puisse
c de 3%, de vie de e dépisté adre du optimiste ,3 QALY ’il serait cinq ans
CLppql’ahpbgd7
r du sein
CONCLUSLe dépistage estpopulation en évitprolonger le dépisquelques années influence d’un dé
aléatoire (niveau dhypothèses raisonperte en terme debalance bénéficesglobale de bien-êd’étendre le dépis70 à 74 ans.
ION t organisé dans ant notamment dtage jusqu’à l’âgede vie pour un
épistage organisé de preuve très fainnables, cette intee qualité de vie. Ds-risques de ce dêtre de la populstage organisé du
le but d’améliores décès prématu
e de 74 ans devracertain nombre dsur la qualité de ble car basé sur uervention pourrai
Dans ces conditiondépistage pencheation. Il n’est do
u cancer du sein a
rer le bien-être durés. Il est certain
ait permettre de gade femmes. Toutvie est nettemenun modèle). Selot même aboutir àns, il se pourrait qe du côté d’une onc pas recommaux femmes âgée
v
de la n que agner tefois, t plus n des à une que la perte
mandé es de

vi
RECO
a Le KCE re
OMMAND
este seul responsab
DATIONS
ble des recommand
Dé
Sa
• L’invitorgan
• Si unedépistdes in
• Toute de qul’enregorientexigen
• Afin dil impodesso
ations faites aux au
épistage du cancer
tation systématiisé du cancer du
e personne de tage, il importe q
nconvénients pot
mammographiealité, dont notamgistrement et leront la personnnces de qualité.
de minimiser le riorte que le taux
ous du seuil défin
utorités publiques
r du sein
ique des femmeu sein n’est pas r
plus de 70 ans que le médecin vtentiels de celle-
e de dépistage dmment : le contr’optimisation dne qui demande
isque de perte dde rappel après
ni par les critères
es âgées de 70 recommandée.
demande une veille à ce qu’elleci.
oit répondre auxrôle de la qualitéu taux de rap
e un dépistage v
e qualité de vie mammographies européens (<5%
à 74 ans à par
mammographie e soit bien inform
x exigences euroé des installationpel. C’est pour
vers une structur
lié aux résultatse soit le plus bas%).
KCE Report 1
rticiper au dépis
dans un objectmée des avantag
opéennes en mans, la double lecrquoi, les médere qui réponde à
faussement poss possible et res
176B
stage
tif de ges et
atière cture, ecins à ces
sitifs, ste en

KCE Report 176
TABL
6
LE OF COONTENTLILILI
1.2.3.3.3.
4.4.
4.
4.
5.6.
S
TS ST OF FIGURESST OF TABLES .ST OF ABBREVI
SYNTHÈSCONTEXTQUESTIODESCRIPT
1. APPROCH2. APPROCH
3.2.1. O3.2.2. O3.2.3. FMÉTHODO
1. ESTIMATI4.1.1. D4.1.2. A
2. ESTIMATI4.2.1. D
3. APPROCH4.3.1. M4.3.2. D4.3.3. H4.3.4. A4.3.5. ARÉSULTADISCUSS
Screening Breast C
S .......................................................IATIONS .............
SE ........................TE ........................NS POSÉES .......TION DE LA PROHE INTUITIVE .....HE ÉPIDÉMIOLOObjectif à court terObjectif ultime .......Faux positifs et diaOLOGIE ..............ION DES BÉNÉF
Diminution de la mAmélioration de la ION DES INCONV
Diminution de la quHE PAR MODÉLIMesures de la quaDescription du modHypothèses de basAlimentation du moAnalyse de sensibATS ......................ION .....................
Cancer
............................
............................
............................
............................
............................
............................OBLÉMATIQUE .............................GIQUE ...............
rme ..................................................agnostics excéden............................ICES DU DÉPIST
mortalité ................qualité de vie des
VÉNIENTS DU Dualité de vie des pSATION ..............
alité de la vie ........dèle ....................se ........................odèle ...................ilité ..............................................................................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................ntaires .............................................
TAGE ...............................................s patientes ...........ÉPISTAGE ..........participantes ........................................................................................................................................................................................................................................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
1
...... 4
...... 4
...... 5
...... 7
...... 7
...... 7
...... 8
...... 8
...... 8
...... 9
...... 9
...... 9
.... 11
.... 11
.... 11
.... 11
.... 11
.... 11
.... 12
.... 12
.... 12
.... 14
.... 14
.... 14
.... 15
.... 15

2
6.6.
7.7.7.7.8.
1.1.1.1.1.1.2.2.
2.
S
1. AJOUTER2. AJOUTER
6.2.1. T6.2.2. F6.2.3. ECONCLUS
1. FAUT-IL P2. QUE REP3. MESSAGE
RÉFÉREN
SCIENTIFINTRODU
1. CONTEXT2. SCOPE O3. BREAST C4. CLINICAL5. SCIENTIF
LITERATU1. REVIEW O
2.1.1. M2.1.2. D2.1.3. D2.1.4. S2.1.5. K2.1.6. C
2. REVIEW O2.2.1. L2.2.2. S
Screening Breast C
R DES ANNÉES ÀR DE LA (QUALITTraitements moinsFaux positifs .........Excès de diagnostSIONS .................PROLONGER LE ONDRE A LA PEE CLÉ ..................NCES ...................
FIC REPORT ........CTION ................
T OF THIS REPOOF THIS REPORTCANCER SCREE QUESTIONS .....
FIC APPROACH ..URE REVIEWS ...OF CLINICAL STUMethodology .........Description of screDescription of screScreening conditioKey data ...............Conclusion ............OF MODELING SLiterature search sSelection criteria ...
Cancer
À LA VIE ? ...........É DE) VIE AUX A
s agressifs? .....................................tics et de traiteme............................DÉPISTAGE JUS
ERSONNE QUI DE........................................................
............................
............................RT ......................
T ...........................ENING IN BELGIU....................................................................................UDIES .............................................
eening benefit ......eening harms .......ons ...............................................................................
STUDIES ..............strategy ...........................................
............................ANNÉES ? ...................................................................
ents ...................................................SQU’À L’ÂGE DEEMANDE UN DEP........................................................
............................
............................
............................
............................UM ....................................................................................................................................................................................................................................................................................................................................................................................................
............................
............................
............................
............................
............................
............................ 74 ANS ? ..........PISTAGE? ..................................................................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
KCE Report
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
t 176
.... 15
.... 16
.... 16
.... 16
.... 16
.... 16
.... 16
.... 17
.... 17
.... 18
.... 19
.... 19
.... 19
.... 19
.... 19
.... 20
.... 20
.... 21
.... 21
.... 21
.... 22
.... 25
.... 27
.... 28
.... 29
.... 29
.... 29
.... 29

KCE Report 176
6
2.
3.3.3.3.
3.3.4.4.4.4.4.4.4.4.
S
2.2.3. Q2.2.4. S2.2.5. C
3. REVIEW O2.3.1. M2.3.2. R2.3.3. DDECISION
1. DATA SOU2. MODEL D3. DESCRIPT
3.3.1. A3.3.2. B3.3.3. P3.3.4. P3.3.5. R3.3.6. S3.3.7. S3.3.8. Q
4. RESULTS5. DISCUSS
ANSWER 1. BREAST C2. DELAY BE3. OVERALL4. MORBIDIT5. FALSE PO6. ADDITION7. OVER-DIA
Screening Breast C
Quantity of researcSelected studies ...Conclusion ............OF QUALITY OFMethods ................Results .................Discussion ............N ANALYSIS .......URCES ...............
DESCRIPTION .....TION OF THE PA
Age specific overaBreast cancer incidParticipation rate ..Proportion of screeRecall rate ............Stage distribution aStage specific relaQALY ....................S ...........................ION .....................TO CLINICAL Q
CANCER RELATEETWEEN THE SCL MORTALITY .....TY ........................OSITIVE OR FALSNAL DIAGNOSTICAGNOSIS AND O
Cancer
ch available .................................................................LIFE STUDIES ...........................................................................................................................................................................ARAMETERS ......all survival ............dence ..............................................en detected breas............................and stage shift ....
ative survival ............................................................................................
QUESTIONS .........ED MORTALITY .
CREENING AND T........................................................SE NEGATIVE RC TESTS .............
OVER-TREATMEN
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................st cancers ............................................................................................................................................................................................................................................THE MORTALITY........................................................ESULTS ..........................................
NT ........................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................Y REDUCTION ...............................................................................................................................................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
3
.... 30
.... 30
.... 33
.... 33
.... 34
.... 35
.... 43
.... 43
.... 44
.... 44
.... 48
.... 48
.... 48
.... 48
.... 48
.... 48
.... 49
.... 50
.... 51
.... 54
.... 58
.... 60
.... 60
.... 60
.... 60
.... 60
.... 60
.... 60
.... 60

4
LIST OF F
LIST OF T
FIGURES
TABLES
4.5.
FiFiFiFi
TaTaTaTawoTaTaTaTaTapaTaTaTa
S
8. WHAT ATREFEREN
gure 2.1: Health sgure 2.2: Percentgure 3.1: Compargure 3.2: Compar
able 2.1: Data issuable 2.2: Selectionable 2.3: Modelingable 2.4: results omen screened foable 2.5: Article seable 2.6: Health stable 2.7: Descriptable 2.8: Descriptable 3.1: Stage diarticipants, age 50able 3.2: Parametable 3.3 Modelingable 3.4 Modeling
Screening Breast C
TTITUDE SHOULDNCES ...................
states for which uttage change in utirison of the two cortments in the two
ued from clinical ln criteria ..............g studies excludedof the different m
or the different moelection criteria ....tates descriptionsion of a “false posion of the selectedistribution among 0-69, Flemish screters used in the m results: baseline results: sensitivit
Cancer
D BE RECOMME............................
tilities are neededlities ....................
ohorts with and wo cohorts and the t
iterature review ..............................d after full-text assmodels in terms oodels ................................................s for the study of Lsitive” state (Gerad utilities .............screen detected
eening program 2model ....................
, worst and best cty analysis. ..........
NDED FOR WOM............................
d (reflection proce............................ithout a screeningtransitions betwee
............................
............................sessment ............of mortality reduc........................................................
Lidgren et al. ........rd et al)83 .........................................breast cancers, i001-2006. .......................................
case scenario. .................................
MEN IN CASE OF............................
ss) ..................................................g program ............en them ..............
............................
............................
............................ction and years o............................................................................................................................................nterval cancers a................................................................................................................
KCE Report
F SELF REFERRA............................
............................
............................
............................
............................
............................
............................
............................of life gained per............................................................................................................................................
and cancers amon................................................................................................................
t 176
AL?61 .... 62
..................
..................
..................
..................
.............
.............
.............r 1000 .................................................................ng non ....................................................

KCE Report 176
LIST OF A
6
ABBREVIAATIONS ABCPCCCIDCDEBCAHBCDNCIIMINICKCMMNINBNBNHNHNCQAQoRCRR
S
BBREVIATION PG CRT I CIS ET CSC HRQ CR NETB ISNET
MA/AIM NAMI/RIZIV CER CE ST -A IS BSS BCSP HS HS EED CI ALY oL CT R
Screening Breast C
DEFINITION Clinical PracticCochrane CenConfidence IntDuctal CarcinoData ExtractioBreast CancerAgency for HeBelgian CanceDutch NationaCancer InterveIntermutualistiNational InstituIncremental coBelgian HealthMean Sojourn Meta-analysisNational InstituCanadian NatiNorwegian BreNational HealtNHS EconomiNational CancQuality AdjusteQuality of LifeRandomized CRelative Risk
Cancer
ce Guideline ntral Register of Cterval oma in situ on Table r Surveillance Con
ealth Care Researer Registry al Evaluation Teamention and Surveic Agency ute for Health andost-effectiveness rhcare Knowledge
Time
ute for Statistics ional Breast Canceast Cancer Screeth Service (UK) c Evaluation Data
cer Institute (USA)ed Life Year
Controlled Trial
Controlled Trials
nsortium (USA) rch and Quality
m for Breast cancellance Modelling N
d Disability Insuranratio Centre
cer Screening Stuening Programme
abase )
er screening Network
nce
dy es
5

6
SESRSTTTUKUSUS
S
EER R T TO K SA SPSTF
Screening Breast C
Surveillance, ESystematic ReSojourn TimeTime-trade-offUnited KingdoUnites States US Preventive
Cancer
Epidemiology andeview
f om of America
e Services Task F
d End Results (US
orce
SA)
KCE Reportt 176

KCE Report 176
SYNT
6
THÈSE
SScreening Breast C
1Lradd4radral’soCl’SpSdaa
2Ll’àLla
Cancer
1. CONTEXLe KCE a déjà puapport de base
dépistage du cancde risque. Le dépi40-49 ans a fait l’oapport (rapport
dépistage systémapport (rapport 1indentification de
sein. Le rapport organisé du canceCette question esaugmentation rég
Si la plupart desprolongation, les Seuls quatre Etatd’âge des 70-74 autres pays insisteavec elles la prise
2. QUESTILe dépistage orgaâge de 74 ans? S
à la personne qui dLa première questa seconde, les pre
XTE blié trois rapportspublié en 2005
cer du sein en géstage du cancer d
objet d’une mise àN° 129 du KCEatique des femm
172 du KCE), pues femmes expos
actuel pose la er du sein aux femst régulièrement gulière de l’espérs groupes actifs autorités publiquts membres de (la France, les Pent sur la nécesside décision.
IONS POSÉanisé du cancer Si la réponse à cedemande ce dépition concerne plusestataires de soin
s sur le dépistage(rapport N°11 d
énéral, dans la podu sein des femmà jour partielle pubE), le KCE ne
mes de moins de ublié en 2012, a sées à un risquequestion de l’ex
mmes âgées de 70adressée aux po
rance de vie de ldans le dépista
ues font preuve dl’Union européen
Pays-Bas, l’Espagté d’informer les f
ÉES du sein devrait-il
ette question est nstage? s spécifiquement
ns.
du cancer du seu KCE) concern
opulation sans facmes de la tranche bliée en 2010. Darecommandait pa50 ans. Le troisposé le problèm
e accru de cancextension du dépi0 à 74 ans oliticiens en raisoa population fémage demandent de moins d’unannne ciblent la tragne et la Suède)1
femmes et de par
être prolongé junégative, que répo
les pouvoirs publ
7
in. Le ait le
cteurs d’âge ns ce as le sième
me de er du stage
on de inine. cette imité.
anche . Les
rtager
squ’à ondre
lics et

8
3. DESC3.1. ApprocDe façon intuitgénéralement edémontrée par aux Etats-Unis est une bonne diagnostiquer utemps. L’enthod’entre eux le impératif moral3
Cette attitude précoce des cirréalistes de ltéléphoniques psein et le bénrépondantes cprogressive unforme curable ecancer du sein précoce, il grafemmes estimacancers mortelsSchwartz a soupeut détecter ddes répondantefaire de tort à uLe corps médimanière adéqusur le taux del’objectif final dcliniciens parais(faux négatif) q
RIPTION Dhe intuitive tive, le dépistageenthousiastes à l
Schwartz au déa révélé que 87
idée. Trois quart dun cancer à un susiasme des répdépistage n’éta
3. générale que no
cancers sauve dela part des femmpour évaluer coméfice du dépistagconsidérait le c
niforme et croyaitet silencieuse. Enn'est pas détecté
andit, se propageaient que les cancs) sont liés à un éuligné que 94% dedes cancers qui nes sont persuadéne personne qui ncal lui-même n’aate. C’est ainsi qu cancers diagnos
du dépistage est ssent plus sensibu’aux risques liés
DE LA PRO
e du cancer fait l’égard du dépista
ébut du 21e siècle% des adultes codes personnes intstade précoce sa
pondants était si it pas une décis
ous pouvons réses vies” peut avmes. Silverman ment les femmesge par mammogcancer du sein t que tous les can résumé, ces femé par une mammoe et tue. Fortescers avancés (et séchec au niveau des femmes ne savne vont jamais p
ées du fait que lan'a pas de cancerappréhende pas ue de nombreux cstiqués (objectif de diminuer la m
bilisés au risque d aux résultats fau
S
OBLÉMATIQ
sens. Les médage. Cette attitude2. Une enquête onsidéraient que terrogées déclaraauve la vie la plufort que pour la sion à prendre m
sumer ainsi “la dvoir suscité des a réalisé des in considèrent le caraphie4. La majo
comme une ancers débutent mmes pensaient qographie et traité ds de ces croyansans doute la pluu dépistage précovent pas que le dé
progresser. De plua mammographie r du sein5. toujours le dépiscliniciens restent fintermédiaire), al
mortalité. D’autre de méconnaître unssement positifs.
Screening Breast C
QUE
ias sont de a été réalisée dépister
aient que upart du majorité mais un
détection attentes terviews ancer du orité des
maladie par une que si le de façon ces, les part des oce. épistage us, 92% ne peut
stage de focalisés lors que part, les n cancer
3LBtrLc7Nmred7p7
C
1
2
3
4
Rd
Cancer
3.2. ApprocheLe cancer du seBelgique, 10.849 crois quarts des caL’âge moyen au cancer du sein est70 à 75 ans6. Néanmoins, la pamortalité totale diffesponsable de 18
de 13% dans le g74 ans (Rapport pour les femmes â7% pour le groupe
Caractéristiques fo
. Le dépistagContrairemeune plainte dépistage es
2. Le dépistage la maladie.
3. Le dépistage liée à la mala
4. Le principe “pce qui concer
Rappelons que pde 990 sont indem
épidémiologiqin est le cancer cancers du sein oancers du sein somoment du diag
t de 370,7/100.00
rt relative de la mfère en fonction d8% des décès chroupe de 60 à 64N°11 du KCE). Eâgées de 50 à 54
e des 70 à 74 ans
ondamentales d’u
e s’adresse à ent au patient qu
ou d’un symptôst présumée inde
a pour objectif à
a pour objectif udie.
primum non nocerne le dépistage.
pour mille femmemnes du cancer
que le plus fréquen
ont été diagnostiqont diagnostiqués gnostic est de 6200 dans le groupe
mortalité due au ce l’âge. En 1999,
hez les femmes â4 ans et de 6% dEn 2006, cette pr4, 12% pour le gret 5% pour le gro
un dépistage:
des personneui consulte son môme, la personnemne de la malad
à court terme de c
ultime de diminue
re” est particulière
es dépistées entdu sein.
KCE Report
t chez la femmequés en 2008. Pluaprès l’âge de 502 ans. L’incidencdes femmes âgé
cancer du sein da le cancer du sein
âgées de 50 à 54ans le groupe deroportion était de roupe de 60 à 64oupe des 75 à 79
es en bonne médecin en raiso
ne qui participe die recherchée.
confirmer l’absenc
r la mortalité/mor
ement d’applicatio
tre 70 et 74 ans,
t 176
e. En us de 0 ans. ce du es de
ans la n était 4 ans, e 70 à 14%
4 ans, ans6.
santé on d’ à un
ce de
rbidité
on en
plus

KCE Report 176
3.2.1. ObjectLe dépistage apersonne quid’innocence” enqui consulte soconstaté quelqL’objectif du msituations sont diagnostique, leune étiologie àdépistage, le mindispensables.dépistage pour sein. Le formation dauprès de macontre-intuitif po3.2.2. ObjectDiagnostiquer développent etdépistage du cala mortalité spéLe fait que la tpeu avancées étape intermédmais qui n’est pOn peut égalemorbidité liée àinvasifs (masteévitant une part
6
tif à court terme a pour objectif d
participe au dn ce qui concerneon médecin parceque chose d’inh
médecin et les modiamétralement o
e médecin a le de la plainte ou au
médecin a le dev. Ceci afin de minr les 996 femmes
des médecins étlades, ce changeour un clinicien. tif ultime les cancers à t essaiment (méancer. C’est ainsi écifique à la malatechnologie utiliséet donc potenti
iaire dans ce procpas suffisante7. ement émettre l’à la maladie, en pectomies partielletie des évolutions
e confirmer l’absépistage bénéfice le cancer du see qu’elle a une pabituel, devientoyens à mettre eopposés. Dans leevoir de tout mett symptôme. A l’inoir de pratiquer unimiser les risque (/1.000) qui sont
tant essentiellemement de point
un stade précoétastases) est l’h
que l’on attend dadie et conséquemée permette de dellement curablecessus. Il s’agit d
’hypothèse que permettant l’utilisas plutôt que mas vers les stades m
S
sence de la malacie de la “présin. A l’inverse, la
plainte ou parce q“suspecte” de m
en œuvre dans ce cas d’une mise re en œuvre pournverse, dans le cuniquement les e
es et les inconvént indemnes du ca
ent effectuée ende vue est franc
oce avant qu’ils hypothèse fondadu dépistage qu’il mment la mortalitdiagnostiquer deses ne représente’une condition né
le dépistage rédtion de traitementstectomies totalesmétastatiques.
Screening Breast C
adie. La somption patiente
qu’elle a maladie.
ces deux au point r trouver cadre du examens nients du ancer du
n hôpital chement
ne se trice du diminue
té totale. s lésions e qu’une cessaire
duise la ts moins s) et en
3AlaacaLddpcPledccqppénC(vsd
Cancer
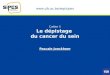
3.2.3. Faux posAvant d’instaurer ua balance avantaavantages. Pour contrebalancer la aux risques induitsLes résultats ditsdehors de la présedépistage du cancpositifs créent decomplémentaires. Plus encore que lee risque majeur diagnostic excédecancer dont l’évocliniquement en l’aque le cancer espersonne est faibpopulation. Très évoluent tellemenn'altèreront pas la Ce rapport a pourvoir Figure 1) de
s’assurer que les de qualité de vie.
sitifs et diagnostiun dépistage orgaages/inconvénience faire, l’ampleperte de qualité ds par le dépistages: “faux-positifs” ence d’un cancer)cer du sein les ple hauts niveaux
es faux–positifs, ldu dépistage de
entaire peut se déolution est telle absence de dépisst d’évolution lenble. Ce risque epeu de femmes
nt lentement quesanté9.
r objectif de quantce dépistage afin bénéfices l'empor
ics excédentaireanisé, il est nécesnts du dépistage eur de la diminude vie consécutivee.
(suspicion de l) sont les effets nus fréquents. Ces
x d'anxiété et so
e risque de diagns femmes âgées
éfinir comme le faqu’il ne se se
stage8. Ce risque nte et que l’espest particulièreme
savent en effet e même s'ils ne
tifier les avantagede pouvoir les m
rtent largement su
es ssaire de s’assure
penche du côtéution de mortalitée aux inconvénie
ésion cancéreuségatifs indésirables résultats fausseont suivis d’exa
nostic excédentairs de 70 à 74 anait de diagnostiqurait jamais manest d’autant plus
pérance de vie dent méconnu da
que certains cae sont pas traité
es et les inconvénmettre en perspect
ur les risques de
9
er que é des é doit nts et
se en es du
ement mens
re est s. Le er un ifesté élevé de la ns la ncers és ils
nients tive et perte

10
Figure 1 mise
Dépistmammo
en perspective d
tage par ographie
des avantages et
Normal
Anormal
S
t des inconvénie
Faux-néga
Résultat +
Faux-pos
Résultat -
Screening Breast C
nts potentiels du
atif
+
sitif
Réin
Ré
Ex
Caninva
Ca
in
Cancer
u dépistage.
éassurance nadéquate
éassurance
xamens compléme
ncer asif
ancer
n situ
Diagnostic r
entaires
Traitement précoce
Traitement précoce
retardé
Diminutde morta
Surtrait
KCE Report
tion alité
tement
t 176

KCE Report 176
4. MÉTHNous avons recdans la littératudonnées nationsuivant les prodans le chapitre
4.1. Estimat4.1.1. DiminuLes principalessein, sont issueessais, on peut1. Le dépista
période debénéficié d
2. Cette diminans après l’espérancede ce grou(données b
Les données ppeuvent donneun seul essai rades femmes âparticipant à cepouvoir mettremortalité. De pl
6
ODOLOGIcherché des élémure clinique, dansnales et internatiocédures en viguee 2 du rapport scie
tion des bénéfiution de la mortas données probanes de huit essaist retenir deux consage entraîne une e suivi de 13 ans d’un dépistage tounution de mortalitle dépistage. Il c
e de vie de la popupe d’âge est de belges de 2009). probantes issues r une réponse coandomisé, l’étude
âgées de 70 à 7et essai était trop f en évidence uus cette étude éta
E ments de réponses les études de
onales. Ces recheeur au KCE. Ellesentifique.
ces du dépistaalité ntes relatives au s contrôlés randostats principaux:diminution de m
pour les femmes us les deux ans. é se manifeste prconvient de la mepulation-cible. L’es
16 ans à 70 ans
de ces essais cmplète à notre qu
e suédoise dite de74 ans et le nofaible (10.000 poun effet statistiquait entachée de bi
S
aux questions prmodélisation et d
erches ont été mes sont décrites en
age
dépistage du caomisés. Sur base
mortalité de 23% de plus de 50 an
rincipalement entrettre en perspectispérance de vie ms et de 13 ans à
contrôlés randomuestion de base. Ees “Two County”, mbre de septuagur les deux group
uement significatifiais méthodologiq
Screening Breast C
récitées, dans les enées en n détails
ancer du e de ces
sur une ns ayant
re 4 et 7 ive avec
moyenne à 74 ans
misés ne En effet, a inclus
génaires es) pour f sur la ues.
4LpmlecLl’immaLp(dIIétrh
44Lp1
2
Cancer
4.1.2. AmélioraLe dépistage ayapetite taille, un demoins agressifs. Nes données factucette attente. Les essais contrôévolution vers lempossible d’infirmmorbidité sur cetteaux métastases esLes données bepermettent pas derapport KCE 150)
de mastectomies I). Près de 90% dégalement un traitraitement de chhormonal.
4.2. Estimation4.2.1. DiminutioLe dépistage provpersonnes dépisté
. Les résultats patientes comcomplémental'inquiétude patelles que les
2. Les diagnosticdiagnosis andscientifique) clourds dont dela survie de la
tion de la qualitént pour objectif des avantages atteNi les données isselles recueillies e
lés randomisés nes stades métasmer ou de confe base. Par contrst inclue dans le melges dont noue valider cette as) font état de 58%totales dans les des bénéficiaires tement par radiothimiothérapie né
n des inconvénon de la qualité dvoque une diminutées. Ceci s'expliqu
faussement posmme de vrais posires n’ont pas pear rapport au cancponctions mammcs excédentaires d over-treatment,conduisent à des es amputations m
a personne.
é de vie des patide mettre en évidendus est de permsues de essais coen Belgique, ne pe
n’ont quantifié ni statiques de la firmer l’hypothèsere, la perte de qumodèle décrit ci-ds disposons acsertion. Les donn
% de chirurgie constades les moinsde la chirurgie c
hérapie, 38% d’eéo-adjuvante et
nients du dépisde vie des partiction de la qualité due par une série dsitifs du dépistagesitifs, aussi longteermis de les infirmcer du sein et aux
maires. et les traitements
, pour plus de dinquiétudes grave
mammaires qui n’o
ientes dence des tumeumettre des traitemontrôlés randomisermettent de conf
le taux de récidivmaladie. Il est
e d’une réductioualité de vie impuessous. ctuellement ne nées les plus récnservatrice versuss avancés (Stadeconservatrice reçontre elles reçoive
41% un traite
stage cipantes de vie d’une partiede facteurs: e sont perçus pamps que les exa
mer. Ils provoquex procédures inva
s qui les suivent (détails, voir le raes et à des traitemont pas d’influenc
11
rs de ments és, ni firmer
ves ni donc
on de utable
nous entes
s 38% s I et oivent ent un ement
e des
ar les mens
ent de asives
(over-apport ments ce sur

12
3. L’avance a
de vie en ble cancer ppatiente dede sa viindépendad’évoluer, sans que influencer s
4.3. ApprocLes revues de le poids des bspécifique danrechercher les dépistage et à l4.3.1. MesureDifférents instrCertains instrumpar exemple, latteintes d'un cTreatment of Cfonctionnementpas possible dimensionnellesindice global d(QALY). Les Qde vie. Les recommanle questionnairest un des meAvec cet instruen prenant enpersonne, les dépression. Popossibles. Cell
au diagnostic peubonne santé. Le dplus précocementevient de ce fait me. Toutefois, snte de son cancelle aura été “macette avance au
son espérance de
he par modélislittérature précitée
bénéfices et des s ce but. La coétudes relatives àa qualité de vie d
res de la qualité uments sont dispments sont spécle questionnaire
cancer du sein de Cancer (EORTC).t physiologique, lde prendre en s dans un modède qualité de vieALYs sont le nom
dations pharmace appelé EQ-5D eilleurs instrumenment, la qualité d compte cinq di
activités couraour chacune de ces-ci reflètent le
ut entrainer une pdépistage a pour t que ne le ferait umalade du canceri cette patientecer avant que cealade du cancer” u diagnostic et ae vie10.
sation es ne nous ayantrisques, nous avnstruction de ce à la qualité de viees patientes au cde la vie ponibles pour meifiquement adaptrelatif à la quall'European Organ
. Ces outils évalua peur de la réccompte ces do
èle. Elles doivene, à savoir, le Qmbre d’années de
co-économiques d(European Qual
nts disponibles pde la vie liée à l'émensions: la moantes, la douleces dimensions, niveau de sévé
S
perte de plusieursobjectif de diagn
un diagnostic clinr plus tôt dans le e décède d’uneelui-ci n’ait eu lequelques annéesau traitement n’a
t pas permis de qvons construit un
modèle a nécee des femmes peours de leur mala
esurer la qualité és à la maladie, ité de vie des pnization for Reseauent l'image du cidive… Toutefois
onnées de santént être convertiesQuality-Adjusted Le vie ajustées à la
du KCE, considèrity of Life-5 Dime
pour évaluer les tat de santé est m
obilité, l’autonomieur/la gêne, l’a
plusieurs réponsrité du problème
Screening Breast C
années nostiquer nique. La
décours e cause e temps s trop tôt aient pu
quantifier modèle
ssité de endant le adie.
de vie. comme
patientes arch and corps, le , il n'est é multi-s en un Life-Year a qualité
rent que ensions) QALYs.
mesurée ie de la nxiété/la ses sont e (aucun
ppsdpdbs1
2
PcssLcqrémplele4LcL
Cancer
problème, quelquproblèmes gravessoit en ce qui concdu cancer du seinpersonnes atteintd’identifier trois étbase de ces étudesont estimées com
. La perte de faussement ppour infirmermoyenne 45données AIM
2. Pour les patiele diagnostic (estimée à 16Pendant les a6% pour les pour les stade
Plusieurs limitatiochiffres avec précsaxons. Le questiosanitaires généralLes mesures conccompte l’impact questionnaire ayaésultats ne reflè
malades ne pouvapourraient expliques patientes ayanes patientes ayan4.3.2. DescriptioLe modèle compaconstituées de 10Le schéma ci-dess
ues problèmes, ) Ce questionnaircerne le dépistagn et en ce qui coes de ce cancertudes qui correspes, les variations mme suit:
qualité de vie copositif est estiméer ce faux positif.5 jours (minimum (Agence Intermu
entes cancéreuse(quel que soit le t% pour les stade
années suivantes,stades I,II,III. Ce
es IV. ons de cette appcaution. Il s’agit donnaire utilisé, à es et non les dimcernant les patienà court terme d
ant été utilisé lorètent pas la quaant plus se déplacer le faible changnt un cancer du snt développé des mon du modèle are deux cohorte0.000 femmes dosous représente c
des problèmesre est soumis à la e, une populationoncerne la maladr. La revue de londaient à nos cde la qualité de v
onsécutive à un e à 16% pendant . En Belgique, cm 36, maximum utualiste) s et pendant la praitement), la pert
es I, II, III et à 18 la perte de qualitette perte demeu
proche nous obligde résultats provsavoir, l’EQ-5D m
mensions spécifiquntes ne prennent qdu diagnostic etrs des consultatioalité de vie des cer. Les particulagement de qualitésein et la populatmétastases et cel
es théoriques. Ceont l’évolution est cette évolution:
KCE Report
s modérés, ou population conce
n de femmes indedie, une populatiola littérature a p
critères d’inclusionvie des septuagén
résultat de dépila période néces
cette période dur54 jours) selon
remière année qute de qualité de v
8% pour les stadeté de vie est estimure stationnaire (
gent à interprétevenant de pays amesure les dimenues au cancer du que sommairemet de la chirurgieons ambulatoires
patientes graverités de l’étude ut
é de vie constaté tion générale ou les qui n’en ont pa
es deux cohortessuivie jusqu’à la
t 176
des ernée, mnes on de ermis
n. Sur naires
stage ssaire re en n les
ui suit vie est es IV. mée à (18%)
r ces anglo-nsions
sein. ent en e. Ce s; ses ement tilisée entre entre as.
s sont mort.

KCE Report 176
Cohort
Cohorte
6
Femmes invitées
Femmes non invité
te A
e B
(1) diadép
(4)sit
(2)
(3dgrpa
es
(6dgrin
(7indn
S
cancer invasif gnostiqué lors du pistage
) Cancer canalaire in u
cancer d'intervalle
3) cancer invasif iagnostiqué dans le roupe des non‐articipantes
6) cancer invasif iagnostiqué dans le roupe des non‐nvitées
7) Cancer canalaire n situ diagnostiquédans le groupe des non‐invitées
Screening Breast C
IIIIIIIV
IIIIIIIV
IIIIIIIV
IIIIIIIV
Cancer
(5) Décèscauses co
(8) Décèscauses co
(toutes onfondues)
(toutes onfondues)
13

14
La cohorte A illjusqu’à 74 ansParmi celles-ciet d’autres non cohorte sont rédépistage (1), sessions de dédes invitées/nopeuvent survendans le groupedes femmes cole cancer du seLa cohorte B (cmembres de cefemmes serontcanalaire in situcohorte décèdeLe cancer du sstade le moins d’autant plus lodiagnostic. 4.3.3. HypothL’hypothèse dedépistage, la prque parmi les bénéfice du déstades (stage-sL’autre hypothèfemmes dépenfemme au momdépistage. Les cohortes sparamètres deannée (incidenc
ustre l’hypothèses. Elle est consti, certaines partic(invitées/non-par
épertoriés. Il s’agsoit de cancers dépistage (2), soit on-participantes (nir dans le group
e des invitées/nononstituant cette coein (5). cohorte de contrôette cohorte ne st atteintes d’un u (7). La très granera d’une autre affsein évolue en quavancé. La survie
ourd et plus invas
hèses de base e base est la suiroportion de stade
cancers diagnosépistage provientshift) consécutive èse retenue est dent uniquement
ment du diagnost
sont suivies d’anne transition tels lce) et le taux de s
e d’une prolongatioituée des femmeipent au dépistagrticipantes). Les cgit soit de cancediagnostiqués dade cancer diagn
(3). Enfin, les cape des invitées/pn-participantes (4)ohorte décèdera
ôle) correspond àsont pas invitées cancer invasif (6
nde majorité des fection que le canuatre stades (I, II,e est d’autant mosif que le stade e
ivante: parmi les es peu avancés (Istiqués sur baset des différencesau dépistage. que la survie e
t du stade de la tic, que celui-ci s
née en année et le nombre de fe
survie en fonction
S
on du dépistage oes invitées au dége (invitées/particcancers survenanters diagnostiqués ns l’intervalle ent
nostiqués dans leancers canalairesparticipantes tout ). La très grande d’une autre affec
la situation actueau dépistage. C
6), d’autres d’unfemmes constitua
ncer du sein (8). III, IV). Le stadeins bonne et le trast avancé au mo
cancers détectéI et II) est plus im
e de la clinique. s dans la répartit
et la qualité de tumeur et de l’âg
soit consécutif ou
évoluent en fonemmes atteintes du stade du canc
Screening Breast C
organisé épistage. cipantes) t dans la
lors du tre deux
e groupe s in situ
comme majorité
ction que
elle. Les Certaines n cancer ant cette
e I est le aitement ment du
s par le portante Tout le
tion des
vie des ge de la non au
ction de chaque
cer.
4PndLdfocisBUmla“4Dsnàpdad
a
Cancer
4.3.4. AlimentatPour réaliser cet enotre modèle avedétails dans le chaL’espérance de vide la population fonction de l’âge ecancer (Communassues des prograBruxelles et en CoUne mesure de qmodèle. Le modèla situation la plus “Par essence, tous4.3.5. Analyse dDans notre modèsimplificatrices, ennécessité d’éviter à une incertitudeparamètres et dedifférents types d’iapprofondie utilisadécrits en détails d
citation attrib
tion du modèle exercice, nous avc des données bapitre 3.3. du rappe de la populatio
féminine belge duet des stades de lauté flamande). Lamme actuels (fommunauté Flamaualité de vie a étéle contient un casvraisemblable.
s les modèles sonde sensibilité èle, nous avonsn raison des dol’utilisation d’un m
e liée à la struce la source desincertitude, nous aant différents scédans la table 3.2 d
uée au statisticien G
vons autant que fbelges. Ces paramport. n étudiée provien
u même âge. L’inla maladie provienes données relati
femmes de 50-69ande). é appliquée à chas de base (base c
nt faux mais certa
émis un certain nnées dont nous
modèle trop compcture du modèle informations. Pavons réalisé uneénarios. Ces diffdu rapport scientif
George Box.
KCE Report
faire se peut, alimmètres sont décri
nt des tables de sncidence du cancnt du registre belgives au dépistage9 ans en Wallon
aque compartimecase) qui correspo
ins sont utiles”a
nombre d’hypoths disposions et plexe. Ce choix coe, au bon choix
Pour faire face àe analyse de sensférents scénarios fique.
t 176
menté its en
survie cer en ge du e sont nie, à
ent du ond à
hèses de la onduit x des à ces sibilité sont

KCE Report 176
5. RÉSULe scénario deans permettraitreprésente uned’années de vieL’analyse de sescénario optimiLe scenario pe20%, d’un taux vie de 0,19 perdrésultats). La actuellement daa été appliquéd’estimer un gapour 1000 femcertaines circonpeut aboutir à uLe scenario opd’un taux de fa0,13 perdurant la distribution dépistage orgapermet d’estimepour 1000 femnécessaire d’invpour gagner un
6
LTATS e base montre qut d’éviter 1,3 décèe réduction de 2e sauvées est estiensibilité du modèste . essimiste fait l’hyde faux positifs d
durant pendant 54distribution des
ans le cadre du dée au groupe dain de 8,7 annéemmes participantnstances, au demune perte en termetimiste fait l’hypotux positifs de 2%pendant 36 jourspar stades obs
anisé aux Pays-Ber un gain de 17,
mmes participant viter 62 femmes à QALY.
e la prolongationès pour 1000 fem21% des décès. imé à 13,1 et le gèle comprend un s
ypothèse d’un exde 10%, entrainan4 jours (temps nécancers dépisté
dépistage organisdépisté. Ce scénes de vie mais ut au dépistage. meurant tout à fae de qualité de viethèse d’un excéd
%, entrainant une ps. Ce scénario apservée actuellemBas (70-74 ans)0 années de vie
au dépistage. à participer au dé
S
du dépistage jusmes participantesGlobalement, le ain en QALY à 3,scénario pessimis
xcédent de diagnnt une perte de quécessaire pour infiés par stades oé en Flandre (50-nario pessimiste ne perte de 3,1 Ceci signifie qu
ait réalistes, le dée. ent de diagnosticperte de qualité dpplique au groupement dans le ca). Ce scénario oet un gain de 16,Ceci signifie qu’
épistage pendant c
Screening Breast C
squ’à 74 s, ce qui nombre
9. ste et un
ostic de ualité de irmer les
observée -69 ans)
permet QALYs
ue dans épistage
c de 3%, de vie de e dépisté adre du optimiste ,2 QALY ’il serait cinq ans
6Llafesdc
6LufeppfrLdEa2Ldtocredl’
Cancer
6. DISCUSLes résultats du ma situation de baemmes dépistéessensibilité. A l’invdes hypothèses ccertaines hypothès
6.1. Ajouter deL’augmentation deutilisés pour justifiemme âgée de population des spopulation des sréquence et les caLe nombre de dédeux fois et demi En fait, la populatians, 8% entre 60 2009). Les causes de dédécès dus au canous les décès encomme la mortalesponsables chac
décès, la part de dâge (KCE report
SSION modèle décrit ci-dese, le gain en ans. Ce résultat resverse, les QALYschoisies, allant dses plausibles, un
es années à la e l’espérance de er de poursuivre plus de 69 an
septuagénaires aexagénaires. Il nauses de décès.
écès observé danplus élevé que ceon féminine belgeà 69 ans et 20%
écès varient égalncer du sein passntre 70 et 75 ans.ité cardiovasculacune d’un peu pludécès consécutifs11).
essus indiquent qnnées de vie est ste fiable tout aus varient substand’un gain relativene perte en qualité
vie ? vie de la femme le dépistage du cs. Cet argumen
a les mêmes can’en est rien en
ns la tranche d’âgelui de la tranchee perd 4% de ses% entre 70 à 79
lement. En Belgiqse de 13% entre A cet âge, la mo
aire sont pratiqueus d’un tiers des s au cancer du se
ue en ce qui concde 13 ans pour
u long de l’analysntiellement en fonement faible à, é de vie.
est un des argumcancer du sein cht présuppose qu
aractéristiques qun ce qui concern
ge des 70-79 ane d’âge des 60-69s effectifs entre 50ans (Belgian life
que, la proportion60 et 64 ans à 6ortalité par canceement équivalentdécès. Parmi tou
ein diminue donc
15
cerne 1000
se de nction selon
ments hez la ue la ue la ne la
ns est 9 ans. 0 à 59
table
n des 6% de er tout es et us les
avec

16
6.2. Ajouter 6.2.1. TraitemOutre le gain enest de permedonnées issuesrecueillies en B6.2.2. Faux pDans notre modsource importafaussement pod’attente relativcomplémentairetermes de QAeuropéennes (3Flandre), le gai6.2.3. Excès Le risque de dipour les septua%, on peut s’at108 femmes sutrès vraisemblasurdiagnostic dD’autre part, tscreening deviecas de diagnosannées de vie q
de la (qualité dments moins agrn années de vie, ttre des traitems de essais contrô
Belgique, ne permepositifs dèle, les diagnostnte de perte de q
ositifs (pouvant avement élevé (45es peut amener à
ALY. Si on parvi3,5%) comme c’en en QALY est dede diagnostics eagnostic excéden
agénaires. Si nousttendre à ce que dupplémentaires aablement un traie 10 %, ce nombrtoutes les femmeennent malades dstic clinique. Cecqui leur restent.
de) vie aux annressifs? le principal avantaents moins agreôlés randomisés, ettent de confirme
tics ”faussement qualité de vie. Ualler jusqu’à 10%5 jours en moyeà un résultat totaent à garder ceest le cas dans e 3 pour 1000 femet de traitementsntaire est le risques appliquons un tadans chaque cohuront un diagnostement. Si nous re monte à 367. es dont le cancdu cancer deux oci a un impact n
S
nées ?
age attendu du déessifs. Toutefois,ni les données fa
er cette attente.
positifs” représenn taux élevé de r%) conjugué à uenne) pour les el du dépistage né
e taux dans les une région du p
mmes. s e majeur de ce déaux de surdiagnosorte de 100.000 f
stic de cancer et appliquons un
cer est diagnostiqou trois ans plus tnégatif sur la qua
Screening Breast C
épistage , ni les actuelles
tent une résultats un délai examens égatif en
normes pays (en
épistage stic de 3 femmes, subiront taux de
qué par tôt qu’en alité des
77LCdmdinréppdsLsjuLsdbqsLprécdv
Cancer
7. CONCLU7.1. Faut-il proLa conclusion de Cette affirmation d’autre part sur lemodèle démontredépistées. Toutefondiquent que le ésulter en une pe
pas décisifs en taparticulier d’un dédéfinition à un ispécificité impliquLes trois principessont: les principesustice ou d’équitéLes principes de bsuit: “Ne pas fairedoubler d’un devobienveillance”. Le qui fait intervenir lsens d’une préféreLe dépistage estpopulation en évitésultats obtenus
certaines situationde vie dans la tranviolation du princip
USIONS olonger le dépiscette étude est qest basée, d’une
e contexte spécifiqent un gain de 1ois, certaines hyp
résultat net duerte globale en quant que tels et doépistage organiséndividu qui n’exe d’être d’autant
s éthiques de bass de bienfaisance et le principe d’abienfaisance ou de de mal (primumoir de bienfaisancprincipe de justic
la dimension colleence pour les plust organisé dans tant notamment dpar le modèle n
ns, le dépistage pnche d’âge étudiépe de base ”primu
stage jusqu’à lue la réponse à ce part, sur les réque de cette que13 années de vipothèses qui sont prolongement d
ualité de vie. Ces oivent être interpré. Le dépistage oxprime ni plainte
plus vigilant auxse applicables note ou de non malfautonomie12.
de non malfaisancm non nocere) esce qui va de pairce ou d’équité estective des problèms faibles, les plus le but d’amélior
des décès prémane permettent papuisse affecter née. Dans ces condum non nocere”(ne
KCE Report
’âge de 74 anscette question estésultats du modèstion. Les résultae pour 1000 femt loin d’être irréaldu dépistage porésultats ne sont
rétés dans le conorganisé s’adresse ni demande. x principes éthiqutamment au dépiaisance, le princip
ce sont définis cost le premier. Il dor avec une attitudt: “cette préoccupmes de santé, dadémunis”12.
rer le bien-être daturés. Cependanas d’exclure que égativement la qditions, il y a risque pas faire de ma
t 176
s ? t non. èle et ats du mmes listes, ourrait
donc ntexte e par Cette ues11. stage pe de
omme oit se de de pation ans le
de la nt, les
dans ualité ue de l).

KCE Report 176
D’autre part, ledont l’espérancexiste certes dprononcée. Le être une raisonposée.
7.2. Que répLe contexte deen deux pointssur un plan indbien à cette sitpersonne est lpersonne en dfaire des choix sa conduite (achoix, il imporavantages et personnelle. Leéclairé sont déconsentement base de la lectudevrait idéalemIl convient égademande le déAinsi, une attitu• Information• Prise de d
patiente14.• Orientation
modalités m
6
e dépistage est nce de vie est la dans les autres respect du princ
n supplémentaire
pondre à la per cette question d
s: l’individu est deividuel. Le principuation. Ce principle principe de bécoule ; Il s’agit pour lui-même (a
utogestion)”12. Porte qu’elle soit c
des inconvéniee droit d’être inforécrits dans la loi éclairé de la patiure d’un documenent inclure un éch
alement que le mépistage, une straude articulée en tron spécifique à la trdécision en fonc
n de la personne minimisent les inc
ettement moins eplus basse. Cetranches d’âge
cipe de justice oude répondre par
rsonne qui demdiverge de celui demandeur et le ppe d’autonomie s’pe est défini comase, le respect de reconnaître laautodéterminationour que la persoclairement et corents du dépistarmé (Article 7) et belge relative auente ne peut être
nt d’information. Ilhange d’idées avemédecin dévelopatégie qui en miniois étapes peut êtranche d’âge ction de l’appréc
qui le souhaite veconvénients.
S
efficace pour les tte différence d’emais elle y es
u d’équité se révèla négative à la q
mande un dépise la question pré
problème doit être’applique particulime suit: ”le respede l’autonomie da capacité de l’inn et libre choix) enne puisse faire rrectement informage dans sa sle droit au conse
ux droits des patie obtenu uniquem s’agit d’un proceec le praticien. pe pour sa patiemise les inconvétre recommandée
ciation personnell
ers un dépistage
Screening Breast C
femmes efficacité st moins èle donc question
stage? écédente e évalué èrement
ect de la de cette
ndividu à et à régir
un libre mée des situation
entement ents. Le
ment sur ssus qui
ente qui nients13.
e:
e de la
dont les
Lnuracds
7Lppqqratebb
Cancer
Les critères définnotamment la suutilisés, la double appel1. En Belgiq
critères définis dad’orienter les femmstructures.
7.3. Message Le dépistage estpopulation en évitprolonger le dépisquelques années qualité de vie eaisonnables, cetterme de qualité dbénéfices-risques bien-être de la pop
nis dans le cadrurveillance de lalecture des mamue, les unités de ns le cadre du prmes qui demande
clé t organisé dans ant notamment dtage jusqu’à l’âgede vie. Toutefo
est nettement plte intervention pode vie. Dans ces
de ce dépistage pulation.
re du programmea qualité techniqmographies et l’omammographie a
rogramme européent explicitement
le but d’améliores décès prématu
e de 74 ans devraois, l’influence delus aléatoire. Seourrait même abconditions, il se ppenche du côté d
e européen prévque des équipemoptimisation du tauagréées répondanéen, il est donc loun dépistage ver
rer le bien-être durés. Il est certain
ait permettre de gae cette mesure selon des hypothboutir à une pertpourrait que la bad’une perte globa
17
voient ments ux de nt aux gique
rs ces
de la n que agner sur la hèses te en lance
ale de

18
8. RÉFÉR
1. Perry NL. EuroscreeniOncol.
2. Schwarmammoprevent
3. Schwarfor can8.
4. SilvermFischhomammo2001;2
5. Schwarwomendetectio2000;32
6. Belgian2004-2
7. Paulus Good CKnowleAvailabhttp://kc
RENCES N, Broeders M, deopean guidelinesing and diagnosis2008;19(4):614-2rtz LM, Woloshinography for womtion of breast canrtz LM, Woloshin cer screening in
man E, Woloshin off B. Women's vography: a qualit1(3):231-40. rtz LM, Woloshin
n's attitudes to faon of ductal carci20(7250):1635-40n Cancer Registr005. Brussels; 20D, Mambourg F,
Clinical Practice (Gedge Centre (KCEble from: ce.fgov.be/index_
e Wolf C, Tornbergs for quality assus. Fourth edition--22. n S. News mediaen in their 40s acer. JAMA. 2002;S, Fowler FJ, Jr.the United States
S, Schwartz LMviews on breast ctative interview st
S, Sox HC, Fiscalse positive manoma in situ: cros0. ry, editor. Cance
008. Bonneux L. [Brea
GCP). Brussels: BE); 2005 02/05/200
_en.aspx?SGREF
S
g S, Holland R, vourance in breast-summary docume
a coverage of scand tamoxifen for 287(23):3136-42.., Welch HG. Ents. JAMA. 2004;29
M, Byram SJ, Wecancer risk and sctudy. Med Decis
chhoff B, Welch ammography resuss sectional surve
er incidence in B
ast cancer screenBelgian Health Ca05. KCE Reports
=5221&CREF=93
Screening Breast C
on Karsa t cancer ent. Ann
creening primary
. husiasm
91(1):71-
elch HG, creening Making.
HG. US ults and ey. BMJ.
Belgium,
ing]. re 11
348
8
9
1
1
1
1
1
Cancer
8. MandelblaDraisma different benefits a19;152(2):
9. Woloshin HG. Womdebate. Ar
0. Mandelbladecisions among theClin Onco
1. Doumont organisé.
2. Gallois. DUNAFORM
3. USPSTF. Task ForMedicine 2
4. Woloshin mammogr2010;303(
att JS, Cronin KAG, et al. Effectscreening schednd harms.[Erratum:136]. Ann Intern S, Schwartz LM,
men's understandrch Intern Med. 20att JS, Silliman about the benefitse oldest old withol. 2009;27(4):487-D, Verstraeten
Santé en CommuDépister les caMEC, editor. MédScreening for Br
rce Recommend2011(151):716-26
S, Schwartz raphy screening: (2):164-5.
A, Bailey S, Berrs of mammogradules: model esm appears in AnnMed. 2009;151(10Byram SJ, Sox H
ding of the mam000;160(10):1434R. Hanging in s and harms of br
out a safety net o-90. K. Enjeux éth
unauté Française.ancers, mais à ecine. Paris; 2005reast Cancer: U.Sdation Statement6.
LM. The beneunderstanding t
KCE Report
ry DA, de Koningaphy screening ustimates of pot
n Intern Med. 20100):738-47.
HC, Fischhoff B, Wmmography scre4-40.
the balance: mreast cancer scre
of scientific eviden
hiques du dépi 2012(7):3-7. quelle condition
5. p. 72-7. S. Preventive Sert Annals of Int
efits and harmthe trade-offs. JA
t 176
g HJ, under tential 0 Jan
Welch ening
aking ening
nce. J
stage
n In:
rvices ternal
ms of AMA.

KCE Report 176
SCIE
6
NTIFIC RREPORT
S
T
Screening Breast C
11TbmRthreqoboos
1Tww
1Taaa2ecreinoddbth
Cancer
1. INTROD1.1. Context oThis report is a pbreast cancer scrmade a list of cRepresentatives ohe choice and theelated to each
questions(see KCover three KCE rebreast cancer screof 40-49 years (KCof women at risk foscreening (KCE re
1.2. Scope of This report focusewith mammograpwomen between 7
1.3. Breast caThe Belgian fedagreement in 200aged 50-69 yearsappropriate financ2001, Flanders, theach introduced acontext of alreademains quite freqn the age-group 5older women (>7dominant in the agdrops, mainly becaby means of diagnhat substitution o
DUCTION of this report artial update of teening publishedclinical questionsof stakeholders’ ore wording of the q
question and CE report 172)2. eports. A first KCEeening with mamCE report 129)3. or breast cancer aeport 172)2.
this report es on the extensiohy to older wom
70-74 years of age
ancer screeningderal and regio01 for an organis, to be organiz
cial resources suphe Walloon regionan organized scredy existing practquent in the Wallo50-69, but also a
70 years). In Flage-group 50-69. Iause organized scnostic mammograf screening mamm
he clinical practicd in 20051. Theres related to brearganizations wereuestions, to highlito score the
Selected questioE report published
mmography for woThe second is foand technical met
on of organized brmen. Eligible pope with average ris
g in Belgium nal governmentszed screening p
zed by the regiopplied by the feden and the Brusseeening programmtices. Indeed, opoon and Brussels among younger (4nders, screeningn the age-group 7creening stops at
aphy decreases amography by opp
ce guideline (CPGfore, the KCE exast cancer screee then invited to reight the main probrelevance of cl
ons were then did in 2010 is focuseomen in the age gcused on identificthods for breast ca
reast cancer screpulation is definek of breast cance
s signed a prorogramme for wonal governments
eral government. Sels capital region me within their sppportunistic screregion among wo
40-49 years of ag mammographies70-79 overall coveage 69. The covelso with 3%, indic
portunistic screeni
19
G) on xperts ening. eview blems linical vided ed on group cation ancer
ening ed as r.
otocol omen
s with Since have
pecific ening omen ge) or s are erage erage cating ing at

20
the age of 70 (including both screening) remWalloon region
1.4. ClinicaThis specific re1. What are c
screening i1.1. What
organi1.2. How lo
breast1.3. What
organi1.4. What
organi2. What are
organized sterms
2.2. Harms2.3. Harms2.4. Harms
3. What attitureferral?
is not frequent diagnostic or foll
mains at 18% in F(KCE report 172)
l questions port addresses thclinical benefits ofin women betweeis the effect of anzed screening onong is the delay bt cancer related mis the effect of anzed screening onis the effect of anzed screening onthe specific ha
screening in womof false positive o
s in terms of addits in terms of over-s in terms of overtude should be re
in Flanders. At low up mammogr
Flanders, 33% in )2.
he following questif an extension of
en 70 and 74 yearsn extension (70-74 the breast cancebetween the scree
mortality reduction?n extension (70-74 the overal mortal
n extension (70-74 morbidity? rms of an exte
men between 70 or false negative reional diagnostic te-diagnosis? treatment? ecommended for
S
this age, total craphies and oppoBrussels and 30%
ions: f breast cancer ors? 4 years) of breas
er related mortalityening and the as? 4 years) of breaslity? 4 years) of breas
ension of breast and 74 years?H
esults? ests?
women in case
Screening Breast C
coverage ortunistic % in the
rganized
st cancer y? sociated
st cancer
st cancer
cancer Harms in
e of self
1FpthemB(tacT
Cancer
1.5. Scientific For each clinical performed and disheir scientific coepidemiology, or models. To quanBelgian situation IMA/AIM), cancerables and construcycles. The methodology
approach question, a sys
scussed with the ompetency in se
health economicntify what the im
we applied dar registry and datucted a simple tim
used and the resu
stematic search support of extern
everal fields: gycs. For question
mplications of ourata from the Inta from the literat
me dependent Ma
ults are described
KCE Report
of the literaturenal experts choseynaecology, radion 3, we searcher findings are ontermutualistic Agure on the Belgiarkov chain with a
d in each chapter.
t 176
was en for ology, ed for n the gency an life nnual

KCE Report 176
2. LITER2.1. Review2.1.1. Metho2.1.1.1. SouA broad searcCDSR and DARfor systematic r2.1.1.2. SeaFor searching oin combination screening (or eEMBASE, the 'breast cancer'combined with(SR) or meta-an2.1.1.3. In- Databases werGerman. This r2004), thus wrestriction (Engselection basedwithout breastintervention (mdiagnosis testsanalysis or RC<75 years), anindependently b
6
RATURE REw of clinical studodology urces ch of the electroRE was conductedreviews (SR) and arch terms on Medline databwith usual langua
early detection) (following Emtre
and 'mammograpa standard searc
nalysis (M-A). and exclusion crre searched for Sreport is a update
we used a date lish, Dutch, Frencd on title, abstrat cancer and w
mammography), o, over diagnosis
CT), key questiond original publicaby 2 reviewers (FM
EVIEWS dies
nic databases Od in April 2011. Semeta-analysis (M
ase, the followingage: Breast neop(MESH) and mame terms were u
phy'. These MESHch strategy to ide
riteria SR and M-A in Ee of previous KCE
restriction (2004ch and German).act or full text wwithout particulaoutcome (mortaland over treatme (screening), age
ation. Relevant puM, JR).
S
OVID Medline, EMearch was conduc
M-A).
g MeSH terms welasms (MESH) an
mmography (MESused: 'cancer scrH and Emtree termentify systematic
English, French, DE report1 (search 4-2011) and a laInclusion criteria
were: population ar breast canceity, morbidity, a
ent), design (SR oe of population (>ublications were
Screening Breast C
MBASE, cted first
ere used nd mass SH). For reening', ms were reviews
Dutch or made in anguage used for (women
er risk), dditional or meta->70 and selected
2WquR2eresTeaTs2Tb(wwTu(wT2InwefuwTmd
Cancer
2.1.1.4. AdditioWe identified twoquestion 2. Therupdated by searchReviews from the2008). Additional hensure that no poeference lists of
screening3. The identified stueligible studies, available, the studThe description asearch are in Appe2.1.1.5. QualityThe methodologicbias were rated www.cochrane.nl
was conducted byThe methodologicusing the adeqwww.cochrane.nl
The results of the 2.1.1.6. Identifn the systematic were identified inexcluded on the bull and reviewed were included4-8. The reviews writtemortality as outcodiagnosis and the
onal evidence SR4, 5 as the mrefore the evidehing Medline and search date of thand searching otentially relevant f SR and of ou
dies were selectethe full-text was
dy was not taken innd results of the endix 1.1. ty appraisal cal quality of syst
using the check). The assessmen
y a team of two revcal quality of selecquate checklists ). quality appraisal afied systematic r
search for literan database searbasis of title and in more detail. O
en by Götzsche ome, those from review of Virnig8
more extensive soence-identified th the Cochrane Dthe two SR’s on
of reference lists wstudies were misur previous repo
ed based on titles retrieved. In cnto account. literature searche
tematic reviews aklists of the Dunt of the risk of bviewers (FM, JR).cted additional ev
of the Dutc
are in Appendix 1reviews ture reviews, 53
rches. The majoabstract; 10 citat
On the basis of t
and Nelson4, 5 aBiesheuvel and Jon ductal carcino
ource for the reserough those SRatabase of Syste(search date Nov
was also undertaksed. We also scaort on breast ca
e and abstract. Fcase no full-text
es and flow of st
and associated ritch Cochrane C
bias in the include. vidence was also h Cochrane C
.5.
citations on the ority of citations tions were retrievthe full text, 5 rev
are mainly focuseJorgensen6, 7 on ma in situ (DCIS)
21
earch R-was matic v-Dec ken to anned ancer
For all was
tudies
isk of Centre ed SR
rated Centre
topic were
ved in views
ed on over-.

22
As a first step,determine theirjudged to be ofupdate of onePreventive Tasquality and useThe review writappraisal of seJorgensen7 waswas also judged2.1.1.7. IdenThe evidence wsearching Medfrom the searchsearch for relevApril 2011) idenon the basis offull and reviewstudies were exthe flow of randBy hand searcSwedish RCT’sonly RCT tharandomization. their suitability fquality by Nelsanalysis10. 2.1.1.8. IdenFor diagnostic July 2011 identon the basis oretrieved in fullthose two stucomments on th
, a quality apprar suitability for incf high quality withe other review sk Force9. Humphd here as completten by Biesheuvelected trials not ss judged to be ofd to be of high quntified RCT
was updated usingdline and the Coch date of this SR vant RCTs carrientified 432 citationf title and abstract
wed in more detaxcluded because
domized controlledching of referencs were identified. at includes wom
Quality appraisalfor inclusion. Theon and of low qu
ntified additionaerrors and over-tifying 10 citationof title and abstr and reviewed indies were excluhe two main SR4,
isal of all the revclusion. Götzsche a low risk of biasperformed by H
hrey review was aementary informatel6 was judged to bsufficiently describf high quality. Theality.
g the key words rchrane Databaseon (search date d out in Medline,ns. The majority ot; the other paper
ail. On the basis of the study desd trials from selecce lists of GötzsAmong those, the
men aged 70-74l of this RCT was Two County trial
uality by Götzsche
l evidence -diagnosis, this us. The majority oract; 2 papers on more detail. On ded. Most pape5.
S
views was carriee and Nelson SR4
s. Nelson review5
Humphrey for thalso judged to beion source. be of good qualitybed) and those we review written b
eported in Nelsone of Systematic RNov 2008). The l EMBASE and C
of citations were ers (n=8) were retrof the full text,
sign (not an RCTction to in-or exclusche and Nelsone Two County tria
years at the s carried out to des was judged to be and included fo
pdate was carrieof citations were en diagnostic errothe basis of the
ers are discussio
Screening Breast C
d out to 4, 5 were 5 was an he U.S. e of high
y (quality written by by Virnig
n SR5 by Reviews iterature
CCRT (in excluded rieved in all eight
T) shows sion. 4, 5, the
als is the time of
etermine be of fair or further
ed out in excluded ors were full text,
ons and
FAFcoobsSin2Ins‘smrecp2Ded22Incth((trIn8in
Cancer
For DCIS, this updAll citations were eFor overtreatmentcitations on Medlinof citations were eovertreatment werbasis of the full teselected one pubScreening Programn Appendix 1.4. 2.1.1.9. Ongoin addition to the searched for clinicscreening’ and ‘mmajority of searchelevant trials (NC
considered as ouprotocol. 2.1.1.10. Data eData from systemextraction table (Ddata extraction tab2.1.2. Descript2.1.2.1. Sourcn the years 196conducted randomhe HIP trial (N =phase I and II, N Kopparberg and rial (N= 60 117) inn Canada, the Na835) were initiatedn 1979 in 1980 (N
date was carried excluded on the bt, this update wasne and 7 citationsexcluded on the bre retrieved in fu
ext, we retrieved ablication presentimme11. The desc
ing clinical trials database search
cal trials. The seamammography’ wh results (n=135CT00963911, NCt of scope after
extraction matic reviews andDET) summarizinble are in Appendition of screeningces 60-1980, USA, Smized controlled tr= 60 995) started= 60 076) startedOstergötland, N=
n 1980 and finallyational Breast Scd in 1980. In UniteN=44 268) and th
out in July 2011 basis of title and as carried out in Jus on the Cochranebasis of title and ll and reviewed iagain the SR writing data issued ription and results
hes, the ClinicalTarch terms ‘breastwere used to se5) were ongoing CT00247442) wer
receiving more i
from trials wereng key design feaix 1.6.
g benefit
Sweden, Canada rials of mammograd in 1963. In Sw in 1976 and 1978= 133 065) in 19y the Göteborg triacreening Trials (Ned Kingdom, the Ehe UK Age Trial i
KCE Report
identifying 7 citabstract. uly 2011 identifyine Library. The maabstract; 2 papen more detail. Otten by Götzschefrom the UK B
s of those update
Trials.gov websitet neoplasm’ as warch for studies.trials. Two potenre identified but information on th
e extracted into aatures and result
and United Kingaphy screening. In
weden, the Malmö8, the Two county977-78, the Stockal (N= 51 611) in NBSS-1 and 2, N Edinburgh, trial stin 1991 (trial limit
t 176
tions.
ng 19 ajority ers on n the 4 and
Breast es are
e was well as
. The ntially were
he full
data ts. All
gdom n US, ö trial y Trial kholm 1981. = 89
tarted ted to

KCE Report 176
women aged summarizing thThis part is baPreventive Servon the CochranSwedish Two-CSR10,13,14. Both reviews inMalmö I and Stockholm trialstudy was ratedNelson updatedabout youngerHumphrey pubfrom 50 to 74 women 39 to 74younger than 50Two-County trWe analysedinformation on County trial is therefore threepublication of thby Nelson and Two-County triHealth and WKopparberg andyears were clstratified by socluster. Finallythose, they werand 7 462 in tscreening rounclosed in 1984
6
40-49 years)12. eirs results are noased on the SRvices Task Forcene SR 4. We anaCounty trial (Ost
ncluded the sameII, the Two coun, the Göteborg trd as poor quality bd the meta-analys
women (40-49 yblication for morta
years. Götzsche4 years of age. T0 years and for w
rial the Swedish Tour specific popthe largest of th
e publications thahe initiator10, the pthe last publicatial was commiss
Welfare and includ Östergötland. Inuster-randomized
ocioeconomic stat, 78 085 womenre 10 568 womenthe control groupnds with a screenafter approximate
Numerous publow available.
R (2002) commisse (USPTSF) and alysed more in detergötland) which
e trials in their menty trial, the NBSrial and the UK Aby both authors ansis from Humphreyyears of age). Thality analysis pere4 performed firstThen he did a sepwomen older than 5
Two-County trial ulation (70-74 ye
he first eight randat describe this spublication of Nyson of Tabar publioned by the Swuded women in n 1977-78, 134 8d by geographictus, urban or ruran were invited ton aged 70-74 yea. At this age, woning interval of 3ely 7 years of scre
S
lications and so
sioned to assist its update of 200
etail one RCT nah was included
eta-analysis: the HSS trials (1 and Age Trial. The Ednd excluded therey9 to include new herefore, we referformed on womet a meta-analysisparate analysis for50 years.
in order to finears). The Swedisdomized trials. Wstudy. We used ström13 who was sished in July 201
wedish National Btwo Swedish c
67 women aged 4 area. They weal residency, ando the screening. rs in the screenin
omen were invited33 months. The teening10.
Screening Breast C
ome SR
the US 095,9 and med the by both
HIP trial, 2), the
dinburgh efore4, 9.
findings er to the en aged s among r women
nd more sh Two-
We used the first selected 114. The
Board of counties: 40 to 74 ere also d size of
Among ng group d to two trial was
InthKthmfrUoeFoTAadaNloSnseaOwavCtoca
Cancer
n 2002, Nyström he Malmö, OsteKopparberg trial whe age-dependenmortality relative rrom the OstergötUnfortunately, withof women 70 to 74each group)13. Finally, we found on mammographicTrials quality andAll studies includeas fair5, 9. Götzsdivided his resultsand results based Nevertheless, the ow risk of bias (seSome publicationsnumbers of womesome studies anaexact age at randas suboptimally raOstergötland, a puwitnesses were pralmost twice as hversus 0.0012, p County trial and cao that the validitycommittee (nameda doubtful cause o
performed one rergötland, Stockhwere not availablency of the effectrisks for consecuttland trial. The mhout the Kopparbe4 years of aged e
one publication sc screening effectd bias ed by Humphrey ische assessed ths on results based
on suboptimally rthird meta-analy
ee Appendix 1.5.1s based on The n enrolled. To exalysed results bydomization13. Nevandomized and lublic notary allocaresent. Breast cahigh in Kopparbe
= 0.02). The auause-of-death ass
y of local end poind consensus comof death14.
review of the Swholm, Göteborg e at this time. Thist of screening. Tive 5-years age g
median follow-up erg part of the Swenrolled was low (
summarizing longt on mortality14.
in 2002 and later he randomizationd on adequately rarandomized controyses were judged
). Swedish Two-Coplain this variation
y year-of-birth whvertheless, Götzscikely to be biase
ated the clusters bancer mortality in erg compared to utopsy rate was sessments were nnt committee datamittee) reviewed
wedish RCT’s incltrials. Results os publication asseThe author calcugroup based on retime was 17.9 y
wedish trial, the nu(approximately 50
g term data (29 y
by Nelson were n quality. This aandomized controol trial4. of high quality w
ounty reported van, Nyström replied
hile some others che assessed thised. He argued thby tossing a coin the control groupOstergötland (036% for all the
not blinded4. Accoa was criticized, athe records conta
23
uding of the essed ulated esults years. umber 000 in
years)
rated author ol trial
with a
arying d that used
s trial at for while
p was .0021 Two-
ording a third aining

24
2.1.2.2. BreFor women ageup, the Humphra significant re(RR) 0.84, 95%Risk (RR) 0.81,For women agcontrol trial sho15.8 years (me0.70 to 0.89). Tin terms of brrange13. For women agerandomization mortality at 13 ytrials with subbreast cancer mseven trials comThe review oconservative deat randomizatiomortality at 17.this age group group) and thistogether with N2.1.2.3. DelTabar publisheSwedish Two-Cmortality reductissued from locpresented. Thepresent here cpublication sho(CI) 0.62 to 1.0respectively 10
east cancer related 39 to 74 yearsrey meta-analysiseduction in breas% confidence inte, 95% (CI) (0.74, 0ged 39 to 74 yeowed a significan
edian follow up) oThis study showedreast cancer mor
ed at least 50 y adid not show a
years (Relative Roptimal randomizmortality (RR of 0mbined was 0.77 (of Swedish randetermination of caon, did not show4 years ((RR) 1.1was relatively sm
study is underpoelson that data arlay between screed in July 2011 County Trial14. Ttion in function of cal end point com validity of local econsensus data.
owed specific mor05), 27% ((RR) 00, 15 and 20 to 2
ted mortality reds and at approxims (M-A)9 and the Cst cancer mortaliterval (CI) 0.77 to0.87) respectivelyars, the Review nt reduction in b
of 21% (Relative Rd that the effect ofrtality reduction
at randomization, ta significant redisk (RR) 0.94, 95%zation showed a
0.77 (95% CI 0.67(95% CI 0.69 to 0
domized control ause of death for ww a significant re12, 95% (CI) 0.73mall (approximate
owered13. Conseqre insufficient for teening and specthe last follow-up
This publication mlength of follow u
mmittees and conend point committe
For women agertality reductions 0.73, 95% (CI) 0.29 years of follow
S
duction mately 13 years oCochrane review4
ty of 16% (Relat0.91) and 19% (
y. of Swedish rand
reast cancer moRisk (RR) 0.79, 9f breast cancer scvaries according
three trials with auction in breast % (CI) 0.77 to 1.1
a significant redu7 to 0.83)). The R0.86)4.
trial, applying women aged at leduction in breast3 to 1.72)). Unfortely 5000 womenuently, we must cthis age group5. cific mortality redp result (29-yearmodulated breastup. In this report bnsensus-based daee data was criticed 39 to 74 yeaof 20% ((RR) 0.8.59 to 0.92), and w up. In the sam
Screening Breast C
of follow-showed
ive Risk (Relative
domized rtality at
95% (CI) creening to age
adequate cancer
5). Four uction in RR for all
a more east 70 y t cancer tunately, in each
conclude
duction r) of the t cancer
both data ata were ized, we ars, this 80, 95% 27% at
me time,
dledinpfuaAs(wthsfrAinw2Ta(ysre1Umfrre2Wss
Cancer
deaths from breasength of follow-udeaths prevented ncluded in this sprevents deaths muture. So most oabsence of screenAuthors did not separately. Result77 080 in the scre
were 10 568 womehe control groupscreening rounds rom these cases wAs cited on previon the Swedish Twwomen in each gro2.1.2.4. All-cauThe Cochrane SRaged at least 50 y n=73654) did not
years (Relative Risuboptimal randoeduction in all-ca.02))4.
Unfortunately studmortality reductionraction of all-causeduction would re
2.1.2.5. MorbidWe found no datasources. In other screening reduces
st cancer preventup. They were reat 10, 15, 20, 25
study. Author empmore in the mediuf the breast canc
ning) more than 10calculate mortalits presented are eening group anden aged 70-74 yep. In Kopparberin women aged
were still includedous point, the grouwo-County Trial woup) and this studuse mortality R has reported d
at randomizationt show a significask (RR) 1.00, 95%
omization (n=982use breast cance
dies did not haven. According to thse mortality in caequire inclusion ofdity reduction a related to the cwords, we do no
s the morbidity of t
ted in the study gespectively 50, 9and 29 years of fphasized that breum to long term cer deaths would 0 years after randity relative risks based on 133 06 55 985 in the con
ears in the screenrg, cancers diag70-74 years and
d in the results14.up of women agedwas relatively smady is underpowere
ata on all-cause, two trials with adnt reduction in al% (CI) 0.95 to 1.0
261) also did noer mortality (RR of
statistical power hat disease specincer screening trf millions of subjec
cancer related moot accept or rejethe breast cancer
KCE Report
group increased 99, 114, 122 andfollow-up for all woeast cancer screthan in the immehave occurred (i
domization. for each age g
65 women aged 4ntrol group), whileing group and 7 4
gnosed after the breast cancer d
d 70-74 years incall (approximately ed13.
mortality. For wodequate randomizl-cause mortality 04). The two trialsot show a signif 0.99 (95% CI 0.
to detect an all-cific mortality is a rials, detect a moct.
orbidity in our select the hypothesisr disease.
t 176
along d 126 omen ening
ediate in the
group 40-74 e they 462 in e two eaths
luded 5000
omen zation at 13
s with ficant .97 to
cause small
ortality
ected s that

KCE Report 176
2.1.3. Descr2.1.3.1. SouThis part is basin part 2.3.5, wesearch date. Se2.1.3.2. StuSR written by reviews writtendiagnosis and different methoissued from thpublicly organizwas focused on2.1.3.3. PerThe sensitivity 81% in the Twdifficult to intebecause they replacement th(quality of mamfactors (the exresults of an esensibility mayspecificity of a aged 40-74 yecancer underwvalue of one-timfurther evaluatibiopsy. Positiveto 20% among Nelson reporte(USA) BCSC foa single screencommon amon
6
ription of screenurces sed on the 5 SR see updated those iee more details in
udy description Götzsche and N
n by Biesheuvel asubsequently on
ods to address e first RCTs whized screening prn ductal carcinomarformance of maof first mammog
wo County trial. Trpret. This data are not adjuste
herapy, mammogmmography, numxperience of radioexamination abnoy vary between
single mammogrears. This indicatewent further diagnme mammographion and from 50e predictive valuewomen 70 years
ed data from theor regularly screenning round. False
ng women aged
ing harms
elected in our main July 2011 starti appendix 1.4.
Nelson are descrand Jorgensen6,
n overtreatment. this issue. Biesile Jorgensen anrogrammes. The a in situ (DCIS)8.
ammography graphy for womenThis includes ovecannot be appli
ed for patient fagraphic breast deber of mammogrologists and thei
ormal)9. Provider countries4. In thraphic examinatioes that 4% of wnostic evaluationhy was 12% for a% to 75% for ab increases with aof age or older9. Breast Cancer ned women that ae-positive mamm70-79 years (68
S
in search4-8. As exing from the last l
ribed in point 3.17 were focused oEach author us
heuvel analysed nalysed data issu
review written b
n aged 70-74 yeer-diagnosis and ed to individual actors (use of hensity), technicalraphic views) or r propensity to lafactors may expe Two County t
on was 95.6% forwomen who did n
. The positive pabnormal results rbnormal results r
age and ranged fro
Surveillance Conare based on resuography results .8 per 1000 wom
Screening Breast C
xplained iterature
1.1. The on over-sed very
reports ued from by Virnig
ears was may be patients
hormone factors provider abel the lain that trial, the r women not have redictive requiring requiring om 18%
nsortium ults from are less men per
sliw2Ryhsoswoao2OddaNwebsGRsthbUBYENo
Cancer
screening round). ttle more commo
women per screen2.1.3.4. AdditioRates of additionayears (64.03 per higher among woscreening round) of screen detectedscreen-detected inwomen per screenof invasive breast aged 70 to 79 yeaother imaging test2.1.3.5. Over-dOver-diagnosis ofdetection with screduring the womanabsence of screenNelson reported rawith most from 1exclusion of DCISby age. She conclstatistically5. Götzsche reportedRCT’s that did nosomewhat larger ihe control group.breast cancer in oUSA after beginninBiesheuvel analyYork/HIP, Malm IIEdinburgh) and froNetherlands and over-detection of
Conversely, falseon among womening round)5. onal diagnostic t
al imaging are rela1000 women pe
omen aged 70 tothan among youn
d cancer is highesnvasive cancer aning round. The B
cancer detected ars, 154 women h, and 2 have biopdiagnosis f breast cancer eening of cancer n’s lifetime (and thning)6. ates of over-diagn1% to 10%. She
S cases, by whethluded that the stu
d that the level oot introduce earln the sub optimal He found also a
observational studng of the screeninysed publicationsI, Two County, Com four populatioItaly). He selectinvasive breast
e-negative mammn aged 70 to 79
tests atively low amonger screening rou
o 79 years (12.2nger women. As st in this age ground 1.4 screen-de
BCSC results indicby mammograph
have additional msies5.
at screening mathat would not haherefore would no
nosis varying frome explained variaher cases are inciudies are too hete
f over-diagnosis wy screening in thly randomized tria
a 40% to 60% incdies performed in ng4. s issued from tCanada a and b, on-based programed papers that acancer by mam
mography results 9 years (1.5 per
women aged 70 nd). Biopsy ratesper 1000 womeexpected, the nu
up. Results indicatetected DCIS per cate that for everyhy screening in woammography, 10
ay be defined asave presented clinot be diagnosed i
m less than 1% toations by inclusioident or prevalent
erogeneous to com
was about 30% ihe control groupals before screencrease in incidenAustralia, Europe
the first RCTs Stockholm, Göte
mme (Sweden, Noattempted to est
mmography scree
25
are a 1000
to 79 s are n per
umber te 6.5 1000
y case omen have
s the nically in the
o 30% on or t, and mbine
in the , and ing of
nce of e and
(New eborg, orway, imate
ening.

26
Note that he publications. Bscreened and uand high particcontrol group btime. After excseveral (some being based (definitions of tdescribed befoExcluding DCISaged 60–69 yeaJorgensen anaprogrammes. Hbreast cancer screening. Notehe estimated tscreened popuscreening, he screening withscreened and nmammography for women agebreast cancer Surprisingly, litincidence of bcalculated thatover-diagnosis CI 46% to 58%Discrepancies have led to a loThe approach BZahl, Jorgensewere substantiahypothetical inc
did not include Bias were descriunscreened popucipation in non-scbefore or during foclusion, he selec
overlapping) soon cumulative
terms are in appere, he selected t
S cases, over-detars6. alysed data issHe selected pape
before and afe that when data that they would clation. After exclucompared data
data covering non screened age
screening prograd 70 to 79 years
was closely rettle of this increareast cancer in over-diagnosis foincluding DCIS c)7. between results
ot of controversial Biesheuvel et al. ten and Götzche ally downwardly crease in incidenc
DCIS. He excibed as: differenlation, low participcreening group, oollow up, inappropcted 22 estimatesurces. Publicatio
e-incidence or endix 1.4.3). Excthe least biased otection ranged fro
ued from publicers that publishefter the introduwere present, DC
contribute to 10%usion of the impl
covering at leaat least seven y
e groups. The moammes was 50-6are available. The
elated to the intase was compenwomen older th
for invasive cancecases was 52% in
reported by Biesdiscussions. to adjusting for lea(2008), who statbiased, due to oce based on theo
S
luded potentiallynt breast cancer pation in screeninoffering screeningpriate adjustment s of over-detecti
ons were categorincidence-rate m
cluding biased stuover-detection es
om 7% to 21% for
cly organized scd trends in incidction of mammCIS were included% of the diagnoslementation phasast seven yearsyears after screest common age-r9 years. No data e increase in incidtroduction of scnsated for by a an 70 years. Joer was 35%. Then this meta-analys
sheuvel or by Jo
ad time was conteed that their est
over-adjustment, uretical models an
Screening Breast C
y biased r risk in ng group g to the for lead
on from rized as methods udies as stimates. r women
creening dence of
mography d. If not, ses in a e of the
s before ening in ange for specific
dence of creening.
drop in orgensen e rate of sis (95%
orgensen
ested by imations use of a d use of
locJinstrtoninw2HsinodUsswRTDSccro2uin
Cancer
ong term followconsidered estimaJorgensen & Göncidence with a screening. They arends, following too young to be scnot, the graphs ncidences beforewhom no explanat2.1.3.6. DCIS Historically, DCISsuspicious breasncreasing numbeof the disease is database (SurveilUnited States Nasurvival rate of 9screening was pewhen screening wRecent changes iThis author perfoDCIS in name of She included 63 compared data ocentury data colleose there from 1
2004. Incidence inuse of mammogrncidence8.
w up data that ation unhelpfully wötzsche used line
in an (hypothetassume a linear inhe same pattern creened. It is diffi
the authors pre screening was tion was given.
S was rare and t mass. Since rs of patients werexcellent. Maasslance, Epidemiolotional Cancer Ins96.6% for cases
erformed. The ratewas performed3, 15.
in DCIS incidencormed a SR on
Agency for Heapublications ad
btained before thcted in US where.87 per 100 000
ncreased most in raphy may expla
are considerablywide. ear regression ttical) population ncrease extrapolaas the linear trencult to judge if thiresent show nointroduced in the
diagnosed by sthe wide use
re diagnosed withs reported data isogy and End Restitute). Those das between 1978 e was 98.1% bet
ce in USA were eincidence, treatmlthcare Research
ddressing incidenhe screening (19e screening is com in 1973–1975 towomen older thain some but not
KCE Report
y diluted. They
to compare obsethat did not und
ated from prescrend observed in wois assumption hol
on-linear increasee UK and Norwa
surgical removal of mammograph
h DCIS. The progssued from the S
esults database oata showed a 10
and 1983, whetween 1984 and
emphasized by Vment and outcomh and Quality (AHnce for analysis. 973-1975) with cummon. DCIS incido 32.5 per 100 0an 50 years. Incret all of this incre
t 176
also
erved dergo ening omen lds or es in ay for
of a hy, a gnosis SEER of the 0-year en no 1989,
Virnig. es of
HRQ). She
urrent dence 000 in eased eased

KCE Report 176
2.1.3.7. OveGötzsche repowas significantlrandomization lumpectomies (with suboptima(RR of 1.42 (951.35 (95% CI 1Based on receemphasized ththere were app3500 cases. Aconserving surmethod has remincreasing incidhaving mastect900 in 2007/081
2.1.4. ScreeThe sojourn timdetectable phasimple mathem(mainly Markovthe lead time attainable lead in higher numbgained and high2.1.4.1. LiteIn a first stagMedline was csearch terms Mammography/limited to paperlists of the seleSee more detai
6
ertreatment rted that the numly larger in the sc
showed a sign(Relative Risk (RRl randomization s
5% CI 1.26 to 1.61.26 to 1.44)4. nt data from the e increasing num
proximately 1500 Although, most rgery, the percenmained constant dence of DCIS tretomies has increa11.
ening conditions me (ST) is the avse. Estimation ofmatical estimatev Models)12. Sojou
obtainable. If ttime is correspon
ber of additional her number of yeaerature search e, studies asses
consulted from 19(MESH) were: /. Sojourn time wrs written in Engli
ected studies werels in appendix 1.4
mber of mastectocreened groups. Tnificant increaseR) 1.31, 95% (CI)showed the same1)). The RR for al
UK Breast Screembers of patientscases, but in 200DCIS cases ma
ntage of patientsat 30% during th
eatments, the abssed from just und
verage duration of sojourn time cas or using mic
urn time provides he sojourn time nding long16. A lo
breast cancer dars with cancer du
ssing sojourn tim948 to October WBreast Neoplasm
was included in frish, Dutch, Frence checked for add4.4.
S
omies and lumpeThree trials with ae in mastectomi) 1.22 to 1.42). Tw increase in intervll five trials combi
ening Programmes with DCIS. In 07/08 there were ay be treat by
s being treated wis period. Becaus
solute numbers ofder 500 in 1998/99
of the preclinical an be performed crosimulation tecan absolute uppe
is long, the monger sojourn timedetected, more liue to lead-time17.
me were searcheWeek 1 2011. Thms/ Mass Screeree text. The seach, or German. Reditional relevant c
Screening Breast C
ectomies adequate ies and wo trials ventions ned was
e, Dixon 1998/99 close to breast-
with this se of the f women 9 to over
screen-by from
chniques er limit to maximum e results ife-years
ed. Ovid he main ning/ or
arch was eference citations.
SAc1kEedcreareOscddtwae2SWTeaminsdtoey
Cancer
Selection criteriaAll retrieved refecriteria (in terms o
) in a two-step keywords; followeEstimation of sojexcluding of 3 dudatabases. Of thiscriteria based on etained for full-tex
and 1 did not fetained16, 17, 25-32
Our search was bseveral publicationcited as referencedata published bydata29. Therefore,wo or more artiaccurate for our sextraction table (se2.1.4.2. ResultSojourn times caWe found 4 studiTwo- County Triaestimates of sojouapproximately themodel, but resultsn estimates publisstatistical methodsdeveloped statistico data from the Tearly detection myears (SD, 0.76)27
a erences were asof population, inteprocedure: initial
ed by full-text asjourn time not buplicates, 40 unis total of 40 refetitle and abstra
xt assessment, 6ulfill the outcom
based on ST durans were ST estims by the author. F
y Tabar in 199529
we used originacles based on t
study30, 31. Finally,ee appendix 1.6.7ts
alculated on RCTes based on the
al is described inurn time publishe same data. Both
s were not the samshed by the two as or by discrepanccal methods baseTwo County Trial
modalities as 0.92.
ssessed against ervention, outcom
assessment of ssessment of thebased on data que citations we
erences, 23 did nct evaluation. Am
6 did not fulfill theme criteria24. Fina
ation estimations mations were issueFor example, Zap. Duffy in 200526
al publications. Ifthe same data, 7 publications ar
7).
T’s data results of the Twn chapter 2 (poied by Tabar and h authors used thme. Shen underlinauthors25, 29 may cy in the data. Shed on the maximul. Authors estima
2 (SD, 0.09) and
pre-defined inclmes, and design-Tthe title, abstract
e selected referewere excluded.
ere identified fromnot meet the inclmong the 17 cita population criterally, 10 studies
as search. We fed from others stpa in 200332referrreferred also to one author publwe choose the re summarized in
wo- County Trialint 2.2.1.1.)10, 13. Duffy were base
he same Markov ned that the differbe caused by diffen applied his rec
um likelihood estimated the sensitiviti
the mean ST a
27
usion Table t and
ences. After
m the usion ations ia18-23 were
found tudies red to those ished most
n data
. The First
ed on chain rence ferent cently mates ies of
as 4.4

28
Sojourn times Spratt estimateprevalence rateyears. Thereforincluded in th(Louisville). Forbetween 2.5 y tFracheboud coprogramme for in 1995. Boer use in his MISincrease in prealthough pessimduration with aaged 70-74 yeand subsequenassumption whthe age of 69. strong increasetime17. Weedon constrdo not have fuscreening is cquality, incidenscreening examTherefore, he send to 336 5Programme (Nyears for wome2.1.4.3. DisMost estimatesMarkov chain growth of cancedevelop accordtime must cons
calculated on sced the duration of es at first screeninre, he used data fe Breast Cancer women aged 70to 3.8 y28. ompared the resu
women aged 70-had described o
SCAN model. Opeclinical durationmistic assumptionage33. Based on ars), Fracheboudnt screens increaich assume a coThis increasing
e in detection of c
ructed one inventull registration ofommon. Although
nce data from themination or registrareplaced data la533 women in tBCSP). This new
en aged 60-69 yeacussion s of sojourn timmodels). Such mer. Unfortunately, ding to a chronoequently be interp
creening programbreast cancer be
ng round by incidefrom 10 000 womeer Detection and-74, he estimated
ults of the Dutch -75 with the hypot
optimistic and pesptimistic assumpt
n of breast cancn assumed a furth187 207 screenin
d found that deteased steadily witntinuously increassojourn time of bancers, but also t
ive solution for scf interval cancersh Norwegian rege first screening ation of interval ca
acking by data ishe Norwegian B
w approach gave ars, although STS
e have been bamodels assume a
it remains unknoological sequencepreted with cautio
S
mmes data efore detection by ence rates in the fen aged 35 to 70yd Demonstration d that sojourn time
breast cancer scthesis developed ssimistic assumpttion assumed noer after 65yearsher increase in prng examinationsection rates in both age and got sing sojourn timebreast tumours leto more life- years
creening programs or where oppogistration is of ve
round, interval bancer may be ins
ssued from questBreast Cancer Sc
estimation of MSS was estimated to
ased on Models a chronological s
own whether cance. Estimations of n.
Screening Breast C
dividing following y at start
Project e ranged
creening by Boer tions for o further of age reclinical (women
oth initial close to
e beyond ead to a s in lead
mme who ortunistic ery high between ufficient. tionnaire creening
ST to 6.9 o 60%30.
(mainly stepwise cer really
sojourn
2D
T
Qw
P
In
C
O
M
M
F
F
A
B
Cancer
2.1.5. Key dataData issued from l
Table 2.1: Data is
Question 1: Showomen between
Population
ntervention
Comparison
Outcomes:
Mortality (specifi
Mortality (all caus
FP
FN
Additional imagin
Biopsy
a literature search a
ssued from clinic
ould breast canc70 and 74 years?
Women bebreast canccancer.
Organized
No organiz
c) For womenmortality re23% (RR: County triasignificant r0.92) at 1afterwards.
se) Studies didall-cause m
68.8 per 1screening r
1.5 per 10screening r
ng 64.03 per screening r
12.2 per 1screening r
are summarized in
cal literature revi
cer organized sc?
etween 70-74 ycer and without p
screening with m
ed screening
n >50 y at randoeduction after a fo
0.77, (CI) 0.69 al, specific mortareduction of 27%
15 years of follo.
d not have statistimortality reduction
000 women ageround (BCSC-USA
000 women agedround (BCSC-USA
1000 women ageround (BCSC-USA
000 women ageround (BCSC-USA
KCE Report
n table 2.1.
iew
creening extende
years of age wparticular risk of b
ammography
omization, the spollow-up of 13 yeato 0.86). In the
lity reduction rea(RR: 0.73, (CI) 0
ow up and incre
cal power to dete.
ed 70 to 79 yearA)
d 70 to 79 yearsA)
ed 70 to 79 yearA)
ed 70 to 79 yearA)
t 176
ed in
ithout breast
pecific ars is
Two ach at .59 to eases
ect an
rs per
s per
rs per
rs per

KCE Report 176
DCIS
Over-diagnosi
Over-treatmen
2.1.6. ConclAt this age groadditional imagspecific mortalmortality reducspecific mortaliafter screeningreduction must in our country.On the other pertinent to discin this age-groucancer screenitime bias althoScreening diagthe end of “the diagnosed brea
6
1.4 scre70 to 79
s Over-defrom (7%women a
nt The numwas sig(RR:1.35
lusion oup, performance
ging are relativelyity reduction of tion did not appeity reduction is ng ((RR) 0.80, (Cbe put in perspec
hand, aspects recussion of the benup. First, over-diagng, the risk of o
ough difficult to esnosed breast canlife in good health
ast cancer34.
een-detected DCIS9 years per screen
etection (excludin% to 21%) to 35aged 70 to 79 yea
mber of mastectognificantly larger 5 (95% CI 1.26 to
e of mammograpy low. Breast canc23% to 27% acear in the first yeot statistically sigI) 0.62 to 1.05). ctive with life-expe
elated to quality nefit and harms ognosis being an invertreatment persstimate, may be
ncer and consecuh condition” some
S
S per 1000 womening round (BCSC
g DCIS cases),5% (no data spears are available).
omies and lumpein the screened
o 1.44).
phy is high and cer screening achcording to autho
ears after screenignificant before 1
Breast cancer mectancy for this ag
of life raises qf breast cancer scnevitable consequsists. Secondly, tcrucial for older
utive treatment ma years earlier than
Screening Breast C
en aged C-USA)
ranged ecific for .
ectomies groups
rates of hieves a ors. This ing. The 10 years mortality ge-group
uestions creening uence of the lead women.
ay mean n clinical
22InoessMJliRcTs•••
2Ac2ksdin
Cancer
2.2. Review o2.2.1. Literaturn a first stage, ranon morbidity and meffectiveness of scsources to corresearched35. Medline, Embase,January 2000 up tmited to papers
Reference lists of citations. The keywords usesearch terms (MES Breast Neopla Mass Screeni Mammograph
2.2.2. SelectionAll retrieved refecriteria (in terms o2.2.) in a two-stepkeywords; followeshould be noted digital mammogran KCE report 1722
of modeling studre search strategndomized clinical mortality were seacreening require a
ectly inform deci
, NHS EED and to September 20written in Englishthe selected stud
ed and the resultsSH) were: asms; and ng or Early Detec
hy; and n criteria
erences were asof population, intep procedure: initiaed by full-text ass
that studies assphy) were exclude2.
dies gy trials analysing th
arched (see abova lot of informationsion makers, m
Econlit databases11 (see appendixh, Dutch, French,ies were checked
s are detailed in a
ction of Cancer ; a
ssessed against ervention, outcomeal assessment of sessment of the sessing screeninged because such
he impact of screve). Then, becausn from a wide ranodeling studies
s were consultedx 2.1). The search, Spanish, or Gerd for additional rel
ppendix 2.1. The
and
pre-defined selees, and design - Tf the title, abstracselected referenc
g techniques (suctopic was investig
29
ening se the nge of
were
from h was rman. evant
main
ection Table
ct and ces. It ch as gated

30
Table 2.2: Sele
Population
Intervention
Outcomes
Design
LYG: life-year ga
2.2.3. QuanAfter excluding the databases.citations. Of thicriteria based retained for full15 did not fulfilretained, conceCISNET, 2 appdeveloped by publications17, 3
appendix 2.2.
ection criteria
Inclusion crite
caucasian wombreast cancer particular risk
Screening mam
Morbidity and(e.g. LYG and Q
Modeling studie
ained; QALY: Quality
tity of research a195 duplicates,
. Hand searchings total of 1058 reon title and abs-text assessmentl the design criter
erning 6 models dplications of theseother groups or 36-59. The flow ch
eria Ex
men without and without
OtAs
mmography Otma(e
d Mortality QALYs)
Otdia
es Ot
y-adjusted life-year
available 1058 unique citatg did not allow eferences, 1016 dstract evaluation. t, 2 did not fulfill thria. Finally, 25 modeveloped by mo models on differeauthors, as som
hart of this selec
S
xclusion criteria
ther (e.g. womansian women, etc.)
ther, iammography tec.g. digital mammo
ther outcomes (eagnosis)
ther designs
gained
tions were identifus to identify ad
did not meet the iAmong the 42
he population critodeling publicatiodeling groups invent context and 7
me models have ction is presented
Screening Breast C
n at risk,
ncluding chniques ography)
e.g. over
fied from dditional nclusion citations teria and ons were volved in 7 models
several d in the
T
E
P
In
O
D
22T((cfotodmC(aTcre2eu
Cancer
Table 2.3: Modeli
Exclusion criteria
Population
ntervention
Outcome
Design
2.2.4. Selected2.2.4.1. The CThe Cancer Interhttp://cisnet.canceNCI)-sponsored
cancer control inteor breast cancer. o help determindeveloped their omodeling philosopCenter model37, UMISCAN) model5
and Stanford modThe seven modecontributions of seduction in brea
200077. Mandelblaestimates of poteunder different scr
ing studies exclu
a Studies
Messecar 2
Advisory CAnonymouBonneux 2Koning 20Habbema Rautenstra
d studies CISNET Projectrvention and Surer.gov) is a coninvestigators who
erventions on popThese models are optimal cance
own breast cancphies: The UniverUniversity of Wisc57, Dana-Farber mel51). ls were first usecreening mammost-cancer mortaliatt et all48 used 6ential benefits anreening schedules
uded after full-tex
2000; Wen 20056
Committee on Bus 2000; Barratt 22009; Caplan 20000; Feuer 2002006; Mandelblat
auch 2000, Xu 200
rveillance Modelinnsortium of Natiose focus is moulation trends in i
re also used to prer control strateger models spannrsity of Texas M.consin model, Ge
model44 University
d to assess the ography and adjuity in the United 6 of those CISN
nd harms of mams. One of the 7 mo
KCE Report
xt assessment
0, 61.
Breast Cancer 22002a; Barratt 2001; Carney 2007
04; Grivegnee 2tt 2003; Prevost 20062-76.
ng Network (CISonal Cancer Insodeling the impancidence and mo
roject future trendsgies40. Seven grning a wide rang. D. Anderson Caeorgetown47, Era
y of Rochester mo
relative and absuvant treatment t
States from 197ET models to prmmography screodels, the Univers
t 176
2006; 002b; 7; De 2001; 2000;
SNET) stitute act of ortality s and roups ge of ancer smus odel43
solute o the 75 to rovide ening sity of

KCE Report 176
Texas M. D. Apurely descriptiThe models wethey were comprocess, they aUS datasets B(Surveillance, eand the BerkeleA detailed dispublications anddetail, but sumdiscuss the maThe models espresent the recomparison of policy screeningFeuer et al.40
surveillance mosimulation modthrough the mnumber is gemechanistic orequations desctumor growth aCancer Centermodels could Farber model cmodels (Univehaving some characterizationobservable quaprogression of disease procesThe models statrends without screening use a
6
Anderson Cancer ve. ere developed by
mpared, discussealso used a commBCSC (Breast Caepidemiology andey mortality Databscussion of eachd on the CISNET
mmarize the pooleain limitations anstimated a large
esults of the parta screening pol
g age 50-74. identifies two d
odels used heredels at one end oodel one at a tinerated and indr analytic modelcribe the relationand metastasis. Tr, University of be characterizedcould be charactersity of Rochesteaspects of ea
n runs from bioantities to model t
disease, to epids is modeled (usuart with estimatesscreening and t
and improvements
Center model37
y different grouped and adapted mon set of variabancer Surveillancd end results), Cobase. h of this modelswebsite, we will n
ed comparison ofnd implications foe number of scet relevant to ourlicy screening ag
dimensions to ch. The first dimen
of the spectrum, wime, where at edividual life histols, where a set
nships between kThe University ofWisconsin, Geo
as micro simulaerized as analyticer and Stanford)ch. The secondologic, where ththe underlying disdemiologic, wherually the observabs of breast cancetreatment and ths in survival assoc
S
was not used as
s but not indepeduring the deve
bles and inputs, bce Consortium), Sonnecticut Tumor
s can be foundnot discuss each mf Mandelblatt et aor our research qenarios, but we wr research questge 50-69 to a sc
haracterize the tnsion incorporatewhere individuals ach transition a ories are generat of analytically key health statesf Texas M. D. Aorgetown, and Eation models; thec; and the remain) could be descrd dimension ofhe model goes sease onset, growre only a portionble portion). er incidence and mhen look at the eciated with treatm
Screening Breast C
s it was
endently, elopment ased on SEER 9 r registry
d in the model in al.48 and question. will only tion, the creening
types of es micro
are run random
ated, to derived
s and/or Anderson Erasmus e Dana-ning two ribed as f model
beyond wth, and n of the
mortality effect of
ment.
BpmdidceinoaccasthgTmmmwbotedredpTreligdTmIn
Cancer
Breast cancer is period (sojourn tmammography sedisease in the prdentification of eaclinical detection, estrogen receptor ndependent effecother causes. as age-specific variacharacteristics, trecompeting causesas preclinical detestages of diseasehat followed fromgrowth. The stage distribumodels were alsomodels that use thmodel reductions were used. The habiopsies and overobserved input waerms of QALYs. Mdisease or decreesults living with
diagnosis was notpurposes. Table 2.4 gives teduction and yeamited and there
gained per 1000 deaths averted ranThis class of modemodels are indivndependent valid
assumed to haime) and a clin
ensitivity (or thresreclinical screeninarlier-stage or sm
resulting in redustatus, and tumo
cts on mortality. Wmentioned before
ables for breast eatment algorithms of death. On theectable times (soje, were in these the model struct
utions in unscreeo intermediate ouhis observable vain mortality, life yearmful effects falsr diagnosis followas used, no attemMorbidity associa
ements in qualityh earlier knowlet considered, whic
he results of thears of life gained f
is some variabilitwomen screenednging from 4 to 6.els relies heavily ovidual bases theation was made
ave a preclinical,ical detection poholds of detectionng-detection perioaller tumors than uction in breast cr size– or stage–sWomen can die oe, the 6 models cancer incidence
ms and effects, a other hand, unobourn time), lead models estimatedture and assumpt
ened versus screetcomes, this in c
ariable as input. Aears gained werese positive mamm
wed from the modpt was made to q
ated with surgery y of life associatedge of a cancech makes the mod
e different modelsfor the different mty between moded ranging from 9
on unobservable vey are not alwadifficult because
, screening-detecoint. On the basn), screening idenod and results i might be identifiecancer mortality. specific treatment of breast cancer use a common s
e, mammographyand non-breast cabserved variablestime, dwell time wd intermediate outions concerning t
ened women in tcontrast to some As end output frome calculated, no Qmograms, unneceel, also here no
quantify those harfor screening-detted with false-poer diagnosis or dels less useful fo
s in terms of momodels. Gains are els, with number
to 17 and numb
variables, and as ays very transparesults from trials
31
ctable sis of ntifies n the ed by Age, have or of
set of y test ancer such within utputs tumor
these other
m the QALYs essary direct
rms in ected
ositive over
or our
ortality fairly
years ber of
most arent. s and

32
the main US calibrate the mand some obsvalidity of the calibrate the mo
Table 2.4: resreduction and different mode
Model group abbMedical Center; G_Stanford Univer
Stout et al 200analysis, includ50-74 with age Rue et al.55 adZeelen44 to daton Catalan survUS with CatalObtained resulfound, a morta
ModelMortality (specific) reperiod in %Screening in agegroup Screening in agegroup Incremental mortality reagegroup 50-74 compaagegroup 50-69Years of life Gained pscreenedScreening in agegroup Screening in agegroup Incremental years of lifagegroup 50-74 compaagegroup 50-69 Incremental days of liscreenedScreening in agegroupscreening in agegroup
breast cancer rmodel. Model outp
ervational studiesmodel as data
odel.
sults of the di years of life ga
els
breviations: D _ DanG _ Georgetown Unrsity; W _ University
0656 used the Wisding the use of QAgroups 50 - 69 w
dapted de Dana-Fta in Catalonia. Bvival they combinan data in a prts were very sim
ality reduction of
eduction over the whole
50-69 50-74eduction screening in ared to screening in
per 1000 women
50-69 50-74fe gained screening in ared to screening in
ife gained per women
p 50-74 compared to 50-69 women screened
registries were uputs are similar tos, but this does from those stud
ifferent models ained per 1000 w
na-Farber Cancer Inniversity; M _ M.D. Ay of Wisconsin/Harv
sconsin model toALYs, but compaere not made. Farber Cancer InBecause there waned the survival darevious publicatio
milar to the ones 21% and 131 life
D E G
16 23 1722 27 21
6 4 4
88 107 111106 116 128
18 9 17
6,6 3,3 6,2
S
used to parameto the results fromnot say much ab
dies were partly
in terms of mwomen screened
nstitute; E _ ErasmuAnderson Cancer C
vard
o do a cost effecarisons of the age
stitute model of Las insufficient infoata from the SEE
on of Vilaprinyo, Lee & Zeelen o
e years gained p
M S
16 1521 20
5 5
82 9996 121
14 22
5,1 8,0
Screening Breast C
erize or m RCT’s bout the used to
mortality d for the
us Center; S
ctiveness e groups
Lee and ormation
ER in the 200958.
originally per 1000
winmhqCaTbbTbbcesgdco2CgbthsskRDbjureG
W
2328
5
8495
11
4,0
Cancer
women screened ncremental benefmortality and 2 lifhad no choice thquestion in what Catalan context. Cand Vilaprinyo et aThey found 3990 biannual screeningbiannual screeninThey found 3891 biannual screeningbiannual screenincompared to a schextending the scrscreening from 45gained by extendindid not incorporacalculations, but uover diagnosis. 2.2.4.2. ModelCarter et al, 20053
growth using mainbecause of unreahey assume a fixstages 1, 2 and 3.screening than otknow about stage Rojnik et al, 2008 DCIS, local, regiobut details on howudge how this waeport ICERs so w
Gained and QALY
for a biannual scrfit for biannual sfe years gained phan to use US degree this can
Carles et al, 2011al58 to do a cost elife years gained
g in the age groug 50- 74 of 299 QALYs gained g in the age groug 50- 74 of 277 hedule 50-69. Thereening to 50-74 5- 69, but reporteng the screening ate the results used US survival
ls not related or 39, 78 developed a nly SEER data. Thlistic assumptions
xed survival of 2 y This leads to con
ther models but ispecific survival.produced a time d
onal and distant.w the model was pas done or if asswe have no informYs.
reening in the agescreening 50- 74per 1000 women data for most kereally be called
138 finally used theffectiveness anald for a cohort of p 50-74, with an life years gainedper 100 000 wop 50-74, with an life years gained
ey did not report tfrom 50 -69, as
ed that 186 QALto 45-74 from 45 of Vilaprinyo et
l data. They did
not using CISNEmicro simulation he model lacks crs concerning stagyears for stage 4 nsiderably higher s in absolute con
dependent MarkoOverall model stparameterized aresumptions were rmation on assum
KCE Report
e group 50-74, w4 of 1.7% in term
screened. As auey variables one
an adaptation the results of Rueysis, including QA100 000 women incremental bene
d per 100 000 woomen screened wincremental bene
d per 100 000 wothe QALYs gaineds it was dominateLYs per 100 000
-69. Interestinglyt al,200958 into not take into ac
ET methodologymodel based on tredibility though mge specific survivaand complete cuyears of life gainentradiction to wha
ov model with 4 structure was desce lacking so we careasonable. Theyed gains in Life Y
t 176
ith an ms of uthors e can o the et al ALYs. for a
efit for omen. with a efit for omen d with ed by were
, they their
count
y tumor
mainly al, as re for ed for at we
ages, cribed annot
y only Years

KCE Report 176
Neeser et al dscreening with coverage of 20breast cancer munclear how thranging from 5 years screeninrelevant for ouscreening wouldays) per womsimplistic by nreductions immwas not taken iRauner et al, 2only evaluated rather experimehow they actuaMahnken et al,length bias andonly adjusted HRijnsburger et developed by tCanadian CNB50–59, so their Barratt et al 2cohorts, with oother not, assuthe outcomes oscreening. Thereduction fromlinearly to maxthat benefit descreening. For of 70s, two fewwomen who stonumber of diag
6
developed a sima coverage of
0%. They assummortality with 15%hey come to this
to 20%. They cang beginning at ur research quesd save 41 lives p
men screened for not taking into amediately. No QAnto account.
2010 developed athe effect of scr
ental model is notlly modeled stage, 200846 develope
d over-detection aHazard ratio’s.
al, 200453 usethe Rotterdam57 SS-2 trial on breafindings are not r
200536 constructeone cohort womeming 100% partic
of women over 70ey assume a 37% for non compli
ximal level over fieclines linearly towomen who cont
wer women per op screening (sixnoses of breast c
mple Markov mod70% with opported that the orga% based on the s figure as IARCalculated the yea70 (they evaluat
stion as well. Thper 100 000 and 10 years. The mccount lead time
ALYs were used
an ant colonizatioreening amongst t useful for our pue specific survival.ed a method to and applied this to
ed the MISCAN (see above) to rast cancer screenreally useful for oued a Markov moen undergoing biecipation. Within th
0 years old underg% mortality reducance, and assumrst five years afteo nothing over ftinue screening fothousand die fro
x v eight deaths fcancer in screene
S
del comparing ortunistic screening
anized screening IARC handbook,
C postulates a rears of life gained ted other scheduey found that oradd 0.008 life ye
model is somewhae but applying aand effects on m
on optimization mwomen 50-70 a
urposes. It is also. adjust for lead timSEER data, but p
micro-simulationreplicate the dataning among womur purposes. odel for two hypennial screening his model, they evgoing 10 years of ction, adjusting tme that benefiter starting screenfive years after sor 10 years after m breast cancerfrom breast cancd women is abou
Screening Breast C
rganizes g with a reduces but it is
eduction for a 10 ules not rganized ears (2.9 at overly assumed morbidity
odel but and their o unclear
me bias, provided
n model a of the en aged
othetical and the valuated biennial
the 25% accrues
ning and stopping the age than in
cer). The t 41 and
th5Tin2Matoli
2BimdinhTaeafoDre1
Cancer
he number in uns50% brings the nuThis simple modento account the ef2.2.5. ConclusiModels described adapt them to the o parameterize thfe between 9 an 2
2.3. Review oBecause breast cmpact on the qudimensional healthnformative. It is health outcomes iTo value these madjusted life-year expected length adjustments are mor different healthDetermination of equires two steps. The health s
guidelines of health statessystem. Idealusing a genestates descrdescriptions fr
screened women umber of deaths el has the advantaffects of lead timeion are give useful inBelgian situation
hem. The CISNET22 years per 1000
of quality of life cancer screening
uality of life (QoLh-outcome measuimportant to taken the assessmenultidimensional ou
(QALY) must bof life by the
made using utilitieh states.
utility values, ns: tate description.
f the Belgian Hes should be deslly, the descriptioeric descriptive sriptions from Brom similar patien
about 26. assumin the screened gage of transparen
e and stage-shifts
nsights and elemen as we do not haT models give a m0 women screene
studies g programs are L) of the patientsure in terms of sue into account alnt of breast canceutcomes into a sibe used. QALYs
health-related qes derived from i
eeded for the c
According to theealth Care Knowscribed on a staon should be donsystem, such as Belgian patients nts in other countr
ming a risk reductigroup down 6.2 toncy, but does noton morbidity.
ents but it is difficave the necessarymodest gain in ye
ed.
expected to havs, models with a urvival are not enl the multidimens
er screening progrngle measure, qupermit to adjus
quality of life. Tindividuals’ prefer
calculation of QA
e pharmaco-econwledge Centre (Kandardized descrne by Belgian pa
the EQ-5D. If hare not avai
ries may be used7
33
ion of o 5.1. t take
cult to y data ear of
ve an one-
nough sional rams. uality-st the These rence
ALYs,
nomic KCE), riptive atients health lable,
79.

34
2. The valuat
economic gon a 0 (=vrepresentavalued by collected, discussed7
In this section,describing the treatment) is as2.3.1. Metho2.3.1.1. LiteElectronic dataestimates for screening and end of OctobeEmbase (via E(via OVID). Searches usingheading or texstrategies and t2.3.1.2. SelIdentified refere(in terms of poptwo-step procedfollowed by fuabstract was acitation was asthe selected stu
tion of these heguidelines of the Kvalue for death) toative sample of th
the Belgian popuvaluations from
79. the availability aburden of disea
ssessed. ods erature search stabases were con
different health treatment. System
er 2011 in the fombase.com), HTA
g various qualifierxt word. See appterms used. lection criteria ences were assespulation, intervendure: initial assesll-text assessmen
available and thesessed based on
udies were scrutin
ealth states. AccoKCE, health stateo 1 (=value for phe general publiculation but if no
m other countrie
and the quality oase due to breas
trategy nsulted for origin
states associatmatic searches wollowing databasA and EED (via
rs for “quality of lipendix 3.1 for an
ssed against pre-tion, outcome andssment of the titlent of the selecte
e citation was unn keywords and funized for additiona
S
ording to the phe values should beperfect health) scac. Ideally, they shoriginal Belgian des can be use
of published utilityst cancer (screen
nal publications oted with breast
were carried out uses: Medline (viaCRD NHS) and P
fe” were used asn overview of the
-defined selectiond design –Table 2e, abstract and keed references. Wnclear or ambiguoull-text. Referenceal relevant citation
Screening Breast C
armaco-e valued ale by a hould be data are ed and
y values ning and
on utility cancer
up to the a OVID), Psycinfo
Subject e search
n criteria 2.5) in a eywords;
When no ous, the e lists of
ns.
T
P
In
O
D
QQeHa
Cancer
Table 2.5: Article
I
Population Spcor
ntervention At
Outcome Ua(
Design Do6ms
QoL: Quality of Life. Quality of Life. DALYequivalent; TTO: TimHUI: Health Utility Inanalysis. VAS: visua
selection criteri
Inclusion criteria
Screened or treatpatients for breascancer, with a Caorigin and withoutrisk factors
Any intervention rto the Belgian set
Unique QoL weigallowing to derive(=utilities)
Direct (TTO, PTOor indirect (EQ-5D6D, HUI, QWB) vamethods in primastudies
QALY: Quality adjuY: Disability-Adjusteme-Trade-Off. PTO:ndex. QWB: Quality al analogue scale
ia
a Exclus
ted t ucasian t high
Other dCauca
relevant ttings
InterveBelgium
hts QALYs
Multi-dscores
O, SG) D, SF-aluation ry
LettersCUA wfrom thDirect (not reKCE pguideli
usted life year. HRQed Life-Years. HYE: : Person Trade-Off. of Well Being scale
KCE Report
sion criteria
diseases, non sian, high risk wo
entions not used inm
dimension HRQoLs, DALYs, HYEs, …
s, secondary studiwith QALYs derivehe literature, … valuations using Vcommended in thharmaco-economnes)79.
QoL: Health-Related healthy-years- SG: Standard-Gam
e. CUA: cost-utility
t 176
omen
n
L …
ies, ed
VAS e
mic
d
mble.

KCE Report 176
2.3.1.3. SelThe flowchart osearches on thduplicates, 352searching allowninety (290) ref65 references fat this stage, mOverall, we sele2.3.2. ResulA summary of tbe noted that values and theireported in the The selection o• Determinat• Selection o
Selection oSelection o
• Pooling of 2.3.2.1. DetHealth states foIt should be noreflection proce
6
lection process of the selection p
he databases retu2 unique citationswed us to identifyferences were disfor full-text evaluamostly because ofected 16 primary slts the selected studithis summary onr results. If other summary.
of utilities was dontion of health stateof utilities of a basecase studof other studies selected utilities atermination of heor which utility valuoted that this figess but not the
process is presenurned 524 citations were left (see ay 3 additional citacarded based on tion. Another 49 rf the unmet desigstudies (see appe
ies can be found nly report methoparameters were
ne according to thees for which utilitie
dy
and calculation of ealth states ues are needed a
gure is a schemamodel itself (de
S
nted in appendix 3ns. After exclusionalso appendix 3.2ations. Two-hundtitle and abstract
references were egn and populationendix 3.2).
in appendix 3.3. Iods used to deriv
measured, they w
e following stageses were needed
percentage chan
are listed in Figureatic representationescribed in secti
Screening Breast C
3.2. The n of 172 2). Hand dred and , leaving excluded criteria.
It should ve utility were not
s:
ges
e 2.1. n of the on 3.2).
Cancer 35

KCE Reports vo
Figure 2.1: Hea
Women ag
Before
ol
alth states for wh
ged ≥ 70 years
e screening
hich utilities are
Positive
Negative
False p
True po
Short termof the sc
S
needed (reflecti
results
e results
positive
ositive
m impact reening
Screening Breast C
on process)
Metas
Women aged
Breast cance
Breast cance
Breast cance
After scre(First y
Non me
Breast canc
Cancer
static
≥ 70 years
er stage II
er stage III
er stage IV
eeningyear)
etastatic
cer stage I
Women
Breast
Breast
Breast
Aft(Foll
No
Breast
Metastatic
aged ≥ 70 years
cancer stage II
cancer stage III
cancer stage IV
er screeninglowing years)
on metastatic
t cancer stage I
36

KCE Report 176
2.3.2.2. SelTo select utility by the pharmacdata could be foThen, we triedmodel. The aiminstruments andthe pharmaco-eto use the samquality of life weHowever, no st2.3.2.1 with thestudy with the gand to use it at Selection of thWe found onlymetastatic and the chance thaccording to th5D79. This studyUtility values imethods, i.e. technique) by Sgeneric instrumeconomic guidethese valuationTTO). In this stvalued using UKavailable). Heavalues for nontreatment) and patients are desThis study had
6
lection of utilities values, we first tco-economic guidound. to find the mos
m was to avoid d multiple populaeconomic guidelinme descriptive inseights coming fromtudy assessing ae same design wgreatest number othe starting point
he base case stuy one study havimetastatic patienat this study als
he pharmaco-econy was therefore thin the study of a direct valuatioSwedish patients ment (i.e. the Eelines of the KCEs were retained (tudy, health statesK tariffs (because
alth states descri-metastatic patiethe following yea
scribed in Table 2the following limit
s tried to find Belgiadelines of the KCE
st complete studyas much as pos
ations to derive thnes of the KCE, it strument and them different studiesll of the heath sta
was found. We thof health states coof the selection pdy ing assessed uti
nts, i.e. the study oso used the betnomic guidelines he starting point oLidgren et al.80
on method (i.e. and an indirect v
EQ-5D instrumenE recommend thei.e. utility values fs were described
e no tariffs from thptions can be fonts in the first yars as well as ut2.8. tations:
S
an data as recomE79. However, no
y which best fit wsible the use of em. Indeed, accois strongly recom
e same set of vas79. ates described inherefore tried to orresponding to ouprocess.
lity values for boof Lidgren et al80.tter available insof the KCE, i.e. f our selection prowere derived fr
the time-trade-ofvaluation method nt). Because phe use of the EQ-5from EQ-5D and by Swedish patiee Swedish popula
ound in Table 2.6year (i.e. the yeaility values for m
Screening Breast C
mmended Belgian
with our multiple
ording to mmended alues for
n section find the
ur model
oth non-We had
strument the EQ-
ocess. rom two ff (TTO) using a
armaco-5D, only not from ents and ation are 6. Utility
ar of the etastatic
•
•
•
Cancer
Utility values cancer outpatfollowing limitaUtility values f
the shortthis shorttime and
Utility values palliative only reflefirst year
The short term(not measthis studythe valua
Non-metastatyear of diagnthat after the assumption idifference in uyear 5, 10 and
It should also (primary breapatients werinconstistencyMetastatic p
consultatGeneric instru
relevant specific ionly be uthese ins
were measuringtient clinic (Karolations: for non-metastatict term impact of st term impact wawas therefore notfor metastatic p
care. It was therected the quality of diagnosis.
m impact of diagnsured at the momy reported that thisation (measured thtic patients were dosis and the folloyear of treatmenis supported by utility values (fromd 1581. This US stbe noted that util
ast cancer in the re similar (0.6y may be due to thpatients only incions (best cases)uments such as tchanges in healtinstruments. How
used if validated mtruments are avai
g during out-patieinska University
c patients did not surgery. Howevers expected to cot included in the mpatients did not refore assumed thof life of metasta
nosis is also not fment of the diagnos impact was exphe year of diagnosdivided in only twowing years. It wt, utility values re
an US study m EQ-5D using Utudy is described ity estimates for nfirst year of diag96 and 0.685 he following reasoclude patients . he EQ-5D are lesth in a specific d
wever, diease-spemapping functionsilable, which was
ent visits at a bhospital), implyin
fully take into acr, on an annual b
over a limited lengmodel.
represent patienhat these utility v
atic patients durin
fully taken into acosis), even if authoected to be includsis). wo groups, i.e. thewas therefore assuemained constant
where no signiUS tariffs) was fou
in the appendix 3non metastatic pagnosis) and meta
respectivelly). ons: going in out-p
ss sensitive to cadisease than diseecific instrumentss to derive utilitiesnot the case79.
37
breast g the
count basis, gth of
nts in values ng the
count ors of ded in
e first umed . This ficant
und at .3.
atients astatic
This
atient
apture ease-s can s from

38
Table 2.6: Hea
Primary bcancer (year 0
Recurrence (y1)
Primary bcancer recurrence following year
Metastatic patSelection of otFor other heainstruments for us to identify apopulation stratwith UK tariffs),therefore used For the short tusing the EQ-5assessed utilitytrue negative. Hthe Swedish postates (as in positive” state is
lth states descri
breast -1)
Patients cancer wquestiondisease
year 0- Patients regional prior to metastat
breast and
rs
Patients breast cayear priometastat
ients Patients ther studies lth states, we trthe same popula
a study assessintified by age and , i.e. the study of for women aged 7term impact of p5D instrument way values for false Health states wereopulation) but UKthe other selects given in Table 2
ptions for the st
who had primawithin 1 year or lennaire, no recurre
who had at leaand/or contra-lateanswering the
tic disease.
who had been dancer or their lasor to answering thtic disease.
who had metasta
ried to find studation. The study ong utility values gender using the Burström et al.82
70 and over (see positive results afas identified (Gepositive, true po
e described by thK tariffs were usedted studies). A d2.7.
S
udy of Lidgren e
ary diagnosis bress prior to answeence and no m
st one recurrenceral) within 1 yea
questionnaire,
diagnosed with a t recurrence morehe questionnaire,
atic disease
dies having usedof Lidgren et al.80
for the general Ssame instrument These utility valuTable 2.8).
fter screening, onrard et al.)83. Thsitive, false negae UK population d to valuate thesdescription of th
Screening Breast C
et al.
reast of ering the etastatic
ce (loco-r or less and no
primary e than 1 , and no
d similar allowed
Swedish (EQ-5D
ues were
ne study his study ative and (and not e health e “false
Ainreoaareufawthd•
•
•
UIt3cpDCc•
Cancer
As showed in thisnvited for screenecalled for furth
obtention of a dassessment, only activity; pain/discoemaining two di
unaffected. The qalse positives laswere measured fherefore not be udecided to make th True negativ
population. The short term
the percentag This impact is
screening accet al.82 (generet al.80 (non mwere used.
Utility values for fat should be noted3.3 assessed the complexity and bepositive” in the stuDomeyer et al.84 inConcerning the evcancer in the long
s table, the descrining, having a brher examinationiagnosis, i.e. nothree of the five E
omfort; and anxietmensions (i.e. m
quality of life effecsted 12 months for the remainin
used to measure the following assu
ve patients have
m impact of positge change betwees present until the cording to IMA daral population for metastatic or met
alse positive and t that the study of short term impa
ecause the biopsyudy of Gerard et anto account. volution of utility vterm, no study wa
ption include the reast screen, wais, having furthe
o evidence of brEQ-5D dimensionty/distress and it
mobility and abilcts associated wwhile true positivg life expectancthe short term immptions:
e utility values e
ive results at screen true negative a
diagnosis, i.e. onata. After, either v
false positive) ortastatic disease y
true negative can Domeyer et al.84
ct of biopsy. Howy is included in theal.83, we decided t
alues for patientsas found.
KCE Report
following stage: iting for results, er examinations reast cancer. Fos were used, i.e. was assumed thaity of self-care) ith true negativesve and false neg
cy. These valuesmpact of screening
equal to the ge
eening is measurend false positive.
n average 45 daysvaluations of Bursr valuations of Lid
year 1 for true po
be found in Tabledescribed in app
wever, to avoid me description of a to not take the stu
s with metastatic b
t 176
being being
and or the usual at the were
s and gative s can g. We
eneral
ed by
s after ström dgren
ostive)
e 2.8. pendix model “false
udy of
breast

KCE Report 176
Table 2.7: Des
Routine breast
Further tests
The results of are ready wweek
Quality of life eroutine screening (sho
Receiving invitation
Waiting for ththe appointme
6
cription of a “fal
t screen • S• T• T• A• T
c• S• O• T• T• T• T• F
bthe tests
ithin the • T
effects of breast
ort term)
The Qconti
the • M• S
he day of ent
• M• S
c• P
lse positive” stat
She is invited by lThe appointment The visit at the breA female radiograTo take the X-raycompressed to geShe is asked by leOther tests are neThis visit may takeThe breast X-ray The doctor examiThe doctor may cFluid from the affebetween the X-rayThe tests show no
QoL of some womnue for some time
Most women are Some women are
Most women carrySome women arecarry on with theirPersonal and sex
S
te (Gerard et al)8
etter for routine bis about 2 weeks east screening ce
apher asks about ay she is asked to et the best possibletter to go to the beeded because the up to half a dayis repeated. nes her breasts.arry out an ultrasoected area is takey plates. o evidence of brea
men is affected bye.
pleased to receivee made nervous, a
y on with their usue anxious and depr usual activities aual relationships m
Screening Breast C
3
breast screening.from receiving the
entre takes about any symptoms or undress to the w
le picture. breast screening ce breast X-ray res.
ound examinationen for laboratory a
ast cancer.
y the experience
e the invitation. anxious or depres
ual activities and ipressed, unable toand interests. may be affected.
Cancer
e invitation. half an hour, whichistory of breast
waist. Each breas
centre the followinsult is not clear.
n. analysis using a fin
of routine breast
sed, and are worr
interests. o concentrate, sle
ch may include wadisease and explat is placed in turn
ng week.
ne needle to do th
screening and br
ried about having
ep badly and are
aiting time. ains what will hapn between two sp
his her breast may
reast cancer diag
breast cancer.
moody and irritab
ppen. pecial X-ray plates
y again be compre
nosis. The effects
ble. They are una
39
s and
essed
s may
ble to

40
At the breast sclinic
Waiting for the
Clear results test
Table 2.8: Des
Author (year)
Lidgren et al. (2007)80
Burström et al. (2001)82
Gerard et al. (1999)83
screening • M• M• M• M• S
e results • M• S
t• PIf rec
• M• O
after the • M• S
cription of the se
Instrument Pd
EQ-5D
S(
EQ-5D S(
EQ-5D Wy
Most women are Most women are Most women are Most women find Some women findMost women carrySome women areto carry on with thPersonal and sexcalled for further te
Most women are vOne of the tests, wMost women are Some women rem
elected utilities
Population for hedescription
Sweden patients(Mean age: see h
Sweden patients(Mean age: see h
Women from UK ayears (eligible for
S
nervous, but are nnot embarrassed not unduly worriedthe breast X-ray i
d the breast X-rayy on with their usue anxious and depheir usual activitiesual relationships oests:
very anxious at bewhere the doctor reassured by the
main anxious for u
ealth state Po
ealth states)
UK
UK
UK
ealth states) UK
aged 40-64 screening) UK
Screening Breast C
not anxious or depby the screening d about breast cais uncomfortable a
y very uncomfortabual activities and ipressed, un-able s and interests. of some women m
eing recalled for fremoves fluid fromclear results.
up to a year before
opulation for valu
K tariffs (general p
K tariffs (general p
K tariffs (general p
K tariffs (general p
K tariffs (general p
Cancer
pressed. procedure.
ancer developing.and slightly painfuble and painful. interests. to concentrate, s
may be affected.
urther tests. m the affected are
e they are back to
uation Hea
population) Prim
population) Brea
population) Meta
population) WomWomWom
population) True
ul, but this is short
leep badly and ar
ea, is painful.
o their usual self.
alth state
mary breast cance
ast cancer (follow
astatic patients; M
men aged 50-59men aged 70-79men aged 80-88
e negative
t lived.
re moody and irrit
er (Year 0-1); Mea
wing years); Mean
Mean age 56
KCE Report
table. They are u
Meavalu
an age: 56 0.69
age: 58 0.77
0.68
0.830.790.74
0.94
t 176
nable
n ue
6
9
5
3 2 0
0

KCE Report 176
2.3.2.3. Poo
chaA summary of can be found inal.82 were chos(A)). These valchange relativepercentage chaThe next stageassumed that uvalues in the gutilities betweecalculated, i.e.negative womeafter screening utilities will be m
6
oling of selectedanges selected utilities n Figure 2.2. Theen as the initial vues varied accord
e to these valuesanges did not varye concerns the shutility values for tgeneral populatioen true negative -16% (B). Initia
en and decreased(false or true pos
maintained for 45
d studies and cal
and of calculatioe utility values of alues of the modeding to women ag
s was applied. It y according to the hort term impact true negative wom
on (A). Then, the women and fal
al values were td by 16% for womsitive). As mentiondays.
S
lculation of perc
n of percentage cthe study of Burs
el (first state of thge. Then, the perwas assumed thwomen age (no dof the screening
men were equal percentage decr
se positive womthus maintained men with a positivned in the section
Screening Breast C
entage
changes ström et
he model rcentage at these data). g. It was to utility rease in
men was for true
ve result 0, these
Fvoscwb(Fn1pcth(
Cancer
For the first year values equal to thof the study of Lidstudy of Lidgren changes between women aged 50-5by 16% ((0.696-0.(0.685-0.833)/0.8
For the next yearnon-metastatic or
6% (C) and 18%patients who staycompared to the ghe years after (DG).
of screening, wohe general populadgren et al. wereet al.80 and the values for the sa
59 (and UK tariffs.833)/0.833) for n33) for metastaticrs, people from tmetastatic breas
% (E) respectivelyyed in this staggeneral populatio
D). Metastatic pat
omen without breation (A). For true used.80 To makestudy of Burström
ame population ws). Utility values wnon metastatic pac patients (E). the general popust cancer had utiy (as calculated age had their utilin ((0.779-0.833)/0ients maintained
east cancer had e positive, utility ve the link betweem et al.82, perce
were used, i.e. Swwere therefore redatients (C) and by
ulation who develity values reduce
above). Non-metaity decreased by0.833) and mainttheir utility until d
41
utility values en the ntage
wedish duced y 18%
loped ed by
astatic y 6% ained death

42
Figure 2.2: Per
Women age
Before
rcentage change
ed = 70 years
e screening
A
e in utilities
P
Short termscreeni
S
Positive results
True negative
False positive
True positive
m impact of theing (45 days)
B
A
Screening Breast C
Wome
Brea
Brea
A
N
Brea
Brea
Cancer
en aged = 70 yea
ast cancer stage II
ast cancer stage II
After screening(First year)
C
A
Non metastatic
ast cancer stage I
Metastatic
ast cancer stage IV
F
rs
I
I
VMetastatic
Women aged = 7
Breast cancer st
Breast cancer st
Breast cancer st
After screeni(Following yea
F G
C D
A
Non metasta
Breast cancer s
KCE Report
c
70 years
tage II
tage III
tage IV
ingars)
E
atic
stage I
t 176

KCE Report 176
2.3.3. DiscuTo include thevalues for eachthis chapter waon the KCE phamultiple instrumderived from the• The analys• No Belgian
possible (nUK tariffs results, Be
• The short taccount be
• Even if thethese utilitithis instrumConsequensuch as aimportant instrument low percenwomen in metastatic specific insbecause th
• Finally, thebetween reappendix 3parametersthese para
6
ussion quality of life im
h health state of tas therefore to searmaco-economic
ments and multiple EQ-5D instrume
sis had the followin data were availano access to priminstead of Belgialgian data would bterm impact of su
ecause no valid dae EQ-5D is one oies (according to ment is less senntly, it can be expa mastectomy (pif a disease sphad been used.
ntage change bethe general pop
patients. The assstruments was nehese instruments de review of the eported utility esti3.3), revealing as. Because of thmeters should be
mpact of screeninthe model had to lect these valuesc guidelines79. Wee valuations and ent. ng limitations: able and a transf
mary data). Even ian valuations wobe interesting for urgery and of diagata were availableof the best availathe KCE pharma
nsitive than diseapected that the impartial or total) pecific instrumen This lack of senetween patients pulation or betwsessment of the qevertheless not indo not permit to dliterature showedmates for breast
a high level of uhis uncertainty, a
e done in the chap
S
ng in the analysibe identified. The. The method wae tried to avoid th
focused on utility
ferability analysis if we expected th
ould not greatly infuture models. gnosis was not tae. able instrument toaco-economic guidase specific instrmpact of some cowould have bee
nt instead of a nsitivity could expwith breast caneen metastatic a
quality of life from vestigated in this erive QALYs.
d an important vcancer health sta
uncertainty arouna sensitivity ana
pter on model resu
Screening Breast C
is, utility e aim of
as based e use of y values
was not hat using nfluence
aken into
o assess delines), ruments. onditions en more
generic plain the cer and and non disease chapter
variability ates (see nd these lysis on
ults.
3TsacbwWthsnfiUWththbuh••
•
Cancer
3. DECISIOTo quantify whatsituation we consapproaches. For cancer registry anbelow). For the sewith annual cyclesWe consider perfohan trying to adasituation. Indeed, not available andindings of these mUS) data. We look at the effehe currently existhe current level. Tbaseline without huse of an additionhere: Available data Additional lite
screening and The model us
ON ANALYt the implicationsstructed a decisiothe first simple
nd data from the lecond, we constr
s. orming one Belgiaapt the models dBelgian data nee
d we would memodels, as we wo
ect of introducing ing situation with This has the advahaving to modify nal number of no
a used in this decierature review focd to the breast cansed for this decisio
YSIS s of our findingson analysis modapproach, we apliterature on the Bructed a simple t
an decision analydiscussed in chaeded to parameterely reproduce t
ould be obliged to
mammography sthe opportunistic
antage that we cathen, as this can
on verifiable assu
ision analysis; cused on qualityncer as such; on analysis.
s are on the Beel using two diff
pplied data from Belgian life tablestime dependent c
ysis a better apprapter 2 to the Beerize these modelthe already publo use the same (m
screening in additscreening going
an use Belgian da only be done m
umptions. We des
y of life related t
43
elgian ferent IMA,
s (see cohort
roach elgian ls are ished
mainly
ion to on at
ata as aking scribe
o the

44
3.1. Data soBelgian life tabOverall survivabe.STAT (http:/Belgian CanceThe Belgian Ccollects data cstatistics from tBelgian organAs recommendorganized screeprogram are woprograms ahttp://www.brumdépistage desFrançaise) andhttp://www.zorgIntermutualistiThe Intermutuasickness fundsnational screendefined by theinformation on focus on the tconfirmation anDutch Nation(DNETB)85. The Dutch Npublished a recontaining inforpopulation.
ources ble (2009) al was taken fro//statbel.fgov.be) er Registry (BCRCancer Registry Fconcerning new chese data (http://wized screening
ded by Europeanening programmeomen aged 50 to are organizedmammo.be/), Cens cancers (CCRd BorstKankerOpg-en-gezondheid.bic Agency (IMA)
alistic Agency (IMAs. IMA compiledning program cone program (50-6
persons outsidetests used, delaynd treatments follonal Evaluation
ational Evaluatioeport with their rmation on age s
om the Belgian
R) Foundation is ancancer cases in www.kankerregist
Commission, Bee. The target age 69 years. Belgiand by: Br
ntre CommunautaRef: http://www.cpsporing (BKO) (be/).
A) centralises dat and published
ntaining data on t69 years). IMA e the target ageys between screeowing testing (http
Team for Bre
on Team for Bfindings covering
specific stage dist
S
life table of 200
n public institutioBelgium and ma
ter.org/).
elgium started a groups as define
n breast cancer scrumammo (Baire de Référenceccref.org/) (Comm(Vlaamse Gemee
a coming from allseveral reports
the target age grcomplemented t-group, with a pening tests and p://www.nic-ima.beeast cancer sc
Breast cancer scg the period 19tributions in the s
Screening Breast C
09 from
n which akes up
national d by the creening ruxelles,
e pour le munauté enschap:
Belgian on the
roups as his with
particular possible e/).
creening
creening 90-2007
screened
STNin(lointh
3InmfrB7folelisaaacTdtiT•
Cancer
SEER database The Surveillance, National Cancer Inn an effort to redhttp://seer.cancerocations and sourn 1973. As they hese in the mode
3.2. Model den a first simple amortality caused brom the results oBelgian life table.74 is similar to tollowing Barratt eevel over first fivenearly to nothing
saved can then band effects on quaand stage-shift is approach was onlcomplex approachThe second apprdata on incidenceime dependent stThe model compa A cohort of w
the populationparticipates inby screening,screening. Thcases (intervaThe screen dthan the canc
Epidemiology, annstitute works to duce the burden r.gov/). SEER collrces throughout thused an outdatel.
escription approach we appby screening comof the meta-analWe assume herethe reduction in et al 200536 that e years after startg over five yearse derived from thality of life resultinmore difficult to a
ly used for cross h that makes use oroach makes usee of invasive cancate transition cohres 2 cohorts:
women starting at n in the age gron the screening an, depending on p
here is a mix of scal cancers and cdetected cancers ers not detected b
nd End Results (Sprovide informatioof cancer amon
lects data on canche United States.d distribution we
plied the 22% reduming from RCT alysis of Gøtzschee that the reductio
other age groupbenefit accrues
ting screening ans after stopping he life table. Howng from earlier diaassess in this apvalidation by com
of the stage-shift e of the Belgian Ccer and DCIS forort model with an
age 70 where scup 70-74, where nd where a part oparticipation rate creen detected ancancers amongstwill have a diffe
by screening.
KCE Report
SEER) Program oon on cancer statg the U.S. Popucer cases from va Data collection bcould not incorp
uction in breast cand its range, rese et al, 20084 oon in women ageps. We also asslinearly to a mad that benefit decscreening. Life
wever, effects of hagnosis, over-diagpproach. Thereforemparing it with a caused by screen
Cancer Registry (r the constructionnual cycles.
reening is extenda part of the wo
of the cancers is fand sensitivity o
nd not screen dett unscreend womerent stage distrib
t 176
of the tistics lation
arious began porate
ancer sulting n the
ed 70-sume, aximal clines years
harms gnosis e this more
ning. BCR)
n of a
ded to omen found of the ected
mens). bution

KCE Report 176
• A cohort o
extended bthe stage d
All women are number of QAcompared. OveWe assume tha• Survival an
the tumor women, an
• All benefit in stage-dis
Harm caused accounted for sinterval in theproportion womthe screening roFigure 3.1 showtransitions betwIn the unscreenyear are determ• Incidence o• Stage distr• Stage spec• Age specifOn top of that, fdetermined by s• Lead time a• The propo
found by sc
6
of women startinbeyond the age ofdistribution of the followed to deathLYs and deaths
erall mortality is noat: nd quality of life oat the moment t
nd not on the presof the screening rstribution caused by false positiv
separately, by asse participation wmen that are alive ound actually takews the different c
ween them. ned cohort, transi
mined by: of breast cancer; ribution of unscreecific survival; and ic overall mortalityfor the cohort whesome aspects of tas part of the can
ortion of cancers creening and thei
g at age 70 whef 69 years. For thnon screened.
h. The cumulativeto breast cance
ot compared as in
f the women depethe tumor is detesence or absence results from the sby the screening.
ves at the momesuming 3 screeniomen and applyand without brea
es place. compartments in
itions between co
ened cancers;
y due to other cauere screening takethe screening: cers will be foundfound by scree
r respective stage
S
ere the screeninhis cohort all wom
number of life yer of the two coh
n the end everybod
ends only on the ected and the agof screening; tage-shift, the diff. ent of the screeng rounds with a ying recall ratesast cancer at the
the two cohorts
ompartments from
uses. es place, transitio
d earlier; ening and propore distributions.
Screening Breast C
g is not men have
ears, the horts are dy dies.
stage of e of the
ferences
ening is 2 years
s at the moment
and the
m year to
n is also
rtion not
AddsymTmea
Cancer
As survival and diagnosis in the mdiagnosis and stscreening is applieyears (or 3 in senmanageable. Transitions betweemoment the diagnevolves after treaanymore.
quality of life dmodel, a separateage, and stage ed during 5 years nsitivity analysis)
en stages are notnosis is made follatment it does no
epends on both e compartment is
specific survivaland there is an athe number of co
t included as stagelowed by treatme
ot necessarily go
age and time made for each a
l is than appliedassumed lead timeompartments rem
es are assessed aent. Even if the ca
through the 4 s
45
since age of d. As e of 2 ained
at the ancer tages

46
Figure 3.1: Co
Cohorscree
Cow
scre
mparison of the
Healthy women
Healthy women
rt with ening
ohortwithout eening
two cohorts with
Id
is
S
h and without a s
Invasive cancer detected by screeni
DCIS
interval cancer in screened women
Invasive cancer in unscreened wome
Invasive cancer in unscreened wome
DCIS
Screening Breast C
screening progra
IIIIIIIV
IIIIIIIV
IIIIIIIV
IIIIIIIV
ing
en
en
Cancer
am
All c
All c
cause deaths
cause deaths
KCE Reportt 176

KCE Report 176
Figure 3.2: Co
6
mpartments in th
Healthy women
he two cohorts a
d
S
and the transition
Breastcancer stage I
Breastcancer stage IV
Breastcancer stage II
Breastcancer stage III
DCIS &over‐
diagnosed
Screening Breast C
ns between them
Death
Cancer
m
47

48
3.3. Descrip3.3.1. Age sOverall survivabe.STAT (http:/mortality based3.3.2. BreasFor the baselinethe 4 stages fowere used. Thethe IMA data wmammography 172 on breastassume that anpurposes, so ware less contamFor the situatiogroup will increa• Lead time
because onumber of this shift dused 2 yeaanalysis.
• Over diagbased on review abodiagnosis e
• Over diagdifferent wDCIS per 1place comlimited amcontrast widrop in DC
ption of the parspecific overall sal was taken fro//statbel.fgov.be) on data from thest cancer incidene without screeninr invasive for the
ere is some opporwe infer that in in the past 2 yea
t cancer screenin important part owe choose to useminated by opportuon where screenase with a numbe, cancers that wo
of lead time. This cases in the foll
depends on the aars lead time in t
gnosis invasive the findings in th
ove under 2.1.3.5.excluding DCIS.
gnosis DCIS, weway: we use the o100 000 is twice
mpared to the agemount of opportu
th the Brussels caCIS is much less p
rameters urvival
om the Belgian after adjusting fo Belgian Cancer rnce ng the BCR data oage group 70-74
rtunistic screeningFlanders the covars is 18% (for deng in risk group
of this is also for de data issued fromunistic screening.ning takes place,er of cancers comuld have appearewill lead to a co
lowing years. Theassumed lead timthe baseline and
cancer, we modhe literature as d. We assume a ra
e model the overobservation that iin the group 60-6e-groups 70-74 anistic screening apital region and Wronounced. So we
S
life table of 200or breast cancer register.
on incidence of D4 of the period 20g in that age grouverage with at leetails see the KCps)2. Given that diagnostic and fom Flanders becau , incidence in thing from two sour
ed later but are fouompensatory dece moment and deme (see point 3.2
3 years in the se
deled the over ddescribed in the lange of 2 to 30%
r diagnosis of DCn Flanders the in
69 where screeninand 75-79 wheretakes place. Th
Walloon region we take as an estim
Screening Breast C
09 from specific
DCIS and 04-2008
up. From east one
CE report we can llows up use they
e 70-74 rces: und now rease in egree of 2.2). We ensitivity
iagnosis iterature for over
CIS in a ncidence ng takes e only a his is in
where the mation of
3W3T6c7Ws3WsbsthmApaTthp
Cancer
over diagnosithe age-groupfact that screeDCIS. This brwomen per ye
3.3.3. ParticipaWe used a 70% pa3.3.4. ProportioThe data of the Be69, 49% of the cascancer or not part75% of the found We used a proporscreening of 70%3.3.5. Recall raWe assume a recscreening programbe an extension sensitivity analysishe more pessimmoment in certain As a baseline we plausible range foand adding 20%). The short term imhe percentage chpositive results.
s the difference ips 60-69 and 70-ening coverage isrings us to an oveear. ation rate articipation (plauson of screen detelgian screening pses are found by ticipating in the sccancers are screertion of cancers fo(plausible range 6ate call rate of 3.5%m concerning folloof the screening
s we used 2% in aistic scenario (1regions). assume a delay
or the sensitivity a
mpact of positive rhange in utility va
in DCIS incidence-74, augmented b only 60% as a prer diagnosis of DC
sible range 60% totected breast caprogram show thascreening, and thcreening. Among en-detected and 2ound among the w60% to 80%).
% based on the dow up rounds (as
g among women an optimistic scen0% recall rates
of 45 days, baseanalysis of 36 and
results at screenialues between tr
KCE Report
e in Flanders betby 1.5 to adjust foroxy for overdiagnCIS of 40 per 100
o 80%) as baselinancers at in the age grouhe rest is either in
the screened wo25% is interval cawomen participat
data from the Fles the screening waged 50-69. Fo
nario and 5 and 10are observed fo
ed on IMA data, wd 45 days (subtra
ing were measurerue negative and
t 176
tween or the nosed 0 000
ne.
up 50-terval
omen, ancer. ing in
emish would or the 0% in
or the
with a acting
ed by false

KCE Report 176
3.3.6. StageWe take estimascreened and uprovided by theFor the stage dstage distributioyears 2004 - underestimatedgoing on, see aFor stage distriis based on thecancer screeninfor the age gdistributions frostage shift we tnot have date stage distributiobe the same, baThe Flemish sscreen detecteparticipants, coperiod 2001-20non participants
6
e distribution andations of the stagunscreened from
e Flemish screenindistribution in the on amongst wom2008 a good es
d as there is somabove. bution in the scree data from the Dng report of 2009group 70-74 froom different sourthink this approximon screen detecton of cases amonased on the data screening prograed cancers, interollected amongst06. Stage distribus is very similar.
d stage shift ge distribution fothe BCR data o
ng program. unscreened wom
men in the group 7stimation. The stme opportunistic
eened population, Dutch National Ev9 (DNETB)85 whom 1998-2007. Arces is a suboptmates best the Beted cancer in thisng the non screenfrom the Flemish m provided datarval cancers andt women who gaution of interval ca
S
r breast cancer aon the Flanders a
men, we can cons70-74 in Flandersage shift will bescreening in tha
the base case esvaluation Team foo provide data speAlthough using 2timal way of modelgian situation, as age group. We ned and interval cscreening progra
a on the stagesd cancers amonave their consenancers and cance
Screening Breast C
amongst and data
sider the s for the
e slightly at group
stimation or Breast ecifically 2 stage deling a
as we do assume
cancer to m. among gst non
nt in the r among
TinF
S
I
II
II
IV
T
T
ScsBp2S
Cancer
Table 3.1: Stage nterval cancers Flemish screenin
Screencancer
Stage n
2586
I 1306
II 232
V 15
TOTAL 4139
This baseline stag
Stage distributioncancers not founscreening BCR data (Flemispopulation,70-74y2008) Stage %
I 31.6II 42.3III 16.6IV 9.5
distribution amoand cancers a
ng program 2001
n detected rs
In
% n
62.5% 62
31.6% 65
5.6% 20
0.4% 24
100% 15
ge shift we call Sce
n of nd by
sh y, 2004-
%
6%
3% 6% 5%
ong screen deteamong non part-2006.
nterval cancers
%
24 41.5%
56 43.6%
00 13.3%
4 1.6%
504 100%
enario 1:
StacanscrDascrSt
ected breast canticipants, age 5
Cancers amonon participan
n %
1454 41.8%
1460 42.0%
493 14.2%
71 2.0%
3478 100%
age distribution oncers found by reening
ata of the DNETBreening report 20tage %
I 80%II 18.7III 0.8%IV 0.5%
49
ncers, 50-69,
ngst nts
%
%
%
%
%
of
B 009
% % % %

50
Important remscreen detectecancers and nfound by screeother parameteFor the sensitivAs the stage dBreast cancer scan be achievethe stage-distribfrom the FlemisThis we call Sce
Stage distributcancers not foscreening BCR data (Flempopulation,70-2004-2008) Stage
I 3II 4III 1IV
In a third scenaInstead of usinwomen, we assthe stage distribthe stage distrifor Flanders fro
mark: It is imported cancers and
nonparticipants kening. In most cas
er values of the scvity analysis we usdistribution from screening report od in the Belgian cbution for screen sh cancer screeninenario 2:
tion of ound by
mish -74 years,
%
31.6%
42.3% 16.6% 9.5%
ario we use a slighng stage distributsume that introdubution amongst albution of the wom
om the Belgian bre
tant to note that that in the coho
eep the stage dses this is around creening and variese 2 supplementathe Dutch Natioof 2009 may be mcontext, we used a
detected patientsng program.
htly different modetions amongst sccing screening in ll breast cancer cmen 60-69 in the east cancer regist
S
this shift concerrt with screeningistribution of can50% but depend
es in time. ry scenario’s: nal Evaluation Tmore favorable thas an alternative ss of the age grou
Stage distribucancers foundscreening (Flescreening pro(50-69 years)Stage
I 62II 31III 5IV 0
eling approach. creened and unsthe group 69-74
cases in the popusame period, us
try.
Screening Breast C
rns only interval ncer not s on the
Team for han what scenario up 50-69
ution of d by emish ogramme
%
2.5% 1.6% 5.6% 0.4%
screened will shift
ulation to ing data
T
ScsBp2S
3Ssywasw•
•
Cancer
This we call scena
Stage distributioncancers not founscreening BCR data (Flemispopulation,70-742004-2008) Stage %
I 31.6II 42.3III 16.6IV 9.5%
3.3.7. Stage spStage specific susurvival data (takeyears. We used website (http://wwappendix 4.1). Wescreened and unswe used also: Entirely the
stagegroup. Tfor women areflect the facwell but it is aMoreover, theyears ago, thi
British surviv(http://info.canbut survival isof the problemsurvival of pevolution in br
ario 3
n of nd by
sh years,
6%
3% 6% %
pecific relative survival was takenen from KCE repodata from the D
ww.cijfersoverkanke assumed that sscreened breast c
Dutch survival dThe relative survivbove 70 compar
ct that older womealso possible thate data include pas may also explaival data comingncerresearchuk.ors considerably lowms with 10 year ersons treated areast cancer treat
StaamcanlevlevFlaSta
IIIIIV
urvival n from Belgian ort 150A)86. We oDutch cancer regker.nl) to supplemurvival conditiona
cancer patients. A
data for women val curve shows aed with the overen support the invt there is undertreatients that were in the lower relativg from breast rg/) They provide
wer than the Dutchsurvival data is t
at least 11 yearstment this is a lon
KCE Report
age distribution mongst all breast
ncers if screeninvels are similar tovels among 60-69anders age %
I 45.7% I 35.9% II 12.5% V 5.9%
stage specific aonly have data upgister taken from
ment until 7 yearsal on stage is simAs a sensitivity ana
above 70 yearsa lower relative surall survival. Thisvasive treatmentseatment of the eltreated more tha
ve survival. cancer research10 years surviva
h or Belgian datathe fact that it res ago, given theg time.
t 176
ng o 9 in
nnual p to 5 m the s (see ilar in alysis
s per urvival s may s less derly. an 20
h UK l data . One
eflects e fast

KCE Report 176
• Belgian su
coming frotreatment a
We did not useso that survivaland difficult to iThe survival cu3.3.8. QALYNumber of life was adjusted fo(see point 2.3).We made some• Utility value
age but penot vary acthis). For increase.
• Patients wpopulation.
• In the asseresults, moby screenin
6
urvival data supplom87. The problapply here as for te US SEER data l curves per stagencorporate in the rves can be found
Y years was calculor the quality of l
e assumptions: es at start of the mrcentage changesccording to the agthe sensitivity a
with negative resu. essment of utility obility and ability ong.
emented by Frenlem of the evothe British data. as they use an o
e are not comparmodel.
d in the annex.
lated for each stalife (QALYs), bas
model (before scrs relative to thesege of the women analysis, we app
lts had utility val
values for true neof self-care were a
S
nch 10 year surviolution in breast
outdated staging rable to the other
age and a stage sed on a literature
reening) were strae values were ass(we did not have
ply a 20% redu
ues equal to the
egative and false assumed to be un
Screening Breast C
val data cancer
method, sources
and this e search
atified by sumed to
data on ction or
general
positive naffected
•
•
•
P
Cancer
In the study oonly two grouTherefore papatients) weresupported by same for patquality indicatchange this ptreated by coassumption aimpact of pcorresponding
Utility values fmetastatic paFor non-metastudy showinNevertheless,QALYs for tak
At baseline, wdiscount rates
Parameters used i
of Lidgren et al.80, ps, i.e. the first ye
atients in stage e assumed to hathe fact that for yients in stage I, tors in breast canicture because monservative surge
are not available partial versus tog to our inclusion for non-metastatic
atients were assuastatic patients, thng no significant , as a sensitivity king into account awe did not discous of 1.5%, 3% andin the model are s
non-metastatic pear of diagnosis aI, II, III (groupeve the same utili
years 2001-2006, II, III according
ncer86. Note that any cancer foundery. Neverthelessand we found nootal mastectomycriteria. c patients (after thumed to remain chis assumption isdifferences at y
analysis we applya variation of utilitunt QALYs. For thd 5% were appliedshown in table 3.2
patients were dividand the following yed as non metaty. This assumptthe treatment wato the KCE repomore recent data
d by screening ares, data to proveo study compariny on quality of
he year of surgeryconstant across ys supported by ayear 5, 10, and y a 20% decremety values across yhe sensitivity anad. 2.
51
ded in years. astatic ion is
as the ort on a may e now e this g the f life
y) and years. n US 1581.
ent in years. alysis,

52
Table 3.2: Para
Parame
3.3.1 Age spe
3.3.2 Breast c
Lead tim Over-dia
cancer Over-dia
3.3.3 Participa3.3.4 Proporti
detected3.3.5 Recall r
Durationpositive
QALYs
3.3.6 Stage d
Stage I Stage II
ameters used in
eters
ecific overall surviv
cancer incidence
me agnosis invasive
agnosis DCIS
ation rate ion of screened d cancers ate
n of period after result lost in this period
istribution
the model
No screenin
val Belgian life-
BCR data (Flanders population, 2008)
BCR data (Fpopulation, 74years, 202008)
31.6% 42.3%
S
ng Base c
table Belgian
2004-
BCR dpopulaincreasover-diinvasivDCIS 2 years10.0%
40/100year 70.0%70.0%
3.5% (screen45 day
16.0%
Flemish 70-04-
Data oscreen
80.0%18.7%
Screening Breast C
case
n life-table
ata (Flemish ation, 2004-2008) sed by lead time.iagnosis ve cancer of
s
0 000 women per
Flemish ning program) ys
f the DNETB ning report 2009
Cancer
Sensitivity ana
Belgian life-tabl
BCR data (Flemincreased by leacancer of DCIS
3 years range from 3 to
40/100 000 wom
range from 60%range from 60%
range from 2%
range from 36 t
estimated betw
Scenario 2 Stage distributioFlemish screenprogramme (50
62.5% 31.6%
alysis
le
mish population, 2ad time. over-diag
30%
men per year
% to 80% % to 80%
to 10%
to 54 days
een 13% to 19%
Sceon of ing
0-69)
StagBCR60-6not
45.735.9
2004-2008) gnosis invasive
nario 3 ge distribution of R (Flemish women69 (screened and screened)
7% 9%
KCE Report
n
t 176

KCE Report 176
Stage I Stage IV
3.3.7 Stage s
survival
3.3.8 QALY Stage II
Stage II
Stage IV
Age rela
Discoun
6
II V
pecific relative
III IV
I IV
V
ated QALY
nted QALY
16.6% 9.5%
Belgian stagspecific annsurvival datasupplement7 years by Ddata -constant
-constant
-constant
-constant
S
0.8% 0.5%
ge nual a ed until Dutch
Belgianannualsuppleyears b
- const
-consta
-consta
-consta
Screening Breast C
n stage specific l survival data mented until 7 by Dutch data
tant
ant
ant
ant
Cancer
5.6% 0.4%
Dutch survival osurvival
-20.0% -20.0% -20.0% range from + 20 discounting rate
12.55.9%
or British survival
0% to -20%
e + 1.5%. 3% and
5% %
or Belgian/French
5%
h
53

54
3.4. ResultsIn the baseline of life saved pe395 per 100 00deaths would bbeing a reductioBecause of themodel structureis not due to rasource of inforsensitivity anaprobability-distrTable 3.4 showused for this anand justificationThe number of assumptions. Tdifferent assumuncertain or vagained rather thapart from the vAssumed degreand under the QALY would bslightly, this duenew case in thebut the effect isRecall rates of Ten per cent reAssumptions onimpact on yeaBritish survival loss of QALYs French 10 year
s scenario the mod
er 100 000 (13,1 p00 (3.9 per 1000) be averted per 1on of 21% (numbee considerable une we did an extenandom error but drmation on the palysis, as it waributions in a mea
ws the results of thnalysis was discun of chosen valuesf years of life gainThe number of QAmptions. This is ariable parametehan on mortality, values accorded tee of over-diagno
higher assumedbe lost instead oe to the fact that e model, one couls very small.
10% also can shecall rates are actun the choice of thrs of life gained data increase thein certain scenari
r survival is somew
del predicts that thper 1000) women QALYs. The mod00 000 women ser needed to be oncertainty surrounnsive sensitivity adue to issues relaparameter. We das not possible ningful way.
he sensitivity analussed in 3.3, descs. ned remains fairlyALY gained or lost
partly due to thrs have an impasuch as high rec
to the QALYs. osis has a strong d values of 20%of gained. Years an over diagnosed argue that this i
hift the balance toually found in somhe appropriate sur
and QALYs gaie number of life yos. Belgian survivwhere in between
S
here would be 130invited for screen
del also predicts screened (1.3 pe
offered screening:nding the parametanalysis. Most uncating to the right cid not do a probto choose app
ysis, the plausiblecription of the par
y constant under t varies much mohe fact the a lotact on the qualitcall rates, over dia
impact on QALYsor 30% even imof life gained in
ed case cannot beis somewhat of an
owards a loss of me parts of Belgiumrvival curve have ned. The Dutch
years gained but lval data suppleme.
Screening Breast C
07 years ning and that 128
er 1000), 782). ters and certainty
choice of babilistic propriate
e ranges rameters
different re under t of the y of life agnosis,
s gained mply that ncreases ecome a n artifact
QALYs. m. both an and the ead to a ented by
InoTththQTndsIIegainAQAredp3Aredp1AGsy
Cancer
ncreasing the assof life gained and QThe model’s estimhe valuation of thhe decrease in qQALYs gained, asThe estimations conot vary much in decrement in quascenarios: (i) decrII and IV with 20effect of increasingains in QALYs duas persons in stagn contrast to the LAs could be expecQALYs gained. As a worst case secall rate at 10%
days and using thprogram (scenario307 QALYs per 10As a best case scecall rate at 2%,
days and using thprogram (scenario
626 QALYs per 1Applying the 22%Götzsche et al. tosimilar result, 139 years of life saved
sumed lead time tQALYs.
mation of the numbhese QALYs. Dimquality of life dues could be expecteoming from the Lfunction of the d
ality of life due toreasing stage II II0% or (iii) decreag the number of ue to the stage shge I have in this sLidgren data. cted, introducing d
scenario, we set th%, loss of QALYs he stage distributio 2). This gives a00 000. cenario, we set tloss of QALYs p
he stage distribuo 1). This gives a 100 000. % reduction in mo the Belgian life t
cancers deaths dd.
to 3 years has an
ber of QALYs gainminishing the age e to old age, deced. idgren’s paper areifferent stages. W
o increasing stageI and IV with 20%
asing stage IV wQALYs gained, bhift alone outside cenario a better a
discount rates de
he estimation of oper recall at 0.19ion coming from gain of 872 Yea
he estimation of per recall at 0.13 tion coming fromgain of 1704 Yea
mortality from thtable, as describedue to breast can
KCE Report
n impact on both
ned or lost depenrelated QALYs, t
creases the numb
e fairly uniform anWe introduced a le at diagnosis, w
%, (ii) decreasing ith 20%. This ha
because there arethe effect on mor
assumed quality o
creases the numb
over diagnosis at 9 during a period the Flemish scrers of Life but a lo
over-diagnosis aduring a period
m the Dutch scrers of Life and a g
e meta-analysis ed above, gives ancer avoided and
t 176
years
ds on this is ber of
nd do larger with 3 stage
as the e also rtality, of life,
ber of
20%, of 54 ening
oss of
t 3%, of 36 ening ain of
from a very
1145

KCE Report 176
Table 3.3 Mode
Scenario
Baseline
Worst case
Best case
6
eling results: bas
Assump
Over recall loss of Qduring astage Dutch (scenarioOver recall loss of Qduring astage Flemish (scenarioOver recall loss of Qduring astage Dutch (scenario
seline, worst and
ptions
diagnosis: rate at 3
QALYs per recall a period of 45 distribution comscreening prog
o 1) diagnosis: rate at
QALYs per recall a period of 54 distribution comscreening prog
o 2) diagnosis: rate at
QALYs per recall a period of 36 distribution comscreening prog
o 1)
S
d best case scen
Years of lPer 100 00women
10%3.5%0.16days ming gram
1307 gaine
20%10%0.19 days ming gram
872 gained
3%2%
0.13 days ming gram
1704 gaine
Screening Breast C
nario.
ife 00
Quality adPer 100 00women
ed 395 gained
d 307 lost
ed 1626 gaine
Cancer
djusted years of l00
d
ed
life
55

56
Table 3.4 Mode
Baseline Assumed over0.03 0.05 0.1 0.2 0.3 Recall rate 0.02 0.035 0.05 0.1 Period betweeduration 36 days 45 days 54 days Period betweeQALYs lost QALYs loss peQALYs loss peQALYs loss peParticipation r0.6
eling results: sen
rdiagnosis
en false positive
en false positive
eriod 13% eriod 16% er period 19% rate
nsitivity analysis
e and confirmat
and confirmatio
S
s.
Stagescena
Years1307 13041305130713101314 1307130713071307
ion test:
130713071307
on test:%
130713071307 1120
Screening Breast C
eshift ario 1
s of life QALYs395 526 489 395 208 22 442 395 348 190
417 395 373
416 395 374 281
Cancer
Stageshift scenario 2
Years of life1014 1011 1012 1014 1018 1022 1014 1014 1014 1014
1014 1014 1014
1014 1014 1014 869
Stsc
QALYs Ye186 12 317 12280 12186 120 12-187 12 234 12186 12139 12-19 12
208 12186 12164 12
207 12186 12166 12 102 na
tageshift cenario 3
ears of life QA246 420
245 551245 514246 420249 232251 45
246 459246 420246 380246 249
246 438246 420246 401
246 449246 434246 420
a na
KCE Report
ALYs 0
1 4 0 2
9 0 0 9
8 0 1
9 4 0
t 176

KCE Report 176
0.7 0.8 Effectiveness 0.6 0.7 0.8 Survival curveDutch survivalBritisch survivBelgian survivAssumed leadAll QALYs minAll QALYs plusStage II III IV -2Stage III IV -20Stage IV -20 Discounted QADiscount rate Discount rate 3Discount rate 5
6
screening amon
e by stage from ol val val supplementedd time 3 years nus 20% s 20% 20 0
ALYs 1.5% for QALYs 3% for QALYs 5% for QALYs
ngst participants
other sources
d by French data
S
13071493 112013071493 16071714
a 1460109813071307130713071307 130713071307
Screening Breast C
395 509 281 395 509 710 399 473 118 -948 1587 903 648 450 297 215 138
Cancer
1014 1159 869 1014 1159 1181 1148 1045 875 1014 1014 1014 1014 1014 1014 1014 1014
186 na270 na 102 na186 na270 na 310 14-3 1596 1377 11-1089 121310 12465 12370 12241 12 121 1267 1215 12
a naa na
a naa naa na
481 505585 374365 477169 187246 -78246 153246 na246 na246 na
246 274246 193246 114
5 4 7 7 7
34
4 3 4
57

58
3.5. DiscusUnder baselinelimited impact osaved, amountiin that period andays of life gainThis results fallfound as reportranged from 9 tthat completelyYears of life gachoose a worstfrom 872 to 170on the meta-anthat this estimaestimation methgained are fairlyThe gain in quonly 3.9 QALYwomen) offereddata in anothescreening for 5shows that undin this age groimportant of thcertain parts of addressed befoThe worst casescreened, we mare still reasonelements wereeffect is sometquality of life pQALYs gained This is due to false positives a
sion e assumptions, son breast cancer ding to 1.4 death and 13 years of lifened per women ofl within the rangeted by Mandelblatto 22 per thousan
y different data andained remained fat and best case s04. It correspondsalysis of Götzsch
ation comes from hod. This indicatey robust and consality adjusted life
Ys per 1000 womd screening and uer way by statin5 years to gain
der certain assumoup would actualese is an assum
f Belgium, so thesore proceeding. e scenario would made sure that thnable assumption not considered imes mixed. Brin
per age-group incdepending on ththe fact that intr
and over diagnosi
screening in the deaths avoided a
avoided per 1000 e saved per 1000 ffered screening. e that the modelett et al in 200948, wnd women screend model structureirly constant in thscenario, with yeas also with the sime et al.4 and the Ba completely diff
es that the estimasistent with other s years (QALYs) i
men (1.4 quality ncertainty is large
ng that 250 womone year of life.ptions introducinglly generate a lo
med recall rate ofse high recall rate
imply a loss of 3 e assumptions of
ns and not undulin the worst casging down the bacreases or decreae chosen values
roducing screeninis but gains due to
S
age group 70-74nd number of yeawomen offered scwomen, amountin
ers of the CISNETwhere years of lifened. This, despites were used. e sensitivity analyars of life gained mplified estimatioBelgian life tables,ferent source of dations of the yeastudies. is considerably leadjusted day of
er. One can presemen need to be The sensitivity
g breast cancer scoss of QALYs. Thf 10%, as is the
es should certainly
QALYs per 1000f this worst case sy extreme. A nuse scenario becaaseline estimationases the final nuof the other para
ng induces losseso the stage shift.
Screening Breast C
4 has a ars of life creening ng to 4.7
T project e gained the fact
ysis. We ranging
on based , despite data and rs of life
ess, with life per
ent these offered
analysis creening he most case in
y first be
0 women scenario
umber of ause the n for the umber of ameters. s due to
UsTyupocuuccatooisCZlin51freTitcbandoTsina
Cancer
Under the best cascreened. The higher variabyears of life losuncertainty arounparticular concernother hand rather countries and in uncertainty arounduncertainty concecancer states but cost-effectivenessaddressed if we wo stage IV has onor lost as survival s low. Carles et al. 201Zeelen, found an fe years gained p
not report the QA50-69, as it was
.86 QALYs per 1rom 45-69. Intereet al, 201158 into thThe model takes it does not take cancers would habecause screeninare not life threatenon screen detectdetected cases is of stage, and thatThis indicates thaselection of less anterval cancers hattending screenin
ase scenario one w
bility seen in the t has a numbed key parameter
ning over-diagnosreflects real undBelgium betwee
d the valuation oferning the qualitalso age specific analyses are
want to have meanly a limited impain this stage is s
138, in an adaptincremental bene
per 1000 women cALYs gained with
dominated by sc1 000 were gaineestingly, they did nheir calculations, nto account over-into account leng
ave a slower cling tends to pick-uening. Follow up sted cancer in thebetter than case
t survival of intervat there may indaggressive cancehave a better sung indicates that
would gain 16 QA
estimation of theer of reasons. Trs that determineis. Variability due
derlying differencen regions. Theref the quality of lify of life surrounquality of life in Bconsidered, this
aningful results. Qct on overall numhort and proportio
ation of the CISefit for biannual sccompared to a schextending the screening from 45-
ed by extending tnot incorporate thbut used US surv-diagnosis and leagth bias, the factical course and
up slow growing tstudies of screen
e literature show tes among non parval cases is somdeed be a lengtrs by screening.
urvival than canceother factors also
KCE Report
ALYs per 1000 wo
e QALYs comparThere is considee a loss of QALYe to recall rates oes in practice bete is also considefe, and this is notnding different bBelgium. If in the fs problem shoulQuality of life attribmbers of QALYs g
on of stage IV pa
NET model of Lcreening 50-74 ofhedule 50-69. Thecreening to 50-74- 69, but reportedthe screening to 4he results of Vilapvival data. ad time bias. Howt that screen-dethave a better sutumors some of wdetected cancers
that survival of scrticipants, indepenewhat in betweenth time bias, thrHowever, the facer among womeo play a role, suc
t 176
omen
red to erable Ys, in on the tween erable t only breast future d be buted ained
atients
Lee & f 2.78 ey did from
d that 45-74 prinyo
wever, ected
urvival which s and creen ndent n88-91. rough ct that n not ch as

KCE Report 176
selection bias amongst womeadjustment for sand on effectinecessarily negthreatening canimpact on efficand greater cosWe unfortunateunscreened woMoreover, therecurves that will survival may beAnother majordistributions of on stage distrcancers and thscreening are vWe choose a mshift and its coessentially tumoto stay closer incorporating pathat the model overall effect odetected basedcan only evaluaBelgium, we cahowever needeto use the samewe would just mIn conclusion, tchoice of the pthe results. ThYears of Life gthere is eviden
6
(such as the soen non attending stage. However leveness, as detegatively correlatencers at an earlierciency, as detectist for no benefit toely did not have domen, tumors foe is in general coapply in the futur
e outdated. r source of uncthe diagnosed c
ibution show thae cancer amongs
very similar. modeling approac
onsequences, in cor growth modelsto the data and arameters based is less flexible an
of screening on td on Belgian dataate the effect of thannot vary the sced to parameterizee parameters that
merely replicate ththere is considera
parameters, so a is uncertainty is
gained and QALYce that continuing
ocial class or othscreening) and reength time has no
ection of slow gre with the ability r stage. Length timon of indolent tu
o women. ata on stage spec
ound by screeninonsiderable uncerte, as treatment ev
certainty is the cancers and stageat the stage distst the people who
ch that is essentcontrast to most s. This has the adv
make less use on Belgian data, nd has more simpthe proportion of a in the group 50he screening schereening interval. We the CISNET mot are already usedhem. able structural unlot of caution is nreflected in the
Ys gained in the eg screening until
S
er health relatedesidual confoundo direct impact onrowing tumors dto detect potenti
me has indeed a numors means mo
cific survival for tung and interval ctainty around thevolves and actual
right choice oe-shift. The Flemtributions of the o do not participat
tially based on thCISNET models vantage that it alloof unobserved vabut has the disadplifications. We mcancers that are-69. This implies
edules actually in We do not have
odels and would bd in the published
certainty around needed when intewide range of esend result. Neverthe age of 74 ye
Screening Breast C
d factors ing after efficacy oes not ially life-negative
ore harm
umors in cancers. survival data on
of stage ish data interval
te in the
he stage that are owed us ariables,
dvantage model an e screen
that we place in the data
be forced models,
the right erpreting stimated rtheless, ears has
muthloa
Cancer
modest effect on tuncertainty on thehat under reasonoss of quality adjuacceptable level b
the number of Lifee effect on qualitynable assumptionusted life years. Itefore extending s
e Years Saved buy adjusted life yeas the interventiont is important to b
screening.
ut there is considears, and the data n may even leadbring the recall rat
59
erable show
d to a tes to

60
4. ANSWWhat are clinbreast canceryears?
4.1. Breast What is the effescreening on thfor breast cancobtain an extra predicts that 12(1.3 per 1000),
4.2. Delay bHow long is thcancer relatedbetween 4 and
4.3. OveralWhat is the effescreening on tyears) of breasunclear. Studiemortality reduct
4.4. MorbidWhat is the effescreening on min randomized cor reject the hycancer diseasemorbidity may bcurrently at ourthe most recentconservative sadvanced stage
WER TO CLnical benefits anr organized scre
cancer relatedect of an extensiohe breast cancer rcer between the 13 years of life fo
28 deaths would being a reduction
between the sce delay between
d mortality reduc7 years after scre
l mortality ect of an extensiothe overall mortast cancer organizes did not have tion.
ity ect of an extensio
morbidity? We foucontrol trials. In o
ypothesis that scre. Aim of screeninbe diminish by lesr disposal do not t data (KCE repor
surgery versus 3es (C Stage I an
LINICAL QUnd specific harmeening in wome
d mortality n (70-74 years) orelated mortality?ages of 70 and
or 1,000 women sbe averted per 1
n of 21%.
creening and th the screening action? The morteening
n (70-74 years) oality? The effect zed screening onstatistical power
n (70-74 years) ond no data relatether words, on theening reduces thg is to detect minss aggressive treenable us to ratifrt 150)86 show 58%38% of total mand II). Nearly 90%
S
UESTIONSms of an extenen between 70
f breast cancer orThe continued sc74 makes it pos
screened. The mo00 000 women s
he mortality rednd the associatedtality reduction
f breast cancer orof an extension
n the overall mor to detect an a
f breast cancer ored to the cancer mis basis we do nohe morbidity of thor tumors. Conseatment. The Belgfy this assertion. A% of the interventastectomies in th% of patients und
Screening Breast C
S nsion of
and 74
rganized creening ssible to odel also screened
duction d breast appears
rganized n (70-74 ortality is all-cause
rganized morbidity ot accept e breast
equently, gian data Actually, tions are he least dergoing
ctrtr
4Wre3sans
4Wtoo
4Wtrc7mgTmtoinfi
Cancer
conservative surgereatment of neoreatment.
4.5. False posWhat are the speesults? The Belg
3,5% in Flandersscreening round. Aand rates of false negative results screening round (B
4.6. AdditionaWhat are the speco forty additional offered screening
4.7. Over-diagWhat are the spreatment? Basedcases), ranged fro70 to 79 years amastectomies andgroups (no data sThree trials with amastectomies ando 1.42). Two trincrease in interveive trials combine
ery also receive ro-adjuvant chemo
sitive or false necific harms in tegian data currentlys and of 10% At this age groupnegative results aare 1.5 per 100BCSC-USA).
al diagnostic tescific harms in termpunctures or biop(three rounds).
gnosis and ovepecific harms ind on selected stom (7% to 21%) toare available). Gd lumpectomies wspecific for womeadequate randomid lumpectomies (Rals with subopti
entions (RR of 1.4d was 1.35 (95%
adiotherapy treatmotherapy, and 4
negative resultserms of false posy at our disposalin Walloon and , performance ofare relatively low.00 women aged
sts ms of additional diapsies may be expe
er-treatment n terms of overudies, over-deteco 35% (no data spGötzsche reportedwas significantly len aged 70 to 79ization showed a Relative Risk (RRmal randomizatio
42 (95% CI 1.26 toCI 1.26 to 1.44).
KCE Report
ment, 38% are giv1% receive hor
s sitive or false negl show a recall ra
Brussels regionmammography is For USA, rate of
70 to 79 years
agnostic tests? Twected per 1000 wo
r-diagnosis and ction (excluding pecific for women d that the numblarger in the scre9 years are availa
significant increaR) 1.31, 95% (CI)on showed the o 1.61)). The RR f
t 176
ven a mone
gative ate of n per s high f false s per
wenty omen
over-DCIS aged
ber of eened able). ase in ) 1.22 same for all

KCE Report 176
4.8. What acase of
It is advisable doctor should dIn this way, recommended:• Information• Decision m• Steering of
methods thThe criteria defmake provisionused, the doubthe recall rate95
criteria laid dowtherefore logicatowards these s
6
attitude should f self referral? that when a pat
develop a strategyan attitude stru
n specific to the agmaking according t
f the person whohat minimize the dfined in the frame for the monitorin
ble reading of the5. In Belgium, thewn in the contexal to steer those wstructures.
be recommend tient asks her doy minimizing the ductured around
ge bracket93 to the patient pers
o so wishes towardrawbacks. ework of the Eurong of the technicae mammographiese approved mammxt of the Europeawomen who expl
S
ded for women
ctor for a screendrawbacks of scre
three phases
sonal assessmentrds a screening i
pean Programmel quality of the eqs, and an optimizmography units man Programme, aicitly request a sc
Screening Breast C
n in
ning, the eening92. can be
t94 nvolving
e notably quipment zation of meet the and it is creening
Cancer
61

62
5. REFER1. Paulus
Good KnowleAvailabhttp://kc
2. Verleyerisk foscreenid'experAvailabhttp://wrisk-for-
3. Mambocancer of 40-4Health reports http://kc
4. Gotzscmammo2011(1
5. Nelson ScreenServiceW237-4
6. Bieshestudy moverdetLancet
7. Jorgensmammoinciden
RENCES D, Mambourg F
Clinical Practice edge Centre (KCble ce.fgov.be/index_e L, Desomer A, or breast canceing]. Good clinicartise des soins dble www.kce.fgov.be/p
-breast-cancertecourg F, Robays j,
screening with m49 years ]. Good Care Knowledge
129ce.fgov.be/index_he PC, Nielsenography. Cochra). HD, Tyne K, Naiing for breast ca
es Task Force. 42. uvel C, Barratt A,
methods and biastection with mamOncol. 2007;8(12sen KJ, Götzscheography screenice trends. Bmj. 20
F, Bonneux L. [B(GCP). Brussel
CE); 2005 02/05
_en.aspx?SGREFGailly J, Robays
er/technical methl Practice (GCP).
de santé (KCE);
publication/report/chnical-methods-fo, Camberlin C, V
mammography forClinical Practice e Centre (KCE);9 Av_en.aspx?SGREF M. Screening ane Database o
k A, Bougatsos Cancer: an update
Ann Intern Me
Howard K, Houssses on estimates mography screen
2):1129-38. e PC. Overdiagnong programmes009;339.
S
Breast cancer scrls: Belgian Heal
5/2005. KCE rep
=5221&CREF=93s j. [Identifying wohods for breast
Bruxelles: Centre2012. KCE Repo
identifying-womenor-breast-cancer-slayen J, Gailly J.r women in the a(GCP). Brussels:2010 07/07/201
ailable =14851&CREF=1for breast canc
of Systematic R
C, Chan BK, Hume for the U.S. Preed. 2009;151(10)
sami N, Irwig L. Eof invasive breas
ning: a systematic
osis in publicly or: systematic re
Screening Breast C
reening]. th Care
ports 11 from:
348 omen at
cancer e fédéral orts 172
from: n-at-sc . [Breast gegroup Belgian
10. KCE from:
16581 cer with Reviews.
phrey L. eventive :727-37,
Effects of st cancer c review.
rganised view of
8
9
1
1
1
1
1
1
1
1
Cancer
8. Virnig BA,situ of theoutcomes
9. HumphreyscreeningServices T
0. Tabar L, Grontoft Omass screBreast CaBoard of H
1. Dixon JMmastectom
2. Smith RArandomizelearned? R
3. Nystrom LRutqvist updated 2002;359(
4. Tabar L, Swedish Ton Breast
5. Maass N,Heerlein Ibreast. Arc
6. Duffy SW,time in brboth entryMed. 1995
7. FrachebouVerbeek Alimit for po2006;118(
, Tuttle TM, Sham breast: a system. J Natl Cancer Iny LL, Helfand M: a summary of Task Force. Ann I
Fagerberg CJ, O, et al. Reductioeening with mamancer Screening WHealth and WelfarM. Breast screemies. Breast Canc, Duffy SW, Gabed trials of breaRadiol Clin North L, Andersson I, LE. Long-term overview of the(9310):909-19. Vitak B, Chen T
Two-County TrialCancer Mortality Alkasi O, Baue. Actual managemch Gynecol Obste, Chen HH, Tabarreast cancer screy to and exit from5;14(14):1531-43.ud J, GroenewoudAL, et al. Seventyopulation-based m(8):2020-5.
mliyan T, Kane RLmatic review of incnst. 2010;102(3):1, Chan BK, Woothe evidence fo
ntern Med. 2002;Gad A, Baldeto
on in mortality frommography. RandWorking Group ofre. Lancet. 1985;1ning has increa
cer Res. 2009;11 e R, Tabar L, Ye
ast cancer screeAm. 2004;42(5):7Bjurstam N, Friseeffects of mam Swedish rando
TH, Yen AM, Col: Impact of Mamduring 3 Decades
er M, Jonat W, Sment of ductal caet. 2009;280(5):69r L, Day NE. Estimeening using a Mm the preclinical d. d JH, Boer R, Dra
y-five years is an mammography sc
KCE Report
L. Ductal carcinomcidence, treatment70-8. olf SH. Breast car the U.S. Preve137(5 Part 1):347orp L, Holmbergom breast cancerdomised trial fromf the Swedish Na1(8433):829-32. ased the numbeSuppl 3:S19.
en AM, Chen THening: what have793-806, v. ell J, Nordenskjo
mmography screeomised trials. La
ohen A, Tot T, mmographic Scres. Radiology. 201Souchon R, Meinarcinoma in situ o99-705. mation of mean soMarkov chain moddetectable phase
aisma G, de Bruijappropriate uppe
creening. Int J Ca
t 176
ma in t, and
ancer entive 7-60. g LH, r after m the tional
er of
. The e we
old B, ening: ancet.
et al. ening 1.
nhold-of the
ojourn del of . Stat
n AE, er age ancer.

KCE Report 176
18. Fett MJ
mammoscreeni
19. Shen estimatBiostat
20. Wu JCEstimatnon-raneffects on redTreatm
21. Olsen Overdiamammo2006;12
22. Frisell breast Breast
23. Paci Escreeniin the Journa
24. Boer RcarcinoCancer
25. Duffy Sof breathe Nat
26. Duffy Sin brea2005;92
27. Shen Ybreast
6
J. Computer modographic screenining interval. JournY, Zelen M. Rtion of sensitivity istics. 2005;6(4):6, Hakama M, Antttion of natural hisndomized organizof inter-screeninguction of advancent. 2010;122(2):AH, Agbaje O
agnosis, sojourn ography scree2(4):338-42. J, Eklund G, Hecarcinomas in a Cancer Research
E, Duffy SW. Ming programmes: Florence Distric
l of EpidemiologyR, de Koning Homa screening intr. 1999;86(8):1506SW, Day NE, Tabast tumor progresstional Cancer Inst
SW, Gabe R. Whaast screening p2(3):597-600. Y, Zelen M. Screcancer early de
delling of the Swng and trade offs bnal of Medical ScreRobust modelingy and preclinical 604-14. tila A, Yen AM, Mtory parameters o
zed screening dag interval, sensiticed cancer. Bre553-66.
OF, Myles JP, time, and sensit
ening program
ellstrom L, Somerandomized scre
h & Treatment. 19Modelling the an
sensitivity, lead tct Programme (1. 1991;20(4):852-
HJ, van der Maaerval for women 6-10. ar L, Chen HH, Ssion: some age-stitute. Monographsat should the deterogrammes? Brit
eening sensitivityetection clinical tr
S
wedish two countybetween participaeening. 2001;8(1)
g in screening sojourn time dist
Malila N, Sarkeala of breast cancer bta: subsidiary anavity, and attendaast Cancer Rese
Lynge E, Duftivity in the Copem. Breast
ll A. Analysis of eening trial in Sto987;9(3):219-25. alysis of breast time and predictiv1975-1986). Inter8. as PJ. A longerage older than 65
Smith TC. Markovspecific results. Jos. 1997;22:93-7.ection rates of cantish Journal of
y and sojourn timrials: mammogra
Screening Breast C
y trial of ation and ):39-45. studies:
tribution.
T, et al. based on alysis of nce rate earch &
ffy SW. enhagen Journal.
interval ockholm.
cancer ve value rnational
r breast 5 years?
v models ournal of
ncers be Cancer.
me from ams and
2
2
3
3
3
3
3
3
3
3
Cancer
physical 2001;19(1
28. Spratt JS,duration odetection
29. Tabar L, Fal. Efficacthe Swedi
30. Weedon-FEstimatingquestionnaMedical S
31. Weedon-FEstimatingbreast caMedical S
32. Zappa M, women: eReviews in
33. Boer R, dsearch of J Cancer.
34. Mandelbladecisions among theClin Onco
35. Karnon J, et al. A designing 2007;11(5
36. Barratt A,outcomes informed c
37. Berry DA,Modeling
examinations. 5):3490-9. Greenberg RA, Hof cancer and caby screening. CanFagerberg G, Checy of breast cancesh Two-County T
Fekjaer H, Lindqvg mean sojourn aire data on timecreening. 2008;15
Fekjaer H, Vatteng mean sojourn ncer mammograpcreening. 2005;12Visioli CB, Ciatto
efficacy and cost-n Oncology Hemae Koning HJ, vanthe best upper ag1995;31A(12):20
att JS, Silliman about the benefitse oldest old withol. 2009;27(4):487-Goyder E, Tappereview and crit
screening pro52):iii-iv, ix-xi, 1-14 Howard K, Irwig
of screening mchoices. BMJ. 200, Inoue L, Shen Ythe impact of tre
Journal of
Heuser LS. Geomarcinoma in situ ncer Research. 19en HH, Duffy SWer screening by arial. Cancer. 1995
vist BH, Vatten Ltime and scree
e since previous 5(2):83-90. n LJ, Aalen OO, time and screen
phy screening: n2(4):172-8. o S. Mammograph-effectiveness. Reatology. 2003;46(3n Oortmarssen GJge limit for breast 40-3. R. Hanging in s and harms of br
out a safety net o-90. enden P, McPhie tique of modellinogrammes. Heal45. g L, Salkeld G, Hmammography: in05;330(7497):936Y, Venier J, Coheatment and scre
Clinical Onco
metry, growth ratesof the breast b
986;46(2):970-4. , Smart CR, Gad age. New results5;75(10):2507-17.J, Aalen OO, Tre
ening sensitivity screening. Journ
Lindqvist B, Trening test sensitivew results. Journ
hy screening in eeview 16 refs. C3):235-9. J, van der Maas Pcancer screening
the balance: mreast cancer scre
of scientific eviden
S, Towers I, Brazng in prioritisinglth Technol As
Houssami N. Modnformation to su6. en D, Bondy M, eening on U.S. b
63
ology.
s, and before
A, et from . etli S. using nal of
etli S. vity in nal of
elderly Critical
PJ. In g. Eur
aking ening
nce. J
zier J, and
ssess.
del of upport
et al. breast

64
cancer 2006;M
38. Carles Cost-ef(Spain)
39. Carter and en2005;27
40. Feuer Emammo2000: 2006;M
41. FrybacKuruchEpidem2006;M
42. Gyrd-Hin DenmHealth
43. Hanin RochesCancer
44. Lee S, breast 2006;M
45. Lee SJAnn On
46. Mahnkethe effeevaluatapproa
47. MandeSPECTtreatme
mortality: a BayeMonographs.(36):3
M, Vilaprinyo E, ffectiveness of ea). BMC Cancer. 20KJ, Castro F, Kend ages for ma7(1):40-7. EJ. Modeling the ography on U.S. introduction to th
Monographs.(36):2k DG, Stout Nittham V, Remin
miology SimulatioMonographs.(36):3Hansen D. Cost-bemark based on diCare. 2000;16(3)LG, Miller A, Zo
ster model of brer Inst Monogr. 200Zelen M. A stoch
cancer. JMonographs.(36):7J, Zelen M. Modencol. 2003;14(8):1en JD, Chan W, ects of lead-timeting screening mch. Stat Methods lblatt J, Schechte
TRUM populationent on U.S. bre
esian approach. J 30-6. Cots F, Gregori A
arly detection of b011;11.
essler E, Ericksonmmography scre
impact of adjuvabreast cancer mohe problem. J N2-6. NK, Rosenberg ngton PL. The Won Model. J Na37-47. enefit analysis of iscrete ranking da:811-21.
orin AV, Yakovleeast cancer detec06;Monographs.(3hastic model for pJ Natl Can79-86. elling the early de
199-202. Freeman DH, Jr
e bias, length biamammography: a
Med Res. 2008;1er CB, Lawrencen model of the ieast cancer trend
S
Natl Cancer Inst
A, Pla R, Roman breast cancer in C
n BA. Simulation eening. J Health
ant therapy and scortality between 1atl Cancer Inst
MA, Trentham-DWisconsin Breast atl Cancer Inst
mammography scata. Int J Technol
v AY. The Univection and surviva36):66-78. predicting the moncer Inst
etection of breast
., Freeman JL. Ras and over-detecensored bivaria7(6):643-63. W, Yi B, Cullenmpact of screends from 1975 to
Screening Breast C
Monogr.
R, et al. Catalonia
of begin hc Qual.
creening 975 and Monogr.
Dietz A, Cancer
Monogr.
creening l Assess
ersity of l. J Natl
ortality of Monogr.
cancer.
Reducing ection in ate data
n J. The ning and o 2000:
4
4
5
5
5
5
5
5
Cancer
principles Monogr. 2
48. MandelblaDraisma different benefits a19;152(2):
49. MandelblaJ, Extermolder womscreening 2005;20(6
50. Neeser K,effectivenescreening perspectiv(Structure
51. Plevritis Sstochasticfrom 192006;Mon
52. Rauner MDynamic Based IdOperation
53. RijnsburgeMiller AB,Breast Sc2004;110(
54. Rojnik KProbabilisscreening
55. Rue M, VMarcos-G
and practice of t2006;Monographsatt JS, Cronin KAG, et al. Effectscreening schednd harms.[Erratum:136]. Ann Intern att JS, Schechter
mann M, et al. Tomen: Costs, beby age, biology,
6):487-96. , Szucs T, Bulliardess analysis of
program fromve: quantitative asd abstract). 2007;
SK, Sigal BM, Sc simulation mode975 to 2000. ographs.(36):86-9
MS, Gutjahr WJ, Policy Modeling
dentification of Ps Research. 2010er AJ, van Oortm et al. Mammogrcreening Study-2(5):756-62. , Naversnik K, tic cost-effectivenpolicies in Sloven
Vilaprinyo E, Leeragera R, et al. Ef
the model method.(36):47-55.
A, Bailey S, Berrs of mammogradules: model esm appears in AnnMed. 2009;151(10CB, Yabroff KR,
oward optimal scnefits, and harmand health status
d JL, Bachmann f a quality-cont
m the Swiss ssessment of the ;10(1):42-53.
Salzman P, Roseel of U.S. breast c
J Natl Ca95. Heidenberger Kfor Chronic Dis
Pareto-Optimal S0;58(5):1269-86.
marssen GJ, Boerraphy benefit in t2: a model eval
Mateovic-Rojnikness modeling of nia. Value Health.e S, Martinez-Alffectiveness of ea
KCE Report
ds. J Natl Cance
ry DA, de Koningaphy screening ustimates of pot
n Intern Med. 20100):738-47. Lawrence W, Dig
creening strategiems of breast cas. J. Gen. Intern.
G, Schramm W. trolled mammogrstatutory healthmost influential fa
enberg J, Glynn cancer mortality trncer Inst Mo
, Wagner J, Passeases: MetaheuScreening Strate
r R, Draisma G, Tthe Canadian Nauation. Int J Ca
k T, Primiczakedifferent breast ca 2008;11(2):139-4lonso M, Carles
arly detection on b
t 176
er Inst
g HJ, under tential 0 Jan
gnam es for ancer Med.
Cost-raphy
h-care actors
P. A rends
onogr.
sia J. ristic-egies.
To T, tional
ancer.
lj M. ancer 48.
MD, breast

KCE Report 176
cancer 2009;9
56. Stout NSM, Frscreeni
57. Tan SYJD. Thecancer.
58. VilaprinEstimatsurvivaCancer
59. Wang screenicountiescreeni
60. Messecwithoutquiz 52
61. Wen YPcase o2005;24
62. Advisorcancer 61.
63. Anonymvolledig1997. LBorstka
64. Barratt K, et alBased
65. Barratt Benefit
6
mortality reduct(326).
NK, Rosenberg MAryback DG. Retring mammographY, van Oortmarsse MISCAN-Fadia . J Natl Cancer Innyo E, Rue M, tion of age- an
al functions usingr. 2009;9(98). H, Karesen R, ing in Norway: Re
es and cost-effing. Cancer Causcar DC. Mammogt cognitive impair2-3. P, Sheu ML. A coof breast cance4(6):519-28. ry Committee onin England: past
mous. Landelijk g ingevoerd; resLandelijk Evaluatanker. Ned TijdschA, Irwig L, Glaszi. Relative benefit Healthc. 2002;6(4AL, Les Irwig M
s, harms and cos
tion in Catalonia
A, Trentham-Dietrospective cost-ey. J Natl Cancer I
sen GJ, de Konincontinuous tumost Monogr. 2006;MMarcos-Gragera
nd stage-specific g US and Cata
Hervik A, Thoreesults from the firsfectiveness of es Control. 2001;
graphy screening frment. J Gerontol
ost-benefit analysr screening. Ta
n Breast Cancer and future. J Me
bevolkingsonderultaten van de tie Team voor behr Geneeskd. 200iou P, Salkeld G, of mammography
4):156-7. M, Glasziou PP, S
sts of screening m
S
a (Spain). BMC
tz A, Smith MA, Reffectiveness anaInst. 2006;98(11):ng HJ, Boer R, Hr growth model foMonographs.(36)
R, Martinez-AloCatalan breast
alan survival data
esen SA. Mammst screening rouna modeled na12(1):39-45. for older women wl Nurs. 2000;26(4
is of preventive caiwain J. Public
S. Screening foed Screen. 2006;1
rzoek naar borsimplementatiefaseevolkingsonderzo00;144(23):1124-9Houssami N, Kerly reduces with ag
Salkeld GP, Housmammography in
Screening Breast C
Cancer.
Robinson alysis of 774-82.
Habbema or breast :56-65. onso M.
cancer a. BMC
mography d in four tionwide
with and 4):14-24;
are: The Health.
or breast 13(2):59-
stkanker e 1990-
oek naar 9. likowske e. Evid.-
ssami N. n women
6
6
6
6
7
7
7
7
7
7
Cancer
70 years2002;176(
66. Bonneux voor evidGeneesku
67. Caplan LSscreening 40.
68. Carney PABuist DSMevents umammogr
69. De KoningEur J Rad
70. Feuer EJ, understanfrom mam2004;13(6
71. Grivegneecancer du
72. Habbema U.S. breasmeasures2006;Mon
73. Mandelblaal. The co65 years: Task Forc
74. Prevost Tgeneralizeof breast c
75. Rautenstrawaste of m
s and over: a(6):266-71. L. De voor- en n
dence-based infounde. 2009;153. S. To screen or n
in older women.
A, Abraham LA, M, et al. Factors aused to detecraphy. Am. J. Roeg HJ. Breast canciol. 2000;33(1):32Etzioni R, Cronind the impact of
mmography and 6):421-42. e AR, Autier P. A sein en BelgiqueJD, Tan SY, Cr
st cancer mortality informative? ographs.(36):105
att J, Saha S, Teuost-effectiveness o
a systematic rece. Ann Intern MedTC, Abrams KRed synthesis of evcancer screening.auch J. Is mam
money? MMW-Fo
systematic re
nadelen van borsormatie. Nederla
ot to screen: the . Public Health R
Miglioretti DL, Yaassociated with imct breast cancentgenol. 2007;18cer screening; cos2-7. n KA, Mariotto A. Tscreening on U.SPSA testing. Sta
Approche econome. Rev Med Brux. 2ronin KA. Impact y, 1975-2000: are
J Natl Can5-11. utsch S, Hoerger of screening mameview for the U.Sd. 2003;139(10):8
R, Jones DR. Hvidence: an exam Stat Med. 2000;1
mmography screertschr. Med. 2000
view. Med J
stkankerscreeningands Tijdschrift
issue of breast caRev. 2001;29(2-4)
abroff KR, Sicklesmaging and procecer after scre8(2):385-92.
st-effective in prac
The use of modelS. mortality: examat Methods Med
mique du depistag2001;22(4):A277-
of mammographe intermediate outncer Inst Mo
T, Siu AL, Atkins mography beyond
S. Preventive Ser835-42. ierarchical mode
mple based on st19(24):3359-76. ning only a poin
0;142(12):4-10.
65
Aust.
g: tijd voor
ancer ):231-
s EA, edural ening
ctice?
ing to mples
Res.
ge du -81. hy on come
onogr.
D, et d age rvices
els in tudies
ntless

66
76. Xu W,
women77. Berry D
et al. Ebreast c
78. Carter the stud
79. CleempRecomBelgiqufédéral 78B (D/
80. Lidgrenquality 2007;16
81. Freedmstates ocancer.
82. Burstroof life populat
83. Gerard attributespecific
84. Domeyrelated effects,Outcom
85. Borstkabevolki2010.
86. StordeuEyckenClinicalCentre
Vnenchak P, Sn aged 70 to 79 yeDA, Cronin KA, PleEffect of screenincancer. N Engl J KJ, Castro F, Kesdy of breast canceput I, Van Wilder mandations pour
ue. Health technod'expertise des s
/2008/10.273/24) n M, Wilking N, of life in differen6(6):1073-81.
man GM, Li T, Anof women after co. Breast Cancer R
om K, Johannessoby disease and
tion in Sweden. H K, Johnston K, e health classific health state descyer PJ, Sergentan
quality of life in v, long-term effect
mes. 2010;8(11):2anker LETvbngsonderzoek na
ur S, Vrijens F, n E. Quality indicl Practice (GCP).
(KCE); 2010.
Smucny J. Screears. J. 2000;49(3evritis SK, Frybac
ng and adjuvant tMed. 2005;353(17ssler E, Erickson er. Comput Biol MP, Vrijens F, Huybles évaluations plogy Assessment soins de santé (K Jonsson B, Reh
nt states of breas
nderson PR, Nicoonservative surgerRes Treat. 2010;12on M, Diderichsend socio-economic
Health Policy. 2001Brown J. The roication measure criptions. Health Enis TN, Zagouri vacuum-assisted ts and predictors.2010. bn. Landelijkeaar borstkanker i
Beirens K, Vlaycators in oncologBrussels: BelgianKCE reports 15
S
eening mammogr3):266-7. ck DG, Clarke L, Ztherapy on morta7):1784-92. B. A computer m
Med. 2003;33(4):3brechts M, Ramae
pharmacoéconomi(HTA). Bruxelles
KCE); 2008. KCE
hnberg C. Healthst cancer. Qual L
laou N, Konski Ary and radiation fo21(2):519-26. n F. Health-relatedc group in the 1;55(1):51-69.
ole of a pre-scorein validating co
Econ. 1999;8(8):6F, Zografos GC. breast biopsy: sh Health & Quality
e evaluatie n Nederland 199
yen J, Devriese gy: breast bancen Health Care Kn50C (D/2010/10.2
Screening Breast C
raphy in
Zelen M, lity from
model for 45-60. ekers D. iques en
s: Centre Reports
h related Life Res.
A. Health or breast
d quality general
ed multi-ondition-
685-99. Health-
hort-term y of Life
van 90-2007.
S, Van er. Good owledge 273/101)
8
8
8
9
9
9
9
9
9
Cancer
Available http://kce.f
87. INC. Survétat des lie
88. Mook S, Vvan Leeuwdetection 2011;103(
89. Cortesi L, Prognosispopulation
90. Joensuu HT, Kataja detected 2004;292(
91. Olsson A,J. Tumourby screen
92. PhysiciansPreventive
93. Woloshin mammogr2010;303(
94. Jorgensenfunded sc
95. Perry N, BL. Europescreening Oncol. 200
fgov.be/index_envie attendue des peux. 2010.
Van 't Veer LJ, Ruwen FE, et al. In
in invasive br(7):585-97. Chiuri VE, Rusce
s of screen-deten based study. BMH, Lehtimaki T, Ho
V, et al. Risk foby mammograph(9):1064-73. Borgquist S, Butr-related factors aing. Br J Surg. 20s AAoF. Summae Services. In: AA
S, Schwartz raphy screening: (2):164-5. n KJ, Gotzsche reening mammog
Broeders M, de Wean guidelines fo
and diagnosis. F08;19(4):614-22.
.aspx?SGREF=52patients atteints d
utgers EJ, Ravdin ndependent prognreast cancer. J
elli S, Bellelli V, Nected breast ca
MC Cancer. 2006;olli K, Elomaa L, Tor distant recurre
hy screening or o
tt S, Zackrisson Sand prognosis in b012;99(1):78-87. ary of Recomme
AFP Policy Action LM. The beneunderstanding t
PC. Content of graphy. BMJ. 2006
Wolf C, Tornberg Sor quality assuraFourth edition--sum
KCE Report
211&CREF=1884de cancers en Fra
PM, van de Veldenostic value of scJ Natl Cancer
Negri R, Rashid I, ancers: results 6:17. Turpeenniemi-Hujence of breast caother methods. J
S, Landberg G, Mbreast cancer det
endations for ClAAFP; 2010. efits and harmthe trade-offs. JA
invitations for pu6;332(7540):538-4, Holland R, von K
ance in breast cammary document
t 176
from: 47 ance :
e AO, creen
Inst.
et al. of a
janen ancer Jama.
Manjer ected
linical
ms of AMA.
ublicly 41. Karsa ancer t. Ann

KCE Report 176
cancer 2009;9
56. Stout NSM, Frscreeni
57. Tan SYJD. Thecancer.
58. VilaprinEstimatsurvivaCancer
59. Wang screenicountiescreeni
60. Messecwithoutquiz 52
61. Wen YPcase o2005;24
62. Advisorcancer 61.
63. Anonymvolledig1997. LBorstka
64. Barratt K, et alBased
65. Barratt Benefit
6
mortality reduct(326).
NK, Rosenberg MAryback DG. Retring mammographY, van Oortmarsse MISCAN-Fadia . J Natl Cancer Innyo E, Rue M, tion of age- an
al functions usingr. 2009;9(98). H, Karesen R, ing in Norway: Re
es and cost-effing. Cancer Causcar DC. Mammogt cognitive impair2-3. P, Sheu ML. A coof breast cance4(6):519-28. ry Committee onin England: past
mous. Landelijk g ingevoerd; resLandelijk Evaluatanker. Ned TijdschA, Irwig L, Glaszi. Relative benefit Healthc. 2002;6(4AL, Les Irwig M
s, harms and cos
tion in Catalonia
A, Trentham-Dietrospective cost-ey. J Natl Cancer I
sen GJ, de Konincontinuous tumost Monogr. 2006;MMarcos-Gragera
nd stage-specific g US and Cata
Hervik A, Thoreesults from the firsfectiveness of es Control. 2001;
graphy screening frment. J Gerontol
ost-benefit analysr screening. Ta
n Breast Cancer and future. J Me
bevolkingsonderultaten van de tie Team voor behr Geneeskd. 200iou P, Salkeld G, of mammography
4):156-7. M, Glasziou PP, S
sts of screening m
S
a (Spain). BMC
tz A, Smith MA, Reffectiveness anaInst. 2006;98(11):ng HJ, Boer R, Hr growth model foMonographs.(36)
R, Martinez-AloCatalan breast
alan survival data
esen SA. Mammst screening rouna modeled na12(1):39-45. for older women wl Nurs. 2000;26(4
is of preventive caiwain J. Public
S. Screening foed Screen. 2006;1
rzoek naar borsimplementatiefaseevolkingsonderzo00;144(23):1124-9Houssami N, Kerly reduces with ag
Salkeld GP, Housmammography in
Screening Breast C
Cancer.
Robinson alysis of 774-82.
Habbema or breast :56-65. onso M.
cancer a. BMC
mography d in four tionwide
with and 4):14-24;
are: The Health.
or breast 13(2):59-
stkanker e 1990-
oek naar 9. likowske e. Evid.-
ssami N. n women
6
6
6
6
7
7
7
7
7
7
Cancer
70 years2002;176(
66. Bonneux voor evidGeneesku
67. Caplan LSscreening 40.
68. Carney PABuist DSMevents umammogr
69. De KoningEur J Rad
70. Feuer EJ, understanfrom mam2004;13(6
71. Grivegneecancer du
72. Habbema U.S. breasmeasures2006;Mon
73. Mandelblaal. The co65 years: Task Forc
74. Prevost Tgeneralizeof breast c
75. Rautenstrawaste of m
s and over: a(6):266-71. L. De voor- en n
dence-based infounde. 2009;153. S. To screen or n
in older women.
A, Abraham LA, M, et al. Factors aused to detecraphy. Am. J. Roeg HJ. Breast canciol. 2000;33(1):32Etzioni R, Cronind the impact of
mmography and 6):421-42. e AR, Autier P. A sein en BelgiqueJD, Tan SY, Cr
st cancer mortality informative? ographs.(36):105
att J, Saha S, Teuost-effectiveness o
a systematic rece. Ann Intern MedTC, Abrams KRed synthesis of evcancer screening.auch J. Is mam
money? MMW-Fo
systematic re
nadelen van borsormatie. Nederla
ot to screen: the . Public Health R
Miglioretti DL, Yaassociated with imct breast cancentgenol. 2007;18cer screening; cos2-7. n KA, Mariotto A. Tscreening on U.SPSA testing. Sta
Approche econome. Rev Med Brux. 2ronin KA. Impact y, 1975-2000: are
J Natl Can5-11. utsch S, Hoerger of screening mameview for the U.Sd. 2003;139(10):8
R, Jones DR. Hvidence: an exam Stat Med. 2000;1
mmography screertschr. Med. 2000
view. Med J
stkankerscreeningands Tijdschrift
issue of breast caRev. 2001;29(2-4)
abroff KR, Sicklesmaging and procecer after scre8(2):385-92.
st-effective in prac
The use of modelS. mortality: examat Methods Med
mique du depistag2001;22(4):A277-
of mammographe intermediate outncer Inst Mo
T, Siu AL, Atkins mography beyond
S. Preventive Ser835-42. ierarchical mode
mple based on st19(24):3359-76. ning only a poin
0;142(12):4-10.
67
Aust.
g: tijd voor
ancer ):231-
s EA, edural ening
ctice?
ing to mples
Res.
ge du -81. hy on come
onogr.
D, et d age rvices
els in tudies
ntless

68
76. Xu W,
women77. Berry D
et al. Ebreast c
78. Carter the stud
79. CleempRecomBelgiqufédéral 78B (D/
80. Lidgrenquality 2007;16
81. Freedmstates ocancer.
82. Burstroof life populat
83. Gerard attributespecific
84. Domeyrelated effects,Outcom
85. Borstkabevolki2010.
86. StordeuEyckenClinicalCentre
Vnenchak P, Sn aged 70 to 79 yeDA, Cronin KA, PleEffect of screenincancer. N Engl J KJ, Castro F, Kesdy of breast canceput I, Van Wilder mandations pour
ue. Health technod'expertise des s
/2008/10.273/24) n M, Wilking N, of life in differen6(6):1073-81.
man GM, Li T, Anof women after co. Breast Cancer R
om K, Johannessoby disease and
tion in Sweden. H K, Johnston K, e health classific health state descyer PJ, Sergentan
quality of life in v, long-term effect
mes. 2010;8(11):2anker LETvbngsonderzoek na
ur S, Vrijens F, n E. Quality indicl Practice (GCP).
(KCE); 2010.
Smucny J. Screears. J. 2000;49(3evritis SK, Frybac
ng and adjuvant tMed. 2005;353(17ssler E, Erickson er. Comput Biol MP, Vrijens F, Huybles évaluations plogy Assessment soins de santé (K Jonsson B, Reh
nt states of breas
nderson PR, Nicoonservative surgerRes Treat. 2010;12on M, Diderichsend socio-economic
Health Policy. 2001Brown J. The roication measure criptions. Health Enis TN, Zagouri vacuum-assisted ts and predictors.2010. bn. Landelijkeaar borstkanker i
Beirens K, Vlaycators in oncologBrussels: BelgianKCE reports 15
S
eening mammogr3):266-7. ck DG, Clarke L, Ztherapy on morta7):1784-92. B. A computer m
Med. 2003;33(4):3brechts M, Ramae
pharmacoéconomi(HTA). Bruxelles
KCE); 2008. KCE
hnberg C. Healthst cancer. Qual L
laou N, Konski Ary and radiation fo21(2):519-26. n F. Health-relatedc group in the 1;55(1):51-69.
ole of a pre-scorein validating co
Econ. 1999;8(8):6F, Zografos GC. breast biopsy: sh Health & Quality
e evaluatie n Nederland 199
yen J, Devriese gy: breast bancen Health Care Kn50C (D/2010/10.2
Screening Breast C
raphy in
Zelen M, lity from
model for 45-60. ekers D. iques en
s: Centre Reports
h related Life Res.
A. Health or breast
d quality general
ed multi-ondition-
685-99. Health-
hort-term y of Life
van 90-2007.
S, Van er. Good owledge 273/101)
8
8
8
9
9
9
9
9
9
Cancer
Available http://kce.f
87. INC. Survétat des lie
88. Mook S, Vvan Leeuwdetection 2011;103(
89. Cortesi L, Prognosispopulation
90. Joensuu HT, Kataja detected 2004;292(
91. Olsson A,J. Tumourby screen
92. PhysiciansPreventive
93. Woloshin mammogr2010;303(
94. Jorgensenfunded sc
95. Perry N, BL. Europescreening Oncol. 200
fgov.be/index_envie attendue des peux. 2010.
Van 't Veer LJ, Ruwen FE, et al. In
in invasive br(7):585-97. Chiuri VE, Rusce
s of screen-deten based study. BMH, Lehtimaki T, Ho
V, et al. Risk foby mammograph(9):1064-73. Borgquist S, Butr-related factors aing. Br J Surg. 20s AAoF. Summae Services. In: AA
S, Schwartz raphy screening: (2):164-5. n KJ, Gotzsche reening mammog
Broeders M, de Wean guidelines fo
and diagnosis. F08;19(4):614-22.
.aspx?SGREF=52patients atteints d
utgers EJ, Ravdin ndependent prognreast cancer. J
elli S, Bellelli V, Nected breast ca
MC Cancer. 2006;olli K, Elomaa L, Tor distant recurre
hy screening or o
tt S, Zackrisson Sand prognosis in b012;99(1):78-87. ary of Recomme
AFP Policy Action LM. The beneunderstanding t
PC. Content of graphy. BMJ. 2006
Wolf C, Tornberg Sor quality assuraFourth edition--sum
KCE Report
211&CREF=1884de cancers en Fra
PM, van de Veldenostic value of scJ Natl Cancer
Negri R, Rashid I, ancers: results 6:17. Turpeenniemi-Hujence of breast caother methods. J
S, Landberg G, Mbreast cancer det
endations for ClAAFP; 2010. efits and harmthe trade-offs. JA
invitations for pu6;332(7540):538-4, Holland R, von K
ance in breast cammary document
t 176
from: 47 ance :
e AO, creen
Inst.
et al. of a
janen ancer Jama.
Manjer ected
linical
ms of AMA.
ublicly 41. Karsa ancer t. Ann