Embed Size (px)
Citation preview
Dr Brice Malgras, Dr Clarisse Eveno
Chirurgie Diges+ve et Carcinologique Hôpital Lariboisière, Paris
Alger, 2016
• La chirurgie est le seul traitement cura+f du cancer de l’estomac
• L’étendue de la gastrectomie est bien codifiée
• L’étendue du curage controversée (?)
• Gastrectomie totale: indica+ons • Curage D2: indica+ons • Curage D2: techniques
• (Avant tout) 1) Au siège de la tumeur
• Mais aussi 2) Au type histologique (ADCI)
• Adénocarcinome gastrique à cellules indépendantes (ADCI) • Gastrectomie totale, quelque soit le siège
-‐ Forme diffuse (classifica+on de Lauren)
-‐ Moins différenciée, mal limitée
-‐ Sujets plus jeunes
-‐ Stades plus avancés (N%, carcinose péritonéale)
-‐ Taux de résec+ons R0 plus faible, lymphophilie (Ra+o N+)
-‐ Pronos+c plus sombre, récidive plus fréquente (CP)
Gastrectomie totale
-‐ ADCI
-‐ Cancers proximaux, corps gastrique Buhl Eur J Surg Oncol 1990:404–409 -‐ Pas de gastrectomie proximale (pbs fonc+onnels)
Gastrectomie totale
-‐ ADCI
-‐ Cancers proximaux, corps gastrique Buhl Eur J Surg Oncol 1990:404–409 -‐ Pas de gastrectomie proximale (pbs fonc+onnels)
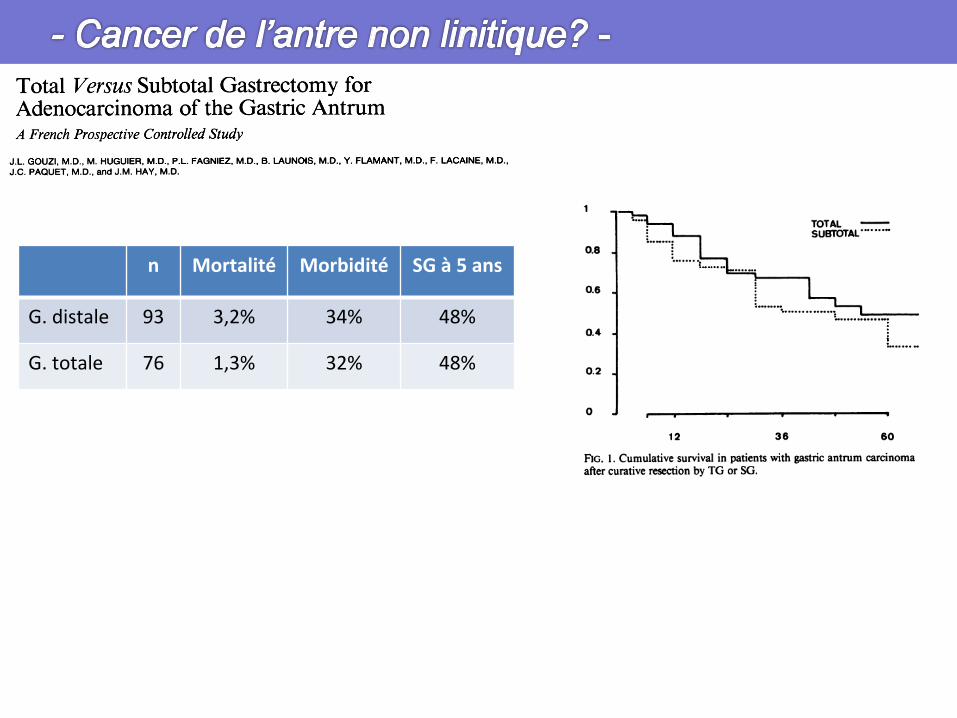
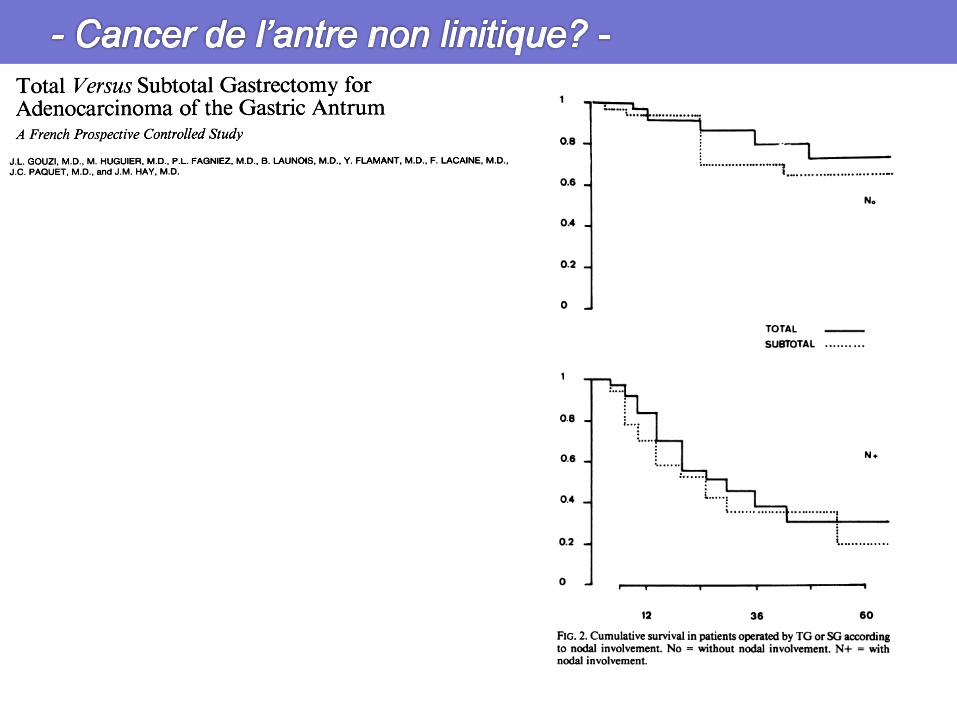
n Mortalité Morbidité SG à 5 ans
G. distale 93 3,2% 34% 48%
G. totale 76 1,3% 32% 48%
n Mortalité Morbidité SG à 5 ans
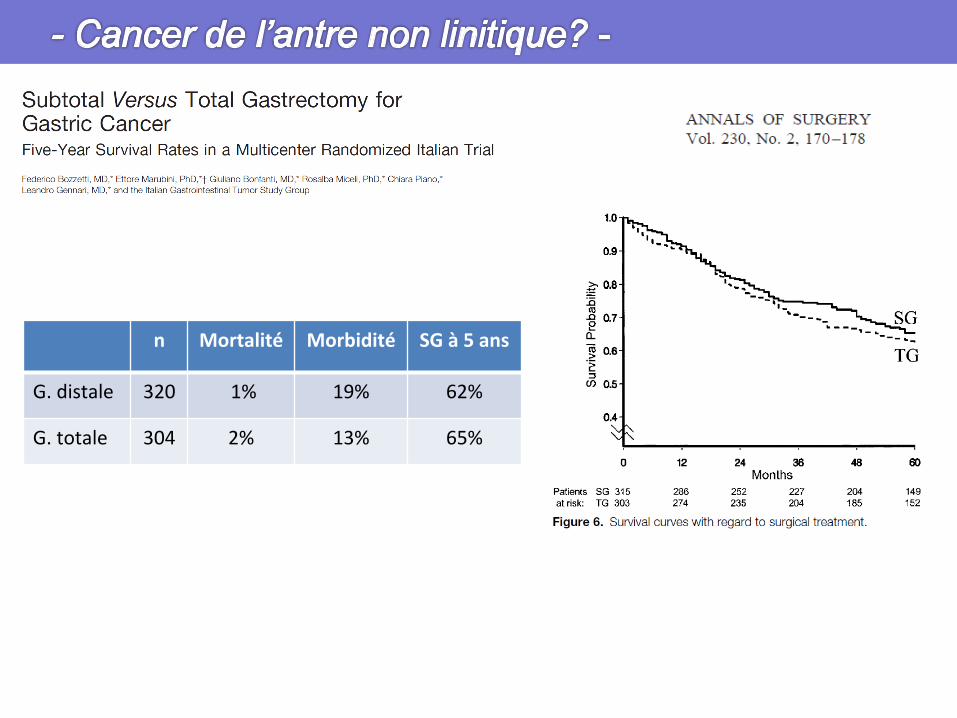
G. distale 320 1% 19% 62%
G. totale 304 2% 13% 65%
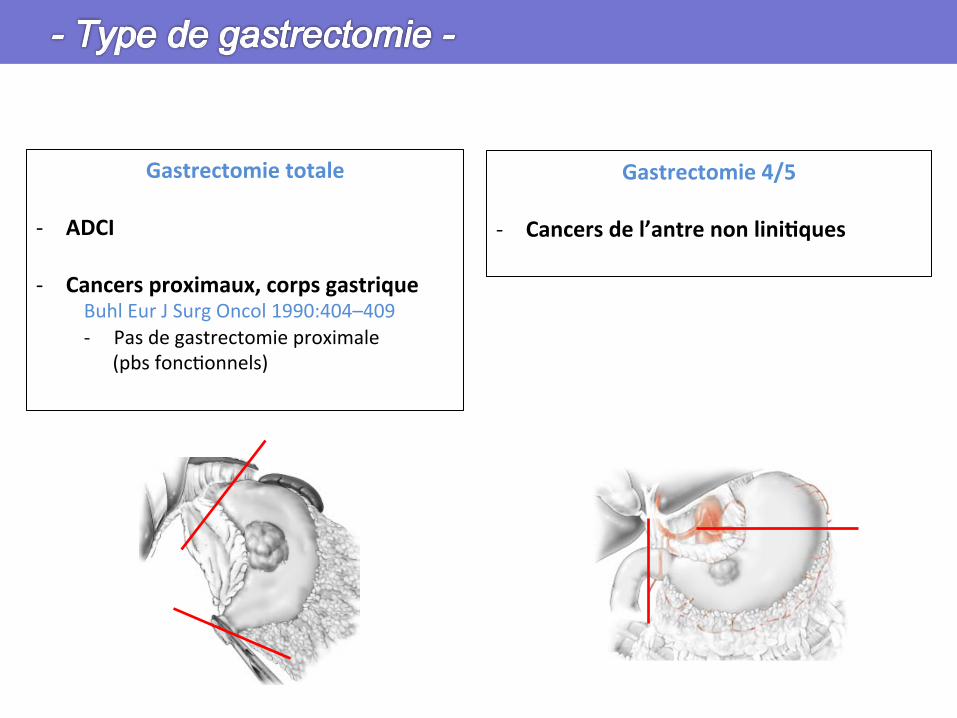
Gastrectomie 4/5
-‐ Cancers de l’antre non liniHques
Gastrectomie totale
-‐ ADCI
-‐ Cancers proximaux, corps gastrique Buhl Eur J Surg Oncol 1990:404–409 -‐ Pas de gastrectomie proximale (pbs fonc+onnels)
• Marge pariétale minimale de sécurité – Type intes+nal: 5 cm – Type diffus: 10 cm (extension sous muqueuse ++) – Résec+on en bloc des organes voisins envahis
(pancréas, rate, lobe gauche, colon…)
• Marge R1
-‐ La re-‐résec+on d’une marge microscopiquement envahie à l’extemporané améliore la survie chez les seuls pa+ents avec 5 ou moins gg envahis
Kim SH J Gastrointest Surg 1999: 24–33
• Il faut faire une gastrectomie TOTALE
1. 1/3 moyen & 1/3 supérieur
2. Linites et formes diffuses
3. Prophylac+que (muta+on Cdh1)
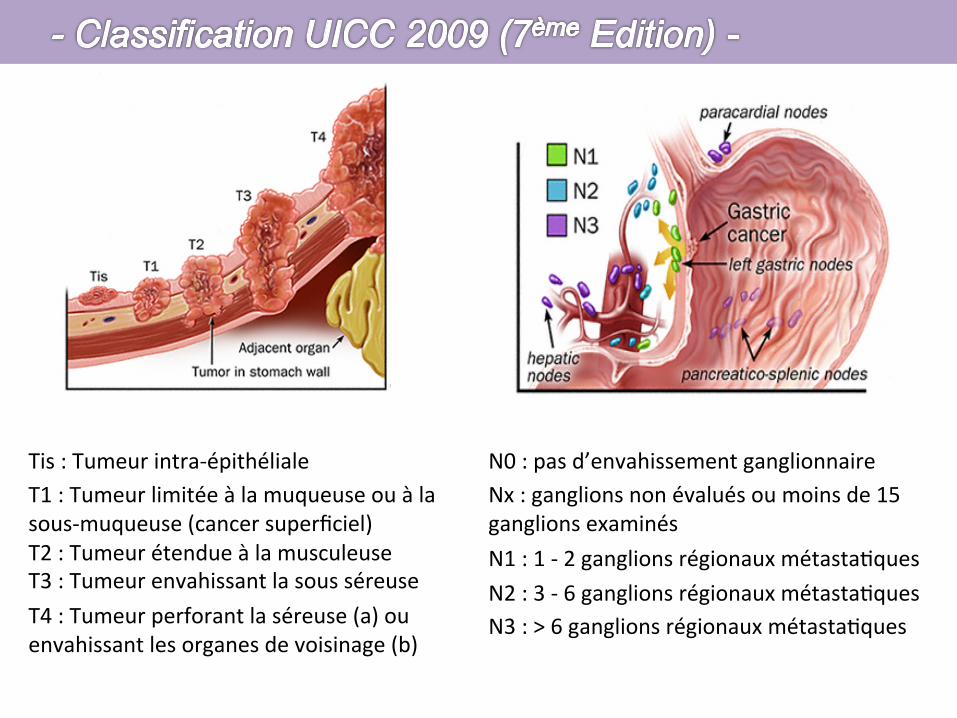
Tis : Tumeur intra-‐épithéliale T1 : Tumeur limitée à la muqueuse ou à la sous-‐muqueuse (cancer superficiel) T2 : Tumeur étendue à la musculeuse T3 : Tumeur envahissant la sous séreuse T4 : Tumeur perforant la séreuse (a) ou envahissant les organes de voisinage (b)
N0 : pas d’envahissement ganglionnaire Nx : ganglions non évalués ou moins de 15 ganglions examinés N1 : 1 -‐ 2 ganglions régionaux métasta+ques N2 : 3 -‐ 6 ganglions régionaux métasta+ques N3 : > 6 ganglions régionaux métasta+ques
• Nomenclature en N • Système standardisé Japanese Research Society for Gastric Cancer (JRSGC 1962) • Relais locorégionaux
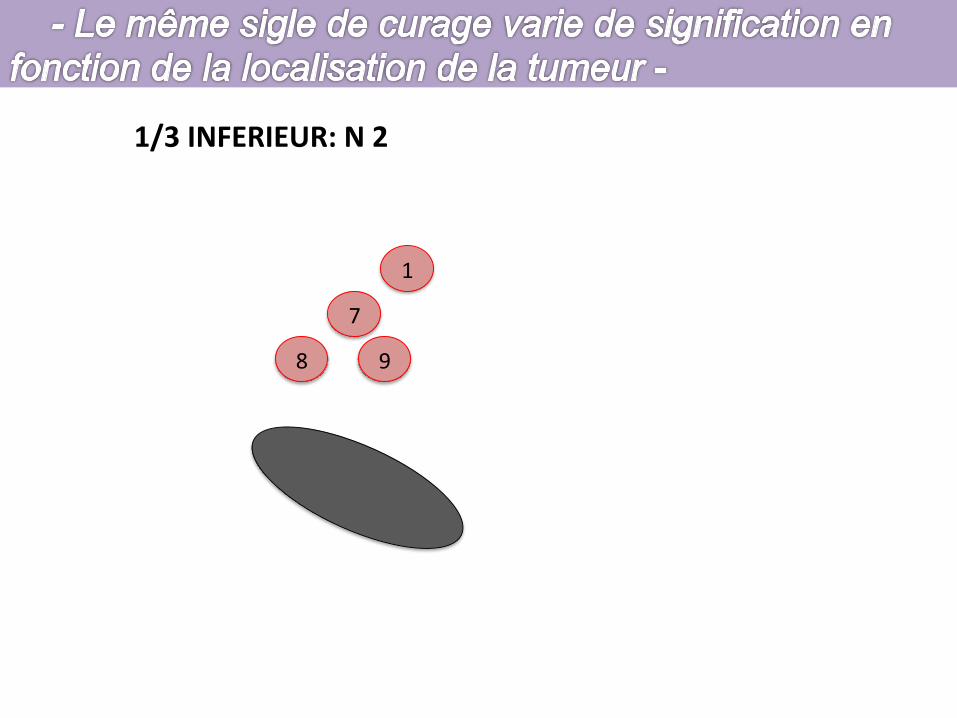
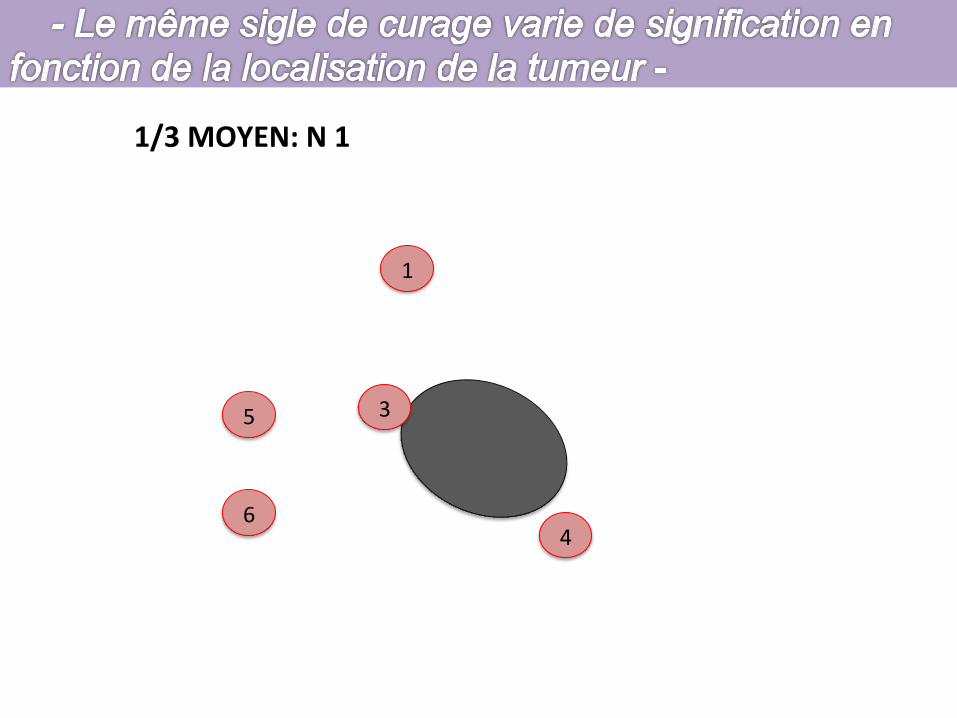
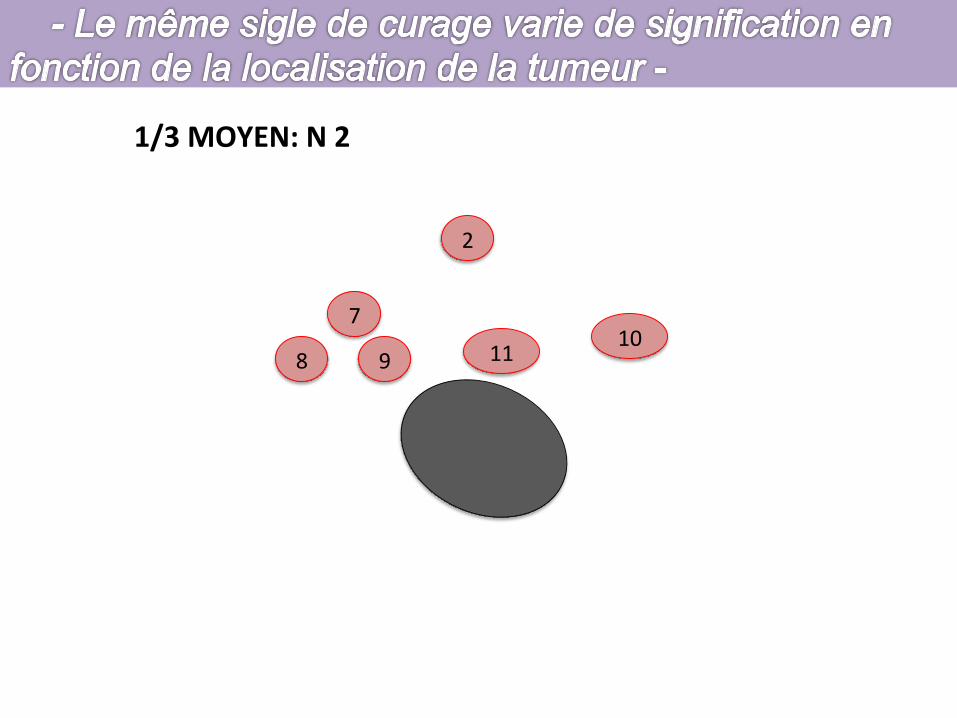
– Groupes ganglionnaires proches = N1 (péri gastriques à de 1 à 6) – Groupes pédiculaires = N2 (branches du tronc cœliaque à de 7 à 11)
• Relais métasta+ques – Groupes distaux = N3, N4 (gros vaisseaux à de 12 à 16)

¶ Vaisseaux courtsLes vaisseaux courts sont constitués de branches terminales del’artère splénique. Ils peuvent se détacher du tronc de l’artèresplénique ou de ses branches terminales. Au nombre de deux à six,ils cheminent du hile splénique à l’estomac par l’épiploongastrosplénique. L’un d’eux, plus volumineux, rejoint la facepostérieure de l’estomac et se ramifie de la grosse tubérosité aucardia : il s’agit de l’artère gastrique postérieure ou artèrecardiotubérositaire postérieure.Entre le dernier vaisseau court et l’origine de l’artèregastroépiploïque gauche existe une fenêtre avasculaire constituéeuniquement de deux feuillets péritonéaux. Leur effondrementpermet d’entrer dans l’arrière-cavité des épiploons en regard del’artère splénique (fig 4).
VASCULARISATION VEINEUSELe système veineux est satellite du réseau artériel, avec une veinepour une artère. Le réseau veineux gastrique droit rejointdirectement la veine porte. Le réseau veineux gastroépiploïque droitrejoint la veine colique supérieure droite pour former le troncveineux gastrocolique (ou tronc de Henle) et se jeter dans la veinemésentérique supérieure avant son abouchement dans la veineporte. Le réseau veineux gastrique gauche rejoint la veine spléniqueaprès son passage dans le ligament gastrosplénique où il est satellitedu réseau artériel.
Anatomie lymphatiqueLa connaissance du système lymphatique remonte à plusieurssiècles. Sa description détaillée est réalisée par Rouvière dès 1932.Les ganglions sont satellites des artères et un même organe peut sedrainer dans plusieurs chaînes ganglionnaires à la fois. Lesganglions sont désignés sous le nom de l’organe auquel ils sontannexés, ou bien sous le nom de l’artère à laquelle ils sont accolés. Ilest ainsi possible d’en effectuer une description topographique [9].Toutefois, la description actuelle du drainage lymphatique gastriquea une orientation chirurgicale et suit les recommandations de laJapanese Research Society for Gastric Cancer (JRSGC) éditée en 1962.Elle représente une description systématique du drainagelymphatique de l’estomac, définissant des groupes d’envahissementganglionnaire de gravité croissante en fonction de la localisation dela tumeur primitive de l’estomac. Nous décrivons dans ce chapitreles 16 sites de drainage ganglionnaire gastrique tels qu’ils sontdéfinis par la classification de la JRSGC. Elle est adoptée aujourd’huipar la majorité des équipes chirurgicales (fig 5) [5]. Nous présentonsles principes chirurgicaux des curages et nous précisons à quelsstades de l’intervention pour gastrectomie ces groupesganglionnaires sont réséqués. Les indications des curages et laconduite à tenir en fonction des tumeurs rencontrées sont traitéesdans l’article Gastrectomies pour cancer, fascicule 40-330-B2 del’Encyclopédie Médico-Chirurgicale.
CLASSIFICATION DES RELAIS GANGLIONNAIRESGASTRIQUES
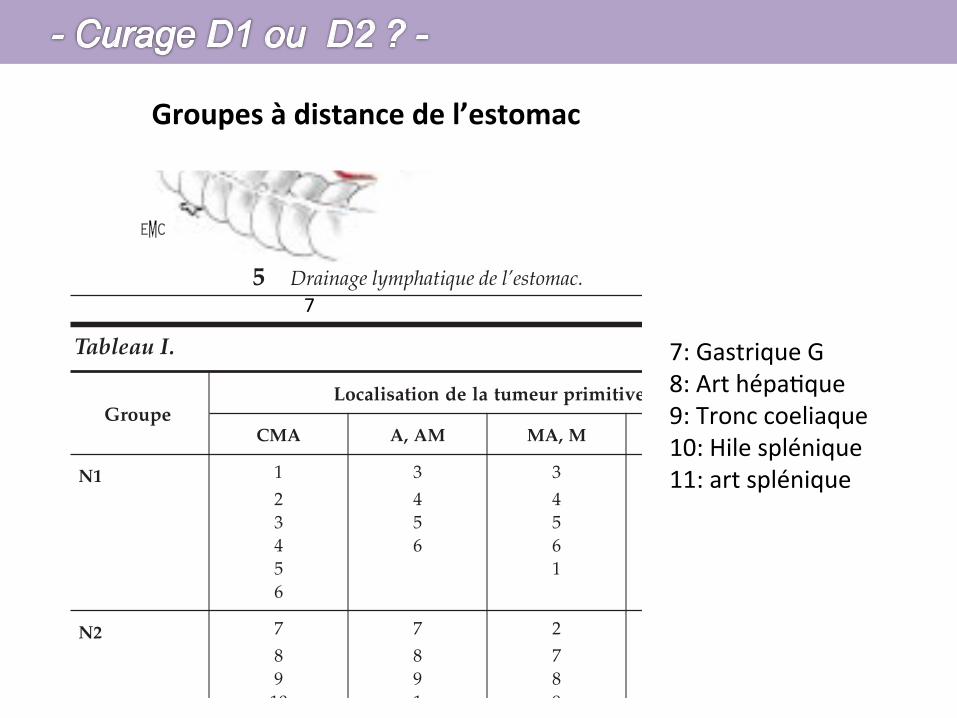
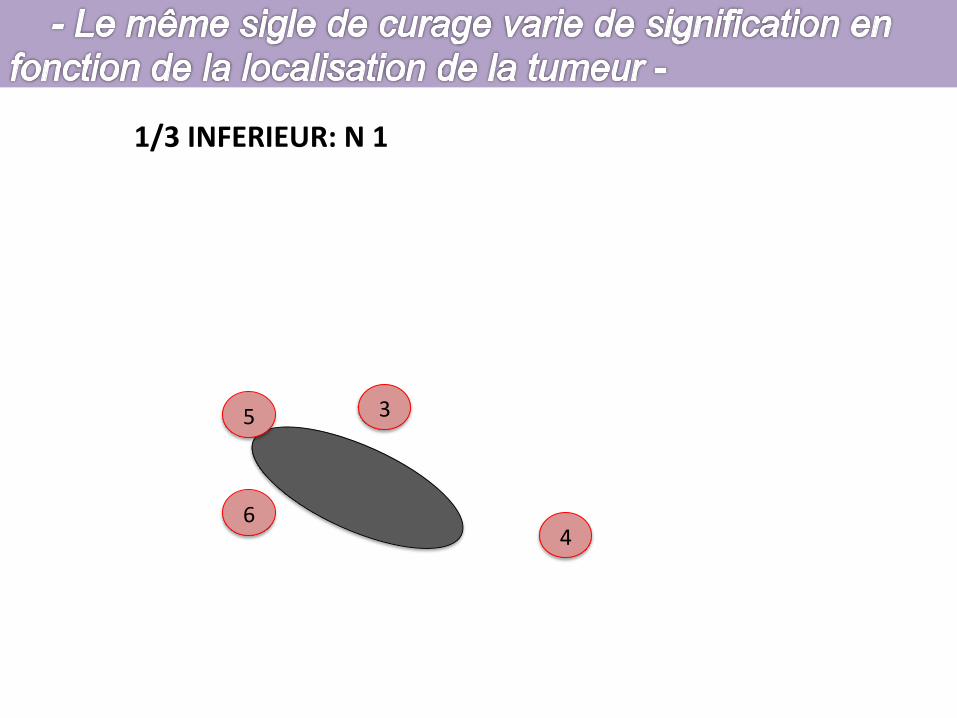
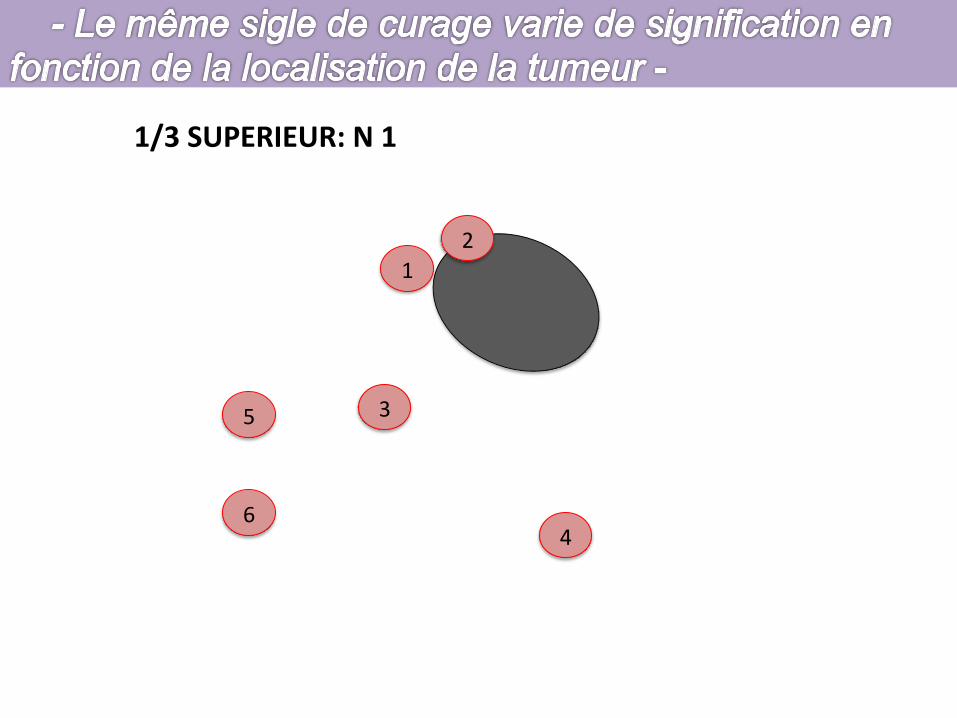
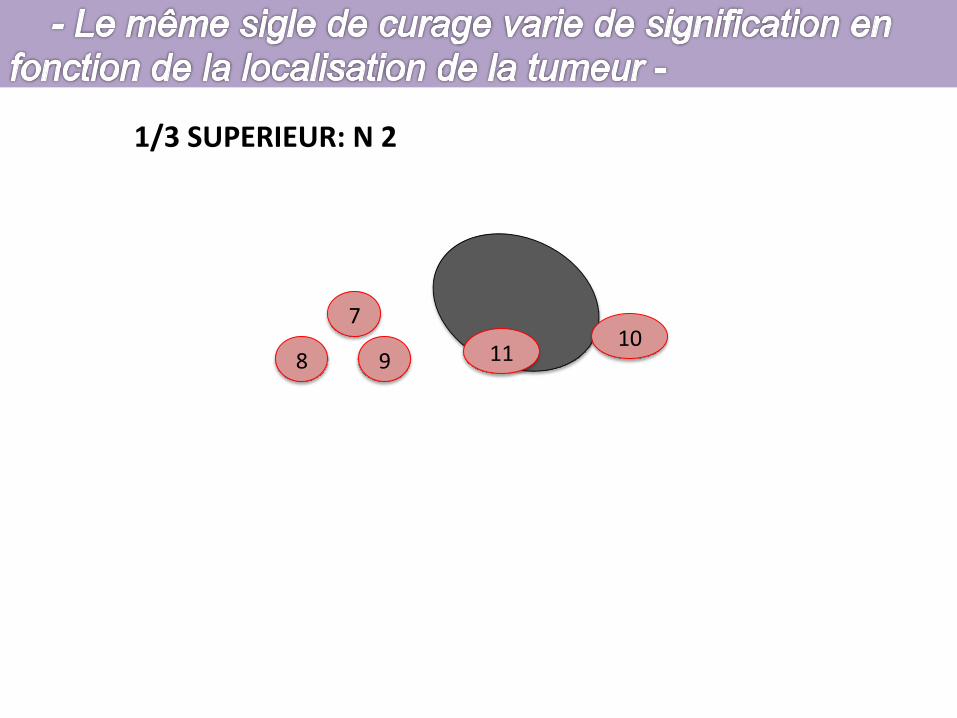
La classification des relais ganglionnaires gastriques (tableau I)permet de distinguer les relais locorégionaux (N1 et N2) et les relaisconsidérés en cas de tumeur comme métastatiques (N3 et N4). Parmiles relais « régionaux », il est possible de distinguer les relaisganglionnaires « de proximité : N1 », qui sont toujours réséqués lorsde la réalisation d’une gastrectomie pour cancer, des relais « distaux :N2 ». Ainsi, les groupes 1, 2, 3 et 4 sont considérés de proximité(N1) pour les cancers du cardia et du corps de l’estomac, et distaux(N2) pour les cancers de l’antre. De la même façon, les groupes 3, 4,5 et 6 sont de proximité (N1) pour les tumeurs antrales et distaux(N2) pour les tumeurs du cardia. Les autres groupes ganglionnairesdistaux sont les groupes 7, 8, 9, 10 (N2). Enfin, les ganglions àdistance situés au-delà de ces limites définissent des atteintesmétastatiques lorsqu’ils sont envahis : ce sont les groupes 12-13 (N3)et 15-16 (N4) (tableau I) [7].
4d
6
83
71
2
9
12a
12b
12p
5
4sb
4sa
4a
11 10
98
12
1614
13
15
5 Drainage lymphatique de l’estomac.
Tableau I.
GroupeLocalisation de la tumeur primitive
CMA A, AM MA, M C, CM, MC
N1 1 3 3 12 4 4 23 5 5 34 6 6 45 16
N2 7 7 2 58 8 7 69 9 8 7
10 1 9 811 10 9
11 1011
N3 12 2 12 1213 10 13 1314 11 14 14
121314
N4 15 15 15 1516 16 16 16
C : tumeur du tiers supérieur ; M : tumeur du tiers moyen ; A : tumeur du tiers inférieur ; groupes N1 et N2 :ganglions régionaux ; groupes N3 et N4 : métastases.
Techniques chirurgicalesGastrectomies pour cancer :
principes généraux, anatomie vasculaire, anatomie lymphatique, curages 40-330-A
3
1: Para-‐cardial Dt 2: Para-‐cardial G 3: Pe+te Courbure 4: Grande Courbure 5: Sus pylorique 6: Sous pylorique
Groupes Péri gastriques
¶ Vaisseaux courtsLes vaisseaux courts sont constitués de branches terminales del’artère splénique. Ils peuvent se détacher du tronc de l’artèresplénique ou de ses branches terminales. Au nombre de deux à six,ils cheminent du hile splénique à l’estomac par l’épiploongastrosplénique. L’un d’eux, plus volumineux, rejoint la facepostérieure de l’estomac et se ramifie de la grosse tubérosité aucardia : il s’agit de l’artère gastrique postérieure ou artèrecardiotubérositaire postérieure.Entre le dernier vaisseau court et l’origine de l’artèregastroépiploïque gauche existe une fenêtre avasculaire constituéeuniquement de deux feuillets péritonéaux. Leur effondrementpermet d’entrer dans l’arrière-cavité des épiploons en regard del’artère splénique (fig 4).
VASCULARISATION VEINEUSELe système veineux est satellite du réseau artériel, avec une veinepour une artère. Le réseau veineux gastrique droit rejointdirectement la veine porte. Le réseau veineux gastroépiploïque droitrejoint la veine colique supérieure droite pour former le troncveineux gastrocolique (ou tronc de Henle) et se jeter dans la veinemésentérique supérieure avant son abouchement dans la veineporte. Le réseau veineux gastrique gauche rejoint la veine spléniqueaprès son passage dans le ligament gastrosplénique où il est satellitedu réseau artériel.
Anatomie lymphatiqueLa connaissance du système lymphatique remonte à plusieurssiècles. Sa description détaillée est réalisée par Rouvière dès 1932.Les ganglions sont satellites des artères et un même organe peut sedrainer dans plusieurs chaînes ganglionnaires à la fois. Lesganglions sont désignés sous le nom de l’organe auquel ils sontannexés, ou bien sous le nom de l’artère à laquelle ils sont accolés. Ilest ainsi possible d’en effectuer une description topographique [9].Toutefois, la description actuelle du drainage lymphatique gastriquea une orientation chirurgicale et suit les recommandations de laJapanese Research Society for Gastric Cancer (JRSGC) éditée en 1962.Elle représente une description systématique du drainagelymphatique de l’estomac, définissant des groupes d’envahissementganglionnaire de gravité croissante en fonction de la localisation dela tumeur primitive de l’estomac. Nous décrivons dans ce chapitreles 16 sites de drainage ganglionnaire gastrique tels qu’ils sontdéfinis par la classification de la JRSGC. Elle est adoptée aujourd’huipar la majorité des équipes chirurgicales (fig 5) [5]. Nous présentonsles principes chirurgicaux des curages et nous précisons à quelsstades de l’intervention pour gastrectomie ces groupesganglionnaires sont réséqués. Les indications des curages et laconduite à tenir en fonction des tumeurs rencontrées sont traitéesdans l’article Gastrectomies pour cancer, fascicule 40-330-B2 del’Encyclopédie Médico-Chirurgicale.
CLASSIFICATION DES RELAIS GANGLIONNAIRESGASTRIQUES
La classification des relais ganglionnaires gastriques (tableau I)permet de distinguer les relais locorégionaux (N1 et N2) et les relaisconsidérés en cas de tumeur comme métastatiques (N3 et N4). Parmiles relais « régionaux », il est possible de distinguer les relaisganglionnaires « de proximité : N1 », qui sont toujours réséqués lorsde la réalisation d’une gastrectomie pour cancer, des relais « distaux :N2 ». Ainsi, les groupes 1, 2, 3 et 4 sont considérés de proximité(N1) pour les cancers du cardia et du corps de l’estomac, et distaux(N2) pour les cancers de l’antre. De la même façon, les groupes 3, 4,5 et 6 sont de proximité (N1) pour les tumeurs antrales et distaux(N2) pour les tumeurs du cardia. Les autres groupes ganglionnairesdistaux sont les groupes 7, 8, 9, 10 (N2). Enfin, les ganglions àdistance situés au-delà de ces limites définissent des atteintesmétastatiques lorsqu’ils sont envahis : ce sont les groupes 12-13 (N3)et 15-16 (N4) (tableau I) [7].
4d
6
83
71
2
9
12a
12b
12p
5
4sb
4sa
4a
11 10
98
12
1614
13
15
5 Drainage lymphatique de l’estomac.
Tableau I.
GroupeLocalisation de la tumeur primitive
CMA A, AM MA, M C, CM, MC
N1 1 3 3 12 4 4 23 5 5 34 6 6 45 16
N2 7 7 2 58 8 7 69 9 8 7
10 1 9 811 10 9
11 1011
N3 12 2 12 1213 10 13 1314 11 14 14
121314
N4 15 15 15 1516 16 16 16
C : tumeur du tiers supérieur ; M : tumeur du tiers moyen ; A : tumeur du tiers inférieur ; groupes N1 et N2 :ganglions régionaux ; groupes N3 et N4 : métastases.
Techniques chirurgicalesGastrectomies pour cancer :
principes généraux, anatomie vasculaire, anatomie lymphatique, curages 40-330-A
3
7
7: Gastrique G 8: Art hépa+que 9: Tronc coeliaque 10: Hile splénique 11: art splénique
Groupes à distance de l’estomac
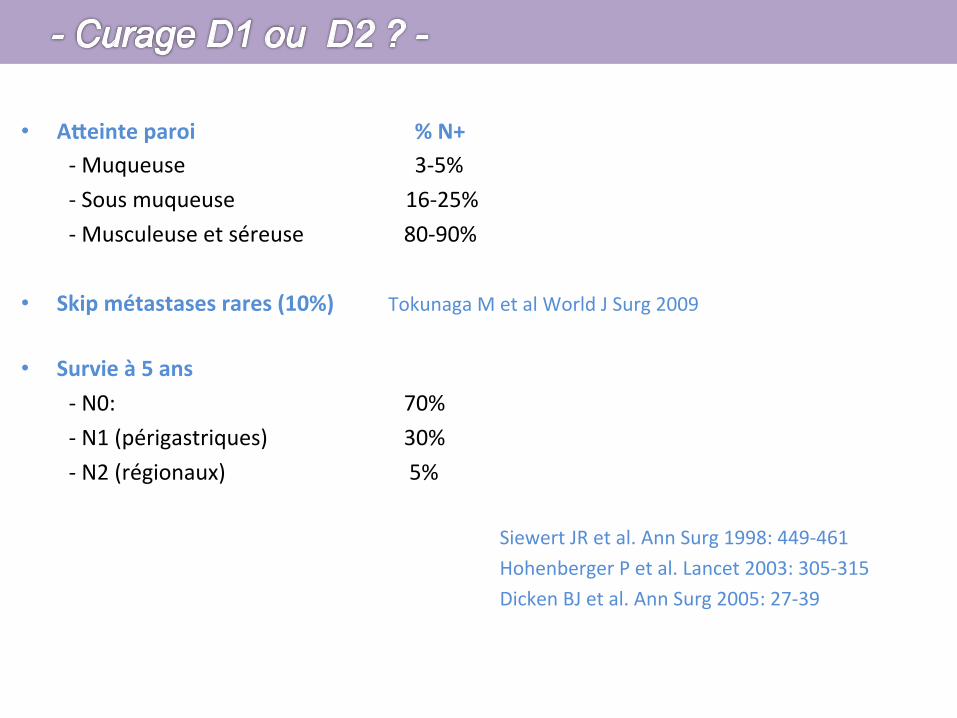
• AReinte paroi % N+ -‐ Muqueuse 3-‐5% -‐ Sous muqueuse 16-‐25% -‐ Musculeuse et séreuse 80-‐90%
• Skip métastases rares (10%) Tokunaga M et al World J Surg 2009
• Survie à 5 ans -‐ N0: 70% -‐ N1 (périgastriques) 30% -‐ N2 (régionaux) 5%
Siewert JR et al. Ann Surg 1998: 449-‐461 Hohenberger P et al. Lancet 2003: 305-‐315 Dicken BJ et al. Ann Surg 2005: 27-‐39
The area extending 2 cm above to 2 cm below the
esophagogastric junction (EGJ) is designated the EGJ area.Tumors having their epicenter in this area are designated
EGJ carcinomas irrespective of histological type. The
location of an EGJ carcinoma is described using the sym-bols E (proximal 2 cm segment) and G (distal 2 cm seg-
ment), with the dominant area of invasion described first,
i.e., E, EG, E=G (both areas equally involved), GE, or G.The distance between the tumor center and the EGJ is
recorded.
The EGJ is defined as the border between the esophagealand gastric muscles. Clinically this is identified by one of
the following: (a) the distal end of the longitudinal pali-
sading small vessels in the lower esophagus at endoscopy;(b) the horizontal level of the angle of His shown by bar-
ium meal examination; (c) the proximal end of the longi-
tudinal folds of the greater curve of the stomach shown atendoscopy or barium meal study; or (d) the level of the
macroscopic caliber change of the resected esophagus and
stomach. It is important to note that the squamocolumnarjunction (SCJ) does not always coincide with the EGJ.
Clinically, the tumor location is often expressed as
cardia, fundus, body, incisura, and antrum.
2.1.2.2 Cross-sectional parts of the stomach The stom-
ach’s cross-sectional circumference is divided into four
equal parts: the lesser (Less) and greater (Gre) curvatures,and the anterior (Ant) and posterior (Post) walls (Fig. 2).
Circumferential involvement is recorded as Circ.
2.1.2.3 Carcinoma in the remnant stomach Carcinoma inthe remnant stomach encompasses all carcinomas arising in
the remnant stomach following a gastrectomy, irrespective ofthe histology of the primary lesion (benign or malignant) or its
risk of recurrence, the extent of resection, or method of
reconstruction. The following information should be recorded,as well as, if available, information on the extent of resection
and type of reconstruction of the previous gastrectomy.
a. The primary lesion at the previous gastrectomy: benign(B), malignant (M), or unknown (X).
b. The time interval elapsed between the previous gastrec-tomy and the current diagnosis, in years (unknown: X).
c. Tumor location in the remnant stomach: anastomotic
site (A), gastric suture line (S), other gastric site (O), ortotal remnant stomach (T). Extension into the esoph-
agus (E), duodenum (D), or jejunum (J) is recorded.
Examples: B-20-S, M-09-AJ.
2.1.3 Macroscopic types
2.1.3.1 Basic classification Gross tumor morphology iscategorized as either superficial or advanced type. Super-
ficial type is typical of T1 tumors while T2–4 tumors
usually manifest as advanced types (Fig. 3). Viewed fromthe mucosal surface, gross tumor appearance is categorized
into six types (Table 2). Type 0 is subdivided according to
the Macroscopic Classification of Early Gastric Cancer(Sect. 2.1.3.2). Although macroscopic type is determined
regardless of the depth of tumor invasion, the T category
should also be recorded.
2.1.3.2 Subclassification of Type 0 (Fig. 4, modified from theJapanese Endoscopy Society Classification of 1962) Super-
ficial tumors with two or more components should have allcomponents recorded in order of the surface area occupied,
e.g. 0-IIc ? III (Table 3).
2.1.3.3 Description of macroscopic type The macro-scopic tumor type should be recorded in both the clinical
and pathological classifications.
Fig. 1 The three portions of the stomach. U upper third, M middlethird, L lower third, E esophagus, D duodenum
Fig. 2 The four equal parts of the gastric circumference. Less lessercurvature, Gre greater curvature, Ant anterior wall, Post posterior wall
Table 1 Clinical and pathological classification
Clinical classification (c) Pathological classification (c)
Physical examination, imagingstudies, endoscopic, laparoscopicand surgical findings, biopsy,cytology, biochemical andbiological investigations.
Histological examination ofsurgically or endoscopicallyresected specimens; peritoneallavage cytology.
102 Japanese Gastric Cancer Association
123
l’arrière-cavité des épiploons. Son ouverture permet d’aborder letronc cœliaque. Celui-ci vascularise le foie, l’estomac, le grandépiploon, la rate et une partie du pancréas. Il naît de la faceantérieure de l’aorte au-dessus du bord supérieur du pancréas, aune longueur de 1 à 3 cm et se termine en se divisant en troisbranches : l’artère gastrique gauche, l’artère hépatique commune etl’artère splénique.
¶ Artère gastrique gauche
L’artère gastrique gauche naît dans 90 % des cas du tronc cœliaque,parfois directement de l’aorte, d’une artère diaphragmatiqueinférieure, d’un tronc gastrosplénique ou d’un tronchépaticogastrique. Elle décrit une crosse qui l’amène le long de lapetite courbure à deux travers de doigt sous le cardia. Lors de laréalisation d’une gastrectomie, elle est liée à son origine en cas depathologie cancéreuse ou au bord de l’estomac en cas de pathologiebénigne. Elle se divise en deux branches, l’une antérieure et l’autrepostérieure, qui descendent appliquées le long de la petite courbure(fig 2). Elles se terminent en s’anastomosant avec les branchesterminales de l’artère gastrique droite ou artère pylorique. L’artèregastrique gauche donne plusieurs branches : une artère hépatiqueinconstante et fonctionnelle dans 30 % des cas ; des artèrescardioœsophagiennes antérieures et postérieures vascularisant lecardia et l’œsophage abdominal.
¶ Artère gastrique droite
L’artère gastrique droite naît habituellement de l’artère hépatiquepropre, plus rarement des artères hépatique commune,gastroduodénale ou hépatique gauche. Elle rejoint le pylore endonnant une de ses principales branches terminales puis se diviseen branches gastriques antérieure et postérieure. Leurs portionsterminales s’anastomosent aux terminaisons de l’artère gastriquegauche au niveau de l’angle de l’estomac, jonction des partiesverticale et horizontale.Les artères gastriques droite et gauche constituent ainsi l’arcvasculaire de la petite courbure (fig 2).
VASCULARISATION DE LA JONCTIONPYLORODUODÉNALE
La réalisation d’une gastrectomie impose le plus souvent une sectionde l’estomac en aval du pylore, sur le premier duodénum. Il estdonc important de préserver autant que possible sa vascularisationafin de limiter les risques de fistule postopératoire. Le duodénummobile est vascularisé par des branches issues pour la plupart del’artère gastroduodénale. La section duodénale s’effectue donc aucontact de l’artère gastroduodénale en veillant à préserver lesrameaux directs entre celle-ci et le duodénum (fig 3).
VASCULARISATION DE LA GRANDE COURBURE
La grande courbure de l’estomac est bordée par le grand épiploonet le ligament gastrosplénique. Le grand épiploon représente lesdeux feuillets du péritoine viscéral gastrique. Il s’étale sur le côlontransverse qu’il dépasse largement vers le bas au niveau du corps etde la portion horizontale de l’estomac et constitue le ligamentgastrosplénique au niveau de la grosse tubérosité. Le feuilletantérieur du grand épiploon contient une arcade vasculairecomposée des vaisseaux gastroépiploïques droits, gauches et desvaisseaux courts.
¶ Artère gastroépiploïque droite
L’artère gastroépiploïque droite naît de la division de l’artèregastroduodénale au bord inférieur du duodénum en artèrespancréaticoduodénale inférieure droite et gastroépiploïque droite(fig 3). Elle chemine de droite à gauche le long de la grande courburede l’estomac, dont elle est toujours distante d’environ 1 cm. Sur sontrajet, elle donne des branches aux deux faces de l’estomac et àl’épiploon.
¶ Artère gastroépiploïque gauche
L’artère gastroépiploïque gauche est une branche de division del’artère splénique. Elle rejoint la grande courbure de l’estomac à sapartie moyenne, chemine dans le ligament gastrocolique ets’anastomose avec les branches terminales de l’artèregastroépiploïque droite.Les artères gastroépiploïques droite et gauche constituent ainsi l’arcvasculaire de la grande courbure (fig 4).
1
2
3
4
5
67
89
2 Vascularisation artérielle de la petite courbure.1. Tronc cœliaque ; 2. artère hépatique propre ; 3. artère hépatique commune ; 4. artèregastrique droite ; 5. artère gastroduodénale ; 6. artère hépatique gauche accessoire ; 7.artère cardioœsophagienne ; 8. artère gastrique gauche ; 9. artère splénique.
1
2
34
3 Vascularisation arté-rielle de la région pyloro-duodénale.1. Artère gastroduodénale ;2. artère pancréaticoduodé-nale supérieure ; 3. artèrepancréaticoduodénale infé-rieure ; 4. artère gastro-épiploïque droite.
1
2
3
45
4 Vascularisation artérielle de la grande courbure.1. Artère gastroépiploïque droite ; 2. vaisseaux courts ; 3. fenêtre avasculaire ; 4. artèresplénique ; 5. artère gastroépiploïque gauche.
40-330-AGastrectomies pour cancer :
principes généraux, anatomie vasculaire, anatomie lymphatique, curages Techniques chirurgicales
2
1/3 INFERIEUR
l’arrière-cavité des épiploons. Son ouverture permet d’aborder letronc cœliaque. Celui-ci vascularise le foie, l’estomac, le grandépiploon, la rate et une partie du pancréas. Il naît de la faceantérieure de l’aorte au-dessus du bord supérieur du pancréas, aune longueur de 1 à 3 cm et se termine en se divisant en troisbranches : l’artère gastrique gauche, l’artère hépatique commune etl’artère splénique.
¶ Artère gastrique gauche
L’artère gastrique gauche naît dans 90 % des cas du tronc cœliaque,parfois directement de l’aorte, d’une artère diaphragmatiqueinférieure, d’un tronc gastrosplénique ou d’un tronchépaticogastrique. Elle décrit une crosse qui l’amène le long de lapetite courbure à deux travers de doigt sous le cardia. Lors de laréalisation d’une gastrectomie, elle est liée à son origine en cas depathologie cancéreuse ou au bord de l’estomac en cas de pathologiebénigne. Elle se divise en deux branches, l’une antérieure et l’autrepostérieure, qui descendent appliquées le long de la petite courbure(fig 2). Elles se terminent en s’anastomosant avec les branchesterminales de l’artère gastrique droite ou artère pylorique. L’artèregastrique gauche donne plusieurs branches : une artère hépatiqueinconstante et fonctionnelle dans 30 % des cas ; des artèrescardioœsophagiennes antérieures et postérieures vascularisant lecardia et l’œsophage abdominal.
¶ Artère gastrique droite
L’artère gastrique droite naît habituellement de l’artère hépatiquepropre, plus rarement des artères hépatique commune,gastroduodénale ou hépatique gauche. Elle rejoint le pylore endonnant une de ses principales branches terminales puis se diviseen branches gastriques antérieure et postérieure. Leurs portionsterminales s’anastomosent aux terminaisons de l’artère gastriquegauche au niveau de l’angle de l’estomac, jonction des partiesverticale et horizontale.Les artères gastriques droite et gauche constituent ainsi l’arcvasculaire de la petite courbure (fig 2).
VASCULARISATION DE LA JONCTIONPYLORODUODÉNALE
La réalisation d’une gastrectomie impose le plus souvent une sectionde l’estomac en aval du pylore, sur le premier duodénum. Il estdonc important de préserver autant que possible sa vascularisationafin de limiter les risques de fistule postopératoire. Le duodénummobile est vascularisé par des branches issues pour la plupart del’artère gastroduodénale. La section duodénale s’effectue donc aucontact de l’artère gastroduodénale en veillant à préserver lesrameaux directs entre celle-ci et le duodénum (fig 3).
VASCULARISATION DE LA GRANDE COURBURE
La grande courbure de l’estomac est bordée par le grand épiploonet le ligament gastrosplénique. Le grand épiploon représente lesdeux feuillets du péritoine viscéral gastrique. Il s’étale sur le côlontransverse qu’il dépasse largement vers le bas au niveau du corps etde la portion horizontale de l’estomac et constitue le ligamentgastrosplénique au niveau de la grosse tubérosité. Le feuilletantérieur du grand épiploon contient une arcade vasculairecomposée des vaisseaux gastroépiploïques droits, gauches et desvaisseaux courts.
¶ Artère gastroépiploïque droite
L’artère gastroépiploïque droite naît de la division de l’artèregastroduodénale au bord inférieur du duodénum en artèrespancréaticoduodénale inférieure droite et gastroépiploïque droite(fig 3). Elle chemine de droite à gauche le long de la grande courburede l’estomac, dont elle est toujours distante d’environ 1 cm. Sur sontrajet, elle donne des branches aux deux faces de l’estomac et àl’épiploon.
¶ Artère gastroépiploïque gauche
L’artère gastroépiploïque gauche est une branche de division del’artère splénique. Elle rejoint la grande courbure de l’estomac à sapartie moyenne, chemine dans le ligament gastrocolique ets’anastomose avec les branches terminales de l’artèregastroépiploïque droite.Les artères gastroépiploïques droite et gauche constituent ainsi l’arcvasculaire de la grande courbure (fig 4).
1
2
3
4
5
67
89
2 Vascularisation artérielle de la petite courbure.1. Tronc cœliaque ; 2. artère hépatique propre ; 3. artère hépatique commune ; 4. artèregastrique droite ; 5. artère gastroduodénale ; 6. artère hépatique gauche accessoire ; 7.artère cardioœsophagienne ; 8. artère gastrique gauche ; 9. artère splénique.
1
2
34
3 Vascularisation arté-rielle de la région pyloro-duodénale.1. Artère gastroduodénale ;2. artère pancréaticoduodé-nale supérieure ; 3. artèrepancréaticoduodénale infé-rieure ; 4. artère gastro-épiploïque droite.
1
2
3
45
4 Vascularisation artérielle de la grande courbure.1. Artère gastroépiploïque droite ; 2. vaisseaux courts ; 3. fenêtre avasculaire ; 4. artèresplénique ; 5. artère gastroépiploïque gauche.
40-330-AGastrectomies pour cancer :
principes généraux, anatomie vasculaire, anatomie lymphatique, curages Techniques chirurgicales
2
6 4
5 3
1/3 INFERIEUR: N 1
l’arrière-cavité des épiploons. Son ouverture permet d’aborder letronc cœliaque. Celui-ci vascularise le foie, l’estomac, le grandépiploon, la rate et une partie du pancréas. Il naît de la faceantérieure de l’aorte au-dessus du bord supérieur du pancréas, aune longueur de 1 à 3 cm et se termine en se divisant en troisbranches : l’artère gastrique gauche, l’artère hépatique commune etl’artère splénique.
¶ Artère gastrique gauche
L’artère gastrique gauche naît dans 90 % des cas du tronc cœliaque,parfois directement de l’aorte, d’une artère diaphragmatiqueinférieure, d’un tronc gastrosplénique ou d’un tronchépaticogastrique. Elle décrit une crosse qui l’amène le long de lapetite courbure à deux travers de doigt sous le cardia. Lors de laréalisation d’une gastrectomie, elle est liée à son origine en cas depathologie cancéreuse ou au bord de l’estomac en cas de pathologiebénigne. Elle se divise en deux branches, l’une antérieure et l’autrepostérieure, qui descendent appliquées le long de la petite courbure(fig 2). Elles se terminent en s’anastomosant avec les branchesterminales de l’artère gastrique droite ou artère pylorique. L’artèregastrique gauche donne plusieurs branches : une artère hépatiqueinconstante et fonctionnelle dans 30 % des cas ; des artèrescardioœsophagiennes antérieures et postérieures vascularisant lecardia et l’œsophage abdominal.
¶ Artère gastrique droite
L’artère gastrique droite naît habituellement de l’artère hépatiquepropre, plus rarement des artères hépatique commune,gastroduodénale ou hépatique gauche. Elle rejoint le pylore endonnant une de ses principales branches terminales puis se diviseen branches gastriques antérieure et postérieure. Leurs portionsterminales s’anastomosent aux terminaisons de l’artère gastriquegauche au niveau de l’angle de l’estomac, jonction des partiesverticale et horizontale.Les artères gastriques droite et gauche constituent ainsi l’arcvasculaire de la petite courbure (fig 2).
VASCULARISATION DE LA JONCTIONPYLORODUODÉNALE
La réalisation d’une gastrectomie impose le plus souvent une sectionde l’estomac en aval du pylore, sur le premier duodénum. Il estdonc important de préserver autant que possible sa vascularisationafin de limiter les risques de fistule postopératoire. Le duodénummobile est vascularisé par des branches issues pour la plupart del’artère gastroduodénale. La section duodénale s’effectue donc aucontact de l’artère gastroduodénale en veillant à préserver lesrameaux directs entre celle-ci et le duodénum (fig 3).
VASCULARISATION DE LA GRANDE COURBURE
La grande courbure de l’estomac est bordée par le grand épiploonet le ligament gastrosplénique. Le grand épiploon représente lesdeux feuillets du péritoine viscéral gastrique. Il s’étale sur le côlontransverse qu’il dépasse largement vers le bas au niveau du corps etde la portion horizontale de l’estomac et constitue le ligamentgastrosplénique au niveau de la grosse tubérosité. Le feuilletantérieur du grand épiploon contient une arcade vasculairecomposée des vaisseaux gastroépiploïques droits, gauches et desvaisseaux courts.
¶ Artère gastroépiploïque droite
L’artère gastroépiploïque droite naît de la division de l’artèregastroduodénale au bord inférieur du duodénum en artèrespancréaticoduodénale inférieure droite et gastroépiploïque droite(fig 3). Elle chemine de droite à gauche le long de la grande courburede l’estomac, dont elle est toujours distante d’environ 1 cm. Sur sontrajet, elle donne des branches aux deux faces de l’estomac et àl’épiploon.
¶ Artère gastroépiploïque gauche
L’artère gastroépiploïque gauche est une branche de division del’artère splénique. Elle rejoint la grande courbure de l’estomac à sapartie moyenne, chemine dans le ligament gastrocolique ets’anastomose avec les branches terminales de l’artèregastroépiploïque droite.Les artères gastroépiploïques droite et gauche constituent ainsi l’arcvasculaire de la grande courbure (fig 4).
1
2
3
4
5
67
89
2 Vascularisation artérielle de la petite courbure.1. Tronc cœliaque ; 2. artère hépatique propre ; 3. artère hépatique commune ; 4. artèregastrique droite ; 5. artère gastroduodénale ; 6. artère hépatique gauche accessoire ; 7.artère cardioœsophagienne ; 8. artère gastrique gauche ; 9. artère splénique.
1
2
34
3 Vascularisation arté-rielle de la région pyloro-duodénale.1. Artère gastroduodénale ;2. artère pancréaticoduodé-nale supérieure ; 3. artèrepancréaticoduodénale infé-rieure ; 4. artère gastro-épiploïque droite.
1
2
3
45
4 Vascularisation artérielle de la grande courbure.1. Artère gastroépiploïque droite ; 2. vaisseaux courts ; 3. fenêtre avasculaire ; 4. artèresplénique ; 5. artère gastroépiploïque gauche.
40-330-AGastrectomies pour cancer :
principes généraux, anatomie vasculaire, anatomie lymphatique, curages Techniques chirurgicales
2
9
1
8
7
1/3 INFERIEUR: N 2
l’arrière-cavité des épiploons. Son ouverture permet d’aborder letronc cœliaque. Celui-ci vascularise le foie, l’estomac, le grandépiploon, la rate et une partie du pancréas. Il naît de la faceantérieure de l’aorte au-dessus du bord supérieur du pancréas, aune longueur de 1 à 3 cm et se termine en se divisant en troisbranches : l’artère gastrique gauche, l’artère hépatique commune etl’artère splénique.
¶ Artère gastrique gauche
L’artère gastrique gauche naît dans 90 % des cas du tronc cœliaque,parfois directement de l’aorte, d’une artère diaphragmatiqueinférieure, d’un tronc gastrosplénique ou d’un tronchépaticogastrique. Elle décrit une crosse qui l’amène le long de lapetite courbure à deux travers de doigt sous le cardia. Lors de laréalisation d’une gastrectomie, elle est liée à son origine en cas depathologie cancéreuse ou au bord de l’estomac en cas de pathologiebénigne. Elle se divise en deux branches, l’une antérieure et l’autrepostérieure, qui descendent appliquées le long de la petite courbure(fig 2). Elles se terminent en s’anastomosant avec les branchesterminales de l’artère gastrique droite ou artère pylorique. L’artèregastrique gauche donne plusieurs branches : une artère hépatiqueinconstante et fonctionnelle dans 30 % des cas ; des artèrescardioœsophagiennes antérieures et postérieures vascularisant lecardia et l’œsophage abdominal.
¶ Artère gastrique droite
L’artère gastrique droite naît habituellement de l’artère hépatiquepropre, plus rarement des artères hépatique commune,gastroduodénale ou hépatique gauche. Elle rejoint le pylore endonnant une de ses principales branches terminales puis se diviseen branches gastriques antérieure et postérieure. Leurs portionsterminales s’anastomosent aux terminaisons de l’artère gastriquegauche au niveau de l’angle de l’estomac, jonction des partiesverticale et horizontale.Les artères gastriques droite et gauche constituent ainsi l’arcvasculaire de la petite courbure (fig 2).
VASCULARISATION DE LA JONCTIONPYLORODUODÉNALE
La réalisation d’une gastrectomie impose le plus souvent une sectionde l’estomac en aval du pylore, sur le premier duodénum. Il estdonc important de préserver autant que possible sa vascularisationafin de limiter les risques de fistule postopératoire. Le duodénummobile est vascularisé par des branches issues pour la plupart del’artère gastroduodénale. La section duodénale s’effectue donc aucontact de l’artère gastroduodénale en veillant à préserver lesrameaux directs entre celle-ci et le duodénum (fig 3).
VASCULARISATION DE LA GRANDE COURBURE
La grande courbure de l’estomac est bordée par le grand épiploonet le ligament gastrosplénique. Le grand épiploon représente lesdeux feuillets du péritoine viscéral gastrique. Il s’étale sur le côlontransverse qu’il dépasse largement vers le bas au niveau du corps etde la portion horizontale de l’estomac et constitue le ligamentgastrosplénique au niveau de la grosse tubérosité. Le feuilletantérieur du grand épiploon contient une arcade vasculairecomposée des vaisseaux gastroépiploïques droits, gauches et desvaisseaux courts.
¶ Artère gastroépiploïque droite
L’artère gastroépiploïque droite naît de la division de l’artèregastroduodénale au bord inférieur du duodénum en artèrespancréaticoduodénale inférieure droite et gastroépiploïque droite(fig 3). Elle chemine de droite à gauche le long de la grande courburede l’estomac, dont elle est toujours distante d’environ 1 cm. Sur sontrajet, elle donne des branches aux deux faces de l’estomac et àl’épiploon.
¶ Artère gastroépiploïque gauche
L’artère gastroépiploïque gauche est une branche de division del’artère splénique. Elle rejoint la grande courbure de l’estomac à sapartie moyenne, chemine dans le ligament gastrocolique ets’anastomose avec les branches terminales de l’artèregastroépiploïque droite.Les artères gastroépiploïques droite et gauche constituent ainsi l’arcvasculaire de la grande courbure (fig 4).
1
2
3
4
5
67
89
2 Vascularisation artérielle de la petite courbure.1. Tronc cœliaque ; 2. artère hépatique propre ; 3. artère hépatique commune ; 4. artèregastrique droite ; 5. artère gastroduodénale ; 6. artère hépatique gauche accessoire ; 7.artère cardioœsophagienne ; 8. artère gastrique gauche ; 9. artère splénique.
1
2
34
3 Vascularisation arté-rielle de la région pyloro-duodénale.1. Artère gastroduodénale ;2. artère pancréaticoduodé-nale supérieure ; 3. artèrepancréaticoduodénale infé-rieure ; 4. artère gastro-épiploïque droite.
1
2
3
45
4 Vascularisation artérielle de la grande courbure.1. Artère gastroépiploïque droite ; 2. vaisseaux courts ; 3. fenêtre avasculaire ; 4. artèresplénique ; 5. artère gastroépiploïque gauche.
40-330-AGastrectomies pour cancer :
principes généraux, anatomie vasculaire, anatomie lymphatique, curages Techniques chirurgicales
2
1/3 MOYEN
l’arrière-cavité des épiploons. Son ouverture permet d’aborder letronc cœliaque. Celui-ci vascularise le foie, l’estomac, le grandépiploon, la rate et une partie du pancréas. Il naît de la faceantérieure de l’aorte au-dessus du bord supérieur du pancréas, aune longueur de 1 à 3 cm et se termine en se divisant en troisbranches : l’artère gastrique gauche, l’artère hépatique commune etl’artère splénique.
¶ Artère gastrique gauche
L’artère gastrique gauche naît dans 90 % des cas du tronc cœliaque,parfois directement de l’aorte, d’une artère diaphragmatiqueinférieure, d’un tronc gastrosplénique ou d’un tronchépaticogastrique. Elle décrit une crosse qui l’amène le long de lapetite courbure à deux travers de doigt sous le cardia. Lors de laréalisation d’une gastrectomie, elle est liée à son origine en cas depathologie cancéreuse ou au bord de l’estomac en cas de pathologiebénigne. Elle se divise en deux branches, l’une antérieure et l’autrepostérieure, qui descendent appliquées le long de la petite courbure(fig 2). Elles se terminent en s’anastomosant avec les branchesterminales de l’artère gastrique droite ou artère pylorique. L’artèregastrique gauche donne plusieurs branches : une artère hépatiqueinconstante et fonctionnelle dans 30 % des cas ; des artèrescardioœsophagiennes antérieures et postérieures vascularisant lecardia et l’œsophage abdominal.
¶ Artère gastrique droite
L’artère gastrique droite naît habituellement de l’artère hépatiquepropre, plus rarement des artères hépatique commune,gastroduodénale ou hépatique gauche. Elle rejoint le pylore endonnant une de ses principales branches terminales puis se diviseen branches gastriques antérieure et postérieure. Leurs portionsterminales s’anastomosent aux terminaisons de l’artère gastriquegauche au niveau de l’angle de l’estomac, jonction des partiesverticale et horizontale.Les artères gastriques droite et gauche constituent ainsi l’arcvasculaire de la petite courbure (fig 2).
VASCULARISATION DE LA JONCTIONPYLORODUODÉNALE
La réalisation d’une gastrectomie impose le plus souvent une sectionde l’estomac en aval du pylore, sur le premier duodénum. Il estdonc important de préserver autant que possible sa vascularisationafin de limiter les risques de fistule postopératoire. Le duodénummobile est vascularisé par des branches issues pour la plupart del’artère gastroduodénale. La section duodénale s’effectue donc aucontact de l’artère gastroduodénale en veillant à préserver lesrameaux directs entre celle-ci et le duodénum (fig 3).
VASCULARISATION DE LA GRANDE COURBURE
La grande courbure de l’estomac est bordée par le grand épiploonet le ligament gastrosplénique. Le grand épiploon représente lesdeux feuillets du péritoine viscéral gastrique. Il s’étale sur le côlontransverse qu’il dépasse largement vers le bas au niveau du corps etde la portion horizontale de l’estomac et constitue le ligamentgastrosplénique au niveau de la grosse tubérosité. Le feuilletantérieur du grand épiploon contient une arcade vasculairecomposée des vaisseaux gastroépiploïques droits, gauches et desvaisseaux courts.
¶ Artère gastroépiploïque droite
L’artère gastroépiploïque droite naît de la division de l’artèregastroduodénale au bord inférieur du duodénum en artèrespancréaticoduodénale inférieure droite et gastroépiploïque droite(fig 3). Elle chemine de droite à gauche le long de la grande courburede l’estomac, dont elle est toujours distante d’environ 1 cm. Sur sontrajet, elle donne des branches aux deux faces de l’estomac et àl’épiploon.
¶ Artère gastroépiploïque gauche
L’artère gastroépiploïque gauche est une branche de division del’artère splénique. Elle rejoint la grande courbure de l’estomac à sapartie moyenne, chemine dans le ligament gastrocolique ets’anastomose avec les branches terminales de l’artèregastroépiploïque droite.Les artères gastroépiploïques droite et gauche constituent ainsi l’arcvasculaire de la grande courbure (fig 4).
1
2
3
4
5
67
89
2 Vascularisation artérielle de la petite courbure.1. Tronc cœliaque ; 2. artère hépatique propre ; 3. artère hépatique commune ; 4. artèregastrique droite ; 5. artère gastroduodénale ; 6. artère hépatique gauche accessoire ; 7.artère cardioœsophagienne ; 8. artère gastrique gauche ; 9. artère splénique.
1
2
34
3 Vascularisation arté-rielle de la région pyloro-duodénale.1. Artère gastroduodénale ;2. artère pancréaticoduodé-nale supérieure ; 3. artèrepancréaticoduodénale infé-rieure ; 4. artère gastro-épiploïque droite.
1
2
3
45
4 Vascularisation artérielle de la grande courbure.1. Artère gastroépiploïque droite ; 2. vaisseaux courts ; 3. fenêtre avasculaire ; 4. artèresplénique ; 5. artère gastroépiploïque gauche.
40-330-AGastrectomies pour cancer :
principes généraux, anatomie vasculaire, anatomie lymphatique, curages Techniques chirurgicales
2
1/3 MOYEN: N 1
6 4
5 3
1
l’arrière-cavité des épiploons. Son ouverture permet d’aborder letronc cœliaque. Celui-ci vascularise le foie, l’estomac, le grandépiploon, la rate et une partie du pancréas. Il naît de la faceantérieure de l’aorte au-dessus du bord supérieur du pancréas, aune longueur de 1 à 3 cm et se termine en se divisant en troisbranches : l’artère gastrique gauche, l’artère hépatique commune etl’artère splénique.
¶ Artère gastrique gauche
L’artère gastrique gauche naît dans 90 % des cas du tronc cœliaque,parfois directement de l’aorte, d’une artère diaphragmatiqueinférieure, d’un tronc gastrosplénique ou d’un tronchépaticogastrique. Elle décrit une crosse qui l’amène le long de lapetite courbure à deux travers de doigt sous le cardia. Lors de laréalisation d’une gastrectomie, elle est liée à son origine en cas depathologie cancéreuse ou au bord de l’estomac en cas de pathologiebénigne. Elle se divise en deux branches, l’une antérieure et l’autrepostérieure, qui descendent appliquées le long de la petite courbure(fig 2). Elles se terminent en s’anastomosant avec les branchesterminales de l’artère gastrique droite ou artère pylorique. L’artèregastrique gauche donne plusieurs branches : une artère hépatiqueinconstante et fonctionnelle dans 30 % des cas ; des artèrescardioœsophagiennes antérieures et postérieures vascularisant lecardia et l’œsophage abdominal.
¶ Artère gastrique droite
L’artère gastrique droite naît habituellement de l’artère hépatiquepropre, plus rarement des artères hépatique commune,gastroduodénale ou hépatique gauche. Elle rejoint le pylore endonnant une de ses principales branches terminales puis se diviseen branches gastriques antérieure et postérieure. Leurs portionsterminales s’anastomosent aux terminaisons de l’artère gastriquegauche au niveau de l’angle de l’estomac, jonction des partiesverticale et horizontale.Les artères gastriques droite et gauche constituent ainsi l’arcvasculaire de la petite courbure (fig 2).
VASCULARISATION DE LA JONCTIONPYLORODUODÉNALE
La réalisation d’une gastrectomie impose le plus souvent une sectionde l’estomac en aval du pylore, sur le premier duodénum. Il estdonc important de préserver autant que possible sa vascularisationafin de limiter les risques de fistule postopératoire. Le duodénummobile est vascularisé par des branches issues pour la plupart del’artère gastroduodénale. La section duodénale s’effectue donc aucontact de l’artère gastroduodénale en veillant à préserver lesrameaux directs entre celle-ci et le duodénum (fig 3).
VASCULARISATION DE LA GRANDE COURBURE
La grande courbure de l’estomac est bordée par le grand épiploonet le ligament gastrosplénique. Le grand épiploon représente lesdeux feuillets du péritoine viscéral gastrique. Il s’étale sur le côlontransverse qu’il dépasse largement vers le bas au niveau du corps etde la portion horizontale de l’estomac et constitue le ligamentgastrosplénique au niveau de la grosse tubérosité. Le feuilletantérieur du grand épiploon contient une arcade vasculairecomposée des vaisseaux gastroépiploïques droits, gauches et desvaisseaux courts.
¶ Artère gastroépiploïque droite
L’artère gastroépiploïque droite naît de la division de l’artèregastroduodénale au bord inférieur du duodénum en artèrespancréaticoduodénale inférieure droite et gastroépiploïque droite(fig 3). Elle chemine de droite à gauche le long de la grande courburede l’estomac, dont elle est toujours distante d’environ 1 cm. Sur sontrajet, elle donne des branches aux deux faces de l’estomac et àl’épiploon.
¶ Artère gastroépiploïque gauche
L’artère gastroépiploïque gauche est une branche de division del’artère splénique. Elle rejoint la grande courbure de l’estomac à sapartie moyenne, chemine dans le ligament gastrocolique ets’anastomose avec les branches terminales de l’artèregastroépiploïque droite.Les artères gastroépiploïques droite et gauche constituent ainsi l’arcvasculaire de la grande courbure (fig 4).
1
2
3
4
5
67
89
2 Vascularisation artérielle de la petite courbure.1. Tronc cœliaque ; 2. artère hépatique propre ; 3. artère hépatique commune ; 4. artèregastrique droite ; 5. artère gastroduodénale ; 6. artère hépatique gauche accessoire ; 7.artère cardioœsophagienne ; 8. artère gastrique gauche ; 9. artère splénique.
1
2
34
3 Vascularisation arté-rielle de la région pyloro-duodénale.1. Artère gastroduodénale ;2. artère pancréaticoduodé-nale supérieure ; 3. artèrepancréaticoduodénale infé-rieure ; 4. artère gastro-épiploïque droite.
1
2
3
45
4 Vascularisation artérielle de la grande courbure.1. Artère gastroépiploïque droite ; 2. vaisseaux courts ; 3. fenêtre avasculaire ; 4. artèresplénique ; 5. artère gastroépiploïque gauche.
40-330-AGastrectomies pour cancer :
principes généraux, anatomie vasculaire, anatomie lymphatique, curages Techniques chirurgicales
2
11
2
1/3 MOYEN: N 2
9 8
7 10
l’arrière-cavité des épiploons. Son ouverture permet d’aborder letronc cœliaque. Celui-ci vascularise le foie, l’estomac, le grandépiploon, la rate et une partie du pancréas. Il naît de la faceantérieure de l’aorte au-dessus du bord supérieur du pancréas, aune longueur de 1 à 3 cm et se termine en se divisant en troisbranches : l’artère gastrique gauche, l’artère hépatique commune etl’artère splénique.
¶ Artère gastrique gauche
L’artère gastrique gauche naît dans 90 % des cas du tronc cœliaque,parfois directement de l’aorte, d’une artère diaphragmatiqueinférieure, d’un tronc gastrosplénique ou d’un tronchépaticogastrique. Elle décrit une crosse qui l’amène le long de lapetite courbure à deux travers de doigt sous le cardia. Lors de laréalisation d’une gastrectomie, elle est liée à son origine en cas depathologie cancéreuse ou au bord de l’estomac en cas de pathologiebénigne. Elle se divise en deux branches, l’une antérieure et l’autrepostérieure, qui descendent appliquées le long de la petite courbure(fig 2). Elles se terminent en s’anastomosant avec les branchesterminales de l’artère gastrique droite ou artère pylorique. L’artèregastrique gauche donne plusieurs branches : une artère hépatiqueinconstante et fonctionnelle dans 30 % des cas ; des artèrescardioœsophagiennes antérieures et postérieures vascularisant lecardia et l’œsophage abdominal.
¶ Artère gastrique droite
L’artère gastrique droite naît habituellement de l’artère hépatiquepropre, plus rarement des artères hépatique commune,gastroduodénale ou hépatique gauche. Elle rejoint le pylore endonnant une de ses principales branches terminales puis se diviseen branches gastriques antérieure et postérieure. Leurs portionsterminales s’anastomosent aux terminaisons de l’artère gastriquegauche au niveau de l’angle de l’estomac, jonction des partiesverticale et horizontale.Les artères gastriques droite et gauche constituent ainsi l’arcvasculaire de la petite courbure (fig 2).
VASCULARISATION DE LA JONCTIONPYLORODUODÉNALE
La réalisation d’une gastrectomie impose le plus souvent une sectionde l’estomac en aval du pylore, sur le premier duodénum. Il estdonc important de préserver autant que possible sa vascularisationafin de limiter les risques de fistule postopératoire. Le duodénummobile est vascularisé par des branches issues pour la plupart del’artère gastroduodénale. La section duodénale s’effectue donc aucontact de l’artère gastroduodénale en veillant à préserver lesrameaux directs entre celle-ci et le duodénum (fig 3).
VASCULARISATION DE LA GRANDE COURBURE
La grande courbure de l’estomac est bordée par le grand épiploonet le ligament gastrosplénique. Le grand épiploon représente lesdeux feuillets du péritoine viscéral gastrique. Il s’étale sur le côlontransverse qu’il dépasse largement vers le bas au niveau du corps etde la portion horizontale de l’estomac et constitue le ligamentgastrosplénique au niveau de la grosse tubérosité. Le feuilletantérieur du grand épiploon contient une arcade vasculairecomposée des vaisseaux gastroépiploïques droits, gauches et desvaisseaux courts.
¶ Artère gastroépiploïque droite
L’artère gastroépiploïque droite naît de la division de l’artèregastroduodénale au bord inférieur du duodénum en artèrespancréaticoduodénale inférieure droite et gastroépiploïque droite(fig 3). Elle chemine de droite à gauche le long de la grande courburede l’estomac, dont elle est toujours distante d’environ 1 cm. Sur sontrajet, elle donne des branches aux deux faces de l’estomac et àl’épiploon.
¶ Artère gastroépiploïque gauche
L’artère gastroépiploïque gauche est une branche de division del’artère splénique. Elle rejoint la grande courbure de l’estomac à sapartie moyenne, chemine dans le ligament gastrocolique ets’anastomose avec les branches terminales de l’artèregastroépiploïque droite.Les artères gastroépiploïques droite et gauche constituent ainsi l’arcvasculaire de la grande courbure (fig 4).
1
2
3
4
5
67
89
2 Vascularisation artérielle de la petite courbure.1. Tronc cœliaque ; 2. artère hépatique propre ; 3. artère hépatique commune ; 4. artèregastrique droite ; 5. artère gastroduodénale ; 6. artère hépatique gauche accessoire ; 7.artère cardioœsophagienne ; 8. artère gastrique gauche ; 9. artère splénique.
1
2
34
3 Vascularisation arté-rielle de la région pyloro-duodénale.1. Artère gastroduodénale ;2. artère pancréaticoduodé-nale supérieure ; 3. artèrepancréaticoduodénale infé-rieure ; 4. artère gastro-épiploïque droite.
1
2
3
45
4 Vascularisation artérielle de la grande courbure.1. Artère gastroépiploïque droite ; 2. vaisseaux courts ; 3. fenêtre avasculaire ; 4. artèresplénique ; 5. artère gastroépiploïque gauche.
40-330-AGastrectomies pour cancer :
principes généraux, anatomie vasculaire, anatomie lymphatique, curages Techniques chirurgicales
2
1/3 SUPERIEUR
l’arrière-cavité des épiploons. Son ouverture permet d’aborder letronc cœliaque. Celui-ci vascularise le foie, l’estomac, le grandépiploon, la rate et une partie du pancréas. Il naît de la faceantérieure de l’aorte au-dessus du bord supérieur du pancréas, aune longueur de 1 à 3 cm et se termine en se divisant en troisbranches : l’artère gastrique gauche, l’artère hépatique commune etl’artère splénique.
¶ Artère gastrique gauche
L’artère gastrique gauche naît dans 90 % des cas du tronc cœliaque,parfois directement de l’aorte, d’une artère diaphragmatiqueinférieure, d’un tronc gastrosplénique ou d’un tronchépaticogastrique. Elle décrit une crosse qui l’amène le long de lapetite courbure à deux travers de doigt sous le cardia. Lors de laréalisation d’une gastrectomie, elle est liée à son origine en cas depathologie cancéreuse ou au bord de l’estomac en cas de pathologiebénigne. Elle se divise en deux branches, l’une antérieure et l’autrepostérieure, qui descendent appliquées le long de la petite courbure(fig 2). Elles se terminent en s’anastomosant avec les branchesterminales de l’artère gastrique droite ou artère pylorique. L’artèregastrique gauche donne plusieurs branches : une artère hépatiqueinconstante et fonctionnelle dans 30 % des cas ; des artèrescardioœsophagiennes antérieures et postérieures vascularisant lecardia et l’œsophage abdominal.
¶ Artère gastrique droite
L’artère gastrique droite naît habituellement de l’artère hépatiquepropre, plus rarement des artères hépatique commune,gastroduodénale ou hépatique gauche. Elle rejoint le pylore endonnant une de ses principales branches terminales puis se diviseen branches gastriques antérieure et postérieure. Leurs portionsterminales s’anastomosent aux terminaisons de l’artère gastriquegauche au niveau de l’angle de l’estomac, jonction des partiesverticale et horizontale.Les artères gastriques droite et gauche constituent ainsi l’arcvasculaire de la petite courbure (fig 2).
VASCULARISATION DE LA JONCTIONPYLORODUODÉNALE
La réalisation d’une gastrectomie impose le plus souvent une sectionde l’estomac en aval du pylore, sur le premier duodénum. Il estdonc important de préserver autant que possible sa vascularisationafin de limiter les risques de fistule postopératoire. Le duodénummobile est vascularisé par des branches issues pour la plupart del’artère gastroduodénale. La section duodénale s’effectue donc aucontact de l’artère gastroduodénale en veillant à préserver lesrameaux directs entre celle-ci et le duodénum (fig 3).
VASCULARISATION DE LA GRANDE COURBURE
La grande courbure de l’estomac est bordée par le grand épiploonet le ligament gastrosplénique. Le grand épiploon représente lesdeux feuillets du péritoine viscéral gastrique. Il s’étale sur le côlontransverse qu’il dépasse largement vers le bas au niveau du corps etde la portion horizontale de l’estomac et constitue le ligamentgastrosplénique au niveau de la grosse tubérosité. Le feuilletantérieur du grand épiploon contient une arcade vasculairecomposée des vaisseaux gastroépiploïques droits, gauches et desvaisseaux courts.
¶ Artère gastroépiploïque droite
L’artère gastroépiploïque droite naît de la division de l’artèregastroduodénale au bord inférieur du duodénum en artèrespancréaticoduodénale inférieure droite et gastroépiploïque droite(fig 3). Elle chemine de droite à gauche le long de la grande courburede l’estomac, dont elle est toujours distante d’environ 1 cm. Sur sontrajet, elle donne des branches aux deux faces de l’estomac et àl’épiploon.
¶ Artère gastroépiploïque gauche
L’artère gastroépiploïque gauche est une branche de division del’artère splénique. Elle rejoint la grande courbure de l’estomac à sapartie moyenne, chemine dans le ligament gastrocolique ets’anastomose avec les branches terminales de l’artèregastroépiploïque droite.Les artères gastroépiploïques droite et gauche constituent ainsi l’arcvasculaire de la grande courbure (fig 4).
1
2
3
4
5
67
89
2 Vascularisation artérielle de la petite courbure.1. Tronc cœliaque ; 2. artère hépatique propre ; 3. artère hépatique commune ; 4. artèregastrique droite ; 5. artère gastroduodénale ; 6. artère hépatique gauche accessoire ; 7.artère cardioœsophagienne ; 8. artère gastrique gauche ; 9. artère splénique.
1
2
34
3 Vascularisation arté-rielle de la région pyloro-duodénale.1. Artère gastroduodénale ;2. artère pancréaticoduodé-nale supérieure ; 3. artèrepancréaticoduodénale infé-rieure ; 4. artère gastro-épiploïque droite.
1
2
3
45
4 Vascularisation artérielle de la grande courbure.1. Artère gastroépiploïque droite ; 2. vaisseaux courts ; 3. fenêtre avasculaire ; 4. artèresplénique ; 5. artère gastroépiploïque gauche.
40-330-AGastrectomies pour cancer :
principes généraux, anatomie vasculaire, anatomie lymphatique, curages Techniques chirurgicales
2
1/3 SUPERIEUR: N 1
6 4
5 3
1 2
l’arrière-cavité des épiploons. Son ouverture permet d’aborder letronc cœliaque. Celui-ci vascularise le foie, l’estomac, le grandépiploon, la rate et une partie du pancréas. Il naît de la faceantérieure de l’aorte au-dessus du bord supérieur du pancréas, aune longueur de 1 à 3 cm et se termine en se divisant en troisbranches : l’artère gastrique gauche, l’artère hépatique commune etl’artère splénique.
¶ Artère gastrique gauche
L’artère gastrique gauche naît dans 90 % des cas du tronc cœliaque,parfois directement de l’aorte, d’une artère diaphragmatiqueinférieure, d’un tronc gastrosplénique ou d’un tronchépaticogastrique. Elle décrit une crosse qui l’amène le long de lapetite courbure à deux travers de doigt sous le cardia. Lors de laréalisation d’une gastrectomie, elle est liée à son origine en cas depathologie cancéreuse ou au bord de l’estomac en cas de pathologiebénigne. Elle se divise en deux branches, l’une antérieure et l’autrepostérieure, qui descendent appliquées le long de la petite courbure(fig 2). Elles se terminent en s’anastomosant avec les branchesterminales de l’artère gastrique droite ou artère pylorique. L’artèregastrique gauche donne plusieurs branches : une artère hépatiqueinconstante et fonctionnelle dans 30 % des cas ; des artèrescardioœsophagiennes antérieures et postérieures vascularisant lecardia et l’œsophage abdominal.
¶ Artère gastrique droite
L’artère gastrique droite naît habituellement de l’artère hépatiquepropre, plus rarement des artères hépatique commune,gastroduodénale ou hépatique gauche. Elle rejoint le pylore endonnant une de ses principales branches terminales puis se diviseen branches gastriques antérieure et postérieure. Leurs portionsterminales s’anastomosent aux terminaisons de l’artère gastriquegauche au niveau de l’angle de l’estomac, jonction des partiesverticale et horizontale.Les artères gastriques droite et gauche constituent ainsi l’arcvasculaire de la petite courbure (fig 2).
VASCULARISATION DE LA JONCTIONPYLORODUODÉNALE
La réalisation d’une gastrectomie impose le plus souvent une sectionde l’estomac en aval du pylore, sur le premier duodénum. Il estdonc important de préserver autant que possible sa vascularisationafin de limiter les risques de fistule postopératoire. Le duodénummobile est vascularisé par des branches issues pour la plupart del’artère gastroduodénale. La section duodénale s’effectue donc aucontact de l’artère gastroduodénale en veillant à préserver lesrameaux directs entre celle-ci et le duodénum (fig 3).
VASCULARISATION DE LA GRANDE COURBURE
La grande courbure de l’estomac est bordée par le grand épiploonet le ligament gastrosplénique. Le grand épiploon représente lesdeux feuillets du péritoine viscéral gastrique. Il s’étale sur le côlontransverse qu’il dépasse largement vers le bas au niveau du corps etde la portion horizontale de l’estomac et constitue le ligamentgastrosplénique au niveau de la grosse tubérosité. Le feuilletantérieur du grand épiploon contient une arcade vasculairecomposée des vaisseaux gastroépiploïques droits, gauches et desvaisseaux courts.
¶ Artère gastroépiploïque droite
L’artère gastroépiploïque droite naît de la division de l’artèregastroduodénale au bord inférieur du duodénum en artèrespancréaticoduodénale inférieure droite et gastroépiploïque droite(fig 3). Elle chemine de droite à gauche le long de la grande courburede l’estomac, dont elle est toujours distante d’environ 1 cm. Sur sontrajet, elle donne des branches aux deux faces de l’estomac et àl’épiploon.
¶ Artère gastroépiploïque gauche
L’artère gastroépiploïque gauche est une branche de division del’artère splénique. Elle rejoint la grande courbure de l’estomac à sapartie moyenne, chemine dans le ligament gastrocolique ets’anastomose avec les branches terminales de l’artèregastroépiploïque droite.Les artères gastroépiploïques droite et gauche constituent ainsi l’arcvasculaire de la grande courbure (fig 4).
1
2
3
4
5
67
89
2 Vascularisation artérielle de la petite courbure.1. Tronc cœliaque ; 2. artère hépatique propre ; 3. artère hépatique commune ; 4. artèregastrique droite ; 5. artère gastroduodénale ; 6. artère hépatique gauche accessoire ; 7.artère cardioœsophagienne ; 8. artère gastrique gauche ; 9. artère splénique.
1
2
34
3 Vascularisation arté-rielle de la région pyloro-duodénale.1. Artère gastroduodénale ;2. artère pancréaticoduodé-nale supérieure ; 3. artèrepancréaticoduodénale infé-rieure ; 4. artère gastro-épiploïque droite.
1
2
3
45
4 Vascularisation artérielle de la grande courbure.1. Artère gastroépiploïque droite ; 2. vaisseaux courts ; 3. fenêtre avasculaire ; 4. artèresplénique ; 5. artère gastroépiploïque gauche.
40-330-AGastrectomies pour cancer :
principes généraux, anatomie vasculaire, anatomie lymphatique, curages Techniques chirurgicales
2
1/3 SUPERIEUR: N 2
8
7 10 11 9
Latéralement, la zone de dissection est limitée par la bifurcation dutronc gastrocolique, en bas par les branches des veines jéjunales eten haut par l’origine de l’artère mésentérique supérieure. Legroupe 15 correspond aux adénopathies situées le long de l’artèrecolique médiane. La dissection suit la veine colique médiane jusqu’àla veine mésentérique. Celle-ci est disséquée jusqu’au troncgastrocolique pour pouvoir réséquer les trois branches veineuses àleur terminaison : la veine gastroépiploïque, la veine colique droiteet la veine pancréaticoduodénale inférieure. La résection du groupe15 implique une colectomie transverse associée et est indiquée dansles tumeurs T4 avec envahissement (fig 16).
– Groupe 16 : ce relais ganglionnaire est satellite de l’aorte et de laveine cave inférieure. Les bords droit et gauche sont représentés parles hiles rénaux correspondants. Envahis par la tumeur, cesganglions sont considérés dans tous les cas comme des métastasesdistantes. La dissection de cette région est habituellement limitée àl’espace situé entre l’artère mésentérique inférieure et le hiatus. Lesrepères sont alors, à gauche, la veine spermatique ou ovarienne et, àdroite, le bord droit de la veine cave. La dissection débute parl’ablation du tissu cellulaire en avant de l’aorte, de la veine rénalegauche à la veine cave. Du bord droit de l’aorte, l’exérèse de tout letissu cellulaire est poursuivie vers la gauche jusqu’à la veinesurrénalienne. L’exérèse du tissu localisé au-dessus de la veinerénale gauche est réalisée en fin d’intervention, après résection dubloc splénopancréatique permettant un jour plus large sur cetterégion (fig 17).
NOMBRE DE GANGLIONS
Le nombre de ganglions pouvant être retirés par les curages peutreprésenter un critère de qualité du curage… ou del’anatomopathologiste. Le nombre moyen de ganglions pouvant êtreretirés par une procédure de type D2 peut varier de 8 à plus de110 [3], la moyenne se situant entre 30 et 50 [3, 10]. Le décompte précisdu nombre de ganglions dans la pièce opératoire, dépendant dugeste chirurgical mais également de l’anatomopathologiste,représente un facteur prédictif d’évolution du cancer de l’estomac.Pour ces raisons, la dernière édition de la classification tumor-nodes-metastases (TNM) prend en compte le nombre de ganglions sur lapièce opératoire dans l’évaluation métastatique du cancer del’estomac. L’absence de ganglions envahis permet alors de classer latumeur : pN0, de un à six ganglions régionaux : pN1, de sept à 15ganglions : pN2 et plus de 15 ganglions : pN3 [12].
Classification des curages
Selon l’extension de l’exérèse ganglionnaire, quatre types de curagessont décrits.
3
2
1
12
14 A. Curage du ligament hépatoduodénal (groupe 12).B. 1 : Ganglions du groupe 12a ; 2 : ganglions du groupe 12b ; 3 : ganglionsdu groupe 12p.
13
15 Exérèse des ganglionsrétroduodénaux (groupe 13).
15
14
16 Dissection des groupes ganglionnaires 14 et 15, situés an contact de l’artère mé-sentérique supérieure et de l’artère colique moyenne.
16
17 Curage extensif aorto-cave et rénal gauche(groupe 16) après réalisa-tion d’une splénopancréa-tectomie pour exposer la ré-gion de dissection.
Techniques chirurgicalesGastrectomies pour cancer :
principes généraux, anatomie vasculaire, anatomie lymphatique, curages 40-330-A
7
Latéralement, la zone de dissection est limitée par la bifurcation dutronc gastrocolique, en bas par les branches des veines jéjunales eten haut par l’origine de l’artère mésentérique supérieure. Legroupe 15 correspond aux adénopathies situées le long de l’artèrecolique médiane. La dissection suit la veine colique médiane jusqu’àla veine mésentérique. Celle-ci est disséquée jusqu’au troncgastrocolique pour pouvoir réséquer les trois branches veineuses àleur terminaison : la veine gastroépiploïque, la veine colique droiteet la veine pancréaticoduodénale inférieure. La résection du groupe15 implique une colectomie transverse associée et est indiquée dansles tumeurs T4 avec envahissement (fig 16).
– Groupe 16 : ce relais ganglionnaire est satellite de l’aorte et de laveine cave inférieure. Les bords droit et gauche sont représentés parles hiles rénaux correspondants. Envahis par la tumeur, cesganglions sont considérés dans tous les cas comme des métastasesdistantes. La dissection de cette région est habituellement limitée àl’espace situé entre l’artère mésentérique inférieure et le hiatus. Lesrepères sont alors, à gauche, la veine spermatique ou ovarienne et, àdroite, le bord droit de la veine cave. La dissection débute parl’ablation du tissu cellulaire en avant de l’aorte, de la veine rénalegauche à la veine cave. Du bord droit de l’aorte, l’exérèse de tout letissu cellulaire est poursuivie vers la gauche jusqu’à la veinesurrénalienne. L’exérèse du tissu localisé au-dessus de la veinerénale gauche est réalisée en fin d’intervention, après résection dubloc splénopancréatique permettant un jour plus large sur cetterégion (fig 17).
NOMBRE DE GANGLIONS
Le nombre de ganglions pouvant être retirés par les curages peutreprésenter un critère de qualité du curage… ou del’anatomopathologiste. Le nombre moyen de ganglions pouvant êtreretirés par une procédure de type D2 peut varier de 8 à plus de110 [3], la moyenne se situant entre 30 et 50 [3, 10]. Le décompte précisdu nombre de ganglions dans la pièce opératoire, dépendant dugeste chirurgical mais également de l’anatomopathologiste,représente un facteur prédictif d’évolution du cancer de l’estomac.Pour ces raisons, la dernière édition de la classification tumor-nodes-metastases (TNM) prend en compte le nombre de ganglions sur lapièce opératoire dans l’évaluation métastatique du cancer del’estomac. L’absence de ganglions envahis permet alors de classer latumeur : pN0, de un à six ganglions régionaux : pN1, de sept à 15ganglions : pN2 et plus de 15 ganglions : pN3 [12].
Classification des curages
Selon l’extension de l’exérèse ganglionnaire, quatre types de curagessont décrits.
3
2
1
12
14 A. Curage du ligament hépatoduodénal (groupe 12).B. 1 : Ganglions du groupe 12a ; 2 : ganglions du groupe 12b ; 3 : ganglionsdu groupe 12p.
13
15 Exérèse des ganglionsrétroduodénaux (groupe 13).
15
14
16 Dissection des groupes ganglionnaires 14 et 15, situés an contact de l’artère mé-sentérique supérieure et de l’artère colique moyenne.
16
17 Curage extensif aorto-cave et rénal gauche(groupe 16) après réalisa-tion d’une splénopancréa-tectomie pour exposer la ré-gion de dissection.
Techniques chirurgicalesGastrectomies pour cancer :
principes généraux, anatomie vasculaire, anatomie lymphatique, curages 40-330-A
7
Abandonné: métasta+que et morbide+++
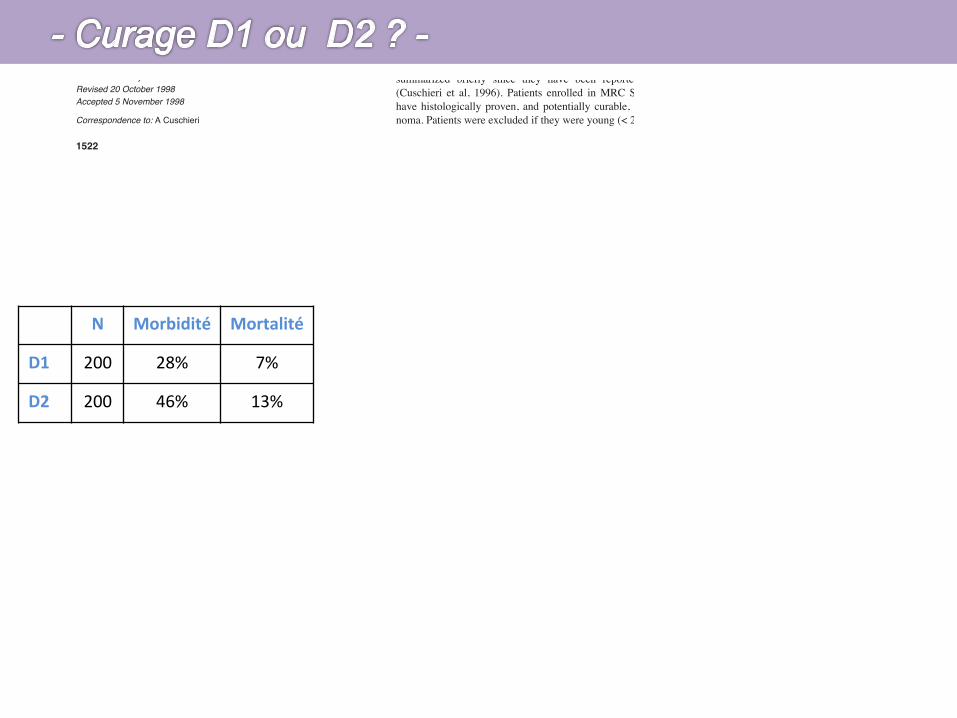
Carcinoma of the stomach remains a major cause of death in mostWestern countries. The only proven effective therapy is surgery,but overall 5-year survival rates remain low after resection. In1981, the Japanese Society for Research in Gastric Cancer(JSRGC) standardized the gastric resections and the extent ofregional lymphadenectomy in accordance with specific rules(updated over the years) based on the location of the tumour andthe respective regional node drainage (Kajitani, 1981). Largeretrospective series from Japan of radical gastrectomy with level-2extended lymphadenectomy (D2 resections) have shown impres-sive 5-year survival rates, certainly much higher than experiencedin the West (Mine et al, 1970; Miwa, 1979; Maruyama et al, 1987;Nakajima and Nishi, 1989). Some non-Japanese centres have alsoreported favourably on D2 resections (Smith et al, 1991; Jaehne etal, 1992; Siewert et al, 1993; Sue-Ling et al, 1993; Mendes et al,1994). However, the benefit of D2 over conventional D1 resections(where only the perigastric nodes within 3.0 cm of the primary areremoved) had not been tested prospectively until the launch of theMedical Research Council (MRC) Gastric Cancer Surgical Trial(ST01) in 1986. This was a randomized comparison of D1 versusD2 resections for potentially curable advanced gastric cancer. At
the time the study was formulated, the Japanese rules dictated thatpancreatico-splenectomy was an integral part of D2 resection forall tumours except antral cancers. For this reason en-bloc removalof these two organs with the stomach was specified by the MRCST01 trial protocol for middle and upper third tumours in the D2arm. In this paper, we report on the long-term outcome of thesetwo surgical treatment arms. Preliminary results of ST01(Cuschieri et al, 1996), and a similar Dutch trial (Bonenkamp et al,1995), have shown that splenectomy and distal hemi-pancreatec-tomy are attended by a significant increase in post-operativemorbidity and mortality. The influence of removal of these organson long-term survival is addressed in this analysis. This is impor-tant as distal hemi-pancreatectomy is no longer considered an inte-gral part of D2 resections by Japanese surgeons, and some Westerncentres are practising spleen- and pancreas-preserving D2 resec-tions with apparent good results (Sue-Ling et al, 1993; Griffith,1995), despite the reported splenic hilar lymph nodes involvementin 15–27% of gastric cancers (Fass and Schumpelick, 1989;Mendes et al, 1994; Mendes et al, 1995; Tsuburaya et al, 1995).
PATIENTS AND METHODS
The organization and preliminary results of the MRC ST01 trial aresummarized briefly since they have been reported previously(Cuschieri et al, 1996). Patients enrolled in MRC ST01 were tohave histologically proven, and potentially curable, gastric carci-noma. Patients were excluded if they were young (< 20 years), had
Patient survival after D1 and D2 resections for gastriccancer: long-term results of the MRC randomizedsurgical trial
A Cuschieri1, S Weeden2, J Fielding3, J Bancewicz4, J Craven5, V Joypaul1, M Sydes2 and P Fayers2, for the SurgicalCo-operative Group1University Department of Surgery, Ninewells Hospital and Medical School, Dundee DD1 9SY, UK; 2Cancer Division MRC Clinical Trials Unit, Cambridge, UK;3Queen Elizabeth Hospital, Birmingham, UK; 4University Department of Surgery, Hope Hospital, Salford, UK; 5Kingstown General Hospital, St Vincents, Jamaica
Summary Controversy still exists on the optimal surgical resection for potentially curable gastric cancer. Much better long-term survival hasbeen reported in retrospective/non-randomized studies with D2 resections that involve a radical extended regional lymphadenectomy thanwith the standard D1 resections. In this paper we report the long-term survival of patients entered into a randomized study, with follow-up todeath or 3 years in 96% of patients and a median follow-up of 6.5 years. In this prospective trial D1 resection (removal of regional perigastricnodes) was compared with D2 resection (extended lymphadenectomy to include level 1 and 2 regional nodes). Central randomization followeda staging laparotomy.
Out of 737 patients with histologically proven gastric adenocarcinoma registered, 337 patients were ineligible by staging laparotomybecause of advanced disease and 400 were randomized. The 5-year survival rates were 35% for D1 resection and 33% for D2 resection(difference –2%, 95% CI = –12%–8%). There was no difference in the overall 5-year survival between the two arms (HR = 1.10, 95% CI0.87–1.39, where HR > 1 implies a survival benefit to D1 surgery). Survival based on death from gastric cancer as the event was similar in theD1 and D2 groups (HR = 1.05, 95% CI 0.79–1.39) as was recurrence-free survival (HR = 1.03, 95% CI 0.82–1.29). In a multivariate analysis,clinical stages II and III, old age, male sex and removal of spleen and pancreas were independently associated with poor survival. Thesefindings indicate that the classical Japanese D2 resection offers no survival advantage over D1 surgery. However, the possibility that D2resection without pancreatico-splenectomy may be better than standard D1 resection cannot be dismissed by the results of this trial.
Keywords: gastric cancer; D1 resection; D2 resection; long-term survival
1522
British Journal of Cancer (1999) 79(9/10), 1522–1530© 1999 Cancer Research CampaignArticle no. bjoc.1998.0243
Received 14 July 1998Revised 20 October 1998Accepted 5 November 1998
Correspondence to: A Cuschieri
Carcinoma of the stomach remains a major cause of death in mostWestern countries. The only proven effective therapy is surgery,but overall 5-year survival rates remain low after resection. In1981, the Japanese Society for Research in Gastric Cancer(JSRGC) standardized the gastric resections and the extent ofregional lymphadenectomy in accordance with specific rules(updated over the years) based on the location of the tumour andthe respective regional node drainage (Kajitani, 1981). Largeretrospective series from Japan of radical gastrectomy with level-2extended lymphadenectomy (D2 resections) have shown impres-sive 5-year survival rates, certainly much higher than experiencedin the West (Mine et al, 1970; Miwa, 1979; Maruyama et al, 1987;Nakajima and Nishi, 1989). Some non-Japanese centres have alsoreported favourably on D2 resections (Smith et al, 1991; Jaehne etal, 1992; Siewert et al, 1993; Sue-Ling et al, 1993; Mendes et al,1994). However, the benefit of D2 over conventional D1 resections(where only the perigastric nodes within 3.0 cm of the primary areremoved) had not been tested prospectively until the launch of theMedical Research Council (MRC) Gastric Cancer Surgical Trial(ST01) in 1986. This was a randomized comparison of D1 versusD2 resections for potentially curable advanced gastric cancer. At
the time the study was formulated, the Japanese rules dictated thatpancreatico-splenectomy was an integral part of D2 resection forall tumours except antral cancers. For this reason en-bloc removalof these two organs with the stomach was specified by the MRCST01 trial protocol for middle and upper third tumours in the D2arm. In this paper, we report on the long-term outcome of thesetwo surgical treatment arms. Preliminary results of ST01(Cuschieri et al, 1996), and a similar Dutch trial (Bonenkamp et al,1995), have shown that splenectomy and distal hemi-pancreatec-tomy are attended by a significant increase in post-operativemorbidity and mortality. The influence of removal of these organson long-term survival is addressed in this analysis. This is impor-tant as distal hemi-pancreatectomy is no longer considered an inte-gral part of D2 resections by Japanese surgeons, and some Westerncentres are practising spleen- and pancreas-preserving D2 resec-tions with apparent good results (Sue-Ling et al, 1993; Griffith,1995), despite the reported splenic hilar lymph nodes involvementin 15–27% of gastric cancers (Fass and Schumpelick, 1989;Mendes et al, 1994; Mendes et al, 1995; Tsuburaya et al, 1995).
PATIENTS AND METHODS
The organization and preliminary results of the MRC ST01 trial aresummarized briefly since they have been reported previously(Cuschieri et al, 1996). Patients enrolled in MRC ST01 were tohave histologically proven, and potentially curable, gastric carci-noma. Patients were excluded if they were young (< 20 years), had
Patient survival after D1 and D2 resections for gastriccancer: long-term results of the MRC randomizedsurgical trial
A Cuschieri1, S Weeden2, J Fielding3, J Bancewicz4, J Craven5, V Joypaul1, M Sydes2 and P Fayers2, for the SurgicalCo-operative Group1University Department of Surgery, Ninewells Hospital and Medical School, Dundee DD1 9SY, UK; 2Cancer Division MRC Clinical Trials Unit, Cambridge, UK;3Queen Elizabeth Hospital, Birmingham, UK; 4University Department of Surgery, Hope Hospital, Salford, UK; 5Kingstown General Hospital, St Vincents, Jamaica
Summary Controversy still exists on the optimal surgical resection for potentially curable gastric cancer. Much better long-term survival hasbeen reported in retrospective/non-randomized studies with D2 resections that involve a radical extended regional lymphadenectomy thanwith the standard D1 resections. In this paper we report the long-term survival of patients entered into a randomized study, with follow-up todeath or 3 years in 96% of patients and a median follow-up of 6.5 years. In this prospective trial D1 resection (removal of regional perigastricnodes) was compared with D2 resection (extended lymphadenectomy to include level 1 and 2 regional nodes). Central randomization followeda staging laparotomy.
Out of 737 patients with histologically proven gastric adenocarcinoma registered, 337 patients were ineligible by staging laparotomybecause of advanced disease and 400 were randomized. The 5-year survival rates were 35% for D1 resection and 33% for D2 resection(difference –2%, 95% CI = –12%–8%). There was no difference in the overall 5-year survival between the two arms (HR = 1.10, 95% CI0.87–1.39, where HR > 1 implies a survival benefit to D1 surgery). Survival based on death from gastric cancer as the event was similar in theD1 and D2 groups (HR = 1.05, 95% CI 0.79–1.39) as was recurrence-free survival (HR = 1.03, 95% CI 0.82–1.29). In a multivariate analysis,clinical stages II and III, old age, male sex and removal of spleen and pancreas were independently associated with poor survival. Thesefindings indicate that the classical Japanese D2 resection offers no survival advantage over D1 surgery. However, the possibility that D2resection without pancreatico-splenectomy may be better than standard D1 resection cannot be dismissed by the results of this trial.
Keywords: gastric cancer; D1 resection; D2 resection; long-term survival
1522
British Journal of Cancer (1999) 79(9/10), 1522–1530© 1999 Cancer Research CampaignArticle no. bjoc.1998.0243
Received 14 July 1998Revised 20 October 1998Accepted 5 November 1998
Correspondence to: A Cuschieri
N Morbidité Mortalité
D1 200 28% 7%
D2 200 46% 13%
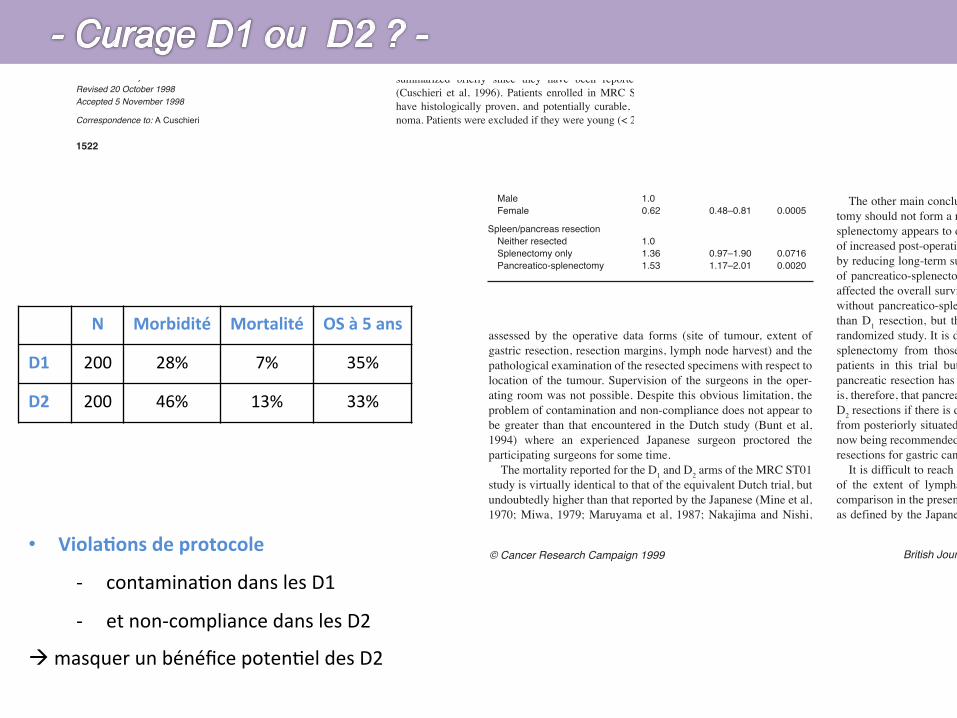
Carcinoma of the stomach remains a major cause of death in mostWestern countries. The only proven effective therapy is surgery,but overall 5-year survival rates remain low after resection. In1981, the Japanese Society for Research in Gastric Cancer(JSRGC) standardized the gastric resections and the extent ofregional lymphadenectomy in accordance with specific rules(updated over the years) based on the location of the tumour andthe respective regional node drainage (Kajitani, 1981). Largeretrospective series from Japan of radical gastrectomy with level-2extended lymphadenectomy (D2 resections) have shown impres-sive 5-year survival rates, certainly much higher than experiencedin the West (Mine et al, 1970; Miwa, 1979; Maruyama et al, 1987;Nakajima and Nishi, 1989). Some non-Japanese centres have alsoreported favourably on D2 resections (Smith et al, 1991; Jaehne etal, 1992; Siewert et al, 1993; Sue-Ling et al, 1993; Mendes et al,1994). However, the benefit of D2 over conventional D1 resections(where only the perigastric nodes within 3.0 cm of the primary areremoved) had not been tested prospectively until the launch of theMedical Research Council (MRC) Gastric Cancer Surgical Trial(ST01) in 1986. This was a randomized comparison of D1 versusD2 resections for potentially curable advanced gastric cancer. At
the time the study was formulated, the Japanese rules dictated thatpancreatico-splenectomy was an integral part of D2 resection forall tumours except antral cancers. For this reason en-bloc removalof these two organs with the stomach was specified by the MRCST01 trial protocol for middle and upper third tumours in the D2arm. In this paper, we report on the long-term outcome of thesetwo surgical treatment arms. Preliminary results of ST01(Cuschieri et al, 1996), and a similar Dutch trial (Bonenkamp et al,1995), have shown that splenectomy and distal hemi-pancreatec-tomy are attended by a significant increase in post-operativemorbidity and mortality. The influence of removal of these organson long-term survival is addressed in this analysis. This is impor-tant as distal hemi-pancreatectomy is no longer considered an inte-gral part of D2 resections by Japanese surgeons, and some Westerncentres are practising spleen- and pancreas-preserving D2 resec-tions with apparent good results (Sue-Ling et al, 1993; Griffith,1995), despite the reported splenic hilar lymph nodes involvementin 15–27% of gastric cancers (Fass and Schumpelick, 1989;Mendes et al, 1994; Mendes et al, 1995; Tsuburaya et al, 1995).
PATIENTS AND METHODS
The organization and preliminary results of the MRC ST01 trial aresummarized briefly since they have been reported previously(Cuschieri et al, 1996). Patients enrolled in MRC ST01 were tohave histologically proven, and potentially curable, gastric carci-noma. Patients were excluded if they were young (< 20 years), had
Patient survival after D1 and D2 resections for gastriccancer: long-term results of the MRC randomizedsurgical trial
A Cuschieri1, S Weeden2, J Fielding3, J Bancewicz4, J Craven5, V Joypaul1, M Sydes2 and P Fayers2, for the SurgicalCo-operative Group1University Department of Surgery, Ninewells Hospital and Medical School, Dundee DD1 9SY, UK; 2Cancer Division MRC Clinical Trials Unit, Cambridge, UK;3Queen Elizabeth Hospital, Birmingham, UK; 4University Department of Surgery, Hope Hospital, Salford, UK; 5Kingstown General Hospital, St Vincents, Jamaica
Summary Controversy still exists on the optimal surgical resection for potentially curable gastric cancer. Much better long-term survival hasbeen reported in retrospective/non-randomized studies with D2 resections that involve a radical extended regional lymphadenectomy thanwith the standard D1 resections. In this paper we report the long-term survival of patients entered into a randomized study, with follow-up todeath or 3 years in 96% of patients and a median follow-up of 6.5 years. In this prospective trial D1 resection (removal of regional perigastricnodes) was compared with D2 resection (extended lymphadenectomy to include level 1 and 2 regional nodes). Central randomization followeda staging laparotomy.
Out of 737 patients with histologically proven gastric adenocarcinoma registered, 337 patients were ineligible by staging laparotomybecause of advanced disease and 400 were randomized. The 5-year survival rates were 35% for D1 resection and 33% for D2 resection(difference –2%, 95% CI = –12%–8%). There was no difference in the overall 5-year survival between the two arms (HR = 1.10, 95% CI0.87–1.39, where HR > 1 implies a survival benefit to D1 surgery). Survival based on death from gastric cancer as the event was similar in theD1 and D2 groups (HR = 1.05, 95% CI 0.79–1.39) as was recurrence-free survival (HR = 1.03, 95% CI 0.82–1.29). In a multivariate analysis,clinical stages II and III, old age, male sex and removal of spleen and pancreas were independently associated with poor survival. Thesefindings indicate that the classical Japanese D2 resection offers no survival advantage over D1 surgery. However, the possibility that D2resection without pancreatico-splenectomy may be better than standard D1 resection cannot be dismissed by the results of this trial.
Keywords: gastric cancer; D1 resection; D2 resection; long-term survival
1522
British Journal of Cancer (1999) 79(9/10), 1522–1530© 1999 Cancer Research CampaignArticle no. bjoc.1998.0243
Received 14 July 1998Revised 20 October 1998Accepted 5 November 1998
Correspondence to: A Cuschieri
Carcinoma of the stomach remains a major cause of death in mostWestern countries. The only proven effective therapy is surgery,but overall 5-year survival rates remain low after resection. In1981, the Japanese Society for Research in Gastric Cancer(JSRGC) standardized the gastric resections and the extent ofregional lymphadenectomy in accordance with specific rules(updated over the years) based on the location of the tumour andthe respective regional node drainage (Kajitani, 1981). Largeretrospective series from Japan of radical gastrectomy with level-2extended lymphadenectomy (D2 resections) have shown impres-sive 5-year survival rates, certainly much higher than experiencedin the West (Mine et al, 1970; Miwa, 1979; Maruyama et al, 1987;Nakajima and Nishi, 1989). Some non-Japanese centres have alsoreported favourably on D2 resections (Smith et al, 1991; Jaehne etal, 1992; Siewert et al, 1993; Sue-Ling et al, 1993; Mendes et al,1994). However, the benefit of D2 over conventional D1 resections(where only the perigastric nodes within 3.0 cm of the primary areremoved) had not been tested prospectively until the launch of theMedical Research Council (MRC) Gastric Cancer Surgical Trial(ST01) in 1986. This was a randomized comparison of D1 versusD2 resections for potentially curable advanced gastric cancer. At
the time the study was formulated, the Japanese rules dictated thatpancreatico-splenectomy was an integral part of D2 resection forall tumours except antral cancers. For this reason en-bloc removalof these two organs with the stomach was specified by the MRCST01 trial protocol for middle and upper third tumours in the D2arm. In this paper, we report on the long-term outcome of thesetwo surgical treatment arms. Preliminary results of ST01(Cuschieri et al, 1996), and a similar Dutch trial (Bonenkamp et al,1995), have shown that splenectomy and distal hemi-pancreatec-tomy are attended by a significant increase in post-operativemorbidity and mortality. The influence of removal of these organson long-term survival is addressed in this analysis. This is impor-tant as distal hemi-pancreatectomy is no longer considered an inte-gral part of D2 resections by Japanese surgeons, and some Westerncentres are practising spleen- and pancreas-preserving D2 resec-tions with apparent good results (Sue-Ling et al, 1993; Griffith,1995), despite the reported splenic hilar lymph nodes involvementin 15–27% of gastric cancers (Fass and Schumpelick, 1989;Mendes et al, 1994; Mendes et al, 1995; Tsuburaya et al, 1995).
PATIENTS AND METHODS
The organization and preliminary results of the MRC ST01 trial aresummarized briefly since they have been reported previously(Cuschieri et al, 1996). Patients enrolled in MRC ST01 were tohave histologically proven, and potentially curable, gastric carci-noma. Patients were excluded if they were young (< 20 years), had
Patient survival after D1 and D2 resections for gastriccancer: long-term results of the MRC randomizedsurgical trial
A Cuschieri1, S Weeden2, J Fielding3, J Bancewicz4, J Craven5, V Joypaul1, M Sydes2 and P Fayers2, for the SurgicalCo-operative Group1University Department of Surgery, Ninewells Hospital and Medical School, Dundee DD1 9SY, UK; 2Cancer Division MRC Clinical Trials Unit, Cambridge, UK;3Queen Elizabeth Hospital, Birmingham, UK; 4University Department of Surgery, Hope Hospital, Salford, UK; 5Kingstown General Hospital, St Vincents, Jamaica
Summary Controversy still exists on the optimal surgical resection for potentially curable gastric cancer. Much better long-term survival hasbeen reported in retrospective/non-randomized studies with D2 resections that involve a radical extended regional lymphadenectomy thanwith the standard D1 resections. In this paper we report the long-term survival of patients entered into a randomized study, with follow-up todeath or 3 years in 96% of patients and a median follow-up of 6.5 years. In this prospective trial D1 resection (removal of regional perigastricnodes) was compared with D2 resection (extended lymphadenectomy to include level 1 and 2 regional nodes). Central randomization followeda staging laparotomy.
Out of 737 patients with histologically proven gastric adenocarcinoma registered, 337 patients were ineligible by staging laparotomybecause of advanced disease and 400 were randomized. The 5-year survival rates were 35% for D1 resection and 33% for D2 resection(difference –2%, 95% CI = –12%–8%). There was no difference in the overall 5-year survival between the two arms (HR = 1.10, 95% CI0.87–1.39, where HR > 1 implies a survival benefit to D1 surgery). Survival based on death from gastric cancer as the event was similar in theD1 and D2 groups (HR = 1.05, 95% CI 0.79–1.39) as was recurrence-free survival (HR = 1.03, 95% CI 0.82–1.29). In a multivariate analysis,clinical stages II and III, old age, male sex and removal of spleen and pancreas were independently associated with poor survival. Thesefindings indicate that the classical Japanese D2 resection offers no survival advantage over D1 surgery. However, the possibility that D2resection without pancreatico-splenectomy may be better than standard D1 resection cannot be dismissed by the results of this trial.
Keywords: gastric cancer; D1 resection; D2 resection; long-term survival
1522
British Journal of Cancer (1999) 79(9/10), 1522–1530© 1999 Cancer Research CampaignArticle no. bjoc.1998.0243
Received 14 July 1998Revised 20 October 1998Accepted 5 November 1998
Correspondence to: A Cuschieri
D1 and D2 resections for gastric cancer 1529
British Journal of Cancer (1999) 79(9/10), 1522–1530© Cancer Research Campaign 1999
assessed by the operative data forms (site of tumour, extent ofgastric resection, resection margins, lymph node harvest) and thepathological examination of the resected specimens with respect tolocation of the tumour. Supervision of the surgeons in the oper-ating room was not possible. Despite this obvious limitation, theproblem of contamination and non-compliance does not appear tobe greater than that encountered in the Dutch study (Bunt et al,1994) where an experienced Japanese surgeon proctored theparticipating surgeons for some time.
The mortality reported for the D1 and D2 arms of the MRC ST01study is virtually identical to that of the equivalent Dutch trial, butundoubtedly higher than that reported by the Japanese (Mine et al,1970; Miwa, 1979; Maruyama et al, 1987; Nakajima and Nishi,
1989) and some Western centres (Smith et al, 1991; Jaehne et al,1992; Siewert et al, 1993; Sue-Ling et al, 1993; Mendes et al,1994). Whilst factors such as experience born of sustained case-load, surgical skill, quality of post-operative care and case selec-tion are important, it is not possible to make valid comparisons onmortality between published series without data on pre-operativerisk stratification of the patients. Subset analysis of the surgeons’results in the ST01 study showed no effect of caseload (number ofpatients entered) on post-operative mortality.
The other main conclusion reached is that pancreatico-splenec-tomy should not form a routine part of D2 resections. Pancreatico-splenectomy appears to disadvantage these patients, both in termsof increased post-operative morbidity and mortality and, probably,by reducing long-term survival. Undoubtedly, the high proportionof pancreatico-splenectomies in the D2 arm must have adverselyaffected the overall survival rate of D2 patients. Hence D2 surgerywithout pancreatico-splenectomy may carry better survival ratesthan D1 resection, but this inference must be tested by a furtherrandomized study. It is difficult to untangle the adverse effects ofsplenectomy from those of pancreatectomy on the survival ofpatients in this trial but the multivariate analysis suggests thatpancreatic resection has the stronger effect. The recommendationis, therefore, that pancreatic resection should only be performed inD2 resections if there is direct extension of disease to the pancreasfrom posteriorly situated tumours. Preservation of the pancreas isnow being recommended and practised by Japanese surgeons in D2resections for gastric cancer (Otsuji et al, 1997).
It is difficult to reach any definite conclusions on the influenceof the extent of lymphadenectomy on long-term survival. Thecomparison in the present trial between radical lymphadenectomy,as defined by the Japanese rules, and those with nodal harvest of
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.00 1 2 3 4 5 6 7
Years
Surv
ival
Patients at risk138 62 69131
(32)(26)(15)(53)
106 36 54 78
(25)(5)
(10)(24)
77314354
(10)(5)(5)
(14)
63243640
(11)(2)(4)(2)
48183035
(7)(1)(2)(3)
34142529
(2)(1)(1)(3)
26 91422
(3)(0)(2)(1)
18 9 917
Events
Events954242
102
Total1386269
131
D1, not removedD1, removedD2, not removedD2, removed
D1, not removedD1, removedD2, not removedD2, removed
Figure 5 Survival by treatment with spleen and distal pancreas removed or not removed
Table 5 Hazards ratios and 95% CIs for the fitted multivariate model
Variable Hazard ratio 95% CI P-value
Clinical stageI 1.0II 2.19 1.54–3.12 < 0.0001III 3.87 2.83–5.28 < 0.0001
Age 1.03 1.01–1.04 0.0001
SexMale 1.0Female 0.62 0.48–0.81 0.0005
Spleen/pancreas resectionNeither resected 1.0Splenectomy only 1.36 0.97–1.90 0.0716Pancreatico-splenectomy 1.53 1.17–2.01 0.0020
N Morbidité Mortalité OS à 5 ans
D1 200 28% 7% 35%
D2 200 46% 13% 33%
• ViolaHons de protocole
-‐ contamina+on dans les D1
-‐ et non-‐compliance dans les D2
à masquer un bénéfice poten+el des D2
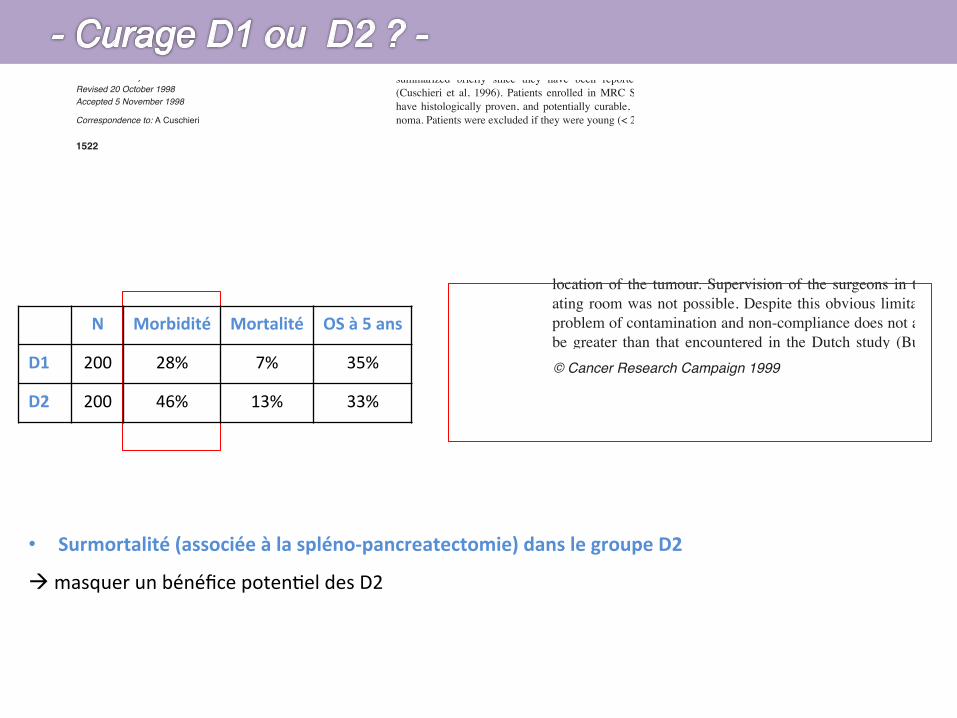
Carcinoma of the stomach remains a major cause of death in mostWestern countries. The only proven effective therapy is surgery,but overall 5-year survival rates remain low after resection. In1981, the Japanese Society for Research in Gastric Cancer(JSRGC) standardized the gastric resections and the extent ofregional lymphadenectomy in accordance with specific rules(updated over the years) based on the location of the tumour andthe respective regional node drainage (Kajitani, 1981). Largeretrospective series from Japan of radical gastrectomy with level-2extended lymphadenectomy (D2 resections) have shown impres-sive 5-year survival rates, certainly much higher than experiencedin the West (Mine et al, 1970; Miwa, 1979; Maruyama et al, 1987;Nakajima and Nishi, 1989). Some non-Japanese centres have alsoreported favourably on D2 resections (Smith et al, 1991; Jaehne etal, 1992; Siewert et al, 1993; Sue-Ling et al, 1993; Mendes et al,1994). However, the benefit of D2 over conventional D1 resections(where only the perigastric nodes within 3.0 cm of the primary areremoved) had not been tested prospectively until the launch of theMedical Research Council (MRC) Gastric Cancer Surgical Trial(ST01) in 1986. This was a randomized comparison of D1 versusD2 resections for potentially curable advanced gastric cancer. At
the time the study was formulated, the Japanese rules dictated thatpancreatico-splenectomy was an integral part of D2 resection forall tumours except antral cancers. For this reason en-bloc removalof these two organs with the stomach was specified by the MRCST01 trial protocol for middle and upper third tumours in the D2arm. In this paper, we report on the long-term outcome of thesetwo surgical treatment arms. Preliminary results of ST01(Cuschieri et al, 1996), and a similar Dutch trial (Bonenkamp et al,1995), have shown that splenectomy and distal hemi-pancreatec-tomy are attended by a significant increase in post-operativemorbidity and mortality. The influence of removal of these organson long-term survival is addressed in this analysis. This is impor-tant as distal hemi-pancreatectomy is no longer considered an inte-gral part of D2 resections by Japanese surgeons, and some Westerncentres are practising spleen- and pancreas-preserving D2 resec-tions with apparent good results (Sue-Ling et al, 1993; Griffith,1995), despite the reported splenic hilar lymph nodes involvementin 15–27% of gastric cancers (Fass and Schumpelick, 1989;Mendes et al, 1994; Mendes et al, 1995; Tsuburaya et al, 1995).
PATIENTS AND METHODS
The organization and preliminary results of the MRC ST01 trial aresummarized briefly since they have been reported previously(Cuschieri et al, 1996). Patients enrolled in MRC ST01 were tohave histologically proven, and potentially curable, gastric carci-noma. Patients were excluded if they were young (< 20 years), had
Patient survival after D1 and D2 resections for gastriccancer: long-term results of the MRC randomizedsurgical trial
A Cuschieri1, S Weeden2, J Fielding3, J Bancewicz4, J Craven5, V Joypaul1, M Sydes2 and P Fayers2, for the SurgicalCo-operative Group1University Department of Surgery, Ninewells Hospital and Medical School, Dundee DD1 9SY, UK; 2Cancer Division MRC Clinical Trials Unit, Cambridge, UK;3Queen Elizabeth Hospital, Birmingham, UK; 4University Department of Surgery, Hope Hospital, Salford, UK; 5Kingstown General Hospital, St Vincents, Jamaica
Summary Controversy still exists on the optimal surgical resection for potentially curable gastric cancer. Much better long-term survival hasbeen reported in retrospective/non-randomized studies with D2 resections that involve a radical extended regional lymphadenectomy thanwith the standard D1 resections. In this paper we report the long-term survival of patients entered into a randomized study, with follow-up todeath or 3 years in 96% of patients and a median follow-up of 6.5 years. In this prospective trial D1 resection (removal of regional perigastricnodes) was compared with D2 resection (extended lymphadenectomy to include level 1 and 2 regional nodes). Central randomization followeda staging laparotomy.
Out of 737 patients with histologically proven gastric adenocarcinoma registered, 337 patients were ineligible by staging laparotomybecause of advanced disease and 400 were randomized. The 5-year survival rates were 35% for D1 resection and 33% for D2 resection(difference –2%, 95% CI = –12%–8%). There was no difference in the overall 5-year survival between the two arms (HR = 1.10, 95% CI0.87–1.39, where HR > 1 implies a survival benefit to D1 surgery). Survival based on death from gastric cancer as the event was similar in theD1 and D2 groups (HR = 1.05, 95% CI 0.79–1.39) as was recurrence-free survival (HR = 1.03, 95% CI 0.82–1.29). In a multivariate analysis,clinical stages II and III, old age, male sex and removal of spleen and pancreas were independently associated with poor survival. Thesefindings indicate that the classical Japanese D2 resection offers no survival advantage over D1 surgery. However, the possibility that D2resection without pancreatico-splenectomy may be better than standard D1 resection cannot be dismissed by the results of this trial.
Keywords: gastric cancer; D1 resection; D2 resection; long-term survival
1522
British Journal of Cancer (1999) 79(9/10), 1522–1530© 1999 Cancer Research CampaignArticle no. bjoc.1998.0243
Received 14 July 1998Revised 20 October 1998Accepted 5 November 1998
Correspondence to: A Cuschieri
Carcinoma of the stomach remains a major cause of death in mostWestern countries. The only proven effective therapy is surgery,but overall 5-year survival rates remain low after resection. In1981, the Japanese Society for Research in Gastric Cancer(JSRGC) standardized the gastric resections and the extent ofregional lymphadenectomy in accordance with specific rules(updated over the years) based on the location of the tumour andthe respective regional node drainage (Kajitani, 1981). Largeretrospective series from Japan of radical gastrectomy with level-2extended lymphadenectomy (D2 resections) have shown impres-sive 5-year survival rates, certainly much higher than experiencedin the West (Mine et al, 1970; Miwa, 1979; Maruyama et al, 1987;Nakajima and Nishi, 1989). Some non-Japanese centres have alsoreported favourably on D2 resections (Smith et al, 1991; Jaehne etal, 1992; Siewert et al, 1993; Sue-Ling et al, 1993; Mendes et al,1994). However, the benefit of D2 over conventional D1 resections(where only the perigastric nodes within 3.0 cm of the primary areremoved) had not been tested prospectively until the launch of theMedical Research Council (MRC) Gastric Cancer Surgical Trial(ST01) in 1986. This was a randomized comparison of D1 versusD2 resections for potentially curable advanced gastric cancer. At
the time the study was formulated, the Japanese rules dictated thatpancreatico-splenectomy was an integral part of D2 resection forall tumours except antral cancers. For this reason en-bloc removalof these two organs with the stomach was specified by the MRCST01 trial protocol for middle and upper third tumours in the D2arm. In this paper, we report on the long-term outcome of thesetwo surgical treatment arms. Preliminary results of ST01(Cuschieri et al, 1996), and a similar Dutch trial (Bonenkamp et al,1995), have shown that splenectomy and distal hemi-pancreatec-tomy are attended by a significant increase in post-operativemorbidity and mortality. The influence of removal of these organson long-term survival is addressed in this analysis. This is impor-tant as distal hemi-pancreatectomy is no longer considered an inte-gral part of D2 resections by Japanese surgeons, and some Westerncentres are practising spleen- and pancreas-preserving D2 resec-tions with apparent good results (Sue-Ling et al, 1993; Griffith,1995), despite the reported splenic hilar lymph nodes involvementin 15–27% of gastric cancers (Fass and Schumpelick, 1989;Mendes et al, 1994; Mendes et al, 1995; Tsuburaya et al, 1995).
PATIENTS AND METHODS
The organization and preliminary results of the MRC ST01 trial aresummarized briefly since they have been reported previously(Cuschieri et al, 1996). Patients enrolled in MRC ST01 were tohave histologically proven, and potentially curable, gastric carci-noma. Patients were excluded if they were young (< 20 years), had
Patient survival after D1 and D2 resections for gastriccancer: long-term results of the MRC randomizedsurgical trial
A Cuschieri1, S Weeden2, J Fielding3, J Bancewicz4, J Craven5, V Joypaul1, M Sydes2 and P Fayers2, for the SurgicalCo-operative Group1University Department of Surgery, Ninewells Hospital and Medical School, Dundee DD1 9SY, UK; 2Cancer Division MRC Clinical Trials Unit, Cambridge, UK;3Queen Elizabeth Hospital, Birmingham, UK; 4University Department of Surgery, Hope Hospital, Salford, UK; 5Kingstown General Hospital, St Vincents, Jamaica
Summary Controversy still exists on the optimal surgical resection for potentially curable gastric cancer. Much better long-term survival hasbeen reported in retrospective/non-randomized studies with D2 resections that involve a radical extended regional lymphadenectomy thanwith the standard D1 resections. In this paper we report the long-term survival of patients entered into a randomized study, with follow-up todeath or 3 years in 96% of patients and a median follow-up of 6.5 years. In this prospective trial D1 resection (removal of regional perigastricnodes) was compared with D2 resection (extended lymphadenectomy to include level 1 and 2 regional nodes). Central randomization followeda staging laparotomy.
Out of 737 patients with histologically proven gastric adenocarcinoma registered, 337 patients were ineligible by staging laparotomybecause of advanced disease and 400 were randomized. The 5-year survival rates were 35% for D1 resection and 33% for D2 resection(difference –2%, 95% CI = –12%–8%). There was no difference in the overall 5-year survival between the two arms (HR = 1.10, 95% CI0.87–1.39, where HR > 1 implies a survival benefit to D1 surgery). Survival based on death from gastric cancer as the event was similar in theD1 and D2 groups (HR = 1.05, 95% CI 0.79–1.39) as was recurrence-free survival (HR = 1.03, 95% CI 0.82–1.29). In a multivariate analysis,clinical stages II and III, old age, male sex and removal of spleen and pancreas were independently associated with poor survival. Thesefindings indicate that the classical Japanese D2 resection offers no survival advantage over D1 surgery. However, the possibility that D2resection without pancreatico-splenectomy may be better than standard D1 resection cannot be dismissed by the results of this trial.
Keywords: gastric cancer; D1 resection; D2 resection; long-term survival
1522
British Journal of Cancer (1999) 79(9/10), 1522–1530© 1999 Cancer Research CampaignArticle no. bjoc.1998.0243
Received 14 July 1998Revised 20 October 1998Accepted 5 November 1998
Correspondence to: A Cuschieri
D1 and D2 resections for gastric cancer 1529
British Journal of Cancer (1999) 79(9/10), 1522–1530© Cancer Research Campaign 1999
assessed by the operative data forms (site of tumour, extent ofgastric resection, resection margins, lymph node harvest) and thepathological examination of the resected specimens with respect tolocation of the tumour. Supervision of the surgeons in the oper-ating room was not possible. Despite this obvious limitation, theproblem of contamination and non-compliance does not appear tobe greater than that encountered in the Dutch study (Bunt et al,1994) where an experienced Japanese surgeon proctored theparticipating surgeons for some time.
The mortality reported for the D1 and D2 arms of the MRC ST01study is virtually identical to that of the equivalent Dutch trial, butundoubtedly higher than that reported by the Japanese (Mine et al,1970; Miwa, 1979; Maruyama et al, 1987; Nakajima and Nishi,
1989) and some Western centres (Smith et al, 1991; Jaehne et al,1992; Siewert et al, 1993; Sue-Ling et al, 1993; Mendes et al,1994). Whilst factors such as experience born of sustained case-load, surgical skill, quality of post-operative care and case selec-tion are important, it is not possible to make valid comparisons onmortality between published series without data on pre-operativerisk stratification of the patients. Subset analysis of the surgeons’results in the ST01 study showed no effect of caseload (number ofpatients entered) on post-operative mortality.
The other main conclusion reached is that pancreatico-splenec-tomy should not form a routine part of D2 resections. Pancreatico-splenectomy appears to disadvantage these patients, both in termsof increased post-operative morbidity and mortality and, probably,by reducing long-term survival. Undoubtedly, the high proportionof pancreatico-splenectomies in the D2 arm must have adverselyaffected the overall survival rate of D2 patients. Hence D2 surgerywithout pancreatico-splenectomy may carry better survival ratesthan D1 resection, but this inference must be tested by a furtherrandomized study. It is difficult to untangle the adverse effects ofsplenectomy from those of pancreatectomy on the survival ofpatients in this trial but the multivariate analysis suggests thatpancreatic resection has the stronger effect. The recommendationis, therefore, that pancreatic resection should only be performed inD2 resections if there is direct extension of disease to the pancreasfrom posteriorly situated tumours. Preservation of the pancreas isnow being recommended and practised by Japanese surgeons in D2resections for gastric cancer (Otsuji et al, 1997).
It is difficult to reach any definite conclusions on the influenceof the extent of lymphadenectomy on long-term survival. Thecomparison in the present trial between radical lymphadenectomy,as defined by the Japanese rules, and those with nodal harvest of
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.00 1 2 3 4 5 6 7
Years
Surv
ival
Patients at risk138 62 69131
(32)(26)(15)(53)
106 36 54 78
(25)(5)
(10)(24)
77314354
(10)(5)(5)
(14)
63243640
(11)(2)(4)(2)
48183035
(7)(1)(2)(3)
34142529
(2)(1)(1)(3)
26 91422
(3)(0)(2)(1)
18 9 917
Events
Events954242
102
Total1386269
131
D1, not removedD1, removedD2, not removedD2, removed
D1, not removedD1, removedD2, not removedD2, removed
Figure 5 Survival by treatment with spleen and distal pancreas removed or not removed
Table 5 Hazards ratios and 95% CIs for the fitted multivariate model
Variable Hazard ratio 95% CI P-value
Clinical stageI 1.0II 2.19 1.54–3.12 < 0.0001III 3.87 2.83–5.28 < 0.0001
Age 1.03 1.01–1.04 0.0001
SexMale 1.0Female 0.62 0.48–0.81 0.0005
Spleen/pancreas resectionNeither resected 1.0Splenectomy only 1.36 0.97–1.90 0.0716Pancreatico-splenectomy 1.53 1.17–2.01 0.0020
D1 and D2 resections for gastric cancer 1529
British Journal of Cancer (1999) 79(9/10), 1522–1530© Cancer Research Campaign 1999
assessed by the operative data forms (site of tumour, extent ofgastric resection, resection margins, lymph node harvest) and thepathological examination of the resected specimens with respect tolocation of the tumour. Supervision of the surgeons in the oper-ating room was not possible. Despite this obvious limitation, theproblem of contamination and non-compliance does not appear tobe greater than that encountered in the Dutch study (Bunt et al,1994) where an experienced Japanese surgeon proctored theparticipating surgeons for some time.
The mortality reported for the D1 and D2 arms of the MRC ST01study is virtually identical to that of the equivalent Dutch trial, butundoubtedly higher than that reported by the Japanese (Mine et al,1970; Miwa, 1979; Maruyama et al, 1987; Nakajima and Nishi,
1989) and some Western centres (Smith et al, 1991; Jaehne et al,1992; Siewert et al, 1993; Sue-Ling et al, 1993; Mendes et al,1994). Whilst factors such as experience born of sustained case-load, surgical skill, quality of post-operative care and case selec-tion are important, it is not possible to make valid comparisons onmortality between published series without data on pre-operativerisk stratification of the patients. Subset analysis of the surgeons’results in the ST01 study showed no effect of caseload (number ofpatients entered) on post-operative mortality.
The other main conclusion reached is that pancreatico-splenec-tomy should not form a routine part of D2 resections. Pancreatico-splenectomy appears to disadvantage these patients, both in termsof increased post-operative morbidity and mortality and, probably,by reducing long-term survival. Undoubtedly, the high proportionof pancreatico-splenectomies in the D2 arm must have adverselyaffected the overall survival rate of D2 patients. Hence D2 surgerywithout pancreatico-splenectomy may carry better survival ratesthan D1 resection, but this inference must be tested by a furtherrandomized study. It is difficult to untangle the adverse effects ofsplenectomy from those of pancreatectomy on the survival ofpatients in this trial but the multivariate analysis suggests thatpancreatic resection has the stronger effect. The recommendationis, therefore, that pancreatic resection should only be performed inD2 resections if there is direct extension of disease to the pancreasfrom posteriorly situated tumours. Preservation of the pancreas isnow being recommended and practised by Japanese surgeons in D2resections for gastric cancer (Otsuji et al, 1997).
It is difficult to reach any definite conclusions on the influenceof the extent of lymphadenectomy on long-term survival. Thecomparison in the present trial between radical lymphadenectomy,as defined by the Japanese rules, and those with nodal harvest of
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.00 1 2 3 4 5 6 7
Years
Surv
ival
Patients at risk138 62 69131
(32)(26)(15)(53)
106 36 54 78
(25)(5)
(10)(24)
77314354
(10)(5)(5)
(14)
63243640
(11)(2)(4)(2)
48183035
(7)(1)(2)(3)
34142529
(2)(1)(1)(3)
26 91422
(3)(0)(2)(1)
18 9 917
Events
Events954242
102
Total1386269
131
D1, not removedD1, removedD2, not removedD2, removed
D1, not removedD1, removedD2, not removedD2, removed
Figure 5 Survival by treatment with spleen and distal pancreas removed or not removed
Table 5 Hazards ratios and 95% CIs for the fitted multivariate model
Variable Hazard ratio 95% CI P-value
Clinical stageI 1.0II 2.19 1.54–3.12 < 0.0001III 3.87 2.83–5.28 < 0.0001
Age 1.03 1.01–1.04 0.0001
SexMale 1.0Female 0.62 0.48–0.81 0.0005
Spleen/pancreas resectionNeither resected 1.0Splenectomy only 1.36 0.97–1.90 0.0716Pancreatico-splenectomy 1.53 1.17–2.01 0.0020
• Surmortalité (associée à la spléno-‐pancreatectomie) dans le groupe D2
à masquer un bénéfice poten+el des D2
N Morbidité Mortalité OS à 5 ans
D1 200 28% 7% 35%
D2 200 46% 13% 33%
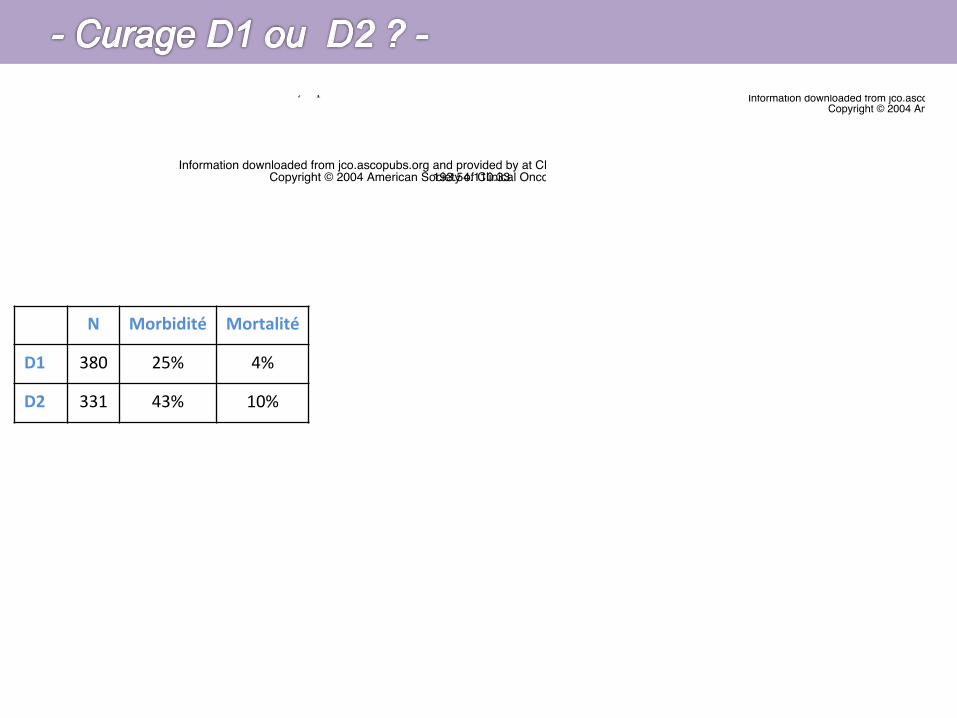
N Morbidité Mortalité
D1 380 25% 4%
D2 331 43% 10%
Extended Lymph Node Dissection for Gastric Cancer:Who May Benefit? Final Results of the RandomizedDutch Gastric Cancer Group TrialH.H. Hartgrink, C.J.H. van de Velde, H. Putter, J.J. Bonenkamp, E. Klein Kranenbarg, I. Songun,K. Welvaart, J.H.J.M. van Krieken, S. Meijer, J.T.M. Plukker, P.J. van Elk, H. Obertop, D.J. Gouma,J.J.B. van Lanschot, C.W. Taat,† P.W. de Graaf, M.F. von Meyenfeldt, H. Tilanus, and M. Sasako
A B S T R A C T
PurposeThe extent of lymph node dissection appropriate for gastric cancer is still under debate. We haveconducted a randomized trial to compare the results of a limited (D1) and extended (D2) lymph nodedissection in terms of morbidity, mortality, long-term survival and cumulative risk of relapse. We havereviewed the results of our trial after follow-up of more than 10 years.
Patients and MethodsBetween August 1989 and June 1993, 1,078 patients with gastric adenocarcinoma were randomlyassigned to undergo a D1 or D2 lymph node dissection. Data were collected prospectively, and patientswere followed for more than 10 years.
ResultsA total of 711 patients (380 in the D1 group and 331 in the D2 group) were treated with curative intent.Morbidity (25% v 43%; P ! .001) and mortality (4% v 10%; P " .004) were significantly higher in theD2 dissection group. After 11 years there is no overall difference in survival (30% v 35%; P " .53). Ofall subgroups analyzed, only patients with N2 disease may benefit of a D2 dissection. The relative riskratio for morbidity and mortality is significantly higher than one for D2 dissections, splenectomy,pancreatectomy, and age older than 70 years.
ConclusionOverall, extended lymph node dissection as defined in this study generated no long-term survivalbenefit. The associated higher postoperative mortality offsets its long-term effect in survival. Forpatients with N2 disease an extended lymph node dissection may offer cure, but it remains difficult toidentify patients who have N2 disease. Morbidity and mortality are greatly influenced by the extent oflymph node dissection, pancreatectomy, splenectomy and age. Extended lymph node dissections maybe of benefit if morbidity and mortality can be avoided.
J Clin Oncol 22:2069-2077. © 2004 by American Society of Clinical Oncology
INTRODUCTION
Gastric cancer is a common malignancy world-wide. Even in a low-incidence country like theNetherlands, it is ranked fifth with respect to in-cidence. Despite declining incidence, mortalityofgastriccancerremainshigh.Surgeryistheonlypossible curative treatment, and results of gas-trectomy have improved throughout the yearswith respect to survival, morbidity, and postop-erative mortality.1,2
It is not clear, however, if extendedlymph node dissection contributes to this
improvement. Despite promising results innonrandomized studies, improved survivalhas never been demonstrated in random-ized trials.3-6 In all these randomized trials,postoperative morbidity and mortality weresignificantly higher in the extended (D2)dissection group. Within the Dutch GastricCancer Trial (DGCT), the number of earlygastric cancers was surprisingly high, and ithas been argued that any beneficial effect ofextended lymph node dissection, whichwould be expected in more advanced dis-ease, might have been attenuated. We have
From the Department of Surgery andthe Department of Medical Statistics,Leiden University Medical Center, Lei-den; Department of Surgery and De-partment of Pathology, University Medi-cal Center St Radboud, Nijmegen;Department of Surgery, University Hos-pital Amsterdam Vrije Universiteit, Am-sterdam; Department of Surgery, Uni-versity Hospital Groningen, Groningen;Department of Surgery, GeertruidenHospital Deventer, Deventer; Depart-ment of Surgery, Academic MedicalCenter Amsterdam, Amsterdam; De-partment of Surgery, Reinier de GraafHospital, Delft; Department of Surgery,University Hospital Maastricht, Maas-tricht; Department of Surgery, ErasmusMedical Center, Rotterdam, the Nether-lands; and the Department of Surgery,National Cancer Center Hospital, Tokyo,Japan.
†Deceased.
Submitted August 5, 2003; acceptedFebruary 18, 2004.
Supported by grants from the DutchHealth Insurance Funds Council and theNetherlands Cancer Foundation.
Authors’ disclosures of potential con-flicts of interest are found at the end ofthis article.
Address reprint requests to H.H.Hartgrink, MD, Department of Surgery,Leiden University Medical Centre, POBox 9600, 2300 RC Leiden, TheNetherlands; e-mail: [email protected].
© 2004 by American Society of ClinicalOncology
0732-183X/04/2211-2069/$20.00
DOI: 10.1200/JCO.2004.08.026
JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T
VOLUME 22 ! NUMBER 11 ! JUNE 1 2004
2069
193.54.110.33Information downloaded from jco.ascopubs.org and provided by at CDMP - APHP on December 18, 2014 from
Copyright © 2004 American Society of Clinical Oncology. All rights reserved.
Extended Lymph Node Dissection for Gastric Cancer:Who May Benefit? Final Results of the RandomizedDutch Gastric Cancer Group TrialH.H. Hartgrink, C.J.H. van de Velde, H. Putter, J.J. Bonenkamp, E. Klein Kranenbarg, I. Songun,K. Welvaart, J.H.J.M. van Krieken, S. Meijer, J.T.M. Plukker, P.J. van Elk, H. Obertop, D.J. Gouma,J.J.B. van Lanschot, C.W. Taat,† P.W. de Graaf, M.F. von Meyenfeldt, H. Tilanus, and M. Sasako
A B S T R A C T
PurposeThe extent of lymph node dissection appropriate for gastric cancer is still under debate. We haveconducted a randomized trial to compare the results of a limited (D1) and extended (D2) lymph nodedissection in terms of morbidity, mortality, long-term survival and cumulative risk of relapse. We havereviewed the results of our trial after follow-up of more than 10 years.
Patients and MethodsBetween August 1989 and June 1993, 1,078 patients with gastric adenocarcinoma were randomlyassigned to undergo a D1 or D2 lymph node dissection. Data were collected prospectively, and patientswere followed for more than 10 years.
ResultsA total of 711 patients (380 in the D1 group and 331 in the D2 group) were treated with curative intent.Morbidity (25% v 43%; P ! .001) and mortality (4% v 10%; P " .004) were significantly higher in theD2 dissection group. After 11 years there is no overall difference in survival (30% v 35%; P " .53). Ofall subgroups analyzed, only patients with N2 disease may benefit of a D2 dissection. The relative riskratio for morbidity and mortality is significantly higher than one for D2 dissections, splenectomy,pancreatectomy, and age older than 70 years.
ConclusionOverall, extended lymph node dissection as defined in this study generated no long-term survivalbenefit. The associated higher postoperative mortality offsets its long-term effect in survival. Forpatients with N2 disease an extended lymph node dissection may offer cure, but it remains difficult toidentify patients who have N2 disease. Morbidity and mortality are greatly influenced by the extent oflymph node dissection, pancreatectomy, splenectomy and age. Extended lymph node dissections maybe of benefit if morbidity and mortality can be avoided.
J Clin Oncol 22:2069-2077. © 2004 by American Society of Clinical Oncology
INTRODUCTION
Gastric cancer is a common malignancy world-wide. Even in a low-incidence country like theNetherlands, it is ranked fifth with respect to in-cidence. Despite declining incidence, mortalityofgastriccancerremainshigh.Surgeryistheonlypossible curative treatment, and results of gas-trectomy have improved throughout the yearswith respect to survival, morbidity, and postop-erative mortality.1,2
It is not clear, however, if extendedlymph node dissection contributes to this
improvement. Despite promising results innonrandomized studies, improved survivalhas never been demonstrated in random-ized trials.3-6 In all these randomized trials,postoperative morbidity and mortality weresignificantly higher in the extended (D2)dissection group. Within the Dutch GastricCancer Trial (DGCT), the number of earlygastric cancers was surprisingly high, and ithas been argued that any beneficial effect ofextended lymph node dissection, whichwould be expected in more advanced dis-ease, might have been attenuated. We have
From the Department of Surgery andthe Department of Medical Statistics,Leiden University Medical Center, Lei-den; Department of Surgery and De-partment of Pathology, University Medi-cal Center St Radboud, Nijmegen;Department of Surgery, University Hos-pital Amsterdam Vrije Universiteit, Am-sterdam; Department of Surgery, Uni-versity Hospital Groningen, Groningen;Department of Surgery, GeertruidenHospital Deventer, Deventer; Depart-ment of Surgery, Academic MedicalCenter Amsterdam, Amsterdam; De-partment of Surgery, Reinier de GraafHospital, Delft; Department of Surgery,University Hospital Maastricht, Maas-tricht; Department of Surgery, ErasmusMedical Center, Rotterdam, the Nether-lands; and the Department of Surgery,National Cancer Center Hospital, Tokyo,Japan.
†Deceased.
Submitted August 5, 2003; acceptedFebruary 18, 2004.
Supported by grants from the DutchHealth Insurance Funds Council and theNetherlands Cancer Foundation.
Authors’ disclosures of potential con-flicts of interest are found at the end ofthis article.
Address reprint requests to H.H.Hartgrink, MD, Department of Surgery,Leiden University Medical Centre, POBox 9600, 2300 RC Leiden, TheNetherlands; e-mail: [email protected].
© 2004 by American Society of ClinicalOncology
0732-183X/04/2211-2069/$20.00
DOI: 10.1200/JCO.2004.08.026
JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T
VOLUME 22 ! NUMBER 11 ! JUNE 1 2004
2069
193.54.110.33Information downloaded from jco.ascopubs.org and provided by at CDMP - APHP on December 18, 2014 from
Copyright © 2004 American Society of Clinical Oncology. All rights reserved.
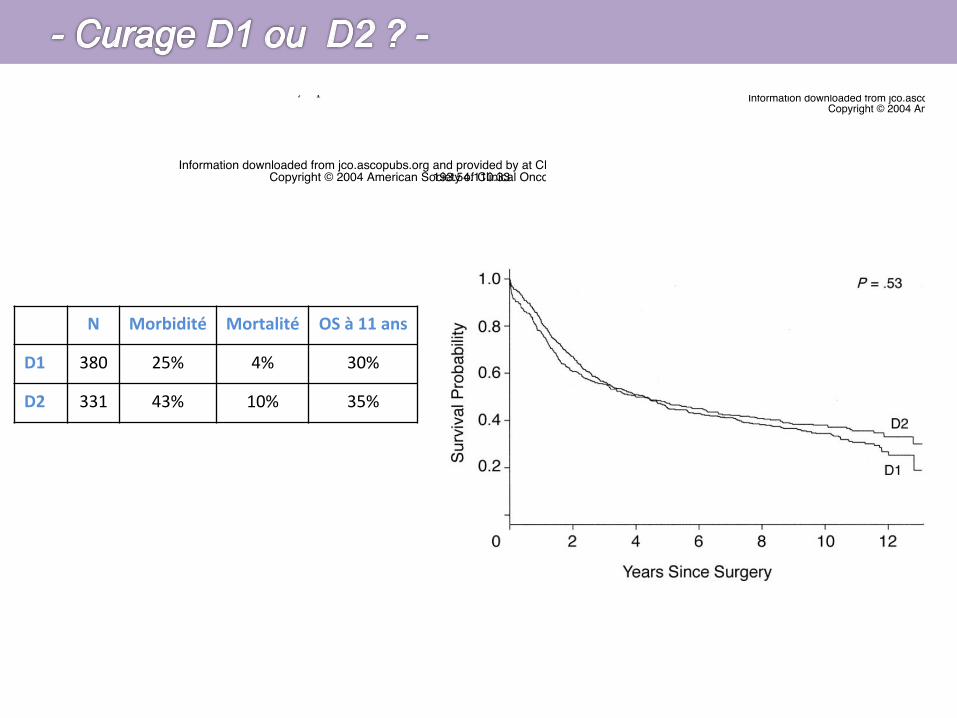
N Morbidité Mortalité OS à 11 ans
D1 380 25% 4% 30%
D2 331 43% 10% 35%
Extended Lymph Node Dissection for Gastric Cancer:Who May Benefit? Final Results of the RandomizedDutch Gastric Cancer Group TrialH.H. Hartgrink, C.J.H. van de Velde, H. Putter, J.J. Bonenkamp, E. Klein Kranenbarg, I. Songun,K. Welvaart, J.H.J.M. van Krieken, S. Meijer, J.T.M. Plukker, P.J. van Elk, H. Obertop, D.J. Gouma,J.J.B. van Lanschot, C.W. Taat,† P.W. de Graaf, M.F. von Meyenfeldt, H. Tilanus, and M. Sasako
A B S T R A C T
PurposeThe extent of lymph node dissection appropriate for gastric cancer is still under debate. We haveconducted a randomized trial to compare the results of a limited (D1) and extended (D2) lymph nodedissection in terms of morbidity, mortality, long-term survival and cumulative risk of relapse. We havereviewed the results of our trial after follow-up of more than 10 years.
Patients and MethodsBetween August 1989 and June 1993, 1,078 patients with gastric adenocarcinoma were randomlyassigned to undergo a D1 or D2 lymph node dissection. Data were collected prospectively, and patientswere followed for more than 10 years.
ResultsA total of 711 patients (380 in the D1 group and 331 in the D2 group) were treated with curative intent.Morbidity (25% v 43%; P ! .001) and mortality (4% v 10%; P " .004) were significantly higher in theD2 dissection group. After 11 years there is no overall difference in survival (30% v 35%; P " .53). Ofall subgroups analyzed, only patients with N2 disease may benefit of a D2 dissection. The relative riskratio for morbidity and mortality is significantly higher than one for D2 dissections, splenectomy,pancreatectomy, and age older than 70 years.
ConclusionOverall, extended lymph node dissection as defined in this study generated no long-term survivalbenefit. The associated higher postoperative mortality offsets its long-term effect in survival. Forpatients with N2 disease an extended lymph node dissection may offer cure, but it remains difficult toidentify patients who have N2 disease. Morbidity and mortality are greatly influenced by the extent oflymph node dissection, pancreatectomy, splenectomy and age. Extended lymph node dissections maybe of benefit if morbidity and mortality can be avoided.
J Clin Oncol 22:2069-2077. © 2004 by American Society of Clinical Oncology
INTRODUCTION
Gastric cancer is a common malignancy world-wide. Even in a low-incidence country like theNetherlands, it is ranked fifth with respect to in-cidence. Despite declining incidence, mortalityofgastriccancerremainshigh.Surgeryistheonlypossible curative treatment, and results of gas-trectomy have improved throughout the yearswith respect to survival, morbidity, and postop-erative mortality.1,2
It is not clear, however, if extendedlymph node dissection contributes to this
improvement. Despite promising results innonrandomized studies, improved survivalhas never been demonstrated in random-ized trials.3-6 In all these randomized trials,postoperative morbidity and mortality weresignificantly higher in the extended (D2)dissection group. Within the Dutch GastricCancer Trial (DGCT), the number of earlygastric cancers was surprisingly high, and ithas been argued that any beneficial effect ofextended lymph node dissection, whichwould be expected in more advanced dis-ease, might have been attenuated. We have
From the Department of Surgery andthe Department of Medical Statistics,Leiden University Medical Center, Lei-den; Department of Surgery and De-partment of Pathology, University Medi-cal Center St Radboud, Nijmegen;Department of Surgery, University Hos-pital Amsterdam Vrije Universiteit, Am-sterdam; Department of Surgery, Uni-versity Hospital Groningen, Groningen;Department of Surgery, GeertruidenHospital Deventer, Deventer; Depart-ment of Surgery, Academic MedicalCenter Amsterdam, Amsterdam; De-partment of Surgery, Reinier de GraafHospital, Delft; Department of Surgery,University Hospital Maastricht, Maas-tricht; Department of Surgery, ErasmusMedical Center, Rotterdam, the Nether-lands; and the Department of Surgery,National Cancer Center Hospital, Tokyo,Japan.
†Deceased.
Submitted August 5, 2003; acceptedFebruary 18, 2004.
Supported by grants from the DutchHealth Insurance Funds Council and theNetherlands Cancer Foundation.
Authors’ disclosures of potential con-flicts of interest are found at the end ofthis article.
Address reprint requests to H.H.Hartgrink, MD, Department of Surgery,Leiden University Medical Centre, POBox 9600, 2300 RC Leiden, TheNetherlands; e-mail: [email protected].
© 2004 by American Society of ClinicalOncology
0732-183X/04/2211-2069/$20.00
DOI: 10.1200/JCO.2004.08.026
JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T
VOLUME 22 ! NUMBER 11 ! JUNE 1 2004
2069
193.54.110.33Information downloaded from jco.ascopubs.org and provided by at CDMP - APHP on December 18, 2014 from
Copyright © 2004 American Society of Clinical Oncology. All rights reserved.
Extended Lymph Node Dissection for Gastric Cancer:Who May Benefit? Final Results of the RandomizedDutch Gastric Cancer Group TrialH.H. Hartgrink, C.J.H. van de Velde, H. Putter, J.J. Bonenkamp, E. Klein Kranenbarg, I. Songun,K. Welvaart, J.H.J.M. van Krieken, S. Meijer, J.T.M. Plukker, P.J. van Elk, H. Obertop, D.J. Gouma,J.J.B. van Lanschot, C.W. Taat,† P.W. de Graaf, M.F. von Meyenfeldt, H. Tilanus, and M. Sasako
A B S T R A C T
PurposeThe extent of lymph node dissection appropriate for gastric cancer is still under debate. We haveconducted a randomized trial to compare the results of a limited (D1) and extended (D2) lymph nodedissection in terms of morbidity, mortality, long-term survival and cumulative risk of relapse. We havereviewed the results of our trial after follow-up of more than 10 years.
Patients and MethodsBetween August 1989 and June 1993, 1,078 patients with gastric adenocarcinoma were randomlyassigned to undergo a D1 or D2 lymph node dissection. Data were collected prospectively, and patientswere followed for more than 10 years.
ResultsA total of 711 patients (380 in the D1 group and 331 in the D2 group) were treated with curative intent.Morbidity (25% v 43%; P ! .001) and mortality (4% v 10%; P " .004) were significantly higher in theD2 dissection group. After 11 years there is no overall difference in survival (30% v 35%; P " .53). Ofall subgroups analyzed, only patients with N2 disease may benefit of a D2 dissection. The relative riskratio for morbidity and mortality is significantly higher than one for D2 dissections, splenectomy,pancreatectomy, and age older than 70 years.
ConclusionOverall, extended lymph node dissection as defined in this study generated no long-term survivalbenefit. The associated higher postoperative mortality offsets its long-term effect in survival. Forpatients with N2 disease an extended lymph node dissection may offer cure, but it remains difficult toidentify patients who have N2 disease. Morbidity and mortality are greatly influenced by the extent oflymph node dissection, pancreatectomy, splenectomy and age. Extended lymph node dissections maybe of benefit if morbidity and mortality can be avoided.
J Clin Oncol 22:2069-2077. © 2004 by American Society of Clinical Oncology
INTRODUCTION
Gastric cancer is a common malignancy world-wide. Even in a low-incidence country like theNetherlands, it is ranked fifth with respect to in-cidence. Despite declining incidence, mortalityofgastriccancerremainshigh.Surgeryistheonlypossible curative treatment, and results of gas-trectomy have improved throughout the yearswith respect to survival, morbidity, and postop-erative mortality.1,2
It is not clear, however, if extendedlymph node dissection contributes to this
improvement. Despite promising results innonrandomized studies, improved survivalhas never been demonstrated in random-ized trials.3-6 In all these randomized trials,postoperative morbidity and mortality weresignificantly higher in the extended (D2)dissection group. Within the Dutch GastricCancer Trial (DGCT), the number of earlygastric cancers was surprisingly high, and ithas been argued that any beneficial effect ofextended lymph node dissection, whichwould be expected in more advanced dis-ease, might have been attenuated. We have
From the Department of Surgery andthe Department of Medical Statistics,Leiden University Medical Center, Lei-den; Department of Surgery and De-partment of Pathology, University Medi-cal Center St Radboud, Nijmegen;Department of Surgery, University Hos-pital Amsterdam Vrije Universiteit, Am-sterdam; Department of Surgery, Uni-versity Hospital Groningen, Groningen;Department of Surgery, GeertruidenHospital Deventer, Deventer; Depart-ment of Surgery, Academic MedicalCenter Amsterdam, Amsterdam; De-partment of Surgery, Reinier de GraafHospital, Delft; Department of Surgery,University Hospital Maastricht, Maas-tricht; Department of Surgery, ErasmusMedical Center, Rotterdam, the Nether-lands; and the Department of Surgery,National Cancer Center Hospital, Tokyo,Japan.
†Deceased.
Submitted August 5, 2003; acceptedFebruary 18, 2004.
Supported by grants from the DutchHealth Insurance Funds Council and theNetherlands Cancer Foundation.
Authors’ disclosures of potential con-flicts of interest are found at the end ofthis article.
Address reprint requests to H.H.Hartgrink, MD, Department of Surgery,Leiden University Medical Centre, POBox 9600, 2300 RC Leiden, TheNetherlands; e-mail: [email protected].
© 2004 by American Society of ClinicalOncology
0732-183X/04/2211-2069/$20.00
DOI: 10.1200/JCO.2004.08.026
JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T
VOLUME 22 ! NUMBER 11 ! JUNE 1 2004
2069
193.54.110.33Information downloaded from jco.ascopubs.org and provided by at CDMP - APHP on December 18, 2014 from
Copyright © 2004 American Society of Clinical Oncology. All rights reserved.
Splenectomy and pancreatectomy are important riskfactors for morbidity and hospital mortality after D2 dissec-tion,16,17 with a significant adverse effect on survival aswell.18 Two Japanese studies showed no beneficial effect onsurvival if pancreatosplenectomy was combined with totalgastrectomy, whereas morbidity was increased in these pa-tients.19,20 A randomized trial in Chile found no survivalbenefit from a splenectomy in patients with total gastrec-tomy, whereas morbidity was again significantly in-creased.21 Another randomized trial to study the effect ofsplenectomy is underway in Japan.22 In our study the riskratio for morbidity and mortality was significant for pan-createctomy and splenectomy. The question is whether asurvival benefit can be achieved with an extended lymphnode dissection, if morbidity- and mortality-increasingprocedures such as pancreatectomy and splenectomy canbe avoided. A randomized English study supports this hy-pothesis for patients with stage II and III disease.23 Pancreasand spleen sparing procedures have now become standardin Japan as well as many Western countries.
The main reason to do pancreatectomy and splenec-tomy in D2 dissection was not to compromise an adequatedissection of lymph node stations 10 and 11. Metastasis in
these lymph nodes, however, confers a poor prognosis. Inour study, patients with metastasis in these lymph nodeshave a survival rate at 11 years of 8% and 11%, respectively,whereas patients without metastases have a survival rate of27% and 35%, respectively. So the relevance of the dissec-tion of these nodes has to be questioned as the survivalbenefit is small and morbidity and hospital mortality aresignificantly increased.
Total gastrectomy has a higher morbidity and hospitalmortality rate than partial gastrectomy. A randomized trialin Italy showed that there is no survival benefit from a totalgastrectomy if resection margins are free of tumor.18 Sototal gastrectomy should only be performed if the localiza-tion of the tumor requires to do so.
With the aging of the populations of industrializedcountries, more elderly patients with gastric cancer will bediagnosed. Population-based data from the Netherlandsshow that from 1982 to 1992, 27% of newly diagnosedpatients were older than 80 years.24 In a study on gastriccancer in the elderly by Klein Kranenbarg et al,25 it wasshown that there is no difference in resectability and cur-ability rate between different age groups, but hospital mor-tality increases with increasing age, especially older than 70
Fig 3. Survival of patients treated with curative intent according to N stage. (A), N0; (B), N1; (C), N2; (D), N3. D1, limited lymph node dissection group; D2, extendedlymph node dissection group.
Hartgrink et al
2074 JOURNAL OF CLINICAL ONCOLOGY
193.54.110.33Information downloaded from jco.ascopubs.org and provided by at CDMP - APHP on December 18, 2014 from
Copyright © 2004 American Society of Clinical Oncology. All rights reserved.
N2
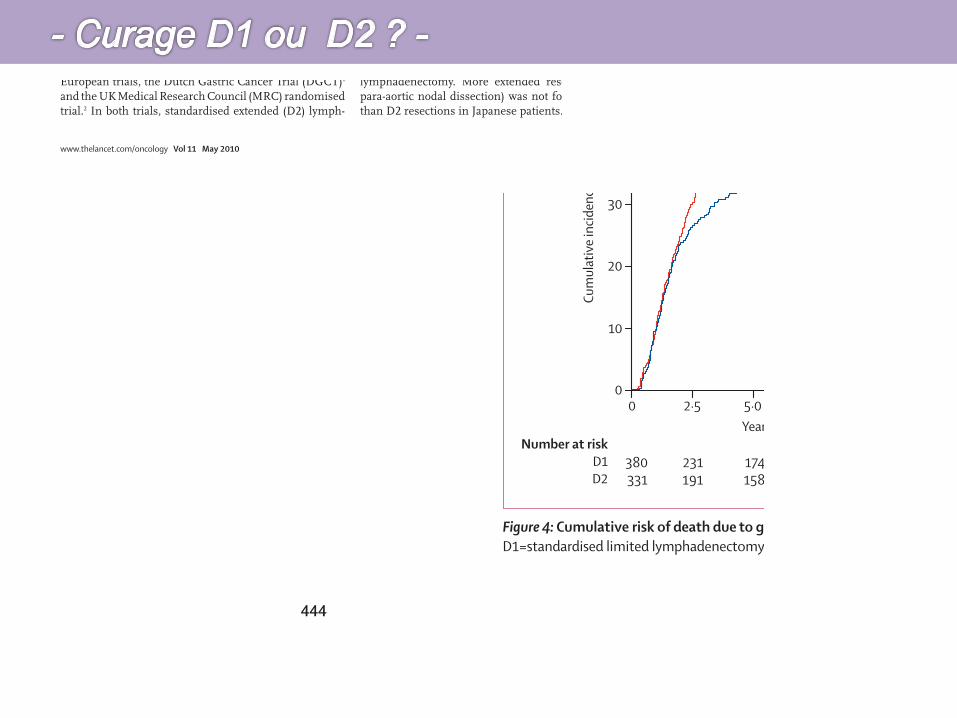
Articles
444 www.thelancet.com/oncology Vol 11 May 2010
and 320 patients (45%) died with recurrence (188 in D1 and 131 in D2). 173 patients (24%) were alive without recurrence (82 in D1 and 91 in D2), and one patient was alive with recurrence in the D2 group. 15-year overall survival for patients who had curative resections was 21% (85 of 380, 95% CI 17–26) for D1 and 29% (98 of 331, 24–34) for D2 (log-rank p=0·34; fi gure 3).
D2 patients had signifi cantly higher operative mortality than D1 patients (32 of 331 [10%] vs 15 of 380 [4%], 95% CI for the diff erence 2–9%, p=0·004), higher complication rate (142 of 331 [43%] vs 94 of 380 [25%], 11–25%, p<0·0001, and higher reoperation rate (59 of 331 [18%] vs 30 of 380 [8%] 5–15%, p<0·00016; previously published9,10). Signifi cant risk factors for postoperative mortality in logistic regression analysis were: age >70 versus ≤70 years (overall risk [OR] 3·55, 95% CI 1·91–6·61, p<0·0001), D2 versus D1 lymphadenectomy (OR 2·64, 1·38–5·04, p=0·003), male versus female (OR 2·50, 1·25–4·99, p=0·01) and total versus partial
gastrectomy (OR 2·04, 1·01–3·79, p=0·02; data not shown). Other factors included in the analysis but that had no signifi cant association with postoperative mortality were T stage, lymph-node involvement (N-negative vs N-positive and N0–N3), and TNM stage. Overall survival for patients who had an R0 resection was 25% (85 of 324, 95% CI 20–30) for D1 and 35% (97 of 268, 30–41) for D2, when postoperative deaths (15 of 380 [4%] in D1 and 32 of 331 [10%] in D2) are excluded (log-rank p=0·08). The reasons for no R0 resection are reported in table 2.
The following analyses are based on the 711 patients who had curative resections. Table 3 shows the results of univariate analyses of 15-year overall survival and hazard ratios (HR), according to subgroups based on several prognostic variables. Overall survival was signifi cantly higher for female patients who had D2 versus D1 dissection (35% vs 21%, p=0·03), and for patients with TNM stage II disease (33% in D2 vs 15% in D1, p=0·03). Patients with N2 disease had better survival after a D2 dissection (19% in D2 vs 0% in D1, p=0·07), as did those who had partial gastrectomy (35% in D2 vs 24% in D1, p=0·08), however this was not statistically signifi cant.
Cause of death was analysed for all patients and the distribution for the D1 and D2 groups is summarised in table 4. Gastric-cancer-related death was signifi cantly higher in the D1 group compared with the D2 group (HR 0·74 for D2 vs D1, 95% CI 0·59–0·93, p=0·01), whereas death due to other causes was not diff erent between groups (HR 1·22 for D2 vs D1, 0·95–1·58, p=0·12; fi gure 4). Five patients in the D1 group had recurrence at the time of death (two patients with locoregional recurrence, two patients with local and distant recurrence,
D1 group (n=380)
D2 group (n=331)
p value
Alive 82 (22%) 92 (28%) 0·34*
Deaths from gastric cancer 182 (48%) 123 (37%) 0·01†
Deaths from other causes 116 (31%) 116 (35%) 0·12†
Other diseases 94 (25%) 77 (23%) ..
Toxicity treatment 15 ( 4%) 32 (10%) ..
Unknown 7 (2%) 7 ( 2%) ..
Data are number of patients (%) or p value. D1=standardised limited lymphadenectomy. D2=standardised extended lymphadenectomy. *Log-rank p value. †Gray’s test p value.
Table 4: Causes of death
Figure 4: Cumulative risk of death due to gastric cancer and due to other causes in patients treated with curative intent (n=711)D1=standardised limited lymphadenectomy. D2=standardised extended lymphadenectomy.
00
10
20
30
40
50
A Death due to gastric cancer
2·5 5·0Years after randomisation
Number at riskD1D2
Cum
ulat
ive i
ncid
ence
(%)
7·5 10·0 12·5 15·0
380331
231191
174158
149138
132125
108110
4770
D1D2
p=0·01
0
B Death due to other causes
2·5 5·0Years after randomisation
7·5 10·0 12·5 15·0
380331
231191
174158
149138
132125
108110
4770
p=0·12
Articles
www.thelancet.com/oncology Vol 11 May 2010 439
Lancet Oncol 2010; 11: 439–49
Published OnlineApril 20, 2010DOI:10.1016/S1470-2045(10)70070-X
See Refl ection and Reactionpage 404
Department of Surgery (I Songun MD, E M-K Kranenbarg Msc, Prof C J H van de Velde MD) and Department of Medical Statistics (H Putter PhD), Leiden University Medical Center, Leiden, the Netherlands; and Department of Surgery, Hyogo College of Medicine, Mukogawa-cho, Nishinomiya, Hyogo, Japan (M Sasako MD)
Correspondence to:Dr Ilfet Songun, Department of Surgery, K6-R Leiden University Medical Center, PO Box 9600, 2300 RC Leiden, the [email protected]
Surgical treatment of gastric cancer: 15-year follow-up results of the randomised nationwide Dutch D1D2 trial Ilfet Songun, Hein Putter, Elma Meershoek-Klein Kranenbarg, Mitsuru Sasako, Cornelis J H van de Velde
Background Historical data and recent studies show that standardised extended (D2) lymphadenectomy leads to better results than standardised limited (D1) lymphadenectomy. Based on these fi ndings, the Dutch D1D2 trial, a nationwide prospectively randomised clinical trial, was undertaken to compare D2 with D1 lymphadenectomy in patients with resectable primary adenocarcinoma of the stomach. The aim of the study was to assess the eff ect of D2 compared with D1 surgery on disease recurrence and survival in patients treated with curative intent.
Methods Between August, 1989, and July, 1993, patients were entered and randomised at 80 participating hospitals by means of a telephone call to the central data centre of the trial. The sequence of randomisation was in blocks of six with stratifi cation for the participating centre. Eligibility criteria were a histologically proven adenocarcinoma of the stomach without evidence of distance metastasis, age younger than 85 years, and adequate physical condition for D1 or D2 lymphadenectomy. Patients were excluded if they had previous or coexisting cancer or had undergone gastrectomy for benign tumours. Strict quality control measures for pathological assessment were implemented and monitored. Analyses were by intention to treat. This study is registered with the NCI trial register, as DUT-KWF-CKVO-8905, EU-90003.
Findings A total of 1078 patients were entered in the study, of whom 996 were eligible. 711 patients underwent the randomly assigned treatment with curative intent (380 in the D1 group and 331 in the D2 group) and 285 had palliative treatment. Data were collected prospectively and all patients were followed up for a median time of 15·2 years (range 6·9–17·9 years). Analyses were done for the 711 patients treated with curative intent and were according to the allocated treatment group. Of the 711 patients, 174 (25%) were alive, all but one without recurrence. Overall 15-year survival was 21% (82 patients) for the D1 group and 29% (92 patients) for the D2 group (p=0·34). Gastric-cancer-related death rate was signifi cantly higher in the D1 group (48%, 182 patients) compared with the D2 group (37%, 123 patients), whereas death due to other diseases was similar in both groups. Local recurrence was 22% (82 patients) in the D1 group versus 12% (40 patients) in D2, and regional recurrence was 19% (73 patients) in D1 versus 13% (43 patients) in D2. Patients who had the D2 procedure had a signifi cantly higher operative mortality rate than those who had D1 (n=32 [10%] vs n=15 [4%]; 95% CI for the diff erence 2–9; p=0·004), higher complication rate (n=142 [43%] vs n=94 [25%]; 11–25; p<0·0001), and higher reoperation rate (n=59 [18%] vs n=30 [8%]; 5–15; p=0·00016).
Interpretation After a median follow-up of 15 years, D2 lymphadenectomy is associated with lower locoregional recurrence and gastric-cancer-related death rates than D1 surgery. The D2 procedure was also associated with signifi cantly higher postoperative mortality, morbidity, and reoperation rates. Because a safer, spleen-preserving D2 resection technique is currently available in high-volume centres, D2 lymphadenectomy is the recommended surgical approach for patients with resectable (curable) gastric cancer.
Funding Dutch Health Insurance Funds Council and the Netherlands Cancer Foundation.
IntroductionAfter several decades of debate on what the optimum surgical treatment of gastric cancer should be, it is now possible to treat patients using evidence-based principles established by well designed and conducted studies. Adequate surgery, the only treatment known to off er cure, is still the cornerstone of gastric-cancer treatment; however, local regional control remains an issue. In western Europe and the USA, optimum local control and survival seemed to be reached with surgery as a single-modality treatment, based mainly on two large European trials, the Dutch Gastric Cancer Trial (DGCT)1 and the UK Medical Research Council (MRC) randomised trial.2 In both trials, standardised extended (D2) lymph-
aden ectomy did not improve survival, and was associated with signifi cantly higher morbidity and mortality compared with standardised limited (D1) lymph-adenectomy. The unfavourable outcomes were mostly associated with pancreatico-splenectomy, which was an integral part of the D2 resection in both trials. In 2004, results from a study by Degiuli and colleagues3 suggested a survival benefi t after pancreas-preserving D2 resections, and in 2006, a Taiwanese single-institution trial4 found that extended lymph-node dissection (D2) led to better results (no postoperative mortality) than D1 lymphadenectomy. More extended resection (D2 plus para-aortic nodal dissection) was not found to be better than D2 resections in Japanese patients.5
Articles
www.thelancet.com/oncology Vol 11 May 2010 439
Lancet Oncol 2010; 11: 439–49
Published OnlineApril 20, 2010DOI:10.1016/S1470-2045(10)70070-X
See Refl ection and Reactionpage 404
Department of Surgery (I Songun MD, E M-K Kranenbarg Msc, Prof C J H van de Velde MD) and Department of Medical Statistics (H Putter PhD), Leiden University Medical Center, Leiden, the Netherlands; and Department of Surgery, Hyogo College of Medicine, Mukogawa-cho, Nishinomiya, Hyogo, Japan (M Sasako MD)
Correspondence to:Dr Ilfet Songun, Department of Surgery, K6-R Leiden University Medical Center, PO Box 9600, 2300 RC Leiden, the [email protected]
Surgical treatment of gastric cancer: 15-year follow-up results of the randomised nationwide Dutch D1D2 trial Ilfet Songun, Hein Putter, Elma Meershoek-Klein Kranenbarg, Mitsuru Sasako, Cornelis J H van de Velde
Background Historical data and recent studies show that standardised extended (D2) lymphadenectomy leads to better results than standardised limited (D1) lymphadenectomy. Based on these fi ndings, the Dutch D1D2 trial, a nationwide prospectively randomised clinical trial, was undertaken to compare D2 with D1 lymphadenectomy in patients with resectable primary adenocarcinoma of the stomach. The aim of the study was to assess the eff ect of D2 compared with D1 surgery on disease recurrence and survival in patients treated with curative intent.
Methods Between August, 1989, and July, 1993, patients were entered and randomised at 80 participating hospitals by means of a telephone call to the central data centre of the trial. The sequence of randomisation was in blocks of six with stratifi cation for the participating centre. Eligibility criteria were a histologically proven adenocarcinoma of the stomach without evidence of distance metastasis, age younger than 85 years, and adequate physical condition for D1 or D2 lymphadenectomy. Patients were excluded if they had previous or coexisting cancer or had undergone gastrectomy for benign tumours. Strict quality control measures for pathological assessment were implemented and monitored. Analyses were by intention to treat. This study is registered with the NCI trial register, as DUT-KWF-CKVO-8905, EU-90003.
Findings A total of 1078 patients were entered in the study, of whom 996 were eligible. 711 patients underwent the randomly assigned treatment with curative intent (380 in the D1 group and 331 in the D2 group) and 285 had palliative treatment. Data were collected prospectively and all patients were followed up for a median time of 15·2 years (range 6·9–17·9 years). Analyses were done for the 711 patients treated with curative intent and were according to the allocated treatment group. Of the 711 patients, 174 (25%) were alive, all but one without recurrence. Overall 15-year survival was 21% (82 patients) for the D1 group and 29% (92 patients) for the D2 group (p=0·34). Gastric-cancer-related death rate was signifi cantly higher in the D1 group (48%, 182 patients) compared with the D2 group (37%, 123 patients), whereas death due to other diseases was similar in both groups. Local recurrence was 22% (82 patients) in the D1 group versus 12% (40 patients) in D2, and regional recurrence was 19% (73 patients) in D1 versus 13% (43 patients) in D2. Patients who had the D2 procedure had a signifi cantly higher operative mortality rate than those who had D1 (n=32 [10%] vs n=15 [4%]; 95% CI for the diff erence 2–9; p=0·004), higher complication rate (n=142 [43%] vs n=94 [25%]; 11–25; p<0·0001), and higher reoperation rate (n=59 [18%] vs n=30 [8%]; 5–15; p=0·00016).
Interpretation After a median follow-up of 15 years, D2 lymphadenectomy is associated with lower locoregional recurrence and gastric-cancer-related death rates than D1 surgery. The D2 procedure was also associated with signifi cantly higher postoperative mortality, morbidity, and reoperation rates. Because a safer, spleen-preserving D2 resection technique is currently available in high-volume centres, D2 lymphadenectomy is the recommended surgical approach for patients with resectable (curable) gastric cancer.
Funding Dutch Health Insurance Funds Council and the Netherlands Cancer Foundation.
IntroductionAfter several decades of debate on what the optimum surgical treatment of gastric cancer should be, it is now possible to treat patients using evidence-based principles established by well designed and conducted studies. Adequate surgery, the only treatment known to off er cure, is still the cornerstone of gastric-cancer treatment; however, local regional control remains an issue. In western Europe and the USA, optimum local control and survival seemed to be reached with surgery as a single-modality treatment, based mainly on two large European trials, the Dutch Gastric Cancer Trial (DGCT)1 and the UK Medical Research Council (MRC) randomised trial.2 In both trials, standardised extended (D2) lymph-
aden ectomy did not improve survival, and was associated with signifi cantly higher morbidity and mortality compared with standardised limited (D1) lymph-adenectomy. The unfavourable outcomes were mostly associated with pancreatico-splenectomy, which was an integral part of the D2 resection in both trials. In 2004, results from a study by Degiuli and colleagues3 suggested a survival benefi t after pancreas-preserving D2 resections, and in 2006, a Taiwanese single-institution trial4 found that extended lymph-node dissection (D2) led to better results (no postoperative mortality) than D1 lymphadenectomy. More extended resection (D2 plus para-aortic nodal dissection) was not found to be better than D2 resections in Japanese patients.5
Articles
www.thelancet.com/oncology Vol 11 May 2010 439
Lancet Oncol 2010; 11: 439–49
Published OnlineApril 20, 2010DOI:10.1016/S1470-2045(10)70070-X
See Refl ection and Reactionpage 404
Department of Surgery (I Songun MD, E M-K Kranenbarg Msc, Prof C J H van de Velde MD) and Department of Medical Statistics (H Putter PhD), Leiden University Medical Center, Leiden, the Netherlands; and Department of Surgery, Hyogo College of Medicine, Mukogawa-cho, Nishinomiya, Hyogo, Japan (M Sasako MD)
Correspondence to:Dr Ilfet Songun, Department of Surgery, K6-R Leiden University Medical Center, PO Box 9600, 2300 RC Leiden, the [email protected]
Surgical treatment of gastric cancer: 15-year follow-up results of the randomised nationwide Dutch D1D2 trial Ilfet Songun, Hein Putter, Elma Meershoek-Klein Kranenbarg, Mitsuru Sasako, Cornelis J H van de Velde
Background Historical data and recent studies show that standardised extended (D2) lymphadenectomy leads to better results than standardised limited (D1) lymphadenectomy. Based on these fi ndings, the Dutch D1D2 trial, a nationwide prospectively randomised clinical trial, was undertaken to compare D2 with D1 lymphadenectomy in patients with resectable primary adenocarcinoma of the stomach. The aim of the study was to assess the eff ect of D2 compared with D1 surgery on disease recurrence and survival in patients treated with curative intent.
Methods Between August, 1989, and July, 1993, patients were entered and randomised at 80 participating hospitals by means of a telephone call to the central data centre of the trial. The sequence of randomisation was in blocks of six with stratifi cation for the participating centre. Eligibility criteria were a histologically proven adenocarcinoma of the stomach without evidence of distance metastasis, age younger than 85 years, and adequate physical condition for D1 or D2 lymphadenectomy. Patients were excluded if they had previous or coexisting cancer or had undergone gastrectomy for benign tumours. Strict quality control measures for pathological assessment were implemented and monitored. Analyses were by intention to treat. This study is registered with the NCI trial register, as DUT-KWF-CKVO-8905, EU-90003.
Findings A total of 1078 patients were entered in the study, of whom 996 were eligible. 711 patients underwent the randomly assigned treatment with curative intent (380 in the D1 group and 331 in the D2 group) and 285 had palliative treatment. Data were collected prospectively and all patients were followed up for a median time of 15·2 years (range 6·9–17·9 years). Analyses were done for the 711 patients treated with curative intent and were according to the allocated treatment group. Of the 711 patients, 174 (25%) were alive, all but one without recurrence. Overall 15-year survival was 21% (82 patients) for the D1 group and 29% (92 patients) for the D2 group (p=0·34). Gastric-cancer-related death rate was signifi cantly higher in the D1 group (48%, 182 patients) compared with the D2 group (37%, 123 patients), whereas death due to other diseases was similar in both groups. Local recurrence was 22% (82 patients) in the D1 group versus 12% (40 patients) in D2, and regional recurrence was 19% (73 patients) in D1 versus 13% (43 patients) in D2. Patients who had the D2 procedure had a signifi cantly higher operative mortality rate than those who had D1 (n=32 [10%] vs n=15 [4%]; 95% CI for the diff erence 2–9; p=0·004), higher complication rate (n=142 [43%] vs n=94 [25%]; 11–25; p<0·0001), and higher reoperation rate (n=59 [18%] vs n=30 [8%]; 5–15; p=0·00016).
Interpretation After a median follow-up of 15 years, D2 lymphadenectomy is associated with lower locoregional recurrence and gastric-cancer-related death rates than D1 surgery. The D2 procedure was also associated with signifi cantly higher postoperative mortality, morbidity, and reoperation rates. Because a safer, spleen-preserving D2 resection technique is currently available in high-volume centres, D2 lymphadenectomy is the recommended surgical approach for patients with resectable (curable) gastric cancer.
Funding Dutch Health Insurance Funds Council and the Netherlands Cancer Foundation.
IntroductionAfter several decades of debate on what the optimum surgical treatment of gastric cancer should be, it is now possible to treat patients using evidence-based principles established by well designed and conducted studies. Adequate surgery, the only treatment known to off er cure, is still the cornerstone of gastric-cancer treatment; however, local regional control remains an issue. In western Europe and the USA, optimum local control and survival seemed to be reached with surgery as a single-modality treatment, based mainly on two large European trials, the Dutch Gastric Cancer Trial (DGCT)1 and the UK Medical Research Council (MRC) randomised trial.2 In both trials, standardised extended (D2) lymph-
aden ectomy did not improve survival, and was associated with signifi cantly higher morbidity and mortality compared with standardised limited (D1) lymph-adenectomy. The unfavourable outcomes were mostly associated with pancreatico-splenectomy, which was an integral part of the D2 resection in both trials. In 2004, results from a study by Degiuli and colleagues3 suggested a survival benefi t after pancreas-preserving D2 resections, and in 2006, a Taiwanese single-institution trial4 found that extended lymph-node dissection (D2) led to better results (no postoperative mortality) than D1 lymphadenectomy. More extended resection (D2 plus para-aortic nodal dissection) was not found to be better than D2 resections in Japanese patients.5
Articles
www.thelancet.com/oncology Vol 11 May 2010 439
Lancet Oncol 2010; 11: 439–49
Published OnlineApril 20, 2010DOI:10.1016/S1470-2045(10)70070-X
See Refl ection and Reactionpage 404
Department of Surgery (I Songun MD, E M-K Kranenbarg Msc, Prof C J H van de Velde MD) and Department of Medical Statistics (H Putter PhD), Leiden University Medical Center, Leiden, the Netherlands; and Department of Surgery, Hyogo College of Medicine, Mukogawa-cho, Nishinomiya, Hyogo, Japan (M Sasako MD)
Correspondence to:Dr Ilfet Songun, Department of Surgery, K6-R Leiden University Medical Center, PO Box 9600, 2300 RC Leiden, the [email protected]
Surgical treatment of gastric cancer: 15-year follow-up results of the randomised nationwide Dutch D1D2 trial Ilfet Songun, Hein Putter, Elma Meershoek-Klein Kranenbarg, Mitsuru Sasako, Cornelis J H van de Velde
Background Historical data and recent studies show that standardised extended (D2) lymphadenectomy leads to better results than standardised limited (D1) lymphadenectomy. Based on these fi ndings, the Dutch D1D2 trial, a nationwide prospectively randomised clinical trial, was undertaken to compare D2 with D1 lymphadenectomy in patients with resectable primary adenocarcinoma of the stomach. The aim of the study was to assess the eff ect of D2 compared with D1 surgery on disease recurrence and survival in patients treated with curative intent.
Methods Between August, 1989, and July, 1993, patients were entered and randomised at 80 participating hospitals by means of a telephone call to the central data centre of the trial. The sequence of randomisation was in blocks of six with stratifi cation for the participating centre. Eligibility criteria were a histologically proven adenocarcinoma of the stomach without evidence of distance metastasis, age younger than 85 years, and adequate physical condition for D1 or D2 lymphadenectomy. Patients were excluded if they had previous or coexisting cancer or had undergone gastrectomy for benign tumours. Strict quality control measures for pathological assessment were implemented and monitored. Analyses were by intention to treat. This study is registered with the NCI trial register, as DUT-KWF-CKVO-8905, EU-90003.
Findings A total of 1078 patients were entered in the study, of whom 996 were eligible. 711 patients underwent the randomly assigned treatment with curative intent (380 in the D1 group and 331 in the D2 group) and 285 had palliative treatment. Data were collected prospectively and all patients were followed up for a median time of 15·2 years (range 6·9–17·9 years). Analyses were done for the 711 patients treated with curative intent and were according to the allocated treatment group. Of the 711 patients, 174 (25%) were alive, all but one without recurrence. Overall 15-year survival was 21% (82 patients) for the D1 group and 29% (92 patients) for the D2 group (p=0·34). Gastric-cancer-related death rate was signifi cantly higher in the D1 group (48%, 182 patients) compared with the D2 group (37%, 123 patients), whereas death due to other diseases was similar in both groups. Local recurrence was 22% (82 patients) in the D1 group versus 12% (40 patients) in D2, and regional recurrence was 19% (73 patients) in D1 versus 13% (43 patients) in D2. Patients who had the D2 procedure had a signifi cantly higher operative mortality rate than those who had D1 (n=32 [10%] vs n=15 [4%]; 95% CI for the diff erence 2–9; p=0·004), higher complication rate (n=142 [43%] vs n=94 [25%]; 11–25; p<0·0001), and higher reoperation rate (n=59 [18%] vs n=30 [8%]; 5–15; p=0·00016).
Interpretation After a median follow-up of 15 years, D2 lymphadenectomy is associated with lower locoregional recurrence and gastric-cancer-related death rates than D1 surgery. The D2 procedure was also associated with signifi cantly higher postoperative mortality, morbidity, and reoperation rates. Because a safer, spleen-preserving D2 resection technique is currently available in high-volume centres, D2 lymphadenectomy is the recommended surgical approach for patients with resectable (curable) gastric cancer.
Funding Dutch Health Insurance Funds Council and the Netherlands Cancer Foundation.
IntroductionAfter several decades of debate on what the optimum surgical treatment of gastric cancer should be, it is now possible to treat patients using evidence-based principles established by well designed and conducted studies. Adequate surgery, the only treatment known to off er cure, is still the cornerstone of gastric-cancer treatment; however, local regional control remains an issue. In western Europe and the USA, optimum local control and survival seemed to be reached with surgery as a single-modality treatment, based mainly on two large European trials, the Dutch Gastric Cancer Trial (DGCT)1 and the UK Medical Research Council (MRC) randomised trial.2 In both trials, standardised extended (D2) lymph-
aden ectomy did not improve survival, and was associated with signifi cantly higher morbidity and mortality compared with standardised limited (D1) lymph-adenectomy. The unfavourable outcomes were mostly associated with pancreatico-splenectomy, which was an integral part of the D2 resection in both trials. In 2004, results from a study by Degiuli and colleagues3 suggested a survival benefi t after pancreas-preserving D2 resections, and in 2006, a Taiwanese single-institution trial4 found that extended lymph-node dissection (D2) led to better results (no postoperative mortality) than D1 lymphadenectomy. More extended resection (D2 plus para-aortic nodal dissection) was not found to be better than D2 resections in Japanese patients.5
Articles
www.thelancet.com/oncology Vol 11 May 2010 445
and one patient with distant recurrence) and seven patients in the D2 group (three patients with locoregional recurrence, three patients with local and distant recurrence, and one patient with distant recurrence), although they died of other causes. In the group of patients who died from gastric cancer, postmortem examinations were done for ten patients in the D1 group and in 18 patients in the D2 group. Except for 31 patients in the D1 group and 25 patients in the D2 group, all recurrences were established by means of additional investigations (CT scan or ultrasonography, or both, biopsy or cytology, chest radiography or bonescan) depending on the recurrence.
Local recurrence was signifi cantly higher in the D1 versus D2 group (82 of 380 [22%] vs 40 of 330 [12%]). Regional recurrence (73 of 380 [19%] in D1 vs 43 of 330 [13%] in D2) and liver metastases (65 of 380 [17%] in D1 vs 37 of 330 [11%] in D2) were also more common in the D1 group (table 5). Locoregional, distant, and distant-only recurrence are reported in table 5. Results for disease-free survival (p=0·31) and risk of recurrence (p=0·10) are shown in fi gure 5. Most patients had recurrence within 2–2·5 years, and after 5 years recurrence occurs less frequently. The diff erence in recurrence rates between the D1 and D2 group seems to present between 2·5 and 5 years of follow-up.
Patients older than 70 years had signifi cantly lower overall survival in both the D1 and the D2 treatment groups, male patients had signifi cantly lower survival compared with female patients in the D2 group (mean 7·07 years vs 8·73 years, p<0·0001), and patients undergoing splenectomy and pancreatectomy had signifi cantly lower overall survival in both D1 and D2 (table 6). Subgroup analysis of patients without pancreatico-splenectomy (339 patients in D1 and 206 in D2, data not shown) shows a signifi cantly higher overall survival in those who had D2 lymphadenectomy, with 15-year survival of 22% (75 of 339, 95% CI 17–26) in D1 and 35% (71 of 206, 29–42) in D2 (HR 1·34, 95% CI 1·09–1·65; log-rank p=0·006).
DiscussionOur fi ndings based on 15-year follow-up data of the DGCT show that D2 lymphadenectomy is associated with lower locoregional recurrence and fewer gastric-cancer-related deaths than D1. The drawback of a D2 resection is its association with signifi cantly higher
Figure 5: Disease-free survival and risk of recurrence in patients treated with curative intent (n=711)D1=standardised limited lymphadenectomy. D2=standardised extended lymphadenectomy.
00
20
40
60
80
100
A
2·5 5·0Years after randomisation
Number at riskD1D2
Dise
ase-
free s
urvi
val (
%)
Recu
rrenc
e (%
)
7·5 10·0 12·5 15·0
380331
218185
168152
144136
130123
100109
4771
D1D2
p=0·31
0
B
2·5 5·0Years after randomisation
7·5 10·0 12·5 15·0
380331
215185
168152
144133
141124
110109
9692
p=0·10
D1 group (n=380) D2 group (n=330)*
Alive, no recurrence† 82 (22%) 91 (28%)
Dead, no recurrence† 110 (29%) 107 (32%)
Dead, with recurrence‡ 188 (49%) 131 (40%)
Local 82 40
Regional 73 43
Adjacent organs 37 26
Liver metastasis 65 37
Lung metastasis 12 6
Other organs 48 38
Dead, local+regional† 58 (15%) 42 (13%)
Dead, local+distant† 100 (26%) 56 (17%)
Dead, distant† 30 ( 8%) 34 (10%)
Data are number of patients (%). D1=standardised limited lymphadenectomy. D2=standardised extended lymphadenectomy. *One patient is alive with recurrence. †Overall p value for recurrence pattern is 0·015. ‡Patients may be included in more than one category.
Table 5: Recurrence sites and patterns at time of death
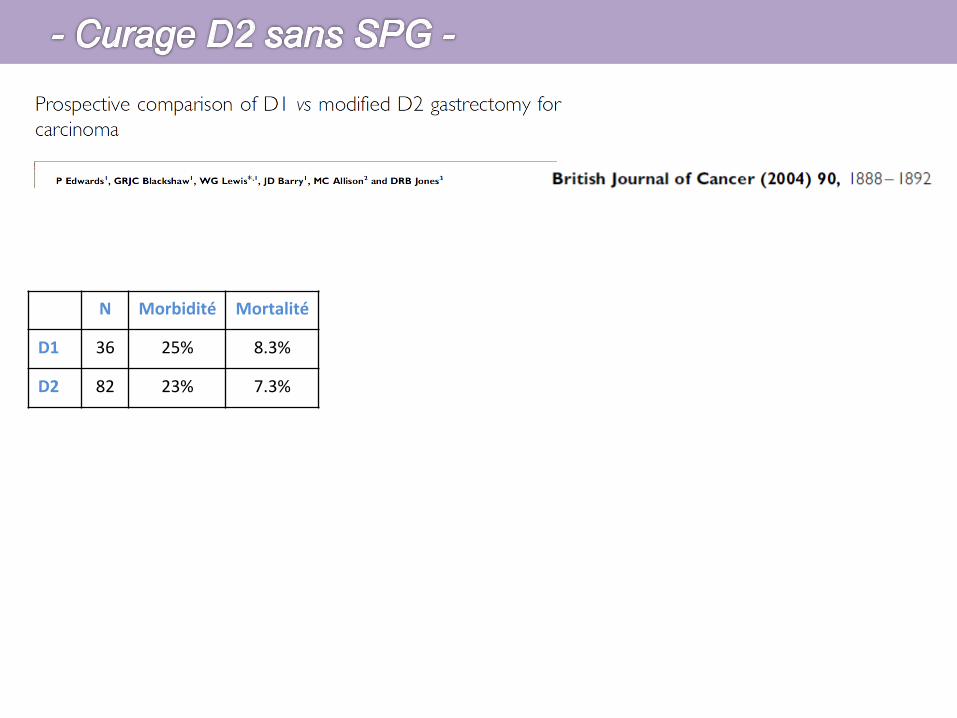
N Morbidité Mortalité
D1 36 25% 8.3%
D2 82 23% 7.3%
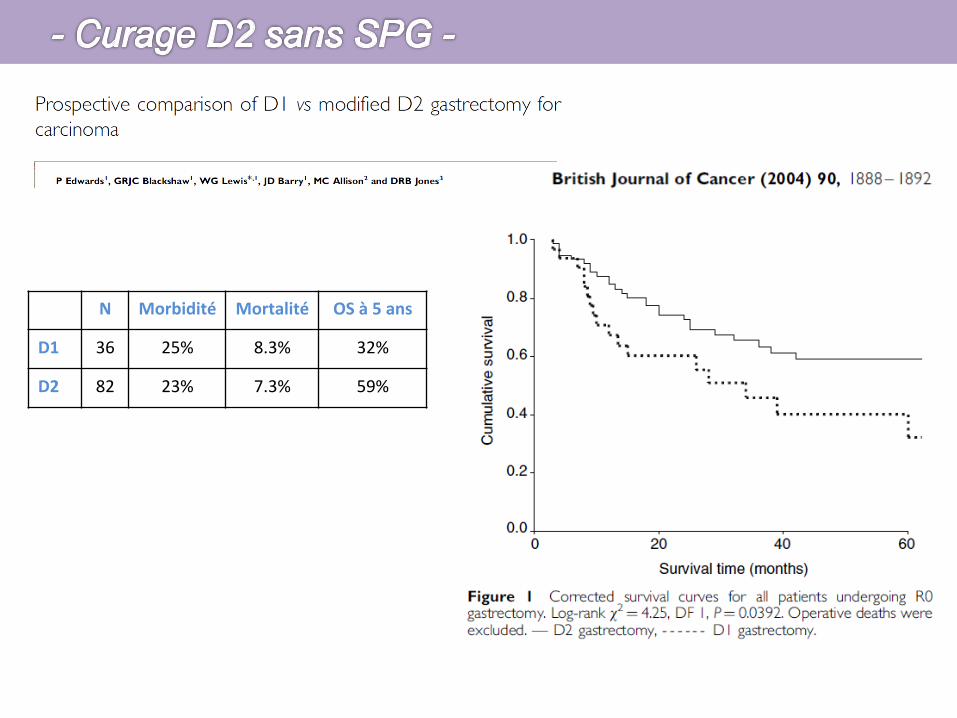
N Morbidité Mortalité OS à 5 ans
D1 36 25% 8.3% 32%
D2 82 23% 7.3% 59%

• 4 essais • Sans SPG systéma+que • D3 emportant les gg para aor+ques
– 3 même morbidité, 1 majora+on morbidité – Mortalité iden+que – Pas de bénéfice du D3 sur la survie
Sano T et al. J Clin Oncol 2004;22:2767-‐2773. Kodera Yet al. J Am Coll Surg 1997;185:65-‐69.
Yonemura Y et al. Hepatogastroenterology 2006;53:389-‐394. Kulig J et al. Am J Surg 2007;193:10-‐15.
Sasako N Engl J Med 2008; 359: 453–62.
• Le curage D2 est le curage de référence • Si une GT est nécessaire,
la préservaHon du pancréas et de la rate doit être privilégiée • > 25 ganglions • Pour les tumeurs du 1/3 inférieur
curage D2 sans inclure les staHons #2, #4sa, #10, #11
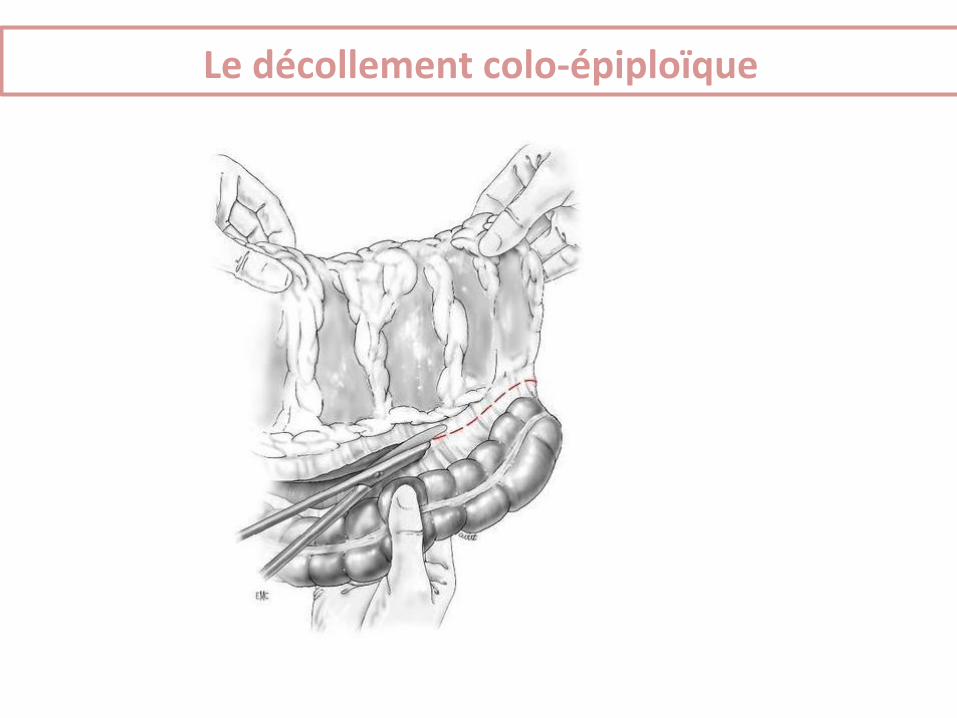
Le décollement colo-‐épiploïque
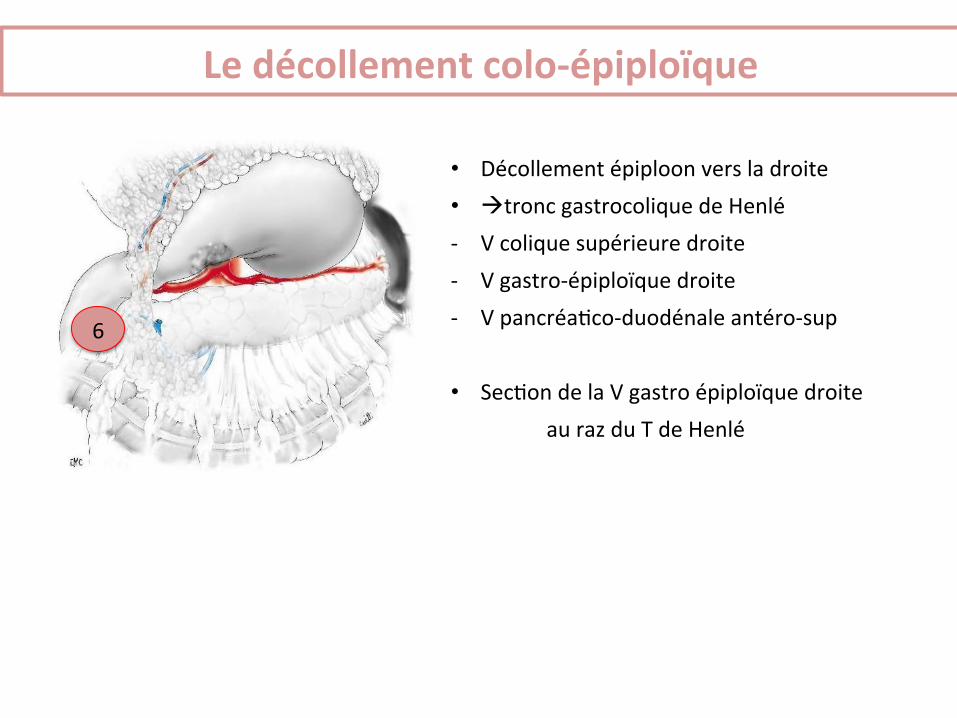
Le décollement colo-‐épiploïque
• Décollement épiploon vers la droite • àtronc gastrocolique de Henlé -‐ V colique supérieure droite -‐ V gastro-‐épiploïque droite -‐ V pancréa+co-‐duodénale antéro-‐sup
• Sec+on de la V gastro épiploïque droite au raz du T de Henlé
6
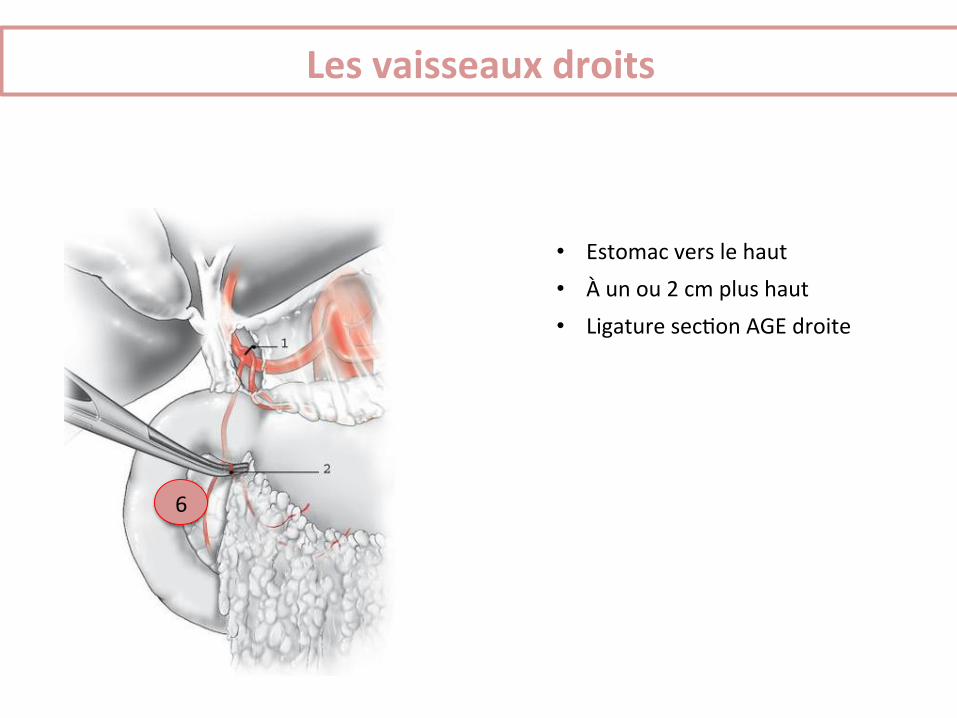
• Estomac vers le haut • À un ou 2 cm plus haut • Ligature sec+on AGE droite
6
Les vaisseaux droits
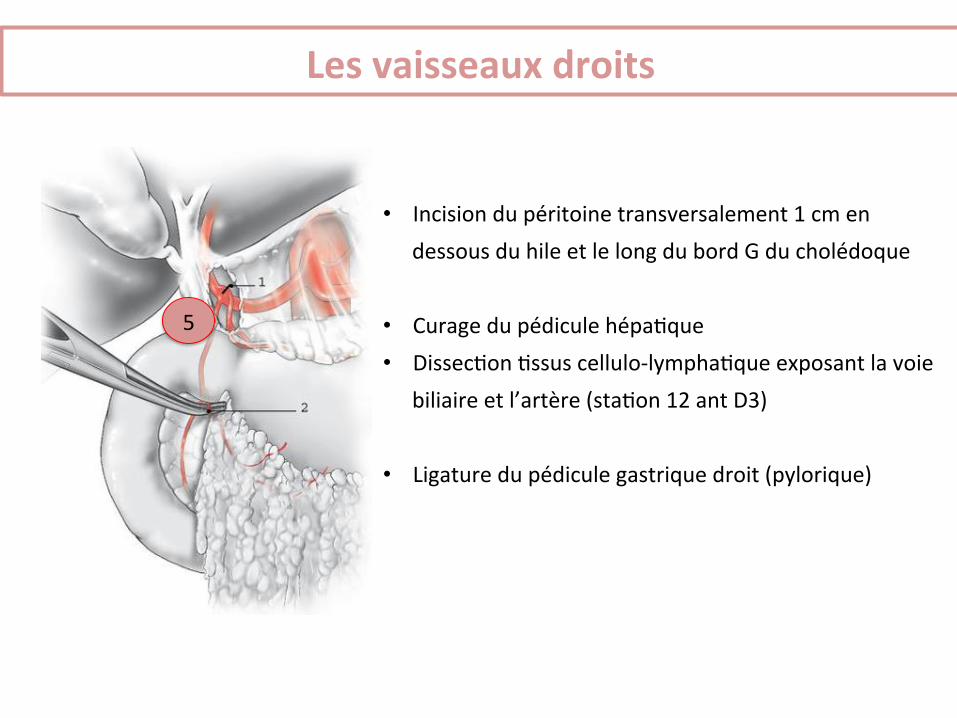
• Incision du péritoine transversalement 1 cm en dessous du hile et le long du bord G du cholédoque
• Curage du pédicule hépa+que • Dissec+on +ssus cellulo-‐lympha+que exposant la voie
biliaire et l’artère (sta+on 12 ant D3)
• Ligature du pédicule gastrique droit (pylorique)
5
Les vaisseaux droits
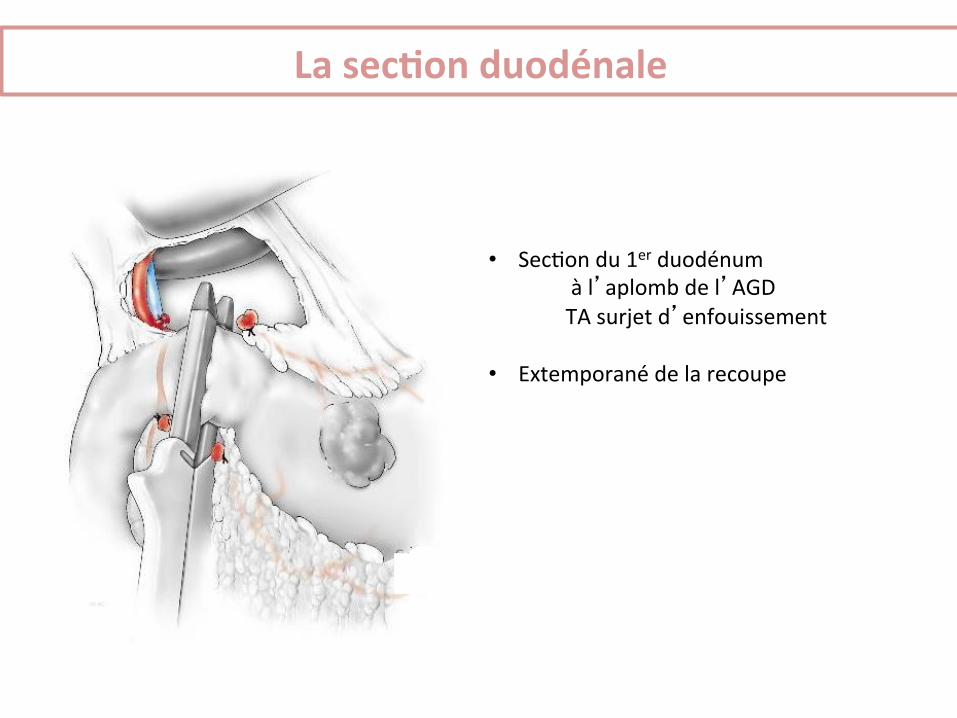
• Sec+on du 1er duodénum à l’aplomb de l’AGD TA surjet d’enfouissement
• Extemporané de la recoupe
La secHon duodénale
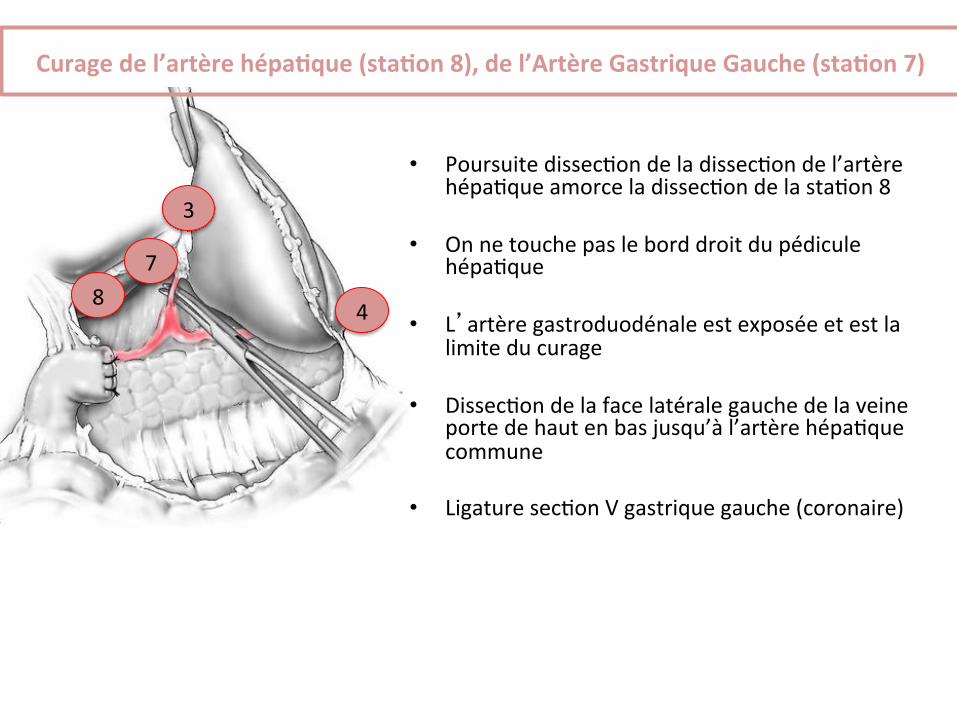
• Poursuite dissec+on de la dissec+on de l’artère hépa+que amorce la dissec+on de la sta+on 8
• On ne touche pas le bord droit du pédicule
hépa+que
• L’artère gastroduodénale est exposée et est la limite du curage
• Dissec+on de la face latérale gauche de la veine porte de haut en bas jusqu’à l’artère hépa+que commune
• Ligature sec+on V gastrique gauche (coronaire)
4
3
8 7
Curage de l’artère hépaHque (staHon 8), de l’Artère Gastrique Gauche (staHon 7)
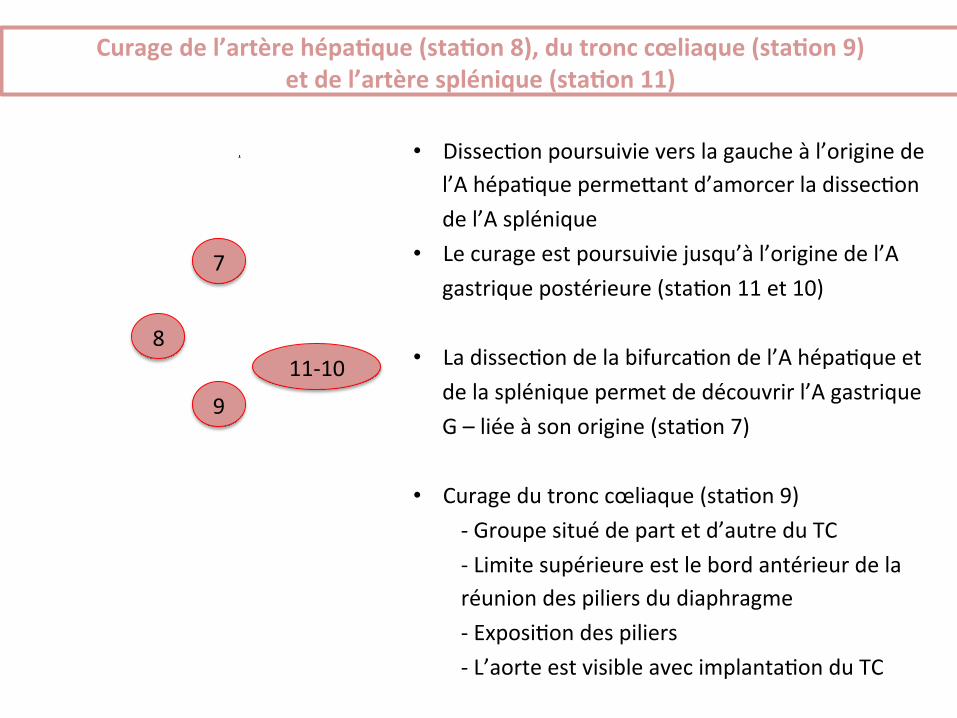
SIXIÈME TEMPS : DISSECTION DE L’ŒSOPHAGE
Après avoir réalisé le curage et la section de l’artère gastriquegauche, l’abord de l’œsophage abdominal et le curage des groupes 1et 2 sont comparables à ceux de la gastrectomie D1. La grossetubérosité n’étant pas totalement libre, la dissection de l’œsophageest moins aisée. La section de l’œsophage permet de présenter et demettre légèrement sous tension la région splénique.
SEPTIÈME TEMPS : EXÉRÈSE SPLÉNOPANCRÉATIQUE
Après section de l’œsophage abdominal, la pièce opératoire ne tientplus que par l’accolement rétrosplénique et pancréatique. Ladissection se porte au pôle inférieur de la rate. Les attachespostérieures de la rate sont sectionnées aux ciseaux, l’usage de lasection électrique étant difficile à cet endroit. Une compresse protègela rate qui est attirée vers la droite. La section du repli péritonéallibère la rate et donne un meilleur accès à la face postérieure dupancréas qui est mobilisée en « monobloc » avec la rate. Ledécollement ne doit pas être poursuivi jusqu’à la veine porte, ou enarrière d’elle. Après décollement complet de la rate, la pièce ne tientplus que par le pancréas. L’artère a déjà été liée. La veine spléniqueest liée et sectionnée à proximité de la veine mésentérique inférieure(fig 13). Il faut prendre garde à ne pas arracher quelques veinesdirectes pancréatiques. Le pancréas est à ce moment totalementdisséqué et il peut être sectionné, achevant de libérer la pièceopératoire. Le moyen le plus rapide et le plus sûr de fermeture de latranche pancréatique est d’appliquer un coup de pince automatiquelinéaire et d’effectuer la section au-delà des rangées d’agrafes(fig 14). Il est parfois nécessaire de compléter l’hémostase de latranche par un ou deux points appuyés. La section de la tranchepancréatique peut également être effectuée au bistouri froid, ou aubistouri électrique, puis la tranche est refermée par un simple ou undouble surjet d’enfouissement.Il faut ensuite envisager le rétablissement de la continuité digestivequi suit les mêmes modalités qu’après gastrectomie D1.
Gastrectomie D3La gastrectomie D3 est réalisée par une gastrectomie totaleemportant tous les groupes ganglionnaires N1 et N2. Le geste estensuite complété par un curage extensif des groupes 12, 13 et 14. Ladissection du groupe ganglionnaire 12 implique une squelettisationdu pédicule hépatique, ainsi qu’une cholécystectomie pourcompléter la dissection des branches artérielles hépatiques droites etgauches. La dissection débute au hile hépatique en prolongeantl’incision qui a permis l’exérèse du petit épiploon au-delà duligament hépatoduodénal. Cette incision est poursuivie au borddroit du ligament. La dissection du tissu cellulograisseux peut alorsêtre réalisée en disséquant les groupes 12b, puis 12p en arrière de laveine porte. La dissection du tissu celluleux est poursuivie en arrièredu pancréas qui comporte le groupe ganglionnaire 13. Le blocduodénopancréatique est basculé par une manœuvre de Kocher etles artères pancréaticoduodénales postérieures supérieures etinférieures sont disséquées et libérées de tout tissu cellulaire. La
12 Curage du tronc cœliaque (groupe 9), de l’artère hépatique (groupe 8), du pédiculehépatique (groupe 12) et de l’artère splénique (groupe 11). Les artères hépatiqueet splénique sont mises sur lacs afin de faciliter la cellulectomie qui peut être réaliséeà l’aide de clips en titane. À noter le sacrifice de la vésicule biliaire et la préparation de larésection à leurs émergences de l’artère et de la veine gastriques gauches.
13 Mobilisation de la rate et de la queue du pancréas.
14 Section du pancréas à la pince linéaire à agrafage et section.
Techniques chirurgicales Gastrectomie pour cancer 40-330-B
9
• Dissec+on poursuivie vers la gauche à l’origine de l’A hépa+que permeyant d’amorcer la dissec+on de l’A splénique
• Le curage est poursuivie jusqu’à l’origine de l’A gastrique postérieure (sta+on 11 et 10)
• La dissec+on de la bifurca+on de l’A hépa+que et
de la splénique permet de découvrir l’A gastrique G – liée à son origine (sta+on 7)
• Curage du tronc cœliaque (sta+on 9)
-‐ Groupe situé de part et d’autre du TC -‐ Limite supérieure est le bord antérieur de la réunion des piliers du diaphragme -‐ Exposi+on des piliers -‐ L’aorte est visible avec implanta+on du TC
9
8
Curage de l’artère hépaHque (staHon 8), du tronc cœliaque (staHon 9) et de l’artère splénique (staHon 11)
11-‐10
7
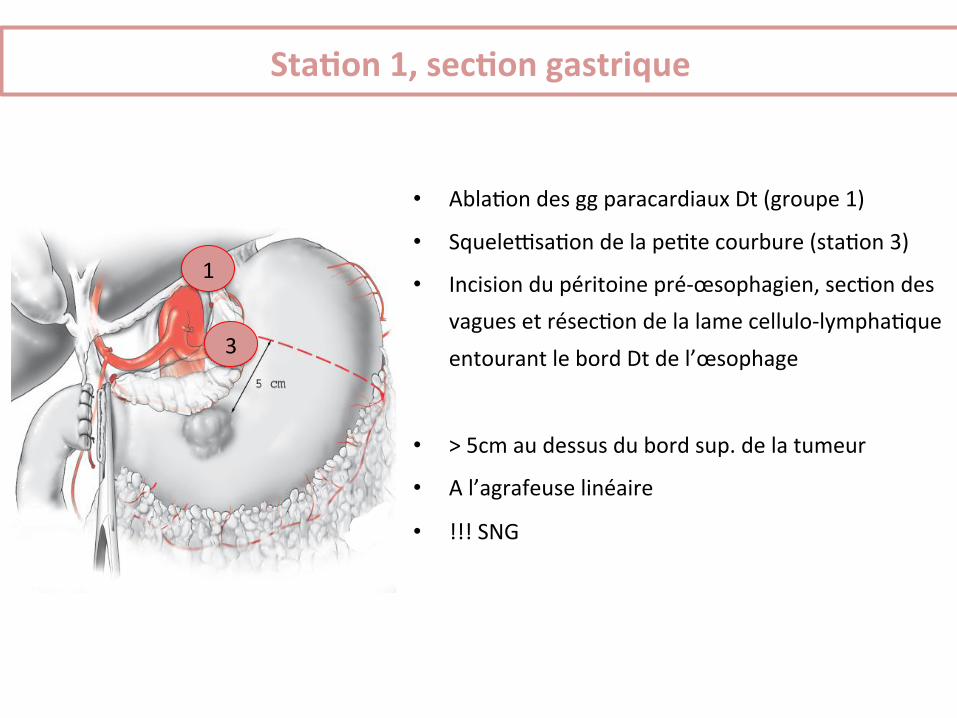
• Abla+on des gg paracardiaux Dt (groupe 1)
• Squelezsa+on de la pe+te courbure (sta+on 3)
• Incision du péritoine pré-‐œsophagien, sec+on des vagues et résec+on de la lame cellulo-‐lympha+que entourant le bord Dt de l’œsophage
• > 5cm au dessus du bord sup. de la tumeur
• A l’agrafeuse linéaire
• !!! SNG
1
StaHon 1, secHon gastrique
3
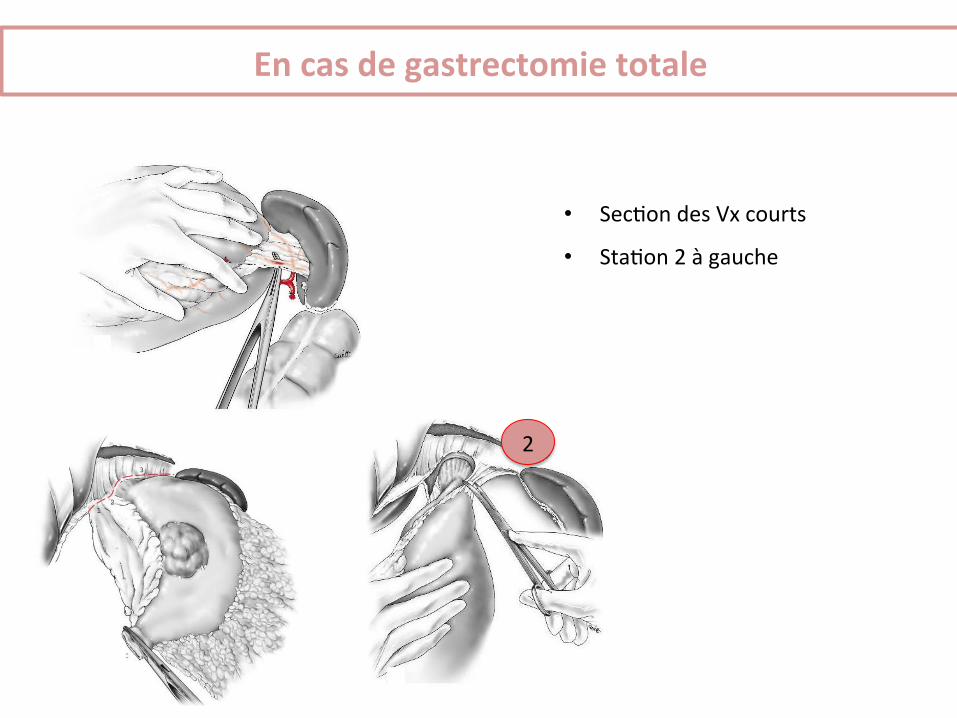
• Sec+on des Vx courts
• Sta+on 2 à gauche
En cas de gastrectomie totale
2
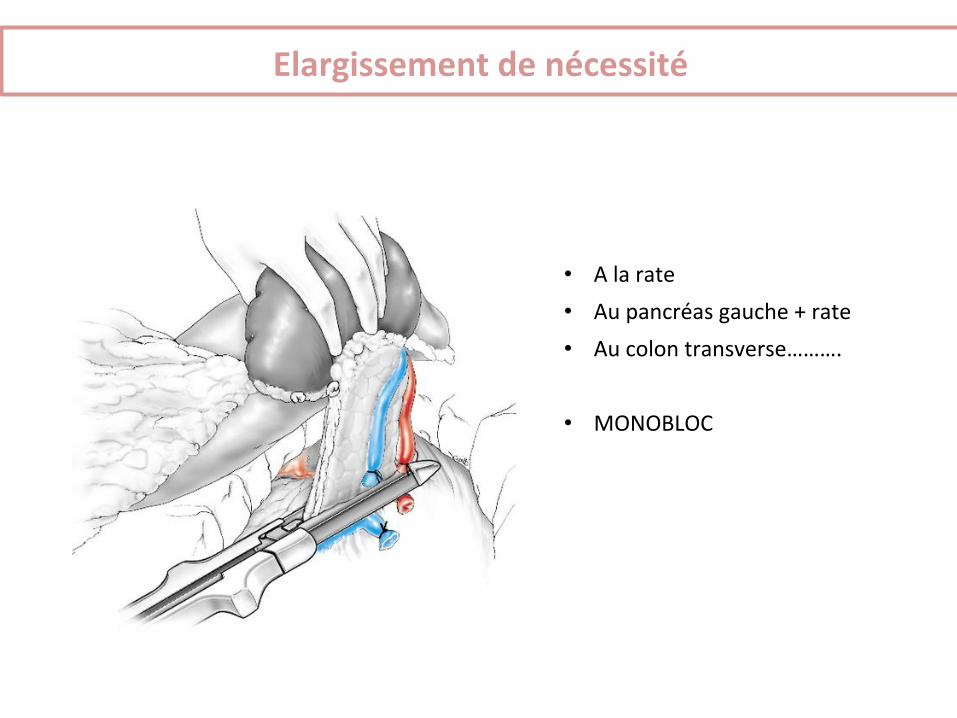
• A la rate • Au pancréas gauche + rate • Au colon transverse……….
• MONOBLOC
Elargissement de nécessité
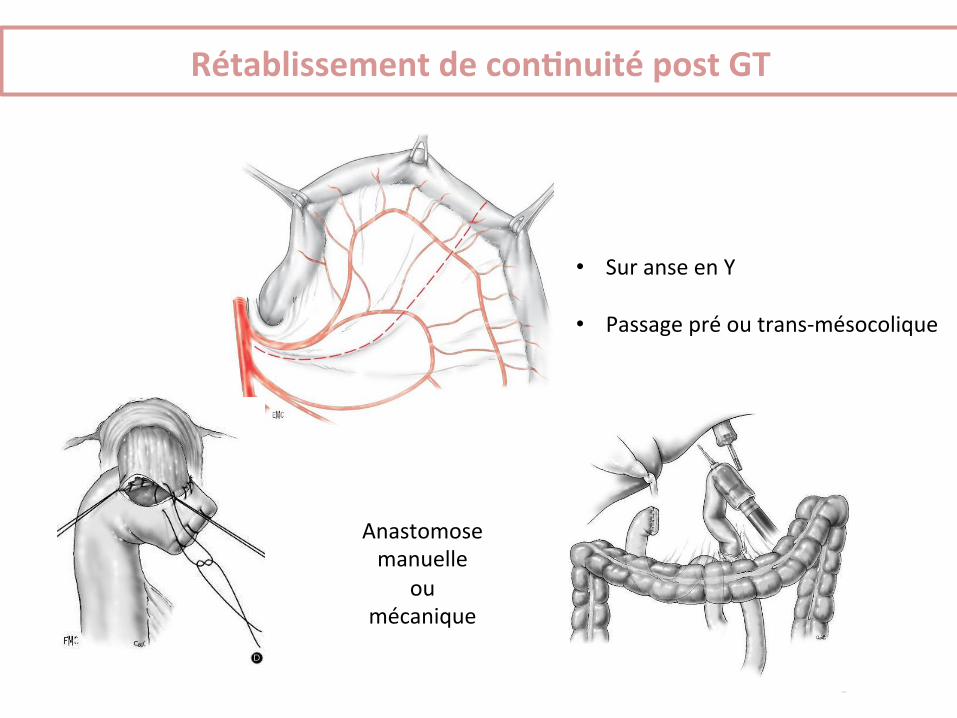
• Sur anse en Y
• Passage pré ou trans-‐mésocolique
Anastomose manuelle
ou mécanique
Rétablissement de conHnuité post GT
• Le curage D2 est le curage de référence • Si une GT est nécessaire,
la préservaHon du pancréas et de la rate doit être privilégiée • > 25 ganglions
Soins post opératoires
• Gastrectomie totale – Pas de SNG – Abla+on SAD J2, péridurale J3 – Début boissons J5 si RAS sinon TDM opacifié – Alimenta+on orale J6 (régime frac+onné/mixé puis pauvre en fibres); PEC diété+cienne
– Pas de jéjunostomie systéma+que – Vitamine B12 4000 UI / 4 mois à vie
Soins post opératoires
• Gastrectomie par+elle – Pas de SNG – Abla+on SAD J2, péridurale J3 – Boissons J1 500 ml puis sans limita+on J2 si ok – Alimenta+on J2 frac+onné, texture molle puis pauvre en fibres J3
– Pas de jéjunostomie
Troubles fonc+onnels
• Sd « pe+t estomac » – plénitude gastrique douloureuse pendant les repas
• « dumping syndrome » – Sd post-‐prandial précoce et tardif
• diarrhées