Embed Size (px)
Citation preview

Gut 1996; 39: 684-689
Increased production of tumour necrosis factor-oL,interleukin-11, and interleukin-6 bymorphologically normal intestinal biopsies frompatients with Crohn's disease
J-M Reimund, C Wittersheim, S Dumont, C D Muller, J S Kenney, R Baumann,P Poindron, B Duclos
Serviced'Hepatogastro-enterologie etd'Assistance Nutritive,CHRU Hautepierre,67098 Strasbourg,Cedex, FranceJ-M ReimundC WittersheimR BaumannB Duclos
Departementd'Immunologie,Immunopharmacologieet Pathologie, Centrede RecherchesPharmaceutiques,67401 Illkirch-Graffenstaden, FranceJ-M ReimundS DumontP Poindron
Unite de RechercheINSERM U381,Avenue Moliere, 67000Strasbourg Cedex,FranceJ-M ReimundB Duclos
Laboratoire deBiophysique,U.R.A. 491 du CNRS,Centre de RecherchesPharmaceutiques,67401 lllkirch-Graffenstaden, FranceC D MullerJ S Kenney
Antibody Solutions,HalfMoon Bay, CA,USAJ S KenneyCorrespondence to:Dr J-M Reimund,Departementd'Immunologie,Immunopharmacologie etPathologie, Centre deRecherchesPharmaceutiques, 74,Route du Rhin, 67401Illkirch-Graffenstaden,France.
Accepted for publication30 May 1996
AbstractBackground-Increasing evidence pointsto a important role for inflammatory cyto-kines for the pathogenesis of Crohn'sdisease.Aim-To compare the secretion rate oftumour necrosis factor-a (TNF-a),interleukin-1 (IL-1 0) and interleukin-6(IL-6) by morphologically normal andinflamed intestinal mucosa from patientswith Crohn's disease.Results-Organ cultures of intestinalbiopsy specimens taken from areas ofaffected mucosa from patients withCrohn's disease spontaneously producedincreased amounts of TNF-a, IL-1,B, andIL-6 compared with controls but alsobiopsy specimens taken in macroscopicallyand microscopically unaffected areas inthe same patients. Concentrations ofIL-1Pand IL-6 measured in the supernatant fluidof biopsy cultures were positively corre-lated with the degree of tissue involvementmeasured by both endoscopic andhistological grading. By contrast, TNF-aconcentrations were not correlated toendoscopic and histological grading.Conclusions-These consistently raisedTNF-a, IL-1"P and IL-6 secretions bynormal appearing mucosa from patientswith Crohn's disease provide evidence fora sustained immune stimulation inCrohn's disease even in the absence ofpatent inflammation. The results shed anew light on the role of inflammatorycytokines in the onset of intestinal tissuedamage in Crohn's disease and suggestthat the range of intestinal lesions inCrohn's disease may be wider than sus-pected on the basis of regular endoscopicand histological examinations.(Gut 1996; 39: 684-689)
Keywords: Crohn's disease, cytokines, organ cultures,inflammation.
Several factors have been suggested as possibleinitiating events in the development of inflam-matory bowel disease, including bacterial orviral organisms, dietary products and environ-mental toxins. These factors are suspected - ingenetically prediposed people - to initiate asequence of chronic immunological processesthat perpetuate a prolonged intestinal immune
response leading to tissue injury and thesubsequent clinical symptoms.
Early recurrence of Crohn's disease afterileal resection and ileocolonic anastomosis inapparently normal intestinal tissue,l and thefinding of granulomas even in endoscopicallynormal areas of mucosa,2 suggest that localsynthesis ofinflammatory mediators may occurin morphologically normal mucosa of patientswith Crohn's disease and that the range ofCrohn's disease may be larger than detected byconventional endoscopic and histologicalexaminations. Among the numerous solublebiochemical mediators released by activatedintestinal cells, particular attention has beengiven to macrophage derived inflammatorycytokines. Recent studies of inflamed mucosafrom patients with inflammatory bowel diseasehave identified intestinal activated macro-phages as the main producers of tumournecrosis factor-ct (TNF-ot) and interleukin- 11p(IL-i1 P),3 as well as the major producers ofinterleukin-6 (IL-6) in conjunction withepithelial cells.3To date, no data on the simultaneous release
of TNF-ot, IL-13, and IL-6 by organ culturesfrom intestinal biopsy specimens from bothnormal appearing (endoscopically and histo-logically) and affected intestinal mucosa frompatients with Crohn's disease has been con-sidered. We therefore examined the spon-taneous release of these three cytokines bymacroscopically and microscopically un-affected intestinal mucosa from patients withCrohn's disease, and compared the results withthose from affected mucosa from patients withCrohn's disease and normal control intestinaltissue.
Patients and Methods
INTESTINAL BIOPSIES
Thirty five patients with Crohn's disease wereprospectively included. The Table shows theclinical data and treatments at the time of thestudy. The activity of disease was assessedaccording to Van Hees et al.6 No patient hadextraintestinal manifestations of Crohn'sdisease or extraintestinal infection. Further-more, serological studies concerning Yersiniaenterocolitica and cytomegalovirus infection, aswell as stool cultures for Clostridium difficilewere negative in all cases. Small bowel andcolonic biopsy specimens were obtained from
684
on July 6, 2020 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.39.5.684 on 1 Novem
ber 1996. Dow
nloaded from

Increased production oftumour necrosis factor-oa, ILI -/3, and IL-6 in Crohn 's disease
Clinical characteristics and treatment at the time ofinclusion of the patients with Crohn's disease (CD). Thedisease activity was based on the Van Hees index6
Patients with CD(n=37)
Age (y) (mean (range)) 36 (20-57)Men/women 18/19Disease activity (n):
Severe 10Moderate 14Mild 13
Bowel involvement (n):Ileum alone 8Colon alone 10Ileocolonic disease 19
Current treatment:Steroids > 10 mg/day 13Azathioprine+steroids 3Mesalazine 10No medication 11
macroscopically and microscopically non-
affected (n=26) or affected (n=26) areas of theintestinal mucosa during colonoscopy inpatients with Crohn's disease. In 17 patientsbiopsy specimens were taken in both affectedand unaffected mucosa. All patients required a
colonoscopy for medical reasons. The controlgroup included 26 patients without inflam-matory bowel disease who underwent endos-copy for polyp or colon cancer surveillance(n=8), irritable bowel syndrome (n= 12), lowergastrointestinal tract bleeding (n=4), andpreoperative controls from female patients withnon-neoplastic extra-intestinal pelvic mass
(n=2). All controls were free of intestinaldisease. In each patient a set of six biopsyspecimens was taken, two were fixed informalin for histological assessment, four were
placed at 4°C in a medium consisting of Ca21and Mg2+ free (CMF) Hank's solution (Gibco-BRL, Cergy Pontoise, France), supplementedby 100 IU/ml penicillin and 100 pug/ml strepto-mycin (Diamant, Puteaux, France).
ENDOSCOPIC GRADING
The severity of inflammation was endos-copically graded according to Wardle et al. 7 Thefour point scale corresponds to: (1)macroscopically normal, (2) granular mucosa,contact bleeding, (3) erythematous and oede-matous mucosa, aphtoid or superficial ulcer-ation, (4) deep ulceration with slough, andinflammatory pseudopolyp formation. Biopsyspecimens were taken from both inflamed(graded 3 or 4), and quiescent (graded 1) areas.
Grade 2 mucosa was not considered for thisstudy to avoid an overlap in biopsy groups.
TISSUE CULTURE
After collection, biopsy specimens were trans-ferred to the laboratory. Within a maximal lag ofthree hours after biopsy, tissue was gentlywashed three times in CMF-Hank's mediumsupplemented by antibiotics, blotted carefully,weighed, and individually placed in 24 welltissue culture plates (1 ml culture medium/well).The culture medium consisted of RPMI-1 640(Gibco) supplemented by 10% heat inactivatedfetal calf serum (Gibco), 2 mM L-glutamine(Gibco), penicillin (100 IU/ml), and streptomy-
cin (100 ,ug/ml). After 18 hours' culture at 37°Cin a humidified 95% air/5%/o CO2 atmosphere,medium was removed, filtered and stored at-80°C until required for cytokine assays.
HISTOLOGY AND HISTOLOGICAL
INFLAMMATION SCORINGBiopsy specimens from each patient were fixedin 10% buffered formalin and embedded inparaffin wax after dehydration, clearing, andimpregnation. Subsequent 4 ,um sections werestained with haematoxylin and eosin. Morpho-metry and calculation of an inflammation scorewere performed. The morphometric assess-ment used a method for the quantitative exam-ination of intestinal mucosal biopsies todetermine an index related to the surface tovolume ratio of the intestinal mucosa as pre-viously described by Dunnil and Whitehead,8and specifically used in inflammatory boweldisease by Dunne et al.9 This technique gavean index of surface area and an index ofmucosal volume. All biopsy specimens forhistology were assigned an overall inflam-mation score adapted from Riley et al. 0 Tissueexamination was performed blindly accordingto the diagnosis and the endoscopic inflam-mation score. Sections were graded using fivehistological features: polymorphonuclear cellinfiltrate in the lamina propria, crypt abscesses,surface epithelium integrity, chronic inflam-matory cell infiltrate (mononuclear cells in thelamina propria), and crypt architecturalintegrity. As this study included only Crohn'sdisease the criterion of mucin depletion usedby Riley et al'` was not taken into account.Each histological feature was graded on a fourpoint intensity scale: none (1 point), mild (2points), moderate (3 points), or severe (4points); therefore, the overall inflammationscore ranged from 5 to 20. Only the biopsyspecimens in which the histological score was5 were used in the control group as well as inthe group of normal appearing biopsies frompatients with Crohn's disease. However, mor-phometry showed that in inflamed mucosafrom patients with Crohn's disease the surfacearea was reduced and the mucosal volume wassignificantly (X 1 *5) increased compared withnormal appearing areas in the patients.
In Crohn's disease, overall (affected andnon-affected mucosa) endoscopic and histo-logical grades were positively correlated (r=0 9;p<o0oool).The structural integrity was assessed by
standard histology and by measurement oflactate dehydrogenase release according toWardle et al.7 After a 18 hour culture nohistological changes were noted as comparedto precultured tissue. Furthermore, the releaseof lactate dehydrogenase in cultured tissueswas significantly lower than in unculturedtissues (data not shown).
IMMUNOASSAYS FOR CYTOKINES
Interleukin production (TNF-ot, IL- 1 f, andIL-6) was measured with specific immuno-assays. Each enzyme linked immunosorbent
685
on July 6, 2020 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.39.5.684 on 1 Novem
ber 1996. Dow
nloaded from

Reimund, Wittersheim, Dumont, Muller, Kenney, Baumann, et al
assay (ELISA) used two monoclonal anti-bodies directed to two different epitopes on thecorresponding interleukin molecule. Themonoclonal antibodies were developed usingpurified recombinant cytokine and do not crossreact with a panel of related and non-relatedcytokines."' Quantitative evaluation of inter-leukins secreted by monocytes was achieved byELISA using conditions described by Kenneyet all" with minor modifications to improve thesensitivity and specificity: Tween (500 ,l/l ofphosphate buffered saline) was preferred tothimerosal in the incubation, blocking, andwashing buffer. Polyvinyl chloride plates(Costar, No 2596) were coated with 50 pl perwell of antibodies (15 ,ug/ml) and incubatedovernight at 4°C. After three washing steps,and the non-specific saturation step, 25 plstandard (human recombinant cytokine) orsample were added to 25 pl secondary bio-tinylated monoclonal antibody (2 ,ug/ml) andthe mixture incubated for two hours at roomtemperature. After the washing steps, 50 pA ofperoxidase-streptavidin (1:3000 in PBS-Triton) was added and the mixture allowed tostand for one hour at room temperature. Acolorimetric reaction (OD at 450 nm) usingo-phenylenediamine dihydrochloride as per-oxidase substrate was performed. Sensitivity ofthe assays was below 20 pg/ml and all samplesgave values within the working range of thestandard curves. Concentrations (pg/ml) ofunknown samples were computed by inter-polation with a standard curve run on eachplate (curve fitting: four parameter logistic). Allsamples were analysed in duplicate. Results ofcytokine concentrations in supernatant fluidswere expressed according to the weight of thecorresponding biopsy specimen (pg/mg tissue/ml culture medium) and the final result foreach patient corresponds to the mean of thefour individual biopsy cultures.
STATISTICS
Data are expressed as mean (SEM). Resultswere compared using Student's t test fornormally distributed data. Non-parametricdata were compared using the Mann-WhitneyU test or the Kruskal-Wallis test if more thantwo groups were compared. Linear regressionor the Spearman r test was used to assesscorrelation. The level of significance was takenas p<005.
Results
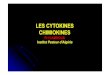
RELEASE OF TNF-Ot BY ORGAN CULTURESConcentrations of TNF-a measured in thesupernatant fluid of control mucosa were verylow (15-7 (5.4) pg/mg tissue) compared withaffected Crohn's disease mucosa (62-3 (11.8)pg/mg tissue) (p<0 001; Fig 1). Non-affectedmucosa samples from patients with Crohn'sdisease produced significantly higher amountsofTNF-a (39.4 (9.7) pg/mg of tissue; p<003)than those of controls. On the other hand theamounts were not significantly different fromaffected samples from patients with Crohn's
- 140
to 120
E 100E
CL 80
*°0 60CD
C 40
C 2000 0
= ControlM Unaffected mucosaM Affected mucosa
h *T
TNF-a IL-lp
Figure 1: Spontaneous release of TNF-ci and IL-1(3fromendoscopic biopsies of normal intestine (control; n=26),unaffected (endoscopically and histologicaly) (n=26) andaffected (n=26) mucosa ofpatients with Crohn's diseasemaintained in organ culturesfor 18 hours. Results areexpressed as mean (SEM) (*p<0.05; **p<0.01 v control).IL-1(8 release was significantly lower in unaffected than inaffected mucosa (p<0.004) whereas TNF-ct release washigh in the two groups (p=0-14).
disease (p=0 14; Fig 1). However, for patientsin whom biopsy specimens were taken fromboth affected and non-affected mucosa(n= 17), TNF-a released by affected areas sig-nificantly exceeded that released by normalappearing areas (Fig 2; p<0 03).
RELEASE OF IL- 1P BY ORGAN CULTURESSupernatants of 19 control biopsy specimenshad no detectable IL-1 13. The seven remainingcontrol intestinal biopsies spontaneouslyreleased small amounts of IL- 1P (5-6 (2.5) pg/mg tissue). Spontaneous secretion of IL-1 13 byaffected mucosa obtained from patients withCrohn's disease (99.8 (23.2) pg/mg tissue) wasmuch increased (Fig 1; p<0 002). Non-affected intestinal biopsy specimens frompatients with Crohn's disease released signifi-cantly higher IL- 1P concentrations (21.5 (5.4)pg/mg tissue) compared with controls(p<0.008). These concentrations were lowerthan those of biopsies from affected mucosa(p<0 004) in patients with Crohn's disease(Fig 1). When biopsies were collected in bothinflamed and macroscopically normal mucosain the same patients (n=17) IL- 13 was signifi-cantly higher in affected areas (Fig 2; p< 0O 1).
RELEASE OF IL-6 BY ORGAN CULTURES
Release of IL-6 was found in supernatants ofcultured intestinal biopsy specimens obtainedfrom controls (1 12.7 (11-5) pg/mg tissue). Foraffected Crohn's disease biopsy specimensIL-6 concentrations were significantly higher(1511-5 (451-5) pg/mg tissue) than samplesfrom control mucosa (Fig 3; p<0004). Biopsyspecimens from non-affected area producedsignificantly smaller amounts of IL-6 (286.2(55.5) pg/mg tissue) than those secreted byaffected Crohn's disease tissue (Fig 3; p<0-0 1).However, these concentrations were signifi-cantly higher than those of controls (p=0.005).When biopsies were performed in the samepatient in both affected and normal appearingmucosa, IL-6 concentrations were higher in
686
on July 6, 2020 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.39.5.684 on 1 Novem
ber 1996. Dow
nloaded from

Increased production oftumour necrosis factor-oa, ILl-p3, and IL-6 in Crohn's disease
1000P<0.03
100
Unaffected AffectedCD mucosa CD mucosa
TNF-a
10 000 rP<0.003
1000 K
100 [
10K
Unaffected AffectedCD mucosa CD mucosa
IL-l f
Unaffected AffectedCD mucosa CD mucosa
IL-6
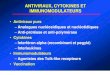
Figure 2: Individual concentrations of TNF-a, IL-1/3, and IL-6 (log scale) in the culture supernatantfluids of intestinal mucosafrom patients withCrohn's disease (n= 17): biopsy specimensfrom both normal appearing (unaffected) and inflamed (affected) areas in the same patient.
the supematants of organ culturestissue (Fig 2; p<0003).
CORRELATION OF CYTOKINE RELEASI
ENDOSCOPIC GRADE
IL-1P and IL-6 secretions were diffithree groups defined by endoscor(respectively p<0 01 and p<0 001Wallis) with a positive correlationcopic grade (Spearman r=0-61, pboth IL- 1 P and IL-6). Secretion of 'not different according to the endos(p=013).
CORRELATION OF CYTOKINE RELEASI
HISTOLOGICAL GRADE
Concentrations of IL-i P and IL-6correlation with histological(Spearman r=0.62, p<0001 forcontrast, TNF-ac did not show anywith histological grading (r=0 19, p
2000
ControlM Unaffected mucosaM Affected mucosa
K~~~~1500 _
1000 _-
500
IL-6
Figure 3: Spontaneous release ofIL-6from bi
normal intestine (control; n=26), unaffected(endoscopically and histologically) (n=26), a(n=26) mucosa ofpatients with Crohn's disecmaintained in organ culturesfor 18 hours. Reexpressed as mean (SEM) (**p<OO1 v contirelease was significantly lower in unaffected thCrohn's disease mucosa (p<O.O1).
Of inflamed
E TO
erent in the?iC gradingI, Kruskal-for endos-<0 001 forF-NF-ot was;copic score
E WITH
CORRELATION BETWEEN CYTOKINES
Concentrations of IL-i1P and IL-6 correlatedpositively with each other (r=0.58, p<0001).There was a weak correlation between IL-i1and TNF-a concentrations (r=043, p<0005)and no correlation between TNF-cx and IL-6concentrations (r=-015, p<03).
RELATION WITH OTHER VARIABLES
Cytokine production by mucosal samples werenot correlated to disease activity or duration,location of bowel involvement, previoussurgery, or type and duration of medical treat-ment (data not shown).
Discussionhad a high In the present study we documented a signifi-assessment cant inflammatory cytokine release by endos-both). By copically and histologically normal mucosa ofcorrelation patients with Crohn's disease: IL-6, IL-1,, and0.2 1). mainly TNF-ax concentrations were signifi-
cantly higher in supematant fluids from non-affected Crohn's disease mucosa than incontrols. This detection of high concentrationsof these cytokines by endoscopically andhistologically normal mucosa strongly suggeststheir involvement in the early step of intestinallesions in Crohn's disease. We also confirmedthat the spontaneous release of TNF-cx, IL- 1,and IL-6 by affected Crohn's disease mucosawas significantly higher than their release bycontrol biopsy specimens.'2-14
Concentrations ofTNF-ox were higher in thesupernatant fluid from both inflamed and non-inflamed Crohn's disease mucosa than in con-trols, with a slight increase in TNF-ot releaseby affected compared with non-affectedCrohn's disease intestine and lack of corre-lation with the histological index. The patho-
opsies of genic role of TNF-oL in Crohn's disease hastnd affected been controversial for a long time as a resultase of contrasting studies about this cytokine insults are6 inflammatory bowel disease. There were
Wan affected discrepancies between authors who investi-gated TNF-ox mRNA by the polymerase chain
1000 r
100 [-
ao
Q
U)
-
0,
mEC.
0
m
0)
0U)
10
1
0
._to
0*
,0
CDCDc
0CD
0U)
687
1
on July 6, 2020 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.39.5.684 on 1 Novem
ber 1996. Dow
nloaded from

688 Reimund, Wittersheim, Dumont, Muller, Kenney, Baumann, et al
reaction and did not find increased concen-trations of the transcripts in Crohn's diseasetissue,'5 16 and studies in which mucosalimmunoreactivity for TNF-u was measuredshowing an increased submucosal perivascularimmunoreactivity related to recruitment ofTNF-ox secreting cells.`7 The second group ofstudies were reinforced by the finding of raisedTNF-oL concentrations in the supernatantfluids of organ cultures of affected mucosafrom patients with Crohn's disease5 12 com-pared with normal controls (as confirmed inthe current study), as well as finding TNF-oamRNA expressing cells in the tissue of patientswith Crohn's disease.'8 These results are inaccordance with the recent report of the thera-peutic efficacy of chimeric anti-TNF-a mono-clonal antibodies in 10 patients with Crohn'sdisease refractory to steroids.'9 Taken together,these previous studies and the present onestrongly support the idea that TNF-oL is ofmajor importance in the pathogenesis ofCrohn's disease.Our data concerning TNF-ot production by
non-affected mucosa of patients with Crohn'sdisease contrast with those of Jones et al.'2However, they are in accordance with thefindings of Breese et al,'7 who reported thatTNF-ox secreting cells were increased inpatients with minor histological abnormalitiesand also showed a lack of a drug effect (exceptcyclosporine) on TNF-oa immunoreactivity.Furthermore, raised TNF-oa concentrationswere recently described by Peeters et alP0 in thesupernatant fluid of macroscopically normalileum and colon from patients with Crohn'sdisease.
Raised IL- 1 , and IL-6 productions byaffected tissue is universally recognised, 12-14but the finding of enhanced release of IL-1,and IL-6 release by non-affected Crohn'sdisease mucosa is more exciting. These resultsare in accordance with the recent data of Scheret al2' and Peeters et al.20 By contrast withTNF-ao production, we found a highly positivecorrelation between IL-i1P and IL-6 concen-trations and histological inflammatory grade.
This chronic production of inflammatorycytokines could be secondary to the stimu-lation of subepithelial macrophages by a non-specific antigen leaking from the lumen acrossthe epithelium as a result of increased epithelialpermeability. As suggested recently it may alsobe the result of an impaired down regulationof cytokine secretions.22Our results fit in with other data concerning
the questions of normality in intestinal mucosafrom patients with Crohn's disease. From amorphometric point of view, Goodman et a123first demonstrated a significant increase inplasma cell density in the lamina propria andin the volume of the lamina propria ofmacroscopically and histologically normalappearing rectal mucosa from patients withCrohn's disease. This study was reinforcedfrom a biochemical point of view by Dunne etal'0 who found, in addition to an increase inmucosal volume, a significant decrease indisaccharidase activity by apparently safe upperjejunal mucosa from patients with Crohn's
disease. More recently evidence has been pro-duced of enhanced complement secretion byunaffected jejunal tissue from patients withCrohn's disease,24 and increased phospholipaseA2 activity.25 Our study provides furtherevidence to support this concept of diffuseinvolvement of the whole intestinal tract inCrohn's disease. In addition, Nagel et al,26 inaccordance with previous reports,27 recentlydescribed early epithelial lesions in apparentlyunaffected mucosa from patients with Crohn'sdisease, detected by scanning electronmicroscopy but not by conventional lightmicroscopic examination; the light microscopeappearing to underscore mucosal integrity.Furthermore, it is interesting to keep in mindthat the pathological figures detected by theseultrastructural investigations may correspondto those observed in early apoptosis and toremember that cytokines participate in thesephenomenon ofprogrammed cell death.28The present results point out that mediators
involved in the initial steps of inflammatory/immune response (inflammatory cytokines)and known to induce cell death may be presentin the normal appearing mucosa from patientswith Crohn's disease. These cytokines repre-sent potential targets of pharmacological inter-vention and therefore, the development ofinflammatory cytokine inhibiting agents, notonly for the treatment of acute relapses but alsofor maintenance treatment.Taken together with recent medical litera-
ture, our results shed a new light on thepotential importance of inflammatory cytokinesin the perpetuation of the intestinal inflamma-tory response in Crohn's disease. They provideevidence for a persisting immune stimulationeven in the absence ofdemonstrable endoscopicor histological inflammation. Furthermore, thepresence of inflammatory cytokines - in par-ticular of TNF-a. - together with other lympho-kines in the normal appearing mucosa frompatients with Crohn's disease29 suggest someexplanation for the frequency of granulomas inotherwise endoscopically and histologicallynormal Crohn's disease mucosa,2 30 and, maybe, the high recurrence rate in the postoperativecourse of surgically treated patients withCrohn's disease.'
This work was partially supported by a fellowship award toJ-MR from BEAUFOUR Pharmaceutical Laboratories, Paris,France, and a grant from the Fondation AUPETIT, France.
1 Rutgeerts P, Geboes K, Vantrappen G, Beyls J, Kerremans R,Hiele M. Predictability of the postoperative course ofCrohn's disease. Gastroenterology 1990; 99: 956-63.
2 Dyer NH, Stansfeld AG, Dawson AM. The value of rectalbiopsy in the diagnosis of Crohn's disease. Scan Y Gastro-enterol 1970; 5: 491-6.
3 Reinecker HC, Steffen M, Witthoeft T, Pflueger I,Schreiber S, McDermott RP, et al. Enhanced secretion oftumor necrosis factor-alpha, IL-6, and IL-1 13 by isolatedlamina propria mononuclear cells from patients withulcerative colitis and Crohn's disease. Clin Exp Immunol1993; 94: 174-81.
4 Kusugami K, FukatsuA, Tanimoto M, Shinoda M, HarutajI,Kuroiwa A, et al. Elevation of interleukin-6 ininflammatory bowel disease is macrophage- and epithelialcell-dependent. Dig Dis Sci 1995; 40: 949-59.
5 Reimund JM, Wittersheim C, Dumont S, Muller CD,Baumann R, Poindron P, et al. Mucosal inflammatorycytokine production by intestinal biopsies in patients withulcerative colitis and Crohn's disease. J Clin Immunol1996; 16: 144-50.
6 Van Hees PAM, Van Elteren PH, Van Lier HJJ, VanTongeren JHM. An index of inflammatory activity inpatients with Crohn's disease. Gut 1980; 21: 279-86.
on July 6, 2020 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.39.5.684 on 1 Novem
ber 1996. Dow
nloaded from

Increased production of tumour necrosis factor-a, ILI-,B, and IL-6 in Crohn's disease 689
7 Wardle TD, Hall L, Tumberg LA. Use of coculture ofcolonic mucosal biopsies to investigate the release ofeicosanoids by inflamed and uninflamed mucosa frompatients with inflammatory bowel disease. Gut 1992; 33:1644-51.
8 Dunnil MS, Whitehead R. A method for the quantitationof small intestinal biopsy specimens. J Clin Pathol 1972;25: 243-6.
9 Dunne wT, Cooke WT, Allan RN. Enzymatic and morpho-metric evidence for Crohn's disease as a diffuse lesion ofthe gastrointestinal tract. Gut 1977; 18: 290-4
10 Riley SA, Mani V, Goodman MJ, Dutt S, Herd ME.Microscopic activity in ulcerative colitis: what does itmean? Gut 1991; 32: 174-8.
11 Kenney JS, Masada MP, Eugui EM, Delustro BM,Mulkins MA, Allison AC. Monoclonal antibodies tohuman recombinant interleukin 1 (ILl) 13: quantificationof IL1,B and inhibition of biological activity. J Immunol1987; 138: 4236-42.
12 Jones SC, Haidar A, Hagan P, Crabtree JE, Banks RE,Axon ATR, et al. Cytokine production in the mucosa ofpatients with inflammatory bowel disease. Eur JGastroenterolHepatol 1993; 5: 607-12.
13 Mahida YR, Wu K, Jewell DP. Enhanced production ofinterleukin 1 beta by mononuclear cells isolated frommucosa with active ulcerative colitis or Crohn's disease.Gut 1989; 30: 835-8.
14 Ligumsky M, Simon PL, Karmeli F, Rachmilewitz D. Roleof interleukin 1 in inflammatory bowel disease-enhancedproduction during active disease. Gut 1990; 31: 686-9.
15 Stevens C, Walz G, Singaram C, Lipman ML, Zanker B,Muggia A, et al. Tumor necrosis factor-a, interleukin-1 1,interleukin-6 expression in inflammatory bowel disease.Dig Dis Sci 1992; 37: 818-26.
16 Isaacs KL, Sartor IR, Haskill S. Cytokine messenger RNAprofiles in inflammatory bowel disease mucosa detectedby polymerase chain reaction amplification. Gastro-enterology 1992; 103: 1587-95.
17 Breese EJ, Michie CA, Nicholls SW, Murch SH,Williams CB, Domizio P, et al. Tumor necrosis factor-aproducing cells in the intestinal mucosa of children withinflammatory bowel disease. Gastroenterology 1994; 106:1455-66.
18 Autschbach F, Schurmann G, Qiao L, Merz H, Wallich R,Meuer SC. Cytokine messenger RNA expression andproliferation status of intestinal mononuclear cells in
noninflamed gut and Crohn's disease. Virchows Arch1995; 426: 51-61.
19 Van Dullemen HM, Van Deventer SJH, Hommes DW,Bijl HA, Jansen J, Tytgat GNJ, et al. Treatment of Crohn'sdisease with anti-tumor necrosis factor chymeric mono-clonal antibody (cA2). Gastroenterology 1995; 109:129-35.
20 Peeters M, D'Haens G, Ceuppens J, Peetermans W,Geboes K, Rutgeerts P. Increased proinflammatorycytokines in macroscopically normal ileum and colon inCrohn's disease. Gastroenterology 1995; 108: A891.
21 Sher ME, D'Angelo AJ, Stein TA, Bailey B, Bums G.Cytokines in Crohn's colitis. Am Jf Surg 1995; 169:133-6.
22 Schreiber S, Heinig T, Panzer U, Reinking R, Bouchard A,Stahl PD, et al. Impaired response of activated mono-nuclear phagocytes to interleukin 4 in inflammatory boweldisease. Gastroenterology 1995; 108: 21-33.
23 Goodman MJ, Skinner HM, Truelove SC. Abnormalities inthe apparently normal bowel mucosa in Crohn's disease.Lancet 1976; i: 275-8.
24 Ahrenstedt 0, Knutson L, Nilsson B, Nilsson-Ekdahl K,Odlind B, Hallgren R. Enhanced local production ofcomplement components in the small intestines ofpatients with Crohn's disease. N Engl Jf Med 1990; 322:1345-9.
25 Olaison G, Sj6dahl R, Tagesson C. Increased phospholipaseA2 activity of ileal mucosa in Crohn's disease. Digestion1988; 41: 136-41.
26 Nagel E, Bartels M, Pichlmayer R. Scanning electron-microscopic lesions in Crohn's disease: relevance for theinterpretation of postoperative recurrence. Gastro-enterology 1995; 108: 376-82.
27 Dvorak AM, Connell AB, Dickersin GR. Crohn's disease:a scanning electron microscopic study. Hum Pathol 1972;10: 165-77.
28 Majno G, Joris I. Apoptosis, oncosis, and necrosis. A reviewof cell death. AmJPathol 1995; 146: 3-15.
29 Breese E, Braegger CP, Corrigan CJ, Walker-Smith JA,MacDonald TT. Interleukin-2 and interferon gammasecreting cells in normal and diseased human intestinalmucosa. Immunology 1993; 78: 127-31.
30 Kindler V, Sappino AP, Gran GE, Piguet PF, Vassali P. Theinducting role oftumor necrosis factor in the developmentof bactericidal granulomas during BCG infection. Cell1989; 56:731-40.
on July 6, 2020 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.39.5.684 on 1 Novem
ber 1996. Dow
nloaded from