Embed Size (px)
Citation preview

La radioembolisation est morte …
Vive la radioembolization

La radioemebolisation est morte …
vive la SIRT (RIS)
• Selective Internal Radiation Therapy / Radiothérapie Interne Sélective
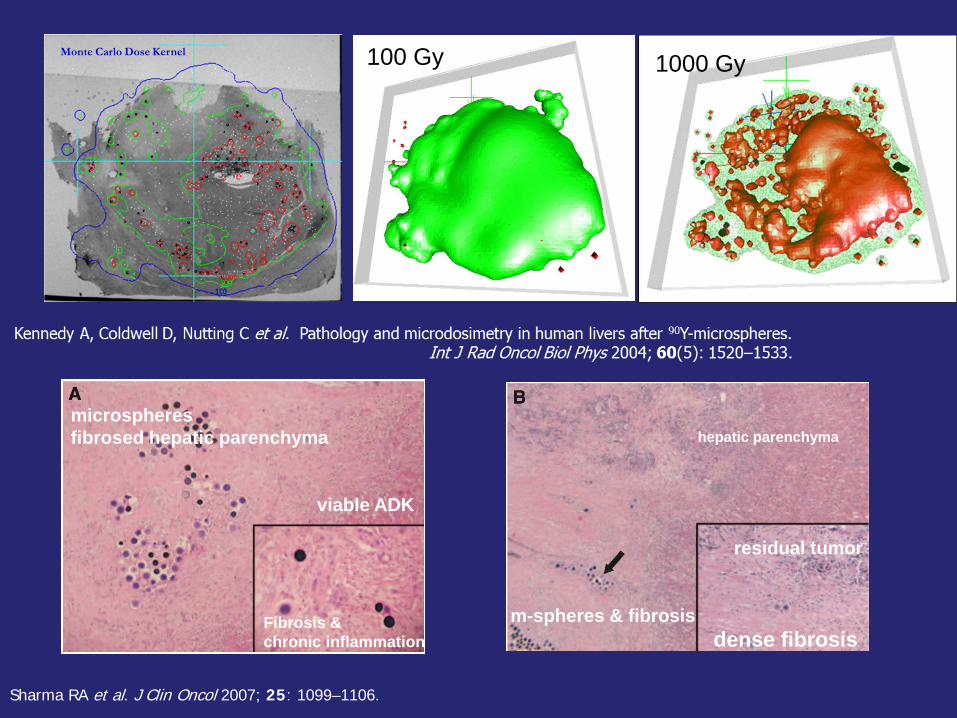
microspheres fibrosed hepatic parenchyma
viable ADK
Fibrosis & chronic inflammation
hepatic parenchyma
m-spheres & fibrosis dense fibrosis
residual tumor
Sharma RA et al. J Clin Oncol 2007; 25: 1099–1106.
1000 Gy 100 Gy
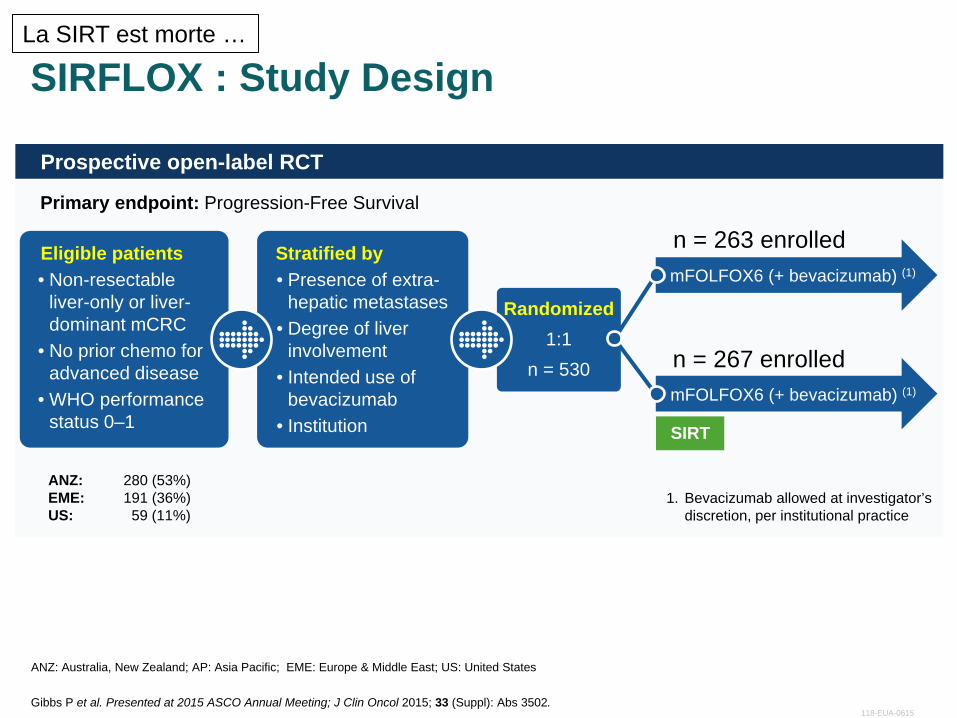
SIRFLOX : Study Design
ANZ: Australia, New Zealand; AP: Asia Pacific; EME: Europe & Middle East; US: United States
Prospective open-label RCT
Primary endpoint: Progression-Free Survival
ANZ: 280 (53%) EME: 191 (36%) US: 59 (11%)
1. Bevacizumab allowed at investigator’s discretion, per institutional practice
Gibbs P et al. Presented at 2015 ASCO Annual Meeting; J Clin Oncol 2015; 33 (Suppl): Abs 3502.
Stratified by • Presence of extra-
hepatic metastases • Degree of liver
involvement • Intended use of
bevacizumab • Institution
Randomized 1:1
n = 530
Eligible patients • Non-resectable
liver-only or liver-dominant mCRC
• No prior chemo for advanced disease
• WHO performance status 0–1
mFOLFOX6 (+ bevacizumab) (1)
SIRT
n = 263 enrolled
n = 267 enrolled mFOLFOX6 (+ bevacizumab) (1)
118-EUA-0615
La SIRT est morte …
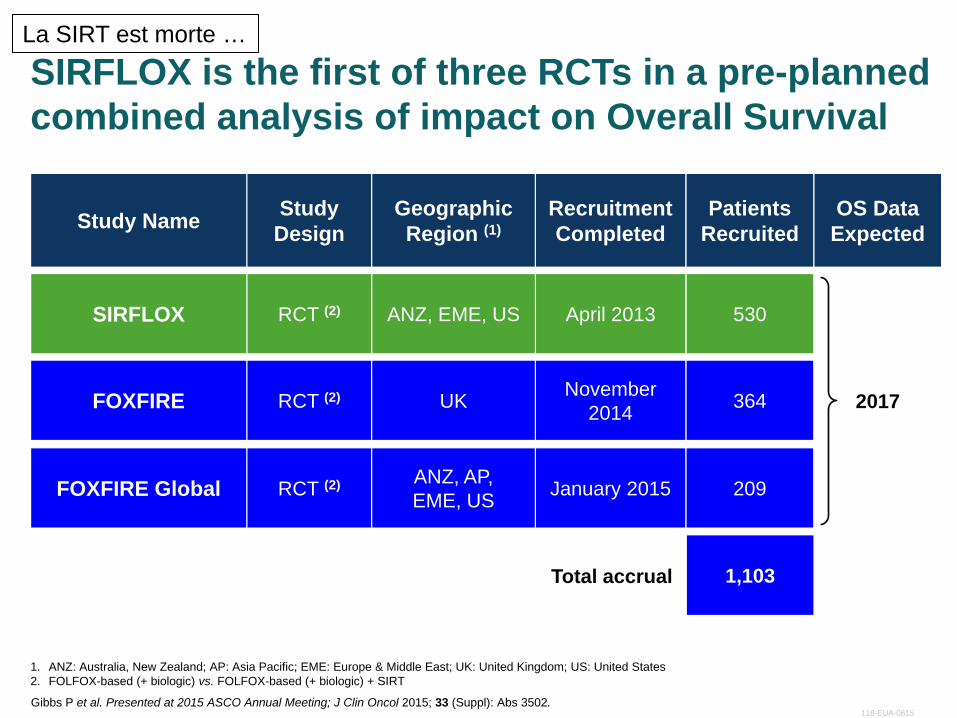
SIRFLOX is the first of three RCTs in a pre-planned combined analysis of impact on Overall Survival
1. ANZ: Australia, New Zealand; AP: Asia Pacific; EME: Europe & Middle East; UK: United Kingdom; US: United States 2. FOLFOX-based (+ biologic) vs. FOLFOX-based (+ biologic) + SIRT
Study Name Study Design
Geographic Region (1)
Recruitment Completed
Patients Recruited
OS Data Expected
SIRFLOX RCT (2) ANZ, EME, US April 2013 530
FOXFIRE RCT (2) UK November 2014 364
FOXFIRE Global RCT (2) ANZ, AP, EME, US January 2015 209
Total accrual 1,103
2017
Gibbs P et al. Presented at 2015 ASCO Annual Meeting; J Clin Oncol 2015; 33 (Suppl): Abs 3502. 118-EUA-0615
La SIRT est morte …
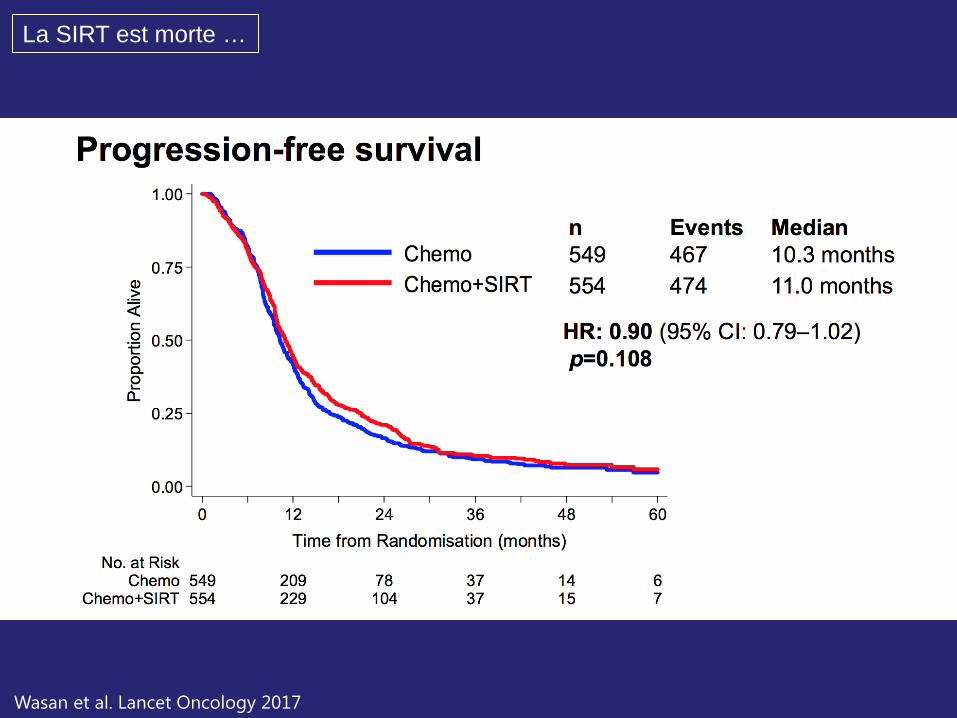
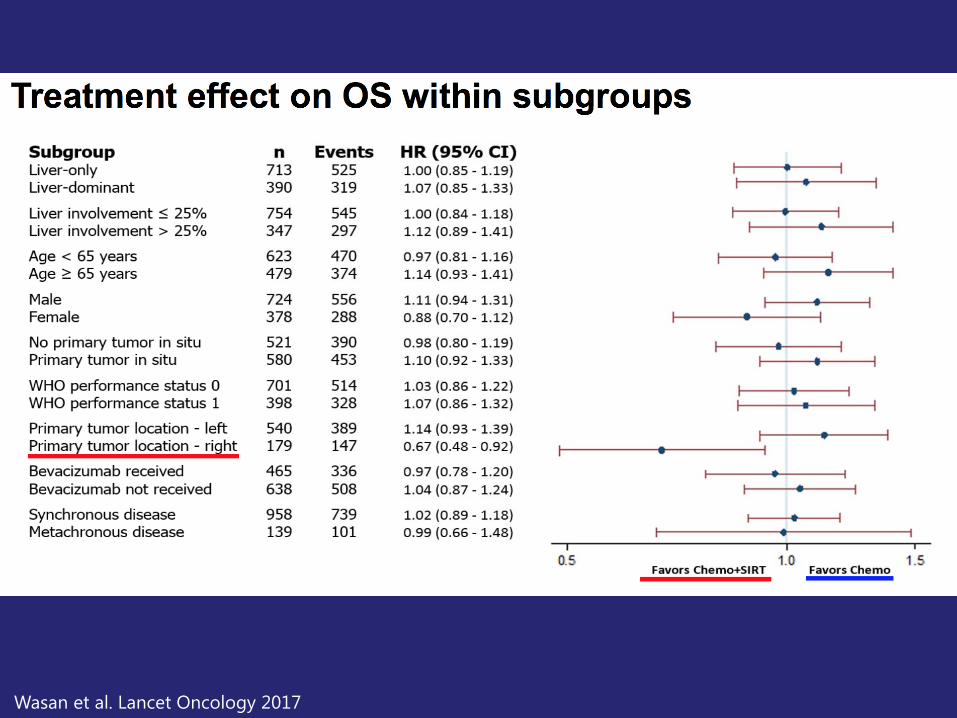
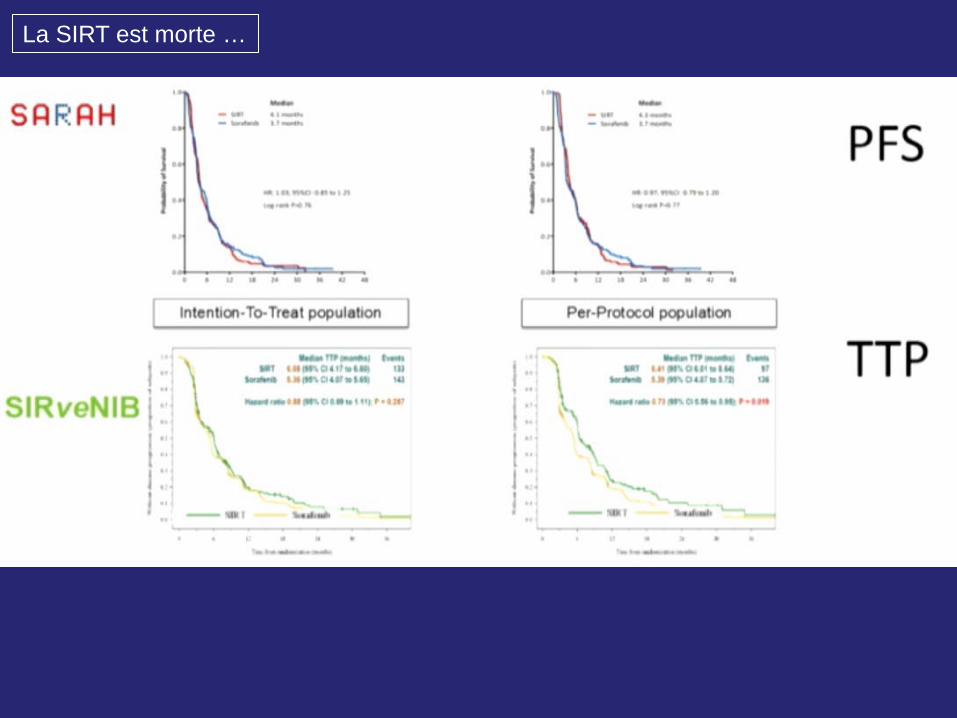
Wasan et al. Lancet Oncology 2017
La SIRT est morte …
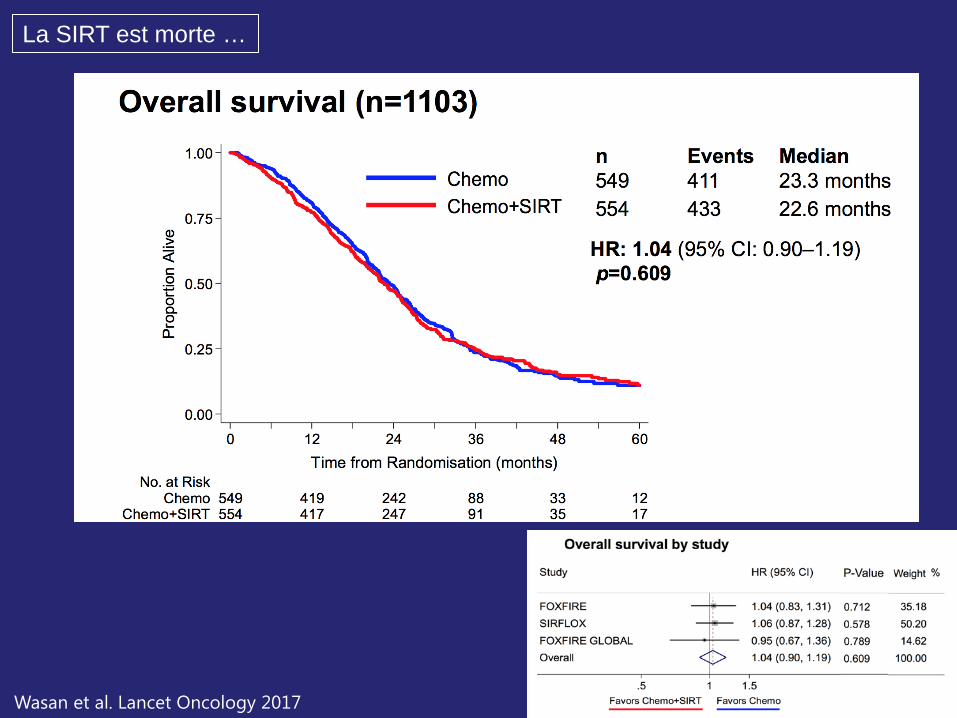
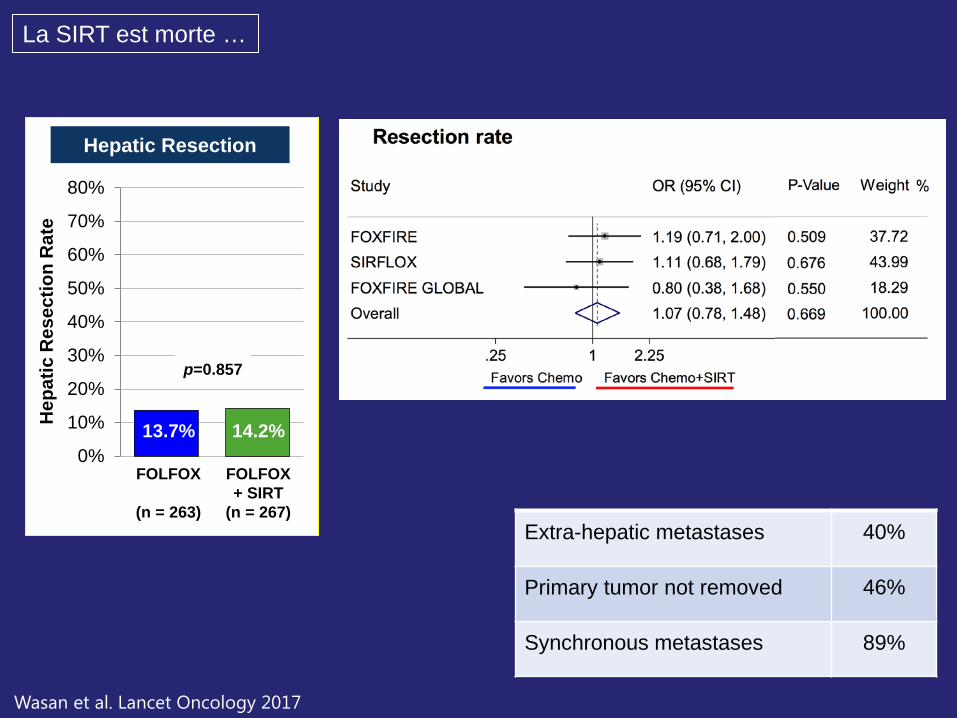
Wasan et al. Lancet Oncology 2017
La SIRT est morte …
Wasan et al. Lancet Oncology 2017
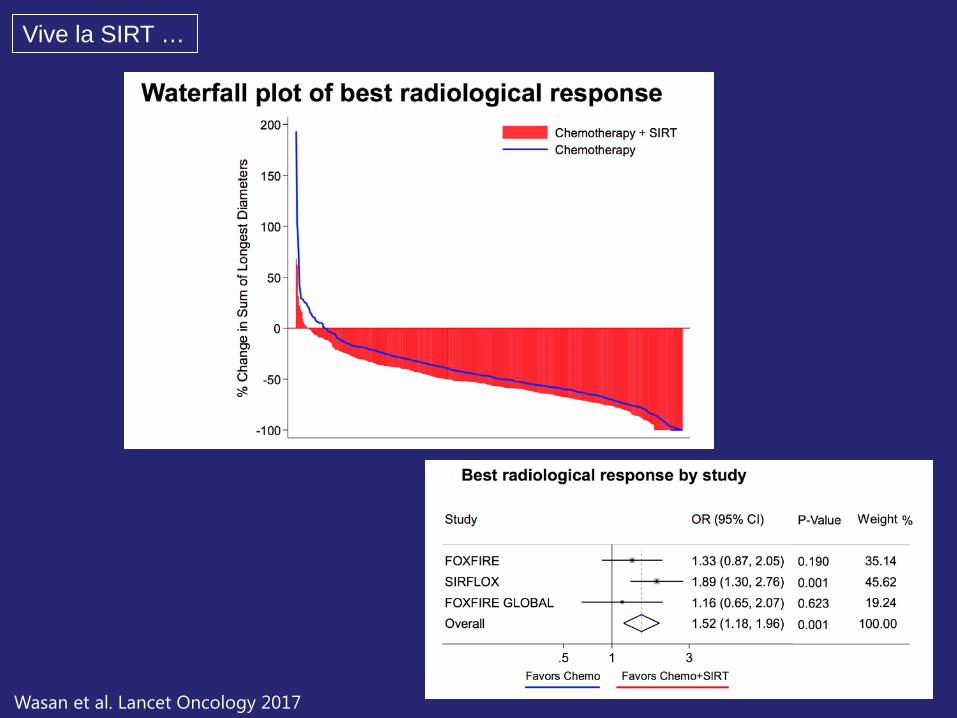
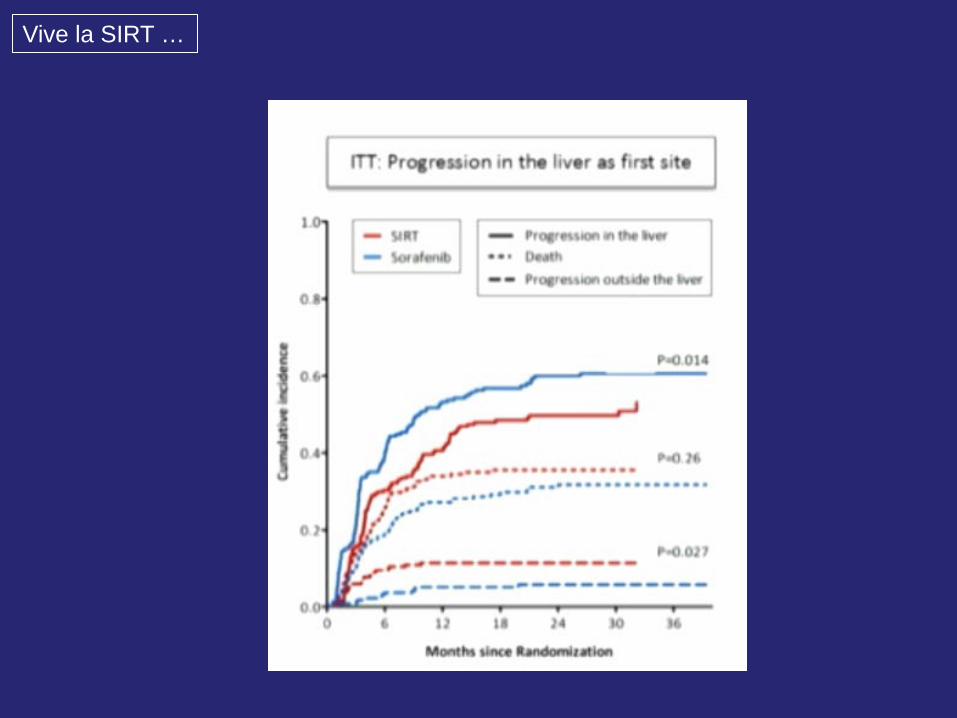
Vive la SIRT …
Wasan et al. Lancet Oncology 2017
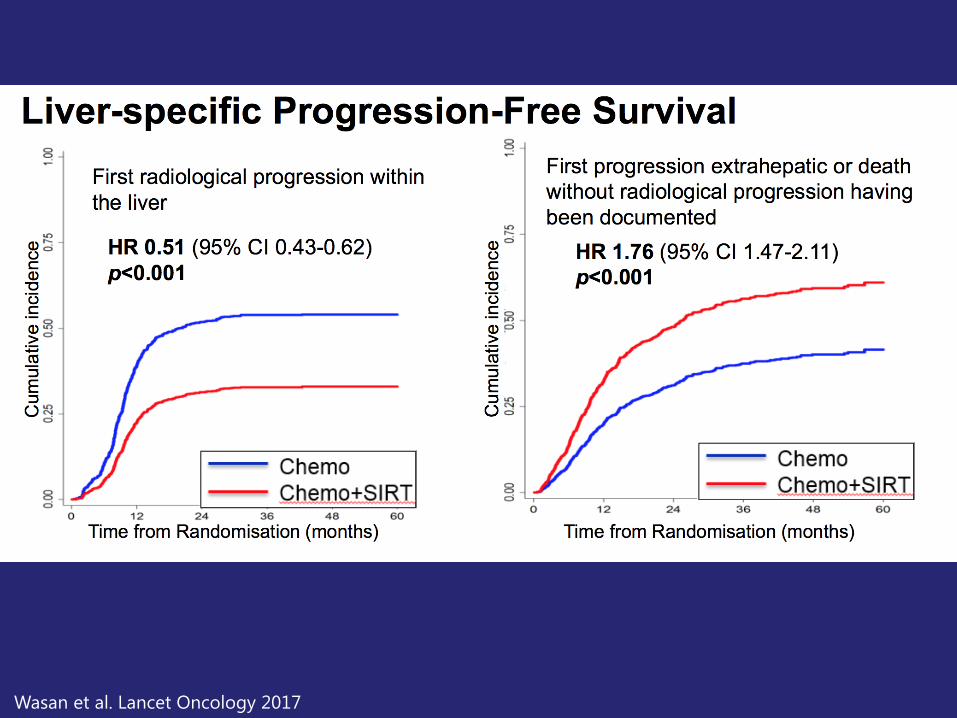
Wasan et al. Lancet Oncology 2017
Wasan et al. Lancet Oncology 2017
Hepatic Resection
FOLFOX + SIRT
(n = 267)
FOLFOX
(n = 263)
Hep
atic
Res
ectio
n R
ate
0%
10%
20%
30%
40%
50%
60%
70%
80%
p=0.857
13.7% 14.2%
La SIRT est morte …
Extra-hepatic metastases 40%
Primary tumor not removed 46%
Synchronous metastases 89%
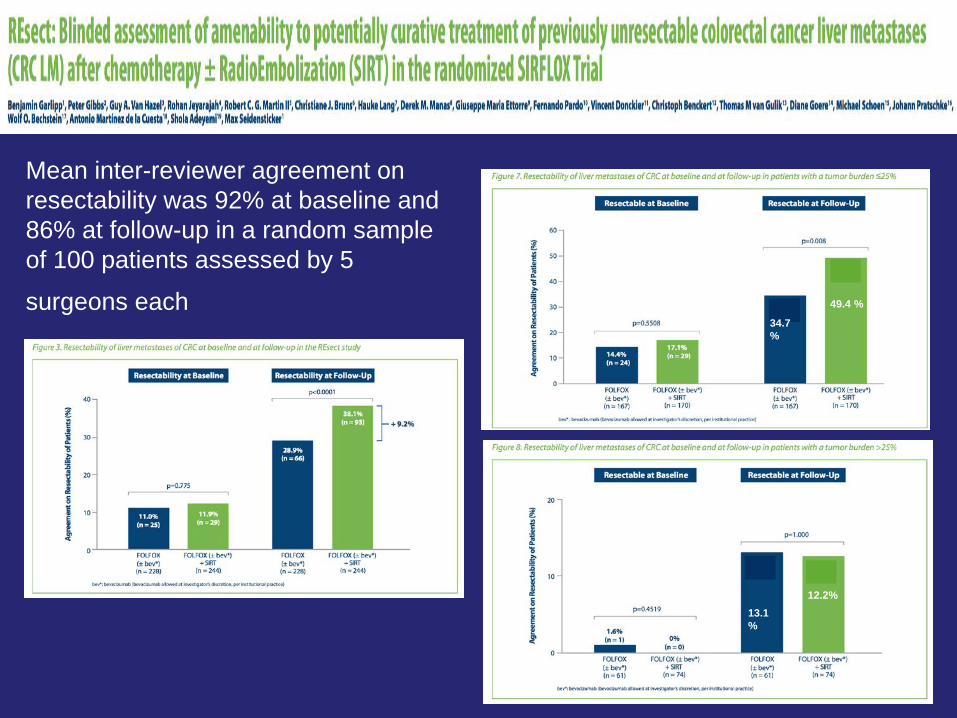
34.7%
49.4 %
13.1%
12.2%
Mean inter-reviewer agreement on resectability was 92% at baseline and 86% at follow-up in a random sample of 100 patients assessed by 5
surgeons each
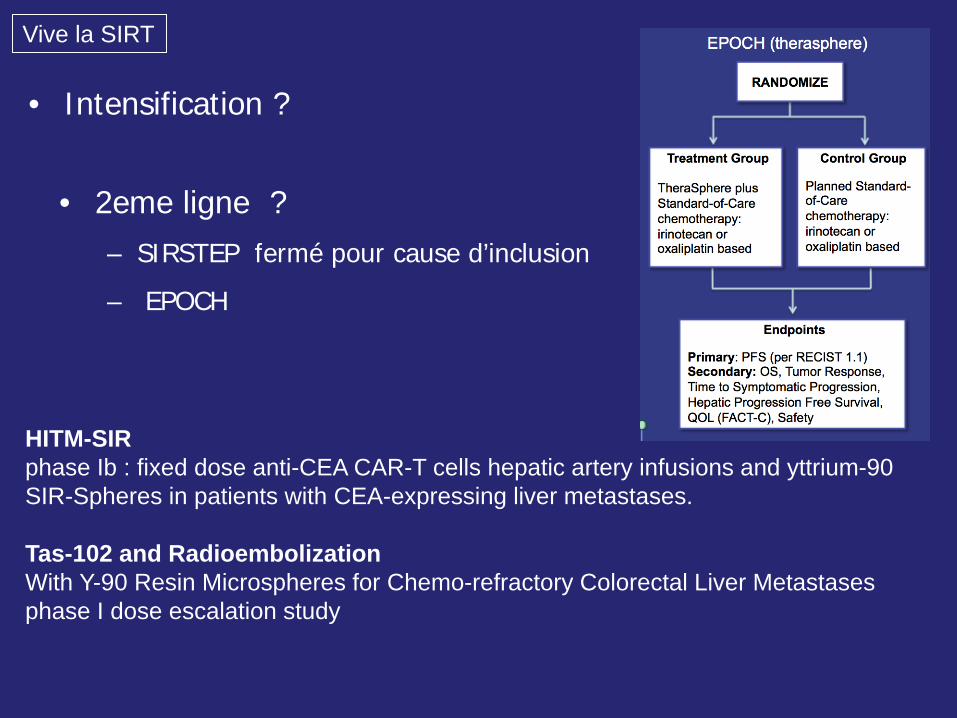
• 2eme ligne ? – SIRSTEP fermé pour cause d’inclusion
– EPOCH
HITM-SIR phase Ib : fixed dose anti-CEA CAR-T cells hepatic artery infusions and yttrium-90 SIR-Spheres in patients with CEA-expressing liver metastases. Tas-102 and Radioembolization With Y-90 Resin Microspheres for Chemo-refractory Colorectal Liver Metastases phase I dose escalation study
Vive la SIRT
• Intensification ?
La SIRT est morte …
Vive la SIRT …
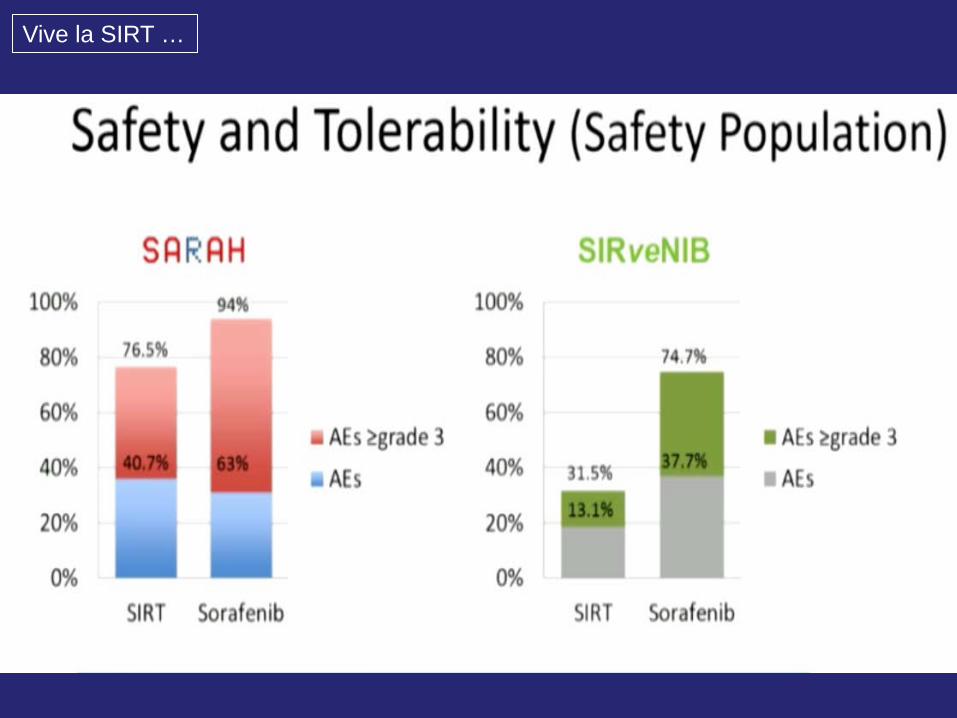
Vive la SIRT …
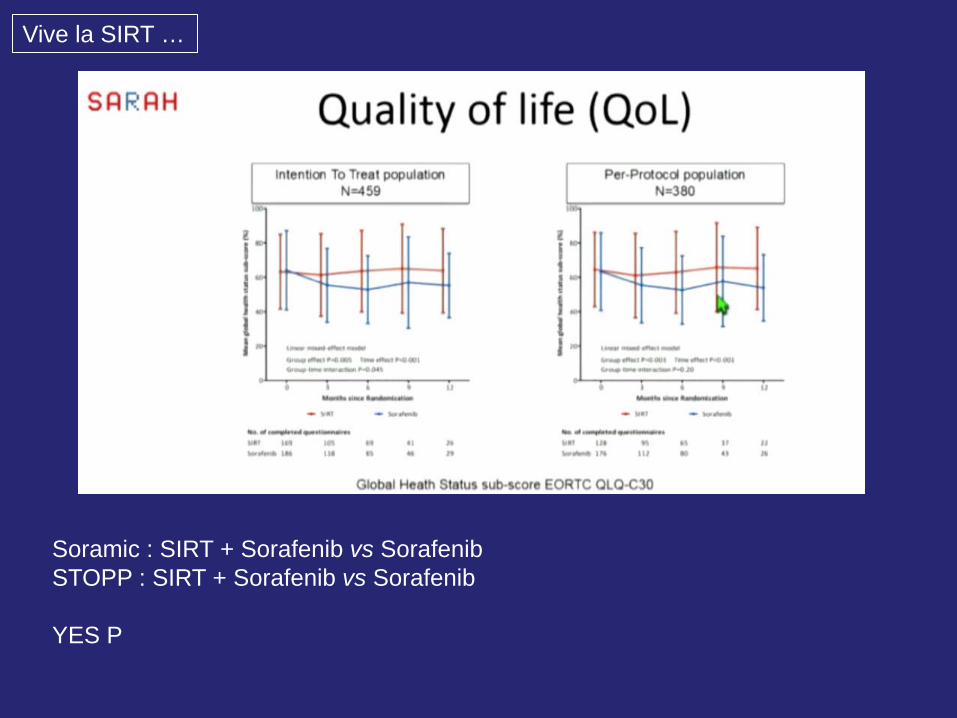
Soramic : SIRT + Sorafenib vs Sorafenib STOPP : SIRT + Sorafenib vs Sorafenib YES P
Vive la SIRT …
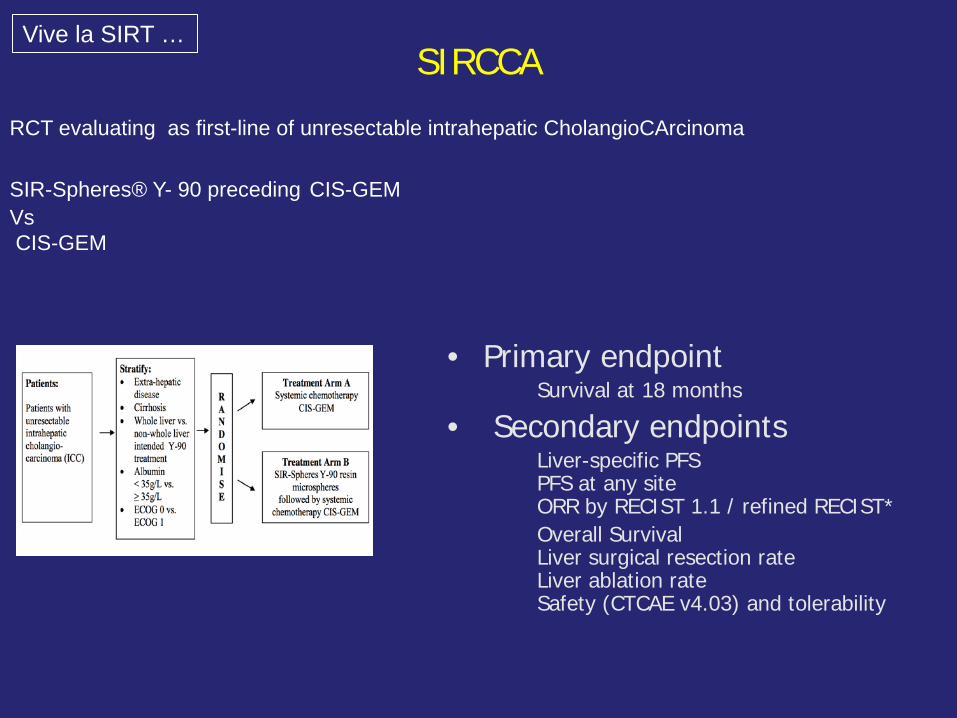
• Primary endpoint Survival at 18 months
• Secondary endpoints Liver-specific PFS PFS at any site ORR by RECIST 1.1 / refined RECIST* Overall Survival Liver surgical resection rate Liver ablation rate Safety (CTCAE v4.03) and tolerability
RCT evaluating as first-line of unresectable intrahepatic CholangioCArcinoma
SIR-Spheres® Y- 90 preceding CIS-GEM Vs CIS-GEM
SIRCCA Vive la SIRT …
Vive la SIRT
Quelle dose ? Quel isotope ? La nouvelle SIRT est elle de droite ou de gauche ?
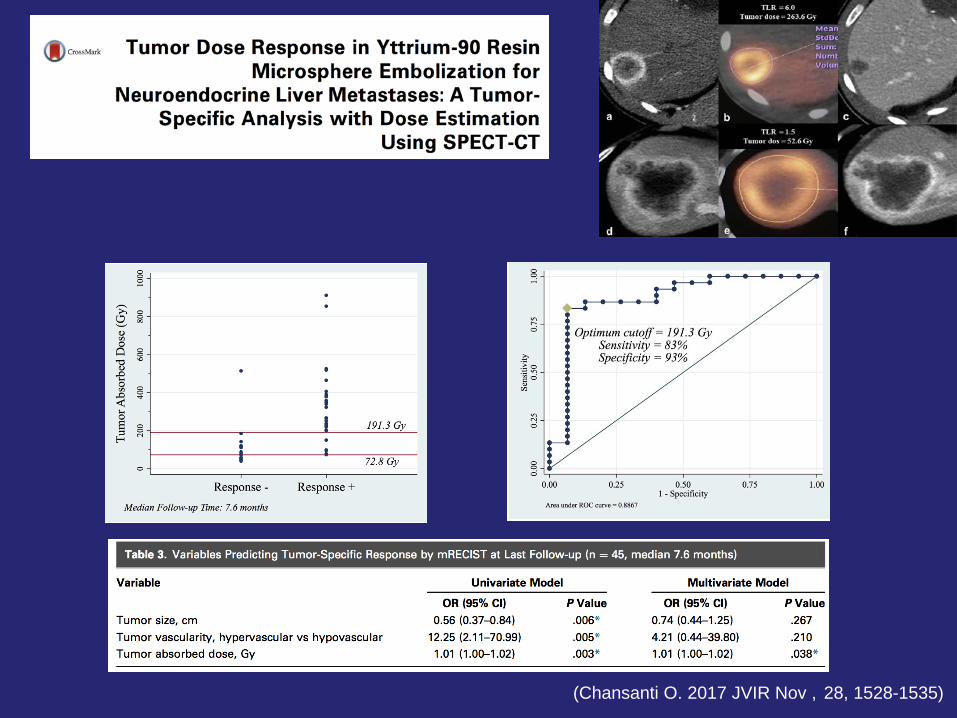
(Chansanti O. 2017 JVIR Nov , 28, 1528-1535)
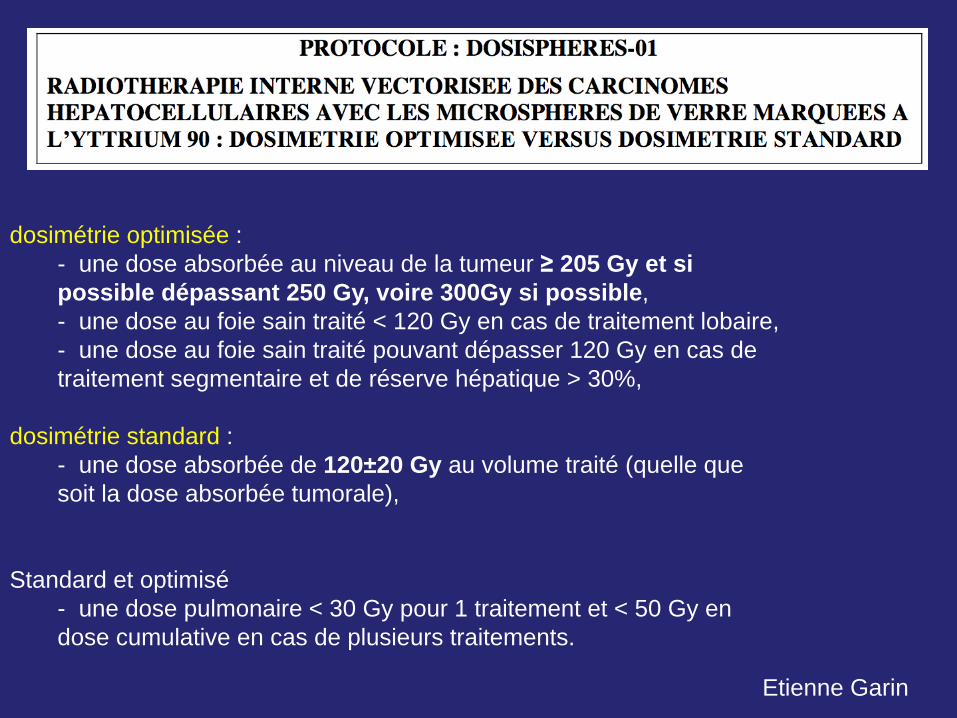
dosimétrie optimisée : - une dose absorbée au niveau de la tumeur ≥ 205 Gy et si
possible dépassant 250 Gy, voire 300Gy si possible, - une dose au foie sain traité < 120 Gy en cas de traitement lobaire, - une dose au foie sain traité pouvant dépasser 120 Gy en cas de traitement segmentaire et de réserve hépatique > 30%,
dosimétrie standard : - une dose absorbée de 120±20 Gy au volume traité (quelle que
soit la dose absorbée tumorale),
Standard et optimisé - une dose pulmonaire < 30 Gy pour 1 traitement et < 50 Gy en dose cumulative en cas de plusieurs traitements.
Etienne Garin
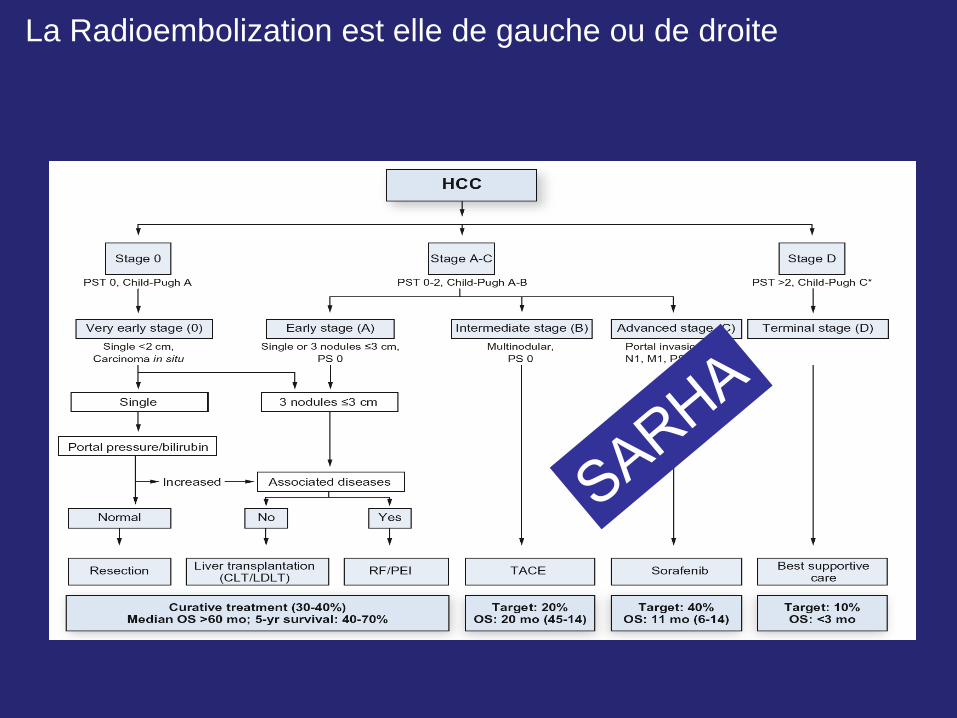
La Radioembolization est elle de gauche ou de droite
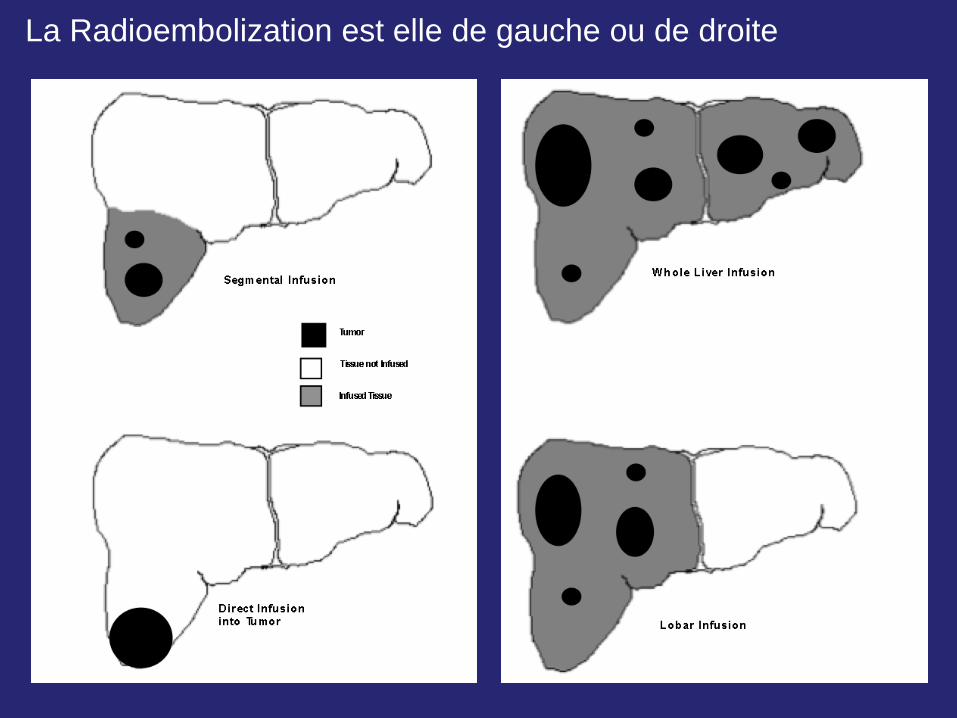
La Radioembolization est elle de gauche ou de droite
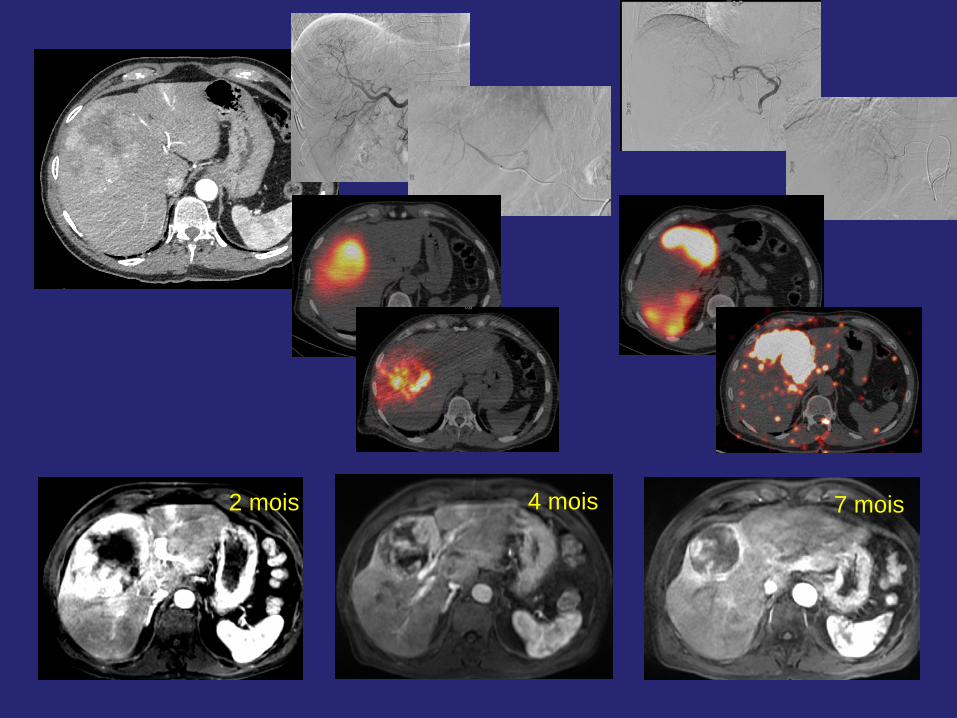
2 mois 4 mois 7 mois
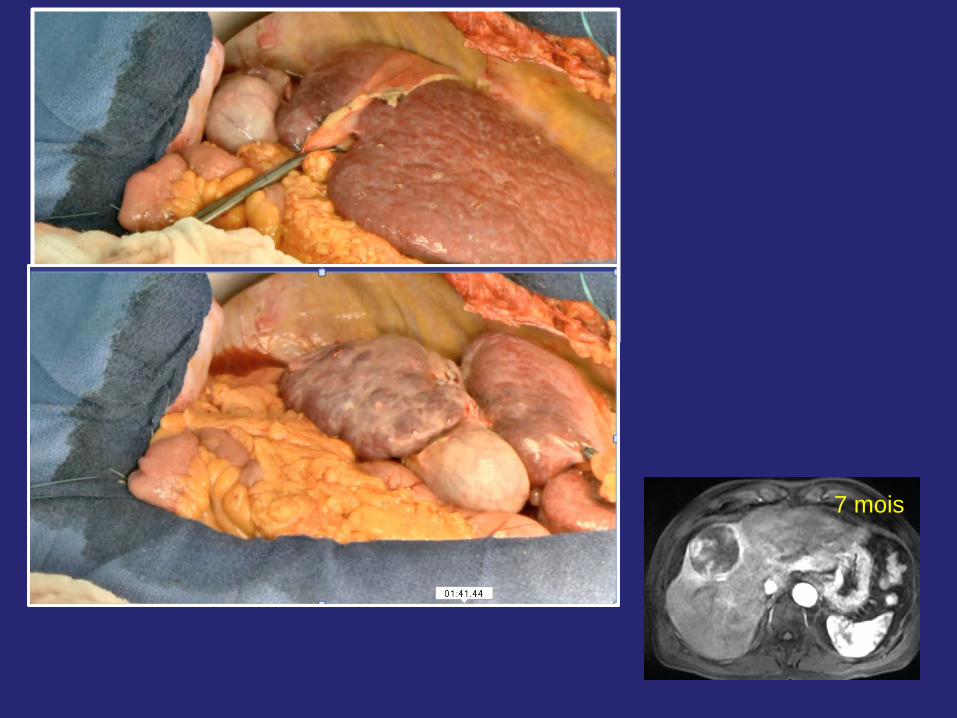
7 mois
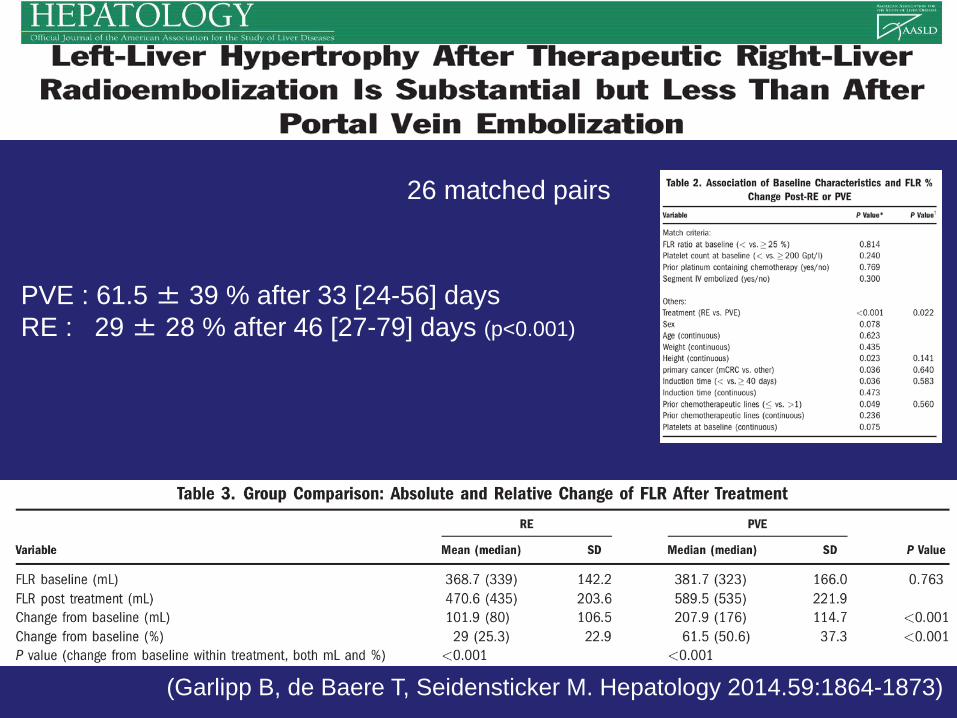
(Garlipp B, de Baere T, Seidensticker M. Hepatology 2014.59:1864-1873)
26 matched pairs
PVE : 61.5 ± 39 % after 33 [24-56] days RE : 29 ± 28 % after 46 [27-79] days (p<0.001)
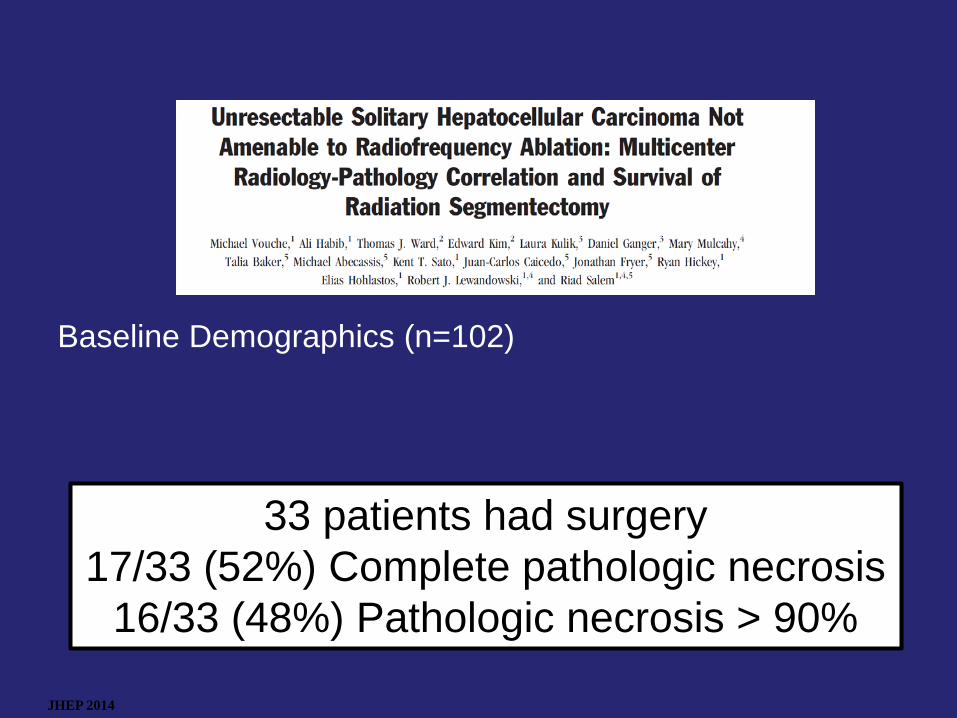
JHEP 2014
33 patients had surgery 17/33 (52%) Complete pathologic necrosis
16/33 (48%) Pathologic necrosis > 90%
Baseline Demographics (n=102)
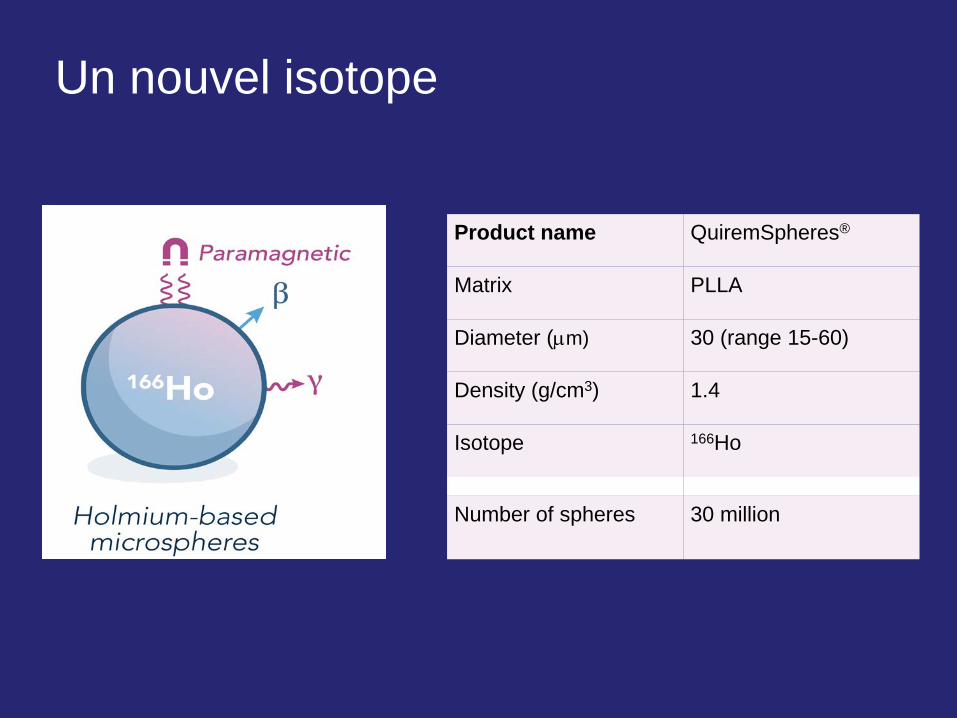
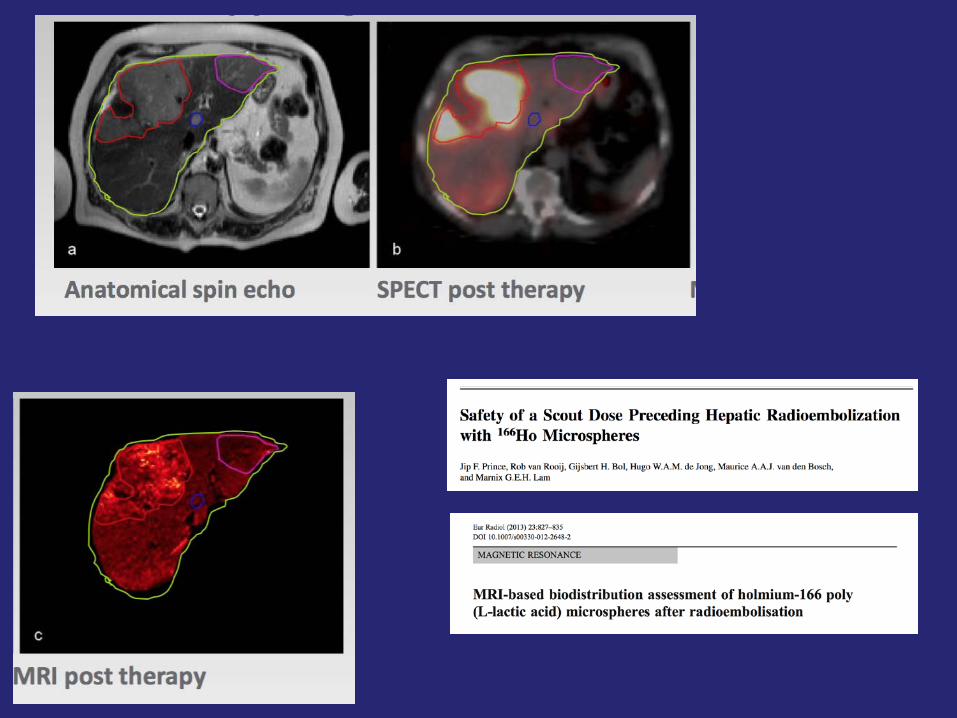
Product name QuiremSpheres®
Matrix PLLA
Diameter (µm) 30 (range 15-60)
Density (g/cm3) 1.4
Isotope 166Ho
Number of spheres 30 million
Un nouvel isotope
0
0,2
0,4
0,6
0,8
1
1,2
1,4
1,6
1,8
0 5 10 15 20
Dos
e ra
te (G
y/h)
Time (days)
holmium-166
yttrium-90
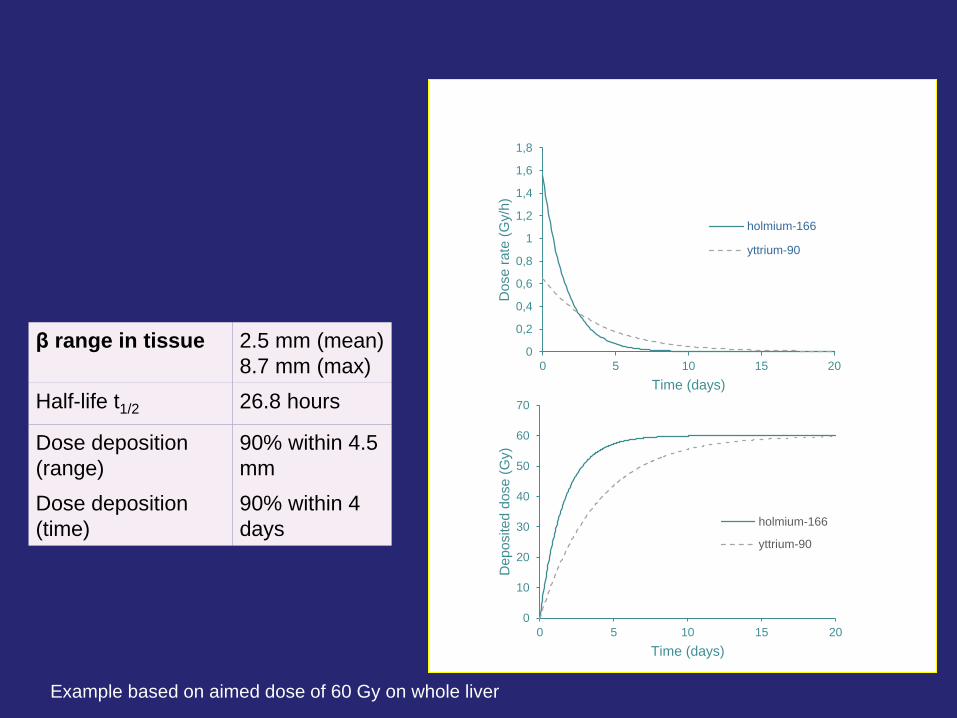
Example based on aimed dose of 60 Gy on whole liver
β range in tissue 2.5 mm (mean) 8.7 mm (max)
Half-life t1/2 26.8 hours
Dose deposition (range)
90% within 4.5 mm
Dose deposition (time)
90% within 4 days
0
10
20
30
40
50
60
70
0 5 10 15 20
Dep
osite
d do
se (G
y)
Time (days)
holmium-166
yttrium-90
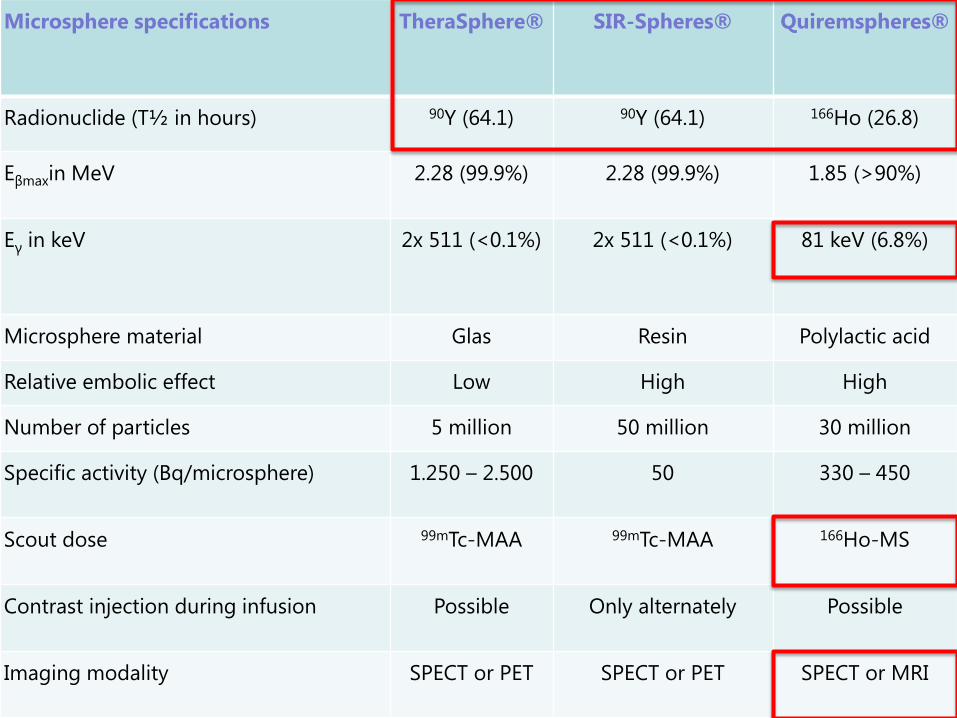
Microsphere specifications TheraSphere® SIR-Spheres® Quiremspheres®
Radionuclide (T½ in hours) 90Y (64.1) 90Y (64.1) 166Ho (26.8)
Eβmaxin MeV 2.28 (99.9%) 2.28 (99.9%) 1.85 (>90%)
Eγ in keV 2x 511 (<0.1%) 2x 511 (<0.1%) 81 keV (6.8%)
Microsphere material Glas Resin Polylactic acid
Relative embolic effect Low High High
Number of particles 5 million 50 million 30 million
Specific activity (Bq/microsphere) 1.250 – 2.500 50 330 – 450
Scout dose 99mTc-MAA 99mTc-MAA 166Ho-MS
Contrast injection during infusion Possible Only alternately Possible
Imaging modality SPECT or PET SPECT or PET SPECT or MRI
• 166-Holmium : scout dose avec le même produit – Meilleur définition de la dose , du rapport dose tumeur/dose au foie
• Sélection des patients sur un Holmium diagnostic – Sélectionner les patients qui peuvent bénéficier des patients qui vont
avoir un effet délétère
Conclusion
• Une seul indication en France : SIRTEX mCCR refractaire chimiothérapie
• Amélioration du contrôle de la maladie hépatqiue
• Optimisation de dose (efficacité / toxicité à long terme)
– Calcul tumeur / foie
– Délivrance lobaire, segmentaire / hypertrophie
• Isostope différent – Scout dose : vrai calcul de dose
– Débit d’irradiation plus fort
• Traitements combinés / immunotrigering
Merci