Embed Size (px)
DESCRIPTION
Le paludisme chez la femme enceinte - Conférence de la 1ère édition du Cours international « Atelier Paludisme » - JAMBOU Ronan
Citation preview
Atelier Paludisme IPM 2003
Le paludisme chez la femme enceinte
Elements de reflexions
Jambou R
Atelier Paludisme IPM 2003
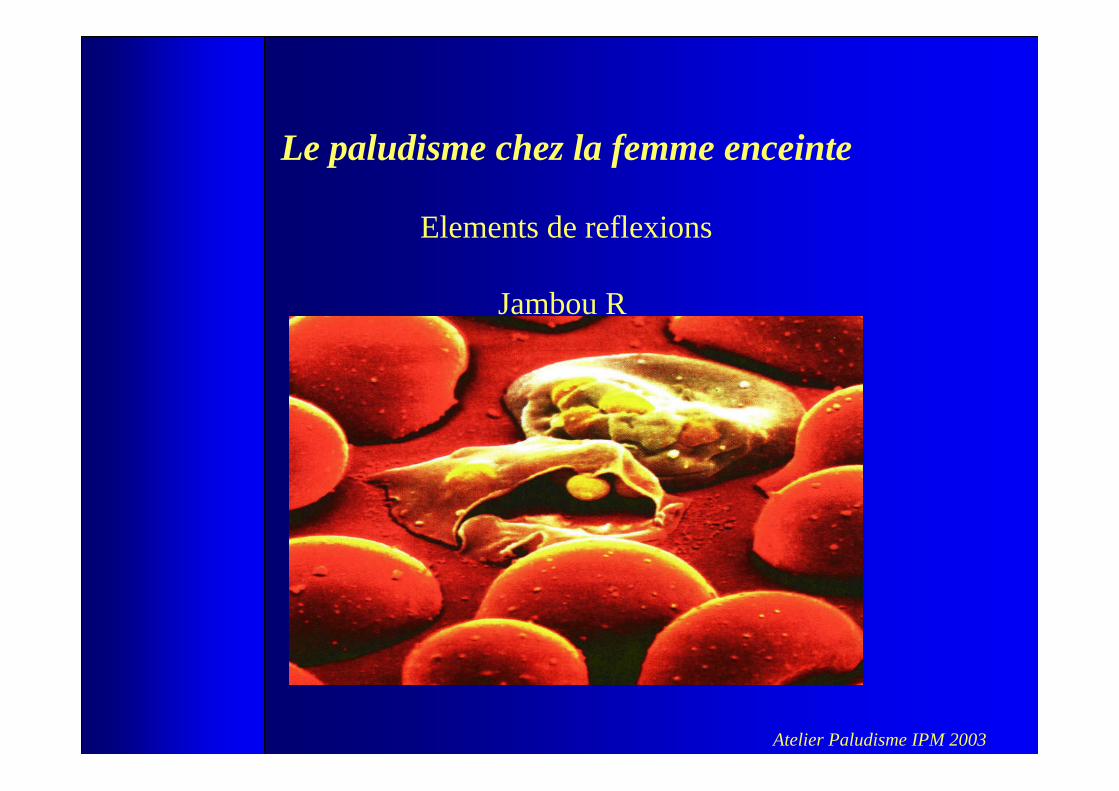
At least 24 millionpregnancies are threatened each year in Africa and malaria causes up to 15 percent of maternal anaemiaand about 35 percent ofpreventable low birth-weight.
WHO
Malaria attack
Placental infection
Atelier Paludisme IPM 2003
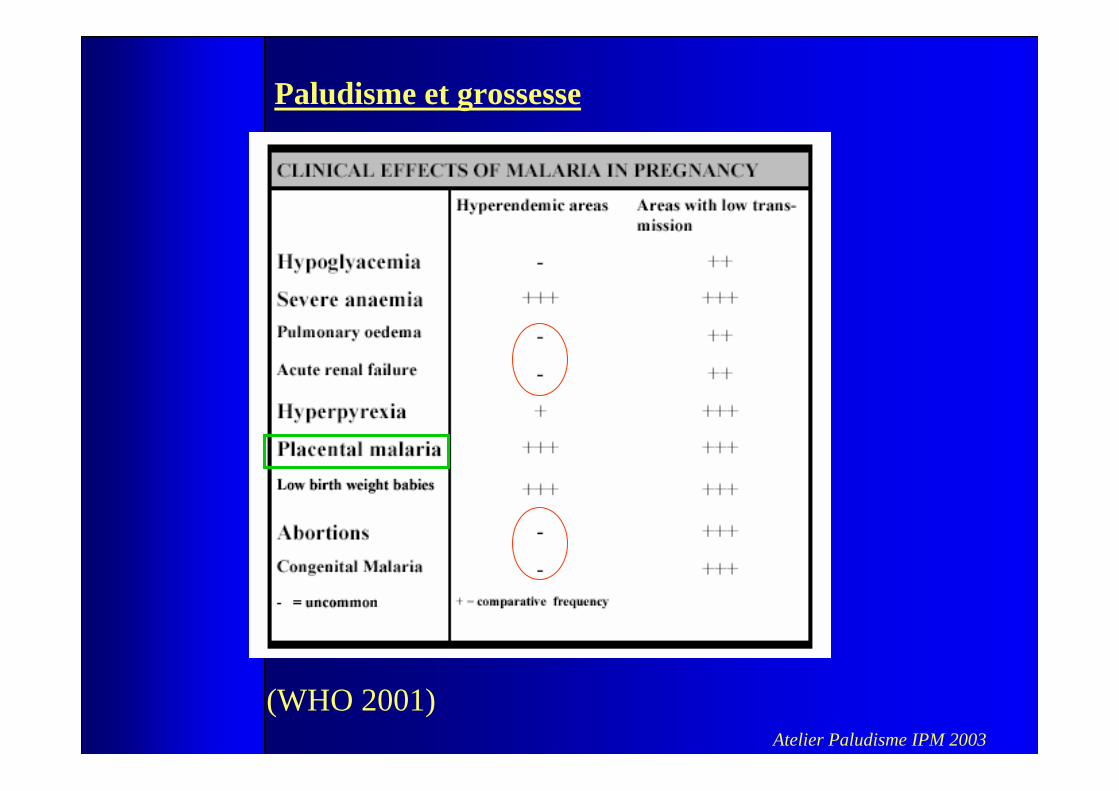
Paludisme et grossesse
La grossesse induit une augmentation du nombre d’accès Jusqu’à deux mois après l’accouchement
=> Projet Dielmo
(Niagne et al)
Atelier Paludisme IPM 2003
(WHO 2001)
Paludisme et grossesse
Atelier Paludisme IPM 2003
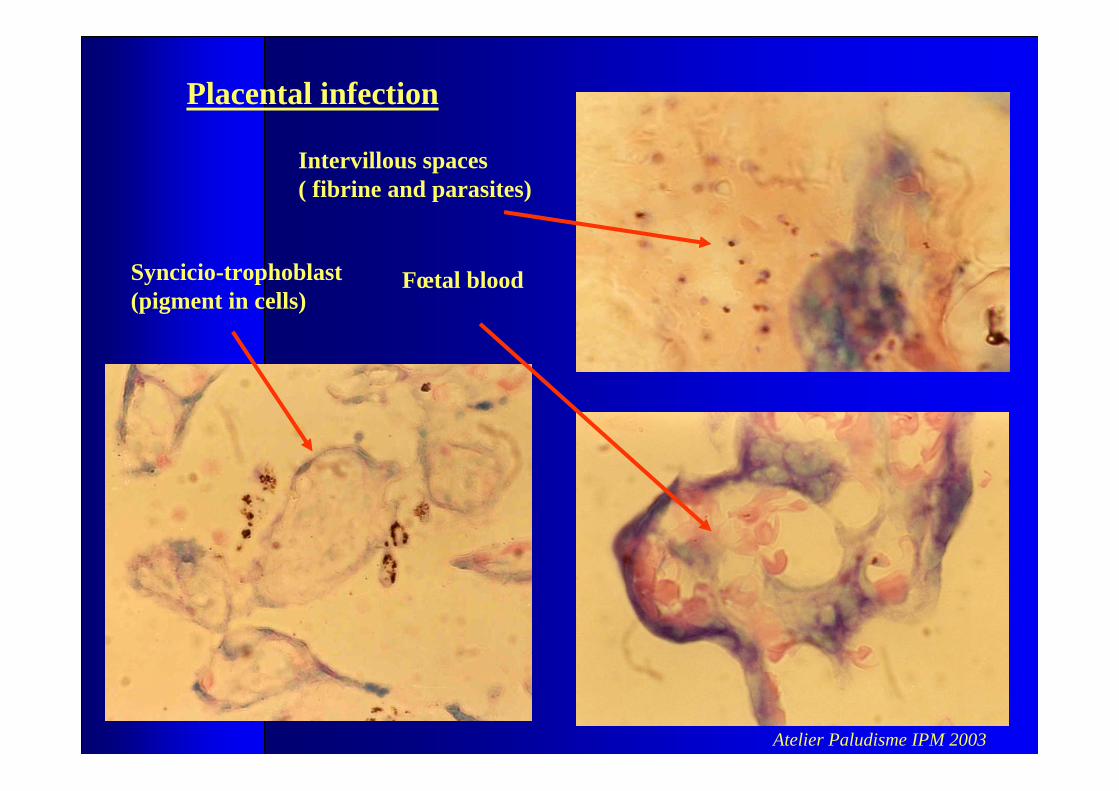
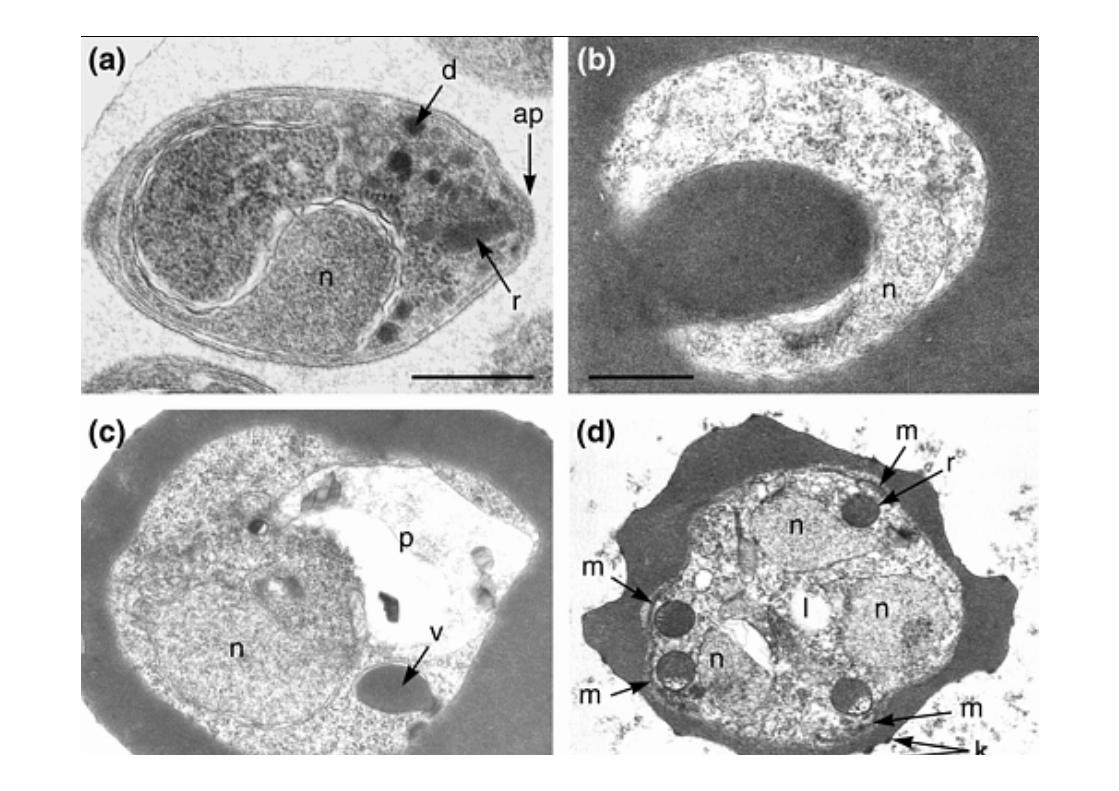
Placental infection
Fœtal blood
Intervillous spaces( fibrine and parasites)
Syncicio-trophoblast(pigment in cells)
Atelier Paludisme IPM 2003
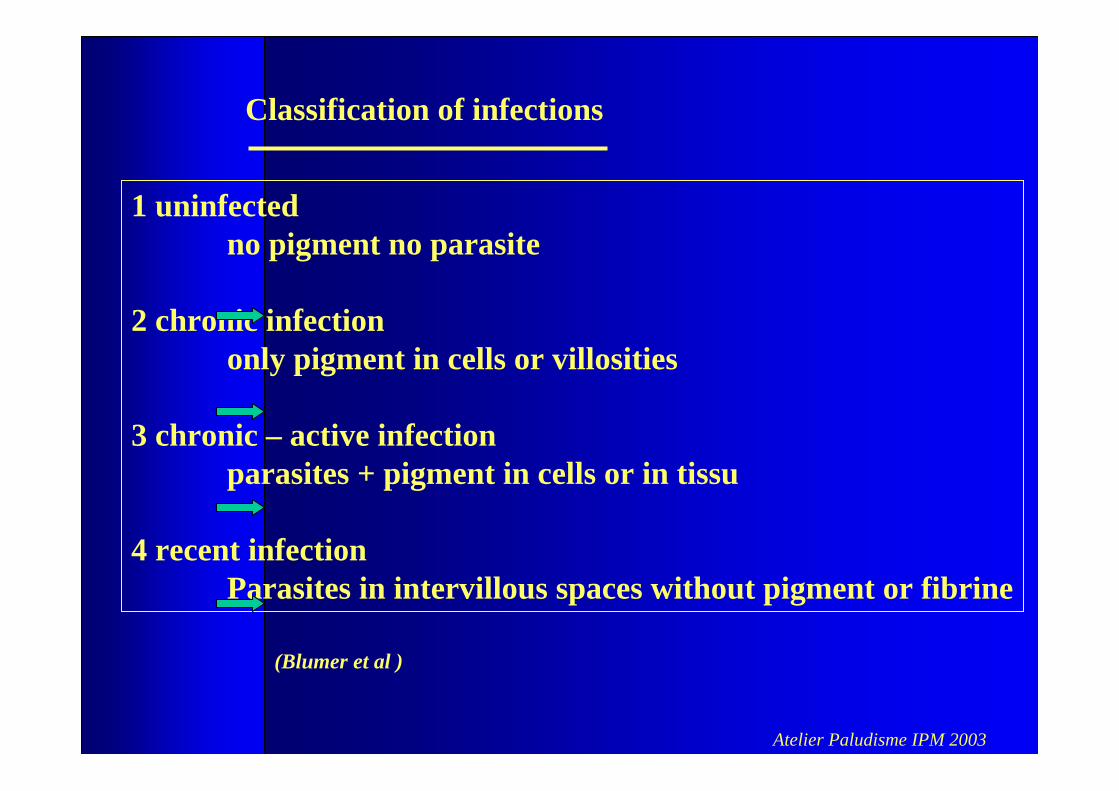
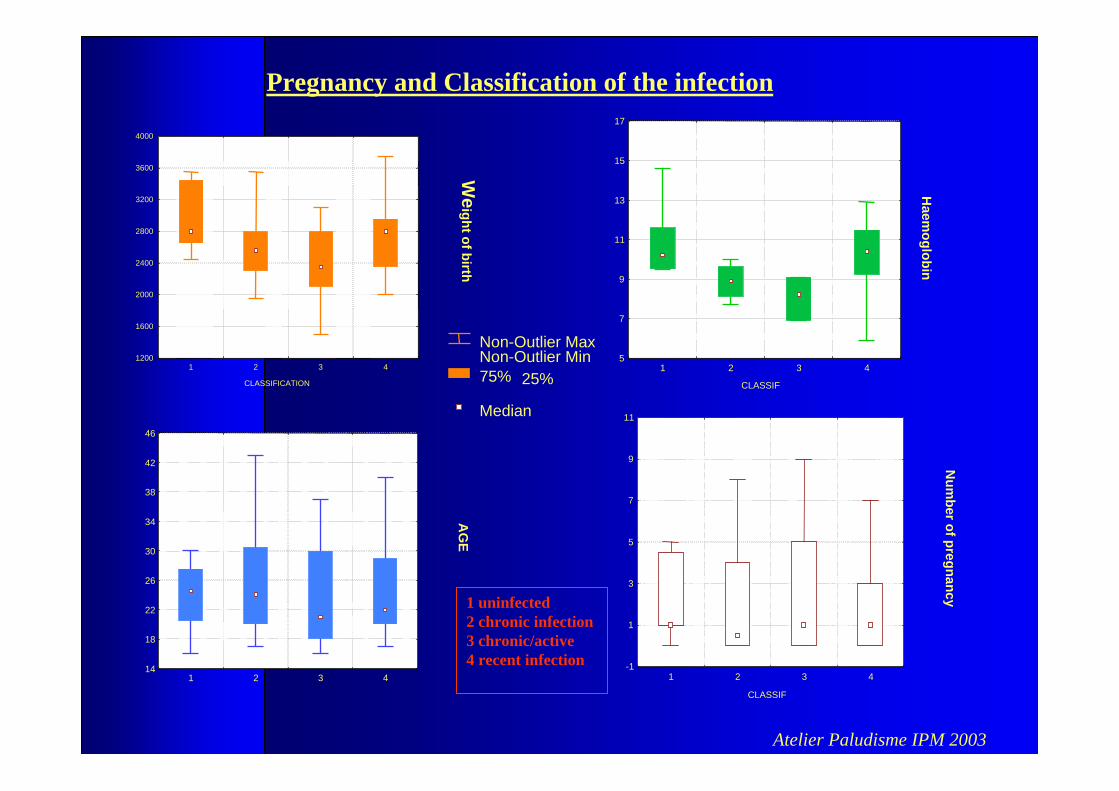
Classification of infections
1 uninfectedno pigment no parasite
2 chronic infection only pigment in cells or villosities
3 chronic – active infection parasites + pigment in cells or in tissu
4 recent infection Parasites in intervillous spaces without pigment or fibrine
(Blumer et al )
Atelier Paludisme IPM 2003
Quel est le poids du paludisme chez les femmes enceintes
en zone urbaine ??
Projet d’étude – Dakar 2000 (AdS) / 2003 (FSP)
Atelier Paludisme IPM 2003
Area of study
Atelier Paludisme IPM 2003
Population studied
Guediawaye- Dakar
Suburb of Dakar - population 600 000 inhabitants
low and seasonal transmission of malaria around water collections (Niayes)
exchange of populations with the rural areas
omen attending the maternity “Roi Baudoin” of Guediawaye for delivery
-from July to December
- Living in the periphery of Dakar
- no travel declared the two months prior to the delivery
- placental infestation (positive detection of HRP II antigen in the placental blood)
Atelier Paludisme IPM 2003
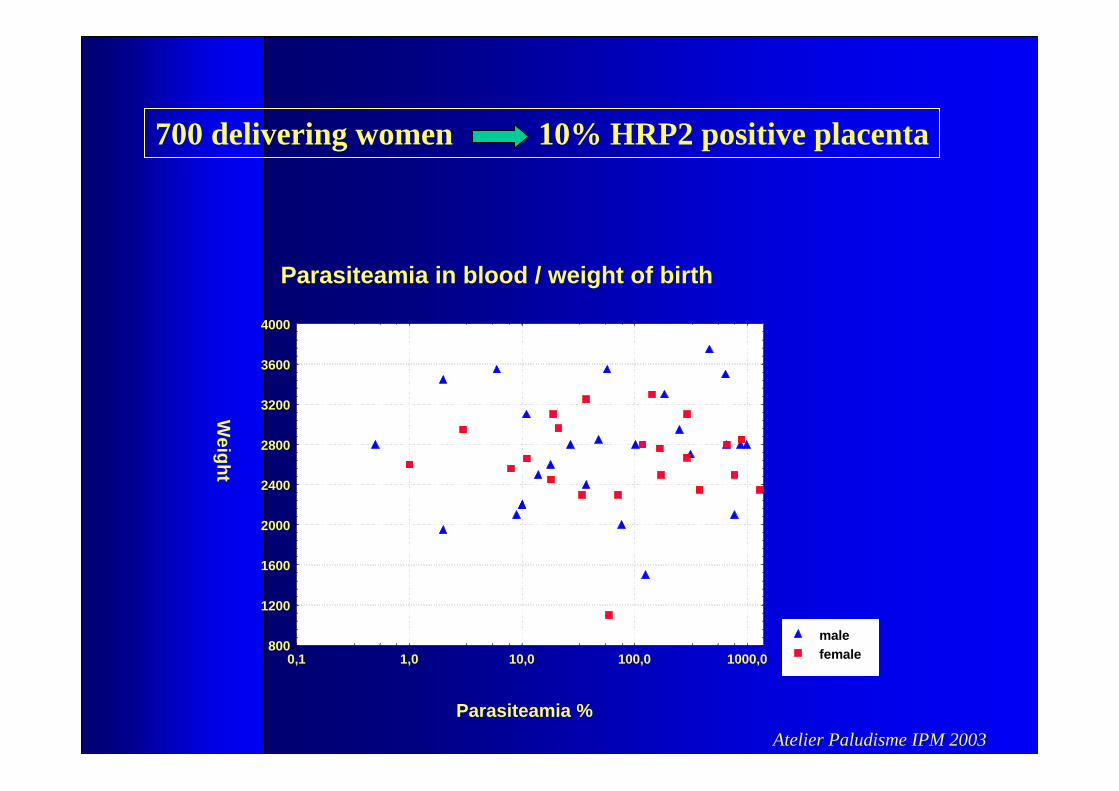
Parasiteamia in blood / weight of birth
malefemale
Parasiteamia %
Weight
800
1200
1600
2000
2400
2800
3200
3600
4000
0,1 1,0 10,0 100,0 1000,0
700 delivering women 10% HRP2 positive placenta
Atelier Paludisme IPM 2003
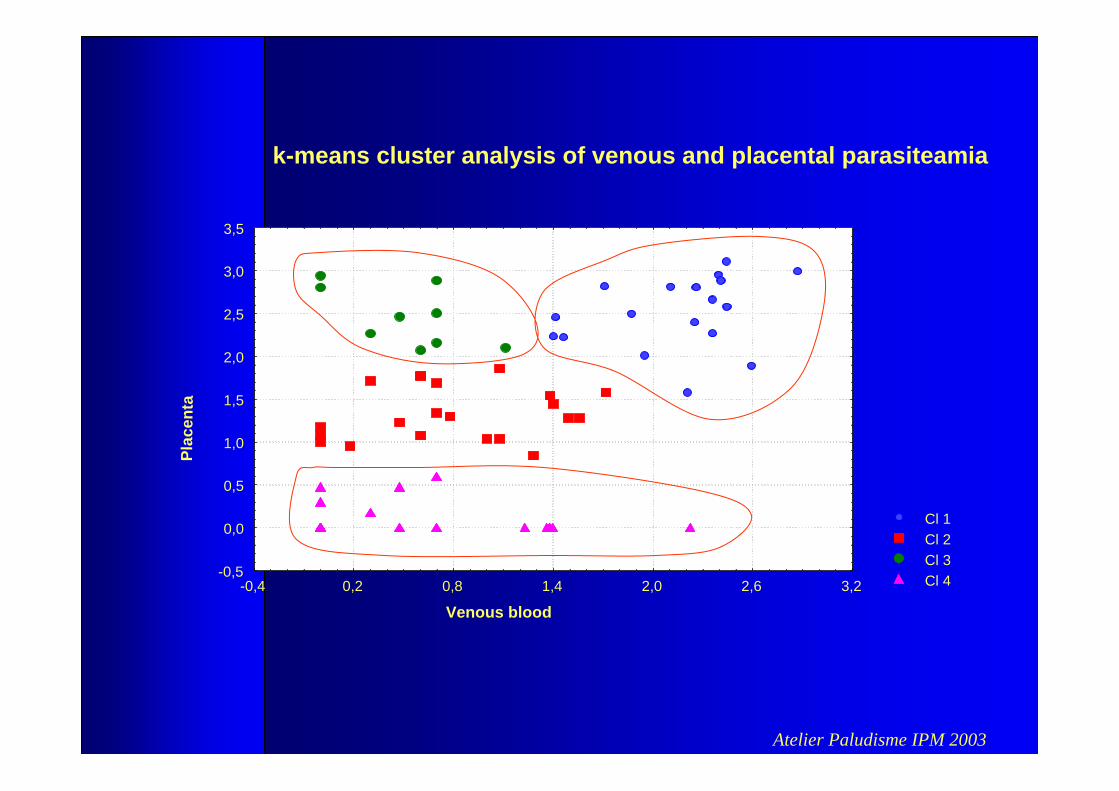
Cl 1Cl 2Cl 3Cl 4
k-means cluster analysis of venous and placental parasiteamia
Venous blood
Plac
enta
-0,5
0,0
0,5
1,0
1,5
2,0
2,5
3,0
3,5
-0,4 0,2 0,8 1,4 2,0 2,6 3,2
Atelier Paludisme IPM 2003
CLASSIFICATION
We
ightofbirth
1200
1600
2000
2400
2800
3200
3600
4000
1 2 3 4
CLASSIF
Haem
oglobin
5
7
9
11
13
15
17
1 2 3 4
AG
E14
18
22
26
30
34
38
42
46
1 2 3 4
CLASSIF
Num
berofpregnancy
-1
1
3
5
7
9
11
1 2 3 4
Non-Outlier MaxNon-Outlier Min75%
Median
25%
Pregnancy and Classification of the infection
1 uninfected2 chronic infection 3 chronic/active 4 recent infection
Atelier Paludisme IPM 2003(Contamin et al)
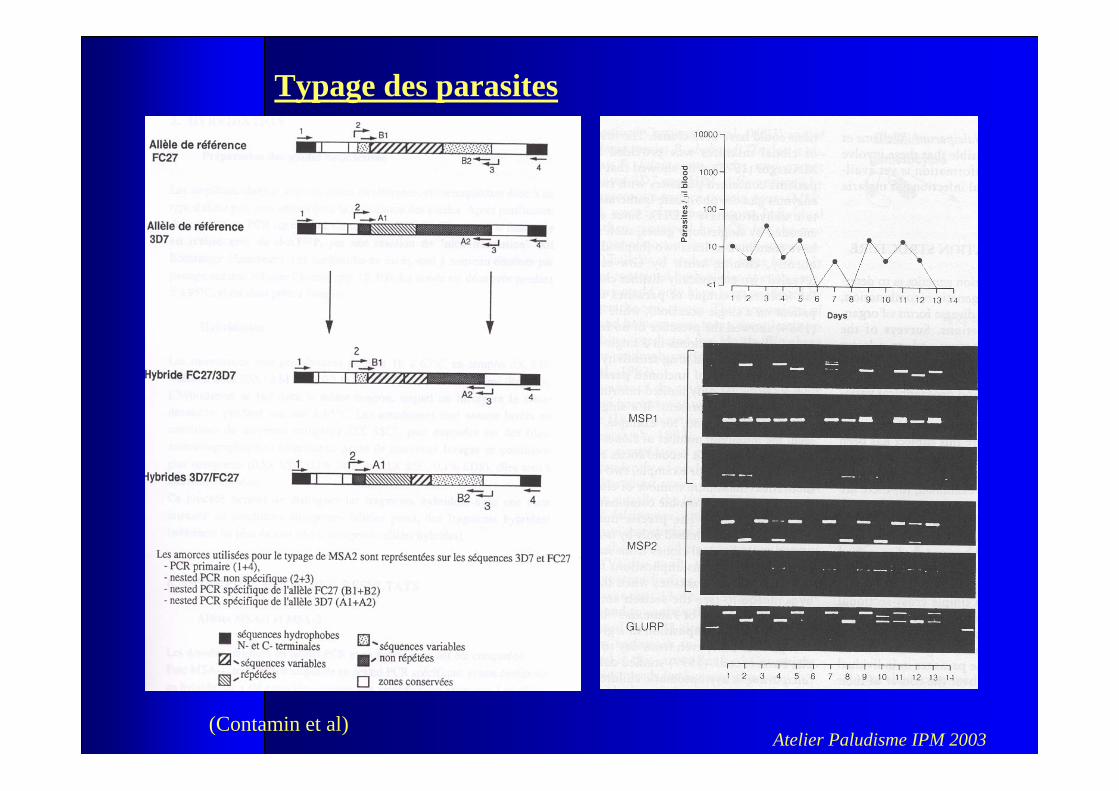
Typage des parasites
Atelier Paludisme IPM 2003
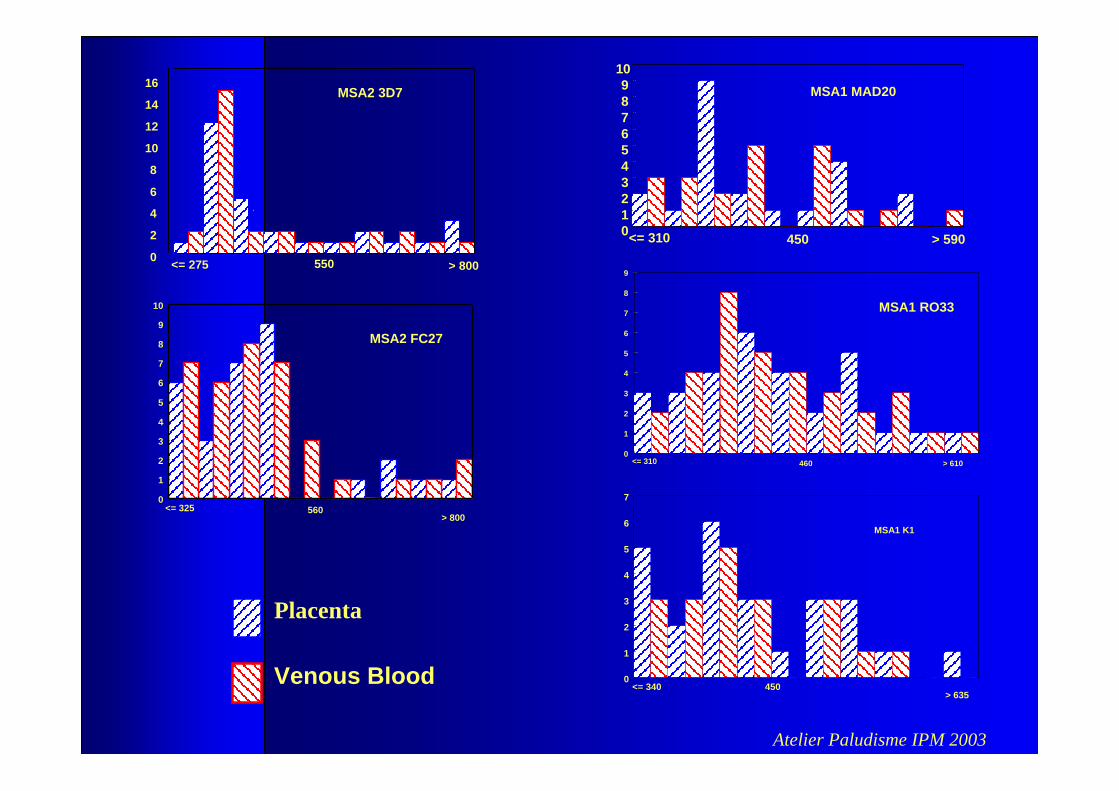
Placenta
Venous Blood
MSA2 3D7
0
2
4
6
8
10
12
14
16
<= 275 550 > 800
MSA1 MAD20
0123456789
10
<= 310 450 > 590
MSA2 FC27
0
1
2
3
4
5
6
7
8
9
10
<= 325 560> 800
MSA1 RO33
0
1
2
3
4
5
6
7
8
9
<= 310 460 > 610
MSA1 K1
0
1
2
3
4
5
6
7
<= 340 450> 635
Atelier Paludisme IPM 2003
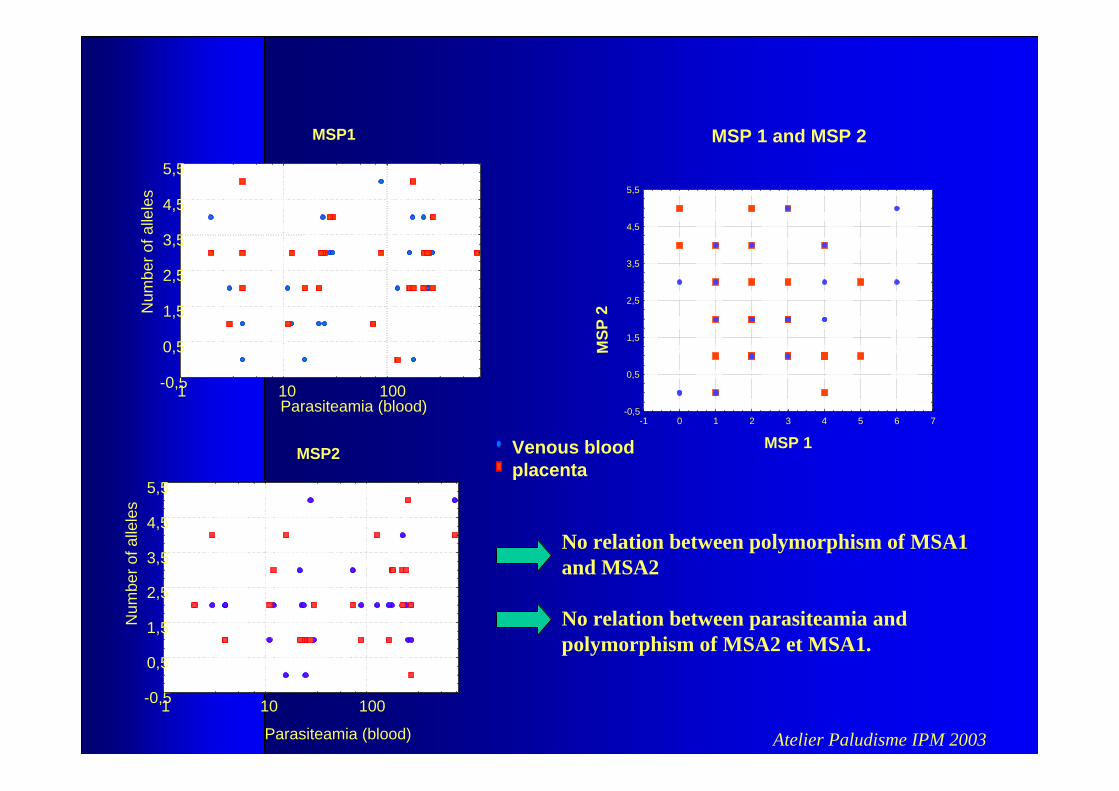
Venous bloodplacenta
MSP1
Parasiteamia (blood)
Num
bero
f alle
les
-0,5
0,5
1,5
2,5
3,5
4,5
5,5
1 10 100
MSP 1 and MSP 2
MSP 1
MSP
2
-0,5
0,5
1,5
2,5
3,5
4,5
5,5
-1 0 1 2 3 4 5 6 7
No relation between polymorphism of MSA1 and MSA2
No relation between parasiteamia and polymorphism of MSA2 et MSA1.
MSP2
-0,5
0,5
1,5
2,5
3,5
4,5
5,5
1 10 100
Parasiteamia (blood)
Num
bero
f alle
les
Atelier Paludisme IPM 2003
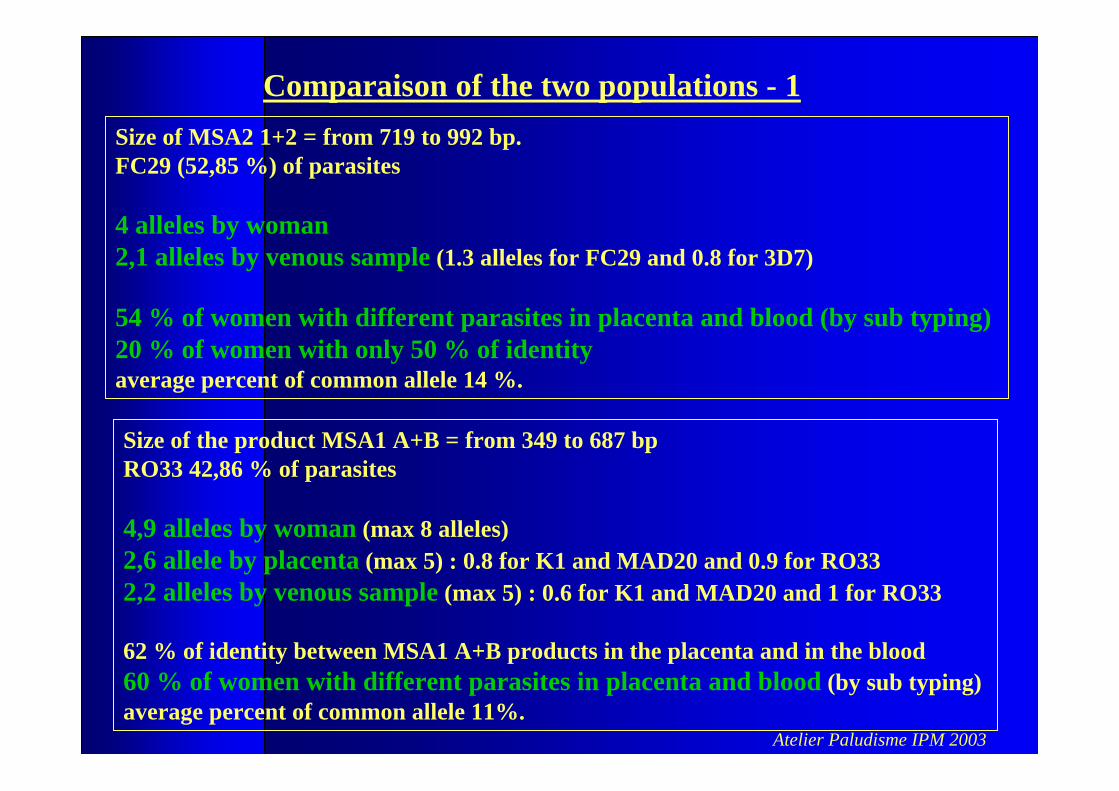
Comparaison of the two populations - 1Size of MSA2 1+2 = from 719 to 992 bp. FC29 (52,85 %) of parasites
4 alleles by woman2,1 alleles by venous sample (1.3 alleles for FC29 and 0.8 for 3D7)
54 % of women with different parasites in placenta and blood (by sub typing) 20 % of women with only 50 % of identityaverage percent of common allele 14 %.
Size of the product MSA1 A+B = from 349 to 687 bp RO33 42,86 % of parasites
4,9 alleles by woman (max 8 alleles) 2,6 allele by placenta (max 5) : 0.8 for K1 and MAD20 and 0.9 for RO332,2 alleles by venous sample (max 5) : 0.6 for K1 and MAD20 and 1 for RO33
62 % of identity between MSA1 A+B products in the placenta and in the blood60 % of women with different parasites in placenta and blood (by sub typing) average percent of common allele 11%.
Atelier Paludisme IPM 2003
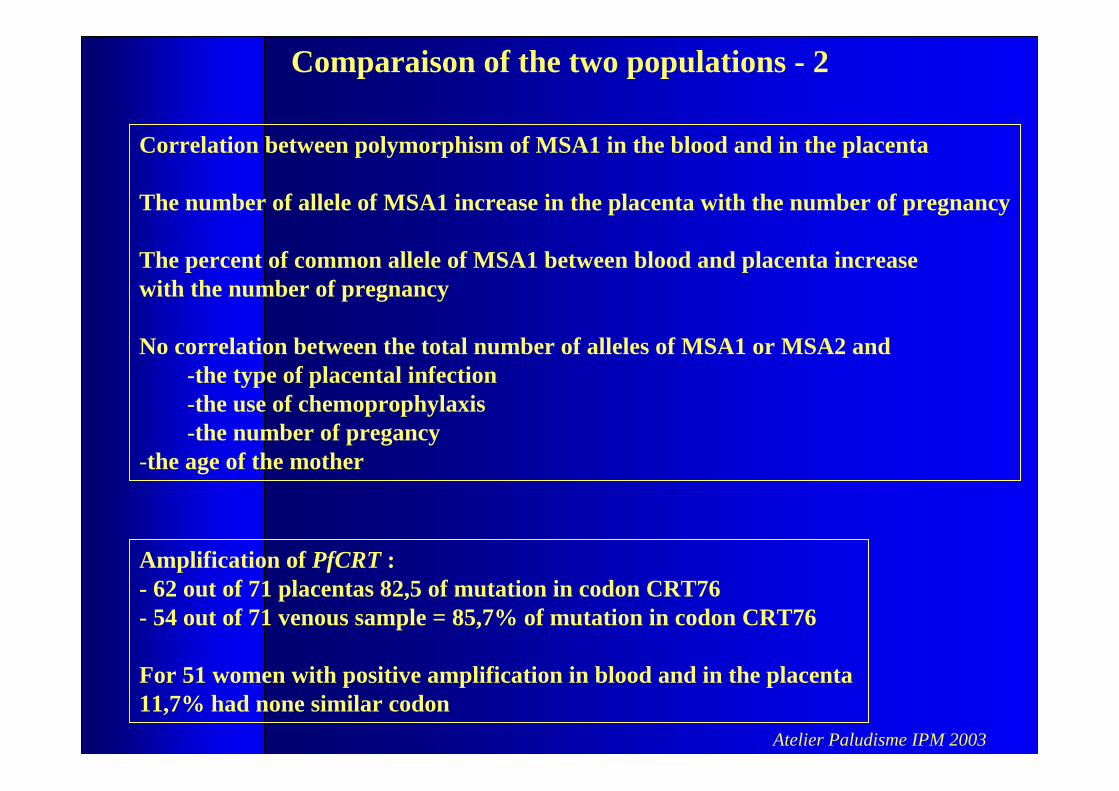
Correlation between polymorphism of MSA1 in the blood and in the placenta
The number of allele of MSA1 increase in the placenta with the number of pregnancy
The percent of common allele of MSA1 between blood and placenta increase with the number of pregnancy
No correlation between the total number of alleles of MSA1 or MSA2 and -the type of placental infection -the use of chemoprophylaxis-the number of pregancy
-the age of the mother
Comparaison of the two populations - 2
Amplification of PfCRT :- 62 out of 71 placentas 82,5 of mutation in codon CRT76- 54 out of 71 venous sample = 85,7% of mutation in codon CRT76
For 51 women with positive amplification in blood and in the placenta 11,7% had none similar codon
Atelier Paludisme IPM 2003
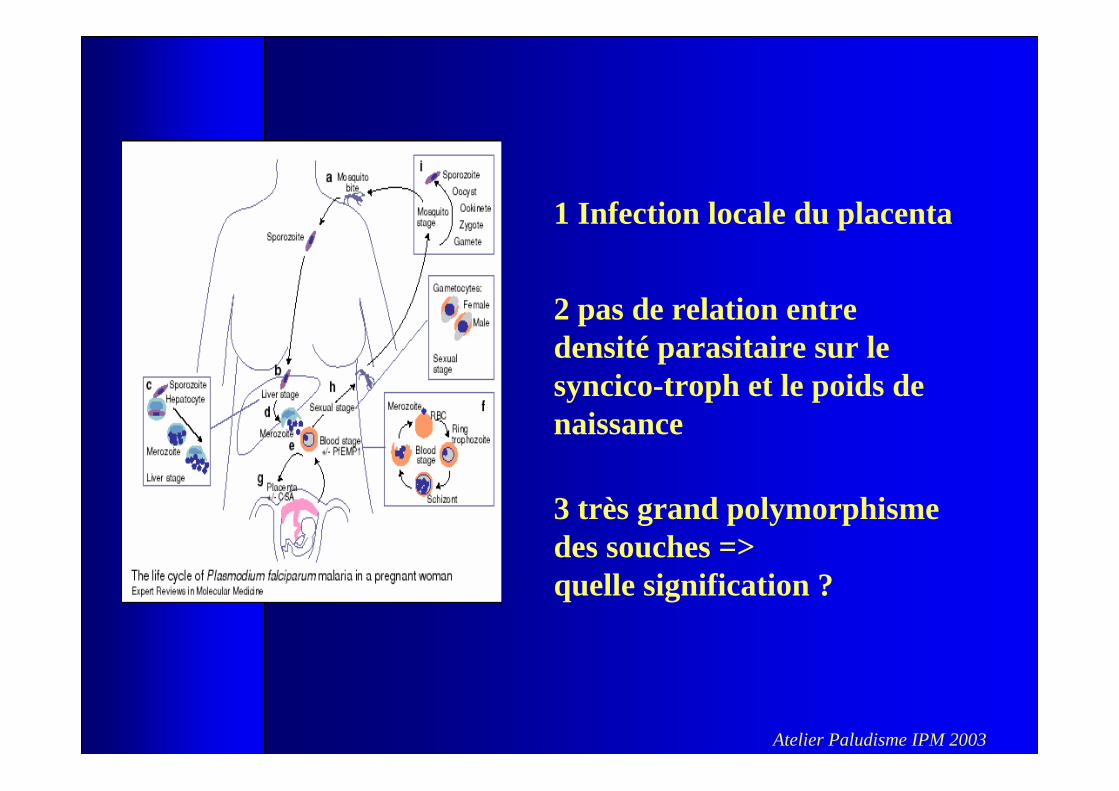
1 Infection locale du placenta
2 pas de relation entre densité parasitaire sur le syncico-troph et le poids de naissance
3 très grand polymorphismedes souches =>quelle signification ?
Atelier Paludisme IPM 2003
Pourquoi existe t il une infection locale
??
Atelier Paludisme IPM 2003
Atelier Paludisme IPM 2003
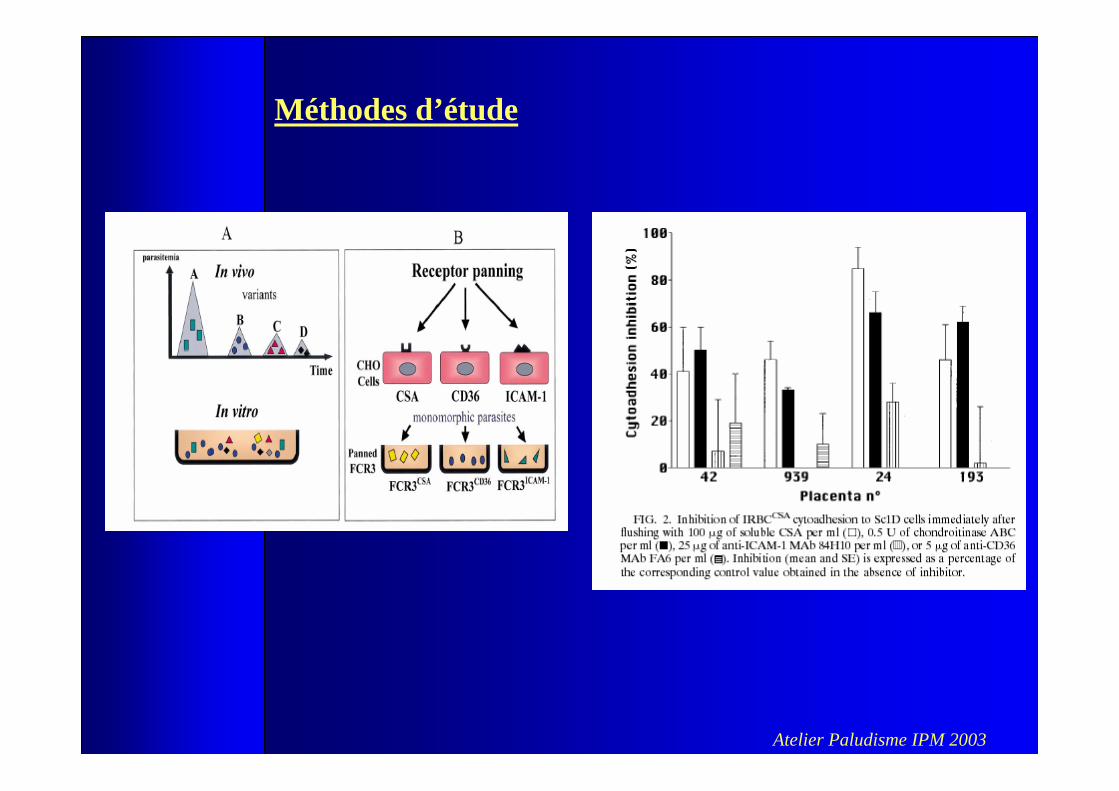
Méthodes d’étude
Atelier Paludisme IPM 2003
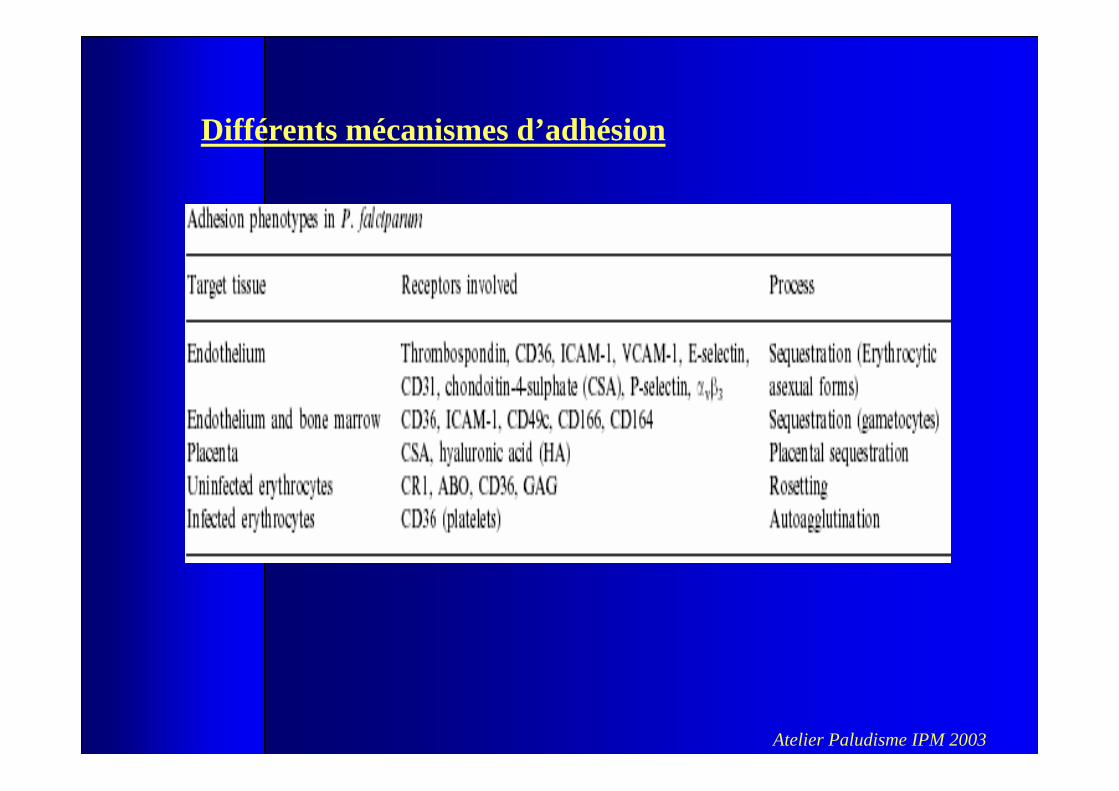
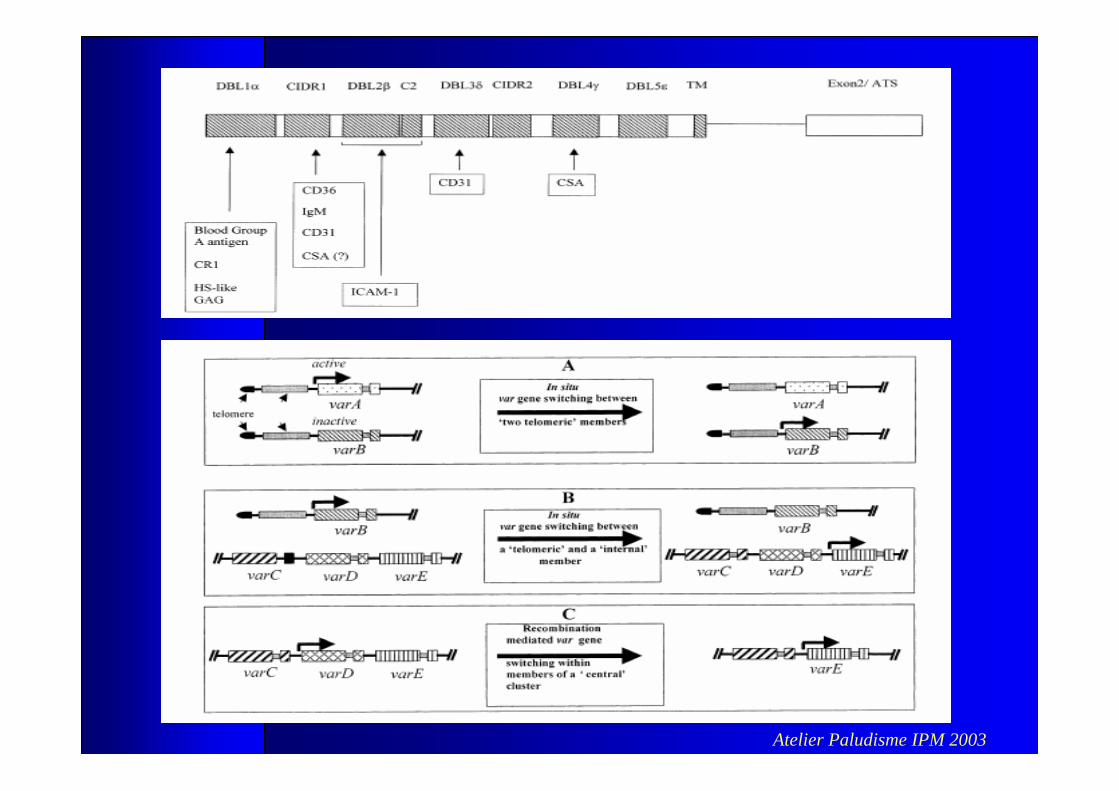
Différents mécanismes d’adhésion
Atelier Paludisme IPM 2003
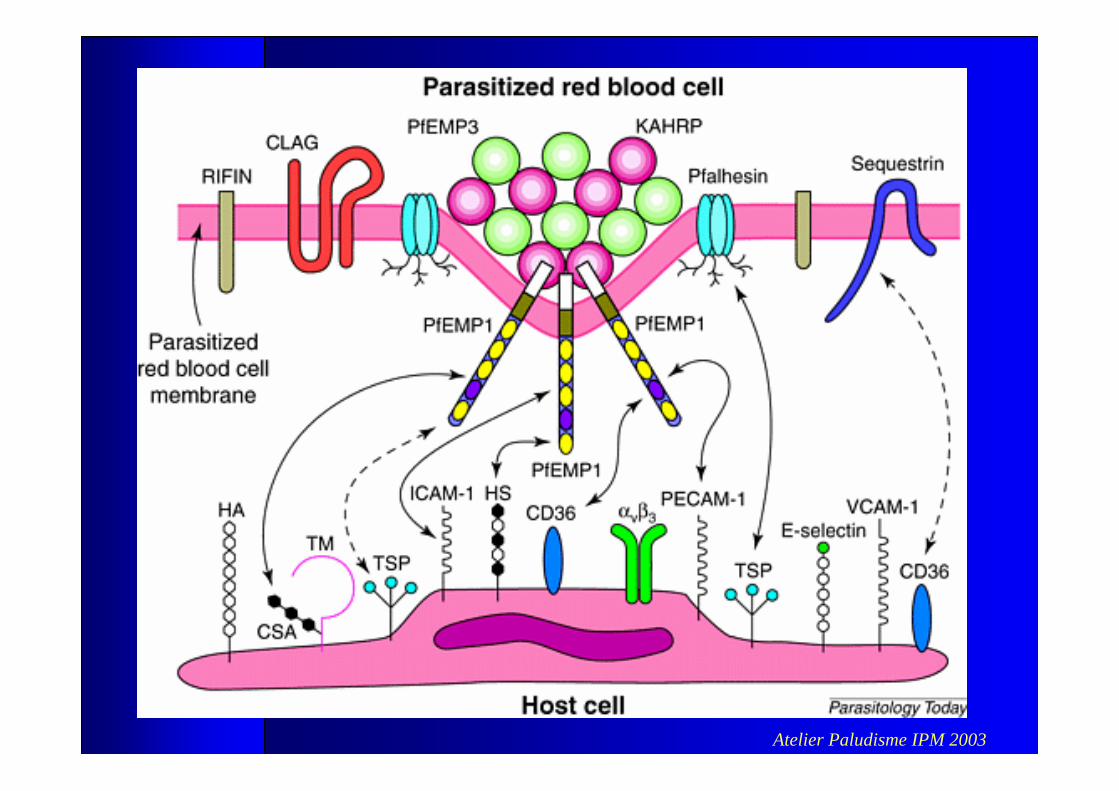
Atelier Paludisme IPM 2003
Atelier Paludisme IPM 2003
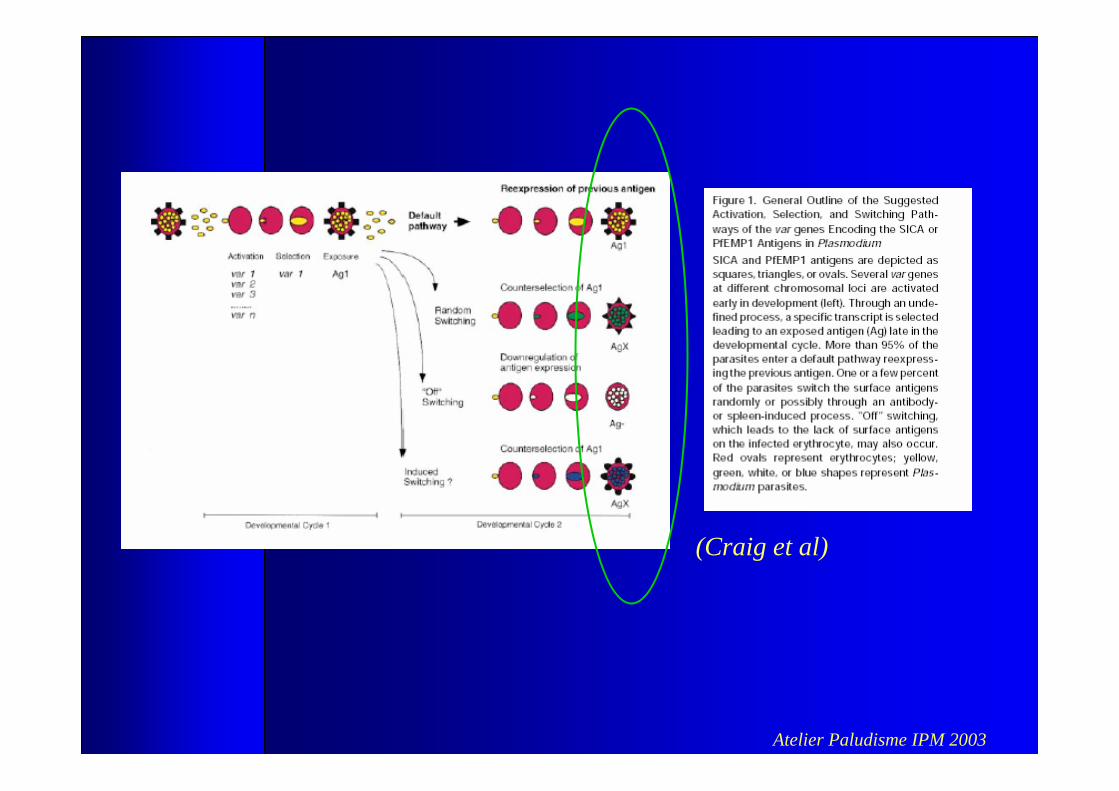
(Craig et al)
Atelier Paludisme IPM 2003
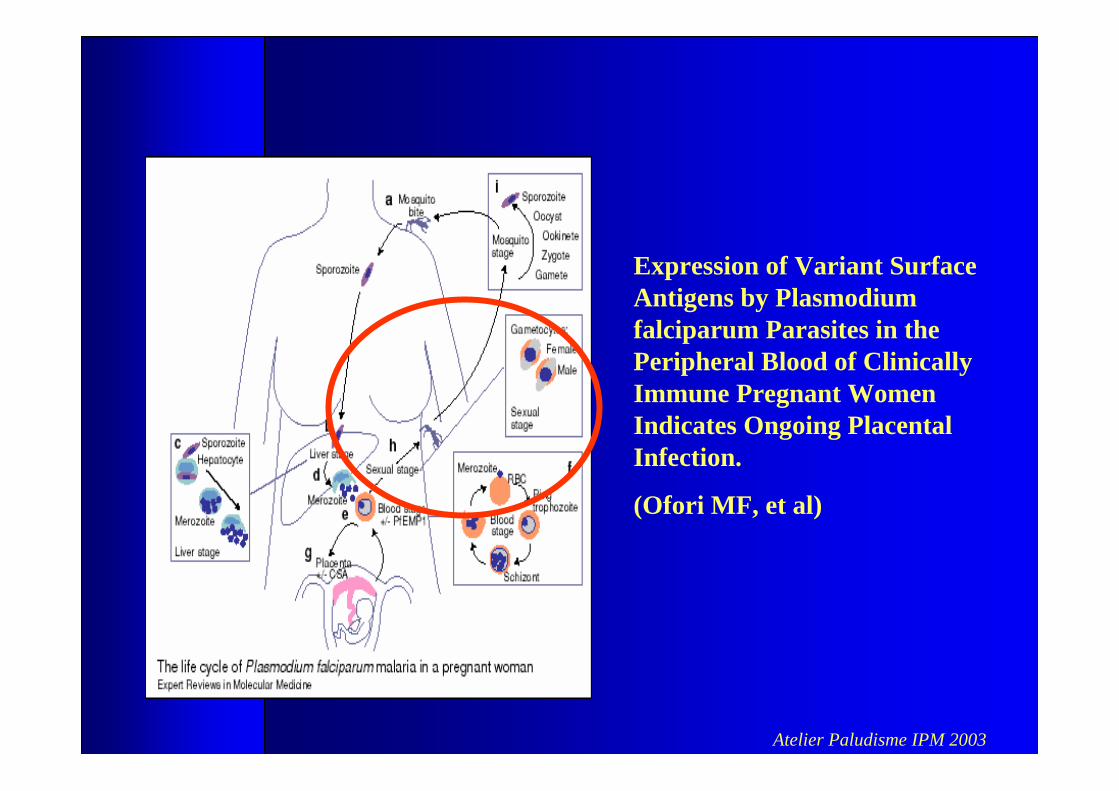
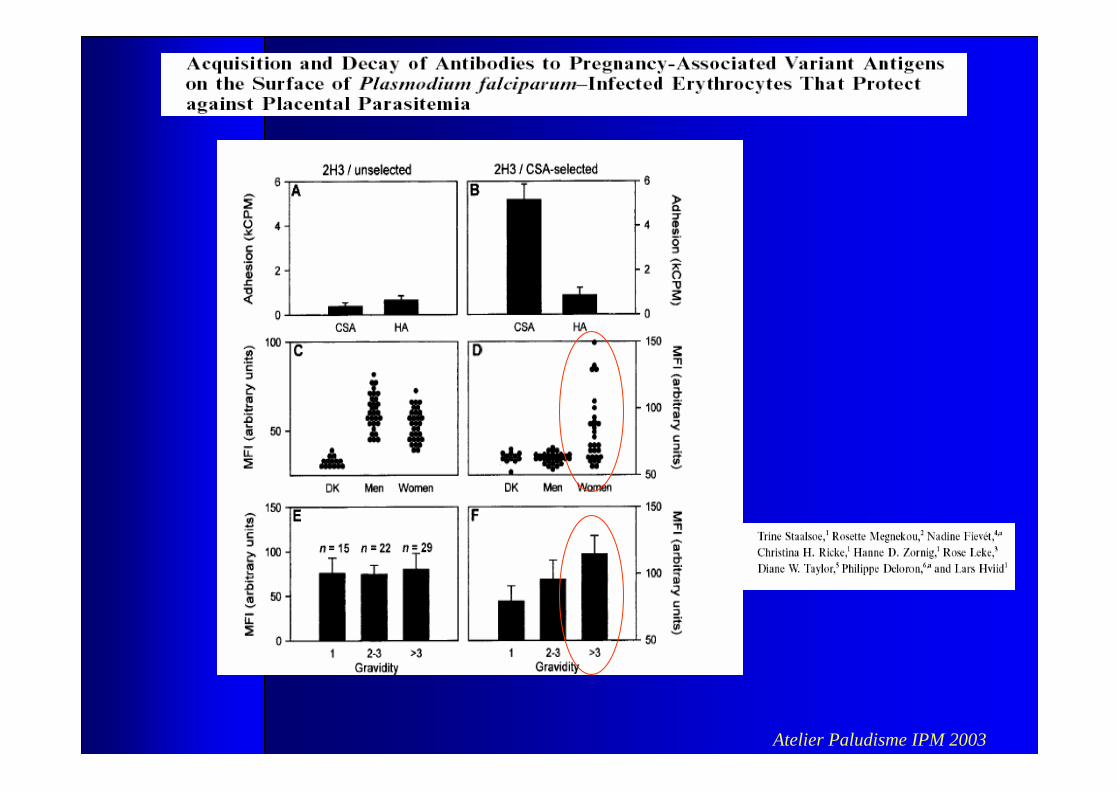
Expression of Variant SurfaceAntigens by Plasmodium falciparum Parasites in the Peripheral Blood of ClinicallyImmune Pregnant Women Indicates Ongoing PlacentalInfection.
(Ofori MF, et al)
Atelier Paludisme IPM 2003
Que faire en Pratique ??
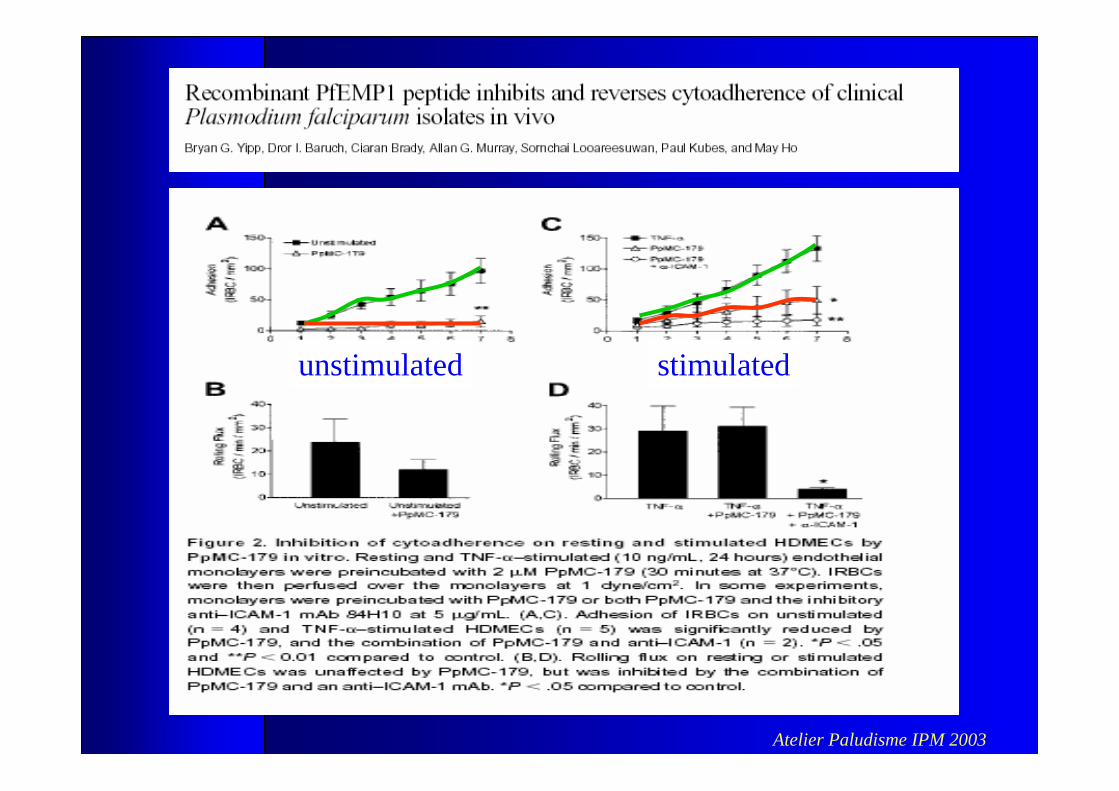
1 Développer un vaccin contre l’infection locale ?
Atelier Paludisme IPM 2003
unstimulated stimulated
Atelier Paludisme IPM 2003
Atelier Paludisme IPM 2003
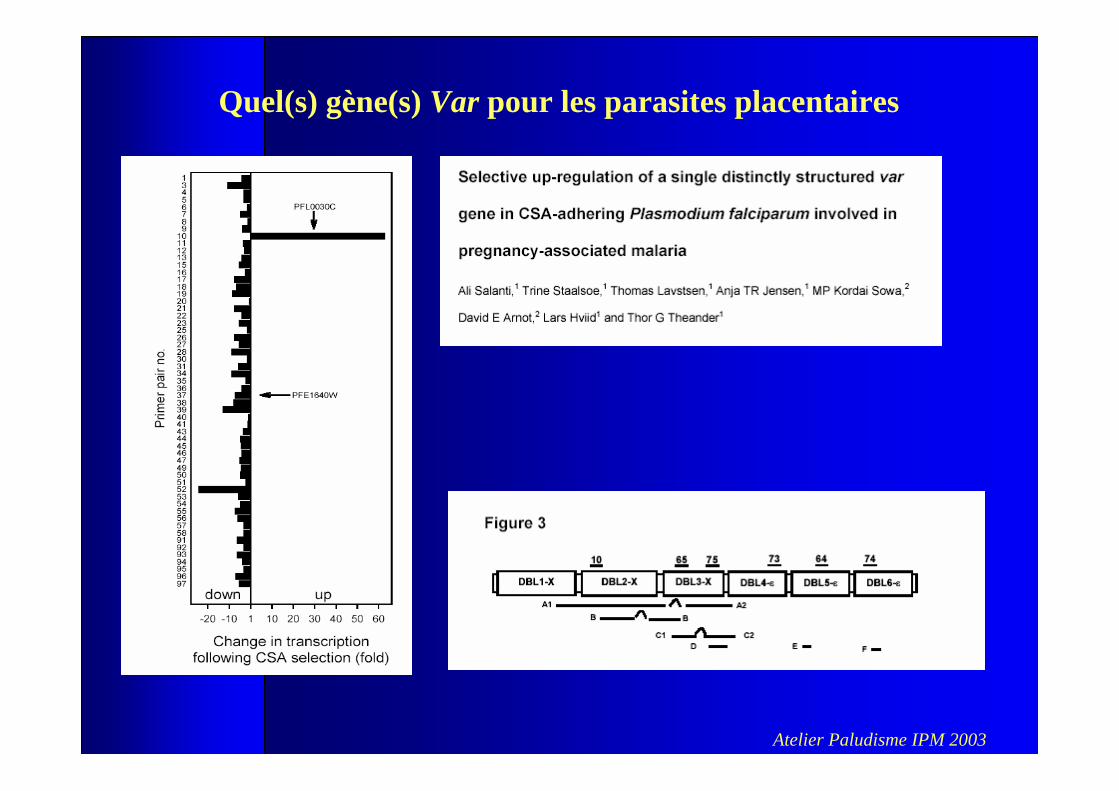
Quel(s) gène(s) Var pour les parasites placentaires
Atelier Paludisme IPM 2003
Que faire en Pratique ??
1 Développer un vaccin ?
2 Prophylaxie et Traitement intermittent ?
Atelier Paludisme IPM 2003
Prophylaxie
Résistance émergeante = données incomplètes = dispensaires
Observance faible = lié au coût / motivation faible
1 ère CPN tardive = rarement avant le 2eme trimestre
Démarche actuelleProphylaxie par la Chloroquine = 300mg/ semRecouvrement des coûts
Les problèmes
Atelier Paludisme IPM 2003
Les traitements intermittents
Etude du Malawi (depuis 1993) infection placentaire : 32 % à 23 % Faible poids de naissance : 23% à 10%.
Proposition : traitement systématique par SP lors des CPN
Problème : résistance rapide à la SP artésunate
Atelier Paludisme IPM 2003
Que faire en Pratique ??
1 Développer un vaccin ?
2 Prophylaxie et Traitement intermittent ?
3 Protéger contre les vecteurs
Atelier Paludisme IPM 2003
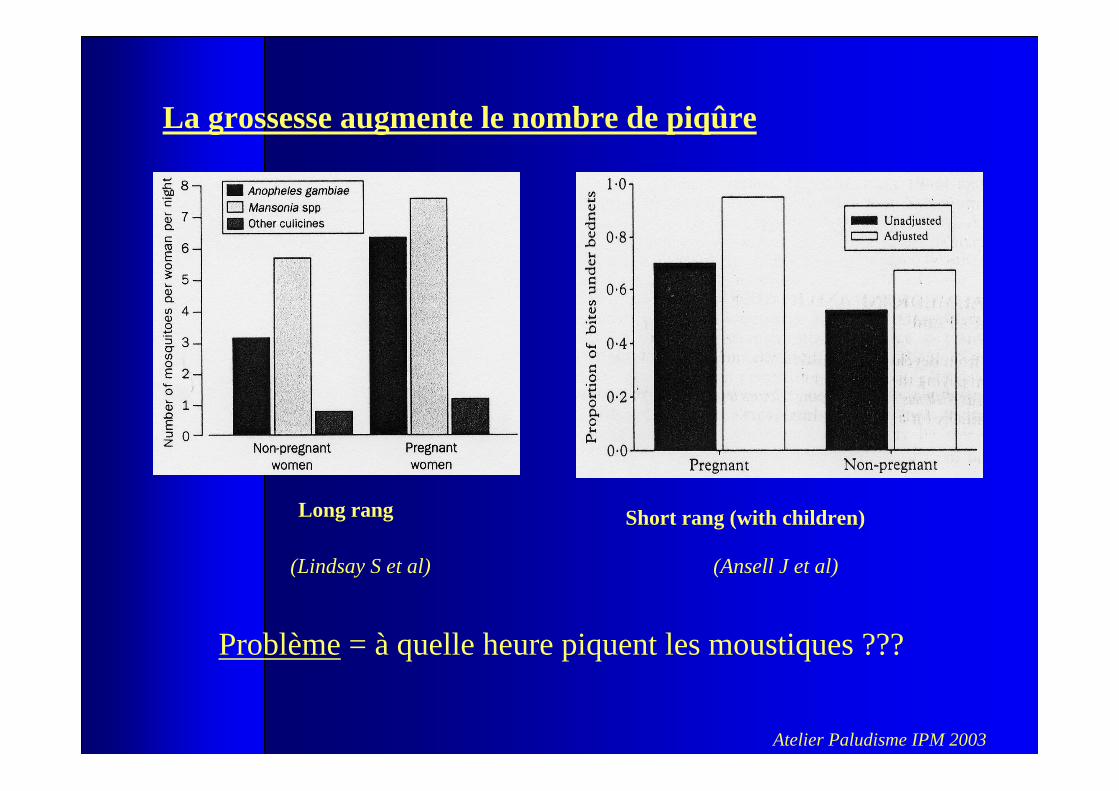
Long rang Short rang (with children)
(Ansell J et al)(Lindsay S et al)
La grossesse augmente le nombre de piqûre
Problème = à quelle heure piquent les moustiques ???
Atelier Paludisme IPM 2003
Que faire en Pratique ??
1 Développer un vaccin ?
2 Prophylaxie et Traitement intermittent ?
3 Protéger contre les vecteurs
4 prendre en charge les carences (fer-folates) Interaction avec les anti-folates ??
5 Améliorer la prise en charge de l’accouchement
Atelier Paludisme IPM 2003
•case management alone is not effective in preventing theadverse effects of malaria
• selection of the currently available preventive toolschemoprophylaxis,intermittent treatment andinsecticide-impregnated bednets
=> determined by local conditions
•all women in endemic areas should receive haematinicsduring pregnancy
• current strategies may be less effective in HIV+ women
MIM conference
Atelier Paludisme IPM 2003
• appropriate tools are needed to monitor the effectiveness ofcurrent programmes
• new methods are needed to improve the implementation and compliance with control strategies
• monitoring the effectiveness of impregnated bednets indifferent endemic settings
• the cost-effectiveness of interventions in different settings needs to be assessed
MIM conference