Embed Size (px)
Citation preview
Les Ateliers Lymphomes et LLC
22 – 24 octobre 2009Le Moulin de la Forge – Le Vaumain (60)

4ème session :Lymphomes indolentsModérée par Guillaume CARTRON
33
Programmedelasession
4èmesession:Lymphomesindolents‐ModéréeparG.Cartron
Anatomopathologie N.Brousse
Facteurspronos8quescliniques Ph.Solal‐Céligny
Facteurspronos8quesbiologiques–Maladierésiduelle
F.Jardin
Stratégiesthérapeu8ques G.Salles
Cascliniqueinterac8f PrésentéparG.Cartron
PathogénieettraitementdesMZL C.Thieblemont
Cascliniqueinterac8f PrésentéparPh.Solal‐Céligny
Stratégiesthérapeu8ques
GillesSallesServiceHématologieClinique,HospicesCivilsdeLyon
Traitements deslymphomes folliculaires
La décision thérapeutique en première ligne
Standards et options pour les patients avec faiblemasse et les stades localisés
Standards et options pour les patients de forte masse– Quelles voies de progrès ?
Les choix thérapeutiques en rechute– Que veut-on obtenir ?– Quels outils, quels bénéfices ?

Traitements deslymphomes folliculaires
La décision thérapeutiqueen première ligne
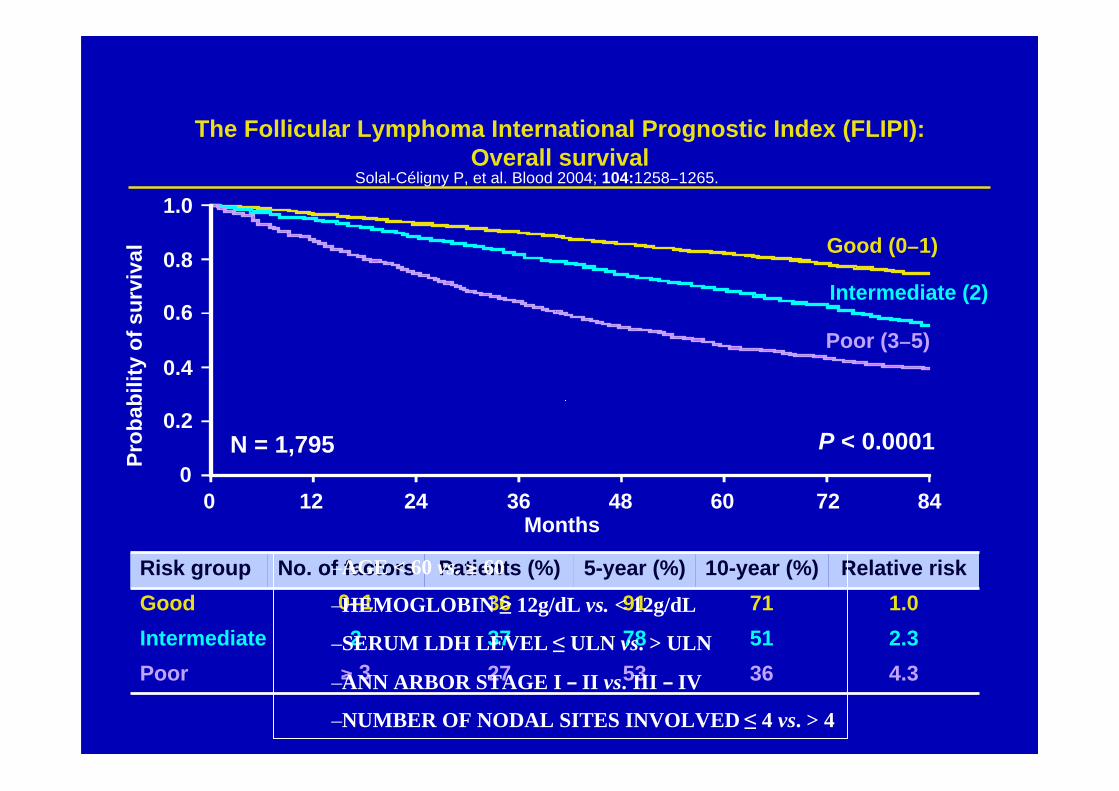
The Follicular Lymphoma International Prognostic Index (FLIPI):Overall survival
Prob
abili
ty o
f sur
viva
l
Months
P < 0.0001
Good (0−1)
Intermediate (2)
Poor (3−5)
1.0
0.8
0.6
0.4
0.2
00 12 24 36 48 60 72 84
N = 1,795
Risk group No. of factors Patients (%) 5-year (%) 10-year (%) Relative riskGood 0−1 36 91 71 1.0Intermediate 2 37 78 51 2.3Poor ≥ 3 27 53 36 4.3
Solal-Céligny P, et al. Blood 2004; 104:1258−1265.
–AGE < 60 vs. ≥ 60
–HEMOGLOBIN ≥ 12g/dL vs. < 12g/dL
–SERUM LDH LEVEL ≤ ULN vs. > ULN
–ANN ARBOR STAGE I – II vs. III – IV
–NUMBER OF NODAL SITES INVOLVED ≤ 4 vs. > 4
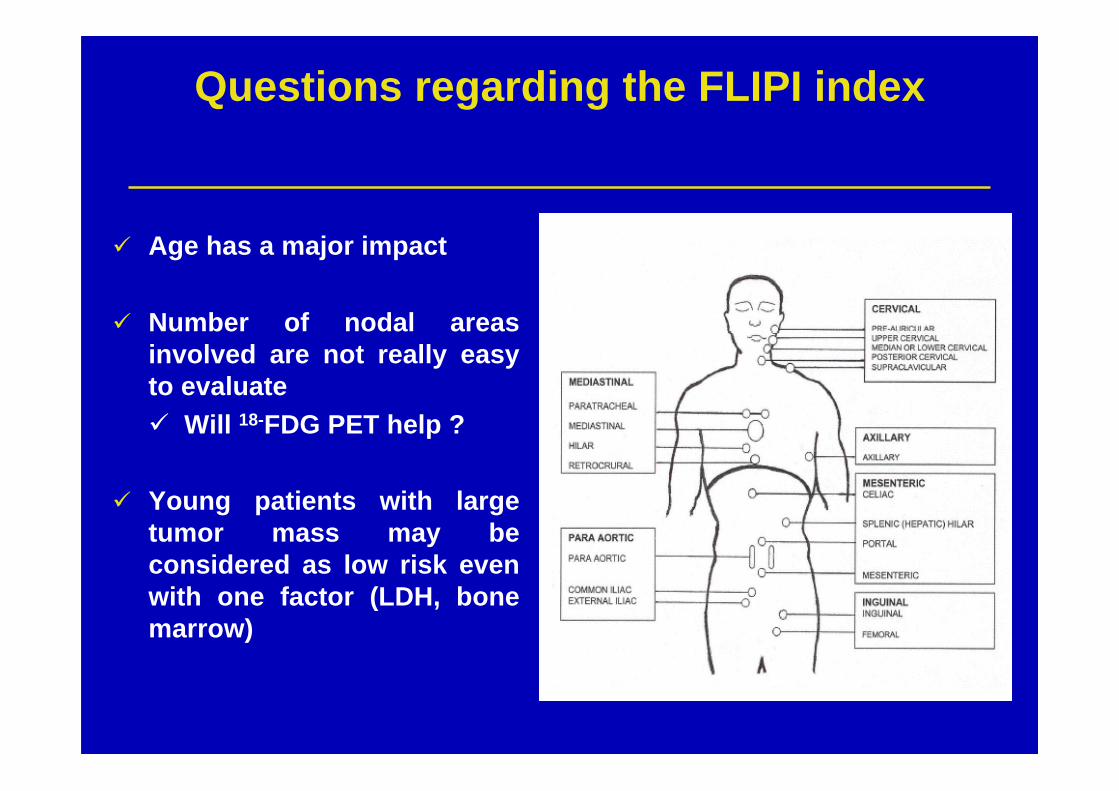
Questions regarding the FLIPI index
Age has a major impact
Number of nodal areasinvolved are not really easyto evaluate Will 18-FDG PET help ?
Young patients with largetumor mass may beconsidered as low risk evenwith one factor (LDH, bonemarrow)
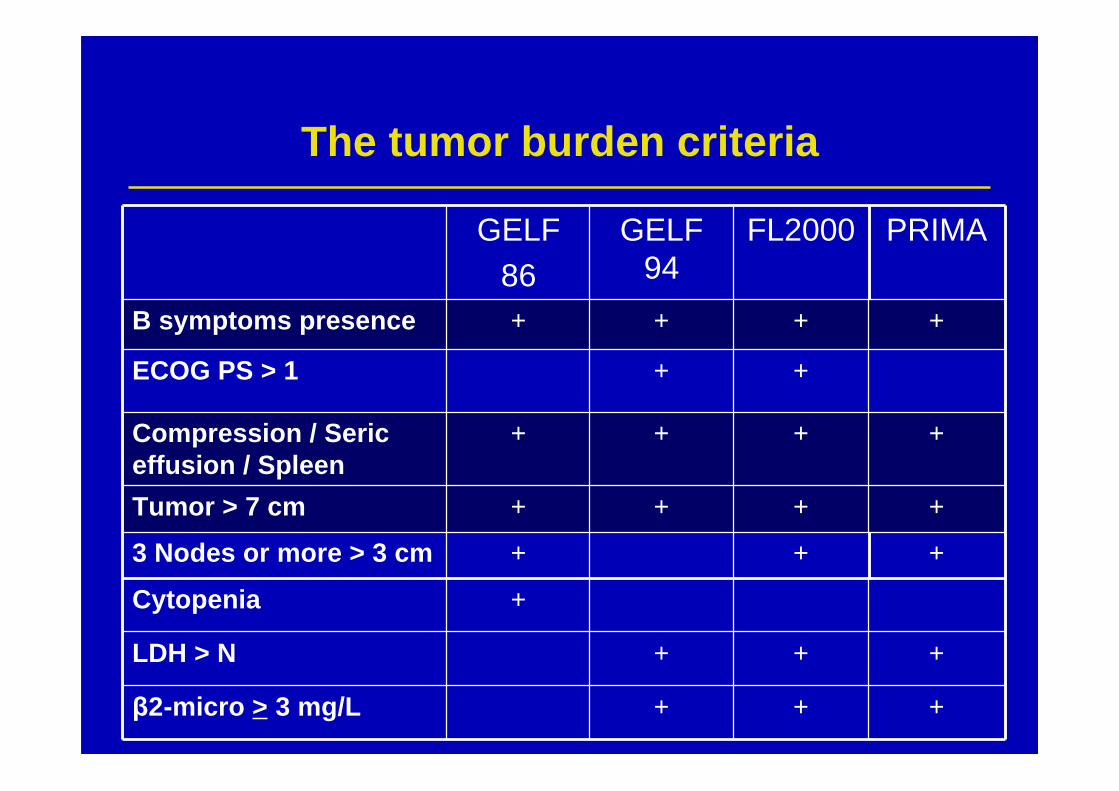
The tumor burden criteria
GELF86
GELF94
FL2000 PRIMA
B symptoms presence + + + +
ECOG PS > 1 + +
Compression / Sericeffusion / Spleen
+ + + +
Tumor > 7 cm + + + +
3 Nodes or more > 3 cm + + +
Cytopenia +
LDH > N + + +
β2-micro > 3 mg/L + + +
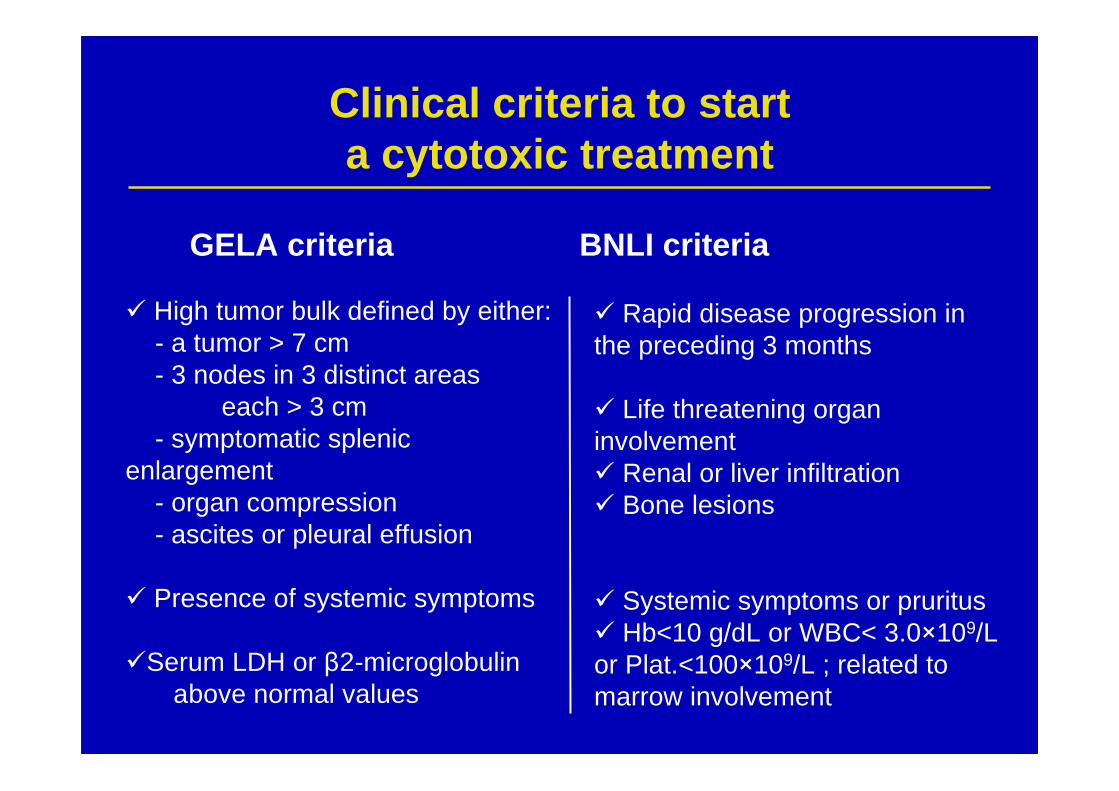
Clinical criteria to starta cytotoxic treatment
GELA criteria BNLI criteria
Rapid disease progression inthe preceding 3 months
Life threatening organinvolvement Renal or liver infiltration Bone lesions
Systemic symptoms or pruritus Hb<10 g/dL or WBC< 3.0×109/Lor Plat.<100×109/L ; related tomarrow involvement
High tumor bulk defined by either: - a tumor > 7 cm - 3 nodes in 3 distinct areas each > 3 cm - symptomatic splenic enlargement - organ compression - ascites or pleural effusion
Presence of systemic symptoms
Serum LDH or β2-microglobulinabove normal values
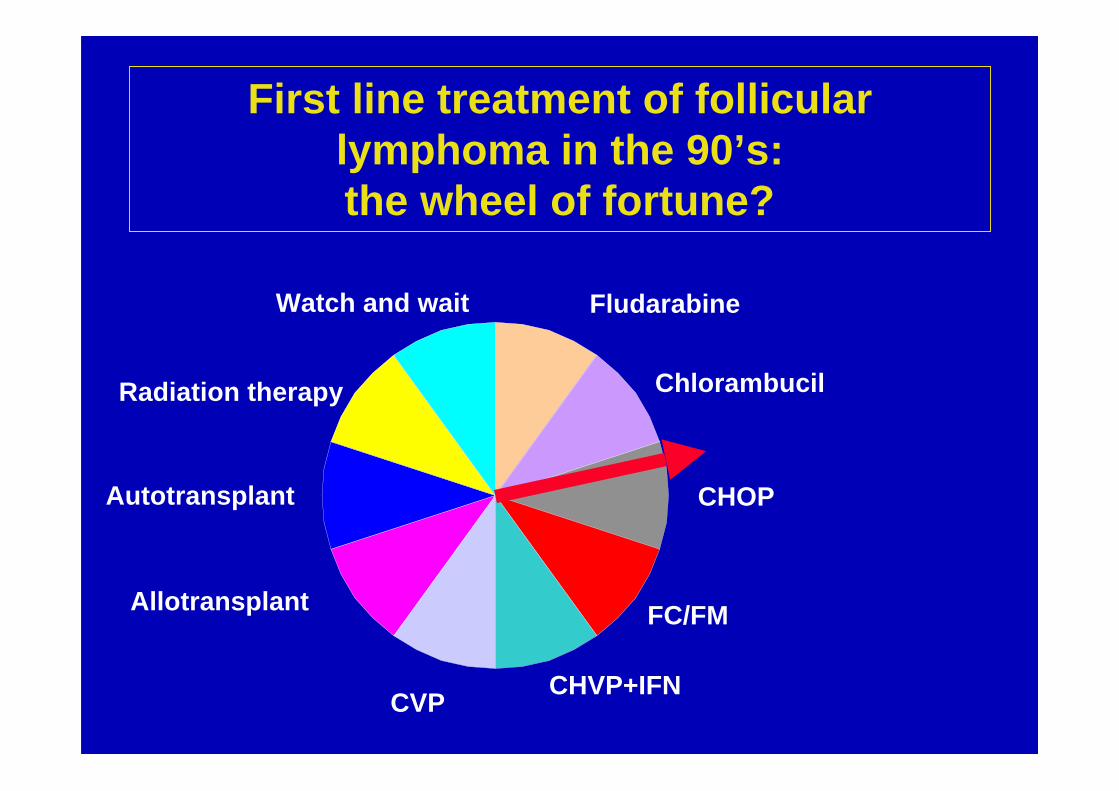
First line treatment of follicularlymphoma in the 90’s:the wheel of fortune?
Chlorambucil
Fludarabine
Radiation therapy
Autotransplant
Allotransplant
Watch and wait
CHVP+IFN
CHOP
CVP
FC/FM

Traitements deslymphomes folliculaires
Standards et options pour lespatients avec faible masse et les
stades localisés
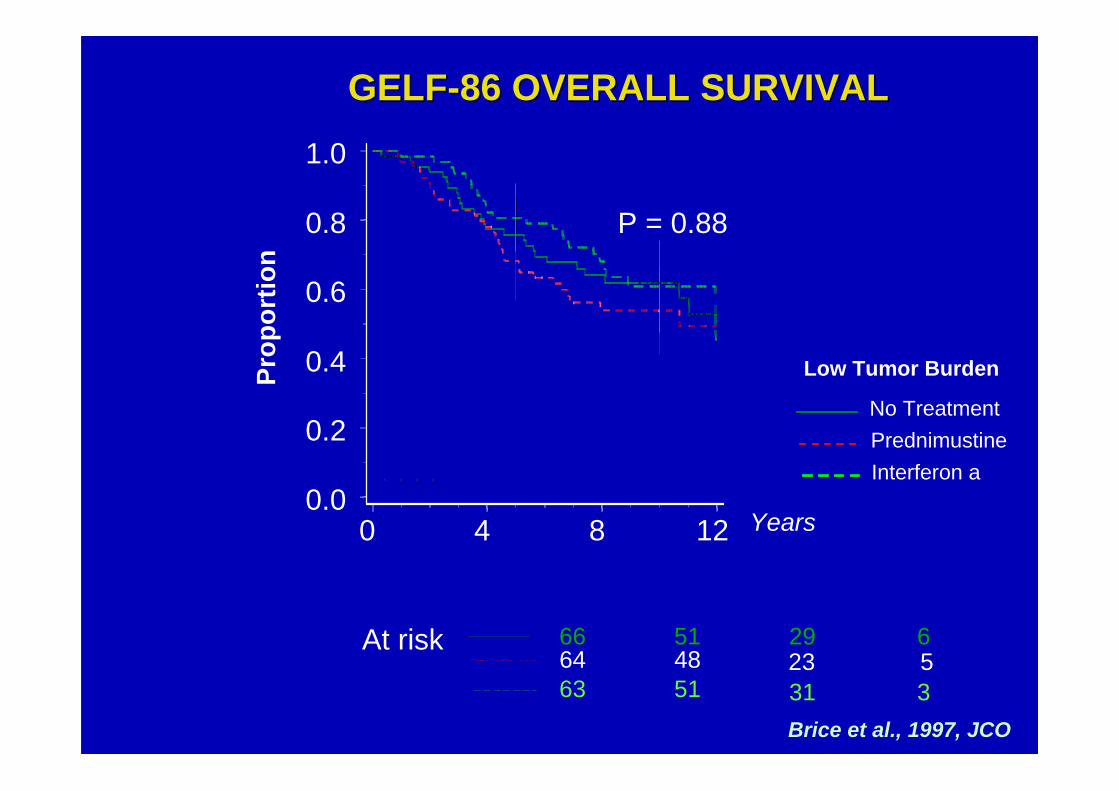
GELF-86 OVERALL SURVIVALGELF-86 OVERALL SURVIVAL
P = 0.88
At risk 66 51 29 6 64 48 23 5 63 51 31 3
Low Tumor Burden
No TreatmentPrednimustineInterferon a
0.0
0.2
0.4
0.6
0.8
1.0
Years0 4 8 12
Prop
ortio
n
Brice et al., 1997, JCO
Retarder la mise en route d’untraitement: surveillance armée
Le Watch and Wait est une option acceptable sur le planscientifique:– chez des patients “à faible risque”– 3 études randomisées
• temps médian pour début du traitement ~ 2 ans• mais 15 à 20% des patients ne seront pas traités
pendant 10 ans
Oui, cependant…– Pas toujours facile à accepter pour le patient– … et sans doute pas à l’origine de “progrés”
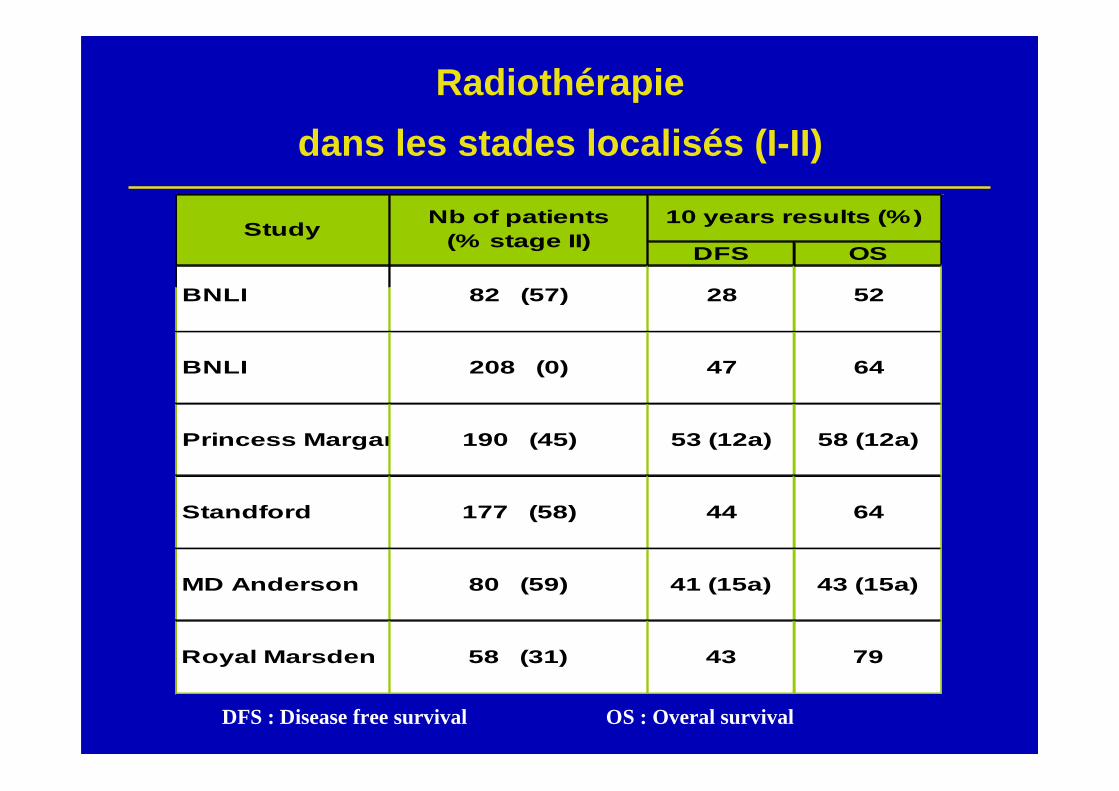
Radiothérapiedans les stades localisés (I-II)
DFS OS
BNLI 82 (57) 28 52
BNLI 208 (0) 47 64
Princess Margaret 190 (45) 53 (12a) 58 (12a)
Standford 177 (58) 44 64
MD Anderson 80 (59) 41 (15a) 43 (15a)
Royal Marsden 58 (31) 43 79
10 years results (%)Study Nb of patients (% stage II)
DFS : Disease free survival OS : Overal survival
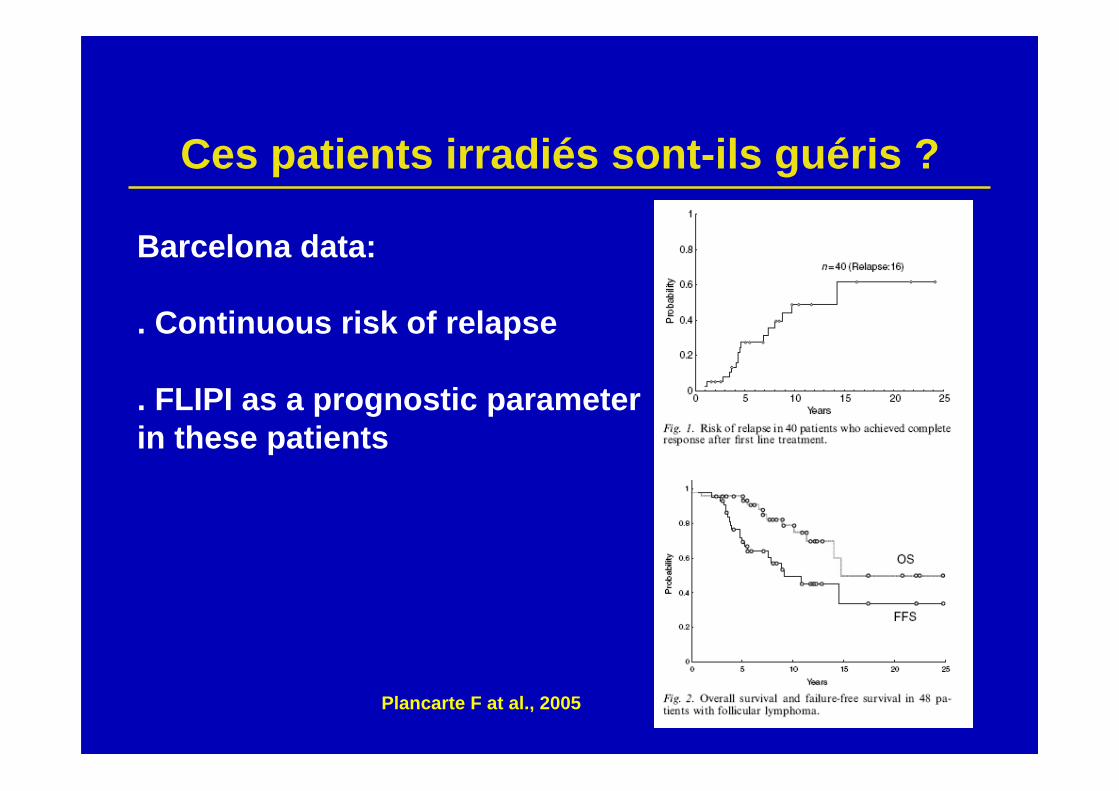
Ces patients irradiés sont-ils guéris ?
Barcelona data:
. Continuous risk of relapse
. FLIPI as a prognostic parameter in these patients
Plancarte F at al., 2005
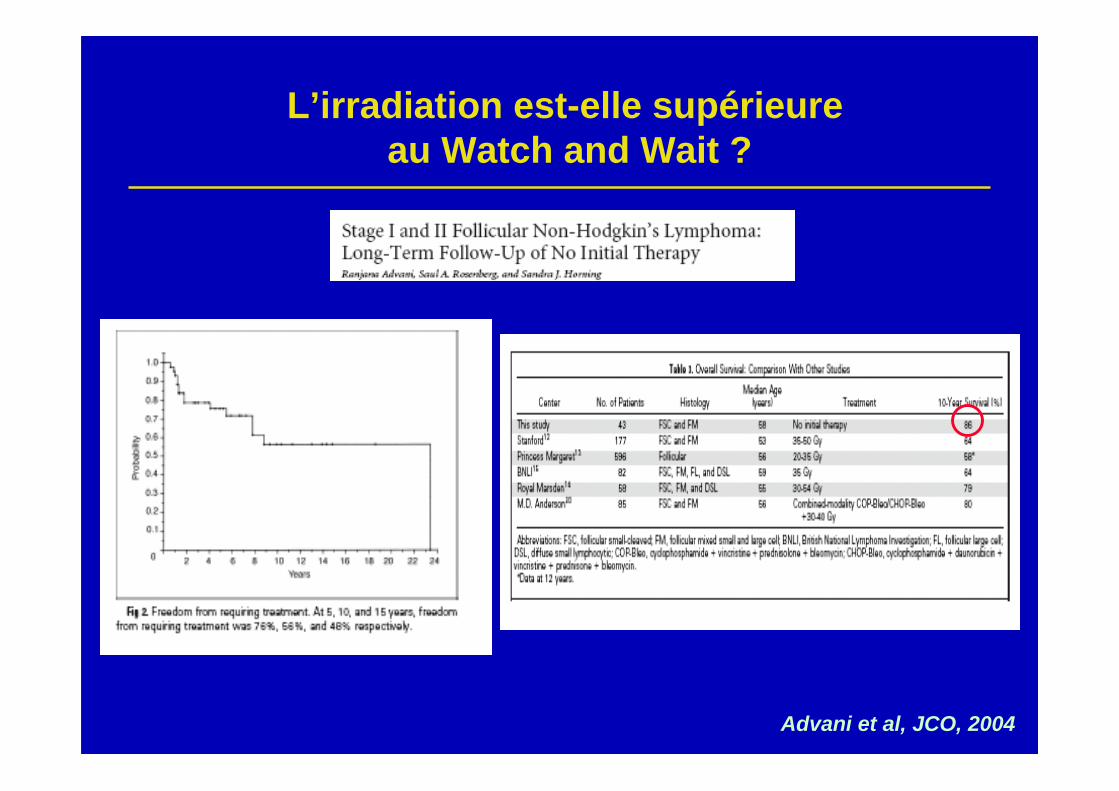
Advani et al, JCO, 2004
L’irradiation est-elle supérieure au Watch and Wait ?
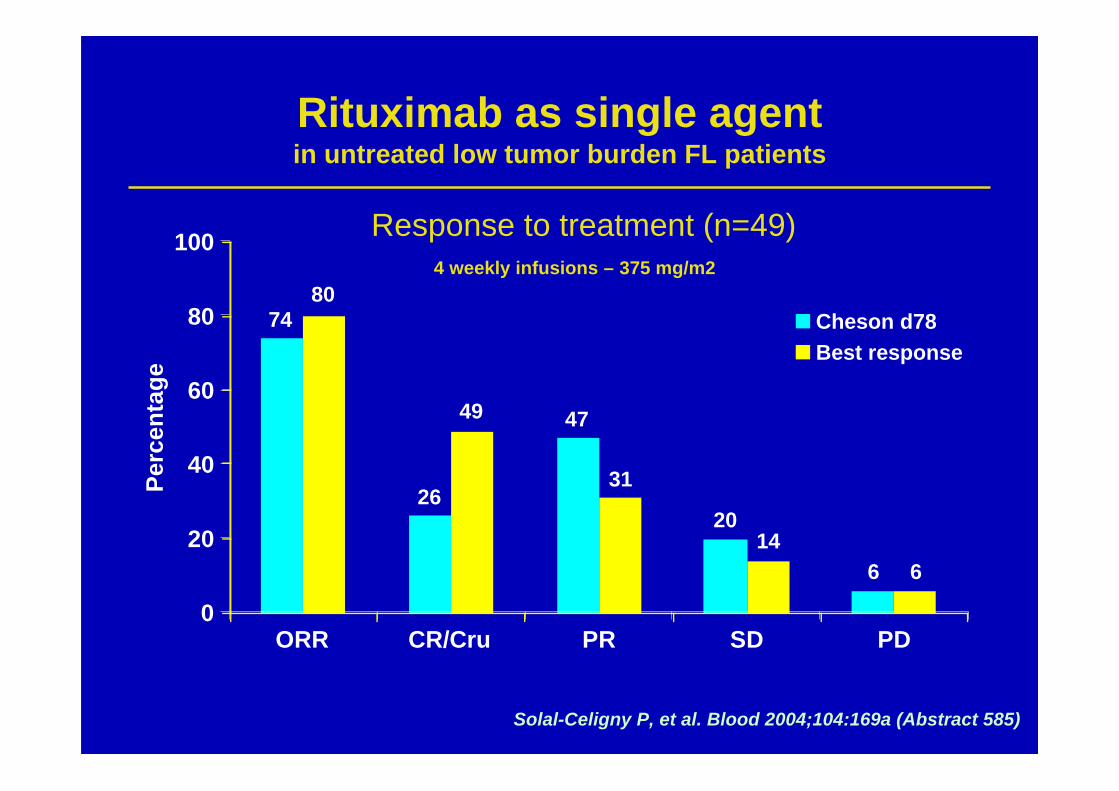
Rituximab as single agentin untreated low tumor burden FL patients
ORR CR/Cru PR SD PD
100
80
60
40
20
0
Perc
enta
ge
Cheson d78Best response
74
26
47
20
6
80
49
31
146
Solal-Celigny P, et al. Blood 2004;104:169a (Abstract 585)
Response to treatment (n=49)4 weekly infusions – 375 mg/m2
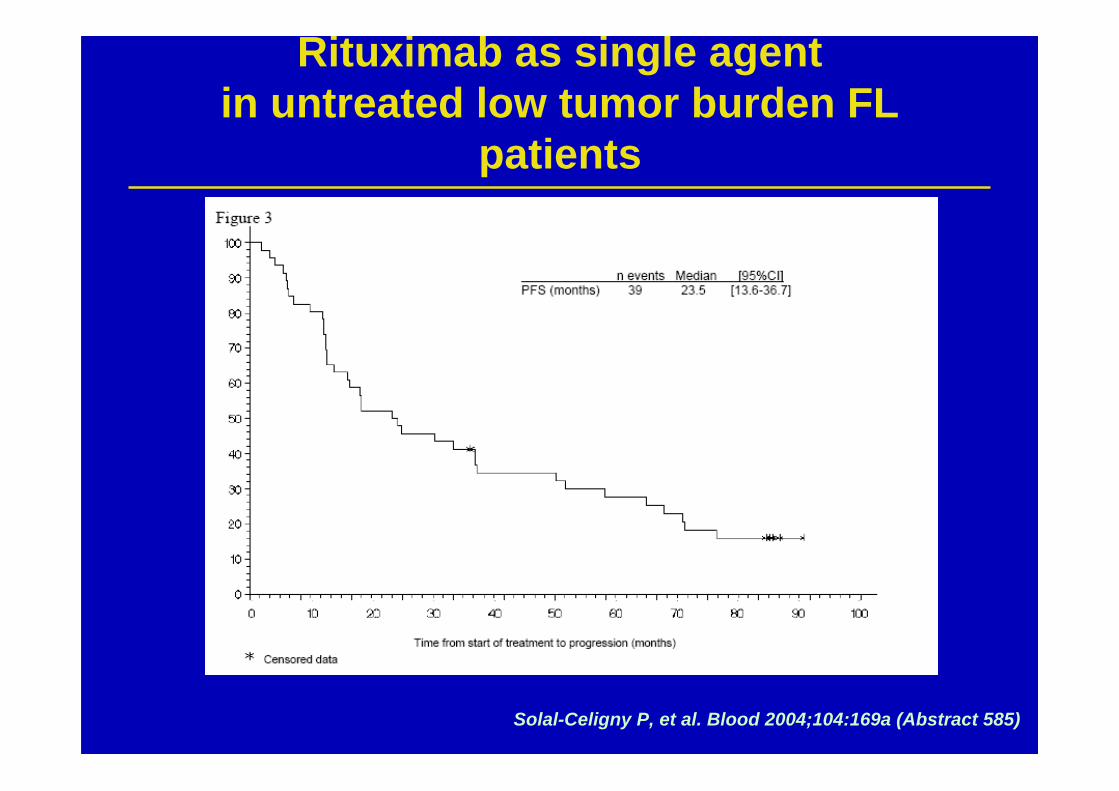
Rituximab as single agentin untreated low tumor burden FL
patients
Solal-Celigny P, et al. Blood 2004;104:169a (Abstract 585)
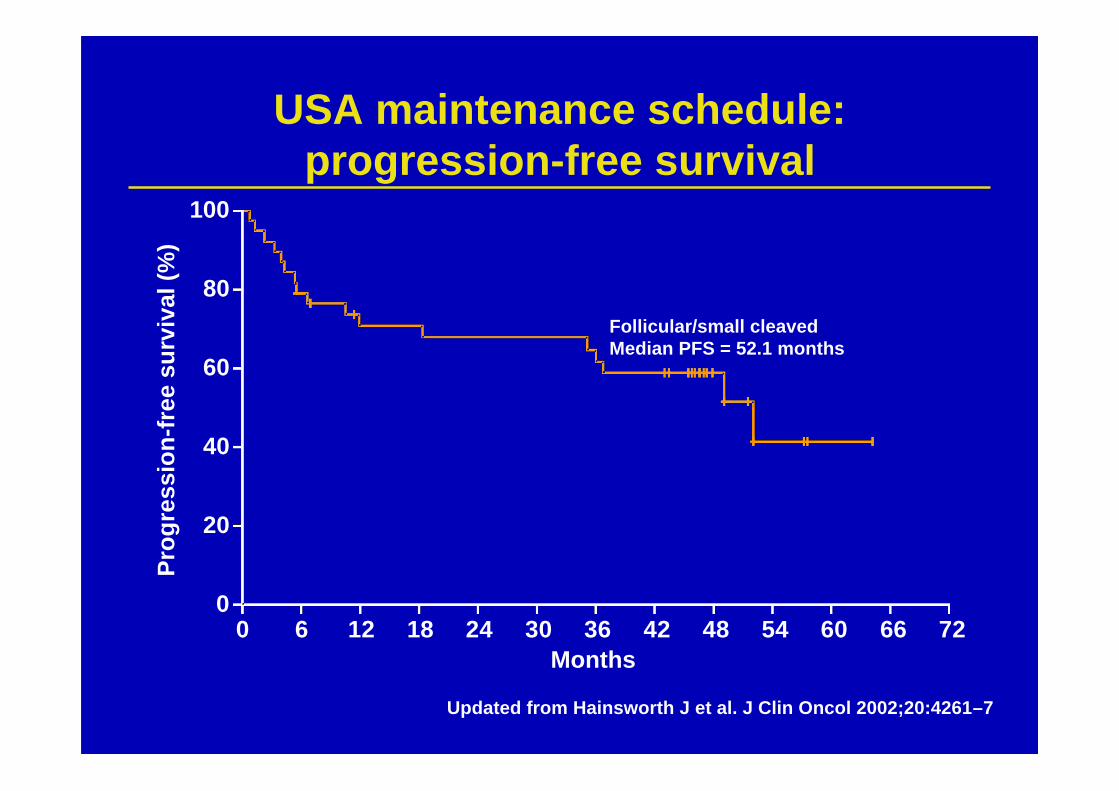
USA maintenance schedule:progression-free survival
Follicular/small cleavedMedian PFS = 52.1 months
Months
Prog
ress
ion-
free
sur
viva
l (%
)
100
80
60
40
20
00 6 12 18 24 30 36 42 48 54 60 66 72
Updated from Hainsworth J et al. J Clin Oncol 2002;20:4261–7
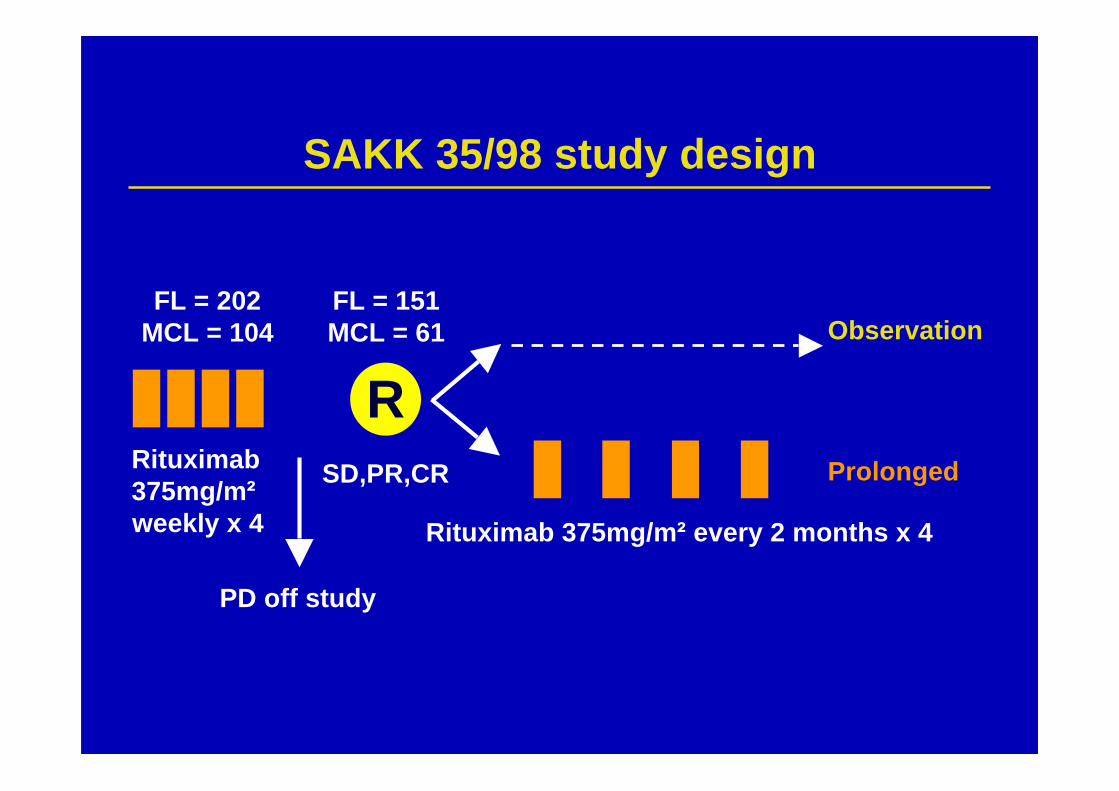
Rituximab 375mg/m² every 2 months x 4
FL = 151MCL = 61
PD off study
FL = 202MCL = 104
ProlongedRituximab375mg/m²weekly x 4
Observation
RSD,PR,CR
SAKK 35/98 study design
0.0
0.2
0.4
0.6
0.8
1.0 |
|| | |||
| | |
| ||||
| | || | || | | | || ||| | | |
0 1 2 3 4 5 6
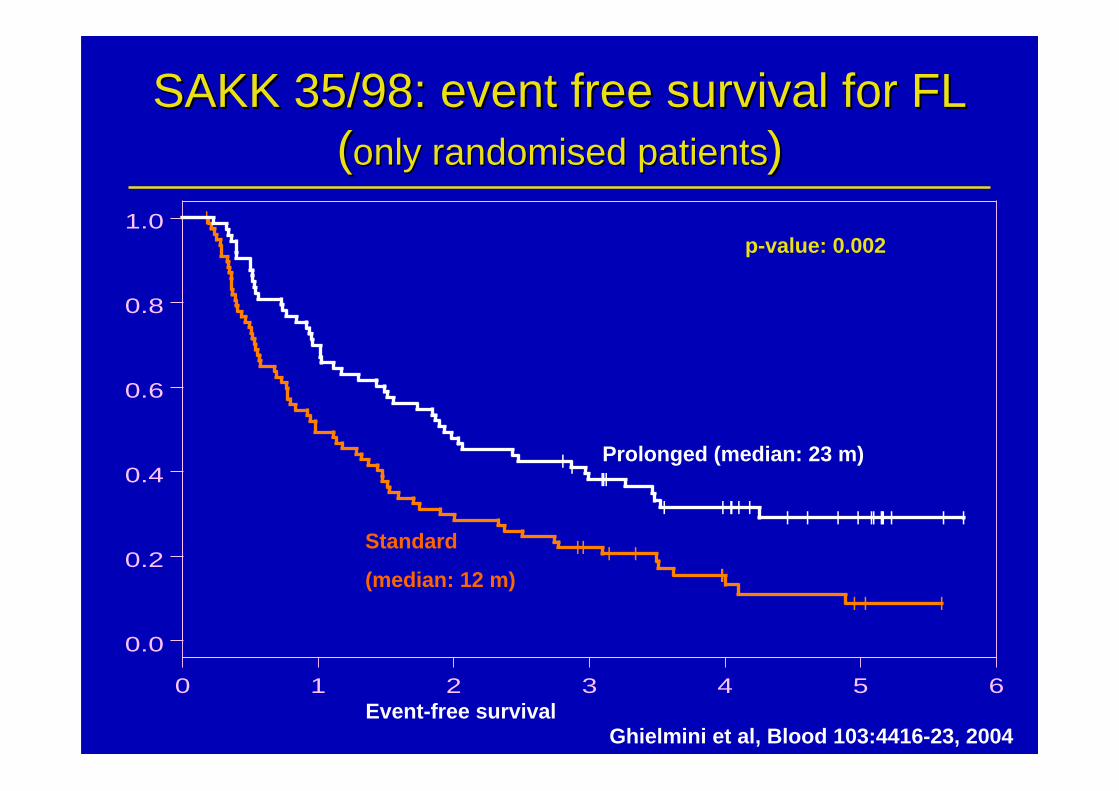
SAKK 35/98: event free survival for FLSAKK 35/98: event free survival for FL((only randomised patientsonly randomised patients))
Event-free survival
Prolonged (median: 23 m)
Standard
(median: 12 m)
p-value: 0.002
Ghielmini et al, Blood 103:4416-23, 2004
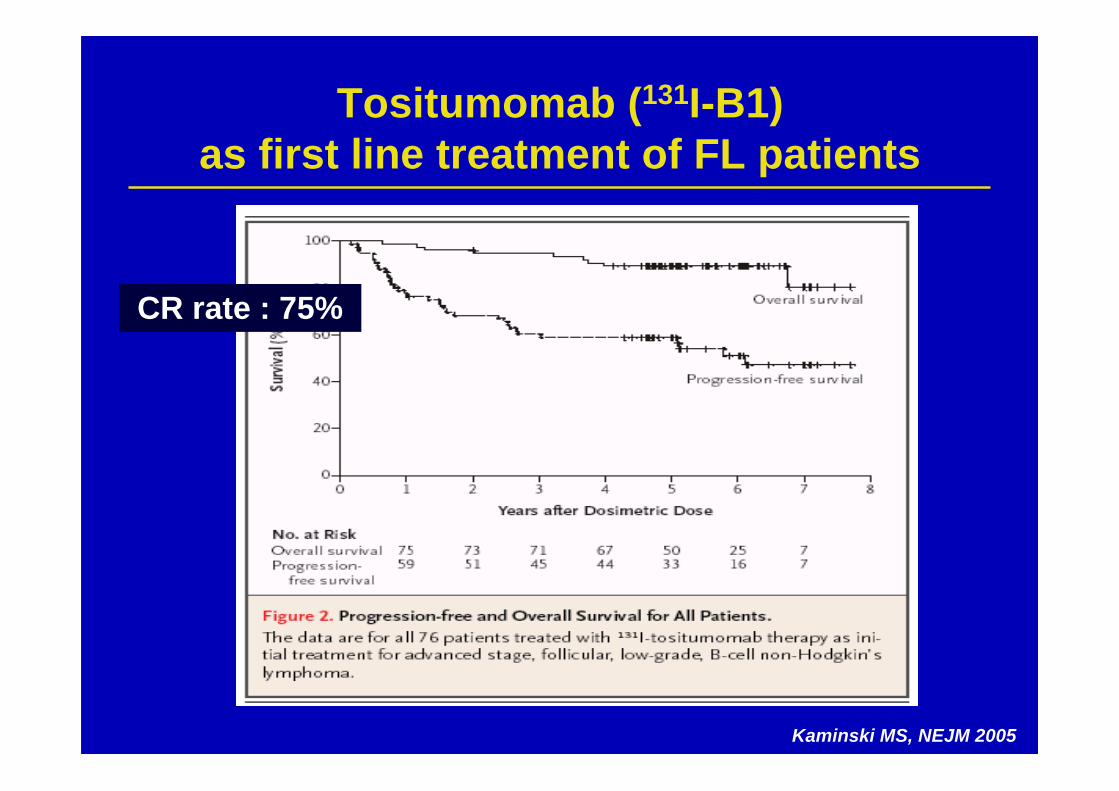
Tositumomab (131I-B1)as first line treatment of FL patients
Kaminski MS, NEJM 2005
CR rate : 75%
Autres optionschez des patients de faible risque ?
1) Anti-CD20: - ttt d’entretien: 3 essais en attente (RESORT, RWW, and SAKK) - doses élevées de rituximab ? Autres anti-CD20 ?
2) Radio-immunotherapie:- disponibilité ? Risques à long terme ?
3) Associer le rituximab avec des cytokines, d’autres Mabs,ou des agents immunomodulateurs ?
- IFN, GM-CSF, IL-2(Davis 2000 ; Sacchi 2001 ; Kimby 2002 ; Bosly 2004, Cartron 2007)- Anti-CD22, -CD40, -CD80, etc…- Lenalidomide = R2 regimen ?

Traitements deslymphomes folliculaires
Standards et options pour lespatients de forte masse
Traitements deslymphomes folliculaires
Ce que nous savons des essais menés avantles anticorps monoclonaux:
– Bénéfice des anthracyclines non démontré– Place des analogues de purines discutée
– Effet positif de l’interféron-α
– Pas de bénéfice évident de l’autogreffe• Peut-être un contrôle de la maladie meilleur pour
les patients les plus graves• Mais au prix d’une toxicité peu acceptable
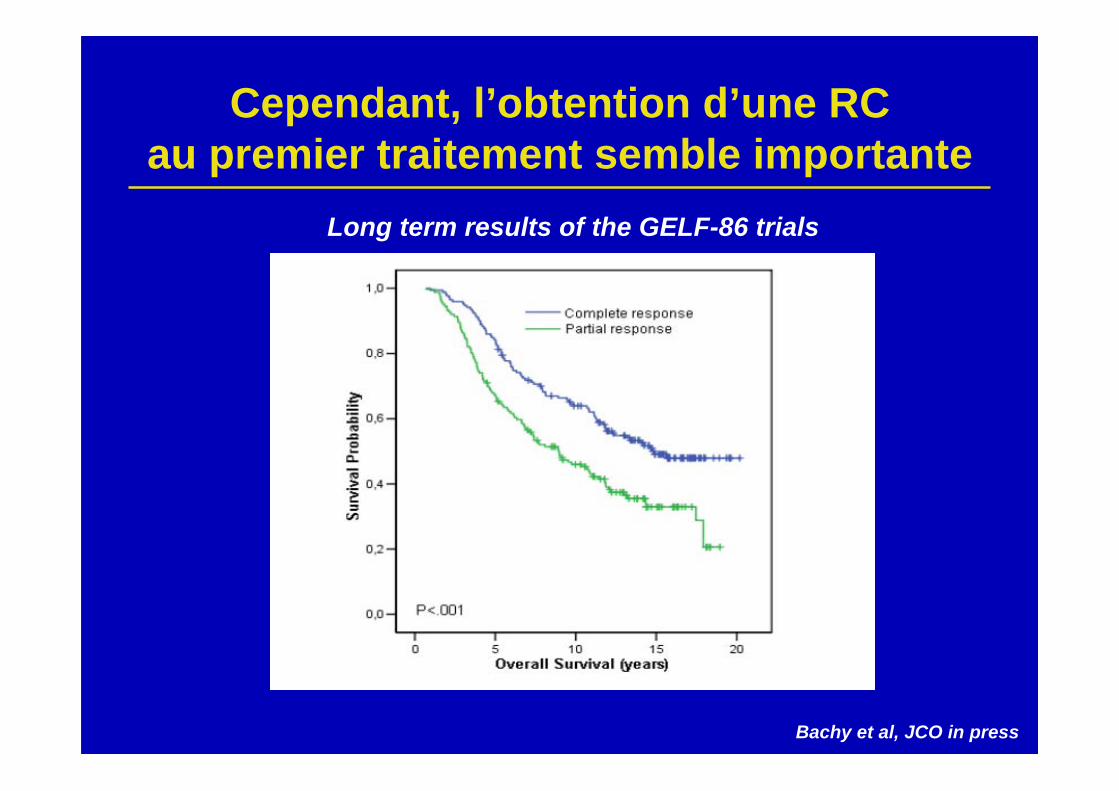
Cependant, l’obtention d’une RCau premier traitement semble importante
Long term results of the GELF-86 trials
Bachy et al, JCO in press
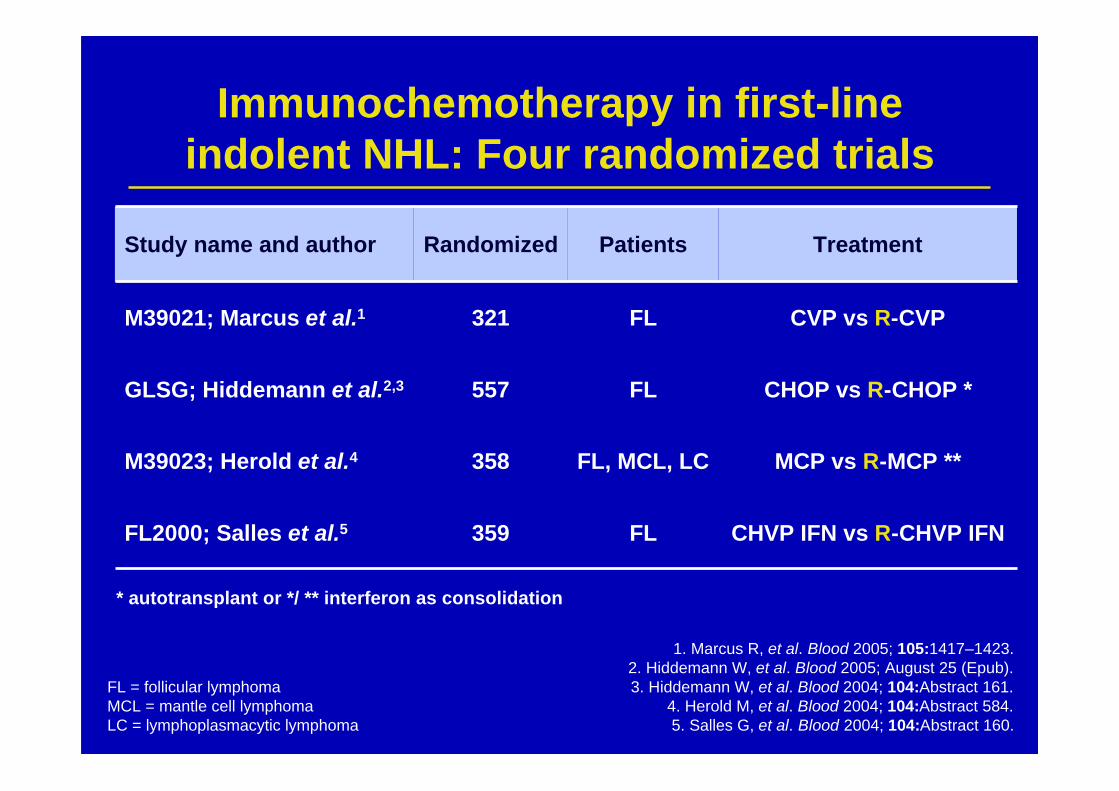
Immunochemotherapy in first-lineindolent NHL: Four randomized trials
1. Marcus R, et al. Blood 2005; 105:1417–1423.2. Hiddemann W, et al. Blood 2005; August 25 (Epub).3. Hiddemann W, et al. Blood 2004; 104:Abstract 161.
4. Herold M, et al. Blood 2004; 104:Abstract 584.5. Salles G, et al. Blood 2004; 104:Abstract 160.
FL = follicular lymphomaMCL = mantle cell lymphomaLC = lymphoplasmacytic lymphoma
Study name and author Randomized Patients Treatment
M39021; Marcus et al.1 321 FL CVP vs R-CVP
GLSG; Hiddemann et al.2,3 557 FL CHOP vs R-CHOP *
M39023; Herold et al.4 358 FL, MCL, LC MCP vs R-MCP **
FL2000; Salles et al.5 359 FL CHVP IFN vs R-CHVP IFN
* autotransplant or */ ** interferon as consolidation
Even
t-fre
e pr
obab
ility
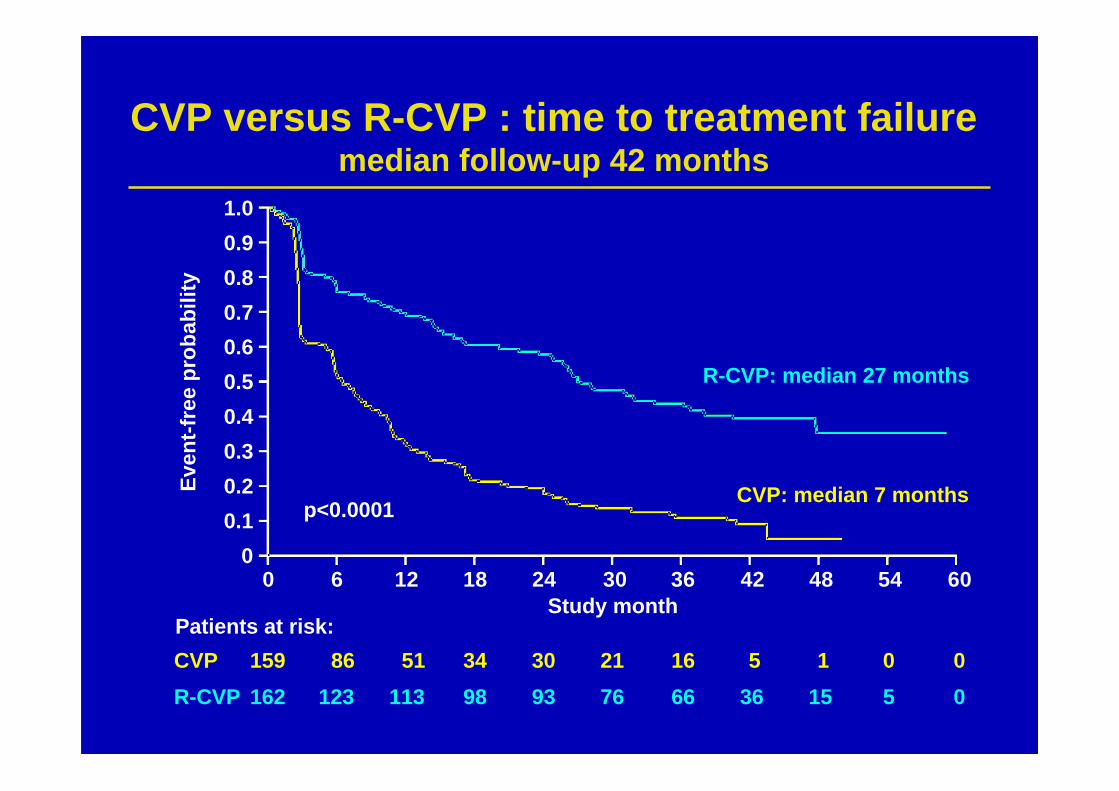
CVP versus R-CVP : time to treatment failuremedian follow-up 42 months
159CVPR-CVP
Patients at risk:
162 86123
51113
3498
3093
2176
1666
536
115
05
00
R-CVP: median 27 months
CVP: median 7 monthsp<0.0001
1.00.90.80.70.60.50.40.30.20.1
00 6 12 18 24 30 36 42 48 54 60
Study month
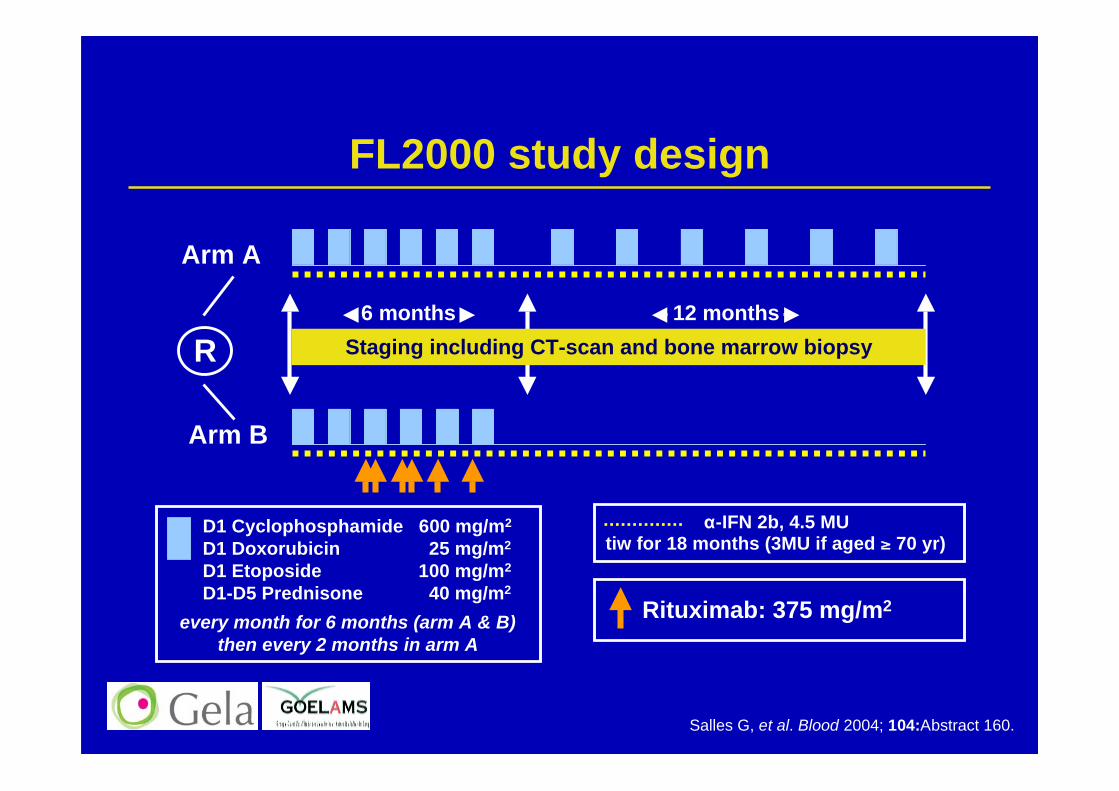
FL2000 study design
α-IFN 2b, 4.5 MUtiw for 18 months (3MU if aged ≥ 70 yr)
D1 Cyclophosphamide 600 mg/m2
D1 Doxorubicin 25 mg/m2
D1 Etoposide 100 mg/m2
D1-D5 Prednisone 40 mg/m2
every month for 6 months (arm A & B)then every 2 months in arm A
Rituximab: 375 mg/m2
R
Arm A
Arm B
Staging including CT-scan and bone marrow biopsy12 months6 months
Salles G, et al. Blood 2004; 104:Abstract 160.
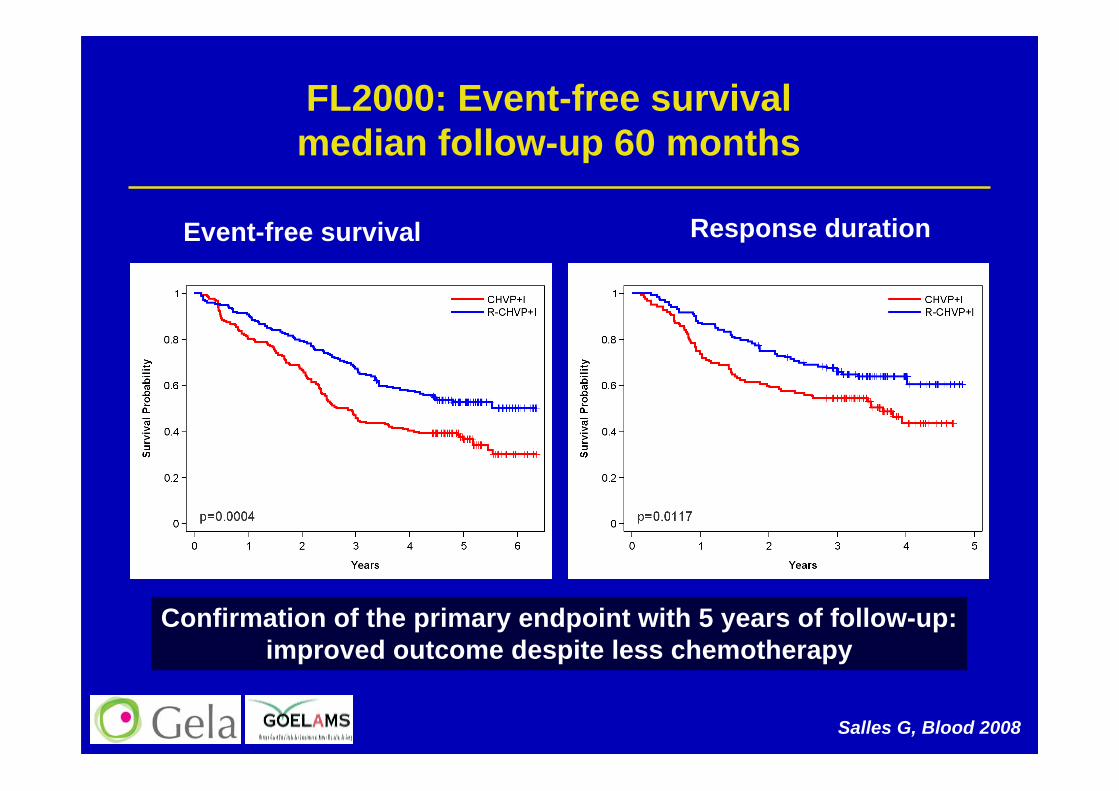
FL2000: Event-free survivalmedian follow-up 60 months
Event-free survival Response duration
Confirmation of the primary endpoint with 5 years of follow-up:improved outcome despite less chemotherapy
Salles G, Blood 2008
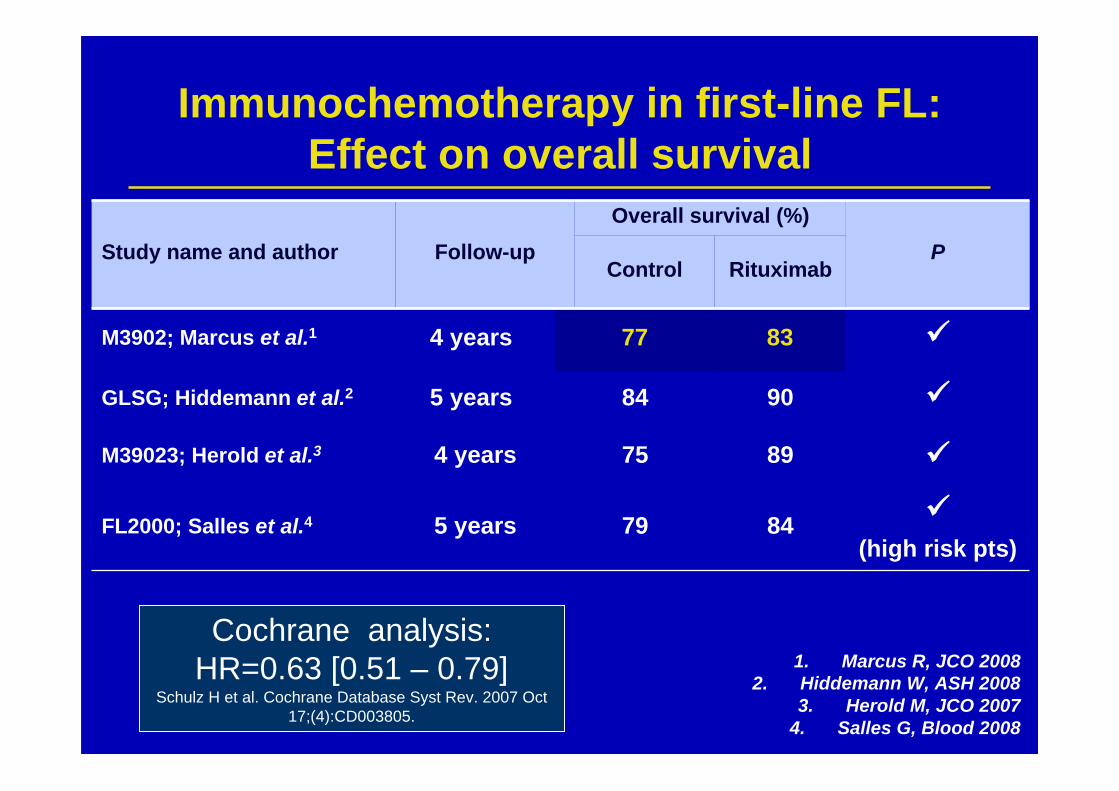
Study name and author Follow-upOverall survival (%)
PControl Rituximab
M3902; Marcus et al.1 4 years 77 83
GLSG; Hiddemann et al.2 5 years 84 90
M39023; Herold et al.3 4 years 75 89
FL2000; Salles et al.4 5 years 79 84 (high risk pts)
Cochrane analysis:HR=0.63 [0.51 – 0.79]
Schulz H et al. Cochrane Database Syst Rev. 2007 Oct17;(4):CD003805.
Immunochemotherapy in first-line FL:Effect on overall survival
1. Marcus R, JCO 20082. Hiddemann W, ASH 2008
3. Herold M, JCO 20074. Salles G, Blood 2008
Fortes masses:
Quelles voies de progrès ?
Follicular lymphoma : the next steps?
6–8xR-CVPorR-CHOP
Maintenancewithrituximab?PRIMAstudy
CombinewithotherMaborcytokines
Intensifywithhigh-doseorRx-Ab?Ri-CHOPstudy;SWOGstudy
Otherchemotherapydrugs?
Fludarabine?Bendamustine?
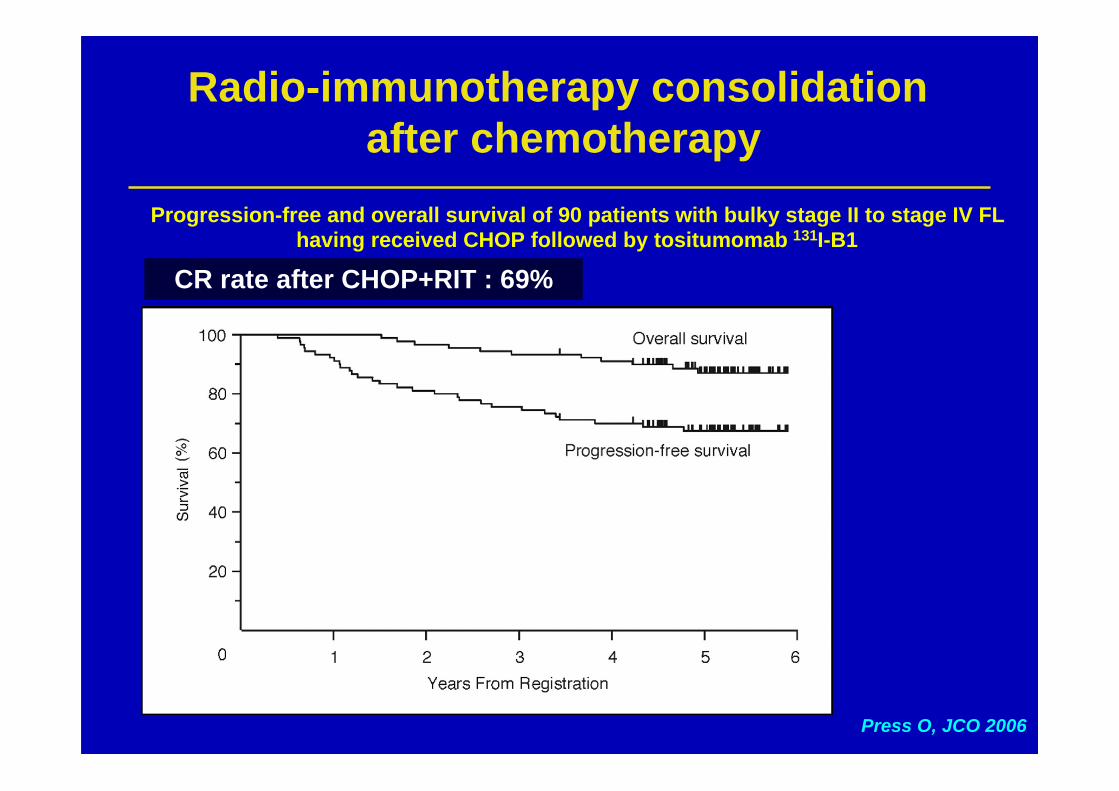
Press O, JCO 2006
Progression-free and overall survival of 90 patients with bulky stage II to stage IV FLhaving received CHOP followed by tositumomab 131I-B1
Radio-immunotherapy consolidation after chemotherapy
CR rate after CHOP+RIT : 69%
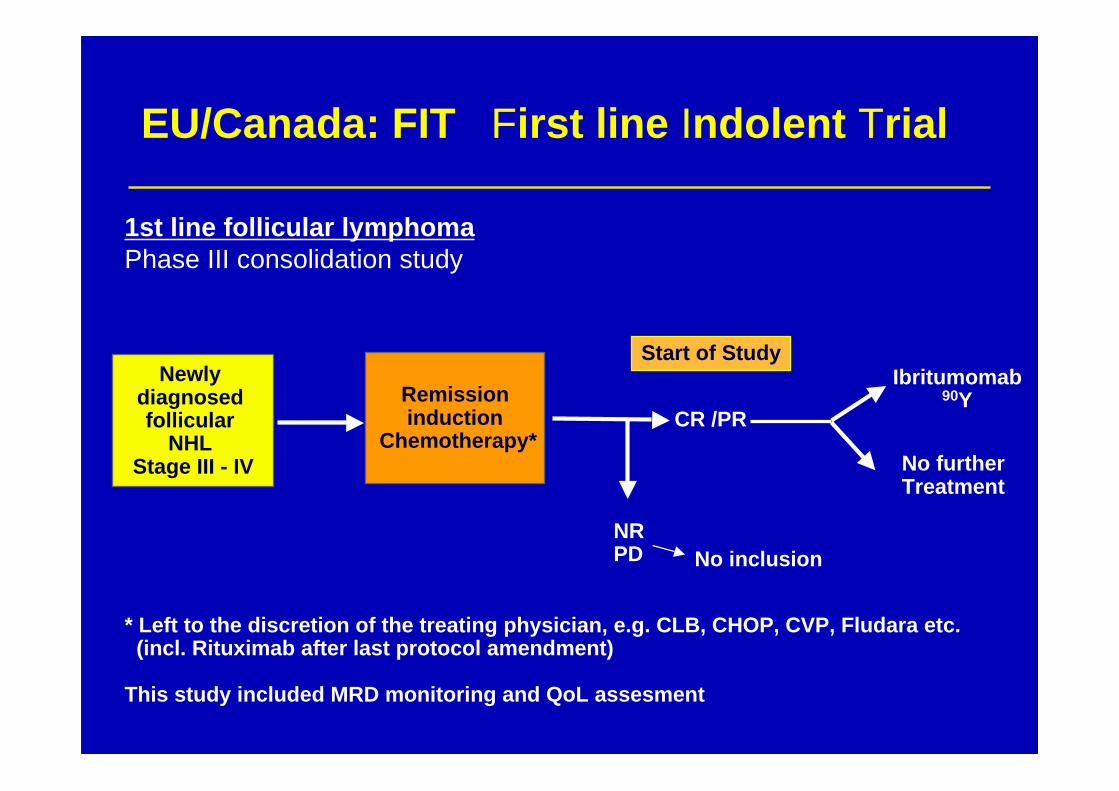
Remissioninduction
Chemotherapy*
Newly diagnosed follicular
NHL Stage III - IV
CR /PR
NRPD No inclusion
Ibritumomab90Y
No furtherTreatment
* Left to the discretion of the treating physician, e.g. CLB, CHOP, CVP, Fludara etc. (incl. Rituximab after last protocol amendment)
This study included MRD monitoring and QoL assesment
Start of Study
EU/Canada: FIT First line Indolent Trial
1st line follicular lymphoma Phase III consolidation study
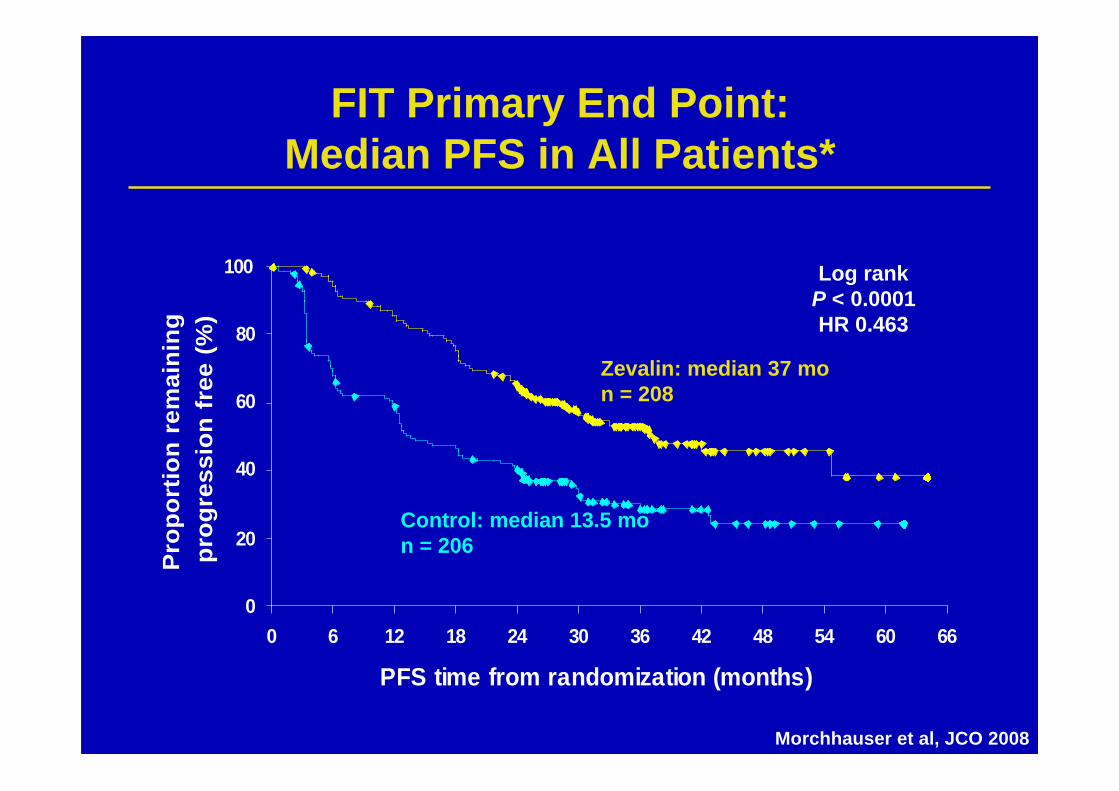
FIT Primary End Point:Median PFS in All Patients*
0
20
40
60
80
100
0 6 12 18 24 30 36 42 48 54 60 66
PFS time from randomization (months)
Pro
port
ion
rem
aini
ng
prog
ress
ion
free
(%
)
Log rankP < 0.0001HR 0.463
Zevalin: median 37 mon = 208
Control: median 13.5 mon = 206
Morchhauser et al, JCO 2008
Rationale fo rituximab maintenance
Maintenance therapy against lymphoma more efficient in a state ofminimal residual disase
Long half life of the antibody in vivo– Target level of 25 µg/ml– 95% will have this level if the drug is given every 3 months– Gordan et al, JCO 23:1096-1102, 2005
Rituximab immunological mediated actions?– ADCC– Antigen presentation by dendritic cells??
Good safety profile of the antibody
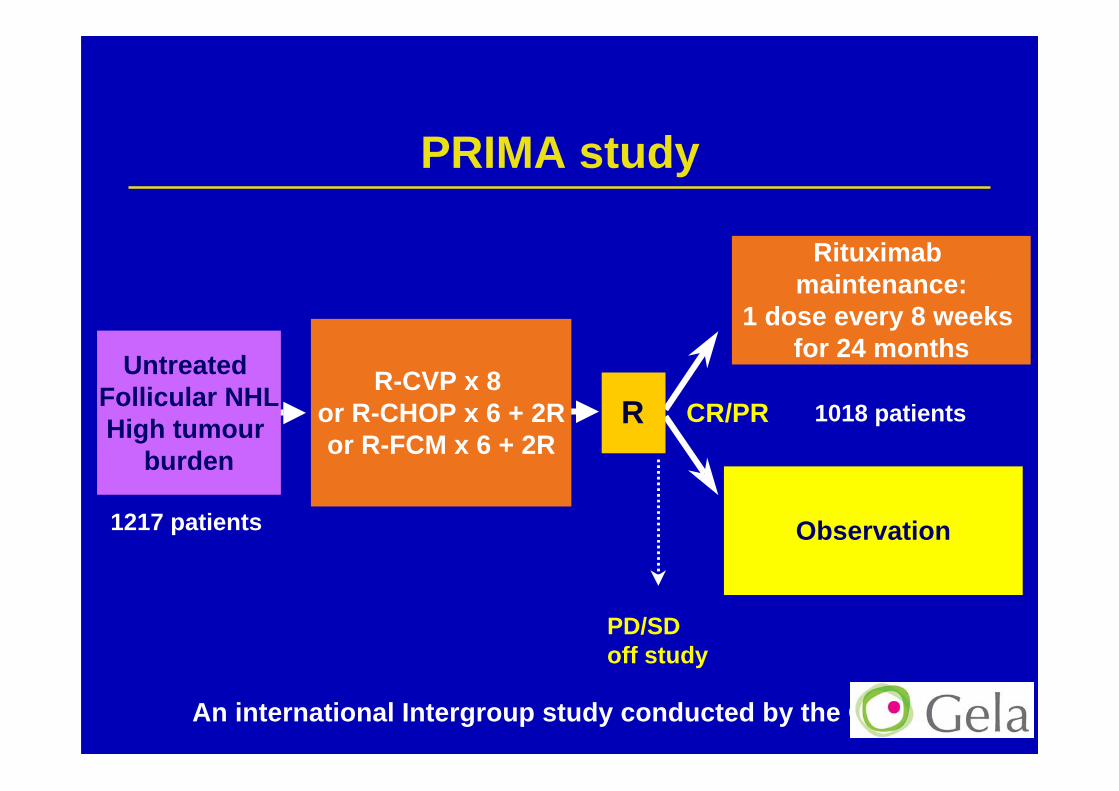
An international Intergroup study conducted by the GELA
PD/SDoff study
Rituximab maintenance:
1 dose every 8 weeks for 24 months
Observation
R CR/PRR-CVP x 8
or R-CHOP x 6 + 2Ror R-FCM x 6 + 2R
Untreated Follicular NHLHigh tumour
burden
PRIMA study
1217 patients
1018 patients
PRIMA: An internationalcollaborative effort
Résultats de PRIMA ?
Soumis à l’ASH 2009 :
RITUXIMAB MAINTENANCE FOR 2-YEARS SIGNIFICANTLY IMPROVESTHE OUTCOME OF PATIENTS WITH UNTREATED HIGH TUMORBURDEN FOLLICULAR LYMPHOMA AFTER RESPONSE TOIMMUNOCHEMOTHERAPY: RESULTS OF THE PRIMA STUDY.
Maintenance : questions to be solved? Optimal scheme?
How long should rituximab maintenance be given?
Safety of rituximab maintenance?
Characteristics of patients relapsing during / afterrituximab maintenance?
Re-treatment after maintenance?
Follicular lymphoma:next steps?
6 - 8R-CVP or R-CHOP
Maintenance withrituximab ?
PRIMA study
Combine with cytokines(IFN, GM-CSF)
Intensify usingASCT
Ri-CHOP study
Other chemotherapy(purine analogues ?)
German study
Consolidateusing RIT ?
FIT
Other drugs?Targeted therapies?(lenalidomide, bortezomib, …)
next generationanti-CD20?
Vaccines
Role of PET??
Traitements deslymphomes folliculaires
Les choix thérapeutiques en rechute
– Que veut-on obtenir ?– Quels outils, quels bénéfices ?– Quelles voies de progrès ?
Au moment de la rechute,le choix thérapeutique devient complexe
Possibilités thérapeutiques:– Ne rien faire et surveiller (W&W)– Le rituximab en monothérapie– Les Ac radiomarqués– Les agents alkylants en monothérapie– Les combinaisons de type (FCM, DHAP, MIV…)– L’autogreffe– Entretien par rituximab après une seconde ligne– L’allogreffe– Essais thérapeutiques et nouvelles drogues…
• Bendamustine• Nouveaux anticorps (anti-CD20, autres)• Immunoconjugués (CMC542)• Inhibiteurs du protéasome• Immunomodulation,• Anti-BCL2….
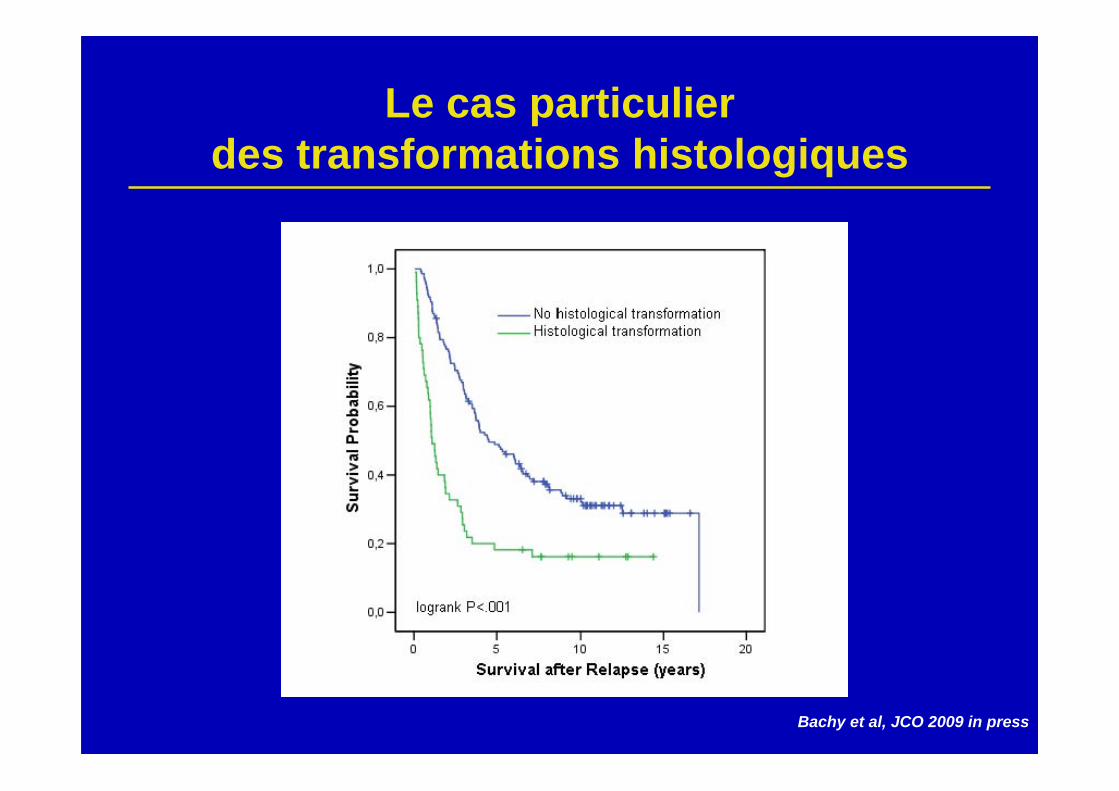
Le cas particulierdes transformations histologiques
Bachy et al, JCO 2009 in press
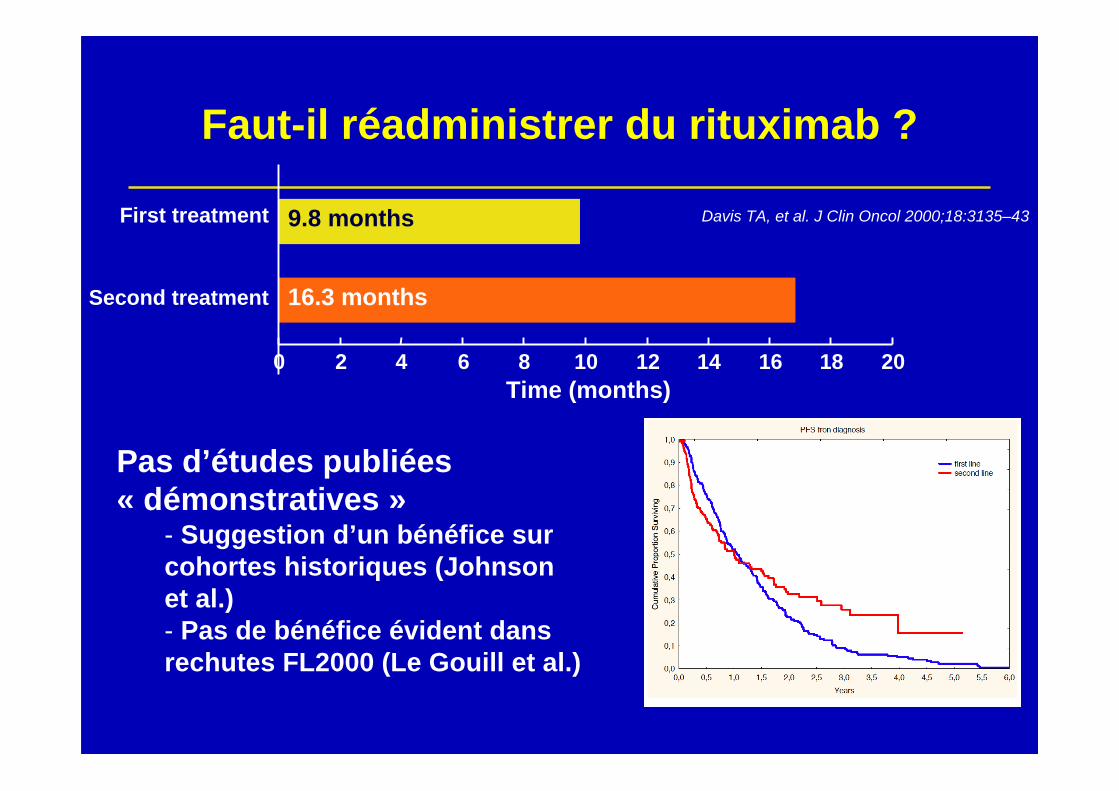
Faut-il réadministrer du rituximab ?
Davis TA, et al. J Clin Oncol 2000;18:3135–43
16.3 months
9.8 months
0 2 4 6 8 10 12 14 16 18 20
Second treatment
First treatment
Time (months)
Pas d’études publiées« démonstratives »
- Suggestion d’un bénéfice surcohortes historiques (Johnsonet al.)- Pas de bénéfice évident dansrechutes FL2000 (Le Gouill et al.)
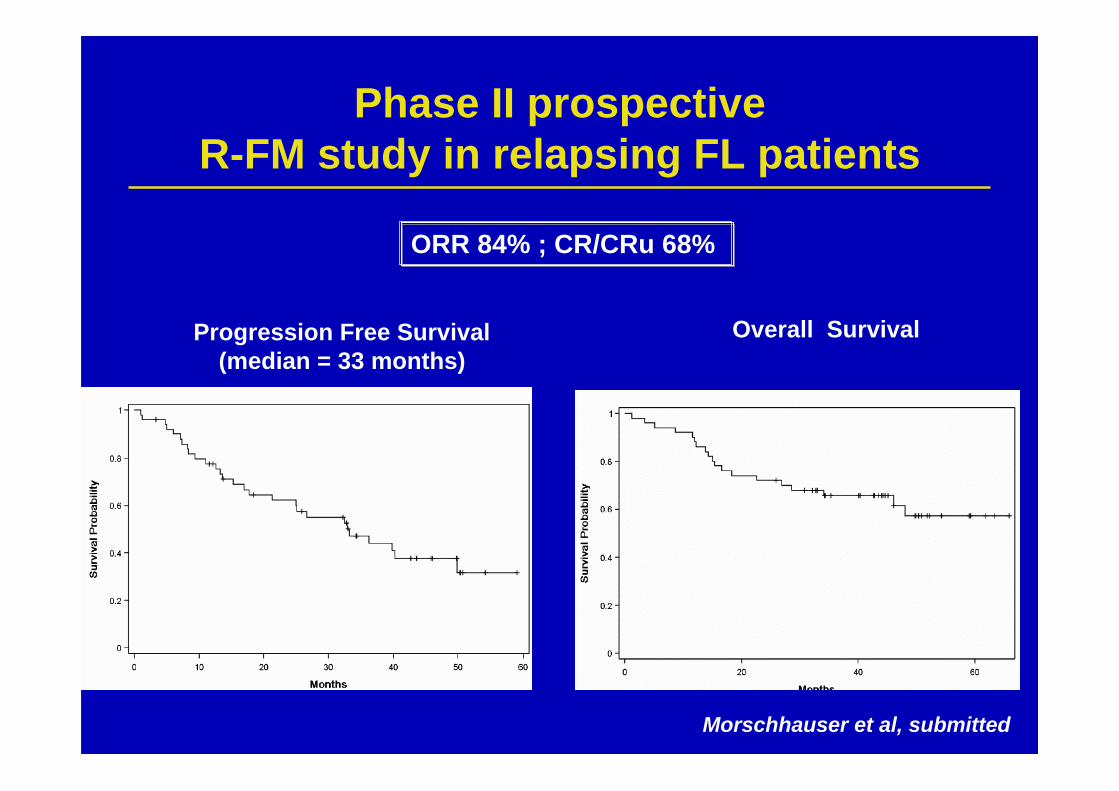
Phase II prospectiveR-FM study in relapsing FL patients
Morschhauser et al, submitted
Progression Free Survival(median = 33 months)
Overall Survival
ORR 84% ; CR/CRu 68%
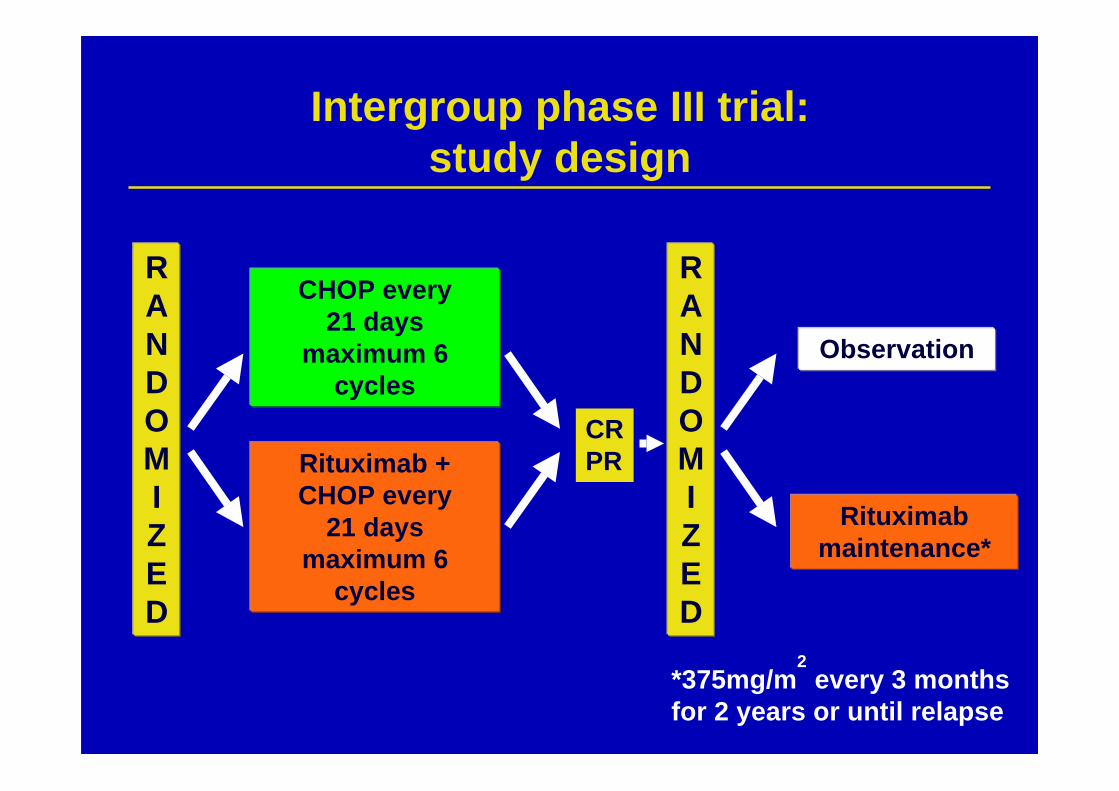
RANDOMIZED
CHOP every21 days
maximum 6cycles
Rituximab +CHOP every
21 daysmaximum 6
cycles
Intergroup phase III trial:study design
RANDOMIZED
Observation
Rituximabmaintenance*
*375mg/m2 every 3 months
for 2 years or until relapse
CRPR
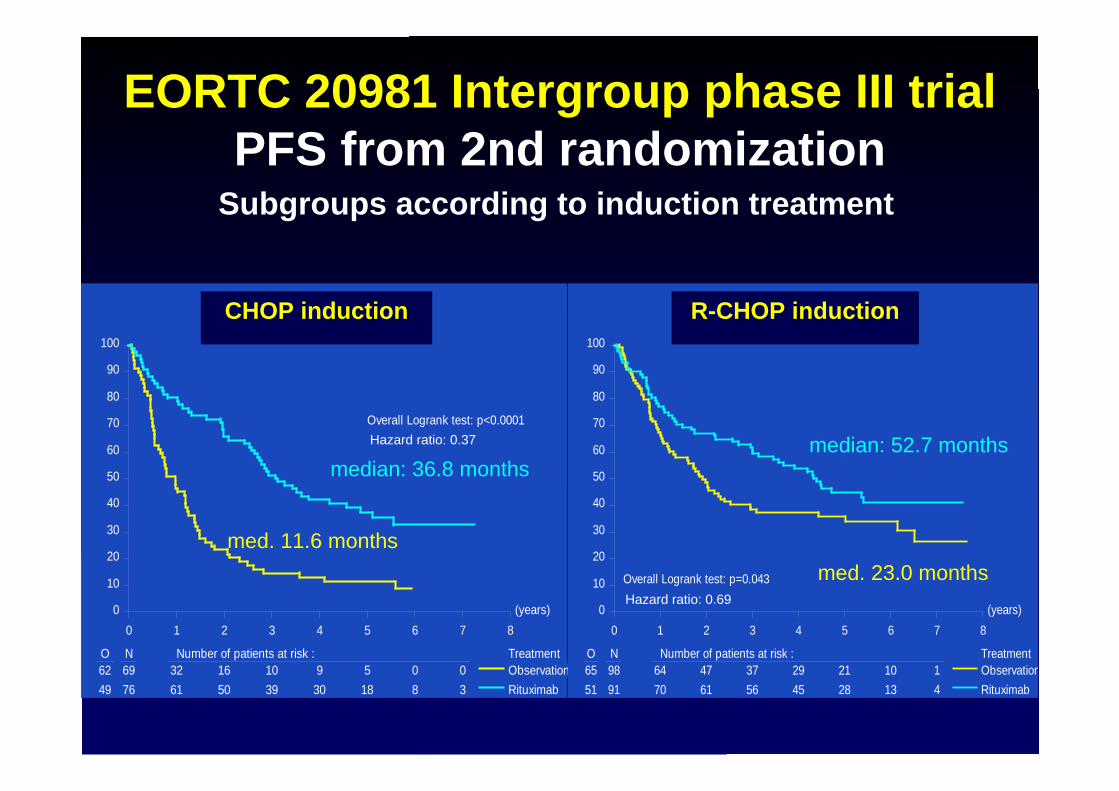
EORTC 20981 Intergroup phase III trialPFS from 2nd randomization
Subgroups according to induction treatment
(years)0 1 2 3 4 5 6 7 8
0
10
20
30
40
50
60
70
80
90
100
O N Number of patients at risk : Treatment62 69 32 16 10 9 5 0 049 76 61 50 39 30 18 8 3
ObservationRituximab
Progression free survivalAfter response to CHOP induction
Overall Logrank test: p<0.0001
(years)0 1 2 3 4 5 6 7 8
0
10
20
30
40
50
60
70
80
90
100
O N Number of patients at risk : Treatment65 98 64 47 37 29 21 10 151 91 70 61 56 45 28 13 4
ObservationRituximab
Progression free survivalAfter response to R-CHOP induction
Overall Logrank test: p=0.043
R-CHOP inductionCHOP induction
median: 36.8 monthsmedian: 52.7 months
med. 11.6 monthsmed. 23.0 months
Hazard ratio: 0.37
Hazard ratio: 0.69
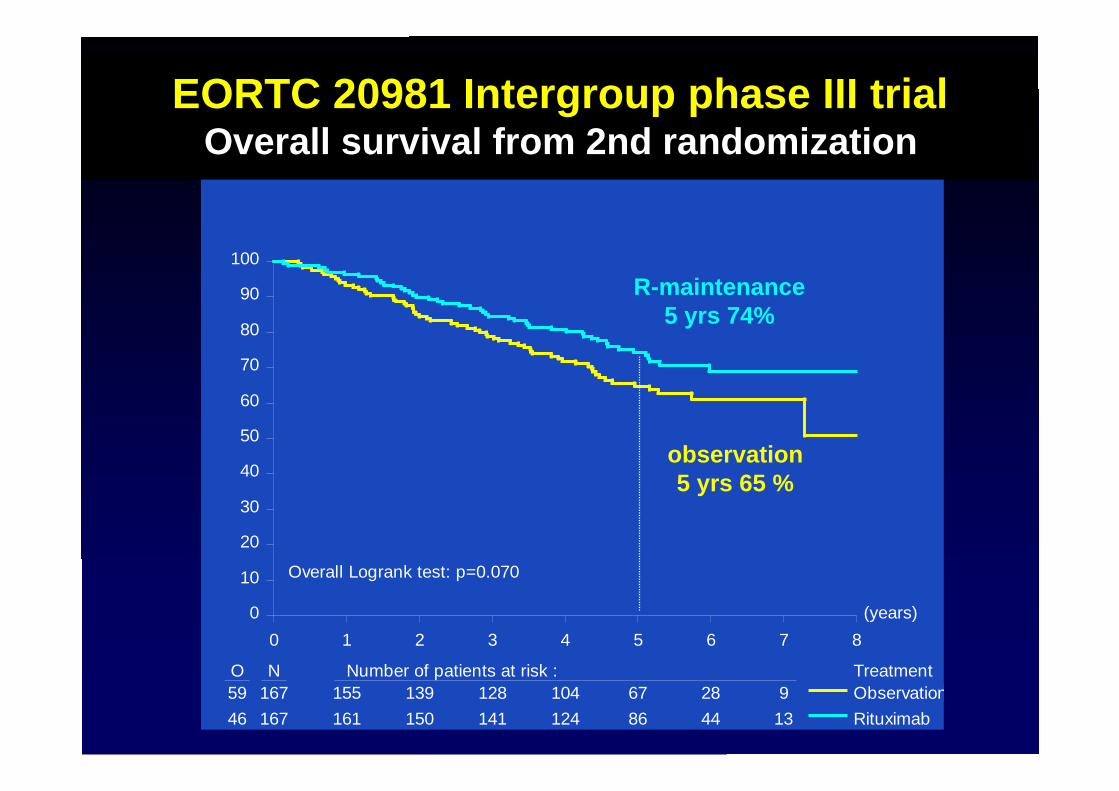
EORTC 20981 Intergroup phase III trialOverall survival from 2nd randomization
(years)0 1 2 3 4 5 6 7 8
0
10
20
30
40
50
60
70
80
90
100
O N Number of patients at risk : Treatment59 167 155 139 128 104 67 28 946 167 161 150 141 124 86 44 13
ObservationRituximab
Overall Logrank test: p=0.070
R-maintenance5 yrs 74%
observation5 yrs 65 %
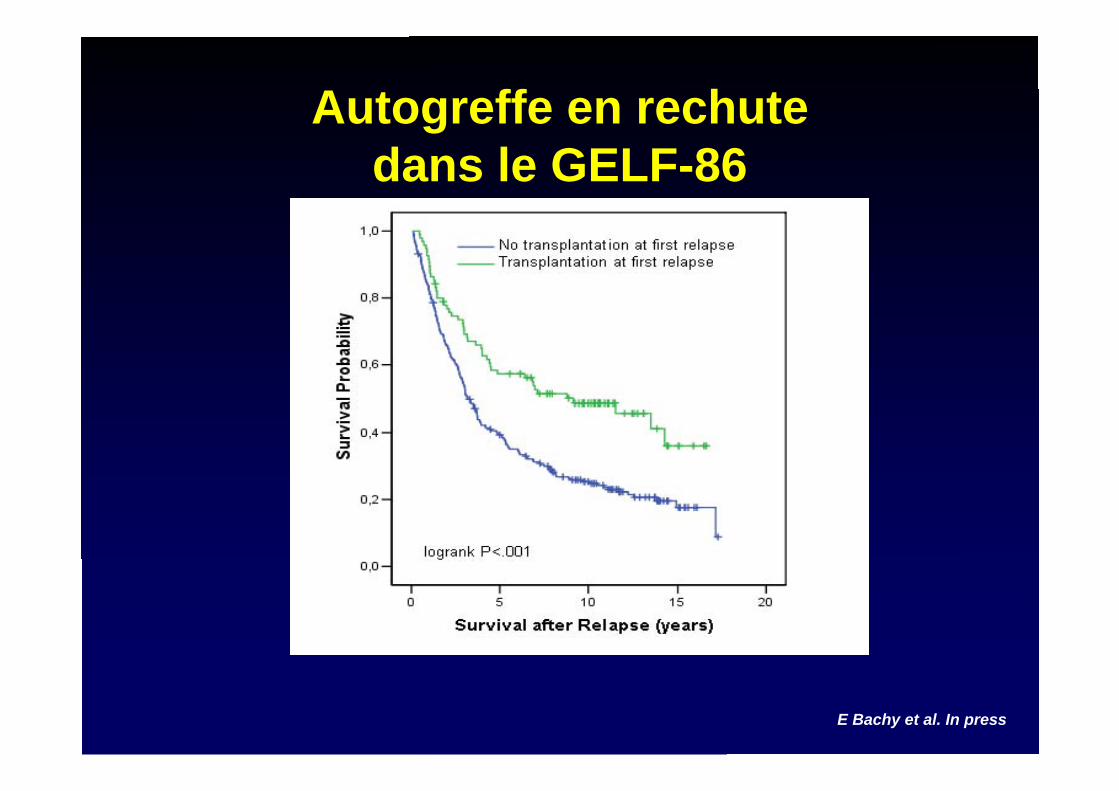
Autogreffe en rechutedans le GELF-86
E Bachy et al. In press
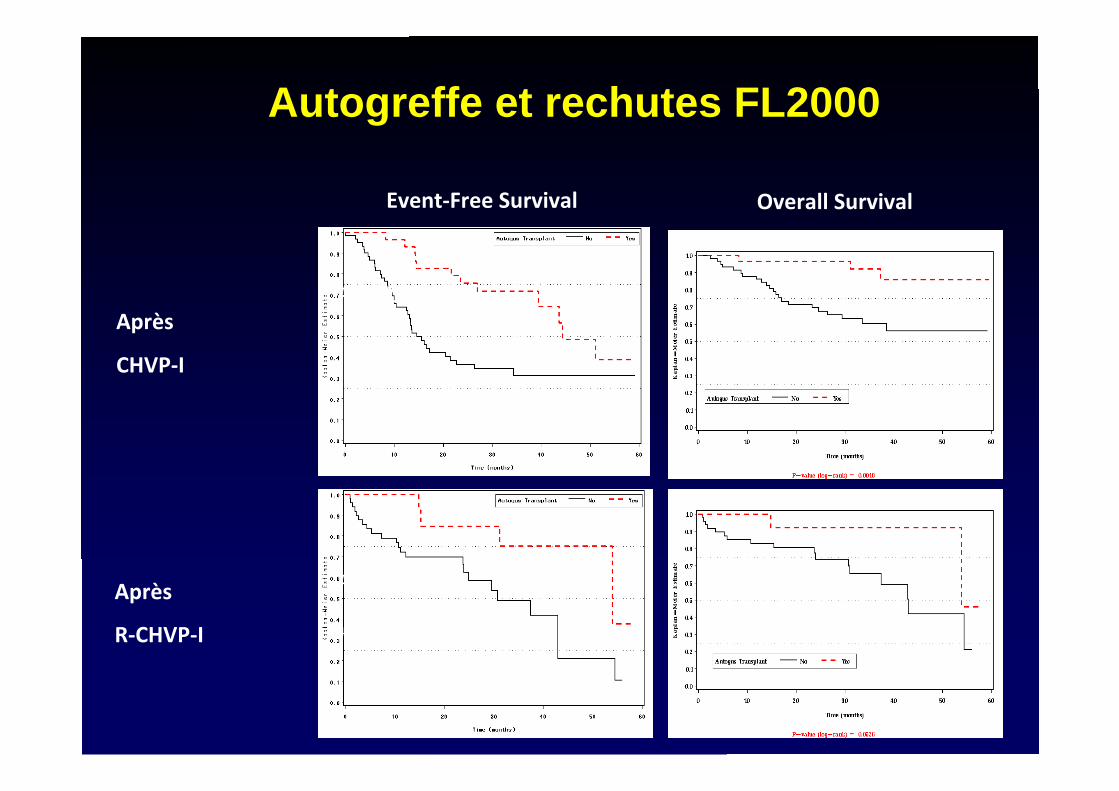
OverallSurvival
Après
CHVP‐I
Après
R‐CHVP‐I
Event‐FreeSurvival
P=.002
P=.05
48.5%[30%;65%]vs75%[41%;91%]
Autogreffe et rechutes FL2000
The Role of Autologous and AllogeneicTransplantation for Follicular Lymphoma
• I favor using autologous transplantation for patients with high-risk diseasewho have early relapse following conventional therapy– Low NRM (<5%)– Risk of MDS/AML with TBI regimens– May provide long term disease free survival– Conditioning regimens including immunotherapy (radioimmunotherapy or
Rituximab) promising• Nonmyeloablative allogeneic transplantation provides a potentially curative
therapy– NRM is significant (15-25%)– May provide salvage even following failed autologous transplant
D Maloney 4th Eur Cong Hematol Malignancies
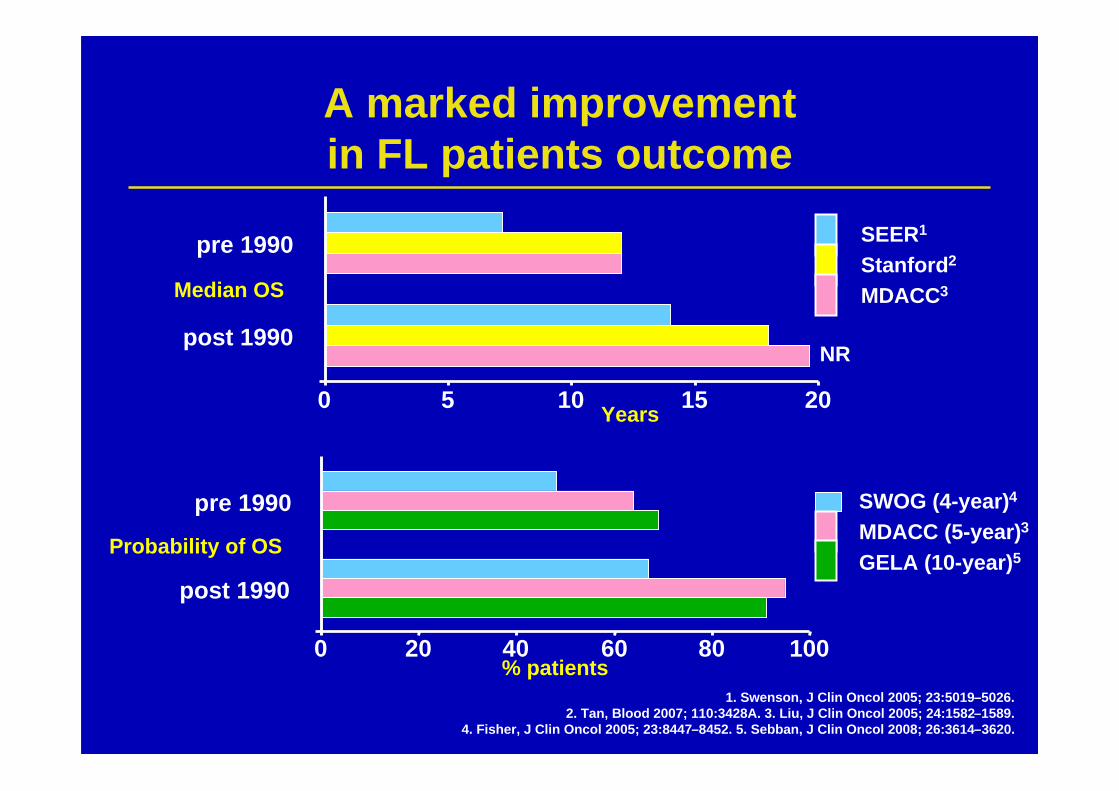
1. Swenson, J Clin Oncol 2005; 23:5019–5026.2. Tan, Blood 2007; 110:3428A. 3. Liu, J Clin Oncol 2005; 24:1582–1589.
4. Fisher, J Clin Oncol 2005; 23:8447–8452. 5. Sebban, J Clin Oncol 2008; 26:3614–3620.
Years
% patients
0 5 10 15 20
post 1990
pre 1990
Median OS
NR
SEER1
Stanford2
MDACC3
0 20 40 60 80 100
post 1990
pre 1990
Probability of OS
SWOG (4-year)4
MDACC (5-year)3
GELA (10-year)5
A marked improvementin FL patients outcome
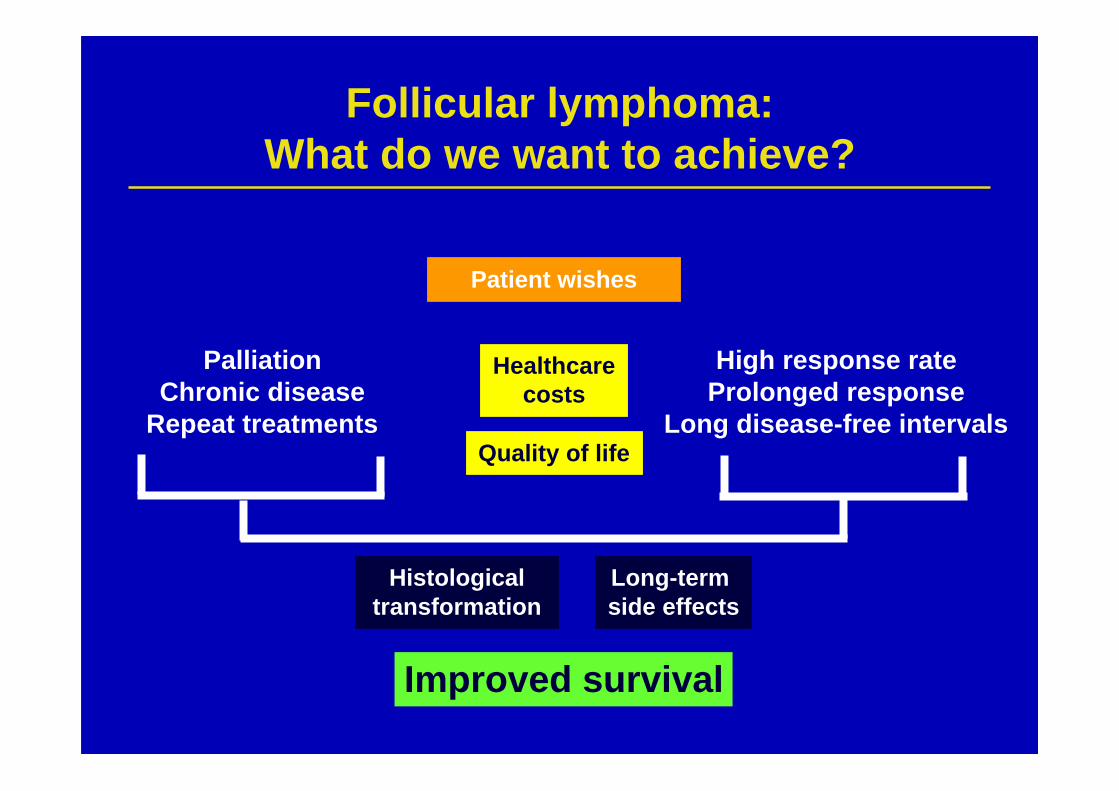
Follicular lymphoma:What do we want to achieve?
PalliationChronic disease
Repeat treatments
High response rateProlonged response
Long disease-free intervalsQuality of life
Long-term side effects
Histologicaltransformation
Healthcarecosts
Patient wishes
Improved survival
Les Ateliers Lymphomes et LLC
22 – 24 octobre 2009Le Moulin de la Forge – Le Vaumain (60)