Embed Size (px)
Citation preview

Nouveaux anticoagulants de la MTEV: encore du neuf
Dr Florence Parent Service de Pneumologie et Soins Intensifs Hôpital Bicêtre, AP-‐HP Inserm U999. Université Paris-‐Sud

DéclaraCon de liens d’intérêts
• Bayer (rivaroxaban) • Boehringer (dabigatran) • Pfizer (apixaban) • Daiichi-‐Sankyo (edoxaban) • Leo Pharma (Cnzaparine)

Rivaroxaban (Xarelto®): AMM pour le traitement de la
TVP et de l’EP non grave

Les études Einstein Randomized, open-label, event-driven, non inferiority study Non inferiority margin: 2.0 Predefined treatment period of 3, 6, or 12 months
15 mg bid
Confirmed DVT without symptomatic PE N=3449
Rivaroxaban
Day 1 Day 21
Enoxaparin bid for at least 5 days +
VKA INR 2.5 (INR range 2–3) Confirmed PE ± symptomatic DVT
20 mg od
N=4833
30-d
ay p
ost-s
tudy
trea
tmen
t per
iod
Rivaroxaban
R
The Einstein Investigators NEJM 2010;363:2499–2510 The Einstein-PE Investigators NEJM 2012;366:1287–97

Rivaroxaban (Xarelto®): Traitement de la TVP et de l’EP non grave
§ Inhibiteur spécifique direct du facteur Xa, par voie orale, sans surveillance biologique
§ Dose: 15 mg x 2 / jour, pendant 3 semaines, puis 20 mg / jour en 1 prise
§ Contre-‐indicaCon: insuffisance rénale sévère (Cl Creat < 15 mL/min)
§ Efficacité: non infériorité par rapport au traitement convenConnel (HBPM – AVK)
§ Saignements: § IdenCque pour l’ensemble des hémorragies § Moins d’hémorragies majeures

EINSTEIN PE: paCents Rivaroxaban (n=2419)
Enoxaparine/AVK (n=2413)
Hommes, % 54.1 51.7 Age, moyenne, ans 57.9 57.5 Indice masse corporelle, moyenne, kg/m2 28.3 28.4 Clairance crea=nine, % <30 ml/min 0.2 <0.1 30–49 ml/min 8.6 7.9 50–79 ml/min 26.3 24.6 ≥80 ml/min 64.3 67.0
Cancer ac=f, % ATCD MTEV, %
4.7 18.8
4.5 20.3
Durée de traitement prévue, % 3 mois 5.3 5.1 6 mois 57.3 57.5 12 mois 37.4 37.5
Extension anatomique de l’EP, % Limitée (1 lobe, obstrucCon ≤ 25%) Intermédiaire Extensive (mulC-‐lobaires, obstrucCon >25%)
12.8 57.5 24.7
12.4 59.0 23.9
ITT population

EINSTEIN PE: critère principal d’efficacité
ITT population
3.0
2.5
2.0
1.5
1.0
0.0
0.5
0 30 60 90 120 150 180 210 240 270 300 330 360
Number of pa=ents at risk
Rivaroxaban 2419 2350 2321 2303 2180 2167 2063 837 794 785 757 725 672
Enoxaparin/VKA 2413 2316 2295 2274 2155 2146 2050 835 787 772 746 722 675
Time to event (days)
Rivaroxaban N=2419
Enoxaparin/VKA N=2413
HR=1.12; p=0.0026 (non-inferiority)
Cum
ulat
ive
even
t rat
e (%
)

EINSTEIN PE: critère principal de tolérance: saignements majeurs + cliniquement significaCfs
Rivaroxaban n/N (%)
Enoxaparin/VKA n/N (%)
HR (95% CI) p-‐value
249/2412 (10.3) 274/2405 (11.4) 0.90 (0.76–1.07)
p=0.23
Safety population
0 30 60 90 120 150 180 210 240 270 300 330 360
15 14
10
13 12 11
9 8 7 6 5 4 3 2 1 0
Number of pa=ents at risk
Rivaroxaban 2412 2183 2133 2024 1953 1913 1211 696 671 632 600 588 313
Enoxaparin/VKA 2405 2184 2115 1990 1923 1887 1092 687 660 620 589 574 251
Time to event (days)
Rivaroxaban N=2412
Enoxaparin/VKA N=2405
Cum
ulat
ive
even
t rat
e (%
)

Safety population
3.0
2.5
2.0
1.5
1.0
0.0
0.5
0 30 60 90 120 150 180 210 240 270 300 330 360
Cum
ulat
ive
even
t rat
e (%
)
Time to event (days)
Rivaroxaban N=2412
Enoxaparin/VKA N=2405
Number of pa=ents at risk
Rivaroxaban 2412 2281 2248 2156 2091 2063 1317 761 735 700 669 659 350
Enoxaparin/VKA 2405 2270 2224 2116 2063 2036 1176 746 719 680 658 642 278
EINSTEIN PE: saignements majeurs Rivaroxaban n/N (%)
Enoxaparin/VKA n/N (%)
HR (95% CI) p-‐value
26/2412 (1.1)
52/2405 (2.2)
0.49 (0.31–0.79) p=0.0032

Evènement Rivaroxaban Enoxaparine/AVK HR
(95% CI) n/N % n/N %
Récidive ETEV
Fragile 21/791 2.7 30/782 3.8 0.68 (0.39–1.18)
Non-‐fragile 65/3359 1.9 65/3349 1.9 0.98 (0.70–1.38)
Saignement majeur
Fragile 10/788 1.3 35/779 4.5 0.27 (0.13–0.54)
Non-‐fragile 30/3342 0.9 37/3337 1.1 0.80 (0.49–1.29)
EINSTEIN DVT et PE: analyse poolée chez les paCents “fragiles*”
*Age >75 ans ou CrCl <50 ml/min ou poids ≤50 kg

Quels nouveaux anticoagulants oraux:
Dabigatran (Pradaxa®) Rivaroxaban (Xarelto®)
PTH / PTG Dose: 75 ou 110 mg x 2 AMM: 03/2008 Disponibilité: 12/2008 ASMR: V
Dose: 10mg x 1 AMM: 09/2008 Disponibilité: 05/2009 ASMR: V
FA non valvulaire Dose: 110 ou 150 mg x 2 AMM: 08-‐2011 Disponibilité: 08/2012 ASMR: V
Dose: 20 mg x 1 (ou 15 mg/j) AMM: 12/2011 Disponibilité : 09/2012 ASMR: V
MTEV -‐-‐-‐-‐-‐-‐-‐-‐
Dose: 15mg x 2/3sem, puis 20mgx1 AMM: 09-‐2012 ASMR: V
En cas d’insuffisance rénale
CI si clearance < 30 mL/min CI si clearance < 15 mL/min AdaptaBon entre 15 et 50 mL/min


0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Total (N=5649)
France (N=1318)
Germany (N=1400)
Italy (N=1348)
Spain (N=686)
UK (N=897)
Perc
enta
ge o
f pat
ient
s
acenocoumarol
fluindione
phenprocoumon
warfarin
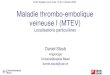
Figure 1: Types of Vitamin K antagonists
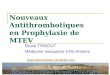
Figure 2: Sites of INR management
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Total (N=7243)
France (N=1532)
Germany (N=1771)
Italy (N=1888)
Spain (N=858)
UK (N=1194)
Perc
enta
ge o
f pat
ient
s
Hospital
Anticoagulation centre
Physician's office
Self-measurement
Other, e.g. biology lab
Figure 3: Time in therapeutic range
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Total (N=7243)
France (N=1532)
Germany (N=1771)
Italy (N=1888)
Spain (N=858)
UK (N=1194)
Perc
enta
ge o
f pat
ient
s
Adequate INR control
Suboptimal INR control
Unstable/high INRs according to physician’s judgement
INTRODUCTION/RATIONALE • The profile of atrial fibrillation (AF) patients in Western Europe is well known, but few comparative data
concerning management decisions in different parts of Europe are available. • Different country specific practices exist with regard to the use of other Vitamin K antagonists (VKA) than
warfarin. • Also the sites where INR measurements are performed, vary across Europe. • The PREFER in AF registry allows a comparison of the quality of INR control, using different types of
VKAs as well as different sites of INR management.
METHODS Design • The PREFER in AF is a multi-national, multi-centre, prospective observational disease registry with the
aim to gain detailed insight on the characteristics and management of AF patients with focus on prevention of thromboembolic events.
• The registry consists of one baseline visit and one follow-up visit after one year. • Patients (pts) were enrolled from January 2012 to January 2013 and baseline data were collected in
seven representative European countries: Austria, France, Germany, Italy, Spain, Switzerland, United Kingdom (UK).
• For regional comparisons, Austria, Switzerland, and Germany were combined into one pre-specified region.
Patients • Pts were included if they were at least 18 years of age, gave written informed consent for participation in
the registry, and had a history of AF documented by electrocardiography or by an implanted pacemaker or defibrillator within the preceding 12 months.
• No explicit exclusion criteria were defined to avoid biased selection of pts and achieve a cohort close to “real-life”.
Statistical analysis • Binary, categorical, and ordinal parameters were summarized by means of absolute and percentage
numbers within the various categories. • Numerical data were summarized by means of standard statistics.
Total France Germany Italy Spain UK (N=7243) (N=1532) (N=1771) (N=1888) (N=858) (N=1194)
Age [years] (mean) 71.5 72.9 71.9 70.9 70.5 70.7
Male (%) 60.1 59.3 63.0 57.0 56.0 64.5
Height [cm] (mean) 169.2 169.1 171.7 167.3 165.5 171.5
Weight [kg] (mean) 80.3 78.3 84.0 76.2 76.9 86.5
Body Mass Index [kg/m2] (mean) 27.9 27.3 28.4 27.2 28.1 29.3
Table 1: Demographic data
Total France Germany Italy Spain UK (N=7243) (N=1532) (N=1771) (N=1888) (N=858) (N=1194)
Hypertension (%) 72.0 63.8 81.9 75.3 72.7 62.1
Diabetes mellitus (%) 22.4 16.8 31.2 19.2 26.4 18.8
Obesity (%) 27.5 24.8 30.8 21.9 25.7 36.0
Coronary artery disease (%) 23.4 18.2 29.6 20.6 21.6 26.6
Prior stroke (%) 8.4 8.9 10.7 6.5 7.7 8.0
Heart failure (%) 21.3 18.2 28.4 19.4 24.4 15.4
CHA2DS2-VASc score (mean) 3.4 3.3 3.7 3.3 3.3 3.2
HAS-BLED score (mean) 2.0 1.9 2.1 2.1 2.0 2.0
Table 2: Risk factors
Total France Germany Italy Spain UK (N=7243) (N=1532) (N=1771) (N=1888) (N=858) (N=1194)
Pts with rhythm control * (%) 50.7 60.7 44.1 59.2 41.8 39.5
Pts with adequate heart rate control (HR 60-100), % 78.6 79.4 81.4 78.7 79.5 72.6
Pts with acceptable heart rate control (HR 50-59 or 101-110), % 14.3 14.9 12.2 13.8 15.5 16.5
Pts without adequate heart rate control (HR<50 or >110), % 7.1 5.7 6.4 7.5 5.1 11.0
Antiplatelet agents (AP), % 22.1 16.9 17.2 27.0 18.7 30.7
Vitamin K antagonists (VKA), % 78.0 86.0 79.1 71.4 80.0 75.1
Combination therapy (VKA + AP), % 9.9 10.1 7.7 8.8 10.3 14.7
Novel oral anticoagulants, % 6.1 6.0 11.6 0.3 11.2 3.7
No antithrombotic therapy, % 6.5 4.1 5.0 10.4 5.7 6.5
* Rhythm control defined as patients with cardioversion, ablation or antiarrhythmic drugs
Table 3: Rate vs rhythm control and anticoagulation
CONCLUSIONS • Despite a relative homogeneity of AF profiles, the anticoagulation management remains different
throughout these countries, mainly concerning the type of Vitamin K antagonists prescribed and the mode of INR surveillance.
• However this does not seem to affect the quality of anticoagulation, as estimated by three INRs at enrolment.
.
ACKNOWLEDGEMENTS • We would like to thank all centres who participated in this registry and all patients who gave their consent
to participate. • Furthermore, we would like to thank Markus Schwertfeger for medical advice and Paul-Egbert Reimitz for
statistical advice and programming (both employees of Daiichi Sankyo Europe).
ANTICOAGULATION MANAGEMENT IN ATRIAL FIBRILLATION: COUNTRY DIFFERENCES IN WESTERN EUROPE - DATA FROM THE PREFER IN AF REGISTRY
Jean-Yves Le Heuzey1, Bettina Ammentorp2, Harald Darius3, Raffaele De Caterina4, Richard John Schilling5, Josef Schmitt2, José Luis Zamorano6, Paulus Kirchhof7,8
1Cardiology and Arrhythmology, Georges Pompidou Hospital, René Descartes University, Paris, France; 2Daiichi Sankyo Europe, Munich, Germany; 3Vivantes Hospital Neukölln, Berlin, Germany; 4Institute of Cardiology G. d'Annunzio, University Chieti-Pescara, Italy; 5Barts and St Thomas Hospital, London, UK; 6Department of Cardiology, University Hospital Ramón y Cajal, Madrid, Spain; 7University of Birmingham Centre for Cardiovascular Sciences and SWBH NHS Trust, Birmingham, UK; 8Department of Cardiovascular Medicine, Hospital of the University of Münster, Germany
RESULTS Patient population • The PREFER in AF registry enrolled 7243 pts. The mean age was 71.5 years, varying from 70.5 (Spain)
to 72.9 years (France). (Table 1) • 72.0 % of pts had hypertension (from 62.1 % in UK to 81.9% in Germany), 22.4 % had diabetes (from
16.8 % in France to 31.2% in Germany). • Obesity (BMI > 30 mg/kg) was observed in 27.5 % (from 21.9 % in Italy to 36.0 % in UK), and 23.4 %
had coronary artery disease (from 18.2 % in France to 29.6 % in Germany). • A previous ischemic stroke was observed in 8.4 % (from 6.5 % in Italy to 10.7 % in Germany), heart
failure in 21.3 % (from 15.4 % in UK to 28.4% in Germany). • The mean CHA2DS2-VASc score was 3.4 (from 3.2 in UK to 3.7 in Germany) and the mean HAS-BLED
score was 2.0 (from 1.9 in France to 2.1 in Germany and Italy). (Table 2) Therapeutic management • A rhythm control strategy was chosen in 50.7% (from 39.5 % in UK to 60.7 % in France) whereas 78.6
% of patients were adequately rate-controlled (from 72.6 % in UK to 81.4 % in Germany). • Despite this overall homogeneity, the anticoagulation management showed important discrepancies: the
proportion of patients receiving Vitamin K antagonists was 86.0 % in France, 80.0 % in Spain, 79.1 % in Germany, 75.1 % in UK and 71.4% in Italy. (Table 3)
• The type of Vitamin K antagonists was very different: the most frequently prescribed VKA was warfarin in UK and Italy (74.9 % and 62.0 %, respectively); phenprocoumon in Germany (74.1 %), acenocoumarol in Spain (67.3 %) and fluindione in France (61.8 %). (Figure 1)
• The sites of INR measurements varied considerably: In France INR measurements were predominantly done at biology labs (93.1 %), whereas in Germany the majority of tests was conducted at the physician’s office (83.2 %).
• Anticoagulation centres were the most frequently used sites for INR measurements in Italy (44.2 %), Spain (32.8 %) and UK (29.1 %). (Figure 2)
• The time in therapeutic range, estimated from the last three INR values prior to enrolment, was comparable in these different countries.
• Patients with adequate INR control, defined as 2 or 3 INR values in range, was seen in 72.1 % of cases (from 63.8 % in Spain to 79.2 % in Germany), but was overestimated by the physicians in almost all countries: unstable/high INRs according to physician’s judgment were reported only in 18.3 % of patients (from 9.8 % in Germany to 29.8 % in Spain). (Figure 3)
LE HEUZEY J.Y. et al. ESC 2013"
Le syndicat des jeunes biologistes médicaux «Crent la sonneue d'alarme» en criCquant l'usage croissant de ces NACO car «l'absence d'anCdote dis-‐po-‐nible fait de ces molé-‐cules une bombe à retardement». Une mise en garde très inquiétante que rejeue en bloc l'Agence du médicament (ANSM). «Il n'y a aucun nouvel élément qui jusCfie une alerte ou qui remeurait en cause le niveau de risque de ces nouveaux médicaments» affirme le Dr Lozi Boudali, en charge de ce type de médicament à l'ANSM.

Dabigatran : Alerte Japonaise dans la FA (été 2011)
¢ Depuis l’autorisation au Japon en janvier 2011 dans la FA (Pradaxa 220 mg/j) : 6 décès par complication hémorragique ; 4 F et 2M, âgés (76 à 100 ans) ; petits poids : 4 patients < 45 kg.
¢ Dans un cas, le rôle du dabigatran est exclu car hémorragie digestive après relais par AVK.
¢ Délai < 3 semaines après l’introduction du Pradaxa® ¢ Facteurs de risque : 3 insuffisances rénales (dont deux Clairance créat < 30
ml/min = CI), 2 traitements concomitants par aspirine. ¢ Un cas d’hématome d’évolution défavorable en hémorragie digestive
malgré diminution de dose à 150 mg/j.

PRADAXA® et XARELTO ® Suivi naConal de pharmacovigilance
Commission de suivi du bénéfice/risque des produits de santé -‐ ANSM 26 novembre 2013 P. Lainé-‐Cessac, CRPV d'Angers A. Lillo-‐Le louët, CRPV HEGP

Historique du suivi naConal de Pharmacovigilance
*12/2008 : Pradaxa® Chir Ortho
*05/2009 : Xarelto® Chir Ortho
1er suivi de PV CNPV 07/2010
*08/2012 : Pradaxa® FA
*08-09/2012 : Xarelto® FA, TVP, EP
2ème suivi de PV CTPV 02/2013
3ème suivi de PV CTPV 11/2013
Tous les cas : • chir ortho
Tous les cas : • Indic Chir ortho • Indic. Med
Cas graves : • Indic Chir ortho • Indic. Med
*Date de mise à disposiCon en France

Méthodologie commune du suivi ¢ Échanges laboratoires /CRPV tous les mois ¢ Recherche doublons ¢ Critères d'exclusion ¢ Réévaluation de tous les cas français graves issus de la
notification spontanée, de la commercialisation au 31/08/2013
¢ Répartition des cas selon l’indication chirurgicale ou médicale. ¢ Définitions des hémorragies et des ETE majeurs similaires à
celle des essais cliniques. ¢ Analyse des PSURs ¢ Recherche bibliographique

PGR
¢ Risque identifié : hémorragies ¢ Risques potentiels :
l Atteinte hépatique l Anaphylaxie
¢ Risque théorique : l SCA
¢ Interactions médicamenteuses (IAM) ¢ Description de la population traitée ¢ Autres points :
l Surdosage (prise en charge) l mésusage l Abus l Utilisation en pédiatrie
¢ Risque identifié : hémorragies ¢ Risques potentiels :
l Atteinte hépatique l Atteinte pancréatique l Atteinte rénale
¢ Études de cohorte observationnelle l XAMOS l XANTUS l XALIA
¢ Études d'utilisation (UK, NL, DE) ¢ Informations manquantes
l Patients ClCr < 30 ml/mn l Grossesse et allaitement l Surdosage (prise en charge) l IAM
PRADAXA XARELTO

DDJ= doses définies journalières
Rapport ansm, novembre 2013 (données Celtipharm)

DDJ= doses définies journalières
Rapport ansm, novembre 2013 (données Celtipharm)

Evolution trimestrielle des ventes des NACO par rapport aux ventes totales des anticoagulants oraux (janvier 2008‐septembre 2013). Rapport ansm, novembre 2013 (données Celtipharm)
AVK ≈70%
NACO ≈30%

Résultats globaux
• 1624 cas retenus • 857 F, 755 H, 12 U • âge moyen 77 ± 10 ans • Indication conforme à AMM dans
97% des cas • Effets inattendus : 34% des cas • Décès 175 cas (11% des cas) :
– Âge: 80 ± 10 ans – Indication: FA dans 61% des
décès – Hémorragies: 116 = 66% des
décès – ETE : 12,5% des décès
• 1566 cas retenus • 814 F, 748 H, 4 U • âge moyen 72 ± 14 ans • Indication conforme à AMM dans
95% des cas • Effets inattendus : 32% des cas • Décès 127 cas (8% des cas) :
– Âge: 79 ans [43-94] – Indication: médicale dans 77%
des décès – Hémorragies: 82 = 65% des
décès (49 HIC, 16 HD) – ETE : 19% des décès
XARELTO PRADAXA

Les hémorragies (hors décès)
¢ 802 cas (55% des cas hors décès) ¢ F 52,4% ; âge moyen 79 ans ± 10 ans ¢ Indication FA : 62% ¢ 211 associées à une anémie (26% des
hémorragies) ¢ Localisation des hémorragies :
l Digestives : 48% l intracrâniennes : 9%
¢ Hémorragies majeures dans 52% des cas
¢ Médicaments associés susceptibles d'interaction dans 26% des cas
¢ Fonction rénale initiale et poids très peu renseignés
¢ 809 cas (57% des cas hors décès) ¢ F 50% ; âge moyen 72 ans ±14 ans ¢ Indication médicale : 71% ¢ 164 associées à une anémie (20% des
hémorragies) ¢ Localisation des hémorragies :
l Digestives : 29 % l intracrâniennes : 10%
¢ Hémorragies majeures dans 42% des cas
¢ Médicaments associés susceptibles d'interaction dans 23% des cas
¢ Fonction rénale initiale et poids très peu renseignés
PRADAXA XARELTO

Répartition des Effets indésirables (EI) retenus (hors décès)
53%
21%
1%
6%
4%
2% 4% 1% 2% 2% 4%
EI hémorragiquesETEEI CV autresEI hématologiquesEI cutanésdigestifsEI hépatobiliairesEI générauxEI neuroΨEI rénauxEI divers
51%
22%
2%6%
3% 3%5% 2% 2% 3% 1%
PRADAXA® : 1541 EI XARELTO® : 1555 EI

Les hémorragies (fatales ou non)
¢ 918 cas ¢ Localisation des hémorragies :
l Digestives : % l intracrâniennes : %
¢ Hémorragies majeures dans % des cas ¢ Fonction rénale initiale et poids très peu
renseignés
¢ 895 cas ¢ Localisation des hémorragies :
l Digestives : 24 % l intracrâniennes : 13%
¢ Hémorragies majeures dans 46% des cas (416 cas)
¢ Fonction rénale initiale et poids très peu renseignés
PRADAXA XARELTO

Les effets thrombo-emboliques
¢ 356 cas (27% des cas hors décès) ¢ F 56%; âge moyen 71 ans ¢ 187 ETE veineux (52% des cas
d'ETE) l 61 EP, 47 TVP, 74 TV l Indication chirurgie 77%
¢ 168 ETE artériels (47%) l 99 AVC ou AIT, 29 IDM, 9 thrombus
auriculaires, 14 thromboses autres l Indication FA : 77%
¢ ETE majeurs dans 79% des cas (168 artériels et 113 veineux)
¢ 321 cas (22% des cas hors décès) ¢ F 60% ; âge moyen 71 ±12 ans ¢ 254 ETE veineux (79% des cas
d'ETE) l 88 EP, 152 TVP, 14 TV l Indication chirurgie 80%
¢ 64 ETE artériels (20%) l 44 AVC ou AIT,7 IDM,1 thrombus
auriculaire, 12 thromboses autres l Indication médicale : 89%
¢ ETE majeurs dans 51% des cas (64 artériels et 101 veineux)
PRADAXA XARELTO

Autres effets d'intérêt
¢ Effets hépatiques : 78 cas (5,4% des cas hors décès) ; cytolyse biologique (51%) ; aucun cas très sévère
¢ Effets cutanés : 39 cas (2,7% des cas hors décès) l 12 réactions d’hypersensibilité dont
2 DRESS l Purpura, purpura vascula i re,
vascularite: 7 cas, dont 4 d’évolution favorable à l’arrêt de Pradaxa®
¢ Effets rénaux : 39 cas (2,7% des cas hors décès); 19 cas d’évolution favorable à l’arrêt de Pradaxa®
¢ Effets coronariens: 29 cas. Âge moyen: 76 ± 9 ans
¢ Effets hépatiques : 68 cas (4% des cas hors décès). Aucun cas très sévère
¢ Effets cutanés : 60 cas (4% des cas hors décès) dont 20 inattendus : l DRESS : 1 l Vascularite et purpura vasculaire :
9 cas ¢ Effets rénaux : 34 cas (2% des cas
hors décès) ¢ Effets pancréatiques : 0 ¢ Thrombopénies : 23 cas (1,5% des
cas hors décès)
PRADAXA XARELTO

Dabigatran and Postmarketing Reports of Bleeding. MR Southworth et al. N Engl J Med 2013, 368; 1272-4

Peut-on mieux appréhender le risque hémorragique en médecine courante?
¢ Comité technique de Pharmacovigilance (début d’uClisaCon a11-‐2013): l Dabigatran: 802 hémorragies non fatales / 116 hémorragies fatales l Rivaroxaban: 809 hémorragies non fatales / 82 hémorragies fatales l Mais….non rapporté au nombre de paCents traités

Evolution trimestrielle des ventes des NACO par rapport aux ventes totales des anticoagulants oraux (janvier 2008‐septembre 2013). Rapport ansm, novembre 2013 (données Celtipharm)
AVK ≈70%
NACO ≈30%

DDJ= doses définies journalières

Peut-on mieux appréhender le risque hémorragique en médecine courante?
¢ EvaluaCon par la CNAM des ventes, en 2013: l AVK ≈ 75% vs NACO ≈ 25% l 1M de patients traités par AVK, 300 000 par NACO
¢ Sous AVK: a 5000 DC par hémorragie par an (BMJ 2001, obtenus par extrapolaCon; pour
700 000 paCents sous AVK). a Actuellement 1M de paCents sous AVK a 7000 décès par hémorragie / an
¢ Sous NACO: Mortalité par hémorragie en 2013 a 5-‐10% de déclaraCon! 1er semestre 2013: 62 décès pour le dabigatran a ProjecCon de 250 DC déclarés en 2013, dont ≈ 60% par hémorragies ≈150 ,
sous NACO a Ce qui pourrait correspondre à 1500-‐3000 en réalité ?
Calcul très grossier, mais absence de signal pour une surmortalité par saignement sous ces anCcoagulants versus AVK

Conclusions ¢ Surveillance de l’ANSM continue avec des rapports semestriels ¢ Meilleure évaluation de l’incidence. ¢ Attention à la fonction rénale, à l’association à d’autres
médicaments et sur les modalités de switch. ¢ Surveiller plus particulièrement :
l Les effets cutanés l Les effets hépatiques l Les effets coronariens (Dabigatran) l Les réactions anaphylactoïdes (Rivaroxaban) ; les
atteintes rénales (Dabigatran) ¢ DECLARER +++ ¢ Attention aux registres qui se constituent et risque de
diminuer la notification spontanée.

Synthèse dans la MTEV Rec.VTE events Major bleeds
EINSTEIN-‐DVT (3,6,12m) RIVA 15mg bid 3w, 20 od 36/1731 (2.1%) 14 (0.8%) Enoxaparin-‐VKA 51/1718 (3.0%) 20 (1.2%)
EINSTEIN-‐PE (3,6,12m) RIVA 15mg bid 3w, 20 od 50/2419 (2.1%) 26 (1.1%)* Enoxaparin-‐VKA 44/2413 (1.8%) 52 (2.2%)
RE-‐COVER (6m) Heps 9d, then DABI 150mg bid 30/1274 (2.4%) 20 (1.6%) Heps 9d, then warfarin 27/1265 (2.1%) 24 (1.9%)

N Engl J Med 2013
• Etude randomisée en double aveugle • 5395 paCents
• Apixaban: 10 mg x 2 / j , 7 jours, puis 5mg x 2 / j, 6 mois • Enoxaparine, relais AVK



critère principal d’efficacité
HR=0.84 [0.6 – 1.18 ] (P<0.001

RR 0.31 [0.17 to 0.55]; P<0.001 for superiority
AMPLIFY: critère principal de tolérance: saignements majeurs


N Engl J Med 2013
• Etude randomisée en double aveugle • 4921 TVP et 3319 EP
• Traitement iniCal par héparine (au moins 5j) • Edoxaban: 60 mg x 1 / j (ou 30 mg/j si clear 30 à 50, ou poids<60) • Versus AVK


HR 0.89 [ 0.70 to 1.13] P<0.001 for non inferiority).

HR 0.81 [0.71 to 0.94] P = 0.004 for superiority
Hokusai: critère principal de tolérance: saignements majeurs + cliniquement significaCfs


Subgroup analysis in Hokusai-‐VTE
" Approximately 90% of PE paCents had a baseline NT-‐proBNP level measured
" In PE paCents with NT-‐proBNP levels ≥500 pg/mL recurrent VTE occurred in 15 of 454 paCents (3.3%) who received edoxaban and in 30 of 484 paCents (6.2%) given warfarin (HR 0.52 [0.28-‐0.98])
" Of the 1002 random sample of paCents measured by CT,
approximately 35% had RV dysfuncCon " Similar results were observed in paCents with RV dysfuncCon
on CT as in those with NT-‐proBNP levels ≥500 pg/mL (HR 0.42 [0.15-‐1.20])
The Hokusai-‐VTE InvesCgators. N Engl J Med 2013

Subgroup analysis in PE pa=ents with NT-‐proBNP ≥500 pg/mL
15/454 30/484
HR=0.52 (95% CI, 0.28-‐0.98)
3.3%
6.2%
The Hokusai-‐VTE InvesCgators. N Engl J Med 2013

Synthèse dans la MTEV Rec.VTE events Major bleeds
EINSTEIN-‐DVT (3,6,12m) RIVA 15mg bid 3w, 20 od 36/1731 (2.1%) 14 (0.8%) Enoxaparin-‐VKA 51/1718 (3.0%) 20 (1.2%)
EINSTEIN-‐PE (3,6,12m) RIVA 15mg bid 3w, 20 od 50/2419 (2.1%) 26 (1.1%)* Enoxaparin-‐VKA 44/2413 (1.8%) 52 (2.2%)
RE-‐COVER (6m) Heps 9d, then DABI 150mg bid 30/1274 (2.4%) 20 (1.6%) Heps 9d, then warfarin 27/1265 (2.1%) 24 (1.9%)
AMPLIFY (6m) API 10mg bid 7d, 5 bid 59/2609 (2.3%) 15 (0.6%)* Enoxaparin-‐warfarin 71/2635 (2.7%) 49 (1.8%)
HOKUSAI (3 to 12m OD) Edoxaban 60mg (30 Cl 30-‐50) 130/4118 (3.2%) 56 (1.4%) Heps ≥5d, warfarin 146/4122 (3.5%) 66 (1.6%)

Conclusions • Le Rivaroxaban est dès maintenant une alternaCve
thérapeuCque pour le traitement d’emblée des EP non graves
• SimplificaCon du traitement des EP. HospitalisaCon plus courte.
• EducaCon thérapeuCque à modifier mais à maintenir +++
• Absence de surveillance biologique spécifique, mais proposer une surveillance de la foncCon rénale, en parCculier chez les paCents âgés et/ou porteurs de plusieurs pathologies et/ou traitements associés.
• Résultats comparables avec les autres anCX et le dabigatran
• Mais schémas thérapeuCques différents

Rivaroxaban= Xarelto® • Contre-‐indicaCons :
– Femme enceinte et allaitement – I. hépaCque sévère avec troubles de coagulaCon – I. Rénale sévère
• Non indicaCons: – Cancer acCf
• Interférences médicamenteuses: – Inhibiteurs : Ketokonazole, ritonavir, clarithromicine augmentent de 50% l’effet
– Inducteurs : rifampicine, phenobarbital diminuent l’effet de 50%

Rivaroxaban: pas de surveillance biologique
• INR très variable selon la thromblasCne uClisée (standardisaCon pour les AVK)
• Tests de dosage spécifique en cours de validaCon, mais pas de seuil validé
• UCle dans des circonstances parCculières • PAS D’INDICATION EN ROUTINE CLINIQUE
Sujet âgé et traitement prolongé: foncCon rénale??

Saignement sous Rivaroxaban
• PPSB • AnCdote: en cours de développement • Einstein: le risque de décéder d’une hémorragie majeure est supérieur sous AVK que sous Rivaroxaban

Rivaroxaban (Xarelto®): AMM pour le traitement de l’EP non grave
§ Contre-‐indicaCon: insuffisance rénale sévère (Cl Creat < 15 mL/min)
§ Dans les études: paCents exclus si Cl Creat < 30 mL/min
§ Dans les études pour la FA: une dose de 15 mg au lieu de 20 mg a été évaluée
§ Dans l’AMM: « possibilité de diminuer à 15 mg/j si Cl Creat< 30 ml/min
§ En praCque: CI si Cl creat < 30 mL/min

Score de gravité clinique de l’EP: score PESI
Score PESI: classe I : <65 ; classe II : 66-‐85 ; classe III:86-‐105 ; classe IV:106-‐125; classe V: >125

Traitement de la MTEV: Parcours de soins
• La simplifica+on du traitement ne doit pas rendre moins exigeant pour le diagnos+c
• Relais avec le médecin traitant • Changement de dose après 3 semaines • EducaCon du paCent. Observance • EducaCon des personnels de santé • InteracCons médicamentauses:
– Inhibiteurs : Ketokonazole, ritonavir, clarithromicine augmentent de 50% l’effet
– Inducteurs : rifampicine, phenobarbital diminuent l’effet de 50%

Traitement prolongé dans la MTEV § RIVAROXABAN: Etude Einstein extension
à Après 6 à 12 mois de traitement pour 1er épisode de MTEV à Etude randomisée en double aveugle, pendant 6 à 12 mois à Dose: 20 mg en 1 prise par jour vs placebo
§ DABIGATRAN : Etudes RE-‐MEDY et RE-‐SONATE à Après au moins 3 mois de traitement pour 1 épisode de MTEV à 2 études randomisées en double aveugle
à 150 mg x 2 / j vs placebo (durée: 6 mois) à 150 mg x 2 / j vs AVK (durée prévue: 18 mois)
§ APIXABAN (anCXa): Etude Amplify extension à Après 6 à 12 mois de traitement pour 1 épisode de MTEV à Etude randomisée en double aveugle, pendant 12 mois à 3 bras: placebo vs 2,5 mg x 2 / j vs 5 mg x 2 / j

Les AVK en praCque quoCdienne


RE-‐COVER : Design
Confirmation
objective de l’ETEV
I R
Suivi 30 jours
Traitement initial parentéral au moins 5j
Simple aveugle
Double aveugle
72 h
6 mois Fin du traitement
Jusqu’à obtention de 2 INR ≥2.0 consécutifs
(8-11 days)
Warfarin warfarine (INR 2.0–3.0)
placebo de dabigatran etexilate
Placebo de warfarine
Dabigatran etexilate 150 mg x2 Warfarin placebo


RE-‐COVER : Design
Confirmation
objective de l’ETEV
I R
Suivi 30 jours
Traitement initial parentéral au moins 5j
Simple aveugle
Double aveugle
72 h
6 mois Fin du traitement
Jusqu’à obtention de 2 INR ≥2.0 consécutifs
(8-11 days)
Warfarin warfarine (INR 2.0–3.0)
placebo de dabigatran etexilate
Placebo de warfarine
Dabigatran etexilate 150 mg x2 Warfarin placebo

Les nouvelles molécules