-
7/30/2019 OSA part 3
1/10
Dr. Supreet Singh Nayyar, AFMC 2012
www.nayyarENT.com 1
SLEEP DISORDERED BREATHING (PART 3)
Treatment for more topics, visitwww.nayyarENT.com
Non-Surgical therapy for OSAHS
Address co-existent, predisposing conditions
Obesity Documented reduction in symptom after weight reduction
Degree of improvement has no linear correlation with weight Few may
not benefit if co-existent craniofacial abnormalities
Life style modification Avoid tobacco /smoking Dietary
modification
Sleep deprivation Avoiding agents affecting sleep Treat
hypothyroidism
Mechanical devices (positive airway pressure)
Body posture modification Sleeping with head and trunk elevated
to 30-60 degree angle to
horizontal reduces OSA
Lateral decubitus is also effective in reducing episodes (sleep
ball)Pharmacological therapy
Protriptyline
Non-sedating tricyclic antidepressant Increasing tone of airway
muscle Statistically significant improvement
Side effects : dry mouth, urinary hesitancy, constipation,
confusion, ataxia Dose: 30 mg/day
Agents with uncertain limited role
Serotonin agonists Affects dilators
http://www.nayyarent.com/http://www.nayyarent.com/http://www.nayyarent.com/http://www.nayyarent.com/
-
7/30/2019 OSA part 3
2/10
Dr. Supreet Singh Nayyar, AFMC 2012
www.nayyarENT.com 2
Busiprone Data insufficient
Stimulants Amphetamines
CVS complication Insufficient data
Continuous Positive Airway Pressure (CPAP)Indications
Mild OSA with EDS Moderate to severe OSA Co-morbidities
Many consider it to be mainstay of OSA treatment
Mechanism:
Acts as pneumatic splintEquipment:
Machine provides fixed pressure or vary pressure depending on
thepresence of apnoeas (Auto CPAP)
Mask is nasal or full face, kept in place by Velcro straps Port
of exhalation Newer machine small and light so portable Humidifier
also available as an optional mode
Compliance
By 3 years 25-40% stop using CPAP Treatment failure Cost
factor
o Regular service and maintenanceo Change of mask
Side effects
Claustrophobia Nasal stuffiness Skin abrasions, nasal bridge
abrasions Leaks are uncomfortable for eyes Air swallowing if
pressure more than esophageal sphincter pressure Pulmonary baro
trauma ( very rare) Treatment Failure
-
7/30/2019 OSA part 3
3/10
Dr. Supreet Singh Nayyar, AFMC 2012
www.nayyarENT.com 3
Surgical managementSURGICAL TREATMENT OPTIONS
Nasal Surgery
1. Nasal septoplasty
2. Inferior turbinectomy
3. Adenoidectomy
4. Nasal tumor or polyp excision
5. Nasal valve reconstruction
Palatal Surgery
1. Uvulopalatopharyngoplasty
2. Uvulopalatal flap
3. Tonsillectomy
4. Transpalatal advancement pharyngoplasty
5. Laser-assisted uvulopalatoplasty
6. Palatal radiofrequency
Hypopharyngeal Surgery
1. Maxillomandibular osteotomy and advancement
2. Mandibular osteotomy with genioglossus advancement
3. Hyoid myotomy and suspension
4. Tongue base radiofrequency
5. Partial glossectomy
6. Lingual tonsillectomy
7. Repose tongue suspension
for more topics, visitwww.nayyarENT.com
http://www.nayyarent.com/http://www.nayyarent.com/http://www.nayyarent.com/http://www.nayyarent.com/
-
7/30/2019 OSA part 3
4/10
Dr. Supreet Singh Nayyar, AFMC 2012
www.nayyarENT.com 4
Indications for surgery
Uvulopalatopharyngoplasty(UPPP)
First described by Ikematsu(1950), Fugita popularized in
1985
Principle:
Stiffen the soft palate by scarring Increase space behind soft
palate
Consists of
Tonsillectomy Reorientation of the anterior and posterior
tonsillar pillars Excision of the uvula and posterior rim of the
soft palate.
Complications:
Nasal regurgitation Swallowing & voice problems Severe post
op pain Hemorrhage Laryngospasm
-
7/30/2019 OSA part 3
5/10
Dr. Supreet Singh Nayyar, AFMC 2012
www.nayyarENT.com 5
Pulmonary edema, hypoxia Not satisfied post surgery
75-95% short term success
Long term
45%Modification:
Preserve uvula
Laser-assisted Uvulopalatoplasty(LAUP)
Described by Kamami in France in 1993
Principle
Stiffen the soft palate Prevent palatal flutter
Surgery
Local anesthesia on soft palate B/l vertical incision in soft
palate followed by partial vaporization of
-
7/30/2019 OSA part 3
6/10
Dr. Supreet Singh Nayyar, AFMC 2012
www.nayyarENT.com 6
uvula with CO2 Laser
Various modification doneComplications
Low Globus like symptom common Post operative pain
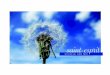
Uvulopalatoplasty
Reversible uvulopalatal flap
A, Preoperative palate anatomy B, Uvula is grasped with a
forceps and reflected back toward the soft-
hard palate junction; note the muscular crease.
C, The mucosa of the oral aspect of the uvula and soft palate in
adiamond shape is removed with cold knife dissection; the uvular
tip is
amputated and the uvular muscle thinned, if necessary
D, Trimmed and sutured flap, with the shaded area indicating
thelocation of the tissue before it is repositioned.
E, Postoperative appearance, with closure up on the soft
palateRadiofrequency tissue volume reduction/Thermal
ablation(RFTVR)
Principle
Similar to diathermy Lower temperature, lower current and
voltage
-
7/30/2019 OSA part 3
7/10
Dr. Supreet Singh Nayyar, AFMC 2012
www.nayyarENT.com 7
Insulated probe delivering radiofrequency energy at a frequency
of465 KHz
Thermal injury to specific submucosal sites in soft palate
causingfibrosis and contraction
Introduced into the base-of-tongue tissue under local
anesthesiaAdvantage
Day care, LA Less post operative pain Significant improvement
reported Good for multi level obstruction Low relapse rate
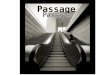
Mandibular osteotomy and genioglossal advancementIntraoral
approach
To enlarge the retrolingual area.
The genial tubercle, which is the anterior attachment of the
genioglossus
muscle, is mobilized by osteotomy
The segment is
advanced and
rotated to allow
bony overlap to
lock the inner
(lingual) surface
of the mandible
and the
geniotubercle at the outer (labial) surface
The fragment is fixed at the inferior aspect of the osteotomy
with a
titanium screw
-
7/30/2019 OSA part 3
8/10
Dr. Supreet Singh Nayyar, AFMC 2012
www.nayyarENT.com 8
Other ProceduresPalatal: Z-pharyngoplasty, palatal implants
Tongue base
RFTVR Laser midline glossectomy
to enlarge the retrolingual airway excision of approximately 2.5
5 cm of midline tongue tissue intraoral approach may also
require
lingual tonsillectomy reduction of the aryepiglottic folds
partial epiglottectomy
usually combined with a tracheotomy for airway protection Tongue
suspension suture Hypoglossal nerve stimulation
Lingualplasty.
Same procedure as the LMG (laser midline glossectomy) Except
that additional tongue tissue is extirpated posteriorly and
laterally to the portion removed by LMG
Epiglottis
epiglottectomyTemporary tracheostomy
Repose tongue suspension.Intraoral incision is made in the
frenulum
Titanium screw is placed at the lingual cortex of the
geniotubercle of the mandiblePermanent suture is passed through the
paramedian tongue musculature along the
length of the tongue, through the tongue base, and then back
through the length of the
tongue musculature
Then anchored to the screw, pulling the tongue base
anteriorlyHyoid myotomy and suspension
Addresses retrolingual area
Can alleviate obstruction caused by redundant lateral pharyngeal
tissue or aretrodisplaced epiglottis
Horizontal cervical incision over the hyoid bone is
preferred
Dissection is carried down to the suprahyoid musculature
-
7/30/2019 OSA part 3
9/10
Dr. Supreet Singh Nayyar, AFMC 2012
www.nayyarENT.com 9
Midline hyoid bone is isolated and then advanced over the
thyroid ala
Secured with two medial and two lateral permanent sutures
Maxillomandibular osteotomy and advancement
Improves retropalatal collapse by stabilizing the superior
pharyngeal muscles and
widening the nasopharyngeal inletAlso improves retrolingual
obstruction by placing the genioglossus muscle under
tension, thereby providing more room in the oral cavity for soft
tissues and also
stabilizing the lateral pharyngeal wall
Outer-table cranial bone graft may be necessary, along with arch
bar placement (ororthodontic banding) before the osteotomies
Usually performed if previous upper airway procedures have not
completely relieved
the sleep-related obstruction.
Clinical OutcomesOverall success rate for UPPP 40%
With multilevel surgical strategy have achieved60% when applying
strict response criteria
80% have been reported when applying commonly accepted measures
of
improvementHowever, the results may be reduced in morbidly obese
patients
-
7/30/2019 OSA part 3
10/10
Dr. Supreet Singh Nayyar, AFMC 2012
www.nayyarENT.com 10
Johnson and Chinnachieved a mean reduction of 44.1 points on the
RDI (from a
preoperative value of 58.7 to a mean postoperative value of
10.5) in patients
undergoing UPPP and genioglossal advancement without HMWhen
defining success as a RDI of less than 10, seven out of nine
patients (78%)
were successfully treatedTroell and colleagues[57]
reported that seven of 11 patients (63.6%) who underwent a
palatopharyngoplasty combined with genioglossus advancement and
HM were cured,
with cure defined as a postoperative RDI of less than 10, with
resolution of EDS
Oral AppliancesTwo basic types of appliancesMandibular
advancement devices
Popular
Positioning the lower jaw and tongue downward and forward The
airway passage is increased Comfortable More effective
Tongue repositioners
Pulling only the tongue forward and not the entire lower jaw.
Teeth, jaw muscles and joints are less affected Less studied
A period of consistent nightly wear is required
Patient motivation and cooperation essential
for more topics, visitwww.nayyarENT.com
http://www.nayyarent.com/http://www.nayyarent.com/http://www.nayyarent.com/http://www.nayyarent.com/