Embed Size (px)
Citation preview

ORIGINAL RESEARCH
Patterns of Diabetes Care Among People with Type1Diabetes During Ramadan: An InternationalProspective Study (DAR-MENA T1DM)
Fatheya F. Al Awadi . Akram Echtay . Monira Al Arouj .
Sobia Sabir Ali . Naim Shehadeh . Abdulrahman Al Shaikh .
Khier Djaballah . Cecile Dessapt-Baradez . Mohamad Omar Abu-Hijleh .
Abdullah Bennakhi . Mohamed El Hassan Gharbi . Khaled El Sayed El Hadidy .
Faris Abdul Kareem Khazaal . Mohamed M. Hassanein
Received: December 17, 2019 / Published online: March 6, 2020� The Author(s) 2020
ABSTRACT
Introduction: To describe the characteristics andcare of participants with type 1 diabetes duringRamadan in the Middle East and North Africa.Methods: The DAR-MENA (Diabetes andRamadan—Middle East and North Africa) studywas a prospective, observational study of adults
with type 1 and type 2 diabetes who were Mus-lim and did/did not intend to fast duringRamadan 2016. Baseline data were collected6 weeks prior to Ramadan, with a follow-up visit1–2 months after Ramadan. This is the analysisof the population with type 1 diabetes. Mea-surements included proportion who fasted,reasons for fasting and not fasting, changes indiabetes treatment, hypoglycemic events, andproportion with access to diabetes education.Results: Of 136 participants with type 1 diabetes,76.9% (100/130) fasted for at least 1 day, 72.3%(94/130) fasted for at least 15 days, and 48.5%(63/130) fasted for 30 days. The majority (63.0%,63/100) reported personal decision as a reason tofast. Fear of diabetic complications (58.6%, 17/29)and previous complications related to fasting
Enhanced Digital Features To view enhanced digitalfeatures for this article go to https://doi.org/10.6084/m9.figshare.11860932.
Electronic Supplementary Material The onlineversion of this article (https://doi.org/10.1007/s12325-020-01267-4) contains supplementary material, which isavailable to authorized users.
F. F. Al Awadi (&) � M. M. HassaneinDubai Hospital, Dubai, United Arab Emiratese-mail: [email protected]
A. EchtayRafic Hariri University Hospital, Beirut, Lebanon
M. Al Arouj � A. BennakhiDasman Diabetes Institute, Kuwait City, Kuwait
S. Sabir AliLady Reading Hospital, Peshawar, Pakistan
N. ShehadehRambam Medical Center, Haifa, Israel
A. Al ShaikhKing Abdulaziz University Hospital, Jeddah, SaudiArabia
K. DjaballahSanofi, Paris, France
C. Dessapt-BaradezSanofi, Guildford, UK
M. Omar Abu-HijlehJordan Hospital, Amman, Jordan
M. El Hassan GharbiIbn Sina Hospital, Rabat, Morocco
K. El Sayed El HadidyBeni Suef University, Beni Suef, Egypt
F. Abdul Kareem KhazaalAlkindy Obesity Center, Baghdad, Iraq
Adv Ther (2020) 37:1550–1563
https://doi.org/10.1007/s12325-020-01267-4

(48.3%, 14/29) were the most common reasonsfor not fasting. Adjustment of diabetic medica-tion regimen occurred for 84.6% (115/136) ofparticipants, and 72.8% (99/136) changed theirtreatment dose. The incidence and number ofadverse events for confirmed and severe hypo-glycemia were similar before and during Rama-dan. Almost half of participants had access todiabetes education (45.6%, 62/136).Conclusion: The DAR-MENA study showed thatdespite the risks associated with fasting for peoplewith type 1 diabetes, almost half fasted for the full30 days of Ramadan with no significant change inhypoglycemia events. Since the current Interna-tional Diabetes Federation and Diabetes andRamadan guidelines do not endorse fasting forpeople with type 1 diabetes, it is important thatthose who insist on fasting work closely with theirhealthcare practitioner to avoid any complications.
Keywords: Epidemiology; Fasting;Hypoglycemia; Ramadan; Type 1 diabetes
Key Summary Points
Why carry out this study?
Despite limited research on fasting duringRamadan in people with type 1 diabetes,and guideline recommendations againstfasting due to the potential of a high riskof complications, many people withtype 1 diabetes still fast during Ramadan.
This observational study was conducted inthe Middle Eastern and North African(MENA) region to provide an epidemiologicanalysis of the characteristics and patternsof care of people with type 1 diabetesduring Ramadan.
What was learned from the study?
The key finding of this study was thatdespite the risks associated with fasting forpeople with type 1 diabetes, almost halffasted for Ramadan (full 30 days) and theyexperienced a significant improvement inglycemic control following Ramadan,with no significant change inhypoglycemia events.
The results of this study provide newinsights into the characteristics andpattern of fasting and care for people withtype 1 diabetes before and duringRamadan, and may help to ensure thesafety of people with type 1 diabetes whochoose to fast during Ramadan.
In particular, the results indicate thatpeople with type 1 diabetes who insist onfasting need to work closely with theirhealthcare practitioner to ensure that theyreduce their risk of complications andhighlight the importance of Ramadan-focused education for patients.
INTRODUCTION
During the lunar-based month of Ramadan,Muslims fast from predawn to sunset. Thelength of the fast each day depends on thegeographic location and season, and may rangefrom a few hours to more than 20 h. Fastingduring Ramadan is compulsory for all healthyadult Muslims, although those with medicalconditions, including many with diabetes, areexempted from fasting according to the Qur’an[1]. During this holy month, there are alsochanges to daily activities and shorter sleepinghours.
For people with type 1 diabetes who fastduring Ramadan, insulin deficiency can lead toexcessive glycogen breakdown, increased glu-coneogenesis, and ketogenesis [2, 3]. Thisresults in a very high risk of complications,including hypoglycemia, hyperglycemia, dia-betic ketoacidosis, dehydration, and thrombosis[2–4]. Compared with type 2 diabetes, the riskof hypoglycemia is higher with type 1 diabetes[3, 5]. As a result of these risks, the InternationalDiabetes Federation and Diabetes and Ramadan(IDF-DAR) Practical Guidelines recommend thatpeople with type 1 diabetes, even if it is wellcontrolled, should not fast [3]; those with ahistory of recurrent hypoglycemia, hypo-glycemia unawareness, poor diabetes control,brittle diabetes, non-compliance with medical
Adv Ther (2020) 37:1550–1563 1551

treatment, or who are unwilling or unable tomonitor their blood glucose levels are consid-ered at very high risk of complications and mustnot fast [3]. Large-scale studies specific to fastingduring Ramadan for type 1 diabetes are limited.One previous study (EPIDIAR [Epidemiology ofDiabetes and Ramadan]) demonstrated thatabout 43% of people with type 1 diabetes fastedfor at least 15 days during Ramadan comparedwith 79% of individuals with type 2 diabetes [5].In the DAR-MENA (Diabetes and Ramadan—Middle East and North Africa) type 2 diabetesmellitus (T2DM) study, 86% of participantsfasted for at least 15 days [6].
Fasting during Ramadan has been associatedwith significant and variable changes in the atti-tudes and behaviors of people with type 1 dia-betes [7]. In one study of people with type 1diabetes, the timing of the main meal at sunset(Iftar) differed widely between individuals. Fur-thermore, a large number of people did not per-form regular self-monitoring of blood glucoseduring fasting, particularly those on multipledaily insulin injections. Studies have shown thatit is possible for people with type 1 diabetes toparticipate safely in prolonged fasts if they workwith their healthcare practitioner and receiveeducation to manage their condition effectively;however, these studies were performed with smallnumbers of participants [8, 9]. A pre-Ramadanmedical assessment is essential, and people withdiabetes should be educated on the risks associ-ated with fasting and techniques to decrease theserisks [3]. Modifications to insulin therapy and/ordosing regimen for the fasting period are neces-sary [3]. Human insulin therapy should be swit-ched to insulin analogues, if possible, and insulindose titration should be performed every 3 daysaccording to blood glucose levels [3].
DAR-MENA was an observational study,which was conducted in the Middle Eastern andNorth African (MENA) region to provide anepidemiologic analysis of the characteristicsand patterns of care of people with type 1 ortype 2 diabetes during Ramadan [6]. This paperreports the findings on daily fasting practicesduring Ramadan for people with type 1 diabetesby capturing data before and during the holymonth, including pattern of care (particularlymedications), changes of insulin regimen and
dosage, glycemic control, hypoglycemia risk,lifestyle changes, and patient education ondiabetes management.
METHODS
Study Design
The study methodology of DAR-MENA and theresults from the type 2 diabetes subpopulationhave been published [6]. Briefly, DAR-MENAwas an international, multicenter, prospective,observational study in the MENA region forRamadan 2016 (fasting period: dawn of June 6to evening of July 5) with a target enrollment of2000 participants with type 1 or type 2 diabetes.In the overall study, the inclusion criteriacomprised adult participants who were aged atleast 18 years with type 1 or type 2 diabetes, andwho were Muslim and did or did not intend tofast. Baseline data were collected in the 6 weeksprior to Ramadan, with a follow-up visit1–2 months after Ramadan. The results shownhere focus on the type 1 diabetes population.
The manuscript followed the STrengtheningthe Reporting of OBservational studies in Epi-demiology (STROBE) guidelines [10]. DAR-MENA was conducted in accordance with theethical principles laid down in the Declarationof Helsinki and complied with all internationalguidelines, as well as national laws and regula-tions of each country in which the registrystudy was performed. The study protocol wasapproved by the ethics committee of each par-ticipating center (please see Table S9 in thesupplementary material for ethics committeenames). Participants signed a consent form toparticipate in the study. Please note that thisstudy was not added to a clinical trial registry asit was a non-interventional, prospective, obser-vational study that did not meet the definitionfor clinical trial registration as specified by theWorld Health Organization.
Measurements
Variables measured or recorded were as follows:mean number of days fasted; number of
1552 Adv Ther (2020) 37:1550–1563

participants who fasted for at least 1 day, atleast 15 days, and 30 days; and reasons for fast-ing and not fasting, as well as diabetes treat-ment among participants who fasted, includingany modifications in antidiabetes medication ordoses of medication. Change in glycemic profile(glycated hemoglobin [HbA1c], fasting plasmaglucose [FPG], and postprandial plasma glucose[PPG]), lipid profiles (total cholesterol, triglyc-erides, high-density lipoprotein, and low-den-sity lipoprotein), and biometric measures(weight, systolic/diastolic blood pressure, waistcircumference, and heart rate) was determinedbetween the period before Ramadan and duringRamadan. Values up to 6 months before base-line were used to determine baseline data forthe glycemic and lipid profiles. Changes inlifestyle and access to education on diabetesmanagement were also recorded.
Incidence and number of adverse events(AEs) were recorded for symptomatic confirmedhypoglycemia, severe hypoglycemia, symp-tomatic confirmed hyperglycemia, and severehyperglycemia during the 1 month (4 weeksbefore visit 1) before Ramadan and during theRamadan fasting period. Symptomatic con-firmed hypoglycemia was defined as an eventwith clinical symptoms that are considered toresult from hypoglycemia and was confirmed bya self-measured plasma glucose (SMPG) level ofless than 70 mg/dL. Severe hypoglycemia wasdefined as a hypoglycemia event requiringassistance due to acute neurologic impairmentdirectly resulting from hypoglycemia. Severeepisodes of hypoglycemia were self-reported byparticipants, and participants were also asked bystudy investigators if they had experienced anyhypoglycemic episodes that required hospital-ization. Symptomatic confirmed hyperglycemiawas defined as an event with clinical symptomsthat are considered to result from hyper-glycemia and was confirmed by an SMPG levelof at least 200 mg/dL.
Statistical Analysis
For biochemical and biometric measures, thepaired t test was used to compare betweenmetric variables, the McNemar–Bowker test was
used to compare between physical activity data,and the McNemar test was used to comparebetween categorical variables before and afterRamadan. For comparisons of hypoglycemia/hyperglycemia data between the 4 weeks beforeRamadan and during Ramadan, the McNemartest was used for paired categorical comparisonand the paired t test was used for pairednumerical comparisons.
Descriptive quantitative variables werereported with mean and standard deviation(SD), and descriptive categorical data werereported by number and percentage of the studypopulation.
As not all data were available for all mea-surements, the total n values vary betweenmeasurements. Imputation of missing data wasnot performed.
RESULTS
Population Demographics and BaselineClinical Characteristics
Participant disposition data for the DAR-MENAstudy have been published [6]. In brief, a total of1894 participants with type 1 and type 2 dia-betes from the MENA region were enrolled inDAR-MENA, of whom 1885 were evaluable. Ofthese eligible participants, 136 had type 1 dia-betes and were included in this present analysis.
People with type 1 diabetes had a mean ageof 32.0 years, had a disease duration of14.0 years, and 55.1% were male (Table 1). Atbaseline, the mean HbA1c was 8.3%(67 mmol/mol). The number of comorbiditiesat baseline was low; the most common werehyperlipidemia, hypertension, and hypothy-roidism (n = 3 for each) (Table S1 in the sup-plementary material). All participants weretaking insulin. There were 87 (64.0%) partici-pants receiving rapid-acting insulin, 10 (7.4%)receiving intermediate-acting insulin, 67(49.3%) receiving basal insulin analogues, and56 (41.2%) receiving premix insulin (Table S2 inthe supplementary material).
Adv Ther (2020) 37:1550–1563 1553

Table 1 Baseline demographics, participant characteristics, lifestyle, and medical history in participants with type 1 diabetes(n = 136)
Characteristic Total n n or mean % or – SD
Men 136 75 55.1
Age [range] (years) 136 32.0 [18.4–66.4] ± 9.5
Weight (kg) 136 74.8 ± 14.3
Waist circumference (cm) 103 89.3 ± 16.3
Body mass index (kg/m2) 136 26.3 ± 4.5
Vital signs
SBP (mmHg) 135 122.1 ± 11.3
DBP (mmHg) 135 76.6 ± 8.5
Heart rate (beats/min) 130 79.1 ± 9.0
Lifestyle
Physical activity
Inactive 135 16 11.9
Low 135 38 28.1
Moderate 135 70 51.9
High 135 11 8.1
Smoking status (yes) 135 14 10.4
Daily working and sleeping hours
Working (h/day) 127 7.7 ± 3.0
Sleeping (h/day) 135 7.8 ± 1.2
Clinical characteristics
HbA1c (%) 134 8.3 ± 1.7
HbA1c (mmol/mol) 134 67 ± 18
FPG (mg/dL) 128 161.4 ± 58.9
PPG (mg/dL) 112 214.3 ± 66.1
LDL (mg/dL) 74 108.2 ± 28.0
HDL (mg/dL) 73 47.2 ± 12.4
Triglycerides (mg/dL) 91 135.2 ± 130.9
Total cholesterol (mg/dL) 90 172.3 ± 38.4
Serum creatinine (mg/dL) 98 1.1 ± 1.0
Medical and surgical history (yes) 136 24 17.6
Concomitant medications (yes) 136 52 ± 38.2
Duration of diabetes (years) 136 14.0 ± 7.7
1554 Adv Ther (2020) 37:1550–1563

Fasting Practice and Pattern of Care Beforeand During Ramadan
A total of 76.9% (n = 100/130 [participants withevaluable data]) of the type 1 diabetes popula-tion fasted during Ramadan for at least 1 day,72.3% fasted for at least 15 days, and 48.5%fasted for the full 30 days (Table S3 in the sup-plementary material). In these participants, themean ± SD duration of fasting was26.9 ± 5.9 days, with a mean ± SD daily fastingduration of 15.8 ± 0.9 h during Ramadan 2016(n = 100).
The majority (63.0%) of people with type 1diabetes listed ‘‘Personal decision’’ as a reason tofast (Table S4 in the supplementary material).‘‘To cope with family and community’’ wasgiven as a reason to fast for 24.0% of partici-pants. The most common reasons for not fast-ing were ‘‘Fear of diabetic complications’’(60.0%) and ‘‘Previous experience of acute dia-betic complication related to fasting’’ (50.0%)(Table S4 in the supplementary material).‘‘Other health-related issues (not related to dia-betes)’’ was a reason not to fast for 10.0% of
Table 1 continued
Characteristic Total n n or mean % or – SD
Family history of diabetes (yes) 135 92 68.1
Late diabetes complications (yes)a (most common listed) 136 46 33.8
Diabetic neuropathy 136 38 27.9
Diabetic retinopathy 136 12 8.8
Diabetic nephropathy 136 11 8.1
Diabetes management before Ramadan, n (%)
Physical activity only 136 0 0
OAD alone 136 0 0
OADsb 136 9 6.6
1 OAD 9 6 66.7
2 OADs 9 2 22.2
3 OADs 9 1 11.1
[3 OADs 9 0 0
Injectable therapy 136 136 100
Insulin 136 136 100
GLP-1 RA 136 0 0
Injectable alone 136 127 93.4
DBP diastolic blood pressure, FPG fasting plasma glucose, GLP-1 RA glucagon-like peptide 1 receptor agonist, HbA1cglycated hemoglobin, HDL high-density lipoprotein, LDL low-density lipoprotein, OAD oral antidiabetes drug, PPGpostprandial plasma glucose, SBP systolic blood pressure, SD standard deviationa Late diabetes complications included diabetic neuropathy, diabetic nephropathy, diabetic retinopathy, coronary arterydisease, myocardial infarction, peripheral vascular disease, stroke, microalbuminuria, and neuropathic arthropathyb Nine participants were taking OADs in combination with insulin at baseline; however, one of these patients reported thatthey planned to stop insulin during Ramadan (please see Table S2 in the supplementary material for more details onantidiabetes therapies used at baseline)
Adv Ther (2020) 37:1550–1563 1555

participants, and only 6.7% had been advisednot to fast by healthcare professionals.
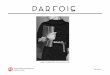
All participants were receiving insulin atbaseline; 84.6% of participants experienced achange in their diabetic treatment regimen, and72.1% experienced modifications in their insu-lin dose (Fig. 1). Of these participants, 80.6%(79/98) had one or more of their insulin dosesreduced. Of the 27.9% of participants who didnot change their insulin dose, the insulin regi-mens were as follows: rapid-acting insulin in60.5% (n = 23), intermediate-acting insulin in7.9% (n = 3), basal insulin analogues in 47.4%(n = 18), premix insulin in 44.7% (n = 17), and‘‘other’’ in 2.6% (n = 1; participant was using aninsulin pump; insulin type was not specified).
Biochemical and Biometric MeasuresBefore and During Ramadan
Compared with before Ramadan, there weresignificant changes in biochemical and bio-metric measures during Ramadan in some cases
(Table 2). Although change in waist circumfer-ence was significant, it was not consideredclinically meaningful and there was no signifi-cant change in weight. The number of workinghours per day decreased significantly by 1.2 h(P\0.0001), but the change in numbers ofhours of sleep was not significant.
The glycemic profile improved duringRamadan compared with before (Table 2). MeanHbA1c decreased by 0.6% (6.2 mmol/mol) to7.8% (62 mmol/mol) (P\ 0.0001), mean FPGdecreased by 21.2 mg/dL to 143.2 mg/dL(P\0.0001), and mean PPG decreased by22.8 mg/dL to 191.9 mg/dL (P\ 0.0001). Meanlipid profile values did not change significantlyduring Ramadan, except for total cholesterol,which was increased by 6.3 mg/dL (P = 0.021).
Hypoglycemia and Hyperglycemia Beforeand During Fasting
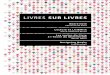
The incidence of confirmed hypoglycemia andnumber of confirmed hypoglycemia AEs did notchange significantly from the 4 weeks beforeRamadan (n = 136; 27.2%, 0.93 events/month/participant) to during Ramadan (n = 130;23.1%, 0.79 events/month/participant) (Fig. 2).During Ramadan, the incidence of severehypoglycemia and number of AEs were low(Fig. 2). There was no significant change in theincidence or number of AEs for severe hypo-glycemia, confirmed hyperglycemia, and severehyperglycemia during Ramadan compared withbefore (Fig. 2; Table S5 in the supplementarymaterial).
Lifestyle Changes and Patient Educationon Diabetes Management
Most people (95.4%) reported lifestyle changesduring Ramadan fasting (Table S6 in the sup-plementary material). Participants reportedchanges for working hours (67.5%), sleep dura-tion (67.2%), physical activity (45.0%), andsmoking (7.8%). Of those reporting a change,working hours decreased in 84.3%, sleep dura-tion decreased in 54.5%, and physical activitydecreased in 60.3%; smoking decreased in all 10participants who reported on this lifestyle
aD
iabe
tes
trea
tmen
ts
Participants with a treatment change (%)
Insulin 84.6% 115/136
84.6% 115/136
OAD 66.7% 6/9
All
0 50 100
b
Dia
bete
s tr
eatm
ents
Participants with a dose change (%)
Insulin 72.1% 98/136
72.8% 99/136
OAD 22.2% 2/9
All
0 50 100
Fig. 1 Modifications in diabetes treatment in participantswith type 1 diabetes (n = 136) for a change in treatmenta
and b change in dose. aChange in treatment is defined asparticipants who had a change in drug and/or dose. OADoral antidiabetes drug
1556 Adv Ther (2020) 37:1550–1563

Table 2 Comparison between before and after Ramadan for biochemical and biometric measures in participants withtype 1 diabetes (n = 136)
Characteristic Before Ramadan After Ramadan Change P value
Totaln
Count/mean
%/
– SD
Totaln
Count/mean
%/
– SD
Weight (kg) 136 74.8 ± 14.3 130 75.0 ± 14.4 0.4 ± 3.8 0.255a
Waist circumference
(cm)
103 89.3 ± 16.3 100 88.7 ± 15.8 -1.4 ± 6.0 0.03a
SBP (mmHg) 135 122.1 ± 11.3 130 121.5 ± 11.9 -0.5 ± 8.7 0.485a
DBP (mmHg) 135 76.6 ± 8.5 130 76.8 ± 8.3 0.08 ± 6.3 0.888a
Heart rate (beats/min) 130 79.1 ± 9.0 126 78.6 ± 6.9 -0.6 ± 7.6 0.360a
Working (h/day) 127 7.7 ± 3.0 124 6.4 ± 2.8 -1.2 ± 1.9 \ 0.0001a
Sleeping (h/day) 135 7.8 ± 1.2 129 7.9 ± 2.0 0.1 ± 1.8 0.574a
Physical activity
Inactive 135 16 11.9 130 17 13.1 0.406b
Low 135 38 28.1 130 45 34.6
Moderate 135 70 51.9 130 58 44.6
High 135 11 8.1 130 10 7.7
Smoker
Yes 135 14 10.4 136 13 9.6 1c
No 135 121 89.6 136 123 90.4
HbA1c (%) 134 8.3 ± 1.7 115 7.8 ± 1.2 -0.6 ± 1.0 \ 0.0001a
HbA1c (mmol/mol) 134 67 ± 18 115 62 ± 14 -6.2 ± 11.1 \ 0.0001a
FPG (mg/dL) 128 161.4 ± 58.9 121 143.2 ± 43.4 -21.2 ± 42.2 \ 0.0001a
PPG (mg/dL) 112 214.3 ± 66.1 106 191.9 ± 53.8 -22.8 ± 58.3 \ 0.0001a
LDL (mg/dL) 74 108.2 ± 28.0 58 116.6 ± 33.7 4.3 ± 20.2 0.152a
HDL (mg/dL) 73 47.2 ± 12.4 58 48.7 ± 15.0 0.4 ± 9.9 0.777a
Triglycerides (mg/dL) 91 135.2 ± 130.9 73 128.1 ± 46.7 -2.2 ± 31.9 0.590a
Total cholesterol (mg/
dL)
90 172.3 ± 38.4 72 181.6 ± 39.2 6.3 ± 20.6 0.021a
DBP diastolic blood pressure, FPG fasting plasma glucose, HbA1c glycated hemoglobin, HDL high-density lipoprotein,LDL low-density lipoprotein, PPG postprandial glucose, SBP systolic blood pressure, SD standard deviationa Paired t test used to compare between metric variables before and after Ramadanb McNemar–Bowker test used to compare between physical activity data before and after Ramadanc McNemar test used to compare between categorical variables before and after Ramadan
Adv Ther (2020) 37:1550–1563 1557

change. Overall food intake during Ramadanwas altered in 62.3% of participants; in thosereporting changes, 51.7% of participants repor-ted a decrease in consumption of carbohydrates,50.8% decreased their sugar intake, 92.6%
increased the amount of protein that theyconsumed, 91.8% increased their vegetable in-take, and 60.5% decreased their consumption offats. Of the 63.1% reporting changes in fluidintake, most reported an increase (80.5%).
a
0
40
35
30
25
20
15
10
5Inci
denc
e of
con
firm
ed h
ypog
lyce
mia
(%
)
P = 0.557a
27.2%37/136
23.1%30/130c
b
Con
firm
ed h
ypog
lyce
mia
AE
s(n
umbe
r of
eve
nts/
mon
th/p
artic
ipan
t)
P = 0.391b
c
Inci
denc
e of
sev
ere
hypo
glyc
emia
(%
)
P = 1a
d
0.0
4.0
3.0
2.0
1.0
2.9%4/136
0.93127/136
2.3%3/130c
0.79103/130c
0.0
1.5
1.0
0.5
0.00
0.05
0.15
0.10
Sev
ere
hypo
glyc
emia
AE
s(n
umbe
r of
eve
nts/
mon
th/p
artic
ipan
t)P = 0.794b
0.0517/136
0.0699/130c
4 weeks before Ramadan During Ramadan
Fig. 2 a Incidence of confirmed hypoglycemia, b con-firmed hypoglycemia AEs, c incidence of severe hypo-glycemia, and d confirmed severe hypoglycemia AEs beforeand during Ramadan in participants with type 1 diabetes
(n = 136). aMcNemar test was used for paired categoricalcomparisons. bPaired t test was used for paired numericalcomparisons. cSix participants with type 1 diabetes weremissing hypoglycemia data. AE adverse event
1558 Adv Ther (2020) 37:1550–1563

Nearly half of participants with type 1 dia-betes had access to diabetes education (45.6%)(Table S7 in the supplementary material). Ofthose receiving education, it was accessiblethrough face-to-face diabetes education sessions(45.2%), diabetes education programs (25.8%),diabetes self-education (27.4%), and website-based diabetes education (21.0%).
DISCUSSION
DAR-MENA is the first prospective, large studyinvestigating diabetes before and during Rama-dan. The type 1 diabetes DAR-MENA analysisprovides in-depth information on the charac-teristics and pattern of care of relatively youngand healthy people with type 1 diabetes beforeand during Ramadan fasting. Importantly, itprovides the reasons (outlined below) thatprompted people to choose whether to fastduring Ramadan. The study found that themajority of people (72.3%) fasted for at least15 days, and nearly half (48.5%) fasted for thefull 30 days of Ramadan without a significantincrease in confirmed and severe hypoglycemiaevents.
The DAR-MENA type 1 diabetes populationwas young, with a mean age of 32 years and alow number of comorbidities at baseline. Themean duration of type 1 diabetes was 14 yearsand glycemic control was relatively poor with amean HbA1c of 8.3% (67 mmol/mol). Asexpected, all participants were taking insulin;49.3% were receiving basal insulin analogues.
The role of structured education for patientsis well established in the management of dia-betes, and guidelines state that this should beextended to Ramadan-focused diabetes educa-tion so that people can make informed deci-sions [3, 4]. In this study, only 45.6% ofparticipants had access to diabetes education, ofwhom 45.2% received face-to-face educationalsessions. Considering that Ramadan-focusededucation can enable individuals to reduce theirrisk of acute complications during fasts [3], thepresent study showed that this is an essentialtool in patient management that is not yetbeing accessed by all patients. Healthcare pro-fessionals also seem to need more education on
managing diabetes during Ramadan. One studyin Pakistan found that almost one-third ofgeneral practitioners lacked knowledge of basicprinciples needed [11].
Of the 100 participants with type 1 diabeteswho chose to fast, 63.0% reported that theirreason was due to a personal decision, whereas24.0% fasted to cope with pressure from theirfamily and community. Of those people whodid not fast, 60.0% reported a fear of diabeticcomplications as a reason for not fasting, and50.0% had had previous experience of acutediabetic complications during fasting. Only6.7% did not fast on the advice of theirhealthcare professional. Working conditionsprompted 3.3% of participants to not fast dur-ing Ramadan.
The mean duration of fasting was 27 dayswith a daily duration of 16 h; during this time,most people reported lifestyle changes. Themajority of participants reported changes inworking hours (67.5%) and sleep duration(67.2%), whereas changes in physical activity(45.0%) and smoking (7.8%) were less common.For those with changes in working hours, most(84.3%) reported a decrease; however, changeswere more balanced for those who reported achange in sleep duration, with 54.5% reportinga decrease and 45.5% reporting an increase.Food intake was also altered during Ramadanfor 62.3% of participants. In those reportingchanges, the proportions with increases anddecreases were approximately equal for carbo-hydrates and sugars, whereas the majority ofparticipants reported increases in protein(92.6%) and vegetables (91.8%) and decreases infats (60.5%). Of the 63.1% reporting changes influid intake, most (80.5%) reported an increase.This change in food and fluid intake wasaccompanied by a change in insulin regimen in84.6% of participants, and 72.1% modified theirinsulin dose.
It was anticipated that a greater proportionof participants (close to 100%) would make achange to their insulin dose, but this was notobserved in this study. In practice, 27.9% ofparticipants did not change their insulin dose(regardless of type: rapid, short, intermediate,basal, or premix). Of these, 60.5% were onrapid-acting insulin. A high proportion of
Adv Ther (2020) 37:1550–1563 1559

participants did not modify their insulin dose,which may have been due to inadequate gly-cemic control before Ramadan.
During Ramadan, not only do participantsabstain from eating and drinking during day-light hours but they also drastically changeaspects of their lifestyle and habits, which canaffect glycemic control. In this study, there wasa significant improvement in mean glycemicprofile (based on HbA1c and FPG) after Rama-dan fasting compared with before Ramadan.This occurred with no significant change in theincidence of confirmed hypoglycemia or num-ber of confirmed hypoglycemic events duringRamadan compared with the previous 4 weeks.The lack of a significant increase in hypo-glycemia in people with type 1 diabetes duringRamadan is clinically important as previousstudies suggest an increase during Ramadan [5],and diabetes guidelines highlight the increasedrisk of hypoglycemia with fasting [3, 4].
In DAR-MENA participants with type 1 dia-betes, lipid levels remained constant through-out Ramadan, except for total cholesterol,which was significantly increased (P = 0.021).In addition, there was no significant weightgain. While those who did not fast said thatthey were fearful of developing diabetic com-plications related to fasting, this did not appearto have happened in this study. Indeed, theincidence and number of AEs for severe hypo-glycemia, confirmed hyperglycemia, and severehyperglycemia did not change significantlyduring Ramadan compared with before. This issupported by a recent survey of 526 people withdiabetes in Tunisia, of whom 51 had type 1diabetes, who had fasted during Ramadan,which found that more than half of people hadbeen treated with insulin and most were able tofast without interruption [12]. A recent litera-ture review also found that Ramadan fasting inpeople with diabetes using insulin is feasible,with negligible major complications reported[13]. In DAR-MENA, diabetes education and thediabetic medication/dosing adjustments (pri-marily dose reductions) may have contributedto the low rates of hypoglycemia observed.
The results of the DAR-MENA type 1 diabetesanalysis provide new up-to-date information onfasting during Ramadan, in comparison with
previous studies, such as the EPIDIAR study,which had used the older insulins [5]. In EPI-DIAR, fasting lasted for at least 15 days duringRamadan in 43% of people, and the meannumber of fasting days was 23 days, which isshorter than the 27 days reported in this study[5]. A higher proportion of people with type 1diabetes in the EPIDIAR study (68%) receivedrecommendations from their healthcare provi-ders about fasting and diabetes during Ramadanthan those who received education in DAR-MENA type 1 diabetes [5]. However, 57% ofparticipants had the same food intake as before,and 65% maintained their insulin dose duringRamadan [5]. The incidences of severe hypo-glycemic episodes in participants with type 1diabetes prior to Ramadan were similar in theDAR-MENA and EPIDIAR studies (0.05 vs0.03 events/month/participant, respectively).
In EPIDIAR, the significant increase(P = 0.0174) in the mean ± SD number of sev-ere hypoglycemic episodes per month per per-son during Ramadan (0.14 ± 0.6 events/month) compared with the preceding year(0.03 ± 0.1 events/month) in the overall type 1diabetes population may reflect the lack of dosechange [5]. It should be noted that this signifi-cant increase roughly equates to only one moresevere hypoglycemic event for each 5 months offasting (?0.02 events/month/participant). Fur-thermore, the EPIDIAR study did not find astatistically significant increase in the mean ±
SD number of severe hypoglycemic episodes permonth per person during Ramadan(0.12 ± 0.48 events/month) compared with thepreceding year (0.02 ± 0.05 events/month) inpatients who fasted for at least 15 days [5].
New technologies for continuous glucosemonitoring, such as glucose sensors and flashglucometers, can make fasting safer for peoplewith type 1 diabetes who fast during Ramadan.Several studies have already shown the poten-tial benefits of using an insulin pump duringRamadan [14]. In one study, those using aninsulin pump performed self-monitoring ofblood glucose more frequently than those onmultiple daily insulin injections [7]. Unfortu-nately, the current high cost of an insulin pumprestricts its use.
1560 Adv Ther (2020) 37:1550–1563

Our analysis has some limitations. Firstly,the DAR-MENA study enrolled people with bothtype 1 and 2 diabetes, and did not require aspecific number of each diabetes type. There is,therefore, a much lower number of participantswith type 1 than type 2 diabetes. This is notunexpected as the proportion of the adultpopulation with type 2 diabetes is higher thanthat with type 1 diabetes, but it does mean thatthis analysis is based on a small number ofparticipants. Secondly, only those who believethat they are fit enough actually fast, and only aproportion of those are able to fast for the wholeof the holy month. The results are, therefore,not representative of the entire type 1 diabetespopulation. While the analysis suggests thatfasting during Ramadan is safe, this cannot beextrapolated to the whole of the type 1 diabetespopulation. Lastly, it is important to note thathypoglycemia, particularly symptomatic con-firmed hypoglycemia, which was based onpatient self-assessment, could potentially beunder-reported as a result of impaired awarenessof hypoglycemia or reluctance to measureSMPG levels. It is possible that participantsperceived symptoms of hypoglycemia but didnot assess SMPG levels; rather, they may havesimply stopped activities and waited for symp-toms to subside, as they may not have wantedto interrupt their fasting. Therefore, it was dif-ficult to capture all hypoglycemic episodes andtheir severity. Ideally, the results of the currentstudy would be validated in a future study basedon continuous glucose monitoring.
CONCLUSION
This analysis of DAR-MENA provides newinsight into the characteristics and pattern offasting and care for people with type 1 diabetesbefore and during Ramadan. Despite the risksassociated with fasting in this population,nearly half of participants fasted for the wholeof the holy month. During Ramadan, meanglycemic control improved and there was nosignificant increase in confirmed and severehypoglycemia events, which may have beendue to pre-Ramadan diabetes education andmodifications in diabetic dosing and regimen.
Although this study showed that confirmed orsevere hypoglycemia and hyperglycemia duringRamadan have a similar incidence as duringpre-Ramadan, the IDF-DAR Practical Guidelinesrecommend that people with type 1 diabetesshould not fast, whether or not their diabetes iswell controlled [3]. Since type 1 diabetes isassociated with other problems such as hyper-glycemia, hypovolemia, and diabetic ketoaci-dosis, those who insist on fasting need to workclosely with their healthcare practitioner toensure that they reduce their risk ofcomplications.
ACKNOWLEDGEMENTS
The authors are grateful to all of the participantsin the study. The authors would like to thank allcontributors of the study, including the inves-tigators from the 113 sites who participated inthe data collection (Table S8 in the supple-mentary material), and the analysts, Soha Ali(Senior Biostatistician, DATACLin CRO) andMohamad Taha (Biostatistics Manager, DATA-CLin CRO), for providing the statistical andanalytical execution of this study. The authorswould also like to acknowledge Helena Ander-sson, Sanofi, for the coordination of the devel-opment of this manuscript.
Funding. Sponsorship for this study wasprovided by Sanofi. This study was conducted incollaboration with DAR International Alliance.Sanofi provided financial support for the con-duct of the study research. All authors had fullaccess to all of the data in this study and takecomplete responsibility for the integrity of thedata and accuracy of the data analysis. Sanofiwas involved in the study design, collection,analysis and interpretation of the data, as wellas data checking of information provided in themanuscript. However, ultimate responsibilityfor opinions, conclusions, and data interpreta-tion lies with the authors. The journal’s RapidService and Open Access Fees were also fundedby Sanofi.
Adv Ther (2020) 37:1550–1563 1561

Medical Writing and Editorial Assis-tance. Editorial assistance in the preparation ofthis article was provided by Breanne Landry andDebby Moss of Caudex (Oxford, UK). Supportfor this assistance was funded by Sanofi.
Authorship. All named authors meet theInternational Committee of Medical JournalEditors (ICMJE) criteria for authorship for thisarticle, take responsibility for the integrity ofthe work as a whole, and have given theirapproval for this version to be published.
Authorship Contributions. Mohamed M.Hassanein and Khier Djaballah developed thestudy concept and design. All authors con-tributed to the data analysis or interpretation ofthe results, and critically revised, provided finalapprovals of, and are accountable for the accu-racy and integrity of the manuscript. Fatheya F.Al Awadi and Khier Djaballah are the guarantorsof this work and, as such, had full access to allthe data in the study and take responsibility forthe integrity of the data and the accuracy of thedata analysis.
Disclosures. Fatheya F. Al Awadi, Sobia SabirAli, Abdulrahman Al Shaikh, Mohamad OmarAbu-Hijleh, and Faris Abdul Kareem Khazaalhave nothing to disclose. Akram Echtay: Advi-sory board member for AstraZeneca, BoehringerIngelheim, Merck, and Novo Nordisk; speakerfor AstraZeneca, Boehringer Ingelheim, Eli Lilly,Merck, Novartis, Novo Nordisk, and Sanofi.Monira Al Arouj: Advisory board member forMerck and Sanofi. Naim Shehadeh: Advisoryboard member for Boehringer Ingelheim, Mer-ck, Novo Nordisk, and Sanofi; consultant forMerck, Novo Nordisk, and Sanofi; recipient ofgrant from Merck, Novo Nordisk, and Sanofi;research investigator for AstraZeneca, Merck,Novo Nordisk, and Sanofi; speaker for Boehrin-ger Ingelheim, Eli Lilly, Novo Nordisk, andSanofi; stock owner from Novo Nordisk. KhierDjaballah: Employee of Sanofi. Cecile Dessapt-Baradez: Employee and shareholder of Sanofi.Abdullah Bennakhi: Advisory board member forMerck and Sanofi. Mohamed El Hassan Gharbi:Advisory board member for Janssen and Servier;research investigator for Sanofi; speaker for
Merck, Novartis, Novo Nordisk, Sanofi, andServier. Khaled El Sayed El Hadidy: Advisoryboard member for Merck and Sanofi; speaker forAstraZeneca, Eli Lilly, Merck, and Sanofi.Mohamed M. Hassanein: Advisory board mem-ber for Boehringer Ingelheim, Novo Nordisk,and Sanofi; speaker for Eli Lilly, Janssen, LifeS-can BI, Merck, Novo Nordisk, and Sanofi.
Compliance with Ethics Guidelines. Themanuscript followed the STrengthening theReporting of OBservational studies in Epidemi-ology (STROBE) guidelines [10]. DAR-MENA wasconducted in accordance with the ethical prin-ciples laid down in the Declaration of Helsinkiand complied with all international guidelines,as well as national laws and regulations of eachcountry in which the registry study was per-formed. The study protocol was approved bythe ethics committee of each participatingcenter (please see Table S9 in the supplementarymaterial for ethics committee names). Partici-pants signed a consent form to participate inthe study. Please note that this study was notadded to a clinical trial registry as it was a non-interventional, prospective, observational studythat did not meet the definition for clinical trialregistration as specified by the World HealthOrganization.
Data Availability. Qualified researchersmay request access to participant-level data andrelated study documents, including the clinicalstudy report, study protocol with any amend-ments, blank case report form, statistical anal-ysis plan, and dataset specifications. Participant-level data will be anonymized, and study doc-uments will be redacted to protect the privacyof trial participants. Further details on Sanofi’sdata sharing criteria, eligible studies, and pro-cess for requesting access can be found athttps://www.clinicalstudydatarequest.com.
Open Access. This article is licensed under aCreative Commons Attribution-NonCommer-cial 4.0 International License, which permitsany non-commercial use, sharing, adaptation,distribution and reproduction in any mediumor format, as long as you give appropriate creditto the original author(s) and the source, provide
1562 Adv Ther (2020) 37:1550–1563

a link to the Creative Commons licence, andindicate if changes were made. The images orother third party material in this article areincluded in the article’s Creative Commonslicence, unless indicated otherwise in a creditline to the material. If material is not includedin the article’s Creative Commons licence andyour intended use is not permitted by statutoryregulation or exceeds the permitted use, youwill need to obtain permission directly from thecopyright holder. To view a copy of this licence,visit http://creativecommons.org/licenses/by-nc/4.0/.
REFERENCES
1. Qur’an. Surah al-Baqarah. 2:185.
2. Al-Arouj M, Bouguerra R, Buse J, et al. Recommen-dations for management of diabetes during Rama-dan. Diabetes Care. 2005;28:2305–11.
3. Hassanein M, Al-Arouj M, Hamdy O, et al. Diabetesand Ramadan: practical guidelines. Diabetes ResClin Pract. 2017;126:303–16.
4. Al-Arouj M, Assaad-Khalil S, Buse J, et al. Recom-mendations for management of diabetes duringRamadan: update 2010. Diabetes Care. 2010;33:1895–902.
5. Salti I, Benard E, Detournay B, et al. A population-based study of diabetes and its characteristics dur-ing the fasting month of Ramadan in 13 countries:results of the epidemiology of diabetes and Rama-dan 1422/2001 (EPIDIAR) study. Diabetes Care.2004;27:2306–11.
6. Hassanein M, Al Awadi FF, El Hadidy KES, et al. Thecharacteristics and pattern of care for the type 2
diabetes mellitus population in the MENA regionduring Ramadan: an international prospectivestudy (DAR-MENA T2DM). Diabetes Res Clin Pract.2019;151:275–84.
7. Alamoudi R, Alsubaiee M, Alqarni A, et al. Attitudesand habits of patients with type 1 diabetes duringfasting Ramadan. J Clin Transl Endocrinol. 2018;14:1–4.
8. Eid YM, Sahmoud SI, Abdelsalam MM, Eichorst B.Empowerment-based diabetes self-managementeducation to maintain glycemic targets duringRamadan fasting in people with diabetes who areon conventional insulin: a feasibility study. Dia-betes Spectr. 2017;30:36–42.
9. Reiter J, Wexler ID, Shehadeh N, Tzur A, Zangen D.Type 1 diabetes and prolonged fasting. Diabet Med.2007;24:436–9.
10. STROBE. STrengthening the Reporting of OBserva-tional studies in Epidemiology. 2014. https://www.strobe-statement.org/index.php?id=strobe-home.Accessed Jul 2018.
11. Ahmedani MY, Hashmi BZ, Ulhaque MS. Ramadanand diabetes—knowledge, attitude and practices ofgeneral practitioners; a cross-sectional study. Pak JMed Sci. 2016;32:846–50.
12. Abid M, Hsairi M, Elleuch M, Ben Aissa E. Survey ondiabetic patients treated with insulin during thefasting month of Ramadan. Int J Gen Med. 2018;11:33–40.
13. Alabbood MH, Ho KW, Simons MR. The effect ofRamadan fasting on glycaemic control in insulindependent diabetic patients: a literature review.Diabetes Metab Syndr. 2017;11:83–7.
14. Ahmed MH, Husain NE, Elmadhoun WM, Noor SK,Khalil AA, Almobarak AO. Diabetes and Ramadan: aconcise and practical update. J Family Med PrimCare. 2017;6:11–8.
Adv Ther (2020) 37:1550–1563 1563