Embed Size (px)
Citation preview

Cas cliniques
DOI of or
Service deSalpetri�ere, As
CorrespondHopital UnivHopitaux de P13, France, E-
Ann Vasc SurDOI: 10.1016/� Annals of V�Edit�e par ELS
Prise en charge chirurgicale d’une coarctationde l’aorte abdominale chez un patient ag�e
Chika Cho, Rapha€el Coscas, Fabien Koskas, Paris, France
La coarctation de l’aorte thoracique basse et/ou de l’aorte abdominale, d�enomm�ee ‘‘middleaortic syndrome’’ (MAS) par les anglo-saxons, est une malformation cardiovasculaire con-g�enitale rare pouvant conduire �a des complications isch�emiques graves. Le diagnostic �etanthabituellement fait au cours de l’enfance ou chez le jeune adulte, la prise en charge du MASchez le patient ag�e est donc exceptionnelle. Nous rapportons le traitement chirurgical d’un MASchez une patiente de 65 ans pr�esentant des signes d’isch�emie menacante r�enale etm�esent�erique. Un pontage thoraco-abdominal implant�e sur l’aorte ascendante et revasculari-sant les art�eres visc�erales �etait r�ealis�e par sterno-laparotomie avec un r�esultat satisfaisant. Lesaspects techniques et th�erapeutiques sont discut�es.
Aortic coarctation is a common congenital cardio-
vascular defect, usually involving the aortic isth-
mus.1 Coarctation of the distal thoracic aorta and/
or the abdominal aorta, namely ‘‘middle aortic
syndrome’’ (MAS), is rare and accounts for 0.5-2.0%
of coarctation cases.2,3 Although diagnosis is usually
made during childhood or in young adulthood, it is
exceptionally made in elderly patients. We here
report the surgical management of a MAS case in a
65-year-old woman.
CASE REPORTS
A 65-year-old woman was referred to our hospital for the
treatment of a complicated MAS. Her past medical history
was consistent for a reno-vascular hypertension in
infancy, for which she underwent a left nephrectomy at
the age of 11 and an aorto-right renal bypass at the age of
iginal article: 10.1016/j.avsg.2009.12.012.
chirurgie vasculaire, Hopital Universitaire de la Piti�e-sistance-Publique Hopitaux de Paris, Paris, France.
ence : Dr Chika Cho, Service de chirurgie vasculaire,ersitaire de la Piti�e-Salpetri�ere, Assistance-Publiquearis, 47-83 boulevard de l’hopital, 75651 Paris, Cedexmail: [email protected]
g 2010; 24: 694.e5-694.e8j.acvfr.2010.12.047ascular Surgery Inc.EVIER MASSON SAS
13. At that time, anMASwas diagnosed but the correction
had not been performed for an unknown reason. She also
had a transient ischemic attack at the age of 45, and she
underwent a partial gastrectomy for bleeding at the age of
63. For 3 years, her renal function has progressively
worsened leading to hemodialysis. At the time of admis-
sion, she had been recently accepted on the waiting list for
renal transplantation. Six months ago, she presented with
an episode of subacute ischemic colitis with severe anemia
(Hb ¼ 2.5 g/dL), treated medically using corticosteroids.
Given the severity of this recent episode, the antecedents
of reno-vascular hypertension, and the need for future
renal transplantation in the setting of an MAS, she was
referred to our department for surgical correction of her
aortic disease. On examination, upper extremity pulses
were normal but femoral pulses were reduced. A mode-
rate hypertension (142/68 mm Hg) despite oral quadri-
therapy was noted. The patient denied any symptom of
intestinal ischemia at the time of examination (no abdo-
minal pain, normal abdominal palpation), or lower limb
claudication. Laboratory tests noted a creatinine at
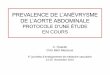
3.6 mg/dL. Computed tomography scan demonstrated an
MAS extending from the celiac trunk level down to right
renal artery level (Fig. 1A). Moreover, a 40% stenosis
associated with a post-stenotic aneurysm was noted at the
origin of the celiac trunk. There was a 60% stenosis on the
two first centimeters of the superior mesenteric artery.
The inferior mesenteric artery was occluded. Of note, the
prior aorto-right renal bypass was patent (Fig. 1B).
Given the risk of intestinal ischemia recurrence, the
persistent hypertension, and the need for an adequate
iliac inflow for a future renal transplantation, a
758.e5

Fig. 1. A Preoperative computed tomographic angio-
graphy showed suprarenal coarctation with celiac artery
stenosis and associated aneurysm, and superior mesen-
teric artery stenosis. B Preoperative computed tomo-
graphic angiography showed the ancien aorto-right renal
artery bypass.
758.e6 Cas cliniques Annales de chirurgie vasculaire
revascularization was decided. Through median sterno-
laparotomy, a 20-mm Dacron graft was proximally anas-
tomosed to the ascending aorta. It was tunnelized to the
abdomen through a small incision in themiddle part of the
diaphragm, and positioned behind the left part of the liver
and the pancreas. The graft was then brought straight
down anteriorly to the left side of the abdominal aorta.
The celiac trunk and the superior mesenteric artery
were directly reimplanted into the graft. The infrarenal
aorta was ligated. Distally, the graft was anastomosed in
an end-to-end manner to a 20/10-mm bifurcated graft
sewn to the common iliac arteries. Therefore, the right
kidney was perfused in a retrograde manner through the
patent aorto-right renal artery bypass. Postoperative
course was uncomplicated. Histopathologic study of vis-
ceral vessels showed intimo-medial fibrosis, but the
absence of inflammatory process.
The follow-up was uneventful (no intestinal symp-
toms, no lower limb claudication, good recovery). At
3 months, the patient remained under hemodialysis but
her blood pressure normalized (105/60 mm Hg) under an
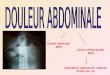
oral monotherapy. The computed tomography -scan does
not show any anomaly and her aortic repair remained
patent (Fig. 2).
Fig. 2. Postoperative computed tomography scan. The
bypass is patent and there is a good perfusion of reim-
planted collaterals.
DISCUSSION
Our case demonstrates that MAS is a potential cause
of visceral/renal malperfusion in the elderly
patients, and can be successfully treated using tho-
racoabdominal bypass.
MASwas first described by Sen et al. in 19634 but
its etiology remains poorly understood5 It can be
caused by Takayasu’s or temporal arteritis, neurofi-
bromatosis, fibromuscular dysplasia, retroperitoneal
fibrosis, mucopolysaccharidosis, Williams syn-
drome, and/or a developmental anomaly in the
fusion of the paired embryonic dorsal aortas.6-9 In
the present case, findings of the histopathological

Vol. 24, No. 5, 2010 Cas cliniques 758.e7
examination were not specific and it is probable that
the etiologywas congenital, as attested by thehistory
of renovascular hypertension during childhood, the
intimo-medial fibrosis, and the absence of any
inflammatory process.
Diagnosis of MAS is usually made during child-
hood or young adulthood. Mean age at diagnosis is
about 20 years.10 Symptoms are mainly related to
hypertension in the central vasculature proximal to
the aortic stenosis and to arterial insufficiency in the
vasculature distal to the stenosis (renal, visceral,
and/or iliac arteries). Uncontrolled renovascular
hypertension may lead to left ventricular hyper-
trophy, cardiomegaly, cerebrovascular accidents,
coronary artery disease, and congestive cardiac fai-
lure. The arterial inflow impairment to the kidneys
secondary to aortic coarctation and renal artery
stenosis may result in renal function impairment
and renal failure, as illustrated by our case. Symp-
toms of bowel ischemia are rarer.
Although patients not appropriately treated
experience premature death,3,11 our patient sur-
vived without undergoing any intervention to cor-
rect her aortic coarctation until the age of 65, despite
the occurrence of various symptoms secondary to
MAS since childhood (hypertension, transient
ischemic attack, chronic renal failure, intestinal
angina). The right renal revascularization at the age
of 13, the left nephrectomy, and the maximal
medical management using a quadritherapy may
have had a role to play in postponing the conse-
quences of hypertension.
Anatomically, the association of MAS with visce-
ral/renal stenoses is frequent, as illustrated by our
case. A recent series of 53 cases12 from the Uni-
versity of Michigan identified suprarenal coarcta-
tion in 69%, inter-renal coarctation in 23%, and
infrarenal coarctation in 8%. Eighty-seven percent
had renal artery narrowings or occlusions, and 62%
had celiac or mesenteric artery stenosis or occlu-
sions, with both vessels involved in 82%.
The primary indication for surgical intervention
is usually the level of hypertension3 However,
malperfusion of mesenteric vessels and the need for
an aorto-iliac inflow for further renal transplanta-
tion were the main indication in our case.
In planning an aortic repair for MAS treatment,
the choice of the technique to use remains in ques-
tion. Thoracoabdominal bypass, graft replacement,
patch angioplasty, and transluminal angioplasty
were successfully reported.3,13 The choice between
these techniques is dependent on the patient’s
general status (age, comorbidities), the exact loca-
tion and extension of the MAS, and the existence of
stenoses on critical aortic collaterals. However,
direct replacement carries a theoretical risk of post-
operative paraplegia; patch angioplasty is associated
with late degeneration, and long-term results of
endoluminal angioplasty are controversial.14-16 In
our case, given the good life expectancy of our
patient and the existence of visceral stenosis, we
elected to perform an open surgical reconstruction
using a thoracoabdominal bypass with direct reim-
plantation of the visceral vessels in the graft. The use
of the ascending aorta as bypass inflow avoided the
clamping of the descending thoracic aorta, thereby
minimizing the risk of postoperative paraplegia
while allowing for direct reimplantation of mesen-
teric vessels.
CONCLUSION
MAS is a rare condition in the elderly patients. This
diagnosis should be suspected in patients presenting
with a history of visceral, renal, and/or lower limb
malperfusion. Thoracoabdominal bypass remains a
useful option whenMAS is associated with stenoses
of critical aortic collaterals.
REFERENCES
1. Rao PS. Coarctation of the aorta. Curr Cardiol Rep 2005;7:
425-434.
2. Bergamini TM, Bernard JD, Mavroudis C, Backer CL,
Muster AJ, Richardson JD. Coarctation of the abdominal
aorta. Ann Vasc Surg 1995;9:352-356.
3. Delis KT, Gloviczki P. Middle aortic syndrome: from pre-
sentation to contemporary open surgical and endovascular
treatment. Perspect Vasc Surg Endovasc Ther 2005;17:
187-203.
4. Sen PK, Kinare SG, Engineer SD, Parulkar GB. The middle
aortic syndrome. Br Heart J 1963;25:610-618.
5. O’Neill JA, Berkowitz JH, Fellows KJ, Harmon CM.
Midaortic syndrome and hypertension in childhood.
J Pediatr Surg 1995;30:164-172.
6. Connolly JE, Wilson SE, Lawrence PL, Fujitani RM. Middle
aortic syndrome: distal thoracic and abdominal coarctation,
a disorder with multiple etiologies. J Am Coll Surg 2002;194:
774-781.
7. Greene JF Jr, Fitzwater JE, Burgess J. Arterial lesions asso-
ciated with neurofibromatosis. Am J Clin Pathol 1974;62:
481-487.
8. Quek SC, Tan L, Quek ST, Yip W, Aw M, Quak SH. Abdo-
minal coarctation and Alagille syndrome. Pediatrics
2000;106:E9.
9. Radford DJ, Pohlner PG. The middle aortic syndrome: an
important feature of Williams’ syndrome. Cardiol Young
2000;10:597-602.
10. Lin YJ, Hwang B, Lee PC, Yang LY, Meng CC. Mid-aortic
syndrome: a case report and review of the literature. Int J
Cardiol 2008;123:348-352.
11. Kirklin JW. Barrett-Boyes BG Cardiac Surgery. 2nd edn.
New York: Churchill Livingstone, 1993. pp 1264-1303.
12. Stanley JC, Criado E, Eliason JL, Upchurch GR Jr,
Berguer R, Rectenwald JE. Abdominal aortic coarctation:
surgical treatment of 53 patients with a thoracoabdominal

758.e8 Cas cliniques Annales de chirurgie vasculaire
bypass, patch aortoplasty, or interposition aortoaortic graft.
J Vasc Surg 2008;48:1073-1082.
13. Hallett JW Jr, Brewster DC, Darling RC, O’Hara PJ. Coarc-
tation of the abdominal aorta: current options in surgical
management. Ann Surg 1980;191:430-437.
14. Sharma S, Bahl VK, Saxena A, Kothari SS, Talwar KK,
Rajani M. Stenosis in the aorta caused by non-specific aor-
titis: results of treatment by percutaneous stent placement.
Clin Radiol 1999;54:46-50.
15. Parodi JC, Ferreira LM, Faella H, La Mura R, Ruslender E,
Henestrosa G. Use of covered stents and endograft as a res-
cue treatment in a patient with a complex form of recurrent
aortic coarctation. J Vasc Surg 2007;45:1263-1267.
16. Trimarchi S, Tolva VS, Grassi V, Frigiola A, Carminati M,
Rampoldi V. Descending thoracic and abdominal aortic
coarctation in the young: surgical treatment after per-
cutaneous approaches failure. J Vasc Surg 2008;47:
865-867.