Embed Size (px)
Citation preview
Universitéde Montréal
Département d’administrationde la santé
Groupe de recherche Interdisciplinaire en santé (GRIS)
The Dr. Joseph Kaufmann Chair in Geriatric MedicineLa Chaire Dr Joseph Kaufman en gériatrie
McGill
Centre de recherche
Institutuniversitaire de
gériatrie de Montréal
Hôpital général juifSir Mortimer B. DavisJewish General Hospital
Centre d’épidémiologie clinique et de recherche en santé publique, Institut Lady Davis
Centre for Clinical Epidemiology and Community Studies, Lady Davis Institute
François Béland, PhD
Département d’administration de la santéUniversité de Montréal
Co-Directeur, SOLIDAGEGroupe de recherche Université de Montréal et McGill sur
les services intégrés aux personnes âgées.
SIPA. An integrated system of care
for frail elderly persons
Réseau canadien de recherche pour les soins dans la communauté,Toronto, 23 Octobre 2006
Universitéde Montréal
Département d’administrationde la santé
Groupe de recherche Interdisciplinaire en santé (GRIS)
The Dr. Joseph Kaufmann Chair in Geriatric MedicineLa Chaire Dr Joseph Kaufman en gériatrie
McGill
Centre de recherche
Institutuniversitaire de
gériatrie de Montréal
Hôpital général juifSir Mortimer B. DavisJewish General Hospital
Centre d’épidémiologie clinique et de recherche en santé publique, Institut Lady Davis
Centre for Clinical Epidemiology and Community Studies, Lady Davis Institute
SIPA. An integrated system of care
for frail elderly persons
François Béland PhD Howard Bergman MDPaule Lebel MD
Pierre Tousignant, Johanne Monette, Jean Louis Denis, André-Pierre Contandriopoulos, Francine Ducharme,
Jean-François Boivin, Stan Shapiro
Kathy Lesperance, Luc Dallaire, Cristian Morales, Claude Richard, Denis Roberge, Nassera Touati, Ellen Leibovitch
Collaboration internationaleDavid Challis, A. Mark Clarfield, Jack Guralnik, Robert Kane
Universitéde Montréal
Département d’administrationde la santé
Groupe de recherche Interdisciplinaire en santé (GRIS)
The Dr. Joseph Kaufmann Chair in Geriatric MedicineLa Chaire Dr Joseph Kaufman en gériatrie
McGill
Centre de recherche
Institutuniversitaire de
gériatrie de Montréal
Hôpital général juifSir Mortimer B. DavisJewish General Hospital
Centre d’épidémiologie clinique et de recherche en santé publique, Institut Lady Davis
Centre for Clinical Epidemiology and Community Studies, Lady Davis Institute
L’équipe de direction clinique:Luce Beauregard,
Régie régionale de la Santéet des Services sociaux de Montréal-Centre
Diane Boutin, Danielle Dubois et Michel Lemieux,Centre local de services communautaires Bordeaux-Cartierville
Lorraine Bouvier, Myriam ProulxCentre local de services communautaires Côte-des-Neiges
SIPA. An integrated system of care
for frail elderly persons
For further informationon SIPA:
www.solidage.ca
Topics:
SIPA: What it is!Results from the experimental demonstrationproject. Some lessons.
SIPA: What it is!
SIPA: «SSystème de soins Intégrés pour Personnes Âgées fragiles»
Community-based system of care responsible for the full range of services:
Social and health care, acute and long-term care, community-and institution-based—including acute care hospitalizations, convalescence care, nursing homes, prescribed drugs, etc.
Responsibility for health outcome, utilization and costs of services for the population of frail elderly persons in a specific catchment area Integration of social and health care through:
Case managementMulti-disciplinary teamCare guidelines and protocols based on best practices
SIPA: An integrated system of care for frail elderly personsA responsive organization able to mobilize resources flexiblyand rapidly to meet needs, and avoid inappropriate utilization:
Availability of intensive community services; Early detection and intervention in:
Medical, social and rehabilitation needs and services. Fast communication and response to frail elderly person, and their family, needs:
On call services, providers linkages; Pre-payment with per capita budget with financial responsibility for the full range of services.Integrated with Canadian Medicare: Universal, single payer, and publicly managed.
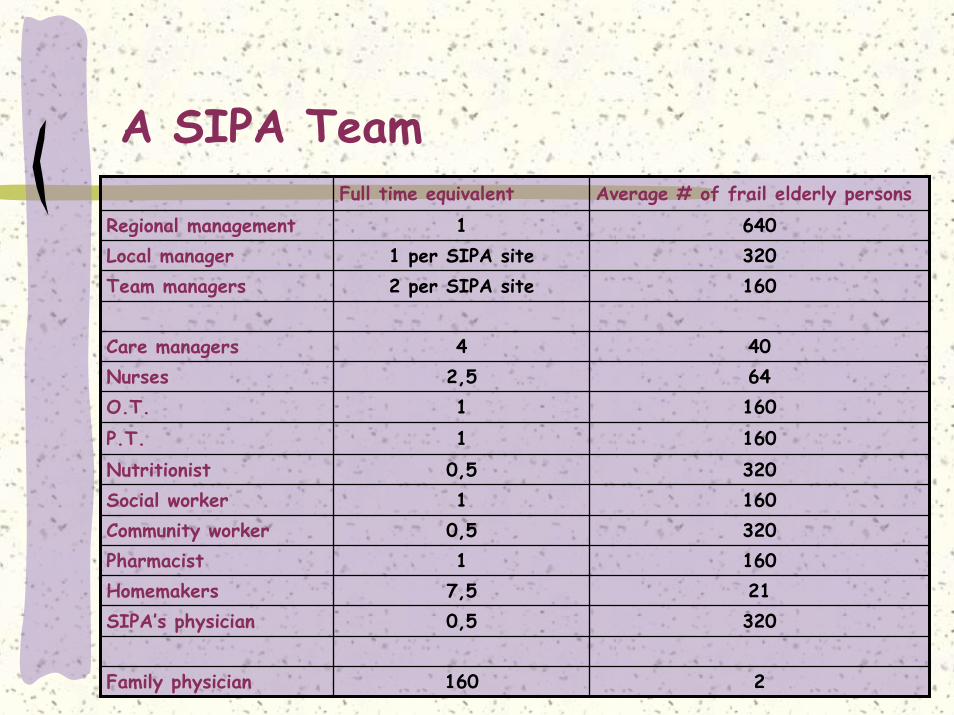
A SIPA TeamFull time equivalent Average # of frail elderly persons
Regional management 1 640Local manager 1 per SIPA site 320Team managers 2 per SIPA site 160
Care managers 4 40Nurses 2,5 64O.T. 1 160P.T. 1 160Nutritionist 0,5 320Social worker 1 160Community worker 0,5 320Pharmacist 1 160Homemakers 7,5 21SIPA’s physician 0,5 320
Family physician 160 2
Issues and HypothesesStudy the feasibility of SIPA:
Implementation and managementObserved changes in health status:
No change in health or functional outcomesEvaluation of quality of care:
Equivalent or improved quality of care, comparable or improved quality of life and increased satisfaction in the SIPA group
Estimate changes in patterns of health services utilization:Integration of health and social careChange in the configuration of utilization by decreasing acute hospital use (in-patient and ER) and institutional-based LTC
Estimate and compare costs:Cost neutral, or decrease total costs
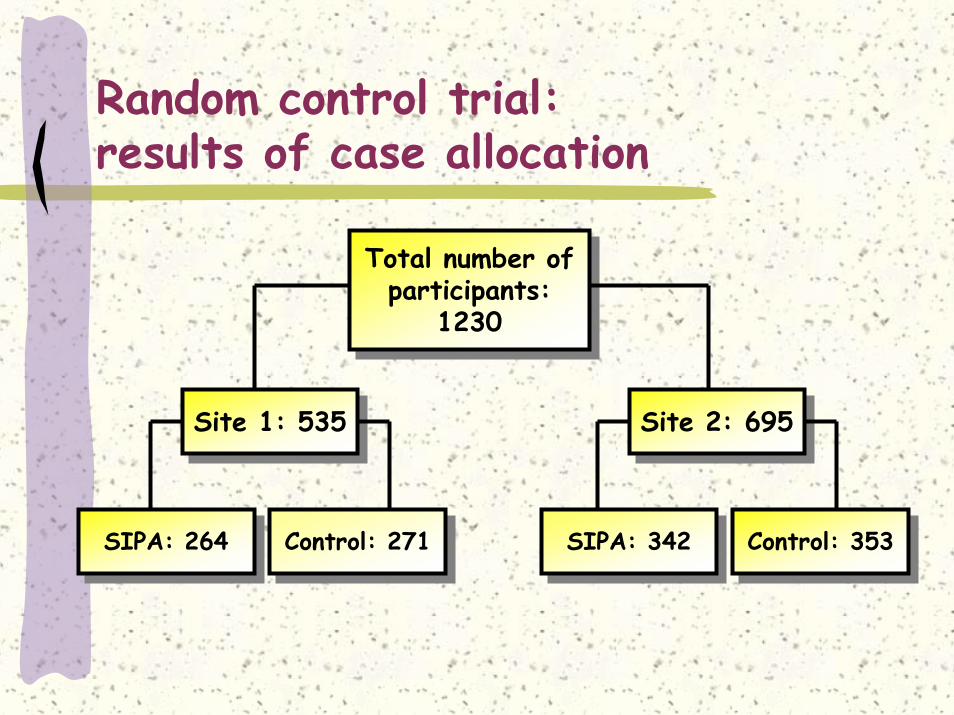
Random control trial: results of case allocation
Total number of participants:
1230
Total number of participants:
1230
Site 2: 695Site 2: 695Site 1: 535Site 1: 535
SIPA: 342SIPA: 342Control: 271Control: 271SIPA: 264SIPA: 264 Control: 353Control: 353
Data sourcesImplementation (12 months):
78 open interviews with staffNon-obstrusive observations of decision-making processesDocuments
Quality of care (12 months): CSQ-8Case studies
Utilization and costs (22 months):Physicians payment, drugs and prostetic equipments (RAMQ)Hospitalizations, emergency, outpatient clinics (MEDécho; records)Institutionalization (RRSSSM-C)Community home-based care (SICC)
Health status (12 months): Questionnaires to participants (T0 and T1); and caregivers (T1)
Results fromthe evaluation
Implantation and organizationAchieved:
Clinical responsibility over the span of services and agenciesOn call services, information sharing between care providers, rapid and flexible use of resourcesInterdisciplinaritySIPA’s physicians involve in the multidisciplinary team
Partially achieved:Case management: learning processFinancial responsibility: concerned with costs
Weaknesses:Cooperation with family physician did not work, but some documented cases of exchange with the SIPA teamCollaboration with partners (hospitals, nursing homes, day centers)
Quality of care
Perceived quality of care is higher in the SIPA group;Case study:
Room for improvements in the management of specific health problemsInsufficient use of protocols (diabetes, falls, depression, chronic heart failures, drugs…) :
Frequency of use less than expectedFollow-up
The analysis of “critical events” does not reveal poor management.
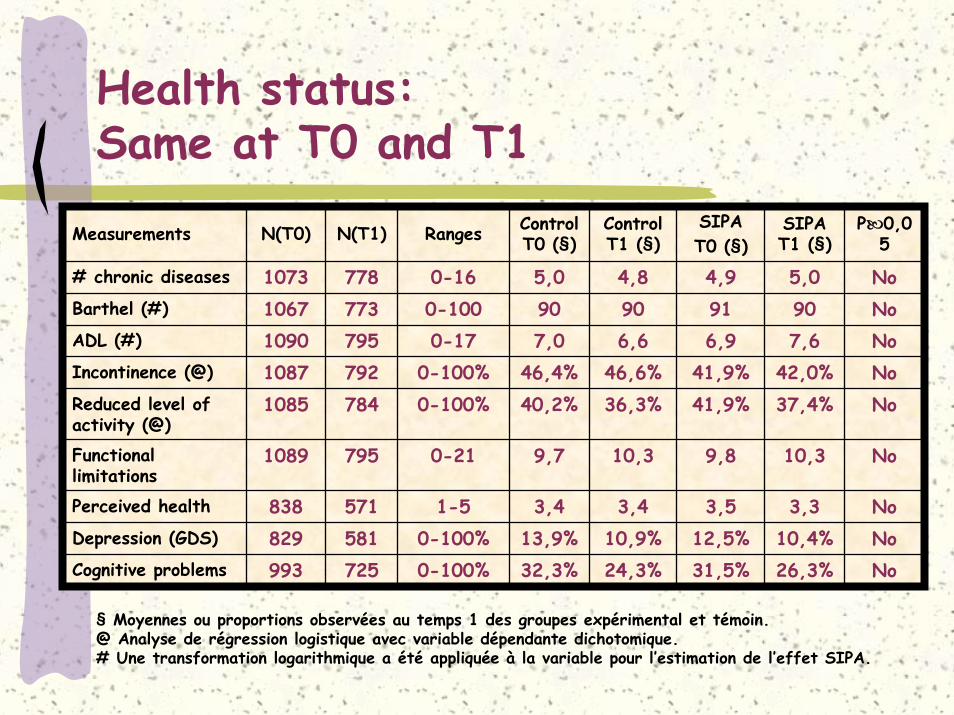
Health status:Same at T0 and T1
Measurements N(T0) N(T1) Ranges ControlT0 (§)
ControlT1 (§)
SIPA T0 (§)
778 4,9916,9
41,9%41,9%
9,8
3,512,5%
Cognitive problems 993 725 0-100% 32,3% 24,3% 31,5% 26,3% No
773795
Incontinence (@) 1087 792 0-100% 46,4% 46,6% 42,0% NoReduced level of activity (@)
1085 784 0-100% 40,2% 36,3% 37,4% No
795
571581
SIPA T1 (§)
P 0,05
# chronic diseases 1073 0-16 5,0 4,8 5,0 NoNoNo
No
NoNo
Barthel (#) 1067 0-100 90 90 90ADL (#) 1090 0-17 7,0 6,6 7,6
Functionallimitations
1089 0-21 9,7 10,3 10,3
Perceived health 838 1-5 3,4 3,4 3,3Depression (GDS) 829 0-100% 13,9% 10,9% 10,4%
§ Moyennes ou proportions observées au temps 1 des groupes expérimental et témoin.@ Analyse de régression logistique avec variable dépendante dichotomique.# Une transformation logarithmique a été appliquée à la variable pour l’estimation de l’effet SIPA.
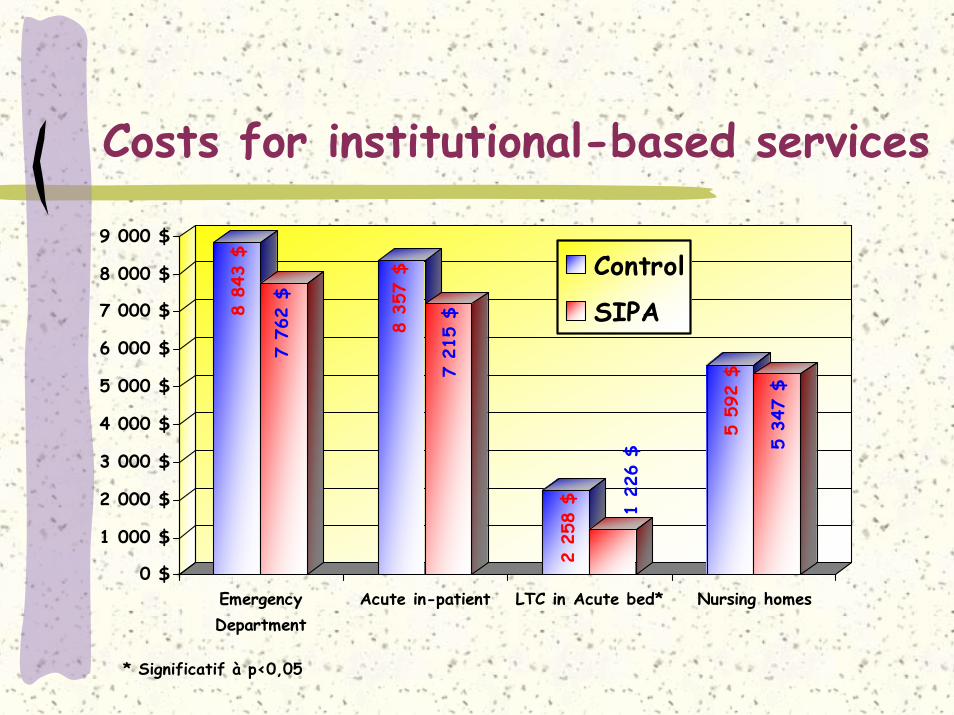
Costs for institutional-based services
8 84
3 $
7 76
2 $
8 35
7 $
7 21
5 $
2 25
8 $ 1 22
6 $
5 59
2 $
5 34
7 $
0 $
1 000 $
2 000 $
3 000 $
4 000 $
5 000 $
6 000 $
7 000 $
8 000 $
9 000 $
EmergencyDepartment
Acute in-patient LTC in Acute bed* Nursing homes
Control
SIPA
* Significatif à p<0,05
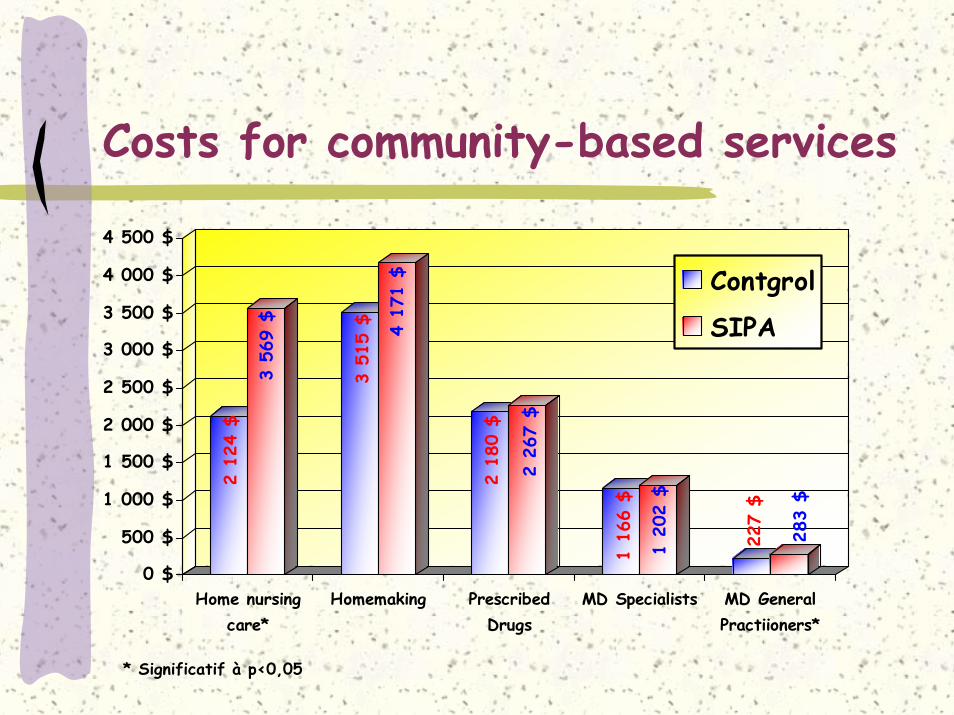
Costs for community-based services
2 12
4 $
3 56
9 $
3 51
5 $ 4 17
1 $
2 18
0 $
2 26
7 $
1 16
6 $
1 20
2 $
227
$
283
$
0 $
500 $
1 000 $
1 500 $
2 000 $
2 500 $
3 000 $
3 500 $
4 000 $
4 500 $
Home nursingcare*
Homemaking PrescribedDrugs
MD Specialists MD GeneralPractiioners*
Contgrol
SIPA
* Significatif à p<0,05
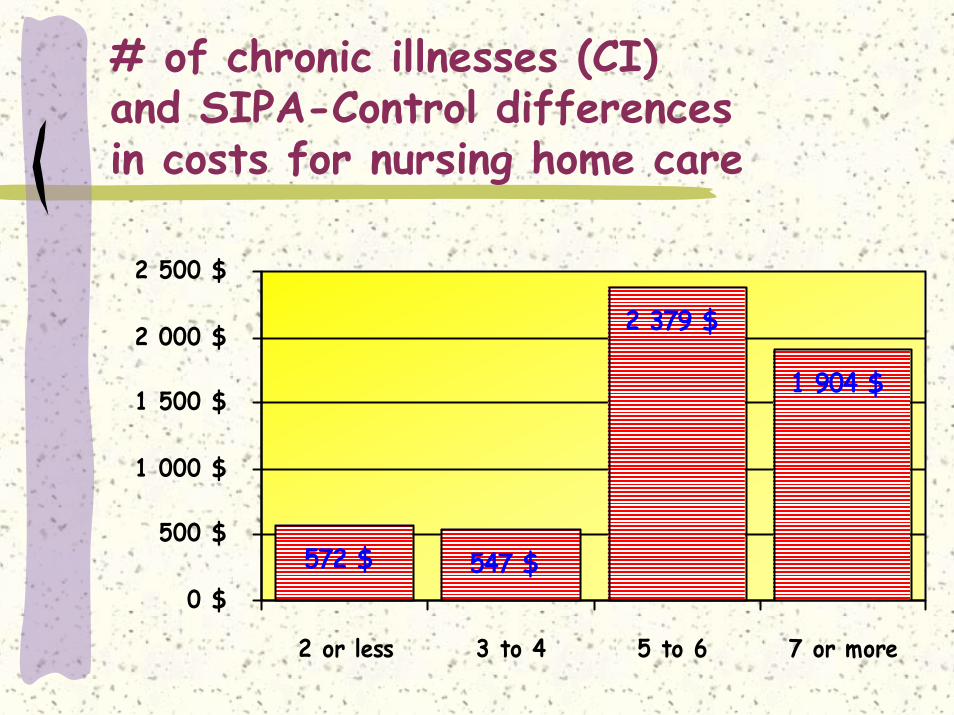
# of chronic illnesses (CI) and SIPA-Control differencesin costs for nursing home care
572 $ 547 $
2 379 $
1 904 $
0 $
500 $
1 000 $
1 500 $
2 000 $
2 500 $
2 or less 3 to 4 5 to 6 7 or more
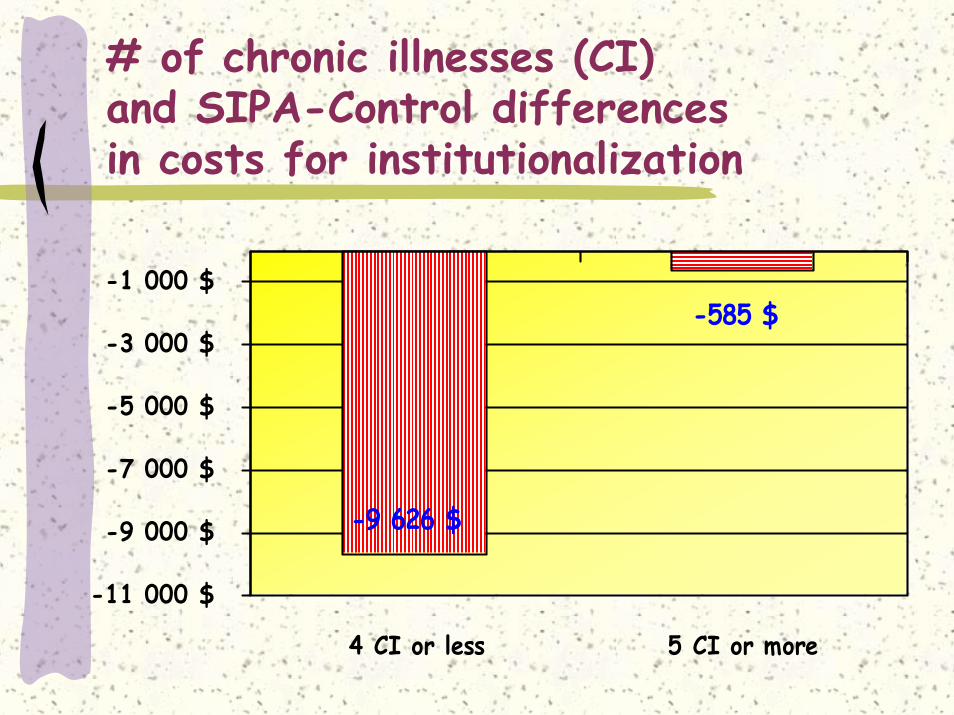
# of chronic illnesses (CI) and SIPA-Control differencesin costs for institutionalization
-585 $
-9 626 $
-11 000 $
-9 000 $
-7 000 $
-5 000 $
-3 000 $
-1 000 $
4 CI or less 5 CI or more
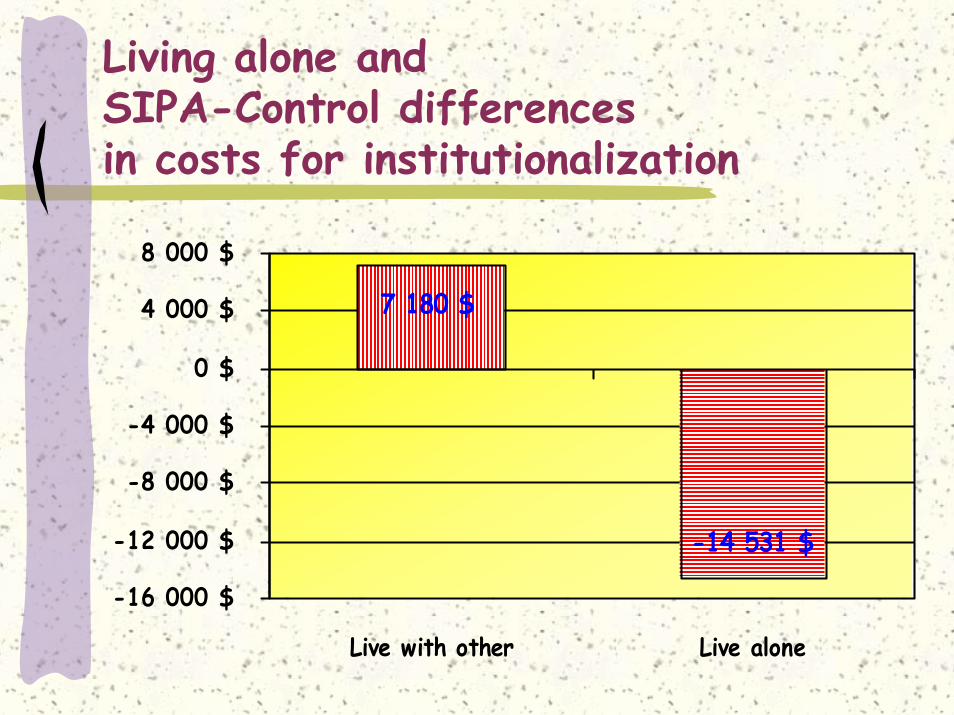
Living alone andSIPA-Control differencesin costs for institutionalization
-14 531 $
7 180 $
-16 000 $
-12 000 $
-8 000 $
-4 000 $
0 $
4 000 $
8 000 $
Live with other Live alone
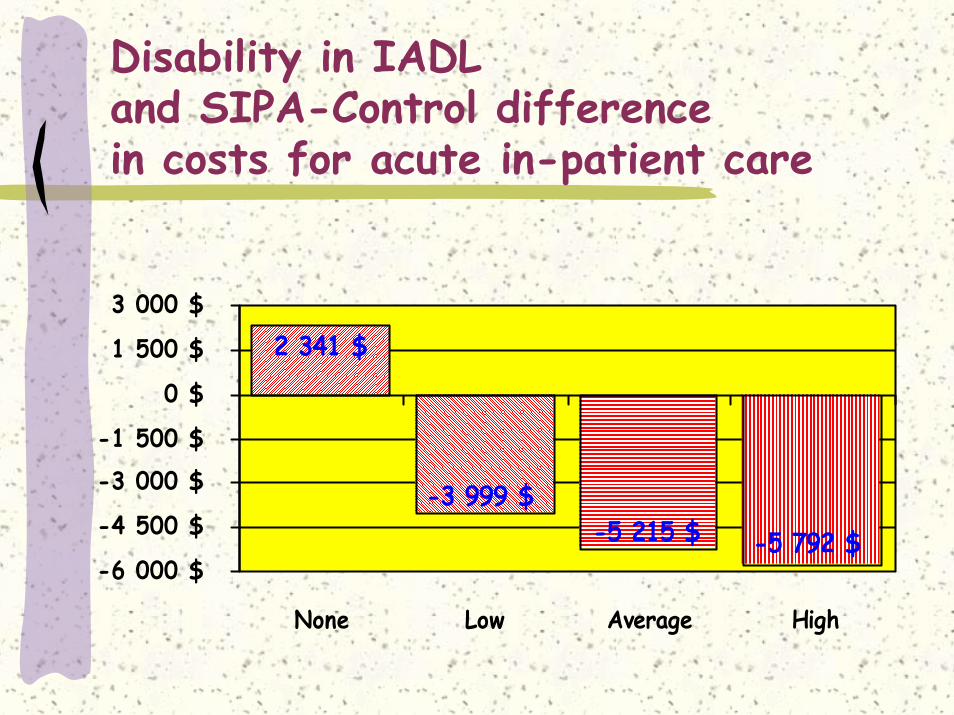
Disability in IADLand SIPA-Control differencein costs for acute in-patient care
-5 215 $ -5 792 $
-3 999 $
2 341 $
-6 000 $
-4 500 $
-3 000 $-1 500 $
0 $
1 500 $
3 000 $
None Low Average High
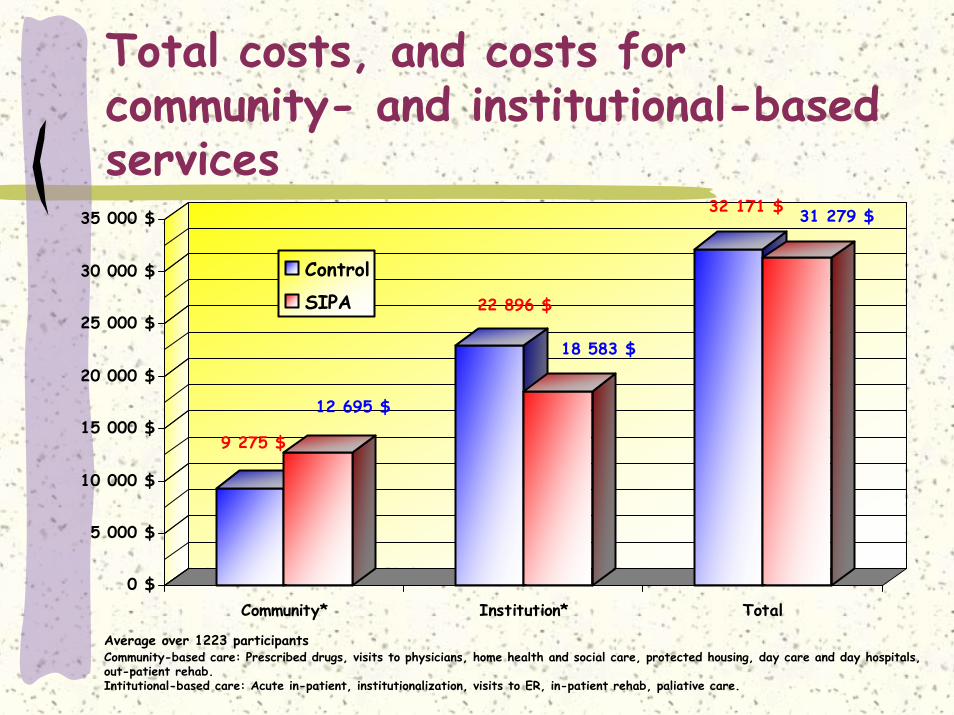
Total costs, and costs for community- and institutional-basedservices
9 275 $
12 695 $
22 896 $
18 583 $
32 171 $ 31 279 $
0 $
5 000 $
10 000 $
15 000 $
20 000 $
25 000 $
30 000 $
35 000 $
Community* Institution* Total
ControlSIPA
Community-based care: Prescribed drugs, visits to physicians, home health and social care, protected housing, day care and day hospitals, out-patient rehab.Intitutional-based care: Acute in-patient, institutionalization, visits to ER, in-patient rehab, paliative care.
Average over 1223 participants
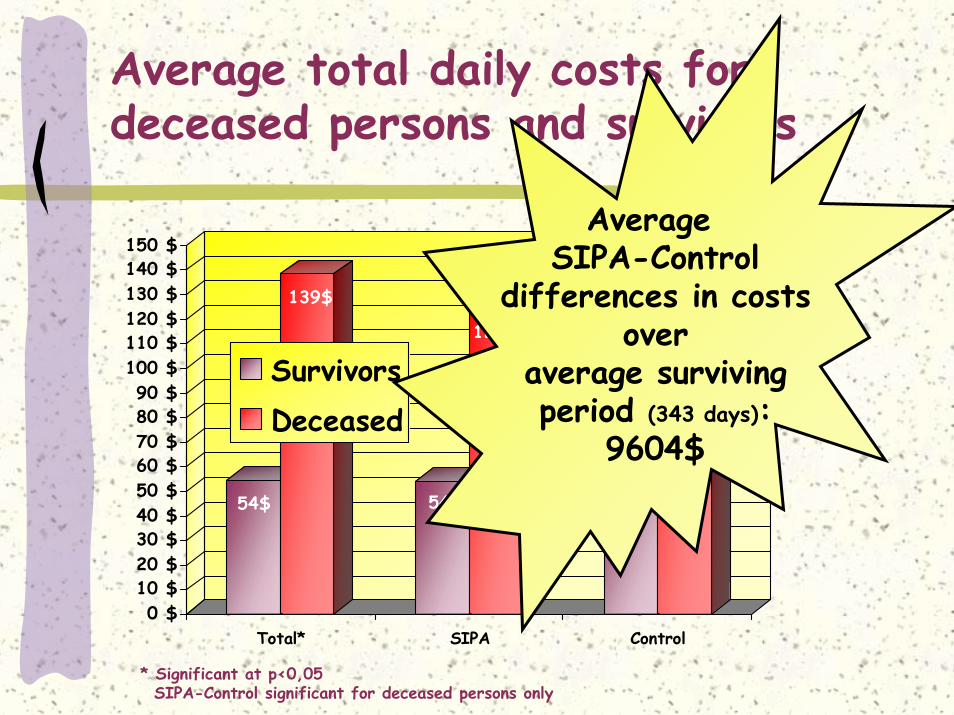
Average total daily costs for deceased persons and survivors
54$
139$
54$
123$
55$
151$
0 $10 $20 $30 $40 $50 $60 $70 $80 $90 $
100 $110 $120 $130 $140 $150 $
Total* SIPA Control
SurvivorsDeceased
* Significant at p<0,05SIPA-Control significant for deceased persons only
AverageSIPA-Control
differences in costsover
average survivingperiod (343 days):
9604$
Lessons and take home
Conditions for a successfulimplementation of SIPA: ClinicIntegration of community-based social and medical care witheasy and fast referal and consultation with geriatric and psycho-geriatric servicesIntegration of family physicians with, or within, the SIPA teamInterdisciplinary protocols and guidelines for screening and care targeted to main sources of disability and chronic diseasesIdentification of persons, and caregivers, with highly complexneeds for integrated services in the communityCare management as a clinical practice, not a management positionThe frail elderly person social and physical environments shouldbe integrated within the care plan
Conditions for a successfulimplementation of SIPA: ManagementA management system:
Respectful of:Frail elderly persons and caregiversStaff delivering the services
Promote decision making by persons responsible for care deliveryPromote imputability by staff and management
Needs for information systems: Useful at the clinical levelUseful for those delivering the servicesUseful for managing and assessing careUseful for assessing responsiveness to needs
Quality assurance at all levels, clinical and managerial:Needs for indicatorsNeeds for the integration of quality assessment at the day to day clinical level.
Training, training, training – everyone, from homemakers to nurses, to physicians
Conditions for a successfulimplementation of SIPA: FinancingFinancing should promote:
Community-based careFlexible use of services at the level of frail elderly personsPerformance and imputability:
To target populationTo regional and ministerial authorities
Financing should be base on population-level needs for services to frail elderly persons in a catchment area





























