Embed Size (px)
Citation preview

NATURE REVIEWS | UROLOGY ADVANCE ONLINE PUBLICATION | 1
Centre de Recherche en Cancérologie de l’Université Laval, CHU de Québec‑L’Hôtel‑Dieu de Québec, 10 McMahon, Québec, QC G1R 3S1, Canada (H. LaRue, C. Ayari, A. Bergeron, Y. Fradet).
Correspondence to: Y. Fradet yves.fradet@ crhdq.ulaval.ca
Toll-like receptors in urothelial cells—targets for cancer immunotherapyHélène LaRue, Cherifa Ayari, Alain Bergeron and Yves Fradet
Abstract | Toll‑like receptors (TLRs) have an important role in the activation of both innate and adaptive immunity in response to pathogens and danger signals. These receptors are expressed in immune cells and in some epithelia. They are expressed in the epithelium of the urinary bladder, where they actively participate in the fight against infection by uropathogens. TLR expression is decreased (although still evident) in bladder tumours, especially in non‑muscle‑invasive tumours. Intravesical immunotherapy with BCG to prevent recurrence of these tumours has been shown to involve the participation of three different TLRs (TLR2, TLR4, and TLR9). However, alternative therapies are needed as BCG fails in some patients and can sometimes cause severe adverse effects that are difficult to tolerate. In recent years, TLR2, TLR4, TLR7, and TLR9 agonists have been tested in vitro and in vivo for their ability to activate an antitumour immune response against bladder cancer. Promising results from these studies have led to the testing of TLR7 and TLR9 agonists in clinical trials.
LaRue, H. et al. Nat. Rev. Urol. advance online publication 27 August 2013; doi:10.1038/nrurol.2013.153
IntroductionBladder cancer is a common cancer worldwide—with average age standardized rates (ASRs) of 10.1 per 100,000 men and 2.5 per 100,000 women1—but has a particularly high incidence in the USA (ASR of 37.9 per 100,000 men and 9.6 per 100,000 women)2 and in Western Europe (ASR of 23.6 per 100,000 men and 5.4 per 100,000 women).1 It is a heterogeneous disease and 75–85% of patients present with non-muscle-invasive tumours (stage pTa, pT1, or pTis) at initial diagnosis.1,3–6 Although the remaining 15–25% of tumours are muscle-invasive life-threatening cancers, non-muscle-invasive bladder cancers (NMIBCs) represent the major burden of bladder- cancer-related care as the high recurrence rate necessitates lifetime monitoring by cystoscopies and treatment of these multiple recurrences by transurethral resection (TUR) followed by intravesical chemotherapy or immunotherapy. As such, bladder cancer costs more to treat per patient than any other cancer in the USA.7
The most successful therapy for decreasing the risk of recurrence and progression of NMIBCs is intra vesical immunotherapy with BCG.1,3,8,9 Intravesical instilla-tions of BCG cause extensive inflammation in the bladder wall, which helps to eliminate tumour cells.10,11 Urothelium—the specialized epithelium that lines the bladder— possesses sensory and signalling properties, as well as the ability to release chemical mediators following physical and chemical signalling stimulation.12 Urothelial cells also undergo phagocytosis, degrade antigens and present antigenic proteins on their surface, secrete pro-inflammatory cytokines, and modulate the recruitment
and activity of immune cells,13,14 suggesting an active host defence function against pathogens. Toll-like receptors (TLRs) are expressed in urothelial cells and are thought to have a role in the response to uropathogens and to immunotherapy with BCG.15–19
In recent years, alternatives to BCG immunotherapy that involve the induction of innate immune responses via TLR activation have been explored using in vitro and in vivo models of bladder cancer, with promising results. Some agents, such as mycobacterial cell wall DNA complexes and imiquimod, have also been tested in clinical assays. In this Review, we focus on the expres-sion and role of TLRs in normal and tumour urothelial cells and the potential use of TLR agonists for bladder cancer treatment.
TLRs and their ligandsTLRs are highly conserved transmembrane proteins, composed of a leucine-rich extracellular or cytoplasmic domain (depending on TLR localization) that recognizes TLR agonists, a transmembrane domain, and a globular toll/interleukin 1 (TIR) domain, which is essential for intracellular signalling.20 TLRs have an e ssential role in innate immunity, specifically in recog nizing pathogen- associated molecular patterns (PAMPs)—which are conserved molecular patterns associ ated with pathogens20–23— and other danger-signalling endogenous ligands that are generated upon cell or tissue damage.21,23 TLRs are also involved in adaptive immunity. They are expressed on immune cells, particularly on dendritic cells, which act as an important interface between innate and adaptive immunity.22,24 Dendritic cells are the most powerful antigen-presenting cells. TLR activation
Competing interestsThe authors declare no competing interests.
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved

2 | ADVANCE ONLINE PUBLICATION www.nature.com/nrurol
promotes their maturation and the production of cyto-kines such as interleukin-12, which signals naive T cells to mature into type 1 helper T cells.25 Epithelial cells that are likely to be in contact with a microbial environment also express these receptors.
Ten and 12 distinct TLRs have been identified in humans and mice, respectively. TLR1-10 genes are conserved in both species, although mouse Tlr10 is not functional. Tlr11, Tlr12, and Tlr13 are present in mice but not in humans.22,26 Each receptor recognizes distinct PAMPs, except for TLR1 and TLR6, which form heterodimers with TLR2 (Table 1). Few natural ligands have been described for most TLRs, although many structurally diverse bacterial compounds have been proposed as ligands for TLR2. However, for some studies, it is suspected that the observed TLR2 activation potential of some of these ligands, such as peptido glycan or lipoteichoic acid, could result from the contamina-tion of candidate ligand preparations with highly active lipoprotein.27–30
TLR1, TLR2, TLR4, TLR5, and TLR6 recognize bacterial or fungal components and are expressed in the plasma membrane. TLR3, TLR7, TLR8, and TLR9 recog nize microbial nucleic acids and are expressed in the membrane of intracellular vesicles such as endosomes, lysosomes, and endolysosomes.22 All TLRs operate via complex signalling pathways, leading to the expression of a diverse array of proteins, including proinflammatory cytokines, chemokines, interferons, and co-stimulation molecules. Signalling diversity is compounded by the recruitment of different TIR-domain-containing adaptor molecules upon activation of TLRs, such as myeloid differ entiation factor 88 (MyD88), TIR-associated protein (TIRAP), TIR-domain-containing adaptor protein indu-cing IFNβ (TRIF), and TRIF-related adaptor molecule (TRAM). MyD88 is recruited by all TLRs except TLR3, whereas TRIF is only recruited by TLR3 and TLR4. MyD88 activates MAPKs and NF-κB (which induce the secretion of proinflammatory cytokines), whereas TRIF activates NF-κB and IRF3 (which induce the secretion of type 1 interferons and proinflammatory cytokines). TIRAP and TRAM are intermediate molecules that recruit TRIF to TLR4 and MyD88 to TLR2 and TLR4, respectively.20,22,24 In one study, the signalling cascade in
three bladder cancer cell lines (5637, T24, and A498) was shown to be similar to that in macrophages.31
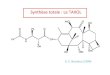
TLRs in normal urothelial cellsThe asymmetric unit membrane on the luminal side of superficial urothelial cells (umbrella cells) constitutes the first barrier against bladder infection by uropathogens. Umbrella cells form a monolayer of highly differentiated and polarized cells linked by tight junctions. Their apical membrane is detergent insoluble and forms a character-istic scalloped aspect comprising plaques and hinges. The major plaque proteins are uroplakins.32 The imper-meability of these umbrella cells and the glycan layer that covers them prevents the adherence of b acteria and the frequent flow of urine helps to dislodge any b acteria that do adhere, making urothelium one of the most diffi cult mucosal surfaces for pathogens to colonize. In addition to this mechanical barrier, pathogens encoun-ter a highly effective immune response in which TLRs, mainly TLR4, TLR5, and Tlr11 (in mice only), have a major role (Figure 1).33 TLR activation leads to the pro-duction of inflammatory mediators such as cytokines, chemokines, and bactericidal peptides that help to clear infections. The relative rarity of UTI (given the proxim-ity of the urinary tract to the gastrointestinal tract) and the fact that urine is a rich medium for bacterial growth attests to the efficacy of these defence mechanisms.32,33 We analysed TLR protein expression (by immunohisto-chemistry) in tissue from 11 normal human bladders and TLR RNA expression in four primary cultures of normal urothelial cells obtained from organ donors, and observed that normal urothelium expressed TLR5 weakly, TLR2, TLR3, and TLR7 moderately, and TLR4 and TLR9 strongly.19 Primary cultures expressed RNA from all TLRs except TLR7, TLR8, and TLR10 (Figure 2).
TLR4TLR4 recognizes lipopolysaccharides from Gram-negative bacteria (Table 1). Its high expression in uro thelial cells most likely reflects the fact that Escherichia coli is a common uropathogen (responsible for up to 85% of UTI).33,34 Urothelial expression of TLR4 was reported in C3H/HeJ mice and susceptibility to UTI was shown to depend on the lipopolysaccharide responsive ness of different mouse strains, later ascribed to the presence of a wild-type or mutant Tlr4 gene.35–37 Studies of mice with different genetic backgrounds (with normal or defective Tlr4) have, however, suggested that susceptibility to uropathogenic E. coli (UPEC) infec-tions does not solely depend on Tlr4 and that other genes are involved. Although such genes have not been positively identified, proposed candidates include Tlr11 and Tlr12.38 The presence of an aspartic acid to glycine mutation in the human TLR4 protein has been associ-ated with an increased risk of Gram-negative infections, including UTI.39,40 Reduced TLR4 expression in neutro-phils has also been associated with asymptomatic UTI in children.41
The first step in the infection of a mucosal surface is bacterial adhesion. The ability of UPEC to infect
Key points
■ Toll‑like receptors (TLRs) are transmembrane proteins present in immune cells and some epithelial cells, which initiate an immune response upon activation by microbial pathogens or danger signals
■ TLRs are expressed and active in normal bladder epithelial cells, where they contribute to resistance against infection by uropathogens
■ Expression of TLRs is maintained, although slightly reduced, in non‑muscle‑invasive bladder cancer cells compared with normal bladder epithelial cells
■ TLR agonists can be used to activate TLR pathways and some have been used successfully to treat various diseases, including some cancers (for example, basal cell carcinomas)
■ TLR agonists have been tested for their ability to treat bladder cancer in vitro and in vivo using animal models, with promising results
■ Some TLR agonists, such as mycobacterial cell wall DNA complexes and imiquimod, have been tested in clinical trials on patients with bladder cancer
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved

NATURE REVIEWS | UROLOGY ADVANCE ONLINE PUBLICATION | 3
urothelial cells is dependent on fimbrial adhesins and cell surface receptors. For example, the P fimbria adhesin protein recognizes glycolipids that are abundant on kidney cells.42 Type 1 fimbriated UPEC, on the other hand, recognize mannose-containing glycoproteins—such as uroplakin-1a, which are highly expressed in the luminal membrane of umbrella cells—and infect uro thelial cells.31,42–44 Upon binding to uroplakin-1a, a signifi cant number of UPEC are internalized into bladder cells. If lipopolysaccharide molecules are involved, the immune response is triggered as soon as contact is made with TLR4. Co-receptors include the extracellular accessory molecule MD-245 and the membrane-bound CD14, which is essential for the effi-cient presentation of lipopolysaccharide to TLR4 and for inducing the expression of proinflammatory cyto-kines.31,46 Type 1 fimbriated UPEC activate TLR4 signal-ling via MyD88, whereas P fimbriated UPEC induce signalling via TRIF.43 An alternative pathway—m ediated by cyclic adenosine monophosphate (cAMP) and its associated transcriptional factor, the cAMP-response-element-binding protein—has been described for TLR4 activation in urothelial cells.33,35,47,48 Activation of this pathway results in faster production of interleukin-6 and interleukin-8, which might protect cells from gastro-intestinal tract contaminants.35,48 The cAMP pathway is active in urothelial cells, cell lines, and primary cul-tures.48 TLR4 also mediates the expulsion of UPEC from infected cells by inducing the apoptosis and shedding of umbrella cells32 and by promoting exocytosis, which is a cAMP-dependent process.33,47
TLR2TLR2 recognizes bacterial components such as lipo-proteins in Gram-positive bacteria and in mycoplasma and mycobacteria (Table 1).46,49,50 The TLR2_G2258A polymorphism has been associated with an increased risk of asymptomatic bacteriuria in a cohort of 1,261 asymptomatic women, supporting a protective role for TLR2 against UTI.51
TLR5 and TLR11TLR5 is also thought to participate in the fight against UTI, by binding to a highly conserved structure of bacteri al flagellin (Table 1).52,53 Tlr5-/- mice are more susceptible to UPEC than wild-type mice54 and pres-ence of the TLR5_C1174T polymorphism—which pre-vents flagellin- induced signalling—was associated with an increased risk of recurrent UTI in a cohort of 987 women.55 In another study, flagellin induced interleukin-6 and interleukin- 8 secretion in proliferating normal cul-tured human urothelial cells that showed neither lipopoly-saccharide binding nor response to lipopolysaccharide, suggesting that the host response to UPEC depends upon the detection of flagellin by TLR5.56 Finally, Tlr11, which is related to Tlr5, is highly expressed in mouse bladder and kidney and thought to have a role in the detection of uropathogenic bacteria as Tlr11-deficient mice are highly susceptible to UTI.22,57 However, the human TLR11 gene is nonfunctional owing to the presence of a stop codon.20
Table 1 | TLRs and some of their ligands20,21,23,24,44,59,68
Natural ligand Organism Synthetic ligand
TLR1/2
Triacyl lipopeptides Gram‑negative bacteria; mycobacteria
Triacyl lipopeptides
TLR2
Lipoproteins; peptidoglycans; lipoteichoic acid; porins; lipoarabinomannan
Gram‑positive bacteria; mycobacteria; mycoplasma
Diacyl and triacyl lipopeptides
Phospholipomannans and glucuronoxyl mannans; zymosan; β‑glucans
Fungi NR
tGPI‑mutin Parasites NR
Haemagglutinin and structural proteins
Viruses NR
HSP70 Human NR
TLR3
dsRNA (produced during replication of ssRNA)
Viruses Poly(I:C); poly(I:C12U)
Certain siRNAs Reoviruses Poly(I:C); poly(I:C12U)
Genomic RNA Reoviruses Poly(I:C); poly(I:C12U)
TLR4
Lipopolysaccharides Gram‑negative bacteria Lipid A mimetics
Mannanes Fungi NR
Structural proteins Viruses NR
Glycoinositol phospholipids Parasites (Trypanosoma) NR
HMGB1; HSP; ECM components (with TLR2)
Human (dying or injured cells)
NR
TLR5
Flagellin Flagellated bacteria Discontinuous 13‑amino acid peptide CBLB502
TLR6/2
Diacyl lipopeptides; lipoteichoic acid
Gram‑positive bacteria; mycoplasma; group B streptococcus
Diacyl lipopeptides
Zymosan Fungus NR
TLR7
ssRNA RNA viruses Imidazoquinoline derivatives; guanine analogues
siRNA Bacteria Poly(U)RNA
Self DNA/LL37; self RNA/LL37 Human NR
TLR8
ssRNA RNA viruses Imidazoquinolines (resiquimod)
TLR9
Nonmethylated CpG DNA Bacteria and mycobacteria CpG ODNs
Haemozoin Plasmodium CpG ODNs
DNA Viruses; parasites CpG ODNs
Self DNA/LL37; self RNA/LL37; self DNA/HMGB1
Human CpG ODNs
TLR11 (mouse)
Profilin‑like molecule Uropathogenic bacteria NR
Profilin‑like molecule Toxoplasma gondii NR
Abbreviations: dsRNA, double‑stranded RNA; ECM, extracellular matrix; HMGB1, high‑mobility group protein B1; HSP, heat shock protein; NR, not reported; ODN, oligodeoxynucleotides; siRNA, small interfering RNAs; ssRNA, single‑stranded RNA; TLR, toll‑like receptor.
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved

4 | ADVANCE ONLINE PUBLICATION www.nature.com/nrurol
TLRs in bladder cancerTLR expression has been reported in several cancers, including lung,58 colorectal,59 and ovarian cancers,60 renal cell carcinomas,61 and melanomas.62 Their role in the regu lation of the immune response enables them to contri bute in the fight against cancer cells. However, several studies have suggested that the production of cytokines and chemokines associated with TLR acti-vation might also contribute to cancer cell survival, angiogenesis, progression, and chemoresistance.50,63 Moreover, NF-κB translocates to the nucleus following TLR activation, targets genes involved in cell prolifera-tion and survival (as well as immune response genes), and is considered to be a tumour promoter.23 In addi-tion, MyD88 was shown to promote tumorigenesis in a mouse model of intestinal adenoma23 and single nucleo-tide polymorphisms in TLR genes or in genes of the TLR pathways have been associated with increased cancer risk.23,64 TLRs are, therefore, poised to have a dual role in tumour biology.50,65
An association has also been demonstrated between presence of bladder cancer and polymorphisms in both TLR2 and TLR4.66,67 We observed a clear decrease in the expression of six TLRs (TLR2, TLR3, TLR4, TLR5, TLR7, and TLR9) in bladder tumours relative to normal uro thelium using immunohistochemistry.19 NMIBCs retained a significant level of TLR expression, with
TLR4 and TLR9 remaining the most strongly expressed, whereas a marked decrease in expression was observed in muscle-invasive bladder cancers. We observed mRNA expression of all 10 TLRs in 15 bladder cancer cell lines; TLR6 and TLR9 were the most frequently expressed and TLR7 and TLR10 were the least frequently expressed (Figure 2). Responses of bladder cancer cell lines to TLR agonists, as measured by the secretion of proinflamma-tory cytokines, showed a predominance of TLR2 and TLR3 responses (similar to that observed with normal cultured urothelial cells).19 MGH-U3, a low-grade bladder cancer cell line that mimics the features of a grade I NMIBC when grown as a xenograft in immuno-deficient mice,68 responded to TLR2, TLR3, TLR5, TLR7, and TLR9 agonists. RT4, another low-grade bladder cancer cell line, responded only to zymosan and flagel-lin (TLR2 and TLR5 agonists, respectively). Only T24, a high-grade bladder cancer cell line, responded to lipo-polysaccharide,19 which supports the reported expression of both TLR4 and CD14 in this cell line.46,69
In one study, the level of interleukin-8 response in four bladder cancer cell lines upon stimulation with lipopoly-saccharide or peptidoglycan was shown to be related to the presence of membrane-anchored CD14.46 The investigators concluded that this membrane protein is a determinant in the inflammatory response to TLR4 and TLR2 agonists in urothelial cells. In RT4 cells, treatment
Antimicrobial peptides and pro-in�ammatory cytokine production Pro-in�ammatory cytokine production
Capsule Flagellin LPS
CD14
Diacylpeptides
Triacylpeptides
Type 1�mbriated
E. coli
Mycobacterial cell wallglycolipids
Diacyl and triacyl peptides
CD14
LPS and othermycobacterialcomponents
Mycobacterium bovis (BCG)
UnmethylatedDNA
MyD88
NF-κB
MyD88
NF-κB
cAMP
CREB
TLR9
a bUropathogen (bacteria)
TLR 1-2 TLR 2-6 TLR4/CD14/MD-2 TLR5
MD-2 MD-2
Figure 1 | Simplified representation of the TLR response to uropathogens and to BCG in the human bladder. a | TLR2, TLR4, and TLR5 are mainly involved in the response to UTI by bacteria. TLR2 recognizes bacterial components such as lipoproteins. Lipopolysaccharides are presented to TLR4 by CD14. Type 1 fimbriated E.coli are recognized by TLR4 in a CD14‑independent manner in urothelial cells. A conserved structure of flagellin is recognized by TLR5. All these ligands initiate a MyD88‑dependent TLR response, leading to proinflammatory cytokine production. The TLR4 response to lipopolysaccharides will also initiate a TRIF‑dependent response. An alternative pathway, mediated by cAMP and leading to transcriptional activation of TLR4 by the cAMP‑response‑element‑binding protein, has also been described in urothelial cells. b | TLR2, TLR4, and TLR9 cooperate in the response to BCG. Mycobacterial lipoproteins and glycolipids are TLR2 ligands. Lipopolysaccharides are the key activators of TLR4, although other mycobacterial components are also presumed to activate TLR4 in urothelial cells. Unmethylated mycobacterial DNA is a TLR9 ligand. Abbreviations: cAMP, cyclic adenosine monophosphate; LPS, lipopolysaccharide; TLR, toll‑like receptor; TRIF, TIR‑domain‑containing adaptor protein inducing IFNβ.
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved

NATURE REVIEWS | UROLOGY ADVANCE ONLINE PUBLICATION | 5
with a combination of interferon-� and lipopolysaccha-� and lipopolysaccha- and lipopolysaccha-rides was necessary to upregulate TLR4 expression and trigger the secretion of macrophage-derived chemokines and interferon-inducible protein-10.70 Another research group demonstrated constitutive expression of TLR4 and CD14 in T24 cells and established that TLR4 acti-vation by lipopolysaccharides upregulated expression of i nterleukin-6 via activation of p38 and ERK kinases.71 This research team also showed that TLR4 activation upregulated expression of B7-H1 (PD-L1) via activa-tion of the mitogen-activated protein kinases ERK and JNK, suggesting a possible mechanism of tumour evasion through inhibition of T-cell immunity.69
TLRs in bladder cancer immunotherapyAlthough TLR activation in tumour cells can trigger both antitumour and protumour responses, many studies have shown a direct cytotoxicity of TLR agonists on bladder cancer cell lines and an antitumour effect in vivo.72–74 Although TLRs are more heavily expressed in normal urothelial cells, their expression and activity persist in tumour cells, offering the possibility of using TLR ligands for therapy. The success of TLR-mediated BCG immuno-therapy for NMIBCs suggests that alternative TLR-based immunotherapies might also be successful for these cancers (Table 2).
TLR-mediated BCG immunotherapyRecent guidelines suggest that all patients with an inter-mediate or high risk of recurrence or progression, based on tumour characteristics, should receive a minimum of 12 months of BCG therapy.1 BCG is an attenuated form of Mycobacterium bovis with preserved b acterial immuno genicity. Intravesical instillation of BCG induces an immune response against mycobacterial antigens and possibly also against tumour antigens. The immune response observed against BCG is similar to that gener-ated upon mycobacterial infection. Adhesion of BCG to the urothelium induces the secretion of proinflam-matory cytokines, which triggers an influx of immune cells through the urothelium, starting with polymorpho-nuclear neutrophils (PMNs). PMNs are followed by monocytes and macrophages, which produce chemo-attractants that induce an influx of lymphocytes and a cytokine shift to a predominantly T helper type-1 (Th1)-like milieu. Clinical data have shown that the establish-ment of a Th1 cytokine profile is crucial to the success of the antitumour response.10,11,13,75–82
Cell response to mycobacteria has been shown to depend on TLR signalling (Figure 1b). For example, MyD88-deficient mice demonstrate reduced resistance to M. tuberculosis compared with wild-type controls,83 whereas the uroepithelial cell line Hu35E6E7 (which expresses many TLRs) induces expression of MyD88 in the presence of BCG.16 Unmethylated mycobacterial DNA acts as a TLR9 ligand (owing to the recognition of unmethylated CpG motifs) whereas mycobacterial lipoproteins are TLR2 ligands.84 Polymorphisms of both TLR2 and TLR9 have been associated with susceptibility to M. tuberculosis in humans.85 TLR4 is also involved in
the response to mycobacteria and an in vitro study on human epithelial cells showed that BCG induced acti-vation of the ERK1/2 MAPK pathway and secretion of interleukin-8 via both TLR2 and TLR4 signalling.17
TLR2-deficient mice are sensitive to BCG infection (at a dose of 1 × 106 colony-forming units [CFU] given via intraperitoneal [i.p.] inoculation), whereas TLR4-deficient mice resist BCG infection, but show increased inflammation. TLR4–/– mice showed defective immunity at higher BCG doses (1 × 107 CFU i.p.).86 In vitro experi-ments have shown that macrophages from TLR2–/– mice failed to secrete proinflammatory cytokines in response to BCG, although BCG uptake and intra cellular growth were similar in TLR2–/–, TLR4–/–, and wild-type mice, suggesting a defective adaptive immunity in TLR2–/– mice but a dependency on TLR2 for cytokine-inducing activity upon BCG treatment.86 When taken together, these data suggest that distinct roles exist for TLR2 and TLR4 in the development of host immunity to BCG. TLR4 signal ling is probably not essential for the early control of BCG infection, but is required for the development of a Th1 response.86,87
TLR1
TLR2
TLR3
TLR4
TLR5
TLR6
TLR7
TLR8
TLR9
TLR10
β-actin
Pos
Ctrl
Cultu
re 1
Cultu
re 4
Cultu
re 3
Cultu
re 2
Neg
Ctrl
MGH
U3M
GHU4
VMCU
B-3
VMCU
B-1
JON
SW78
0SW
1710
SW80
0
RT4
253J
575A
639V
J82
T24
5637
Neg
Ctrl
Primary cultures ofnormal bladder cells Bladder cancer cell lines
Figure 2 | Reverse transcriptase PCR analysis of TLR mRNA expression in four short‑term primary cultures of normal human urothelial cells and 15 bladder cancer cell lines. MGH‑U4 was derived from atypia, MGH‑U3, RT4, SW780, and SW800 were derived from grade I tumours, VMCUB‑1 and 5637 were derived from grade 2 tumours, VMCUB‑3, 575A, 639V and T24 were derived from grade III tumours, 253J was derived from a lymph node, JON was derived from an adenocarcinoma, and J82 originated from a squamous cell carcinoma. Abbreviations: Neg Ctrl, negative control (no RNA); Pos Ctrl, positive control (blood RNA); TLR, toll‑like receptor.
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved

6 | ADVANCE ONLINE PUBLICATION www.nature.com/nrurol
TNF-related-apoptosis-inducing ligand (TRAIL) is released from PMNs via stimulation of TLR2 by BCG and components of the mycobacterial cell wall.18 Secretion of interleukin-8, a strong chemoattractant for monocytes and T-cells, is also induced from PMNs by BCG infection via MyD88-dependent TLR2 and TLR4 activation,88 whereas BCG activation of TLR2 and TLR4 induces TNF-� secre-� secre- secre-tion from dendritic cells and maturation of these cells.15 Although TLR9 CpG ligands have been identified in mycobacterial DNA, the role of TLR9 in response to BCG is unclear. To identify TLRs involved in the response to BCG, one research team infected bone-marrow-derived macrophages and dendritic cells from TLR-knockout mice with BCG.89 The highest decrease in the inflammatory response was observed in TLR2–/– cells, but the maximal reduction in interleukin-12 secretion was observed in cells from TLR2/4/9-deficient mice. Moreover, upregula-tion of CD86—one of the co-stimulatory membrane pro-teins that is essential for T-cell activation—was abolished only in dendritic cells from these mice, confirming the c ontribution of TLR9 to the response to BCG.
Alternate TLR-mediated immunotherapiesAlthough BCG is effective, the use of live bacteria pres-ents a risk of infection. Moreover, treatment fails in some patients and is sometimes difficult to tolerate. The major role of the TLRs in the response to BCG clearly sup-ports the investigation of other TLR agonists for bladder cancer treatment (Table 2). Many TLR agonists have been tested as therapeutic agents.72,73
Bacterial componentsBCG cell wall skeleton (CWS) or purified proteoglycan from BCG CWS can activate TLR signalling as effectively as whole BCG.15,90–93 Viability, apoptosis, and bromo-deoxyuridine incorporation were measured for three bladder cancer cell lines treated with BCG, heat-killed BCG, and BCG CWS. All three treatments produced the same level of growth retardation, supporting the use of BCG-CWS as an alternative to BCG for the treatment of bladder cancer.91 BCG-CWS was shown to provide ligands for TLR2 and TLR4.94 Other promising agents for intravesical immunotherapy are M. phlei myco-bacterial cell wall DNA complexes (MCC),95–98 which are complexes of mycobacterial DNA oligonucleotides with components of the cell wall. Intravesical use of MCC was tested in patients with bladder carcinoma in situ, some
of whom had failed BCG therapy.98 MCC showed anti-neoplastic activity, with reduced toxicity compared with BCG. Mycobacterial DNA was proposed to be the active ingredient in MCC.96
CpG oligodeoxynucleotidesBacterial DNA, including DNA from mycobacteria, con-tains many unmethylated CpG motifs, which are mostly absent from human DNA (as CpGs are generally methyl-ated). CpGs are recognized as a PAMP by TLR999,100 and, as such, have been tested as BCG surrogates in the treat-ment of bladder cancer. One group of researchers treated cultured dendritic cells obtained from murine bone marrow with both BCG and CpG-rich oligodeoxynucleo-tides (ODNs).101 BCG stimulation resulted in the produc-tion of unfocused proinflammatory cytokines; increased levels of interleukin-12 and interleukin-10 represented Th1 and Th2 responses, respectively. CpG-ODN stimu-lation of dendritic cells, on the other hand, resulted in a focused Th1 response with production of interleukin-12 alone, suggesting the superiority of CpG over BCG with respect to eliciting an immune response. Many studies have shown reduced tumour growth of both subcutane-ous and orthotopic tumours in the MB49 mouse bladder cancer model upon treatment with CpG-ODN.102–106 Subsequent rechallenge of CpG-ODN-cured mice with MB49 cells has shown that these mice acquire tumour-specific immunity.103 MB49 cells do not express TLR9. Thus, the observed immunological responses seem to be mediated by immune cells, with no direct effect of tumour cells.106 Combining CpG treatment with anti bodies against cytotoxic T lymphocyte antigen-4 (CTLA4) or programmed death receptor-1 (PD1) further increased survival relative to treatment with either agent alone.107
Helicobacter pylori neutrophil-activating proteinAs TLR2 is involved in the response to BCG, TLR2 ligands have potential roles in immunotherapy. The Helicobacter pylori neutrophil-activating protein (HPNAP) is a TLR2 ligand that induces an inter leukin-12-enriched milieu that drives a Th1 response. In MB49 mice, local administration of HPNAP decreased tumour growth by inducing tumour necrosis and a signifi cant accumu lation of CD4+ and CD8+ IFN-�-secreting cells in a TLR2-dependent process.108
Poly(I:C) and synthetic small moleculesWe have reported the expression of many TLRs in normal urothelium and non-muscle-invasive bladder tumours. In addition, we have demonstrated the functionality of TLR2 and TLR3 in normal cultured urothelial cells and in bladder cancer cell lines, suggesting potential roles of TLR2 and TLR3 agonists in antitumour immuno therapy for non-muscle-invasive bladder cancers.19 TLR3 is involved in the defence response against viral infections by recognizing double-stranded RNA (dsRNA) and can be mimicked by synthetic poly(I:C) dsRNA. We have shown that poly(I:C) dsRNA can induce the secretion of proinflammatory cytokines by normal and cancerous cultured urothelial cells.19
Table 2 | Proposed ligands for TLR‑mediated immunotherapy for bladder cancer
Ligand TLRs Clinical phase
BCG1,10,11 TLR2; TLR4; TLR9 Standard of care
BCG CWS (SM‑105)15,89–92 TLR2; TLR4 Preclinical
MCC94–97 TLR9 Phase III
CpG ODNs98–105 TLR9 Preclinical
HP‑NAP106 TLR2 Preclinical
Imiquimod (R‑837; TMX‑101; TMX‑202)108–112 TLR7 Phase II
Abbreviations: CWS, cell wall skeleton; HP‑NAP, Helicobacter pylori neutrophil‑activating‑protein; MCC, mycobacterial cell‑wall DNA complexes; ODN, oligodeoxynucleotides; TLR, toll‑like receptor.
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved

NATURE REVIEWS | UROLOGY ADVANCE ONLINE PUBLICATION | 7
TLR7 and TLR8 are involved in virus recognition and the natural ligands of these receptors are single-stranded RNAs. TLR7 also recognizes poly(U)RNA and certain small interfering RNAs.22 TLR7 and TLR8 can also be activated by synthetic small molecules such as imidazoquinolines and nucleoside analogues (Table 1).72 Aldara™—a topical formulation of imiqui-mod (an imidazo quinoline)— has been approved for the treatment of basal cell carcinoma by the FDA and the European Medicines Agency.72 Imiquimod decreased cell viability and induced apoptosis and cytokine pro-duction in bladder cancer cell lines.109 It also drasti-cally reduced tumour growth and produced an intense inflammatory response in the bladder wall in an ortho-topic murine model of bladder cancer.109 Another group found that orthotopic tumour loads were significantly reduced follow ing intravesical instillation of imiquimod (R-837) in MB49 mice compared with vehicle-treated or untreated mice. The investigators observed substantial infiltration of mononuclear cells in the lamina propria after three R-837 instillations.110 R-837 and the more-specific TLR7 agonist TMX-202 also demonstrated antitumour activity without toxicity in an orthotopic rat bladder cancer model.111 TMX-101, a liquid form of imiquimod, was shown to be safe for intravesical use in a group of 16 patients with NMIBCs112 and is now being tested in a phase II study of patients with carcinoma in situ bladder cancers.113
LipopolysaccharidesLipopolysaccharide and their derivatives are potent TLR4 agonists and antitumour agents, but their use is limited by high levels of associated toxicity.114,115 However, one research group showed increased antitumour activity by treating murine MBT-2 bladder cancer cells with a combination of fragmented E.coli DNA and modified lipopolysaccharide (devoid of lipid A) compared with either agent alone or BCG.115 However, this detoxified
lipopolysaccharide has probably lost its ability to act as a TLR4 agonist and bacterial DNA is likely to be the active ingredient in the complex.
ConclusionsThe data reported herein clearly attest to the importance of TLR proteins in urinary bladder immunity. These pro-teins have a major role in the remarkable resistance of urothelium to infections. Moreover, TLR2, TLR4, and TLR9 are involved in the immune response to BCG in patients with bladder cancer. The success of that immuno therapy indicates the potential of TLR-mediated therapies for preventing recurrence of NMIBCs. Many TLR agonists have been considered as candidates for bladder cancer immunotherapy, with a particular focus on TLR7 agonists (imiquimod, TMX-101, and TMX-202), which have been tested in clinical trials of patients with bladder cancer. Mycobacterial cell wall DNA complex has shown antineoplastic activity in patients with bladder carcinoma in situ. CpG-ODN (a TLR9 agonist) has been shown to be superior to BCG in the MB49 murine model of bladder cancer, whereas administration of HP-NAP (a TLR2 agonist) decreased tumour growth in the same animal model. Finally, we have shown that poly(I:C), a TLR3 agonist, can elicit an immune response in uro thelial cells. Undoubtedly, bladder cancer care will benefit from the intensive research that is currently underway into TLR agonists that can complement or replace BCG.
Review criteria
The PubMed database was searched using the terms “toll‑like receptors”, “TLR”, “bladder”, “bladder cancer”, “bladder infection”, “urinary tract infection”, “cancer”, “immunotherapy”, “BCG”, “MCC”, and “imiquimod”, to retrieve articles published in the English language from 1980 to 2013. The reference lists of some articles were also reviewed to retrieve additional pertinent articles.
1. Babjuk, M. et al. EAU guidelines on non‑muscle‑invasive urothelial carcinoma of the bladder, the 2011 update. Eur. Urol. 59, 997–1008 (2011).
2. Jemal, A. et al. Cancer statistics, 2008. CA Cancer J. Clin. 58, 71–96 (2008).
3. van Rhijn, B. W. et al. Recurrence and progression of disease in non‑muscle‑invasive bladder cancer: from epidemiology to treatment strategy. Eur. Urol. 56, 430–442 (2009).
4. Brausi, M. et al. A review of current guidelines and best practice recommendations for the management of nonmuscle invasive bladder cancer by the International Bladder Cancer Group. J. Urol. 186, 2158–2167 (2011).
5. Feifer, A. H., Taylor, J. M., Tarin, T. V. & Herr, H. W. Maximizing cure for muscle‑invasive bladder cancer: integration of surgery and chemotherapy. Eur. Urol. 59, 978–984 (2011).
6. van den Bosch, S. & Alfred, W. J. Long‑term cancer‑specific survival in patients with high‑risk, non‑muscle‑invasive bladder cancer and tumour progression: a systematic review. Eur. Urol. 60, 493–500 (2011).
7. Botteman, M. F., Pashos, C. L., Redaelli, A., Laskin, B. & Hauser, R. The health economics of
bladder cancer: a comprehensive review of the published literature. Pharmacoeconomics 21, 1315–1330 (2003).
8. Herr, H. W. et al. Intravesical bacillus Calmette‑Guerin therapy prevents tumour progression and death from superficial bladder cancer: ten‑year follow‑up of a prospective randomized trial. J. Clin. Oncol. 13, 1404–1408 (1995).
9. Malmstrom, P. U. et al. An individual patient data meta‑analysis of the long‑term outcome of randomised studies comparing intravesical mitomycin C versus bacillus Calmette‑Guerin for non‑muscle‑invasive bladder cancer. Eur. Urol. 56, 247–256 (2009).
10. Kresowik, T. P. & Griffith, T. S. Bacillus Calmette‑Guerin immunotherapy for urothelial carcinoma of the bladder. Immunotherapy 1, 281–288 (2009).
11. Brandau, S. & Suttmann, H. Thirty years of BCG immunotherapy for non‑muscle invasive bladder cancer: a success story with room for improvement. Biomed. Pharmacother. 61, 299–305 (2007).
12. Birder, L. A. Urinary bladder urothelium: molecular sensors of chemical/thermal/mechanical stimuli. Vascul. Pharmacol. 45, 221–226 (2006).
13. Bevers, R. F., Kurth, K. H. & Schamhart, D. H. Role of urothelial cells in BCG immunotherapy for superficial bladder cancer. Br. J. Cancer 91, 607–612 (2004).
14. Lattime, E. C., Gomella, L. G. & McCue, P. A. Murine bladder carcinoma cells present antigen to BCG‑specific CD4+ T‑ cells. Cancer Res. 52, 4286–4290 (1992).
15. Tsuji, S. et al. Maturation of human dendritic cells by cell wall skeleton of Mycobacterium bovis bacillus Calmette‑Guerin: involvement of toll‑like receptors. Infect. Immun. 68, 6883–6890 (2000).
16. Miyazaki, J. et al. Uroepithelial cells can directly respond to Mycobacterium bovis bacillus Calmette‑Guerin through Toll‑like receptor signalling. BJU Int. 97, 860–864 (2006).
17. Mendez‑Samperio, P., Belmont, L. & Miranda, E. Mycobacterium bovis BCG Toll‑like receptors 2 and 4 cooperation increases the innate epithelial immune response. Arch. Med. Res. 39, 33–39 (2008).
18. Simons, M. P., O’Donnell, M. A. & Griffith, T. S. Role of neutrophils in BCG immunotherapy for bladder cancer. Urol. Oncol. 26, 341–345 (2008).
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved

8 | ADVANCE ONLINE PUBLICATION www.nature.com/nrurol
19. Ayari, C., Bergeron, A., LaRue, H., Menard, C. & Fradet, Y. Toll‑like receptors in normal and malignant human bladders. J. Urol. 185, 1915–1921 (2011).
20. Akira, S., Uematsu, S. & Takeuchi, O. Pathogen recognition and innate immunity. Cell 124, 783–801 (2006).
21. Zhang, Z. & Schluesener, H. J. Mammalian toll‑like receptors: from endogenous ligands to tissue regeneration. Cell Mol. Life Sci. 63, 2901–2907 (2006).
22. Kawai, T. & Akira, S. The role of pattern‑recognition receptors in innate immunity: update on Toll‑like receptors. Nat. Immunol. 11, 373–384 (2010).
23. Li, X., Jiang, S. & Tapping, R. I. Toll‑like receptor signalling in cell proliferation and survival. Cytokine 49, 1–9 (2010).
24. Kawai, T. & Akira, S. Toll‑like receptors and their crosstalk with other innate receptors in infection and immunity. Immunity 34, 637–650 (2011).
25. Trinchieri, G. Interleukin‑12 and the regulation of innate resistance and adaptive immunity. Nat. Rev. Immunol. 3, 133–146 (2003).
26. Yamamoto, M. & Takeda, K. Current views of toll‑like receptor signalling pathways. Gastroenterol. Res. Pract. 240, 365 (2010).
27. Zahringer, U., Lindner, B., Inamura, S., Heine, H. & Alexander, C. TLR2 ‑ promiscuous or specific? A critical re‑evaluation of a receptor apparent broad specificity. Immunobiology 213, 205–224 (2008).
28. Hashimoto, M. et al. Not lipoteichoic acid but lipoproteins appear to be the dominant immunobiologically active compounds in Staphylococcus aureus. J. Immunol. 177, 3162–3169 (2006).
29. Tsan, M. F. & Gao, B. Pathogen‑associated molecular pattern contamination as putative endogenous ligands of Toll‑like receptors. J. Endotoxin. Res. 13, 6–14 (2007).
30. Travassos, L. H. et al. Toll‑like receptor 2‑dependent bacterial sensing does not occur via peptidoglycan recognition. EMBO Rep. 5, 1000–1006 (2004).
31. Schilling, J. D. et al. CD14‑ and toll‑like receptor‑dependent activation of bladder epithelial cell by lipopolysaccharide and type 1 piliated Escherichia coli. Infect. Immun. 71, 1470–1480 (2003).
32. Khandelwal, P., Abraham, S. N. & Apodaca, G. Cell biology and physiology of the uroepithelium. Am. J. Physiol. Renal Physiol. 297, F1477–F1501 (2009).
33. Song, J. & Abraham, S. N. TLR‑mediated immune responses in the urinary tract. Curr. Opin. Microbiol. 11, 66–73 (2008).
34. Hooton, T. M. & Stamm, W. E. Diagnosis and treatment of uncomplicated urinary tract infection. Infect. Dis. Clin. North Am. 11, 551–581 (1997).
35. Song, J., Bishop, B. L., Li, G., Duncan, M. J. & Abraham, S. N. TLR4‑initiated and cAMP‑mediated abrogation of bacterial invasion of the bladder. Cell Host. Microbe 1, 287–298 (2007).
36. Hagberg, L. et al. Difference in susceptibility to gram‑negative urinary tract infection between C3H/HeJ and C3H/HeN mice. Infect. Immun. 46, 839–844 (1984).
37. Shahin, R. D., Engberg, I., Hagberg, L. & Svanborg, E. C. Neutrophil recruitment and bacterial clearance correlated with LPS responsiveness in local gram‑negative infection. J. Immunol. 138, 3475–3480 (1987).
38. Suhs, K. A., Marthaler, B. R., Welch, R. A. & Hopkins, W. J. Lack of association between the Tlr4 (Lpsd/Lpsd) genotype and increased susceptibility to Escherichia coli bladder
infections in female C3H/HeJ mice. MBio. 2, e00094–e00111 (2011).
39. Agnese, D. M. et al. Human toll‑like receptor 4 mutations but not CD14 polymorphisms are associated with an increased risk of gram‑negative infections. J. Infect. Dis. 186, 1522–1525 (2002).
40. Karoly, E. et al. Heat shock protein 72 (HSPA1B) gene polymorphism and Toll‑like receptor (TLR) 4 mutation are associated with increased risk of urinary tract infection in children. Paediatr. Res. 61, 371–374 (2007).
41. Ragnarsdottir, B. et al. Reduced toll‑like receptor 4 expression in children with asymptomatic bacteriuria. J. Infect. Dis. 196, 475–484 (2007).
42. Godaly, G. & Svanborg, C. Urinary tract infections revisited. Kidney Int. 71, 721–723 (2007).
43. Fischer, H., Yamamoto, M., Akira, S., Beutler, B. & Svanborg, C. Mechanism of pathogen‑specific TLR4 activation in the mucosa: fimbriae, recognition receptors and adaptor protein selection. Eur. J. Immunol. 36, 267–277 (2006).
44. Svanborg, C. et al. Uropathogenic Escherichia coli as a model of host‑parasite interaction. Curr. Opin. Microbiol. 9, 33–39 (2006).
45. Nagai, Y. et al. Essential role of MD‑2 in LPS responsiveness and TLR4 distribution. Nat. Immunol. 3, 667–672 (2002).
46. Shimizu, T. et al. Membrane‑anchored CD14 is important for induction of interleukin‑8 by lipopolysaccharide and peptidoglycan in uroepithelial cells. Clin. Diagn. Lab. Immunol. 11, 969–976 (2004).
47. Song, J. & Abraham, S. N. Innate and adaptive immune responses in the urinary tract. Eur. J. Clin. Invest. 38 (Suppl. 2), 21–28 (2008).
48. Song, J. et al. A novel TLR4‑mediated signalling pathway leading to IL‑6 responses in human bladder epithelial cells. PLoS Pathog. 3, e60 (2007).
49. Ozinsky, A. et al. The repertoire for pattern recognition of pathogens by the innate immune system is defined by cooperation between toll‑like receptors. Proc. Natl Acad. Sci. USA 97, 13766–13771 (2000).
50. Basith, S., Manavalan, B., Yoo, T. H., Kim, S. G. & Choi, S. Roles of toll‑like receptors in cancer: a double‑edged sword for defence and offense. Arch. Pharm. Res. 35, 1297–1316 (2012).
51. Hawn, T. R. et al. Genetic variation of the human urinary tract innate immune response and asymptomatic bacteriuria in women. PLoS ONE 4, e8300 (2009).
52. Hayashi, F. et al. The innate immune response to bacterial flagellin is mediated by Toll‑like receptor 5. Nature 410, 1099–1103 (2001).
53. Smith, K. D. et al. Toll‑like receptor 5 recognizes a conserved site on flagellin required for protofilament formation and bacterial motility. Nat. Immunol. 4, 1247–1253 (2003).
54. Andersen‑Nissen, E. et al. Cutting edge: Tlr5‑/‑ mice are more susceptible to Escherichia coli urinary tract infection. J. Immunol. 178, 4717–4720 (2007).
55. Hawn, T. R. et al. Toll‑like receptor polymorphisms and susceptibility to urinary tract infections in adult women. PLoS ONE 4, e5990 (2009).
56. Smith, N. J. et al. Toll‑like receptor responses of normal human urothelial cells to bacterial flagellin and lipopolysaccharide. J. Urol. 186, 1084–1092 (2011).
57. Zhang, D. et al. A toll‑like receptor that prevents infection by uropathogenic bacteria. Science 303, 1522–1526 (2004).
58. Pinto, A., Morello, S. & Sorrentino, R. Lung cancer and Toll‑like receptors. Cancer Immunol. Immunother. 60, 1211–1220 (2011).
59. Niedzielska, I. et al. Toll‑like receptors and the tendency of normal mucous membrane to transform to polyp or colorectal cancer. J. Physiol. Pharmacol. 60 (Suppl. 1), 65–71 (2009).
60. Zhou, M. et al. Toll‑like receptor expression in normal ovary and ovarian tumours. Cancer Immunol. Immunother. 58, 1375–1385 (2009).
61. Morikawa, T. et al. Identification of Toll‑like receptor 3 as a potential therapeutic target in clear cell renal cell carcinoma. Clin. Cancer Res. 13, 5703–5709 (2007).
62. Salaun, B., Lebecque, S., Matikainen, S., Rimoldi, D. & Romero, P. Toll‑like receptor 3 expressed by melanoma cells as a target for therapy? Clin. Cancer Res. 13, 4565–4574 (2007).
63. Chen, R., Alvero, A. B., Silasi, D. A., Steffensen, K. D. & Mor, G. Cancers take their Toll‑‑the function and regulation of Toll‑like receptors in cancer cells. Oncogene 27, 225–233 (2008).
64. Kutikhin, A. G. Association of polymorphisms in TLR genes and in genes of the Toll‑like receptor signalling pathway with cancer risk. Hum. Immunol. 72, 1095–1116 (2011).
65. Huang, B., Zhao, J., Unkeless, J. C., Feng, Z. H. & Xiong, H. TLR signalling by tumour and immune cells: a double‑edged sword. Oncogene 27, 218–224 (2008).
66. Shen, Y., Liu, Y., Liu, S. & Zhang, A. Toll‑like receptor 4 gene polymorphisms and susceptibility to bladder cancer. Pathol. Oncol. Res. 19, 275–280 (2012).
67. Singh, V., Srivastava, N., Kapoor, R. & Mittal, R. D. Single‑nucleotide polymorphisms in genes encoding Toll‑like receptor ‑2, ‑3, ‑4, and ‑9 in a case‑control study with bladder cancer susceptibility in a North Indian population. Arch. Med. Res. 44, 54–61 (2013).
68. LaRue, H., Parent‑Vaugeois, C., Bergeron, A., Champetier, S. & Fradet, Y. Influence of spatial configuration on the expression of carcinoembryonic antigen and mucin antigens in human bladder cancer. Int. J. Cancer 71, 986–992 (1997).
69. Qian, Y. et al. TLR4 signalling induces B7‑H1 expression through MAPK pathways in bladder cancer cells. Cancer Invest. 26, 816–821 (2008).
70. Yamada, H., Odonnell, M. A., Matsumoto, T. & Luo, Y. Interferon‑gamma upregulates toll‑like receptor 4 and cooperates with lipopolysaccharide to produce macrophage‑derived chemokine and interferon‑gamma inducible protein‑10 in human bladder cancer cell line RT4. J. Urol. 174, 1119–1123 (2005).
71. Qian, Y. et al. Regulation of TLR4‑induced IL‑6 response in bladder cancer cells by opposing actions of MAPK and PI3K signalling. J. Cancer Res. Clin. Oncol. 135, 379–386 (2009).
72. Goutagny, N., Estornes, Y., Hasan, U., Lebecque, S. & Caux, C. Targeting pattern recognition receptors in cancer immunotherapy. Target. Oncol. 7, 29–54 (2012).
73. Hennessy, E. J., Parker, A. E. & O’Neill, L. A. Targeting Toll‑like receptors: emerging therapeutics? Nat. Rev. Drug Discov. 9, 293–307 (2010).
74. So, E. Y. & Ouchi, T. The application of Toll like receptors for cancer therapy. Int. J. Biol. Sci. 6, 675–681 (2010).
75. Kavoussi, L. R., Brown, E. J., Ritchey, J. K. & Ratliff, T. L. Fibronectin‑mediated Calmette‑Guerin bacillus attachment to murine bladder mucosa. Requirement for the expression of an antitumour response. J. Clin. Invest 85, 62–67 (1990).
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved

NATURE REVIEWS | UROLOGY ADVANCE ONLINE PUBLICATION | 9
76. Hudson, M. A., Brown, E. J., Ritchey, J. K. & Ratliff, T. L. Modulation of fibronectin‑mediated Bacillus Calmette‑Guerin attachment to murine bladder mucosa by drugs influencing the coagulation pathways. Cancer Res. 51, 3726–3732 (1991).
77. De Reijke, T. M. et al. Cytokine production by the human bladder carcinoma cell line T24 in the presence of bacillus Calmette‑Guerin (BCG). Urol. Res. 21, 349–352 (1993).
78. Esuvaranathan, K. et al. Interleukin‑6 production by bladder tumours is upregulated by BCG immunotherapy. J. Urol. 154, 572–575 (1995).
79. Bohle, A. & Brandau, S. Immune mechanisms in bacillus Calmette‑Guerin immunotherapy for superficial bladder cancer. J. Urol. 170, 964–969 (2003).
80. Suttmann, H. et al. Neutrophil granulocytes are required for effective Bacillus Calmette‑Guerin immunotherapy of bladder cancer and orchestrate local immune responses. Cancer Res. 66, 8250–8257 (2006).
81. Suttmann, H., Lehan, N., Bohle, A. & Brandau, S. Stimulation of neutrophil granulocytes with Mycobacterium bovis bacillus Calmette‑Guerin induces changes in phenotype and gene expression and inhibits spontaneous apoptosis. Infect. Immun. 71, 4647–4656 (2003).
82. Bohle, A., Gerdes, J., Ulmer, A. J., Hofstetter, A. G. & Flad, H. D. Effects of local bacillus Calmette‑Guerin therapy in patients with bladder carcinoma on immunocompetent cells of the bladder wall. J. Urol. 144, 53–58 (1990).
83. Scanga, C. A. et al. MyD88‑deficient mice display a profound loss in resistance to Mycobacterium tuberculosis associated with partially impaired Th1 cytokine and nitric oxide synthase 2 expression. Infect. Immun. 72, 2400–2404 (2004).
84. Simmons, D. P. et al. Mycobacterium tuberculosis and TLR2 agonists inhibit induction of type I IFN and class I MHC antigen cross processing by TLR9. J. Immunol. 185, 2405–2415 (2010).
85. Huynh, K. K., Joshi, S. A. & Brown, E. J. A delicate dance: host response to mycobacteria. Curr. Opin. Immunol. 23, 464–472 (2011).
86. Heldwein, K. A. et al. TLR2 and TLR4 serve distinct roles in the host immune response against Mycobacterium bovis BCG. J. Leukoc. Biol. 74, 277–286 (2003).
87. Fremond, C. M., Nicolle, D. M., Torres, D. S. & Quesniaux, V. F. Control of Mycobacterium bovis BCG infection with increased inflammation in TLR4‑deficient mice. Microbes Infect. 5, 1070–1081 (2003).
88. Godaly, G. & Young, D. B. Mycobacterium bovis bacille Calmette Guerin infection of human neutrophils induces CXCL8 secretion by MyD88‑dependent TLR2 and TLR4 activation. Cell Microbiol. 7, 591–601 (2005).
89. von Meyenn, F. et al. Toll‑like receptor 9 contributes to recognition of Mycobacterium bovis Bacillus Calmette‑Guerin by Flt3‑ligand
generated dendritic cells. Immunobiology 211, 557–565 (2006).
90. Uehori, J. et al. Simultaneous blocking of human Toll‑like receptors 2 and 4 suppresses myeloid dendritic cell activation induced by Mycobacterium bovis bacillus Calmette‑Guerin peptidoglycan. Infect. Immun. 71, 4238–4249 (2003).
91. Kato, T. et al. Bacillus Calmette‑Guerin and BCG cell wall skeleton suppressed viability of bladder cancer cells in vitro. Anticancer Res. 30, 4089–4096 (2010).
92. Murata, M. Activation of Toll‑like receptor 2 by a novel preparation of cell wall skeleton from Mycobacterium bovis BCG Tokyo (SMP‑105) sufficiently enhances immune responses against tumours. Cancer Sci. 99, 1435–1440 (2008).
93. Uenishi, Y., Kawabe, K., Nomura, T., Nakai, M. & Sunagawa, M. Morphological study on Mycobacterium bovis BCG Tokyo 172 cell wall skeleton (SMP‑105). J. Microbiol. Methods 77, 139–144 (2009).
94. Akazawa, T. et al. Adjuvant engineering for cancer immunotherapy: Development of a synthetic TLR2 ligand with increased cell adhesion. Cancer Sci. 101, 1596–1603 (2010).
95. Filion, M. C., Lepicier, P., Morales, A. & Phillips, N. C. Mycobacterium phlei cell wall complex directly induces apoptosis in human bladder cancer cells. Br. J. Cancer 79, 229–235 (1999).
96. Filion, M. C. & Phillips, N. C. Therapeutic potential of mycobacterial cell wall‑DNA complexes. Expert Opin. Investig. Drugs 10, 2157–2165 (2001).
97. Morales, A. Evolution of intravesical immunotherapy for bladder cancer: mycobacterial cell wall preparation as a promising agent. Expert Opin. Investig. Drugs 17, 1067–1073 (2008).
98. Morales, A., Phadke, K. & Steinhoff, G. Intravesical mycobacterial cell wall‑DNA complex in the treatment of carcinoma in situ of the bladder after standard intravesical therapy has failed. J. Urol. 181, 1040–1045 (2009).
99. Takeshita, F. et al. Cutting edge: Role of Toll‑like receptor 9 in CpG DNA‑induced activation of human cells. J. Immunol. 167, 3555–3558 (2001).
100. Haemmi, H. et al. A Toll‑like receptor recognizes bacterial DNA. Nature 408, 740–745 (2000).
101. Atkins, H., Davies, B. R., Kirby, J. A. & Kelly, J. D. Polarisation of a T‑helper cell immune response by activation of dendritic cells with CpG‑containing oligonucleotides: a potential therapeutic regime for bladder cancer immunotherapy. Br. J. Cancer 89, 2312–2319 (2003).
102. Ninalga, C., Loskog, A., Klevenfeldt, M., Essand, M. & Totterman, T. H. CpG oligonucleotide therapy cures subcutaneous and orthotopic tumours and evokes protective immunity in murine bladder cancer. J. Immunother. 28, 20–27 (2005).
103. Mangsbo, S. M., Ninalga, C., Essand, M., Loskog, A. & Totterman, T. H. CpG therapy is superior to BCG in an orthotopic bladder cancer model and generates CD4+ T‑cell immunity. J. Immunother. 31, 34–42 (2008).
104. Hegele, A. et al. Antineoplastic effect of immunostimulatory DNA (CpG‑ODN) in a murine C57‑BL6/MB‑49 transitional cell carcinoma model. Anticancer Res. 24, 2225–2230 (2004).
105. Hegele, A. et al. Immunostimulatory CpG oligonucleotides reduce tumour burden after intravesical administration in an orthotopic murine bladder cancer model. Tumour Biol. 26, 274–280 (2005).
106. Olbert, P. J. et al. In vitro and in vivo effects of CpG‑Oligodeoxynucleotides (CpG‑ODN) on murine transitional cell carcinoma and on the native murine urinary bladder wall. Anticancer Res. 29, 2067–2076 (2009).
107. Mangsbo, S. M. et al. Enhanced tumour eradication by combining CTLA‑4 or PD‑1 blockade with CpG therapy. J. Immunother. 33, 225–235 (2010).
108. Codolo, G. et al. HP‑NAP inhibits the growth of bladder cancer in mice by activating a cytotoxic Th1 response. Cancer Immunol. Immunother. 61, 31–40 (2012).
109. Smith, E. B. et al. Antitumour effects of imidazoquinolines in urothelial cell carcinoma of the bladder. J. Urol. 177, 2347–2351 (2007).
110. Hayashi, T. et al. Intravesical Toll‑like receptor 7 agonist R‑837: optimization of its formulation in an orthotopic mouse model of bladder cancer. Int. J. Urol. 17, 483–490 (2010).
111. Falke, J. et al. A preclinical placebo controlled efficacy study with R‑837 and TMX‑202 in an orthotopic rat bladder cancer model. Eur. Urol. 10, 80 (2011).
112. Falke, J. et al. Results of a phase 1 dose escalation study of intravesical TMX‑101 in patients with non‑muscle invasive bladder cancer. J. Urol. 19, 275–280 (2012).
113. US National Library of Medicine. ClinicalTrials.gov [online], http://clinicaltrials.gov/ct2/show/ NCT01731652?term=bladder+cancer+tmx‑ 101&rank=1 (2013).
114. de Bono, J. S. et al. Phase I study of ONO‑4007, a synthetic analogue of the lipid A moiety of bacterial lipopolysaccharide. Clin. Cancer Res. 6, 397–405 (2000).
115. Cho, Y. J., Ahn, B. Y., Lee, N. G., Lee, D. H. & Kim, D. S. A combination of E. coli DNA fragments and modified lipopolysaccharides as a cancer immunotherapy. Vaccine 24, 5862–5871 (2006).
116. Vacchelli, E. et al. Trial watch: FDA‑approved Toll‑like receptor agonists for cancer therapy. Onco-immunology 1, 894–907 (2012).
Author contributionsH. LaRue, C. Ayari, and A. Bergeron researched, wrote, edited, and discussed this Review article. Y. Fradet made substantial contributions towards discussions of contents and reviewed the manuscript before submission.
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved