Embed Size (px)
DESCRIPTION
Autologous pBSC transplantation for refractory or relapsed DBLCL Report of the « CNGMO, Tunis». 9 ème Congrès Magrébin d’Hématologie Dr Torjemane L 25/05/2012. Introduction. - PowerPoint PPT Presentation
Citation preview
AUTOLOGOUS PBSC TRANSPLANTATION FOR
REFRACTORY OR RELAPSED DBLCL REPORT OF THE « CNGMO, TUNIS»
9ème Congrès Magrébin d’Hématologie Dr Torjemane L
25/05/2012
Introduction • High dose chemotherapy (HDC) followed by
autologous peripheral stem cell transplantation (APSCT) is indicated in case of relapsed or refractory NHL.
• From June 2000 to December 2011, a total of 28 autologous PSCT were performed at the « CNGMO » for DLCBCL in second line
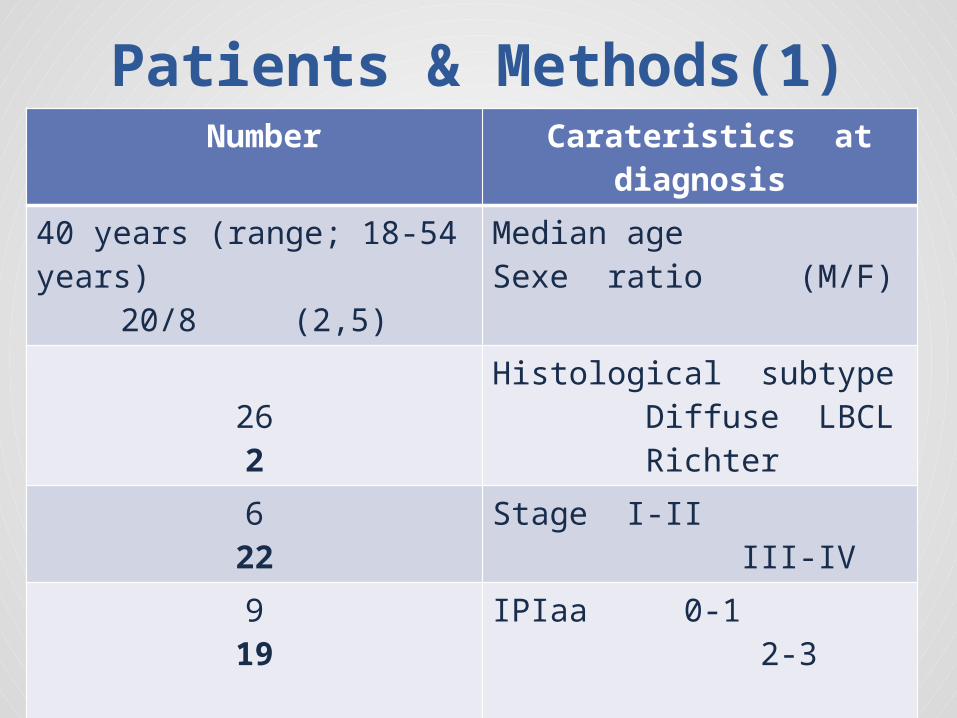
Patients & Methods(1)Number Carateristics at
diagnosis40 years (range; 18-54 years)
20/8 (2,5)
Median ageSexe ratio (M/F)
262
Histological subtype Diffuse LBCL Richter
622
Stage I-II III-IV
919
IPIaa 0-1 2-3
123
Bulky diseaseBM involvement
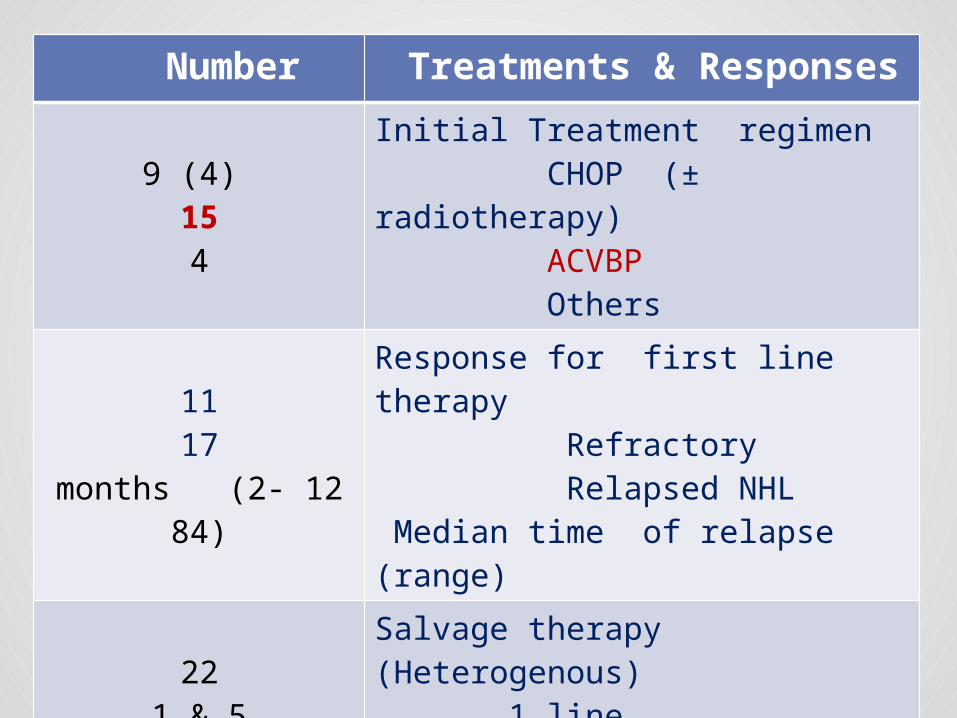
Number Treatments & Responses
9 (4) 154
Initial Treatment regimen CHOP (± radiotherapy) ACVBP Others
1117
12 months (2-84)
Response for first line therapy Refractory Relapsed NHL Median time of relapse (range)
225 &1
18 2
Salvage therapy (Heterogenous) 1 line 2 to 3 lines + Rituximab + Radiotherapy
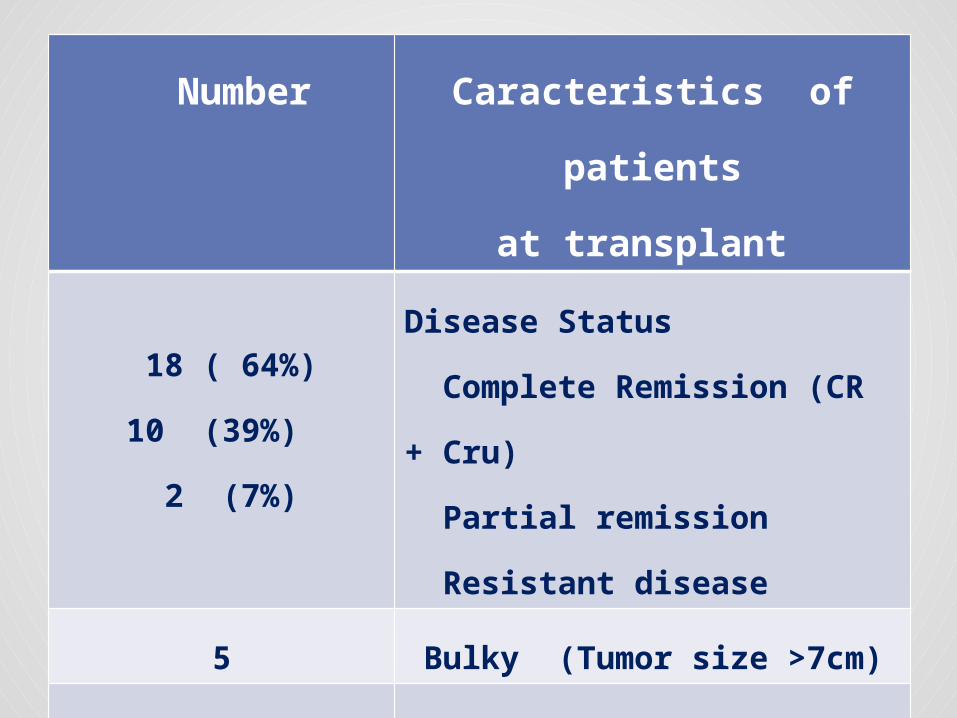
Number Caracteristics of
patients
at transplant
18 ( 64%)
10 (39%)
2 (7%)
Disease Status
Complete Remission (CR
+ Cru)
Partial remission
Resistant disease
5 Bulky (Tumor size >7cm)
34 days (21-120)
21 months (5-
122)
Median time, (range)
Last chemotherapy –
ASCT
Diagnosis- ASCT
Transplant procedure• Conditioning regimen consisted in BEAM
regimen (BICNU, Etoposid, Cytarabin, Melphalan)
• Adjustment of dose of Melphalan (50%) to renal function: 2 patients
• PBSC : 6,03 x106 CD34+/kg (range; 1,44- 13 x106).
(PBSC + Bone marrow : 2 patients)
Results Hematopoietic
Engraftment • The medians numbers of days to reach:
-Granulocytes > 500/mm3: 10 days ( range:
9 - 35)
- Platelets ≥ 20 000/mm3: 15 days
( range; 12- 62)
• Transfusion Requirements
- RBC : 4 Units (range: 0- 19)
- PCA: 6 Units (range: 2- 19)
Transplant-related toxicity
o Stomatitis grade 3-4: 85%
o Infectious complication: 100%
- A median of 2 febrile neutropenia (range;1-4)
- Pneumonia : n= 6, Abdominal pain
- Septicemia (19%) : Gram + (n=6)
Gram- (n=4)
, Candida parapsilosis
(n=2)
Transplant-related toxicity
o Renal toxicity (grade 1-2): n= 6 (21%)
o Hepatic toxicity/VOD : n=1 (3,5%)
o Cytomegalovirus Infections: n=4 (14%)
o Treatment related Mortality: n=2 (7%)
( Interstitiel Pneumonia + Septic choc)
Therapeutic results • At 3 months after Transplants:
- Complete Remission : 15/26 ( 58%)
- Partial Remission: 8/26 (30%)
- Resistant disease: 3/26 (12 %)
• Complementary radiotherapy (2 resistant diseases)
:
- 1 Complete Remission / negative TEP scanner
- 1 Stable Partial Remission
Therapeutic results • Relapse rate: 10/26 (38%)
• Median delai of relapse: 6 months (range; 3- 20)
• After a median time of follow-up of 24 months, (range : 8- 120 months) 16 ( 57%) patients were alive and well.
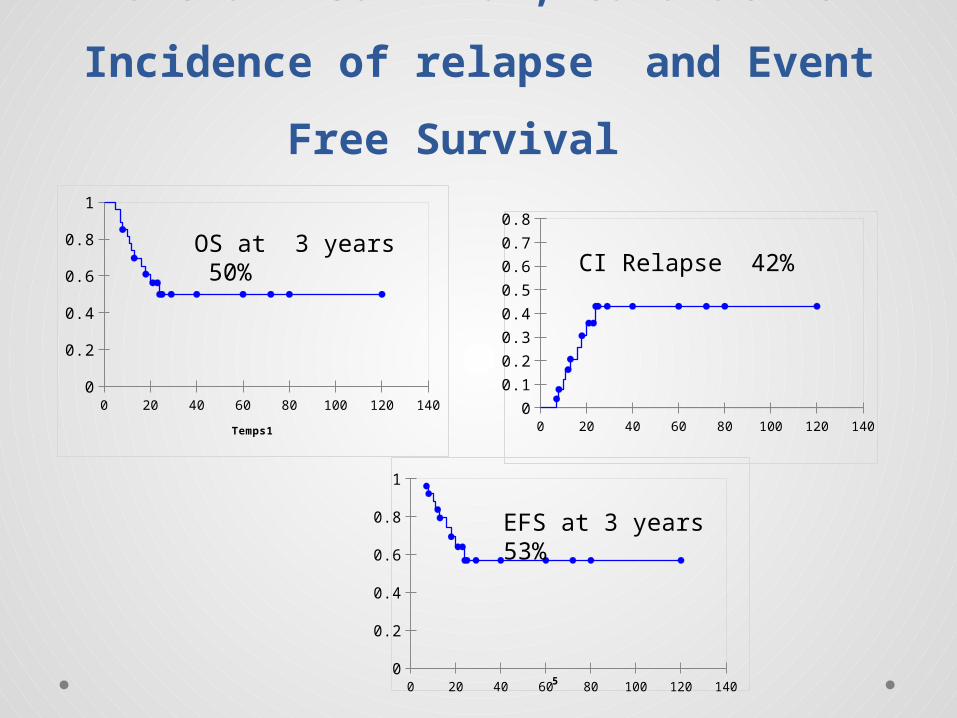
Overall survival, Cumulative
Incidence of relapse and Event
Free Survival
0 20 40 60 80 100 120 1400
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0 20 40 60 80 100 120 1400
0.10.20.30.40.50.60.70.80.9
1
5
0 20 40 60 80 100 120 1400
0.2
0.4
0.6
0.8
1
Temps1
OS at 3 years 50% CI Relapse 42%
EFS at 3 years 53%
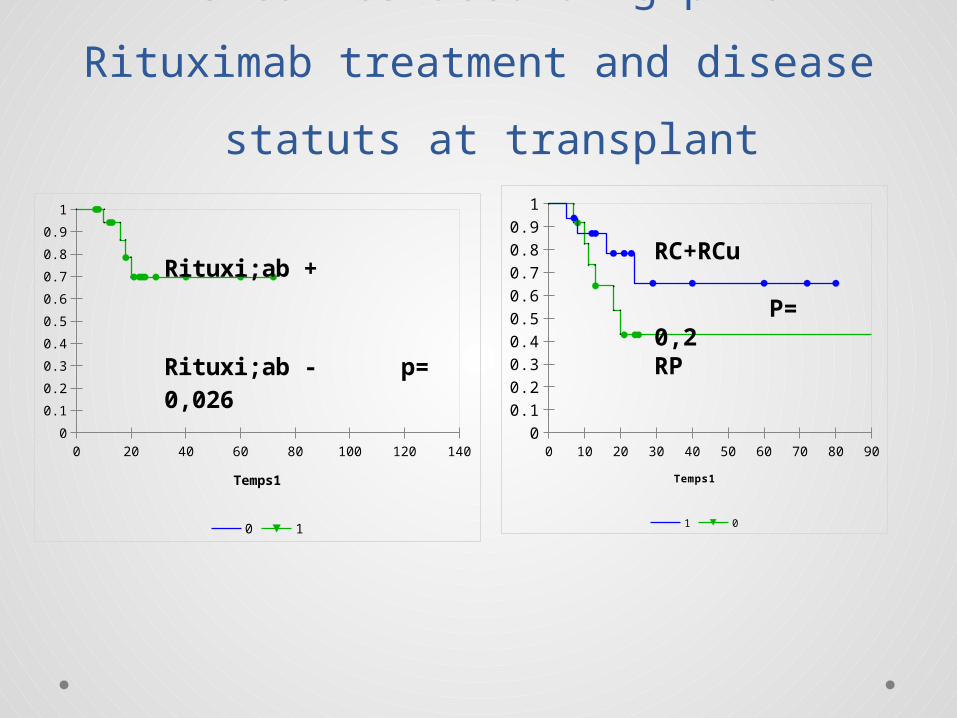
EFS curves according prior Rituximab
treatment and disease statuts at
transplant
0 20 40 60 80 100 120 1400
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 1
Temps1
Rituxi;ab +
Rituxi;ab - p= 0,026
0 10 20 30 40 50 60 70 80 900
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
1 0
Temps1
RC+RCu
P= 0,2RP
Conclusion • The present results demonstrate the
efficacy and moderate toxicity of the HDC followed by autologous stem cell support in refractory or relapsed high-risk DLBCL
• Addition of Rituximab significantly reduce the risk of relapse.
• Equipe d’Hhématologie de l’Hôpital Hédi Chaker, Sfax• Equipe de Carcinologie Médicale de l’hôpital Hédi Chaker, Sfax• Equipe d’Hématologie de l’hôpital Farhat Hached, Sousse• Equipe de Carcinologie Médicale de l’hôpital Farhat Hached,
Sousse• Equipe d’Hématologie de l’Hôpital de Monastir• Equipe d’Hématologie de l’Hôpital Aziza Othmana, Tunis• Equipe d’Hématologie de l’Hôpital Militaire de Tunis • Equipe de Carcinologie Médicale de l’Institut Salah Azaiez de
Tunis • Médecins Hématologues et Oncologues du Privé (Tunis,
Sousse, Sfax)
THANKS





























