Embed Size (px)
Citation preview
Antithrombotiques
• Antiagrégants plaquettaires
• Anticoagulants
Les Antiagrégants Plaquettaires
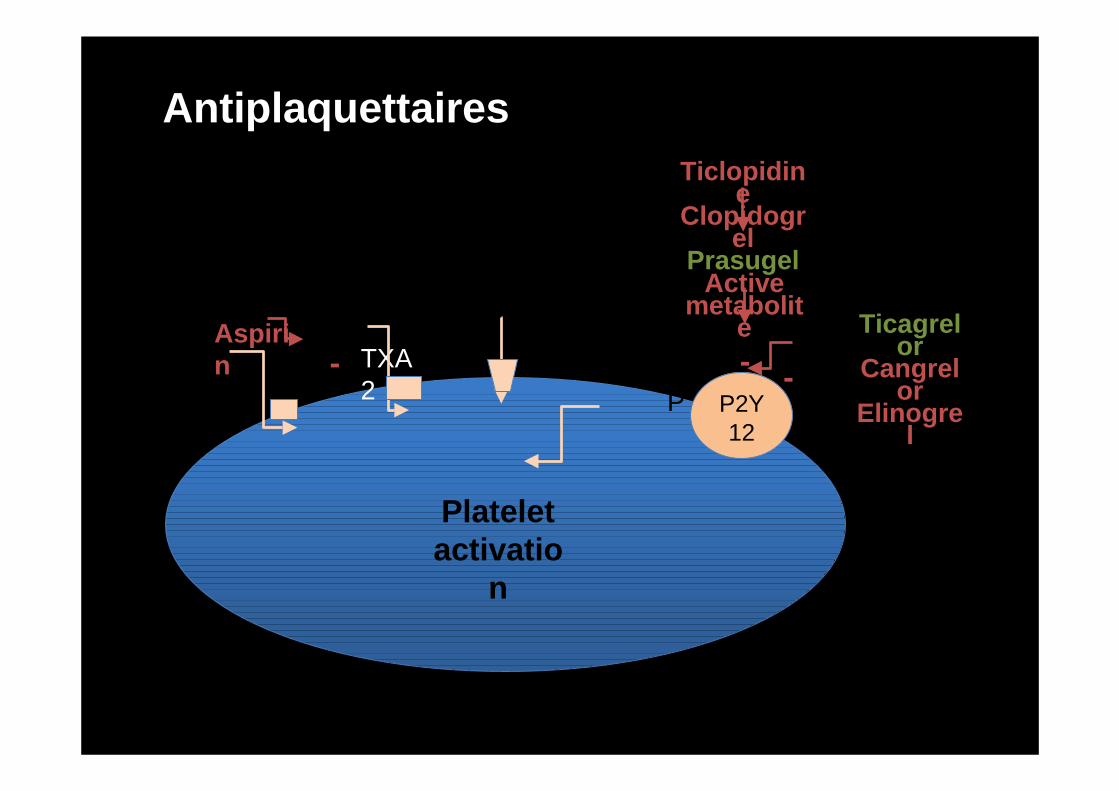
P2Y12
Plateletactivatio
n
TXA2
Aspirin -
Ticlopidine
Clopidogrel
Prasugel
-ADP
Antiplaquettaires
Activemetabolit
e
-
Ticagrelor
Cangrelor
Elinogrel
Les indications
• Toutes les localisations de l’athérosclérose
– Maladie coronaire stable– Syndrome coronarien aigu (SCA) (infarctus –
angor instable)– Angioplastie coronaire percutanée– Artériopathie– AVC/AIT (si Absence indication à
l’anticoagulation)
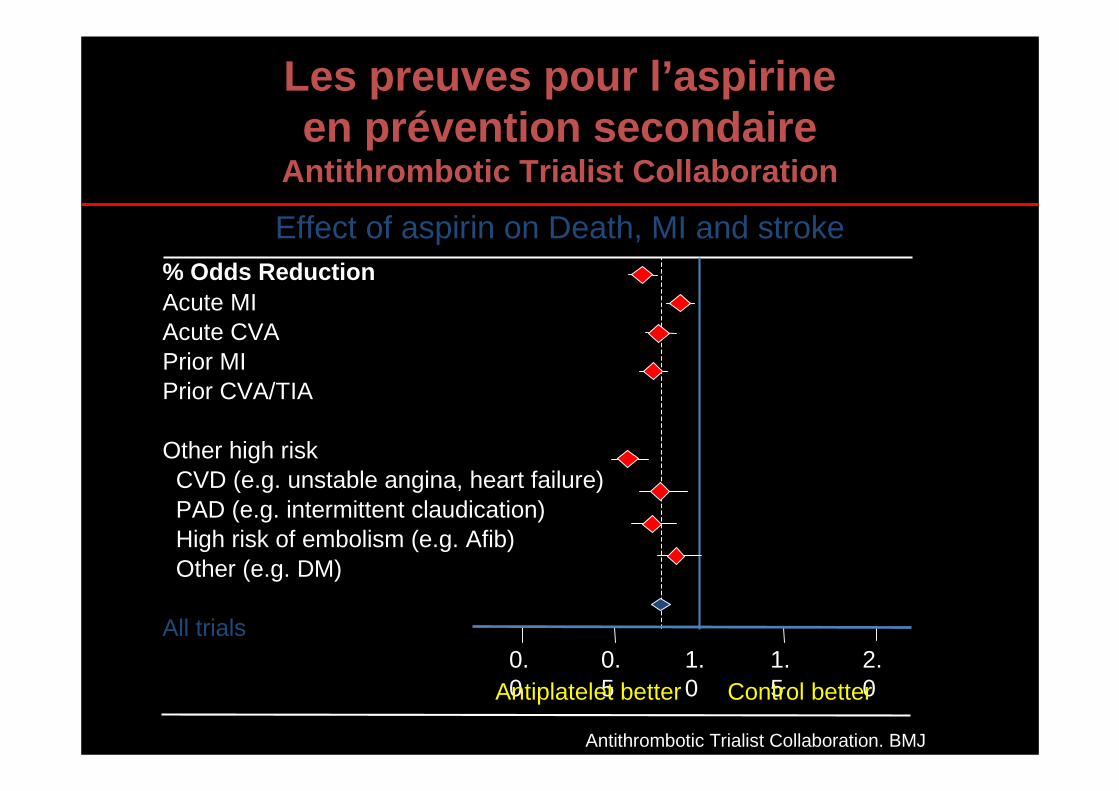
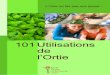
Les preuves pour l’aspirine en prévention secondaire
Antithrombotic Trialist Collaboration
Antithrombotic Trialist Collaboration. BMJ2002;324:71–86
% Odds ReductionAcute MIAcute CVA Prior MIPrior CVA/TIA
Other high riskCVD (e.g. unstable angina, heart failure)PAD (e.g. intermittent claudication)High risk of embolism (e.g. Afib)Other (e.g. DM)
All trials1.0
0.5
0.0
1.5
2.0Control betterAntiplatelet better
Effect of aspirin on Death, MI and stroke
Les associations d’AAP
• Indication des associations de plusieurs antiagrégants plaquettaires
– SCA pendant 1 an avec ou sans angioplastie coronaire
– Angioplastie coronaire percutanée pendant 1 mois à 1 an selon les cas
• Aspirine plus un des Inhibiteurs du récepteur P2Y12 à l’ADP
Aucune indication à ce jour à associer
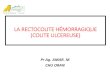
Clopidogrel + ASA*
3 6 9
Placebo + ASA*
Months of Follow-Up
11.4%
9.3%
0 12
* In combination with standard therapy
Primary End Point - MI/Stroke/CV-DeathCURE
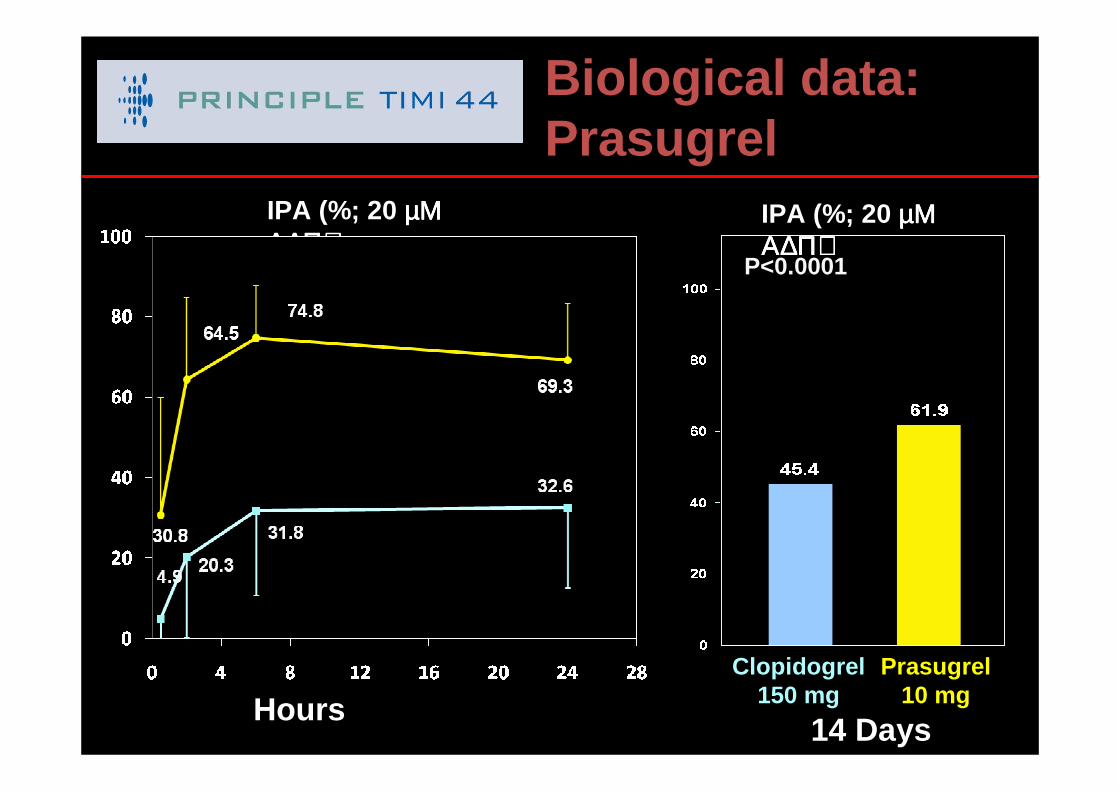
Biological data: Prasugrel
14 Days
IPA (%; 20 µΜ µΜ µΜ µΜ Α∆Π)Α∆Π)Α∆Π)Α∆Π)
P<0.0001
Prasugrel 10 mg
Clopidogrel 150 mg
IPA (%; 20 µΜ µΜ µΜ µΜ Α∆Π)Α∆Π)Α∆Π)Α∆Π)
Hours
P<0.0001 for eachn=201
Prasugrel 60 mg
Clopidogrel 600 mg
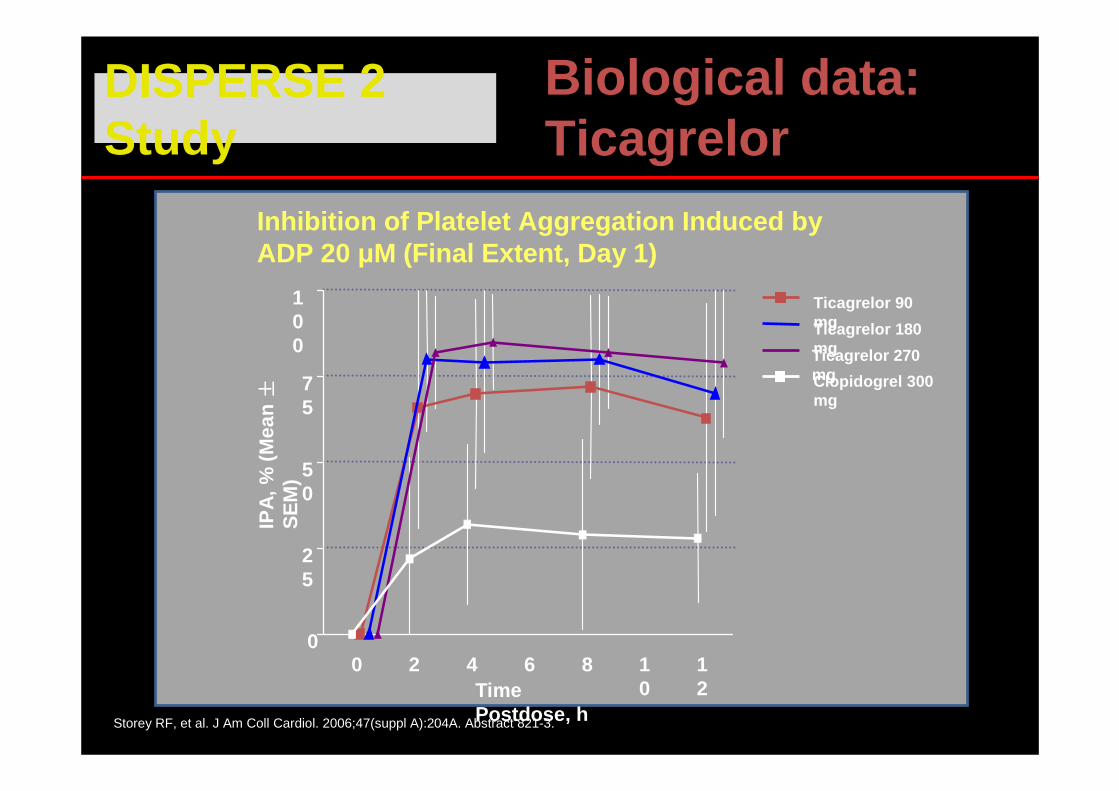
DISPERSE 2 Study
Storey RF, et al. J Am Coll Cardiol. 2006;47(suppl A):204A. Abstract 821-3.
Inhibition of Platelet Aggregation Induced by ADP 20 µM (Final Extent, Day 1)
Ticagrelor 90 mgTicagrelor 180 mgTicagrelor 270 mgClopidogrel 300 mg
0 2 4 6 8 10
12
0
25
50
75
100
Time Postdose, h
IPA
, % (
Mea
n ±± ±±
SE
M)
Biological data: Ticagrelor
0
5
10
15
0 30
60
90
180
270
360
450
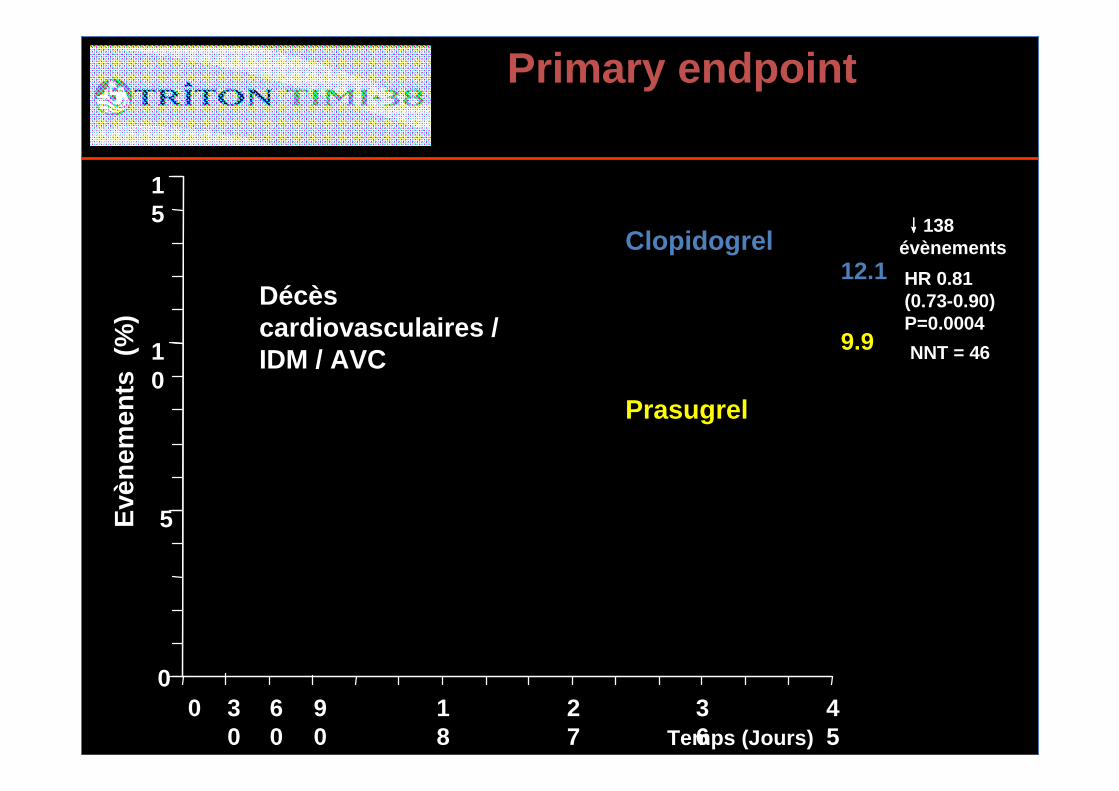
HR 0.81(0.73-0.90)P=0.0004
Prasugrel
Clopidogrel
Temps (Jours)
Evè
nem
ents
(%
)
12.1
9.9
↓↓↓↓138évènements
Primary endpoint
Décès cardiovasculaires / IDM / AVC NNT = 46
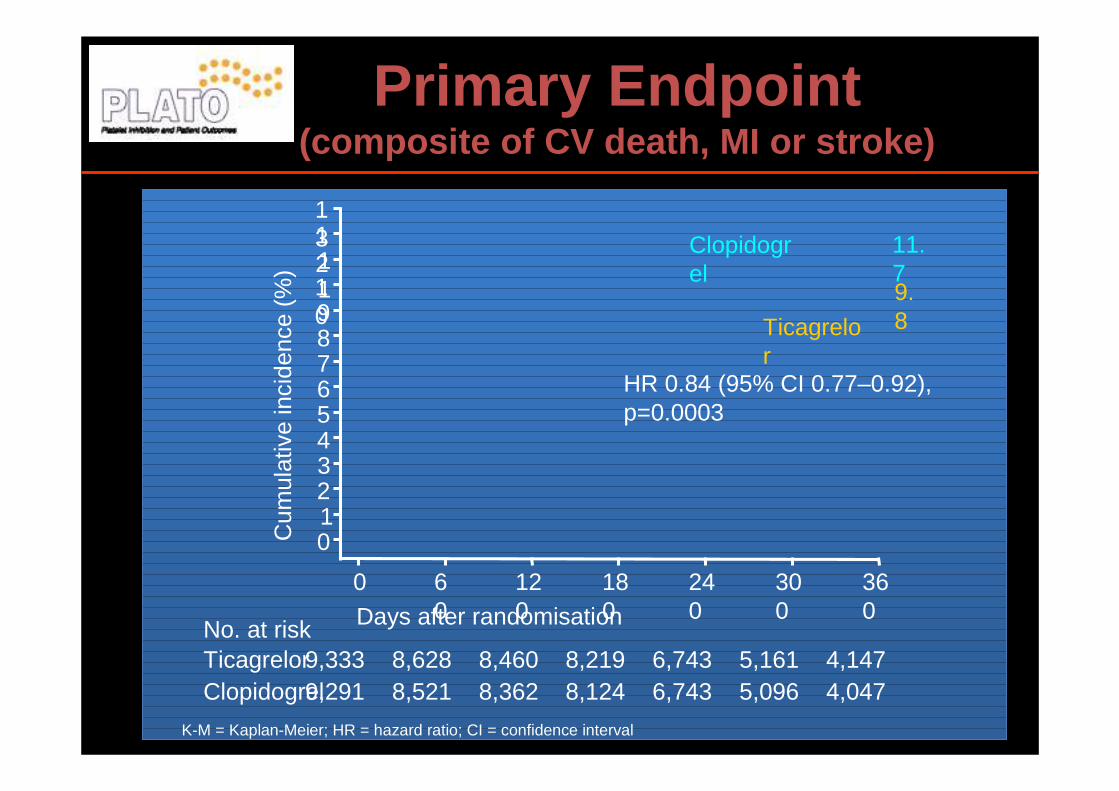
Primary Endpoint (composite of CV death, MI or stroke)
No. at risk
ClopidogrelTicagrelor
9,2919,333
8,5218,628
8,3628,460
8,124
Days after randomisation
6,7436,743
5,0965,161
4,0474,147
0 60
120
180
240
300
360
1211109876543210
13
Cum
ulat
ive
inci
denc
e (%
)9.8
11.7
8,219
HR 0.84 (95% CI 0.77–0.92), p=0.0003
Clopidogrel
Ticagrelor
K-M = Kaplan-Meier; HR = hazard ratio; CI = confidence interval
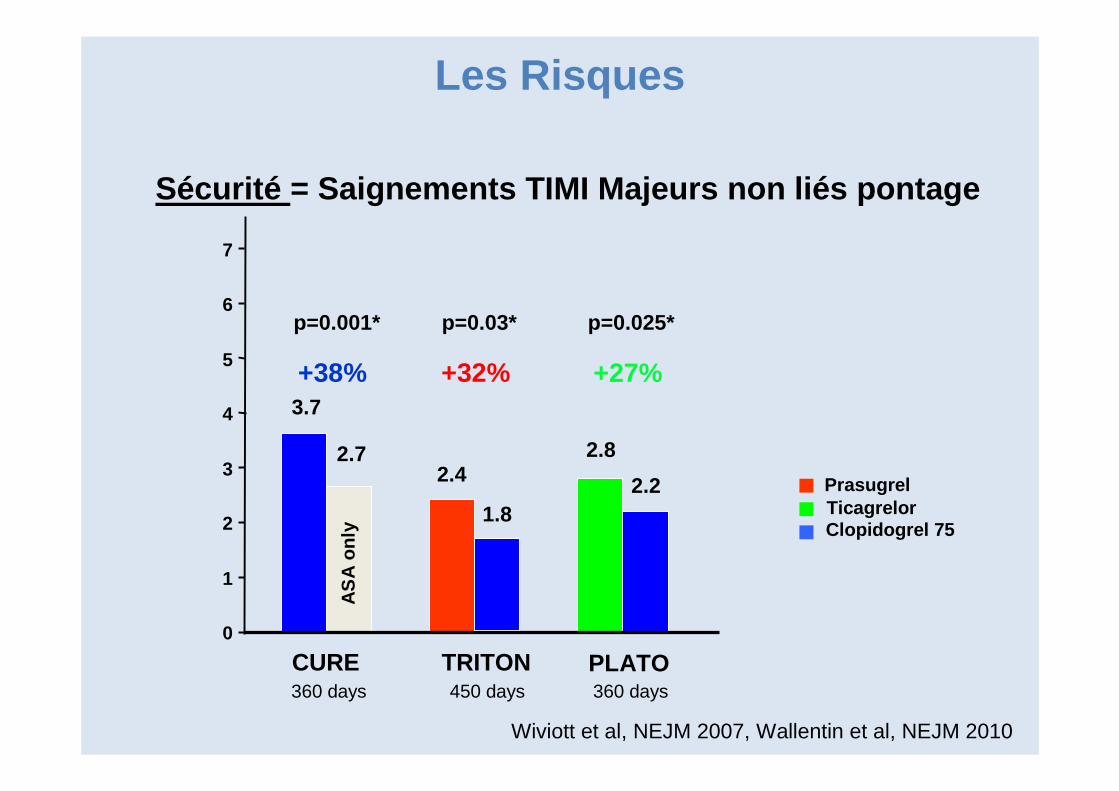
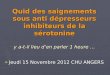
p=0.03* p=0.025*
7
6
5
4
3
2
1
0
2.8
2.2
Sécurité = Saignements TIMI Majeurs non liés pontage
1.8
2.4
p=0.001*
2.7
3.7
450 days
AS
A o
nly
360 days360 days
+38% +32% +27%
TicagrelorClopidogrel 75
Prasugrel
TRITON PLATOCURE
Wiviott et al, NEJM 2007, Wallentin et al, NEJM 2010
Les Risques
Les Anticoagulants(per os)
Les principales indications
� Fibrillation atriale
� Thrombus dans les cavités cardiaques
� Phlébite, embolie pulmonaire et Prévention de TVP
� Prothèses valvulaires mécaniques aortique, mitrale
AVK
� Inhibe les facteurs II, VII, IX et X
� modifient l’INR => mode de surveillance biologique
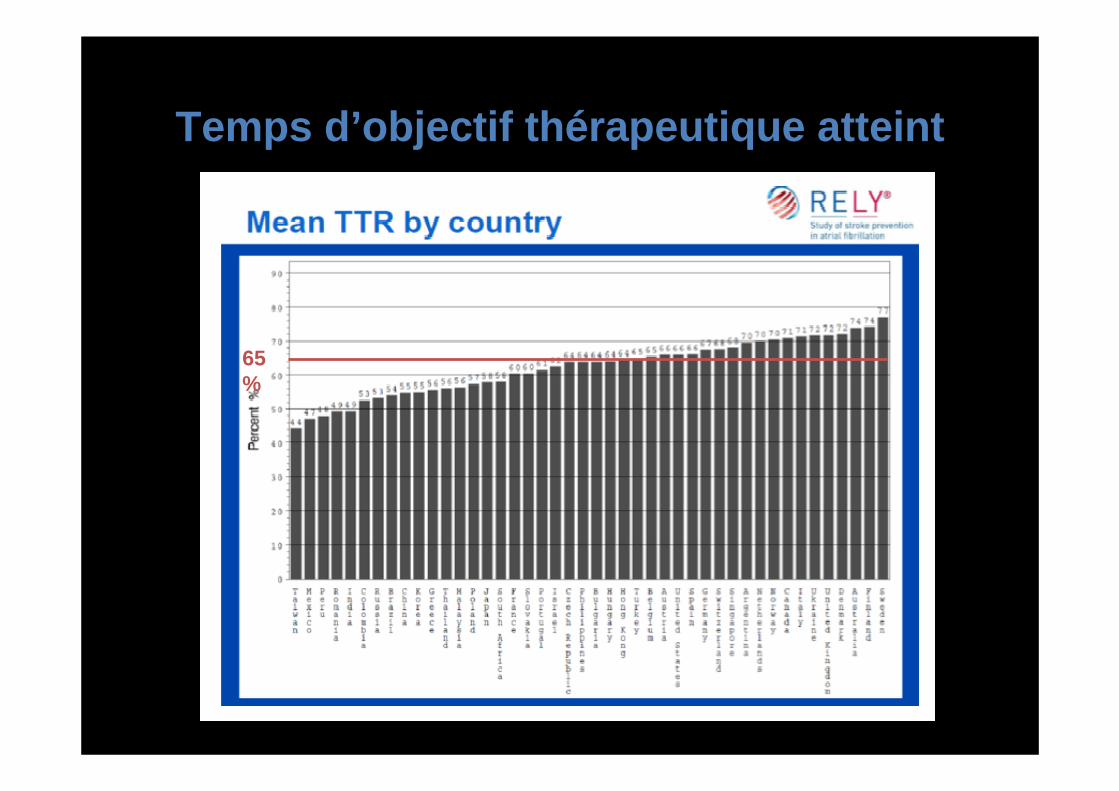
Temps d’objectif thérapeutique atteint
65%
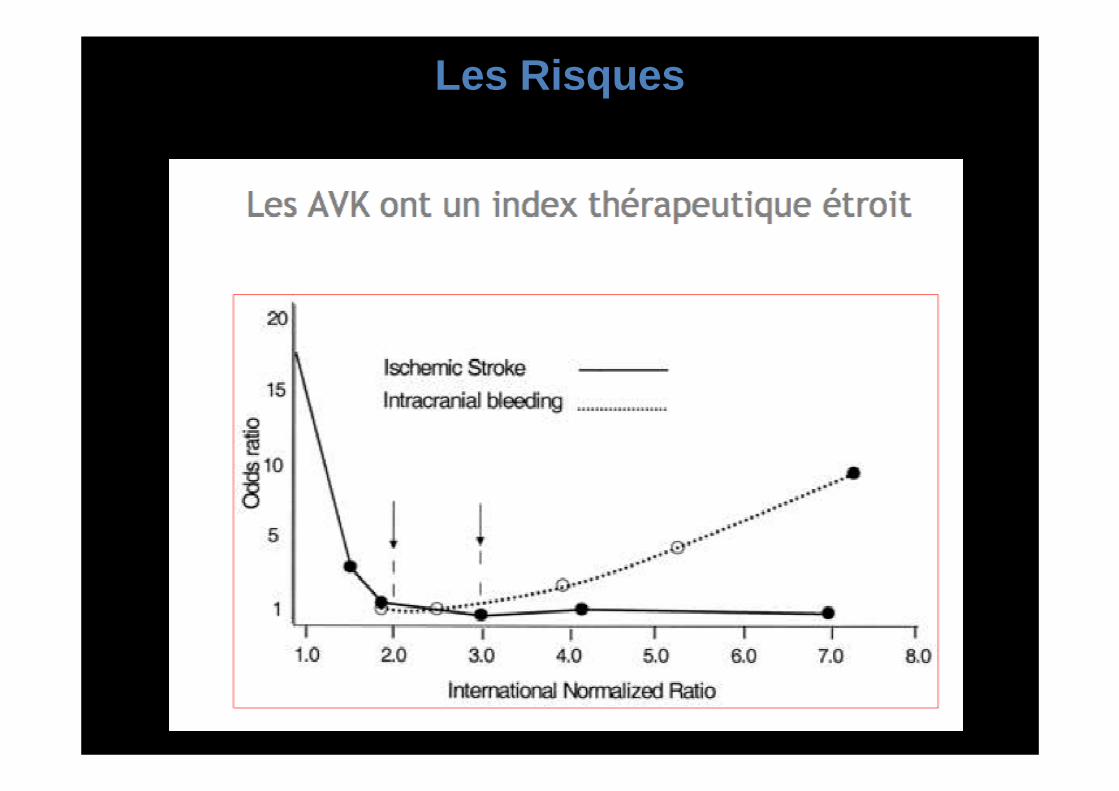
Les Risques
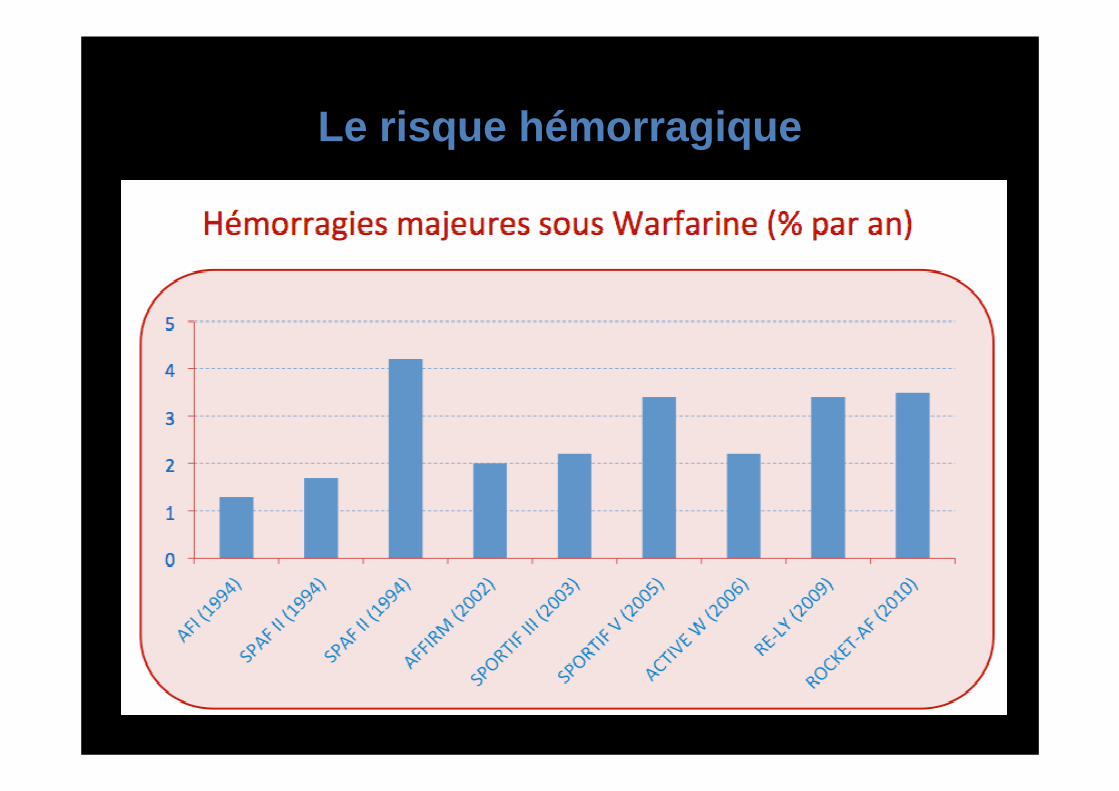
Le risque hémorragique
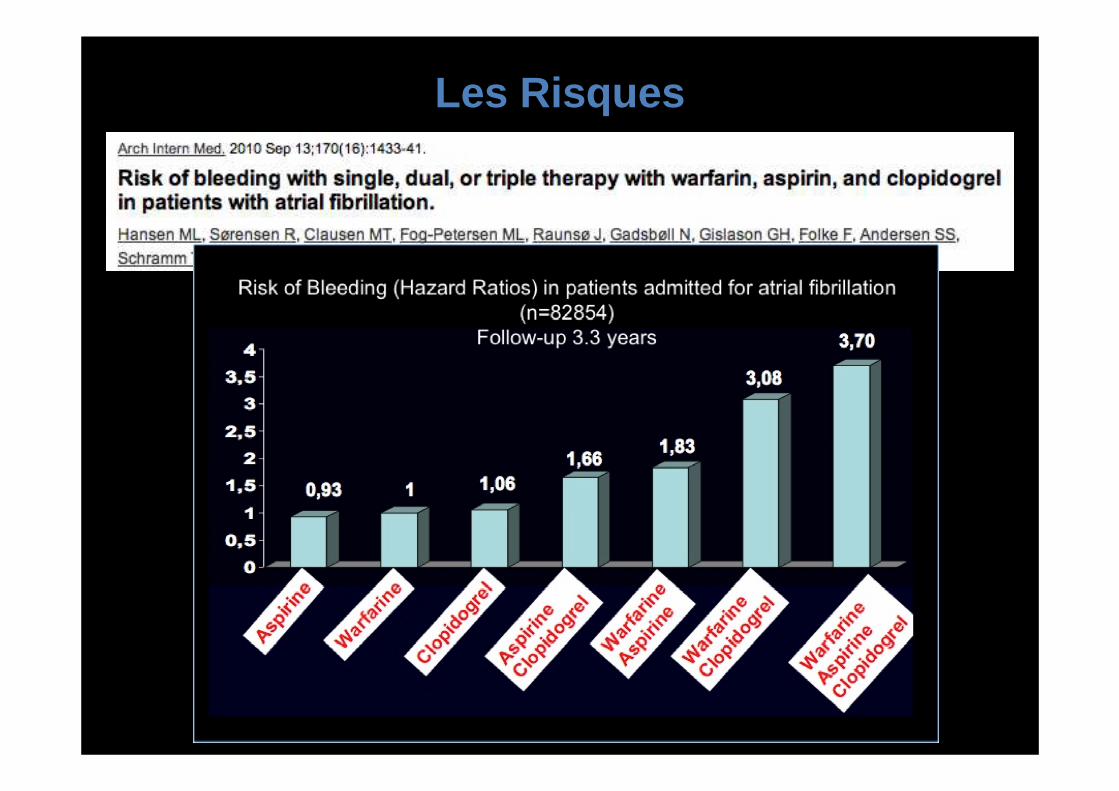
Les Risques
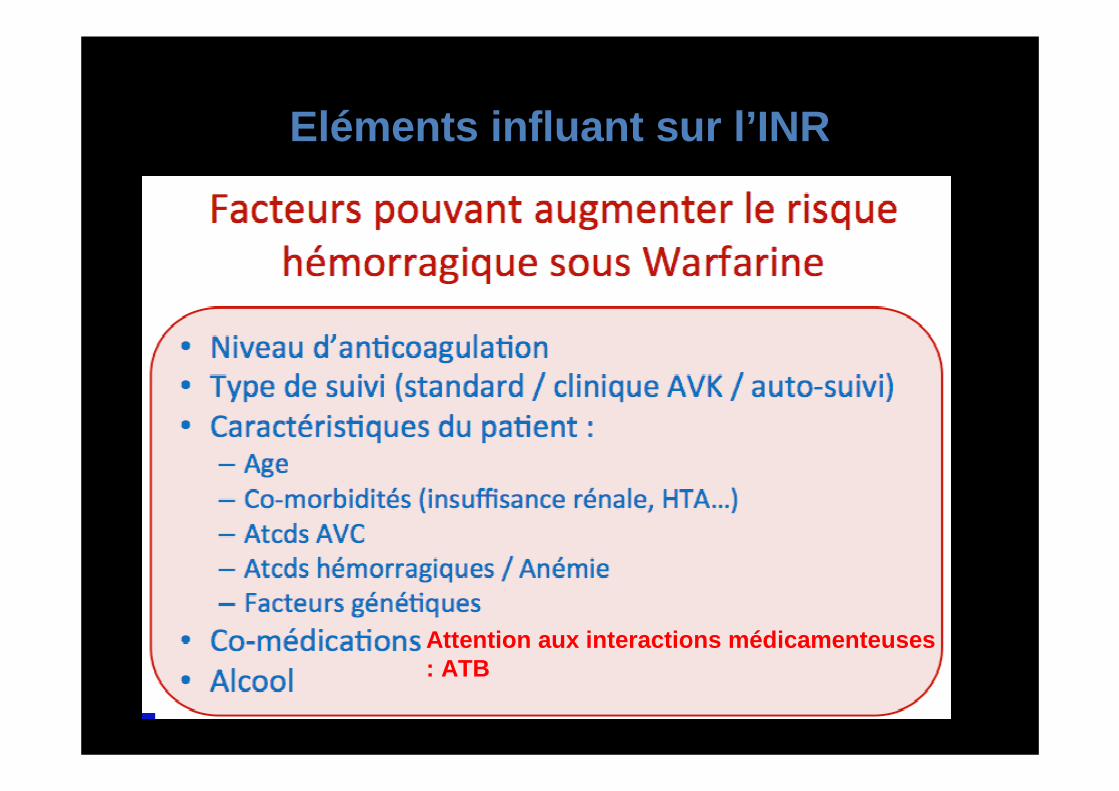
Eléments influant sur l’INR
Attention aux interactions médicamenteuses : ATB
Antidote des AVK
• Vitamine K ou les facteurs de coagulation
Nouveaux anticoagulants
• Dabigatran (PRADAXA*) :Inhibiteur directe de la thrombine. Elimination rapide 24h.
• Rivaroxaban (XARELTO*) : Anti Xa per os. Elimination en 24h.
• Apixaban (ELIQUIS*) : Anti Xa per os. Elimination en 24h.
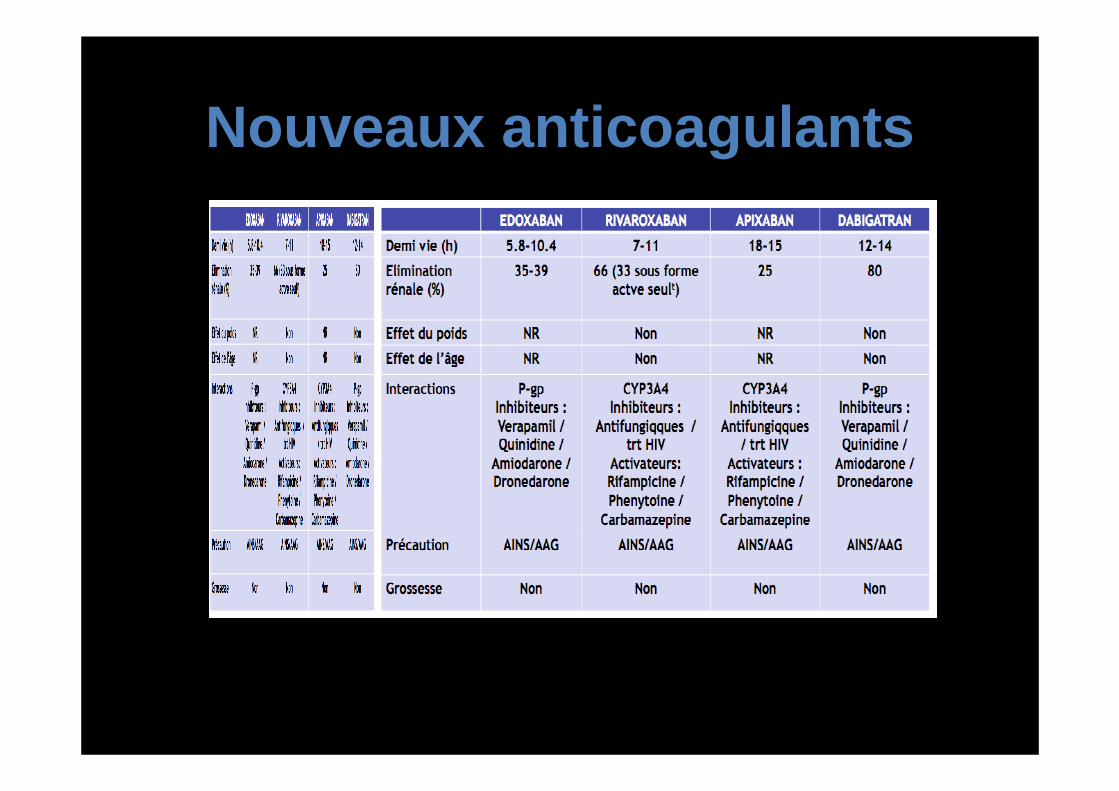
Nouveaux anticoagulants
• Indication : prévention phlébite post-op et traitement de EP
• FA• Pas d’indication dans les valvulopathies• Avantages : pas d’INR, demi-vie courte• Inconvénients : Pas d’antidote pour le
moment, pas de surveillance possible de la prise et de compliance
Nouveaux anticoagulants
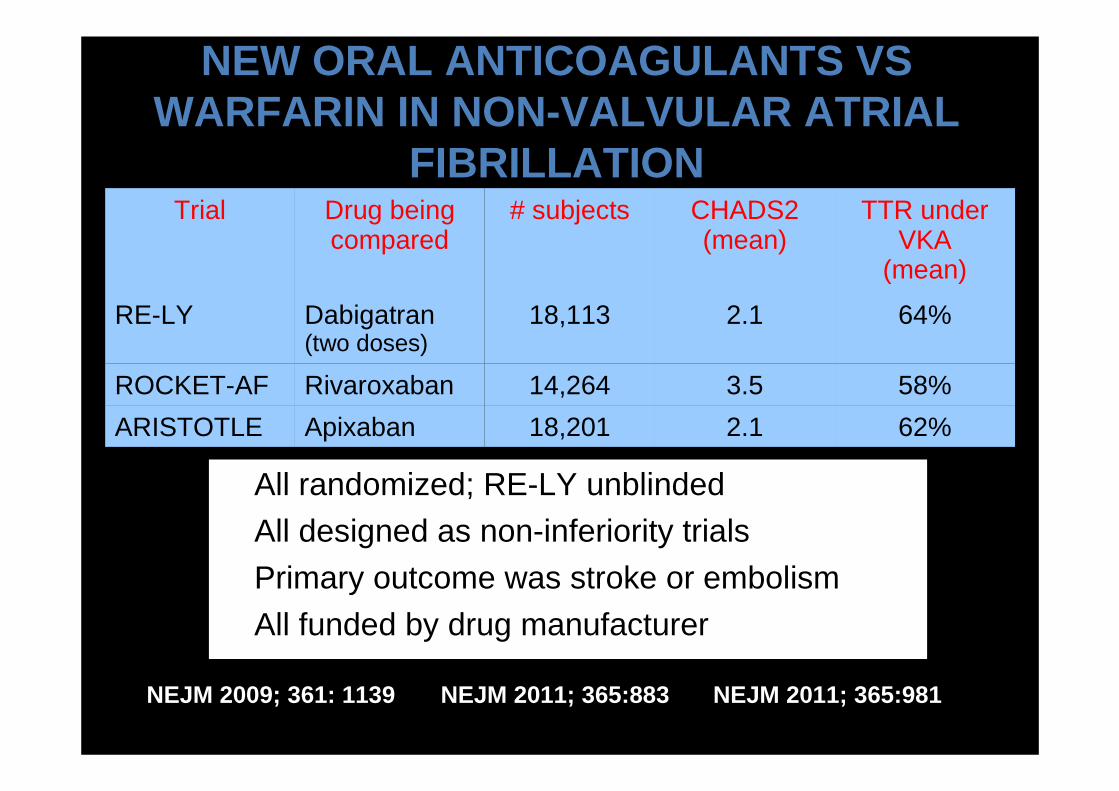
NEW ORAL ANTICOAGULANTS VS WARFARIN IN NON-VALVULAR ATRIAL
FIBRILLATION
• All randomized; RE-LY unblinded
• All designed as non-inferiority trials
• Primary outcome was stroke or embolism
• All funded by drug manufacturer
Trial Drug being compared
# subjects CHADS2(mean)
TTR under VKA
(mean)
RE-LY Dabigatran(two doses)
18,113 2.1 64%
ROCKET-AF Rivaroxaban 14,264 3.5 58%
ARISTOTLE Apixaban 18,201 2.1 62%
NEJM 2009; 361: 1139 NEJM 2011; 365:883 NEJM 2011; 365:981
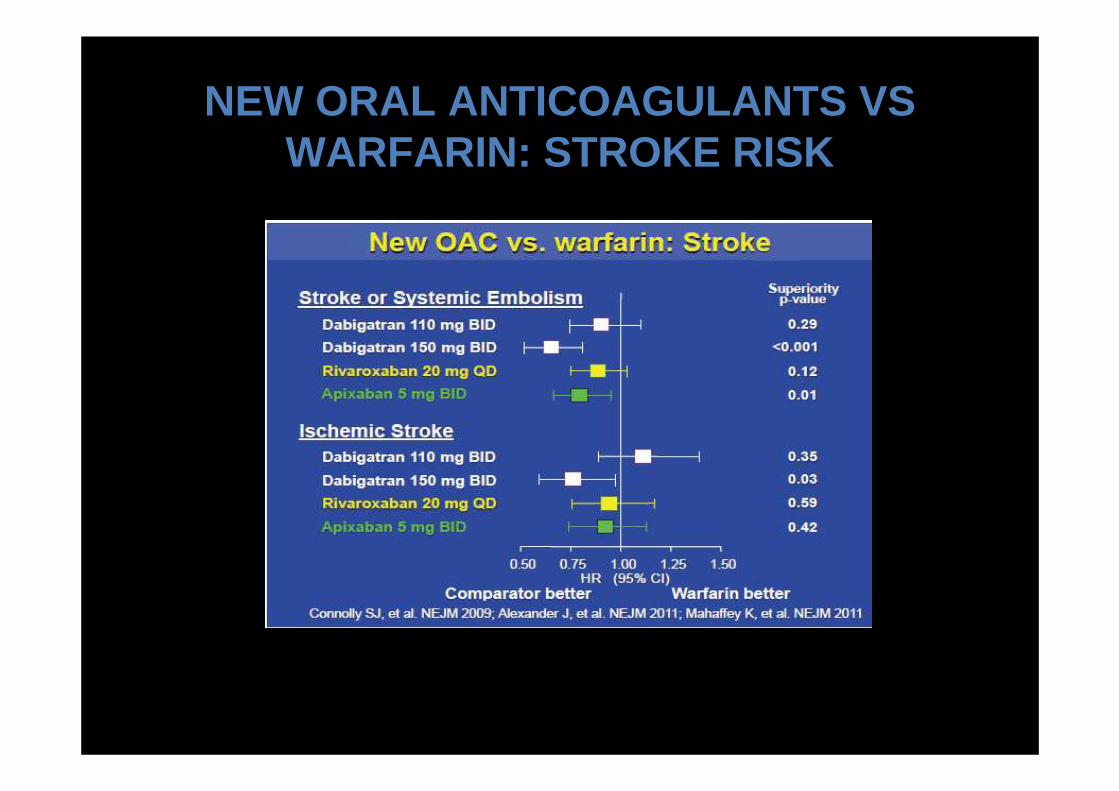
NEW ORAL ANTICOAGULANTS VS WARFARIN: STROKE RISK
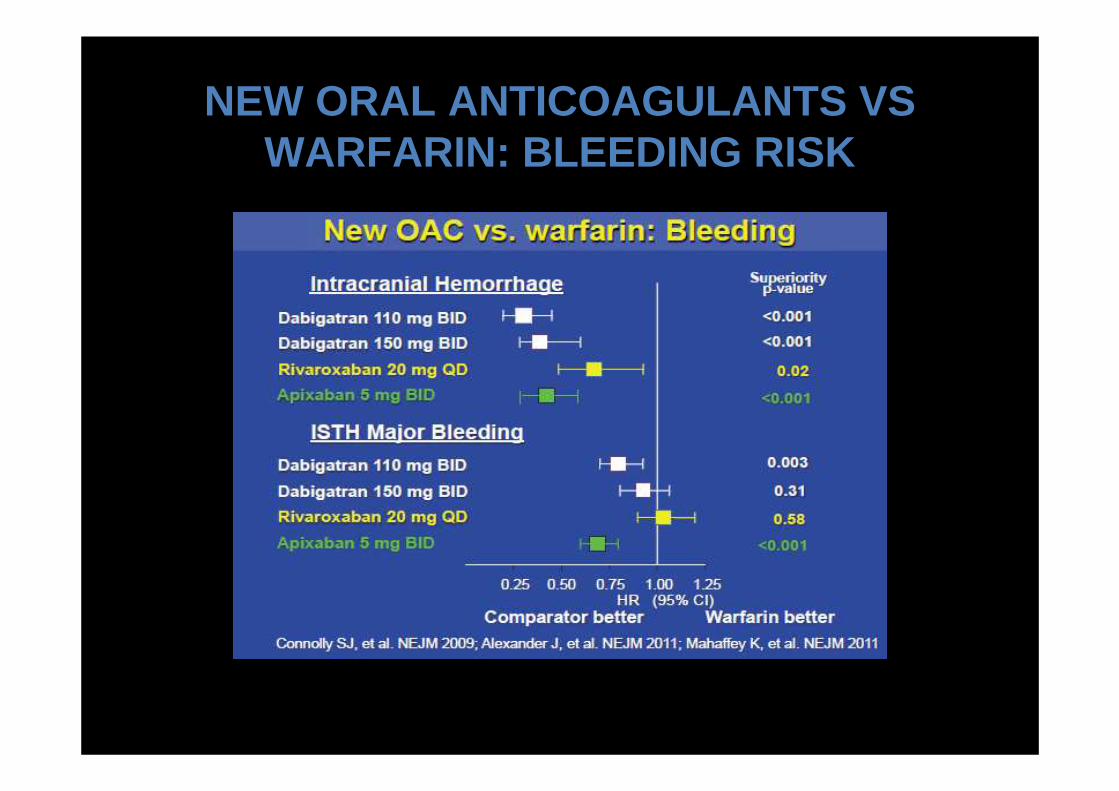
NEW ORAL ANTICOAGULANTS VS WARFARIN: BLEEDING RISK
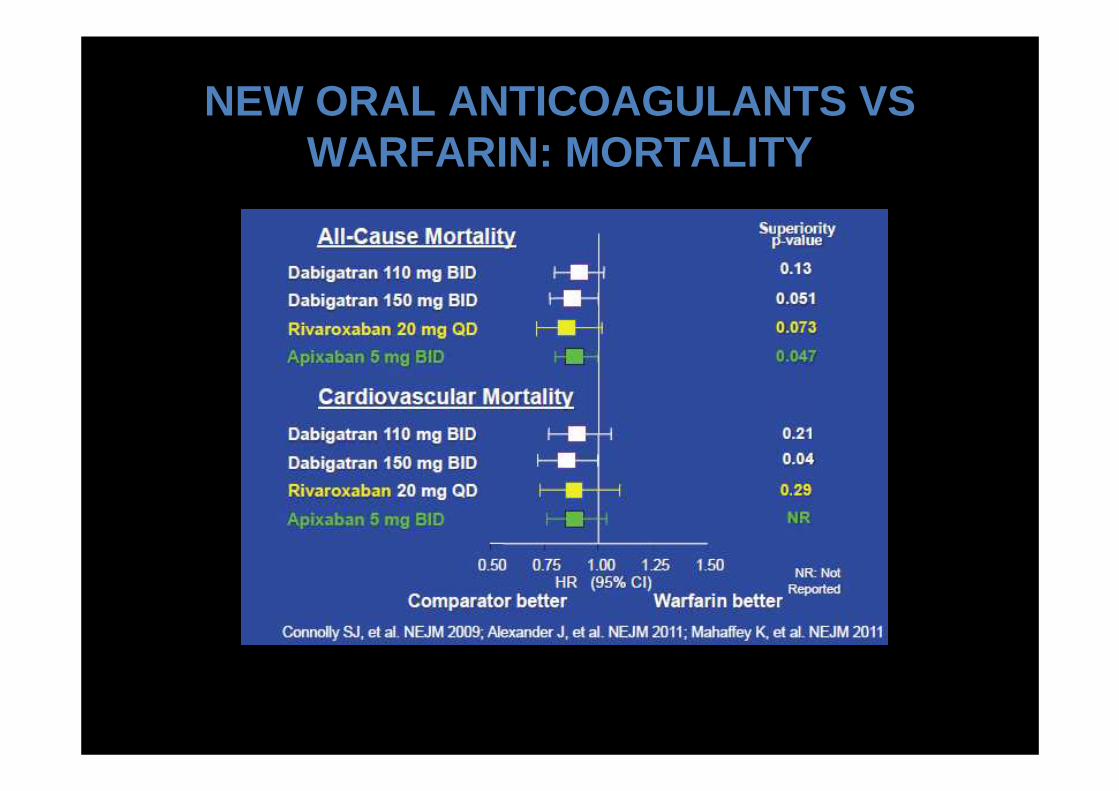
NEW ORAL ANTICOAGULANTS VS WARFARIN: MORTALITY
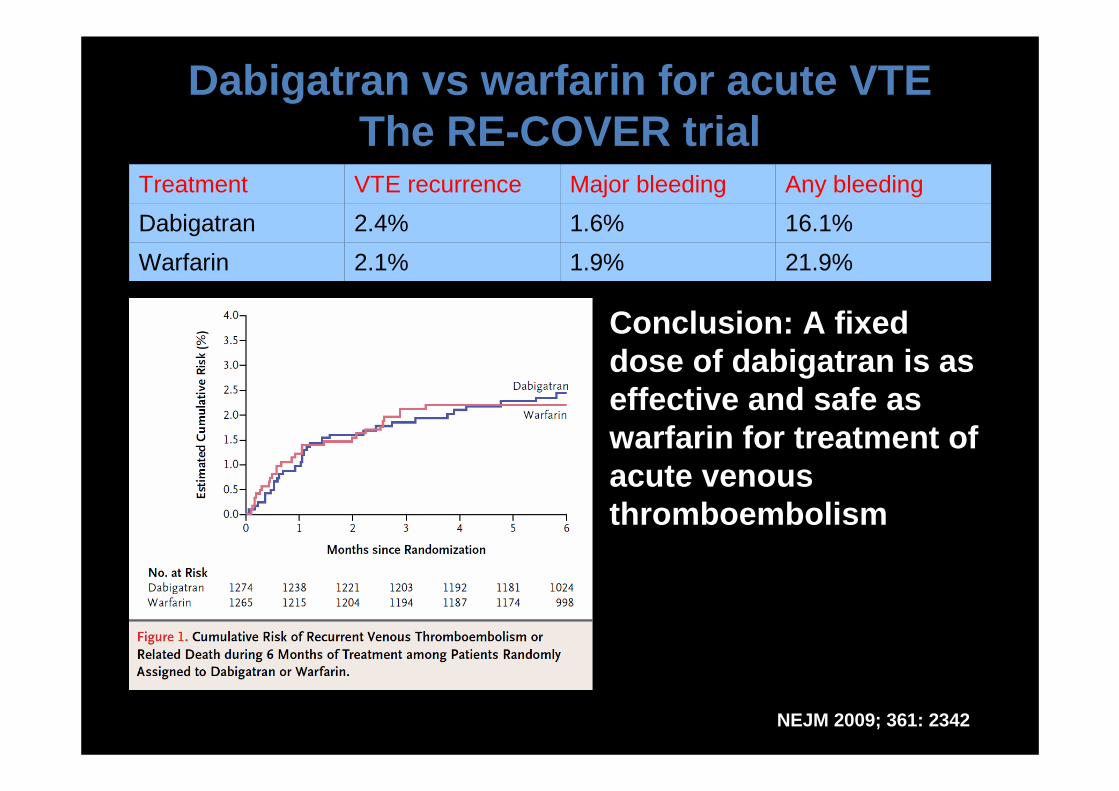
Dabigatran vs warfarin for acute VTEThe RE-COVER trial
Treatment VTE recurrence Major bleeding Any bleeding
Dabigatran 2.4% 1.6% 16.1%
Warfarin 2.1% 1.9% 21.9%
NEJM 2009; 361: 2342
Conclusion: A fixed dose of dabigatran is as effective and safe as warfarin for treatment of acute venous thromboembolism
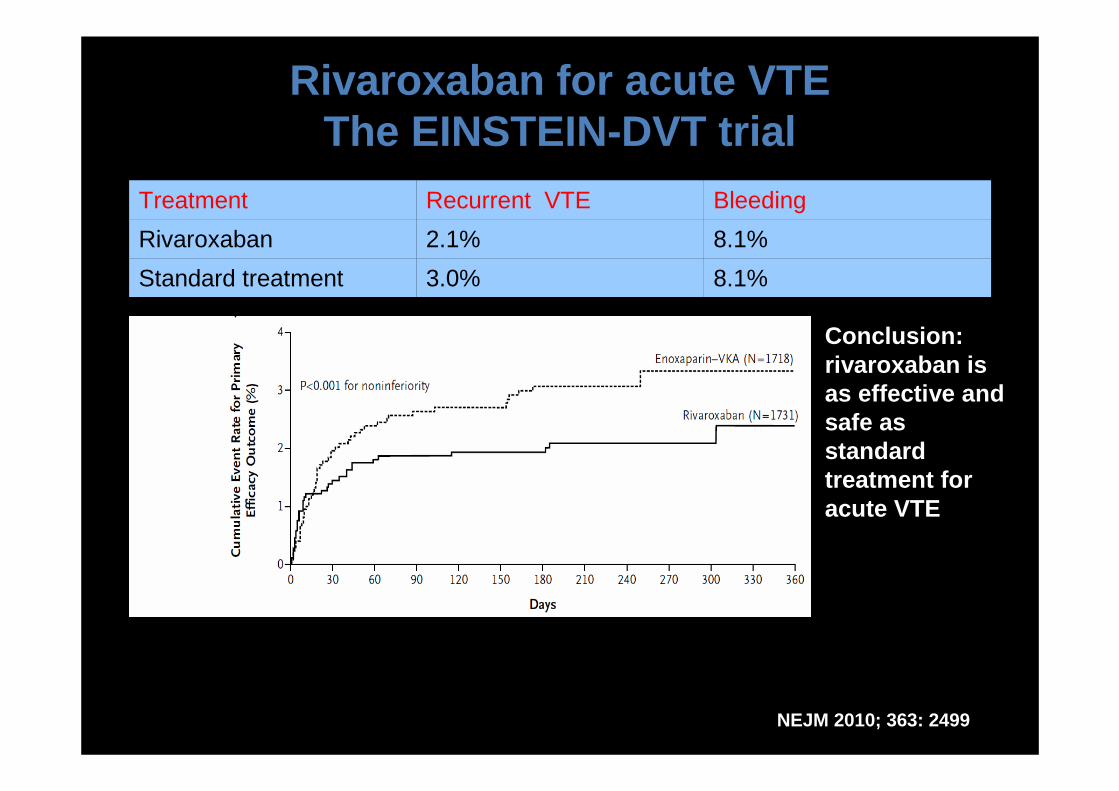
Rivaroxaban for acute VTEThe EINSTEIN-DVT trial
Treatment Recurrent VTE Bleeding
Rivaroxaban 2.1% 8.1%
Standard treatment 3.0% 8.1%
NEJM 2010; 363: 2499
Conclusion: rivaroxaban is as effective and safe as standard treatment for acute VTE
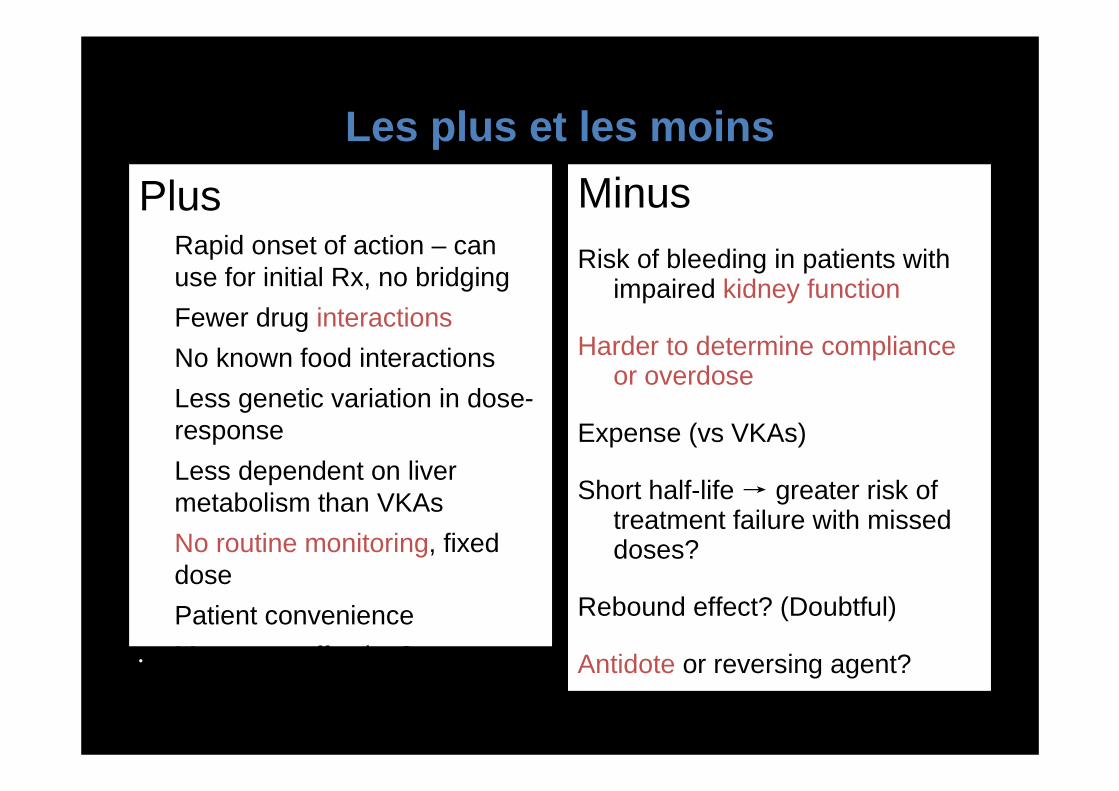
Plus• Rapid onset of action – can
use for initial Rx, no bridging
• Fewer drug interactions
• No known food interactions
• Less genetic variation in dose-response
• Less dependent on liver metabolism than VKAs
• No routine monitoring, fixed dose
• Patient convenience
• More cost-effective?
MinusRisk of bleeding in patients with
impaired kidney function
Harder to determine compliance or overdose
Expense (vs VKAs)
Short half-life → greater risk of treatment failure with missed doses?
Rebound effect? (Doubtful)
Antidote or reversing agent?
Potential for overuse?
Les plus et les moins
merci