Embed Size (px)
Citation preview
Aspects of tropical ulcerating diseases
proefschrift Zegelaars.indb 1 4-2-2008 9:22:14
Printing of this thesis was financially supported by: Huidstichting Chanfleury van
IJsselsteijn, Faculteit der Geneeskunde van de Universiteit van Amsterdam, Abbott
BV, Galderma Nederland, Wyeth Pharmaceuticals BV, Medi Nederland BV, Johnson &
Johnson Medical BV Wound Managment, Bauerfind Benelux BV, Bayer Schering Pharma,
EuroTec BV, GlaxoSmithKline, Leo Pharma, Medizorg Home Care&Tecnology, Novartis
Pharma BV, Schering-Plough BV, Meda Pharma, Smith & Nephew, Serono BV
Lay-out: Chris Bor, Medische Fotografie en Illustratie, AMC
Printed by: Uitgeverij Buijten & Schipperheijn
ISBN: 978-90-9022849-5.
Cover: Tabula Anemographica, made by Johannes Janssonius in1700.
They represent the races that inhabit the areas of the earth from which the
winds blow as seen through European eyes. For more information, http://www.
atlasenkaart.nl/nederlands/toonkaart.php?kaart=26
proefschrift Zegelaars.indb 2 4-2-2008 9:22:14
Aspects of tropical ulcerating diseases
ACADEMISCH PROEFSCHRIFT
ter verkrijging van de graad van doctoraan de Universiteit van Amsterdamop gezag van de Rector Magnificus
prof. dr. D.C van den Boom
ten overstaan van een door het college voor promotiesingestelde commissie,
in het openbaar te verdedigen in de Agnietenkapel
op vrijdag 7 maart 2008, te 12:00 uur
door
James Edward Zeegelaar
geboren te Paramaribo, Suriname
proefschrift Zegelaars.indb 3 4-2-2008 9:22:14
PromotiecommissiePromotor Prof. dr. W.R. Faber
Overige leden Prof. dr J.D. Bos Prof. dr. P.A. Kager Dr. J.R. Mekkes Prof. dr. R.F.M. Lai A Fat Prof. dr. H.A.M. Neumann Dr. D de Hoop
Faculteit der Geneeskunde
proefschrift Zegelaars.indb 4 4-2-2008 9:22:14
ContentsChapter 1 Introduction and aims of this thesis
Cutaneous ulcers in and from the tropics7
Accepted in short version in: Am J Clin Dermatol 2007
Chapter 2 Microcirculatory changes in travellers to a tropical country 49
Int J Dermatol 2002;41(2):93-5
Chapter 3 Bacterial colonization, anti-microbial resistance and the aetiology of wounds in three different tropical countries
57
Chapter 4 Etiology and incidence of chronic ulcers in Blantyre, Malawi 67
Int J Dermatol 2006;45(8):933-6
Chapter 5 Tolerability and efficacy of hydrocolloid dressings in the treatment of venous leg ulcers under tropical conditions; an open prospective study
77
J Eur Acad Dermatol Venereol 2001;15(3):234-7
Chapter 6 Changing pattern of imported cutaneous leishmaniasis in the Netherlands
85
Clin Exp Dermatol 2005;30(1):1-5
Chapter 7 First reported case of Mycobacterium ulcerans infection in a patient from China
95
Trans R Soc Trop Med Hyg 2000;94(3):277-9
Chapter 8 Summary/conclusion 103
Chapter 9 Samenvatting/conclusies 109
Dankwoord 115
proefschrift Zegelaars.indb 5 4-2-2008 9:22:15
proefschrift Zegelaars.indb 6 4-2-2008 9:22:15
Chapter
1Introduction and aims of the thesisCutaneous ulcers in and from the tropics
Jim E. Zeegelaar and William R. Faber
Accepted in short version for publication in: American Journal of Clinical Dermatology
proefschrift Zegelaars.indb 7 4-2-2008 9:22:15

proefschrift Zegelaars.indb 8 4-2-2008 9:22:15
Chapter 1
Introduction and aim
s of the thesis
9
IntroductionSkin ulcers are a regular reason for consultations at the departments for tropical diseases in the Western World.1-5 It is likely that the incidence of imported ulcers will rise because of frequent travel to and from tropical countries. This is most evidently illustrated by the rising incidence of imported cutaneous leishmaniasis.6
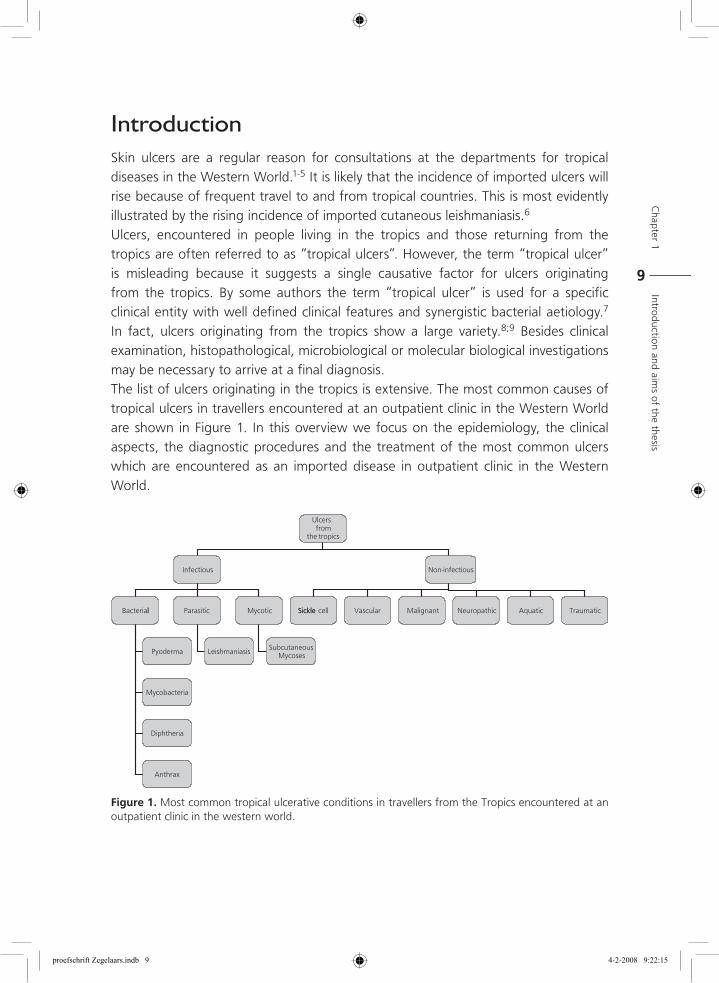
Ulcers, encountered in people living in the tropics and those returning from the tropics are often referred to as “tropical ulcers”. However, the term “tropical ulcer” is misleading because it suggests a single causative factor for ulcers originating from the tropics. By some authors the term “tropical ulcer” is used for a specific clinical entity with well defined clinical features and synergistic bacterial aetiology.7 In fact, ulcers originating from the tropics show a large variety.8;9 Besides clinical examination, histopathological, microbiological or molecular biological investigations may be necessary to arrive at a final diagnosis.The list of ulcers originating in the tropics is extensive. The most common causes of tropical ulcers in travellers encountered at an outpatient clinic in the Western World are shown in Figure 1. In this overview we focus on the epidemiology, the clinical aspects, the diagnostic procedures and the treatment of the most common ulcers which are encountered as an imported disease in outpatient clinic in the Western World.
Figure 1. Most common tropical ulcerative conditions in travellers from the Tropics encountered at an outpatient clinic in the western world.
proefschrift Zegelaars.indb 9 4-2-2008 9:22:15
10
Bacterial infections
Pyoderma
IntroductionPyoderma includes several clinically distinct types of skin lesions that are caused by Staphylococcus aureus and/or β-haemolytic streptococci group A.10-14 It is a common cause of (purulent) ulcerative skin lesions in the tropics.15;16
At the departments for tropical and imported skin diseases, severe (ulcerating) pyodermas, especially in the lower legs, are regularly encountered in travellers.2;3;17;18 As far as we are aware, the incidence of these pyodermas remains unknown. It is also not known whether the prevalence and the virulence of streptococci and staphylococci that cause these pyodermas are higher in the tropics than that in the Western World.
Epidemiology
Although ulcerating pyoderma is encountered all over the World, it seems to be more prevalent in the tropics. Environmental conditions such as temperature and humidity may also contribute. However, there are only a few published studies on the prevalence or the incidence of pyoderma in tropical countries.15;19-21
Clinical aspects
Staphylococcus aureus and β-haemolytic streptococcus group A are the two main micro-organisms that are responsible for the ulcerating skin infections. Superficial skin infection may extend more deeply into the dermis and produce shallow ulcers known as ecthyma.20;22-25 It usually starts as a vesicle or vesiculopustule on an erythematous base, which later ulcerates. The ulcer is covered with a dark-brown, bloody crust. A tender punched-out ulcer remains once the crust is removed. It is usually found on the dorsal feet, shins and thighs, but less often on the upper part of the body. There are usually few lesions, but new lesions may develop without adequate treatment. Pyoderma in travellers is most commonly encountered as a secondary infection in skin lesions caused by environmental insults, such as insect bites, abrasions and atopic dermatitis.3
proefschrift Zegelaars.indb 10 4-2-2008 9:22:15

Chapter 1
Introduction and aim
s of the thesis
11
Diagnosis
The diagnosis is often based on the clinical picture of persistent painful ulceration especially in the lower legs. One should perform a bacterial culture if facilities are available. Ideally, tissue obtained by biopsy or needle aspiration should be cultured.26 In daily practice this is often not routinely performed because it is more time-consuming and inconvenient for the patient. However, adequate culture results were obtained using the swab technique.27-29 Susceptibility tests in vitro are preferable. Methicillin-resistant Staphylococcus aureus and tetracycline-resistant streptococci and staphylococci are frequently encountered in many areas of the tropics.30;31
Treatment
Treatment of ulcerative pyoderma is initially based on the clinical assessment. Gram-stained smears of the exudate may be helpful in starting empirical antimicrobial treatment. However, antibiotic treatment should be preferably based on culture outcome. If culture result is not yet available and the clinical condition requires antibiotic treatment one may start, in case of a community acquired ulcerative pyoderma, with flucloxacillin orally for at least 10 days as the drug of first choice. The antibacterial activity of flucloxacillin is evident on Gram-positive bacteria and above all on penicillinase-producing staphylococci.32-36 With the global spreading of macrolide-resistant Staphylococcus aureus and β-haemolytic streptococci, these antibiotics should be prescribed with caution. Clindamycin is recommended in penicillin-allergic patients.37As an alternative vancomycin may be used, although the first vancomycin-resistant Staphylococcus aureus (VRSA) have been reported.38
Besides antimicrobial treatment, appropriate wound dressings are important, but often neglected. It is generally accepted that ulcers heal more rapidly under occlusive (moist) dressings than under dry circumstances.31;39 Special attention should be paid to ulceration in the lower legs where (sub) clinical oedema is often present. This oedema may delay or even complicate healing. Oedema may be eliminated by adequate compression therapy with elastic or non-elastic bandages or stockings.
Mycobacteria
Mycobacterial infections comprise infections that are caused by the different species of the genus Mycobacterium. Most mycobacteria cause localized and often harmless infections of the skin.40 Cutaneous disease may be due to inoculation, by trauma or iatrogenic; may be
proefschrift Zegelaars.indb 11 4-2-2008 9:22:15
12
contiguous with underlying osteomyelitis or lymphadenitis or may be a part of disseminated disease.In immune competent patients the disease is in generally localized, although lymphatic spread, the so-called nodular lymphangitis, is well known in for instance M. marinum infections.As mycobacteria are intracellular micro-organisms, the immunological response of the host is a cell-mediated immune reaction resulting in a granulomatous tissue reaction. Infections with non-tuberculous mycobacteria in immune compromised patients may lead to severe disease. After tuberculosis and leprosy, M. ulcerans is the most common mycobacterial disease and the most important cause of cutaneous ulceration.The list of mycobacteria which are potential pathogens and may cause ulceration include M. scrofulaceum, M. fortuitum, M. chelona-abscessus, and M. avium complex.41 More rare infections are caused by M. szulgai, M. kansasii and M. haemophilum.42-44 These mycobacteria are only rarely seen as causing ulceration in the skin and will therefore not be discussed further. Besides M. ulcerans and M. tuberculosis , M. marinum may cause skin ulceration and will therefore be discussed. M. leprae will not be discussed because the ulceration is the consequence of neuropathy which may develop as nerve damage occurs during leprosy reactions. Infection with M. leprae it self does not lead to ulcerating conditions.
Mycobacterium ulcerans
Introduction
Buruli ulcer is a chronic ulcerating disease of the skin, subcutaneous tissue and bone caused by M. ulcerans. It was named after the Buruli district in Uganda where the prevalence was high.45 M. ulcerans has been cultured from several species in areas endemic for Buruli ulcer and is believed to be an environmental mycobacterium.46;47
Trauma by vegetation seems to be essential for the introduction of M, ulcerans into the skin.42 Insects may play a role in the transmission of the infection.48 HIV infection seems not to be a risk factor for Buruli ulcer and it does not appear to influence the treatment outcome of Buruli ulcer.49
Epidemiology
The largest number of patients is found in Africa. Before 1980, reports came mainly from the Democratic Republic of the Congo and Uganda. After 1980, new foci emerged in West Africa particularly in distinct regions of Benin, Ivory coast and
proefschrift Zegelaars.indb 12 4-2-2008 9:22:15

Chapter 1
Introduction and aim
s of the thesis
13
Ghana.49-52It has been reported in Asia, South America and the Western World. The majority of the cases are children younger than 15 years, with lesions mostly located on the extremities (legs more than arms). Buruli ulcer has been described as an imported disease in the Western World.53-55
The major endemic foci are located in wet lands, especially those with slow-flowing or stagnant water in tropical and sub-tropical countries. It appears that natural or man-made changes in water management influence the outbreak of Buruli ulcer. 49;52;56;57
Clinical aspects
Whether the disease develops after exposure to M. ulcerans depends largely on the host defences. In most cases M. ulcerans will probably be cleared, disease may develop or it may lead to sub-clinical or asymptomatic infection.58
A Buruli ulcer is characterised by a painless nodule, papule, plaque or oedema, evolving into a painless ulcer with undermined edges, often leading to invalidating sequelae.57
Diagnosis
Diagnosis is established on the basis of clinical picture which is associated with non-specific features, especially in the pre-ulcerative stage. Therefore, every nodule and ulcer in an endemic area is suspected to be M. ulcerans disease.57
The histopathological picture of an early lesion is characterised by circumscribed necrosis in the deep dermis with little or acute inflammatory reaction. This is followed by a septal panniculitis with ulceration of the subcutaneous tissue. Besides an acute also a chronic or granulomatous reaction can be observed. Acid-fast bacilli are especially found extracellularly in the necrotic areas.59
M. ulcerans can be cultured from clinical specimens, although care should be taken to collect the material from sites where bacilli are normally present e.g. the necrotic base of the lesion or the undermined edges of the ulcer.60;61 Primary cultures may take between 6 and 8 weeks.Polymerase chain reaction (PCR) has been developed as a diagnostic technique for the identification of the micro-organism.62-64. This enables rapid diagnosis, which is important because at present the standard treatment is by excision of the lesion. Confirmation with PCR is helpful also in circumstances where M. ulcerans disease is a part of a differential diagnosis. PCR can be performed using (biopsy) tissue, from swabs taken from under the undermined edge of the ulcer and from environmental samples.
proefschrift Zegelaars.indb 13 4-2-2008 9:22:15
14
Treatment
Surgical excision followed by skin grafting is the therapeutic measure of choice. However, a combination of rifampicin and streptomycin may be effective against early forms of Buruli ulcer.65A combination of amikacin and rifampicin was shown to be effective in a Buruli ulcer model in mice.66
Mycobacterium marinum (Swimming pool granuloma)
Introduction
Swimming pool granuloma is caused M. marinum, a mycobacterium belonging to the non-tuberculous mycobacteria, which causes disease in fresh- and salt water fish, and occasionally in humans.67 It is the most common cause of non-tuberculous mycobacterial infections.
Epidemiology
As initial reports of cutaneous disease by M. marinum were associated with swimming pools it was called swimming pool granuloma.68 Infection in swimming pools nowadays is rare due to proper chlorination. The distribution is World Wide, occurring in fresh-brackish as well as salt water, and is prevalent in heated water (for instance in tropical aquaria) in temperate climates, and in pools and the sea in more tropical climates. In principle any water-related activity carries a potential risk for infection. Generally infection occurs through superficially traumatised skin.
Clinical aspects
The initial lesions starts as an inflammatory papule after a relatively long incubation period of 2 to 6 weeks. As infection is preceded by trauma majority of the lesions are located on the back of the fingers or the hand or around the knee. The papule then gradually enlarges into a bluish-red inflammatory nodule or plaque, which may ulcerate or show a warty surface. There is generally a delay of months to even years before a doctor’s opinion is sought because the lesions are painless and enlarge slowly. The lesions may heal spontaneously. However, this may take months to years. Less often deep infections such as tenosynovitis, osteomyelitis, arthritis and bursitis may occur. M. marinum infections are one of the causes of nodular lymphangitis (also called sporotrichoid extensions after the lymphatic spread of sporotrichosis). Clinically, there are nodules and/or ulcerating lesions resulting from spread along the lymphatic vessels. Deep infections and nodular lymphangitis do not heal spontaneously.
proefschrift Zegelaars.indb 14 4-2-2008 9:22:15
Chapter 1
Introduction and aim
s of the thesis
15
Diagnosis
The clinical picture, the preferential location combined with a history of aquatic activity with a skin trauma should provide high index of suspicion. The clinical diagnosis should be confirmed by diagnostic tests. At present PCR techniques using biopsy material provide a diagnosis within days.69Histopathological examination of a skin biopsy can be non-specific in the early stage of the disease. A granulomatous reaction develops after 6 months. The presence of acid-fast bacilli by special staining techniques is reported in varying percentage. Absence does not rule out M. marinum infection. Cultures can be performed using aspirates or biopsies. The optimal growth is at 30 to 32˚C, and cultures should be maintained for 6 weeks.
TreatmentSeveral treatment options exist. Treatment regimens consist of combinations containing clarithromycin, rifampicin or ethambutol. More recently the new macrolides such as clarithromycin are proposed as a single drug therapy.70;71 However, no randomised studies have been performed. Response to treatment is slow and is continued till clinical cure.
Mycobacterium tuberculosis
IntroductionCutaneous tuberculosis has today become a rare disease in inhabitants of the Western World. Therefore, the majority of cutaneous tuberculosis cases are diagnosed in immigrants.72
EpidemiologyCutaneous tuberculosis was diagnosed in 2 to 4% of the out-patients at dermatological clinics in Great Britain at the beginning of the 20th century. The same figures have been reported in studies from Asia in the middle of the last century, but appear to be decreasing.
Clinical aspectsUlcerated lesions may be encountered in primary tuberculosis, but may also be a manifestation of secondary tuberculosis. Only cutaneous tuberculosis with clinical manifestation of ulceration are discussed.
proefschrift Zegelaars.indb 15 4-2-2008 9:22:16

16
Primary infection
Primary infection accounts for only 2 % of all cases of cutaneous tuberculosis. It is caused by exogenous inoculation of M. tuberculosis. The lesion starts 2 to 4 weeks after inoculation as a smooth papule or nodule, which enlarges during the course of several weeks to a plaque, which ulcerates forming a so-called ‘tuberculoid chancre’. The ulcer shows undermined edges and is painless. After 3 to 8 weeks non-tender regional lymphadenopathy develops, which may suppurate to form a “cold” abscess, which then may spontaneously drain with sinus tract formation. This process in general heals spontaneously with atrophic scarring in 3 to 12 months. Primary lesions are mainly located on the face and the extremities in children, but inoculation by injections and surgical procedures is also possible.
Secondary infection
Scrofuloderma
Due to contiguous spread from a deeper localised infection such as lymph node or in some cases bone. Initially there is an indurated inflammatory area overlying the deeper infection. Due to suppuration fluctuating nodules develop, which ulcerate with formation of sinus tracks. In the course of time cordlike scars or keloids develop. The lesions are mostly localised over the lymph glands in the neck.
Lupus vulgarisLupus vulgaris was the most common manifestation of cutaneous tuberculosis in Europe before World War II. Today it is common in developing countries. It is caused by re-activation of the disease in patients with a high degree of cell-mediated immunity after earlier haematogenous dissemination. The lesions start as brown-red papules, which in the classical form extend into plaques with peripheral activity with an irregular border and central healing with atrophic scar formation and depigmentation. The clinical picture may be variable. Besides the plaque form, there is a hypertrophic form with nodules, which may form a hyperkeratotic mass. The ulcerative form is the most destructive variant. It may erode cartilage and bone, and result in extensive scarring and even deformities. Lesions may become chronic and may persist for decades with gradual extension with progressive scarring and deformity and function loss. The most common location is the face, with the nose, the checks, the mouth and the earlobes as preferential sites. Lesions on the legs and the buttocks are common in Asia and Africa.
proefschrift Zegelaars.indb 16 4-2-2008 9:22:16
Chapter 1
Introduction and aim
s of the thesis
17
Tuberculous gumma
Tuberculous gumma or metastatic tuberculous ulcer is caused by haematogenous dissemination from a primary focus during periods of lowered resistance in bacillaemia. The lesion starts as a subcutaneous nodule or a fluctuant swelling. The overlying skin breaks, resulting in an undermined ulcer with sinus formation. Then it resembles scrofuloderma.
Diagnosis
The clinical picture and epidemiological history of the patient are important. The acid-fast mycobacteria are observed by microscopic investigation of the tissue, especially of early lesions. Culture may be performed using Löwestein-Jenssen medium. PCR is performed in many laboratories and provides reliable, rapid and accurate results for the diagnosis of different types of cutaneous tuberculosis.73;74
Treatment
Treatment of cutaneous tuberculosis is commonly with a multiple drug regimen consisting of isoniazid, ethambutol, pyrazinamide and rifampicin.
General comments
A high index of suspicion is warranted because the clinical picture of mycobacterial infection of the skin can be non-specific. Investigation for mycobacteria is indicated in cases of persistent infiltrative lesions or non-healing ulcers.
Diphtheria
Introduction
Cutaneous diphtheria is an infectious bacterial disease caused by Corynebacterium diphtheriae or more rarely, Corynebacterium ulcerans.75;76 It is transmitted by direct contact with cutaneous carriers and to a lesser extent via vomit. The species of C. diphtheriae produces a toxin which is responsible for the disease diphtheria. The micro-organism (both toxigenic and non-toxigenic strains) may be harboured in the nasopharynx, skin and other sites of asymptomatic carriers. C. diphtheriae is often found secondarily in pre-existing ulcers like echtyma or as superinfection in eczema.77 In immunized individuals systemic toxic complications such as myocarditis and neuritis are rare. The skin lesions may be an important reservoir of infection. Contacts should
proefschrift Zegelaars.indb 17 4-2-2008 9:22:16
18
be investigated and treated if necessary because there is a potential for secondary transmission.78
Epidemiology
Cutaneous diphtheria is still endemic in many tropical countries. It is currently rare in the developed World because of the routine active immunization, but is generally travel-related.75;79;80 The incidence of cutaneous diphtheria is not known.
Clinical aspects
The characteristic of a primary lesion ranges from a tender pustule to a chronic, non-healing ulcer with a punched-out appearance and an adherent membrane with a slightly undermined margin. In the first 2 weeks it is painful, later the lesion becomes painless and after (spontaneous) removal of the adhering membrane, the haemorrhagic base appears. In many cases lesions are less distinctive. Secondary infection in any pre-existing wound and superinfection of eczematous skin lesions is common and often overlooked. Cutaneous diphtheria may persist for 6 to 12 weeks.A high awareness in clinicians and microbiologists is necessary because cutaneous diphtheria ulcers are non-specific.80
Diagnosis
The initial diagnosis is clinical. The definitive diagnosis is made by isolating and identifying C. diphtheriae from the ulcer and demonstrating its toxigenicity. The physician must inform the laboratory in advance of the clinical suspicion because C. diphtheriae is not isolated by routine culturing.
Treatment
Corynebacterium diphtheriae is susceptible to a variety of antibiotics. Erythromycin and penicillin are both effective. If the diagnosis is suspected anti-toxin should be administered intramuscularly. However, isolates from chronic skin lesions are often not toxigenic or produce only little toxin, so that the role of anti-diphtheria serum is doubtful in such cases.77
proefschrift Zegelaars.indb 18 4-2-2008 9:22:16

Chapter 1
Introduction and aim
s of the thesis
19
Anthrax
Introduction
Anthrax is caused by the gram-positive, spore-forming Bacillus anthracis. It is primarily a disease of animals that is occasionally transmitted to humans. Its incidence has dramatically decreased during the last century, probably because of the control of animal anthrax, immunization and improved hygiene.The cutaneous form is the most common, but it can be fatal in cases of systemic infection. Patients often have a history of occupational contact with animals or animal discharges or products. Anthrax has been occasionally reported in travellers and may be related to physical contact with dead animals in nature.81
The endospores can survive in the soil for decades under favourable conditions; they are resistant to drying, heat, gamma radiation and disinfectants.82 The microbe secretes several plasmid-mediated exo-toxins that are responsible for the oedema and necrosis, which occur during infection.83
Epidemiology
Anthrax infections are still endemic in parts of Africa, Asia, the Middle East, Central and South America and the Caribbean.7 Patients often have a history of occupational contact with animals or animal products in the endemic areas. It is encountered infrequently in travellers.
Clinical aspects
Cutaneous anthrax usually begins 3-5 days after inoculation of endospores of Bacillus anthracis. The cutaneous form accounts for 95% of the cases and primarily affects the exposed parts of the body, usually the forearm or the hand. There is usually a single lesion, but multiple lesions are also possible. The lesion starts as a painless papule at the inoculation site. The papule evolves into a haemorrhagic blister within 24-36 hours. The blister dries centrally and forms a haemorrhagic crust, the so-called malignant pustule. The involved area is rarely painful, The crust sloughs within a couple of weeks, leaving behind a shallow ulcer that heals by granulation.84
Diagnosis
If there is clinical suspicion of anthrax, a gram stain and culture should be performed on material from the blister or wound fluid from the ulcer base. However, the rate of positive culture does not exceed 60-65%, even before the use of antibiotics. A
proefschrift Zegelaars.indb 19 4-2-2008 9:22:16
20
biopsy should be taken for histological examination. Serologic testing is useful only retrospectively.85
Treatment
Cutaneous anthrax may be self-limiting. However, treatment is recommended to prevent life-threatening complications. Penicillin and doxycycline are used. In case of systemic involvement intravenous administration of penicillin G should be started as soon as possible. Therapy should be continued for at least 14 days after symptoms abate.82 Asymptomatic carriers may be treated with a six-week course of doxycycline or ciprofloxacin.
LeishmaniasisIntroduction
Cutaneous leishmaniases (CL) is one of the most important causes of chronic ulcers in some parts of the tropical World.86-89 It is caused by protozoan parasites belonging to the genus Leishmania, which are divided into two subgenera, L. (Viannia) spp. and L. (Leishmania) spp. Further classification is based on a variety of biochemical, immunological, and molecular criteria.90-92
In the New World CL is caused by at least eight different species, primarily of the L. (V.) braziliensis and L. (L.) mexicana complexes. Old World CL is caused by four species; L. major, L. tropica, L. aethiopica and L. infantum.93-96
The parasites are transmitted to humans via the bite of the female phlebotomine sand fly which has fed on an infected mammal. Of the sub-family Phlebotominae, the genera Phlebotomus in the Old World and Lutzomyia in the New World are known vectors.97;98
Epidemiology
The disease occurs throughout the tropical and the subtropical regions and is endemic in 88 countries. Old World CL is found in the Mediterranean, Northern Africa, the Sub-Saharan, the Middle East, and South-West Asia. New World CL extends from Southern Texas to the highlands of Northern Argentina; with 90% of cases of CL in Afghanistan, Algeria, Brazil, Iran, Peru, Saudi Arabia and Syria.In the past decades, there is a definite increase in the incidence of CL. This is because of several factors such as rural to urban migration as seen in Kabul, Afghanistan, development of new agro-industrial projects, re-locating non-immune community in endemic areas, movement of army troops into endemic regions and the termination
proefschrift Zegelaars.indb 20 4-2-2008 9:22:16

Chapter 1
Introduction and aim
s of the thesis
21
of insecticide spraying. Emerging of the disease in travellers is caused by the increase in eco-tourism to especially jungle areas in South and Middle America, with hotspots as Manu National Park in Peru, Madidi National Park the Tuichi river in Bolivia, and several areas in Costa Rica. HIV infection does not seem to increase the risk of CL infection, but may influence treatment response.99;100
It is estimated that 1 to 1.5 million cases of CL occur annually. 86 It is one of the 10 most frequent (skin) diseases encountered in travellers returning from tropical countries with an increased incidence.6;101-103
Clinical aspects
The clinical picture of CL varies with the endemic region and depends on the species involved, the immune status of the host, genetics and probably on the transmitting sand fly. A lesion may start as a papule or a nodule, which develops into an ulcer with or without a scab. At this stage most patients consult a physician. The lesions are usually painless; if painful there is generally a secondary infection present.Lesions caused by L. major are often nodular, nodulo-ulcerative and ulcerative. The lesions develop slowly over months and generally resolve in 6 months.104 Lesions caused by L. tropica may persist as an erythematous papule for more than a year. Presentation is often as nodulo-ulcerative plaques with a necrotic base and indurated margin that are frequently covered by a firm adherent crust.87;105-107 The time period for spontaneous resolution is not well known. It has been reported that leishmaniasis caused by L. tropica may affect the nose or the mouth as is seen in mucocutaneous leishmaniasis from the New World. However, this is probably because of direct extension from skin lesions rather than from the dissemination of the parasite.108;109
Skin lesions of the New World CL caused by species of the subgenus Leishmania will generally resolve even without treatment in 6 months, whereas lesions caused by the subgenus Viannia often do not resolve spontaneously. First a nodule develops, which then enlarges and eventually ulcerates.110 A nodular lymphangitis may be present.111 Mucocutaneous leishmaniasis, although uncommon, may develop in approximately 3-5% of the patients as a complication of New World CL caused by Leishmania (V.) braziliensis, but also occurs in infections with Leishmaniasis (V.) panamensis.112;113 Disseminated leishmaniasis has been reported as an emerging form of leishmaniasis in North-Eastern Brazil. It shows multiple pleomorphic lesions ranging from acneiform, papular, nodular and ulcerating lesions.114-116
proefschrift Zegelaars.indb 21 4-2-2008 9:22:16
22
Diagnosis
The initial diagnosis is based on the clinical picture and on the visit of the patient to an endemic area.117;118
Laboratory tests include histopathological examination of the biopsies taken from the ulcer border, direct smears from the ulcer border stained with Giemsa, culture of the material obtained by needle aspiration or by biopsy. If facilities are available, amplification of DNA using PCR may be used. None of the laboratory methods has a 100% sensitivity.119-121 Best results have been obtained by a combination of laboratory tests.122;123
Histopathological picture may range from a mixed inflammatory cell infiltrate with a large number of macrophages containing the Leishmania parasite, to a highly organized and predominantly epitheloid cell granuloma with very few demonstrable parasites.122;124 Identification of the parasite by PCR is important in areas where more than one species are present, especially in case of possible infection with L. vianna braziliensis. The choice and the duration of the treatment may depend on isolation of the specific species.
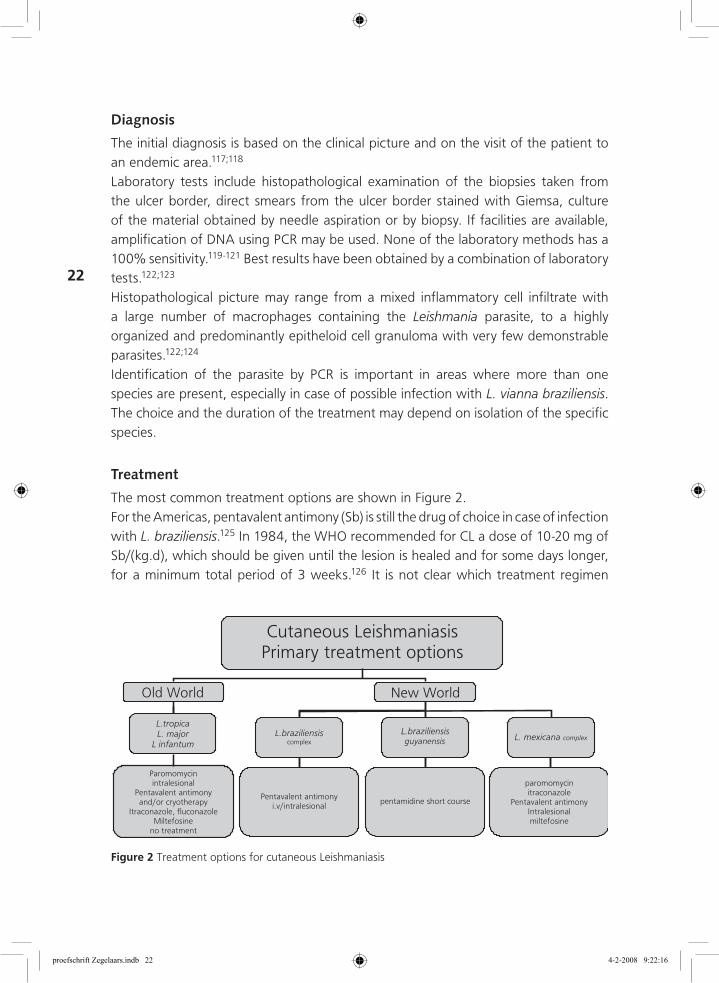
Treatment
The most common treatment options are shown in Figure 2. For the Americas, pentavalent antimony (Sb) is still the drug of choice in case of infection with L. braziliensis.125 In 1984, the WHO recommended for CL a dose of 10-20 mg of Sb/(kg.d), which should be given until the lesion is healed and for some days longer, for a minimum total period of 3 weeks.126 It is not clear which treatment regimen
Figure 2 Treatment options for cutaneous Leishmaniasis
proefschrift Zegelaars.indb 22 4-2-2008 9:22:16
Chapter 1
Introduction and aim
s of the thesis
23
should be used. In some areas very low cure rate was found with this recommended drug regime.127For some endemic areas, a lower dose of 10 mg of Sb /(kg.d) or for a shorter period may be sufficient.128 In areas where mucocutaneous Leishmaniasis is rare and when there are no clinical signs of dissemination of the disease, intralesional therapy with Sb without or in combination with cryotherapy has proven to be an effective and safe treatment in the New orld cutaneous leishmaniasis.129;130
Pentamidine is the drug of first choice in case of infection with L.(V.) guyanensis.127;131 As the risk of mucosal leishmaniasis is very low in the Old World cutaneous leishmaniasis, topical treatment is often used. Paromomycin ointment has shown to be effective in the treatment of cutaneous leishmaniasis caused by L major.132;133 Different studies reported good results with intralesional therapy with antimonials (sodium stibogluconate and meglumine antimonate).130;134;135 It was shown that intralesional therapy was more effectively combined with cryotherapy.136 Fluconazole 200 mg daily for 6 weeks showed good response in Iran caused by L. major.137 Ketoconazole was reported to be effective against L. major in Israel.138 No randomized, placebo-controlled clinical studies have been reported for L. tropica and L. infantum.. Thermotherapy was found to be effective in a randomized, controlled trial to treat cutaneous leishmaniasis caused by L. tropica in Afghanistan.139
Miltefosine is an alkyl-phosphocholine compound that is the first oral drug for treatment of visceral leishmaniasis.140 The drug may be promising in the treatment of severe cutaneous infection as well as in areas where mucosal leishmaniasis is prevalent.141;142
Subcutaneous mycosesSubcutaneous mycoses are characterized by a heterogeneous group of infections that often result from direct penetration of the fungus into the dermis and subcutaneous tissue through traumatic injury. This group of micro-organism is discussed in this chapter because it may cause ulceration of the skin. Subcutaneous mycoses are restricted to certain regions, travellers are seldom infected. Most cases are encountered in those living and working in an endemic area with little availability of health resources. The most common subcutaneous mycoses, which may show ulceration are sporotrichosis, chromo(blasto)mycosis and mycetoma. Only sporotrichosis has a single specific aetiological agent, whereas chromoblastomycosis and mycetoma are clinical syndromes with multiple fungal or bacterial aetiologies.
proefschrift Zegelaars.indb 23 4-2-2008 9:22:16
24
Sporotrichosis
Sporotrichosis is caused by Sporothrix schenckii, which is a dimorphic fungus that occurs in nature as a saprophyte in soil, decaying organic material and on surfaces of various plants. Infection results via traumatic inoculation of materials containing the fungus, particular wood splinters or thorns through the skin.143 Zoonotic transmission has been described.144;145 The organism is particularly found in warm temperate and humid tropical climates and is one of the most common subcutaneous mycoses.146;147
Epidemiology
Individuals with activities, which expose them to the environment are at risk. Several large outbreaks of the disease have been reported. In South Africa 3000 cases were reported among gold miners from 1941 to 1944. It was believed that the fungus was inoculated through the skin via splinters of contaminated timber.148;149 Sporothrichosis has a World Wide distribution. However, most cases at present are reported in South and Central America.
Clinical aspects
The incubation period is probably a few weeks. Sporothrichosis very rarely affects internal organs. It is mostly encountered as lymphocutaneous or sporothrichoid form or less common as a localized or fixed cutaneous form. The primary cutaneous lesions may appear as papular, nodular, or pustular lesions that develop into either a superficial ulcer or a verrucous plaque.150 During progression, the lymphocutaneous form shows multiple subcutaneous nodules that are formed along the course of the locally draining lymphatics (sporotrichoid spread). The localized form shows no lymphatic spread and is characterized by indurated or verrucous plaques and occasional ulcers. Dissemination is rare and usually encountered in immunodeficient individuals.151
Diagnosis
The initial clinical diagnosis may be confirmed by histopathological investigation and culture of the fungus. Primary lesions usually show prominent pseudoepitheliomatous hyperplasia. Fresh lesions show a non-specific inflammatory infiltrate composed of neutrophils, lymphocytes, plasma cells and histiocytes. Several types of granulomas including tuberculoid, histiocyte and supperative granulomas are observed within the dermis of older lesions. Fungal elements may be observed after PAS or haematoxylin and eosin staining. However, they are seldom found because of their small size,
proefschrift Zegelaars.indb 24 4-2-2008 9:22:16
Chapter 1
Introduction and aim
s of the thesis
25
varying shape and often low numbers.152 The finding of asteroid bodies which are mycotic cells surrounded by radiated, eosinophilic elongations is characteristic.Definite diagnosis depends on culturing the organism from pus or tissue. The organism grows within a week on all media commonly used in medical mycology.
Treatment
There are no randomized, comparative trials available for evaluating the treatment of sporotrichosis. The treatment of choice for fixed cutaneous or lymphocutaneous sporotrichosis is itraconazole, which was effective at a dose of 100-200 mg a day for 3 to 6 months.153;154 However, terbinafine has showed to be effectieve in a dose of 1000 mg a day after 12 – 24 weeks of treatment.155 It is generally accepted that potassium iodide is an effective therapy.156 Its mechanism of action is still not understood. In adults, the orally saturated solution of potassium iodide 3 times daily 5 drops, which is increased weekly by 5 drops until 40-50 drops at the time for 2-3 months, or for 1 month after the clinical and mycological cure is achieved, is recommended.157 Severe infection requires treatment with amphotericin B. Immunosuppressed patients respond poorly to potassium iodide, and treatment with amphotericin B or itraconazole is required.154
Chromo(blasto)mycosis
Chromoblastomycosis is a chronic (sub)cutaneous mycotic disease that occurs more frequently in tropical and sub-tropical areas and is caused by several dematiaceous (darkely pigmented) fungi of which Fonsecaea pedrosoi, Phialophora verrucosa and Cladophialophora carrionii are the main species.158;159 The disease is caused by saprophytic fungi that are found in soil and wood. It is a difficult-to-treat mycosis with low cure rates and a high rate of relapses.
Epidemiology
The disease is most prevalent in tropical and sub-tropical America and Africa.160 It has also been reported in several foci in the USA.161
Clinical aspects
The disease occurs typically on the foot or the leg. After inoculation of the fungus through the skin slowly growing scaly wart-like nodules develop and ulceration may also occur. Clinically, it may be indistinguishable from verrucous cutaneous tuberculosis and localised sporotrichosis. It grows slowly, is painless and lymphatic spread is only seen occasionally. Moderate itching is often mentioned.158 It seldom involves bones
proefschrift Zegelaars.indb 25 4-2-2008 9:22:16
26
and remains limited to the subcutaneous tissues. This may be relevant because scratching may contribute to inoculation of the fungus in adjacent areas. Scratching may also cause secondary infections, which is the most frequent complication of chromoblastomycosis. It occurs mainly in farmers and rural workers who work barefoot. 159
Diagnosis
Histological investigation is most important for diagnosis of chromoblastomycosis. Sclerotic bodies can be observed after haematoxylin-eosin staining of tissue biopsy or from fungal culture.158
Treatment
Surgery and antifungal therapy have been used in chromoblastomycosis, but results in advanced disease are disappointing.162
Mycetoma
Mycetoma is a chronic granulomatous infection of the skin and the subcutaneous tissue characterized by deformation and increased volume of the involved subcutaneous tissue and in the advanced stages causes the destruction of underlining bone structures.163 It is caused either by true fungi (eumycetoma) or filamentous bacteria (actinomycetoma). Nodules and openings of fistulae through which exudate containing grains, is noticed on the skin surface. The grains, also known as sclerotia, are aggregation of hyphae produced by some species of fungi or the bacterial filaments from aerobic actinomycetes. Mycetoma has also been called “Madura foot” because of the initial descriptions of the disease in the district Madura in India. In 1860 it was called mycetoma by Vandyke Carter who demonstrated its mycotic origin.164
Actinomycetic mycetoma is caused by aerobic species of the Actinomycetes group, such as Nocordia brasiliensis, Nocordia asteroids and Nocordia caviae, and the Streptomyces group, Streptomyces pelletieri, Streptomyces somaliensis and Actinomadura madurae. They are filamentous ramified bacteria that when cultured create colonies similar to fungi.165 The maduromycotic (eumycetic) mycetoma is caused by several fungi such as Madurella mycetomatis, Madurella grisea, Pseudallescheria boydii, etc.159
It is mainly a disease of the tropical climates and is more frequently seen in the rural areas where people work in farms under unprotected rudimentary conditions.163 Probably repeated punctures or abrasion of the skin are required for the inoculation of the organisms prior to the infection. The infection develops very slowly over the years.
proefschrift Zegelaars.indb 26 4-2-2008 9:22:17
Chapter 1
Introduction and aim
s of the thesis
27
Therefore, it is not likely to be encountered in travellers from tropical countries. Most cases encountered in the Western World are immigrants from endemic regions.
Epidemiology
Mycetoma is endemic in (sub)tropical regions with a low annual rainfall. These include parts of Central America, Venezuela, Brazil, Sudan, Somalia, Senegal, the Middle East, India, Pakistan and Bangladesh.165 Its true incidence is unknown. The disease is more frequently encountered in rural areas in where people are more exposed to contaminated soil.
Clinical aspects
Mycetoma is most often seen on the lower limbs (65-70%). However, any body region may be affected after exposure to the agent. Clinically, it is characterized by a slow progressive swelling, deformity of the tissue involved, nodular lesions and fistulae exudate containing grains. The incubation period is not exactly known and may range from several weeks to months.166
Diagnosis
Clinically, the diagnosis is suspected in the presence of an increased volume of the affected tissue, formation of abscesses and fistulae exudate containing grains. Histopathological investigation of the lesion is important for the diagnosis of mycetomas. The epidermis shows hyperkeratosis and hyperplasia of varying degree. There is an inflammatory infiltrate within the dermis, microabscesses with polymorphonuclear leukocytes, generally surrounded by many macrophages, plasma cells and lymphocytes. Granules are observed in the centre. Sometimes, tuberculoid granulomas are also observed. The giant cells that appear are of Langhans or foreign body type.167
Gram stained and potassium hydroxide preparations, may be used for direct observations. It is important to undertake cultures to identify the causal micro-organism. Secretions from fistulae and abscess or tissue biopsies can be used for culture in media to isolate the fungi or the bacteria. Identification is performed using their macroscopic and microscopic features.168
Treatment
Choice of treatment depends on the micro-organism involved and the extent of tissue invasion. Eumycetoma is very difficult to treat, surgery is still the most common
proefschrift Zegelaars.indb 27 4-2-2008 9:22:17

28
treatment in most cases.165;166 There are a few reports on treatment with ketoconazole and itraconazole.166
Actinomycetoma with Nocardia spp are treated with a combination of dapsone plus sulfametoxazole-trimethoprim and recently, amikacin for 2 to 3 years.165;169;170 As an alternative treatment amoxicillin-clavulanate has been reported.171
Summary
Patients with infectious ulcers that are endemic to the tropics occasionally present to dermatologists in the Western World. It is likely that the incidence of imported ulcers will rise because travel to and from tropical countries is becoming more frequent. Therefore it is important that physicians be familiar with the manifestations of such infections and that they be prepared to diagnose most common imported ulcers and treat these patients.
Non-infectiousSickle cell
Sickle cell disease is caused by an abnormality in the gene encoding the β chain of haemoglobin. When deoxygenated, sickle cell haemoglobin interacts hydrophobically with other haemoglobin molecules, it tends to aggregate and polymerize resulting in the characteristic sickle shape. The rigidity of these deformed cells contribute to the vaso-occlusive episodes that characterizes the acute crises in the disease. 172;173 Activation of both blood coagulation and platelets was reported in some studies. 174 It is uncertain whether hypercoagubility is the primary or the secondary event. The pathogenesis of leg ulceration in sickle cell is not completely understood. Abnormal adherence of the sickle cell to endothelial cells has been postulated to be important in the initiation and/or progression of vaso-occlusive events leading to infarction in the skin. Oedema appears to precede the onset of ulceration, although evidence for venous insufficiency has never been found in patients who have sickle cell disease and leg ulcers.175-177 The sickle cell ulcers are commonly seen in adult males with homozygous sickle cell disease (HbSS) and are unusual in patients with sickle cell haemoglobin-C disease (HbSC) as well as those with sickle cell beta+ thalassaemia.
Epidemiology Ulcers are a common cause of morbidity among African American and African Caribbean patients with homozygous sickle cell (SS) disease in whom prevalence of 75% have been reported.178 The reported incidence from Africa is much lower
proefschrift Zegelaars.indb 28 4-2-2008 9:22:17
Chapter 1
Introduction and aim
s of the thesis
29
and from 5%-9.6%.179 The reason for these differences is not known. However, age distribution of the population and genetic factors may play a role.180;181
Clinical aspects
Ulcers are more common in adult males with homozygous sickle cell disease and show more severe clinical manifestations than in those with heterozygous disease. The incidence is very low in children younger than 10 years and markedly increased for those older than 50 years.182 Ulcers persist for months to years, heal slowly and, often recur. Most ulcers are located in the ankle area over the medial or lateral malleoli.178 The size of the ulcers varies from a few millimetres to large circumferential ulcers. Ulceration is preceded by prodromal pain and is often spontaneous or after a minor trauma. The ulcer has a punched-out appearance with raised margins and a deep base. Radiographs often show some periostal reaction, which makes it difficult to rule out osteomyelitis.182;183 Secondary infection is found very often and may delay wound healing.184Pain is often very severe and probably the major problem. It has a great impact on the quality of life of these patients.185
Diagnosis
Diagnosis is established after clinical observation of a painful leg ulcer, mostly in the ankle area in patients with sickle cell anaemia. Pathological investigations show obstruction of vessels with intimal proliferation and neovascularization.178 Oedema is often present.177
Treatment
Leg ulcers caused by sickle cell anaemia are very recalcitrant. Many treatments have been promoted, although no controlled clinical trials are available.186 Oedema must be treated with compression bandages or elastic stockings. If unsuccessful, strict bed rest is effective. Secondary infection should be treated with systemic or topically applied antibiotics; after culture outcome when resistance pattern is known. Different wound dressings can be used. Hydrocolloid dressing can be used to initiate debridement. These dressings often relieve pain. Skin grafts using split-skin, or full-thickness punch grafts may be considered, but are not always effective. Hyperbaric oxygen therapy was postulated to be successful in leg ulcers, but no controlled studies in patients with sickle cell leg ulcers have been published.187 Hyperbaric oxygen showed no effect on the morphology of sickle cells in vitro.188 New therapies in sickle cell anaemia that interrupt the sickling process may be helpful.189
proefschrift Zegelaars.indb 29 4-2-2008 9:22:17
30
Vascular
Vascular disease seems to be generally rare in tropical countries.190 In the Western World chronic venous insufficiency is responsible for about 70% of the ulcers in the lower limbs.191-194 Studies in the tropics revealed a very low or no prevalence of vascular ulcers.8;195;196However, a study in Brazil in 1755 adults attending a university clinic for various reasons signs of chronic venous insufficiency were noted in 3.6%. This figure is comparable with that in the Western World.197
The incidence of arterial disease is still increasing in the Western World. It is expected that arterial disease will become more prevalent in the developing countries because people are converting to Western life style. Because vascular ulcers are not specific for tropical disease it will not further be discussed.
MalignantMost cases, which are seen are malignant transformations in chronic traumatized or inflamed skin as seen in chronic leg ulcers, particularly after burns. It has also been described in chronic plantar ulcers in patients of leprosy.198;199 Most common are squamous cell carcinoma (SCC), to a lesser extent basal cell carcinoma (BCC) and there are also some reports on sarcomas and melanomas associated with scars.200;201
Epidemiology
No data are available of malignant ulcerations in the skin as an imported disease. There are only a few studies available on this subject from tropical countries.195
The development of squamous cell carcinoma in traumatic scars seems to be most important. A large study in Nigeria showed a preponderance of SCC in the leg related to neglected, poorly managed and chronic ulcers or scars from burns or injuries. Malignant melanoma was found on the feet, dermatofibrosarcoma affected the trunk and Kaposi sarcoma affected the limbs. Basal cell carcinoma comprised only 2% of all skin cancers. Albino patients had a higher frequency of both SCC and BCC mostly on the head and the neck.202 A study performed in Malawi showed a surprisingly large number of malignancies in skin ulcers.195 It was reported that the prevalence of HIV disease, which is very high in this population may be responsible. A 3 to 5 fold increased risk of developing a non-melanoma skin cancer was reported in patients with AIDS.203;204, More aggressive types of both BCC and SCC were reported.205;206 Unique examples of burn scar ulcers are the Kangri burn cancer in India and the Kairo burn cancer in Japan. Both are a result of the use of hot coals in utensils applied to
proefschrift Zegelaars.indb 30 4-2-2008 9:22:17
Chapter 1
Introduction and aim
s of the thesis
31
the abdomen in order to provide heat. Many users of these devices develop SCC in the abdominal wall.207
Clinical aspects
Carcinomas that arises in repeatedly traumatized or chronically inflamed skin are called Marjolin’s ulcers after Jean-Nicolas Marjolin who in 1828 described malignant ulceration in burn scars. Today the term “Marjolin’s ulcer” is used to describe malignant tumours arising in many different types of cutaneous scars and chronic wounds, such as burn scars, chronic venous ulcers and pressure ulcers.208
Signs and symptoms associated with the development of the carcinoma include a change in the scar with the formation of a mass or an ulcer, possibly with increased pain, increasing discharge, foul odour and bleeding. These symptoms may be ascribed to the colonization of bacteria in these wounds. Mean latent periods with a range of between 8 and 63 years were reported.166 Burn scar cancer occurs in areas of full-thickness or deep non-grafted burns, and has a predilection for the extremities, specifically for flexion creases of the extremities, where blood supply is decreased and trauma is increased.209
Diagnosis
In all non-healing ulceration of the skin biopsy remains the most important definitive diagnostic aid. A biopsy should be obtained from any suspicious lesion or any chronic ulceration, especially those with any recent change in appearance.210
Treatment
The first choice of treatment is generally surgery, application of adjunctive measures such as radiotherapy, chemotherapy or the use of immunomodulatory drugs depend on histopathological findings, tumour site and size, level of invasion and other specific parameters. Enlarged regional nodes should be investigated first.211-213
Neuropathic
Neuropathy may be encountered in several diseases. Neuropathy caused by leprosy and diabetes mellitus is clinically most important. Leprosy is an infectious disease caused by Mycobacterium leprae, which mainly infects macrophages and Schwann cells. Nerve invasion is a unique characteristic of Mycobacterium leprae and results in nerve damage. This usually becomes chronic and results in nerve function loss. The so called reaction may occur during the course of the disease. These reactions are episodes of acute inflammation in which the skin and the nerves may be involved
proefschrift Zegelaars.indb 31 4-2-2008 9:22:17
32
resulting in further damage to nerves. It is estimated that 20-30% of the leprosy patients have foot problems due to loss of nerve function. As a result, injury to the skin and the deeper layer of especially the feet and the hands may occur. Diabetes mellitus was once considered to be a disease of the developed World. However it has become a Worldwide pandemic with two-thirds of the global diabetic population living in the developing countries.214 The burden of diabetes foot problems will therefore continue to increase in the coming years. However, diabetes is not a typical tropical disease and will therefore not be discussed in this chapter. This chapter will focus on one of the most common complications of neuropathy caused by leprosy, which is plantar ulcers.
Epidemiology
Leprosy is still endemic in Middle and South America, in Sub-Saharan Africa and in Asia from Iran to Indonesia, on some islands in the Pacific and in the Northern Territory of Australia. The most endemic countries with 85% of the leprosy patients are India, Brasil, Indonesia, Nepal, Mozambique, Madagascar, United Republic of Tanzania, Democratic Republic of the Congo and Central Africa.215
Clinical aspects
Damage of peripheral nerves causes function loss in the sensory, the motor and the autonomic nerve fibres. Damage to the common peroneal nerve at the side where the nerve passes around the neck of the fibula results in sensory loss of the lateral side of the leg and the dorsum of the foot. Impaired innervation of the peroneal muscles and dorsiflexors of the foot results in decreased dorsiflexion. This may result in a drop foot. Sensory loss in the sole of the foot occurs when the posterior tibial nerve is damaged, usually where it passes around the medial malleolus. Besides sensory loss, damage to the nerve also gives rise to paralysis of the intrinsic muscles of the foot resulting in a hollow foot and in clawed toes. Ulcers will occur were most pressure is applied, that is on the metatarsophalangeal heads, the PIP-joints and tip of the toes. During type-I (Reversal reaction) and type-II (Erythema Nodosum Leprosum) reaction, further damage to the nerves also may occur.
Diagnosis
Diagnosis is based on specific skin signs and nerve function-loss.Clinical examination of the foot may reveal changes in the shape of the foot. Sensory loss may be found by testing with monofilaments or with the two point discrimination test.216 Motor function should be assessed. Autonomic loss results in loss of sweating with dry skin. The presence of a plantar ulcer will result in a local
proefschrift Zegelaars.indb 32 4-2-2008 9:22:17
Chapter 1
Introduction and aim
s of the thesis
33
increase in temperature, which can be measured by thermometry or palpation on the dorsal side of the foot.217
Treatment
The basic treatment is relieving pressure on the ulcer by means of special footwear, plaster or bed rest.218 Necrotic tissue should be removed, either surgically or non-invasively if necessary. Pathogens should be ruled out by culture of tissue. Bone should be cultured if osteomyelitis is suspected. Choice of antibiotics should be based on the outcome of the culture. There are many wound dressings available. However, there is no single wound dressing which has proved to be superior to others.194
AquaticWater sports as scuba diving are popular among travellers to tropical countries. During such recreational activities there is a risk of contact with potentially dangerous sea creatures. The skin may be mechanically traumatized by punctures, and venom may be involved.219
Epidemiology
Epidemiological data are scarce. Most data are on life threatening severe envenomation.220;221
Clinical aspects
Trauma to the skin may be caused by stings (hydroids, Portuguese man-of-war, shells), puncture, suction wounds (cephalopods (Octopi)), abrasion and cuts (corals, fish spines).
Diagnosis
Ulcers may be traumatic or caused by punctures or lacerations and, secondary infection may occur. Pain is immediate after puncture by sting rays. Systemic reactions may occur.222 Barracudas (Sphyraena spp.) and moray eels may also strike if they are disturbed.223
Sea-urchin stings may produce injurious and venomous wounds. There are hundreds of species of the sea urchin. In some species the spines that are mostly located on the upper surface have poisonous tips. Envenomation may also be caused by the seizing organs (pedicellariae) on the lower surface. Pedicullarial stings are reported to be dangerous. However, there are little clinical data. People step on sea urchins or brush
proefschrift Zegelaars.indb 33 4-2-2008 9:22:17
34
against them. Puncture wounds may be numerous, pain is immediate and intense. The broken spines remain embedded or leave the skin unbroken. A “tattooing” pattern is frequently seen. Most of the fragments are absorbed after a while or eliminated through the epidermis. Destruction and synovitis may occur if the spines enter near a joint. The development of foreign body granulomas is a regular finding after such injuries in the skin.220;224
Treatment
Treatment is symptomatic. Several therapies are recommended by local people, but their use has never been reported in studies. It is recommended to rinse the wounds thoroughly with clean water. Vinegar may be used to inactivate nematocysts and isopropylalcohol should be used to disinfect.225 Antibiotic prophylaxis may be used. Wounds are self-limiting but secondary infection is not rare.226 Topical steroids may be useful for persistent inflammatory reactions 227.
TraumaticTraumatic wounds can be defined as a cutaneous lesion resulting from an acute exposure to energy (mechanical, thermal, electrical, chemical or radiant). Road traffic injuries and intentional injuries (self-inflicted injuries, interpersonal violence and war-related injuries) are most important causes of traumatic wounds.228
Epidemiology
Injury is a significant health problem throughout the World. Annually 5,168000 (9% of the total deaths) people die of violence, accidents or suicides and several thousand more are injured.229 By far the largest part of the total burden of injury, approximately 90%, occurs in low- and middle-income countries.230 The risk factors for road accidents are increasing in some developing countries; for example, motor vehicle ownership may double within five years clogging the streets and the highways with inadequately maintained vehicles.231 The global burden of disease because of road traffic injuries is expected to move from the ninth position in 1990 to the third position by 2020.232 It is also estimated that if low-and middle-income countries do not act immediately, up to 1% of a country’s gross domestic product will be consumed by road traffic injuries.233
proefschrift Zegelaars.indb 34 4-2-2008 9:22:17
Chapter 1
Introduction and aim
s of the thesis
35
Clinical aspects
The clinical picture depends on the response of the damaged tissue to trauma. Secondary factors such as arterial or venous flow, nutritional status of the patient, the presence of auto-immune diseases, medication, diabetes mellitus and smoking will also affect the clinical presentation.
Diagnosis
A carefully obtained medical history is most important in revealing the origin of the ulcer. Attention must be paid to other factors, which may negatively affect the healing. If the ulcer is traumatic in origin, it should be defined in terms of high impact, low impact, repetitive, temperature-related, caustic, radiation-induced, type of bite, presence of drug abuse, and so on. In chronic ulcers, the age of the wound is important because long-standing wounds can be malignant (Marjolin’s ulcer). Previous topical therapy to the ulcer should be delineated because certain topical agents can contribute to the ulcer’s chronicity (e.g. caustic agents such as hydrogen peroxide, 10% iodine, Dakin’s solution and so on) .
Treatment
In general traumatic wounds without damage to the underlying tissue should be treated conservatively. Necrotic tissue should be removed by surgery. The most important surgical step in treating any wound is to undertake adequate débridement to remove all foreign matter and unhealthy or nonviable tissue until the wound edges and base consist only of normal and healthy tissue. A chronic wound has to be converted by débridement to an acute wound, so that it can proceed through the normal healing phases. Deep tissue cultures should always be analyzed for pathogenic bacteria and to obtain sensitivities to potential therapeutic agents. In addition, the débrided tissue should be sent for pathological examination for confirming the specific diagnosis of osteomyelitis, vasculitis, or cancer.234
Aims of the thesisMany “tropical” doctors are familiar with slowly healing ulcers in travellers in or from tropical areas. No scientific studies have been published on this subject, but it is an observation by doctors working in the tropics or at outpatient clinics for tropical diseases in the western world. Various aspects of skin ulcers in patients in tropical areas or in travellers in and from such areas were investigated and are presented in this thesis.
proefschrift Zegelaars.indb 35 4-2-2008 9:22:17
36
Ulcers originating from the tropics show great variations. In the introduction an overview of the most frequently encountered wounds in travellers at an outpatient clinic in the western world is given. This overview is based on clinical experience and an extensive search of the literature. A guideline for clinicians dealing with “tropical ulcers” is also described.At our outpatient clinic for tropical and imported skin diseases, serious (ulcerating) pyodermas, especially in the lower leg, are regularly encountered in otherwise healthy individuals who have visited a tropical country. There are several factors that may influence the healing of these ulcers.Many of us are aware of oedema, which develops in the lower legs during travel, especially after arrival in tropics. It is well known that wound healing is delayed when oedema is present. In studies described in chapter 2, we hypothesized that in travellers to tropical areas, a change from temperate to hot humid climate may result in a subsequent change in the microcirculation of the dermal plexus. An adaptation to higher temperatures could lead to distension of dermal capillaries, which may cause oedema. In this study we determined the capillary filtration rate (CFR) as a measure for micro-oedema. Changes in tissue volume of the mid-calf caused by the CFR were calculated from changes in the diameter of the limb measured with a (mercury in rubber) strain gauge plethysmograph. The purpose of this study was to investigate whether CFR increased in travellers, who had recently arrived in the tropics from a temperate climate and thereby support the hypothesis that (micro)-oedema impairs wound healingIn studies in chapter 3, we focussed on the bacterial colonisation, the resistance of the bacteria to anti-bacterial agents and the aetiology of wounds encountered in tropical countries.Although chronic ulcers are an important cause of morbidity in tropical countries, in contrast to developed countries, little is known on the prevalence and the aetiology of skin ulcers. The prevalence and the aetiology of chronic skin ulcers was investigated in patients at the Queen Elizabeth Central Hospital (QECH) in Blantyre, Malawi in order to obtain further insight into this subject (chapter 4). Data on the history and physical examination were collected; on indication skin biopsies were taken for histological examination and bacterial cultures were set-up when infection was clinically suspected. In studies pursued in chapter 5, a hydrocolloid dressing was tested under tropical conditions. Hydrocolloid dressings are widely used for treating wounds. However, little is known on their tolerability and efficacy under tropical conditions. Besides the financial factors, alleged increase in the frequency of wound infection may be an important reason that these semi-occlusive dressings are not used regularly under these conditions. Therefore, a clinical study in which the tolerability and the efficacy
proefschrift Zegelaars.indb 36 4-2-2008 9:22:17
Chapter 1
Introduction and aim
s of the thesis
37
of a hydrocolloid dressing in the treatment of venous leg ulcers under the humid and hot conditions of tropical Suriname was performed.The import of skin ulcers caused by 2 emerging infectious diseases is described in chapters 6 and 7. Cutaneous leishmaniasis (CL) is seen as an imported skin disease, with a rising incidence in the last 20 years. It is highly endemic in some countries and travellers from these areas may be at risk. The clinical picture is diverse and may vary from one or more papules to ulcers with or without a scab. A previous Dutch study reported 49 patients with CL, in the period 1979-1989; Mediterranean countries were the most important source of infection. We were interested in investigating whether a change in this pattern had occurred in the subsequent years. The sensitivity of our diagnostic procedures, the mode of treatments and the results of treatment were examined. The incidence, the clinical picture, the treatment modalities and the response of patients diagnosed with CL from January 1990 to January 2000 at our hospital were retrospectively studied (chapter 6).A patient who developed a Buruli ulcer after travelling in the Shan Dong Province in the People’s Republic of China is described in chapter 7. It is the first reported case of Buruli ulcer in People’s Republic of China and proves that M. ulcerans infection is also present in the temperate climatic zone in the Northern Hemisphere.
Reference List 1. Ryan ET, Wilson ME, Kain KC. Illness after international travel. N.Engl.J Med 2002; 347: 505-
16.
2. Wilson ME. Skin problems in the traveler. Infect.Dis.Clin.North Am. 1998; 12: 471-88.
3. Wilson ME, Chen LH. Dermatologic Infectious Diseases in International Travelers. Curr.Infect.Dis.Rep. 2004; 6: 54-62.
4. Lucchina LC, Wilson ME, Drake LA. Dermatology and the recently returned traveler: infectious diseases with dermatologic manifestations. Int.J Dermatol. 1997; 36: 167-81.
5. Freedman DO, Weld LH, Kozarsky PE et al. Spectrum of disease and relation to place of exposure among ill returned travelers. N.Engl.J.Med. 2006; 354: 119-30.
6. Zeegelaar JE, Steketee WH, van Thiel PP et al. Changing pattern of imported cutaneous leishmaniasis in the Netherlands. Clin.Exp.Dermatol. 2005; 30: 1-5.
7. Lupi O, Madkan V, Tyring SK. Tropical dermatology: bacterial tropical diseases. J.Am.Acad.Dermatol. 2006; 54: 559-78.
8. Gupta SK, Shukla VK. Leg ulcers in the tropics. Int.J.Low Extrem.Wounds. 2002; 1: 58-61.
9. Oluwasanmi JO, Alao MO, Ofodile FA. Tropical ulcers. Plast.Reconstr.Surg. 1979; 64: 41-6.
10. Maddox JS, Ware JC, Dillon HC, Jr. The natural history of streptococcal skin infection: prevention with topical antibiotics. J Am.Acad.Dermatol. 1985; 13: 207-12.
11. Greene SL, Su WP, Muller SA. Ecthyma gangrenosum: report of clinical, histopathologic, and bacteriologic aspects of eight cases. J Am.Acad.Dermatol. 1984; 11: 781-7.
proefschrift Zegelaars.indb 37 4-2-2008 9:22:17
38
12. Dillon HC, Jr. Post-streptococcal glomerulonephritis following pyoderma. Rev.Infect.Dis. 1979; 1: 935-45.
13. Alausa OK, Montefiore D. Bacterial infections, sensitivity patterns, and chemotherapy among hospital patients in the tropics. Scand.J Infect.Dis. 1978; 10: 295-302.
14. Rotta J, Tikhomirov E. Streptococcal diseases worldwide: present status and prospects. Bull.World Health Organ 1987; 65: 769-77.
15. Mahe A, Prual A, Konate M et al. Skin diseases of children in Mali: a public health problem. Trans.R.Soc.Trop.Med Hyg. 1995; 89: 467-70.
16. Brahmadathan KN, Koshi G. Epidemiology of streptococcal pyoderma in an orphanage community of a tropical country. J Trop.Med Hyg. 1988; 91: 306-14.
17. Caumes E, Carriere J, Guermonprez G et al. Dermatoses associated with travel to tropical countries: a prospective study of the diagnosis and management of 269 patients presenting to a tropical disease unit. Clin.Infect.Dis. 1995; 20: 542-8.
18. Naafs B. Tropical holiday memories. Eur.J Dermatol. 1999; 9: 500-5.
19. Brahmadathan KN, Koshi G. Importance of group G streptococci in human pyogenic infections. J Trop.Med Hyg. 1989; 92: 35-8.
20. Suite M. Cutaneous infections in Trinidad. Int.J Dermatol. 1990; 29: 31-4.
21. Allen AM, Taplin D, Twigg L. Cutaneous streptococcal infections in Vietnam. Arch.Dermatol. 1971; 104: 271-80.
22. Sheagren JN. Staphylococcal infections of the skin and skin structures. Cutis 1985; 36: 2-6.
23. Bisno AL, Stevens DL. Streptococcal infections of skin and soft tissues. N.Engl.J Med 1996; 334: 240-5.
24. Lowy FD. Staphylococcus aureus infections. N.Engl.J Med 1998; 339: 520-32.
25. Martin JM, Green M. Group A streptococcus. Semin.Pediatr.Infect.Dis. 2006; 17: 140-8.
26. Basak S, Dutta SK, Gupta S et al. Bacteriology of wound infection: evaluation by surface swab and quantitative full thickness wound biopsy culture. J Indian Med Assoc. 1992; 90: 33-4.
27. Slater RA, Lazarovitch T, Boldur I et al. Swab cultures accurately identify bacterial pathogens in diabetic foot wounds not involving bone. Diabet.Med 2004; 21: 705-9.
28. Bill TJ, Ratliff CR, Donovan AM et al. Quantitative swab culture versus tissue biopsy: a comparison in chronic wounds. Ostomy.Wound.Manage. 2001; 47: 34-7.
29. Perry CR, Pearson RL, Miller GA. Accuracy of cultures of material from swabbing of the superficial aspect of the wound and needle biopsy in the preoperative assessment of osteomyelitis. J Bone Joint Surg.Am. 1991; 73: 745-9.
30. Nagaraju U, Bhat G, Kuruvila M et al. Methicillin-resistant Staphylococcus aureus in community-acquired pyoderma. Int.J Dermatol. 2004; 43: 412-4.
31. Zeegelaar IE, Langenberg W, Hu R et al. Tolerability and efficacy of hydrocolloid dressings in the treatment of venous leg ulcers under tropical conditions: an open prospective study. J Eur.Acad.Dermatol.Venereol. 2001; 15: 234-7.
32. Price JD, Harding JW. Flucloxacillin in the treatment of infectious conditions in children. Curr.Med Res.Opin. 1975; 3: 77-82.
33. Duncan JT. A clinical appraisal of flucloxacillin in the management of skin and soft tissue infections in Nigeria. J Int.Med Res. 1984; 12: 210-5.
proefschrift Zegelaars.indb 38 4-2-2008 9:22:18
Chapter 1
Introduction and aim
s of the thesis
39
34. Crofts HG. Flucloxacillin (floxapen) in the treatment of skin and upper respiratory tract infections. N.Z.Med J 1978; 87: 308-11.
35. Korting HC, Neubert U, Abeck D. Current antimicrobial susceptibility of cutaneous bacteria to first line antibiotics. Int.J Antimicrob.Agents 1998; 10: 165-8.
36. Moellering RC, Jr. Past, present, and future of antimicrobial agents. Am.J Med 1995; 99: 11S-8S.
37. Fung HB, Chang JY, Kuczynski S. A practical guide to the treatment of complicated skin and soft tissue infections. Drugs 2003; 63: 1459-80.
38. Staphylococcus aureus resistant to vancomycin--United States, 2002. MMWR Morb.Mortal.Wkly.Rep. 2002; 51: 565-7.
39. Winter GD, Scales JT. Effect of air drying and dressings on the surface of a wound. Nature 1963; 197: 91-2.
40. Hautmann G, Lotti T. Atypical mycobacterial infections of the skin. Dermatol.Clin. 1994; 12: 657-68.
41. Dodiuk-Gad R, Dyachenko P, Ziv M et al. Nontuberculous mycobacterial infections of the skin: A retrospective study of 25 cases. J.Am.Acad.Dermatol. 2007.
42. Portaels F. Epidemiology of mycobacterial diseases. Clin.Dermatol. 1995; 13: 207-22.
43. Wayne LG, Sramek HA. Agents of newly recognized or infrequently encountered mycobacterial diseases. Clin.Microbiol.Rev. 1992; 5: 1-25.
44. Street ML, Umbert-Millet IJ, Roberts GD et al. Nontuberculous mycobacterial infections of the skin. Report of fourteen cases and review of the literature. J Am.Acad.Dermatol. 1991; 24: 208-15.
45. Clancey JK. Mycobacterial skin ulcers in Uganda: description of a new mycobacterium (Mycobacterium buruli). J Pathol.Bacteriol. 1964; 88: 175-87.
46. Portaels F, Chemlal K, Elsen P et al. Mycobacterium ulcerans in wild animals. Rev.Sci.Tech. 2001; 20: 252-64.
47. Eddyani M, Ofori-Adjei D, Teugels G et al. Potential role for fish in transmission of Mycobacterium ulcerans disease (Buruli ulcer): an environmental study. Appl.Environ.Microbiol. 2004; 70: 5679-81.
48. Portaels F, Elsen P, Guimaraes-Peres A et al. Insects in the transmission of Mycobacterium ulcerans infection. Lancet 1999; 353: 986.
49. Marston BJ, Diallo MO, Horsburgh CR, Jr. et al. Emergence of Buruli ulcer disease in the Daloa region of Cote d’Ivoire. Am.J Trop.Med Hyg. 1995; 52: 219-24.
50. Debacker M, Aguiar J, Steunou C et al. Buruli ulcer recurrence, Benin. Emerg.Infect.Dis. 2005; 11: 584-9.
51. Amofah G, Bonsu F, Tetteh C et al. Buruli ulcer in Ghana: results of a national case search. Emerg.Infect.Dis. 2002; 8: 167-70.
52. Barker DJ. Epidemiology of Mycobacterium ulcerans infection. Trans.R.Soc.Trop.Med Hyg. 1973; 67: 43-50.
53. Semret M, Koromihis G, MacLean JD et al. Mycobacterium ulcerans infection (Buruli ulcer): first reported case in a traveler. Am.J Trop.Med Hyg. 1999; 61: 689-93.
54. Faber WR, Arias-Bouda LM, Zeegelaar JE et al. First reported case of Mycobacterium ulcerans infection in a patient from China. Trans.R.Soc.Trop.Med Hyg. 2000; 94: 277-9.
proefschrift Zegelaars.indb 39 4-2-2008 9:22:18
40
55. Evans MR, Mawdsley J, Bull R et al. Buruli ulcer in a visitor to London. Br.J Dermatol. 2003; 149: 907-9.
56. Ross BC, Johnson PD, Oppedisano F et al. Detection of Mycobacterium ulcerans in environmental samples during an outbreak of ulcerative disease. Appl.Environ.Microbiol. 1997; 63: 4135-8.
57. van der Werf TS, van der Graaf WT, Tappero JW et al. Mycobacterium ulcerans infection. Lancet 1999; 354: 1013-8.
58. Portaels, F. and Meyers, W. M. Buruli ulcer. 2006. In Imported skin diseases. Faber W.R., Hay R.J., Naafs B. ed Elsevier, Maarssen 2006.
59. Hayman J. Out of Africa: observations on the histopathology of Mycobacterium ulcerans infection. J Clin.Pathol. 1993; 46: 5-9.
60. Meyers WM, Shelly WM, Connor DH. Heat treatment of Mycobacterium ulcerans infections without surgical excision. Am.J Trop.Med Hyg. 1974; 23: 924-9.
61. Palomino JC, Obiang AM, Realini L et al. Effect of oxygen on growth of Mycobacterium ulcerans in the BACTEC system. J Clin.Microbiol. 1998; 36: 3420-2.
62. Roberts B, Hirst R. Immunomagnetic separation and PCR for detection of Mycobacterium ulcerans. J Clin.Microbiol. 1997; 35: 2709-11.
63. Ross BC, Marino L, Oppedisano F et al. Development of a PCR assay for rapid diagnosis of Mycobacterium ulcerans infection. J Clin.Microbiol. 1997; 35: 1696-700.
64. Stienstra Y, van der Werf TS, Guarner J et al. Analysis of an IS2404-based nested PCR for diagnosis of Buruli ulcer disease in regions of Ghana where the disease is endemic. J Clin.Microbiol. 2003; 41: 794-7.
65. Buruli ulcer disease. Wkly.Epidemiol.Rec. 2004; 79: 194-9.
66. Dega H, Bentoucha A, Robert J et al. Bactericidal activity of rifampin-amikacin against Mycobacterium ulcerans in mice. Antimicrob.Agents Chemother. 2002; 46: 3193-6.
67. Gluckman SJ. Mycobacterium marinum. Clin.Dermatol. 1995; 13: 273-6.
68. Lewis FM, Marsh BJ, von Reyn CF. Fish tank exposure and cutaneous infections due to Mycobacterium marinum: tuberculin skin testing, treatment, and prevention. Clin.Infect.Dis. 2003; 37: 390-7.
69. Chemlal K, Portaels F. Molecular diagnosis of nontuberculous mycobacteria. Curr.Opin.Infect.Dis. 2003; 16: 77-83.
70. Braback M, Riesbeck K, Forsgren A. Susceptibilities of Mycobacterium marinum to gatifloxacin, gemifloxacin, levofloxacin, linezolid, moxifloxacin, telithromycin, and quinupristin-dalfopristin (Synercid) compared to its susceptibilities to reference macrolides and quinolones. Antimicrob.Agents Chemother. 2002; 46: 1114-6.
71. Gimenez GR, Sanchez RS, Iban Ochoa RM et al. Fish tank granuloma: response to treatment with clarithromycin. J.Eur.Acad.Dermatol.Venereol. 1999; 12: 81-2.
72. Yates VM, Ormerod LP. Cutaneous tuberculosis in Blackburn district (U.K.): a 15-year prospective series, 1981-95. Br.J.Dermatol. 1997; 136: 483-9.
73. Beutner EH. Tuberculosis of the skin: historical perspectives on tuberculin and Bacille Calmette Guerin. Int.J.Dermatol. 1997; 36: 73-7.
74. Seckin D, Akpolat T, Ceyhan M et al. Polymerase chain reaction in cutaneous tuberculosis. Int.J.Dermatol. 1997; 36: 51-4.
75. Hofler W. Cutaneous diphtheria. Int.J Dermatol. 1991; 30: 845-7.
proefschrift Zegelaars.indb 40 4-2-2008 9:22:18
Chapter 1
Introduction and aim
s of the thesis
41
76. Wagner J, Ignatius R, Voss S et al. Infection of the skin caused by Corynebacterium ulcerans and mimicking classical cutaneous diphtheria. Clin.Infect.Dis. 2001; 33: 1598-600.
77. Pandit N, Yeshwanth M. Cutaneous diphtheria in a child. Int.J Dermatol. 1999; 38: 298-9.
78. Koopman JS, Campbell J. The role of cutaneous diphtheria infections in a diphtheria epidemic. J Infect.Dis. 1975; 131: 239-44.
79. Kjeldsen K, Simonsen O, Heron I. Immunity against diphtheria 25-30 years after primary vaccination in childhood. Lancet 1985; 1: 900-2.
80. de Benoist AC, White JM, Efstratiou A et al. Imported cutaneous diphtheria, United Kingdom. Emerg.Infect.Dis. 2004; 10: 511-3.
81. Van den EE, Van GA, Van EM. Cutaneous anthrax, Belgian traveler. Emerg.Infect.Dis. 2006; 12: 523-5.
82. Swartz MN. Recognition and management of anthrax--an update. N.Engl.J.Med. 2001; 345: 1621-6.
83. Dixon TC, Meselson M, Guillemin J et al. Anthrax. N.Engl.J.Med. 1999; 341: 815-26.
84. Sternbach G. The history of anthrax. J.Emerg.Med. 2003; 24: 463-7.
85. Shlyakhov E, Rubinstein E. Evaluation of the anthraxin skin test for diagnosis of acute and past human anthrax. Eur.J.Clin.Microbiol.Infect.Dis. 1996; 15: 242-5.
86. Desjeux P. Leishmaniasis. Public health aspects and control. Clin.Dermatol. 1996; 14: 417-23.
87. Uzun S, Uslular C, Yucel A et al. Cutaneous leishmaniasis: evaluation of 3,074 cases in the Cukurova region of Turkey. Br.J Dermatol. 1999; 140: 347-50.
88. Rowland M, Munir A, Durrani N et al. An outbreak of cutaneous leishmaniasis in an Afghan refugee settlement in north-west Pakistan. Trans.R.Soc.Trop.Med Hyg. 1999; 93: 133-6.
89. Brooker S, Mohammed N, Adil K et al. Leishmaniasis in refugee and local Pakistani populations. Emerg.Infect.Dis. 2004; 10: 1681-4.
90. Cupolillo E, Aguiar AF, Brahim LR et al. Recent advances in the taxonomy of the New World leishmanial parasites. Med Microbiol.Immunol.(Berl) 2001; 190: 57-60.
91. Cupolillo E, Brahim LR, Toaldo CB et al. Genetic polymorphism and molecular epidemiology of Leishmania (Viannia) braziliensis from different hosts and geographic areas in Brazil. J Clin.Microbiol. 2003; 41: 3126-32.
92. Marfurt J, Niederwieser I, Makia ND et al. Diagnostic genotyping of Old and New World Leishmania species by PCR-RFLP. Diagn.Microbiol.Infect.Dis. 2003; 46: 115-24.
93. Cupolillo E, Momen H, Grimaldi G, Jr. Genetic diversity in natural populations of New World Leishmania. Mem.Inst.Oswaldo Cruz 1998; 93: 663-8.
94. Lainson R, Shaw JJ. The laboratory mix-up of Leishmania strains. Trans.R.Soc.Trop.Med Hyg. 1990; 84: 753.
95. Shaw JJ. Taxonomy of the genus Leishmania: present and future trends and their implications. Mem.Inst.Oswaldo Cruz 1994; 89: 471-8.
96. Rioux JA, Lanotte G, Serres E et al. Taxonomy of Leishmania. Use of isoenzymes. Suggestions for a new classification. Ann.Parasitol.Hum.Comp 1990; 65: 111-25.
97. Killick-Kendrick R. Phlebotomine vectors of the leishmaniases: a review. Med Vet.Entomol. 1990; 4: 1-24.
proefschrift Zegelaars.indb 41 4-2-2008 9:22:18
42
98. Killick-Kendrick R. The biology and control of phlebotomine sand flies. Clin.Dermatol. 1999; 17: 279-89.
99. Guiguemde RT, Sawadogo OS, Bories C et al. Leishmania major and HIV co-infection in Burkina Faso. Trans.R.Soc.Trop.Med Hyg. 2003; 97: 168-9.
100. Desjeux P. Leishmaniasis: current situation and new perspectives. Comp Immunol.Microbiol.Infect.Dis. 2004; 27: 305-18.
101. El Hajj L, Thellier M, Carriere J et al. Localized cutaneous leishmaniasis imported into Paris: a review of 39 cases. Int.J Dermatol. 2004; 43: 120-5.
102. Harms G, Schonian G, Feldmeier H. Leishmaniasis in Germany. Emerg.Infect.Dis. 2003; 9: 872-5.
103. Schwartz E, Hatz C, Blum J. New world cutaneous leishmaniasis in travellers. Lancet Infect.Dis. 2006; 6: 342-9.
104. Uthman MA, Satir AA, Tabbara KS. Clinical and histopathological features of zoonotic cutaneous leishmaniasis in Saudi Arabia. J Eur.Acad.Dermatol.Venereol. 2005; 19: 431-6.
105. Jacobson RL, Eisenberger CL, Svobodova M et al. Outbreak of cutaneous leishmaniasis in northern Israel. J Infect.Dis. 2003; 188: 1065-73.
106. Al Tawfiq JA, AbuKhamsin A. Cutaneous leishmaniasis: a 46-year study of the epidemiology and clinical features in Saudi Arabia (1956-2002). Int.J Infect.Dis. 2004; 8: 244-50.
107. Sharma NL, Mahajan VK, Kanga A et al. Localized cutaneous leishmaniasis due to Leishmania donovani and Leishmania tropica: preliminary findings of the study of 161 new cases from a new endemic focus in himachal pradesh, India. Am.J Trop.Med Hyg. 2005; 72: 819-24.
108. Barnetson RS, Ridley RS, Wheate HW. A form of muco-cutaneous leishmaniasis in the Old World. Trans.R.Soc.Trop.Med Hyg. 1978; 72: 516-8.
109. Morsy TA, Khalil NM, Salama MM et al. Mucosal leishmaniasis caused by Leishmania tropica in Saudi Arabia. J Egypt.Soc.Parasitol. 1995; 25: 73-9.
110. Oliveira CC, Lacerda HG, Martins DR et al. Changing epidemiology of American cutaneous leishmaniasis (ACL) in Brazil: a disease of the urban-rural interface. Acta Trop. 2004; 90: 155-62.
111. Romero GA, Ishikawa E, Cupolillo E et al. The rarity of infection with Leishmania (Viannia) braziliensis among patients from the Manaus region of Amazonas state, Brazil, who have cutaneous leishmaniasis. Ann.Trop.Med Parasitol. 2002; 96: 131-6.
112. Corredor A, Kreutzer RD, Tesh RB et al. Distribution and etiology of leishmaniasis in Colombia. Am.J Trop.Med Hyg. 1990; 42: 206-14.
113. Velez I, Agudelo S, Robledo S et al. Diffuse cutaneous leishmaniasis with mucosal involvement in Colombia, caused by an enzymatic variant of Leishmania panamensis. Trans.R.Soc.Trop.Med Hyg. 1994; 88: 199.
114. Turetz ML, Machado PR, Ko AI et al. Disseminated leishmaniasis: a new and emerging form of leishmaniasis observed in northeastern Brazil. J Infect.Dis. 2002; 186: 1829-34.
115. Silveira FT, Lainson R, Corbett CE. Clinical and immunopathological spectrum of American cutaneous leishmaniasis with special reference to the disease in Amazonian Brazil: a review. Mem.Inst.Oswaldo Cruz 2004; 99: 239-51.
116. Silveira FT, Lainson R, Corbett CE. Further observations on clinical, histopathological, and immunological features of borderline disseminated cutaneous leishmaniasis caused by Leishmania (Leishmania) amazonensis. Mem.Inst.Oswaldo Cruz 2005; 100: 525-34.
proefschrift Zegelaars.indb 42 4-2-2008 9:22:18
Chapter 1
Introduction and aim
s of the thesis
43
117. Reithinger R, Aadil K, Hami S et al. Cutaneous leishmaniasis, northern Afghanistan. Emerg.Infect.Dis. 2004; 10: 966-7.
118. Magill AJ. Epidemiology of the leishmaniases. Dermatol.Clin. 1995; 13: 505-23.
119. Navin TR, Arana FE, de Merida AM et al. Cutaneous leishmaniasis in Guatemala: comparison of diagnostic methods. Am.J Trop.Med Hyg. 1990; 42: 36-42.
120. De Bruijn MH, Barker DC. Diagnosis of New World leishmaniasis: specific detection of species of the Leishmania braziliensis complex by amplification of kinetoplast DNA. Acta Trop. 1992; 52: 45-58.
121. Weigle KA, de Davalos M, Heredia P et al. Diagnosis of cutaneous and mucocutaneous leishmaniasis in Colombia: a comparison of seven methods. Am.J Trop.Med Hyg. 1987; 36: 489-96.
122. Kalter DC. Laboratory tests for the diagnosis and evaluation of leishmaniasis. Dermatol.Clin. 1994; 12: 37-50.
123. Faber WR, Oskam L, van Gool T et al. Value of diagnostic techniques for cutaneous leishmaniasis. J Am.Acad.Dermatol. 2003; 49: 70-4.
124. Sarantopoulos GP, Binder S, Wortmann G et al. Old world cutaneous leishmaniasis in Los Angeles: a case report, overview of the current literature, and guide for the treating dermatopathologist. Am.J Dermatopathol. 2003; 25: 321-6.
125. Herwaldt BL, Berman JD. Recommendations for treating leishmaniasis with sodium stibogluconate (Pentostam) and review of pertinent clinical studies. Am.J Trop.Med Hyg. 1992; 46: 296-306.
126. World Health Organisation. The leishmaniasis. WHO technical report series. Geneva: WHO. Vol 701. 1984.
127. Romero GA, Guerra MV, Paes MG et al. Comparison of cutaneous leishmaniasis due to Leishmania (Viannia) braziliensis and L. (V.) guyanensis in Brazil: therapeutic response to meglumine antimoniate. Am.J Trop.Med Hyg. 2001; 65: 456-65.
128. Oliveira-Neto MP, Schubach A, Mattos M et al. Treatment of American cutaneous leishmaniasis: a comparison between low dosage (5 mg/kg/day) and high dosage (20 mg/kg/day) antimony regimens. Pathol.Biol.(Paris) 1997; 45: 496-9.
129. Oliveira-Neto MP, Schubach A, Mattos M et al. Intralesional therapy of American cutaneous leishmaniasis with pentavalent antimony in Rio de Janeiro, Brazil- -an area of Leishmania (V.) braziliensis transmission. Int.J Dermatol. 1997; 36: 463-8.
130. Blum J, Desjeux P, Schwartz E et al. Treatment of cutaneous leishmaniasis among travellers. J Antimicrob.Chemother. 2004; 53: 158-66.
131. Lai AFE, Vrede MA, Soetosenojo RM et al. Pentamidine, the drug of choice for the treatment of cutaneous leishmaniasis in Surinam. Int.J Dermatol. 2002; 41: 796-800.
132. El Safi SH, Murphy AG, Bryceson AD et al. A double-blind clinical trial of the treatment of cutaneous leishmaniasis with paromomycin ointment. Trans.R.Soc.Trop.Med Hyg. 1990; 84: 690-1.
133. El On J, Halevy S, Grunwald MH et al. Topical treatment of Old World cutaneous leishmaniasis caused by Leishmania major: a double-blind control study. J Am.Acad.Dermatol. 1992; 27: 227-31.
134. Gurei MS, Tatli N, Ozbilge H et al. Efficacy of cryotherapy and intralesional pentostam in treatment of cutaneous leishmaniasis. J Egypt.Soc.Parasitol. 2000; 30: 169-76.
proefschrift Zegelaars.indb 43 4-2-2008 9:22:18
44
135. Faris RM, Jarallah JS, Khoja TA et al. Intralesional treatment of cutaneous leishmaniasis with sodium stibogluconate antimony. Int.J Dermatol. 1993; 32: 610-2.
136. Asilian A, Sadeghinia A, Faghihi G et al. Comparative study of the efficacy of combined cryotherapy and intralesional meglumine antimoniate (Glucantime) vs. cryotherapy and intralesional meglumine antimoniate (Glucantime) alone for the treatment of cutaneous leishmaniasis. Int.J Dermatol. 2004; 43: 281-3.
137. Alrajhi AA, Ibrahim EA, De Vol EB et al. Fluconazole for the treatment of cutaneous leishmaniasis caused by Leishmania major. N.Engl.J Med 2002; 346: 891-5.
138. Weinrauch L, Livshin R, El On J. Ketoconazole in cutaneous leishmaniasis. Br.J Dermatol. 1987; 117: 666-8.
139. Reithinger R, Mohsen M, Wahid M et al. Efficacy of thermotherapy to treat cutaneous leishmaniasis caused by Leishmania tropica in Kabul, Afghanistan: a randomized, controlled trial. Clin.Infect.Dis. 2005; 40: 1148-55.
140. Berman J. Miltefosine to treat leishmaniasis. Expert.Opin.Pharmacother. 2005; 6: 1381-8.
141. Soto J, Soto P. Miltefosine: oral treatment of leishmaniasis. Expert.Rev.Anti.Infect.Ther. 2006; 4: 177-85.
142. Soto J, Toledo J, Valda L et al. Treatment of Bolivian mucosal leishmaniasis with miltefosine. Clin.Infect.Dis. 2007; 44: 350-6.
143. De Araujo T, Marques AC, Kerdel F. Sporotrichosis. Int.J Dermatol. 2001; 40: 737-42.
144. Barros MB, Schubach AO, do Valle AC et al. Cat-transmitted sporotrichosis epidemic in Rio de Janeiro, Brazil: description of a series of cases. Clin.Infect.Dis. 2004; 38: 529-35.
145. Schubach A, Schubach TM, Barros MB et al. Cat-transmitted sporotrichosis, Rio de Janeiro, Brazil. Emerg.Infect.Dis. 2005; 11: 1952-4.
146. da Rosa AC, Scroferneker ML, Vettorato R et al. Epidemiology of sporotrichosis: a study of 304 cases in Brazil. J Am.Acad.Dermatol. 2005; 52: 451-9.
147. Neyra E, Fonteyne PA, Swinne D et al. Epidemiology of human sporotrichosis investigated by amplified fragment length polymorphism. J Clin.Microbiol. 2005; 43: 1348-52.
148. Bustamante B, Campos PE. Endemic sporotrichosis. Curr.Opin.Infect.Dis. 2001; 14: 145-9.
149. Quintal D. Sporotrichosis infection on mines of the Witwatersrand. J Cutan.Med Surg. 2000; 4: 51-4.
150. Werner AH, Werner BE. Sporotrichosis in man and animal. Int.J Dermatol. 1994; 33: 692-700.
151. Carvalho MT, de Castro AP, Baby C et al. Disseminated cutaneous sporotrichosis in a patient with AIDS: report of a case. Rev.Soc.Bras.Med Trop. 2002; 35: 655-9.
152. Bullpitt P, Weedon D. Sporotrichosis: a review of 39 cases. Pathology 1978; 10: 249-56.
153. Winn RE, Anderson J, Piper J et al. Systemic sporotrichosis treated with itraconazole. Clin.Infect.Dis. 1993; 17: 210-7.
154. Conti D, I, Civila E, Gezuele E et al. Treatment of human cutaneous sporotrichosis with itraconazole. Mycoses 1992; 35: 153-6.
155. Chapman SW, Pappas P, Kauffmann C et al. Comparative evaluation of the efficacy and safety of two doses of terbinafine (500 and 1000 mg day(-1)) in the treatment of cutaneous or lymphocutaneous sporotrichosis. Mycoses 2004; 47: 62-8.
proefschrift Zegelaars.indb 44 4-2-2008 9:22:18
Chapter 1
Introduction and aim
s of the thesis
45
156. Cabezas C, Bustamante B, Holgado W et al. Treatment of cutaneous sporotrichosis with one daily dose of potassium iodide. Pediatr.Infect.Dis.J 1996; 15: 352-4.
157. Kauffman CA. Old and new therapies for sporotrichosis. Clin.Infect.Dis. 1995; 21: 981-5.
158. Bonifaz A, Carrasco-Gerard E, Saul A. Chromoblastomycosis: clinical and mycologic experience of 51 cases. Mycoses 2001; 44: 1-7.
159. Lupi O, Tyring SK, McGinnis MR. Tropical dermatology: fungal tropical diseases. J Am.Acad.Dermatol. 2005; 53: 931-51, quiz.
160. Rivitti EA, Aoki V. Deep fungal infections in tropical countries. Clin.Dermatol. 1999; 17: 171-90.
161. Howles JK, Kennedy CB, Garvin WH et al. Chromoblastomycosis: report of nine cases from a single area in Louisiana. AMA.Arch.Derm.Syphilol. 1954; 69: 83-90.
162. Bonifaz A, Paredes-Solis V, Saul A. Treating chromoblastomycosis with systemic antifungals. Expert.Opin.Pharmacother. 2004; 5: 247-54.
163. Magana M, Magana-Garcia M. Mycetoma. Dermatol.Clin. 1989; 7: 203-17.
164. McGinnis MR. Mycetoma. Dermatol.Clin. 1996; 14: 97-104.
165. Lichon V, Khachemoune A. Mycetoma : a review. Am.J.Clin.Dermatol. 2006; 7: 315-21.
166. Fahal AH. Mycetoma: a thorn in the flesh. Trans.R.Soc.Trop.Med Hyg. 2004; 98: 3-11.
167. Fahal AH, Sharfi AR, Sheik HE et al. Internal fistula formation: an unusual complication of mycetoma. Trans.R.Soc.Trop.Med.Hyg. 1996; 90: 550-2.
168. Fahal AH, Hassan MA. Mycetoma. Br.J.Surg. 1992; 79: 1138-41.
169. Welsh O, Salinas MC, Rodriguez MA. Treatment of eumycetoma and actinomycetoma. Curr.Top.Med Mycol. 1995; 6: 47-71.
170. Welsh O. Mycetoma. Current concepts in treatment. Int.J Dermatol. 1991; 30: 387-98.
171. Bonifaz A, Flores P, Saul A et al. Treatment of actinomycetoma due to Nocardia spp. with amoxicillin-clavulanate. Br.J.Dermatol. 2007; 156: 308-11.
172. Bunn HF. Pathogenesis and treatment of sickle cell disease. N.Engl.J Med 1997; 337: 762-9.
173. Steinberg MH. Management of sickle cell disease. N.Engl.J Med 1999; 340: 1021-30.
174. Ataga KI, Orringer EP. Hypercoagulability in sickle cell disease: a curious paradox. Am.J Med 2003; 115: 721-8.
175. Gniadecka M, Gniadecki R, Serup J et al. Microvascular reactions to postural changes in patients with sickle cell anaemia. Acta Derm.Venereol. 1994; 74: 191-3.
176. Billett HH, Patel Y, Rivers SP. Venous insufficiency is not the cause of leg ulcers in sickle cell disease. Am.J Hematol. 1991; 37: 133-4.
177. Clare A, FitzHenley M, Harris J et al. Chronic leg ulceration in homozygous sickle cell disease: the role of venous incompetence. Br.J Haematol. 2002; 119: 567-71.
178. Serjeant GR. The clinical features in adults sickle cell anaemia in Jamaica. West Indian Med J 1970; 19: 1-8.
179. Durosinmi MA, Gevao SM, Esan GJ. Chronic leg ulcers in sickle cell disease: experience in Ibadan, Nigeria. Afr J Med Med Sci. 1991; 20: 11-4.
180. Konotey-Ahulu FI. Maintenance of high sickling rate in Africa--role of polygamy. J Trop.Med Hyg. 1970; 73: 19-21.
proefschrift Zegelaars.indb 45 4-2-2008 9:22:18
46
181. Serjeant G, Gueri M. Sickle cell trait and leg ulceration. Br.Med J 1970; 1: 820.
182. Koshy M, Entsuah R, Koranda A et al. Leg ulcers in patients with sickle cell disease. Blood 1989; 74: 1403-8.
183. Serjeant GR. Leg ulceration in sickle cell anemia. Arch.Intern.Med 1974; 133: 690-4.
184. Baum KF, MacFarlane DE, Maude GH et al. Topical antibiotics in chronic sickle cell leg ulcers. Trans.R.Soc.Trop.Med Hyg. 1987; 81: 847-9.
185. Phillips T, Stanton B, Provan A et al. A study of the impact of leg ulcers on quality of life: financial, social, and psychologic implications. J Am.Acad.Dermatol. 1994; 31: 49-53.
186. Chung C, Cackovic M, Kerstein MD. Leg ulcers in patients with sickle cell disease. Adv.Wound.Care 1996; 9: 46-50.
187. Hammarlund C, Sundberg T. Hyperbaric oxygen reduced size of chronic leg ulcers: a randomized double-blind study. Plast.Reconstr.Surg. 1994; 93: 829-33.
188. Mychaskiw G, Woodyard SA, Brunson CD et al. In vitro effects of hyperbaric oxygen on sickle cell morphology. J Clin.Anesth. 2001; 13: 255-8.
189. Vichinsky E. New therapies in sickle cell disease. Lancet 2002; 360: 629-31.
190. Cheng SW, Wong J. Chronic venous insufficiency in a Chinese population: an anatomic and functional study by continuous-wave Doppler and photoplethysmography. Ann.Vasc.Surg. 1995; 9: 274-9.
191. Bergqvist D, Lindholm C, Nelzen O. Chronic leg ulcers: the impact of venous disease. J.Vasc.Surg. 1999; 29: 752-5.
192. Evans CJ, Fowkes FG, Ruckley CV et al. Prevalence of varicose veins and chronic venous insufficiency in men and women in the general population: Edinburgh Vein Study. J.Epidemiol.Community Health 1999; 53: 149-53.
193. Kurz X, Kahn SR, Abenhaim L et al. Chronic venous disorders of the leg: epidemiology, outcomes, diagnosis and management. Summary of an evidence-based report of the VEINES task force. Venous Insufficiency Epidemiologic and Economic Studies. Int.Angiol. 1999; 18: 83-102.
194. Mekkes JR, Loots MA, van der Wal AC et al. Causes, investigation and treatment of leg ulceration. Br.J.Dermatol. 2003; 148: 388-401.
195. Zeegelaar JE, Stroink AC, Steketee WH et al. Etiology and incidence of chronic ulcers in Blantyre, Malawi. Int.J.Dermatol. 2006; 45: 933-6.
196. Abbade LP, Lastoria S. Venous ulcer: epidemiology, physiopathology, diagnosis and treatment. Int.J.Dermatol. 2005; 44: 449-56.
197. Maffei FH, Magaldi C, Pinho SZ et al. Varicose veins and chronic venous insufficiency in Brazil: prevalence among 1755 inhabitants of a country town. Int.J.Epidemiol. 1986; 15: 210-7.
198. Grauwin MY, Mane I, Cartel JL. [Tumoral proliferations in chronic plantar ulcers: how to treat?]. Acta Leprol. 1996; 10: 101-4.
199. Kontochristopoulos G, Kyriakis K, Symeonidou S et al. Squamous cell carcinoma in chronic trophic ulcers of leprosy patients. J.Eur.Acad.Dermatol.Venereol. 2000; 14: 230-1.
200. Alconchel MD, Olivares C, Alvarez R. Squamous cell carcinoma, malignant melanoma and malignant fibrous histiocytoma arising in burn scars. Br.J.Dermatol. 1997; 137: 793-8.
201. Oluwasanmi JO, Ofodile FA, Abioye AA. Neoplastic change in chronic leg ulcer. Int.Surg. 1982; 67: 407-8.
proefschrift Zegelaars.indb 46 4-2-2008 9:22:19
Chapter 1
Introduction and aim
s of the thesis
47
202. Yakubu A, Mabogunje OA. Skin cancer in Zaria, Nigeria. Trop.Doct. 1995; 25 Suppl 1: 63-7.
203. Wilkins K, Turner R, Dolev JC et al. Cutaneous malignancy and human immunodeficiency virus disease. J.Am.Acad.Dermatol. 2006; 54: 189-206.
204. Goedert JJ, Cote TR, Virgo P et al. Spectrum of AIDS-associated malignant disorders. Lancet 1998; 351: 1833-9.
205. Sitz KV, Keppen M, Johnson DF. Metastatic basal cell carcinoma in acquired immunodeficiency syndrome-related complex. JAMA 1987; 257: 340-3.
206. Nguyen P, Vin-Christian K, Ming ME et al. Aggressive squamous cell carcinomas in persons infected with the human immunodeficiency virus. Arch.Dermatol. 2002; 138: 758-63.
207. Chowdri NA, Darzi MA. Postburn scar carcinomas in Kashmiris. Burns 1996; 22: 477-82.
208. Abbas JS, Beecham JE. Burn wound carcinoma: case report and review of the literature. Burns Incl.Therm.Inj. 1988; 14: 222-4.
209. Novick M, Gard DA, Hardy SB et al. Burn scar carcinoma: a review and analysis of 46 cases. J.Trauma 1977; 17: 809-17.
210. Engler HS, fernandez A, Bliven FE et al. Cancer arisng in scars of old burns and in chronic osteomyelitis, ulcers, anddrainage sites. Surgery 1964; 55: 654-64.
211. Copcu E, Aktas A, Sisman N et al. Thirty-one cases of Marjolin’s ulcer. Clin.Exp.Dermatol. 2003; 28: 138-41.
212. Esther RJ, Lamps L, Schwartz HS. Marjolin ulcers: secondary carcinomas in chronic wounds. J.South.Orthop.Assoc. 1999; 8: 181-7.
213. Phillips TJ, Salman SM, Bhawan J et al. Burn scar carcinoma. Diagnosis and management. Dermatol.Surg. 1998; 24: 561-5.
214. gogo-Jack S. Primary prevention of type-2 diabetes in developing countries. J.Natl.Med.Assoc. 2006; 98: 415-9.
215. Faber, W. R., Hay, R. J., and Naafs, B. imported skin diseases. chapter 7, Leprosy. 2006. Elsevier, Maarsen 2006.
216. Naafs B, Dagne T. Sensory testing: a sensitive method in the follow-up of nerve involvement. Int.J.Lepr.Other Mycobact.Dis. 1977; 45: 364-8.
217. Hoeksma AF, Faber WR. Assessment of skin temperature by palpation in leprosy patients: interobserver reliability and correlation with infrared thermometry. Int.J.Lepr.Other Mycobact.Dis. 2000; 68: 65-7.
218. Coleman WC, Brand PW, Birke JA. The total contact cast. A therapy for plantar ulceration on insensitive feet. J.Am.Podiatry.Assoc. 1984; 74: 548-52.
219. Auerbach PS. Marine envenomations. N.Engl.J Med 1991; 325: 486-93.
220. Fenner PJ, Williamson JA. Worldwide deaths and severe envenomation from jellyfish stings. Med J Aust. 1996; 165: 658-61.
221. de Pender AM, Winkel KD, Ligthelm RJ. A probable case of Irukandji syndrome in Thailand. J.Travel.Med. 2006; 13: 240-3.
222. Fenner PJ. Stingray envenomation: a suggested new treatment. Med J Aust. 1995; 163: 655.
223. Auerbach PS. Hazardous marine animals. Emerg.Med Clin.North Am. 1984; 2: 531-44.
224. Gaastra, M. T. W. Aquatic skin disorders. Faber, W. R. and Hay, R. J. Imported skin diseases. 279-289. 2006. Elsevier gezondheidszorg, Maarssen 2006.
proefschrift Zegelaars.indb 47 4-2-2008 9:22:19
48
225. Auerbach PS. Envenomations from jellyfish and related species. J Emerg.Nurs. 1997; 23: 555-65.
226. Noonburg GE. Management of extremity trauma and related infections occurring in the aquatic environment. J.Am.Acad.Orthop.Surg. 2005; 13: 243-53.
227. Mandojana RM. Introduction to Aquatic Dermatology. Joseph Demis D and ed. Clinical Dermatology. (23rd edition), 18-29. 1996. Philadelphia: Lippincott-Raven.
228. Peden, M, McGee, K, and Sharma, G. The injury chart book: a graphical overview of the global burden of injuries. 2002. Genava, World Health Organization, 2002.
229. Fauci AS, Touchette NA, Folkers GK. Emerging infectious diseases: a 10-year perspective from the National Institute of Allergy and Infectious Diseases. Emerg.Infect.Dis. 2005; 11: 519-25.
230. World Health Organization, Regional Office for South-East Asia New Delhi. Strategic plan for injury prevention and control in South-East Asia. 2002.
231. World Health Organization, Regional Office for South-East Asia, New Delhi. Injury prevention and control in South-East Asia Region. 2002.
232. Gururaj, G. Assignment Report for WHO, Regional Office for South-East Asia, New Delhi 2000 - 2001.
233. Nantulya VM, Reich MR. The neglected epidemic: road traffic injuries in developing countries. BMJ 2002; 324: 1139-41.
234. Attinger CE, Janis JE, Steinberg J et al. Clinical approach to wounds: debridement and wound bed preparation including the use of dressings and wound-healing adjuvants. Plast.Reconstr.Surg. 2006; 117: 72S-109S.
proefschrift Zegelaars.indb 48 4-2-2008 9:22:19
Chapter
2Microcirculatory changes in travellers to a tropical country
Jim E. Zeegelaar, Annemieke de Feijter, Henry J.C. de Vries, Rudy F.M. Lai A Fat, Martino A.M. Neumann and William R. Faber.
Published in: International Journal of Dermatology 2002 Feb;41(2):93-5.
proefschrift Zegelaars.indb 49 4-2-2008 9:22:19
50
AbstractBackground Travellers to tropical areas seem to be affected by nonhealing leg ulcers more frequently. One of the factors that can affect wound healing in a negative manner is leg edema. This study was performed to determine whether there is increased leg edema in travelers to tropical areas.
Method In this study, we measured the capillary filtration rate (CFR) of the lower leg by strain gauge plethysmography, as a measure of leg edema, on location in Surinam. Three groups were included: A, travelers in the first few weeks after arrival; B, travelers who had stayed in the tropics for a minimum of 2 months; C, native inhabitants.
Results The mean CFR (mL/100 mL tissue/min) was significantly higher in group A than in groups B and C; the difference between groups B and C was not significant (group A 0.05 mL/100 mL tissue/min (standard deviation (SD), 0.03) vs. group B 0.02 mL/100 mL tissue/min (SD, 0.02), P = 0.01, and vs. group C 0.02 mL/100 mL tissue/min (SD, 0.02), P = 0.01).
Conclusions Travellers to tropical areas are affected by increased CFR in the first few weeks after arrival. A prolonged stay leads to the normalization of the CFR. Compression therapy is recommended for travelers to the tropics.
proefschrift Zegelaars.indb 50 4-2-2008 9:22:19

Chapter 2
Micro
circulatory changes in travellers to a tropical country
51
Introductiona well-known problem in the Department for Tropical and Imported Skin Diseases, Academic Medical Centre, Amsterdam, The Netherlands is the presence of serious (ulcerating) pyodermas, especially of the lower leg, in otherwise healthy patients returning home from a tropical country. To our knowledge, no studies have been performed on this subject, and the incidence of these pyodermas is unknown. In our clinical experience, these imported pyodermas seem to occur more often and last longer despite appropriate antimicrobial treatment than those acquired in a temperate climate. This may be the consequence of impaired wound healing. We hypothesized that, in travelers to tropical areas, a change from a temperate to hot climate may result in a subsequent change in the microcirculation of the dermal plexus. Adaptation to higher temperatures could lead to the distension of dermal capillaries, which may result in edema. It is well known that edema may delay wound healing.1 This is especially seen in venous insufficiency, where there is a marked increase in pressure in the veins of the lower leg, causing distension of dermal capillary beds and consequent widening of the endothelial pores.2;3 Blood elements leak out through the capillary wall into the surrounding tissue and form a specific microedema, which gives rise to a hypoxic block between the capillaries and the skin cells. Microedema can be eliminated by adequate compression therapy with elastic or nonelastic bandages.4
The purpose of this study was to determine whether increased leg edema could be found in travellers who had recently arrived in the tropics from a temperate climate. We measured the capillary filtration rate (CFR), as a measure of microedema, in travelers from The Netherlands who had just arrived in Surinam, South America, and compared the values with those of travelers from The Netherlands who had stayed in the tropics for a minimum of 2 months and with those of healthy native inhabitants.
Materials and methods Patients
Three groups of healthy volunteers without a history or clinical signs of arterial or venous vascular diseases, and who were not taking any medication, were studied. None of the patients had consumed alcohol or had smoked during the day of the investigation. Group A consisted of Dutch students (12 Caucasians and one person of mixed Hindustani/Caucasian origin; five men and eight women; aged between 21 and 56 years; mean age, 37 years) who were investigated between 10 and 21 days after arrival by aeroplane in Surinam from The Netherlands. Group B, consisting of 13 Dutch Caucasian students (five women and eight men; aged between 21 and
proefschrift Zegelaars.indb 51 4-2-2008 9:22:19

52
37 years; mean age, 26 years), had stayed in Surinam for at least 2 months. Group C consisted of 14 local inhabitants of mixed black, Chinese, Indian, or Caucasian origin (nine women and five men; aged between 32 and 51 years; mean age, 42 years). No randomization was performed. Eight persons of group C were also investigated while visiting The Netherlands. They were all investigated 1 week after arrival in The Netherlands. Student’s t-test was performed.
MethodsChanges in tissue volume of the mid-calf caused by the CFR were calculated from changes in the diameter of the limb measured using a (mercury in rubber) strain gauge plethysmograph (Medasonics, model SPG-16).5-7 Despite possible variations in results, due to the inaccuracy of the strain gauge depending on temperature or the exact position of fixation to the person investigated, this method was chosen as it is noninvasive, simple, portable, and repeatable without patient discomfort, and can be applied under field conditions in the tropics.The person is rested for 15 min in the supine position; the leg is flexed slightly, the strain gauge is attached around the mid-calf at its widest diameter, and a pneumatic cuff is placed on the thigh. The cuff is then inflated to 60 mmHg, which provides venous occlusion without obstructing arterial inflow, thus preventing venous return and causing an increase in calf circumference and stretching of the strain gauge. The changed circumference of the strain gauge causes a difference in electric resistance, which is automatically interpreted and recorded by the apparatus. Obstructing the venous flow leads to an initial rapid volume increase in the lower leg (Fig. 1). After about 2 min, the maximum venous capacity is obtained, defined as the change in milliliters per 100 mL tissue. In the subsequent phase, a slight volume expansion occurs, caused by the filtration of fluid through the vessel wall into the surrounding tissue. The filtration rate is calculated as the filtration (mL/100 mL tissue) in time (min) measured between 6 and 15 min after venous obstruction (Fig. 1).In this setting, we did not make use of a climate room as has been used in other studies, as the influence of the climate as a whole on CFR was our study object. As local temperature and humidity may interfere with capillary filtration, however, all measurements in Surinam were performed in the afternoon with a temperature around 32 °C and a humidity around 95%.
proefschrift Zegelaars.indb 52 4-2-2008 9:22:19
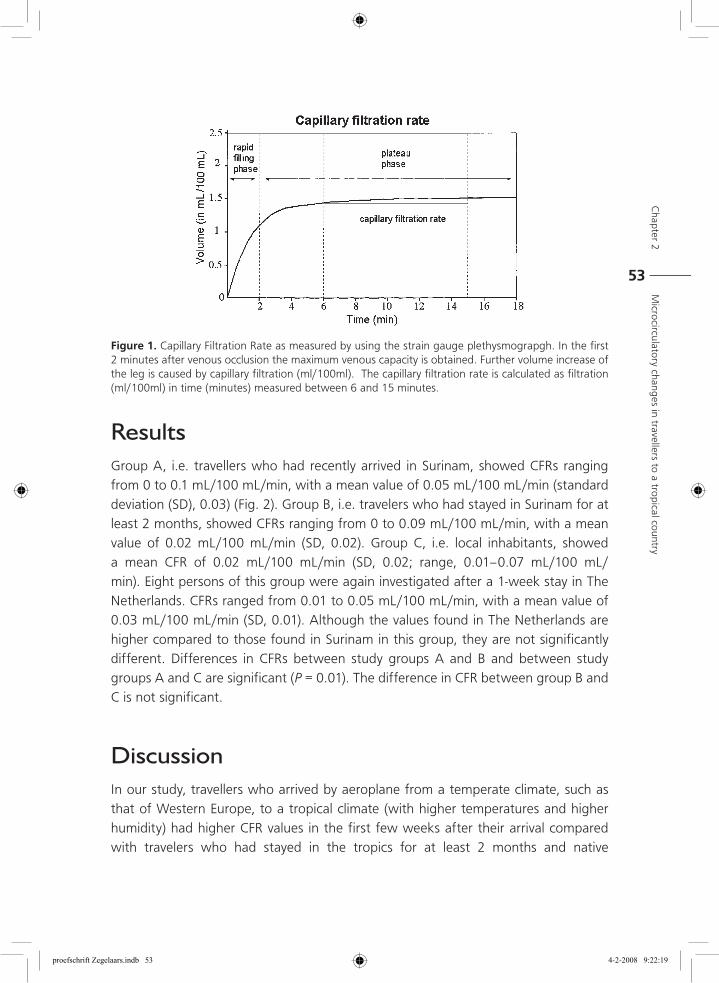
Chapter 2
Micro
circulatory changes in travellers to a tropical country
53
ResultsGroup A, i.e. travellers who had recently arrived in Surinam, showed CFRs ranging from 0 to 0.1 mL/100 mL/min, with a mean value of 0.05 mL/100 mL/min (standard deviation (SD), 0.03) (Fig. 2). Group B, i.e. travelers who had stayed in Surinam for at least 2 months, showed CFRs ranging from 0 to 0.09 mL/100 mL/min, with a mean value of 0.02 mL/100 mL/min (SD, 0.02). Group C, i.e. local inhabitants, showed a mean CFR of 0.02 mL/100 mL/min (SD, 0.02; range, 0.01–0.07 mL/100 mL/min). Eight persons of this group were again investigated after a 1-week stay in The Netherlands. CFRs ranged from 0.01 to 0.05 mL/100 mL/min, with a mean value of 0.03 mL/100 mL/min (SD, 0.01). Although the values found in The Netherlands are higher compared to those found in Surinam in this group, they are not significantly different. Differences in CFRs between study groups A and B and between study groups A and C are significant (P = 0.01). The difference in CFR between group B and C is not significant.
DiscussionIn our study, travellers who arrived by aeroplane from a temperate climate, such as that of Western Europe, to a tropical climate (with higher temperatures and higher humidity) had higher CFR values in the first few weeks after their arrival compared with travelers who had stayed in the tropics for at least 2 months and native
Figure 1. Capillary Filtration Rate as measured by using the strain gauge plethysmograpgh. In the first 2 minutes after venous occlusion the maximum venous capacity is obtained. Further volume increase of the leg is caused by capillary filtration (ml/100ml). The capillary filtration rate is calculated as filtration (ml/100ml) in time (minutes) measured between 6 and 15 minutes.
proefschrift Zegelaars.indb 53 4-2-2008 9:22:19
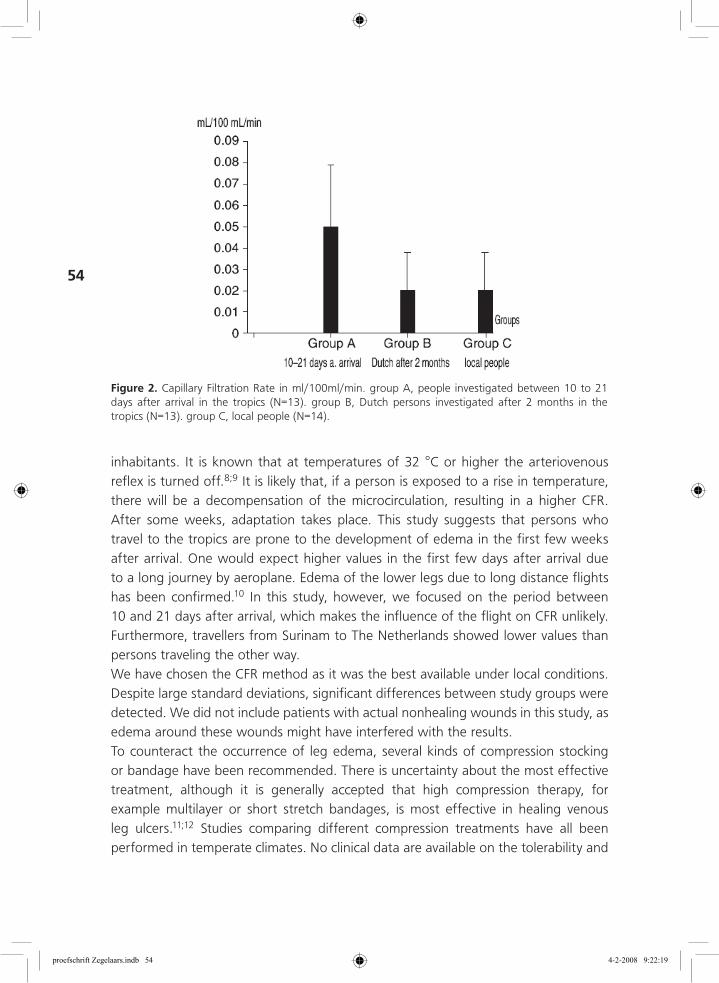
54
inhabitants. It is known that at temperatures of 32 °C or higher the arteriovenous reflex is turned off.8;9 It is likely that, if a person is exposed to a rise in temperature, there will be a decompensation of the microcirculation, resulting in a higher CFR. After some weeks, adaptation takes place. This study suggests that persons who travel to the tropics are prone to the development of edema in the first few weeks after arrival. One would expect higher values in the first few days after arrival due to a long journey by aeroplane. Edema of the lower legs due to long distance flights has been confirmed.10 In this study, however, we focused on the period between 10 and 21 days after arrival, which makes the influence of the flight on CFR unlikely. Furthermore, travellers from Surinam to The Netherlands showed lower values than persons traveling the other way.We have chosen the CFR method as it was the best available under local conditions. Despite large standard deviations, significant differences between study groups were detected. We did not include patients with actual nonhealing wounds in this study, as edema around these wounds might have interfered with the results.To counteract the occurrence of leg edema, several kinds of compression stocking or bandage have been recommended. There is uncertainty about the most effective treatment, although it is generally accepted that high compression therapy, for example multilayer or short stretch bandages, is most effective in healing venous leg ulcers.11;12 Studies comparing different compression treatments have all been performed in temperate climates. No clinical data are available on the tolerability and
Figure 2. Capillary Filtration Rate in ml/100ml/min. group A, people investigated between 10 to 21 days after arrival in the tropics (N=13). group B, Dutch persons investigated after 2 months in the tropics (N=13). group C, local people (N=14).
proefschrift Zegelaars.indb 54 4-2-2008 9:22:19
Chapter 2
Micro
circulatory changes in travellers to a tropical country
55
efficacy of compression therapy in tropical conditions. Our personal experience is that bandages or stockings for high compression therapy, because of the high humidity and high temperatures, are often not well tolerated for periods longer than a few hours a day. Therefore, we are still cautious to recommend compression therapy for (ulcerating) pyodermas in the tropics; however, compression therapy could be an option for travellers with (ulcerating) pyodermas of the lower extremities after having returned from the tropics.
Reference List 1. Prasad A, Ali Khan AA, Mortimer PS. Leg ulcers and oedema: A study exploring the prevalence,
aetiology and possible significance of oedema in venous ulcers. Phlebology 1990; 5: 181-7.
2. Coleridge Smith PD, Thomas P, Scurr JH et al. Causes of venous ulceration: a new hypothesis. Br.Med.J.(Clin.Res.Ed) 1988; 296: 1726-7.
3. Burton CS. Venous ulcers. Am.J.Surg. 1994; 167: 37S-40S.
4. Gaylarde PM, Sarkany I, Dodd HJ. The effect of compression on venous stasis. Br.J.Dermatol. 1993; 128: 255-8.
5. Gamble J, Gartside IB, Christ F. A reassessment of mercury in silastic strain gauge plethysmography for microvascular permeability assessment in man. J.Physiol 1993; 464: 407-22.
6. Mostbeck A. [Methodological aspects of the determination of the capillary filtrate in the extremities. Simultaneous measurement of leg and regional blood volume by plethysmography and Tc-99m-labeled erythrocytes]. Vasa 1986; 15: 233-40.
7. KITCHIN AH. Peripheral blood flow and capillary filtration rates. Br.Med.Bull. 1963; 19: 155-60.
8. Brakkee AJ, Vendrik AJ. Strain-gauge plethysmography; theoretical and practical notes on a new design. J.Appl.Physiol 1966; 21: 701-4.
9. Hidd BS, Lyons SM. The distensibility of the blood vessels of the human calf determined by graded venous congestion. J Physiol 1985; 140: 122-8.
10. Landgraf H, Vanselow B, Schulte-Huermann D et al. Economy class syndrome: rheology, fluid balance, and lower leg edema during a simulated 12-hour long distance flight. Aviat.Space Environ.Med. 1994; 65: 930-5.
11. Fletcher A, Cullum N, Sheldon TA. A systematic review of compression treatment for venous leg ulcers. BMJ 1997; 315: 576-80.
12. Gniadecka M, Karlsmark T, Bertram A. Removal of dermal edema with class I and II compression stockings in patients with lipodermatosclerosis. J.Am.Acad.Dermatol. 1998; 39: 966-70.
proefschrift Zegelaars.indb 55 4-2-2008 9:22:19

proefschrift Zegelaars.indb 56 4-2-2008 9:22:20
Chapter
3Bacterial colonization, anti-microbial resistance and the aetiology of wounds in three different tropical countries
Jim E. Zeegelaar, Wies Langenberg, Eefje Jong, Hardjanto Soebono, Douwe Verkuyl, William R.Faber.
proefschrift Zegelaars.indb 57 4-2-2008 9:22:20
58
SummaryThis study was conducted to evaluate the colonization of wounds with micro-organisms and the anti-microbial resistance in three different tropical countries, Suriname (Latin America), Indonesia (Asia) and Zimbabwe (Africa). Bacterial swabs were obtained from the wound surface after clinical examination. Swabs were stored in 8% glycerol/peptone and subsequently deep frozen. They were transported by air to The Netherlands, where they were processed further. In Suriname, 45 wounds which were frequently venous leg ulcers were investigated. Cultures were set-up from the swabs obtained from all wounds. Staphylococcus aureus was encountered in 13 of the cultures (6 tetracycline resistant), Streptococcus pyogenes in 2 (both tetracycline resistant), haemolytic streptococci (non-group A) in 4 (all tetracycline resistant), Enterobacteriaceae (coliform Gram-negative rods) in 10 and Pseudomonas aeroginosa in 5. In Zimbabwe, 23 wounds which were frequently traumatic wounds, were investigated. Cultures were set-up from the swabs obtained from all wounds. Staphylococcus aureus was encountered in 7 of the cultures (1 methicillin resistant, 5 tetracycline resistant), Streptococcus pyogenes in 1 (tetracycline resistant), coliform rods in 3 and Pseudomonas aeruginosa in 1. In Indonesia, 31 wounds which were frequently diabetic wounds, were investigated. Cultures were set-up from the swabs obtained from all wounds. Staphylococcus aureus was found in 11 of the cultures (9 tetracycline and 6 methicillin resistant), Streptococcus pyogenes in 2 (both tetracycline resistant), Haemolytic streptococci (non-group A) in 5 (2 tetracycline resistant), enterococci in 1, coliform Gram-negative rods in 14 (11 gentamicin, -10 ciprofloxacin resistant and 5 extended spectrum β lactamase-producing), Pseudomonas aeruginosa in 5 (4 tobramycin-, 2 ciprofloxacin- and 3 ceftazidime resistant). The differences in aetiology of the wounds encountered in the three countries were probably because of organizational differences. The influence of the bacterial resistance and its effect on wound healing should be explored further.
proefschrift Zegelaars.indb 58 4-2-2008 9:22:20
Chapter 3
Bacterial co
lonization, anti-micro
bial resistance and the aetiolo
gy of w
ounds in three different tropical countries
59
IntroductionChronic wounds are a serious problem in many tropical countries.1;2 This may be attributed to the low standard of living, more traumatic accidents or poorly available health services and trained personnel. There are only few reported studies dealing with this subject.3 Wounds are generally contaminated with a large number of bacteria.4;5 The bacteria present do not necessarily influence the healing process.6;7 However, knowledge on the bacterial colonization of wounds in a given area and their anti-microbial sensitivity is useful not only for epidemiological reasons, but also for choosing the most effective anti-microbial treatment for wound infections. Furthermore, at our out-patient clinic for tropical and imported skin diseases, serious (ulcerating) pyodermas, especially of the lower leg, are regularly encountered in otherwise healthy individuals who have visited a tropical country. To our knowledge, the incidence of these pyodermas remains unknown. It is not known whether the prevalence of bacteria such as streptococci and staphylococci that cause these pyodermas is higher in the tropics. Nonetheless, it is known that bacterial resistance to anti-microbial agents is an increasing problem in many tropical countries.8 In this study the influence of micro-organisms on wound healing was not specifically investigated, but instead their colonization in general. This study was pursued to gain more information on the bacterial colonization, the resistance of the bacteria to anti-bacterial agents and the aetiology of wounds encountered in tropical countries.
Patients and MethodsPatients with wounds were examined at three participating institutions. Presence of the wound and any relevant underlying disease were recorded. The aetiology of the wounds was retrieved from the patient medical file and evaluated on clinical grounds since other diagnostic procedures were usually not available at the three institutions. Data on the used antibiotics in the preceding 3 weeks were also extracted from the medical files. All patients who presented with chronic skin ulcers were asked to participate in the study. New patients with chronic skin ulcers were traced by screening the registration books at the nurse stations and by ward rounds with the doctors on duty. Swabs for culture were obtained from wounds present for at least 3 weeks without any tendency to heal. Swabs for culture were obtained.The out-patient clinics of the departments of Dermatology and Surgery of the Academic Hospital Paramaribo, Suriname, South America were participants. Swabs were obtained from June until July 1999.
proefschrift Zegelaars.indb 59 4-2-2008 9:22:20
60
In Indonesia the out-patient clinics of Dermatology, Internal Medicine and Surgery at Sardjito hospital, Gadjah Mada University, Djokjakarta, participated. Swabs were obtained from august until September 2000.In Zimbabwe the out-patient clinic of the Department of Surgery of the Bulawayo Central Hospital, Bulawayo, participated. This is a regional hospital at which a wide variety of wounds are seen. Swabs were obtained from May until June 2001.For bacterial culture, the wounds were thoroughly cleaned with water-soaked gauze. Dacron swabs were used to collect material from the wound surface and if possible from under the margins of the wounds. The swabs were then immediately placed in 400 μl 8% glycerol/peptone in a sterile screw-cap container and placed in a freezer at -20 0C. All the containers were stored deep frozen and transported on dry ice by air to the Department of Medical Microbiology at the Academic Medical Centre in Amsterdam, The Netherlands. Here, they were stored at -70 0C until further processing. The containers from Suriname were stored frozen for 7 months, the containers from Zimbabwe for 5 months, and the containers from Indonesia for 5 months. The specimens were then defrosted and processed according to the standard laboratory procedures for samples from chronic wounds. The swabs were inoculated on selective and non-selective agars and incubated at 37 0C in air, 7% CO2 and anaerobic conditions for at least 2 days. Suspected Staphylococcus aureus, beta-haemolytic streptococci and Pseudomonas aeruginosa were selected for definite identification and sensitivity testing in all cases. Other potential pathogens such as coliform bacteria, anaerobes and aerobic gram-positive rods were only investigated if they were considered significant (as indicated by the Gram stain, or by growth in pure culture, or in abundance with minimal or moderate involvement of non-pathogenic flora). In other cases, the presence of coliforms or (mixed) anaerobic growth was just recorded without further investigation. Sensitivity testing of aerobic micro-organisms was performed by agar diffusion, using Rosco tablets and the MIC-breakpoints of the Dutch CRG. Methicillin resistance in S. aureus was defined as an inhibition zone of less than 16 mm around a 1 μg oxacillin tablet on Columbia agar after incubation for 48 hours at 30 0C. Tests for extended spectrum beta-lactamase (ESBL) production in coliform bacteria were only performed when the routine anti-biogram showed resistance to third generation cephalosporins. The tests used were both the ESBL E-test and the double tablet synergy test. To examine the effects of freezing and storage of swabs on the culture results, a study was conducted in 17 patients at the Department of Dermatology of the Academic Medical Centre in Amsterdam. Using the techniques and methods described above, two swabs were obtained from the wound. One swab was placed in a transport medium and cultured on the same day, while the other was placed in 8% glycerol/peptone and stored at -70 0C for periods varying from 2 to 22 months (median 5
proefschrift Zegelaars.indb 60 4-2-2008 9:22:20

Chapter 3
Bacterial co
lonization, anti-micro
bial resistance and the aetiolo
gy of w
ounds in three different tropical countries
61
months) until further processing. The results of this validation study revealed that freezing and storage of the swabs had no influence on culturing
ResultsThe 27 men and 18 women attending the out-patient clinic in Suriname all lived in Paramaribo, the capital city of Suriname, or in the outskirts of the city. Their age ranged from 50 to 83 years (mean 63 years). A total of 45 wounds were investigated, mostly at the department of Surgery. The venous leg ulcers were all examined at the Department of Dermatology. Most prevalent were venous leg ulcers, diabetic ulcers and traumatic wounds (Table 1). The duration of the wounds was between 3 weeks and 7 years. Table 2 shows the isolation rate of three important wound pathogens (S. aureus, beta-haemolytic streptococci and P. aeruginosa) and of some potential pathogens that frequently exhibit problematic anti-microbial resistance in the industrialized world. The number of resistant strains in each category is also shown. Table 3 lists all the bacterial species grown from the swabs obtained at the three institutions. In Table 4 all recorded antibiotics given before or during examination of the patients are shown.In the swabs from Suriname S. aureus, coliform bacteria and P. aeruginosa were the species most frequently encountered. In total 48 prescriptions for antibiotics were recorded, mean 1.1 prescriptions per patient.
Table 1. Aetiology of wounds at three different tropical locations.
Suriname45 patients
Zimbabwe23 patients
Indonesia31 patients
Venous leg ulcers 12
Traumatic ulcers 8 8 7
Diabetes wounds 10 14
Burns 1 1
Neuropathic leprosy ulcers 4 2
Arterial disease 6 1
Pressure ulcer 1 1 1
Delayed wound healing after: surgery
4 6
carcinoma
genital infection 2
unknown 5 1
4
proefschrift Zegelaars.indb 61 4-2-2008 9:22:20
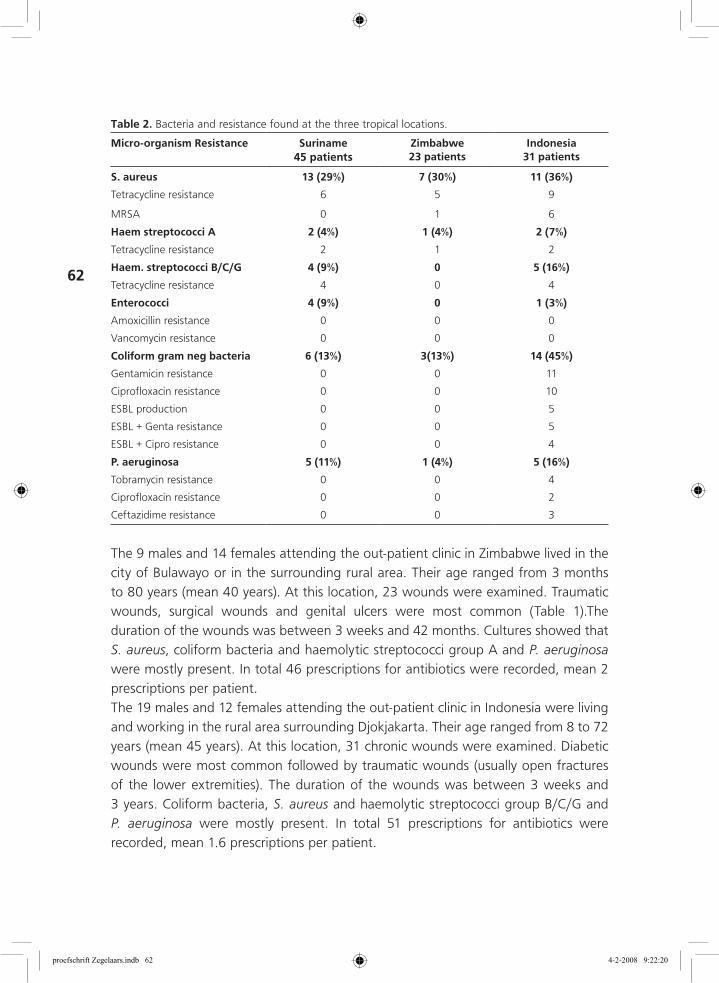
62
The 9 males and 14 females attending the out-patient clinic in Zimbabwe lived in the city of Bulawayo or in the surrounding rural area. Their age ranged from 3 months to 80 years (mean 40 years). At this location, 23 wounds were examined. Traumatic wounds, surgical wounds and genital ulcers were most common (Table 1).The duration of the wounds was between 3 weeks and 42 months. Cultures showed that S. aureus, coliform bacteria and haemolytic streptococci group A and P. aeruginosa were mostly present. In total 46 prescriptions for antibiotics were recorded, mean 2 prescriptions per patient.The 19 males and 12 females attending the out-patient clinic in Indonesia were living and working in the rural area surrounding Djokjakarta. Their age ranged from 8 to 72 years (mean 45 years). At this location, 31 chronic wounds were examined. Diabetic wounds were most common followed by traumatic wounds (usually open fractures of the lower extremities). The duration of the wounds was between 3 weeks and 3 years. Coliform bacteria, S. aureus and haemolytic streptococci group B/C/G and P. aeruginosa were mostly present. In total 51 prescriptions for antibiotics were recorded, mean 1.6 prescriptions per patient.
Table 2. Bacteria and resistance found at the three tropical locations.
Micro-organism Resistance Suriname45 patients
Zimbabwe23 patients
Indonesia31 patients
S. aureus 13 (29%) 7 (30%) 11 (36%)
Tetracycline resistance 6 5 9
MRSA 0 1 6
Haem streptococci A 2 (4%) 1 (4%) 2 (7%)
Tetracycline resistance 2 1 2
Haem. streptococci B/C/G 4 (9%) 0 5 (16%)
Tetracycline resistance 4 0 4
Enterococci 4 (9%) 0 1 (3%)
Amoxicillin resistance 0 0 0
Vancomycin resistance 0 0 0
Coliform gram neg bacteria 6 (13%) 3(13%) 14 (45%)
Gentamicin resistance 0 0 11
Ciprofloxacin resistance 0 0 10
ESBL production 0 0 5
ESBL + Genta resistance 0 0 5
ESBL + Cipro resistance 0 0 4
P. aeruginosa 5 (11%) 1 (4%) 5 (16%)
Tobramycin resistance 0 0 4
Ciprofloxacin resistance 0 0 2
Ceftazidime resistance 0 0 3
proefschrift Zegelaars.indb 62 4-2-2008 9:22:20

Chapter 3
Bacterial co
lonization, anti-micro
bial resistance and the aetiolo
gy of w
ounds in three different tropical countries
63
Table 3. Bacterial species cultured from the samples collected at the three locations.
Suriname 45 patients
Zimbabwe23 patients
Indonesia31 patients
S. aureus S. aureus S. aureus
Coagulase negative staphyloccoci
S. pyogenes S. pyogenes S. pyogenes
Haemolytic streptococci group B Haemolytic streptococci group B
Haemolytic streptococci group C Haemolytic streptococci group C
Haemolytic streptococci group G
Enterococcus sp Enterococcus sp
S.milleri group S.milleri group
Streptococcus sp Streptococcus sp
Bacillus sp.
Citrobacter sp.
E.coli E.coli E.coli
E.cloacea
K.oytoca
K. pneumoniae K. pneumoniae
Proteus sp Proteus sp
P.mirabilis P.mirabilis P.mirabilis
P.Penneri
P.vulgaris
Providencia rettgeri
Providencia stuartii
Serratia marcescens Serratia marcescens
Coliform gram neg bacteria Coliform gram neg bacteria Coliform gram neg bacteria
Acinobacter sp. Acinobacter sp. Acinobacter sp.
Alcaligenes faecalis
P.aeroginosa P.aeroginosa P.aeroginosa
S.maltophilia S.maltophilia
B.fragilis
Peptostreptococcus anaerobius
Anaerobic gram pos cocci
mixed anaerobes mixed anaerobes
C.albicans
Yeast
Commensal flora Commensal flora Commensal flora
Skin flora Skin flora Skin flora
Mixed flora
No growth 6 X No growth 1 X
proefschrift Zegelaars.indb 63 4-2-2008 9:22:20
64
DiscussionWounds, especially leg ulcers, are generally a major health problem. The prevalence of wounds in most of the tropical countries is not known because there are only a few reported studies on this subject.3 It seems that traumatic wounds which are secondarily infected play a major role. In our study, traumatic wounds were also commonly encountered, although diabetes played an important role in Indonesia as well as in Suriname. The high prevalence of venous leg ulcers in Suriname is probably because of by the fact that most wounds were seen at the department of Dermatology. Diabetes is a major health problem both in Suriname and in Indonesia, with a high prevalence as compared with that in Zimbabwe.9-12 This may be reflected in the high prevalence of diabetic wounds encountered in these locations in Suriname and Indonesia.Although, in ulcers of Dutch patients who have travelled in the tropics, group A beta-haemolytic streptococci are, in our experience, by far the most common pathogens, these bacteria did not predominate in the wound swabs from the locations in the three tropical countries examined in this study. On the whole, we found no gross differences between the microbial colonization of the wounds at the three tropical locations and that in the wounds seen at our dermatological out-patient clinic in Amsterdam, even though the swabs were obtained under different climatic conditions and from different patient populations.The most striking result overall and the most striking apparent difference between the three tropical locations, is the prevalence of anti-microbial resistance. Resistance among staphylococci and streptococci against tetracycline was high at all three locations. There was very little resistance against other anti-microbial agents in the isolates from Suriname, whereas in the Indonesian samples the prevalence of methicillin resistant S. aureus (MRSA) was substantial, as well as the anti-microbial resistance of the gram-negative bacteria, both against older agents such as gentamicin and tobramycin and against newer anti-microbial agents like ciprofloxacin and the third generation cephalosporins. In Zimbabwe, the picture seems to be more favourable, as only one of 23 examined patients had a wound colonized with MRSA. On the one hand, the prevalence of extended spectrum β lactamase (ESBL) producing gram-negative bacilli, may have been underestimated because of the insensitivity of the routine susceptibility method employed here as a means of screening for ESBL production. On the other hand, although MRSA was frequently found in the Indonesian samples this may to be due to the spread of one MRSA strain among the patients in the wards from which our swabs were obtained, or among the population served by the Sardjito hospital, rather than to the circulation of many different MRSA strains in Indonesia. This explanation is indicated by the MRSA-phage typing of
proefschrift Zegelaars.indb 64 4-2-2008 9:22:20

Chapter 3
Bacterial co
lonization, anti-micro
bial resistance and the aetiolo
gy of w
ounds in three different tropical countries
65
the Indonesian isolates carried out at the National Institute for Public Health and Environment (RIVM), The Netherlands, which showed that the isolates were all of the same type (dr. W.J.B. Wannet, personal communication)The observed difference between the three tropical locations could have been caused by the prescription behaviour and over the counter availability of antibiotics. In Suriname drugs are only available on prescription and antibiotics, especially the new, more expensive ones are often difficult to obtain. Consequently, older agents like amoxicillin and cotrimoxazole are frequently used, whereas the use of gentamicin is rare, and the third generation cephalosporins are not used at all (Table 4)What our findings do make clear is the presence in the tropics of resistant micro-organisms that are commonly associated with industrialized countries. These findings have also been reported by others.8;13;14 Resistant microbe strains may spread very quickly and cause the failure of the locally available antibiotic regimens, not only in patients with wounds, but also in patients with more immediately life-threatening infections, in countries where the means to detect various forms of anti-microbial resistance and/or to implement appropriate infection control measures within hospitals are unavailable.The technique of long-term storage and long-distance transport that we describe here was developed to make it possible to use our laboratory in Amsterdam for the investigation of the swabs obtained at the three tropical locations for this study. The technique proved to be useful in that it allowed the isolation of common wound pathogens, including anaerobic micro-organisms, and also the detection of MRSA and ESBL-producing coliform bacteria. The results of this study indicate that wounds in tropical countries are not more often colonized with S. pyogenes or S. aureus than that in the western world. Anti-microbial resistance was found to be present in a substantial number of wounds that were investigated. The observed differences in aetiology of wounds at the three investigated tropical locations in this study probably reflects the differences in patient populations.
Acknowledgement
The authors thank dr. W.J.B. Wannet of the National Institute for Public Health and Environment, Bilthoven, The Netherlands for phage typing of the Indonesian MRSA isolates.
proefschrift Zegelaars.indb 65 4-2-2008 9:22:20
66
Reference List 1. Sturm AW, Jamil B, McAdam KP et al. Microbial colonizers in leprosy skin ulcers and intensity
of inflammation. Int.J.Lepr.Other Mycobact.Dis. 1996; 64: 274-81.
2. Robinson DC, Hay RJ. Tropical ulcer in Zambia. Trans.R.Soc.Trop.Med.Hyg. 1986; 80: 132-7.
3. Ohanaka EC, Osarenkhoe O. In-patient management of leg ulcers. East Afr.Med.J. 1999; 76: 687-9.
4. Bowler PG, Duerden BI, Armstrong DG. Wound microbiology and associated approaches to wound management. Clin.Microbiol.Rev. 2001; 14: 244-69.
5. Brook I, Frazier EH. Aerobic and anaerobic microbiology of chronic venous ulcers. Int.J.Dermatol. 1998; 37: 426-8.
6. Eriksson G, Eklund AE, Kallings LO. The clinical significance of bacterial growth in venous leg ulcers. Scand.J.Infect.Dis. 1984; 16: 175-80.
7. Filius PM, Gyssens IC. Impact of increasing antimicrobial resistance on wound management. Am.J.Clin.Dermatol. 2002; 3: 1-7.
8. Shears P. Antibiotic resistance in the tropics. Epidemiology and surveillance of antimicrobial resistance in the tropics. Trans.R.Soc.Trop.Med.Hyg. 2001; 95: 127-30.
9. Konsten J, Ketele PO, Girjasing R et al. [General surgery in Paramaribo University Hospital]. Ned.Tijdschr.Geneeskd. 1999; 143: 2432-6.
10. Middelkoop BJ, Kesarlal-Sadhoeram SM, Ramsaransing GN et al. Diabetes mellitus among South Asian inhabitants of The Hague: high prevalence and an age-specific socioeconomic gradient. Int.J.Epidemiol. 1999; 28: 1119-23.
11. Sutanegara D, Budhiarta AA. The epidemiology and management of diabetes mellitus in Indonesia. Diabetes Res.Clin.Pract. 2000; 50 Suppl 2: S9-S16.
12. Mudiayi TK, Onyanga-Omara A, Gelman ML. Trends of morbidity in general medicine at United Bulawayo Hospitals, Bulawayo, Zimbabwe. Cent.Afr.J.Med. 1997; 43: 213-9.
13. Alausa OK, Montefiore D. Bacterial infections, sensitivity patterns, and chemotherapy among hospital patients in the tropics. Scand.J Infect.Dis. 1978; 10: 295-302.
14. Shears P. Antimicrobial resistance in the tropics. Trop.Doct. 2000; 30: 114-6.
proefschrift Zegelaars.indb 66 4-2-2008 9:22:21
Chapter
4Etiology and incidence of chronic ulcers in Blantyre, Malawi
Jim E. Zeegelaar, Aimee C. Stroïnk, Willemijn H. Steketee, William R. Faber, Allard C. van der Wal, Isaac O.O. Komolafe, Charles Dzamalala, Cecilia Chibwana, Hans F. Wendte, Ed E.Zijlstra.
Published in: International Journal of Dermatology 2006 Aug;45(8):933-6.
proefschrift Zegelaars.indb 67 4-2-2008 9:22:21
68
AbstractBackground Little information is available on the incidence and etiology of chronic ulcers in the tropics. Therefore, the incidence and etiology of chronic skin ulcers were assessed in out-patients at the Department of Dermatology and in in-patients at the Departments of Dermatology, Surgery, Medicine, and Pediatrics, Queen Elizabeth Central Hospital (QECH), Blantyre, Malawi.
Method In a 10-week study period, 44 patients (31 males, 70%) with chronic skin ulcers were diagnosed from 6292 patients seen by the departments involved.
Results The mean age of patients with ulcers was 38 years (range, 9 months to 82 years). The most frequent cause of ulcers was bacterial infection (n = 22), followed by malignancy (n = 11) and trauma (n = 7).
Conclusion In contrast with developed countries, venous and diabetic ulcers were uncommon. In addition to bacterial infections, a surprisingly large number of malignancies were found in this study. We speculate that human immunodeficiency virus (HIV) infection, which is seen with a high prevalence at QECH, is a contributing factor. Because of the large number of malignancies, we recommend early histopathologic investigation of chronic ulcers in this part of Africa..
proefschrift Zegelaars.indb 68 4-2-2008 9:22:21

Chapter 4
Etiolo
gy and incidence of chronic ulcers in B
lantyre, Malaw
i
69
IntroductionChronic ulcers are an important cause of morbidity in developing countries.1;2 This may be explained by the poor socioeconomic conditions and poor health services. In contrast with developed countries, little is known about the prevalence and etiology of skin ulcers in these areas. One study from Nigeria reported that the most common etiologic factors of leg ulcers were trauma, diabetes mellitus, and sickle cell disease3. Depending on the region, infectious causes, such as cutaneous leishmaniasis or Buruli ulcer, may be encountered.4;5 In contrast, venous ulcers on the legs are the most common cause of ulcers in developed countries, and are reported to be uncommon in tropical countries.6
Data from Malawi are scanty; one study showed trauma to be the most important cause of chronic wounds.7 We undertook this study to investigate the incidence and etiology of chronic skin ulcers presenting to the Queen Elizabeth Central Hospital (QECH) in Blantyre, Malawi.
MethodsThe study was performed at QECH, Blantyre, Malawi, which is the teaching hospital of the College of Medicine and the largest referral hospital in Malawi, with over 1000 beds. Blantyre is the commercial capital and main industrial center of Malawi with a population of around 800,000 people. The study was performed during a 10-week period in the dry season (May to July) when daytime temperatures were around 25–30 °C.All patients presenting with chronic ulcers at the outpatient clinic of the Department of Dermatology were included; in addition, the wards of the Departments of Dermatology, Surgery, Medicine, and Pediatrics were visited twice daily and any patient who had an ulcer was recruited into the study, irrespective of whether this was the main reason for admission or a comorbidity. All patients were informed about the purpose and methods of the study and were included after written consent had been obtained. The study was approved by the College of Medicine Research and Ethics Committee.Chronic skin ulcers were defined as round or irregularly shaped excavations of the skin that had resulted from a loss of the epithelium and dermis, or even deeper, and had existed for more than 4 weeks.Data were entered onto a case record form: age, gender, previous treatment, and underlying disease (e.g. diabetes mellitus, leprosy or sickle cell disease). A detailed description of the ulcer was made, including the number, duration, location, size,
proefschrift Zegelaars.indb 69 4-2-2008 9:22:21
70
aspect of the surrounding tissue, shape, edge, presence of exudate, and color. The presence or absence of varicose veins was noted. The arterial circulation was examined by palpating the dorsalis pedis artery and the posterior tibial artery.Clinical signs of inflammation (redness, pain, swelling, and increased temperature) were noted. Ulcerating pyoderma was defined as a purulent ulceration with signs of inflammation. Secondary ulcerating pyoderma was defined as a purulent ulceration of a pre-existing skin lesion, for example eczema or insect bites.A first clinical diagnosis was made by two investigators (ACS, WHS); a second opinion was obtained by examination of digital pictures in The Netherlands (JEZ, WRF). Swabs for Gram stain and bacterial culture were taken from the wound surface after thorough cleaning with water-soaked gauze. The swabs were inoculated onto appropriate agar media and a Gram stain was performed.If required for diagnosis, 4-mm punch biopsies were taken from the edge of the ulcer after local infiltration with 1% lidocaine. The specimens were fixed in formalin and embedded in paraffin. Slides were stained with hematoxylin and eosin; when indicated, additional slides were stained with Ziehl–Neelsen stain for the detection of acid-fast bacilli and with periodic acid–Schiff (PAS) and silver stains for the detection of fungi. After initial reading in Malawi, two unstained slides of each biopsy were shipped to The Netherlands for confirmation. A final diagnosis was made by taking into account the clinical presentation and the results of the microbiologic and histologic examinations.The study had a case series design. In addition, the incidence of skin ulcers in each department was estimated as the number of patients presenting with ulcers divided by the total number of patients seen at the out-patient department or as admissions during the study period.
ResultsClinical findings
In the study period, 3320 patients (12 with chronic ulcers; 3.6/1000) were seen as out-patients in the Department of Dermatology, and 44 patients (one with a chronic ulcer; 23/1000) were admitted. In the other clinical departments these numbers were: Medicine, 1650 admissions (four chronic ulcers; 2.4/1000); Surgery, 688 admissions (23 chronic ulcers; 34/1000); Pediatrics, 590 admissions (four chronic ulcers; 6.8/1000). All 44 patients (0.7% of all patients screened) who were diagnosed as having a chronic skin ulcer consented to be enrolled into the study. The age range was 9 months to 82 years, with a mean age of 38 years. The mean age in children was 4.5 years and in adults was 43.5 years. The age distribution is shown in Fig 1.
proefschrift Zegelaars.indb 70 4-2-2008 9:22:21
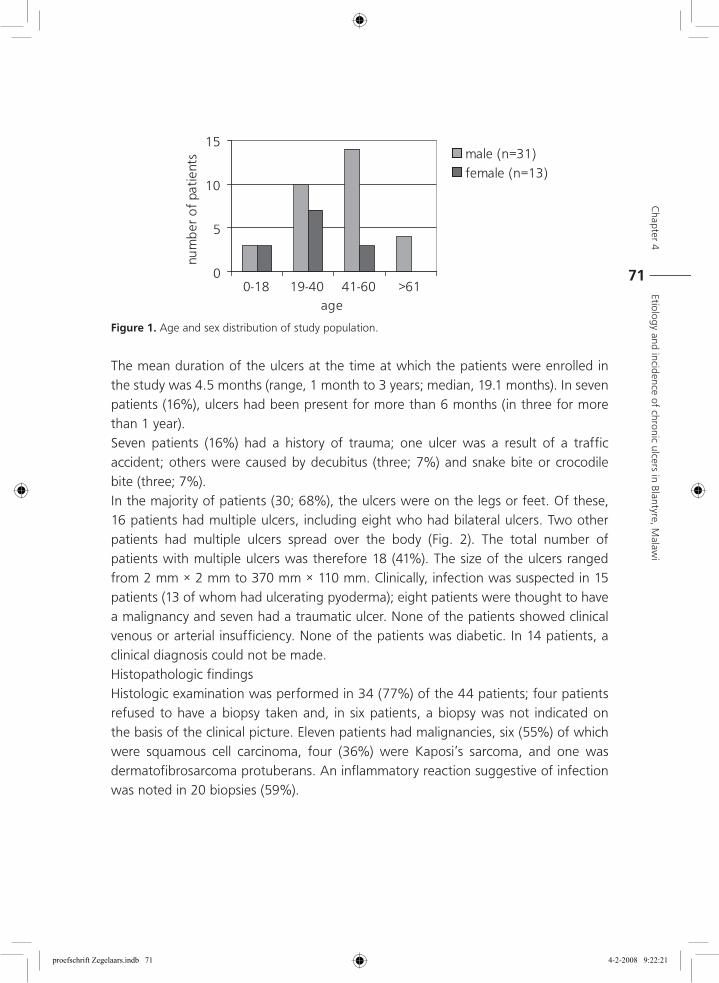
Chapter 4
Etiolo
gy and incidence of chronic ulcers in B
lantyre, Malaw
i
71
The mean duration of the ulcers at the time at which the patients were enrolled in the study was 4.5 months (range, 1 month to 3 years; median, 19.1 months). In seven patients (16%), ulcers had been present for more than 6 months (in three for more than 1 year).Seven patients (16%) had a history of trauma; one ulcer was a result of a traffic accident; others were caused by decubitus (three; 7%) and snake bite or crocodile bite (three; 7%).In the majority of patients (30; 68%), the ulcers were on the legs or feet. Of these, 16 patients had multiple ulcers, including eight who had bilateral ulcers. Two other patients had multiple ulcers spread over the body (Fig. 2). The total number of patients with multiple ulcers was therefore 18 (41%). The size of the ulcers ranged from 2 mm × 2 mm to 370 mm × 110 mm. Clinically, infection was suspected in 15 patients (13 of whom had ulcerating pyoderma); eight patients were thought to have a malignancy and seven had a traumatic ulcer. None of the patients showed clinical venous or arterial insufficiency. None of the patients was diabetic. In 14 patients, a clinical diagnosis could not be made.Histopathologic findingsHistologic examination was performed in 34 (77%) of the 44 patients; four patients refused to have a biopsy taken and, in six patients, a biopsy was not indicated on the basis of the clinical picture. Eleven patients had malignancies, six (55%) of which were squamous cell carcinoma, four (36%) were Kaposi’s sarcoma, and one was dermatofibrosarcoma protuberans. An inflammatory reaction suggestive of infection was noted in 20 biopsies (59%).
Figure 1. Age and sex distribution of study population.
0
5
10
15
0-18 19-40 41-60 >61age
num
ber
of
pati
ents male (n=31)
female (n=13)
proefschrift Zegelaars.indb 71 4-2-2008 9:22:21
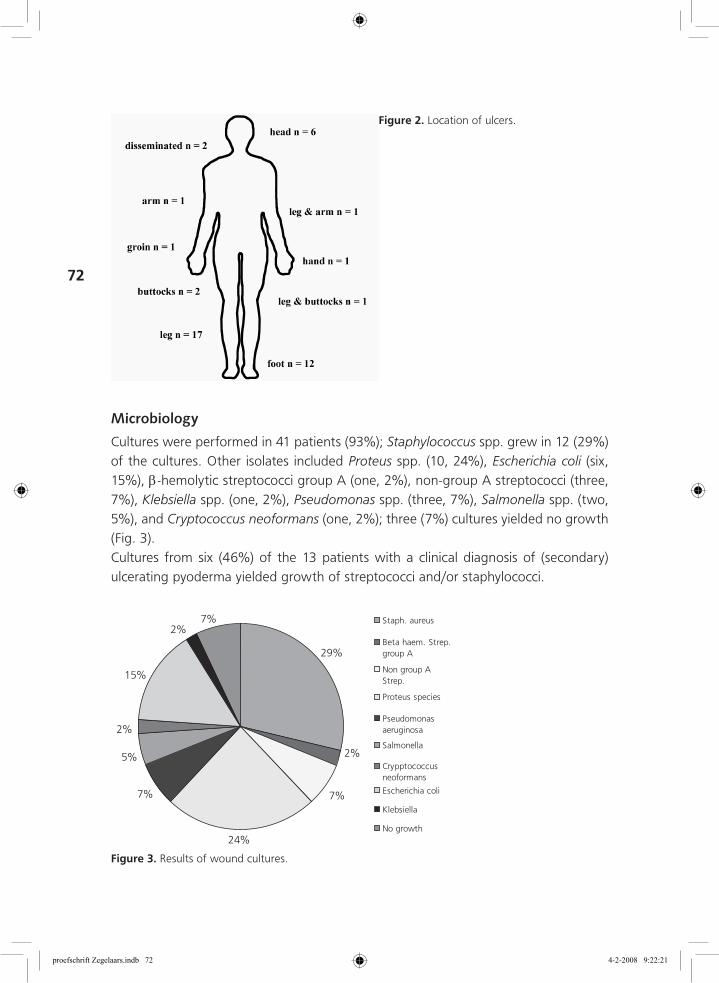
72
Microbiology
Cultures were performed in 41 patients (93%); Staphylococcus spp. grew in 12 (29%) of the cultures. Other isolates included Proteus spp. (10, 24%), Escherichia coli (six, 15%), β-hemolytic streptococci group A (one, 2%), non-group A streptococci (three, 7%), Klebsiella spp. (one, 2%), Pseudomonas spp. (three, 7%), Salmonella spp. (two, 5%), and Cryptococcus neoformans (one, 2%); three (7%) cultures yielded no growth (Fig. 3).Cultures from six (46%) of the 13 patients with a clinical diagnosis of (secondary) ulcerating pyoderma yielded growth of streptococci and/or staphylococci.
Figure 2. Location of ulcers.
2%
7%
24%
7%
5%
7%
29%
2%
15%
2%
Staph. aureus
Beta haem. Strep.group A
Non group AStrep.
Proteus species
Pseudomonasaeruginosa
Salmonella
Crypptococcusneoformans
Escherichia coli
Klebsiella
No growth
Figure 3. Results of wound cultures.
proefschrift Zegelaars.indb 72 4-2-2008 9:22:21
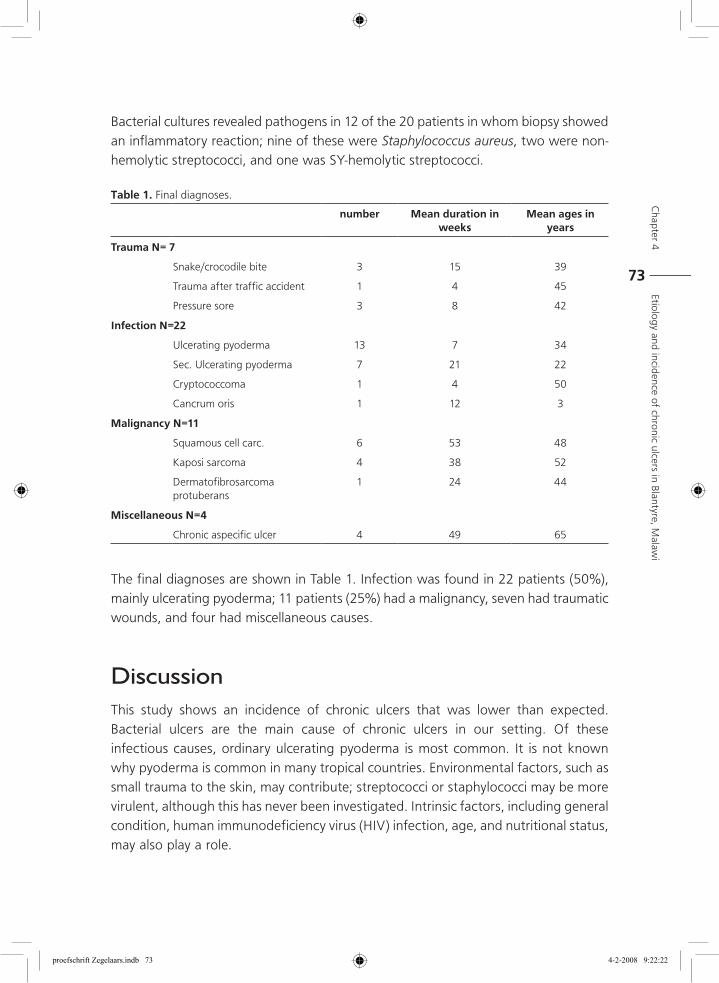
Chapter 4
Etiolo
gy and incidence of chronic ulcers in B
lantyre, Malaw
i
73
Bacterial cultures revealed pathogens in 12 of the 20 patients in whom biopsy showed an inflammatory reaction; nine of these were Staphylococcus aureus, two were non-hemolytic streptococci, and one was SY-hemolytic streptococci.
Table 1. Final diagnoses.
number Mean duration in weeks
Mean ages in years
Trauma N= 7
Snake/crocodile bite 3 15 39
Trauma after traffic accident 1 4 45
Pressure sore 3 8 42
Infection N=22
Ulcerating pyoderma 13 7 34
Sec. Ulcerating pyoderma 7 21 22
Cryptococcoma 1 4 50
Cancrum oris 1 12 3
Malignancy N=11
Squamous cell carc. 6 53 48
Kaposi sarcoma 4 38 52
Dermatofibrosarcoma protuberans
1 24 44
Miscellaneous N=4
Chronic aspecific ulcer 4 49 65
The final diagnoses are shown in Table 1. Infection was found in 22 patients (50%), mainly ulcerating pyoderma; 11 patients (25%) had a malignancy, seven had traumatic wounds, and four had miscellaneous causes.
DiscussionThis study shows an incidence of chronic ulcers that was lower than expected. Bacterial ulcers are the main cause of chronic ulcers in our setting. Of these infectious causes, ordinary ulcerating pyoderma is most common. It is not known why pyoderma is common in many tropical countries. Environmental factors, such as small trauma to the skin, may contribute; streptococci or staphylococci may be more virulent, although this has never been investigated. Intrinsic factors, including general condition, human immunodeficiency virus (HIV) infection, age, and nutritional status, may also play a role.
proefschrift Zegelaars.indb 73 4-2-2008 9:22:22
74
A surprisingly large number of malignancies were found. The occurrence of squamous cell carcinoma in long-standing chronic ulcers in Africans is well recognized.8 Delayed wound healing results in chronic inflammation, which can give rise to the phenomenon of “scar cancers.” Most patients did not report a long duration of their ulcers. One may speculate that these malignant ulcers existed for a much longer period than reported by the patients. A recent study at QECH showed an HIV prevalence of 70% and 36% amongst medical and surgical admissions, respectively.9 In our study group, HIV prevalence may therefore be suspected to be high; five patients had acquired immunodeficiency syndrome (AIDS)-defining illnesses (four Kaposi’s sarcoma and one cryptococcoma). HIV infection might contribute to impaired wound healing. There is also evidence that suppressed cell-mediated immune responses and angiogenesis, and reduced apoptosis, as seen in HIV infection, may favor the development of malignancies.10 We speculate that this might explain the large number of malignancies seen in this study.No diabetic, venous, or arterial ulcers were found. This is in contrast with the results observed in developed countries, and also in studies performed in other African countries, in which diabetes, in particular, seems to be an important cause of chronic ulcers.11
Mycobacterial ulcers, which have been reported to occur in Malawi, were not detected in this study.In conclusion, bacterial infections are the most common cause of chronic skin ulcers in Malawi. A surprisingly large number of malignancies were found in this study. One may speculate that HIV infection is a contributing factor. Because of the large number of malignancies, we recommend early histopathologic investigation of chronic ulcers in this part of Africa.
Acknowledgements
We thank the staff of the Department of Dermatology and the Departments of Medicine, Surgery and Pediatrics for their assistance. This study was supported by a grant from the Netherlands Society for Tropical Medicine.
References 1. Sturm AW, Jamil B, McAdam KPWJ, Khan KZ, Parveen S, Chiang T, Hussain R. Microbial
colonizers in leprosy skin ulcers and intensity of inflammation. Int J Lepr 1996; 64: 274-281.
2. Robinson DC, Hay RJ. Tropical ulcer in Zambia. Trans R Soc Trop Med Hyg 1986; 80: 132-137.
3. Ohanaka EC, Osarenkhoe O. In-patient management of leg ulcers. East Afr Med J 1999; 76: 687-689.
proefschrift Zegelaars.indb 74 4-2-2008 9:22:22
Chapter 4
Etiolo
gy and incidence of chronic ulcers in B
lantyre, Malaw
i
75
4. Herwaldt BL. Leishmaniasis. Lancet 1999; 354: 1191-1199.
5. van der Werf TS, van der Graaf WT, Tappero JW, Asiedu K. Mycobacterium ulcerans infection. Lancet 1999; 354: 1013-8.
6. Sarkar PK, Ballantyre S. Management of leg ulcers. Postgrad Med J 2000; 76: 674-682.
7. Komolafe OO, Mangani CB. Chronic wounds at QECH, Malawi Med J 2001; 13: 19-20.
8. Yakubu A, Mabogunje OA. Squamous cell carcinoma of the skin in Africans. Trop Geogr Med 1995: 2; 91-93.
9. Lewis DK, Callaghan M, Phiri K, Chipwete J, Kublin JG, Borgstein E, Zijlstra EE. Prevalence and indicators of HIV and AIDS among adults admitted to medical and surgical wards in Blantyre, Malawi. Trans R Soc Trop Med Hyg 2003; 97 (1): 91-96.
10. Dalgleish AG, O’Byrne KJ. Chronic immune activation and inflammation in the pathogenesis of AIDS and cancer. Adv Cancer Res 2002; 84: 231-76.
11. Motala AA, Omar MA, Pirie FJ. Diabetes in Africa. Epidemiology of type 1 and type 2 diabetes in Africa. J Cardiovasc Risk. 2003; 10 (2): 77-83.
proefschrift Zegelaars.indb 75 4-2-2008 9:22:22

proefschrift Zegelaars.indb 76 4-2-2008 9:22:22
Chapter
5Tolerability and efficacy of hydrocolloid dressings in the treatment of venous leg ulcers under tropical conditions: an open prospective study
Jim E. Zeegelaar, Wies Langenberg, Ricardo Hu, Rudy F.M. Lai A Fat, William R. Faber
Published in: Journal of the European Academy of Dermatology and Venereology 2001;15(3):234-7
proefschrift Zegelaars.indb 77 4-2-2008 9:22:22
78
AbstractIn the Western world, hydrocolloid dressings are widely used in wound treatment. However, little is known about their tolerability and efficacy under tropical conditions. The purpose of this study was to assess the tolerability and efficacy of a hydrocolloid dressing in combination with short stretch compressive bandages under tropical conditions. Seventeen patients with venous leg ulcers attending an outpatient clinic in Surinam were enrolled in the study for a period of 6 weeks. Swabs for bacterial cultures were taken at the beginning and end of the study. All ulcers showed a good healing tendency. Percentage of granulation tissue in the ulcers improved from mean 27% at start to 92% at the end. Mean circumference at start was 9.9 cm, at the end 4.9 cm. Exudation diminished from moderate in six and severe in eight ulcers, to moderate in 10 and almost none in two ulcers. In general, the dressing was very well accepted, pain was never reported. Leakage was noticed 39 times in the 164 dressing changes. This study revealed no differences in the rate of bacterial infections or colonization of wounds compared with studies performed in temperate regions. Our data indicate that hydrocolloid dressings can be used under tropical conditions.
proefschrift Zegelaars.indb 78 4-2-2008 9:22:22
Chapter 5
Tolerability and efficacy of hydrocolloid dressings in the treatm
ent of venous leg ulcers under tropical conditions
79
IntroductionSeveral studies have shown that a moist environment favours wound healing.1;2 For this reason, many (semi)occlusive dressings have been developed. One of these dressings is the hydrocolloid dressing.3-8 These opaque, absorbent dressings consist of hydrocolloid granules embedded in an adhesive matrix covered by a polyurethane foam. In the Western world, these dressings are now widely used in the management of (leg) ulcers. However, little is known about their use under tropical conditions. Alleged increases in the frequency of wound infection may be an important reason that hydrocolloids are not used regularly under these conditions.9-11 One study performed in a south Indian hospital described good results in treating chronic ulcers mostly secondary to leprosy; however, no bacterial studies were performed.12 We studied the tolerability and efficacy of a hydrocolloid dressing for venous leg ulcers under humid tropical conditions.
Patient and MethodsThe study was performed in Paramaribo, which is the capital city of Surinam. It has a tropical climate with annual temperatures between 22.8 °C and 32.2 °C and more than 2032 mm of rainfall per year. The study was carried out during the rainy season with a humidity fluctuating at about 95%.All patients received written and spoken information, and written informed consent was obtained. The study was approved by the local Ethics Committee.Patients with a venous leg ulcer attending the outpatient clinic at the Department of Dermatology of the Academic Hospital Paramaribo in Surinam were included; the ulcers were less than 6 cm length and less than 4 cm wide and diagnosis was based on clinical signs for venous insufficiency, other diagnostic procedures were not available. Specific exclusion criteria were diabetes mellitus, congestive heart failure, malignancy or ankle/brachial index less then 0.75.All ulcers were treated with a hydrocolloid dressing (Comfeel Plus TransparantR and Comfeel Plus UlcerR, Coloplast, Humlebaek, Denmark) for a period of 6 weeks. Dressing and bandages (ElkoR, Lohmann, Neuwied, Germany) were normally changed twice weekly, but more often when necessary. Short stretch bandages were applied. The bandages remained on day and night. All patients were mobile.Evaluations were recorded at every visit until the end of the study or until the ulcer showed 100% granulation or complete re-epithelialization. Ulcer outline was traced on a transparent pouch and pictures were taken. The ulcer area was measured from the transparent pouch using a computer image analysis system. Clinical improvement
proefschrift Zegelaars.indb 79 4-2-2008 9:22:22
80
was recorded by means of percentage of granulation tissue on a scale of 0%, 25%, 50% or 100%. The amount of exudate was defined as almost none, moderate or strong. The skin around the ulcer was inspected and maceration and redness were recorded; user friendliness of the dressing (defined as easy or difficult to apply) and patient comfort (painful, not painful) were documented. Clinical signs of infection of the ulcer (redness, warmth, pain) were recorded. Scoring was performed by one observer.Swabs were taken for bacterial cultures at the beginning and at the end of the study. The swabs were immediately placed in 400 mL 8% glycerol/Pepton in a sterile screw-cap container. The containers, containing specimens were placed in a freezer at −20 °C. Also, smears were taken for Gram staining.Specimens were transported to the diagnostic laboratory of microbiology in the Netherlands on dry ice and stored at −70 °C until further processing. Specimens were defrosted and subsequently inoculated and incubated according to standard procedures on selective and non-selective agars in air, 7% CO2 and anaerobic conditions. When necessary additional media and/or incubation conditions were applied depending on the Gram stain used.
ResultsSeventeen patients (10 men and seven women) were included of whom 14 patients completed the study. Three patients dropped out because of non-compliance. The average age of the patients was 59 years (range 38–87). All patients had unilateral ulcers, 14 ulcers were localized on the medial and three on the lateral gaiter area of the leg. The mean duration of ulceration at the start of the study was 13 months (range 2 months to 10 years). The mean size of the ulcers was 9.9 cm2 (range 5.5–18.7 cm2) at start and 4.9 cm2 (range 0–10.5) at the end of the study; two ulcers showed complete re-epithelialization during the study period (one at week 3 and one at week 4).Percentage of granulation tissue formation improved from mean of 27% at start to 92% at the end of the study. Nine ulcers showed 100% granulation and three ulcers showed less than 90% granulation tissue at week 6 (Table 1).Exudation of all ulcers was moderate in eight ulcers and strong in nine ulcers at the start of the study. At the end all ulcers that had not yet closed showed moderate exudation in 10 ulcers and almost none in two ulcers. The dressings were easy to handle and could be removed without causing pain. Patients described the dressing as comfortable and pain was never reported. Leakage of the dressing was noticed
proefschrift Zegelaars.indb 80 4-2-2008 9:22:22
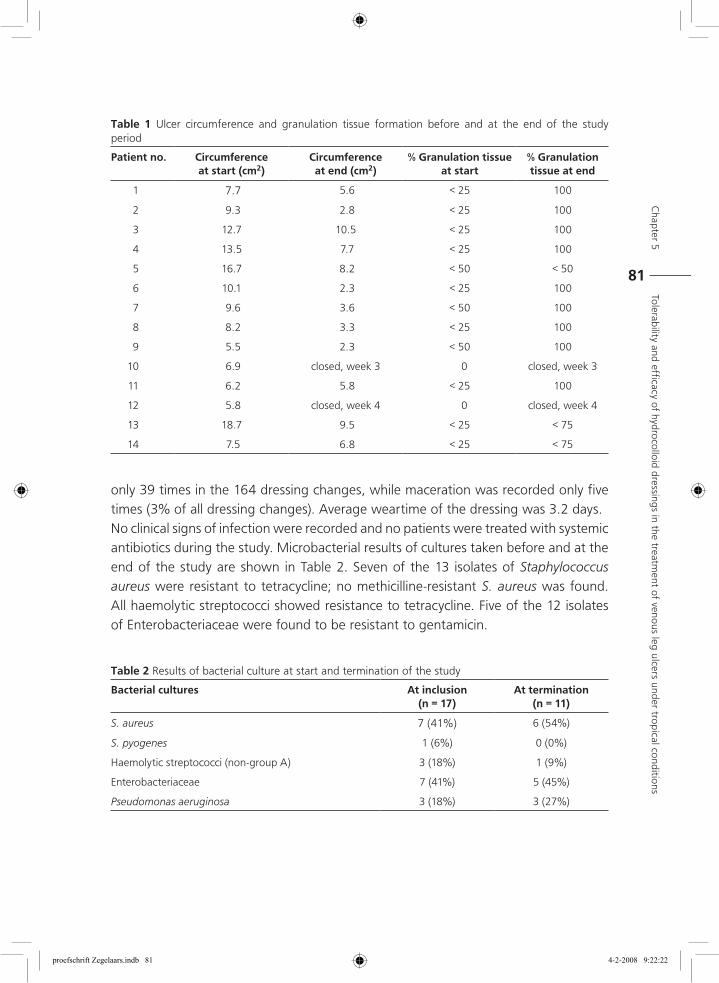
Chapter 5
Tolerability and efficacy of hydrocolloid dressings in the treatm
ent of venous leg ulcers under tropical conditions
81
only 39 times in the 164 dressing changes, while maceration was recorded only five times (3% of all dressing changes). Average weartime of the dressing was 3.2 days.No clinical signs of infection were recorded and no patients were treated with systemic antibiotics during the study. Microbacterial results of cultures taken before and at the end of the study are shown in Table 2. Seven of the 13 isolates of Staphylococcus aureus were resistant to tetracycline; no methicilline-resistant S. aureus was found. All haemolytic streptococci showed resistance to tetracycline. Five of the 12 isolates of Enterobacteriaceae were found to be resistant to gentamicin.
Table 1 Ulcer circumference and granulation tissue formation before and at the end of the study period
Patient no. Circumference at start (cm2)
Circumference at end (cm2)
% Granulation tissue at start
% Granulation tissue at end
1 7.7 5.6 < 25 100
2 9.3 2.8 < 25 100
3 12.7 10.5 < 25 100
4 13.5 7.7 < 25 100
5 16.7 8.2 < 50 < 50
6 10.1 2.3 < 25 100
7 9.6 3.6 < 50 100
8 8.2 3.3 < 25 100
9 5.5 2.3 < 50 100
10 6.9 closed, week 3 0 closed, week 3
11 6.2 5.8 < 25 100
12 5.8 closed, week 4 0 closed, week 4
13 18.7 9.5 < 25 < 75
14 7.5 6.8 < 25 < 75
Table 2 Results of bacterial culture at start and termination of the study
Bacterial cultures At inclusion (n = 17)
At termination (n = 11)
S. aureus 7 (41%) 6 (54%)
S. pyogenes 1 (6%) 0 (0%)
Haemolytic streptococci (non-group A) 3 (18%) 1 (9%)
Enterobacteriaceae 7 (41%) 5 (45%)
Pseudomonas aeruginosa 3 (18%) 3 (27%)
proefschrift Zegelaars.indb 81 4-2-2008 9:22:22
82
DiscussionIn developing countries chronic leg ulcers present an important health problem. Ulcers caused by venous disease may play a minor part and ulcers caused by infectious disease or sickle-cell anaemia may be more important.13;14 It is important to treat the cause of ulceration; if the underlying causes are not treated then even the best dressings are not effective.15 Because of financial problems hydrocolloid dressings are often not used in many developing countries. However, economic analyses show that the financial aspect of these dressings compared with classic dressings, such as cotton gauze, may be in favour of hydrocolloid dressings.16,17 Although the costs of hydrocolloid dressings are much higher than other dressings, hydrocolloid dressings can be changed every 2–5 days, sometimes even once a week. In this study, dressings were changed twice weekly because of hygienic considerations; in this hot and humid climate compressive dressings become easily wet and dirty.This pilot study clearly shows that hydrocolloids are very well tolerated by patients in a tropical climate. There were no problems with the adhering capacity of the hydrocolloid used. All ulcers showed a very good healing tendency and apart from maceration in three patients no adverse events were noticed. It is important to note that during this study compression therapy was given, this may explain the quick wound closure seen with some patients.In this study no infections were noted, which is consistent with the use of hydrocolloid dressings in moderate climates.11 The microorganisms found are not much different from those found in studies performed in the Western world.18-20 Pathogenic microorganisms were not found more often, and the presence of bacteria do not appear to have interfered with wound healing.The high rate of bacterial strains resistant to tetracycline and gentamicin may be explained by the extensive use of these antibiotics in ointments for wound care in Suriname. The use of antibiotic containing ointments is not recommended because of the possible development of bacterial resistance and the risk of causing contact allergic reactions.21;22 Moreover, in most chronic wounds use of antibiotics appears to be unnecessary.23
ConclusionThis study indicates that hydrocolloid dressings may function well in the extreme humid conditions of a tropical climate. No infections were noted in the group studied. This
proefschrift Zegelaars.indb 82 4-2-2008 9:22:22
Chapter 5
Tolerability and efficacy of hydrocolloid dressings in the treatm
ent of venous leg ulcers under tropical conditions
83
study revealed no differences in the frequency of bacterial infection or colonization of the wound from those recorded in studies performed in temperate regions.
Aknowledgement
This study was supported by Coloplast AS Danmark. With kind regards to Surinam Airways for shipping the medical equipment.
References 1 Winter GD. Formation of scab and the rate of epithelization of superficial wounds in the skin
of the domestic pig. Nature. 1962; 193: 293–294.
2 Dyson M, Young S, Pendle CL et al. Comparison of the effects of moist and dry conditions on dermal repair. J Invest. Dermatol. 1988; 91: 434–439.
3 Friedman JS & Su WPD. Management of leg ulcers with hydrocolloid occlusive dressing. Arch. Dermatol. 1984; 120: 1329–1336.
4 Nemeth AJ & Eaglstein WH. Wound dressings and local treatment. In: Westerhof W editor. Leg Ulcers; Diagnosis and Treatment. Elsevier Science Publishers, Amsterdam, 1993: 325–333.
5 Eaglestein WH. Occlusive dressings. J Dermatol. Surg. Oncol. 1993; 19: 716–720.
6 Schilling RSF, Roberts M, Goodman N. Clinical trial of occlusive plastic dressings. Lancet. 1950; 18: 293–296.
7 Gamborg Np Munk Madsen S & Stromberg L. Treatment of chronic leg ulcers with a hydrocolloid dressing. Acta Derm. Venereol. (Stockh) 1990; Suppl. 152: 1–12.
8 Falanga V. Occlusive wound dressings: Why, When, Which? Arch. Dermatol. 1988; 124: 872–906.
9 Mertz PM & Eaglstein WH. The effect of a semiocclusive dressing on the microbial population in superficial wounds. Arch. Surg. 1984; 119: 287–289.
10 Aly R, Shirley C, Cunico B, Maibach HI. Effect of prolonged occlusion on the microbial flora, pH, carbon dioxide, and transepidermal water loss on human skin. J Invest. Dermatol. 1978; 71: 378–381.
11 Hutchinson JJ & Lawrence JC. Wound infection under occlusive dressing. Hosp. Infect. 1991; 17: 83–68.
12 Mumford JW & Mumford SP. Occlusive hydrocolloid dressings applied to chronic neuropathic ulcers. In.t J Dermatol. 1988; 27: 190–192.
13 Worsfold JT. Varicose veins in Tropical Africa. Lancet 1974; ii: 1322–1323.
14 Daynes G & Beighton P. Prevalence of varicose veins in Africans. Br. Med. J. 1973; 3: 354.
15 de Vries HJC, van Zuijlen PPM, Middelkoop E, Westerhof W. Die function von Hautersatz bei der behandlung nichtt heilender wunden. Z Hautkr. 1999; 74: 675–682.
16 Ohlsson P, Larsson K, Lindholm C, Möller M. A cost effectiveness study of leg ulcer treatment in primary care. Comparison of saline-gauze and DuodermR – treatment in a prospective, randomized study. In: Lindholm C, Thesis. Leg Ulcer Patients. Malmö. Chapter IV, 1993.
proefschrift Zegelaars.indb 83 4-2-2008 9:22:22
84
17 Apelqvist J, Ragnarson-Tennvall G, Larsson J. Topical treatment of diabetic foot ulcers: an economic analysis of treatment alternatives and strategies. Diabet.Med. 1995; 12: 123–128.
18 Erikson G, Eklund AE, Kallings LO. The clinical significance of bacterial growth in venous leg ulcers. Scand.J Infect.Dis. 1984; 16: 175–180.
19 Lookingbill DP, Miller SH, Knowles RC. Bacteriology of chronic leg ulcers. Arch. Dermatol. 1978; 114: 1765–1768.
20 Niedner R & Schopf E. Wound infections and antibacterial therapy. In: Leg Ulcers: Diagnosis and Treatment (Westerhof W. eds). Elsevier Science Publishers, Amsterdam, 1993: 293–303.
21 Breit R. Allergen change in stasis dermatitis. Contact Dermatitis.1977; 3: 309–311.
22 Fraki JE, Peltonen L, Hopsu-Havu VK. Allergy to various components of topical preparations in stasis dermatitis and leg ulcer. Contact Dermatitis. 1979; 5: 97–100.
23 Alinovi A, Bassissi P, Pini M. Systemic administration of antibiotics in the management of venous ulcers. J Am. Acad. Dermatol. 1986; 15: 186–191.
proefschrift Zegelaars.indb 84 4-2-2008 9:22:22
Chapter
6Changing pattern of imported cutaneous leishmaniasis in The Netherlands
Jim E.Zeegelaar, Willemijn H. Steketee, Pieter A.M. van Thiel , Jose C.F.M. Wetsteyn, Piet A.Kager, William R.Faber.
Published in: Clinical and Experimental Dermatology. 2005 Jan;30(1):1-5.
proefschrift Zegelaars.indb 85 4-2-2008 9:22:22
86
SummaryCutaneous leishmaniasis (CL) in western countries seems to be appearing more frequently. Our aim was to determine if there has been a shift in countries where CL is acquired and whether the incidence has changed, and to assess current diagnostic procedures and treatment modalities. In a retrospective study medical records of patients with the diagnosis of CL at the Departments of Tropical Dermatology and Tropical Medicine, Academic Medical Cnter, Amsterdam, the Netherlands, from 1990 to 2000 were analysed. CL was diagnosed in 78 patients. The majority was acquired in Belize, Surinam, French Guyana and Bolivia. Giemsa stains were positive for the parasite in impression smears from 43% and in biopsies from 71%. Seventy-eight per cent of cases were culture-positive and 89% were PCR-positive. Sixty-two patients were treated systemically: pentavalent antimony (32), pentamidine isetionate (11), itraconazole (19), and 13 locally, the majority with a combination of cryosurgery and intralesional pentavalent antimony. Imported CL is becoming more frequent, with South and Middle American countries being important sources of infection. Multiple tests, of which PCR is the most sensitive, are required to confirm the diagnosis. Systemic treatment was given to the majority of the patients.
proefschrift Zegelaars.indb 86 4-2-2008 9:22:23
Chapter 6
Changing pattern of im
ported cutaneous leishm
aniasis in The Netherlands
87
Introductionleishmaniases are visceral, cutaneous and mucocutaneous diseases caused by parasites belonging to the genus Leishmania.1 Although cutaneous leishmaniasis (CL) is the mildest clinical form, it can cause considerable morbidity, and after healing often leaves disfiguring scars.2;3 All varieties are transmitted to humans by phlebotomine sandflies.4 The disease occurs throughout the tropical and subtropical regions of the world with an estimated 1.5–2 million cases per year, of which the majority is CL.5
The clinical picture is diverse and may vary from one or more papules, to ulcers with or without a scab. Lymphangitis may be present.6 Mucocutaneous leishmaniasis, although uncommon, may develop as a complication of New World-CL. The clinical picture depends on the species involved, the immune response of the host, host genetics, and probably the transmitting vector.7;8 Indications for treatment and current recommended treatment regimes vary.9-11 There are only a few double-blind clinical trials in which the exact Leishmania species is known. However, some treatments are well established.12;13
In the Netherlands leishmaniasis is seen as an imported skin disease, with a rising incidence in the last 10 years. A Dutch study described 49 patients with CL in the period 1979–1989; Mediterranean countries were the most important sources of infection.14 We found it of interest to see if a change in this pattern had occurred in the following years, and additionally, how sensitive our diagnostic procedures were, which treatments were given and how effective the results of treatment were. For this reason, incidence, clinical picture, treatment modalities and response of patients diagnosed with CL from January 1990 to January 2000 in our hospital were studied retrospectively.
Patients and methodfrom the records of 78 patients diagnosed with CL from January 1990 to January 2000 at the Academic Medical Center, the following data were extracted: age; area visited, reason for visit, dates of visit in endemic area; date that a lesion was first noticed; number, size and site of the lesions; results of histological examination of the lesion, of culture, impression smear and, if performed, PCR. Treatment modalities used, dose, duration and side effects, if they occurred, were also recorded. Response to treatment was defined as resolution of the lesion as assessed by the physicians. All patients were closely monitored during treatment until at least 6 weeks after finishing treatment by physicians of the Department of Dermatology and/or the Department
proefschrift Zegelaars.indb 87 4-2-2008 9:22:23
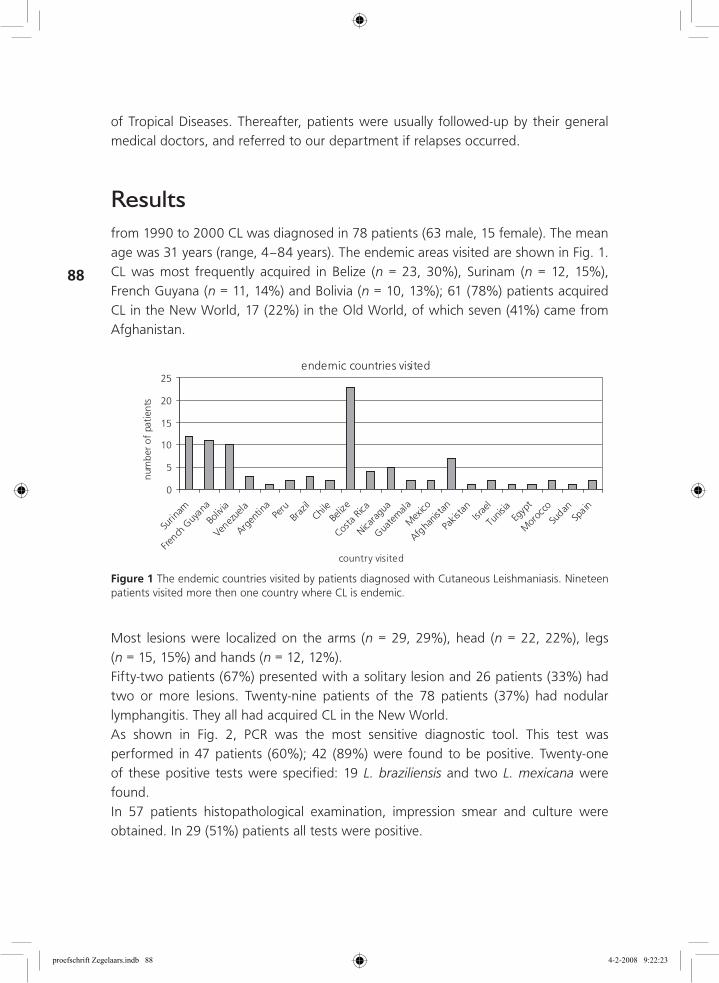
88
of Tropical Diseases. Thereafter, patients were usually followed-up by their general medical doctors, and referred to our department if relapses occurred.
Resultsfrom 1990 to 2000 CL was diagnosed in 78 patients (63 male, 15 female). The mean age was 31 years (range, 4–84 years). The endemic areas visited are shown in Fig. 1. CL was most frequently acquired in Belize (n = 23, 30%), Surinam (n = 12, 15%), French Guyana (n = 11, 14%) and Bolivia (n = 10, 13%); 61 (78%) patients acquired CL in the New World, 17 (22%) in the Old World, of which seven (41%) came from Afghanistan.
endemic countries visited
0
5
10
15
20
25
Surin
am
French
Guy
ana
Boliv
ia
Venez
uela
Argen
tina
Peru
Braz
ilChil
eBe
lize
Costa
Rica
Nicara
gua
Guate
mala
Mex
ico
Afgha
nista
n
Pakis
tan
Israe
l
Tunis
iaEg
ypt
Mor
occo
Sudan
Spain
country visited
num
ber
of
pati
ents
Figure 1 The endemic countries visited by patients diagnosed with Cutaneous Leishmaniasis. Nineteen patients visited more then one country where CL is endemic.
Most lesions were localized on the arms (n = 29, 29%), head (n = 22, 22%), legs (n = 15, 15%) and hands (n = 12, 12%).Fifty-two patients (67%) presented with a solitary lesion and 26 patients (33%) had two or more lesions. Twenty-nine patients of the 78 patients (37%) had nodular lymphangitis. They all had acquired CL in the New World.As shown in Fig. 2, PCR was the most sensitive diagnostic tool. This test was performed in 47 patients (60%); 42 (89%) were found to be positive. Twenty-one of these positive tests were specified: 19 L. braziliensis and two L. mexicana were found.In 57 patients histopathological examination, impression smear and culture were obtained. In 29 (51%) patients all tests were positive.
proefschrift Zegelaars.indb 88 4-2-2008 9:22:23
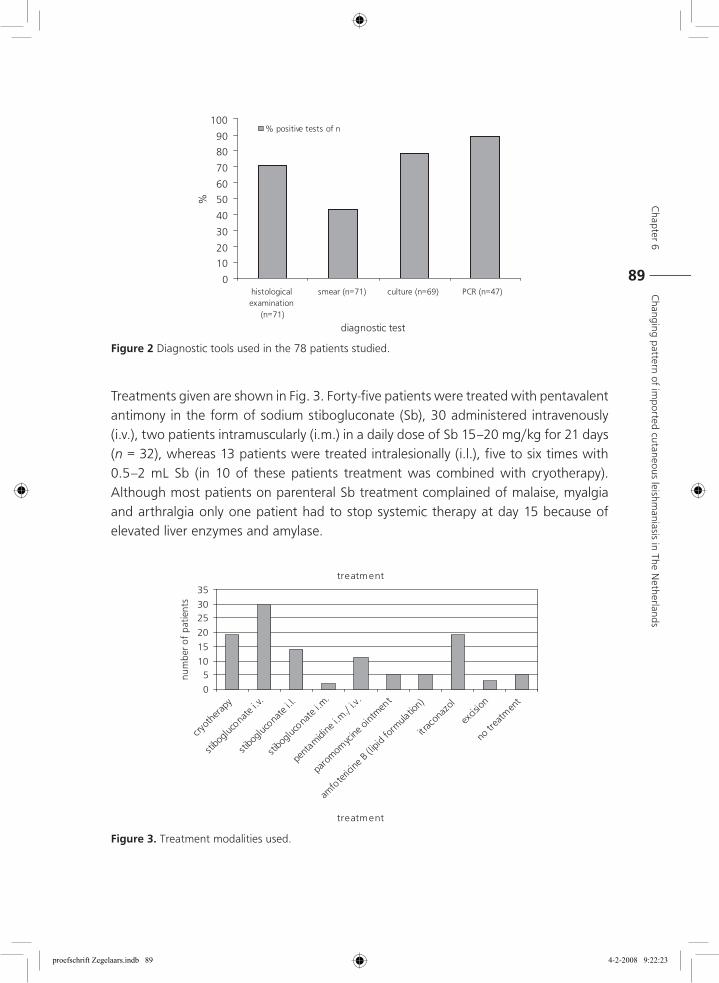
Chapter 6
Changing pattern of im
ported cutaneous leishm
aniasis in The Netherlands
89
Treatments given are shown in Fig. 3. Forty-five patients were treated with pentavalent antimony in the form of sodium stibogluconate (Sb), 30 administered intravenously (i.v.), two patients intramuscularly (i.m.) in a daily dose of Sb 15–20 mg/kg for 21 days (n = 32), whereas 13 patients were treated intralesionally (i.l.), five to six times with 0.5–2 mL Sb (in 10 of these patients treatment was combined with cryotherapy). Although most patients on parenteral Sb treatment complained of malaise, myalgia and arthralgia only one patient had to stop systemic therapy at day 15 because of elevated liver enzymes and amylase.
0
10
20
30
40
50
60
70
80
90
100
histologicalexamination
(n=71)
smear (n=71) culture (n=69) PCR (n=47)
diagnostic test
%
% positive tests of n
Figure 2 Diagnostic tools used in the 78 patients studied.
treatment
0
510
15
20
2530
35
cryot
hera
py
stibo
gluco
nate
i.v.
stibo
gluco
nate
i.l.
stibo
gluco
nate
i.m.
pent
amidi
ne i.m
./ i.v
.
paro
momyc
ine o
intmen
t
amfo
teric
ine B
(lipid
form
ulatio
n)
itrac
onaz
ol
excis
ion
no tr
eatm
ent
treatment
num
ber o
f pa
tient
s
Figure 3. Treatment modalities used.
proefschrift Zegelaars.indb 89 4-2-2008 9:22:23
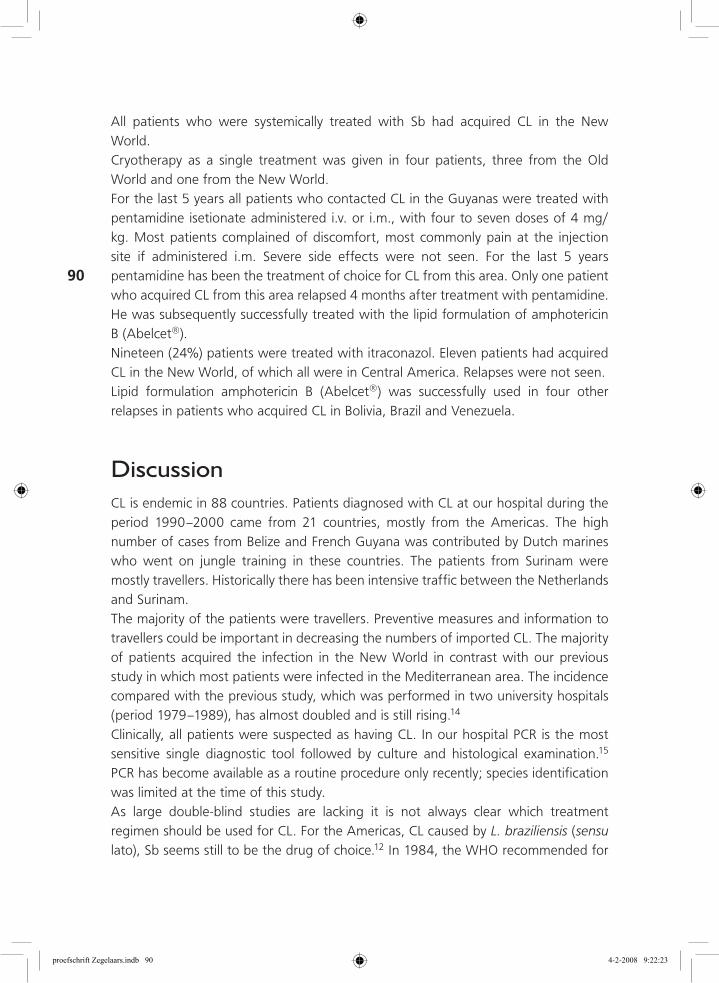
90
All patients who were systemically treated with Sb had acquired CL in the New World.Cryotherapy as a single treatment was given in four patients, three from the Old World and one from the New World.For the last 5 years all patients who contacted CL in the Guyanas were treated with pentamidine isetionate administered i.v. or i.m., with four to seven doses of 4 mg/kg. Most patients complained of discomfort, most commonly pain at the injection site if administered i.m. Severe side effects were not seen. For the last 5 years pentamidine has been the treatment of choice for CL from this area. Only one patient who acquired CL from this area relapsed 4 months after treatment with pentamidine. He was subsequently successfully treated with the lipid formulation of amphotericin B (Abelcet®).Nineteen (24%) patients were treated with itraconazol. Eleven patients had acquired CL in the New World, of which all were in Central America. Relapses were not seen.Lipid formulation amphotericin B (Abelcet®) was successfully used in four other relapses in patients who acquired CL in Bolivia, Brazil and Venezuela.
DiscussionCL is endemic in 88 countries. Patients diagnosed with CL at our hospital during the period 1990–2000 came from 21 countries, mostly from the Americas. The high number of cases from Belize and French Guyana was contributed by Dutch marines who went on jungle training in these countries. The patients from Surinam were mostly travellers. Historically there has been intensive traffic between the Netherlands and Surinam.The majority of the patients were travellers. Preventive measures and information to travellers could be important in decreasing the numbers of imported CL. The majority of patients acquired the infection in the New World in contrast with our previous study in which most patients were infected in the Mediterranean area. The incidence compared with the previous study, which was performed in two university hospitals (period 1979–1989), has almost doubled and is still rising.14
Clinically, all patients were suspected as having CL. In our hospital PCR is the most sensitive single diagnostic tool followed by culture and histological examination.15 PCR has become available as a routine procedure only recently; species identification was limited at the time of this study.As large double-blind studies are lacking it is not always clear which treatment regimen should be used for CL. For the Americas, CL caused by L. braziliensis (sensu lato), Sb seems still to be the drug of choice.12 In 1984, the WHO recommended for
proefschrift Zegelaars.indb 90 4-2-2008 9:22:23
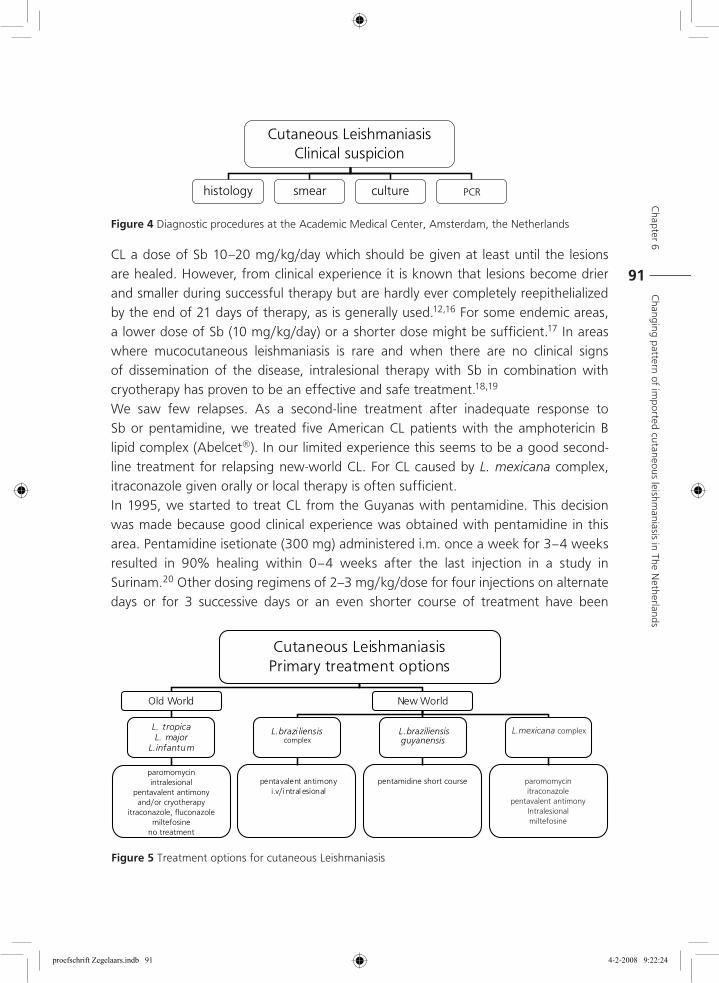
Chapter 6
Changing pattern of im
ported cutaneous leishm
aniasis in The Netherlands
91CL a dose of Sb 10–20 mg/kg/day which should be given at least until the lesions are healed. However, from clinical experience it is known that lesions become drier and smaller during successful therapy but are hardly ever completely reepithelialized by the end of 21 days of therapy, as is generally used.12,16 For some endemic areas, a lower dose of Sb (10 mg/kg/day) or a shorter dose might be sufficient.17 In areas where mucocutaneous leishmaniasis is rare and when there are no clinical signs of dissemination of the disease, intralesional therapy with Sb in combination with cryotherapy has proven to be an effective and safe treatment.18,19
We saw few relapses. As a second-line treatment after inadequate response to Sb or pentamidine, we treated five American CL patients with the amphotericin B lipid complex (Abelcet®). In our limited experience this seems to be a good second-line treatment for relapsing new-world CL. For CL caused by L. mexicana complex, itraconazole given orally or local therapy is often sufficient.In 1995, we started to treat CL from the Guyanas with pentamidine. This decision was made because good clinical experience was obtained with pentamidine in this area. Pentamidine isetionate (300 mg) administered i.m. once a week for 3–4 weeks resulted in 90% healing within 0–4 weeks after the last injection in a study in Surinam.20 Other dosing regimens of 2–3 mg/kg/dose for four injections on alternate days or for 3 successive days or an even shorter course of treatment have been
Cutaneous LeishmaniasisClinical suspicion
histology smear culture PCR
Figure 4 Diagnostic procedures at the Academic Medical Center, Amsterdam, the Netherlands
Cutaneous LeishmaniasisPrimary treatment options
Old World New World
L. tropicaL. major
L.infantum
L.brazi liensiscomplex
L. braziliensisguyanensis
pentavalent antimonyi.v/i ntral esional
paromomycinintralesional
pentavalent antimonyand/or cryotherapy
itraconazole, fluconazolemiltefosine
no treatment
pentamidine short course paromomycinitraconazole
pentavalent antimonyIntralesionalmiltefosine
L.mexicana complex
Figure 5 Treatment options for cutaneous Leishmaniasis
proefschrift Zegelaars.indb 91 4-2-2008 9:22:24
92
reported from French Guyana, Guyana and Colombia.21,22 In most studies parasites were not cultured.Old World-CL often does not require treatment because of the tendency of spontaneous cure. To speed up healing, intralesional Sb until blanching (generally 0.5–4 mL) on alternate days (four to five injections) is highly effective. It can be combined with cryotherapy. Itraconazole given orally 100 mg twice a day is reported to be effective; however, studies are limited.23 Our experience with itraconazole is too limited to draw conclusions. Recently, a study performed in Saudi Arabia showed that a 6-week course of oral fluconazole is safe and effective for CL caused by L. major.24 Flowcharts for diagnostic procedures and treatments given in our hospital are given in Fig. 4 and Fig. 5.It can be concluded that in our hospital, imported CL is seen with a rising incidence. South American countries have become more important origins of infection. This rising incidence was caused by marines on training in the jungle and by travellers. PCR is the most sensitive single diagnostic test. If L. braziliensis (sensu lato) is suspected, Sb is still the drug of choice. The doses and duration of therapy with Sb might be lower or shorter in some endemic areas, but if the recommended dose and duration of treatment in a specific area is not known a schedule of 20 mg/kg/day for 21 days is almost always sufficient. For infection with L. mexicana, itraconazole is our drug of choice. For L. braziliensis guyanensis acquired in the Guyanas, four injections of pentamidine at 4 mg/kg seems to be the drug of choice.20-22 If facilities are available it is recommended that culture be performed to characterize and specify the parasite, so that treatment can be based on the species involved.
Acknowledgements
With special thanks for performing PCR to the Department of Parasitology, Academic Medical Center, Amsterdam (Head, T.van Gool) and the Department of Parasitology, Leiden University Medical Centre, Leiden, the Netherlands (Head, A.M. Polderman).
References 1 Dedet JP, Pratlong F, Lanotte G, Ravel C. Cutaneous leishmaniasis. The parasite. Clin. Dermatol.
1999; 17: 261-8.
2 Salman SM, Rubeiz NG, Kibbi A-G. Cutaneous Leishmaniasis: clinical features and diagnosis. Clin Dermatol. 1999; 17: 291-296.
3 Grevelink SA, Lerner EA. Leishmaniasis. J Am. Acad. Dermatol. 1996; 34: 257-272.
4 Killick-Kendrick R. The biology and control of phlebotomine sand flies. Clin. Dermatol. 1999; 17: 279-89.
proefschrift Zegelaars.indb 92 4-2-2008 9:22:24
Chapter 6
Changing pattern of im
ported cutaneous leishm
aniasis in The Netherlands
93
5 Desjeux P. Leishmaniasis. Public health aspects and control. Clin. Dermatol. 1996; 14: 417-23.
6 Choi CM, Lerner EA. Leishmaniasis as an emerging infection. J Investig. Dermatol. Symp Proc. 2001; 6: 175-82.
7 el-Hassan AM, Zijlstra EE. Leishmaniasis in Sudan. Mucosal leishmaniasis. Trans. R. Soc. Trop. Med. Hyg. 2001; 95 (Suppl 1): S19-26.
8 Herwaldt BL. Leishmaniasis. Lancet. 1999; 354: 1191-9.
9 Morris RV, Shoemaker CB, David JR, Lanzaro GC, Titus RG. Sandfly maxadilan exacerbates infection with Leishmania major and vaccinating against it protects against L. major infection. J Immunol. 2001; 167: 5226-30.
10 Koff AB, Rosen T. Treatment of cutaneous leishmaniasis. J Am. Acad. Dermatol. 1994; 31: 696-708.
11 Berman JD. Human Leishmaniasis: clinical, diagnostic, and chemotherapeutic developments in the last 10 years. Clin. Inf. Dis. 1997; 24: 684-703.
12 Herwaldt BL, Berman JD. Recommendations for treating leishmaniasis with sodium stibogluconate (pentostam) and review of pertinent clinical studies. Am. J Trop. Med. Hyg. 1992; 46: 296-306.
13 Kager P.A. Leishmania species (Leishmaniasis). In: antimicrobial therapy and vaccines. Ed: Yu VL, Weber R, Raoult D. Apple Trees Productions, LLC 2002:1555-1580.
14 Faber WR, Becht M, van Ginkel CJ, et al. Cutaneous leishmaniasis in 49 patients in The Netherlands. Ned. Tijdschr. Geneeskd. 1991;135: 229-33. Dutch.
15 Faber WR, Oskam L, Gool T van, et al. Value of diagnostic techniques for cutaneous leishmaniasis. J Am. Acad. Dermatol. 2003;49 (1):70-4.
16 The leishmaniases. Report of WHO Expert Committee. WHO Tech Rep Ser 1984; 701: 99-109.
17 Oliveira-Neto MP, Schubach A, Mattos M, et al. A low-dose antimony treatment in 159 patients with American cutaneous leishmaniasis: extensive follow-up studies (up to 10 years). Am. J Trop. Med. Hyg. 1997; 57: 651-5
18 Gurei MS, Tatli N, Ozbilge H, et al. Efficacy of cryotherapy and intralesional pentostam in treatment of cutaneous leishmaniasis. J Egypt Soc.Parasitol. 2000; 30:169-76.
19 Tallab TM, Bahamdam KA, Mirdad S, et al. Cutaneous leishmaniasis: schedules for intralesional treatment with sodium stibogluconate. Int. J Dermatol. 1996; 35: 594-7.
20 Lai A Fat EJ, Vrede MA, Soetosenojo RM, Lai A Fat RF. Pentamidine, the drug of choice for the treatment of cutaneous leishmaniasis in Surinam. Int. J Dermatol. 2002; 41: 796-800
21 Soto-Mancipe J, Grogl M, Berman JD. Evaluation of pentamidine for the treatment of cutaneous leishmaniasis in Colombia. Clin. Infect. Dis. 1993; 16: 417-25.
22 Nacher M, Carme B, Ste Marie D, et al. Influence of clinical presentation on the efficacy of a short course of pentamidine in the treatment of cutaneous leishmaniasis in French Guyana. Ann of Tropical Med. Parasit 2001; 95: 331-336.
23 Momeni AZ, Jalayer T, Emamjomeh M, et al. Treatment of cutaneous leishmaniasis with itraconazole. Randomized double-blind study. Arch. Dermatol. 1996; 32: 784-6.
24 Alrajhi AA, Ibrahim EA, De Vol EB, et al. Fluconazole for the treatment of cutaneous leishmaniasis caused by Leishmania major. N. Engl. J Med. 2002; 346: 891-5.
proefschrift Zegelaars.indb 93 4-2-2008 9:22:24
proefschrift Zegelaars.indb 94 4-2-2008 9:22:24
Chapter
7First reported case of Mycobacterium ulcerans infection in a patient from China
William R. Faber, Lenka M. Pereira Arias-Bouda, Jim E. Zeegelaar, Arend H.J. Kolk, Pierre-Alain Fonteyne, Johan Toonstra and Francoise Portaels.
Published in: Transactions of the Royal Society of Tropical Medicine and Hygiene 2000 May-Jun;94(3):277-9.
proefschrift Zegelaars.indb 95 4-2-2008 9:22:24
96
AbstractBuruli ulcers have not been previously described in China, and only once at higher latitudes on the Northern Hemisphere. A patient who travelled in the Shan Dong Province in the Peoples Republic of China developed an ulcer which was proven to be a Buruli ulcer. The clinical picture and histopathological findings from biopsy are characteristic for a Buruli ulcer, and also the growth in culture (Coletsos medium) at a restricted temperature of 30 0C. A multiplex polymerase chain reaction (PCR) based on the amplification of the gene encoding for 16 S ribosomal RNA and a nested PCR based on the M. ulcerans specific repeated sequence 2404 were performed. These PCR investigations identified the bacteria as M. ulcerans, subspecies shinshuense. The patient was initially treated with clarithromycin and rifampicin, which was changed to ciprofloxacin and rifabutin when rifampicin resistance of the first isolate was established. There were no signs of reactivation of the disease six months after the end of treatment.M. ulcerans infection occurs above 300 latitude on the Northern hemisphere in China and is caused by M. ulcerans, subspecies shinshuense. This case appears to be cured by chemotherapy alone, in contrast to the general experience that surgical treatment is indicated. The granulomatous reaction with only fragments of acid fast bacteria in the biopsy at the end of treatment may indicate the development of an adequate cell mediated immune response leading to resistance to the infection.
proefschrift Zegelaars.indb 96 4-2-2008 9:22:24
Chapter 7
First reported case of M
ycobacterium
ulcerans infection in a patient from C
hina
97
IntroductionMycobacterium ulcerans infections are most common in tropical regions but have also been observed in temperate climatic areas of Australia.1 Until now, only 1 patient (from Japan) infected above the latitude 300 N has been reported.2
Recently, we observed a leg ulcer in a woman who had travelled in the Shan Dong province, Peoples Republic of China. In this report we describe the properties of the mycobacterium isolated from this lesion. It is the first reported case of Buruli ulcer in the Peoples Republic of China, and proves that M. ulcerans infection is also found in the temperate climatic zone of the Northern Hemisphere.
Clinical findings
A 40 year old Chinese woman, who grew up in the Peoples Republic of China, had been living in Europe for 9 years. She travelled in July and august 1997 in the Peoples Republic of China where she walked barelegged in the grass between fruit trees outside Ri Zao city, 200 km south of Qingdao city, Shan Dong province. She noticed many so-called ‘mosquito bites’. Three months later she noticed a swelling at the front of her left lower leg which later developed a pale slightly depressed centre. There were no systemic symptoms. Four months later, when again visiting China, a surgeon excised the lesion; according to the patient there was no bleeding and the excised tissue was pale and firm. The lesion did not heal and showed ulceration. A Chinese doctor, specialised in infectious diseases, who was visiting her in The Netherlands, suggested that it might be tuberculosis of the skin, and a smear of the ulcer bed was made by her general practitioner. Ziehl-Neelsen staining revealed acid fast bacteria. She was referred to a dermatologist (J.T.) and subsequently to the Department of Dermatology, Section Tropical Dermatology of the Academic Medical Centre, Amsterdam. On examination there was a painless ulcer with a diameter of 3 x 3.5 cm with an undermined border and a necrotic ulcer bed. At the cranial side there was a small skin colored swelling (Figure 1). There were no other skin lesions.
Diagnostic procedures
Histopathological examination of the biopsies taken from the ulcer border showed acanthotic broadening of the epidermis, extensive eosinophilic necrosis in the deeper dermis and the subcutaneous tissue, with a mild scattered mononuclear cell infiltrate. In the basis of the lesion there was a large thrombosed and recanalised vessel (Figure 2). In the Ziehl-Neelsen staining acid fast bacteria were seen scattered and in clumps.
proefschrift Zegelaars.indb 97 4-2-2008 9:22:24
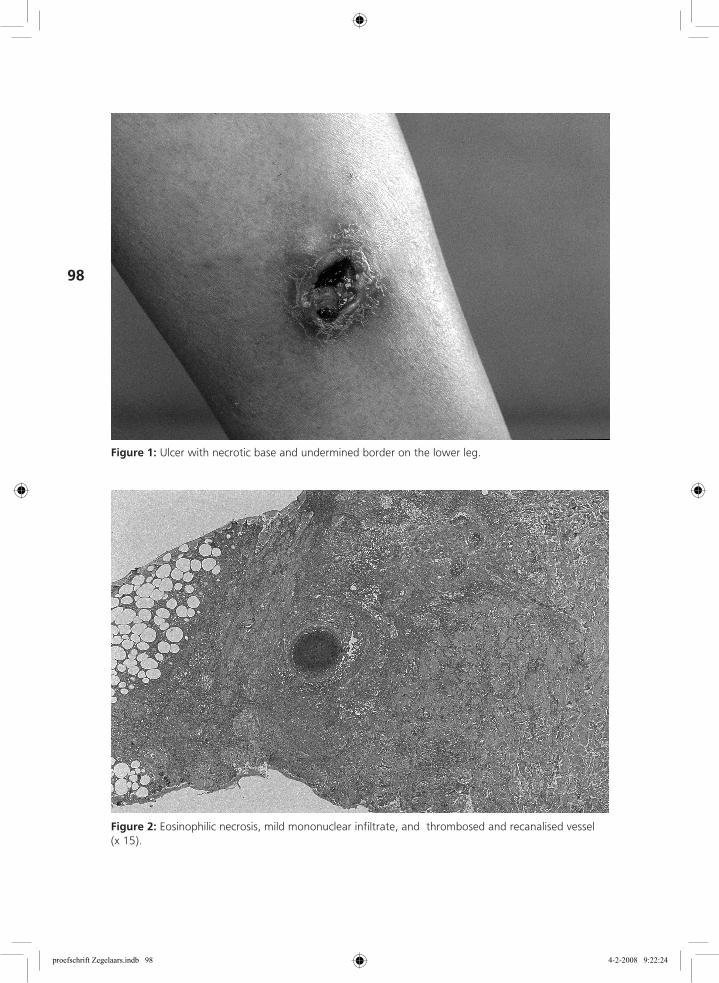
98
Figure 1: Ulcer with necrotic base and undermined border on the lower leg.
Figure 2: Eosinophilic necrosis, mild mononuclear infiltrate, and thrombosed and recanalised vessel (x 15).
proefschrift Zegelaars.indb 98 4-2-2008 9:22:24
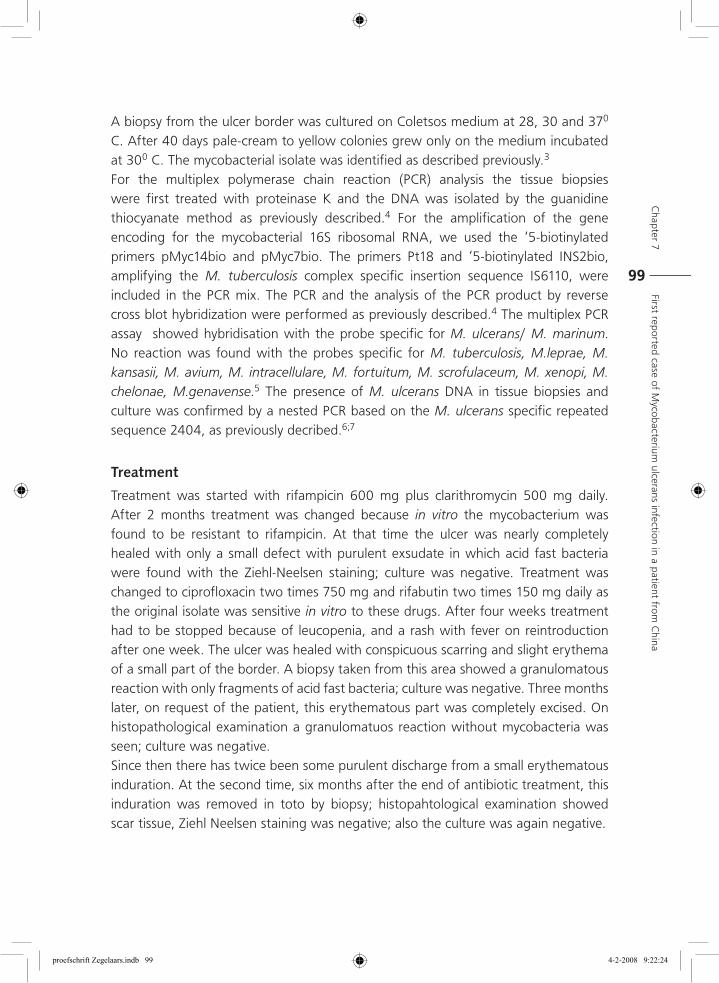
Chapter 7
First reported case of M
ycobacterium
ulcerans infection in a patient from C
hina
99
A biopsy from the ulcer border was cultured on Coletsos medium at 28, 30 and 370 C. After 40 days pale-cream to yellow colonies grew only on the medium incubated at 300 C. The mycobacterial isolate was identified as described previously.3
For the multiplex polymerase chain reaction (PCR) analysis the tissue biopsies were first treated with proteinase K and the DNA was isolated by the guanidine thiocyanate method as previously described.4 For the amplification of the gene encoding for the mycobacterial 16S ribosomal RNA, we used the ‘5-biotinylated primers pMyc14bio and pMyc7bio. The primers Pt18 and ‘5-biotinylated INS2bio, amplifying the M. tuberculosis complex specific insertion sequence IS6110, were included in the PCR mix. The PCR and the analysis of the PCR product by reverse cross blot hybridization were performed as previously described.4 The multiplex PCR assay showed hybridisation with the probe specific for M. ulcerans/ M. marinum. No reaction was found with the probes specific for M. tuberculosis, M.leprae, M. kansasii, M. avium, M. intracellulare, M. fortuitum, M. scrofulaceum, M. xenopi, M. chelonae, M.genavense.5 The presence of M. ulcerans DNA in tissue biopsies and culture was confirmed by a nested PCR based on the M. ulcerans specific repeated sequence 2404, as previously decribed.6;7
Treatment
Treatment was started with rifampicin 600 mg plus clarithromycin 500 mg daily. After 2 months treatment was changed because in vitro the mycobacterium was found to be resistant to rifampicin. At that time the ulcer was nearly completely healed with only a small defect with purulent exsudate in which acid fast bacteria were found with the Ziehl-Neelsen staining; culture was negative. Treatment was changed to ciprofloxacin two times 750 mg and rifabutin two times 150 mg daily as the original isolate was sensitive in vitro to these drugs. After four weeks treatment had to be stopped because of leucopenia, and a rash with fever on reintroduction after one week. The ulcer was healed with conspicuous scarring and slight erythema of a small part of the border. A biopsy taken from this area showed a granulomatous reaction with only fragments of acid fast bacteria; culture was negative. Three months later, on request of the patient, this erythematous part was completely excised. On histopathological examination a granulomatuos reaction without mycobacteria was seen; culture was negative.Since then there has twice been some purulent discharge from a small erythematous induration. At the second time, six months after the end of antibiotic treatment, this induration was removed in toto by biopsy; histopahtological examination showed scar tissue, Ziehl Neelsen staining was negative; also the culture was again negative.
proefschrift Zegelaars.indb 99 4-2-2008 9:22:24
100
DiscussionThe clinical picture and histopathological findings in this patient are characteristic for Buruli ulcer. In contrast to other mycobacterial infections no granulomatous inflammatory reaction is seen except in the healing stage.8 Furthermore, the typical growth of the bacteria at a restricted temperature of 30 0C is compatible with M. ulcerans, and the diagnosis was confirmed by PCR investigations. PCR analyses of the biopsies and the culture performed at different periods in time produced identical results. Using classical identification schemes the isolate was identified as M. ulcerans, subspecies shinshuense.9
The discovery of M. ulcerans, subspecies shinshuense in a patient infected in the Shan Dong province in China, confirms that the disease is not only found in tropical regions and temperate climatic areas of Australia, but occurs also above latitude 30 north. Until now, only one case has been reported above this latitude. In october 1979 an ulcer was seen on the left arm of a 19-year-old girl who lived in Japan.10 Acid-fast bacilli were isolated on two occasions from the lesion. Taxonomic study of these isolates demonstrated that they clustered together with M. ulcerans but belonged to a distinct subgroup. The authors named their isolates M. ulcerans, subspecies shinshuense.10
We consider “M. shinshuense” as representing a subgroup within the species M. ulcerans as do the African, Australian and American strains.9 We propose that M. shinshuense should be considered an Asiatic variant of M. ulcerans.Buruli ulcer occurs mainly in patients aged < 15 years of age; this might be explained by an absence of antimycobacterial immunity at this age, combined with frequent contact with the microbial source.11;12 Also elderly people (aged > 60 years) are more commonly affected, which could be owing to a diminishing immune response or perhaps reactivation of a latent infection.13 As mentioned before, medical treatment of Buruli ulcer is usually disappointing, leaving wide surgical excision followed by skin grafting as the only alternative.14
Only pre-ulcerative nodular lesions and early small ulcerated lesions can be effectively treated by rifampicin alone.15 The Japanese patient described in 1982 presented with an ulcer with a maximum diameter of about 5 cm. The lesion healed after only two weeks of oral rifampicin. Failure of antibiotic regimens for advanced M. ulcerans infection has been attributed to poor penetration of drugs into necrotic tissue.2 The rapid success of rifampicin therapy in the Japanese patient may be due to the absence of significant necrosis, therefore permitting the penetration of the drug into the lesion. Our patient was initially treated with a combination of rifampicin and clarithromycin as both drugs have been shown to have strong activity against M.
proefschrift Zegelaars.indb 100 4-2-2008 9:22:25
Chapter 7
First reported case of M
ycobacterium
ulcerans infection in a patient from C
hina
101
ulcerans in vitro.15 The favourable response in our patient, suggests that this subtype may be more sensitive to antimycobacterial drugs in vivo.Because of the potentially disfiguring character of the disease an early diagnosis is important. First, people in the endemic areas must become familiar with the clinical signs, to minimize patients’ delay. Secondly, medical doctors should be aware of the fact that Buruli ulcer is a mycobacterial disease which doesn’t occur in tropical regions only. Moreover, as this case shows, Buruli ulcer can also be seen as an imported skin disease in Western countries. Since adventurous journeys have become more popular, imported “tropical”skin diseases are seen more frequently and doctors in Western countries should be more aware of imported skin diseases. The multiplex PCR offers a reliable and rapid method of diagnosis enabling treatment to be started at an early stage when minimal damage has occured.5
In conclusion, we believe this to be the first reported case of M. ulcerans subspecies shinshuense infection in the Peoples Republic of China as no other report of Buruli ulcer has been received by WHO (WHO, personal communication).Our findings show that M.ulcerans infection also occurs above 300 latitude on the Northern hemisphere and must be considered in the differential diagnosis of skin ulcers in those returning from travel in China.
Reference List 1. Horsburgh C.R, Meyers W. M. Buruli Ulcer. In: Pathology of Emerging Infections. Horsburgh C.
R, Nelson A. M (eds) Washington DC. American Society for Microbiology chapter 7, 119-134. 1997.
2. Tsukamura M, Mikoshiba H. A new Mycobacterium which caused skin infection. Microbiol.Immunol. 1982; 26: 951-5.
3. Levy-Frebault VV, Portaels F. Proposed minimal standards for the genus Mycobacterium and for description of new slowly growing Mycobacterium species. Int.J.Syst.Bacteriol. 1992; 42: 315-23.
4. Kox LF, van LJ, Knijper S et al. PCR assay based on DNA coding for 16S rRNA for detection and identification of mycobacteria in clinical samples. J.Clin.Microbiol. 1995; 33: 3225-33.
5. Kox LF, Jansen HM, Kuijper S et al. Multiplex PCR assay for immediate identification of the infecting species in patients with mycobacterial disease. J.Clin.Microbiol. 1997; 35: 1492-8.
6. Ross BC, Marino L, Oppedisano F et al. Development of a PCR assay for rapid diagnosis of Mycobacterium ulcerans infection. J Clin.Microbiol. 1997; 35: 1696-700.
7. Guimaraes-Peres A, Portaels F, de RP et al. Comparison of two PCRs for detection of Mycobacterium ulcerans. J.Clin.Microbiol. 1999; 37: 206-8.
8. Hayman J. Out of Africa: observations on the histopathology of Mycobacterium ulcerans infection. J Clin.Pathol. 1993; 46: 5-9.
proefschrift Zegelaars.indb 101 4-2-2008 9:22:25
102
9. Portaels F, Fonteyene PA, de Beenhouwer H et al. Variability in 3’ end of 16S rRNA sequence of Mycobacterium ulcerans is related to geographic origin of isolates. J Clin.Microbiol. 1996; 34: 962-5.
10. Tsukamura M, Kaneda K, Imaeda T et al. [A taxonomic study on a mycobacterium which caused a skin ulcer in a Japanese girl and resembled Mycobacterium ulcerans]. Kekkaku 1989; 64: 691-7.
11. Josse R, Guedenon A, Darie H et al. [Mycobacterium ulcerans cutaneous infections: Buruli ulcers]. Med.Trop.(Mars.) 1995; 55: 363-73.
12. Smith M. Studies on Mycobacterium ulcerans infections in the Douglasshire of far North Queensland, Australia. Master of Sciences thesis, James Cook University, Queensland. 1996.
13. Aguiar J, Domingo M. C Guédénon A Meyers W. M Steunou C Portaels F. L’ulcère de Buruli, une maladie mycobactérienne importante et en recrudescence au Bénin. ARSOM Bull Séances. 3, 325-356. 1997.
14. Aguiar J, Stenou C. [Buruli ulcers in rural areas of Benin: management of 635 cases]. Med.Trop.(Mars.) 1997; 57: 83-90.
15. Portaels F, Traore H, De RK et al. In vitro susceptibility of Mycobacterium ulcerans to clarithromycin. Antimicrob.Agents Chemother. 1998; 42: 2070-3.
proefschrift Zegelaars.indb 102 4-2-2008 9:22:25
Chapter
8Summary & conclusion
proefschrift Zegelaars.indb 103 4-2-2008 9:22:25
proefschrift Zegelaars.indb 104 4-2-2008 9:22:25
Chapter 8
Summ
ary & conclusion
105
SummaryA well known problem doctors are aware of are non- or very slowly healing ulcers in patients in tropical areas or travellers in or from such areas. No scientific studies have been published on this subject, but it is an observation by clinicians working in the tropics or at outpatient clinics for tropical diseases in the western world. Various aspects related to healing of skin ulcers in patients in tropical areas or in travellers in and from such areas are described in this thesis.An introduction of the thesis is presented in Chapter one. Epidemiology, clinical aspects, diagnostic procedures and treatment of the most common ulcers which are encountered as an imported disease in outpatient clinic in the western world are presented.It is likely that the incidence of imported ulcers will rise because travel to and from tropical countries is becoming more frequent. Ulcers originating from the tropics show great variations. Besides clinical examination, histopathological, microbiological or molecular biological investigations may be necessary to reach a final diagnosis. A guideline for clinicians dealing with “tropical ulcers” is also described in this Chapter. In Chapter two, a study in which changes in the microcirculation in travellers to the tropics were investigated is described. We hypothesized that in travellers to tropical areas, a change from temperate to hot humid climate may result in a subsequent change in the microcirculation of the dermal plexus. An adaptation to higher temperatures could lead to distension of dermal capillaries, which may cause oedema. It is well known that oedema may delay wound healing. In this study we determined the capillary filtration rate (CFR) as a measure for micro-oedema mainly in Caucasians who had just arrived in Suriname and South-America from The Netherlands, and compared this with Caucasian volunteers who had stayed in the tropics for at least 2 months, and to healthy native volunteers. The purpose of this study was to investigate whether CFR was increased in travellers who had recently arrived in the tropics from a temperate climate and thereby support the hypothesis that (micro)-oedema impairs wound healing. Mean CFR was significantly higher in travellers who had just arrived in Suriname compared with those who had stayed there for a longer period. Our results indicated that the tendency to develop (sub)clinical oedema may play a role in delayed wound healing. Therefore, compression therapy is recommended for non-healing wounds in travellers from the tropics to temperate climates.A study which was conducted to evaluate colonisation of wounds with micro-organisms and the anti-microbial resistance in Suriname, Indonesia and Zimbabwe is described in Chapter three . This study was undertaken to obtain further insight into the bacterial colonisation and the resistance of the bacteria present in wounds
proefschrift Zegelaars.indb 105 4-2-2008 9:22:25
106
in the tropics. Knowledge of the bacterial colonisation of wounds in a given area and their anti-microbial sensitivity is useful not only for epidemiological reasons, but also for determining the most effective anti-microbial treatment. Ninety- nine swabs were taken from the surface of chronic wounds. They were stored and transported to The Netherlands for further processing. The results showed that there were no significant differences in bacterial colonisation of the chronic wounds in the different locations. Moreover, it seemed that there was also no difference in the bacterial colonisation of chronic wounds in comparison to those encountered in the western world.The most striking finding overall was the difference in the prevalence of anti-microbial resistance between the three tropical countries. Resistance of staphylococci and streptococci to tetracycline was high in all three countries. Low resistance against other anti-microbial agents was found in the isolates from Suriname, whereas in the Indonesian samples the prevalence of methicillin resistant S. aureus (MRSA) was substantial, as well as the anti-microbial resistance of the gram-negative bacteria both to older agents like gentamicin and tobramycin and to newer anti-microbial agents like ciprofloxacin and the third generation cephalosporins. The observed differences may be explained on the basis of either prescription behaviour of medical doctors or the free over the counter availability of medication in the three countries..A study in which the prevalence and the aetiology of chronic skin ulcers was assessed in patients at the Queen Elizabeth Central Hospital (QECH) in Blantyre, Malawi is presented in Chapter four. Although chronic ulcers are an important cause of morbidity in tropical countries, in contrast to developed countries, little is known on the prevalence and the aetiology of skin ulcers. Data on the history and physical examination were collected; on indication skin biopsies were taken for histological examination and bacterial cultures were set-up when infection was clinically suspected. In the 10 week study period, 45 of the 5988 patients who were admitted at the departments had chronic skin ulcers. The most important causes of ulcers was bacterial infection, followed by malignancy and trauma. In contrast to the western world, venous and arterial ulcers were encountered in only few cases. A surprisingly high number of malignancies was found. Squamous cell carcinoma in long-standing chronic ulcers in Africans is well known. If wound healing is delayed, this results in chronic inflammation, which can give rise to the phenomenon of “scar cancers”. Most patients did not report a long duration of their ulcers. One may speculate that these malignant ulcers existed for a much longer period than reported by the patient. However, it is known that HIV infection is endemic in the studied group of patients. HIV infection may contribute to impaired wound healing. We speculate that this may explain the high number of malignancies encountered in this study.
proefschrift Zegelaars.indb 106 4-2-2008 9:22:25
Chapter 8
Summ
ary & conclusion
107
A clinical study in which the tolerability and the efficacy of a hydrocolloid dressing for treating venous leg ulcers under humid and hot conditions in Surinam was investigated is described in Chapter five. Hydrocolloid dressings are widely used for treating wounds. However, little is known on their tolerability and efficacy under tropical conditions. Besides the financial factors, alleged increase in the frequency of wound infection may be an important reason that these semi-occlusive dressings are not used regularly under hot and humid conditions. Seventeen patients with venous leg ulcers were enrolled into the study for a period of 6 weeks. Hydrocolloid dressing were changed twice a week, short stretch compressive bandages were applied. The results showed that all ulcers showed a good healing tendency. A clear improvement in the percentage of granulation tissue and the circumference together with reduced exudates was observed. The dressing was generally well accepted. There were no differences in the rate of bacterial infection or colonisation of ulcers compared with those in studies in the temperate regions were noted.The import of cutaneous leishmaniasis (CL) in the Netherlands from 1990 to 2000 is dealt with in Chapter six. Leishmaniases are visceral, cutaneous and mucocutaneous diseases caused by parasites belonging to the genus Leishmania. Although cutaneous CL is the mildest clinical form, it may cause considerable morbidity, and after healing often leaves disfiguring scars. All varieties are transmitted to humans by sand-flies. The disease occurs throughout the tropical and sub-tropical regions of the world with an estimated 1.5 to 2 million cases per year of which the majority is CL. The clinical picture is diverse and may vary from one or more papules to ulcers with or without a scab. Lymphangitis may be present. Mucocutaneous leishmaniasis, although uncommon, may develop as a complication of new-world CL.Leishmaniasis is considered to be an imported skin disease with a rising incidence in the last 10 years in the Netherlands.. A Dutch study reported 49 patients with CL, in the period 1979-1989; Mediterranean countries were the most important source of infection. We were interested to investigate whether a change in this pattern had occurred in the subsequent years. The sensitivity of our diagnostic procedures, the mode of treatments and the results of treatments were examined. The incidence, the clinical picture, the treatment modalities and the response of patients diagnosed with CL from January 1990 to January 2000 at our hospital were retrospectively investigated. From 1990 to 2000, CL was diagnosed in 78 patients. The disease had most frequently been acquired in Belize, Suriname, French Guyana and Bolivia. The most sensitive diagnostic tool was PCR., Antimony (Sb) is still the drug of choice in the Americas. If infection with L. mexicana is suspected itraconazol is our drug of choice. Pentamidine seems to be the drug of choice for CL acquired in the Guyanas.
proefschrift Zegelaars.indb 107 4-2-2008 9:22:25

108
It is recommended to culture and characterise the parasite if facilities are available so that treatment can be directed at the particular species involved.A patient who developed a Buruli ulcer after travelling in the Shan Dong Province in the People’s Republic of China is described in Chapter seven. It is the first reported case of Buruli ulcer in the People’s Republic of China and proves that M. ulcerans infection is also present in the temperate climate zone in the Northern Hemisphere.
Concluding remarks Changes in the microcirculation in travellers to the tropics may lead to oedema, especially in the lower legs. Oedema is treated by compression therapy. A lot of experience on compression therapy is available in the western world. However, no studies on compression therapy under tropical conditions have yet been published. Compressive bandages or Compression stockings are often poorly tolerated in the hot and humid conditions in the tropics. Studies in this field under tropical conditions are warranted and would be useful.Traumatic skin ulcers which are secondarily infected are mainly encountered in travellers from tropical areas. These ulcers are often colonised by S. aureus or streptococci and more difficult to manage than ulcers encountered in the western world. It seems that these bacteria are not more prevalent in the tropics, at least not in chronic wounds according to the results of our studies. It would be interesting to investigate whether these bacteria are more virulent in the tropics. Therefore, it would be interesting to undertake studies on the virulence of these bacteria. There are only few reported studies on the use and effectiveness of wound dressings in the tropics. Despite the frequent use of antibiotic-containing ointments in many tropical countries with increased antibiotic resistant bacteria, more research into cheap, easy to apply wound dressings for the tropics is warranted.Cutaneous leishmaniasis should always be ruled out in travellers with wounds from endemic areas. Specifying the parasite is important for choosing the optimum treatment. However, the reported indications for treatment and the currently recommended treatment regimes vary considerably. Some treatments are well established. However, there are only a few double-blind clinical trials in which different treatment modalities were investigated. Generally, sufficient numbers of patients for conducting clinical trials are only available in the endemic areas.Therefore, it is imperative that we support investigators in the endemic areas in pursuing clincal trials.
proefschrift Zegelaars.indb 108 4-2-2008 9:22:25
Chapter
9Samenvatting
proefschrift Zegelaars.indb 109 4-2-2008 9:22:25
proefschrift Zegelaars.indb 110 4-2-2008 9:22:25
Chapter 9
Samenvatting
111
SamenvattingEen observatie van menig in de tropen - of op een polikliniek voor tropische ziekten werkzame arts is dat wonden bij reizigers in of uit de tropen moeizaam genezen. Er zijn hierover nauwelijks wetenschappelijke studies gepubliceerd. Het is een waarneming gegrond op klinische bevindingen van vele “tropendokters”. Om hier meer “evidence based” inzicht in te krijgen, hebben wij studies verricht naar verschillende aspecten die met wonden in en komend uit de tropen te maken hebben. Dit met als doel adviezen voor de klinische praktijk te kunnen aandragen. Hoofdstuk 1 is een inleidend hoofdstuk waarin een overzicht wordt gegeven van de meest voorkomende tropische wonden. Het geeft een handvat voor de clinicus om te kunnen differentiëren tussen de meest verschillende wonden waarmee patiënten zich kunnen presenteren.Hoofdstuk 2 beschrijft een onderzoek naar veranderingen in de microcirculatie bij reizigers naar de tropen. Aanpassing aan een warm vochtig klimaat zou kunnen leiden tot uitzetting van haarvaatjes in de huid, wat weer tot de vorming van oedeem zou kunnen leiden. Het is bekend dat oedeem de wondgenezing vertraagd kan doen verlopen. Het ontstaan van oedeem zou kunnen verklaren dat wonden bij reizigers in of uit de tropen moeizaam genezen. Om veranderingen in de microcirculatie te meten werd de capillary filtration rate (CFR) aan het onderbeen met behulp van kwikrekstrookplethysmografie gemeten. Met behulp van de kwikrekstrookplethysmograaf werd bij Nederlandse studenten die recent in Suriname waren aangekomen de CFR bepaald. Deze groep werd vergeleken met studenten die al minimaal twee maanden in Suriname verbleven en met een groep inwoners van Suriname. Uit deze studie bleek dat mensen die pas in Suriname zijn aangekomen een verhoogde CFR hebben vergeleken met de controle groepen. Een verhoogde CFR zou dus tijdelijk, na aankomst in de tropen, kunnen leiden tot het ontstaan van (sub)klinisch oedeem, wat weer de vertraging van wondgenezing zou kunnen verklaren. Bij langer verblijf in de tropen gaat dit fenomeen niet meer op.Hoofdstuk 3 beschrijft het onderzoek naar de bacteriële kolonisatie en antimicrobiële resistentie van bacteriën in chronische wonden van patiënten in ziekenhuizen in Indonesië, Zimbabwe en Suriname. Dit onderzoek is gedaan om een beeld te krijgen van het wel of niet vaker voorkomen van pathogene bacteriën in deze wonden in de tropen. Kennis hiervan is van belang in de keuze van antimicrobiële behandeling. Het meer voorkomen van pathogene bacteriën zoals Staphylococcus aureus of beta-hemolytische streptococcen zouden eveneens een verklaring kunnen geven voor het feit dat pyodermieën vaak in de tropen of als import huidziekten gezien worden.Uit 99 wonden werd materiaal afgenomen. Dit werd ingevroren en op een later tijdstip in Nederland gekweekt. Er werden geen significante verschillen in kolonisatie
proefschrift Zegelaars.indb 111 4-2-2008 9:22:25
112
van de chronische wonden in de verschillende geografische locaties aangetoond. Ook werden geen grote verschillen gevonden tussen de locaties in de tropen en landen in de westerse wereld. Het meest opvallend waren de verschillen in de aanwezigheid van antimicrobiële resistenties. Op alle tropische locaties werden verhoogde aantallen staphylococcen en streptococcen resistent tegen tetracycline gevonden. In kweken uit Suriname en Zimbabwe werd weinig resistentie tegen andere antibiotica gevonden. In Indonesië werd veel methicilline resistente Staphylococcus aureus (MRSA) gevonden, en tevens veel resistente gram negatieve bacteriën tegen zowel oude antibiotica (gentamycine, tobramycine) als tegen nieuwere middelen zoals ciproflaxcine en derde generatie cephalosporinen. De geobserveerde verschillen kunnen mogelijk verklaard worden uit voorschrijfgedrag van artsen en het zonder recept kunnen verkrijgen van antibiotica. Hoofdstuk 4 beschrijft de aanwezigheid van chronische wonden in een groot regionaal ziekenhuis in Malawi. Er is heel veel bekend over het voorkomen van en de etiologie van chronische wonden in de westerse wereld. Echter, van chronische wonden in de tropen is weinig bekend ondanks het feit dat dit een belangrijke oorzaak van morbiditeit is. De diagnose van de wonden werd gesteld op grond van het klinische beeld; aanvullend werd microbiologisch en histopathologisch onderzoek verricht. In tien weken tijd werden op de verschillende afdelingen 5.988 patiënten gezien; 45 patiënten daarvan hadden chronische wonden. De meest voorkomende oorzaak was een bacteriële infectie, gevolgd door maligniteiten en trauma. In tegenstelling tot de westerse wereld werden nauwelijks veneuze of arteriële wonden gezien. Verrassend veel maligniteiten werden aangetroffen. Het is bekend dat in langer bestaande wonden voornamelijk het plaveiselcel carcinoom kan ontstaan. Opvallend in deze studie was echter dat de patiënten aangaven dat veel van deze wonden slechts enkele maanden bestonden. Het kan zijn dat deze wonden toch langer bestonden dan door de patiënten gerapporteerd werd, ook is het goed mogelijk dat de HIV infectie die bij een groot deel van deze patiënten voorkomt van invloed is op het ontstaan van maligniteiten. Aangeraden wordt om in deze patiëntengroep, in gebieden waar HIV endemisch voorkomt, al in een vroeg stadium aanvullend histopathologisch onderzoek te verrichten om een eventuele maligniteit uit te sluiten. Andersom zal bij het ontstaan van een maligniteit in een chronische wond aan HIV gedacht moeten worden. Hoofdstuk 5 geeft het klinisch onderzoek naar de toepassing van hydrocolloid verbanden weer bij de behandeling van het veneuze ulcus cruris onder de tropische omstandigheden, met de hoge vochtigheidsgraad van Suriname. Dit type verband wordt in de westerse wereld veel gebruikt, echter over de toepassing in de tropen is weinig bekend. Behalve economische factoren speelt daarbij mogelijk de angst voor bacteriële wondinfecties tijdens het gebruik van deze semi-occlusieve verbanden
proefschrift Zegelaars.indb 112 4-2-2008 9:22:25
Chapter 9
Samenvatting
113
een rol. Zeventien patiënten met een veneus ulcus cruris werden zes weken lang met een hydrocolloid verband in combinatie met ambulante compressietherapie met kortrekszwachtels behandeld. Alle wonden reageerden goed op deze behandeling. Er was een duidelijke toename van granulatie weefsel, een afname van het wondexsudaat en een afname van het wondoppervlak. Er werden geen bijwerkingen gevonden, met name geen wondinfecties. Bacteriële kweken leverden min of meer dezelfde kolonisaties van veneuze ulcera op als die in een meer gematigd klimaat gezien kunnen worden. In hoofdstuk 6 komt het onderzoek naar de import van Cutane Leishmaniasis (CL) in Nederland aan de orde. CL, een ulcererende parasitaire infectie van de huid, wordt in toenemende mate als importziekte in veel westerse landen gezien. Wereldwijd zijn er naar schatting 1.5 tot 2 miljoen nieuwe gevallen van CL per jaar. De aandoening wordt veroorzaakt door een parasiet welke wordt overgebracht door een klein vliegje, de zogenaamde sandfly. Leishmaniasis is endemisch in vele (sub)tropische gebieden, waarvan Afghanistan, Saoedi-Arabië, Iran, Peru en Brazilië de hoogste incidentie hebben. Het klinisch beeld is zeer divers. CL kan zich presenteren als een papel tot een ulcerende laesie. Mucocutane Leishmaniasis kan als complicatie gezien worden met name bij patiënten met CL uit Zuid-Amerika. In een eerdere studie bleken de landen rondom het Middellandse-Zeegebied het belangrijkste gebied te zijn van waaruit CL in Nederland werd geïmporteerd. Retrospectief is geanalyseerd waar patiënten CL opliepen, welke diagnostische middelen werden gebruikt en welke geneesmiddelen werden ingezet. De medische dossiers van alle patiënten die voor CL in het Academisch Medisch Centrum in de periode 1990 tot 2000 waren behandeld, werden hiertoe geanalyseerd. CL werd bij 78 patiënten gediagnosticeerd. De incidentie van CL was ten opzichte van de periode 1979-1989 gestegen. Zuid- en Midden-Amerikaanse landen, met name Belize, Suriname, Frans-Guyana en Bolivia, waren nu de meest belangrijke bron van infectie in deze periode geweest. PCR was de meest sensitieve test om CL aan te tonen. Voor Zuid-Amerika is natriumstibugluconaat nog steeds het medicijn van eerste keus bij de behandeling van CL uit Zuid-Amerika, behalve voor de Guyanas. Hoofdstuk 7 beschrijft een patiënt met een Buruli ulcus welke is opgelopen in de Shan Dong provincie in China. Dit is de eerste patiënt waarvan beschreven is dat een Buruli ulcus werd opgelopen in China. Het Buruli ulcus wordt veroorzaakt door Mycobacterium ulcerans en komt vooral voor in de tropen, maar is ook beschreven in de meer gematigde klimaten van Australië. Gezien de toename van deze mycobacteriële infectie is het goed mogelijk dat het Buruli ulcus in de komende jaren vaker gezien zal worden als geïmporteerde huidziekte.
proefschrift Zegelaars.indb 113 4-2-2008 9:22:25
114
ConclusiesTijdens een kort verblijf in de tropen treden veranderingen in de microcirculatie op. Hierdoor kan oedeem ontstaan wat van invloed op de wondgenezing kan zijn. Oedeem kan door middel van compressietherapie behandeld worden. Er is veel ervaring met compressietherapie in de westerse wereld. Van gebruik onder tropische omstandigheden is echter weinig over bekend. Zwachtels en therapeutisch elastische kousen worden meestal slecht verdragen onder de warme vochtige tropische omstandigheden. Het is daarom van belang dat er onderzoek naar de toepassing van compressie therapie onder tropische omstandigheden gedaan gaat worden.Bij reizigers uit de tropen worden vooral traumatisch ontstane ulcera welke secundair geïnfecteerd zijn gezien. Deze ulcera zijn vaak gekoloniseerd door S. aureus of hemolytische streptococcen groep A en moeilijker te behandelen dan ulcera welke in een meer gematigd klimaat zijn ontstaan. Er zijn geen aanwijzingen dat S. aureus en hemolytische streptococcen groep A meer voorkomen in de tropen, in ieder geval blijkt uit onze studies dat deze bacteriën niet vaker in chronische wonden voorkomen. Het zou interessant zijn om in de toekomst onderzoek naar virulentie factoren van deze bacteriën uit wonden die in de tropen zijn ontstaan te verrichten.Er is slechts weinig bekend over het gebruik en effectiviteit van wondbedekkers in de tropen. De ervaring is dat vaak gebruik gemaakt wordt van antibiotica bevattende dressings, deze kunnen resistentie van bacteriën in de hand werken. Daarom is het van belang dat er in de tropen onderzoek gedaan wordt naar gemakkelijk te gebruiken goedkope wondbedekkers.Cutane leishmaniasis moet altijd uitgesloten worden bij reizigers die zich met een wond uit voor leishmaniasis endemische gebieden presenteren. Om de juiste behandeling te kunnen geven is het van belang om de parasiet te specificeren. Aanbevolen behandelingen variëren echter nogal, de aanbevelingen van de WHO zijn gedateerd en er zijn slechts weinig goede studies beschikbaar. In de westerse wereld waar de middelen voor klinisch onderzoek beschikbaar zijn ontbreken grote groepen patiënten, welke nodig zijn voor onderzoek. Derhalve is het van belang dat het rijke westen klinisch onderzoek in de endemische gebieden ondersteund.Het is mogelijk dat maligniteiten in een vroeg stadium bij mensen met HIV ontstaan; daarom wordt geadviseerd in een vroeg stadium aanvullend histopathologisch onderzoek te verrichten.
proefschrift Zegelaars.indb 114 4-2-2008 9:22:26
Chapter
Dankwoord
proefschrift Zegelaars.indb 115 4-2-2008 9:22:26
proefschrift Zegelaars.indb 116 4-2-2008 9:22:26
Dankw
oord
117
DankwoordProfessor Faber, beste William mijn promotor, mijn dank gaat in eerste instantie naar jou uit, in de loop der jaren hebben wij een speciale band opgebouwd. Dat er tenslotte toch nog een promotie uit is gerold is een bekroning op onze vriendschap. Professor Bos, beste Jan, mijn opleider, ik dank je voor de immer stimulerende woorden. Jij hebt tijdens mijn opleiding er in toe gestemd dat ik enkele maanden in Suriname werd opgeleid waardoor het uiteindelijk mogelijk werd een begin aan dit proefschrift te maken.Professor Lai A Fat, beste Rudy. Op jouw afdeling in het Academisch Ziekenhuis Paramaribo is de basis voor dit proefschrift gelegd. Ik dank je hartelijk voor je gastvrijheid, maar ook bovenal voor de gezellige etentjes samen.Ook de overige leden van de promotiecommissie: prof. dr. Kager, dr. Mekkes, prof. dr. Neumann en dr. de Hoop ben ik zeer erkentelijk voor het vrijmaken van hun tijd om dit proefschrift te kunnen beoordelen.Ricardo Hu, jij hebt mij de weg op de afdeling Dermatologie in het Academisch Ziekenhuis Paramaribo gewezen. Ik dank je voor de periode dat jij mij de ruimte gaf om een stukje opleiding in Suriname te krijgen. Ook Ramon Soetosenojo die zijn warme plaats in het Academisch Ziekenhuis Paramaribo verruilde voor een koude plaats in het AMC dank ik. Zonder deze ruil had ik tijdens mijn opleiding nooit enige tijd in Suriname kunnen doorbrengen. Henry de Vries, vriend en collega. Ik dank je voor jouw altijd kritische kanttekeningen. Jij kwam met de suggestie van de omslag van dit proefschrift.Henk Menke, jij zal je wel in al je bescheidenheid afvragen waarom ik je dank. Maar je was toch achter de schermen met name tijdens de laatste lootjes aanwezig, moedigde vanaf de zijlijn aan. Je vertrouwen in mij heb ik zeer gewaardeerd. Leonard Witkamp, ik dank je voor het corrigeren van artikelen in dit proefschrift. Telkens weer corrigeerde je in zeer rap tempo de eerste versies en vroeg vervolgens waar het volgende artikel bleef. Als het aan jou had gelegen was ik 8 jaar geleden al gepromoveerd.Mijn collega’s Roël Chin-A-Lien, Irina Cairo en Wim Roest. Ik dank jullie voor jullie geduld en de vrijheid die jullie mij de afgelopen jaren hebben gegeven. We vormen een hechte maatschap en zullen ons de komende jaren verder profileren. Ook de zusters van de afdeling Dermatologie van het Flevoziekenhuis dank ik voor hun altijd stimulerende aanmoediging. Ja, ik ben nu eindelijk afgestudeerd, laten we een feestje vieren. Martin Wagtmans, collega MDL-arts in het Flevoziekenhuis, dank ik voor het helpen met een literatuurbestand. Deze marathon is uitgelopen, op naar de volgende. Mijn
proefschrift Zegelaars.indb 117 4-2-2008 9:22:26
118
collega’s en het management van het Flevoziekenhuis dank ik voor de plezierige werkomgeving waarin ik de afgelopen jaren heb mogen werken.Pieter van Thiel, bedankt voor de vele gezellige maandagen die wij zwoegend doorbrachten om de stroom patiënten met cutane leishmaniasis te behandelen.Ook gaat mijn dank uit naar de studenten die in de loop der jaren het nodige werk, beschreven in dit proefschrift hebben uitgevoerd.Mijn moeder dank ik voor haar nimmer aflatende steun. Helaas zal mijn vader er niet bij zijn. Mijn familie, hoewel ik niet altijd even duidelijk was over wat ik nou precies aan het doen was, zijn altijd interesse blijven tonen, ik dank jullie hiervoor.En last but not least Manoushka, Zera en Milan. Dit proefschrift is geschreven in de spaarzame uurtjes wanneer jullie eindelijk in bed lagen en Manoushka op toneel ergens in het land stond, maar ook tijdens de weekends en in de vakanties. Het is tijd om mijn bureau op te ruimen en meer plezier met jullie te hebben.
proefschrift Zegelaars.indb 118 4-2-2008 9:22:26





























