Upload
jean-paul-nguessan
View
216
Download
0
Embed Size (px)
Citation preview
8/3/2019 EARSS Organisation
1/10
EUROSURVEILLANCE VOL. 4 - N4 AVRIL-A PRIL 1999 41
Systme Europen de Surveillance de la RsistanceAntimicrobienne (EARSS) : objectifs et organisationS.L.A.M. Bronzwaer1, W. Goettsch1, B. Olsson-Liljequist 2, M.C.J. Wale3, A.C. Vatopoulos4, M.J.W. Sprenger 11 National Institute of Public Health and the Environment, Bilthoven, Pays-Bas2 Swedish Institute f or Infectious Disease Control, Stockholm, Sude3 PHLS Antimicrobial Susceptibility Surveillance Unit, Nottingham, Royaume-Uni4 Universit dAthnes, Athnes, Grce
Introduction
Pour tre efficace, une surveillance europenne doit bnficier de laccord de tousles participants et de leur participation active concluait la confrence europenne sur lancessit dune surveillance des microorganismes rsistants (the microbial threat) quisest tenue au Danemark en septembre 1998 (1). Les profils de rsistance aux anti-biotiques sont trs variables dun pays lautre au sein de lUnion Europenne (2,3). Plu-sieurs tudes suggrent que les politiques et les recommandations sur lutilisation desantibiotiques peuvent avoir des consquences sur la prvalence de la rsistance (4,5).Dun point de vue pidmiologique et mthodologique, il est trs difficile de comparer lestaux de rsistance aux antibiotiques du fait des diffrences entre les antibiotiques tests,les procdures dchantillonage, les systmes de tests de sensibilit utiliss et les limitesadoptes.
Afin davoir des donnes fiables et comparables, la Direction Gnrale V (DGV) de laCommission europenne finance actuellement un systme de surveillance europen de larsistance antimicrobienne (EARSS). Ce systme, auquel tous les pays membres plus lIslande,la Norvge et la Suisse participent (tableau 1), est coordonn par le Rijksinstituut voor deVolksgezondheid en Milieu (RIVM), lInstitut national de Sant Publique et dEnvironnementdes Pays-Bas. Plus de 400 laboratoires ont exprim leur volont de participer ce rseaueuropen des maladies transmissibles, dont les objectifs et lorganisation sont dcritsdans cet article.
Objectifs
EARSS est un rseau international des systmes de surveillance nationaux. Son objec-tif est de rassembler des donnes comparables et fiables sur la rsistance antimicro-bienne au profit de la sant publique en Europe. En tenant compte des mthodes delaboratoire et des principes pidmiologiques, EARSS explorera, au cours dune tudede 18 mois, la faisabilit danalyser les diffrences rgionales, dvaluer les facteurs de
risque, et dassurer, par voie lectronique, un retour dinformation. Les microbiologistes
European Antimicrobial Resistance SurveillanceSystem (EARSS): objectives and organisationS.L.A.M. Bronzwaer1, W. Goettsch1, B. Olsson-Liljequist 2, M.C.J. Wale3, A.C. Vatopoulos4, M.J.W. Sprenger 11 National Institute of Public Health and the Environment, Bilthoven, The Netherlands2 Swedish Institute for Infectious Disease Control, Stockholm, Sweden3 PHLS Antimicrobial Susceptibility Surveillance Unit, Nottingham, United Kingdom4 Athens University, Athens, Greece
Introduction
Effective European surveillance must have the agreement and active involvementof all participants, concluded a European Union (EU) conference on the need forsurveillance of resistant microorganisms (the microbial threat), held in September1998 in Denmark (1). Patterns of antibiotic resistance differ widely between memberstates of the EU (2,3). Studies suggest that policies and guidelines on antibioticusage may affect the prevalence of resistance (4,5). From an epidemiological andmethodological standpoint it is very difficult to compare antimicrobial resistancerates because of differences in antimicrobial agents tested, sampling policies,susceptibility test systems used, and breakpoints adopted.
To obtain more comparable and reliable data, the Directorate General V (DGV)of the European Commission is funding a European antimicrobial resistance
surveillance system (EARSS). This system, in which all member states of the EU,plus Iceland, Norway, and Switzerland are taking part (table 1), is coordinated bythe Rijksinstituut voor de Volksgezondheid en Milieu (RIVM); the National Instituteof Public Health and the Environment of the Netherlands. More than 400 laboratoriesexpressed willingness to take part in this European communicable disease net-work. This report describes its objectives and organisation.
Objectives
EARSS is an international network of national surveillance systems, which aimsto aggregate comparable and reliable antimicrobial resistance data to benefitpublic health across Europe. Taking into account laboratory methods as well asepidemiological principles, EARSS will explore the feasibility of analysing regionaldifferences, assessing risk factors, and providing electronic feedback in astudy of 18 months duration. Microbiologists and epidemiologists from participatingcountries aim to collect quantitative susceptibility data on penicillin and cephalo-
sporins for community acquired Streptococcus pneumoniaefrom blood and
S O M M A I R E / C O N T E N T S Ni la CommissionEuropenne,ni aucune personneagissant en son nomnest responsable delusage qui pourraittre fait desinformations ci-aprs.
Neither the EuropeanCommission norany person actingon behalf of theCommission isresponsible for theuse which might bemade of the followinginformation.
Eurosynthse / Systme Europen de Surveillance de la Rsistance Antimicrobienne (EARSS) : objectifs et organisationEuroroundup European Antimicrobial Resistance Surveillance System (EARSS): objectives and organisation
Rapport de surveillance / Leptospirose au Portugal : situation pidmiologique de 1991 1997Surveillance report Leptospirosis in Portugal: epidemiology from 1991 to 1997
Rapport dinvestigation Epidmie dintoxications alimentaires Salmonella enteritidisprovenant dun fromage de fabrication industrielleOutbreak report An outbreak of Salmonella enteritidisfood poisoning from an commercially produced cheese
Dans les bulletins nationaux... / In the national bulletins... Contacts / Contacts
BULLETIN EUROPEN SUR LES MALADIES TRANSMISSIBLES / EUROPEAN COMMUNICABLE DISEASE BULLETINFUNDED BY DGV OF THE COMMISSION OF THE EUROPEAN COMMUNITIESFINANC PAR LA DGV DE LA COMMISSION DES COMMUNAUTS EUROPENNES
Vol. 4 N4 AVRIL / APRIL 1999
EUROSYNTHSE EUROROUNDUP
8/3/2019 EARSS Organisation
2/10
42 EUROSURVEILLANCE VOL. 4 - N4 AVRIL-APRIL 1999
cerebrospinal fluid; and to collect data on methicillin resistance for Staphylo-coccus aureusfrom blood cultures.
Organisation
Each participating country has appointed a national representative microbiologistand a representative epidemiologist. These representatives will also work togetherto analyse the data for other epidemiological studies. One of the representatives
from each country acts as the national coordinator. His/her main task is to coordinateactivities of the participating laboratories; arrange distribution and collection ofquestionnaires on susceptibility testing; and to collect and forward resistance dataeach quarter for international collation. Standardisation and microbiological qualitycontrol methods are being developed in consultation with the European Society ofClinical Microbiology and Infectious Diseases (ESCMID). EARSS is a component ofthe network-of-networks being established by the World Health Organization (WHO)for global surveillance.
Select ion of partic ipating laboratories
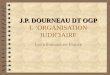
EARSS recommended that the national coordinators should select enoughlaboratories in their countries to cover at least 20%of the total population. Forcommunity acquired pathogens the catchment population of the laboratories (thenumber of people living in the area they serve) will be considered as thedenominator. The 400 or so laboratories participating in EARSS will cover well
over 20% of the population in manycountries (figure 1). Most of theselaboratories are first-line clinical labora-tories, rather than reference laborato-ries. Academic and non-academichospitals are represented, and thespectrum extends from nursing homesto tertiary referral hospitals.
Epidemiological data
EARSS collects the following infor-mation by means of isolate record formsand questionnaires: information about an isolate and itssusceptibility test results
information about patients information about the laboratorymethods used and denominator data data about the hospital(s) served bythe laboratory used to generate thedenominator.
Isolate record form. This formcollects information about patients andisolates. EARSS requires the followinginformation: sex, month and year ofbirth, date of specimen collection, nameor code of hospital, hospital department,origin of patient, isolate specimennumber, laboratory code, and antibiotic
susceptibility testing results as specified in the protocol. Furthermore, the isolaterecord form allows other optional data to be collected: patient identifier (ID),clinical diagnosis, and susceptibility to other antibiotics.
Questionnaire on susceptibility testing. This questionnaire asks about testmethods used, and collects denominator data from a laboratory and fromthe hospital(s) it serves. The facilities the hospital offers (intensive care unit,renal, transplant, cardiac surgery) and the number of bed days are requested.For nosocomial pathogens the number of bed days will be considered as thedenominator. Data on patients and isolates can be related to information aboutthe laboratory and hospital by means of a unique laboratory code that will befilled out on all isolate record forms and questionnaires. The authors areaware that the catchment population estimated by a laboratory may over-estimate the true catchment population. True catchment populations can becalculated using postal codes of the patients f rom whom isolates are obtained.
et pidmiologistes des pays participants collecteront les donnes quantitatives surla sensibilit la pnicilline et aux cphalosporines des Streptococcus pneumoniaedin-fections communautaires, isols du sang ou du liquide cphalo-rachidien, ainsi que lesdonnes sur la rsistance la mthicilline des Staphylococcus aureusisols du sang.
Organisation
Chaque pays participant a dsign deux reprsentants nationaux : un microbiologiste
et un pidmiologiste. Ils travailleront ensemble lanalyse des donnes provenant dautrestudes pidmiologiques et lun dentre eux assumera le rle de coordinateur national.Sa principale mission est de coordonner les activits des laboratoires participants, degrer la distribution et la collecte des questionnaires sur les tests de sensibilit aux anti-biotiques, et de recueillir chaque trimestre, les donnes de rsistance et de les trans-mettre lorganisation de centralisation internationale. Les mthodes de standardisationet de contrle de qualit microbiologique ont t mises au point avec le concours de lEu-ropean Society of Clinical Microbiology and Infectious Diseases (ESCMID). EARSS fait par-tie du rseau des rseaux mis en place par lOrganisation Mondiale de la Sant (OMS)pour la surveillance internationale.
Slect ion des laboratoires partic ipants
EARSS recommande aux coordinateurs nationaux de slectionner, dans leur pays, unnombre de laboratoires permettant de couvrir au moins 20%de lensemble de la popu-lation. Dans le cas des agents pathognes provenant dinfections communautaires, la
population de rfrence des laboratoires(nombre de personnes vivant dans la zonequils desservent) sera prise comme dno-minateur. Dans bon nombre de pays, lesquelques 400 laboratoires participants EARSS couvriront bien plus de 20%de lapopulation (figure 1). La plupart sont deslaboratoires de routine plutt que des labo-ratoires de rfrence. Tous les hpitauxsont reprsents, quils soient universitairesou non, depuis les cliniques jusquaux hpi-taux spcialiss.
Donnes pidmiologiques
Par le biais de formulaires denregis-
trement de lisolat et de questionnaires,EARSS recueille les informations suivantes : informations sur un isolat et rsultats desa sensibilit aux antibiotiques informations concernant les patients informations sur les mthodes utilisespar le laboratoire et donnes concernantle dnominateur donnes sur le ou les hpitaux dpen-dant du laboratoire, servant estimer lednominateur.
Formulaire denregistrement de
lisolat. Il contient les informations concer-nant les patients et les isolats. Les infor-
mations suivantes y sont demandes par EARSS : sexe, mois et anne de naissance,date du recueil de lchantillon, nom ou code de lhpital, dpartement de lhpital, ori-gine du patient, numro dchantillon de lisolat, code du laboratoire, et rsultats des testsde sensibilit aux antibiotiques conformment aux dtails du protocole. Par ailleurs, y figu-rent des informations optionnelles : identificateur du patient, diagnostic clinique, et don-nes de sensibilit dautres antibiotiques.
Questionnaire sur la sensibilit aux antibiotiques.Y figurent des questions relativesaux tests employs, et des informations concernant le dnominateur : donnes sur lelaboratoire et les hpitaux qui en dpendent, les services disponibles dans lhpital (unitde soins intensifs, chirurgie rnale et cardiaque, service de transplantation) et le nombrede journes dhospitalisation. Cette dernire donne sera prise comme dnominateurdans le cas des infections nosocomiales. Les donnes relatives aux patients et aux iso-lats peuvent tre associes linformation sur le laboratoire et les hpitaux par le biaisdun code de laboratoire unique qui figurera sur tous les formulaires denregistrement et
Autriche / Austria (AT) H. Mitt ermayer / W. Koller
Belgique / Belgium (BE) H. Goossens / F. van Loock
Danemark / Denmark (DK) T. Soerensen / D. Mon net
Finlande / Finland (FI) P. Huovinen / O. Lyytikinen
France (FR) P. Courvalin / H. Aub ry-Damon / J. Drucker
Allemagne / Germany (DE) W. Wit te / F. Tieman
Grce / Greece (GR) N. Legakis / A. Vatopo ulos
Islande / Iceland (IS) K. Kristinsson / H. Briem
Irlande / Ireland (IE) L. Fenelon / D. OFlanagan
Italie / Italy (IT) G. Cornaglia / M.L. Moro
Luxembourg (LU) R. Hemmer
Pays-Bas / Netherlands (NL) H. de Neeling / W. Goettsch
Norvge / Norway (NO) E. Hoiby / P. Aavit sland
Portugal (PT) M. Cania / M. Paixo
Espagne / Spain (ES) F. Baquero / J. Campos
Sude / Sweden (SE) O. Cars / B. Olsson-Liljequist
Suisse / Swit zerland (CH) K. Mhlemann / J. Bille
Royaume-Uni / United Kingdom (UK) D. Livermore / M . Wale
Collaborateurs / Collaborators: OMS / WHO R.Will iams / J. Stel ling
ESCMID I. Phillips / M. Struelens
Responsable du projet / project leader M.J.W. Sprenger
Coordinateur du projet / project coordinator S.L.A.M. Bronzwaer
Tableau 1 / Table 1Pays participants, coordinateurs natio naux
et collaborat eurs de EARSS / Participating countri es, nat ionalcoordinators and collaborators in EARSS.
8/3/2019 EARSS Organisation
3/10
EUROSURVEILLANCE VOL. 4 - N4 AVRIL-A PRIL 1999 43
To preserve confidentiality this must be done at a national level.
Duplicates
To prevent duplicate isolates from being reported, laboratories are asked tosend information only about the first isolate of each strain from each patient.These are referred to as patient-isolates. To be able to correct for duplicate isolates,the isolate record form asks for patient ID/ code. This is marked as optional
information, since in many countries there are legal limitations on the inclusionof patient identifiers. For the same reason we do not ask for date of birth, butmonth and year of birth. A code is needed, however, to exclude duplicates at thenational level. If a patient identifier cannot be used in a particular country, we asklaboratories to use another (encrypted) code for a specif ic patient. In countrieswithout legal limitations the national coordinator will use the patient identifier toexclude repeat isolates, removing the identifier before sending data to thecentral database.
Data processing
Participating laboratories are offered two methods of data entry: electronicand on paper. Details vary from country to country, but if a laboratory opts forelectronic data t ransfer they can use an existing laboratory information systemor make use of Whonet (and/ or Whonet-Baclink). WHO revised t he existingmicrobiology laboratory database software Whonet4 for EARSS. Laboratories that
do not process data electronically will forward the isolate record forms to theirnational coordinator, who will enter thedata and send them each quarter to theRIVM in ASCII format. On receipt, the datawill be checked for syntax errors (forexample, dates and test results), and linkedto denominator information collected bymeans of the questionnaire on susceptibilitytesting. After this validation, tables, figures,and geographical maps can be generatedand published on an internet site. Theaggregated data sets will also be usedfor more complex epidemiological studies,for example investigating relationshipsbetween geographical locations and anti-biotic resistance.
Feedback
Sufficient and timely feedback is essentialfor all surveillance systems. As well asinformation letters and a newsletter, datawill be shared using the electronic infra-structure Interchange of Data betweenAdministrations (IDA) network of t he EU.
Within IDA an internet application will be developed to enable participatinglaboratories to export their ASCII data to the central EARSS database and to obtainselected information from the central database.
Quarterly feedback will be given on: the total number of S. aureuscases in blood and the proportion that are methicillin
resistant (MRSA) prevalence of MRSA cases in blood per 100 patients incidence of MRSA cases in blood per 1000 patient days prevalence of oxacillin (penicillin) resistance of S. pneumoniaecases in blood andcerebrospinal fluid quarterly incidence of penicillin resistant S. pneumoniaecases in blood andcerebrospinal fluid per million population during the study.
Results
About 400 laboratories will take part by sending data via national coordinatorsto the central EARSS database. Data collection began in some countries on1 October 1998, and the first results are expected in April 1999. An EARSS manualthat is downloadable from the website has been prepared, and a printed booklet isbeing distributed to participating laboratories.
les questionnaires. Les auteurs sont conscients que lestimation de la population de rf-rence faite par les laboratoires peut tre surestime. Cependant, la valeur relle de cettepopulation peut tre calcule partir des codes postaux correspondant aux patients dontproviennent les isolats. Pour prserver lanonymat, ce calcul doit tre fait lchelon national.
Doublons
Afin dviter les doublons, les laboratoires ne doivent envoyer, pour chaque patient,
que les informations concernant le premier isolat de chaque souche. Celles-ci sont enre-gistres sous la forme patient-isolats. Dans le formulaire denregistrement de lisolatfigure un item sur lidentificateur (ID/code) du patient, servant reprer les doublons.Cette information est optionnelle car de nombreux pays ont des restrictions rglemen-taires quant linclusion de paramtres didentification des patients. Pour cette mme rai-son, seuls le mois et lanne de naissance, et non le jour, sont demands. Quoi quil ensoit, il est ncessaire de disposer dun code permettant dexclure les doublons lche-lon national. Pour les pays o lon ne peut se servir dun identificateur, les laboratoiresdoivent utiliser pour chaque patient un autre code (crypt). Pour ceux nayant pas de tellesrestrictions rglementaires, le coordinateur national se basera sur lidentificateur du patientpour exclure les rptitions, puis lenlvera du fichier avant denvoyer les donnes labase de donnes centrale.
Trait ement des donnes
Les laboratoires participants disposent de deux mthodes pour saisir les donnes :
par voie lectronique ou sur papier. Les dtails varient dun pays lautre, mais lorsquunlaboratoire choisit le transfert lectro-nique, il peut utiliser soit un systmedinformation de laboratoire existant,soit le logiciel de base de donnes delaboratoires de microbiologie de lOMS,Whonet (et/ ou Whonet-Baclink), dont laversion 4 a t mise au point pourEARSS. Les laboratoires ne traitant pasles donnes par voie lectronique exp-dieront les formulaires denregistrementde lisolat au coordinateur national. Celui-ci se chargera de la saisie des donneset de leur transmission au RIVM sousforme ASCII chaque trimestre. Dsrception, les donnes seront soumises un contrle des erreurs de syntaxe(par exemple, dates et rsultats destests), puis associes aux informationsrelatives au dnominateur recueillies parle biais du questionnaire sur la sensibi-lit aux antibiotiques. Aprs cette tapede validation, les tableaux, figures etcartes gographiques seront ralisspuis diffuss sur le site internet. Len-semble des donnes agrges serviront galement pour des tudes pidmiologiquesplus complexes, telles que la recherche de relations entre zones gographiques et rsis-tance aux antibiotiques.
Retour des informations
Un retour dinformations de qualit est essentiel pour tout systme de surveillance.Hormis la publication de lettres dinformation et dune newsletter, les donnes seront par-tages via linfrastructure du rseau lectronique europen Interchange of Data betweenAdministrations (IDA). Une application internet sera dveloppe au sein dIDA pour queles laboratoires part icipants puissent dune part exporter leurs donnes sous forme ASCII la base de donnes centrale dEARSS et dautre part obtenir des informations slec-tives partir de cette base.
Les informations suivantes seront accessibles chaque trimestre : nombre total des cas de S. aureusdans le sang et proportion rsistante la mthicil-line (MRSA) prvalence des cas de MRSA dans le sang pour 100 patients incidence des cas de MRSA dans le sang pour 1000 patient jours prvalence des cas de S. pneumoniaersistants loxacilline (pnicilline) dans le sangou le liquide cphalo-rachidien.
0
10
20
30
40
50
60
70
80
90
Laboratoires participants EARSS (~440) et pourcentage de la populationcouverte (estimation) / Partipat ing laboratories (~440)and percentage of population (estimate) in EARSS
Figure 1
AT BE DK FI FR DE GR IS IE IT LU NL NO PT ES SE UK
% couverture / % coverage nombre de laboratoires/ number of laboratories
8/3/2019 EARSS Organisation
4/10
44 EUROSURVEILLANCE VOL. 4 - N4 AVRIL-APRIL 1999
incidence trimestrielle des cas de S. pneumoniaersistants la pnicilline dans lesang ou le liquide cphalo-rachidien par million dhabitants durant ltude.
Rsultats
Prs de 400 laboratoires participeront et enverront leurs donnes la base de don-nes centrale dEARSS par lintermdiaire des coordinateurs nationaux. Dans certainspays, le recueil des donnes a dbut le 1er octobre 1998, et les premiers rsultats sont
attendus pour avril 1999. Un manuel sur EARSS est accessible sur le site web dEARSS,et une brochure dinformation est distribue aux laboratoires participants.
Conclusion
Lors de la mise au point du protocole et du questionnaire, la difficult a t de trou-ver un quilibre entre la validit scientifique et la faisabilit. Premier rsultat : les pid-miologistes et microbiologistes impliqus dans le projet ont trouv un accord communquant au protocole et aux principes logistiques. Dores et dj, EARSS sert de catalyseurpour les systmes de surveillance nationaux.
Pour plus dinformations : voir le site web (http:/ / www.earss.r ivm.nl), ou contacter lecoordinateur du projet Stef Bronzwaer ([email protected]), ou lun des coordinateursnationaux dont les adresses e-mail figurent sur le site. s
Conclusion
In developing the protocol and questionnaire, the challenge was to balancescientific validity and feasibility. A first result is that consensus has been reachedby leading microbiologists and epidemiologists on the protocol and logisticalframework. EARSS is already acting as a catalyst for national surveillance systems.
For more information: see the EARSS website (http:/ / www.earss.rivm.nl), contact
the project coordinator Stef Bronzwaer ([email protected]), or a national coordi-nator by means of an email addresses on the website. s
References
1. Thamdrup Rosdahl V, Borge Pederson K. Report from the invitational EU conference on the microbial threat.September 1998. (http:/ / www.microbial.threat.dk)
2. Rahal K, Wang F, Schindler J, Rowe B, Cookson B, Houvinen P, et al. Reports on surveillance of antimicrobialresistance in individual countries. Clin Infect Dis1997; 24(Suppl 1): S69-75.
3. Kresken M, Wiedemann B. Development of resistance in the past decade in central Europe. J AntimicrobChemother1986; 18 (suppl C): 23 5-42.
4. Seppala H, Klaukka T, Vuopio-Varkila J, Muotiala A, Helenius H, Lager K, et al. The effect of changes in theconsumption of macrolide antibiotics on erythromycin resistance in group A streptococci in Finland. N EnglJ Med1997; 337 : 441-6.
5. Pradier, C, Dunais H, Carsenti-Etesse, Dellamonica P. Pneumococcal resistance in Europe. Eur J Clin MicrobiolInfect Dis1997; 16 : 644-7.
RAPPORT DE SURVEILLANCE SURVEILLANCE REPORT
IntroductionLe terme leptospirose sapplique une
srie daffections causes par un membrede lordre des Spirochaetales, essentielle-ment lespce Leptospira interrogans. Lin-fection peut tre asymptomatique, maisune maladie de gravit variable et aux
tableaux cliniques varis (suggrant sou-vent une mningite, une encphalite ou unegrippe) peut se dvelopper. La dure de laleptospirose varie de quelques jours plu-sieurs semaines, selon la gravit et le trai-tement. Le taux de mortalit est faible, maispeut dpasser les 20%chez des sujets quidveloppent une insuffisance hpatique ournale (maladie de Weil) ou chez les per-sonnes ges.
Linfection se transmet essentiellementpar contact de la peau ou des muqueusesavec de leau, le sol ou dautres lmentscontamins par de lurine danimaux infec-ts. La maladie constitue un risque pro-fessionnel chez les travailleurs exposs de leau contamine - par exemple les fer-miers, les mineurs, les employs desgouts et les soldats. La t ransmission peutaussi survenir au cours de loisirs tels quela baignade ou la nage dans des rivires oudes lacs contamins (1,2).
La leptospirose a peu retenu dattentionau Portugal car cest une maladie rare.Cependant, les disparits rgionales de ladistribution de la maladie et laugmentationdu nombre de cas identifis par le systmede dclaration obligatoire en 1997, justi-
fient de faire le point de lpidmiologie dela leptospirose au Portugal, depuis 1991
jusquen 1997 (3).
MthodesDonnesLanalyse a t ralise partir des don-
nes de routine de trois systmes dinforma-tion : 1) Doenas de Declarao Obrigatria- Dclaration obligatoire des maladies, 2)Grupos de Diagnsticos Homogneos -Diagnostics des sort ies dhospitalisation,3) Mortalidade - Mortalit.
Pour ces systmes, les cas sont dfinissur la base des donnes cliniques et delaboratoire. Les donnes tels que lge, lesexe et le diagnostic sont recueillies.
Le systme de notification, sous la res-ponsabilit de la Direction gnrale de laSant (Direco Geral da Sade), rassembleles cas notifis dune srie de maladiesinfectieuses dont la leptospirose (4).
Le systme des diagnostics hospitaliersest assur par lInstituto de Gesto Inform-tica e Financeira do Ministrio da Sade(Institut de Gestion Informatique et Finan-cire du Ministre portugais de la Sant).Il dtient des informations sur toutes lesadmissions dans les hpitaux publics duPortugal ( lexception des rgions auto-nomes des Aores et de Madre) (5).
Quant au systme de mortalit, troi-sime source dinformation, il est pris en
IntroductionThe term leptospirosis describes a
group of diseases caused by membersof the order Spirochaetales, mainly thespecies Leptospira interrogans. Infectioncan be asymptomatic but disease ofdiffering severity and clinical features
(often suggestive of meningitis, ence-phalitis, or influenza) can occur. Theduration of leptospirosis varies from afew days to several weeks, accordingto severity and treatment. Case fatalityis low but can exceed 20%in patientswho develop liver and kidney failure(Weils disease) and in elderly people.
The infection is transmitted mainly bycontact of the skin or mucous membraneswith water, soil, or other elementscontaminated by t he urine of infectedanimals. The disease is an occupationalhazard of workers exposed to conta-minated water - for example, farmers,miners, sewerage workers, and soldiers.Transmission can also occur during leisureactivities like bathing and swimming incontaminated rivers or lakes (1,2).
Leptospirosis has received littleattention in Portugal because it is rare.Nevertheless, regional differences ofdisease distribution and an increasein the number of cases identified bythe compulsory notification system in1997 made it relevant to review theepidemiology of leptospirosis in Portugal,from 1991 to 1997 (3).
MethodsDataRoutine data from three information
systems were analysed: 1) Doenas deDeclarao Obrigatria - mandatorynotifications, 2) Grupos de DiagnsticosHomogneos - hospital discharge
diagnosis, 3) Mortalidade - mortality.These systems define cases on thebasis of clinical and laboratory data andcollect data on age, sex, and diagnosis.
The notification system is managedby Direco Geral da Sade(GeneralDirectorate of Health), and gathersnotifications of cases on a series ofinfectious diseases, including lepto-spirosis (4).
The hospital discharge system isled by Instituto de Gesto Informticae Financeira do Ministrio da Sade(Institute of Computational and FinancialManagement of the Portuguese Ministryof Health). It generates information aboutall admissions to public hospitals ofPortugal (excluding autonomous regions(AR) of Azores and Madeira) (5).
The mortality system, managed byInstituto Nacional de Estatstica(NationalInstitute of Statistics), was the third datasource.
Data from the notification and mor-tality systems were processed directlyfrom their respective databases and
Leptospirose au Portugal :situation pidmiologique de 1991 1997J.M. Falco, P.J. Nogueira, C. Matias Dias, Z.P. PimentaObservatrio Nacional de Sade, Instituto Nacional de Sade Dr. Ricardo Jorge, Lisbonne, Portugal
Leptospirosis in Portugal:epidemiology from 1991 to 1997J.M. Falco, P.J. Nogueira, C. Matias Dias, Z.P. PimentaObservatrio Nacional de Sade, Instituto Nacional de Sade Dr. Ricardo Jorge, Lisbon, Portugal
8/3/2019 EARSS Organisation
5/10
EUROSURVEILLANCE VOL. 4 - N4 AVRIL-APRIL 1999 45
charge par lInstituto Nacional de Estatstica(Institut national de statistiques).
Les donnes des systmes de notifi-cation et de mortalit ont t rcupresdirectement partir de leurs bases de don-nes respectives puis analyses avec lelogiciel SPSS (Statistical Package for Social
Sciences) (6).
Estimation de lincidenceLes nombres de cas ont t extraits
dune part des bases de donnes de dia-gnostics hospitaliers (1993-1997) et demortalit (1991-1996) correspondant auxcodes internationaux ICD-9 de 100,0 100,9 (7), et dautre part, des rapportsannuels de notification (1991-1997) (4).
Les estimations de la population (parrgion, genre et groupe dge) au 30 juin1994, milieu de la priode prise en comptedans lanalyse, ont t utilises commednominateurs. Tous les taux ont t expri-
ms en cas ou dcs par million dhabi-tants.
Correction de lincidence estimeLes donnes des systmes de notifi-
cation obligatoire et de diagnostics de sor-ties hospitalires sous-estiment lincidencede la maladie. Ces estimations peuventcependant tre corriges en multipliant lenombre total de dcs (considr commedpourvu derreurs significatives) par lin-verse du ratio nombre de dcs/nombrede cas. La leptospirose tant une affectionaigu, ce ratio, pour une priode donne,reprsente approximativement le taux demortalit (3).
Afin de rduire la variation associe auxpetits nombres, nous nous sommes basssur le nombre total de dcs par leptospi-rose observs entre 1991 et 1996 (lesdonnes de 1997 ntant pas disponiblesau moment de ltude).
En se rfrant lanalyse des donnesrgionales publies (3), trois diffrents ratiosont t slectionns, correspondant destaux de mortalit respectivement fort,moyen et faible. La valeur suprieure taitde 0,13 (Aores), correspondant une fortemortalit, et la valeur moyenne de 0,10,relative au territoire continental et extraite
des donnes de sorties hospitalires de1993 1996. Enfin, le troisime ratio taitde 0,05, choisi arbitrairement comme tauxde mortalit faible.
Lincidence moyenne annuelle brute dela leptospirose a t obtenue en divisantchacune de ces trois estimations rgionalespar six fois lestimation de la population rsi-dente de 1994 (7).
RsultatsIncidence bruteLincidence de la leptospirose estime
daprs les notifications est reste relati-vement stable entre 1991 et 1996, puis
a augment en 1997 (tableau 1). Pourtoute la priode considre, les tauxtaient suprieurs chez les hommes avecun ratio hommes/femmes de 2,7 (variantde 1,5 en 1992 5,2 en 1995) (tableau 1).
Les diagnostics de sorties hospitaliresconduisent une incidence de la leptospi-rose suprieure celle obtenue avec la noti-fication. Lexcs chez les hommes estretrouv avec un ratio de 2,4 pour lapriode 1993-1997 (allant de 1,8 3,6)(tableau 1).
De 1993 1997, le nombre de cas ta-bli par le systme des diagnostics des sor-
ties hospitalires (552) tait environ 2,5fois suprieur celui tabli daprs le sys-tme de notification. En ralit, ce rapportest sans doute plus lev du fait que le sys-tme de diagnostics hospitaliers ninclutpas les rgions autonomes, les Aores etMadre (figure 1).
studied using the statistical packageSPSS (6).
Estimation of incidenceNumbers of cases were extracted
from the hospital discharge (1993-97)and mortality (1991-96) databasescorresponding to the ICD-9 codes 100.0
to 100.9 (7), and directly from the annualreports of notifications (1991-97) (4).
As a denominator we used estimatesof population on 30 June 1994 (byregion, sex, and age group), the mid-point of the period considered in theanalysis (1991 to 1997). All rates wereexpressed in cases or deaths per millioninhabitants.
Correction of incidence estimatesData from both notification and
hospital discharge diagnosis systemsunderestimate the incidence of thedisease. Estimates of incidence can be
corrected by multiplying the total numberof deaths (assumed to have no relevanterrors) by the inverse of the ratio numberof death/number of cases. Consideringthat leptospirosis is an acute disease,the ratio number of death/number ofcases, in a given period of time, isassumed to be approximately the casefatality rate (3).
In order to reduce the error associatedwith small numbers we worked with thesum of all leptospirosis deaths observedbetween 1991 and 1996 (1997 data werenot available at the time of the study).
Based on the regional data analysispublished elsewhere (3) three differentratios were selected, corresponding tohigh, medium, and low case fatality rate.The highest value was 0.13 (AR Azores),corresponding to a quite high case fatality;the second was 0.10, corresponding to
the mainland and derived from hospitaldischarge data from 1993 to 1996, andthe third was 0.05, arbitrarily chosen asa low case fatality.
The annual mean crude incidence ofleptospirosis was obtained by dividingeach of the three estimates for the
regions by six times the estimate of theresident population estimate for the year1994 (7).
ResultsCrude incidenceThe incidence of leptospirosis esti-
mated by notifications was relativelystable between 1991 and 1996 but notin 1997 (table 1). Rates were higher inmen than in women throughout, by aratio of 2.7 (range 1.5 in 1992 to 5.2in 1995) (table 1).
Hospital discharge data yieldedhigher values for the incidence of lep-
tospirosis than did notifications. Malesoutnumbered females (overall rate ratio2.4 from 1993 to 1997 (range 1.8 to3.6) (table 1).
From 1993 to 1997 the number ofcases ascertained by the hospitaldischarge system (552) was about 2.5times larger than in the notificationsystem. The true ratio must have beenhigher since hospital discharge data donot include the autonomous regions ofAzores and Madeira (figure 1)
Age distributionTaking the period 1991-97 and both
sexes together, the age specific incidenceestimated from both notifications andhospital discharges increased with ageto peak in the 55-64 year age group,beyond which notifications declined buthospital discharge data continued toshow the same high rate (figure 2).
1991 1992 1993 1994 1995 1996 1997 Total
Diagnostics des sorties hospitalires (continent) / Hospital discharge diagnosis (mainland) (1)
Hommes / Male NA NA 13.2 12.1 10.2 20.7 30.0 17.3
(60) (55) (46) (94) (136) (391)
Femmes / Female NA NA 4.9 6.4 5.3 5.3 11.1 6.6
(24) (31) (26) (26) (54) (161)
Notification obligatoire (Portugal) / Mandatory notification (Portugal) (2)
Hommes / Male 3.8 2.5 4.8 5.2 6.5 3.4 11.1 5.8
(18) (12) (23) (25) (31) (16) (53) (194)
Femmes / Female 1.6 1.6 2.9 2.5 1.2 1.4 2.7 2.0
(8) (8) (15) (13) (6) (7) (14) (71)
Mortalit / Mortality (3)
Portugal 0.7 1.2 1.4 0.3 0.9 1.9 NA 1.1
(7) (12) (14) (3) (9) (19) NA ( 64)
(1) Instit ut de Gestio n Inf ormatiq ue et Financire, Ministre de la Sant, Portugal / Institute of Computational and Financial Management, Ministry of Health, Portugal .
(2) Direction Gnrale de la Sant /General Directorate of Health.
(3) Instit ut National d e Stat istiqu es /National Institu te of Stat istics.
(...) : nombre de cas /number o f cases
NA : Non disponible /Not available
Tableau 1 / Table 1Incidence de la leptospirose estime daprs deux systmes dinformation et taux de mortalit (/10 6 hab)
Incidence of leptospirosis from two information systems and death rate (/10 6 inhab)
8/3/2019 EARSS Organisation
6/10
MortalitySince 1991, fewer than 20 deaths
due to leptospirosis have been reported
each year. No clear trend emerged butthe crude mortality rate was highest (1.9deaths/106) in 1996 (table 1).
Estimation of the total number of
casesTwo hundred and nine cases were
notified in the whole country from1991 to 1996 (35 cases per year) and362 were ascertained from hospitaldischarges (mainland only, 91 casesper year). Using the number of deaths/number of cases ratios estimated fromthe regional analysis (3), the actualnumber of cases in Portugal from 1991
to 1996 could have ranged from aminimum of 492 cases (about 82 casesper year) to a maximum of 1280 (about213 cases per year) (table 2).
After correction the mean annualcrude incidence for Portugal rangedfrom 8.3 to 21.5 /106 (table 2).
DiscussionOur results show that the incidence
of leptospirosis is lower when estimatedby the notification system than whenestimated from hospital discharges.The notification should theoreticallyreceive reports of all cases diagnosed
in Portugal, but it depends heavily onthe efficiency of the information systemand it is not surprising that it under-estimates cases. The hospital dischargesystem, based on the compulsoryregistration of all diagnoses associatedwith hospital discharges, is an easierand more complete method of ascertain-ment. Some cases may be registeredby the hospital discharge system morethan once, however, making an over-estimate of the incidence possible. Forexample, a patient transferred betweenhospitals after the diagnosis of the sameepisode of disease would generate tworecords as would a patient admittedtwice during the same episode. At thesame time, the incidence may be under-estimated because not all cases areadmitted to hospital.
Results from both notification andhospital discharge systems are highlyconsistent regarding the sex and agespecific incidence.
Given the available data it is importantto improve estimates of incidence usingdata from mortality, which are likely tobe more reliable, and by consideringthree values of the ratio number of
deaths/number of cases. The limitationof mortality data is the small number ofevents, even when deaths from a periodof six years are summarised.
The results from our study suggestthat:
1. The incidence of leptospirosis inPortugal is probably higher than estimatesobtained by notifications and hospitaldischarge data;
2. Hospital discharge data suggestthat the number of cases of leptospirosisincreased in 1996 and 1997. Thisobservation is supported by an increase
46 EUROSURVEILLANCE VOL. 4 - N4 AVRIL-APRIL 1999
Distribution selon lgePour la priode 1991-1997, hommes
et femmes confondus, lestimation de lin-cidence en fonction de lge, que ce soitdaprs le systme de notification obliga-toire ou le systme de notification hospi-talire, augmentait avec lge jusquaux55-64 ans, puis diminuait chez les sujets
plus gs. Les donnes se maintenaientcependant des valeurs hautes chez lesplus de 65 ans daprs le systme de noti-fication hospitalire (figure 2).
MortalitDepuis 1991, moins de 20 dcs dus
la leptospirose ont t rapports chaqueanne. Aucune tendance nette na merg,mais le taux de mortalit brut le plus lev(1,9 dcs par million dhabitants) taitobserv en 1996 (tableau 1).
Estimation du nombre total de casDe 1991 1996, 209 cas (35 cas par
an) ont t notifis pour lensemble du pays
et 362 ont t tablis daprs les dia-gnostics de sorties hospitalires (91 caspar an pour le seul territoire continental).Si lon se base sur le ratio nombre de dcs/nombre de cas estim daprs lanalysergionale (3), le nombre rel de cas au Por-tugal de 1991 1996 pourrait tre com-pris entre 492 (environ 82 cas par an) et1280 (environ 213 cas par an) (tableau 2).
Aprs correct ion, lincidence annuellemoyenne brute au Portugal allait de 8,3 21,5 par million dhabitants (tableau 2).
DiscussionDaprs nos rsultats, lincidence de la
leptospirose estime daprs le systmede notification est plus faible que celleestime avec les donnes du systme dediagnostics de sorties hospitalires. Tho-riquement, lensemble des cas diagnosti-qus au Portugal devrait tre rapport ausystme de dclaration obligatoire, maiscela dpend fortement de lefficacit dusystme dinformation. Il nest donc passurprenant quil y ait une sous-estimationdes cas.
Le systme des diagnostics hospitaliers,bas sur lenregistrement obligatoire detous les diagnostics tablis lors des sor-
ties hospitalires, est une mthode de vri-fication plus facile et plus exhaustive.Certains cas peuvent cependant y tre enre-gistrs plus dune fois, rsultant en une sur-estimation de lincidence possible. Parexemple, un patient transfr dun hpital un autre aprs que le diagnostic dumme pisode ait t pos pourra fairelobjet de deux enregistrements ; de mme,si un patient a t admis deux fois pour unmme pisode. Inversement, lincidencepeut tre sous-estime du fait que tous lespatients ne sont pas hospitaliss.
Les rsultats obtenus avec les deux
systmes, notification obligatoire et dcla-ration hospitalire, sont cohrents pour cequi est de lincidence selon le sexe et lge.
Au vu des donnes disponibles, il estimportant damliorer les estimations delincidence en utilisant les donnes de mor-talit, a priori plus fiables, et de prendre encompte les trois valeurs du ratio nombre
de dcs/nombre de cas. La faiblesse desdonnes de mortalit est le petit nombre
Rat io dcs/cas / Nombre de cas total / Incidence annuelle (/ 106 hab) /
Deaths/Cases rat io (1) Total cases number Annual incidence ( /106 inhab)
0.13 492 8,3
0.10 640 10,8
0.05 1280 21.5
(1) le nombre t otal de dcs est 64 /Total number o f d eaths is 64
Tableau 2 / Table 2Estimations du nombre de cas de leptospirose et incidence annuelle
(Portugal, 1991-1996) / Estimates of the number of cases of Leptospirosisand annual incidence (Portugal, 1991-1996)
0
Taux brut dhospitalisations dues la lept ospirose (HD, continent)et incidence brute (MN, tout le territoire portugais) /Crude rates of hospital admissions by leptospirosis (HD, in the continent)and crude rates (MN, in Portugal)
Figure 1
1991 1992 1993 1994 1995 1996 1997
(/106)
5
10
15
20
25
Donnesnon disponibles/ Data not availableHD : Diagnosticsdes sortieshospitalires/ Hospital Discharge DiagnosisMN : Dclarationsobligatoires/ Madatory Notifications
MN HD
0
Incidences annuelles moyennes de la leptospirose par groupe dge /Annual mean incidence rates of leptospirosis by age group
Figure 2
< 15 15-24 25-34 35-44 45-54 55-64 65
(/106)
5
10
15
20
25
HD : Diagnosticsdessorties hospitaliresde 1993 1997, territoire continental /Hospital Discharge Diagnosisfrom 1993 to 1997 , continent only
MN : Dclarationsobligatoiresde 1991 1997, t erritoire continental et rgion autonome de Madre /Madatory Notificationsfrom 1991 to 1997, continent + autonomousregion of Madeira
MN HD
8/3/2019 EARSS Organisation
7/10
EUROSURVEILLANCE VOL. 4 - N4 AVRIL-APRIL 1999 47
dvnements, y compris lorsque les don-nes sont cumules sur six annes.
Les rsultats de notre tude suggrentdonc que :
1. Lincidence de la leptospirose au Por-tugal est vraisemblablement suprieure celle estime daprs les notifications et
les donnes de sorties hospitalires.2. Daprs les donnes du systme din-formation des hpitaux, il y a eu une aug-mentation du nombre de cas deleptospirose en 1996 et en 1997. Cetteobservation est corrobore par laugmen-tation du nombre des cas notifis en 1997.
3. Lincidence de la leptospirose est plusimportante chez les hommes que chez lesfemmes et augmente nettement autour dela soixantaine.
Nous pensons que le poids de la lepto-spirose est plus important que ne le lais-sent paratre les donnes de routine. Notre
prochain objectif est dtudier les modesde transmission les plus courants de lamaladie et les srotypes associs la lep-tospirose. Nos conclusions ont t com-muniques aux autorits sanitaires afindamliorer la surveillance et de promou-voir les actions prventives. Des rsultatsplus dtaills, dont les donnes de lana-
lyse rgionale vont tre publis dans unerevue portugaise (3).
RemerciementsNous tenons remercier lInstituto de
Gesto Informtica e Financeira du Minis-trio da Sade et lInstituto Nacional deEstatsticaqui nous ont permis dutiliser leurbases de donnes, et la Direction Gnralede la Sant qui nous a fourni des donnesnon encore publies. s
in the number of cases notified in 1997.3. The incidence of leptospirosis is
higher in men than in women and peaksin late middle age.
We suspect that the burden of lepto-spirosis is greater than routine incidencedata appear to indicate. We plan to study
the commoner modes of transmissionof the disease and investigate theserovars associated with leptospirosis.Our findings have been reported to thehealth authorities in order to increasesurveillance and promote preventiveactions. More detailed results, includingthe regional data analysis will be publishedin a Portuguese journal (3).
AcknowledgementsWe are grateful to Instituto de Gesto
Informtica e Financeira of the Ministrioda Sade and to Instituto Nacional deEstatsticafor the use of their databases,
and to Direco Geral da Sade forproviding data not yet published. s
References
1. Benenson AS. Control of communicable diseasesin man 15th edition- Washington DC: AmericanPublic Health Association, 199 0.
2. Cruickshank R, Duguid JP, Marmion BP, SwainRHA. Medical microbiology Twelfth edition. City:
Churchill-Livingstone, 1973.3. Falco JM, Nogueira PJ, Matias Dias C, PimentaZP. Leptospiroses em Portugal: a situao epide-miolgica recente. Revista Portuguesa de SadePblica(in press).
4. Portugal Direco Geral da Sade.Direco deServios de Informao e Anlise. Diviso deEpidemiologia. Doenas de Declarao Obrigatr ia1991/1995, 1992/1996, 1997.
5. Urbano J, Bentes M. Definio da produo dohospital: os grupos de diagnsticos homogneos.Rev Port Sade Pblica1990; 8; 1: 49-60.
6. Norusis, MJ. SPSS for Windows professionalstatistics. Chicago: Statistical Package for SocialSciences, 1993.
7. Classificao Internacional de Doenas-9 Reviso1975, 3 edio. Ministrio da Sade, Universi-dade de S.Paulo, Brasil: Organizao Mundial daSade, Centro da OMS para Classificao deDoenas em Portugus, 197 5.
Epidmie dintoxications alimentaires Salmonella enteritidisprovenant dun fromagede fabrication industrielleM.G.Panico1, F. Primiano2, F. Nappi3, F.Attena41 Servizio di Epidemiologia e Prevenzione - A.S.L., Naples 4, Italie2 Distretto Sanitario 78 - A.S.L. Naples 4, Italie3 Distretto Sanitario 74 - A.S.L. Naples 4, Italie4 Istituto di Igiene e Medicina Preventiva - Seconda Universit di Napoli - Naples, Italie
Introduction
Entre le 30 juin et le 2 juillet 1998, trois hpitaux ont dclar neuf cas suspectsdintoxications alimentaires au service dpidmiologie et de prvention (Servizio diEpidemiologia e Prevenzione - SEP) des autorits sanitaires locales de la rgion de Naples(Azienda Sanitaria Locale, ASL NA 4). Le SEP dbuta aussitt une enqute.
Enqute pidmiologiqueLes neuf patients rsidaient Roccarainola, un village denviron 7000 habitants et
appartenaient quatre familles prsentant des liens de parent. Il sagissait dhommeset de femmes gs de deux 67 ans (moyenne 32 ans). Tous ont souffert dune diar-rhe, six ont eu des douleurs abdominales, cinq des vomissements, quatre de la fivreet un a eu une migraine. La priode dincubation allait de neuf 27 heures (moyenne 17).Le seul aliment quils avaient tous consomms, le 28 juin, tait un tiramis.
Le tiramis est un gteau prpar sans cuisson avec les ingrdients suivants : sucre,mascarpone pasteuris sous emballage scell (fromage industriel base de crme frache),
crme frache fouette, boudoirs, ufs et caf froid. Le gteau en question avait t pr-par le 27 juin par lun des patients, puis conserv temprature ambiante jusqu saconsommation.
Les restes du gteau, conservs au conglateur - 18C, ont t rcuprs sondomicile le 1er juillet, ainsi que des boudoirs, et un uf provenant de son poulailler. Desinvestigations ont t menes le mme jour sur les lieux dachat des ingrdients et, parmesure de prcaution, des chantillons des aliments pouvant tre incrimins ont tsaisis : boudoirs, mascarpone emball appartenant au mme lot que celui ayant servi prparer le dessert, crme frache fouette et ufs.
Enqute microbiologiqueSalmonella enteritidisa t mise en vidence dans le gteau et dans lchantillon de
mascarpone. Les autres chantillons taient ngatifs pour les salmonelles et autres patho-gnes associs des intoxications alimentaires. Des salmonelles du groupe D, dont
An outbreak of Salmonella enteritidisfood poisoning from an commercially producedcheeseM.G.Panico1, F. Primiano2, F. Nappi3, F.Attena41 Servizio di Epidemiologia e Prevenzione - A.S.L., Napoli 4, Italy2 Distretto Sanitario 78 - A.S.L. Napoli 4, Italy3 Distretto Sanitario 74 - A.S.L. Napoli 4, Italy4 Istituto di Igiene e Medicina Preventiva - Seconda Universit di Napoli - Napoli 4, Italy
Introduction
Nine suspected cases of food poisoning were reported from three hospitals tothe epidemiology and prevention service (Servizio di Epidemiologia e Prevenzione- SEP) of the local health authority in Naples district (Azienda Sanitaria Locale,ASL NA 4) between 30 June and 2 July 1998. The SEP immediately started toinvestigate the outbreak.
Epidemiological investigationAll nine cases lived Roccarainola, a rural area of about 7000 inhabitants, and
belonged to four related families. They were aged 2 to 67 years (mean 32) and ofboth sexes. All had diarrhoea, six had abdominal pain, five vomiting, four fever, andone headache. The incubation period was between 9 and 27 hours (mean 17). Theonly food item they had all eaten was tiramis cake, on 28 June.
Tiramis cake is prepared without cooking. It is made from sugar, pasteurisedand sealed mascarpone (a commercially prepared fresh cream cheese), loose
fresh whipped cream, sponge biscuits, eggs, and cold coffee. One of the patientshad made it on 27 June, and kept it at room temperature until it was eaten.
On 1 July, the following food items were retrieved from his home: leftovertiramis stored in the freezer at -18C, sponge finger biscuits, and one egg fromthe hens kept at home. The shops where the ingredients had been bought wereinvestigated on the same day. Samples of the possible food items involved weretaken and seized as a precaution: sponge biscuits and sealed mascarpone fromthe same batch used to prepare the cake, fresh whipped cream, and eggs.
Laboratory investigationSalmonella enteritidiswas found both in the home-made tiramis cake and in
the sealed sample of mascarpone. Other samples were negative for salmonellaand other pathogens associated with food poisoning. Salmonella of group D,to which S. enteritidisbelongs, was isolated from six cases and non-typhoid
RAP P O RT D I NV E S T I GAT I O N OUTBREAK REPORT
8/3/2019 EARSS Organisation
8/10
48 EUROSURVEILLANCE VOL. 4 - N4 AVRIL-APRIL 1999
IMPRESSION:REFLEXGRAPHIC
RESPONSABLES SCIENTIFIQUES /SCIENTIFIC EDITORS J.C. Desenclos
Rseau National de SantPublique - Saint-Maurice - France
J. DruckerRseau National de SantPublique - Saint-Maurice - France
N. GillP.H.L.S - Communicable DiseaseSurveillance Centre - London -United Kingdom
S. HandysidesP.H.L.S - Communicable DiseaseSurveillance Centre - London -United Kingdom
S. SalmasoIstituto Superiore di Sanit - Italy
L. WijgergangsRijksinstituut Voor Volksgezondheiden Milieu - Netherlands
COMIT DE RDACTION /EDITORIAL BOARD P. Christie
SCIEH Weekly Report- Scotland K. Ekdahl
Smittskydd- Sweden S. Handysides
Communicable Disease Report-England and Wales
A. Karait ianou-VelonakiMinistry of Health, Welfare andSocial Security - Greece
W. KiehlEpidemiologisches Bulletin-Germany
J.P. KleinBundesministerium fr Gesundheit -Austria
M. Le Quellec-NathanBulletin EpidmiologiqueHebdomadaire- France
G. LimaSade em Nmeros- Portugal
J. F. Martinez NavarroBoletn Epidemiolgico Semanal-Spain
H. NohynekKansanterveys- Finland
T. RnneEPI-NEWS- Denmark
S. SalmasoIstituto Superiore di Sanit - Italy
M. SprengerInfectieziekten Bulletin- Netherlands
L. ThorntonInfectious Diseases Bulletin-Ireland
F. Van LoockEpidemiologisch Bulletin van deGezondheidsinspectie van deVlaamse Gemeenschap -Sant et communaut- Belgium
DIRECTEUR DE LA PUBLICATION /MANAGING EDITOR J. B. Brunet
Centre Europen pour laSurveillance Epidmiologiquedu Sida - Saint-Maurice - France
RDACTEURS ADJOINTS /DEPUTY EDITORS C. Akehurst
P.H.L.S - Communicable DiseaseSurveillance Centre - 61 ColindaleAvenue London NW9 5EQ -United KingdomTel. (44) (0) 181 200 6868Fax. (44) (0) 181 200 7868
H. TherreCentre Europen pour laSurveillance Epidmiologiquedu SIDA - 14 rue du Val dOsne94410 Saint-Maurice - France -Tel. (33) (1) 41 79 68 [email protected]
SECRTARIAT / SECRETARY A. Goldschmidt F. MihoubSaint-Maurice - France
EUROSURVEILLANCEHpital National de Saint-Maurice14, rue du Val dOsne94410 Saint-MauriceTel. (33) (1) 41 79 68 32Fax. (33) (1) 41 79 68 01ISSN: 1025 - 496X
EUROSURVEILLANCE (mensuel / monthly) http:/ / www.ceses.org/ eurosurvEUROSURVEILLANCE WEEKLY http:/ / www.eurosurv.org
E U R O SU R V E I L L A N C E O N T H E W E B
fait partie S enteriditis, ont t isoles chez six cas et des sal-monelles non-typhiques chez deux autres. Pour le dernier patient,un test de Widal (anticorps agglutinants anti-O) avait t ralis parlhpital car il y avait une suspicion de fivre typhode. Les rsultats(anti-O=1:640) taient compatibles avec une infection par S. enteritidisdu fait de la possibilit, avec le test de Widal, de ractions croisesavec les salmonelles non-typhiques du groupe D (1).
Enqute environnementaleSi le SEP a pu vrifier que le mascarpone avait t achet le jourmme de la prparation du gteau, en revanche, il na pu sassurerque ce fromage avait t gard au frais dans la boutique. Le mas-carpone contamin tant fabriqu par une socit de renom situeloin de Roccarainola, lpidmie a t dclare aux autorits publiquescentrales et, suite cette notification, le lot de mascarpone conta-min a t retir de la vente. Une enqute, mene par les autoritssanitaires locales dans lusine de fabrication et auprs du person-nel, a conclu que les standards dhygine taient respects.
DiscussionDun point de vue pidmiologique, cette pidmie parat simple
du fait que lagent tiologique, le vhicule de linfection et lalimentcontamin ont t rapidement identifis. Les laboratoires hospita-liers ntaient pas quips pour identif ier les salmonelles de manire
spcifique, mais il semble probable que les salmonelles de groupeD isoles chez les patients taient identiques S. enteritidismiseen vidence dans le mascarpone et le gteau. Lidentification de S.enteritidisdans des produits sous emballages scells montre que lacontamination sest produite soit lusine, soit plus tt au niveau desmatires premires. Un facteur important lorigine de cette pi-dmie peut tre le fait que le gteau avait t prpar un jour avantdtre consomm et conserv temprature ambiante, conditionsfavorables au dveloppement des salmonelles. De plus, on ne peutexclure la possibilit que le mascarpone nait pas t conserv aufrais dans la boutique, un problme qui a dj t soulev dans cettergion.
Aux termes de lenqute ultrieure mene dans lusine de fabri-cation, aucun point crit ique de contamination possible na t relev.Il est possible que cette enqute nait pas t ralise correctementou que le point critique ait t limin auparavant.
Les pidmies dinfection Salmonella enteritidisconstituent unproblme de sant publique en Italie (2), en Europe (3) et aux Etats-Unis (4). Cette enqute confirme que le tiramis est souvent impli-qu dans ce type dpidmie (5-7), sa prparation requrant desingrdients crus sans tape de cuisson. Lors des autres pidmiesles ufs ont t identifis comme tant les vhicules de linfection.Lincident dcrit ici est quelque peu inhabituel, car il a mis en causeun fromage la crme frache de fabrication industrielle. s
salmonella from two. In the last case, Widal test (aggluti-nating antibodies anti-O) wasperformed in the hospital becausetyphoid fever was suspected. The results (anti-O=1:640) werecompatible with S. enteritidisinfection, cross-reactions ofWidal test occurring with non-typhoid group D salmonella (1).
Environmental investigationThe SEP ascertained that the mascarpone had been bought
the same day the cake was prepared, but could not establishwhether it had been refrigerated in the shop. The contaminatedmascarpone was produced by a well known company far fromRoccarainola and SEP therefore reported the outbreak to thecentral public authorities. This notification resulted in the batchof contaminated mascarpone being withdrawn from sale. Aninvestigation of the processing plant and the staff carried outby the local health authority concluded that both met thestandards required.
DiscussionThis outbreak appeared to be straightforward in epide-
miological terms, in that the aetiological agent, the vehicle,and the contaminated food item were identified swiftly. Thehospital laboratories were not equipped to identify salmonellasspecifically but it seems likely that the group D salmonellas
isolated from cases were the same as the S. enteritidisfound inthe mascarpone and the cake. The identification of S. enteritidisin sealed product shows that contamination either arose atthe plant or earlier in raw materials. An important factor incausing the outbreak may be that the cake was made the daybefore consumption and that it was kept at room temperature,providing conditions in which salmonellas thrive. In addition,we cannot exclude the possibility that the mascarpone wasnot kept refrigerated in the shop, a problem that has alreadybeen noted in this area.
The subsequent investigation of the manufacturing plantfound no critical point of possible contamination. It may bethat the investigation was not adequately carried out or thatthe critical point had been eliminated beforehand.
Outbreaks of Salmonella enteritidisinfection are a publichealth problem in Italy (2), Europe (3), and the United States(4). The present investigation confirms that in Italy the tiramiscake is often implicated in this type of outbreak (5-7) becauseraw ingredients are used and the preparation involves nocooking. Other outbreaks have identified eggs as the vehicle ofinfection. This incident was somewhat unusual as it implicateda commercially produced fresh cream cheese. s
1. Schroeder SA. Interpretation of serologic test for typhod fever. JAMA 1968; 206 : 839-40.2. Nastasi A, Mammina C. Epidemiology of Salmonella enterica serotype Enterit idis infect ions in southern Italy during the years 198 0-1994 . Res Microbiol1996;
147 : 393-403.3. Centers for Disease Control. Outbreaks of Salmonella serotype enteritidis infection associated with consumption of raw shell eggs - United States 1994-
1995. JAMA 1996; 276 (13): 1017-9.4. WHO Surveillance programme for Control of Foodborne Infections and Intoxications in Europe. Sixth Report, 1990-1992. Berlin: Federal Institute for
Health Protection of Consumers and Veterinary Medicine, 1995.5. Cinquetti S, Collareta A, Mazzer R, Scagnelli M, Raris M, Paludetti P, et al. Un episodio di tossinfezione da S. enteritidis associato a consumo di dolcepreparato ar tigianalmente. Igiene Moderna1991; 96 : 333-40.
6. Delia S, Lagan P, Quartone F. Un grave episodio di tossinfezione alimentare da S. enteritidis: riflessioni e suggerimenti. Rivista Italiana di Igiene1993; 53 :40-51.
7. Delia S, Lagan P. Un caso di tossinfezione alimentare da S. enteritidis fagotipo 6. Rivista italiana di Igiene 1995; 55 : 59-63.
References
8/3/2019 EARSS Organisation
9/10
D A N S L E S B UL L E T I N S N A T I O N A U X I N T H E N A T I O N A L B U LL ET I N S
Une slection dans les derniers numros parus A selection from current issues
Vol. 4 N4 AVRIL / APRIL 1999
INDEX
BOTULISME / BOTULISM- Wound botulism in Switzerland.
Eurosurveillance Weekly1999; 3:990225. (http:/ / www.eurosurv.org/ )
DIPHTRIE / DIPHTHERIA- Diphtheria in WHOs European region.
Epidemiologisches Bulletin1999; (4):21-2. [29 January. Germany]
- Diphtheria: case report from Denmark.Epidemiologisches Bulletin1999;(4): 22-3. [29 January. Germany]
EAU / WATER- Water related surveillance in Europe.
Eurosurveillance Weekly1999; 3:990304. (http:/ / www.eurosurv.org/ )
- Outbreak of gastroenteritis associatedwith contamination of a private boreholewater supply. Commun Dis PublicHealth1999; 2(1): 27-31.[March. England and Wales]
- Microbiological quality of drinking waterfrom office water dispensers. CommunDis Public Health1999; 2(1): 67-8.[March. England and Wales]
- Surveillance of waterborne disease andwater quality: July to December 1998.Commun Dis Rep CDR Wkly1999; 9(8):73-5. [19 February. England and Wales]
- Preventing waterborne epidemics isworth the effort for municipalities.Kansanterveys1999; (2): 1.[February. Finland]
- Waterborne epidemics can be preventedby good quality processing ofhousehold water. Kansanterveys1999;(2): 2-3. [February. Finland]
- Nitrifying bacteria in the network ofwaterpipes. Kansanterveys1999; (2): 3.[February. Finland]
- Bacteria embedded in the pipes -
cleaning up the water pipes improvedthe quality of drinking water.Kansanterveys1999; (2): 3-4.[February. Finland]
ESCHERICHIA COLI- Escherichia coli O157 infection
associated with a farm open to membersof the public. Commun Dis PublicHealth1999; 2(1): 22-6.[March. England and Wales]
- Enterohaemorrhagic Escherichia coliinfection and haemolytic uraemicsyndrome become notifiable in Germany.Eurosurveillance Weekly1999; 3:990211. (http://www.eurosurv.org/)
- E. coli O157 surveillance, NorthernIreland. Communicable Diseases1998;7(10). [Wks 37-40. Northern Ireland]
EUROPE- Health policy in the European Union.
Epidemiologisches Bulletin1999;(5): 29. [5 February. Germany]
- Antibiotics: EU ban on four antibiotics asgrowth promoters in animal husbandry.Epidemiologisches Bulletin1999;(4): 24. [29 January. Germany]
GRIPPE / INFLUENZA- Acute respiratory infections, and
influenza vaccine for 1999/ 2000.Commun Dis Rep CDR Wkly1999; 9(10):87-90. [5 March. England and Wales]
- Influenza activity in Europe.Eurosurveillance Weekly1999;3: 990304.(http:/ / www.eurosurv.org/ )
- Influenza vaccine components for thenorthern hemisphere 1999-2000.Eurosurveillance Weekly1999;3: 990304.
(http:/ / www.eurosurv.org/ )- Infectious disease adviser: 1. Influenza.
Epidemiologisches Bulletin1999;(7): 42-3. [19 February. Germany]
- Influenza. EPI-NEWS1999; (7).[17 February. Denmark]
- Influenza/acute respiratory infections:current situation. EpidemiologischesBulletin1999; (4): 24. [29 January];ibid(5): 31. [5 February]; ibid(6): 37.[12 February. Germany]
- Respiratory infections in the Netherlands:influenza virus and respiratory syncytialvirus. Infectieziekten Bulletin1999;10(2): 32-3. [February. Netherlands]
- Current information on influenza on the
internet. Kansanterveys1999; (1): 7.[January. Finland]
HANTAVIRUS- Risk factors for Hantavirus infection:
case control study in the Belgianand French Ardennes. Bulletinpidmiologique Hebdomadaire1999;(8): 30-1. [23 February. France]
HPATITE / HEPATITIS- Comparison between the risks of first
attack of acute central demyelinationand the benefits of vaccination againsthepatitis B. Bulletin pidmiologiqueHebdomadaire1999; (9): 33-5.[3 March. France]
- Outbreak of hepatitis A in Rotterdamassociated with visits to darkrooms ingay bars. Commun Dis PublicHealth1999; 2(1): 43-6.[March. England and Wales]
- Hepatitis C 1997-1998. EPI-NEWS1999; (8). [24 February. Denmark]
- Hepatitis A: an outbreak report.
Epidemiologisches Bulletin 1999;(5): 30-1. [5 February. Germany]/Eurosurveillance Weekly1999;3: 990304.(http:/ / www.eurosurv.org/ )
- Hepatitis C. Communicable Diseases1998; 7(11).[Wks 41-44. Northern Ireland]
INFECTION MENINGOCOQUE /MENINGOCOCCAL DISEASE- Enhanced surveillance of suspected
meningococcal disease. Commun DisRep CDR Wkly1999; 9(9): 78-9.[26 February. England and Wales]
- Meningococcal disease in adults.SCIEH Weekly Report1999; 33(9): 69.
[23 February. Scotland]- Outbreak of meningococcal disease inSouth Wales - update. Commun Dis RepCDR Wkly1999; 9(8): 65. [19 February.England and Wales]/ EurosurveillanceWeekly1999; 3: 990218.(http:/ / www.eurosurv.org/ )
- Meningococcal outbreak in Wales.SCIEH Weekly Report1999; 33(7): 61.[16 February. Scotland]
- Outbreak of meningococcal disease inSouth Wales follows general increase indisease activity. Commun Dis Rep CDRWkly1999; 9(7): 57, 60. [12 February.England and Wales]/ EurosurveillanceWeekly1999; 3: 990211.(http:/ / www.eurosurv.org/ )
- Meningococcal infection.Communicable Diseases1998; 7(11).[Wks 41-44. Northern Ireland]
INFECTIONS NOSOCOMIALES /NOSOCOMIAL INFECTION- Surveillance network of nosocomial
infections in intensive care.The experience of RA south east.Bulletin pidmiologique Hebdomadaire1999; (5): 17-9. [2 February. France]
INTOXICATIONS ALIMENTAIRES /FOOD POISONING- Gastro-intestinal infect ions. SCIEH
Weekly Report1999; 33 (9): 74-5.[2 March. Scotland]
- Investigation of an outbreak ofgastroenteritis at hospital for patientswith learning difficulties. CommunDis Public Health1999; 2(1): 35-8.[March. England and Wales]
- An outbreak of campylobacter foodpoisoning at a university campus.Commun Dis Public Health1999; 2(1):
39-42. [March. England and Wales]- Outbreak of gastro-enteritis in Tayside.
SCIEH Weekly Report1999; 33(8): 65.[23 February. Scotland]
- Outbreak of gastroenteritis in ForthValley. SCIEH Weekly Report1999;33(7): 61. [16 February. Scotland]
- Update on infectious intestinal diseaseoutbreak in Ayrshire and Arran. SCIEHWeekly Report1999; 33 (6): 57.[9 February. Scotland]
- The Gvle festival did not resultin outbreak of gastro-enteritis.Smittskydd1999; 5(1): 3-4.[January. Sweden]
- Campylobacter epidemic in Haukipudas
in August 1998. Kansanterveys1999;(1): 9. [January. Finland]
- Communication was an important partof handling the Haukipudascampylobacter epidemic. Kansanterveys1999; (1): 9-10. [January. Finland]
- Food poisoning from a meat dish in aGreek fest ival. Kansanterveys1999;(1): 7-8. [January. Finland]
- Outbreak report. CommunicableDiseases1998; 7(11).[Wks 41-44. Northern Ireland]
LEGIONELLOSE / LEGIONELLOSIS- Legionellosis in Ayrshire and Arran.
SCIEH Weekly Report1999; 33(6): 57.[9 February. Scotland]
- Legionellosis reported in Francein 1997. Bulletin pidmiologiqueHebdomadaire1999; (6): 21-2.[9 February. France]
MALADIE DE CREUTZFELDT-JAKOB /CREUTZFELDT-JAKOB DISEASE- Bovine spongiform encephalopathy
and new variant Creutzfeldt-Jakobdisease: an overview. Commun DisPublic Health1999; 2(1): 5-13.[March. England and Wales]
- New variant Creutzfeldt-Jakob disease inthe United Kingdom. EurosurveillanceWeekly1999; 3: 990211; ibid990304.(http:/ / www.eurosurv.org/ )
EUROSURVEILLANCE VOL. 4 - N4 AVRIL-A PRIL 199 9 49
8/3/2019 EARSS Organisation
10/10
50 EUROSURVEILLANCE VOL.4 - N4 AVRIL-APRIL 1999
EUROSURVEILLANCE (mensuel / monthly) http:/ / www.ceses.org/ eurosurv
EUROSURVEILLANCE WEEKLY http:/ / www.eurosurv.org
E U R O SU R V E I L L A N CE O N T H E W E B
Bundesministerium fr Arbeit, Gesundheit und Soziales -
Austria - Tel: (43) 1 711 72 41 03 - Fax: (43) 1 713 86 14
Epidemiologisch Bulletin van de Gezondheidsinspectie
van de Vlaamse Gemeenschap- Belgium -
Tel: (32) 3 224 62 05 - Fax: (32) 3 224 62 01
Institut Scientifique de la Sant Publique Louis Pasteur -
Belgium - Tel: (32) 2 642 51 11 - Fax: (32) 2 642 54 10
EPI - NEWS- Denmark -
Tel: (45) 32 683 268 - Fax: (45) 32 683 874
(http:/ / www.ssi.dk)
Communicable Disease Report- England and Wales -
Tel: (44) (0) 181 200 6868 - Fax: (44) (0) 181 200 7868
- (http:/ / www.phls.co.uk/ publications)
Kansanterveys- Finland - Tel: (358) 9 4744 82 46 -
Fax: (358) 9 4744 86 75 - (http:/ / www.ktl.fi)
Bulletin Epidmiologique Hebdomadaire- France -
Tel: (33) (1) 40 56 45 40 - Fax: (33) (1) 40 56 50 56 -
(http:/ / www.b3e.jussieu.fr/rnsp/beh/ index.html)
Epidemiologisches Bulletin- Germany -
Tel: (49) 30 45 47 34 06 - Fax: (49) 30 45 47 35 44
(http:/ / www.rki.de/ INFEKT/ EPIBULL/EPI.HTM)
Ministry of Health, Welfare - Greece -
Tel: (301) 646 67 11 - Fax: (301) 646 67 45
I.D. Bulletin- Ireland -
Tel: (353) (1) 668 15 77 - Fax: (353) (1) 671 06 06
Infoscan, Southern Communicable Disease Report-
Ireland - Tel: (353) 21 343 926
(http:/ / www.ucc.ie/ faculties/ medical/infoscan/ )
Notiziario dellIstituto Superiore di Sanit- Italy -
Tel: (39) 06 49 38 726 15 - Fax: (39) 06 49 38 72 92
(http:/ / www.iss.it/ pubblicazioni/ Notiziar.htm)
Infectieziekten Bulletin- Netherlands -
Tel: (31) 30 274 3551 - Fax: (31) 30 274 44 09 -
(http:/ / www.isis.rivm.nl/ )
Communicable Diseases- Northern Ireland -
Tel: (44) (0) 1232 520 716
Sade em Nmeros- Portugal -
Tel: (351) 1 847 55 15 - Fax: (351) 1 847 66 39 -
(http:/ / www.telepac.pt/ dgsdeb/ )
SCIEH Weekly Report - Scotland -
Tel: (44) 141 300 11 00 - Fax: (44) 141 300 11 70
Boletn Epidemiolgico Semanal- Spain -
Tel: (34) 91 387 78 02 - Fax: (34) 91 387 78 16
(http:/ / www.isciii.es/cne)
Smittskydd- Sweden -
Tel: (46) (8) 457 2379 - Fax: (46) (8) 300 626
- Monthly surveillance figures forCreutzfeldt-Jakob disease. SCIEHWeekly Report1999; 33(6): 57.[9 February. Scotland]
MST / STDs- Sexually transmitted diseases. SCIEH
Weekly Report1999; 33 (7): 62-3.[16 February. Scotland]
- Chlamydia 1997. EPI-NEWS1999; (5).[3 February. Denmark]
MALADIES TRANSMISSIBLES /INFECTIOUS DISEASES- Public health early warning system:
Andalusia, Spain. EurosurveillanceWeekly1999; 3: 990304.(http:/ / www.eurosurv.org/)
- Respiratory infections. SCIEH WeeklyReport1999; 33(6): 58-9.[9 February. Scotland]
- Expansion of feedback on notifiableinfectious diseases via the internet.Infectieziekten Bulletin1999;10 (2): 34-5.[February. Netherlands]
- The value of medical microbiologylaboratories for 5 notifiable diseases.Infectieziekten Bulletin1999;10 (2): 27-31.[February. Netherlands]
- Infectious diseases in Englandand Wales. Commun Dis Rep CDR Wkly1999; 9(suppl 2): S1-20.[February. England and Wales]
- Mortality in Spain 1995. Mortalitygeneral and principal causes of deathand by years of potential life lost. I.Boletn Epidemiolgico Semanal1998;6(11): 105-11. [14 October]; ibidII.(12): 117-24. [14 October 1998. Spain]
PSITTACOSE / PSITTACOSIS- Psittacosis 1995-1998. EPI-NEWS
1999; (6). [10 February. Denmark]/Eurosurveillance Weekly1999; 3:990225. (http:/ / www.eurosurv.org/ )
RAGE / RABIES- Rabies: risk of infection associated with
travel. Epidemiologisches Bulletin1999;(6): 35-6. [12 February. Germany]
RSISTANCE ANTIMICROBIENNE /ANTIMICROBIAL RESISTANCE- Methicillin resistance in Staphylococcus
aureus isolated from blood in Englandand Wales: 1994 to 1998. Commun DisRep CDR Wkly1999; 9(8): 65, 68.[19 February. England and Wales]
- Vancomycin-resistant enterococci (VRE)in man and animals in the Netherlandsand Europe. Infectieziekten Bulletin1999; 10 (1): 3-7.[January. The Netherlands]
- Surveillance of resistant pathogensat the European level. InfectieziektenBulletin1999; 10(1): 7-10.[January. Netherlands]
- All-Ireland study of methicillin resistantStaphylococcus aureus (MRSA).Communicable Diseases1998; 7(11).[Wks 41-44. Northern Ireland]
ROTAVIRUS- Rotavirus in Spain. Notifications to
microbiological information system.Boletn Epidemiolgico Semanal1998;6(11): 111. [14 October 1998. Spain]
SALMONELLOSE / SALMONELLOSIS- Common source outbreak
of salmonellosis in a food factory.Commun Dis Public Health1999;2(1): 32-4. [March. England and Wales]
- Undercooked hens eggs remain a riskfactor for sporadic Salmonella enteritidisinfection. Commun Dis Public Health1999; 2(1): 66-7.[March. England and Wales]
- Salmonella java phage type Dundee -rise in cases. Commun Dis Rep CDRWkly1999; 9(9): 77. [26 February.England and Wales]/ Eurosurveillance
Weekly1999; 3: 990225.(http:/ / www.eurosurv.org/ )
SIDA / AIDS- AIDS and HIV infection in the United
Kingdom: monthly report. Commun DisRep CDR Wkly1999; 9(9): 85-6.[26 February. England and Wales]
- HIV infection reporting - the valueof linking data sources. EurosurveillanceWeekly1999; 3: 990218.(http:/ / www.eurosurv.org/ )
- Free tests for the detection of HIV. 1997update and development. Bulletinpidmiologique Hebdomadaire1999;(7): 25-7. [2 February. France]
- Importance of HIV subtypes to estimate
viral load. Kansanterveys1999; (2): 7.[February. Finland]
- HIV and AIDS, 4th quarter. Smittskydd1999; 5(1): 3-4.[January. Sweden]
- Picture of the month: decrease in AIDSdeaths in Western Europe in years1994-98. Kansanterveys1999; (1): 11.[January. Finland]
STREPTOCOCCUS- Surveillance of neonatal group B
streptococcal infection in Sunderland.Commun Dis Public Health1999;2(1): 64-5. [March. England and Wales]
TUBERCULOSE / TUBERCULOSIS- New system for enhanced surveillance
of tuberculosis in England and Wales.Commun Dis Rep CDR Wkly1999;9(10): 90. [5 March. England and Wales]
- New born babies exposed to smearpositive tuberculosis. Commun Dis RepCDR Wkly1999; 9(7): 57, 60.[12 February. England and Wales]
VACCINATION / IMMUNISATION- Measles, mumps, and rubella vaccine
coverage in 2 year old children in EastLancashire - better than it looks.Commun Dis Public Health1999;2(1): 50-3. [March. England and Wales]
- Vaccine-preventable and childhooddiseases. SCIEH Weekly Report1999;33 (8): 66-7.[23 February. Scotland]
- Diphtheria and tetanus vaccination.EPI-NEWS1999; (7).[17 February. Denmark]
- Rotavirus vaccine. EurosurveillanceWeekly1999; 3: 990211.(http:/ / www.eurosurv.org/ )
- National inquiry into the seroprevalenceof vaccine preventable diseases.Year 1996. Boletn EpidemiolgicoSemanal1998; 6(10): 93-100.[8 October 1998. Spain]
VOYAGE / TRAVEL- Year 1999 Finnish vaccination manual
and international travel and health.Kansanterveys1999; (2): 12.[February. Finland]
- The value of malaria self testsfor t ropical travel. InfectieziektenBulletin1999; 10(1): 10-3.[January. Netherlands]
BUL L ET I N S NAT I O NA UX - CONT ACT S / NATIONAL BULLETINS - CONTACTS