Embed Size (px)
Citation preview
FACULTE DE MÉDECINE ET DES SCIENCES DE LA SANTÉ — Department of Obstetrics and Gynecology— Sherbrooke, Québec, Canada
P17.07- Chorioangiomas with signs of fetal compromise on ultrasound evaluation: a case
series. Isabelle Hardy, MD1. Geneviève Bérubé, MD1. Evelyne Raiche, MD, FRCSC1. Marie-Ève Roy-Lacroix, MD, FRCSC1. Annie Ouellet, MD, FRCSC1. — 1: Obstetrics and
Gynecology division, Université de Sherbrooke.
INTRODUCTIONChorioangiomas (ChAs) are benign placental tumors that occur in around
0.6% of pregnancies (1). Giant ChAs, which are greater than 4cm in
diameter, can disrupt fetal circulation and pregnancies with this condition
are more likely to present growth restriction, fetal heart failure,
polyhydramnios, fetal anemia, premature delivery, and intra-uterine demise
(IUD) (2). When ChAs are diagnosed antenatally, close ultrasound
examination is recommended, but the optimal ultrasound management is
unknown (3).
We report our experience in the management of four cases of ChAs
diagnosed at our center between 2016 and 2019. All cases were diagnosed
at the routine second trimester scan and followed thereafter with serial
ultrasounds performed at least every two weeks to evaluate fetal growth,
and wellbeing, and systematic Doppler evaluation of the middle cerebral
artery peak systematic velocity (MCA PSV), ductus venosus (DV), and
umbilical artery (UA). The diagnoses of ChA were confirmed by placental
pathologic examination.
CASE 1•21+3 weeks: Diagnosis of 6.4x 5.3 cm ChA with polyhydramnios.
•27+6: Corticosteroids administered for increasing polyhydramnios.
•28+6: ChA increased up to 10.4x 8.0x 5.9 cm and amniotic fluid index
(AFI) to 38.7 cm with short cervical length of 13 mm. Normal Doppler of
the MCA PSV, UA, and DV.
•29+0: Amnioreduction of 1.5L performed for maternal discomfort.
•29+1: The patient entered preterm labor overnight and cesarean was
performed for footling presentation.
•Birth of a 1450g female, Apgar 5-7-8. Cord hemoglobin (Hgb) 99g/L.
The neonate was anemic but no transfusion was required.
•Diagnosed with grade 2 intraventricular hemorrhage, severe
bronchopulmonary dysplasia, and stage 1 retinopathy. Discharged from the
NICU without oxygen at day 54 of life.
CASE 2•22+2 weeks: 4.7x 1.9 cm ChA with normal AFI.
•28+2: ChA had grown to 8x 3.5cm with normal AFI and Doppler.
•32+4: Increase of the MCA PSV to 1.5 MoM with normal cardiac
function.
•32+5: Evaluation for cordocentesis: decision not to perform it because of
the advanced gestational age with stable MCA PSV at 1.6 MoM.
•32+6 : Corticosteroid administered. MCA PSV remained stable.
•Given the risk of fetal anemia delivery was scheduled at 34 weeks.
•34+2: Elective cesarean section.
• Birth of a 2530g male, Apgar 3-5-7. Cord Hgb 98g/L.
•No transfusion was required. Discharged home after 4 days.
CONCLUSIONIn pregnancies with giant ChA, the systematic serial evaluation of
fetal growth and wellbeing, amniotic fluid, MCA PSV, DV, and
UA Doppler can help determine the tipping point between the
risks of fetal distress in utero and the risks of iatrogenic
prematurity in order to optimize neonatal outcomes.
CASE 3•23+ 6 weeks: 42.6 mm ChA with high vascularization, normal AFI.
•31+0: ChA had grown to 8.7 cm with polyhydramnios up to 25. 2 cm AFI.
Normal ACM PSV, DV, UA. Cardiac hyperdynamism noted without
cardiac failure.
•32+0: Increase of MCA PSV to 1.53 MoM: admission and administration
of corticosteroids.
•32+1: De novo reversed cerebroplacental ratio and umbilical vein (UV)
pulsatility.
•32+1: Emergency cesarean for abnormal fetal wellbeing.
• Birth of a 1785g male, Apgar 4-6-9. Cord Hgb 134 g/L.
•No transfusion was required. Discharged home after 36 days without
respiratory or neurological sequelae.
CASE 4•20+6 weeks: 3.7x 2.7x 3.85 ChA near cord insertion with large nourishing
vessel, normal AFI.
•MCA PSV remained normal throughout pregnancy.
•34+1: Maximal growth of the ChA at 8.3 cm, normal AFI.
•30+0 -34+6: Deeper DV A wave and on and off pulsatility of the UV.
•30, 33+6, and 35+4: Normal fetal cardiac ultrasounds.
•The couple was counseled on the pros and cons of expectant management
and preferred to deliver as late as possible.
•35+4: Delivered by elective cesarean section.
•Birth of a 2600g female, Apgar 8-8. Cord Hgb 114 g/L.
•No transfusion was required. Discharged home after 2 days.
REFERENCES1.Guschmann M, Henrich W, Entezami M, Dudenhausen JW. Chorioangioma--new insights into a
well-known problem. I. Results of a clinical and morphological study of 136 cases. J Perinat Med.
2003;31(2):163-9.
2. Al Wattar BH, Hillman SC, Marton T, Foster K, Kilby MD. Placenta chorioangioma: a rare case
and systematic review of literature. J Matern-Fetal Neonatal Med Off J Eur Assoc Perinat Med Fed
Asia Ocean Perinat Soc Int Soc Perinat Obstet. juill 2014;27(10):1055-63.
3. Abdalla N, Piórkowski R, Stanirowski P, Pazura M, Cendrowski K, Sawicki W. Can ultrasound be
helpful in selecting optimal management methods for pregnancies complicated by placental non-
trophoblastic tumors? J Ultrason. juin 2017;17(69):116-22.
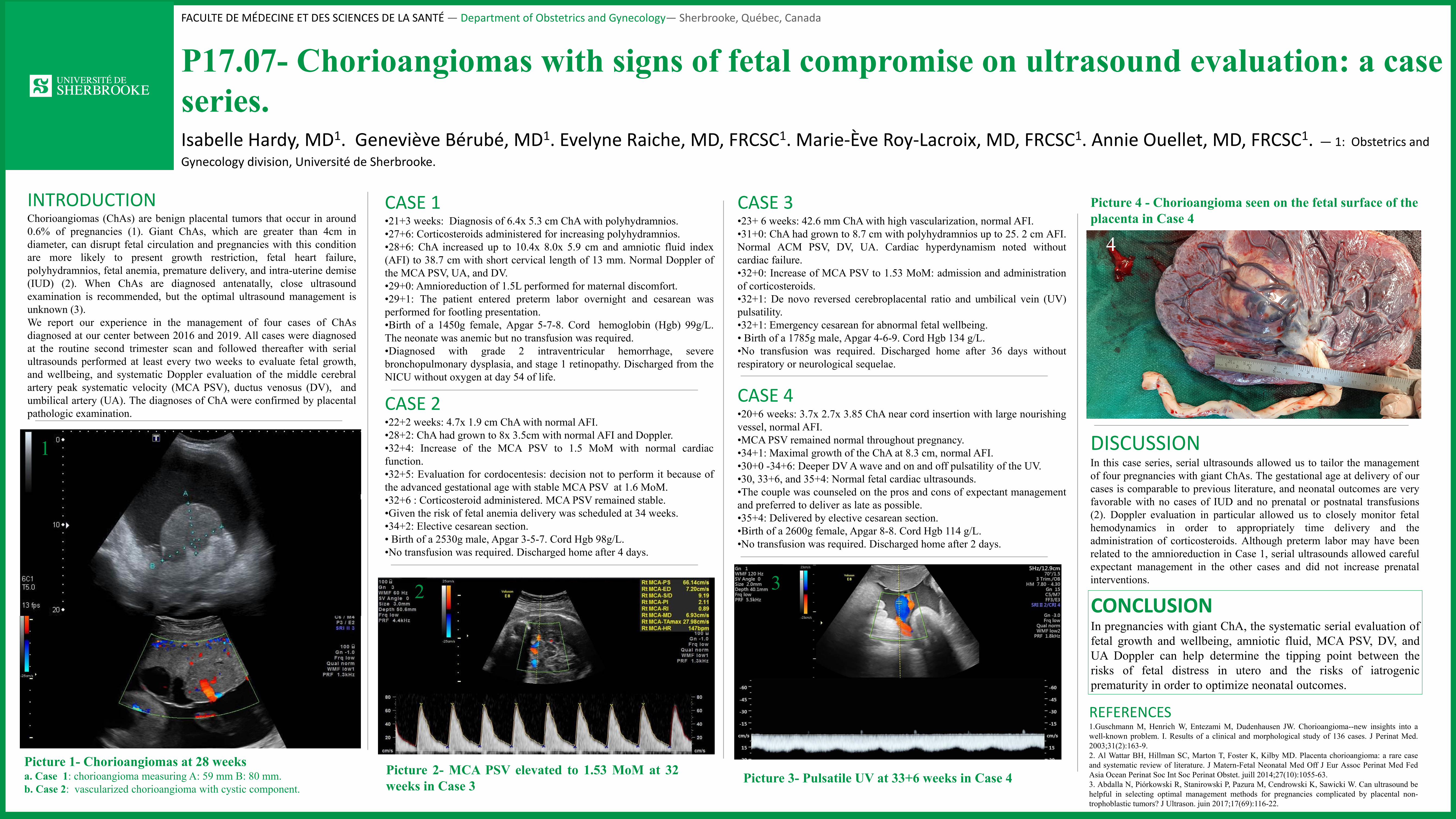
Picture 4 - Chorioangioma seen on the fetal surface of the
placenta in Case 4
DISCUSSIONIn this case series, serial ultrasounds allowed us to tailor the management
of four pregnancies with giant ChAs. The gestational age at delivery of our
cases is comparable to previous literature, and neonatal outcomes are very
favorable with no cases of IUD and no prenatal or postnatal transfusions
(2). Doppler evaluation in particular allowed us to closely monitor fetal
hemodynamics in order to appropriately time delivery and the
administration of corticosteroids. Although preterm labor may have been
related to the amnioreduction in Case 1, serial ultrasounds allowed careful
expectant management in the other cases and did not increase prenatal
interventions.
a.
b.
1
2 3
4
Picture 1- Chorioangiomas at 28 weeksa. Case 1: chorioangioma measuring A: 59 mm B: 80 mm.
b. Case 2: vascularized chorioangioma with cystic component.Picture 3- Pulsatile UV at 33+6 weeks in Case 4
Picture 2- MCA PSV elevated to 1.53 MoM at 32
weeks in Case 3





























