-
Atypical Atrial Flutter
Frédéric Anselme
CHU de Rouen
DIU Rythmologie 2020
-
Définition
• Flutter auriculaire : Tachycardie auriculaire régulière, >
240/min, avec absence de retour à la ligne isoélectrique entre 2
déflections auriculaires dans au moins 1 dérivation ECG.
Mécanisme : macro-réentrée auriculaire
• Atypique : dont le circuit de réentrée ne dépend pas de
l’isthme cavo-tricuspide.
En Pratique
• ECG ECG de flutter typique
• Diagnostic établi par la cartographie
-
• Plus rares que le flutter typique
• Patients avec cardiopathie
• Association fréquente avec AC/FA
• Post ablation de FA ++
• Localisation auriculaire droite ou gauche
Flutters Auriculaires Atypiques
Circuits de macro-réentrée
• Autour d’obstacles anatomiques (ostia, anneau mitral, Crista
terminalis, sinus coronaire)
• Autour de cicatrices chirurgicales ou de patchs
• Autour de zones inexcitables (cardiopathies)
-
Moyens d’investigation
• Cathéters multipolaires et cartographie utilisant la technique
de l’entraînement
• Systèmes de cartographie tridimensionnelle- Carto, NavX,
Rhythmia …
-
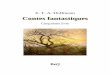
Technique de l’entraînement
t Cycle = xCycle de retour
=cycle tachyc. + 2t
P stim. P tachyc.
I
CS-P
Isthm
Halo-D
Halo-M
Halo-P
II
III
aVR
V1
V6
380380 420 420
Cycle = x
Cycle = x
Cycle de retour =
cycle tachyc.
P stim. P tachyc.
Cycle de retour =
cycle tachyc.
P stim. = P tachyc.
-
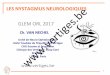
• I- Les FlA isthmiques dépendants à ECG atypique
- Flutter isthm. dépendant, à rot. anti-horaire, à ECG
atypique
- Flutter isthm. dépendant à rot. horaire
• II- Les tachycardies atriales focales avec aspect ECG de
flutter atypique
• III- Les FlA atypiques
-
I
II
III
aVL
aVF
V1V2
V3
V4
V5
aVR
V6
II
III
V1
Isthm.
H1H2
H3H4
H5H6
H7H8
H9H10
H11H12
H13H14
Flutter Auriculaire AtypiqueÀ ECG de Flutter Typique
-
• I- Les FlA isthmiques dépendants à ECG atypique
• II- Les tachycardies atriales focales avec aspect ECG de
flutter atypique
• III-Les FlA atypiques
-
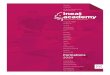
Tachycardie Atriale Focale Avec Aspect ECG de Flutter A.
Atypique
I
II
III
aVr
aVlaVf
V1
V2
V3
V4
V5
V6
Aspect ECG ne préjuge pas
du mécanisme de l’arythmie
-
• I- Les FlA isthmiques dépendants à ECG atypique
• II- Les tachycardies atriales focales avec aspect ECG de
flutter atypique
• III-Les FlA atypiques
- Macro-réentrée auriculaire droite non incisionelle -
Macro-réentrée auriculaire droite incisionelle- Macro-réentrée
auriculaire gauche- Macro-réentrée utilisant la musculature du
SC
-
Flutter par Réentrée SupérieureIntra-Auriculaire Droite
CT
FO
SC
IVC
SVC
AT
ER
-
Flutter par Réentrée SupérieureIntra-Auriculaire Droite
- Patients sans ATCD de chir. Card.
- Incidence faible (8/150 pts avec ECG de flutter typique ou
atypique)
- Ablation au niveau du gap de conduction dans la Crista
Terminalis
Ching-Tai T et al, JACC 2002;40:746Incidence OPD
-
I
II
III
aVr
aVl
aVf
V1
V2
V3V4
V5V6
Flutter Auriculaire Post-Atriotomie
-
Flutter Auriculaire Post-Atriotomie
-
Double Réentrée auriculaire droite- 10/21pts souffrants de
Flutter après correction chir. de CIA
- Atriotomie antérieure et incomplète vers la VCI
Shah DP et al, Circulation 2000 15;101:631
-
Flutters Auriculaires Gauches
Jais P, et al, Circulation 2000;101:2928P + en V1
-
When should we consider LA Flutter ?
• ECG: Predominantly positive F wave in V1
Low voltage F Waves in inferior leads
In all pt with an ECG not characteristic of typical atrial
flutter
• Presence of hemodynamically significant left HD
• History of open heart surgery
• History of AFib ablation procedure
• Entrainment mapping excluding RA during EP study
Bochoeyer, Yang et Al. Circulation. 2003;108:6
Diagnosis is not a problem
-
Jaïs et Al:
Circulation 2000,
101: 2928
Various Types of LA CircuitsIn absence of prior LA « surgery
»
• Low incidence
• Conventional entrainment mapping , look for fractionated
egm
• 3D mapping systems +++
• Electrically silent areas in 50% of the pts
• Multiple circuits bounded by anatomical structures and scar
zones
-
Ablation of « spontaneous » LA FlutterThe Bordeaux
experience
• N= 22 pts
• 1, 2, 3 sessions in 14, 7, and 1 patients respectively
• Cumulative procedure time: 339±113 min
• Cumulative fluo. time: 95±42 min
Jaïs et Al: Circulation 2000, 101: 2928
• Incomplete map in 5/22 pts
• 1 pt with reversible stroke
• Acute success (SR): 20/22 pts
• Mid term FU: Permanent Afib in 1, atypical AF in 5 pts
(23%)
-
Ablation of LA FlutterThe Hamburg experience
• 28 pts
• Critical isthmus identification in 89% during AFl
• Isthmus identification in SR in 2 pts
• Isthmus width: 12±6mm
• AFl termination in 23 pts
• PT: 384±145 min
• FT: 18.4±8.8 min
Ouyang F, et al. Circulation 2002;105:1934
-
Validation of isthmus conduction blockduring SR or pacing
• LA flutter recurrences in 3/28 pts (11%)
• No recurrences if validated isthmus conduction block
• Afib in 6/28 (21%) at a median FU of 14 months
Ouyang F, et al.
Circulation
2002;105:1934
-
Septal LA flutter In absence of prior LA « surgery »
Marrouche n, et Al: Circulation 2004, 109: 2440• High amplitude
in V1
• Flat in inferior leads
-
Left Septal Flutter Ablation
• SP-MA isthmus ablation more efficient than that of SP-RPV
isthmus
• Acute success in 10/11 pts
• Recurrences in 2/11 pts
• Afib in 2/11 pts
Marrouche n, et Al: Circulation 2004, 109: 2440
-
Organized Arrhythmia post-AFib Ablation
• Incidence ~ 8% after AFib ablation (1.2-21%)
higher if linear lesions applied during the index procedure
• PV tachycardia with LA reconnection
• Reentry at gaps within the ablation line
• Macro-reentry bounded by PVs and scar zones
• Localized LA reentry
Jais P, et al. JCE 2006;17:279
-
Correlation ECG/Mechanism• Continuous electrical activity in
at
least 1 ECG lead• Lack of continuous electrical
activity in all ECG leads
III
III
aVL
aVF
V1
V2
V3
V4
V5
V6
aVR
III
III
aVL
aVF
V1
V2
V3
V4
V5
V6
aVR
Atrial Tachycardia Atrial Flutter
Focus
Macro-reentry
In patients with prior Afib ablation, LAMRT should always be
considered whatever the ECG pattern
-
Stepwise Approach to Diagnose Post Afib AT
• 1- Assessment of AT CL stability with a decapolar CS
catheter:
- CS activation sequence
- TCL variability > 15% suggests focal AT
• 2- Exclude typical flutter using IVC-TA isthmus entrainment
maneuvers
I
II
III
aVL
aVF
V1
V2
V3
V4
V5
aVR
V6
II
III
V1
Isthm.
H1H2
H3H4
H5H6
H7H8
H9H10
H11H12
H13H14
-
• 3- Exclude PV dependent AT by checking PV isolation with a
lasso cath.
Stepwise Approach to Diagnose Post Afib AT
RSPV Mapping RSPV Isolation
-
• 4- Diagnosis of macroreentry circuits :
Stepwise Approach to Diagnose Post Afib AT
* **
• 2 possible isthmuses:
- LA roof
- Mitral isthmus
-
• 4- Diagnosis of macroreentry circuits :
Stepwise Approach to Diagnose Post Afib AT
• Activation mapping with
a roving catheter•Both ant and post walls
activated in the same direction
excludes roof dependent
macroreentry
• Entrainment maneuvers
at opposite LA walls:
- MI & septal
- post & ant •PPI>TCL+30 ms at one of the
opposite walls excludes
perimitral or roof dependent
macroreentry respectively
Reference potential at the CS
****
-
Musculature du Sinus Coronaire Arythmogène
Olgin JE, et al. JCE 1998;9:1094
Macro-réentrée utilisant la musc. du SC
-
Schéma du Flutter Auriculaire Atypiquedépendant de la
musculature du sinus coronaire
Olgin JE, et al. JCE 1998;9:1094
Site d’ablation
-
Long term outcome after LA Flutter Ablation
• Up to 20% of LA Flutter recurrences
less if validated isthmus conduction block
• High incidence of AFib likely due to the progression of the
underlying heart disease
-
Baseline ECGClinical Case #1
-
CS Mapping at Start
-
LA Roof Entrainment
PPI = TCL + 100 msec
-
LA Septal Entrainment
PPI = TCL
-
MI Entrainment
PPI = TCL
-
Question # 1• LA roof is not part of the tachycardia circuit
• Result of MI entrainment is sufficient enough to diagnose
perimitral macrorentry
• Result of MI entrainment is sufficient enough to perform MI
ablation
Roof entrainment
MI entrainment
-
Tachycardia termination during MI ablation
Answer # 1• LA roof is not part of the tachycardia circuit:
PPI>>> TCL
• Result of MI entrainment is sufficient enough to diagnose
perimitral macrorentry
• Result of MI entrainment is sufficient enough to perform MI
ablation
- Both LA septal and MI
entrainment are required to
diagnose perimitral flutter.
Other macroreentries
utilizing MI are possible
- As soon as the MI is
recognized as part of the
tachycardia circuit, MI
ablation can be perform
-
LAA Pacing
-
Question # 2
• I pace the lateral part of the MI line to confirm clockwise MI
block
• I pace the CS to confirm counterclockwise MI block
• There is complete MI block, I stop the ablation procedure
• There is still residual MI conduction
LAA pacing
-
Answer # 2
• I pace the lateral part of the MI line to confirm clockwise MI
block
• I pace the CS to confirm counterclockwise MI block
• There is complete MI block, I stop the ablation procedure
• There is still residual MI conduction
LAA pacing
CS activation is from distal to proximal which identifies
residual MI conduction
-
**
During MI ablation
-
dCS Pacing at septal side of the MI line
*****
Abl Cath on MI line
Wide double potentials recorded at MI line
identifying counterclockwise MI block
**
* * * *
-
Baseline ECGClinical Case #2
-
CS Mapping at Start
-
Question # 3
• CS activation is typical of perimitral macroreentry and I
start ablating the MI?
• CS electrograms reflect LA and CS musculature activation ?
• I ablate within the CS to disconnect CS musculature ?
• I perform activation mapping with the LA?
• I perform entrainment at IVC-TA isthmus ?
-
Answer # 3
• CS activation is typical of perimitral
macroreentry and I start ablating the MI?
• CS electrograms reflect LA and CS musculature
activation ?
• I ablate within the CS to disconnect CS
musculature ?
• I perform activation mapping with the LA?
• I perform entrainment at IVC-TA isthmus ?
-CS is activated almost synchronously, which does not suggest
perimitral
macroreentry
-Always best to understand tachycardia mechanism before
ablation
-It is worth to do IVC-TA entrainment to exclude typical flutter
even if the surface
ECG and the CS activation are not suggestive. Prior extensive
LA/RA ablation (CS
os) may modify the usual typical flutter ECG pattern and atrial
activation
-
MI Entrainment
LA Roof Entrainment
-
Question # 4• MI entrainment suggest MI dependent
macroreentry
• LA roof entrainment suggest roof dependent macroreentry
• I cannot conclude and I perform anterior and posterior
activation mapping
• I proceed to roof line ablation
• I perform LA septal entrainment
MI Entrainment
LA Roof Entrainment
-
Answer # 4
• MI entrainment suggest MI dependent macroreentry
• LA roof entrainment suggest roof dependent macroreentry
• I cannot conclude and I perform anterior and posterior
activation mapping
• I proceed to do roof line ablation
• I perform LA septal entrainment
-Long PPI excludes MI from the tachycardia circuit
-LA septal entrainment is not mandatory, result from LA roof
entrainment is enough to proceed to do roof line ablation
MI Entrainment
PPI>TCL+30 msec
-
CS Mapping after Roof Line Ablation
-
Question # 5• The macroreentry was not LA roof dependent
• Conduction gap within the roof line cannot be excluded
• CS 7-8 shows continuous fragmented atrial electrograms
covering more than 70% of the TCL supporting ablation at that
site
• I perform MI and/or LA septal entrainment
• I do activation mapping around the mitral annulus
-
Answer # 5• The macroreentry was not LA roof dependent
• Conduction gap within the roof line cannot be excluded
• CS 7-8 shows continuous fragmented atrial electrograms
covering more than 70% of the TCL supporting ablation at that
site
• I perform MI and/or LA septal entrainment
• I do activation mapping around the mitral annulus
-TCL prolongation suggests the tachycardia was LA roof
dependent
-Even if CS activation sequence is modified, LA roof line
conduction gap can not be excluded
-Intermittent block within CS fragmented potentials suggests
dead end pathway
-
MI Entrainment
PPI = TCL + 20 msec : this site is part of the tachy circuit
-
During Endocardial MI Ablation
-
Question # 6
• There is block at the MI
• I check the roof line
• I perform MI entrainment
• I perform LA septal entrainment
• I look for a focal atrial tachycardia
-
Answer # 6• There is block at the MI
• I check the roof line
• I perform MI entrainment
• I perform LA septal entrainment
• I look for a focal atrial tachycardia
- Identical CS activation sequence suggests residual conduction
MI
- Need to map the epicardial side of the MI
-
dCS Entrainment
PPI=TCL: Epicardial MI ablation is performed
-
After Epicardial MI Ablation
Prolongation of the TCL (468 to 492 msec)
Modification of the CS activation sequence
-
Question # 7
• There is complete block at the MI
• I perform IVC-TA entrainment
• I perform MI entrainment
• I perform LA septal entrainment
• I look for a focal atrial tachycardia
-
Answer # 7
• There is complete block at the MI
• I perform IVC-TA entrainment
• I perform MI entrainment
• I perform LA septal entrainment
• I look for a focal atrial tachycardia
-Change of CS activation sequence and TCL prolongation suggest
tachycardia
circuit does not depend on MI anymore
-However, residual MI conduction cannot be excluded
-Because of the CS activation sequence (pCS dCS) IVC-TA and LA
septal
entrainment are useful to exclude RA or septal macroreentry
-
Mapping with the Lasso Catheter between LAA and LPVs
-
Question # 8
• Electrograms recorded at the lasso catheter are far field
potentials from both LAA and PVs
• Lasso 15-16 electrograms may reflect localized reentry
• I perform entrainment maneuvers at Lasso 15-16
• I perform entrainment maneuvers at dAbl
• I move the Lasso catheter to another area
-
Answer # 8• Electrograms recorded at the lasso catheter are far
field
potentials from both LAA and PVs
• Lasso 15-16 electrograms may reflect localized reentry
• I perform entrainment maneuvers at Lasso 15-16
• I perform entrainment maneuvers at dAbl
• I move the Lasso catheter to another area
-
SR Restoration during RF Ablation
- Lasso has been moved towards LAA
- Ablation performed at site where the lasso
15-16 electrodes had been positioned