Embed Size (px)
DESCRIPTION
IL FAUT METTRE EN HYPOTHERMIE TOUS LES ARR ÊTS CARDIAQUES RECUPERES. Julie casoetto; Mattéo Miquet Des Anesthésie-Réanimation. Saint-Etienne Desc Réanimation médicale Grenoble Mai 2006. Physiopathologie. La diminution de 1° c abaisse de 7% la consommation de glucose et d’O2. - PowerPoint PPT Presentation
Citation preview

IL FAUT METTRE EN HYPOTHERMIE TOUS LES
ARRÊTS CARDIAQUES RECUPERES
Julie casoetto; Mattéo Miquet
Des Anesthésie-Réanimation. Saint-Etienne
Desc Réanimation médicale Grenoble Mai 2006

Physiopathologie
La diminution de 1°c abaisse de 7% la consommation de glucose et d’O2
L’hypothermie diminue l’apoptose :
- inhibition de la caspase
- amélioration du fonctionnement mitochondriale
- inhibition de la cascade neuroexitatrice

Ischémie
Pompe Na-K ATPase
Efflux de NA et afflux de Ca++
glutamate
Afflux de Ca++
hypothermie

Ischémie-reperfusion
TNFalpha IL-1
Activation leucocytaire
Phagocytose et enzymes cytotoxiques
Dommages cellulaires
hypothermie

Ischémie- reperfusion
Radicaux libres
Péroxydation (lipidique, proteique..)
Mort cellulaire
hypothermie

Ischémie
Altération de la barrière hémato-encéphalique
Œdème cérébral
Mort cellulaire
hypothermie

Ischémie - reperfusion
Altération membranaire
Acidose intracellulaire
Processus de destruction
hypothermie

Important : ces perturbations perdurent >48H
Intérêt majeur d’une thérapeutique précoce
Physiopathologie

Certaine région du cerveau ont une température 2 à 3° > température corporelle
L’hypothermie permet d’assurer au moins la normothermie à l’ensemble du cerveau
Thermo dispersion

Hypothermie vs normothermie
• 2 Etudes multicentriques randomisées controlées en simple aveugle
• Hypothermie modérée entre 32-34°C pendant 12-24h
• Arrêt cardio-circulatoire chez l’adulte : – Avec rythme initial de FV ou TV– Arrivée des 1ers secours entre 5 et 15 min– Durée du collapsus<60 min– Etat comateux persistant– Exclusion des états de choc (PAS<90
mmHg,PAM<60mmHg) et hypoxie sévère (SpO2<85%)– Exclusion des comas d’autres étiologies
• Pronostic neurologique (catégories de performance cérébrale)

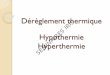
Treatement of comatose survivors of out-of-hospital cardiac arrest with
induced hypothermia
• 4 centres à Melbourne de Sept 1996 à Juin 1999
• 77 patients• Hypothermie précoce dès le transport
en ambulance avec température cible de 33° pendant 12h via pack de glace
• 1er Critère : survie avec bon devenir neurologique (normal ou incapacité minime ou modérée)
Bernard et al NEJM 2002

49% 26%
P=0,046
OR 5,2595% IC 1,47-18,76P=0,011
Défaillance cardiaque 5 4
Mort cérébrale 1 1
Bernard et al NEJM 2002

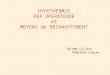
Mild therapeutic hypothermia to improve the neurologic outcome
after cardiac arrest• 9 centres 5 pays européens 275 patients
de Mars 1996-Juillet 2000• Hypothermie instaurée plus tardivement
(105 min) entre 32-34°C pendant 24h via air pulsé puis réchauffement passif
• Critères : – Devenir neurologique favorable à 6 mois
(catégories de performance cérébrale de Pittsburgh)
– Taux de mortalité à 6 mois– Taux de complications les 7 1ers jours
(infections, TdR…)
Hypothermia after Cardiac Arrest Study Group.NEJM 2002

Hypothermia after Cardiac Arrest Study Group.NEJM 2002
Il faut traiter 6 patients pour prévenir 1 mauvaise évolution neurologiqueIl faut traiter 7 patients pour prévenir 1 décès


Prévention des effets secondaires
• Effets cardiovasculaires– Arythmies : Monitorage thermique+++– Hypotension : remplissage, amines
• Infections : – ↑ si hypothermie>48-72h, – = si Hypothermie < 24h
Schwab Stroke 2001 vs Hypothermia after Cardiac Arrest Study Group.NEJM 2002
• Coagulopathie : Pool plaquettaire, PFC si gestes• Hyperglycémie, insulinorésistance
Van den Berghe NEJM 2001
• Hypo Ph, hypo K, hypo Mg• Frissons ↑VO2 de 40 à 100%
Sédation, opiacés, curares
Correction tbles métaboliques

From evidence to clinical practice: effective implementation of therapeutic hypothermia to
improve patient outcome after cardiac arrest
• Etude rétrospective • 109 patients aucun critère d’exclusion• Hypothermie 33°C pendant 24h vs
normothermie• Résultats :
- Patients FV, TV : 86 patientsBon pronostic neuro : 55,8% vs 25,6% p=0,004Etat de choc (31 patients) : 29,4% vs 0% p=0,027
- Asystolie : décès 20/23 Oddo Crit Care Med 2006

Conclusion
I) Guidelines européens : «The new guidelines recommend that this cooling treatement (therapeutic hypothermia) is used for some patients admitted to intensive care units after cardiac arrest. » Oxford, 25 novembre 2005; European Resuscitation Council
II) Guidelines américains : « cardiac arrest should be cooled to 32°C to 34°C for 12 to 24 hours when the initial rhythm was VF. Cooling to 32°C to 34°C for 12 to 24 hours may be considered for cardiac arrest from any other rhythm . »
Circulation 2005


Bibliographie
Povlishock JT, 1999. Acta Neurochir Suppl.
Xu L, 2002. J Cereb Blood Flow Metab.
Adachi M, 2001. Pedriatr Res.
Ning XH, 2002. J Appl Physiol.
Auer RN, 2001. Ann NY Acad Sci.
Busto R, 1987. J Cereb Blood Flow Metab.
Winfree CJ, 1996. Neurosurgery.
Globus MY-T, 1995. J Neurochem.
Baker AJ, 1991. Stroke.
Busto R, 1989. Stoke.

Dempsey RJ, 1987. Neurosurgery.
Kaibara T, 1999. J Neurosurg.
Dietrich WD, 1996. Adv Neurol.
Negrovsky VA, 1988. Crit Care Med.
Natale JA, 1989. Stoke.
Kimura A, 2002. Crit Care Med.
Aibiki M, 1999. J Neurotrauma.
Huang ZG, 1999. Can J Neuro Sci.
Chi OZ, 2001. Anesthesiology.
Jurkovich GJ, 1988. J Surg Res.

Kinishita K, 2002. J Neurosurg.
Ghajar J, 2000. Lancet.
Reinert MM, 1999. Neurol Res.
Morimoto Y, 1993. Crit Care Med.
Fischer S, 1999. Brain Res Mol.
Ding D, 2000. Exp Neurol.
Chopp M, 1989. J Cereb Blood Flow Metab.
Mellergard P, 1991. Neurosurgery.
Schwab S, 1997. Neurology.
Verlooy J, 1995. Acta Neurochir.
Kilpatrick MM, 2000. Neurosurgery.
Lanier WL, 1995. J Neurosurg Anesthesio.
Soukup J, 2002. Neurol Res.
Kimura T, 2002. Exp Brain Res.

• Bernard SA, Gray TW, Buist MD, et al. Treatment of comatose survivors of out-of-hospital cardiac arrest with induced hypothermia. N Engl J Med 2002; 346: 557-563.
• Hypothermia after Cardiac Arrest Study Group. Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. N Engl J Med 2002; 346: 549-556
• Bernard SA, Buist MD, Monteiro O, Smith K. Induced hypothermia using large volume, ice-cold intravenous fluid in comatose survivors of out-of-hospital cardiac arrest: a preliminary report. Resuscitation 2003; 56: 9-13
• Bernard SA. Outcome from prehospital cardiac arrest in Melbourne, Australia. Emerg Med 1998; 10: 25-29.
• Seetha Shankaran Whole-Body Hypothermia for Neonates with Hypoxic–Ischemic Encephalopathy ,N Engl J Med 2005;353:1574-84
• Gluckman Selective head cooling with mild systemic hypothermia after neonatal encephalopathy: multicentre randomised trial, Lancet 2005:365;663-670
• Schwab Stroke 2001 • Van den Berghe NEJM 2001• Said Hachimi-Idrissi *, Mild hypothermia induced by a helmet device: a clinical feasibility study
Resuscitation 51 (2001) 275–281• Clifton et al.,Lack of effect of induction of hypothermia after acute brain injury,N Eng J Med
February 2001:344(8);556-563• Polderman et al , Induction of hypothermia in patients with various types of neurologic injury
with use of large volumes of ice-cold intravenous fluid,Crit Care Med 2005:33(12);2744-2751• Oddo et al, From evidence to clinical practice: effective implementation of therapeutic
hypothermia to improve patient outcome after cardiac arrest,Crit Care Med 2006• Therapeutic hypothermia after cardiac arrest : now a standard of care, Crit Care Med
2006(34);923-924