Embed Size (px)
DESCRIPTION
Imagerie de Diffusion Organes Mobiles et Corps Entier. Alain Luciani , Frederic Pigneur , Emmanuel Itti , Alain Rahmouni CHU Henri Mondor, Universite Paris Est Creteil [email protected]. Imagerie Diffusion Corps entier – WB-DWI. Couverture anatomique . Imagerie Fonctionnelle. - PowerPoint PPT Presentation
Citation preview
Imagerie de Diffusion Organes Mobiles et Corps Entier
Alain Luciani, Frederic Pigneur, Emmanuel Itti, Alain Rahmouni
CHU Henri Mondor, Universite Paris Est [email protected]
« Tout en un »
Imagerie Fonctionnelle
Couverture anatomique
Imagerie Diffusion Corps entier – WB-DWI
Comment je fais ?
Applications Cliniques
Antennes
DWI-MRI• Pré-requis technologiques et instrumentaux
Séquences
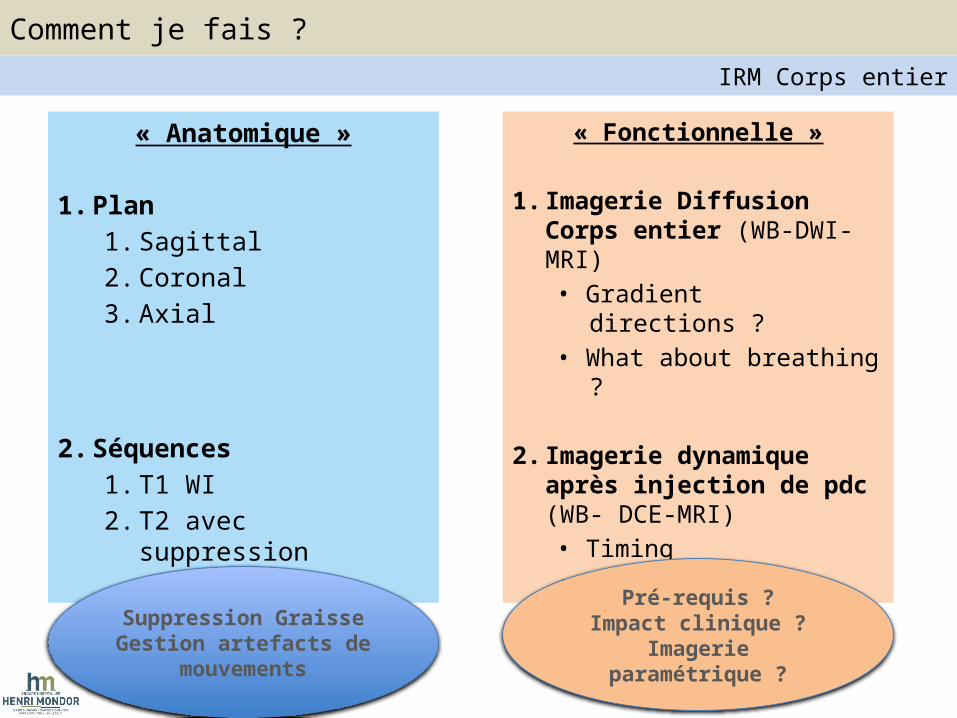
« Anatomique »
1. Plan1. Sagittal2. Coronal3. Axial
2. Séquences1. T1 WI2. T2 avec suppression
graisse
« Fonctionnelle »
1. Imagerie Diffusion Corps entier (WB-DWI-MRI)• Gradient directions ?• What about breathing ?
2. Imagerie dynamique après injection de pdc (WB- DCE-MRI)• Timing• Plans de coupes
Suppression GraisseGestion artefacts de
mouvements
Pré-requis ?Impact clinique ?
Imagerie paramétrique ?
Comment je fais ?IRM Corps entier
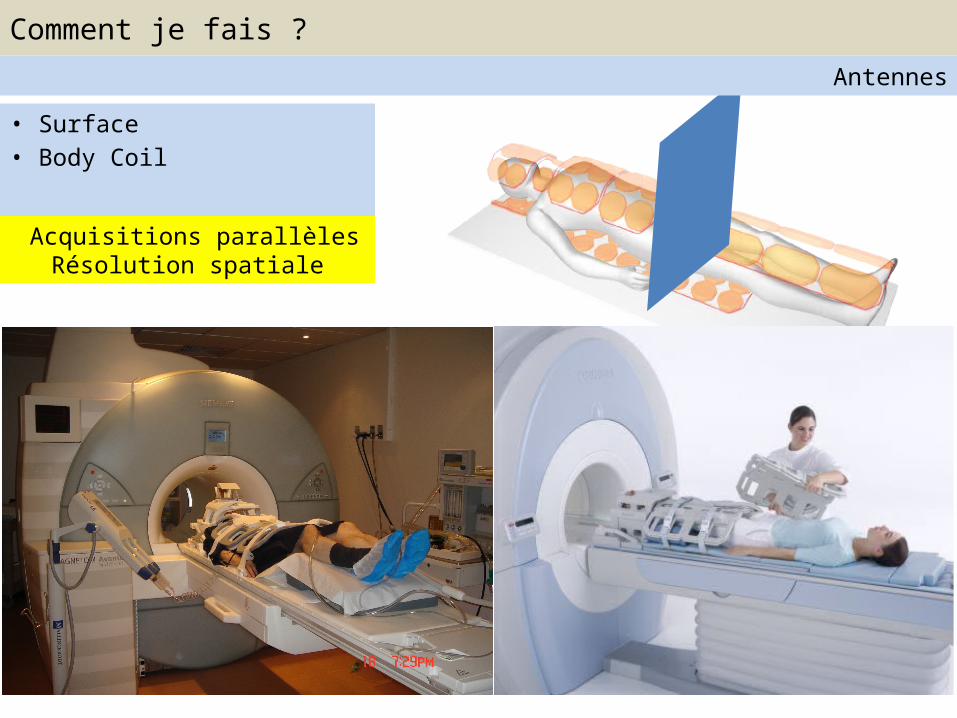
• Surface• Body Coil
Acquisitions parallèlesRésolution spatiale
Comment je fais ?Antennes
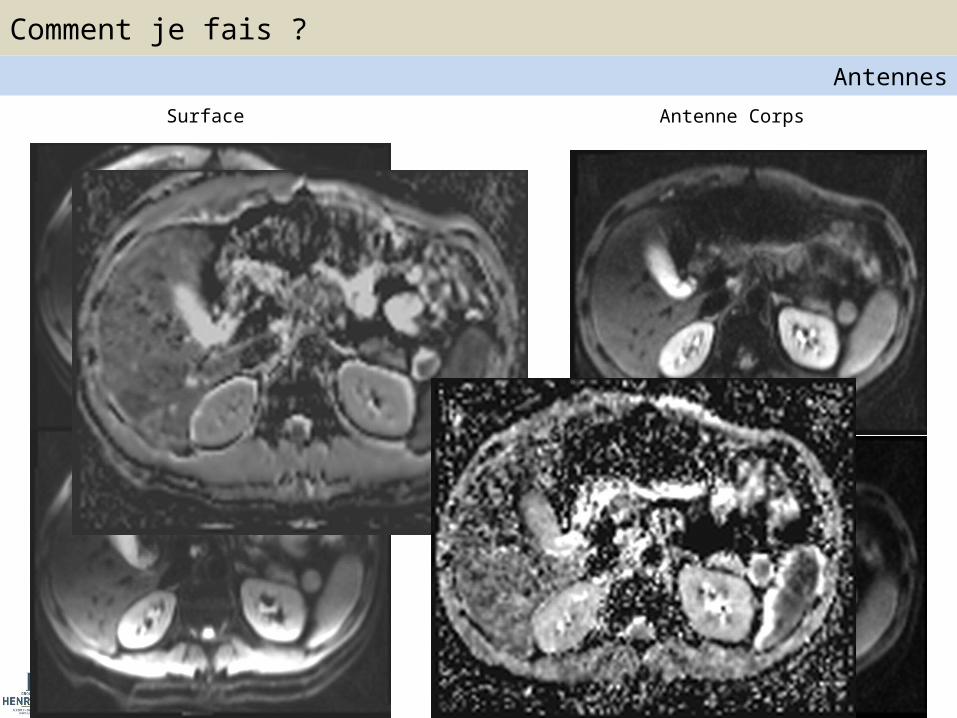
Surface Antenne Corps
Comment je fais ?Antennes
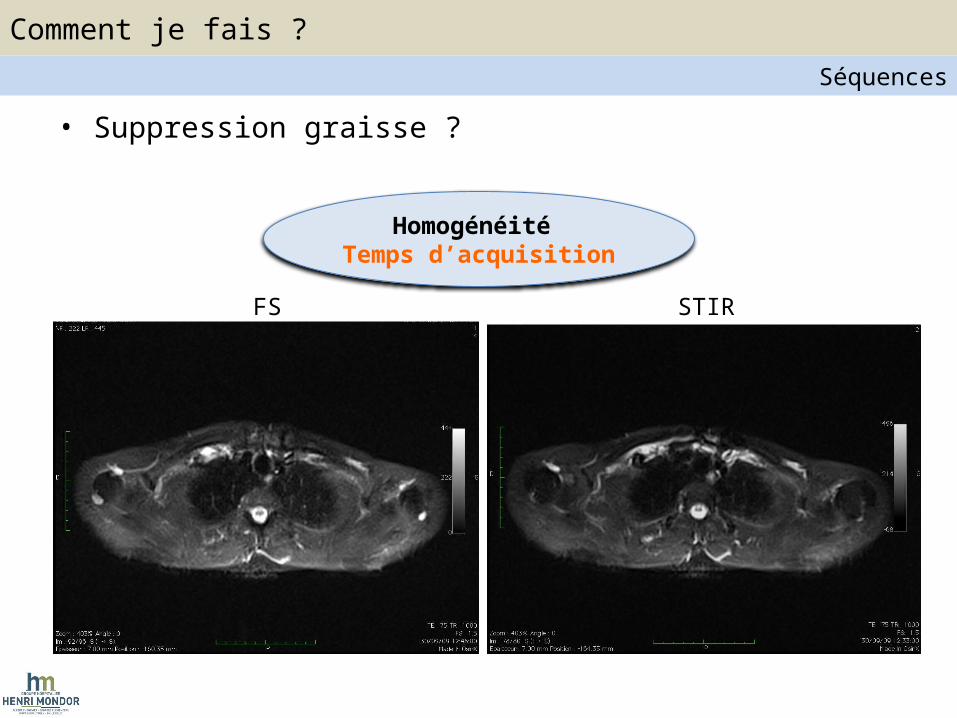
• Suppression graisse ?
FS STIR
Homogénéité Temps d’acquisition
Comment je fais ?Séquences
• Respiration – Libre + multiple Nex– Gating : Ceinture (pressure sensor)• Cycle respiratoire• Fin d’expiration => Acquisition
– Trigger :
Comment je fais ?Séquences
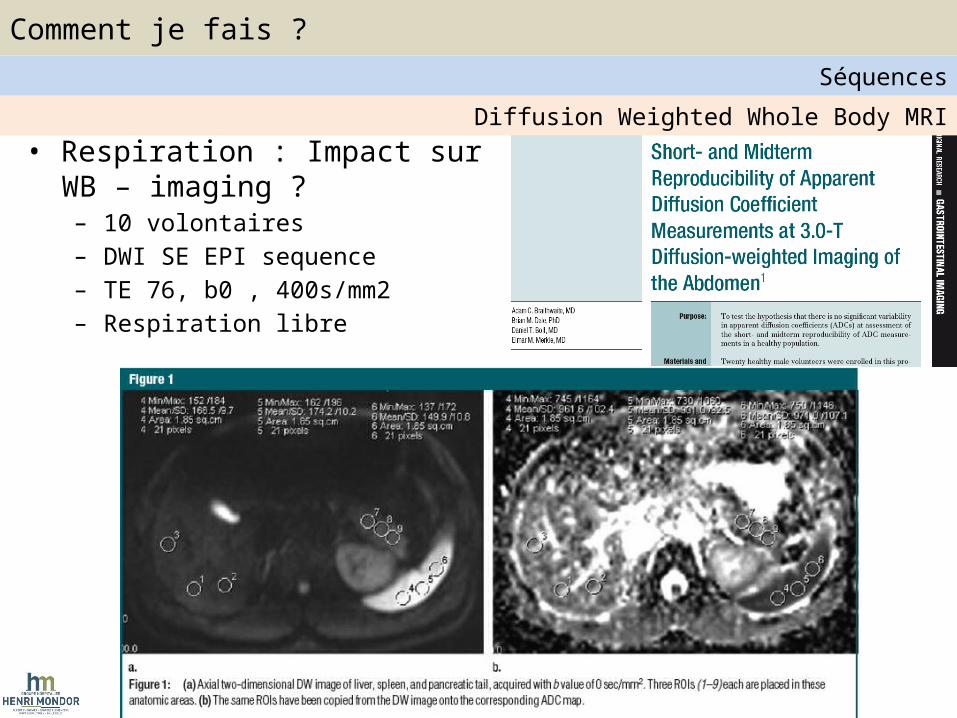
• Respiration : Impact sur WB – imaging ?– 10 volontaires – DWI SE EPI sequence– TE 76, b0 , 400s/mm2– Respiration libre
Diffusion Weighted Whole Body MRI
Comment je fais ?Séquences
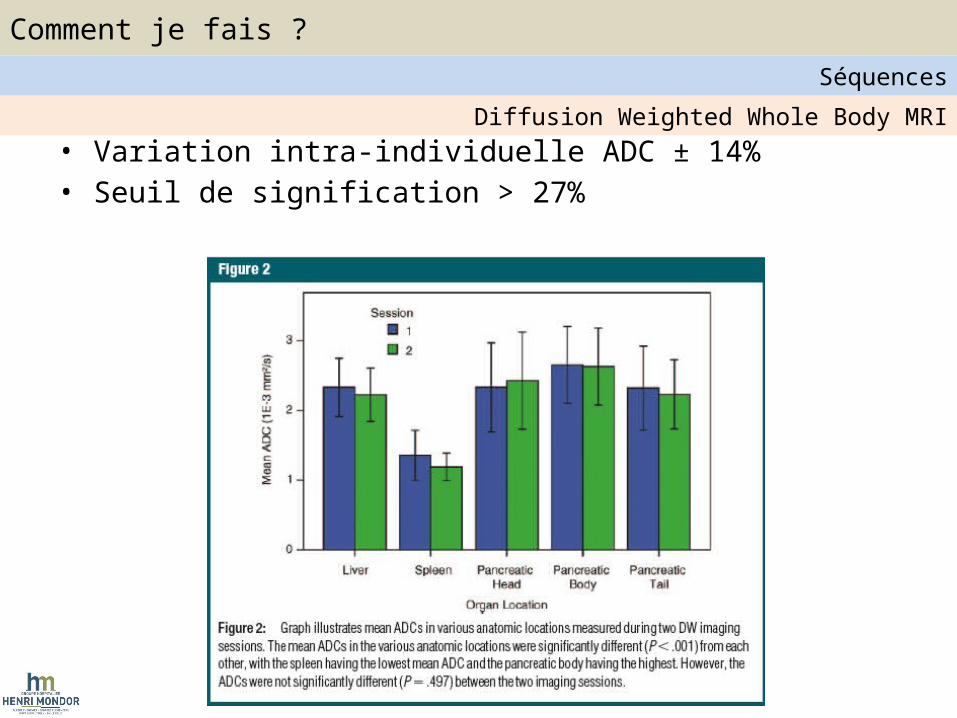
• Variation intra-individuelle ADC ± 14%• Seuil de signification > 27%
Diffusion Weighted Whole Body MRI
Comment je fais ?Séquences
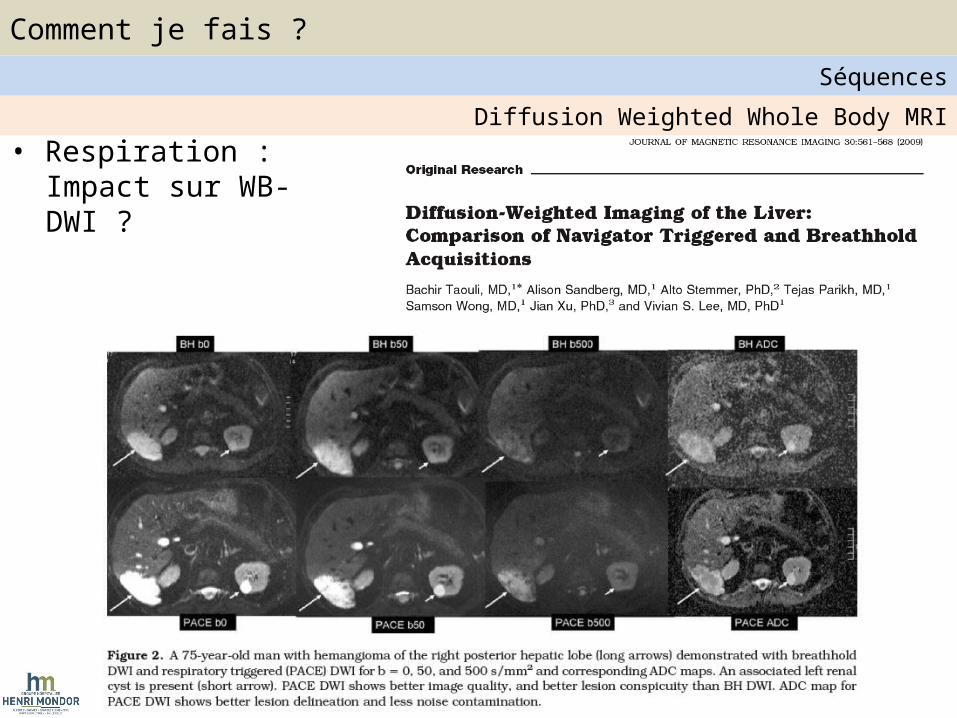
• Respiration : Impact sur WB-DWI ?
Diffusion Weighted Whole Body MRI
Comment je fais ?Séquences
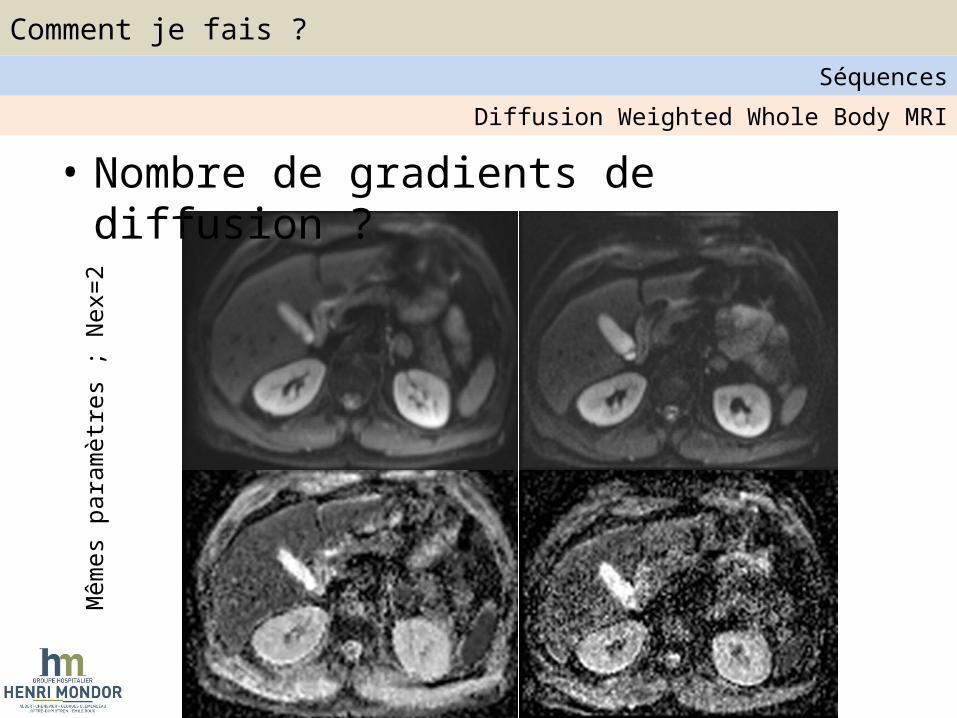
Mêm
es p
aram
ètre
s ; N
ex=2
• Nombre de gradients de diffusion ?Diffusion Weighted Whole Body MRI
Comment je fais ?Séquences
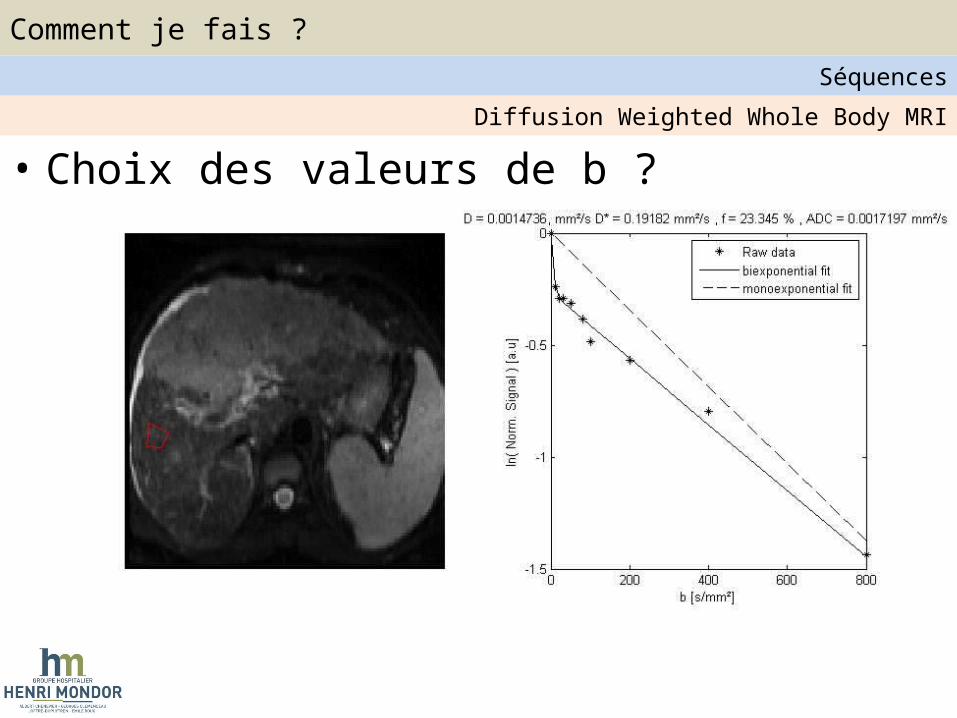
• Choix des valeurs de b ?Diffusion Weighted Whole Body MRI
Comment je fais ?Séquences
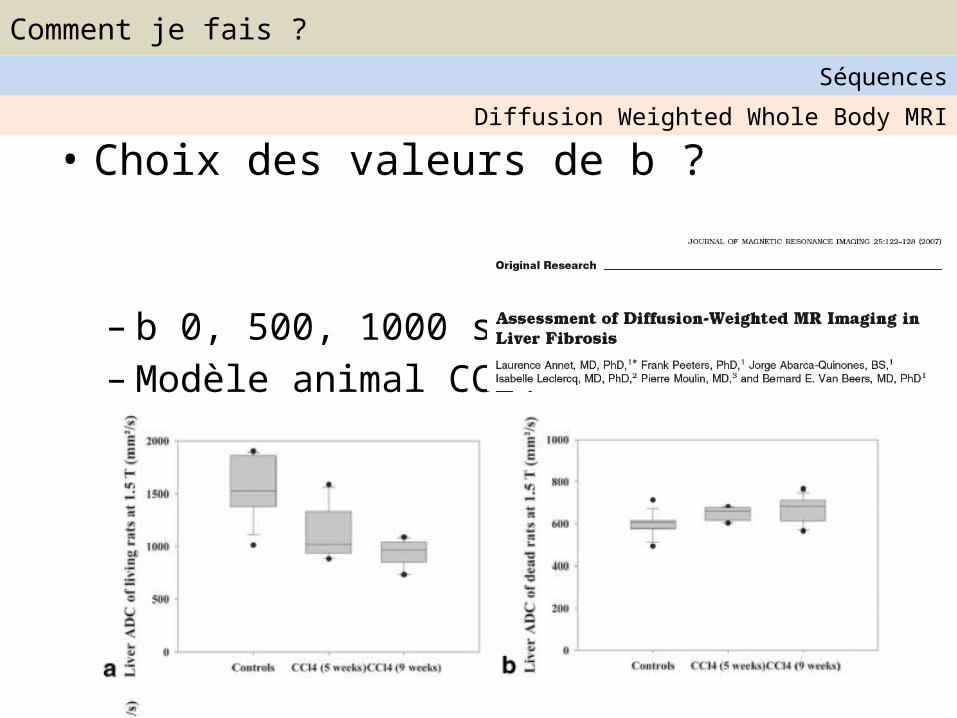
• Choix des valeurs de b ?
– b 0, 500, 1000 s/mm2
– Modèle animal CCl4
Diffusion Weighted Whole Body MRI
Comment je fais ?Séquences
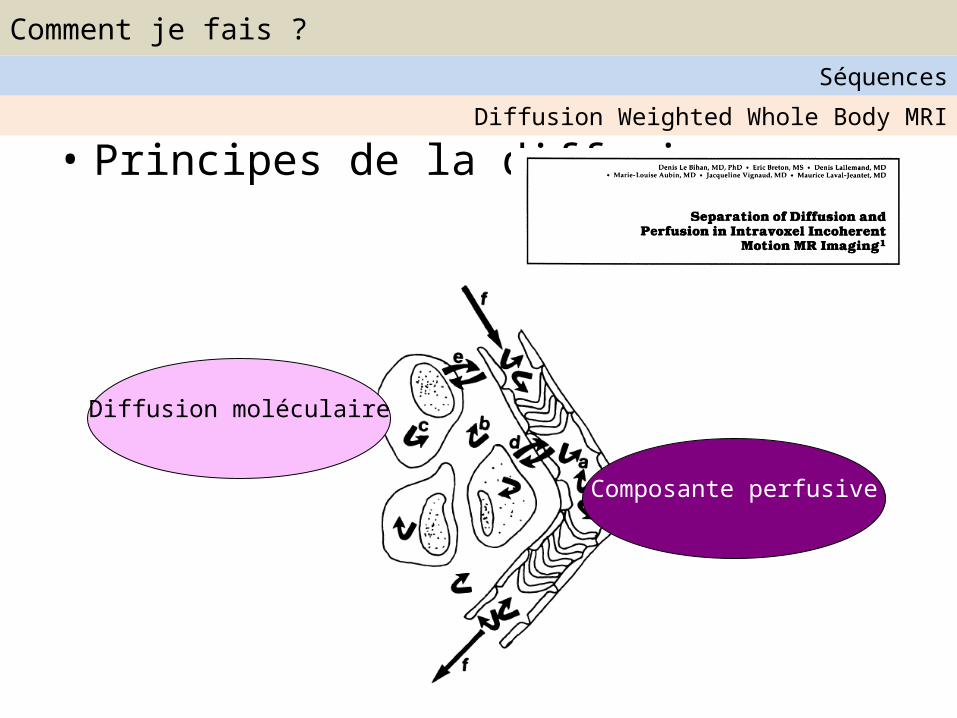
• Principes de la diffusion
Composante perfusive
Diffusion moléculaire
Diffusion Weighted Whole Body MRI
Comment je fais ?Séquences
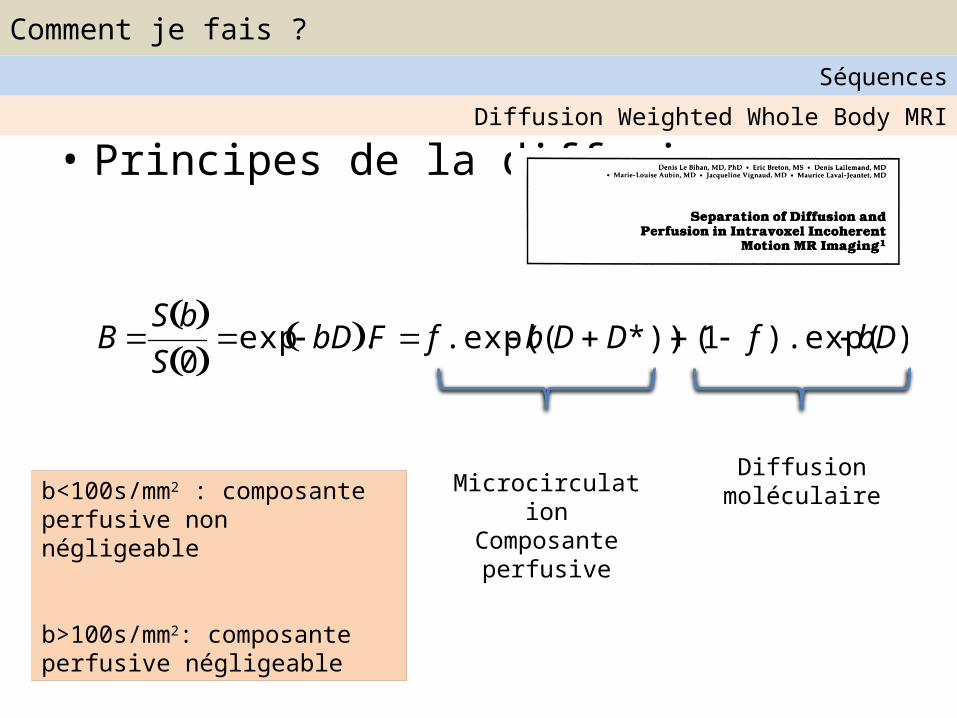
• Principes de la diffusion
BS b S 0
exp bD .F f .exp( b(DD*)) (1 f ).exp( bD)
Diffusion moléculaireMicrocirculation
Composante perfusive
b<100s/mm2 : composante perfusive non négligeable
b>100s/mm2: composante perfusive négligeable
Diffusion Weighted Whole Body MRI
Comment je fais ?Séquences
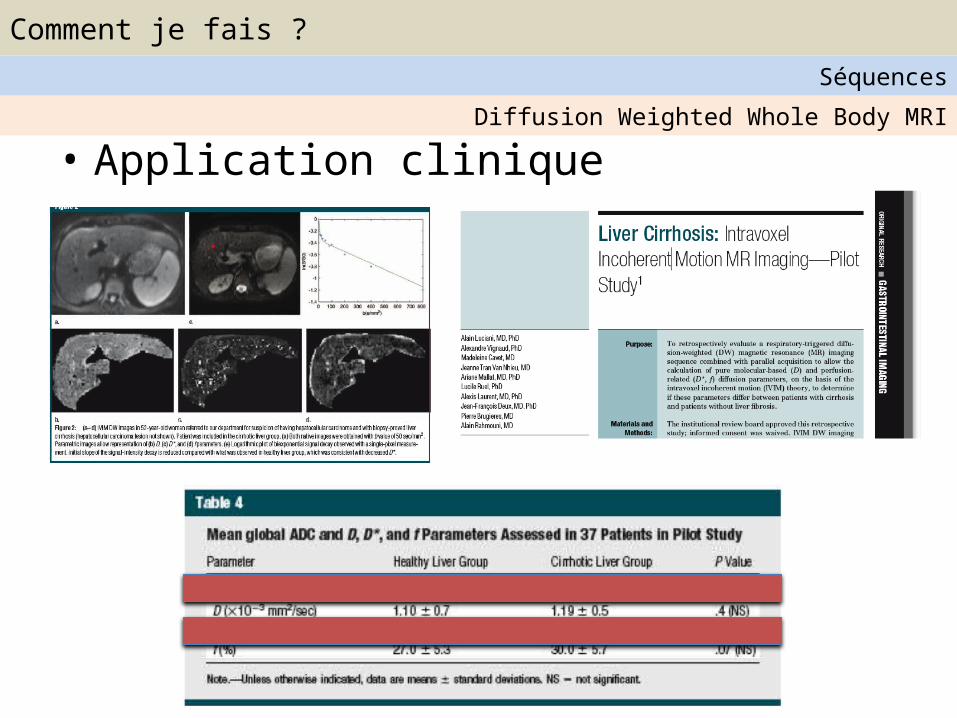
• Application cliniqueDiffusion Weighted Whole Body MRI
Comment je fais ?Séquences
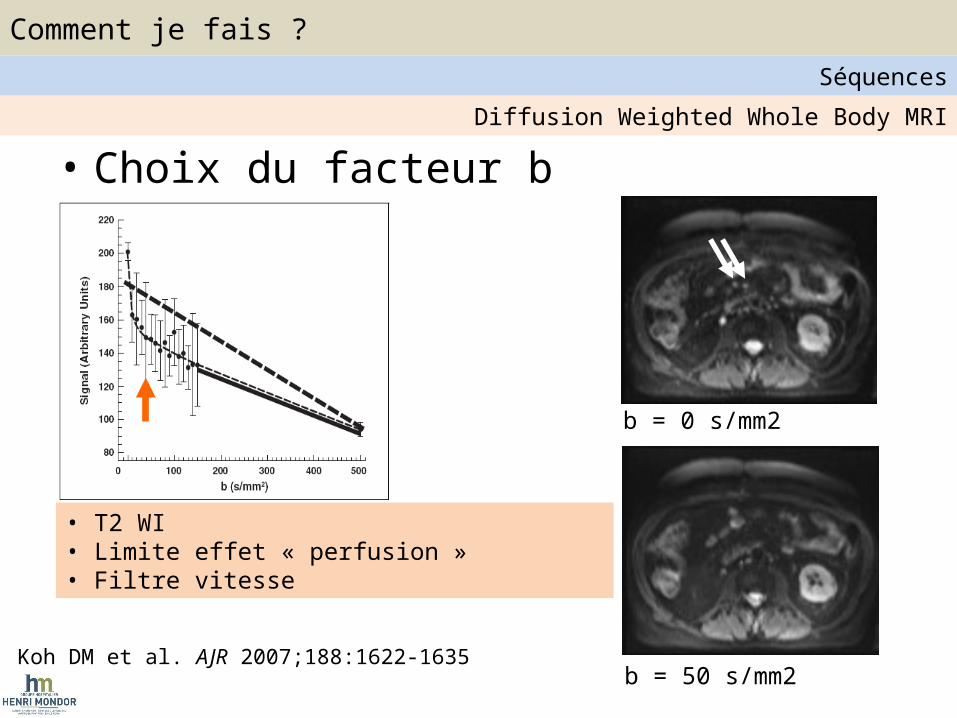
• Choix du facteur b
Koh DM et al. AJR 2007;188:1622-1635b = 50 s/mm2
b = 0 s/mm2
• T2 WI• Limite effet « perfusion »• Filtre vitesse
Diffusion Weighted Whole Body MRI
Comment je fais ?Séquences
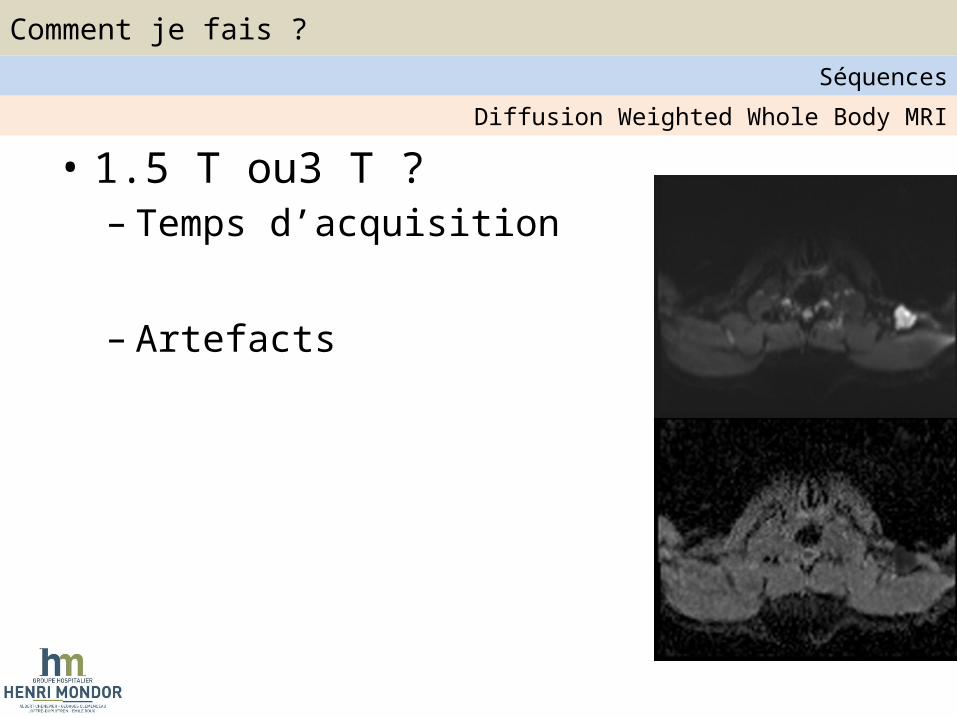
• 1.5 T ou3 T ?– Temps d’acquisition
– Artefacts
Diffusion Weighted Whole Body MRI
Comment je fais ?Séquences
1. Antennes2. Imagerie parallèle3. Gating respiratoire4. Suppression graisse5. Injection ?6. DWI imaging :
1. TR/TE2. Direction de gradients3. Epaisseur de coupe / Gap4. Choix des valeurs de b
Messages Clés
Comment je fais ?Séquences
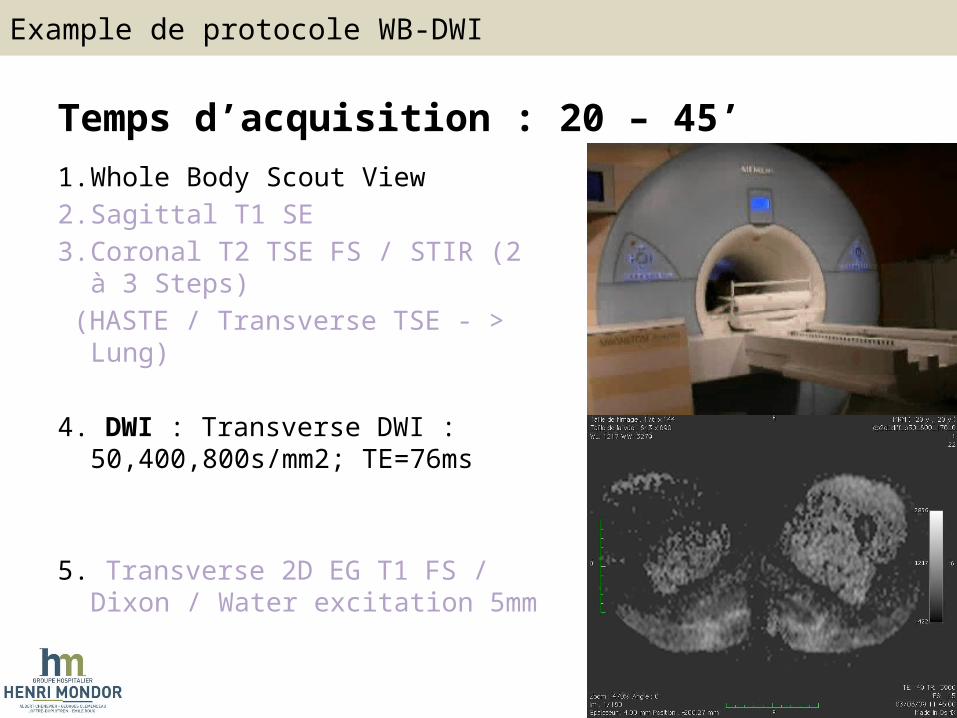
Temps d’acquisition : 20 – 45’1. Whole Body Scout View2. Sagittal T1 SE3. Coronal T2 TSE FS / STIR (2 à 3 Steps) (HASTE / Transverse TSE - > Lung)
4. DWI : Transverse DWI : 50,400,800s/mm2; TE=76ms
5. Transverse 2D EG T1 FS / Dixon / Water excitation 5mm
Example de protocole WB-DWI
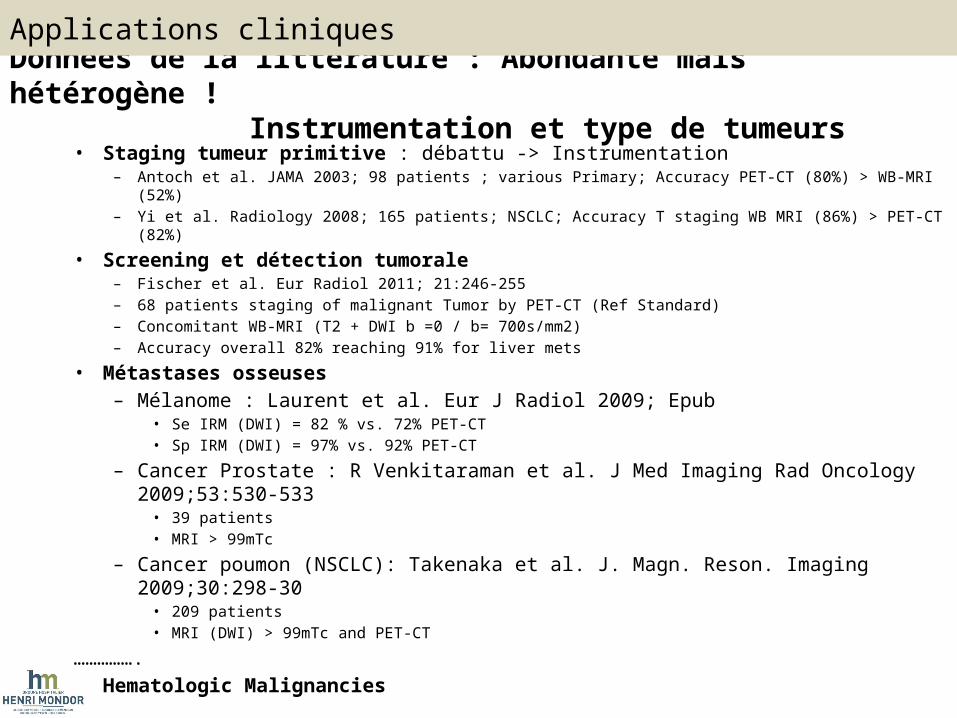
Données de la littérature : Abondante mais hétérogène ! Instrumentation et type de
tumeurs • Staging tumeur primitive : débattu -> Instrumentation
– Antoch et al. JAMA 2003; 98 patients ; various Primary; Accuracy PET-CT (80%) > WB-MRI (52%)– Yi et al. Radiology 2008; 165 patients; NSCLC; Accuracy T staging WB MRI (86%) > PET-CT (82%)
• Screening et détection tumorale– Fischer et al. Eur Radiol 2011; 21:246-255– 68 patients staging of malignant Tumor by PET-CT (Ref Standard)– Concomitant WB-MRI (T2 + DWI b =0 / b= 700s/mm2) – Accuracy overall 82% reaching 91% for liver mets
• Métastases osseuses– Mélanome : Laurent et al. Eur J Radiol 2009; Epub
• Se IRM (DWI) = 82 % vs. 72% PET-CT• Sp IRM (DWI) = 97% vs. 92% PET-CT
– Cancer Prostate : R Venkitaraman et al. J Med Imaging Rad Oncology 2009;53:530-533• 39 patients• MRI > 99mTc
– Cancer poumon (NSCLC): Takenaka et al. J. Magn. Reson. Imaging 2009;30:298-30• 209 patients• MRI (DWI) > 99mTc and PET-CT
…………….• Hematologic Malignancies
Applications cliniques
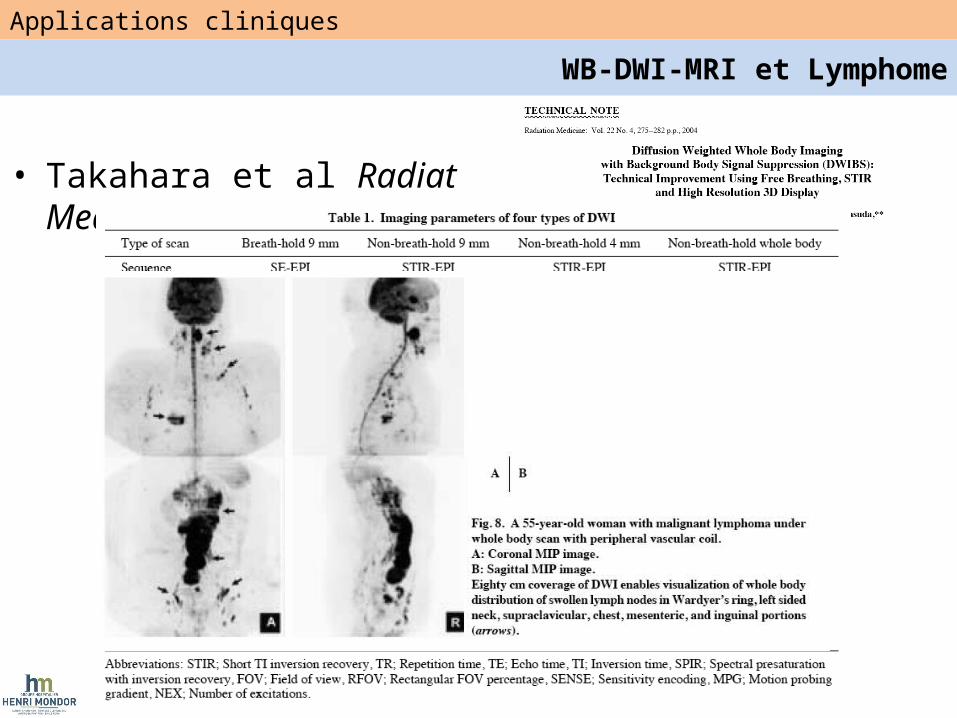
• Takahara et al Radiat Med. 2004
Applications cliniques
WB-DWI-MRI et Lymphome
Applications cliniques
WB-DWI-MRI et Lymphome
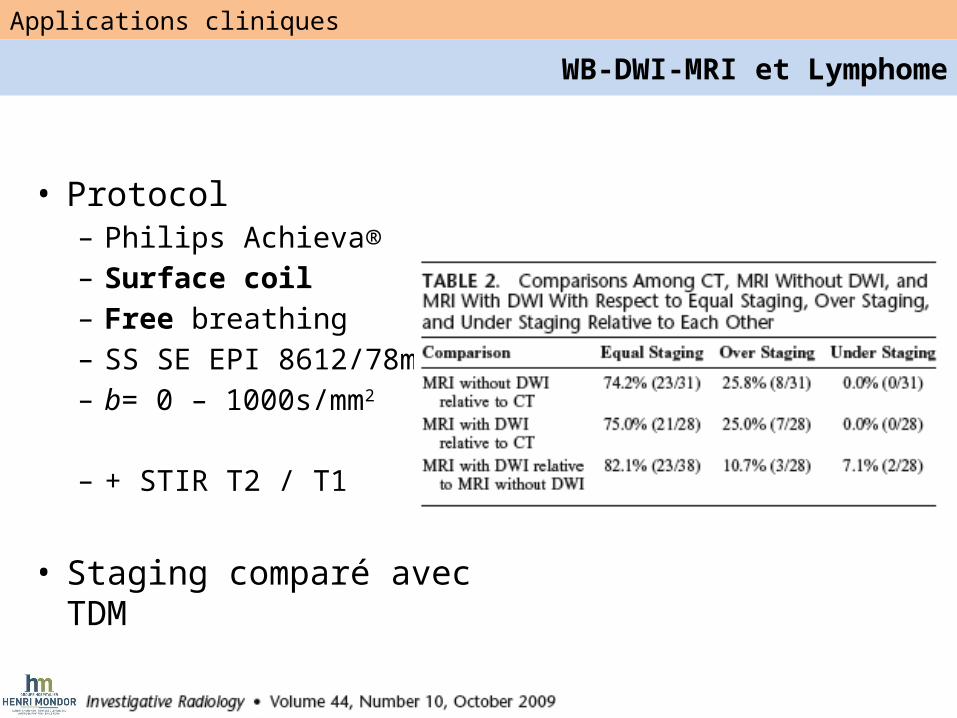
• Protocol– Philips Achieva®– Surface coil– Free breathing– SS SE EPI 8612/78ms– b= 0 – 1000s/mm2
– + STIR T2 / T1
• Staging comparé avec TDM
Applications cliniques
WB-DWI-MRI et Lymphome
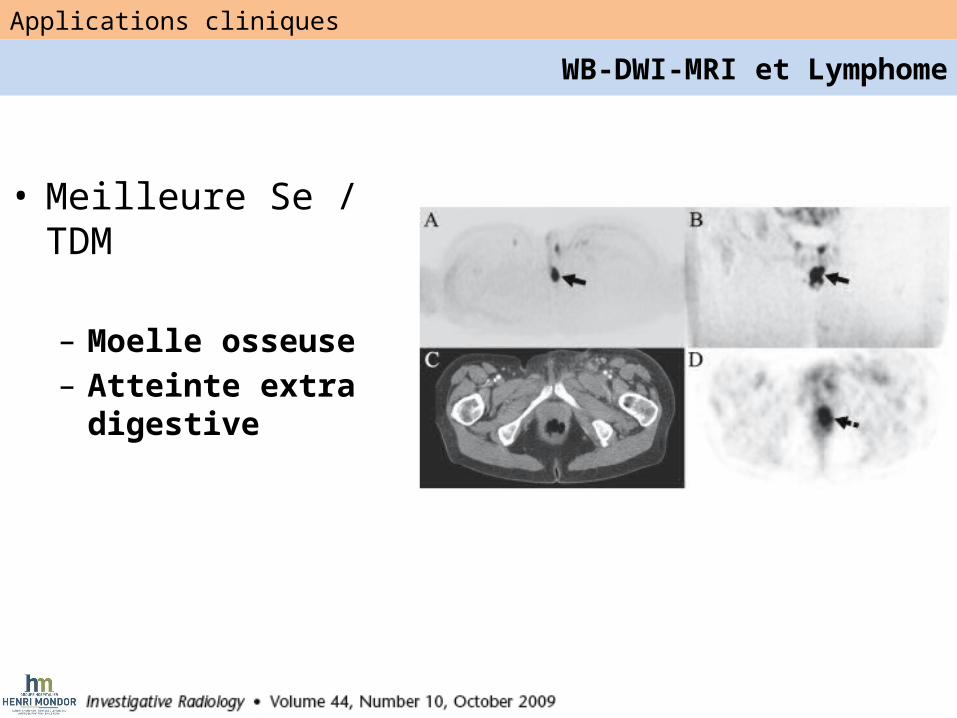
• Meilleure Se / TDM
– Moelle osseuse– Atteinte extra digestive
Applications cliniques
WB-DWI-MRI et Lymphome
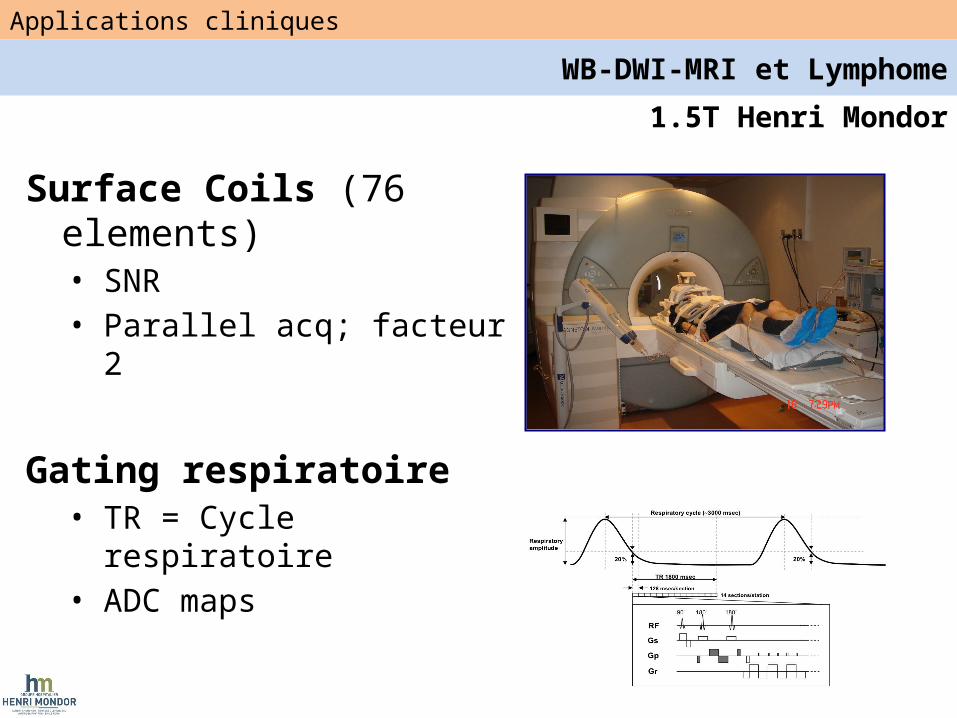
1.5T Henri Mondor
Surface Coils (76 elements)• SNR• Parallel acq; facteur 2
Gating respiratoire• TR = Cycle respiratoire• ADC maps
Applications cliniques
WB-DWI-MRI et Lymphome
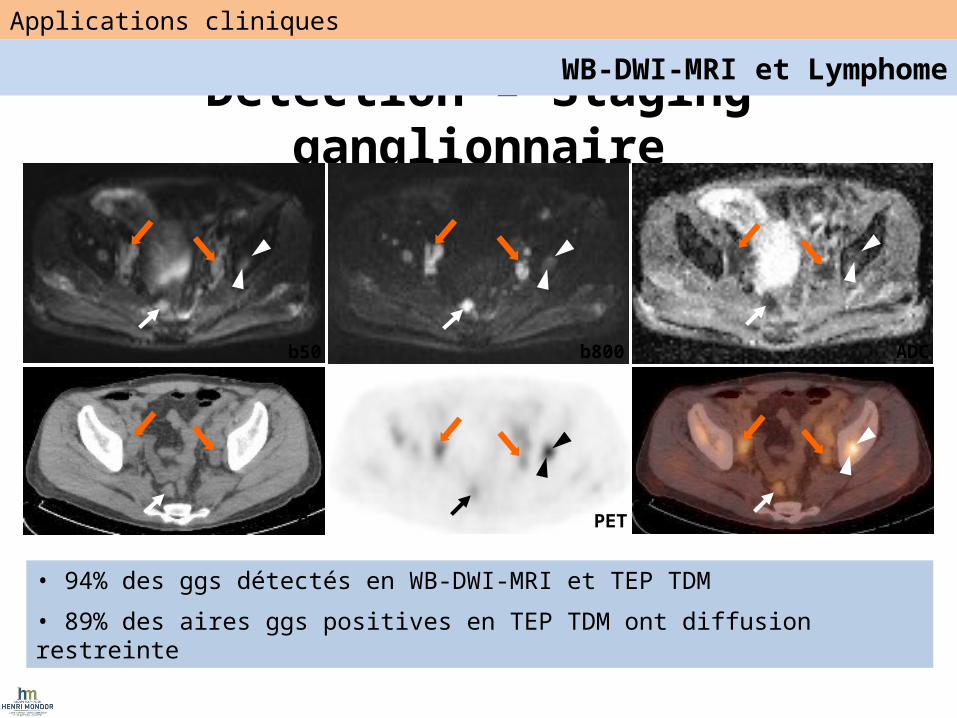
Detection – Staging ganglionnaire
CT
ADCb800b50
PET PET/CT
• 94% des ggs détectés en WB-DWI-MRI et TEP TDM
• 89% des aires ggs positives en TEP TDM ont diffusion restreinte
Applications cliniques
WB-DWI-MRI et Lymphome
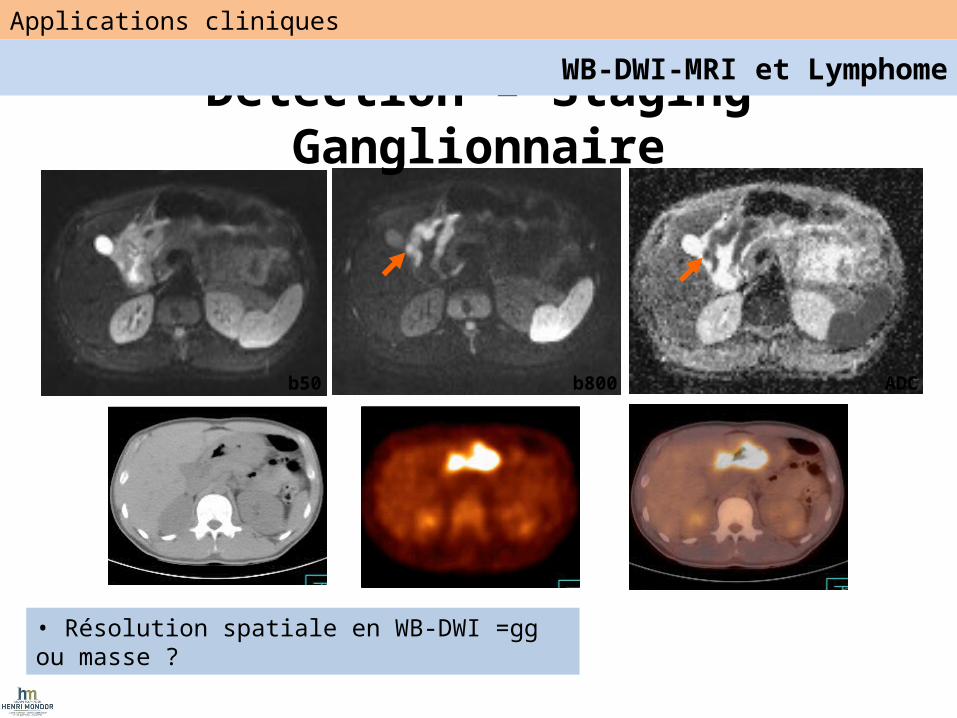
• Résolution spatiale en WB-DWI =gg ou masse ?
b50 b800 ADC
Detection – Staging Ganglionnaire
Applications cliniques
WB-DWI-MRI et Lymphome
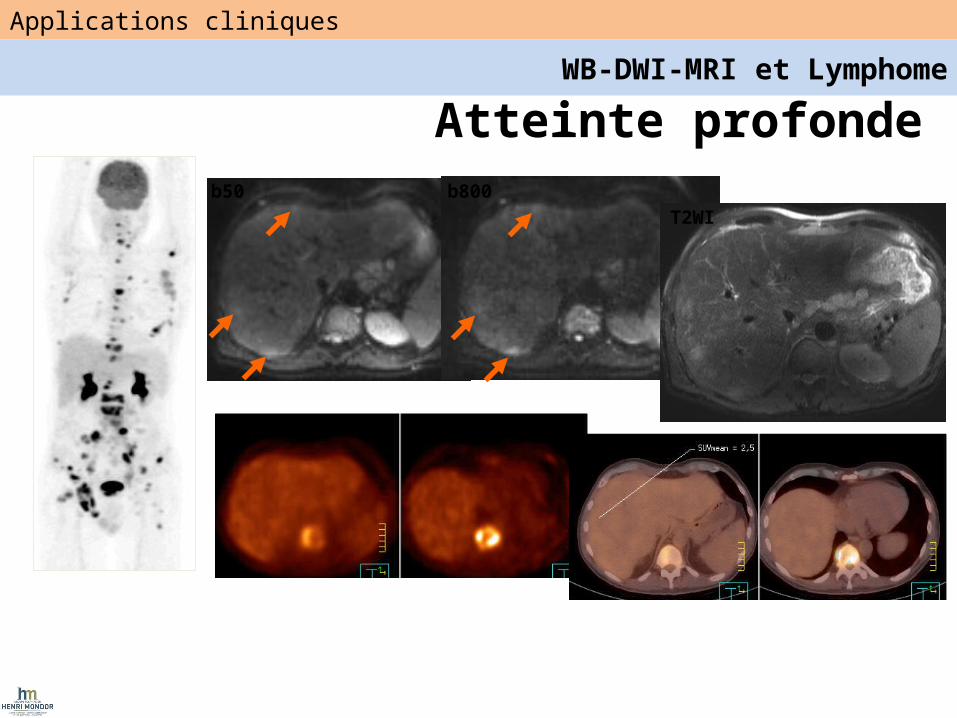
Atteinte profondeb50 b800
T2WI
Applications cliniques
WB-DWI-MRI et Lymphome
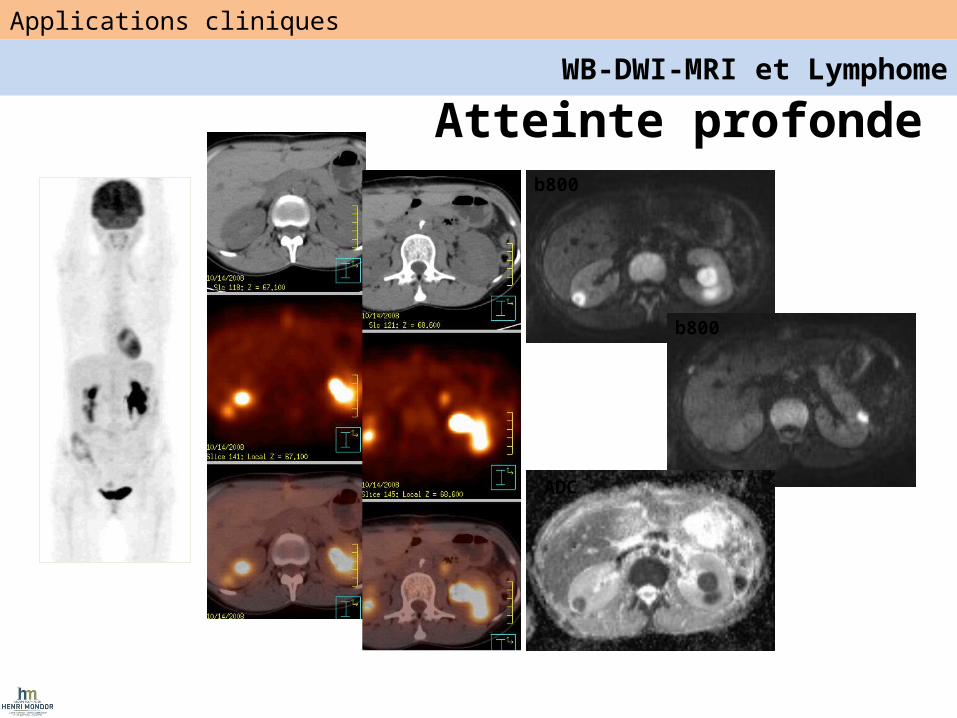
b800
b800
ADC
Atteinte profonde
Applications cliniques
WB-DWI-MRI et Lymphome
b50
b50
b800 ADC
b800 ADC
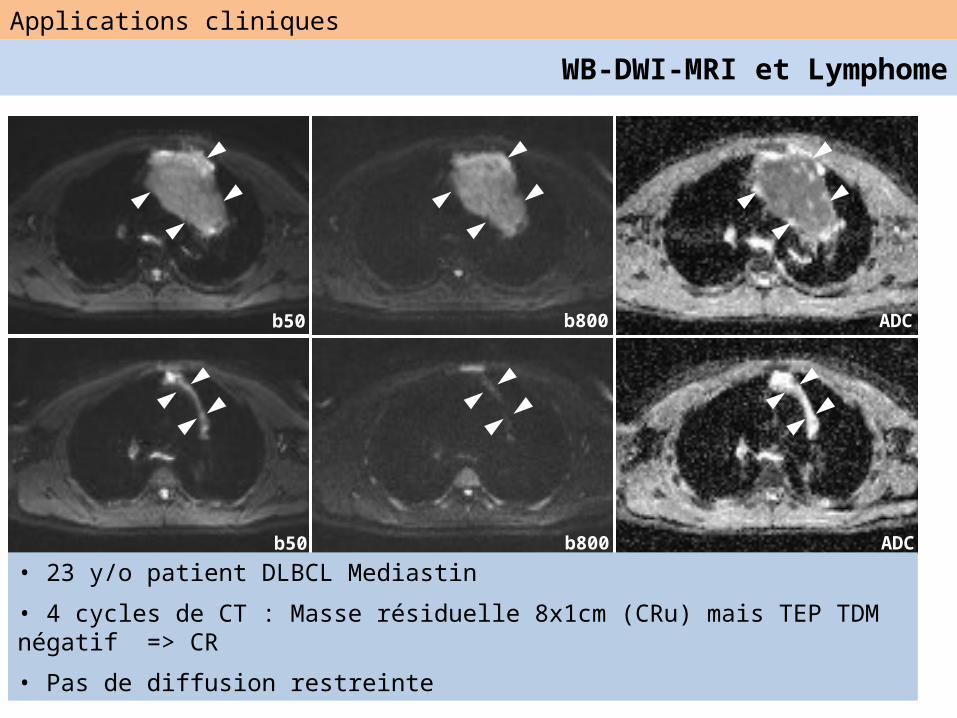
• 23 y/o patient DLBCL Mediastin
• 4 cycles de CT : Masse résiduelle 8x1cm (CRu) mais TEP TDM négatif => CR
• Pas de diffusion restreinte
Applications cliniques
WB-DWI-MRI et Lymphome
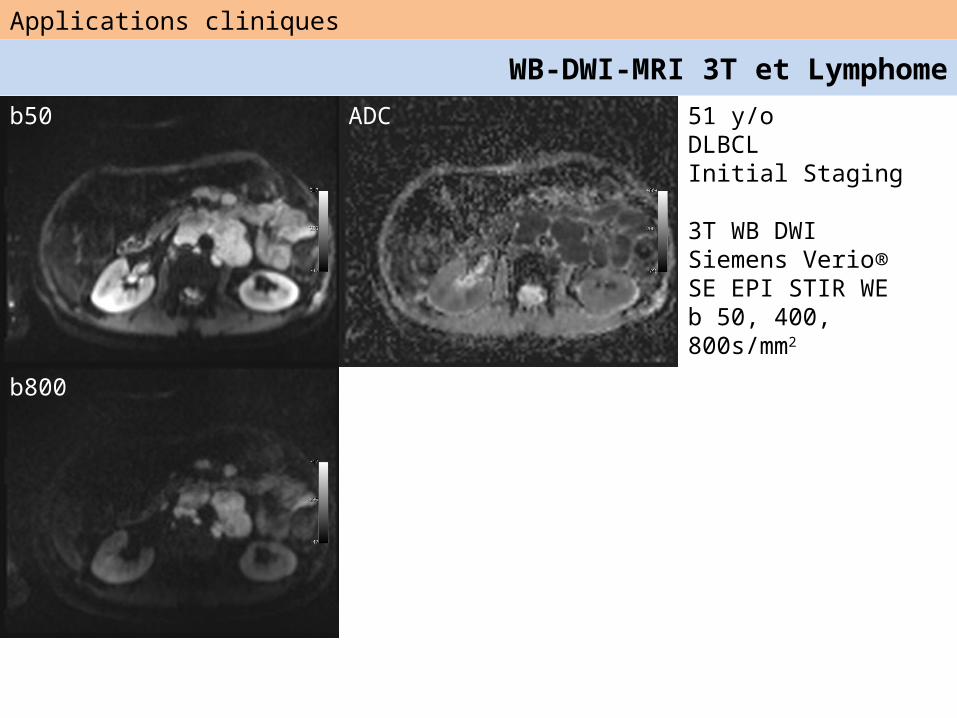
51 y/oDLBCLInitial Staging
3T WB DWISiemens Verio®SE EPI STIR WEb 50, 400, 800s/mm2
b50
b800
ADC
Applications cliniques
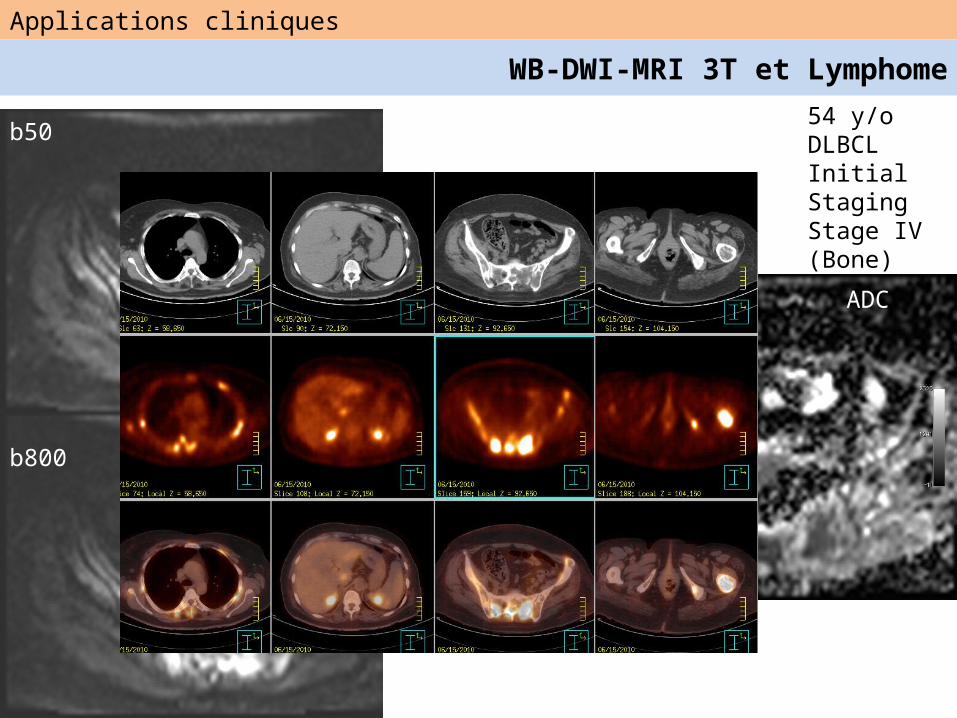
WB-DWI-MRI 3T et Lymphome
b50
b800
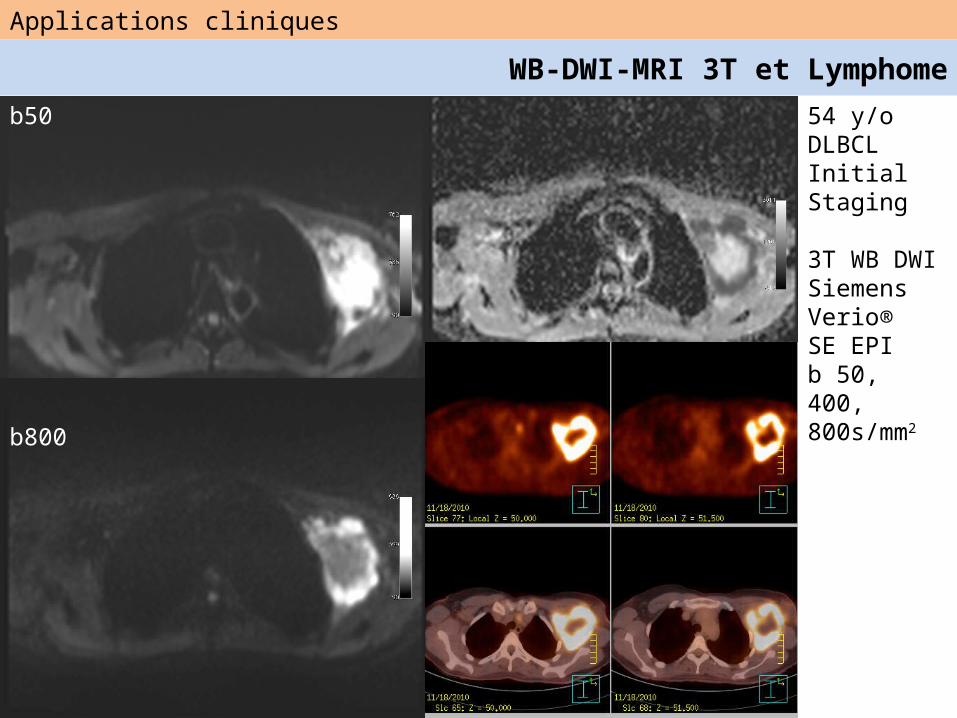
54 y/oDLBCLInitial Staging
3T WB DWISiemens Verio®SE EPIb 50, 400, 800s/mm2
Applications cliniques
WB-DWI-MRI 3T et Lymphome
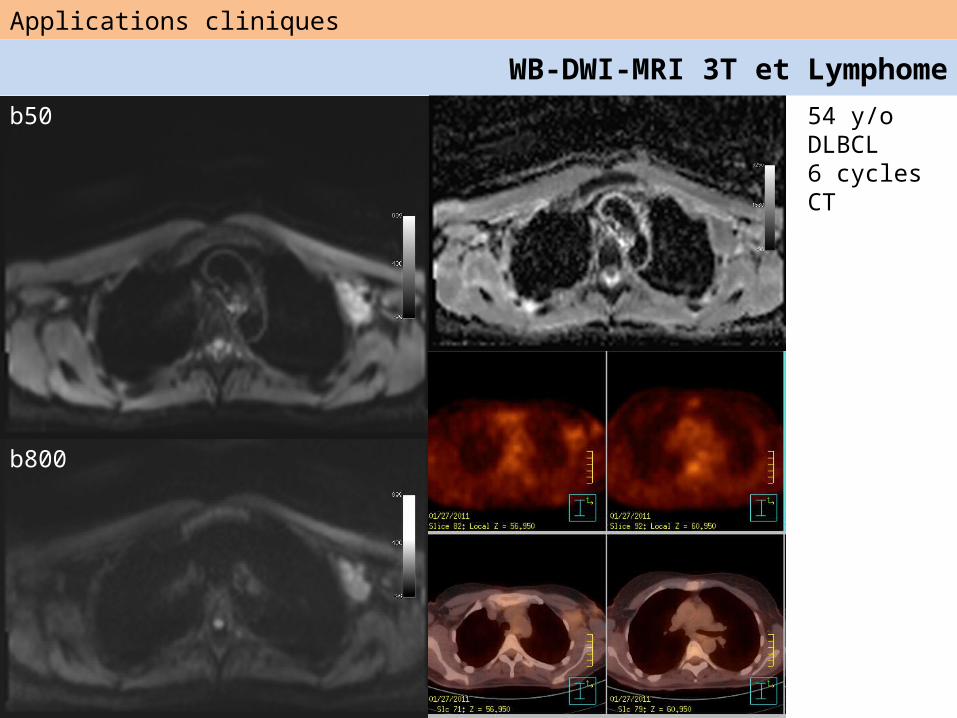
54 y/oDLBCL6 cycles CT
b50
b800
Applications cliniques
WB-DWI-MRI 3T et Lymphome
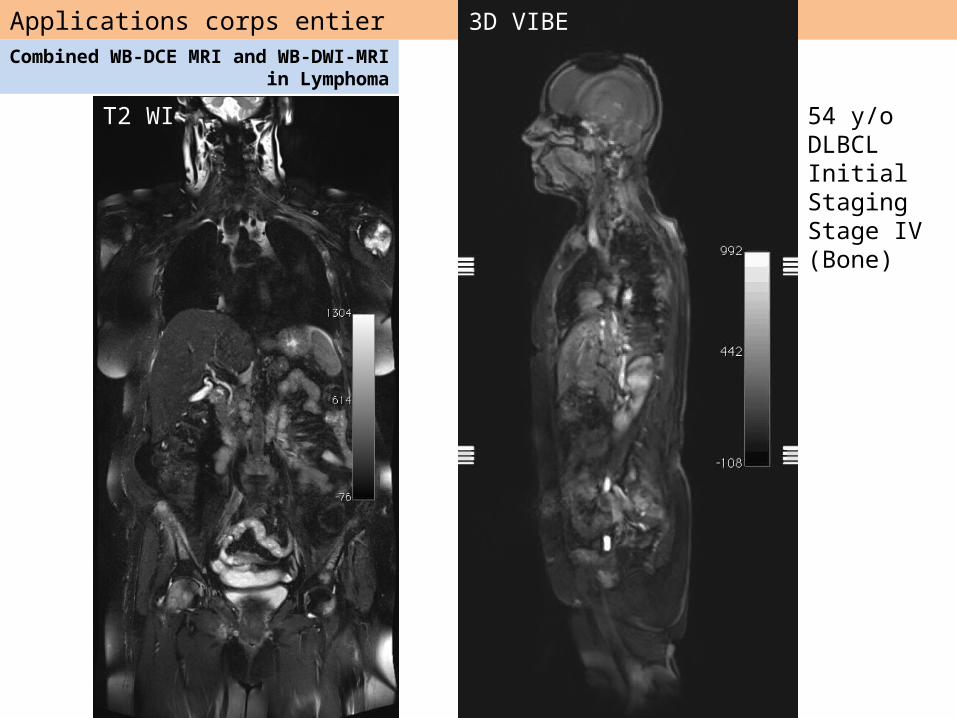
Applications corps entier
54 y/oDLBCLInitial StagingStage IV (Bone)
b50 ADC mapT2 WI
Combined WB-DCE MRI and WB-DWI-MRI in Lymphoma
3D VIBE
54 y/oDLBCLInitial StagingStage IV (Bone)
b800
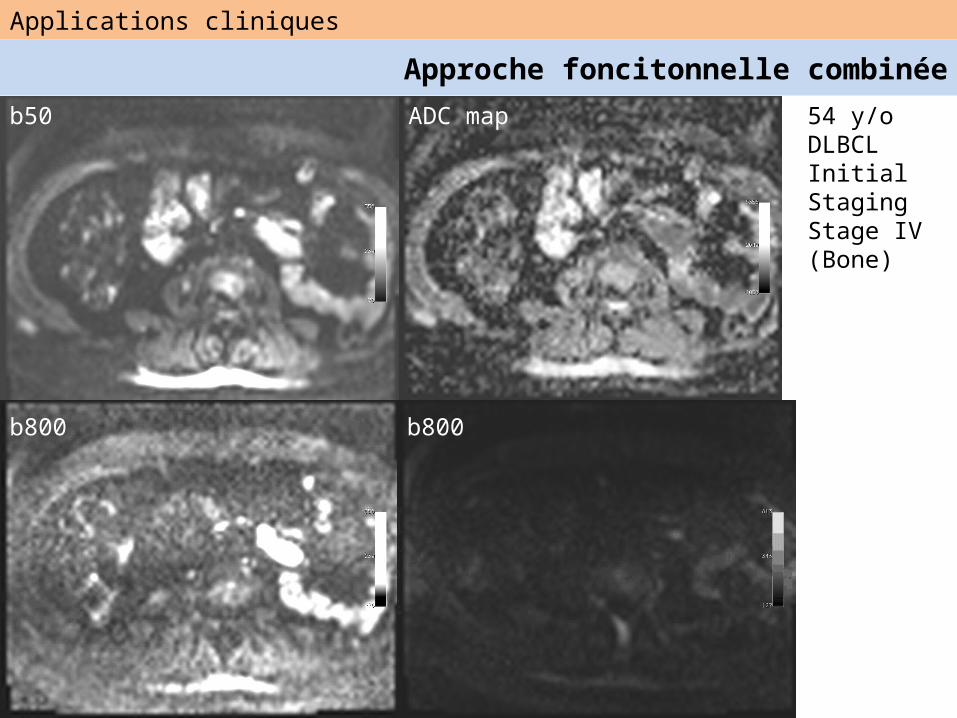
b50 ADC map
Applications cliniques
Approche foncitonnelle combinée
b800
54 y/oDLBCLInitial StagingStage IV (Bone)
b50
b800
ADC
Applications cliniques
WB-DWI-MRI 3T et Lymphome
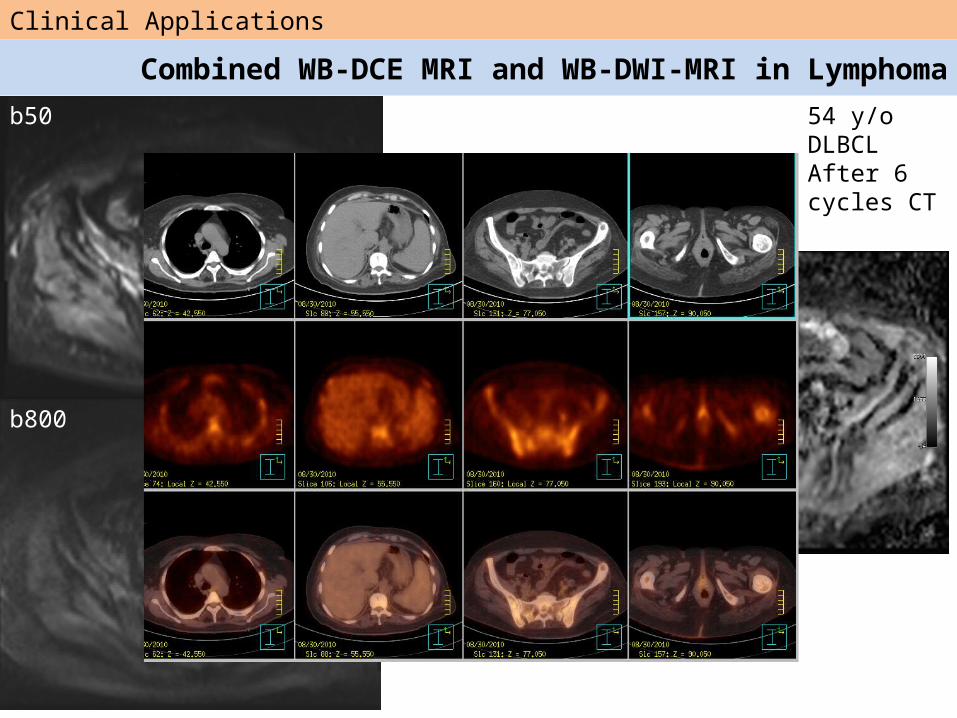
Clinical Applications
Combined WB-DCE MRI and WB-DWI-MRI in Lymphoma54 y/oDLBCLAfter 6 cycles CT
b800
b50
ADC
Messages
• Instrumentation
• Instrumentation
• Instrumentation
1
2
3
Applications cliniques
• Pas encore définies ….• Standardisation ?• Sélectionner études cliniques adaptées….