Embed Size (px)
Citation preview

Conflits d’intérêt
M. Buysschaert est membre de comités d’experts et/ou a participé à des conférences et études organisées par Eli Lilly, NovoNordisk, Servier, MSD, BMS, Astra Zeneca, Novartis, Sanofi-Aventis.

10
1
0.55 7 9
IM fatal et non-fatal
Niv
eau
de r
isqu
e
p<0.0001
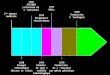
14% réduction du risque par 1% de diminution en HbA1c
5 7 9
Endpoints microvasculaires
Niv
eau
de r
isqu
e
10
1
0.5
p<0.0001
37% réduction du risque par 1% de diminution en HbA1c
IM = Infarctus du Myocarde .Stratton I, et al. BMJ 2000;321:405―12.
HbA1c (%)
Corrélation épidémiologique entre le contrôle glycémique et le risque de complications
HbA1c (%)

Glycaemic targets for the management of type 2diabetes
• Glycaemic targets for the management of people with type 2 diabetes as recommended by various organisations1–5
1. Nathan DM, et al. Diabetologia. 2009;52:17-30. 2. IDF. Global Guidelines 2005. 3. Rodbard HW, et al. Endocr Pract. 2007;13(Suppl. 1):1-68. 4. NICE clinical guideline 87. Quick reference guide. May 2009. 5. Matthaei S, et al. German Diabetes Association guidelines. October 2008.
Organisation HbA1c (%) FPG (mmol/L) PPG (mmol/L)
ADA-EASD1 <7 — —
IDF-Europe2 <6.5 <6.0 (<110*) <8.0 (<145*)
AACE3 ≤6.5 <6.1 (<110*) <7.8 (<140*)
NICE4 <6.5** — <8.5 (<153*)
DDG5 <6.5 — —
*mg/dL
**<7.5% for people receiving ≥2 oral glucose-lowering drugs or those requiring insulin
FPG, fasting plasma glucose; PPG, postprandial glucose; ADA, American Diabetes Association; IDF, International Diabetes Federation; AACE, American Association of Clinical Endocrinologists; NICE, National Institute of Clinical Excellence; DDG, Deutschen Diabetes-Gesellschaft (German Diabetes Association)

HbA1c : 7.9 ±1.6 %
Patients avec HbA1c < 7% : 30%
Acta Clinica Belgica, 2005

HbA1c: 8.8 ±2.3%
Acta Clinica Belgica,2006

6BY/ELB/11/209/462
Key challenge of type 2 diabetes: outcome
43% of patients do not
achieve glycaemic targets (HbA1c<7%)
Ford et al (NHANES). Diabetes Care 2008;31:102–4

7BY/ELB/11/209/462
Distribution of Risk Factors for Microvascular and MacrovascularDistribution of Risk Factors for Microvascular and Macrovascular Complications among U.SComplications among U.S. . Adults with Diabetes, 1999Adults with Diabetes, 1999––2010.2010.
Ali MK et al. N Engl J Med 2013;368:1613Ali MK et al. N Engl J Med 2013;368:1613--16241624

Barrières pour un bon contrôle
PatientPatient--Effets indEffets indéésirablessirables
--PolymPolyméédicationdication--HypoglycHypoglycéémiemie--Prise de poidsPrise de poids
MaladieMaladie--Chronique Chronique
--AsymptomatiqueAsymptomatique--Epuisement progressif Epuisement progressif
des cellules bêtades cellules bêta
MMéédecindecin--Inertie cliniqueInertie clinique
--Suivi & monitoringSuivi & monitoring--Augmentation de la Augmentation de la
mméédicationdication

7
6
9
8HbA
1c(%
)
10
OAD* monotherapy
Diet andexercise
OAD combination
OAD + basal insulin
OAD monotherapyup-titration
Duration of diabetes
OAD + multiple daily
insulin injections
Conservative management of glycemia:traditional stepwise approach
HbA1c = 6.5%
Campbell IW. Br J Cardiol 2000; 7:625–631.
HbA1c = 7%
*OAD = oral antidiabetic


Diabetes Care,Diabetes Care, Diabetologia. Diabetologia. 1919 April 2012 [Epub ahead of print]April 2012 [Epub ahead of print](Adapted with permission from: Ismail(Adapted with permission from: Ismail--Beigi F, et al. Beigi F, et al. Ann Intern MedAnn Intern Med 2011;154:554)2011;154:554)

DPP-4 comme 2e choix après la metformineDPPDPP--4 comme 24 comme 2ee choix aprchoix aprèès la metformines la metformine
AdaptAdaptéé dd’’apraprèès Inzucchi et al. Diabetes Care 2012;35:1364s Inzucchi et al. Diabetes Care 2012;35:1364--13791379..
Two drug Two drug combinationscombinations
Efficacy (Efficacy (↓↓ HbAHbA1c1c))HypoglycemiaHypoglycemiaWeightWeightMajor side effect(s)Major side effect(s)CostsCosts
MetforminMetformin
+ Sulfonylurea+ Sulfonylurea
HighHighModerate riskModerate riskGainGainHypoglycemiaHypoglycemiaLowLow
MetforminMetformin
+ Thiazolidinedione+ Thiazolidinedione
HighHighLow riskLow riskGainGainEdema, HF, fxEdema, HF, fx’’ssHighHigh
MetforminMetformin
+ DDP+ DDP--4 inhibitor4 inhibitor
IntermediateIntermediateLow riskLow riskNeutralNeutralRareRareHighHigh
MetforminMetformin
+ + GLPGLP--1 receptor 1 receptor agonistagonist
HighHighLow riskLow riskLossLossGIGIHighHigh
MetforminMetformin
++ Insulin Insulin (usually basal)(usually basal)
HighestHighestHigh riskHigh riskGainGainHypoglycemiaHypoglycemiaVariableVariable
If needed to reach individualized HbAIf needed to reach individualized HbA1c1c target after ~3 months, proceed to 3target after ~3 months, proceed to 3--drug combination drug combination (order not meant to denote any specific preference):(order not meant to denote any specific preference):
HEALTHY EATING, WEIGHT CONTROL, INCREASED PHYSICAL ACTIVITYHEALTHY EATING, WEIGHT CONTROL, INCREASED PHYSICAL ACTIVITYInitial drug Initial drug monotherapymonotherapy
Efficacy (Efficacy (↓↓ HbAHbA1c1c))HypoglycemiaHypoglycemiaWeightWeightSide effectsSide effectsCostsCosts
HighHighLow riskLow riskNeutral / lossNeutral / lossGI / lactic acidosisGI / lactic acidosisLowLow
If needed to reach individualized HbAIf needed to reach individualized HbA1c1c target after ~3 months, proceed to 2target after ~3 months, proceed to 2--drug combination drug combination (order not meant to denote any specific preference):(order not meant to denote any specific preference):
MetforminMetformin
More complex More complex insulin strategiesinsulin strategies
InsulinInsulin(multipe daily doses)(multipe daily doses)
Three drug Three drug combinationscombinations MetforminMetformin
+ Sulfonylurea+ Sulfonylurea
MetforminMetformin
+ Thiazolidinedione+ Thiazolidinedione
MetforminMetformin
+ DDP+ DDP--4 inhibitor4 inhibitor
MetforminMetformin
+ + GLPGLP--1 receptor 1 receptor agonistagonist
MetforminMetformin
+ + Insulin Insulin (usually basal)(usually basal)
TZDTZD
DDPDDP--44--ii
GLPGLP--11--RARA
InsulinInsulin
++ ++ ++ ++ ++
oror oror oror oror oror
oror oror oror oror oror
oror oror
SUSU
DDPDDP--44--ii
GLPGLP--11--RARA
InsulinInsulin
SUSU
TZDTZD
InsulinInsulin
SUSU
TZDTZD
InsulinInsulin
TZDTZD
DDPDDP--44--ii
GLPGLP--11--RARA
If combination therapy that includes basal insulin has failed toIf combination therapy that includes basal insulin has failed to achieve HbAachieve HbA1c1c target after 3target after 3--6 months,6 months,proceed to a more complex insulin strategy, usually in combinatiproceed to a more complex insulin strategy, usually in combination with 1on with 1--2 non2 non--insulin agents:insulin agents:
Recommandations ADA/ EASD 2012

Adapted Recommendations: Adapted Recommendations: When Goal is to Avoid Weight GainWhen Goal is to Avoid Weight Gain
Diabetes Care,Diabetes Care, Diabetologia. Diabetologia. 1919 April April 2012 [Epub ahead of print]2012 [Epub ahead of print]
TR/E
LB/0
5/20
12/2
36TR
/ELB
/05/
2012
/236

Time (min)
The Incretin Effect Demonstrates the Response to Oral vs IV Glucose1
Mean ± SE; n = 6; *p≤0.05; 01-02 = glucose infusion time.1. Nauck MA, et al. J Clin Endocrinol Metab. 1986;63:492–498.
Veno
us P
lasm
a G
luco
se (m
mol
/L)
C-p
eptid
e (n
mol
/L)
11
5.5
001 60 120 180 01 60 120 180
0.0
0.5
1.0
1.5
2.0
Time (min)02 02
Incretin Effect
Oral Glucose IV Glucose
*
*
*
**
**
La Barre La Barre «« Sur les possibilitSur les possibilitéés ds d’’un traitement du diabun traitement du diabèète par lte par l’’incrincréétinetine »», , Bulletin de Bulletin de ll’’AcadAcadéémie Royale de Mmie Royale de Méédecine de Belgiquedecine de Belgique, 1932, 12, 620, 1932, 12, 620--634634

INCRETINS
Glucagon-like peptide 1[GLP-1]
Gastric inhibitory polypeptide [GIP]
L cellsGlucose dependant
Inactivation by DPP-4Reduced secretion in diabetes
K cellsGlucose dependant
Inactivation by DPP-4Normal secretion and
reduced effect in diabetes

GLP-1 Effects in Humans: Understanding the Glucoregulatory Role of Incretins1–4
Promotes satiety and reduces appetite
Beta cells:Enhances glucose-dependent insulin
secretion
1. Adapted from Flint A, et al. J Clin Invest. 1998;101:515–520. 2. Adapted from Larsson H, et al. Acta Physiol Scand. 1997;160:413–422. 3. Adapted from Nauck MA, et al. Diabetologia. 1996;39:1546–1553. 4. Adapted from Drucker DJ. Diabetes. 1998;47:159–169.
Liver:↓ Glucagon reduces
hepatic glucose output
Alpha cells:↓ Postprandial
glucagon secretion
Stomach:Helps regulate
gastric emptying
GLP-1 secreted upon the ingestion of food

09-A
ug-2
008-
JAN
-200
7-B
E-12
63-S
S
GLP-1 Preserved Morphology of Human Islet Cells In Vitro
Day 1
GLP-1–treated cellsControl
Day 3
Day 5
Adapted from Farilla L et al Endocrinology 2003;144:5149–5158.
Islets treated with GLP-1 in culture were able to maintain their integrity for a longer period of time.

GLP-1 actions in the heart
CELL METABOLISM 3, 153–165, MARCH 2006. The biology of incretin hormones ReviewDaniel J. Drucker


09-A
ug-2
008-
JAN
-200
7-B
E-12
63-S
S
* * **
**
*p<0.05, type 2 diabetes vs. NGT Meal started at time 0 and finished at 10–15 minutes.Adapted from Toft-Nielsen M-B et al J Clin Endocrinol Metab 2001;86:3717–3723.
GLP-1 Levels Decreased in Type 2 Diabetes
NGT (n=33)Type 2 diabetes (n=54)
0
5
10
15
20
0 60 120 180 240
Time (minutes)
GLP
-1 (p
mol
/L)
*
Meal Test Study

21BY/ELB/11/2009/462
Incretin Effect
Intravenous glucose
T2DControl Subjects
Glu
cose
†[m
mol
/L]
Glu
cose
†[m
mol
/L]
Insu
lin†
[pm
ol/L
]
Insu
lin†
[pm
ol/L
]
* * *
* * * * * *
5
0
10
15
20
5
0
10
15
20
0
100
200
300
400
500
Time (min)60 120 1800
0
100
200
300
400
500
60 120 1800
Time (min)60 120 1800
Time (min)60 120 1800
Time (min)
Oral glucose
Incretin Effect The incretin effect is diminished in patients
with type 2 diabetes (T2D)
*p<.05; †PlasmaAdapted from Nauck MA, et al. Diabetologia. 1986;29:46-52.

Rapid Inactivation (1–2 minutes) of GLP-1
DPP-4: Dipeptidyl peptidase-4.Adapted from Drucker DJ Expert Opin Invest Drugs 2003;12(1):87–100; Ahrén B Curr Diab Rep 2003;3:365–372.
IntestinalGLP-1release
GLP-1 (9-36)inactive
Mixed meal
GLP-1 (7-36)Active
(half-life <2 mins)
DPP-4inhibitor
DPP-4

Inhibiteurs DPPInhibiteurs DPP--44
Nom de Nom de substancesubstance
Nom de Nom de spspéécialitcialitéé
LaboratoireLaboratoire Dosage recommandDosage recommandéé
SitagliptineSitagliptine JanuviaJanuvia MSDMSD 100 mg/jour p.o.100 mg/jour p.o.
VildagliptineVildagliptine GalvusGalvus NovartisNovartis 2 x 50 mg/jour p.o.2 x 50 mg/jour p.o.
SaxagliptineSaxagliptine OnglyzaOnglyza BMS / Astra BMS / Astra ZenecaZeneca
5 mg/jour p.o. 5 mg/jour p.o.
LinagliptineLinagliptine TrajentaTrajenta Boeringher/LBoeringher/Lillillyy 5 mg/jour p.o.5 mg/jour p.o.

Efficacité
*Diminution moyenne de HbA1c versus placebo. **pas d*Diminution moyenne de HbA1c versus placebo. **pas d’é’étude comparative existante entre les difftude comparative existante entre les difféérentes molrentes moléécules.cules.1. R1. Réésumsuméé des caractdes caractééristiques du produit Trajentaristiques du produit Trajenta®®, 2. R, 2. Réésumsuméé des caractdes caractééristiques du produit Onglyzaristiques du produit Onglyza®®, ,
3. R3. Réésumsuméé des du produit Januviades du produit Januvia®®, 4. R, 4. Réésumsuméé des Caractdes Caractééristiques du produit Galvusristiques du produit Galvus®®..
Compilation graphique de lCompilation graphique de l’’effet theffet théérapeutique de diffrapeutique de difféérents inhibiteurs de la DPPrents inhibiteurs de la DPP--4 en monoth4 en monothéérapie comme rapie comme mentionnmentionnéé dans le Rdans le Réésumsuméé des Caractdes Caractééristiques du Produit (RCP). Pour le changement moyen en HbAristiques du Produit (RCP). Pour le changement moyen en HbA1c1c corrigcorrigéé par par placebo, aprplacebo, aprèès 18 / 24 semaines de traitement par rapport s 18 / 24 semaines de traitement par rapport àà la valeur de basela valeur de base****
Linagliptine1 Saxagliptine2 Sitagliptine3 Vildagliptine4
Dosage 5 mg QD 5 mg QD 5 mg QD 5 mg QD 100 mg QD 100 mg QD 50 mg BID 50 mg BID
n = 147 272 69 103 193 229 90 79
Valeur p* < 0,0001 < 0,0001 < 0,0059 < 0,0001 < 0,0001 < 0,0001 < 0,05 < 0,05
Valeur initiale HbA1c
8,1% 8,0% 7,9% 8,0% 8,0% 8,0% 8,6% 8,4%
--0,6%0,6%
--0,7%0,7%
--0,4%0,4%
--0,6%0,6% --0,6%0,6%
--0,8%0,8%
--0,5%0,5%
--0,7%0,7%
Dim
inut
ion
moy
enne
de
HbA
Dim
inut
ion
moy
enne
de
HbA
1c1c**

Chemistry Metabolism Elimination route
Sitagliptin β-amino acid-based Not appreciably metabolised Renal (~80% unchanged as parent)
Vildagliptin CyanopyrrolidineHepatically hydrolysed to inactive metabolite (P450 enzyme independent)
Renal (22% as parent, 55% as metabolite)
Saxagliptin Cyanopyrrolidine Hepatically metabolised to active metabolite (via P450 3A4/5)
Renal (12-29% as parent, 21-52% as metabolite)
Alogliptin Modified pyrimidinedione Not appreciably metabolised Renal (>70% unchanged
as parent)
Linagliptin Xanthine-based Not appreciably metabolised Biliary (unchanged as parent); <6% via kidney
Characteristics of DPPCharacteristics of DPP--4 Inhibitors4 Inhibitors
TR/ELB/04/2012/169TR/ELB/04/2012/169
Deacon CF, Diabetes, Obesity and Metabolism , 2011, 13: 7Deacon CF, Diabetes, Obesity and Metabolism , 2011, 13: 7––1818

11‐‐4: Trajenta, Januvia, Galvus, Onglyza, Summaries of Product 4: Trajenta, Januvia, Galvus, Onglyza, Summaries of Product Characteristics, consulted on line march 2012, www.afmps.beCharacteristics, consulted on line march 2012, www.afmps.be

DPPDPP--4 Inhibitors Have Different Durations of Action4 Inhibitors Have Different Durations of Action
% Plasma % Plasma DPPDPP--4 inhibition4 inhibition
VildagliptinVildagliptin
SitagliptinSitagliptin, ,
4040
100100
8080
00
6060
2020
PlaceboPlaceboSaxagliptin Saxagliptin (5 mg qd)(5 mg qd)
SaxagliptinSaxagliptin
Day 10Day 10
Adapted from Adapted from Boulton et alBoulton et alPoster 0606Poster 0606--P; ADA 2007 P; ADA 2007
4040
100100
8080
00
6060
2020
PlaceboPlaceboAlogliptin Alogliptin (25 mg qd)(25 mg qd)
Day 14Day 14
--2020
Adapted from Adapted from Covington et al, Covington et al, Clin Ther 2008Clin Ther 2008
4040
100100
8080
00
6060
2020
PlaceboPlaceboLinagliptin Linagliptin (5 mg qd)(5 mg qd)
Day 12Day 12
Adapted from Heise et al, Adapted from Heise et al, Diab Obes Metab 2009Diab Obes Metab 2009
% Plasma % Plasma DPPDPP--4 inhibition4 inhibition
00 44 88 1212 1616 2020 2424Time (hr)Time (hr)
AlogliptinAlogliptin
LinagliptinLinagliptin
Sitagliptin Sitagliptin (100 mg qd)(100 mg qd)PlaceboPlacebo
00 44 88 1212 1616 2020 2424Time (hr)Time (hr)
00
2020
40406060
8080
100100
Nb: No direct comparisons of degree of inhibition Nb: No direct comparisons of degree of inhibition attained by different inhibitors attained by different inhibitors
Adapted from HeAdapted from He et alet alJ Clin Pharmacol 2007 J Clin Pharmacol 2007
100100
8080
6060
4040
202000
Day 1Day 1
Vilda Vilda (50 mg)(50 mg)PlaceboPlacebo
Vilda Vilda (100 mg)(100 mg)
Deacon CF, Diabetes, Obesity and Metabolism , 2011, 13: 7Deacon CF, Diabetes, Obesity and Metabolism , 2011, 13: 7––1818
Adapted from Bergman et alAdapted from Bergman et alClin Ther 2006Clin Ther 2006..

Selectivity QPP/DPP II PEP FAPα DPP-8 DPP-9
Sitagliptin High >5 550 >5 550 >5 550 >2 660 >5 550
Vildagliptin Moderate >100 000 60 000 285 270 32
Saxagliptin Moderate >50 000 ? >4 000 390 77
Alogliptin High >14 000 >14 000 >14 000 >14 000 >14 000
Linagliptin Moderate >100 000 >100 000 89 40 000 >10 000
DPPDPP--4 Inhibitor 4 Inhibitor in vitro in vitro SelectivitySelectivity(Fold Selectivity for DPP(Fold Selectivity for DPP--4 vs Other Enzymes4 vs Other Enzymes))

Sitagliptine + MetformineSitagliptine + Metformine
7,0
7,2
7,4
7,6
7,8
8,0
8,2
0 6 12 18 24
Semaines
HbA1C
Placebo (n=224)
Sitagliptine 100 mg (n=453)
0 6 12 18 24
8.0
8.5
9.0
9.5
10.0
10.5
Semaines
Placebo (n=226)
Sitagliptine 100 mg (n=454)
Glycémie à jeun
Sitagliptine + Metformine vs. Metformine + Placebo
24 semaines
Charbonnel et al. Diabetes Care 2006; 29: 2368-2643
- 0.65 %p<0.001 - 0.9 mmol/L
p<0.001

? 1305-04-2010
VildagliptinAdd-on to metformin
Adapted from: Ferrannini E, et al. Diabetes Obes Metab. 2009;11:157-66.
Similar to glimepiride in reducing HbA1c when added to metformin
Vildagliptin100 mg/day, n = 1118 1081 1062 1081 1037 1023 992
Glimepiride upto 6 mg/day, n = 1072 1042 1011 1039 1001 989 976
0
6.50
7.00
7.25
7.50
-4 12 24 32 40 52
Vildagliptin 100 mg/day+ metformin
Glimepiride up to 6 mg/day+ metformin
Week
6.75
0 16
Mea
n H
bA
1C
(%)

Sitagliptine Sitagliptine vsvs. Sulfamides. SulfamidesH
bA
1c
(% ±
SE
)
Nauck et al. Diabetes Obes Metab 2007; 9: 194–205
Semaines
5.8
6.0
6.2
6.4
6.6
6.8
7.0
7.2
7.4
7.6
7.8
0 6 12 18 24 30 38 46 52
Sulfamide + metformine (n=411)
Sitagliptine + metformine (n=382)
Sitagliptine + Metformine vs.Glipizide + Metformine
52 semaines
- 0.67 %
Poids:Poids:--1.5 kg 1.5 kg SitagliptineSitagliptine+ 1.1 kg + 1.1 kg GlipizideGlipizide
HypoglycHypoglycéémies:mies:5 % 5 % SitagliptineSitagliptine32 % 32 %

Comparative efficacy of DPP4iComparative efficacy of DPP4i’’s vs oral antidiabetic drugs s vs oral antidiabetic drugs Head to head trials in drug naive and metforminHead to head trials in drug naive and metformin--treated patientstreated patients
•• MetforminMetformin : greater reduction in HbA1c and weight: greater reduction in HbA1c and weight•• SUSU : no significant difference in HbA1c but : no significant difference in HbA1c but greater weight gain and higher incidence of greater weight gain and higher incidence of hypohypo’’s, more s, more ““escapeescape”” with secondary increase in HbA1cwith secondary increase in HbA1c••TZD TZD : slightly greater reduction in HbA1c but : slightly greater reduction in HbA1c but greater weight gaingreater weight gain•• DPP4iDPP4i’’s s : No expected differences in efficacy in the class (shown for sa: No expected differences in efficacy in the class (shown for saxa vs sitagliptin)xa vs sitagliptin)
Mean changes in HbA1cMean changes in HbA1c
Mean changes in body weightMean changes in body weight
Scheen AJ, Diabetes & Metabolism, available on line, march 2012Scheen AJ, Diabetes & Metabolism, available on line, march 2012 TR/ELB/04/2012/169TR/ELB/04/2012/169

Résultats : effet sur l’HbA1c
- 0.6 %
p<0.001
0 %
Même diminution HbA1c en fonction des traitements prémix ou insuline basaleMême diminution HbA1c selon prise ou non de metformineMême diminution HbA1c après ajustement pour poids, BMI et race
Vilsboll et al, 2010

Linagliptine – Tolerability profile
•• Overall incidence of Adverse Events or Serious AE, with linaglipOverall incidence of Adverse Events or Serious AE, with linagliptin, was tin, was similar to placebo similar to placebo ((AEAE’’ss : 53,8% vs 55,0% , serious AE: 53,8% vs 55,0% , serious AE’’s: 2.8% vs 2.7%)s: 2.8% vs 2.7%)
•• InfectionsInfections: 19.5% Linagliptin vs 21.4% placebo: 19.5% Linagliptin vs 21.4% placebo
•• Upper respiratory tract : 3.3% vs 4.9%Upper respiratory tract : 3.3% vs 4.9%
•• Nasopharyngitis : 5.9% vs 5.1%Nasopharyngitis : 5.9% vs 5.1%
•• Urinary tract : 2.2% vs 2.7%Urinary tract : 2.2% vs 2.7%
•• Diarrhoea : 2.1% vs 2.1%Diarrhoea : 2.1% vs 2.1%
•• HeadacheHeadache : 2.9% vs 3.1%: 2.9% vs 3.1%
•• Blood and lymphatic disorders : 1.0% vs 1.2%Blood and lymphatic disorders : 1.0% vs 1.2%
•• Hypersensitivity : 0.1% vs 0.1%Hypersensitivity : 0.1% vs 0.1%
•• Hepatic enzyme increase: 0.1% vs 0.1%Hepatic enzyme increase: 0.1% vs 0.1%
•• Serum creatinine increase : 0.0% vs 0.1%Serum creatinine increase : 0.0% vs 0.1%
•• Chronic pancreatitis Chronic pancreatitis : 1 patient Linagliptin : 1 patient Linagliptin
•• Neoplasms Neoplasms benign, malignant and unspecified : 0.2% vs 0.5%benign, malignant and unspecified : 0.2% vs 0.5%
•• Less discontinuation of study drug with linagliptin because ofLess discontinuation of study drug with linagliptin because of AEAE’’s s : 2.2% vs 2.9% placebo: 2.2% vs 2.9% placebo
Pooled analysis of 8 monotherapy and combination trials vs plaPooled analysis of 8 monotherapy and combination trials vs placebocebo2523 patients on linagliptin vs 1049 patients on placebo2523 patients on linagliptin vs 1049 patients on placebo
Schernthaner G et al , Diab Obes Metab 2012, available on line, Schernthaner G et al , Diab Obes Metab 2012, available on line, april 2012april 2012
including including hypoglycemiahypoglycemia and and weightweight

BMS/AZ Highly Confidential - For training purposes only- Not be copied, circulated or used in any context before approval from BMS and before the Marketing Authorization for Saxagliptin has been granted
? 1305-04-2010
Cardiovascular events: Saxagliptin controlled Phase 2b/3 pooled population
Patients at risk
Control 1,251 935 860 774 545 288 144 123 102 57All saxagliptin 3,356 2,615 2,419 2,209 1,638 994 498 436 373 197
All saxagliptin
Control
Time to onset of first primary Major Adverse Cardiovascular Event (MACE)
0 24 37 50 63 76 89 102 115 1280
1
2
3
4
5
Weeks
Firs
t ad
vers
e ev
ent
(%)
Saxagliptin, FDA’s Endocrinologic and Metabolic Drugs Advisory Committee Briefing Document for April 2009 Meeting: NDA 22-350. Available at http://www.fda.gov/OHRMS/DOCKETS/ac/09/briefing/2009-4422b1-02-Bristol.pdf. Accessed: 7 May, 09.

Risk ratio for major CV eventsRisk ratio for major CV events11‐‐55
11. . Johansen OJohansen O‐‐E., et al. E., et al. Cardiovascular Diabetology 2012, 11:3; Cardiovascular Diabetology 2012, 11:3; 2. 2. WilliamsWilliams‐‐Herman D, et al. Herman D, et al. BMC Endocr DisordBMC Endocr Disord. 2010;10:7. 2010;10:7..3. 3. Schweizer A, et al. Schweizer A, et al. Diabetes Obes MetabDiabetes Obes Metab. 2010;12(6):485. 2010;12(6):485––494494; ; 4. 4. Frederich R, et al. Frederich R, et al. Postgrad MedPostgrad Med. 2010;122(3):16. 2010;122(3):16––2727;;5. 5. White et al. 2010, ADA Scientific Sessions. Abstract 391White et al. 2010, ADA Scientific Sessions. Abstract 391‐‐PPPP
Total patients Total patients in analysisin analysis
5,2395,239
10,24610,246
10,98810,988
4,6074,607
3,4893,489
PrimaryPrimaryendpointendpoint
CV death, MI, stroke,CV death, MI, stroke,hospitalisation due to hospitalisation due to angina pectorisangina pectoris
Med DRA termsMed DRA termsfor MACEfor MACE
Acute coronary syndrome, Acute coronary syndrome, transient ischaemic attack, transient ischaemic attack, stroke, CV deathstroke, CV death
MI, stroke, CV deathMI, stroke, CV death
NonNon‐‐fatal MI, nonfatal MI, non‐‐fatalfatalstroke, CV deathstroke, CV death
CommentsComments
PrePre‐‐specified/specified/independent independent adjudicationadjudication
No formal No formal adjudication;adjudication;PostPost‐‐hoc analysishoc analysis
PrePre‐‐specified/specified/Independent Independent adjudicationadjudication
PrePre‐‐specified/specified/Independent Independent adjudicationadjudication
PrePre‐‐specified/specified/Independent Independent adjudicationadjudication
DPPDPP‐‐4 inhibitor better4 inhibitor better Comparator betterComparator better
111/21/21/41/41/81/8 22 44 88
LinagliptinLinagliptin11
SitagliptinSitagliptin22
VildagliptinVildagliptin33
SaxagliptinSaxagliptin44
AlogliptinAlogliptin55
0.340.34
0.680.68
0.840.84
0.420.42
0.630.63
0.150.15 0.740.74
0.410.41 1.121.12
0.620.62 1.141.14
0.230.23 0.800.80
0.210.21 1.191.19
No increased risk of CV events was observed in patients No increased risk of CV events was observed in patients treated with DPPtreated with DPP--4 inhibitors 4 inhibitors ( retrospective analyses of existing trials)( retrospective analyses of existing trials)

Rapid Inactivation (1–2 minutes) of GLP-1
DPP-4: Dipeptidyl peptidase-4.Adapted from Drucker DJ Expert Opin Invest Drugs 2003;12(1):87–100; Ahrén B Curr Diab Rep 2003;3:365–372.
IntestinalGLP-1release
GLP-1 (9-36)inactive
Mixed meal
GLP-1 (7-36)Active
(half-life <2 mins)
DPP-4inhibitor
DPP-4

Analogue du GLP-1 humain97% d’homologie
Analogue GLP-1 d’origine animale 53% homologie/ GLP-1 humain
44 AA
Analogues du GLP-1 :Structure et origine
Analogue du GLP-1 humain97% d’homologie
31 AARésistance à la dégradation par les DPP-4
- Auto-aggrégation- Liaison à l’albumine
Demi-vie longue (t½= 13 h)
Lixisenatide ( Lyxumia Lixisenatide ( Lyxumia ))

LEAD programme: reductions in HbA1c when adding liraglutide
Chan
ge
in H
bA
1c
(%)
SU combination
LEAD-1
Met combination
LEAD-2
Met + TZD combination
LEAD-4
−1.3*
−1.5*−1.5*
Monotherapy
LEAD-3
51% 43%
−1.4*−1.3
−1.1
−1.6*
−1.2*
−1.5*
Change in HbA1c from baseline for: overall population (LEAD-4,-5); add-on to diet and exercise failure (LEAD-3); add-on to previous oral antidiabetic (OAD) monotherapy (LEAD-2,-1); or add-on to met and/or SU (LEAD-6).; *Significant vs. comparator
−0.9
−1.3
−0.8
−1.1
−0.5
8.3 8.18.68.58.38.68.58.2 8.28.6 8.6 8.48.4 8.4
−1.1*
−0.8
Met and/or SU
LEAD-6
8.2 8.1
Liraglutide 1.8 mgLiraglutide 1.2 mg Glimepiride Rosiglitazone Glargine Placebo Exenatide
0.0
−0.2
−0.4
−0.6
−1.0
−1.2
−1.4
−1.6
Met + SU combination
LEAD-5 Baseline A1c %
Marre et al. Diabetic Medicine 2009;10.1111/j.1464-5491.2009.02666.x (LEAD-1); Nauck et al. Diabetes Care 2009;32;84–90 (LEAD-2); Garber et al. Lancet 2009;373:473–81 (LEAD-3); Zinman et al. Diabetologia 2008;51(Suppl. 1):S359 (A898) (LEAD-4); Russell-Jones et al. Diabetes 2008;57(Suppl. 1):A159 (LEAD-5); Blonde et al. Can J Diabetes 2008;32 (Suppl.):A107 (LEAD-6)
−0.8

40BY/ELB/11/2009/462
HbA1c Evolution
-1.2%
7,7
Results are presented as mean and (standard deviation) Buysschaert et al ,2010

41BY/ELB/11/2009/462
Weight evolution
All changes from baseline : p< 0.001
Results are presented as mean and (standard deviation)

Results
T0 T6 p
HOMA-B (%) 33 ± 24 43 ± 23 0.0210
HOMA-S (%) 58 ± 35 61 ± 40 0.6150
Product BxS (%) 15 ± 7.0 22 ± 15.0 0.0055
in the fasting state, after discontinuation for 24h of all antihyperglycemic drugs,including exenatide.
Preumont et al, 2010Preumont et al, 2010

BY/ELB/12/2008/486 43
Change in Weight and HbA1c Over 3-Years of Exenatide
N=217 Mean±SE
Baseline 99.3 ± 1.2 kg
0 26 52 78 104 130 156-6
-4
-2
0 Week 156-5.3 kg (95% CI: -6.0 to -4.5 kg)
Treatment (week)
Wei
ght C
hang
e fr
om B
asel
ine
(kg)
Klonoff DC, et al. Curr Med Res Opin 2008;24:275-286.
HbA
0 26 52 78 104 130 1564
5
6
7
8
9
10Baseline 8.2 ± 0.1%
Week 156-1.0% (95% CI:-1.1 to -0.8%)
Treatment (week)1c
(%)

44BY/ELB/11/2009/462
ABDOMINAL PAIN UPPER: 2 (0.70%)
ADVERSE EVENT: 6 (2.1%)
BLOOD AMYLASE INCREASED: 1 (0.35%)
CHOLECYSTITIS: 1 (0.35%)
DUODENAL ULCER: 1 (0.35%)
DYSPNOEA: 1 (0.35%)
FOOD AVERSION: 1 (0.35%)
GASTROINTESTINAL DISORDER: 64 (22.5 %)
• 31% had Nausea-gastrointestinal disorder
• 3.5% had Hypoglycemia
SAFETY
HYPERSENSITIVITY: 1 (0.35%)
HYPOGLYCEMIA: 10 (3.5%)
INJECTION SITE REACTION: 1 (0.35%)
LIPASE INCREASED : 1 (0.35%)
NAUSEA: 21 (7.4%)
OEDEMA : 1 (0.35%)
SKIN REACTION: 1 (0.35%)
URTICARIA: 1 (0.35%)
VOMITING: 2 (0.70%)
• 93 patients (33%) reported any adverse effect (safety set n=284)
Data on file


Preumont, Baeck, Dumoutier et Buysschaert, SFD,2013Preumont, Baeck, Dumoutier et Buysschaert, SFD,2013

Gæde P. et al. New Eng J Med 2008, 358 (6): 580-591.
STENO-2 FOLLOW-UP: résultats après 13.3 années

48BY/ELB/11/209/462