Embed Size (px)
Citation preview

Original articleArticle original
� 2011 CEOPublished by / Edite par Elsevier Masson SAS
All rights reserved / Tous droits reserves
Variation with age of dental cephalometricvariables in Class II, division 2 patients
Modifications avec l’age des variables dentairesc�ephalom�etriques chez des patients en classe II/2
Nikolaos TOPOUZELIS*, Eleni MARKOVITSI, Andreas ZAFIRIADIS
Department of Orthodontics, Dental School, Aristotle University of Thessaloniki, 54124Thessaloniki, Greece
Available online: 24 August 2011 / Disponible en ligne : 24 aout 2011
SummaryThe treatment of Angle Class II/2 malocclusion requires anunderstanding not only of the dental and maxillofacial featuresbut also of the changes occurring with age in the dental rela-tionships. This paper attempts to determine certain dental rela-tionships in patients with Angle II/2 malocclusion and anychanges that might occur with age. The study material included96 lateral cephalometric X-rays of patients with Angle II/2malocclusion, the youngest of whom was 7 years old and theeldest 35. Six cephalometric measurements were performed onevery cephalometric X-ray. Statistical processing of dataincluded one-variable analyses and correlations of two vari-ables. Statistical one-variable analysis used methods fromdescriptive statistics. Methods of inferential statistics have beenapplied in order to revel statistical significance. The evaluationof the findings of this research study concluded that, in patientswith Angle II/2 malocclusion, maxillary central incisors pre-sented pronounced palatal tipping, which exacerbated signifi-cantly with age, while mandibular incisors displayed reducedlabial tipping and projection, which significantly reduced withage. Furthermore, it was found that there was pronouncedincisor overjet, which increased with age, due to increasedprotrusion of mandibular incisors.
� 2011 CEO. Published by Elsevier Masson SAS. All rightsreserved
110
R�esum�e
Le traitement des malocclusions de Class II/2 d’Angle requiertune bonne connaissance non seulement des aspects den-taires et maxillofaciaux mais �egalement des changementsqui se produisent avec l’age au niveau des relations dentaires.Cet article tente de d�eterminer certaines relations dentaireschez des patients avec une malocclusion de la Classe II/2d’Angle ainsi que les changements qui peuvent se produireavec l’age. Les documents utilis�es comprenaient 96t�el�eradiographies lat�erales de patients pr�esentant une mal-occlusion de Classe II/2 d’Angle, dont le plus jeune avait septans et le plus ag�e 35 ans. Six mesures c�ephalom�etriques ont�et�e r�ealis�ees sur chaque t�el�eradiographie. Le traitement sta-tistique des donn�ees comprenait des analyses univariables etdes corr�elations entre deux variables. L’analyse statistiqueunivariable utilisait des m�ethodes emprunt�ees a la statistiquedescriptive. La statistique inf�erentielle a permis de d�eterminerla signification statistique. L’�evaluation des r�esultats de notrerecherche a r�ev�el�e que, chez les patients ayant une maloc-clusion de Classe II/2 d’Angle, les incisives centrales maxil-laires pr�esentaient une version corono-palatine prononc�eequi s’aggravait de facon significative avec l’age, alors queles incisives mandibulaires montraient une version corono-vestibulaire et une projection ant�erieure, qui diminuaient defacon significative avec l’age. Par ailleurs, nous avons trouv�eun overjet prononc�e du secteur ant�erieur, qui augmentait avecl’age en raison de l’aggravation de la protrusion des incisivesmandibulaires.� 2011 CEO. Edite par Elsevier Masson SAS. Tous droitsreserves
*Correspondence and reprints / Correspondance et tir�es a part :
Nikolaos TOPOUZELIS, Department of Orthodontics, Dental School, AristotleUniversity of Thessaloniki, 54124 Thessaloniki, Greece.e-mail address / Adresse e-mail : [email protected]
International Orthodontics 2012 ; 10 : 110-121doi:10.1016/j.ortho.2011.07.003

Variation with age of dental cephalometric variables in Class II, division 2 patientsModifications avec l’age des variables dentaires c�ephalom�etriques chez des patients en classe II/2
Key-words
·Class II/2.
·Dental relationship. ·Cephalometric analysis. ·Age.Introduction
Maxillodental features and the type and evolution of maxillo-facial growth are decisive factors for the treatment planning ofmaxillodental disorders.It is believed that the appearance of Angle II/2 malocclusion isaffected by heredity; there is a combined expression of genet-ically-determined anatomical features involving more than asingle gene, which controls this type of malocclusion [1].There is also evidence supporting a view that Angle II/2malocclusion is not a primary skeletal syndrome but a dys-morphy mainly due to intense palatal tipping of maxillarycentral incisors [2–9].
This palatal tipping is attributed to the position and function ofthe lower lip, which affects permanent maxillary incisors assoon as they erupt [10,11], and to the fact that there isincreased peri-oral muscular force in individuals with AngleII/2 malocclusion disorders [12–14]. This palatal tipping alsodepends on the overjet scale [15]. As for the increased over-bite, this has been attributed to protrusion of anterior teeth,retrusion of posterior teeth or a combination of the two [16].Other papers indicate a normal position in the vertical relationof maxillary and mandibular incisors [10,17–19], while someresearchers assume that increased overjet is the result ofskeletal rather than dentoalveolar etiology [19,20].
These various views on the dental features of Angle II/2 dis-orders lead to a need for further investigation into such dis-orders and, particularly, their development with age, which isas important and relevant for the needs of clinical orthodon-tists as an accurate and well-defined description of themalocclusion.
The aims of the study are:— to examine possible differences in dental cephalometricmeasurements among the three age groups of Angle Class IIdivision 2 malocclusion patients;— to investigate possible correlations between patient ageand those cephalometric measurements examined.
Subjects and methods
Research material included 96 lateral cephalometric X-raysof Angle Class II, division 2 malocclusion patients who had
International Orthodontics 2012 ; 10 : 110-121
Mots-cl�es
·Classe II/2.
·Relation dentaire.� �
·Analyse cephalometrique.ˆ
·Age.Introduction
Les �el�ements maxillofaciaux, ainsi que le type et l’�evolution dela croissance maxillofaciale, sont des facteurs d�ecisifs pour letraitement des troubles maxillofaciaux.Il est g�en�eralement consid�er�e que l’av�enement d’une maloc-clusion de Classe II/2 est influenc�e par l’h�er�edit�e. En effet, cetype de malocclusion est d�etermin�e par l’expression conjointede ph�enom�enes anatomiques g�en�etiquement conditionn�esimpliquant plus d’un g�ene [1]. Il existe �egalement des indica-tions probantes qui laissent croire que la Classe II/2 d’Anglen’est pas un syndrome squelettique primaire mais une dys-morphose due principalement a la version corono-palatinemarqu�ee des incisives centrales maxillaires [2–9].Cette version corono-palatine est attribu�ee a la position et a lafonction de la l�evre inf�erieure, qui influe sur les incisivessup�erieures permanentes d�es leur �eruption [10,11] ainsiqu’a l’augmentation de la force musculaire p�eri-orale chezles sujets pr�esentant des troubles li�es a une malocclusion deClasse II/2 [12–14]. Cette version corono-palatine d�epend�egalement de l’importance du d�ecalage sagittal [15]. Quanta l’augmentation de la supraclusion, celle-ci a �et�e attribu�eea la protrusion des dentsmaxillaires ant�erieures, a la r�etrusiondes dents mandibulaires ou a une combinaison des deux [16].Des �etudes ont observ�e une position normale dans la relationverticale des incisives maxillaires et mandibulaires [10,17–19], alors que certains chercheurs ont conclu que l’aug-mentation de l’overjet est le r�esultat d’une �etiologie squelet-tique plutot que dento-alv�eolaire [19,20].Ces diff�erents points de vue a l’�egard des caract�eristiquesdentaires desmalocclusions de Classe II/2 d’Angle soulignentle besoin de recherches suppl�ementaires autour de tellesanomalies. En particulier, en ce qui concerne leur �evolutionavec l’age, facteur aussi important et pertinent pour la cliniqueorthodontique qu’une description pr�ecise et bien d�efinie decette malocclusion.Les objectifs de cette �etude sont :— d’�etudier les diff�erences �eventuelles entre les mesuresdentaires et c�ephalom�etriques chez des patients en ClasseII/2 d’Angle et r�epartis en trois groupes d’age ;— d’examiner les corr�elations �eventuelles entre l’age despatients et les mesures c�ephalom�etriques �etudi�ees.
Sujets et m�ethodes
Le mat�eriel de recherche comprenait 96 t�el�eradiographiessagittales de patients en Classe II, division 2 d’Angle et qui
111
Nikolaos TOPOUZELIS et al.
never had any type of orthodontic treatment. Selection wasbased on dental occlusion relationships and patients’ ages, outof a total number of 174 cases of Angle Class II, division 2malocclusion patients who asked for orthodontic treatment.The X-rays of patients selected were divided into three groups.
The first one was a children’s group and included 33 X-rays ofpatients, 13 of whom were boys and 20 of whom were girls.Mean age was 9.5 years. The youngest was 7 and the oldest11 years old. Their dentition was mixed and there was no caseof having lost a deciduous tooth early or missing a permanenttooth.The second one was the group of adolescents, which included31 X-rays of patients; 13 of them were boys and 18 were girls.Mean age was 14 years. The youngest was 13 and the oldest15.5 years. Their dentition was permanent and there was notooth missing in any of the cases.The third one was the adults’ group and included 32 X-rays ofpatients, 11 of whom were men and 21 women. Mean age was21 years. The youngest was 17 and the oldest 35 years of age.Their dentition was permanent and there was no tooth missingin any of the cases.
Cephalometric variables
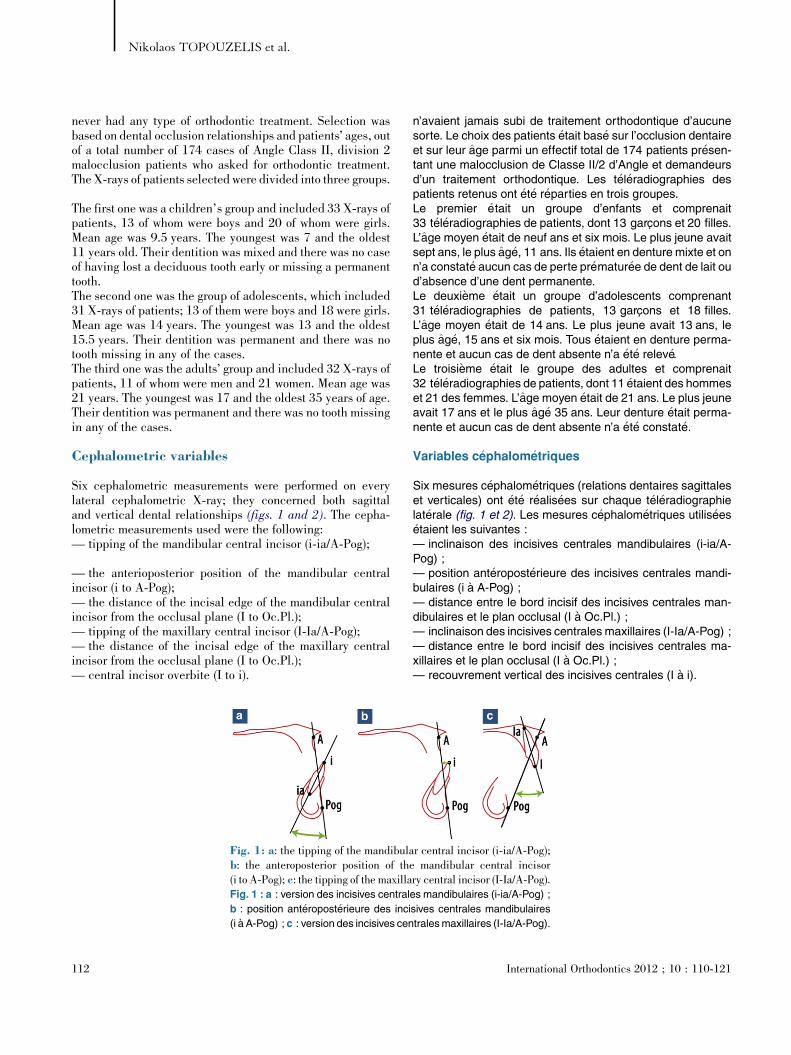
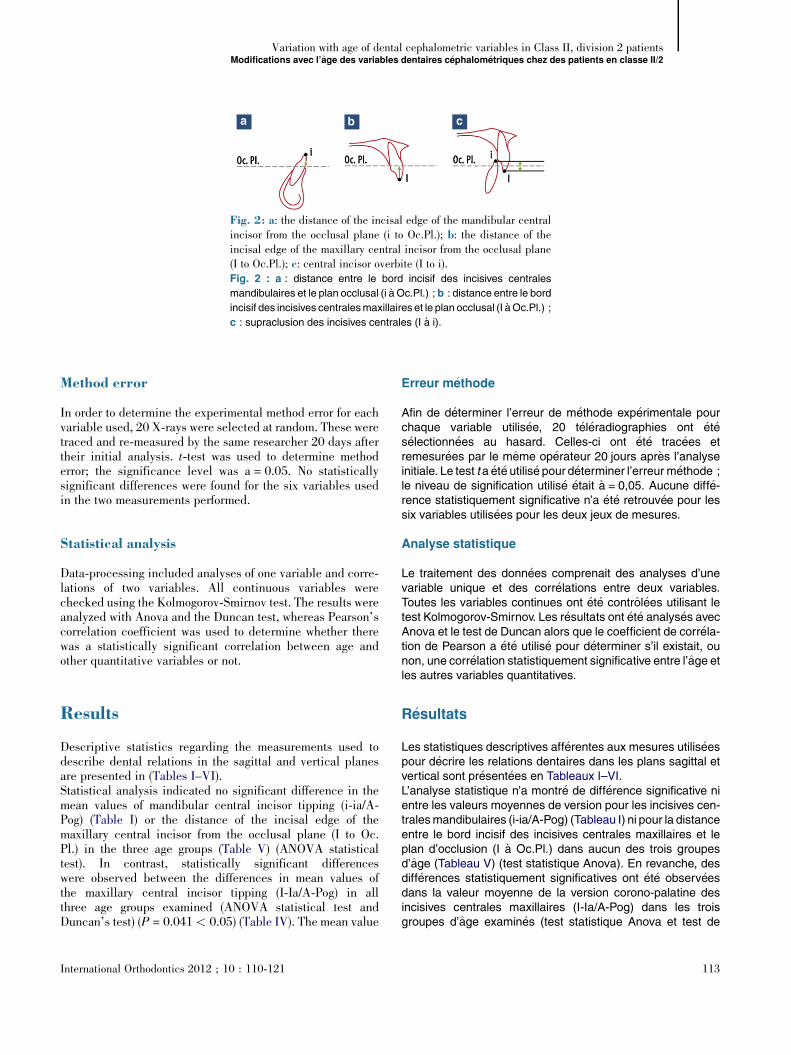
Six cephalometric measurements were performed on everylateral cephalometric X-ray; they concerned both sagittaland vertical dental relationships (figs. 1 and 2). The cepha-lometric measurements used were the following:— tipping of the mandibular central incisor (i-ia/A-Pog);
— the anterioposterior position of the mandibular centralincisor (i to A-Pog);— the distance of the incisal edge of the mandibular centralincisor from the occlusal plane (I to Oc.Pl.);— tipping of the maxillary central incisor (I-Ia/A-Pog);— the distance of the incisal edge of the maxillary centralincisor from the occlusal plane (I to Oc.Pl.);— central incisor overbite (I to i).
[(Fig._1)TD$FIG]
Fig. 1: a: the tipping of the mandibulab: the anteroposterior position of the(i to A-Pog); c: the tipping of the maxillaFig. 1 : a : version des incisives central
b : position ant�eropost�erieure des inci
(i a A-Pog) ; c : version des incisives cen
112
n’avaient jamais subi de traitement orthodontique d’aucunesorte. Le choix des patients �etait bas�e sur l’occlusion dentaireet sur leur age parmi un effectif total de 174 patients pr�esen-tant une malocclusion de Classe II/2 d’Angle et demandeursd’un traitement orthodontique. Les t�el�eradiographies despatients retenus ont �et�e r�eparties en trois groupes.Le premier �etait un groupe d’enfants et comprenait33 t�el�eradiographies de patients, dont 13 garcons et 20 filles.L’age moyen �etait de neuf ans et six mois. Le plus jeune avaitsept ans, le plus ag�e, 11 ans. Ils �etaient en denture mixte et onn’a constat�e aucun cas de perte pr�ematur�ee de dent de lait oud’absence d’une dent permanente.Le deuxi�eme �etait un groupe d’adolescents comprenant31 t�el�eradiographies de patients, 13 garcons et 18 filles.L’age moyen �etait de 14 ans. Le plus jeune avait 13 ans, leplus ag�e, 15 ans et six mois. Tous �etaient en denture perma-nente et aucun cas de dent absente n’a �et�e relev�e.Le troisi�eme �etait le groupe des adultes et comprenait32 t�el�eradiographies de patients, dont 11 �etaient des hommeset 21 des femmes. L’age moyen �etait de 21 ans. Le plus jeuneavait 17 ans et le plus ag�e 35 ans. Leur denture �etait perma-nente et aucun cas de dent absente n’a �et�e constat�e.
Variables c�ephalom�etriques
Six mesures c�ephalom�etriques (relations dentaires sagittaleset verticales) ont �et�e r�ealis�ees sur chaque t�el�eradiographielat�erale (fig. 1 et 2). Les mesures c�ephalom�etriques utilis�ees�etaient les suivantes :— inclinaison des incisives centrales mandibulaires (i-ia/A-Pog) ;— position ant�eropost�erieure des incisives centrales mandi-bulaires (i a A-Pog) ;— distance entre le bord incisif des incisives centrales man-dibulaires et le plan occlusal (I a Oc.Pl.) ;— inclinaison des incisives centrales maxillaires (I-Ia/A-Pog) ;— distance entre le bord incisif des incisives centrales ma-xillaires et le plan occlusal (I a Oc.Pl.) ;— recouvrement vertical des incisives centrales (I a i).
r central incisor (i-ia/A-Pog);mandibular central incisor
ry central incisor (I-Ia/A-Pog).es mandibulaires (i-ia/A-Pog) ;
sives centrales mandibulaires
tralesmaxillaires (I-Ia/A-Pog).
International Orthodontics 2012 ; 10 : 110-121
[(Fig._2)TD$FIG]
Fig. 2: a: the distance of the incisal edge of the mandibular centralincisor from the occlusal plane (i to Oc.Pl.); b: the distance of theincisal edge of the maxillary central incisor from the occlusal plane(I to Oc.Pl.); c: central incisor overbite (I to i).Fig. 2 : a : distance entre le bord incisif des incisives centrales
mandibulaires et le plan occlusal (i a Oc.Pl.) ; b : distance entre le bord
incisif des incisives centralesmaxillaires et le plan occlusal (I a Oc.Pl.) ;
c : supraclusion des incisives centrales (I a i).
Variation with age of dental cephalometric variables in Class II, division 2 patientsModifications avec l’age des variables dentaires c�ephalom�etriques chez des patients en classe II/2
Method error
In order to determine the experimental method error for eachvariable used, 20 X-rays were selected at random. These weretraced and re-measured by the same researcher 20 days aftertheir initial analysis. t-test was used to determine methoderror; the significance level was a = 0.05. No statisticallysignificant differences were found for the six variables usedin the two measurements performed.
Statistical analysis
Data-processing included analyses of one variable and corre-lations of two variables. All continuous variables werechecked using the Kolmogorov-Smirnov test. The results wereanalyzed with Anova and the Duncan test, whereas Pearson’scorrelation coefficient was used to determine whether therewas a statistically significant correlation between age andother quantitative variables or not.
Results
Descriptive statistics regarding the measurements used todescribe dental relations in the sagittal and vertical planesare presented in (Tables I–VI).Statistical analysis indicated no significant difference in themean values of mandibular central incisor tipping (i-ia/A-Pog) (Table I) or the distance of the incisal edge of themaxillary central incisor from the occlusal plane (I to Oc.Pl.) in the three age groups (Table V) (ANOVA statisticaltest). In contrast, statistically significant differenceswere observed between the differences in mean values ofthe maxillary central incisor tipping (I-Ia/A-Pog) in allthree age groups examined (ANOVA statistical test andDuncan’s test) (P = 0.041 < 0.05) (Table IV). The mean value
International Orthodontics 2012 ; 10 : 110-121
Erreur m�ethode
Afin de d�eterminer l’erreur de m�ethode exp�erimentale pourchaque variable utilis�ee, 20 t�el�eradiographies ont �et�es�electionn�ees au hasard. Celles-ci ont �et�e trac�ees etremesur�ees par le meme op�erateur 20 jours apr�es l’analyseinitiale. Le test t a �et�e utilis�e pour d�eterminer l’erreur m�ethode ;le niveau de signification utilis�e �etait a = 0,05. Aucune diff�e-rence statistiquement significative n’a �et�e retrouv�ee pour lessix variables utilis�ees pour les deux jeux de mesures.
Analyse statistique
Le traitement des donn�ees comprenait des analyses d’unevariable unique et des corr�elations entre deux variables.Toutes les variables continues ont �et�e control�ees utilisant letest Kolmogorov-Smirnov. Les r�esultats ont �et�e analys�es avecAnova et le test de Duncan alors que le coefficient de corr�ela-tion de Pearson a �et�e utilis�e pour d�eterminer s’il existait, ounon, une corr�elation statistiquement significative entre l’age etles autres variables quantitatives.
R�esultats
Les statistiques descriptives aff�erentes aux mesures utilis�eespour d�ecrire les relations dentaires dans les plans sagittal etvertical sont pr�esent�ees en Tableaux I–VI.L’analyse statistique n’a montr�e de diff�erence significative nientre les valeurs moyennes de version pour les incisives cen-tralesmandibulaires (i-ia/A-Pog) (Tableau I) ni pour la distanceentre le bord incisif des incisives centrales maxillaires et leplan d’occlusion (I a Oc.Pl.) dans aucun des trois groupesd’age (Tableau V) (test statistique Anova). En revanche, desdiff�erences statistiquement significatives ont �et�e observ�eesdans la valeur moyenne de la version corono-palatine desincisives centrales maxillaires (I-Ia/A-Pog) dans les troisgroupes d’age examin�es (test statistique Anova et test de
113
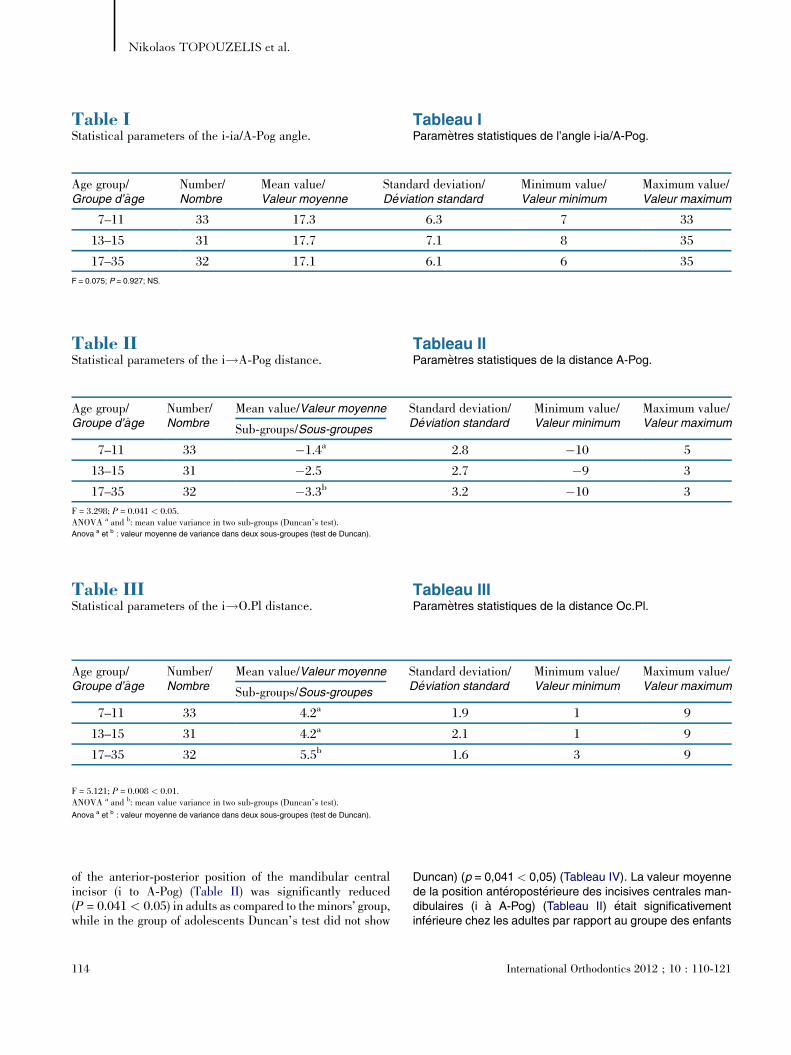
Table IStatistical parameters of the i-ia/A-Pog angle.
Tableau IParam�etres statistiques de l’angle i-ia/A-Pog.
Age group/Groupe d’age
Number/Nombre
Mean value/Valeur moyenne
Standard deviation/D�eviation standard
Minimum value/Valeur minimum
Maximum value/Valeur maximum
7–11 33 17.3 6.3 7 33
13–15 31 17.7 7.1 8 35
17–35 32 17.1 6.1 6 35
F = 0.075; P = 0.927; NS.
Table IIIStatistical parameters of the i!O.Pl distance.
Tableau IIIParam�etres statistiques de la distance Oc.Pl.
Age group/Groupe d’age
Number/Nombre
Mean value/Valeur moyenne Standard deviation/D�eviation standard
Minimum value/Valeur minimum
Maximum value/Valeur maximumSub-groups/Sous-groupes
7–11 33 4.2a 1.9 1 9
13–15 31 4.2a 2.1 1 9
17–35 32 5.5b 1.6 3 9
F = 5.121; P = 0.008 < 0.01.ANOVA a and b: mean value variance in two sub-groups (Duncan’s test).
Anova a et b : valeur moyenne de variance dans deux sous-groupes (test de Duncan).
Table IIStatistical parameters of the i!A-Pog distance.
Tableau IIParam�etres statistiques de la distance A-Pog.
Age group/Groupe d’age
Number/Nombre
Mean value/Valeur moyenne Standard deviation/D�eviation standard
Minimum value/Valeur minimum
Maximum value/Valeur maximumSub-groups/Sous-groupes
7–11 33 �1.4a 2.8 �10 5
13–15 31 �2.5 2.7 �9 3
17–35 32 �3.3b 3.2 �10 3
F = 3.298; P = 0.041 < 0.05.ANOVA a and b: mean value variance in two sub-groups (Duncan’s test).Anova a et b : valeur moyenne de variance dans deux sous-groupes (test de Duncan).
Nikolaos TOPOUZELIS et al.
of the anterior-posterior position of the mandibular centralincisor (i to A-Pog) (Table II) was significantly reduced(P = 0.041 < 0.05) in adults as compared to the minors’ group,while in the group of adolescents Duncan’s test did not show
114
Duncan) (p = 0,041 < 0,05) (Tableau IV). La valeur moyennede la position ant�eropost�erieure des incisives centrales man-dibulaires (i a A-Pog) (Tableau II) �etait significativementinf�erieure chez les adultes par rapport au groupe des enfants
International Orthodontics 2012 ; 10 : 110-121
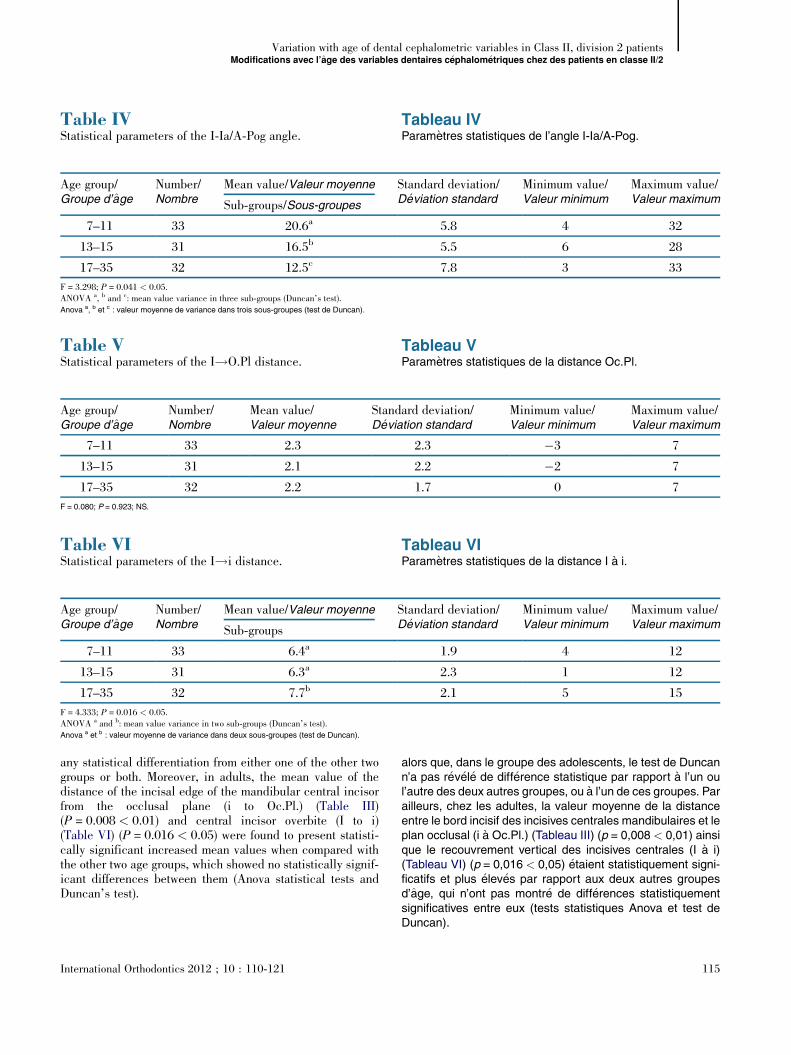
Table VIStatistical parameters of the I!i distance.
Tableau VIParam�etres statistiques de la distance I a i.
Age group/Groupe d’age
Number/Nombre
Mean value/Valeur moyenne Standard deviation/D�eviation standard
Minimum value/Valeur minimum
Maximum value/Valeur maximumSub-groups
7–11 33 6.4a 1.9 4 12
13–15 31 6.3a 2.3 1 12
17–35 32 7.7b 2.1 5 15
F = 4.333; P = 0.016 < 0.05.ANOVA a and b: mean value variance in two sub-groups (Duncan’s test).Anova a et b : valeur moyenne de variance dans deux sous-groupes (test de Duncan).
Table IVStatistical parameters of the I-Ia/A-Pog angle.
Tableau IVParam�etres statistiques de l’angle I-Ia/A-Pog.
Age group/Groupe d’age
Number/Nombre
Mean value/Valeur moyenne Standard deviation/D�eviation standard
Minimum value/Valeur minimum
Maximum value/Valeur maximumSub-groups/Sous-groupes
7–11 33 20.6a 5.8 4 32
13–15 31 16.5b 5.5 6 28
17–35 32 12.5c 7.8 3 33
F = 3.298; P = 0.041 < 0.05.ANOVA a, b and c: mean value variance in three sub-groups (Duncan’s test).Anova a, b et c : valeur moyenne de variance dans trois sous-groupes (test de Duncan).
Table VStatistical parameters of the I!O.Pl distance.
Tableau VParam�etres statistiques de la distance Oc.Pl.
Age group/Groupe d’age
Number/Nombre
Mean value/Valeur moyenne
Standard deviation/D�eviation standard
Minimum value/Valeur minimum
Maximum value/Valeur maximum
7–11 33 2.3 2.3 �3 7
13–15 31 2.1 2.2 �2 7
17–35 32 2.2 1.7 0 7
F = 0.080; P = 0.923; NS.
Variation with age of dental cephalometric variables in Class II, division 2 patientsModifications avec l’age des variables dentaires c�ephalom�etriques chez des patients en classe II/2
any statistical differentiation from either one of the other twogroups or both. Moreover, in adults, the mean value of thedistance of the incisal edge of the mandibular central incisorfrom the occlusal plane (i to Oc.Pl.) (Table III)(P = 0.008 < 0.01) and central incisor overbite (I to i)(Table VI) (P = 0.016 < 0.05) were found to present statisti-cally significant increased mean values when compared withthe other two age groups, which showed no statistically signif-icant differences between them (Anova statistical tests andDuncan’s test).
International Orthodontics 2012 ; 10 : 110-121
alors que, dans le groupe des adolescents, le test de Duncann’a pas r�ev�el�e de diff�erence statistique par rapport a l’un oul’autre des deux autres groupes, ou a l’un de ces groupes. Parailleurs, chez les adultes, la valeur moyenne de la distanceentre le bord incisif des incisives centrales mandibulaires et leplan occlusal (i a Oc.Pl.) (Tableau III) (p = 0,008 < 0,01) ainsique le recouvrement vertical des incisives centrales (I a i)(Tableau VI) (p = 0,016 < 0,05) �etaient statistiquement signi-ficatifs et plus �elev�es par rapport aux deux autres groupesd’age, qui n’ont pas montr�e de diff�erences statistiquementsignificatives entre eux (tests statistiques Anova et test deDuncan).
115
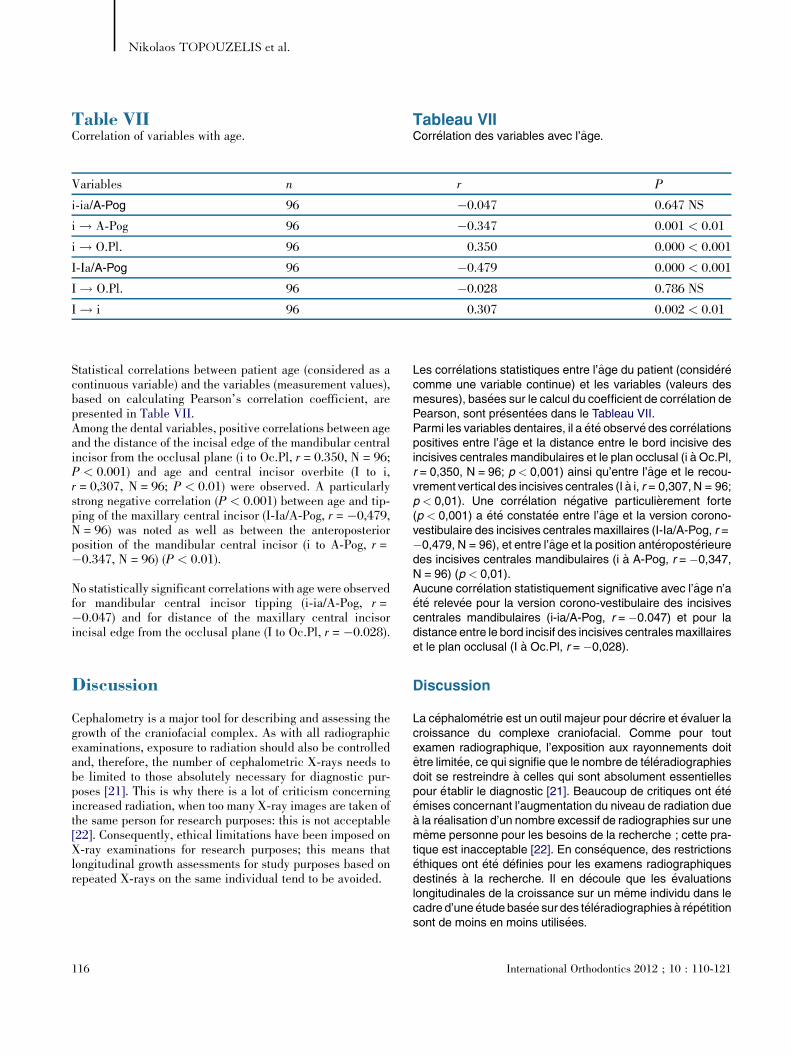
Table VIICorrelation of variables with age.
Tableau VIICorr�elation des variables avec l’age.
Variables n r P
i-ia/A-Pog 96 �0.047 0.647 NS
i ! A-Pog 96 �0.347 0.001 < 0.01
i ! O.Pl. 96 0.350 0.000 < 0.001
I-Ia/A-Pog 96 �0.479 0.000 < 0.001
I ! O.Pl. 96 �0.028 0.786 NS
I ! i 96 0.307 0.002 < 0.01
Nikolaos TOPOUZELIS et al.
Statistical correlations between patient age (considered as acontinuous variable) and the variables (measurement values),based on calculating Pearson’s correlation coefficient, arepresented in Table VII.Among the dental variables, positive correlations between ageand the distance of the incisal edge of the mandibular centralincisor from the occlusal plane (i to Oc.Pl, r = 0.350, N = 96;P < 0.001) and age and central incisor overbite (I to i,r = 0,307, N = 96; P < 0.01) were observed. A particularlystrong negative correlation (P < 0.001) between age and tip-ping of the maxillary central incisor (I-Ia/A-Pog, r = �0,479,N = 96) was noted as well as between the anteroposteriorposition of the mandibular central incisor (i to A-Pog, r =�0.347, N = 96) (P < 0.01).
No statistically significant correlations with age were observedfor mandibular central incisor tipping (i-ia/A-Pog, r =�0.047) and for distance of the maxillary central incisorincisal edge from the occlusal plane (I to Oc.Pl, r = �0.028).
Discussion
Cephalometry is a major tool for describing and assessing thegrowth of the craniofacial complex. As with all radiographicexaminations, exposure to radiation should also be controlledand, therefore, the number of cephalometric X-rays needs tobe limited to those absolutely necessary for diagnostic pur-poses [21]. This is why there is a lot of criticism concerningincreased radiation, when too many X-ray images are taken ofthe same person for research purposes: this is not acceptable[22]. Consequently, ethical limitations have been imposed onX-ray examinations for research purposes; this means thatlongitudinal growth assessments for study purposes based onrepeated X-rays on the same individual tend to be avoided.
116
Les corr�elations statistiques entre l’age du patient (consid�er�ecomme une variable continue) et les variables (valeurs desmesures), bas�ees sur le calcul du coefficient de corr�elation dePearson, sont pr�esent�ees dans le Tableau VII.Parmi les variables dentaires, il a �et�e observ�e des corr�elationspositives entre l’age et la distance entre le bord incisive desincisives centrales mandibulaires et le plan occlusal (i a Oc.Pl,r = 0,350, N = 96; p < 0,001) ainsi qu’entre l’age et le recou-vrement vertical des incisives centrales (I a i, r = 0,307, N = 96;p < 0,01). Une corr�elation n�egative particuli�erement forte(p < 0,001) a �et�e constat�ee entre l’age et la version corono-vestibulaire des incisives centralesmaxillaires (I-Ia/A-Pog, r =�0,479, N = 96), et entre l’age et la position ant�eropost�erieuredes incisives centrales mandibulaires (i a A-Pog, r = �0,347,N = 96) (p < 0,01).Aucune corr�elation statistiquement significative avec l’age n’a�et�e relev�ee pour la version corono-vestibulaire des incisivescentrales mandibulaires (i-ia/A-Pog, r = �0.047) et pour ladistance entre le bord incisif des incisives centralesmaxillaireset le plan occlusal (I a Oc.Pl, r = �0,028).
Discussion
La c�ephalom�etrie est un outil majeur pour d�ecrire et �evaluer lacroissance du complexe craniofacial. Comme pour toutexamen radiographique, l’exposition aux rayonnements doitetre limit�ee, ce qui signifie que le nombre de t�el�eradiographiesdoit se restreindre a celles qui sont absolument essentiellespour �etablir le diagnostic [21]. Beaucoup de critiques ont �et�e�emises concernant l’augmentation du niveau de radiation duea la r�ealisation d’un nombre excessif de radiographies sur unememe personne pour les besoins de la recherche ; cette pra-tique est inacceptable [22]. En cons�equence, des restrictions�ethiques ont �et�e d�efinies pour les examens radiographiquesdestin�es a la recherche. Il en d�ecoule que les �evaluationslongitudinales de la croissance sur un meme individu dans lecadre d’une �etude bas�ee sur des t�el�eradiographies a r�ep�etitionsont de moins en moins utilis�ees.
International Orthodontics 2012 ; 10 : 110-121

Variation with age of dental cephalometric variables in Class II, division 2 patientsModifications avec l’age des variables dentaires c�ephalom�etriques chez des patients en classe II/2
This study mainly aimed at studying Angle II/2 malocclusiondevelopment over time and at determining the improvement orexacerbation of dental relationships with age. Due to the eth-ical limitations described above, the study material comprisedinitial lateral cephalometric X-rays of patients, ranging in agefrom 7 to 35 years, who were seeking treatment for Angle II/2malocclusion.
Initially, seven cephalometric measurements were recorded todetermine dental relationships in cases of Angle Class II/2malocclusion in three age groups of patients: children, ado-lescents and adults. Then, differences between the groupswere identified and an analysis was performed, in the patientsas a whole, to determine whether the measurements used wereaffected by the age of the patients.
The tipping angle of maxillary central incisors (I-Ia/A-Pog)was found to have particularly lower values in all three groupsexamined when compared with the ‘normal’ values recom-mended [23]. This finding is confirmed by universal agree-ment in the relevant literature that patients with Angle II/2malocclusion present pronounced palatal tipping of maxillarycentral incisors [1,2,4,5,10,16,18,19,24–28], which is attrib-uted to the fact that peri-oral forces in individuals with ClassII/2 malocclusion are increased when compared with ‘normal’individuals or persons with other disorders [12–14]. Palatalcrown tipping of maxillary central incisors varied significantlyin the three groups examined, since it was pronounced amongadolescents and even more pronounced among adults whencompared with the children’s group. Furthermore, patients asa whole presented significant variance since I-Ia/A-Pogincreased with age.
The labial tipping of mandibular central incisors (i-ia/A-Pog)was found to have lower values in all three groups examinedwhen compared with the ‘normal’ values proposed [23,29,30].This concords with the view expressed by numerous authorswho describe mandibular incisors as being lingually tipped inpatients with Angle II/2 malocclusion [4,10,18]. However,there are other authors who consider the tipping of mandibularincisors ‘normal’ [1,2,27]. In their study, Brezniak et al. [19]found both: lingual tipping of mandibular incisors in relationto the inter-jaw A-Pog plane and ‘normal’ tipping in relation tothe mandibular Go-Me plane. In their view, these resultsexplain the fact that there are controversial findings in theliterature in regards to mandibular incisor tipping in patientswith Angle II/2 malocclusion.
There was no variation in mandibular incisor tipping in thethree groups examined, since the angle between the longitu-dinal axis of the mandibular incisor and the A-Pog plane,
International Orthodontics 2012 ; 10 : 110-121
Cette �etude s’est focalis�ee sur l’examen de l’�evolution dans letemps des malocclusions de la Classe II/2 d’Angle et sur lad�etermination de l’am�elioration ou de l’aggravation des rela-tions dentaires avec l’age. En raison des contraintes �ethiquespr�ec�edemment mentionn�ees, le mat�eriel de l’�etude compre-nait les t�el�eradiographies lat�erales initiales de patients ag�esde sept a 35 ans qui �etaient demandeurs de traitement pourune malocclusion de Classe II/2.Initialement, sept mesures c�ephalom�etriques ont �et�eenregistr�ees afin de d�eterminer les relations dentaires initialesdans des cas demalocclusion deClasse II/2 d’Angle chez troisgroupes de patients r�epartis selon leur tranche d’age :enfants, adolescents et adultes. Ensuite, les diff�erences entreles groupes ont �et�e identifi�ees et une analyse a �et�e effectu�ee,chez l’ensemble des patients, afin de d�eterminer si lesmesures utilis�ees ont �et�e influenc�ees par l’age des patients.L’angle de l’inclinaison des incisives centralesmaxillaires (I-Ia/A-Pog) compar�e aux valeurs « normales » recommand�ees[23], montrait des valeurs particuli�erement faibles dans lestrois groupes de l’�etude. Ce r�esultat est confirm�e par le constatuniversel dans la litt�erature pertinente que les patients avecune malocclusion de Classe II/2 d’Angle pr�esentent une ver-sion corono-palatine prononc�ee des incisives centrales ma-xillaires [1,2,4,5,10,16,18,19,24–28] qui est attribu�ee au faitque, chez les individus avec ce type de malocclusion, lesforces p�eri-orales augmentent par rapport aux individus« normaux » ou a des sujets porteurs de malocclusionsdiff�erentes [12–14]. La version corono-palatine des incisivescentralesmaxillaires variait de facon significative dans les troisgroupes examin�es puisqu’elle �etait prononc�ee chez les ado-lescents et encore plus prononc�ee chez les adultes par rap-port au groupe des enfants. Par ailleurs, les patients, dans leurensemble, ont pr�esent�e une variance significative puisque l’i-ia/A-Pog augmentait avec l’age.Il a �et�e constat�e que la version corono-vestibulaire des inci-sives centrales mandibulaires (i-ia/A-Pog) avait des valeursinf�erieures dans les trois groupes par rapport aux valeurs« normales » conventionnelles [23,29,30]. Cette observa-tion coıncide avec le point de vue exprim�e par de nombreuxauteurs qui d�ecrivent les incisives mandibulaires comme�etant en version corono-linguale chez les patients atteintsd’une malocclusion de Classe II/2 d’Angle [4,10,18].D’autres auteurs, cependant, estiment que la versioncorono-linguale des incisives mandibulaires est unph�enom�ene « normal » [1,2,27]. Dans leur �etude, Brezniaket al. [19] ont trouv�e les deux : une version corono-lingualedes incisives mandibulaires par rapport au plan maxilloman-dibulaire A-Pog et une version « normale » par rapport auplan mandibulaire Go-Me. A leur avis, ces r�esultats expli-quent l’existence de r�esultats contradictoires dans la litt�era-ture en ce qui concerne la version corono-vestibulaire desincisives mandibulaires chez les patients avec une maloc-clusion de Classe II/2.Aucune variation n’a �et�e relev�ee au niveau de la versioncorono-vestibulaire des incisives mandibulaires dans les troisgroupes de l’�etude puisque l’angle de l’axe longitudinal des
117

Nikolaos TOPOUZELIS et al.
which was the measurement assessed, presented almost thesamemean value in all three groups. Additionally, the patientsas a whole showed no variance in regards to age.
The distance of the incisal edge of the mandibular incisor fromthe inter-jaw plane A-Pog (i to A-Pog), which expresses theprojection of the mandibular incisor and reflects the antero-posterior position of the mandibular dentoloalveolar arch, wasfound to have negative mean values in all three groups whencompared with ‘normal’ recommended values, which are allpositive [23,29,30].The distance of the mandibular incisor incisal edge from theinter-jaw plane A-Pog was found to be significantly lower inthe adult group when compared to the children’s group, whilein the adolescent group this distance showed no differencewhen compared to the other two groups. This finding concordswith the old observation by Grosse-Wienker [31] that themandibular dentoalveolar arch in Angle II/2 malocclusionpatients presents restricted antero-posterior growth, which isobserved in the mixed dentition and becomes more pro-nounced in the permanent dentition. In the patients as awhole, the projection of the mandibular incisor showed nega-tive correlation with age, since the older the person, the lowerthe i to A-Pog. This finding supports the claim that in Angle II/2 cases, anterior growth of the dentoloalveolar arch is heldback and prevented by palatal tipping of maxillary incisorsand deep bite [32–36].
In the three groups examined, the distance of the maxillarycentral incisor incisal edge from the occlusal plane (I to Oc.Pl)showed no variance, since its mean value was almost the samein all three groups. Furthermore, the patients as a wholeshowed no significant variance of I to Oc.Pl with age. Thesefindings support the finding that, in the Class II/2 patientsexamined, there was no increase in the protrusion of maxillarycentral incisors with age, despite their increased palatal tip-ping and the increased incisor overbite.
The distance of the mandibular central incisors’ incisal edgefrom the occlusal plane (i to Oc.Pl), which reflects their pro-trusion, was found to have definitely higher mean values in thethree groups examined than ‘normal’ values propose [23,29].This means that Angle Class II/2 patients presented increasedprotrusion of mandibular incisors. The protrusion of mandib-ular incisors in the groups of children and adolescents showedno difference, while in the adult group this was significantlyincreased as compared to the other two groups. The patients asa whole showed a strong positive correlation regarding man-dibular incisor protrusion with age, since the older they were,the greater the protrusion. Protrusion and crowding of man-dibular incisors are attributed to anterior rotation of the man-dible with growth and restriction of the inter-canine distance,due to the fact that pronounced deep bite in Angle II/2 patients
118
incisives mandibulaires avec le plan A-Pog, qui �etait la mesure�evalu�ee, pr�esentait pratiquement la meme valeur moyennedans les trois groupes. De plus, les patients dans leur ensem-ble n’ont r�ev�el�e aucune variance en fonction de l’age.La distance entre le bord incisif des incisives mandibulaires etle plan maxillomandibulaire A-Pog (i a A-Pog), qui exprime laprojection des incisives mandibulaires et refl�ete la positionant�eropost�erieure de l’arcade dento-alv�eolaire mandibulaire,a montr�e des valeurs n�egatives dans les trois groupes parrapport aux valeurs « normales » recommand�ees, qui sonttoutes positives [23,29,30].La distance entre le bord incisif des incisives mandibulaires etle plan maxillo-mandibulaire A-Pog s’est av�er�ee significative-ment inf�erieure dans le groupe des adultes par rapport augroupe des enfants, alors que dans le groupe des adoles-cents, cette distance n’amontr�e aucune diff�erence par rapportaux deux autres groupes. Ces r�esultats s’accordent avecl’observation plus ancienne de Grosse-Wienker [31] quiconstatait que, chez les patients avec une Classe II/2d’Angle, l’arcade dento-alv�eolaire mandibulaire pr�esentaitune croissance ant�eropost�erieure limit�ee, ph�enom�ene quis’observe d�eja en denture mixte et qui devient plus prononc�een denture permanente. Chez tous les patients, la projectiondes incisives mandibulaires montrait une corr�elation n�egativeavec l’age, puisque plus le sujet �etait ag�e, plus l’i a A-Pog �etaitfaible. Ce r�esultat renforce l’opinion selon laquelle, dans lescas de Classe II/2 d’Angle, la croissance vers l’avant del’arcade dento-alv�eolaire est frein�ee et empech�ee par la ver-sion corono-palatine des incisives maxillaires et par la supra-clusion incisive [32–36].Dans les trois groupes �etudi�es, la distance entre le bordincisif des incisives centrales maxillaires et le plan d’occlu-sion (I a Oc.Pl) n’a montr�e aucune variance puisque savaleur moyenne �etait presque identique dans les troisgroupes. Par ailleurs, les patients dans leur ensemblen’ont pas montr�e de variance significative avec l’age de lavariable I a Oc.Pl. Ces r�esultats renforcent l’observationque, chez les patients en Classe II/2 �etudi�es, la protrusiondes incisives centrales maxillaires n’augmentait pas avecl’age malgr�e l’augmentation de leur version corono-palatineet de la supraclusion incisive.La distance entre le bord incisif des incisives centrales man-dibulaires et le plan d’occlusion (i a Oc.Pl), qui indique leurdegr�e de protrusion, avait des valeurs moyennes nettementsup�erieures dans les trois groupes examin�es par rapport auxvaleurs « normales » habituellement propos�ees [23,29]. Celasignifie que les patients avec une Classe II/2 d’Angle pr�esen-taient une protrusion des incisives mandibulaires. La protru-sion des incisivesmandibulaires dans les groupes d’enfants etd’adolescents ne montrait aucune diff�erence alors que, dansle groupe des adultes, elle �etait significativement plus grandepar rapport aux deux autres groupes. Dans leur ensemble, lespatients ont montr�e une corr�elation positive forte en ce quiconcerne la protrusion des incisives mandibulaires et l’agepuisque, plus les patients �etaient ag�es, plus la protrusion �etaitgrande. La protrusion et l’encombrement des incisives
International Orthodontics 2012 ; 10 : 110-121

Variation with age of dental cephalometric variables in Class II, division 2 patientsModifications avec l’age des variables dentaires c�ephalom�etriques chez des patients en classe II/2
prevents anterior growth of the mandibular dentoalveolar com-plex [37].
Incisor overbite (i to I) was found to be definitely greater in thethree groups examined when compared to ‘normal’ valuesrecommended [23,29]. This means that the Angle II/2 patientsexamined showed increased incisor overbite, a finding com-monly accepted in the relevant literature [4,10,24]. Incisoroverbite showed no difference in the children and adolescentgroups, while it was significantly increased in the adultpatients’ group as compared to the other two. The patients asa whole showed a strong positive correlation between incisoroverbite and age, since the older they were, the more pro-nounced the overbite. This finding was attributed to a corre-sponding increase in the protrusion of mandibular incisors,since maxillary incisors showed no variance in protrusion.There is a view claiming that increased overbite with age inAngle II/2 patients is of skeletal rather than of dentoalveolaretiology and it is held to be due to significant anterior rotationof the mandible [19,37,38]. Bj€ork and Skieller [38] refer to acase of Angle Class II/2 malocclusion where the patient’soverbite increased by 4 mm between the ages of 12 and18 years.
The clinical significance of the above is that the increasedpalatal tipping of maxillary central incisors and the protrusionof mandibular central incisors – leading to incisor overbite inAngle II/2 cases – should be treated during childhood toavoids them giving rise to more pronounced occlusal relation-ships at an older age. This is why it has been proposed that, inpatients who are still growing and present deep bite, theirincreased incisor overbite might obstruct the anterior migra-tion of their dentoalveolar complex. However, if overbite iscorrected in time, the dentoalveolar complex comes moreforward with the growth of the underlying skeletal structuresmore than it would have done if these patients had received notreatment.
Conclusions
The cephalometric study and the assessment of the findings inthis research study, which concerned possible variance ofdental relationships in children, adolescents and adults withAngle Class II/2 malocclusion, have led to the followingconclusions:
International Orthodontics 2012 ; 10 : 110-121
mandibulaires sont attribuables a la rotation ant�erieure de lamandibule au cours de la croissance et a la limitation de ladistance inter-canine du fait de la supraclusion incisiveprononc�ee observ�ee chez les patients en Classe II/2 et quiempeche la croissance ant�erieure du complexe dento-alv�eolaire mandibulaire [37].La supraclusion incisive (i a l) �etait nettement plus importantedans les trois groupes �etudi�es par rapport aux valeurs« normales » recommand�ees [23,29]. Cela veut dire que lespatients enClasse II/2 d’Angle que nous avons �etudi�es avaientune supraclusion incisive augment�ee, un r�esultat fr�equem-ment retrouv�e dans la litt�erature pertinente [4,10,24]. Lasupraclusion incisive �etait identique dans les groupes desenfants et des adolescents, alors qu’elle �etait plus importante,et de facon significative, dans le groupe des adultes par rap-port aux deux autres. Les patients dans leur ensemble ontmontr�e une corr�elation positive forte entre la supraclusionincisive et l’age, puisque plus les patients �etaient ag�es, plusla supraclusion �etait prononc�ee. Ce r�esultat est attribuablea une augmentation correspondante de la protrusion des inci-sives mandibulaires, puisque les incisives maxillaires n’ontpas montr�e de variance en ce qui concerne la protrusion.Certains auteurs consid�erent que l’augmentation de la supra-clusion incisive avec l’age chez les patients avec uneClasse II/2 d’Angle a une �etiologie squelettique plutot que dento-alv�eolaire qu’ils estiment due a la bascule ant�erieure signifi-cative de lamandibule [19,37,38]. Bj€orket-Skieller [38] citent lecas d’une malocclusion de Classe II/2 d’Angle ou la supraclu-sion incisive du patient a augment�e de 4 mm entre 12 et18 ans.La cons�equence clinique des r�esultats mentionn�es ci-dessusest que la version corono-palatine accrue des incisives cen-trales maxillaires et la protrusion des incisives centrales man-dibulaires – aboutissant a une supraclusion incisive dans lescas de II/2 d’Angle – doivent etre trait�ees pendant l’enfancepour �eviter qu’elles ne donnent lieu, plus tard, a des relationsocclusales plus perturb�ees. C’est pour cette raison qu’il a �et�esugg�er�e que, chez les patients en cours de croissance quipr�esentent une supraclusion incisive, l’aggravation de cettesupraclusion pourrait faire obstacle au d�eveloppement versl’avant de leur complexe dento-alv�eolaire. Cependant, si lasupraclusion incisive est corrig�ee a temps, le complexedento-alv�eolaire peut avancer suivant la croissance des struc-tures squelettiques sous-jacentes plus qu’il ne l’aurait fait sices patients n’avaient pas recu de traitement.
Conclusion
L’�etude c�ephalom�etrique et l’�evaluation de ses r�esultats, quiportait sur les possibles variations au niveau des relationsdentaires chez des enfants, des adolescents et des adultespr�esentant une malocclusion de Classe II/2 d’Angle, ontdonn�e lieu aux conclusions suivantes :
119

Nikolaos TOPOUZELIS et al.
— maxillary central incisors in all three patient groups pre-sented pronounced palatal tipping, which significantly exac-erbated with age;— mandibular incisors in all three patient groups presentedreduced labial tipping and projection. Labial tipping showedno significant variation with age, as opposed to projection,which kept decreasing significantly;
— incisor overbite in the three patient groups was found to bepronounced and increased with age due to protrusion of man-dibular incisors.
Disclosure of interest
The authors declare that they have no conflicts of interestconcerning this article.
References/R�ef�erences
1. Peck S, Peck L, Kataja M. Cteeth in well-developed jaws
2. Godiawala R, Joshi M. A cepsion and normal occlusion. A
3. Fletcher G. The retroclined4. Hitchcock H. The cephalom
Orthod 1976;69:447–54.5. Fischer-Brandies H, Fischer
Angle Class II, Division 21985;12:158–62.
6. Totah F. Classe II, division 27. Zieber K, Pancherz H. Ceph
Eur J Orthod 1995;17:462.8. Nanda R, Ghosh J. Longitud
mandible. Am J Orthod Den9. Nanda R. The rates of growt
metric roentgenograms. Am10. Mills J. The problem of overb
48.11. Leighton C, Adams C. Incis
1986;8:98-105.12. Posen A. The influence of m
Orthod 1972;42:285-309.13. Posen A. The application of
and treatment planning. Ang14. Lowe A, Takada K. Associat
muscle activity and craniofa15. Lapathki B, Mager A, Schulte
and resting lip pressure in C16. Karlsen A. Craniofacial cha
occlusion combined with ext
120
— les incisives centralesmaxillaires, chez les trois groupes depatients, pr�esentaient une version corono-palatine prononc�eequi s’est consid�erablement aggrav�ee avec l’age ;— les incisives mandibulaires chez les trois groupes depatients pr�esentaient une version corono-vestibulaire et uneprojection r�eduites. Aucune variation significative n’a �et�eobserv�ee avec l’age au niveau de la version corono-vestibu-laire. En revanche, la protrusion a continu�e a diminuer demani�ere significative ;— la supraclusion incisive chez les trois groupes de patients�etait prononc�ee et augmentait avec l’age en raison de la pro-trusion des incisives mandibulaires.
D�eclaration d’int�erets
Les auteurs d�eclarent ne pas avoir de conflits d’int�erets enrelation avec cet article.
lass II, Division 2 malocclusion: a heritage pattern of small? Angle Orthod 1998;68(1):9-20.halometric comparison between Class II, Division 2 malocclu-ngle Orthod 1974;44:262–7.upper incisor. Br J Orthod 1975;2:207–16.etric distinction of Class II, Division 2 malocclusion. Am J
-Brandies E, Konig A. A cephalometric comparison betweenmalocclusion and normal occlusion in adults. Br J Orthod
d’angle. Symptome ou diagnostic ? Orthod Fr 1980;51:275–7.alometric characteristics of Class II, division 2 malocclusions.
inal growth changes in the sagittal relationship of maxilla andtofacial Orthop 1995;107:79-90.h of several facial components measured from serial cephalo-J Orthod Dentofacial Orthop 1955;41:658–73.ite in Class II, division 2malocclusion. Br J Orthod 1973;1:34-
or inclination in Class II, div. 2 malocclusions. Eur J Orthod
aximum perioral and tongue force on the incisor teeth. Angle
quantitative perioral assessment to orthodontic case analysisle Orthod 1976;46:118–43.ions between anterior temporal, masseter, and orbicularis oriscial morphology in children. Am J Orthod 1984;86:319–30.-Moenting J, Jonas I. The importance of the level of the lip linelass II, Division 2 malocclusion. J Dent Res 2002;81:323–8.racteristics in children with Angle Class II division 2 mal-reme deep bite. Angle Orthod 1994;64:123–30.
International Orthodontics 2012 ; 10 : 110-121

17. Smeets H. A roentgenocephalometric study of the skeletal morphology of Class II division 2in adult cases. Eur Orthod Soc Rep 1962;38:247–59.
18. Ingervall B, Lennartsson B. Cranial morphology and dental arch dimensions in childrenwith Angle Class II division 2 malocclusion. Odontol Revy 1973;24(2):149–60.
19. Brezniak N, Arad A, Heller M, Dinbar A, Dinte A, Wasserstein A. Pathognomonic cephalo-metric characteristics of Angle Class II Division 2 malocclusion. Angle Orthod2002;72:251–7.
20. Kopecky G, Fishman L. Timing of cervical headgear treatment based on skeletal matura-tion. Am J Orthod Dentofacial Orthop 1993;104(2):162–9.
21. Statement by the Deutsche Gesellschaft f€ur Kieferothop€adie. Indication and frequency ofX-ray in connection with orthodontic treatment. J Orofacial Orthop 1997;58:286–7.
22. Melsen B, Baumrind S. Clinical research applications of cephalometry. In: Athanasiou AE.(Ed.), Orthodontic cephalometry. Mosby-Wolfe, London, 181-202 1998.
23. Ricketts R, Roth R, Chaconas S, Schulhof R, Engel G. Orthodontic diagnosis and planning(Vol 1). Rocky Mountain Data Systems, USA 1982.
24. Wallis S. Integration of certain variants of the facial skeleton in Class II division 2malocclusion. Angle Orthod 1963;33:60–7.
25. Robertson N, Hilton R. Feature of upper central incisors in Class II, Division 2. AngleOrthod 1965;35:51–3.
26. Hirschfelder U, Boulouchou O, Fleischer-Peters A. Dentoskeletal characteristics of ClassII, division 2 malocclusion. Eur J Orthod 1992;14:390.
27. Pancherz H, Zieber K, Hoyer B. Cephalometric characteristics of Class II division 1 andClass II division 2 malocclusion: a comparative study in children. Angle Orthod1997;67:111–20.
28. Kinzel J, Aberschek P, Mischak I, Droschl H. Study of the extent of torque, protrusion andintrusion of the incisors in the context of class II, division 2 treatment in adults. J OrofacOrthop 2002;63:283–99.
29. Langlade M. Diagnostic orthodontique. Maloine SA, �editeur. Paris: 1981.30. Slavicek R, Schadlbauer E. �Etude et comparaison de valeurs c�ephalometriques r�egionales
en Autriche et en Allemagne. Rev Orthop Dentofac 1982;16:417–71.31. Grosse-Winker M. Beitrag zur Behandlung des Deckbisses, insbesondere des oft stark
komprimierten und untersich gehenden Unterkieferzahnbogens. Fortschr Kieferorthop1953;14:116–21.
32. Korkhaus G. Uber den Aufbau des Gesichtschadels beim Deckbiss. Fortschr Kieferorthop1953;14:162–71.
33. Ruf S, Pancherz H. The mechanism of Class II correction during Herbst therapy in relationto the vertical jaw base relationship: a cephalometric roentgenographic study. Angle Orthod1997;64:271–6.
34. Mills CM, McCulloch KJ. Case report: modified use of the Jasper jumper appliance in askeletal Class II mixed dentition case requiring palatal expansion. Angle Orthod1997;67:277–82.
35. Shroff B, YoonWM, Lindauer SJ, Burstone CJ. Simultaneous intrusion and retraction usinga three-piece base arch. Angle Orthod 1997;67:455–61.
36. De Baets J, Pseudo-Class. I reevaluation of traditional Class II treatment. J Clin Orthod1997;31(9):624–48.
37. Walkow T, Peck S. Dental arch width in Class II Division 2 deep-bite malocclusion. Am JOrthod Dentofacial Orthop 2002;122(6):608–13.
38. Bj€ork A, Skieller V. Facial development and tooth eruption. An implant study at the age ofpuberty. Am J Orthod 1972;62:339–83.
International Orthodontics 2012 ; 10 : 110-121 121
Variation with age of dental cephalometric variables in Class II, division 2 patientsModifications avec l’age des variables dentaires c�ephalom�etriques chez des patients en classe II/2