Embed Size (px)
Citation preview

Cas cliniques
DOI of or1Service de
Louvain, Belgi2Service d
Louvain, Louv
CorrespondSurgery, UnivBelgium, E-m
Ann Vasc SurDOI: 10.1016/� Annals of V�Edit�e par ELS
Parapar�esie apr�es r�ealignement d’uneendoproth�ese thoracique pour uneendofuite de type III non reconnue
David Volders,1 Inge Fourneau,1 Kim Daenens,1 Sabrina Houthoofd,1 Geert Maleux,2
Andr�e Nevelsteen,1 Louvain, Belgique
Objectifs : Nous avons examin�e les raisons pour ne pas avoir retrouv�e une endofuite de type IIIsur l’imagerie conventionnelle et la pathophysiologie d’une parapar�esie apr�es le r�ealignementd’une endoproth�ese.M�ethodes et r�esultats : Un homme de 46 ans a �et�e trait�e par une endoproth�ese thoraciquepour la rupture thoracique d’une dissection chronique thoraco-abdominale de type B avecd�eg�en�erescence an�evrysmale. Au cours d’une deuxi�eme intervention, la revascularisationr�etrograde des art�eres visc�erales et r�enales a �et�e r�ealis�ee en association avec l’insertion d’uneendoproth�ese abdominale. Apr�es un r�etr�ecissement initial du sac an�evrismal, le diam�etre del’aorte thoracique a commenc�e �a croitre de nouveau. Les angioscanners cons�ecutifs ne mon-traient aucune endofuite. En raison d’une douleur dorsale insupportable, une exploration chi-rurgicale ouverte a �et�e effectu�ee. Celle-ci montrait une endofuite de type III. Le r�ealignement del’endoproth�ese thoracique a �et�e fait, mais une parapar�esie s’est d�evelopp�ee.Conclusion : Chez les patients pr�esentant une augmentation non expliqu�ee du sac an�evrys-mal, l’angio-IRM avec injection de produit de contraste paut permettre de documenter uneendofuite. Le concept de r�eseau de collat�erales peut expliquer les l�esions de la moelle �epini�erepar des modifications h�emodynamiques meme mineures.
CASE REPORT
A 46-year-old man was transferred to our university hos-
pital because of exacerbating acute thoracic back pain. At
arrival the patient was in a stable hemodynamic condi-
tion. Contrast-enhanced computed tomographic (CT)
scanning showed a thoracoabdominal aneurysm type II,
based on a chronic type B thoracoabdominal dissection.
The maximum diameter in the descending aorta was
iginal article: 10.1016/j.avsg.2009.08.016.
chirurgie vasculaire, hopital universitaire de Louvain,que.
e radiologie interventionnelle, hopital universitaire deain, Belgique.
ence : Inge Fourneau, MD, PhD, Department of Vascularersity Hospital Leuven, Herestraat 49, B-3000 Leuven,ail: [email protected]
g 2010; 24: 550.e5-550.e9j.acvfr.2010.11.005ascular Surgery Inc.EVIER MASSON SAS
80 mm. The maximum diameter in the supraceliac tho-
racic segment was 40 mm and that in the infrarenal
abdominal segment was 86 mm. There was a contained
rupture at the level of the sixth thoracic vertebra. There
were no signs of malperfusion of the viscera. He had a
history ofmorbid obesity in spite of a gastric bypass 2 years
before and bad tolerance of effort.
To avoid extracorporeal circulation and deep hypo-
thermia in this unfit patient, a hybrid therapy was plan-
ned in two stages, giving priority to the rupture. In a
first stage an 8mm silver-coated Dacron carotidecarotidesubclavian bypass (InterGard Silver�; Intervascular, La
Ciotat, France) was performed as an emergency pro-
cedure, immediately followed by deployment of three
thoracic stent grafts (Valiant� straight graft; Medtronic,
Minneapolis, MN) from just distal to the brachiocephalic
trunk to the level of the twelfth thoracic vertebra, proxi-
mal to the celiac trunk.
Two weeks later, a control CT scan showed a further
increase of the maximal thoracic diameter to 100 mm as
a result of the persistent distal dissection and a stable
maximum abdominal diameter. The residual abdominal
600.e5

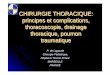
Fig. 1. CT reconstruction of the renal and visceral
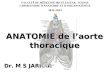
revascularization and thoracoabdominal stent graft.Fig. 2. Transverse CT section through the eighth verte-
bra (arterial phase) showing mural intraluminal throm-
bus (arrow) at the right.
600.e6 Cas cliniques Annales de chirurgie vasculaire
aneurysm was treated as an elective procedure. First,
through a median laparotomy, an iliorenalehepaticbypass was performed to the right using an 8 mm Dacron
graft (Gelsoft�; Vascutek, Inchinnin, UK). Second, an
iliorenalesuperior mesenteric bypass was performed to
the left using an 8 mm Dacron graft (Gelsoft). The pro-
cedure was finished with extension of the previously
deployed thoracic stent graft to the common iliac arteries
by an abdominal bifurcation stent graft (Valiant straight
and Talent� bifurcated graft, Medtronic) (Fig. 1). The
patient was discharged 1 month after this second inter-
vention in good condition. Recovery was uneventful.
Follow-up was planned with three-phase helical CT
scan and plain X-ray.
Three months after the first procedure, a control CT
scan showed good function of the stent grafts with
complete thrombosis of the false lumen, a slight reduction
of themaximal diameter of both the descending and abdo-
minal aorta (89 and 81 mm, respectively), no signs of
endoleak, and good opacification of the visceral bypasses.
A control CT scan at 7 months confirmed further shrin-
kage of the false lumen in both the thoracic and the abdo-
minal aorta (86 and 68 mm, respectively).
Fourteen months after the first procedure, a new
control CT scan showed an increased maximal diameter
of the descending aorta to 93 mm with appearance of
mural thrombus in the true lumen on the right (Fig. 2).
No endoleaks were observed. The maximal diameter of
the abdominal aorta was decreased to 60mm.At this point
no intervention was planned.
A new control CT scan 4months later showed a further
increase of the maximal diameter of the thoracic aorta to
98 mm without endoleaks and further enlargement of
the mural thrombus. Another control CT scan 1 month
later showed no further increase of the maximal diameter
but enlargement of the mural thrombus. Since the patient
was asymptomatic and there were no signs of endoleak,
this was considered as endotension and we decided to fol-
low the patient carefully with 3-monthly CT scans.
Another control CT scan 21months after the first inter-
vention showed a further increase of the maximal diame-
ter of the descending aorta to 110 mm, still without
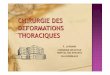
detectable endoleak. Erosive damage of the anterior side
of the ninth and tenth thoracic vertebrae was detected
(Fig. 3). At none of these time points did plain X-ray
show any sign of stent fracture or migration.
Twenty-two months after the first admission, our
patient presented with unbearable paravertebral pain. A
new three-phase helical CT showed enlargement of the
known mural thrombus on the right of the true lumen of
the descending aorta as the only change compared to the
same investigation 1 month earlier. The tentative diag-
nosis was endotension with erosion of the vertebra.
At this time we decided to intervene and to drain the
aneurysm in order to relieve the pressure on the vertebral
column. We had no evidence at all for a structural graft
defect. A left thoracotomy was performed. Due to exten-
sive stickiness of the lung, a resection of the lower left
lobe was needed. After incision of the thoracic aneurysm,
the thrombotic content was removed and major arterial
bleeding occurred, which could be stopped only by clamp-
ing the endoprosthesis. Inspection showed amajor (>2mm)
fabric disruption in the graft material (endoleak type III).
The hole was located in the middle portion of the second
thoracic stent graft at the transition zone with the proxi-
mal bare stent of the third stent graft. This endoleak was
sutured with polypropylene 3/0 reinforced with Teflon

Fig. 3. Transverse CT section through the ninth thoracic
vertebra (venous phase) at 7 months (A) and 21 months
(B) showing increase of the diameter of the descending
aorta and development of erosion of the vertebra.
Vol. 24, No. 4, 2010 Cas cliniques 600.e7
patches and spouted with a fibrin glue (Tissucol�; Baxter,
Vienna, Austria). It was felt safer to try to reline the ori-
ginal stent graft with a new stent graft. However, it was
impossible to introduce a new stent graft, either by a left or
a right femoral approach, due to severe tortuosity and loss
of flexibility at the transition zone with the abdominal
stent graft.
Two days later, the patient developed acute thoracic
hemorrhage with hemodynamic shock. The patient was
intubated, resuscitated, and immediately brought to the
operating theater, where we made another attempt to
reline the thoracic stent graft. Through a sternotomy, a
10 mm Dacron graft (Gelsoft) was sutured on the ascend-
ing aorta as a conduit for two Talent stent grafts that reli-
ned the previously inserted thoracic stent graft precisely.
After extubation on the sixth postoperative day, para-
paresis with sensibility disturbances extending to the
back and the abdomen was obvious. Magnetic resonance
imaging (MRI) of the spine at 1 month showed no defects
in the spinal cord.MRI of the skull did not reveal an expla-
nation for the neurological defects.
Over the next months, the patient improved through
multidisciplinary revalidation. The sensibility and
strength in both legs improved. At themoment the patient
is able to walk with walkers. The paravertebral pain disap-
peared. Every 6 months a follow-up three-phase helical
CT scan is performed. The last CT showed good position of
the stent grafts without endoleaks and with good vascu-
larization of the viscera. The aneurysmal dilatation of the
descending aorta remained stable at a maximum diameter
of 98 mm.
DISCUSSION
This case drew our attention for three reasons. First,
endoleak type III is a rare type of endoleak, espe-
cially if caused by a fabric tear. Second, how could
that the diagnosis of a type III endoleak be missed
in spite of close follow-up with conventional imag-
ing? Third, why did paraparesis develop after
relining of the thoracic stent graft, although no
additional side branches were sacrificed?
Type III endoleaks occur when there is a structu-
ral failure of the stent graft. This includes stent-graft
fractures, fabric tears, and junctional separations
seen with modular devices. However, due to conti-
nuous improvement of the stent grafts, type III
endoleaks are currently quite unusual. Type III
endoleaks are responsible for 20% of all endoleaks.1
We hypothesize that the fabric tear was caused by
repetitive friction between the fabric of the second
stent graft and the bare stent of the third stent graft.
To our knowledge this is the first case of a type III
endoleak due to a fabric tear in a Valiant stent graft.
For our patient, follow-up was organized with
three-phase helical CT scan and plain X-ray. Helical
CT angiography is a standard method for the post-
procedural assessment of aortic stent grafts.2
However, there is evidence that MRI is superior to
CT angiography at detecting endoleaks, at least for
nitinol stent grafts. The Valiant stent graft we used
consists of a nitinol wire scaffolding attached to a
low-profile polyester monofilament weave and is
suitable for MRI-based surveillance.3 According to
Pitton et al.,4 the sensitivity of endoleak detection in
nitinol stent grafts is 92.9%, 44.0%, 34.8%, and
38.3% for contrast-enhanced MRI, biphasic CT,

600.e8 Cas cliniques Annales de chirurgie vasculaire
uniphasic arterial CT, and uniphasic late CT, res-
pectively. The corresponding negative predictive
values are 91.7%, 58.4%, 54.7%, and 56.1%. A
review by Stavropoulos and Charagundla in 20075
on imaging techniques for the detection and
management of endoleaks after endovascular aortic
aneurysm repair concluded that although CT
angiography is currently the standard imaging
modality for endoleak detection, contrast-enhanced
MRI and ultrasound will continue to have an
expanding role in the future. As in our patient CT
angiography showed an unexplained increase of the
aneurysm diameter, contrast-enhanced MRI could
have been a good supplement to the diagnostic
work-up and could have helped to illuminate the
phenomenon of ‘‘endotension’’ in our patient.
Endotension is defined as a persistent or recur-
rent pressurization of the aneurysm sac following
endovascular repair. Gilling-Smith et al.6 reco-
gnized three types of endotension: grade I (high
flow), grade II (low flow), and grade III (no flow).
They hypothesized that one of the possible expla-
nations for grade III endotension was transmission
of pressure through the thrombus that seals an
endoleak. During surgery in our patient we found
thrombus sealing the type III endoleak as an
explanation for why the endoleak was not visuali-
zed on consecutive CT scans. However, as pressure
was transmitted through this thrombus, the aneu-
rysm diameter started increasing after an initial
tendency to shrink.
Spinal cord injury is the most dreaded complica-
tion of repair of descending thoracic and thoracoab-
dominal aneurysms and is often explained by
sacrifice of critical intercostal and lumbar arteries.
The incidence of paraplegia/paraparesis after thora-
cic stent-graft procedures as reported in the litera-
ture varies between 1.5% and 8.7%, the most
important risk factor being the length of the covered
aorta.7-9 However, our patient did not develop
paraplegia after the first intervention, although all
intercostal and lumbar arteries had been covered at
that moment, but 2 years later during relining of an
existing stent graft without sacrifice of additional
arteries. According to the literature, delayed-onset
paraplegia hours or even weeks postoperatively
accounts for up to one-third of cases of post-
operative permanent spinal cord injury.10
To study potential explanations for this phenome-
non, Etz et al.11 retrospectively looked at 10 cases of
paraplegia that developed within 48 hr after surgical
intervention despite intact somatosensory evoked
potentials throughout the operation and compared
them with 10 matched control patients who reco-
veredwithout spinal cord injury. They hypothesized
that differences in postoperative management dis-
tinguished those patients who subsequently had
paraplegia from those who recovered seemingly
normal function and that paraplegia can be caused
byminor differences in postoperative hemodynamic
andfluidmanagement. Notice that the indication for
semiurgent relining of the thoracic stent graft was
hemodynamic and respiratory instability.
That even quite subtle changes in blood pressure
can affect the development of spinal cord injury fits
in the collateral circulation concept as synthesized
by Griepp and Griepp12 and based on many labo-
ratory studies as well as clinical experience.9,13,14
After surgical sacrifice of segmental arteries, perfu-
sion of the spinal cord depends on the stabilization
of a collateral network fed from below by the
hypogastric arteries and from above by the internal
thoracic artery and other branches from the sub-
clavian arteries. This explains why routine sacrifice
of segmental aortic branches can be justified in
surgical and endovascular therapy, without risking
postoperative neurological damage. On the other
hand, the inflow of such a collateral network is very
precarious and depends principally on arterial
pressure, which is largely determined by cardiac
output, blood volume, and the competing demands
of viscera and muscle tissue connected to the same
collateral network. This concept is also supported
by the findings of Buth et al.9 that perioperative
paraplegia or paraparesis is significantly associated
with blockage of the left subclavian artery without
revascularization.
In our patient the first stent graft started distal of
the truncus brachiocephalicus and ended on the
level of the capping of thoracic vertebra 12. The
second one relined precisely the first one without
sacrificing extra vessels. We hypothesize that with
the placement of the first stent graft, the sacrifice
of segmental arteries was compensated for by the
collateral network and no neurological disturbances
occurred. However, hemodynamic instability pre-
ceding the relining procedure disturbed this preca-
rious balance in blood supply to the spinal cord.
The absence of neurological disturbances after a tho-
racic stent-graft procedure therefore does not abso-
lutely exclude the possibility of spinal cord ischemia
during relining of the same stent graft.
Perfusion-weighted MRI has been used increa-
singly in the investigation of acute cerebral
infarcts.15 Unfortunately, there are few reports of
the spinal cord. However, Yanaka et al.16 demons-
trated vasogenic edema of the spinal cord using
perfusion-weighted MRI. We suggest that transient
hypoperfusion of the spinal cord can create vaso-
genic edema, which can resolve once the circulation

Vol. 24, No. 4, 2010 Cas cliniques 600.e9
has restored itself. This would explain why the
paraparesis was transient.
There are several studies suggesting techniques to
reduce the chances of spinal cord ischemia. Jacobs
and Mess17 described in 2003 that the combination
of monitoring motor-evoked potentials, cere-
brospinal fluid drainage, distal aortic perfusion, and
epidural cooling could prevent neurological deficit
in 98% of patients with open thoracoabdominal
aortic aneurysm repair. They confirmed this in an
extensive study in 2006.18 Rigorous perioperative
hemodynamic and fluid management could help to
overcome delayed-onset paraplegia.11 Aware of
these findings, we always use prophylactic cere-
brospinal fluid drainage when covering the distal
third of the descending aorta. However, in this
patient we did not as we wrongly felt that a simple
relining of the graft would have no consequences on
the medullar circulation.
In conclusion, a fabric tear resulting in a type III
endoleak can happen. In patients with unexplained
increase of the aneurysmal sac, contrast-enhanced
MRI could help to illuminate the underlying endo-
leak. The collateral network concept can explain
spinal cord injury by even minor hemodynamic
changes.
REFERENCES
1. Parmer S, Carpenter J, Stavropoulos W, et coll. Endoleaks
after endovascular repair of thoracic aortic aneurysms.
J Vasc Surg 2006;44:447-452.
2. Thurnher S, Cejna M. Imaging of aortic stent-grafts and
endoleaks. Radiol Clin North Am 2002;40:799-833.
3. van der Laan M, Bartels L, Bakker C, et coll. Suitability of
7 aortic stent-graft models for MRI-based surveillance.
J Endovasc Ther 2004;11:366-371.
4. Pitton MB, Schweitzer H, Herber S, et coll. MRI versus
helical CT for endoleak detection after endovascular aneu-
rysm repair. AJR Am J Roentgenol 2005;185:1275-1281.
5. Stavropoulos SW, Charagundla SR. Imaging techniques for
detection and management of endoleaks after endovascular
aortic aneurysm repair. Radiology 2007;243:641-655.
6. Gilling-Smith G, Brennan J, Harris P, et coll. Endotension
after endovascular aneurysm repair: definition, classifi-
cation, and strategies for surveillance and intervention.
J Endovasc Surg 1999;6:305-307.
7. Khoynezhad A, Donayre C, Bui H, et coll. Risk factors of
neurologic deficit after thoracic aortic endografting. Ann
Thorac Surg 2007;83:S882-S889.
8. Fairman R, Criado F, Farber M, et coll. Pivotal results of the
Medtronic vascular Talent thoracic stent graft system: the
VALOR trial. J Vasc Surg 2008;48:546-554.
9. Buth J, Harris PL, Hobo R, et coll. Neurologic complications
associated with endovascular repair of thoracic aortic
pathology: incidence and risk factors. A study from the
European Collaborators on Stent/Graft Techniques for Aor-
tic Aneurysm Repair (EUROSTAR) registry. J Vasc Surg
2007;46:1103-1110.
10. Wong DR, Coselli JS, Amerman K, et coll. Delayed spinal
cord deficits after thoracoabdominal aortic aneurysm repair.
Ann Thorac Surg 2007;83:1345-1355.
11. Etz CD, Luehr M, Kari FA, et coll. Paraplegia after extensive
thoracic and thoracoabdominal aortic aneurysm repair: does
critical spinal cord ischemia occur postoperatively? J Thorac
Cardiovasc Surg 2008;135:324-330.
12. Griepp RB, Griepp EB. Spinal cord perfusion and protection
during descending thoracic and thoracoabdominal aortic
surgery: the collateral network concept. Ann Thorac Surg
2007;83:865-869.
13. Jacobs MJ, de Mol BA, Ellenbaas T, et coll. Spinal cord blood
supply in patients with thoracoabdominal aortic aneurysms.
J Vasc Surg 2002;35:30-37.
14. Schurink GW, Nijenhuis RJ, Backes WH, et coll. Assessment
of spinal cord circulation and function in endovascular
treatment of thoracic aortic aneurysms. Ann Thorac Surg
2007;83:S877-S881.
15. Neumann-Haefelin T, Wittsack HJ, Fink GR, et coll. Diffu-
sion- and perfusion-weighted MRI: influence of severe
carotid artery stenosis on the DWI/PWI mismatch in acute
stroke. Stroke 2000;31:1311-1317.
16. Yanaka K, Matsumaru Y, Uemura K, et coll. Perfusion-
weighted MRI of spinal dural arteriovenous fistula. Neuro-
radiology 2003;45:744-747.
17. Jacobs MJ, Mess WH. The role of evoked potential moni-
toring in operative management of type I and type II tho-
racoabdominal aortic aneurysms. Semin Thorac Cardiovasc
Surg 2003;15:353-364.
18. Jacobs MJ, Mess W, Mochtar B, et coll. The value of motor
evoked potentials in reducing paraplegia during thora-
coabdominal aneurysm repair. J Vasc Surg 2006;43:
239-246.