Embed Size (px)
Citation preview

R E V I S T A P O R T U G U E S A D E P N E U M O L O G I A
Vol XII N.º 2 Março/Abril 2006
93
Participação das vias aéreas centrais na doença vibroacústicaJosé Reis Ferreira, Miguel B. Monteiro, Fernanda Tavares, Isabel Serrano, Emanuel Monteiro, Carla P Mendes,Mariana Alves-Pereira, Nuno A A Castelo Branco
Participação das vias aéreas centrais na doençavibroacústica
Involvement of central airways in vibroacoustic diseasepatients
José Reis Ferreira1
Miguel B Monteiro2
Fernanda Tavares3
Isabel Serrano4
Emanuel Monteiro5
Carla P Mendes6
Mariana Alves-Pereira7
Nuno A A Castelo Branco8
ResumoResumoResumoResumoResumoNos últimos vinte cinco anos constatou-se que oaparelho respiratório constitui um alvo do ruídode baixa frequência (RFB <500Hz, incluindo in-fra-sons). Denomina-se doença vibroacústica(VAD) a patologia sistémica causada pela exposiçãoexcessiva a RBF. Em ratos Wistar expostos a RBF,as alterações morfológicas observadas nos tecidosdas vias aéreas centrais explicam, parcialmente, ossintomas apresentados pelos doentes com a VAD.Apesar disso, muitas perguntas permanecem porresponder. Recentemente, voluntários com a doençavibroacústica submeteram-se a exames broncos-
Prémio Thomé Villar/Boehringer Ingelheim 2004*
Thomé Villar/Boehringer Ingelheim Award 2004 *
AbstractAbstractAbstractAbstractAbstractIntroduction. Vibroacoustic disease (VAD) is thewhole-body pathology caused by excessive expo-sure to LFN. For the past 25 years, it has beenknow that low frequency noise (LFN, <500 Hz,including infrasound) targets the respiratory sys-tem. In LFN-exposed rodents, the morphologicalchanges of respiratory tract tissue partially ex-plained some respiratory symptoms reported byVAD patients. However, many questions remainunanswered. Recently, some volunteer VAD pa-tients underwent bronchoscopy in order to ascer-tain possible damage that could be associated with
* Trabalho vencedor ex-aequo (Secção A)1 Médico pneumologista/Pulmonologist. Unidade de Estudo Funcional Respiratório, Hospital da Força Aérea, Lisboa2 Médico pneumologista/Pulmonologist. Unidade de Pneumologia, Centro Hospitalar de Cascais3 Médica anatomopatologista/Anatomo-pathologist. Centro de Patologia Humana, Oeiras4 Médica anatomopatologista/Anatomo-pathologist. Centro Hospitalar de Cascais5 Técnico de anatomia/Anatomy technician. Instituto de Ciências Biomédicas Abel Salazar, Universidade do Porto6 Médico pneumologista/Pulmonologist. Unidade de Estudo Funcional Respiratório, Hospital da Força Aérea, Lisboa7 Mestre em engenharia biomédica/M.A.in Biomedical engeneering. Departamento de Ciências e Engenharia do Ambiente, Universidade Nova de Lisboa8 Médico anatomopatologista/Anatomo-pathologist. Presidente do Conselho Científico/President of the Scientific Board, Centro da Performance Humana, [email protected]
Recebido/aceite para publicação/received/accepted for publication: 05.11.12

R E V I S T A P O R T U G U E S A D E P N E U M O L O G I A
Vol XII N.º 2 Março/Abril 2006
94
Participação das vias aéreas centrais na doença vibroacústicaJosé Reis Ferreira, Miguel B. Monteiro, Fernanda Tavares, Isabel Serrano, Emanuel Monteiro, Carla P Mendes,
Mariana Alves-Pereira, Nuno A A Castelo Branco
their respiratory complaints. Methods. Fourteenfully-informed and volunteer VAD patients weresubmitted to bronchoscopy, and biopsies wereremoved for analysis. Results. All patients exhi-bited small submucosal vascular-like lesions nearthe spurs, consisting of increased collagen and elas-tin fibres. Histology disclosed cilliary abnormali-ties, basal membrane hyperplasia, and thickeningof vessel walls. In five patients, collagen bundlesappeared degenerative and disrupted. No inflam-matory process was ever identified, and no diffe-rences were seen between smokers and non-smo-kers. Discussion. Data is in accordance with whatwas observed in LFN-exposed animal models andalso in 8 VAD patients who developed lung tu-mours. Collagen disruption and degeneration wasalso observed in electron microscopy images of therespiratory tract of LFN-exposed rodents. Thi-ckened blood and lymphatic vessel walls have beenconsistently seen in images of VAD patients andof LFN-exposed rodents. During bronchoscopyperformed by other reasons, this sort of structuralaspects is not frequently seen. Taken together, itis strongly suggested that these findings could beVAD-specific.
Rev Port Pneumol 2006; XII (2): 93-105
Key-words: Low frequency noise, vibroacousticdisease, vascular lesions, displasia, auto-imune di-sorders, collagen disease, ciliar structure, apoptosis,mecano-transduction.
cópicos para esclarecer e, se possível, demonstrarpossíveis lesões das vias aéreas centrais que estariamassociadas com as queixas respiratórias. Trezedoentes voluntários, exaustivamente esclarecidossobre este exame, submeteram-se a broncoscopias,durante as quais se colheram fragmentos para examehistológico e ultra-estrutural. Em todos os indiví-duos se observaram lesões de tipo vascular na sub-mucosa próximas das bifurcações das vias aéreas.Estas lesões caracterizavam-se por numerosospequenos vasos com paredes espessadas, mergu-lhados em feixes de colagénio e algumas fibras deelastina. Em cinco indivíduos as lesões evidenciavamdegenerescência e ruptura do colagénio. Histologica-mente, na mucosa normal observaram-se alteraçõesciliares, hiperplasia da membrana basal e espessamentodos vasos sanguíneos. Em nenhum caso se obser-varam infiltrados celulares de natureza inflama-tória. O estudo da ultra-estrutura revelou numero-sos axonemas (de dois a oito) contidos numamembrana ciliar comum, algumas vesículas ema-nando dos cílios, imagens de apoptose com reforçodo citosqueleto celular e das ligações intercelulares.Não se observaram diferenças entre fumadores enão fumadores. Estes dados estão de acordo com oque já fora observado nas vias aéreas centrais deoito doentes com carcinoma pavimento-celular dopulmão e também com as imagens observadas emratos expostos a RBF. Em broncoscopias efectuadasem doentes sem a doença vibroacústica, não é nor-mal observar-se este tipo de lesões vasculares.Assim, estas lesões vasculares das vias aéreas centraispodem ser específicas da doença vibroacústica.
Rev Port Pneumol 2006; XII (2): 93-105
Palavras-chave: Ruído de baixa frequência, doençavibroacústica, lesões vasculares, displasia, doençaauto-imune, doença do colagénio, estrutura ciliar,apoptose, mecano-transdução.

R E V I S T A P O R T U G U E S A D E P N E U M O L O G I A
Vol XII N.º 2 Março/Abril 2006
95
Participação das vias aéreas centrais na doença vibroacústicaJosé Reis Ferreira, Miguel B. Monteiro, Fernanda Tavares, Isabel Serrano, Emanuel Monteiro, Carla P Mendes,Mariana Alves-Pereira, Nuno A A Castelo Branco
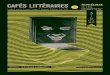
IntrIntrIntrIntrIntroductionoductionoductionoductionoductionExcessive exposure to low frequency noise(LFN) (≤500 Hz, including infrasound)can lead to the development of vibro-acoustic disease (VAD)1,2. VAD is a sys-temic pathology with an insidious and si-lent progression, characterized by theabnormal proliferation of extra-cellarmatrices, namely collagen and elastin.Pericardial thickening in the absence ofan inflammatory process and with noadiastole is VAD specific3, and can be as-sessed through echocardiography4. Otherdiagnostic tests such as brainstem auditoryevoked potentials5, P300 wave6 and thePCO2 respiratory drive test are available,7,8. However, to date, no medical diagnos-tic test has been found to readily assesspathognomonic signs.Respiratory pathology in VAD was notimmediately acknowledged because thefirst VAD study group consisted of air-craft technicians who are often exposedto airborne agents that could justify theirrespiratory complaints. These included (inboth smokers and non-smokers alike)non-productive cough, repeated oropha-rynx infections, bronchitis and unex-plained hoarseness2. Most of these situa-tions, however, were not responsive to thetypical therapeutics. Several cases of pleu-ral effusion of unknown aetiology alsodeveloped among these workers. Unex-plained lung fibrosis was a 1987 autopsyfinding in a deceased VAD patient9.All these circumstances prompted the1892 investigations of the respiratory tractof LFN-exposed rats10-18. Here, significantmorphological changes of respiratory epi-thelia such as abnormal amounts of colla-gen, thickened blood vessel walls, and
damaged cilia, were observed through elec-tron microscopy. Pleura investigations inthese rats showed that in addition to themorphological changes, mesothelial cellslost their phagocytic ability15,17. Mesothe-lial changes in the rat pleura are of thesame morphological type as those ob-served in the respiratory epithelial cells:de-differentiation, reinforcement ofcytoskeletal structures, and abnormallyhigh frequency of apoptotic processes.Increased collagen in tracheal subepithe-lial cells, in lung parenchyma, and in pleu-ral structures disclosed foci of foamy-likedegeneration (Figs. 1 and 2).Noise-induced respiratory pathology havealso been studied by other authors overthe past 4 decades19-24. Results show thatacoustic phenomena have a direct effecton respiratory system structures, whetherthe exposure is long-term or short-term.In 2003, this team was contacted by a cou-ple from Dublin, Ireland, suspected ofsuffering from VAD due to excessive in-home exposure to LFN caused by Dub-lin buses. Upon their trip to Lisbon, aVAD diagnosis was confirmed, and thecase proceeded through the Irish courtswith success for the plaintiffs. As in pre-vious VAD patients, non-productivecough, unexplained hoarseness and fre-quent, atypical oropharynx infectionswere reported by the 54 year-old female,a mild smoker. She promptly agreed toundergo a bronchoscopic examination inorder to better characterize the nature ofher complaints and, possibly, to providethe Irish courts with additional data fa-vourable to their case.Fiberbronchoscopy was performed. Pinklesions were identified in small submu-
VAD is a systemicpathology with aninsidious and silentprogression,characterized by theabnormalproliferation ofextra-cellar matrices,namely collagen andelastin
Acoustic phenomenahave a direct effecton respiratorysystem structures,whether the exposureis long-term orshort-term

R E V I S T A P O R T U G U E S A D E P N E U M O L O G I A
Vol XII N.º 2 Março/Abril 2006
96
Participação das vias aéreas centrais na doença vibroacústicaJosé Reis Ferreira, Miguel B. Monteiro, Fernanda Tavares, Isabel Serrano, Emanuel Monteiro, Carla P Mendes,
Mariana Alves-Pereira, Nuno A A Castelo Branco
cosal vascular-like lesions, located distallyin both tracheal and bronchial trees, anduniformly distributed bilaterally near thespurs. Informal calculations indicated thatthe diameter of these lesions was not over3mm. No biopsy was initially taken fromthe pink areas. Given the possibility thatthese areas could be of a vascular nature,biopsy could lead to bleeding with possi-bly serious consequences. Histologicalstudies of the non-pink areas disclosed ab-normal amounts of collagen, damaged ciliaand thickened blood vessel walls.These observations confirmed previousfindings in LFN-exposed rats, as well asin 3 other VAD patients who underwentbronchoscopic biopsies for other purposes
– neoplasm screening. In these 3 otherindividuals, biopsies of the pink areas werenever performed due to the suspicion oftheir vascular nature.The results were submitted to the Hospi-tal Ethics Committee to obtain authori-zation to perform a biopsy in the pinkareas, with the necessary precautions.Authorization was obtained. The Irishfemale volunteered for a second biopsy,fully-informed of the procedure and therisks, while additional medical staff waspresent, as well as thoracic surgeons. Todate, 13 bronchoscopic examinations havebeen performed on volunteer VAD pa-tients with biopsy of the pink areas.The goal of this report is to describe thehistological results of bronchoscopic bio-psies with relevance to the pink areas iden-tified in VAD patients.
MethodsMethodsMethodsMethodsMethodsThirteen patients volunteered for thisstudy, as described in Table I. All had beenpreviously diagnosed with VAD and ex-hibited pericardial and cardiac valve thi-ckening, as assessed through echocardio-graphy. Brainstem auditory evokedpotentials and the P300 wave disclosed theusual changes in VAD patients, and all hadimpaired respiratory drive with simulta-neous normal pulmonary function tests.They performed routine lab tests, C-Rea-ctive Protein and serum antinuclear anti-bodies (ANA).The procedures were conducted undergeneral anesthesia, with jet ventilationsystem (Sanders-Venturi valve) and throughrigid bronchoscope (Efer-Dumon,France). After identification of the lesion,it was punctured with a Wang needle
AB
C
A
C B
C
C
Fig. 1 – Transmission electronmicroscopy of control rat respiratoryepithelia. Ciliated cell (A) next to aserous cell (B), over a normal subepi-thelial layer of collagen.Numerouscilliary vesicles are patent. (x5600).
Fig. 2 – Transmission electronmicroscopy of LFN-exposed rat res-piratory epithelia (2438 hrs of total ex-posure). Brush cell (A) with 2vacuoles and surrounded by serouscells, both de-differentiated. Scarcecilliary vesicles are present. Under-neath is a layer of hyperplastic colla-gen with multiple foci of “foamy” (C)degenerated bundles. (x5600).
A
BC
C

R E V I S T A P O R T U G U E S A D E P N E U M O L O G I A
Vol XII N.º 2 Março/Abril 2006
97
Participação das vias aéreas centrais na doença vibroacústicaJosé Reis Ferreira, Miguel B. Monteiro, Fernanda Tavares, Isabel Serrano, Emanuel Monteiro, Carla P Mendes,Mariana Alves-Pereira, Nuno A A Castelo Branco
which produced a slight and self limitedhaemorrhage. Biopsies were obtainedwith standard bronchofiberscope flexibleforceps (Olympus, Japan). For safety rea-sons only small volumes of biopsy mate-rial were removed.Specimens for light microscopy werefixed in 10% buffered formalin, sectionedand prepared for histological observationusing standard methods. The sections werestained with hematoxylin-eosin, Massontrichrome solution, chronotrop anilineblue, and PAS.Specimens for electron microscopy wereplaced in a solution of 3% gluteraldehydein 0.1 M phosphate buffer, pH 7.2 and
Case #(Male/Female)
Age Exposuretype
Smoker
1 – Male 48 Aircrafttechnician
Mild
2 – Male 37 Merchantmarine
No
3 – Female 56 Nurse(helicopter)
No
4 – Female 36 Flightattendant
No
5 – Male 61 Combat pilot No6 – Female 54 Home-maker Mild7 – Female 59 Home-maker No8 – Male 52 Aircraft
technicianNo
9 – Male 59 Aircrafttechnician
Mild
10 – Male 59 Helicopterpilot
Moderate
11 – Male 54 Aircraft pilot No12 - Female 39 Flight
attendantNo
13 - Female 40 Flightattendant
No
Table I – Description of study population then washed with several changes of 5%sucrose in 0.1 M phosphate buffer, pH 7.2,for ultrastructural studies.For TEM, samples were fixed at roomtemperature in an aldehyde mixture con-sisting of 4% paraformaldehyde, 1.25%glutaraldehyde, and 10mM CaCl2 in 0.05M cacodylate buffer, and pH 7.2. Speci-mens were washed in buffer, and postfixedin a ferricyanide-reduced osmium solutionmade up of 1% potassium ferricyanide and1% osmium tetroxide in distilled water,dehydrated through a graded ethanol se-ries, and embedded in Epon. The sampleswere sectioned in an ultramicrotome(LKB, Sweden) and the thin sectionsstained with uranyl acetate and leadcitrate. Preparations were then examinedwith electron microscopy (JEOL 100C,Japan).
ResultsResultsResultsResultsResultsIn all patients, bronchoscopy observationdisclosed small submucosal vascular-likelesions located distally in both trachealand bronchial trees, and uniformly distri-buted bilaterally near the spurs (Fig. 3).Biopsies were performed on the abnor-mal mucosa (pink areas) and apparentlynormal mucosa (outside the pink areas).Pink areas did not bleed as would be ex-pected from typical vascular lesions. Noother abnormalities were observed.Light microscopy of the non-pink areasdisclosed irregular cilia distribution, withsome areas with large groupings, whileothers had scarce damaged cilia. Displasticfoci were identified as well as basalhiperplasia (Fig. 4). The basal membranewas thickened with an abnormal amountof collagen, and some blood vessels with

R E V I S T A P O R T U G U E S A D E P N E U M O L O G I A
Vol XII N.º 2 Março/Abril 2006
98
Participação das vias aéreas centrais na doença vibroacústicaJosé Reis Ferreira, Miguel B. Monteiro, Fernanda Tavares, Isabel Serrano, Emanuel Monteiro, Carla P Mendes,
Mariana Alves-Pereira, Nuno A A Castelo Branco
thickened walls were visible.In the pink areas, the number of ciliatedcells and the cilia were also abnormallydistributed. The basal membrane appearedeven thicker than in the non-pink areaswith very large amounts of collagen. Theentire basal membrane featured an abnor-
mal neo-vascularization, disclosing verythickened small blood vessel walls withscarce lumen. Lymphatic vessel walls werealso thickened. This intense neo-vasculari-zation was embedded within the collagenbundles. The amount of elastic fibres wasalso increased when compared with thenon-pink areas. No inflammatorycellularity nor processes were observed,nor was retraction of neighbouring struc-tures observed in the vicinity of collagenfibres (Figs. 5-8).In five patients (cases 1-4, 13), some colla-gen fibres disclosed images of degenera-tion and disruption. These five cases alsotested positive for anti-nuclear antibodies.No inflammatory cellularity was identi-fied. In TEM, the most noticeable featureof gross changes in ciliary morphology arethe multiple ciliary axonemes surroundedby a common membrane (Fig. 9). The celllife-cycle seems to be greatly acceleratedgiven the frequency of apoptotic imagesin all epithelial cell ultramicrographs. All
Fig. 4 – Patient #7: Light microscopy. Tracheal “normal”epithelium of the female VAD patient, non-smoker. Basalhyperplasia and partial destruction of cilia are visible, withsubepithelial loose tissue. (x 200) (H&E)
Fig. 3 – Patient #5: Pink area lesion (arrow) as seen throughbronchoscopy.
Fig. 5 – Patient #4: Cilliary changes are visible with su-bepithelial fibrosis, as well as vascular hyperplasia withinsubepithelial loose tissue. A longitudinal cut of a lymphaticvessel (arrow) shows thickened walls (x100) (Masson tri-chrome solution staining).

R E V I S T A P O R T U G U E S A D E P N E U M O L O G I A
Vol XII N.º 2 Março/Abril 2006
99
Participação das vias aéreas centrais na doença vibroacústicaJosé Reis Ferreira, Miguel B. Monteiro, Fernanda Tavares, Isabel Serrano, Emanuel Monteiro, Carla P Mendes,Mariana Alves-Pereira, Nuno A A Castelo Branco
Fig. 6 – Patient #4: Subepithial loose tissue. Deep abnor-mal collagen proliferation with neo-vascular formations.(x200) (Masson trichrome solution staining).
Fig. 7 – Patient #4: Cillary changes are visible, as well asfibrosis and numerous elastic fibres. Some collagen bun-dles disclose degeneration and disruptions (x200)(chronotrop aniline blue staining).
Fig. 8 – Patient #4: Histological cut showing cilliary changeswith subepithelial loose tissue. Deep fibrosis with neo-vas-cular proliferation. (x200) (Masson trichrome solution stai-ning).
Fig. 9 – Patient #7: TEM. Tracheal epithelium of non-smokerfemale VAD patient. An apoptotic cell and abnormal ciliawith more than one axoneme per membrane. Two ciliaryvesicles are visible. (x16000).
Fig. 10 – Patient #7: TEM - Tracheal epithelium of non-smoker female VAD patient. Ciliated cell under apoptosis.In this tangential cut, the cell death process is seen to reachthe basal bodies. (x20000).
cell structures seem to be under the sameprocess of death (Figs. 9-11), in contrastwith a marked reinforcement of the cy-toskeleton and intercellular junctions.

R E V I S T A P O R T U G U E S A D E P N E U M O L O G I A
Vol XII N.º 2 Março/Abril 2006
100
Participação das vias aéreas centrais na doença vibroacústicaJosé Reis Ferreira, Miguel B. Monteiro, Fernanda Tavares, Isabel Serrano, Emanuel Monteiro, Carla P Mendes,
Mariana Alves-Pereira, Nuno A A Castelo Branco
DiscussionDiscussionDiscussionDiscussionDiscussionThirteen subjects may seem to be a smallnumber of cases. Bronchoscopic exami-nations are very invasive procedures, andeven though all aspects are explained tovolunteer patients before the examination,it naturally frightens many individuals.Nevertheless, this is already an importantnumber considering that all (100%) havedisclosed the same type of lesions, eventhough they have distinct types of LFNexposure – occupational and environmen-tal, with different frequency distributions.Additionally, the vascular component isthe same in all cases observed – thickenedblood vessel walls – as has already been seenin autopsy9, in LFN-exposed rats10-14, aswell as in pericardial fragments of VADpatients25,26. Lymphatic vessel abnormali-ties were also similar to those seen in LFN-exposed rats27, as were those observed inblood vessels28. Electron microscopy stu-dies of biopsy material are still underway.In an inflammatory process, the growth
of collagen is not well organized, and doesnot include embedded neo-vasculariza-tion, as is seen in these patients. In theformation of scar tissue, there is retrac-tion of the neighbouring structures thatis not observed here. This does not meanthat the inflammatory cascade is notpresent; however the classical inflamma-tory response, with collagen productionas an end result, is not exhibited by VADpatients. The inflammatory cascadewithin the scope of LFN-exposure is thefocus of an independent and ongoingproject.In cases 1-4 and 13, collagen degenerativeprocesses were observed. Although noneof these five patients have been diagnosedwith collagen diseases, namely systemiclupus erythematosus, other VAD patientshave indeed been diagnosed with this formof collagen disease, and other auto-im-mune disorders29,30. The airway pink le-sions described herein have also been ob-served in systemic lupus erythematosus31.The involvement of the immune systemin VAD patients has long been recognized.Previous studies have demonstrated thatlupus-prone mice have an earlier onset andincreased mortality when exposed toLFN32, while circulating CD4+ and CD8+
lymphocytes suffer modulations withLFN exposure in aircraft technicians33.Collagen plays a key role in maintainingstructural integrity of biological tissue,allowing movement without rupture. Thedifferent arrangements of collagen fibres,relative angular organization and interlac-ing of elastic fibres provide tissues withthe ability to sustain movement withoutrupture, to maintain functionality despite(mechanical) disturbances. Production of
Fig. 11 – Patient #9: TEM - Tracheal epithelium of a maleVAD patient, smoker. Intercellular junctions of two apoptoticepithelial cells with impressive desmosomes and a markedreinforcement of the cytoskeleton. (x40000).
Collagen plays a keyrole in maintainingstructural integrity ofbiological tissue,allowing movementwithout rupture

R E V I S T A P O R T U G U E S A D E P N E U M O L O G I A
Vol XII N.º 2 Março/Abril 2006
101
Participação das vias aéreas centrais na doença vibroacústicaJosé Reis Ferreira, Miguel B. Monteiro, Fernanda Tavares, Isabel Serrano, Emanuel Monteiro, Carla P Mendes,Mariana Alves-Pereira, Nuno A A Castelo Branco
collagen, therefore, can be elicited by bio-logical structural requirements.Vibratory stress, such as that induced byLFN exposure, can threaten the structuralintegrity of almost any type of biological(and non-biological) material. In aircraftfuselage, for example, vibratory stress cangive rise to micro-fractures that, in turn,can jeopardize flight safety. In biologicaltissue, LFN-induced vibratory stress, aspotentially related to pathological evolu-tions, is an underdeveloped scientific field.In biological tissue, vibratory stress canplay a key role in the maintenance of thetissue’s structural integrity. However,unlike aircraft, a biological organism canmount a response associated with assuringthat structural integrity is not lost or, inother words, that functionality is main-tained – at least at a required minimumfor immediate and/or long-term survivalof the organism.Maintenance of structural integrity can beachieved by structural reinforcement. Inlayman’s term: if it’s shaking, tie it down.The possibility of rupture along tissuesurfaces can elicit a biological responsethat counteracts by reinforcing the sur-face. This structural reinforcement can beachieved through the production of col-lagen – a strong, tensile material. If enoughelastic fibres are simultaneously produced,it is possible for the tissue surface to main-tain its functionality while assimilatingabnormal vibratory stress.Considering that respiratory airways canbe thought of as flexible hoses and thatLFN exposure translates into vibratorystress, it is not difficult to speculate on areason for the existence of these respira-tory tract lesions. Indeed, they can be
thought of as the equivalent of micro-frac-tures that appear along aircraft fuselageas a result of excessive vibratory stress.Following this line of reasoning, the bio-logical response of increased collagen andelastic fibres is not surprising if maintai-ning structural integrity is an issue. Bio-tensegrity concepts, continuous tensionwith zero torque, may be the guidingpathways for this occurrence34-39. Mecha-notransduction signalling is an importantpathway for cell signalling. It is achievedthrough the biopolymers that composeboth the cytoskeleton and the extra-cel-lular matrix. Given the morphologicalchanges seen in FLN noise exposed hu-mans and animals, it is pertinent and logi-cal to view VAD as a mechanotanductiondisease.However, disruptions in the collagen bun-dles, giving them their “foamy” appea-rance, and reproducing previous resultsin LFN-exposed rats, strongly suggeststhat functionality is not being fully main-tained.Vesicles. Cilliary vesicles cannot be ig-nored given their recurring presence inboth non-exposed (Fig. 1) and exposed(Fig. 2) rats and humans (Fig 9). No refe-rence to this feature was found in the li-terature except for one micrograph40 It istherefore unknown if they are a productof exocytosis (coated vesicles?) or some-thing else. Regardless of their contents orbiochemical role, their physical presencealone as microspheres spewed into therespiratory fluid can have important con-sequences on drainage processes. Thenumber of vesicles is decreased in the ex-posed specimens, which suggests that theirfunction might be compromised. This
Vibratory stress,such as that inducedby LFN exposure,can threaten thestructural integrity ofalmost any type ofbiological (andnon-biological)material

R E V I S T A P O R T U G U E S A D E P N E U M O L O G I A
Vol XII N.º 2 Março/Abril 2006
102
Participação das vias aéreas centrais na doença vibroacústicaJosé Reis Ferreira, Miguel B. Monteiro, Fernanda Tavares, Isabel Serrano, Emanuel Monteiro, Carla P Mendes,
Mariana Alves-Pereira, Nuno A A Castelo Branco
would not be entirely surprising sinceother functional capabilities such as thephagocytic ability of the pleural me-sothelial cells18 are known to be lost dueto LFN exposure.Low Frequency Noise. LFN targets therespiratory epithelia. This has been sus-pected for decades. In 1987, Svigovyi etal. investigated the effects of infrasoundon the pulmonary ultra structure of whitemice22. Noise was characterized as 2, 4, 8,or 16 Hz, at 90-140 dB. The mice wereexposed for 3 hr daily, for 1, 5, 10, 15, 24and 40 days. After 3 h of exposure, “point,mosaic-type” hemorrhages were identifiedover the entire lung surface. Thesehemorrhages were observed beneath thepleura for exposures of 2-4 Hz at 92-100dB, and large bleeding spots were identi-fied in lung exposed to 8-16 Hz, at 120-140 dB. After 10-15 d of exposure, partsof the lung tissue are filled with blood andthe walls between alveoli are swollen andthick. Dramatic morphological changes ofalveolar, cellular, and blood vessel struc-tures are described after exposures of 24-40 days, at 8-16 Hz and 120 dB. These in-cluded deformation of nuclei andconcentration of chromatin under the nu-clear membrane in type I and IIpneumocytes, and disruption and defor-mation of alveolar sacs, destruction of al-veolar walls, and burst capillaries andlarger vessels.In 1969, Ponomarkov et al. explored theeffects of wide-band noise at 105-155 dB(no frequency distribution informationwas provided) on dogs20. After 1.5-2 h ofexposure, the animals were sacrificed.Autopsy results revealed hemorrhages upto 3 mm in diameter in the lungs of the
animals exposed to about 126 dB, locatedbeneath the pleura in the form of convexvesicles. They were most common in thecostal surface of the upper lobe of the rightlung. The authors claim that as the dBlevel of the noise increased, the numberof the hemorrhages increased, but theynever exceeded 3mm in diameter. Micro-scopic analysis of the hemorrhaged sec-tion of lung tissue revealed ruptured cap-illaries and larger vessels. Microscopicanalysis of the emphysematous areasshowed focal enlargement of the alveoli,stretching of the connective-tissue struc-tures of the alveolar walls, and compres-sion of lung tissue. They conclude theirreport by giving a possible explanation forthis pathology: “The lungs, as a systemopen to the external environment, are sub-jected to the greatest influence of changesin pressure in this medium. Depending onthe magnitude of the pressure differentialcreated by sound in the lungs during itstransformation, and of the threshold ofresistance of the lung tissue to pressurechanges, the severity of the lung lesionsgradually increases.”The effects of LFN on human populationshave been partially studied in the past andconfirm that this acoustic stressor is a po-tential agent of respiratory illness. An in-teresting study was conducted in the mid-60’s19. Unfortunately the number ofsubjects involved (N=5, all military per-sonnel) renders them statistically non-sig-nificant. However, the acoustic simula-tion facilities used were unique: theyallowed simultaneous subjective and ob-jective stress responses during exposure toa well-defined acoustic environment,which provided detailed information on
Dramaticmorphologicalchanges of alveolar,cellular, and bloodvessel structures aredescribed afterexposures of 24-40days, at 8-16 Hz and120 dB

R E V I S T A P O R T U G U E S A D E P N E U M O L O G I A
Vol XII N.º 2 Março/Abril 2006
103
Participação das vias aéreas centrais na doença vibroacústicaJosé Reis Ferreira, Miguel B. Monteiro, Fernanda Tavares, Isabel Serrano, Emanuel Monteiro, Carla P Mendes,Mariana Alves-Pereira, Nuno A A Castelo Branco
amplitude (95-140 dB), frequency (spikesat 30-100 Hz), and exposure time (25 sec-5 min). Subjective complaints involvingthe respiratory tract are abundant andincluded coughing, gagging sensations,chest wall and throat pressure, and painon swallowing.LFN is not currently legislated, nor is itassessed during routine noise evaluations,hence this agent of disease is ubiquitousin modern society with the potential con-sequences if imolies for Public Health.That LFN exposure induces severe lesionsof the respiratory system is a fact. Theevidence gathered with animal modelsclearly shows that the respiratory epithe-lia are not, at all, impervious to acousticphenomena. Despite the immune depres-sion of VAD patients, many of their im-mediate and long-term respiratory ill-nesses are certainly due to the directimpact of this agent of disease. The in-volvement of the CNS in LFN-inducedrespiratory pathology is still understudiedand cannot be excluded.Unfortunately, noise-exposed workers areonly required to undergo an audiogramin order to evaluate hearing loss, particu-lar at the 4000 Hz notch. VAD patientsnormally have loss at the 250-500 Hzrange, which, if observed, is normallyoverlooked as a curiosity. In fact, the mostcommon auditory complaint of VADpatients is that “they hear too much, can’tstand any type of sound, not even musicor television”.Commentary. Regarding LFN as a muta-genic and genotoxic agent raises unsettlingconcerns41-43. Not only because LFN isrampant in our society, but also becausethe cause of many malignancies are being
erroneously imputed to other causes. Forexample, given the information providedhere, what is the validity of studies con-cerning the respiratory system where theacoustic environments of the study popu-lation are unknown? Many animal labo-ratories are kept in basements, where hot/cool air conditioning systems, as well aselectromechanical laboratory equipment,are powerful sources of LFN. Likewise,many human subjects have an extensivehistory of LFN exposure that must betaken into account if their respiratorytract is under study or monitoring.The fact that LFN is not legislated, notevaluated during routine noise assessmentprocedures, and that LFN-exposed wor-kers are not afforded any protectionagainst this agent of disease is a very wor-risome state of affairs. In fact, a large partof the medical community still believesthat acoustic phenomena only impacts theauditory system, producing hearing loss,or via the auditory system, producingannoyance. It is painfully clear that a newattitude toward noise-exposed people isurgently warranted.
ConclusionsConclusionsConclusionsConclusionsConclusionsDespite the small number of subjects(n=13), all have disclosed the same typeof lesions even though their LFN expo-sures are distinct. This type of lesion isconsidered to be pathognomonic of VADbut, given the invasive nature of bron-choscopic examinations, the search forthis sign should be reserved for criticaldiagnosis, namely for forensic purposes.The results herein further substantiatethat VAD is in fact a mecano-transduc-tion disease.
A large part of themedical communitystill believes thatacoustic phenomenaonly impacts theauditory system

R E V I S T A P O R T U G U E S A D E P N E U M O L O G I A
Vol XII N.º 2 Março/Abril 2006
104
Participação das vias aéreas centrais na doença vibroacústicaJosé Reis Ferreira, Miguel B. Monteiro, Fernanda Tavares, Isabel Serrano, Emanuel Monteiro, Carla P Mendes,
Mariana Alves-Pereira, Nuno A A Castelo Branco
AcknowledgementsAcknowledgementsAcknowledgementsAcknowledgementsAcknowledgementsThe authors deeply appreciate the collabo-ration and assistance of the Cabin CrewUnion (SNPVAC).
BibliographyBibliographyBibliographyBibliographyBibliography1.Castelo Branco NAA, Alves-Pereira M. Vibro-acoustic disease. Noise & Health 2004; 6(23): 3-20.2.Castelo Branco NAA. The clinical stages ofvibroacoustic disease. Aviat Space Environ Med 1999;70 (3, Suppl): A32-9.3. Holt BD. “The pericardium. In: Hurst’s The Heart,V. Furster, R. Wayne Alexander, and F. Alexander(eds.), McGraw-Hill Professional Publishing, NewYork, 2001; 2061-82.4. Marciniak W, Rodriguez E, Olsowska K, BotvinI, Araujo A, Pais F, Soares Ribeiro C, Bordalo A,Loureiro J, Prazeres de Sá E, Ferreira D, CasteloBranco MSNAA, Castelo Branco NAA. Echocar-diography in 485 aeronautical workers exposed todifferent noise environments. Aviat Space EnvironMed 1999; 70 (3, Suppl): A46-53.5. Martinho Pimenta AJF, Castelo Branco NAA.Neurological aspects of vibroacoustic disease. AviatSpace Environ Med 1999; 70 (3, Suppl): A91-5.6. Gomes L, Martinho Pimenta AJF, Castelo BrancoNAA. Effects of occupational exposure to low fre-quency noise on cognition. Aviat Space Environ Med1999; 70 (3, Suppl): A115-8.7. Reis Ferreira J, Albuquerque E Sousa J, Mendes CP,Antunes M, Alves-Pereira M, Castelo Branco NAA.Loss of neurological control of breathing in vibro-acoustic disease patients. Proc. 11th Intern Cong Sound& Vib, July, St. Petersburg, Russia, 1745-52, 2004.8. Reis Ferreira J, Mendes CP, Antunes M, MartinhoPimenta AJF, Monteiro E, Alves-Pereira M, CasteloBranco NAA. Diagnosis of vibroacoustic disease –preliminary report. Proc 8th Intern Cong Noise as aPublic Health Problem, July, Rotterdam, Holland,112-4 (2003).9. Castelo Branco NAA. A unique case of vibroacousticdisease. A tribute to an extraordinary patient. AviatSpace Environ Med 1999; 70 (3, Suppl): A27-31.10. Castelo Branco NAA, Alves-Pereira M, Martinsdos Santos J, Monteiro E. SEM and TEM study of ratrespiratory epithelia exposed to low frequency noise.
In: Science and Technology Education in Microscopy:An Overview, A. Mendez-Vilas (Ed.), Formatex:Badajoz, Spain, 2002, Vol. II: 505-33.11. Castelo Branco NAA, Monteiro E, Costa e SilvaA, Reis Ferreira J, Alves-Pereira M. Respiratory epi-thelia in Wistar rats. Rev Port Pneumol 2003; IX-5:381-388.12. Castelo Branco NAA, Gomes-Ferreira P,Monteiro E, Costa e Silva A, Reis Ferreira J, Alves-Pereira M. Respiratory epithelia in Wistar rats after48 hours of continuous exposure to low frequencynoise. Rev Port Pneumol 2003; IX-6: 473-470.13. Castelo Branco NAA, Monteiro E, Costa e SilvaA, Reis Ferreira J, Alves-Pereira M. Respiratory epi-thelia in Wistar rats born in low frequency noise plusvarying amounts of additional exposure. Rev PortPneumol 2003; IX-6: 481-492.14. Castelo Branco NAA, Monteiro E, Costa e SilvaA, Reis Ferreira J, Alves-Pereira M. The lung paren-chyma in low frequency noise exposed rats. Rev PortPneumol 2004; X-1: 77-85.15. Sousa Pereira A, Águas A, Grande NR, CasteloBranco NAA. The effect of low frequency noise onrat tracheal epithelium. AviatSpace Environ Med1999; 70 (3, Suppl): A86-90.16. Grande N, Águas AP, Sousa Pereira A, MonteiroE, Castelo Branco NAA. Morphological changes inthe rat lungparenchyma exposed to low frequencynoise. Aviat Space Environ Med1999; 70 (3, Suppl):A70-7.17. Oliveira MJR, Sousa Pereira A, Águas AP,Monteiro E, Grande NR, Castelo Branco NAA. Ef-fects of low frequency noise upon the reaction of pleu-ral milky spots to mycobacterial infection. Aviat SpaceEnviron Med 1999; 70 (March, Suppl): A137-40.18. Sousa Pereira A, Grande NR, Castelo BrancoMSN, Castelo Branco NAA. Morphofunctionalstudy of rat pleural mesothelial cells exposed to lowfrequency noise. Aviat Space Environ Med 1999; 70(3, Suppl): A78-85.19. Mohr GC, Cole JN, Guild E, Von Gierke HE.Effects of low-frequency and infrasonic noise on man.Aerospace Med 1965; 36: 817-24.20. Ponomarkov VI, Tysik Ayu, Kudryavtseva VI,Barer AS, et al. Biological action of intense wide-bandnoise on animals. Problems of Space Biology NASATT F-529 1969; 7(May): 307-9.

R E V I S T A P O R T U G U E S A D E P N E U M O L O G I A
Vol XII N.º 2 Março/Abril 2006
105
Participação das vias aéreas centrais na doença vibroacústicaJosé Reis Ferreira, Miguel B. Monteiro, Fernanda Tavares, Isabel Serrano, Emanuel Monteiro, Carla P Mendes,Mariana Alves-Pereira, Nuno A A Castelo Branco
21. Cohen A. The influence of a company hearingconservation program on extra-auditory problems inworkers. J Safety Res 1976; 8: 146-62.22. Svigovyi VI, Glinchikov VV. The effect ofinfrasound on lung structure. Gig Truda Prof Zabol1987; 1: 34-7.23. Alves-Pereira M, Reis Ferreira J, Joanaz de MeloJ, Motylewski J, Kotlicka E, Castelo Branco NAA.Noise and the respiratory system. Rev Port Pneumol2003; IX-5: 367-79.24. Alves-Pereira M. Extra-aural noise-induced pa-thology. A review and commentary. Aviat SpaceEnviron Med 1999; 70 (March, Suppl): A7-21.25. Castelo Branco NAA, Fragata J, Monteiro E, Alves--Pereira M. Pericardial features in vibroacoustic diseasepatients. Proc 8th Intern Cong Noise as a Public HealthProblem, July, Rotterdam, Holland, 380-1, 2003.26. Castelo Branco NAA, Águas AP, Sousa Pereira A,Monteiro E, Fragata JIG, Tavares F, Grande NR. Thehuman pericardium in vibroacoustic disease. AviatSpace Environ Med 1999; 70 (March, Suppl): A54-62.27. Martins dos Santos J, Grande NR, Castelo BrancoNAA, Zagalo C, Oliveira P, Alves-Pereira M. Lym-phatic lesions and vibroacoustic disease. Eur JLymphology 2004; 12(40): 17-20.28. Martins dos Santos J, Grande NR, Castelo BrancoNAA, Zagalo C, Oliveira P. Vascular lesions andvibroacoustic disease. Eur J Anat 2002; 6(1): 17-21.29. Araújo A, Pais F, Lopo Tuna JMC, Alves-PereiraM, Castelo Branco NAA. Echocardiography in noise-exposed flight crew. Proc. Internoise 2001, TheHague, Holland 2001: 1007-10.30. Torres R, Tirado G, Roman A, Ramirez R, Co-lon H, Araujo A, Pais F, Marciniak W, Nóbrega J,Bordalo e Sá A, Lopo Tuna JMC, Castelo BrancoMSNAA, Alves-Pereira M, Castelo Branco NAA.Vibroacoustic disease induced by long-term exposureto sonic booms. Proc Internoise 2001, The Hague,Holland: 1095-98.31. Aiello M, Chetta A, Marangio E, Zompatori M,Olivieri D. Pleural involvement in systemic disorders.Curr. Drug Targets Inflamm Allergy 2004; 3(4): 441-7.32. Águas AP, Esaguy N, Castro AP, Grande NR,Castelo Branco NAA. Acceleration of lupus ery-thematosus-like processes by low frequency noise inthe hybrid NZB/W mouse model. Aviat Space
Environ Med 1999; 70 (March, Suppl): A132-6.33. Castro AP, Aguas AP, Grande NR, Monteiro E,Castelo Branco NAA. Increase in CD8+ and CD4+T lymphocytes in patients with vibroacoustic disease.Aviat Space Environ Med 1999; 70 (March, Suppl):A141-4.34. Ingber DE. Mechanochemical basis of cell and tis-sue regulation. NAE Bridge 2004; 34(3): 4-10.35. Ingber DE. Mechanobiology and diseases ofmechanotransduction. Ann Med 2003; 35: 1-14.36. Wang N, Butler JP, Ingber DE. Mechanotrans-duction across the cell surface and through the cy-toskeleton. Science (in Reports), New Series, 1993;260(5111): 1124-1127.37. Matthews BD, Overby DR, Alenghat FJ, KaravitisJ, Numaguchi Y, Allen PG, Ingber DE. Mechanicalproperties of individual focal adhesions probed witha magnetic microneedle. Biochem Biophys ResComm 2004; 313: 758–764.38. Alenghat FJ, Nauli SM, Kolb R, Zhou J, IngberDE. Global cytoskeletal control of mechanotrans-duction in kidney epithelial cells. Exp Cell Res 2004;301: 23-30.39. Alves-Pereira M, Joanaz de Melo J, MotylewskiJ, Kotlicka E, Castelo Branco NAA. Vibroacousticdisease II: The biological and acoustical basis of lowfrequency noise induced pathology. Proc InstituteAcoustics (UK) 2003; Vol 25, Pt 2: 73-9.40. Sanderson MJ, Dirksen ER, Satir P. Electronmicroscopy of respiratory tract cilia. In: DESchraufnagel (eds.) Electron Microscopy of the Lung.Marcel Dekker, Inc. New York-Baselp, 1990: 54.41. Silva MJ, Carothers A, Castelo Branco NAA, DiasA, Boavida MG. Sister chromatid exchanges workersexposed to noise and vibration. Aviation, Space andEnvironmental Medicine 1999; 70 (3, Suppl): A40-5.42. Silva MJ, Carothers A, Castelo Branco NAA, DiasA, Boavida MG. Increased levels of sister chromatidexchanges in military aircraft pilots. Mut Res - GenTox & Environ Mutag 1999; 44(1): 129-34.43. Silva MJ, Dias A, Nogueira PJ, Castelo BrancoNAA, Boavida MG. Low frequency noise andwhole-body vibration cause increased levels of sis-ter chromatid exchange in splenocytes of exposedmice. Teratogenesis Carcinogenesis Mutagenesis2002; 22(3): 195-203.

R E V I S T A P O R T U G U E S A D E P N E U M O L O G I A
Vol XII N.º 2 Março/Abril 2006
106
Participação das vias aéreas centrais na doença vibroacústicaJosé Reis Ferreira, Miguel B. Monteiro, Fernanda Tavares, Isabel Serrano, Emanuel Monteiro, Carla P Mendes,
Mariana Alves-Pereira, Nuno A A Castelo Branco








![Gamme de produits - bonfiglioli.fr · 9 Type Couple [Nm] C 05 C 12 C 22 C 32 C 36 C 41 C 51 C 61 C 70 C 80 C 90 C 100 7200 4000 2300 1600 1000 600 450 300 200 100 45 12000 Lorsque](https://img.pdfslide.fr/doc/110x75/5c644d3b09d3f26b1f8c80a5/gamme-de-produits-9-type-couple-nm-c-05-c-12-c-22-c-32-c-36-c-41-c-51-c.jpg)

















![Par Hortense BOHLER-HAAS hortense.bohler@luxroots.com … · 2016. 2. 25. · [=laboureur] ex Michelbuch et Maria Elisabetha MERGEN, Nicolai MERGEN et Dorotheae THOMé p.m.[= piae](https://img.pdfslide.fr/doc/110x75/60caa3d3c9df3a2c316a8dbb/par-hortense-bohler-haas-luxrootscom-2016-2-25-laboureur-ex-michelbuch.jpg)