-
7/29/2019 surgery Lec 2
1/26
wound
Management of wounds; Everybody of us are responsible to get
awound.
-we divided the Traumatic wounds to :-Sharp, penetrating: by
knife, sharp thin wire.
-Blunt: stone
-Bullet:
Types of wound:
We have a division of wounds due to the cause of it, and if
the
cause settles inside the body, or stroke the body without
settling
inside:
Cut wounds: during shaving, cutting meat.
Learning points of
this lecture are
about:
Wound, ulcer,
fistula, cyst
The wound either be
traumatic surgicalhappens by
accidents
made by
surgeons
most ofour talk will be
about
traumatic
wounds which
cause by Car
accidents, by
Falling from
high places,,,
etc.
-
7/29/2019 surgery Lec 2
2/26
Lacerated wounds: when someone strikes u by a stone or stick
andu get a wound, and u can describe that wound that its Broken
and
irregular.
Crushed wounds: when a stone fall into someone or car hit
him.
Wounds with skin loss : by a drill, piece from skin loss in
place ofaccident.
Examination of Wounds: its a very important step, u must care
ofit.-By examine the wound I can know :-the extension of the
wounds,
-how its deep, -if there is any associated injures.
Associated injuries:
In emergency room there is a lot of cases about people
come with a horrible look, their heads covers with blood,
butwhen uput them on the table and remove the blood, cut the
covering hair, may
found thats a very small wound, anyway, u must examine the
wound
carefully, maybe inside that a small wound there is a stone,
glass,
breakage of bone, so the examination of the wound is very
important, to
know the extent of the wounds, and to know if we have
associated
injures,
Always the people concern about the superficial wound, but
often
there are things inside are more serious, so we must care about
the
muscles, vessels, tendons, and bones that there location in, or
near the
injured site.
Eg; A patient with an injured wrist by a knife, we
haveunderneath that area artery and tendons that moven the fingers,
there
is a nerve that moven the muscle, and the nerves that get us
the
Examination
of Wounds
It's as
important as
history if the
patient was
unconscious.
-
7/29/2019 surgery Lec 2
3/26
sensations, and any one of them may get associated injure, so we
have
to examinecarefully.
Abdominal cavity: Eg; patient have an injury in the abdomen by
athin sharp wire as example,,, so we must be aware about everything
in
the place of injury, to impose the injury was near the spleen,
we must
think about the stomach, the colon, the kidney, even if it
looks
superficially not deep, but in deep may there is a server
bleeding.
Chest cavity: we must be aware about the lung the heart,
maybethere is a collection of air or blood in plural space.
cranial cavity: Eg; someone striking with stone, he come
tohospital walking as normal, the wound was small, the Dr suture
it, but
after six hours the patient come back in a coma, after a new
examination, the Dr found that the patient has a broken cranial
bone,
there is sub- cranial bleeding, that compress the brain
associatedinjury.
Types of Suturing:
- Primary suturing :if the wound was in the skin and clean we
suture
it.
-Excision and primary suturing: we cutting from the wound
and
then do suturing.
-Delayed primary suturing: I want to delay the suturing to
next
day or like that.
-Secondary suturing: suturing after a week, I can't suture it
today
or tomorrow.
-Skin grafting.
so u have
to ensure
there is no
associated
injuries
-
7/29/2019 surgery Lec 2
4/26
: if we dont suture the wound ,,,The big questionwhat will
happen??
-The wound will heal ,,, as simple as this >> the
explanation is:Our Great Creator gives us all the mechanism of
healing, so we asDoctors, we just accelerate this mechanism,
because if we dont do
suturing the process of healing will delayed and inflammation
will
occurs, and the final result will be a large scar.
How do we think to choice thetype of suturing????!! when the
wound is clean "there edges very regular and there is no debrison
it" we do primary suturing-after antiseptic for sure-
when the wound is polluted with debris like soil and glass, and
thereedges not regular, so we need first of all to regulate the
edges and clean
the wound then suture it so we do excision and primary
suturing,
If the wound was" a crashed wound"; we have hematoma,
swelling,broken bone underneath it, obstructing vessels
>>> we can't do suturing to
it, how we deal with it: we clean it, and wait to second day
third day until
the inflammation gone and the suturing become possible so we
dodelay primary suturing.
if the suture delay more than that time- like a week- we name
thesuturing a secondary suturing.
-
7/29/2019 surgery Lec 2
5/26
But when we do suturing; we lower the distance between edgesof
the skin, so the space that must filled with granulation tissue
will
be very minimum, and that of course mean that the process of
healing become easier for the body, and the scar that forming
will be
very minimum.
,contractionthe wound will??occursHow the healing-
the space between the walls of wound will filled with tissues
that will
forms from the edges of the wound, with blood supply will
form
granulation tissues, and after filled, it will convert to
fibrous tissuethe skin will growth and form epithelium
"epithelization".
Phases of healing:that-macrophagesneutrophil,
and,phagocytesthe,:Lag phase
doing phagocytosis- will go to site of wound to remove the
damaged
tissue and any sign of inflammation.
the phase that the granulation tissue:Proliferation phase
will form.
tissue form andfibrouswhen:(differentiation)Maturation
cover the skin(epithelization).
---------------------------------------------------------------------
is the granulation tissue which is forms and:The organ of
repairfills the cavity, and form a new cavity instead of tissue
which was lost
in the accident.
-------------------------------------------------------------------------------
Elements of
healing:
contractiongranulationtissue the
epithelization
.
-
7/29/2019 surgery Lec 2
6/26
------------------------------------------------
from the wound, andbiopsyif we take a:Wound histologyexamine it
in the lab, what are the cells that are proliferating
there???
amount, they goplenty"neutrophils" are there, byfirst dayat
the-
out of the capillary and get into the tissue, and engulf the
foreign
bodies by phagocytosis,
we find monocyte, the monocyte have the same:hrs.after 24-
function as phagocytes,
since thefibroblast; which working in building unit,:6
days-after 5-
fibroblast is the cells that form the connective tissue, this
fibroblast
appears in the surrounding tissue,
6 day-will appear by the 5the capillary-
.dayth
after 4collagenthe-
thebuildingsstartit6 days-Once the wound in the 5
collagen that forms from fibroblast, , and in the same duration
in the
wound, the microbes release an enzymes that lysing the
collagen
"collagenase", but if the immunity of the person is good the
collagen
synthesis will overcome the collagen lysis ..
Factor affecting healing
: does after suturing and healingwound strength
occur the strength of the skin will back to original one?
When I open the muscle and go to the abdomen and then
suture them,, does the strength of the muscle come back
as it was??
No,, it will never come back to normal, usually by six
month it will have maximum strength which is less than
the original one (come back to 60, 70 % of their original
strength )
neutrophils
represent
the firstline
defense.
the collagen
is the
connective
fibers which
gives
strength to
the tissue
-
7/29/2019 surgery Lec 2
7/26
What are the factor delay healing?? Why w e findpeople with fast
healing and others are not??-the age: healing in young and children
is better than elderly.
-the nutrition: if the person have protein, ascorbic acid or
zinc
deficiency, this will delay healing.
-vascularity: if the tissues have good blood supply, the healing
will be
quick.
-sepsis: if the wound infected the healing will delay.
-oxygenation: its related to vascularity.
-Wound dressing: if the wound contaminated we have to repeat
dressing.
if the wound is clean, we dont repeat dressing,but clean wound
that will interrupt with thebecause repeat dressing in a.healing
process, and this will delay the healing
types of healingfirst intention: if I suture the wound, the
spaces between twoedges become too minimum, so the healing is
quick.
Second intention: if the wound is wide, and it remains open all
thetime, it will need to fill this cavity-in a month maybe-, at the
end we
get a scar which is very wide and thick.
bullet injures- it has many types: high velocity missile,
shockwaves,
temporary cavitation.
-
7/29/2019 surgery Lec 2
8/26
high velocity missile: the bullet inter the abdomen -as
example,andinjures the liver or colon, then it may go out or remain
inside. It can
also pass just through the skin.
Even if it pass just through the skin, the shock waves that
Generated
by it, will damage the liver, even if it doesnt pass through
it.
the temporary cavitation: if the bullet pass the liver from
point toanother point, the damage will not only in the tract "that
made by
passing the bullet", the damage will extend to the surroundings
of
the tract, by the effect of cavitation.
:slast injursometime we will have complex blast waves: no only
the explosion
will make a shock wave, but the shrapnels too, and even ifwe
dont
hit directly by the blast, we may have injury by the" mass
air
movement"because the air in this area if it has an explosion the
air
will move to another side rapidly and can shattered.
Surgical woundsMade by surgeon in a regular way , under
anesthesia, under
complete aseptic condition, so there will be no
contamination.
surgical wound
clean
contaminated
dirty
cleancontaminated
high velocity
missile: whichis the
automatic
weapons like "
Kalashnikov"
and the velocity
of them is very
high, more
than 16m/sec,
and we have
the low
velocities, and
blast waves
-
7/29/2019 surgery Lec 2
9/26
patient: Dr u will do to me "a thyroid operation",
what's the possibility that my wound will get inflamed??
Dr :very minimal,, because the operation is clean.
Patient: Why clean??
Dr: the thyroid is sterile, it dont have any microbe, the wound
will be
clean, the possibility of wound infection is very minimum.
-petiant2: Dr u will remove my Gallbladder, what's the
possibility
that my wound will get inflamed??
Dr: HERE the possibility of wound infected is more,
WHY??Because
while I cutting through the duct, I open the biliary system, and
the
biliary system which have bile which have microbes, those
microbe
which lives normally inside the body, can contaminate the wound,
so
this wound is clean contaminated.
Petient3: Dr u will remove my appendix, what the possibility
to
wound infection??
Dr: according to the appendix, if it is inflamed so,, its fill
of
microorganism and pus cells, so whatever u do to isolate it
going to
contaminate, so the % from 15-20 %,BUTifthe appendix was
gangrenous or the colon have gangrene and it has a lot of stool,
sothis wound get infected in highly percent may reach to 40%, so
this
wound we can classified it" dirty".
So if the operation was mastectomy >>> clean.
Hernia>>> clean
Gallbladder and it acutely inflamed>>>
contaminated.
In first case
the
possibility of
wound
infection b/w
0-2%, the
second case
like 10%
-
7/29/2019 surgery Lec 2
10/26
Now, why we classifying this like that???
Because we want to inspect how much inflammation we get, to try
to
reduce this incidence, so; in clean operation we dont give
the
patient antibiotics, like in thyroid operations, that considers
a mistake
if we give the patient of thyroid operation an antibiotic.
While, clean contamination, like gallbladder operation in case
it is
not inflamed but have a stone, we give the patient one dose
antibiotic
which called prophylactic antibiotic- because while am
removing
gallbladder and during explosior of contaminations, we have
high
level of antibiotics in blood, so I reduce the possibility of
infection, andsometime, we may give in the
contaminatedcasesprophylactic and
wait to three days, In dirtycases we wait till five days or week
maybe.
So this is to gauge how much the wound will affect by
infections,
and to decide which patient we should give an antibiotic at
which
time, and for how long.
:actors which affect healingMalnutrition, ureamia, malignancy,
radiothempy,:General-
cytotoxic drugs, diabetes, "vit c" deficiency.
,and FBBlood supply, presence of necrotic tissue-Local
Factors:-
presence of hematoma, excessive cauterization, rough
manipulation,
" THE GOAL of suturing the wound is toinfection, Tension in
wound
approximate the edges but not to strangulate the wound, if
the
edges of wound dont meet together I should not put intension, if
Iin wound where will be no blood supplying and themake
intention
.healing will delay"
Now,, after we manage the wound, what's the problems
that may happen??
Prophylactic
antibiotics
gives in all
cases of
surgical
wound
except: the
clean one
-
7/29/2019 surgery Lec 2
11/26
the sings of wound infections??what's,, but,,,wound
infection
Redness, swelling, pain, fever, tachycardia..
When the wound get infected,,, what I should do??
-I dont give the patient antibiotic but I open the wound or part
of it,,
so the collection of pus will go out, and give antibiotics if
there is a
surrounding cellulitis.
if we open the wound in first few days of suturing, it will be
very:Pseasy to open and maybe it opens by itself by the effect of
collection
and pus, but with passaging of time the wound become harder
and
harder.
while the surgeon work in abdomen, like:Wound dehiscence
bowel obstruction operation, in the end of it, he sutures the
layers of
abdominal wall, and the most important layers is the
aponeuroticlayer- muscular layer- and suture it by no absorbable
suturing
filament, in the end of 7th
day after operation that there is a swelling
in wound and fluid coming out, and when we examine we may
found
that the bowels coming out between the muscles and collecting
below
the skin directly which we call it" Wound dehiscence". and that
may
occur because of increase in the abdominal pressure, so
after
operation we should for many days avoid occurring the intra-
abdominal pressure which may occurs by intension, sever
cough,
sever constipation,
-Hyper trophied scar, keloid:
When the patient has thyroid swelling, asking for operation,
after he
considers in his mind the cosmetic appearance for sure, and we
do a
plastic cosmetic operation and after the 7th
day we look at it , we find
it very fine, very thin, difficulty to seen it, but after a
month he come
back, and his wound is thick and red in color" hyper trophied
scar"
-
7/29/2019 surgery Lec 2
12/26
Why that happens??!!
It's not caused by the surgery, its sometimes due to the
patient, to
the area.
The story is the wound after it heal,, it continue growing, and
become
red in color with an itching state, and this case is more in
pregnant
woman, and in wound that in bony contours, so I try to
overcome
doing insegen in the shoulder, over the sternum, which is the
areas of
probability of trophied scar to occur.
Anyway, we said to patientdont worry, we will wait for six
weeks,
and it will reduce by itself and sometime we inject in it a
corticosteroid and sometimes using laser to reduce it.
:loidkecalledin thingproblemThe more big
It's rare, I do the surgery, in appropriate manner, but after 2
to 3
month the wound gets growth, after 6 month it still growing,
andinvade the surrounding areas and it may reach areas we dont
wound
it,,, this is keloid, and its due to the body itself, growing a
lot of cells
more than needed and even if we remove it , it will recur and
need
many operations.
IS THERE A POSSIPLITY OF LATENCY OF THE
INFECTION TO INFECT THE WOUND?:?
USUALLYTHE infection of the wound occurs in the end of the
week,
and if the wound completely healed after one or two weeks,
it's
unlikely to get wound infections after month or two, except in
some
cases, when there is a retained foreign bodied-stone, glasses-,
deep
-
7/29/2019 surgery Lec 2
13/26
in the wound,, or there is non-absorbable Internal stitch, it
may get
infected.
the time rate of the injury to heal?
The healing in the skin and the appearance of epithelization
ends in
the first week almost, However; the wound itself not mature
enough,
it will continue maturing till 6 month, and that include the
bone, since
when we have bone fracture, we use plaster to confirm the bone
and
prevent the patient from walking if the fracture was in his leg
till 3
month,, until his fracture healing become more strength.
can we associate more than one type of wound with
another, during surgery??
-if I was doing a hernia surgery and in the same time the
patient was
having a mass in his inguinal region and we removed it
normally
BUT, IF I WANT to remove perforated appendix, and I found a
hernia near of it, I can't do it in the same time, because the
first one
is contaminated, and will infect the other.
What is the Difference between clean contaminated
and contaminated??
-clean contaminated means that there is a possibility of
contamination but not always, for example, if I open the
stomach,
which have an acid, so usually the microorganisms in it very
low, if I
open the common bile duct usually it's not having microorganism,
if Iopen the pelvis of the kidney, its unlikely to have
microorganisms but,
-
7/29/2019 surgery Lec 2
14/26
if have some infection, it can contain, while if I open the
colon, this is
absolutely contaminated,
how can we differentiate between contaminated and
dirty??
-this depends upon the degree of contaminations, like, sometimes
I
go and remove the appendix, pus is coming out from
appendix-its
contaminated- but sometimes I go to remove the appendix and
I
found that the abdominal cavity is full of pus and feces, and
the smell
of the theater is full of feces, so this is dirty, so when
the
contaminated is very massive its dirty.
lcersU
Ulcer: is a break in continuity of the skin, or its any
discontinuity in any epithelial surface, orits a microscopic
discontinuity of normal epithelium, epithelium like skin and
mucous membrane, the mucosa of the mouth, mucosa of
the stomach, so ulcer may happen in skin, mouth, stomach,
intestine, , , and if the discontinuity are microscopic we
call
it erosion.
Ulcers are non-healing wounds that develop on the skin,
mucous membranes or eye. Although they have many
causes, they are marked by:
1-Loss of integrity of the area
-
7/29/2019 surgery Lec 2
15/26
2-Secondary infection of the site by bacteria, fungus or
virus
3-Generalized weakness of the patient
4-Delayed healing
:ocation-Lower limbs: most ulcers of the foot and leg are caused
by
underlying vascular insufficiency . The skin breaks down or
fails to heal because of repeated insult or trauma.
-Mouth ulcers: by fungal, or virus infections.
-Ulcers in sacrum: like diabetic patient which has ulcers in
their legs, and it's not healing, because he has delay in
the
healing mechanism.
-Peptic ulcers: this kind of ulcer occur by digestion of the
entire acids and enzymes to the mucosa of the stomach or
duodenum, so it will ulcerate. This includes ulcers of the
esophagus, stomach, large and small intestine.
-Genitalia: May be penile, vulvar or labial. Most often are
due to sexually-transmitted disease.
:ausesin form of wound,sforms, it startitUsually the ulcers
when
, and otherbacteriathecalculatesand it does not heal, so it
.which inflame the wound and delay the healmicrobes
-
7/29/2019 surgery Lec 2
16/26
And some time there is no infection, there is a cancer,
likepatient comes to Dr and said he has a mass in his face and
then it ulcerated, from 6 month and it does not heal,, so
this
not ulcerthis is cancer.
another patient came with Venous stasis, in her lowerlimps, for
the last five years, but recently, her leg gets
ulcerated "that does not heal", this is venous ulcer.
Arterial insufficiency:patient with ischemia in lower limps,
the blood supply to his lower limps is occluded, the wound
is
very painful.
-Diabetes: the diabetic patient with wound for 6 month or
more and not heal, if the diabetic patient has wound
infection, and ulcer in his leg it's like to be as a fire in
the
forest, the ulcer will spread, why??,,,, because all the
factor
that needed in the healing process is defective.And the
blood supply in diabetic patient; he has arteries sclerosis,
the
sensation is absent" neuropathy", he does not feeling in any
kind of pain" loss of sensation", he has retinopathy, he has
impaired immunity, so the wound dont heal quickly, in
contrast it spread quickly.
-Loss of mobility: in Patient which is incapable of
movement,
large ages, which need someone to change his position, hewill
get ulcer, as a result of pressure with no blood supply.
:escriptionyou have to describe the features of the ulcer; Site,
Size,
shape, base, edges, tenderness, discharge and surrounding
tissue and lymphatic's.
Those should be
describe
because it will
give usimpression if
the ulcer will
heal or not
-
7/29/2019 surgery Lec 2
17/26
I
:lcerationschemic- those patient with lower limp arteries
sclerosis are more
acceptable to get ulcer, because there is no blood supply,
- In elderly , who also have symptoms of coronary vascular
disease.
this patient has problem in the -blood supply and has ulcer
in
the dorsum of the index.
this is an ulcer in the tip of
pecto, and this ulcer may is ischemic ulcer, or diabetic
patient.
Practices:
Ifthe patient has ulcer in the upper half of the face, and
its
shape is circular, the edges is rolled, so I said these is
:basal cell carcinoma"
Ifthe ulcer found in the foot and its very painful to
patient,
so I said this is "ischemic ulcer"
Ifthe ulcer in the foot and their smell awful, and it give
out
a pus, and the patient dont feel anything,, so I said this
patient is "diabetic".
-
7/29/2019 surgery Lec 2
18/26
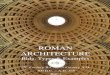
-When we see this picture, we can
notice that the base of ulcer is red,
andthats a good sign of healing,
because when we find the floorblack, and have pus, this is
infected
ulcer.
-Look to the edges we call it sloped edges, and also is a
sign
of healing.
ents havei; loss of sensation, occur in patulcerNeuropathic
diabetic, paraplegia.
:Causes
-peripheral nerve lesions diabetes ,nerve injuries
-Spinal cord lesions
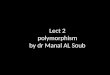
This is pic of ulcer in diabetic patient, the ulcer
occurs in the pressure areas.
,femalesoccurs usually in:The venous ulcers:
This is a venous ulcer, you will seevaricosities,_"varicosities
is venous
veins which is congested and dilated".
It's found everywhere, and we found pigmentation on it, in
the
-
7/29/2019 surgery Lec 2
19/26
middle aspect of the lower third of the leg, this area
called:"
gatal area".,,,,,,,,,,,,,,,,,,,,,,,,,, MAY ALLAH PROTECT US
.
what's the cause of gastric ulcer??
-the stomach HCL main function is to digest the protein,
BUT,
sometimes due to excessive production of IT, it will digest
the
mucosa of the gastric, new thing is explorer recently that
thereis a bacteria called "helocapterpylori " may exist in the
stomach and react with the HCl and cause ulceration, so we
can stop this bacteria by reducing HCL production.
estulasDefinition: Fistulas is an abnormal communication
between tow epithelial -or endothelial- surfaces.
The
medications
given;
lansoprazole
, and
antibiotics.
-
7/29/2019 surgery Lec 2
20/26
,edthe feces collectin itwe see the anal canal which:picIn
then it will go out by auns canal, thats the normal
scenario.
But,,, there is some people have another opening for feces,
this opening is end of a canal, which having another opening
inside to anus canal, so its abnormal communication between
the skin and the lining of anal canal, so the feces and
secretion
will discharge to go out from the extra abnormal canal.
Why that happens??
-before the canal form, an abscess form with pain sensation,
this abscess is open in and out, but the patient dontaware
only
to the out one, and at the way of the abscess we found a
track,
which is not closed and this is the fistula. This is acquired
fistula.
-May all of us hear about new baby born with difficulty in
breathing, when his family fed it the food go to the lung,
Types of
fistula:
Congenital
Ac uiredexternal
Arteriovenous fistulas
Internal abdominal fistulas
External abdominal fistulas
Congenital and acquired(traumatic or
iatrogenic)
-
7/29/2019 surgery Lec 2
21/26
because of abnormal communication between the trachea and
,fistulacongenital, this is athe esophagus
-Sometimes the fistula may happen between vain and
artery"".fistulasArteriovenous
-A patientwith mammal fistula," abscess in the breast",
happen in pregnant woman or after delivery, after the
abscess
opened, at the site of drainage of the abscess the milk
eject,"
the milk come out not from the nipple but from nearby" this is
a
fistula between the ducts of milk and the skin.
-A patientget operation, he remove the gallbladder, the
biliary
canal-common bile duct- tied, but after a while I found that
the
"bile isfistulabiliary,,, this is abile come out of the
wound
coming from the wound", there is abnormal communication
between the biliary tree and skin.
-A patientwith bullet inside his body, the bullet get inside
the
pancreas "the pancreas produced pancreatic juice",
The pancreatic juice will go to the bowel but since the
wound
reach the pancreas, so the pancreatic juices coming out
through
the wounds, and after 2-3 month the pancreatic juice will
apancreatic fistula"the,,,,, this iscoming on skin by the
woundcommunication between the skin and the pancreas".
get a hit with knife, the: a patientfistulaGastrocutaneous
knife go inside the stomach , in operation the stab wound in
the
stomach closed, but it was a big stab, in the next day he have
a
wound infection, in the 7ht-8th
day when he start eating, the
food go out from the wound, the stomach opens in the skin thisis
Gastrocutaneous fistula.
-
7/29/2019 surgery Lec 2
22/26
.jejunumandstomachbetween:Gastrojejunocolic fistula-
do operation to him, we cuta patient we:mall bowel fistulaS-part
of his bowel that is gangrenous as example then we suture
the bowel with each other -that called" anastomosis"
After week -10 days the wound secret pus and intestinal
contents. Because there is opening between small bowel and
stomach.
had operation in his colon,patienta:fistulaExternal colonic-
suture the colon after trauma and suture the skin
overlaying,
after few days the feces go out from the wound, and have a
complications between the colon and skin.
ladies,that happens with:and colovaginal fistulasColovesical
in cases of obstructed labor, so the head of the baby get
necrotic in the neck of uterus, and it will open on the
bladder,
and the urea go up from the bladder to the uterus and the
anus,
".covaginal fistulavesi"That called
.
The colon can also open in the vagina and the feces go:PSout
from the vagina.
:yst, normal orlined cavity or sac-closed epitheliumany
abnormal, usually containing liquid or semisolid material.
-
7/29/2019 surgery Lec 2
23/26
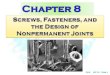
:cysts in the neck
Branchial cleft cysts: In imperiology phase there is arches,
and it will disappear and some of
it may remain, so may a baby born
with a cyst in his neck, and that
because one of this clefts did not
obliterated, this is a brainchial
cyst.
Thyroglossal duct cysts: When the thyroid gland formed, its
formed by Thyroglossal duct, this
duct will extend from the
posterior of the tongue to the
neck region, once the thyroid
gland form and the duct
disappear, sometimes some ofthe remnants' form a cyst "
Thyroglossal cyst".Dermoid cysts: after 1-2years of
born of baby, we notice a swelling inthe outer border of the
eyebrow, its
congenital because there is a part of
skin cells implanted under the skin
and make the dermoid cyst,, we
remove it by excision.
-
7/29/2019 surgery Lec 2
24/26
Sebaceous cysts: its a small cyst
in the scalp, highly prevalence, and
its mobile attach to skin, contain
sebaceous materials.
a child with a swelling in the:in pic
midline under the chin directly,
when he swallow saliva it moves
and when he rise his tongue it will
go up.
Thats it
All extra info in slides are not included.
Malaysian brothers and sisters,,, for u, I did best what I can
do
,,,:D
For my wonderful batch:
( , )
DONE BY: Asmaa Almawas
-
7/29/2019 surgery Lec 2
25/26
-
7/29/2019 surgery Lec 2
26/26