Embed Size (px)
Citation preview

Cas cliniques
DOI of or1Unit of V
Hospital, Ferra2Departme
of Ferrara, Fe
Correspondvascular Surg44100 Ferrara
Ann Vasc SurDOI: 10.1016/� Annals of V�Edit�e par ELS
Traitement d’un faux an�evrysme carotidienpar un stentgraft enduit d’h�eparine
Tsolaki Elpiniki,1 Elisabetta Salviato,2 Tiberio Rocca,1 Lucia Braccini,1 Roberto Galeotti,2
Francesco Mascoli,1 Ferrara, Italie
Les faux an�evrysmes carotidiens sont une cons�equence rare de la chirurgie, des traumatismes,et des infections carotidiens. Historiquement, les an�evrysmes et les faux an�evrysmes carotidiensont �et�e trait�es chirurgicalement. Cependant, les techniques endovasculaires sont r�ecemmentdevenues une alternative valide pour le traitement des faux an�evrysmes carotidiens. Le casd’un homme de 57 ans avec un faux an�evrysme de l’art�ere carotide interne droite est d�ecrit.Le malade �etait venu dans notre unit�e avec une masse indolore et pulsatile du cou, qui sed�eveloppait lentement. Cinq ans plus tot, il avait eu une chirurgie d’un an�evrysme sacculairesitu�e sur le segment extra-cranien distal de l’art�ere carotide interne droite. Le faux an�evrysme�etait trait�e avec succ�es avec un stentgraft Viabahn enduit d’h�eparine (WL Gore, Flagstaff, AZ,USA). Les stentgrafts enduits d’h�eparine peuvent etre employ�es pour le traitement des l�esionscarotidiennes et peuvent offrir une protection contre l’hyperplasie intimale et la thrombose.D’autres �etudes sont n�ecessaires pour �evaluer les r�esultats �a long terme.
Carotid pseudoaneurysms occur after carotid artery
surgery, traumas, neck surgery, and infections.1,2
They are usually painless, continue to grow slowly,
and manifest as a pulsatile mass in the neck.3
However, they can manifest with more severe
symptoms such as hemorrhage caused by rupture or
with neurological symptoms caused by cerebral
embolization.4,5 Although historically carotid
aneurysms and pseudoaneurysms were treated
surgically,6 covered stents or stent-grafts have
become a recent alternative treatment for this
pathology with encouraging mid-term results. This
iginal article: 10.1016/j.avsg.2010.02.046.
ascular and Endovascular Surgery, S. Anna Universityra, Italie.
nt of Vascular and Interventional Radiology, Universityrrara, Italie.
ence : Tsolaki Elpiniki, Unit Of Vascular And Endo-ery, S. Anna University Hospital, corso Giovecca 203, Italie, E-mail: [email protected]
g 2010; 24: 952.e9-952.e12j.acvfr.2011.03.009ascular Surgery Inc.EVIER MASSON SAS
case report describes the use of a covered stent to
treat a carotid pseudoaneurysm.We believe that the
use of a covered stent with a heparinized surface
may have advantages as compared with other
stents, in terms of decreasing the risk of thrombosis
and perhaps intimal hyperplasia.
METHODS
A 57-year-old man came to our unit with a painless,
progressively growing and pulsating neckmass. Five
years earlier he had undergone surgery to remove a
saccular aneurysm located on the distal extracranial
segment of the right internal carotid artery (ICA).
The treatment consisted of aneurysmectomy and
end-to-end anastomosis. His medical history was
unremarkable and he did not show signs of dys-
phagia, fever, respiratory difficulties, or central
neurological symptoms such as transient ischemic
attack or stroke.
The ultrasound examination showed a partially
thrombosed pseudoaneurysm, involving the third
distal extracranial segment of the right ICA. It mea-
sured 40 � 60 mm and was caused by a dehiscence
1036.e1

Fig. 1. Preoperative computed tomography angio scan
showing the carotid pseudoaneurysm (arrow).
1036.e2 Cas cliniques Annales de chirurgie vasculaire
of the surgical anastomosis. The head and neck
computed tomography angio scan confirmed the
ultrasound findings (Fig. 1).
Urgent endovascular management was proposed
and the patient gave his informed consent after the
potential risks and benefits of the proposed treat-
ment had been explained to him. The patient was
not administered clopidogrel before surgery. In the
operating theatre, after administration of 5,000units
of heparin, a selective angiogramof the carotid bifur-
cationwas performed through a right femoral percu-
taneous access under local anesthesia. A 0.035 in
guidewire (Implants Super stiff, Boston Scientific,
Natick,MA)was placed in the external carotid artery
after a 7F introducer sheath was placed in the
common carotid artery and a roadmapwas obtained
to localize the lesion more precisely. After catheteri-
zation of the ICA by a 0.035 in Terumo guidewire
(Terumo Medical Corporation, Japan), a 5 mm �2.5 cm Viabahn stent-graft with heparin surface
(Gore AL, Flagstaff, AZ) was placed on the ICA to
cover the dehiscence (Figs. 2A, B). No cerebral pro-
tection device was used because there was no evi-
dence of atherosclerotic lesions or dissection. The
completion angiography demonstrated an endoleak
caused by incomplete expansion of the stent-graft,
which was successfully treated by dilation with an
angioplasty balloon catheter (Ultrasoft 5 � 2 mm,
Boston Scientific, Natick, MA). The final angio-
graphy showed the complete exclusion of the pseu-
doaneurysm and patency of the carotid arteries
(Fig. 2C). An Angio-seal closure device (St. Jude
Medical St. Paul, MN) was used to seal the femoral
artery puncture.
The postoperative stage was uneventful and the
patient was discharged on the second postoperative
day with double antiplatelet therapy (clopidogrel,
75 mg; aspirin, 325 mg).
Clinical and ultrasound follow-ups were per-
formed, as well as angiography, 1, 3, and 6 months
postoperatively. They showed complete exclusion of
the lesion and patency of the ICA, with no evidence
of stenosis or intimal hyperplasia (Figs. 3A-C).
DISCUSSION
Carotid pseudoaneurysms occur after carotid artery
surgery, traumas, neck surgery, and infections.1
Surgical treatment is not always feasible, especially
when lesions are situated near the base of the skull,
because of difficult exposure, distal vascular control,
and the high rates of associated cranial nerve inju-
ries (3-13%).
Recently, endovascular techniques have become
a valid alternative for the treatment of carotid
pseudoaneurysms. Hoppe et al. report encouraging
short- and mid-term results after stent-graft place-
ment in cases of carotid aneurysms, pseudo-
aneurysms, and carotid blowout syndrome.7
However, distal embolization,8 stent thrombosis,
dissection, and restenosis are some of the most
severe complications following carotid stenting,
even when antiplatelet therapy is administrated.9 It
is believed that intimal injury of the artery during
carotid stenting triggers platelet activation and
aggregation, as well as the inflammatory cascade
with subsequent smooth muscle proliferation. Fur-
thermore, thrombus formation immediately after
carotid stenting and embolization to distal sites can
cause serious postprocedural complications. The
most important factors contributing to stent
thrombosis include the small size of the vessel, stent
under-dilation, and the presence of proximal or
distal dissection.10 Chaturvedi et al. and McKevitt
et al.11,12 suggest that double antiplatelet therapy
after carotid stenting plays an important role in
reducing adverse neurological outcomes without
further complications of increased bleeding.
With our patient, the decision to give him endo-
vascular treatment was based on the perceived diffi-
culty of exposing the ICA because of previous
surgical repair and the distal extent of the lesion.
Thus, placement of a short, self-expanding stent-
graft was considered an applicable and minimally
invasive therapeutic approach as the pseudo-
aneurysm was caused by dehiscence on the ICA
anastomosis. The choice of a heparin-surface stent
was based on the possibility of additional protection
against intimal hyperplasia and thrombosis. In the
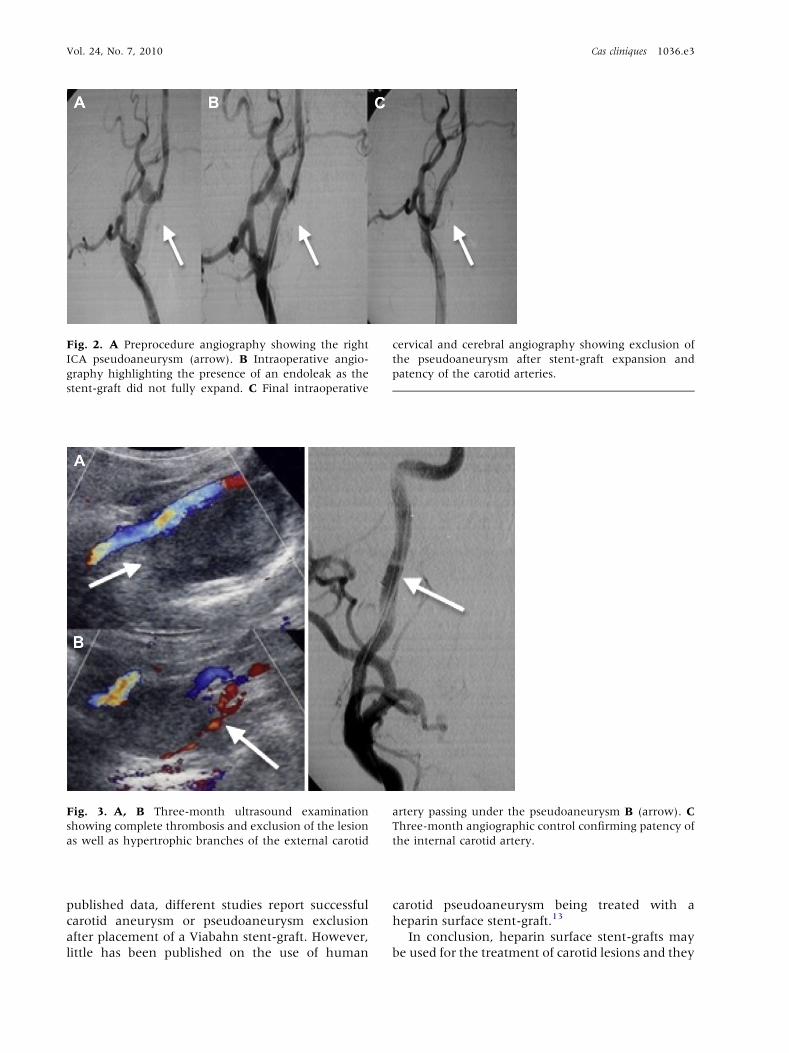
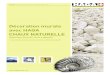
Fig. 2. A Preprocedure angiography showing the right
ICA pseudoaneurysm (arrow). B Intraoperative angio-
graphy highlighting the presence of an endoleak as the
stent-graft did not fully expand. C Final intraoperative
cervical and cerebral angiography showing exclusion of
the pseudoaneurysm after stent-graft expansion and
patency of the carotid arteries.
Fig. 3. A, B Three-month ultrasound examination
showing complete thrombosis and exclusion of the lesion
as well as hypertrophic branches of the external carotid
artery passing under the pseudoaneurysm B (arrow). C
Three-month angiographic control confirming patency of
the internal carotid artery.
Vol. 24, No. 7, 2010 Cas cliniques 1036.e3
published data, different studies report successful
carotid aneurysm or pseudoaneurysm exclusion
after placement of a Viabahn stent-graft. However,
little has been published on the use of human
carotid pseudoaneurysm being treated with a
heparin surface stent-graft.13
In conclusion, heparin surface stent-grafts may
be used for the treatment of carotid lesions and they

1036.e4 Cas cliniques Annales de chirurgie vasculaire
offer additional protection against intimal hyper-
plasia and thrombosis. Further studies are needed to
evaluate the long-term results for this new device.
REFERENCES
1. Raptis S, Baker SR. Infected false aneurysms of the carotid
arteries after carotid endarterectomy. Eur J Vasc Endovasc
Surg 1996;11:148-152.
2. Wyers MC, Powell RJ. Management of carotid injuries in a
hostile neck using endovascular grafts. J Vasc Surg 2004;39:
1335-1339.
3. Pratschke E, Sch€afer K, Reimer J, et al. Extracranial aneu-
rysms of the carotid artery. Thorac Cardiovasc Surg 1980;28:
354-358.
4. Ahuja V, Tefera G. Successful covered stent-graft exclusion
of carotid artery pseudo-aneurysm: two case reports and
review of literature. Ann Vasc Surg 2007;21:367-372.
5. Khan MI, Tariq M, Rashid D. Transient ischaemic attacks
due to a pulsating mass in the neck produced after incision
and drainage of parapharyngeal abscess. J Ayub Med Coll.
Abbottabad 2008;20:143-145.
6. Attigah N, K€ulkens S, Zausig N, et al. Surgical therapy of
extracranial carotid artery aneurysms: long-term results
over a 24-year period. Eur J Vasc Endovasc Surg 2009;37:
127-133.
7. Hoppe H, Barnwell SL, Nesbit GM, Petersen BD. Stent-grafts
in the treatment of emergent or urgent carotid artery disease:
review of 25 cases. J Vasc Interv Radiol 2008;19:31-34.
8. May J, White G, Waugh R, Brennan J. Endoluminal repair
of internal carotid artery aneurysm: a feasible but hazardous
procedure. J Vasc Surg 1997;26:1055-1059.
9. McCreadyRA,Divelbiss JL,BryantMA,DenardoAJ, Scott JA.
Endoluminal repair of carotid artery pseudoaneurysms: a
word of caution. J Vasc Surg 2004;40:1020-1023.
10. Maras D, Lioupis C, Magoufis G, et al. Covered stent-graft
treatment of traumatic internal carotid artery pseudo-
aneurysms: a review. Cardiovasc Intervent Radiol 2006;29:
958-968.
11. Chaturvedi S, Yadav JS. The role of antiplatelet therapy in
carotid stenting for ischemic stroke prevention. Stroke
2006;37:1572-1577.
12. McKevitt FM, Randall MS, Cleveland TJ, et al. The benefits
of combined anti-platelet treatment in carotid artery stent-
ing. Eur J Vasc Endovasc Surg 2005;29:522-527.
13. Lin PH, Chronos NA, Marijianowski MM, et al. Carotid
stenting using heparin-coated balloon-expandable stent
reduces intimal hyperplasia in a baboon model. J Surg Res
2003;112:84-90.