Embed Size (px)
Citation preview

CEREBRAL MALARIA
Dr. Muhammad Sajjad Sabir
MCPS, FCPS (Paediatrics)

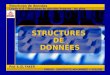
GLOBAL BURDEN OF MALARIA
GLOBALLY 300 MILLION MALARIA CASES A YEAR
1 MILLION DEATHS, 90% IN CHILDREN IN
AFRICA

MALARIA EPIDEMIOLOGY

LIFE CYCLE

WHAT IS CEREBRAL MALARIA?Sever form of malaria caused by P. falciparum Patient with malaria manifesting cerebral
dysfunction →cerebral malariamanifested by
Coma Convulsion and / or Hemoglobinuria

INCUBATION PERIOD
P. vivax and P. ovale 13~15 days
P. malariae 24~30 days
P. falciparum 7~12 days

EPIDEMIOLOGY
More Sever in children as No of parasites same in adult & child (proportionately smaller size)
Blood Gp A&B more protective than Gp O
Hb E & C more protective HbF , sickle cell trait & G6PD deficiency
lesser tendency for falciparum malaria
Malnutrition protective – immunity is low



Section of brain showing blood vessels
blocked with developing P. falciparum parasites

CLINICAL FEATURESPRODROMAL PHASE
FEBRILE PHASE
COMPLICATIONS –CEREBRAL MALARIA

CAUSES OF CNS DYSFUNCTION IN MALARIA
•HYPOGLYCEMIA•HIGH GRADE FEVER ALONE
•RENAL FAILURE•HEPATIC FAILURE
•SEPTICEMIA•SHOCK

CEREBRAL MALARIA FEATURESHigh grade fever, Seizures & SOMI -VE IMPAIRMENT OF CONSIOUSNESS –delerium
stupor,obtundation ,coma SIEZURES – focal /generalised (common in children)
MENINGISMUS NEURO-OPHTHALMOLOGIC SIGNS (gaze
deviation, oculomotor palsy, nystagmus)RETINAL HEMORRHAGE (in 15% patients) FOCAL NEUROLOGIC SIGNS (less common)(aphasia, hemiplegia, ataxia, chorea, and
tremor)

SEQUALETransient neurologic sequelae -
ataxia, hemiparesis, memory disturbance, visual field defects, cognitive impairment, and behavioral abnormalities
A postmalaria neurological syndrome characterized by acute onset of confusion, seizure, ataxia, myoclonus, tremor, and aphasia

COMPLICATIONS Severe anaemia Renal failure Pulmonary oedema Shock Spontaneous bleeding Repeated generalized convulsions
Acidemia or acidosisHypoglycemia

PROGNOSTIC FACTORSthe level of consciousness presence of other organ
dysfunctionRecurrent seizures,decerebration retinal hemorrhage, age < 3 years, heavy parasitemia, (>20%), lactic acidosis, elevated CSF lactate serum transaminase

DIFFERENTIAL DIAGNOSISPyogenic meningitis Viral encephalitis Febrile fitsSOLHepatic comaHypoglycemic comaUremia

DIAGNOSISDemonstration of asexual form of P. falciparum in peripheral blood smear, in thick and thin blood smear films stained by Giemsa stain.

LIGHT MICROSCOPY
Thick blood film- enhanced sensitivity , low levels of parasitemia
Thin blood film.- identification of the parasite to the species level
Recommendations At least 3 smears 6 h apart should be examined before excluding cerebral malaria
Negative if anti-malarial given Upto 20% RBC’s may be infected
Thick & Thin film most specific

P. FALCIPARUM RINGS P. FACIPARUM GAMETOCYTES

Schizont stage –p vivax TROPHOZOITE P. FACIPARUM

CSF EXAMINATIONNecessary to exclude other causes of febrile
encephalopathy CSF is generally normal in cerebral
malaria Mild pleocytosis (10–50 cells/mm3) Protein rise up to 200 mg/dL Glucose - Normal

OTHER TESTS Immuno Chromatographic Assay (ICT-
Malaria) Malaria antigen detection tests are a group of commercially available rapid diagnostic tests that allow quick diagnosis of malaria by people who are not otherwise skilled in traditional laboratory techniques
CBC Leucopenia Monocytosis Low Hb ↑sed Retics
BSR – hypoglycemia Serum electrolytes

CT Scan and MRI usually normal or show edema cortical or subcortical infarcts
EEG nonspecific abnormalities
diffuse slowing, spike wave discharges burst suppression pattern

MANAGEMENT
Neurologic emergency requiring urgent intervention.
In endemic area, treatment should be started without waiting for confirmation of the diagnosis

SPECIFIC THERAPY
TREATMENT OF MULTI ORGAN DYSFUNCTION
TREATMENT OF COMPLICATIONS
MANAGEMENT

TREATMENT OF CEREBRAL MALARIA
Severe malaria should always be treated with parenteral antimalarials
Drug of choice for cerebral malaria – Quinine Parenteral artemisinin derivatives or (widespread resistance to chloroquine)

QUININE a continuous and uniform flow of IV quinine
in dextrose solution should be maintained over a period of four hours
MONITORING Pulse Blood pressure Blood glucose QTc interval .
Quinine should be discontinued if QTc interval exceeds 25% of the basal value
IM injection carries the risk of necrosis at the injection site and the injection is very painful
never give as INTRAVENOUS push

IV quinine over 4Hrs in dextrose solution1mg diluted in 1ml of 5% dextrose
solution20mg/kg I.V stat10mg/kg I.V 8Hrly For 07 days Shift to oral when patient can take orally
10mg/kg/dose TDS for 7 days
QUININE

ARTEMETHER Injectable 3.2 mg /kg I.M stat then 1.6 mg /kg I.M BD for 2 daysCHLOROQUINE 25 mg/kg body weight divided over
three days i.e.10mg/kg on day 110mg/kg on day 2 and 5mg/kg on day 3

SUPPORTIVE MANAGEMENTHydration by administration of fluids
Oral fluids should be given if the patient is conscious and can swallow
High fever Paracetamol Brufen Tepid water sponging

MANAGEMENT OF COMPLICATIONS
INTENSIVE CARE UNIT VENTILATORY SUPPORT
Pulmonary oedema RENAL FAILURE
Care of hydrationDialysis(HEMODIALYSIS)1/3 ↓ dose of antimalarials

MANGEMENT OF COMPLICATIONSSevere anaemia
RCC transusion if Hb <6g/dlHypoglycemia
Glucose bolus I.V(50%, 25%, 10%)Repeated generalized convulsions
Diazepam Phenobarbitone
Acidemia or acidosisSoda bicarb

PROGNOSISMortality 10-30 %
Death mostly within 24 Hrs of admission
Residual neurological deficit in 10% of survivors

?