Embed Size (px)
Citation preview

Laurent CASTERA
Service d’Hépatologie, Hôpital Beaujon, Université Paris VII
Alternatives à la PBH : mesure de l’élasticité
hépatique
DU Hépatites Virales Cytokines et Antiviraux
Pitie, Paris, 12 Janvier 2015

Méthodes non invasives disponibles 2 approches différentes mais complémentaires
Biomarqueurs
Approche « biologique »
Castera & Pinzani. Lancet 2010; 375: 419-20
Approche « physique »
Elasticité hépatique

Mesure de l’élasticité hépatique
ARFI SSI FibroScan

◆ Principe & limites
◆ Performances diagnostiques
◆ Comparaison avec les biomarqueurs
◆ Suivi de la progression de la fibrose
◆ Nouvelles techniques
Plan

Elastométrie (FibroScan)
= 100 x
Biopsie foie 2.5 cm
Volume exploré
4 cm
1 cm ∅

% -5
0
5
Dep
th (m
m)
Time (ms) 0 20 40 60
10 20 30 40 50 60
E = 3.0 kPa F0
Sandrin et al. UMB 2003; 12: 1705-13
VS = 1.0 m/s
E = 27.0 kPa F4
VS = 3.0 m/s
Principe “Plus le foie est dur, plus l’onde se propage vite”

Mesure de l’élasticité hépatique
75 kPa 3
15 65 5.5
Normale
Roulot et al. J Hepatol 2008; 48: 606-13

Variability of transient elastography
Nascimbeni et al. Clin Gastroenterol Hepatol 2014; In press
531 paired liver stiffness measurements < 1 year from 452 patients
classes change in 9.8%. There was a significant positivecorrelation between LSM1 values and fibrosis classchanges (r ¼ 0.414, P < .001), and the higher the decileof LSM1, the greater the probability of class changes(Figure 2A). Patients with significant or severe fibrosishad an alarmingly high rate of "1 fibrosis class changeon a second TE measurement (Figure 2B). Figure 2Ashows that only patients with LSM1 <6.5 kPa hadreduced probability of fibrosis class change on repeatedmeasurements. The best LSM1 cutoff value for predictingat least 1 fibrosis class change was 7.15 kPa, close to thecutoff value for significant fibrosis (SupplementaryFigure 3).
The subanalyses according to maximum IQR/Mbetween baseline and follow-up TE displayed anincreasing prevalence of discordance and fibrosis class
changes for higher IQR/M groups (Figure 3 andSupplementary Material).
Overall, there were no significant modificationsbetween baseline and follow-up TE readings for themean values of the tested anthropometric andbiochemical variables (Table 1).
Factors Associated With Variability BetweenBaseline and Follow-up Paired LiverStiffness Measurements
We first assessed the determinants of >20%, >30%,and >50% relative discordance (Supplementary Table 2and Table 2). Both the presence of 2 different operatorsand at least 1 non-senior operator were significantly
Figure 1. Correlation between baseline liver stiffness measurement (LSM1) and variability between paired LSMs. (A) Corre-lation between logarithmic LSM1 and logarithmic absolute variability [log (LSM2-LSM1)] between paired LSMs (r ¼ 0.542; P <.001). (B) Correlation between logarithmic LSM1 and logarithmic relative variability {log [(LSM2-LSM1)/LSM1*100]} betweenpaired LSMs (r ¼ 0.150; P ¼ .001). (C) Correlation between percentile group (decile) of LSM1 and mean þ SD absolutevariability (LSM2-LSM1) between paired LSMs. Analysis of variance (ANOVA) P for trend < .001. *Tenth decile group signif-icantly differs from other groups according to one-way ANOVA test with post hoc Bonferroni analysis (P < .001). (D) Corre-lation between percentile group (decile) of LSM1 and mean þ SD relative variability [(LSM2-LSM1)/LSM1*100] between pairedLSMs. ANOVA P for trend: .234. No significant differences were found between decile groups according to one-way ANOVAtest with post hoc Bonferroni analysis.
4 Nascimbeni et al Clinical Gastroenterology and Hepatology Vol. -, No. -
Variation > 30% 34%
Variation > 50% 12%
Variation > 20% 50%
2 different operators IQR / M
LSM > 7 kPa
BMI
ALT levels

How to interpret FibroScan results manufacturer’s recommendations
Success rate > 60%
10 validated measures IQR < 30% median
Castera, Forns & Alberti. J Hepatol 2008; 48: 835-47

Applicability of transient elastography
Unreliable 15.8%
IQR/LSM > 30% 9.2%
SR < 60% 8.1%
VS < 10 3.1%
Failure 3.1%
Valid shot = 0
Castéra et al. Hepatology 2010; 51: 828-35
FibroScan not applicable
in 20% of cases
N=13669 examinations
Obesity Operator experience

Unreliable
IQR/LSM > 30%
SR < 60%
VS < 10
Failure
Valid shot = 0
XL Probe: Does it really overcome the limitations of M probe ?
XL vs. M probe: 1% vs. 16%
N= 276 patients with BMI > 28 kg/m2
Myers et al. Hepatology 2012; 55:199-208.
XL vs. M probe: 27% vs. 50%

Discussion
In this prospective multicenter study, we confirmedthe feasibility and performance of LSM using theFibroScan XL probe in overweight and obese patientswith a variety of liver disorders. The major advantageof this new probe designed specifically for use in obesepatients is that it facilitates LSM in more patients thanis feasible with the standard M probe. For example,failure of LSM occurred in only 1% of patients withthe XL probe compared with 16% with the M probe.Corresponding failure rates in patients with extremeobesity (BMI !40 kg/m2) were 5% and 59%, respec-tively. Similarly, at least 10 valid LSMs were obtainedin 93% of patients with the XL probe compared withonly 65% with the M probe; 81% of patients withfewer than 10 LSMs with the M probe were success-fully assessed using the XL probe. These encouraging
results confirm data from two small pilot studies evalu-ating the XL probe.15,16 Among 17 patients with aBMI !30 kg/m2, Friedrich-Rust et al.16 obtained 10valid measurements in 94% of patients with the XLprobe versus only 65% with the M probe. Similarly,de Ledinghen et al.15 reported that 59% of obesepatients for whom it was impossible to obtain 10 validLSMs with the M probe were successfully measuredusing an XL probe prototype (which differed in severalrespects from the probe currently under study). Thelower rates of success in the French study likely reflectthe higher mean BMI of their cohort (41.5 versus34.3 kg/m2 in our study), who were hospitalized spe-cifically for obesity management. Considering the ris-ing prevalence of obesity and NAFLD, these findingsrepresent an important advance in the management ofpatients with chronic liver disease. With recent esti-mates suggesting that over 100 million Americans areobese, and that the majority of obese individuals haveNAFLD,14 noninvasive and widely applicable
Fig. 5. (A) Correlation between liver stiffness values measured usingthe M and XL probes in 178 patients with !10 valid measurementswith both probes (q ¼ 0.86; P < 0.0005). (B) Bland-Altman plot ofthe difference between liver stiffness measured using the M and XLprobes versus the mean. A greater difference in liver stiffness betweenprobes was observed at higher mean liver stiffness values (P <0.0005). The solid horizontal line represents the mean differencebetween probes (2.3 kPa; 95% CI 1.6-3.0) and the dashed lines the95% limits of agreement (#6.8 to 11.5 kPa).
Fig. 6. Relationship between liver stiffness measured using the Mand XL probes and the stage of liver fibrosis in patients with (A) viralhepatitis (n ¼ 69) and (B) NAFLD (n ¼ 75). Analyses are limited topatients with !10 valid measurements with both probes and interpret-able liver biopsies.
HEPATOLOGY, Vol. 55, No. 1, 2012 MYERS ET AL. 205
XL Probe: the cut-off issue
N= 65 NAFLD patients Myers et al. Hepatology 2012; 55:199-208.
7.8 vs. 6.4 kPa M vs. XL

Boursier et al. Hepatology 2013; 57: 1182-91
N=1165 patients with CLD; 70% HCV
Independent predictors were the same when variableswere introduced as dichotomous results (IQR/M!0.30, LSE success rate "60%, reliable versus unreli-able biopsy) in the multivariate analyses (details notshown).
Classification of LSE AccuracyWe develop here a classification using the preceding
independent predictors of accuracy.IQR/M. LSE accuracy as a function of increasing
intervals of IQR/M is depicted in Table S3. Briefly,LSE accuracy decreased when IQR/M increased andthree subgroups of LSE were identified: IQR/M!0.10 (16.6% of patients); 0.10< IQR/M !0.30(69.0%); IQR/M >0.30 (14.5%). LSE with IQR/M!0.10 had significantly higher accuracy than LSE withIQR/M >0.10 (Table 4). LSE with 0.10< IQR/M!0.30 had higher accuracy than LSE with IQR/M>0.30, but the difference did not reach statisticalsignificance.LSE Median. By using 7.1 kPa as a diagnostic cut-
off,12 the rate of well-classified patients for significantfibrosis was very good in LSE medians "7.1 kPa, butonly fair in LSE medians <7.1 kPa: 81.5% versus64.5%, respectively (P < 10#3). By using 12.5 kPa asa diagnostic cutoff,12 the rate of well-classified patientsfor cirrhosis was excellent in LSE medians <12.5 kPa,but only fair in LSE medians "12.5 kPa: 94.3% ver-sus 60.4%, respectively (P < 10#3). LSE thus demon-strated excellent negative predictive value for cirrhosisand very good positive predictive value for significantfibrosis. Conversely, it had insufficient positive predic-tive value for cirrhosis and insufficient negative predic-tive value for significant fibrosis. Finally, the rate ofwell-classified patients by the LSE classification derivedfrom Castera et al. cutoffs was not significantly differ-ent among its three classes, FFS0/1: 64.5%, FFS2/3:60.4%, and FFS4: 60.4% (P ¼ 0.379).
IQR/M and LSE Median. In patients with LSEmedian <7.1 kPa, the diagnostic accuracy of the LSEclassification derived from Castera et al. cutoffs wasnot significantly different among the three IQR/Msubgroups (P ¼ 0.458; Fig. 1). Conversely, in patientswith LSE median "7.1 kPa the diagnostic accuracy ofthe LSE classification was significantly lower in LSEwith IQR/M >0.30 compared to LSE with IQR/M!0.30 (43.8% versus 64.1%, P < 10#3; Fig. 1). Therates of well-classified patients for the binary diagnosesof significant fibrosis or cirrhosis as a function of IQR/M and LSE median are detailed in Supporting Fig.S1. Briefly, in patients with LSE median "7.1 kPa,LSE with IQR/M >0.30 had lower accuracy for signif-icant fibrosis than LSE with IQR/M !0.30 (67.6%versus 84.3%, P < 10#3). In patients with LSE me-dian "12.5 kPa, LSE with IQR/M >0.30 had loweraccuracy for cirrhosis than LSE with IQR/M !0.30(45.1% versus 64.0%, P ¼ 0.011).
Table 4. Accuracy of LSE Median as a Function of IQR/M
Diagnostic Target:
AUROC Diagnostic Accuracy (%)*
FM"2 FM"3 FM4 FM"2 FM4 LSE Classification
IQR/M !0.10 0.886 6 0.024 0.937 6 0.018 0.970 6 0.011 77.1 90.4 69.10.10< and !0.30 0.822 6 0.015 0.868 6 0.013 0.895 6 0.015 75.6 84.7 62.6>0.30 0.785 6 0.035 0.842 6 0.032 0.898 6 0.031 69.1 80.6 53.9
Comparison (P):!0.10 vs. 0.10< and !0.30 0.024 0.002 <10#3 0.661 0.043 0.092!0.10 vs. >0.30 0.017 0.010 0.029 0.088 0.008 0.0030.10< and !0.30 vs. >0.30 0.331 0.451 0.931 0.081 0.196 0.039Linear trend † # # # 0.091 0.009 0.003
*Rate of well-classified patients using 7.1 kPa as the LSE cutoff for the diagnosis of significant fibrosis (FM"2), 12.5 kPa for the diagnosis of cirrhosis (FM4), orLSE classification (FFS0/1, FFS2/3, FFS4) derived from the 2 previous diagnostic cutoffs (12).†P for linear trend of diagnostic accuracy across the 3 subgroups of IQR/M.
Fig. 1. Rate of well-classified patients by the LSE classificationderived from Castera et al.12 cutoffs, as a function of the threeclasses of the classification and IQR/M.
1186 BOURSIER ET AL. HEPATOLOGY, March 2013
P=NS
How does applicability translates into accuracy?

Boursier et al. Hepatology 2013; 57: 1182-91
N=1165 patients with CLD; 70% HCV
How does applicability translates into accuracy?
Proposal for New Reliability Criteria in LSEThe previous findings led us to develop new criteria
for the interpretation of LSE results (Table 5). LSE ac-curacy in the subgroup of LSE with IQR/M !0.10was higher than in the whole population (Table 6).LSEs in this subgroup were thus considered ‘‘very reli-able.’’ LSE with 0.10< IQR/M !0.30 or with IQR/M >0.30 and LSE median <7.1 kPa provided accu-racy similar to that of the whole population and werethus considered ‘‘reliable.’’ Finally, LSE with IQR/M>0.30 and LSE median "7.1 kPa provided accuracylower than that of the whole population and were thusconsidered ‘‘poorly reliable.’’According to these new criteria, 16.6% of LSE were
considered ‘‘very reliable,’’ 74.3% ‘‘reliable,’’ and 9.1%‘‘poorly reliable.’’ Importantly, LSE AUROCs anddiagnostic accuracies were significantly different amongthese three subgroups (Table 6). Finally, the rate ofpoorly reliable LSE according to the new criteria wassignificantly lower than that of unreliable LSE accord-ing to the usual definition (9.1% versus 24.3%, P <10#3).
Sensitivity AnalysisWe evaluated our new criteria for LSE reliability as a
function of several potential influencing characteristics:cause of liver disease (CHC versus others), diagnosticindexes (AUROC, binary diagnosis of significant fibrosisor cirrhosis, LSE classification), and diagnostic cutoffspublished by Ziol et al.,13 Stebbing et al.,14 and Frie-drich-Rust et al.15 The detailed results are presented inTables S4 and S5. Briefly, whatever the potential influ-encing factor, a decrease in LSE reliability, according toour new criteria, was associated with a decrease in LSEaccuracy. Body mass index (<25 versus "25 kg/m2)did not influence LSE accuracy in any of the three newcategories of LSE reliability (details not shown). Becauseof the few numbers of patients with hepatitis B, alcoholabuse, or NAFLD, it was not possible to perform a sen-sitivity analysis for these causes of chronic liver disease.
Discussion
There is currently a critical need in clinical practiceand in clinical research to precisely define the
Table 5. New Reliability Criteria for LSE and Ensuing Interpretation as Very Reliable (white), Reliable (gray),and Poorly Reliable (dark gray) LSE
LSE Median
<7.1 7.1 ! and <12.5 "12.5Patient Rate (%)LSE Diagnosis *: FFS0/1 FFS2/3 FFS4
IQR/M !0.10 Very reliable LSE 16.60.10< and !0.30 Reliable LSE 74.3 †>0.30 Poorly reliable LSE 9.1
Because it is quick and easy in most cases, LSE should include 10 valid measurements whatever the LSE success rate.*LSE diagnosis after categorization of LSE median into estimated Metavir fibrosis stages (FFS) according to the diagnostic cutoffs of Castera et al.: 7.1 kPa for
significant fibrosis and 12.5 kPa for cirrhosis (12).†Including the subgroup with IQR/M >0.30 and LSE median <7.1.
Table 6. Accuracy of LSE as a Function of LSE Reliability Defined by the New Criteria
Diagnostic Target:
AUROC Diagnostic Accuracy (%) *
FM"2 FM"3 FM4 FM"2 FM4 LSE Classification
LSE: All † 0.822 6 0.012 0.872 6 0.010 0.910 6 0.011 74.9 85.0 62.4Very reliable 0.886 6 0.024 0.937 6 0.018 0.970 6 0.011 77.1 90.4 69.1Reliable 0.823 6 0.014 0.876 6 0.012 0.904 6 0.014 75.3 85.8 63.2Poorly reliable 0.773 6 0.045 0.745 6 0.049 0.819 6 0.052 67.6 69.5 43.8
Comparison (P):Very reliable vs. reliable 0.023 0.005 <10#3 0.603 0.090 0.125Very reliable vs. poorly reliable 0.027 <10#3 0.004 0.076 <10#3 <10#3
Reliable vs. poorly reliable 0.289 0.009 0.115 0.088 <10#3 <10#3
Linear trend‡ 0.107 <10#3 <10#3
*Rate of well-classified patients using 7.1 kPa as the LSE cutoff for the diagnosis of significant fibrosis (FM"2), 12.5 kPa for the diagnosis of cirrhosis (FM4), orLSE classification (FFS0/1, FFS2/3, FFS4) derived from the 2 previous diagnostic cutoffs (12).†This result, already presented in table 2, is provided here for comparison with subgroups.‡P for linear trend of diagnostic accuracy across the 3 subgroups of LSE.
HEPATOLOGY, Vol. 57, No. 3, 2013 BOURSIER ET AL. 1187
Proposal for New Reliability Criteria in LSEThe previous findings led us to develop new criteria
for the interpretation of LSE results (Table 5). LSE ac-curacy in the subgroup of LSE with IQR/M !0.10was higher than in the whole population (Table 6).LSEs in this subgroup were thus considered ‘‘very reli-able.’’ LSE with 0.10< IQR/M !0.30 or with IQR/M >0.30 and LSE median <7.1 kPa provided accu-racy similar to that of the whole population and werethus considered ‘‘reliable.’’ Finally, LSE with IQR/M>0.30 and LSE median "7.1 kPa provided accuracylower than that of the whole population and were thusconsidered ‘‘poorly reliable.’’According to these new criteria, 16.6% of LSE were
considered ‘‘very reliable,’’ 74.3% ‘‘reliable,’’ and 9.1%‘‘poorly reliable.’’ Importantly, LSE AUROCs anddiagnostic accuracies were significantly different amongthese three subgroups (Table 6). Finally, the rate ofpoorly reliable LSE according to the new criteria wassignificantly lower than that of unreliable LSE accord-ing to the usual definition (9.1% versus 24.3%, P <10#3).
Sensitivity AnalysisWe evaluated our new criteria for LSE reliability as a
function of several potential influencing characteristics:cause of liver disease (CHC versus others), diagnosticindexes (AUROC, binary diagnosis of significant fibrosisor cirrhosis, LSE classification), and diagnostic cutoffspublished by Ziol et al.,13 Stebbing et al.,14 and Frie-drich-Rust et al.15 The detailed results are presented inTables S4 and S5. Briefly, whatever the potential influ-encing factor, a decrease in LSE reliability, according toour new criteria, was associated with a decrease in LSEaccuracy. Body mass index (<25 versus "25 kg/m2)did not influence LSE accuracy in any of the three newcategories of LSE reliability (details not shown). Becauseof the few numbers of patients with hepatitis B, alcoholabuse, or NAFLD, it was not possible to perform a sen-sitivity analysis for these causes of chronic liver disease.
Discussion
There is currently a critical need in clinical practiceand in clinical research to precisely define the
Table 5. New Reliability Criteria for LSE and Ensuing Interpretation as Very Reliable (white), Reliable (gray),and Poorly Reliable (dark gray) LSE
LSE Median
<7.1 7.1 ! and <12.5 "12.5Patient Rate (%)LSE Diagnosis *: FFS0/1 FFS2/3 FFS4
IQR/M !0.10 Very reliable LSE 16.60.10< and !0.30 Reliable LSE 74.3 †>0.30 Poorly reliable LSE 9.1
Because it is quick and easy in most cases, LSE should include 10 valid measurements whatever the LSE success rate.*LSE diagnosis after categorization of LSE median into estimated Metavir fibrosis stages (FFS) according to the diagnostic cutoffs of Castera et al.: 7.1 kPa for
significant fibrosis and 12.5 kPa for cirrhosis (12).†Including the subgroup with IQR/M >0.30 and LSE median <7.1.
Table 6. Accuracy of LSE as a Function of LSE Reliability Defined by the New Criteria
Diagnostic Target:
AUROC Diagnostic Accuracy (%) *
FM"2 FM"3 FM4 FM"2 FM4 LSE Classification
LSE: All † 0.822 6 0.012 0.872 6 0.010 0.910 6 0.011 74.9 85.0 62.4Very reliable 0.886 6 0.024 0.937 6 0.018 0.970 6 0.011 77.1 90.4 69.1Reliable 0.823 6 0.014 0.876 6 0.012 0.904 6 0.014 75.3 85.8 63.2Poorly reliable 0.773 6 0.045 0.745 6 0.049 0.819 6 0.052 67.6 69.5 43.8
Comparison (P):Very reliable vs. reliable 0.023 0.005 <10#3 0.603 0.090 0.125Very reliable vs. poorly reliable 0.027 <10#3 0.004 0.076 <10#3 <10#3
Reliable vs. poorly reliable 0.289 0.009 0.115 0.088 <10#3 <10#3
Linear trend‡ 0.107 <10#3 <10#3
*Rate of well-classified patients using 7.1 kPa as the LSE cutoff for the diagnosis of significant fibrosis (FM"2), 12.5 kPa for the diagnosis of cirrhosis (FM4), orLSE classification (FFS0/1, FFS2/3, FFS4) derived from the 2 previous diagnostic cutoffs (12).†This result, already presented in table 2, is provided here for comparison with subgroups.‡P for linear trend of diagnostic accuracy across the 3 subgroups of LSE.
HEPATOLOGY, Vol. 57, No. 3, 2013 BOURSIER ET AL. 1187
Proposal for New Reliability Criteria in LSEThe previous findings led us to develop new criteria
for the interpretation of LSE results (Table 5). LSE ac-curacy in the subgroup of LSE with IQR/M !0.10was higher than in the whole population (Table 6).LSEs in this subgroup were thus considered ‘‘very reli-able.’’ LSE with 0.10< IQR/M !0.30 or with IQR/M >0.30 and LSE median <7.1 kPa provided accu-racy similar to that of the whole population and werethus considered ‘‘reliable.’’ Finally, LSE with IQR/M>0.30 and LSE median "7.1 kPa provided accuracylower than that of the whole population and were thusconsidered ‘‘poorly reliable.’’According to these new criteria, 16.6% of LSE were
considered ‘‘very reliable,’’ 74.3% ‘‘reliable,’’ and 9.1%‘‘poorly reliable.’’ Importantly, LSE AUROCs anddiagnostic accuracies were significantly different amongthese three subgroups (Table 6). Finally, the rate ofpoorly reliable LSE according to the new criteria wassignificantly lower than that of unreliable LSE accord-ing to the usual definition (9.1% versus 24.3%, P <10#3).
Sensitivity AnalysisWe evaluated our new criteria for LSE reliability as a
function of several potential influencing characteristics:cause of liver disease (CHC versus others), diagnosticindexes (AUROC, binary diagnosis of significant fibrosisor cirrhosis, LSE classification), and diagnostic cutoffspublished by Ziol et al.,13 Stebbing et al.,14 and Frie-drich-Rust et al.15 The detailed results are presented inTables S4 and S5. Briefly, whatever the potential influ-encing factor, a decrease in LSE reliability, according toour new criteria, was associated with a decrease in LSEaccuracy. Body mass index (<25 versus "25 kg/m2)did not influence LSE accuracy in any of the three newcategories of LSE reliability (details not shown). Becauseof the few numbers of patients with hepatitis B, alcoholabuse, or NAFLD, it was not possible to perform a sen-sitivity analysis for these causes of chronic liver disease.
Discussion
There is currently a critical need in clinical practiceand in clinical research to precisely define the
Table 5. New Reliability Criteria for LSE and Ensuing Interpretation as Very Reliable (white), Reliable (gray),and Poorly Reliable (dark gray) LSE
LSE Median
<7.1 7.1 ! and <12.5 "12.5Patient Rate (%)LSE Diagnosis *: FFS0/1 FFS2/3 FFS4
IQR/M !0.10 Very reliable LSE 16.60.10< and !0.30 Reliable LSE 74.3 †>0.30 Poorly reliable LSE 9.1
Because it is quick and easy in most cases, LSE should include 10 valid measurements whatever the LSE success rate.*LSE diagnosis after categorization of LSE median into estimated Metavir fibrosis stages (FFS) according to the diagnostic cutoffs of Castera et al.: 7.1 kPa for
significant fibrosis and 12.5 kPa for cirrhosis (12).†Including the subgroup with IQR/M >0.30 and LSE median <7.1.
Table 6. Accuracy of LSE as a Function of LSE Reliability Defined by the New Criteria
Diagnostic Target:
AUROC Diagnostic Accuracy (%) *
FM"2 FM"3 FM4 FM"2 FM4 LSE Classification
LSE: All † 0.822 6 0.012 0.872 6 0.010 0.910 6 0.011 74.9 85.0 62.4Very reliable 0.886 6 0.024 0.937 6 0.018 0.970 6 0.011 77.1 90.4 69.1Reliable 0.823 6 0.014 0.876 6 0.012 0.904 6 0.014 75.3 85.8 63.2Poorly reliable 0.773 6 0.045 0.745 6 0.049 0.819 6 0.052 67.6 69.5 43.8
Comparison (P):Very reliable vs. reliable 0.023 0.005 <10#3 0.603 0.090 0.125Very reliable vs. poorly reliable 0.027 <10#3 0.004 0.076 <10#3 <10#3
Reliable vs. poorly reliable 0.289 0.009 0.115 0.088 <10#3 <10#3
Linear trend‡ 0.107 <10#3 <10#3
*Rate of well-classified patients using 7.1 kPa as the LSE cutoff for the diagnosis of significant fibrosis (FM"2), 12.5 kPa for the diagnosis of cirrhosis (FM4), orLSE classification (FFS0/1, FFS2/3, FFS4) derived from the 2 previous diagnostic cutoffs (12).†This result, already presented in table 2, is provided here for comparison with subgroups.‡P for linear trend of diagnostic accuracy across the 3 subgroups of LSE.
HEPATOLOGY, Vol. 57, No. 3, 2013 BOURSIER ET AL. 1187
Proposal for New Reliability Criteria in LSEThe previous findings led us to develop new criteria
for the interpretation of LSE results (Table 5). LSE ac-curacy in the subgroup of LSE with IQR/M !0.10was higher than in the whole population (Table 6).LSEs in this subgroup were thus considered ‘‘very reli-able.’’ LSE with 0.10< IQR/M !0.30 or with IQR/M >0.30 and LSE median <7.1 kPa provided accu-racy similar to that of the whole population and werethus considered ‘‘reliable.’’ Finally, LSE with IQR/M>0.30 and LSE median "7.1 kPa provided accuracylower than that of the whole population and were thusconsidered ‘‘poorly reliable.’’According to these new criteria, 16.6% of LSE were
considered ‘‘very reliable,’’ 74.3% ‘‘reliable,’’ and 9.1%‘‘poorly reliable.’’ Importantly, LSE AUROCs anddiagnostic accuracies were significantly different amongthese three subgroups (Table 6). Finally, the rate ofpoorly reliable LSE according to the new criteria wassignificantly lower than that of unreliable LSE accord-ing to the usual definition (9.1% versus 24.3%, P <10#3).
Sensitivity AnalysisWe evaluated our new criteria for LSE reliability as a
function of several potential influencing characteristics:cause of liver disease (CHC versus others), diagnosticindexes (AUROC, binary diagnosis of significant fibrosisor cirrhosis, LSE classification), and diagnostic cutoffspublished by Ziol et al.,13 Stebbing et al.,14 and Frie-drich-Rust et al.15 The detailed results are presented inTables S4 and S5. Briefly, whatever the potential influ-encing factor, a decrease in LSE reliability, according toour new criteria, was associated with a decrease in LSEaccuracy. Body mass index (<25 versus "25 kg/m2)did not influence LSE accuracy in any of the three newcategories of LSE reliability (details not shown). Becauseof the few numbers of patients with hepatitis B, alcoholabuse, or NAFLD, it was not possible to perform a sen-sitivity analysis for these causes of chronic liver disease.
Discussion
There is currently a critical need in clinical practiceand in clinical research to precisely define the
Table 5. New Reliability Criteria for LSE and Ensuing Interpretation as Very Reliable (white), Reliable (gray),and Poorly Reliable (dark gray) LSE
LSE Median
<7.1 7.1 ! and <12.5 "12.5Patient Rate (%)LSE Diagnosis *: FFS0/1 FFS2/3 FFS4
IQR/M !0.10 Very reliable LSE 16.60.10< and !0.30 Reliable LSE 74.3 †>0.30 Poorly reliable LSE 9.1
Because it is quick and easy in most cases, LSE should include 10 valid measurements whatever the LSE success rate.*LSE diagnosis after categorization of LSE median into estimated Metavir fibrosis stages (FFS) according to the diagnostic cutoffs of Castera et al.: 7.1 kPa for
significant fibrosis and 12.5 kPa for cirrhosis (12).†Including the subgroup with IQR/M >0.30 and LSE median <7.1.
Table 6. Accuracy of LSE as a Function of LSE Reliability Defined by the New Criteria
Diagnostic Target:
AUROC Diagnostic Accuracy (%) *
FM"2 FM"3 FM4 FM"2 FM4 LSE Classification
LSE: All † 0.822 6 0.012 0.872 6 0.010 0.910 6 0.011 74.9 85.0 62.4Very reliable 0.886 6 0.024 0.937 6 0.018 0.970 6 0.011 77.1 90.4 69.1Reliable 0.823 6 0.014 0.876 6 0.012 0.904 6 0.014 75.3 85.8 63.2Poorly reliable 0.773 6 0.045 0.745 6 0.049 0.819 6 0.052 67.6 69.5 43.8
Comparison (P):Very reliable vs. reliable 0.023 0.005 <10#3 0.603 0.090 0.125Very reliable vs. poorly reliable 0.027 <10#3 0.004 0.076 <10#3 <10#3
Reliable vs. poorly reliable 0.289 0.009 0.115 0.088 <10#3 <10#3
Linear trend‡ 0.107 <10#3 <10#3
*Rate of well-classified patients using 7.1 kPa as the LSE cutoff for the diagnosis of significant fibrosis (FM"2), 12.5 kPa for the diagnosis of cirrhosis (FM4), orLSE classification (FFS0/1, FFS2/3, FFS4) derived from the 2 previous diagnostic cutoffs (12).†This result, already presented in table 2, is provided here for comparison with subgroups.‡P for linear trend of diagnostic accuracy across the 3 subgroups of LSE.
HEPATOLOGY, Vol. 57, No. 3, 2013 BOURSIER ET AL. 1187
Proposal for New Reliability Criteria in LSEThe previous findings led us to develop new criteria
for the interpretation of LSE results (Table 5). LSE ac-curacy in the subgroup of LSE with IQR/M !0.10was higher than in the whole population (Table 6).LSEs in this subgroup were thus considered ‘‘very reli-able.’’ LSE with 0.10< IQR/M !0.30 or with IQR/M >0.30 and LSE median <7.1 kPa provided accu-racy similar to that of the whole population and werethus considered ‘‘reliable.’’ Finally, LSE with IQR/M>0.30 and LSE median "7.1 kPa provided accuracylower than that of the whole population and were thusconsidered ‘‘poorly reliable.’’According to these new criteria, 16.6% of LSE were
considered ‘‘very reliable,’’ 74.3% ‘‘reliable,’’ and 9.1%‘‘poorly reliable.’’ Importantly, LSE AUROCs anddiagnostic accuracies were significantly different amongthese three subgroups (Table 6). Finally, the rate ofpoorly reliable LSE according to the new criteria wassignificantly lower than that of unreliable LSE accord-ing to the usual definition (9.1% versus 24.3%, P <10#3).
Sensitivity AnalysisWe evaluated our new criteria for LSE reliability as a
function of several potential influencing characteristics:cause of liver disease (CHC versus others), diagnosticindexes (AUROC, binary diagnosis of significant fibrosisor cirrhosis, LSE classification), and diagnostic cutoffspublished by Ziol et al.,13 Stebbing et al.,14 and Frie-drich-Rust et al.15 The detailed results are presented inTables S4 and S5. Briefly, whatever the potential influ-encing factor, a decrease in LSE reliability, according toour new criteria, was associated with a decrease in LSEaccuracy. Body mass index (<25 versus "25 kg/m2)did not influence LSE accuracy in any of the three newcategories of LSE reliability (details not shown). Becauseof the few numbers of patients with hepatitis B, alcoholabuse, or NAFLD, it was not possible to perform a sen-sitivity analysis for these causes of chronic liver disease.
Discussion
There is currently a critical need in clinical practiceand in clinical research to precisely define the
Table 5. New Reliability Criteria for LSE and Ensuing Interpretation as Very Reliable (white), Reliable (gray),and Poorly Reliable (dark gray) LSE
LSE Median
<7.1 7.1 ! and <12.5 "12.5Patient Rate (%)LSE Diagnosis *: FFS0/1 FFS2/3 FFS4
IQR/M !0.10 Very reliable LSE 16.60.10< and !0.30 Reliable LSE 74.3 †>0.30 Poorly reliable LSE 9.1
Because it is quick and easy in most cases, LSE should include 10 valid measurements whatever the LSE success rate.*LSE diagnosis after categorization of LSE median into estimated Metavir fibrosis stages (FFS) according to the diagnostic cutoffs of Castera et al.: 7.1 kPa for
significant fibrosis and 12.5 kPa for cirrhosis (12).†Including the subgroup with IQR/M >0.30 and LSE median <7.1.
Table 6. Accuracy of LSE as a Function of LSE Reliability Defined by the New Criteria
Diagnostic Target:
AUROC Diagnostic Accuracy (%) *
FM"2 FM"3 FM4 FM"2 FM4 LSE Classification
LSE: All † 0.822 6 0.012 0.872 6 0.010 0.910 6 0.011 74.9 85.0 62.4Very reliable 0.886 6 0.024 0.937 6 0.018 0.970 6 0.011 77.1 90.4 69.1Reliable 0.823 6 0.014 0.876 6 0.012 0.904 6 0.014 75.3 85.8 63.2Poorly reliable 0.773 6 0.045 0.745 6 0.049 0.819 6 0.052 67.6 69.5 43.8
Comparison (P):Very reliable vs. reliable 0.023 0.005 <10#3 0.603 0.090 0.125Very reliable vs. poorly reliable 0.027 <10#3 0.004 0.076 <10#3 <10#3
Reliable vs. poorly reliable 0.289 0.009 0.115 0.088 <10#3 <10#3
Linear trend‡ 0.107 <10#3 <10#3
*Rate of well-classified patients using 7.1 kPa as the LSE cutoff for the diagnosis of significant fibrosis (FM"2), 12.5 kPa for the diagnosis of cirrhosis (FM4), orLSE classification (FFS0/1, FFS2/3, FFS4) derived from the 2 previous diagnostic cutoffs (12).†This result, already presented in table 2, is provided here for comparison with subgroups.‡P for linear trend of diagnostic accuracy across the 3 subgroups of LSE.
HEPATOLOGY, Vol. 57, No. 3, 2013 BOURSIER ET AL. 1187
Proposal for New Reliability Criteria in LSEThe previous findings led us to develop new criteria
for the interpretation of LSE results (Table 5). LSE ac-curacy in the subgroup of LSE with IQR/M !0.10was higher than in the whole population (Table 6).LSEs in this subgroup were thus considered ‘‘very reli-able.’’ LSE with 0.10< IQR/M !0.30 or with IQR/M >0.30 and LSE median <7.1 kPa provided accu-racy similar to that of the whole population and werethus considered ‘‘reliable.’’ Finally, LSE with IQR/M>0.30 and LSE median "7.1 kPa provided accuracylower than that of the whole population and were thusconsidered ‘‘poorly reliable.’’According to these new criteria, 16.6% of LSE were
considered ‘‘very reliable,’’ 74.3% ‘‘reliable,’’ and 9.1%‘‘poorly reliable.’’ Importantly, LSE AUROCs anddiagnostic accuracies were significantly different amongthese three subgroups (Table 6). Finally, the rate ofpoorly reliable LSE according to the new criteria wassignificantly lower than that of unreliable LSE accord-ing to the usual definition (9.1% versus 24.3%, P <10#3).
Sensitivity AnalysisWe evaluated our new criteria for LSE reliability as a
function of several potential influencing characteristics:cause of liver disease (CHC versus others), diagnosticindexes (AUROC, binary diagnosis of significant fibrosisor cirrhosis, LSE classification), and diagnostic cutoffspublished by Ziol et al.,13 Stebbing et al.,14 and Frie-drich-Rust et al.15 The detailed results are presented inTables S4 and S5. Briefly, whatever the potential influ-encing factor, a decrease in LSE reliability, according toour new criteria, was associated with a decrease in LSEaccuracy. Body mass index (<25 versus "25 kg/m2)did not influence LSE accuracy in any of the three newcategories of LSE reliability (details not shown). Becauseof the few numbers of patients with hepatitis B, alcoholabuse, or NAFLD, it was not possible to perform a sen-sitivity analysis for these causes of chronic liver disease.
Discussion
There is currently a critical need in clinical practiceand in clinical research to precisely define the
Table 5. New Reliability Criteria for LSE and Ensuing Interpretation as Very Reliable (white), Reliable (gray),and Poorly Reliable (dark gray) LSE
LSE Median
<7.1 7.1 ! and <12.5 "12.5Patient Rate (%)LSE Diagnosis *: FFS0/1 FFS2/3 FFS4
IQR/M !0.10 Very reliable LSE 16.60.10< and !0.30 Reliable LSE 74.3 †>0.30 Poorly reliable LSE 9.1
Because it is quick and easy in most cases, LSE should include 10 valid measurements whatever the LSE success rate.*LSE diagnosis after categorization of LSE median into estimated Metavir fibrosis stages (FFS) according to the diagnostic cutoffs of Castera et al.: 7.1 kPa for
significant fibrosis and 12.5 kPa for cirrhosis (12).†Including the subgroup with IQR/M >0.30 and LSE median <7.1.
Table 6. Accuracy of LSE as a Function of LSE Reliability Defined by the New Criteria
Diagnostic Target:
AUROC Diagnostic Accuracy (%) *
FM"2 FM"3 FM4 FM"2 FM4 LSE Classification
LSE: All † 0.822 6 0.012 0.872 6 0.010 0.910 6 0.011 74.9 85.0 62.4Very reliable 0.886 6 0.024 0.937 6 0.018 0.970 6 0.011 77.1 90.4 69.1Reliable 0.823 6 0.014 0.876 6 0.012 0.904 6 0.014 75.3 85.8 63.2Poorly reliable 0.773 6 0.045 0.745 6 0.049 0.819 6 0.052 67.6 69.5 43.8
Comparison (P):Very reliable vs. reliable 0.023 0.005 <10#3 0.603 0.090 0.125Very reliable vs. poorly reliable 0.027 <10#3 0.004 0.076 <10#3 <10#3
Reliable vs. poorly reliable 0.289 0.009 0.115 0.088 <10#3 <10#3
Linear trend‡ 0.107 <10#3 <10#3
*Rate of well-classified patients using 7.1 kPa as the LSE cutoff for the diagnosis of significant fibrosis (FM"2), 12.5 kPa for the diagnosis of cirrhosis (FM4), orLSE classification (FFS0/1, FFS2/3, FFS4) derived from the 2 previous diagnostic cutoffs (12).†This result, already presented in table 2, is provided here for comparison with subgroups.‡P for linear trend of diagnostic accuracy across the 3 subgroups of LSE.
HEPATOLOGY, Vol. 57, No. 3, 2013 BOURSIER ET AL. 1187

each liver stiffness determination were used to calculatethe significance of intraindividual changes after foodintake. For subgroup analysis, patients were groupedaccording to the presumed stage of fibrosis: low liverstiffness (o6 kPa), intermediate liver stiffness (6–10 kPa)and individuals with high liver stiffness (410 kPa).
Statistical analysis
The Wilcoxon test was used to analyse differences be-tween liver stiffness at different time points. Student’st-test for unpaired data was used for analysis of intrain-dividual changes based on single measurements of eachliver stiffness determination.
Laboratory findings and liver stiffness in patientsas well as the baseline characteristics of patients andcontrols were analysed using the Kruskal–Wallis test and
the Mann–Whitney U-test. Differences were consideredsignificant at P ! 0.01. Statistical analyses were per-formed using SPSS, version 15.0.1 (SPSS, Munich, Ger-many).
Results
The proof-of-concept study performed in eight patientswith chronic hepatitis C demonstrated a significantincrease in liver stiffness immediately after finishing foodintake (0 min), 15 and 60 min later (P = 0.01). Liverstiffness normalized 3 h after finishing breakfast (Fig. 1).These data served to define time points of " 30, 0 and60 min for the subsequent study.
In the larger cohort of the second part of this study, wesearched for significant changes of liver stiffness after ameal using an intraindividual analysis based on the singlemeasurements that constitute a liver stiffness determina-tion. For every single patient, at least 10 individualmeasurements at fasting were compared with at least 10individual measurements either directly after finishingfood intake or 1 h later. A statistically significant change(Po 0.01) was observed in 33 out of 56 patients (59%).Of these, 27 patients showed a significant increase, whilesix presented with a decrease of liver stiffness. In thecontrols, liver stiffness significantly increased in eight of19 (42%) subjects.
For further analysis according to the presumed stage offibrosis (i.e. no significant fibrosis, significant fibrosisand advanced fibrosis), patients and controls weregrouped according to their fasting liver stiffness. Valuesof o 6, 6–10 and 4 10 kPa were measured in 23, 20 and13 patients respectively. All but one control had an initialliver stiffness of o 6 kPa. The baseline characteristics ofpatients and controls are presented in Table 1.
A statistically significant increase was observed in 22out of 43 patients (51%) with an initial liver stiffnesso 10 kPa. Table 2 shows the individual responses to foodintake according to the different liver stiffness categories.
Mean of 8 patients (± SEM)
–60 –30 0 30 60 90 120 150 1804
6
8
10
Time (min)
Live
r st
iffne
ss (
kPa)
P = 0.01
Break-fast
Fig. 1. Proof-of-concept pilot trial. Patients (n = 8) were evaluatedfor liver stiffness over a total time period of 240 min. Between timepoints "30 and 0 min, patients ingested a standardized meal. Dataare presented as mean# SEM. Significance as calculated by theWilcoxon test. SEM, standard error of mean.
Table 2. Intraindividual analysis of at least 10 single measurements of one liver stiffness determination at fasting and after food intake ofpatients in the second part of the study
Fasting stiffness Number Mean# SD Range
o6 kPa 23Decrease (Po 0.01) 1 1.3 NAIncrease (Po 0.01) 12 2.1# 2.2 0.4–8.8No significant change 10 0.7# 0.5 0.2–1.5
6–10 kPa 20Decrease (Po 0.01) 1 1.6 NAIncrease (Po 0.01) 10 2.8# 1.4 0.3–4.8No significant change 9 0.5# 0.5 "0.3–1.4
410 kPa 13Decrease (Po 0.01) 4 3.4# 2.0 0.6–5.4Increase (Po 0.01) 5 7.2# 6.5 3.2–18.7No significant change 4 0.8# 3.7 "3.6–5.2
Number of patients with significant decrease/increase or no significant change as well as mean change and range are presented.
Liver International (2009)1502 c$ 2009 John Wiley & Sons A/S
Food intake increases liver stiffness Mederacke et al.
Influence of food intake
test, respectively; Smin ¼ minimum value of stiffness,Smax ¼ maximum value of stiffness, Sdelta (kPa) ¼(maximal stiffness " basal stiffness), Sdelta (%) ¼(maximal stiffness " basal stiffness) / basal stiffness #100. With the exception of Sdelta (%), which showed adecreasing trend, all stiffness indexes showed anincreasing trend for increasing stages of fibrosis (P <0.0001 for all, Jonckheere-Terpstra test), as also illus-trated in Fig. 2 for Sdelta (kPa).Probability of Detecting the Stage of Fibrosis at Dif-
ferent Timepoints After a Standardized Meal. Sincemost centers do not apply a fasting time before theTE procedure, the probability of detecting fibrosisstage at each timepoint: basal, 15, 30, 45, and 60minutes postmeal was evaluated (Fig. 3). It is evidentfrom the comparison of the probability curves that noother timepoint was superior than S0 in detecting anystage of fibrosis.The same analysis was applied to the comparison of
basal stiffness and delta stiffness based on the peakchange irrespective of the postmeal timepoint. Figure4 illustrates the probability (point estimate and 95%confidence intervals) of fibrosis stage (F0-F1, F2-F3,andF4) on the basis of S0 (kPa) and Sdelta (kPa). Valuesof S0 $18 kPa were associated with a probability ofF4 fibrosis $92%, confirming our previous observa-tions in a different series of patients with HCV-induced CLD.3 Even if the probability of fibrosis wasalso associated with Sdelta (kPa), this latter was clearlynot superior to S0 in detecting the probability of liverfibrosis. The worse performance of the predictionbased on Sdelta was also evident by the comparison ofits BIC value (332) with that of the S0 model (179).
Probability of Detecting the Child-Pugh Stageand the Presence of Esophageal Varices From BasalStiffness and Delta Stiffness After a StandardizedMeal. Although the between-group difference in Sdelta(kPa) was significant (exact-P ¼ 0.037), it was not use-ful for discriminating between Child-Pugh stage A andB because of substantial overlap (data not shown). Thesame conclusion applies to the ability of Sdelta (kPa) todiscriminate between the presence or the absence ofesophageal varices (exact-P ¼ 0.0009). In both cases,the use of Sdelta (kPa) did not show any advantagewhen compared to S0 (kPa) (data not shown).
Discussion
During the past decade, TE has been shown to rep-resent an important tool for the assessment of thefibrotic evolution of CLD, particularly chronic HCVhepatitis. In this context, the integration of TE andother noninvasive methods with liver biopsy hasbrought definite advantages in the allocation of patientsin different classes of disease progression.1,17 Because ofthe increasing use of TE in the everyday managementof patients with chronic HCV hepatitis, major effortsare dedicated to the optimal standardization of thismethodology in view of its inclusion in clinical practiceguidelines. Along these lines, the identification of fac-tors negatively affecting the diagnostic accuracy of TE,i.e., ‘‘confounding factors,’’ is absolutely crucial.The work by Mederacke at al.7 highlighted the
possibility that LS values may be affected if TE is per-formed shortly after a meal. Considering that in mostcenters TE is scheduled during the whole working dayand that there are not precise recommendations concern-ing fasting prior to the performance of TE, overestima-tion of LS values is likely a frequent occurrence. Even aminor overestimation of 3-4 kPa may have a significantimpact on the interpretation of this noninvasive method,
Fig. 2. Relationship between delta stiffness and stage of fibrosis.
Table 3. Baseline and Postmeal Liver Stiffness Values in the125 Patients Included in the Study Stratified by Liver
Fibrosis Stage
F0-1(n ¼ 50)Median IQR
F2-3 (n¼ 35)Median IQR
F4(n ¼ 40)Median IQR JT test P Value
S0 (kPa) 5.0 1.4 10.7 3.4 21.2 25.7 <0.001S15 (kPa) 5.9 1.7 12.2 4.3 24.5 27.3 <0.001S30 (kPa) 6.2 1.8 14.2 5.1 24.9 27.3 <0.001S45 (kPa) 5.7 1.4 12.1 5.0 24.9 28.4 <0.001S60 (kPa) 5.5 1.3 11 4.2 22.7 27.7 <0.001Smin (kPa) 5.0 1.4 10.7 3.4 21.2 25.9 <0.001Smax (kPa) 6.7 1.9 13.2 5.0 25.4 28.7 <0.001Sdelta (kPa) 1.9 0.9 2.7 0.8 4.7 2.8 <0.001Sdelta (%) 33.6 21.1 25.3 8.6 16.6 7.5 <0.001
Abbreviations: F0-F4, METAVIR stage of fibrosis; IQR, interquartile range; JT,Jonckheere-Terpstra test; S0-S60, stiffness values at different time points duringthe meal test; Smin, minimal stiffness value during the meal test; Smax, maximalstiffness value during the meal test; Sdelta (kPa), difference between maximaland minimal stiffness value during the test meal; Sdelta (%), [(maximal stiffnessbasal stiffness) / basal stiffness] x 100.
HEPATOLOGY, Vol. 58, No. 1, 2013 ARENA, LUPSOR PLATON, ET AL. 69
Arena et al. Hepatology 2013; 58: 65-72
Mederacke et al. Liver Int 2009; 29: 1500-6
TE should be performed in fasting patients

Confounders of liver stiffness summary for clinical practice
Tapper, Castera, Afdhal. Clin Gastroenterol Hepatol 2015; In press

◆ Principe & limites
◆ Performances diagnostiques
◆ Comparaison avec les biomarqueurs
◆ Suivi de la progression de la fibrose
◆ Nouvelles techniques
Plan

FibroScan: meta-analyses
Chon et al. PLoS ONE 2012
might have produced false-positive results[27] and reduced theoverall sensitivity and specificity of TE in our study.The optimal cutoff values in our study were 7.9 kPa for $F2,
8.8 kPa for $F3, and 11.7 kPa for F4. However, Stebbing et al. [16]determined higher cutoff values (7.81 kPa for $F2 and 15.56 kPafor F4), which increased further when calculated only for patientswith CHC (8.44 kPa for $F2 and 16.14 kPa for F4). Fredrich-rustet al. [17] and Tsochatzis et al. [18] also adopted higher cutoff values(13.01 and 15.0 kPa, respectively) for determining F4 comparedwith that found in our study (11.7 kPa; Table 4). This tendency oflow cutoff TE values in our study may be explained by two uniquefeatures of CHB. First, Sturm et al. [46] concluded recently that thetotal amount of liver fibrosis reflected by the fibrosis area wassignificantly lower in patients with CHB, because the fibrous septamight be thinner in these patients than in those with CHC withthe same histological stage (F4). Second, because CHB tends toprogress to cirrhosis with larger nodules (macronodular cirrhosis)than CHC, the TE pulse is more likely to pass through the normalliver parenchyma between fibrotic bands in patients with CHBthan in those with CHC. [47] These two observations might have
resulted in a lower cutoff TE value for patients with CHBcompared with patients with CHC. Thus, physicians should beaware of the pitfalls of TE, such as false negativity or lower cutoffvalues resulting from macro nodular cirrhosis and thin fibroussepta, and false positivity or lower performance resulting from highALT levels. [48] Accordingly, TE results should be interpretedwithin the clinical context.Based on the results of our meta-analysis, TE seems to be a good
tool for assessing liver fibrosis in patients with CHB, but it is notexcellent. However, because LB is not a perfect gold standard, it isnearly impossible to achieve an AUROC close to 1 in an analysisbased on LB data, even with a hypothetically perfect noninvasiveliver fibrosis measurement tool. [49] Although TE is inferior tohistological evaluation in principle, TE is superior to clinicaldiagnostic criteria in diagnosing compensated cirrhosis. [19,50]Thus, the performance of TE in our study (AUROC=0.93) forpredicting cirrhosis is sufficiently accurate. Accurate evaluation ofTE diagnostic performance will only be possible after establishingan optimal reference standard, such as laparoscopic biopsy froma designated liver location.
Figure 1. Forest plot from meta-analysis of AUROC value using a random-effect model for fibrosis stages (a) significant fibrosis (b)severe fibrosis (c) cirrhosis. The distribution is depicted according to the sample size and the length of the horizontal line represents the 95% CI. :AUROC of the studies with patients with CHB only. : AUROC of the studies with mixed etiologies with available sub-group analysis for patients withCHB.doi:10.1371/journal.pone.0044930.g001
Table 4. Characteristics of previous reported meta-analyses versus current study.
Number ofincludedstudies
Number ofincluded subjectsfor analysis AUROC
Sensitivity/Specificity (%) Cutoff values (kPa)
$ F2 $ F3 F4 $ F2 F4 $ F2 $ F3 F4
Talwalkar15 9 2,083 0.870 N/A 0.957 70/84 87/91 N/A N/A N/A
Stebbing16 22 4,760 0.84 0.89 0.94 70/84 87/91 7.81 N/A 15.56
Fredrich-rust et al17 50 8,206 0.84 0.89 0.94 N/A N/A 7.65 N/A 13.01
Tsochatzis et al18 40 7,723 N/A N/A N/A 79/78 83/89 7.3 10.2 15.0
Chon et al 18 2,772 0.859 0.887 0.929 74.3/78.3 84.6/81.5 7.9 8.8 11.7
AUROC, area under the receiver operating characteristic curve; kPa, kilopascal.doi:10.1371/journal.pone.0044930.t004
A Meta-Analysis on Performance of TE
PLOS ONE | www.plosone.org 5 September 2012 | Volume 7 | Issue 9 | e44930
might have produced false-positive results[27] and reduced theoverall sensitivity and specificity of TE in our study.The optimal cutoff values in our study were 7.9 kPa for $F2,
8.8 kPa for $F3, and 11.7 kPa for F4. However, Stebbing et al. [16]determined higher cutoff values (7.81 kPa for $F2 and 15.56 kPafor F4), which increased further when calculated only for patientswith CHC (8.44 kPa for $F2 and 16.14 kPa for F4). Fredrich-rustet al. [17] and Tsochatzis et al. [18] also adopted higher cutoff values(13.01 and 15.0 kPa, respectively) for determining F4 comparedwith that found in our study (11.7 kPa; Table 4). This tendency oflow cutoff TE values in our study may be explained by two uniquefeatures of CHB. First, Sturm et al. [46] concluded recently that thetotal amount of liver fibrosis reflected by the fibrosis area wassignificantly lower in patients with CHB, because the fibrous septamight be thinner in these patients than in those with CHC withthe same histological stage (F4). Second, because CHB tends toprogress to cirrhosis with larger nodules (macronodular cirrhosis)than CHC, the TE pulse is more likely to pass through the normalliver parenchyma between fibrotic bands in patients with CHBthan in those with CHC. [47] These two observations might have
resulted in a lower cutoff TE value for patients with CHBcompared with patients with CHC. Thus, physicians should beaware of the pitfalls of TE, such as false negativity or lower cutoffvalues resulting from macro nodular cirrhosis and thin fibroussepta, and false positivity or lower performance resulting from highALT levels. [48] Accordingly, TE results should be interpretedwithin the clinical context.Based on the results of our meta-analysis, TE seems to be a good
tool for assessing liver fibrosis in patients with CHB, but it is notexcellent. However, because LB is not a perfect gold standard, it isnearly impossible to achieve an AUROC close to 1 in an analysisbased on LB data, even with a hypothetically perfect noninvasiveliver fibrosis measurement tool. [49] Although TE is inferior tohistological evaluation in principle, TE is superior to clinicaldiagnostic criteria in diagnosing compensated cirrhosis. [19,50]Thus, the performance of TE in our study (AUROC=0.93) forpredicting cirrhosis is sufficiently accurate. Accurate evaluation ofTE diagnostic performance will only be possible after establishingan optimal reference standard, such as laparoscopic biopsy froma designated liver location.
Figure 1. Forest plot from meta-analysis of AUROC value using a random-effect model for fibrosis stages (a) significant fibrosis (b)severe fibrosis (c) cirrhosis. The distribution is depicted according to the sample size and the length of the horizontal line represents the 95% CI. :AUROC of the studies with patients with CHB only. : AUROC of the studies with mixed etiologies with available sub-group analysis for patients withCHB.doi:10.1371/journal.pone.0044930.g001
Table 4. Characteristics of previous reported meta-analyses versus current study.
Number ofincludedstudies
Number ofincluded subjectsfor analysis AUROC
Sensitivity/Specificity (%) Cutoff values (kPa)
$ F2 $ F3 F4 $ F2 F4 $ F2 $ F3 F4
Talwalkar15 9 2,083 0.870 N/A 0.957 70/84 87/91 N/A N/A N/A
Stebbing16 22 4,760 0.84 0.89 0.94 70/84 87/91 7.81 N/A 15.56
Fredrich-rust et al17 50 8,206 0.84 0.89 0.94 N/A N/A 7.65 N/A 13.01
Tsochatzis et al18 40 7,723 N/A N/A N/A 79/78 83/89 7.3 10.2 15.0
Chon et al 18 2,772 0.859 0.887 0.929 74.3/78.3 84.6/81.5 7.9 8.8 11.7
AUROC, area under the receiver operating characteristic curve; kPa, kilopascal.doi:10.1371/journal.pone.0044930.t004
A Meta-Analysis on Performance of TE
PLOS ONE | www.plosone.org 5 September 2012 | Volume 7 | Issue 9 | e44930
Talwalkar et al. CGH 2007 Friedrich-Rust et al. Gastroenterology 2008
Tsochatzis et al. J Hepatol 2011 Stebbing et al. APT 2010

14.6
Transient elastography for cirrhosis (n=1007 patients with various CLD, 165 with cirrhosis)
3 75
correctly classified 92 %
Ganne-Carrié et al. Hepatology 2006; 44: 1511-7
F = 4 74%
4.5% misclassified
17%
3.5 % misclassified
F < 4 96%
83%

75 KPa 3
FibroScan : which cut-offs ?
de Ledinghen et al. JAIDS 2006
12.5
HCV
11.0
HBV
Marcellin et al. Liver Int 2009 Castera et al. Gastroenterology 2005
F4:
17.1
PBC/PSC
Corpechot et al. Hepatology 2006
8% 25%
11.8
HIV-HCV
24% 19%

Cirrhosis: Post-test probabilities (pre-test:14%)
N=1307 patients with viral hepatitis; 14% with cirrhosis
Post
test
pro
babi
litie
s of
cirr
hosi
s 72%
50% 40% 10%
0-3%
7-27%
< 7kPa 7-17kPa >17kPa
Degos et al. J Hepatol 2010; 53: 1013-21

◆ Principe & limites
◆ Performances diagnostiques
◆ Comparaison avec les biomarqueurs
◆ Suivi de la progression de la fibrose
◆ Nouvelles techniques
Plan

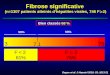
Castera et al. Gastroenterology 2005; 128: 343-50.
Comparaison des approches fibrose significative
P=NS
Degos et al. J Hepatol 2010; 53: 1013-21
P=NS

N= 1307 patients; F4: 25% .
P<0.0001
Comparaison des approches cirrhose
Degos et al. J Hepatol 2010; 53: 1013-21

N= 436 patients; F4: 14% .
Comparaison des approches cirrhose
Zarski et al. J Hepatol 2012; 56: 55-62
ZARSKI
superior to the best blood tests or Fibroscan™ alone in the ‘‘per-protocol’’ analysis (382 patients). However, when we consideredthe population of 436 patients (‘‘intention to diagnose popula-tion’’) the combination of Fibroscan™ plus a blood test markedlyimproved the percentage of well classified patients for both sig-nificant fibrosis and cirrhosis.
Other analyses
Wealso calculated thenumberof ‘‘theoretically avoided liver biop-sies’’ for the diagnosis of significant fibrosis using negative andpositive predictive values of 90% (Supplementary Table S7). No dif-ference was found between Fibrometer! (36.6%), Fibrotest!
(35.6%), Hepascore! (30.5%), and interpretable Fibroscan™(45.8%).
Discussion
Blood tests and Fibroscan™ have been recently developed asalternatives to liver biopsy [24]. Retrospective studies[14,25,26] have compared several of these markers to liver biopsybut to our knowledge this is one of the first independent prospec-tive validation of all relevant blood tests, and Fibroscan™ com-pared to liver biopsy in untreated patients with CHC. The trueindicator of liver disease status would be the histological analysisof the entire liver, but impossible to obtain in routine practiceand thus liver biopsy is considered at best as an ‘‘imperfect goldstandard’’ [27]. Reduced sensitivity for the detection of significantfibrosis has been demonstrated with biopsies of less than 30 mm,fragmented specimens and steatosis. Concerning errors consecu-tive to the biopsy itself, Metha et al. [28] have demonstrated thatthe AUROC for a perfect marker would not exceed 0.90 or 0.83according to 40% or 50% prevalence of significant disease in esti-mations where liver biopsy accuracy is highest (sensitivity andspecificity of 90%). However, our study especially takes into con-sideration the methodological aspects so as to optimize the inter-pretation of the stage of fibrosis. Firstly, the liver specimens hadto answer to quality criteria [29] to prevent a high risk of discor-dance for fibrosis staging [3,4,30]. Until now no study hasincluded patients with such a high mean length of biopsy withoutfragmentation, cirrhosis excepted. By using the METAVIR scoringsystem, 65% of liver biopsies with a length of 15 mm are usually
classified. This percentage increases to 75% for a length of 25 mm[3]. Also, a 25 mm biopsy is considered the optimal length foraccurate liver evaluation. Considering this, in our study a sam-pling error for liver biopsy remains since only 50% of patientshad a liver biopsy length greater than 25 mm. In addition, twosenior liver pathologists independently reviewed biopsies [4]which were re-examined to reach a consensus in cases of dis-agreement. The agreement between the two expert pathologistswas better than those previously published [4]. In order toexclude inter-laboratory variability the biochemical analyseswere centralized with standardized methods and enzymatic cal-ibration [31]. All serum samples were stored at !80 "C since thestability of different parameters could be affected by storage [32]such as marked transaminase activity loss at !20 "C [33].
The AUROCs of each test were comparable to those reported inthe original publications [6–15,18,20] when expressed usingobserved-AUROCs according to the prevalence of stages definingadvanced and non-advanced fibrosis. We observed similar AUR-OCs to those reported in meta-analyses [34–36] for the most val-idated biomarkers, Fibrotest!, Fibrometer!, and Apri and withoutmajor differences with interpretable Fibroscan™, Hepascore!, andELFG. In diagnosing cirrhosis, the ‘‘Fibrostic’’ study [37] showed asignificantly better performance of Fibroscan™ compared toserum markers while in contrast, our study shows that all thetests performed equivalently. This difference between these tworecent multicentre studies might be due to differences in design.Indeed in the ‘‘Fibrostic’’ study, Fibroscan™ was used in firstintent and analysed apart from blood tests, while in our studywe tried to compare in first intent all tests in ‘‘intention to diag-nose’’. The methodology used for Fibroscan™ was equivalent inthe two studies but the blood tests were performed in each centrein the Fibrostic study, using assay methods that might possiblyhave not always been homogeneous, while they were centralizedin the Fibrostar study, except when impossible, and rigorouslystandardized analytical conditions were respected.
For differentiating between adjacent stages, F1 vs. F2, onlyHyaluronate was inferior to Fibrometer!. For this adjacent com-parison, AUROCs could appear low, but the performances weresimilar relative to liver biopsy. Indeed comparison between abiopsy of 25 mm (mean length in our study) and the true goldstandard consisting of a large surgical sample showed 25% offalse negative/positives and an AUROC evaluated at 85% for F2vs. F1 [3].
Table 3. Performance of blood tests and Fibroscan™ for the diagnosis of cirrhosis (F4).
n = 436* n = 382‡
AUROC 95% CI p Sidak AUROC 95% CI p Sidak
FIBROMETER® 0.89 [0.86;0.93] 0.90 [0.86;0.93]
FIBROTEST® 0.86 [0.83;0.90] 0.325 0.87 [0.82;0.91] 0.321
APRI 0.86 [0.81;0.91] 0.141 0.87 [0.82;0.91] 0.410
ELFG 0.88 [0.83;0.92] 0.883 0.87 [0.83;0.92] 0.860
HEPASCORE® 0.89 [0.86;0.93] 1.000 0.89 [0.85;0.92] 0.998
FIB4 0.83 [0.76;0.89] 0.018 0.84 [0.77;0.90] 0.069
FIBROSCAN™ (interpretable results)
- - - 0.93 [0.89;0.96] 0.559
⁄CHC patients having all blood tests; !CHC patients with all the tests and interpretable Fibroscan™.
JOURNAL OF HEPATOLOGY
Journal of Hepatology 2012 vol. 56 j 55–62 59

Summary: significant fibrosis
Transient elastography Serum markers
=

Summary: cirrhosis
Transient elastography Serum markers
<

Qu’en est-il de la combinaison
des méthodes?

Castera et al. Gastroenterology 2005; 128: 343-50.
Elastométrie Marqueurs sériques
+ Bien
classés F≥2: 75%
La combinaison augmente les performances diagnostiques

Poynard et al. Plos One 2008
Concordance in world without gold standard: a new way to increase diagnostic accuracy

Boursier et al. Am J Gastroenterol 2011; 106: 1255-63 N= 729 patients with CHC
La combinaison augmente les performances diagnostiques

• Good reproducibility • High applicability (95%) • Low cost & wide availability (non patented)
• Advantages FibroScan
• Genuine property of the liver • High performance for cirrhosis • User-friendly
• Advantages Biomarkers
• Disadvantages • Non specific of the liver • Performance for cirrhosis • Cost & availability (patented)
• Disadvantages
• Low applicability (80%) • False positive (inflammation) • Requires a dedicated device-
Biomarkers vs. FibroScan summary
Castera L . Gastroenterology 2012; 142: 1293-302

◆ Principe & limites
◆ Performances diagnostiques
◆ Comparaison avec les biomarqueurs
◆ Suivi de la progression de la fibrose
◆ Nouvelles techniques
Plan

varices (stage 2). However, staging of compensated cir-rhosis could be further refined as (1) no portal hyperten-sion (HVPG !6 mmHg); (2) portal hypertension that isnot clinically significant (HVPG between 6 and 10mmHg); and (3) clinically significant portal hypertension(HVPG " 10 mmHg or presence of collaterals). Substag-ing of decompensated cirrhosis is not as well-defined butwould likely be classified according to both the degree ofportal hypertension and the degree of liver/circulatorydysfunction (with recurrent variceal hemorrhage, refrac-tory ascites, and hepatorenal syndrome representing moresevere stages) (Fig. 1). It remains possible that additionaltechnologies apart from HVPG will emerge that can fur-ther discriminate the pathological and functional state ofthe liver. Such information could be vital to optimize thetiming and nature of antifibrotic therapies, or the need forliver transplantation. Thus far, liver stiffness measure-ment (LSM) obtained by transient elastography is themost promising noninvasive approach for monitoring fi-brosis progression associated with worsening portal hy-pertension. LSM has an excellent correlation with HVPGvalues below a threshold of 10-12 mmHg.29,30 Althoughthese findings need to be further substantiated in largerindependent studies, they suggest that LSM may be usefulin the detection of clinically significant portal hyperten-sion and, thereby, in further subclassifying compensated
cirrhosis. On the other hand, LSM may not be accurate indecompensated cirrhosis where, in addition to intrahe-patic vascular resistance, there are complex hemodynamicchanges.31 Nonetheless, it will be important to evaluate,in longitudinal studies, whether single LSM values or dy-namic changes over time are predictive of initial or furtherdecompensation, or the response to pharmacologicaltherapy.32,33
We encourage the practicing community, patholo-gists, and investigators to move beyond the simple char-acterization of cirrhosis as a single stage and instead beginthinking of cirrhosis as a series of critical steps that, if leftunchecked, culminate in hepatic decompensation. A newframework for classifying cirrhosis will require integrationof both current and emerging knowledge about liverstructure and function. From one stage, there shouldemerge many.
References1. Pinzani M, Rombouts K, Colagrande S. Fibrosis in chronic liver diseases:
diagnosis and management. J Hepatol 2005;42(Suppl. 1):S22-S36.2. Anthony PP, Ishak KG, Nayak NC, Poulsen HE, Scheuer PJ, Sobin LH.
The morphology of cirrhosis. Recommendations on definition, nomencla-ture, and classification by a working group sponsored by the World HealthOrganization. J Clin Pathol 1978;31:395-414.
3. Poynard T, Bedossa P, Opolon P, for the OBSVIRC MCADg. Naturalhistory of liver fibrosis progression in patients with chronic hepatitis C.Lancet 1997;349:825-832.
Fig. 1. Classification of chronic liver disease based on histological, clinical, hemodynamic, and biological parameters. In the noncirrhotic stage(METAVIR F1-F3), there is no clinical evidence of cirrhosis, the HVPG is below 6 mmHg, and at this stage there is fibrogenesis and neovascularization.The cirrhotic stage (METAVIR F4) is broadly classified into two stages: compensated and decompensated, with clinical decompensation being definedby the development of ascites, variceal hemorrhage (VH), encephalopathy, and jaundice. Within the compensated stage, patients can be subclassifiedinto those without varices (stage 1) and those with varices (stage 2). Those without varices can be further subclassified into those with an hepaticvenous pressure gradient (HVPG) ! or " 10 mmHg, which is the threshold pressure that predicts development of varices and decompensation.HVPG " 10 mmHg (clinically significant portal hypertension) correlates with thick scar and small nodules. In the decompensated stage, the scar isresistant to degradation. Complex circulatory (splanchnic and systemic) abnormalities that occur at this decompensated stage contribute to furtherdecompensation, i.e., recurrent variceal hemorrhage, refractory ascites, and hepatorenal syndrome, and although HVPG retains prognostic value, otherparameters that take into account liver insufficiency and a deranged circulatory state, such as the MELD score, are more predictive of death (notdepicted in figure). Figure is modified from Friedman.23
1448 GARCIA-TSAO ET AL. HEPATOLOGY, April 2010
varices (stage 2). However, staging of compensated cir-rhosis could be further refined as (1) no portal hyperten-sion (HVPG !6 mmHg); (2) portal hypertension that isnot clinically significant (HVPG between 6 and 10mmHg); and (3) clinically significant portal hypertension(HVPG " 10 mmHg or presence of collaterals). Substag-ing of decompensated cirrhosis is not as well-defined butwould likely be classified according to both the degree ofportal hypertension and the degree of liver/circulatorydysfunction (with recurrent variceal hemorrhage, refrac-tory ascites, and hepatorenal syndrome representing moresevere stages) (Fig. 1). It remains possible that additionaltechnologies apart from HVPG will emerge that can fur-ther discriminate the pathological and functional state ofthe liver. Such information could be vital to optimize thetiming and nature of antifibrotic therapies, or the need forliver transplantation. Thus far, liver stiffness measure-ment (LSM) obtained by transient elastography is themost promising noninvasive approach for monitoring fi-brosis progression associated with worsening portal hy-pertension. LSM has an excellent correlation with HVPGvalues below a threshold of 10-12 mmHg.29,30 Althoughthese findings need to be further substantiated in largerindependent studies, they suggest that LSM may be usefulin the detection of clinically significant portal hyperten-sion and, thereby, in further subclassifying compensated
cirrhosis. On the other hand, LSM may not be accurate indecompensated cirrhosis where, in addition to intrahe-patic vascular resistance, there are complex hemodynamicchanges.31 Nonetheless, it will be important to evaluate,in longitudinal studies, whether single LSM values or dy-namic changes over time are predictive of initial or furtherdecompensation, or the response to pharmacologicaltherapy.32,33
We encourage the practicing community, patholo-gists, and investigators to move beyond the simple char-acterization of cirrhosis as a single stage and instead beginthinking of cirrhosis as a series of critical steps that, if leftunchecked, culminate in hepatic decompensation. A newframework for classifying cirrhosis will require integrationof both current and emerging knowledge about liverstructure and function. From one stage, there shouldemerge many.
References1. Pinzani M, Rombouts K, Colagrande S. Fibrosis in chronic liver diseases:
diagnosis and management. J Hepatol 2005;42(Suppl. 1):S22-S36.2. Anthony PP, Ishak KG, Nayak NC, Poulsen HE, Scheuer PJ, Sobin LH.
The morphology of cirrhosis. Recommendations on definition, nomencla-ture, and classification by a working group sponsored by the World HealthOrganization. J Clin Pathol 1978;31:395-414.
3. Poynard T, Bedossa P, Opolon P, for the OBSVIRC MCADg. Naturalhistory of liver fibrosis progression in patients with chronic hepatitis C.Lancet 1997;349:825-832.
Fig. 1. Classification of chronic liver disease based on histological, clinical, hemodynamic, and biological parameters. In the noncirrhotic stage(METAVIR F1-F3), there is no clinical evidence of cirrhosis, the HVPG is below 6 mmHg, and at this stage there is fibrogenesis and neovascularization.The cirrhotic stage (METAVIR F4) is broadly classified into two stages: compensated and decompensated, with clinical decompensation being definedby the development of ascites, variceal hemorrhage (VH), encephalopathy, and jaundice. Within the compensated stage, patients can be subclassifiedinto those without varices (stage 1) and those with varices (stage 2). Those without varices can be further subclassified into those with an hepaticvenous pressure gradient (HVPG) ! or " 10 mmHg, which is the threshold pressure that predicts development of varices and decompensation.HVPG " 10 mmHg (clinically significant portal hypertension) correlates with thick scar and small nodules. In the decompensated stage, the scar isresistant to degradation. Complex circulatory (splanchnic and systemic) abnormalities that occur at this decompensated stage contribute to furtherdecompensation, i.e., recurrent variceal hemorrhage, refractory ascites, and hepatorenal syndrome, and although HVPG retains prognostic value, otherparameters that take into account liver insufficiency and a deranged circulatory state, such as the MELD score, are more predictive of death (notdepicted in figure). Figure is modified from Friedman.23
1448 GARCIA-TSAO ET AL. HEPATOLOGY, April 2010
varices (stage 2). However, staging of compensated cir-rhosis could be further refined as (1) no portal hyperten-sion (HVPG !6 mmHg); (2) portal hypertension that isnot clinically significant (HVPG between 6 and 10mmHg); and (3) clinically significant portal hypertension(HVPG " 10 mmHg or presence of collaterals). Substag-ing of decompensated cirrhosis is not as well-defined butwould likely be classified according to both the degree ofportal hypertension and the degree of liver/circulatorydysfunction (with recurrent variceal hemorrhage, refrac-tory ascites, and hepatorenal syndrome representing moresevere stages) (Fig. 1). It remains possible that additionaltechnologies apart from HVPG will emerge that can fur-ther discriminate the pathological and functional state ofthe liver. Such information could be vital to optimize thetiming and nature of antifibrotic therapies, or the need forliver transplantation. Thus far, liver stiffness measure-ment (LSM) obtained by transient elastography is themost promising noninvasive approach for monitoring fi-brosis progression associated with worsening portal hy-pertension. LSM has an excellent correlation with HVPGvalues below a threshold of 10-12 mmHg.29,30 Althoughthese findings need to be further substantiated in largerindependent studies, they suggest that LSM may be usefulin the detection of clinically significant portal hyperten-sion and, thereby, in further subclassifying compensated
cirrhosis. On the other hand, LSM may not be accurate indecompensated cirrhosis where, in addition to intrahe-patic vascular resistance, there are complex hemodynamicchanges.31 Nonetheless, it will be important to evaluate,in longitudinal studies, whether single LSM values or dy-namic changes over time are predictive of initial or furtherdecompensation, or the response to pharmacologicaltherapy.32,33
We encourage the practicing community, patholo-gists, and investigators to move beyond the simple char-acterization of cirrhosis as a single stage and instead beginthinking of cirrhosis as a series of critical steps that, if leftunchecked, culminate in hepatic decompensation. A newframework for classifying cirrhosis will require integrationof both current and emerging knowledge about liverstructure and function. From one stage, there shouldemerge many.
References1. Pinzani M, Rombouts K, Colagrande S. Fibrosis in chronic liver diseases:
diagnosis and management. J Hepatol 2005;42(Suppl. 1):S22-S36.2. Anthony PP, Ishak KG, Nayak NC, Poulsen HE, Scheuer PJ, Sobin LH.
The morphology of cirrhosis. Recommendations on definition, nomencla-ture, and classification by a working group sponsored by the World HealthOrganization. J Clin Pathol 1978;31:395-414.
3. Poynard T, Bedossa P, Opolon P, for the OBSVIRC MCADg. Naturalhistory of liver fibrosis progression in patients with chronic hepatitis C.Lancet 1997;349:825-832.
Fig. 1. Classification of chronic liver disease based on histological, clinical, hemodynamic, and biological parameters. In the noncirrhotic stage(METAVIR F1-F3), there is no clinical evidence of cirrhosis, the HVPG is below 6 mmHg, and at this stage there is fibrogenesis and neovascularization.The cirrhotic stage (METAVIR F4) is broadly classified into two stages: compensated and decompensated, with clinical decompensation being definedby the development of ascites, variceal hemorrhage (VH), encephalopathy, and jaundice. Within the compensated stage, patients can be subclassifiedinto those without varices (stage 1) and those with varices (stage 2). Those without varices can be further subclassified into those with an hepaticvenous pressure gradient (HVPG) ! or " 10 mmHg, which is the threshold pressure that predicts development of varices and decompensation.HVPG " 10 mmHg (clinically significant portal hypertension) correlates with thick scar and small nodules. In the decompensated stage, the scar isresistant to degradation. Complex circulatory (splanchnic and systemic) abnormalities that occur at this decompensated stage contribute to furtherdecompensation, i.e., recurrent variceal hemorrhage, refractory ascites, and hepatorenal syndrome, and although HVPG retains prognostic value, otherparameters that take into account liver insufficiency and a deranged circulatory state, such as the MELD score, are more predictive of death (notdepicted in figure). Figure is modified from Friedman.23
1448 GARCIA-TSAO ET AL. HEPATOLOGY, April 2010
varices (stage 2). However, staging of compensated cir-rhosis could be further refined as (1) no portal hyperten-sion (HVPG !6 mmHg); (2) portal hypertension that isnot clinically significant (HVPG between 6 and 10mmHg); and (3) clinically significant portal hypertension(HVPG " 10 mmHg or presence of collaterals). Substag-ing of decompensated cirrhosis is not as well-defined butwould likely be classified according to both the degree ofportal hypertension and the degree of liver/circulatorydysfunction (with recurrent variceal hemorrhage, refrac-tory ascites, and hepatorenal syndrome representing moresevere stages) (Fig. 1). It remains possible that additionaltechnologies apart from HVPG will emerge that can fur-ther discriminate the pathological and functional state ofthe liver. Such information could be vital to optimize thetiming and nature of antifibrotic therapies, or the need forliver transplantation. Thus far, liver stiffness measure-ment (LSM) obtained by transient elastography is themost promising noninvasive approach for monitoring fi-brosis progression associated with worsening portal hy-pertension. LSM has an excellent correlation with HVPGvalues below a threshold of 10-12 mmHg.29,30 Althoughthese findings need to be further substantiated in largerindependent studies, they suggest that LSM may be usefulin the detection of clinically significant portal hyperten-sion and, thereby, in further subclassifying compensated
cirrhosis. On the other hand, LSM may not be accurate indecompensated cirrhosis where, in addition to intrahe-patic vascular resistance, there are complex hemodynamicchanges.31 Nonetheless, it will be important to evaluate,in longitudinal studies, whether single LSM values or dy-namic changes over time are predictive of initial or furtherdecompensation, or the response to pharmacologicaltherapy.32,33
We encourage the practicing community, patholo-gists, and investigators to move beyond the simple char-acterization of cirrhosis as a single stage and instead beginthinking of cirrhosis as a series of critical steps that, if leftunchecked, culminate in hepatic decompensation. A newframework for classifying cirrhosis will require integrationof both current and emerging knowledge about liverstructure and function. From one stage, there shouldemerge many.
References1. Pinzani M, Rombouts K, Colagrande S. Fibrosis in chronic liver diseases:
diagnosis and management. J Hepatol 2005;42(Suppl. 1):S22-S36.2. Anthony PP, Ishak KG, Nayak NC, Poulsen HE, Scheuer PJ, Sobin LH.
The morphology of cirrhosis. Recommendations on definition, nomencla-ture, and classification by a working group sponsored by the World HealthOrganization. J Clin Pathol 1978;31:395-414.
3. Poynard T, Bedossa P, Opolon P, for the OBSVIRC MCADg. Naturalhistory of liver fibrosis progression in patients with chronic hepatitis C.Lancet 1997;349:825-832.
Fig. 1. Classification of chronic liver disease based on histological, clinical, hemodynamic, and biological parameters. In the noncirrhotic stage(METAVIR F1-F3), there is no clinical evidence of cirrhosis, the HVPG is below 6 mmHg, and at this stage there is fibrogenesis and neovascularization.The cirrhotic stage (METAVIR F4) is broadly classified into two stages: compensated and decompensated, with clinical decompensation being definedby the development of ascites, variceal hemorrhage (VH), encephalopathy, and jaundice. Within the compensated stage, patients can be subclassifiedinto those without varices (stage 1) and those with varices (stage 2). Those without varices can be further subclassified into those with an hepaticvenous pressure gradient (HVPG) ! or " 10 mmHg, which is the threshold pressure that predicts development of varices and decompensation.HVPG " 10 mmHg (clinically significant portal hypertension) correlates with thick scar and small nodules. In the decompensated stage, the scar isresistant to degradation. Complex circulatory (splanchnic and systemic) abnormalities that occur at this decompensated stage contribute to furtherdecompensation, i.e., recurrent variceal hemorrhage, refractory ascites, and hepatorenal syndrome, and although HVPG retains prognostic value, otherparameters that take into account liver insufficiency and a deranged circulatory state, such as the MELD score, are more predictive of death (notdepicted in figure). Figure is modified from Friedman.23
1448 GARCIA-TSAO ET AL. HEPATOLOGY, April 2010
Garcia-Tsao et al. Hepatology 2010; 51: 1445-9
Now There Are Many (Stages) Where Before ThereWas One: In Search of a Pathophysiological
Classification of CirrhosisGuadalupe Garcia-Tsao,1 Scott Friedman,2 John Iredale,3 and Massimo Pinzani4
For more than a century and a half, the descriptionof a liver as “cirrhotic” was sufficient to connoteboth a pathological and clinical status, and to as-
sign the prognosis of a patient with liver disease. How-ever, as our interventions to treat advanced liver diseasehave progressed (e.g., antiviral therapies), the inadequacyof a simple one-stage description for advanced fibroticliver disease has become increasingly evident. Until re-cently, refining the diagnosis of cirrhosis into more thanone stage hardly seemed necessary when there were nointerventions available to arrest its progression. Now,however, understanding the range of potential outcomesbased on the severity of cirrhosis is essential in order topredict outcomes and individualize therapy. This positionpaper, rather than providing clinical guidelines, attemptsto catalyze a reformulation of the concept of cirrhosisfrom a static to a dynamic one, creating a template forfurther refinement of this concept in the future.
We already make the clinical distinction between com-pensated and decompensated cirrhosis, and are incremen-tally linking these clinical entities to quantitative variablessuch as portal pressure measurements and emerging non-invasive diagnostics. Moreover, mounting evidence sug-gests that cirrhosis encompasses a pathological spectrumwhich is neither static nor relentlessly progressive, butrather dynamic and bidirectional, at least in some pa-tients. Thus, there is a pressing need to redefine cirrhosisin a manner that better recognizes its underlying relation-ship to portal hypertension and related circulatory
changes, and more faithfully reflects its progression, re-versibility and prognosis, ultimately linking these param-eters to clinically relevant outcomes and therapeuticstrategies. The Child-Pugh and Model for End-StageLiver Disease (MELD) scores are currently deployed todefine prognosis by modeling hepatic dysfunction, but donot provide direct evidence of the stage or dynamic stateof cirrhosis. The need for more refined cirrhosis staging isespecially germane given the increasing use of effectiveantiviral treatments in patients with hepatitis B virus(HBV) and hepatitis C virus (HCV) cirrhosis and theemergence of effective antifibrotic agents, wherein wemust define favorable or unfavorable endpoints that cor-relate with a discrete clinical outcome in patients withcirrhosis.
The normal liver has only a small amount of fibroustissue in relation to its size. As a result of continued liverinjury, however, there is progressive accumulation of ex-tracellular matrix, or scar. Although different chronic liverdiseases are characterized by distinct patterns of fibrosisdeposition,1 the development of cirrhosis represents acommon outcome leading to similar clinical conse-quences that impose an increasing burden in clinical prac-tice.
Anatomical-Pathological ContextCirrhosis is defined histologically as a diffuse process in
which the normal anatomical lobules are replaced by ar-chitecturally abnormal nodules separated by fibrous tis-sue.2 Progressive histological stages have been defined inthe process leading to the development of cirrhosis.Among the more common staging systems, the META-VIR scale is distinguished by four stages, with stage F0representing lack of fibrosis; stage F1, portal fibrosis; stageF2, periportal fibrosis; stage F3, bridging fibrosis; and,finally, stage F4 representing cirrhosis.3 Similarly, theIshak4 and Scheuer scoring systems5,6 attempt to semi-quantitatively define progressive fibrosis based on the pat-tern and relative amounts of scar within a liver biopsyspecimen. In this context, once fibrosis reaches the finalstages, the diagnosis of cirrhosis is established and the
Abbreviations: HVPG, hepatic venous pressure gradient; LSM, liver stiffnessmeasurement.
From the 1Section of Digestive Diseases, Yale University School of Medicine, VAConnecticut Healthcare System, New Haven, CT; 2Division of Liver Diseases,Mount Sinai School of Medicine, New York, NY; 3Medical Research CouncilCentre for Inflammation Research, University of Edinburgh, Edinburgh, UK; and4Department of Internal Medicine, Center for Research, High Education andTransfer “DENOThe”, Universita degli Studi di Firenze, Firenze, Italy.
Received September 1, 2009; accepted October 29, 2009.Address reprint requests to: Scott L. Friedman, M.D., Box 1123, Mount Sinai
School of Medicine, 1425 Madison Avenue, Room 11-70C, New York, NY 10029-6574. E-mail: [email protected]; fax: 212-849-2574.
Copyright © 2009 by the American Association for the Study of Liver Diseases.Published online in Wiley InterScience (www.interscience.wiley.com).DOI 10.1002/hep.23478Potential conflict of interest: Nothing to report.
1445
notably activated hepatic stellate cells and portal myofi-broblasts, as well as key cytokines such as platelet-derivedgrowth factor and transforming growth factor beta.23 Theroles of bone marrow–derived cells and those arising fromepithelial-mesenchymal transition are still under evalua-tion, but it is unlikely that these sources of fibrogenic cellsprovide a major contribution to hepatic extracellular ma-trix in chronic human liver disease. Cellular sources ofproteases that degrade scar and the pathways that regulatethem are better understood. Moreover, a more nuancedunderstanding of distinctive pathogenic features of fibro-sis at different stages and from different etiologies meansthat fibrosis may be customized according to its durationand underlying cause.
Cirrhosis in experimental models and human diseasemay be reversible.24 Following withdrawal of an injuriousstimulus, a dense micronodular cirrhosis can undergo re-modeling to a more attenuated, macronodular pattern.However, some septa will persist, likely representing thoselaid down early in the injury and are therefore the most“mature” (i.e., cross-linked).
Moreover, in experimental models, such mature scarsmay be the site of neoangiogenesis. Such angiogenesis isalready present in chronic inflammatory liver diseases25
concurrent with the fibrogenic process and may also playa role in the pathogenesis of portal hypertension.26 Theeffectiveness of therapeutic angiogenic inhibitors in notonly improving fibrosis, but also in reducing portal pres-sure, is suggested by data from animal models but has notbeen established in humans.27 Although there are no datalinking septal remodeling to portal pressure changes, re-cent work correlating increased portal hypertension withsmaller nodule size and septal thickening suggests thatreversal of these events might lower portal pressure.20
These rodent models and human studies throw intorelief the inadequacy of a simple one stage classification,because although the micronodular and remodeled atten-uated macronodular cirrhosis are very different, they areboth defined by the same original pathologic description:“cirrhosis”. These same experimental models have alsofacilitated the comparative study of reversible and irre-versible septa. Specific septal changes that are associatedwith irreversibility include: matrix modification withcross-linking, elastin-rich scars, and septal neovasculariza-tion. Additionally, the loss of cells that drive matrix turn-over from the septa combined with vascular extinctionmay both limit reversibility. Lastly, of course, the persis-tence and intensity of the initiating injury will affect theprogression of cirrhosis via recurrent cycles of inflamma-tion and repair, regardless of the capacity of the liver torestore a more normal architecture.
Should antifibrotic therapies emerge, the challenges oftherapeutically resorbing fibrosis in a cirrhotic liver will bequite different from those of a noncirrhotic liver for sev-eral reasons. First, whereas evidence clearly indicates re-versibility of fibrosis in precirrhotic disease, thedeterminants of fibrosis regression in cirrhosis are notsufficiently clear, and the point at which cirrhosis is trulyirreversible is not established, either in morphologic orfunctional terms. Second, there is a heightened sense ofurgency in attempting to regress fibrosis in cirrhosis, be-cause continued progression might lead to imminent de-compensation, whereas noncirrhotic disease could bedecades away from clinical consequences. Thus, the speedof regression in cirrhosis may need to be greater, yet, thecirrhotic liver with its thicker, more cross-linked septa anddistorted vasculature may be less amenable to treatment.On the other hand, since fibrosis is part of a chronicwound healing reaction to encapsulate tissue damage,preventing the formation of scar tissue without removingthe cause of damage might be detrimental by amplifyingthe injury. Ideally, therefore, administration of an antifi-brotic agent would be most useful when coupled with aneffective treatment for the underlying liver disease (e.g.,antiviral drugs in patients with HBV or HCV). In con-trast, in cirrhotic liver, where the ultimate goal is thereduction of portal pressure, the use of antifibrotic agentscoupled with effective treatments to reduce portal pres-sure and its hemodynamic consequences might be morerational.
What Is Cirrhosis?Currently, the diagnosis of cirrhosis in diffuse disease
(viral hepatitis, alcohol) relies primarily on histopatholog-ical evidence of late-stage fibrosis (e.g., stage 4 fibrosisusing the METAVIR system, or stages 5 or 6 in the Ishakscoring system). In this context, and particularly inchronic hepatitis C, sampling errors may lead to underdi-agnosis28 or overdiagnosis of cirrhosis.19 Regardless, whenusing these and related staging systems, “cirrhosis” is astatic diagnosis reflecting the end stage of the wound heal-ing process, without adequately signifying the complexityof its pathogenesis, or its functional, hemodynamic andprognostic correlates. Because these collective changes arefundamental to provoking the transition from compen-sated to decompensated cirrhosis, we need a far morerefined pathophysiological classification of compensatedcirrhosis based on morphological, functional, and clinicaldata (Fig. 1).
At the least, a revised staging of cirrhosis should startwith its main classification of compensated and decom-pensated cirrhosis. Compensated cirrhosis in turn wouldcomprise two substages: without varices (stage 1) or with
HEPATOLOGY, Vol. 51, No. 4, 2010 GARCIA-TSAO ET AL. 1447
varices (stage 2). However, staging of compensated cir-rhosis could be further refined as (1) no portal hyperten-sion (HVPG !6 mmHg); (2) portal hypertension that isnot clinically significant (HVPG between 6 and 10mmHg); and (3) clinically significant portal hypertension(HVPG " 10 mmHg or presence of collaterals). Substag-ing of decompensated cirrhosis is not as well-defined butwould likely be classified according to both the degree ofportal hypertension and the degree of liver/circulatorydysfunction (with recurrent variceal hemorrhage, refrac-tory ascites, and hepatorenal syndrome representing moresevere stages) (Fig. 1). It remains possible that additionaltechnologies apart from HVPG will emerge that can fur-ther discriminate the pathological and functional state ofthe liver. Such information could be vital to optimize thetiming and nature of antifibrotic therapies, or the need forliver transplantation. Thus far, liver stiffness measure-ment (LSM) obtained by transient elastography is themost promising noninvasive approach for monitoring fi-brosis progression associated with worsening portal hy-pertension. LSM has an excellent correlation with HVPGvalues below a threshold of 10-12 mmHg.29,30 Althoughthese findings need to be further substantiated in largerindependent studies, they suggest that LSM may be usefulin the detection of clinically significant portal hyperten-sion and, thereby, in further subclassifying compensated
cirrhosis. On the other hand, LSM may not be accurate indecompensated cirrhosis where, in addition to intrahe-patic vascular resistance, there are complex hemodynamicchanges.31 Nonetheless, it will be important to evaluate,in longitudinal studies, whether single LSM values or dy-namic changes over time are predictive of initial or furtherdecompensation, or the response to pharmacologicaltherapy.32,33
We encourage the practicing community, patholo-gists, and investigators to move beyond the simple char-acterization of cirrhosis as a single stage and instead beginthinking of cirrhosis as a series of critical steps that, if leftunchecked, culminate in hepatic decompensation. A newframework for classifying cirrhosis will require integrationof both current and emerging knowledge about liverstructure and function. From one stage, there shouldemerge many.
References1. Pinzani M, Rombouts K, Colagrande S. Fibrosis in chronic liver diseases:
diagnosis and management. J Hepatol 2005;42(Suppl. 1):S22-S36.2. Anthony PP, Ishak KG, Nayak NC, Poulsen HE, Scheuer PJ, Sobin LH.
The morphology of cirrhosis. Recommendations on definition, nomencla-ture, and classification by a working group sponsored by the World HealthOrganization. J Clin Pathol 1978;31:395-414.
3. Poynard T, Bedossa P, Opolon P, for the OBSVIRC MCADg. Naturalhistory of liver fibrosis progression in patients with chronic hepatitis C.Lancet 1997;349:825-832.
Fig. 1. Classification of chronic liver disease based on histological, clinical, hemodynamic, and biological parameters. In the noncirrhotic stage(METAVIR F1-F3), there is no clinical evidence of cirrhosis, the HVPG is below 6 mmHg, and at this stage there is fibrogenesis and neovascularization.The cirrhotic stage (METAVIR F4) is broadly classified into two stages: compensated and decompensated, with clinical decompensation being definedby the development of ascites, variceal hemorrhage (VH), encephalopathy, and jaundice. Within the compensated stage, patients can be subclassifiedinto those without varices (stage 1) and those with varices (stage 2). Those without varices can be further subclassified into those with an hepaticvenous pressure gradient (HVPG) ! or " 10 mmHg, which is the threshold pressure that predicts development of varices and decompensation.HVPG " 10 mmHg (clinically significant portal hypertension) correlates with thick scar and small nodules. In the decompensated stage, the scar isresistant to degradation. Complex circulatory (splanchnic and systemic) abnormalities that occur at this decompensated stage contribute to furtherdecompensation, i.e., recurrent variceal hemorrhage, refractory ascites, and hepatorenal syndrome, and although HVPG retains prognostic value, otherparameters that take into account liver insufficiency and a deranged circulatory state, such as the MELD score, are more predictive of death (notdepicted in figure). Figure is modified from Friedman.23
1448 GARCIA-TSAO ET AL. HEPATOLOGY, April 2010
75 kPa 3 5.5 15 65

OV grade II / III
27
Ascites
49
HCC
54
Bleeding
63 kPa 12 75
Foucher et al. Gut 2006; 55: 403-8.
Complications de la cirrhose
711 patients with liver diseases F3F4 144

TE for predicting PTH, OV, LOV meta-analysis
Shi et al. Liver Int 2013; 56: 62-71 ‘positive’ measurement. Furthermore, a ‘negative’ mea-surement was also informative, as significant portalhypertension was present in only 11% of patients. Inthis respect, TE is promising and worthy to translateinto clinical practice in detecting significant portalhypertension that it is a reliable and non-invasive proce-dure. Therefore, TE could be integrated in the detectionof significant portal hypertension in untreated patientsfor PHT. TE might also be useful to select suspiciouspatients with CLD for HVPG measurement. Neverthe-less, when the pre-test probability of significant portalhypertension was as low as 25%, the probability of cor-rectly identifying significant portal hypertensiondecreased markedly. This suggests that an accurate selec-tion of patients is necessary to exploit the performanceof TE at its best. In addition, in patients with significantportal hypertension, TE might be used in monitoringthe hemodynamic response and the effect of drugsreducing portal pressure.
Although the pooled sensitivities for both detectionof oesophageal varices and large oesophageal varicesexceeded 0.85, the pooled specificities were rather low,0.53 (95% CI, 0.36–0.69) for oesophageal varices detec-tion and 0.59 (95% CI, 0.45–0.72) for large oesophagealvarices detection. In addition, the PPV and NPV of TEin diagnosing oesophageal varices or large oesophagealvarices were really low. For this indication, TE alonecannot be used sufficiently in detecting oesophageal var-ices or large oesophageal varices. In addition, the accu-racy of TE for detecting significant portal hypertension,oesophageal varices or large oesophageal varices was dif-ferent in the studies with the different population evalu-ated, different experience of operators. Therefore, theseresults were not robust. Nevertheless, taking intoaccount good performance of TE for diagnosis of liverfibrosis, significant fibrosis and cirrhosis, TE could be a
helpful tool for management patients with PHT inchronic liver diseases (33).
The above results, especially the significant portalhypertension detection using TE, have been consideredencouraging in individual studies and in some reviews.However, the major drawback was that the TE cut-offvalue was different across studies and has not been vali-dated either significant portal hypertension detection orpresence and size of oesophageal varices evaluation. Pool-ing such ‘optimal’ results from these studies might artifi-cially increase the summary sensitivity and specificity.Because of a scarcity of publications, we could notaddress these important issues. The efficacy of TE in thedetection of significant portal hypertension, oesophagealvarices, or large oesophageal varices should be furtherevaluated in more studies in the future. In this context,only a meta-analysis with individual data would allowto evaluate the diagnosis performance of relevant cut-off values. Furthermore, although TE showed the gooddiagnostic accuracy for the detection significant portalhypertension, the performances of some validated bio-markers were similar to that of TE in diagnosingoesophageal varices or large oesophageal varices (20,34). Some studies thus have shown that the inclusion ofTE in an algorithm with a combination of non-invasiveserum markers could further improve the diagnosticaccuracy, especially for the diagnosis of oesophageal var-ices or large oesophageal varices (23). Additional studiesare needed to be performed to verifying theses results.In addition, although TE inter-observer and intra-observer agreement has been shown to be excellent, itcan be easily influenced by limited operator experienceand characteristics of patient, such as obesity or narrowintercostal space. However, with the development oftechnology, the learning curve was not a real difficultyin some studies. XL probe or ARFI method can improve
(A) (B) (C)
Fig. 2. HSROC curve of the TE for evaluation of PHT. (A) TE detection for significant portal hypertension; (B) TE detection for oesophagealvarices; (C) TE detection for large oesophageal varices; The size of the dots for 1-specificity and sensitivity of the single studies in the ROCspace was derived from the respective sample size. HSROC for significant portal hypertension was 0.93, for oesophageal varices detectionwas 0.84, and for large oesophageal varices detection was 0.78. HSROC, hierarchical summary receiver operating characteristic; PHT, portalhypertension; TE, transient elastograpy.
Liver International (2013)© 2012 John Wiley & Sons A/S68
TE for portal hypertension Shi et al.
‘positive’ measurement. Furthermore, a ‘negative’ mea-surement was also informative, as significant portalhypertension was present in only 11% of patients. Inthis respect, TE is promising and worthy to translateinto clinical practice in detecting significant portalhypertension that it is a reliable and non-invasive proce-dure. Therefore, TE could be integrated in the detectionof significant portal hypertension in untreated patientsfor PHT. TE might also be useful to select suspiciouspatients with CLD for HVPG measurement. Neverthe-less, when the pre-test probability of significant portalhypertension was as low as 25%, the probability of cor-rectly identifying significant portal hypertensiondecreased markedly. This suggests that an accurate selec-tion of patients is necessary to exploit the performanceof TE at its best. In addition, in patients with significantportal hypertension, TE might be used in monitoringthe hemodynamic response and the effect of drugsreducing portal pressure.
Although the pooled sensitivities for both detectionof oesophageal varices and large oesophageal varicesexceeded 0.85, the pooled specificities were rather low,0.53 (95% CI, 0.36–0.69) for oesophageal varices detec-tion and 0.59 (95% CI, 0.45–0.72) for large oesophagealvarices detection. In addition, the PPV and NPV of TEin diagnosing oesophageal varices or large oesophagealvarices were really low. For this indication, TE alonecannot be used sufficiently in detecting oesophageal var-ices or large oesophageal varices. In addition, the accu-racy of TE for detecting significant portal hypertension,oesophageal varices or large oesophageal varices was dif-ferent in the studies with the different population evalu-ated, different experience of operators. Therefore, theseresults were not robust. Nevertheless, taking intoaccount good performance of TE for diagnosis of liverfibrosis, significant fibrosis and cirrhosis, TE could be a
helpful tool for management patients with PHT inchronic liver diseases (33).
The above results, especially the significant portalhypertension detection using TE, have been consideredencouraging in individual studies and in some reviews.However, the major drawback was that the TE cut-offvalue was different across studies and has not been vali-dated either significant portal hypertension detection orpresence and size of oesophageal varices evaluation. Pool-ing such ‘optimal’ results from these studies might artifi-cially increase the summary sensitivity and specificity.Because of a scarcity of publications, we could notaddress these important issues. The efficacy of TE in thedetection of significant portal hypertension, oesophagealvarices, or large oesophageal varices should be furtherevaluated in more studies in the future. In this context,only a meta-analysis with individual data would allowto evaluate the diagnosis performance of relevant cut-off values. Furthermore, although TE showed the gooddiagnostic accuracy for the detection significant portalhypertension, the performances of some validated bio-markers were similar to that of TE in diagnosingoesophageal varices or large oesophageal varices (20,34). Some studies thus have shown that the inclusion ofTE in an algorithm with a combination of non-invasiveserum markers could further improve the diagnosticaccuracy, especially for the diagnosis of oesophageal var-ices or large oesophageal varices (23). Additional studiesare needed to be performed to verifying theses results.In addition, although TE inter-observer and intra-observer agreement has been shown to be excellent, itcan be easily influenced by limited operator experienceand characteristics of patient, such as obesity or narrowintercostal space. However, with the development oftechnology, the learning curve was not a real difficultyin some studies. XL probe or ARFI method can improve
(A) (B) (C)
Fig. 2. HSROC curve of the TE for evaluation of PHT. (A) TE detection for significant portal hypertension; (B) TE detection for oesophagealvarices; (C) TE detection for large oesophageal varices; The size of the dots for 1-specificity and sensitivity of the single studies in the ROCspace was derived from the respective sample size. HSROC for significant portal hypertension was 0.93, for oesophageal varices detectionwas 0.84, and for large oesophageal varices detection was 0.78. HSROC, hierarchical summary receiver operating characteristic; PHT, portalhypertension; TE, transient elastograpy.
Liver International (2013)© 2012 John Wiley & Sons A/S68
TE for portal hypertension Shi et al.
‘positive’ measurement. Furthermore, a ‘negative’ mea-surement was also informative, as significant portalhypertension was present in only 11% of patients. Inthis respect, TE is promising and worthy to translateinto clinical practice in detecting significant portalhypertension that it is a reliable and non-invasive proce-dure. Therefore, TE could be integrated in the detectionof significant portal hypertension in untreated patientsfor PHT. TE might also be useful to select suspiciouspatients with CLD for HVPG measurement. Neverthe-less, when the pre-test probability of significant portalhypertension was as low as 25%, the probability of cor-rectly identifying significant portal hypertensiondecreased markedly. This suggests that an accurate selec-tion of patients is necessary to exploit the performanceof TE at its best. In addition, in patients with significantportal hypertension, TE might be used in monitoringthe hemodynamic response and the effect of drugsreducing portal pressure.
Although the pooled sensitivities for both detectionof oesophageal varices and large oesophageal varicesexceeded 0.85, the pooled specificities were rather low,0.53 (95% CI, 0.36–0.69) for oesophageal varices detec-tion and 0.59 (95% CI, 0.45–0.72) for large oesophagealvarices detection. In addition, the PPV and NPV of TEin diagnosing oesophageal varices or large oesophagealvarices were really low. For this indication, TE alonecannot be used sufficiently in detecting oesophageal var-ices or large oesophageal varices. In addition, the accu-racy of TE for detecting significant portal hypertension,oesophageal varices or large oesophageal varices was dif-ferent in the studies with the different population evalu-ated, different experience of operators. Therefore, theseresults were not robust. Nevertheless, taking intoaccount good performance of TE for diagnosis of liverfibrosis, significant fibrosis and cirrhosis, TE could be a
helpful tool for management patients with PHT inchronic liver diseases (33).
The above results, especially the significant portalhypertension detection using TE, have been consideredencouraging in individual studies and in some reviews.However, the major drawback was that the TE cut-offvalue was different across studies and has not been vali-dated either significant portal hypertension detection orpresence and size of oesophageal varices evaluation. Pool-ing such ‘optimal’ results from these studies might artifi-cially increase the summary sensitivity and specificity.Because of a scarcity of publications, we could notaddress these important issues. The efficacy of TE in thedetection of significant portal hypertension, oesophagealvarices, or large oesophageal varices should be furtherevaluated in more studies in the future. In this context,only a meta-analysis with individual data would allowto evaluate the diagnosis performance of relevant cut-off values. Furthermore, although TE showed the gooddiagnostic accuracy for the detection significant portalhypertension, the performances of some validated bio-markers were similar to that of TE in diagnosingoesophageal varices or large oesophageal varices (20,34). Some studies thus have shown that the inclusion ofTE in an algorithm with a combination of non-invasiveserum markers could further improve the diagnosticaccuracy, especially for the diagnosis of oesophageal var-ices or large oesophageal varices (23). Additional studiesare needed to be performed to verifying theses results.In addition, although TE inter-observer and intra-observer agreement has been shown to be excellent, itcan be easily influenced by limited operator experienceand characteristics of patient, such as obesity or narrowintercostal space. However, with the development oftechnology, the learning curve was not a real difficultyin some studies. XL probe or ARFI method can improve
(A) (B) (C)
Fig. 2. HSROC curve of the TE for evaluation of PHT. (A) TE detection for significant portal hypertension; (B) TE detection for oesophagealvarices; (C) TE detection for large oesophageal varices; The size of the dots for 1-specificity and sensitivity of the single studies in the ROCspace was derived from the respective sample size. HSROC for significant portal hypertension was 0.93, for oesophageal varices detectionwas 0.84, and for large oesophageal varices detection was 0.78. HSROC, hierarchical summary receiver operating characteristic; PHT, portalhypertension; TE, transient elastograpy.
Liver International (2013)© 2012 John Wiley & Sons A/S68
TE for portal hypertension Shi et al.
18 studies; N= 3644 patients
PTH OV LOV
AUC: 0.93 AUC: 0.84 AUC: 0.78

Résumé
◆ L’élasticité hépatique est bien corrélée avec le
gradient portal et la présence (taille?) des VO.
◆ Les performances de l’élastométrie et des
biomarqueurs sont cependant insuffisantes pour
remplacer la fibroscopie pour la recherche de
VO.

Liver stiffness Relationship with liver-related events
peritonitis (SBP), and hepatorenal syndrome (HRS). At the end ofthe follow-up period (March 2011), one patient had died due toHCC and another had undergone liver transplantation afterascitic decompensation.
Primary endpointThe primary endpoint was the development of LREs, including
hepatic decompensation (variceal bleeding, ascites, HE, SBP, andHRS) and HCC.
Definition of hepatic decompensationVariceal bleeding was diagnosed endoscopically if hemorrhage
from the dilated veins in the distal esophagus or proximal stomachcaused by elevated pressure in the portal venous system was noted[20]. Ascites was diagnosed by imaging, such as computedtomography (CT) or ultrasonography, if fluid collection withinthe abdominal cavity associated with cirrhosis was noted [21]. HEwas diagnosed if confusion, altered level of consciousness, andcoma developed as a result of liver failure, after the exclusion ofknown brain disease [22]. SBP was defined as an ascitic fluidinfection without an intra-abdominal, surgically treatable source[23]. Diagnosis was established by a positive ascitic fluid bacterialculture and an elevated ascitic fluid absolute polymorphonuclearleukocyte count ($250 cells/mm3). HRS was diagnosed whenacute renal failure developed in association with advanced chronicliver disease, after the exclusion of other causes of renal failure[24].
Diagnosis of HCCHCC was diagnosed based on the guidelines of the American
Association for the Study of Liver Diseases (AASLD) [25]. Briefly,patients were diagnosed with HCC if they had a tumor witha maximum diameter .2 cm, features typical of HCC ondynamic CT (hyperattenuation in the arterial phase and earlywashout in the portal phase), and AFP .200 ng/mL. If themaximum diameter of the tumor was 1–2 cm, dynamic CT andmagnetic resonance imaging were performed and HCC was
diagnosed if coincidental typical features of HCC were noted. Ifthe tumor did not satisfy the above criteria, a biopsy wasperformed. When the tumor was ,1 cm, ultrasonographicexamination was repeated after 3 months.
Statistical analysesData are expressed as the mean 6 standard deviation (SD),
median (range), or n (%), as appropriate. Baseline characteristics ofpatients with and without LRE development were compared usingthe chi-squared and Fisher’s exact tests. To identify independentpredictors of LRE development, univariate and subsequentmultivariate Cox proportional hazard regression analyses wereused. Hazard ratios (HRs) and corresponding 95% confidenceintervals (CIs) are indicated. Time-dependent receiver operatingcharacteristic (ROC) curves and areas under the ROC (AUROC)were used to calculate the optimal LSM cutoff value for theprediction of LRE development, which maximized the sum ofsensitivity and specificity. The annual incidence rates of HCCwere expressed in person-years. The cumulative incidence rates ofHCC were calculated using the Kaplan–Meier method. A Pvalue,0.05 on a two-tailed test was considered statisticallysignificant. Statistical analyses were performed using SPSSsoftware (ver. 18.0; SPSS Inc., Chicago, IL, USA).
Results
Baseline characteristicsThe baseline characteristics of 128 patients at enrollment are
summarized in Table 1. The mean age of the patients (72 menand 56 women) was 52.2 years. All patients with cirrhosis showedpreserved liver function of Child–Pugh class A. The mean bodymass index (BMI) and ALT were 24.0 kg/m2 and 44.4 IU/L,respectively, and the median LSM value was 12.9 kPa.F3 and F4 fibrosis stages were noted in 18 (14.1%) and 110
(85.9%) patients, respectively, and most patients (n=97, 75.8%)had a necroinflammatory activity grade of 1–2 (Table 1). S0–1steatosis was identified in 127 (99.2%) patients and S2 in one(0.8%), whereas none showed S3 steatosis.
LRE development and comparisons between patientswith and without LREsDuring the follow-up period [median, 27.8 (range, 12.6–61.6)
months] constituting a total of 297 person-years, LREs developedin 19 (14.8%) patients (6.4/100 person-years; five cases withdecompensation, 13 with HCC, and one with both decompensa-tion and HCC; Table 2). The six cases of hepatic decompensationincluded variceal bleeding in two patients, ascites development intwo, and HE in two. SBP and HRS did not develop during thefollow-up period. The cumulative incidence rates of LREs at 1, 2,and 3 years were 3.1%, 11.7%, and 16.2%, respectively(Figure 1). The incidence rate of HCC and hepatic decompen-sation was 4.7/100 and 2.0/100 person-years, respectively.When we compared the baseline characteristics of patients with
and without LRE development, serum albumin, prothrombintime, and platelet count were significantly higher in patientswithout LREs, whereas age, AFP, and LSM values weresignificantly higher among those with LRE development (allP,0.05; Table 2). No significant difference was observed in theproportion of fibrosis stage, activity grade, or steatosis betweenpatients with and without LRE development (all P.0.05;Table 2).
Figure 2. Cumulative incidence rates of LREs based onstratified LSM values (Kaplan-Meier plot). Patients with LSMvalue .19 kPa were at a significantly greater risk of LREs developmentwith a hazard ratio of 7.176 [95% confidence interval, 2.257–22.812;P= 0.001], as compared to those with LSM value #19 kPa. LSM, liverstiffness measurement; kPa, kilopascal. LRE, liver-related event.doi:10.1371/journal.pone.0036676.g002
Fibroscan for Predicting Liver-Related Events
PLoS ONE | www.plosone.org 4 May 2012 | Volume 7 | Issue 5 | e36676
Kim et al. PloSOne 2012; 7: e36676 N=128 HBV patientsF3-F4

Elasticité hépatique survie sans complications
Robic et al. J Hepatol 2011; 55: 1017-24 N=100 patients CLD
liver related complication were 32.2% and 84.1%, respectively(Log Rank p <0.001) (Fig. 2A).
The actuarial rates of remaining free of any complicationrelated to the liver disease were 29.5% and 85.4%, respectively,if LS was P21.1 kPa or <21.1 kPa (Log Rank p <0.001) (Fig. 2B).
Performance of LS and HVPG in predicting the risk of PHT relatedcomplications
The AUROC of HVPG and LS values in predicting PHT related com-plications were 0.830 [0.751–0.910] and 0.845 [0.767–0.923](Fig. 3A). When considering only cirrhotic patients, HVPGand LS had similar performances, AUROC values being 0.725[0.602–0.849] and 0.734 [0.609–0.859], respectively. (Fig. 3B).
According to the presence or the absence of significant PHT(HVPG P10 mmHg), the actuarial rates of remaining free ofPHT complications were 51.3% and 100%, respectively (Log Rankp <0.001) (Fig. 4A). In fact, none of the patients with aHVPG <10 mmHg developed PHT related complications. In thesubgroup of cirrhotic patients, the HVPG with a 10 mmHg thresh-old had a sensitivity of 100%, a specificity of 36.1%, a PPV of 37.5%,and a NPV of 100%. In this subgroup, the actuarial rates ofremaining free of PHT complications with a HVPG P10 mmHgor <10 mmHg were 47.8% and 100%, respectively.
When LS value was P21.1 kPa or <21.1 kPa, the actuarial ratesof remaining free of PHT related complications were 47.5% and100%, respectively (Log Rank p <0.001) (Fig. 4B). No patient witha LS value <21.1 kPa experienced PHT related complications. Forthe subgroup of patients with cirrhosis, LS with a 21.1 kPa cutoffhad a 100% sensitivity, 41% specificity, 41% PPV, and 100% NPV.The actuarial rates of remaining free of PHT complications withLS P21.1 kPa or <21.1 kPa were 47% and 100%, respectively.
Discussion
The present study shows a strong relationship between LS andthe risk of decompensation in patients with chronic liver disease,regardless of the presence of cirrhosis.
To the best of our knowledge this is the first study that pro-spectively assessed the performance of LS for predicting clinicalcomplications and that compared it with HVPG measurement.HVPG is a well established index in different clinical settingsfor patients with cirrhosis [2,3]. However, the only availablemethod to assess HVPG is a direct measurement of pressure ina hepatic vein. This method is not available in all medical centersand is considered invasive, cost-ineffective, and hardly reproduc-ible by most authors [18]. Until now, most non-invasiveapproaches for assessing short-term prognosis in patients withchronic liver disease have proved inaccurate. The need for pro-spective longitudinal studies to assess new non-invasive proce-dures was recommended at the Baveno IV ConsensusConference [19].
Foucher et al. have previously found a correlation between LSand severity of cirrhosis [20]. However, in this study, PHT compli-cations were retrospectively assessed as a history of ascites or
0.0
0.2
0.4
0.6
0.8
1.0
0.8 1.00.60.40.20
Sens
itivi
ty
1-specificity
Liver stiffnessAUROC: 0.837 (0.754-0.920)
HVPGAUROC: 0.815 (0.727-0.903)
Fig. 1. Performance of liver stiffness and HVPG for the prediction of liverrelated complications.
0.0
0.2
0.4
0.6
0.8
1.0
Surv
ival
free
of
any
com
plic
atio
ns
Days
HVPG <10 mmHg
HVPG ≥10 mmHg
0.0
0.2
0.4
0.6
0.8
1.0
0 200 400 600 800
0 200 400 600 800
Surv
ival
free
of
any
com
plic
atio
ns
Days
LS <21.1 kPa
LS ≥21.1 kPa
A
B
Fig. 2. Risk of liver related complications according to HVPG or liver stiffness.(A) Probability of remaining free of liver related complications according to the10 mmHg-threshold for HVPG. (B) Probability of remaining free of liver relatedcomplications according to the 21.1 kPa-threshold for liver stiffness.
JOURNAL OF HEPATOLOGY
Journal of Hepatology 2011 vol. 55 j 1017–1024 1021

Elasticité hépatique & survie
Vergniol et al. Gastroenterology 2011;
4.00*FibroTest ! 1.12* LSM in 3 classes (0: LSM ! 7, 1: 7" LSM ! 12.5, 2: LSM # 12.5) $1.68*treatment in 3classes (0: no treatment, 1: nonresponder, 2: sustained viro-logical response). In the core group the corresponding prog-nostic AUROC for survival was 0.907 (95% CI: 0.825–0.952;P " .0001). In the whole group, the corresponding prog-nostic AUROC for survival was 0.888 (95% CI: 0.843–0.921;P " .0001).
As obesity has been recognized as an independent predic-tor of prognosis in chronic liver disease, in a sensitivityanalysis we added body mass index as another possibleprognostic factor in model 5; there was not significantprognostic value (hazard ratio % 0.98; 95% CI: 0.92–1.04).
As HIV infection has been recognized as an independentpredictor of prognosis in chronic liver disease, in a sensitiv-ity analysis we added HIV infection as another possible
Figure 2. Overall survival probability according to liver stiffness, biomarkers, and liver biopsy. (A) Overall survival according to published cut-offs forthe diagnosis of severe fibrosis or cirrhosis. (B) Overall survival according to different cut-offs of liver stiffness (kPa). Overall survival (95% confidenceinterval) using liver stiffness: !9.5 kPa: 96% (94%–98%); #9.5 kPa: 77% (72%–82%); #20 kPa: 66% (61%–71%); #30 kPa: 57% (50%–64%); #40kPa: 47% (37%–57%); #50 kPa: 42% (29%–55%). (C) Overall survival according to different cut-offs of FibroTest. Overall survival (95% confidenceinterval) using FibroTest: !0.75: 97% (96%–98%); #0.75 and !0.80: 87% (78%–95%); #0.80 and !0.85: 84% (75%–94%); #0.85 and !0.90:75% (61%–90%); #0.90 and !0.95: 69% (54%–84%); #0.95 to 1: 0% (0%–22%).
CLIN
ICA
L–LIVER
,PA
NCREA
S,A
ND
BILIA
RY
TRA
CT
1976 VERGNIOL ET AL GASTROENTEROLOGY Vol. 140, No. 7
4.00*FibroTest ! 1.12* LSM in 3 classes (0: LSM ! 7, 1: 7" LSM ! 12.5, 2: LSM # 12.5) $1.68*treatment in 3classes (0: no treatment, 1: nonresponder, 2: sustained viro-logical response). In the core group the corresponding prog-nostic AUROC for survival was 0.907 (95% CI: 0.825–0.952;P " .0001). In the whole group, the corresponding prog-nostic AUROC for survival was 0.888 (95% CI: 0.843–0.921;P " .0001).
As obesity has been recognized as an independent predic-tor of prognosis in chronic liver disease, in a sensitivityanalysis we added body mass index as another possibleprognostic factor in model 5; there was not significantprognostic value (hazard ratio % 0.98; 95% CI: 0.92–1.04).
As HIV infection has been recognized as an independentpredictor of prognosis in chronic liver disease, in a sensitiv-ity analysis we added HIV infection as another possible
Figure 2. Overall survival probability according to liver stiffness, biomarkers, and liver biopsy. (A) Overall survival according to published cut-offs forthe diagnosis of severe fibrosis or cirrhosis. (B) Overall survival according to different cut-offs of liver stiffness (kPa). Overall survival (95% confidenceinterval) using liver stiffness: !9.5 kPa: 96% (94%–98%); #9.5 kPa: 77% (72%–82%); #20 kPa: 66% (61%–71%); #30 kPa: 57% (50%–64%); #40kPa: 47% (37%–57%); #50 kPa: 42% (29%–55%). (C) Overall survival according to different cut-offs of FibroTest. Overall survival (95% confidenceinterval) using FibroTest: !0.75: 97% (96%–98%); #0.75 and !0.80: 87% (78%–95%); #0.80 and !0.85: 84% (75%–94%); #0.85 and !0.90:75% (61%–90%); #0.90 and !0.95: 69% (54%–84%); #0.95 to 1: 0% (0%–22%).
CLIN
ICA
L–LIVER
,PA
NCREA
S,A
ND
BILIA
RY
TRA
CT
1976 VERGNIOL ET AL GASTROENTEROLOGY Vol. 140, No. 7
N=1457 patients VHC

Elasticité hépatique & survie
Corpechot et al. Gastroenterology 2014; N=168 patients CSP

Elasticité hépatique & survie
Corpechot et al. Gastroenterology 2014; N=168 patients CSP

◆ Principe & limites
◆ Performances diagnostiques
◆ Comparaison avec les biomarqueurs
◆ Suivi de la progression de la fibrose
◆ Nouvelles techniques
Plan

Friedrich-Rust et al. Radiology 2009 ; 252: 595-604
Challengers for measuring liver stiffness ARFI (VirtualTouch®))
Nightingale et al. UMB 2002 ; 28: 227-35

Challenger for measuring liver stiffness Supersonic shear Imaging (Aixplorer®)
Muller et al. UMB 2009; 35: 219-29
Bavu et al. UMB 2011;37: 1361-73
Contrary to FS, as vibration induced by the radiationforce creates a short transient excitation, the frequencybandwidth of the generated shear wave is large, typicallyranging from 60 to 600 Hz (Fig. 3). Such wideband‘‘shear wave spectroscopy’’ can give a refined analysisof the complex mechanical behavior of tissue. As shownin Figure 3, the shear wave dispersion law can be assessedfrom displacement movies in the region-of-interest.
Thus, the global elasticity imaged by SSI makes useof higher frequency content and is also influenced by thedispersive properties of the liver tissues because it aver-ages the full mechanical response of the liver tissuesover a large bandwidth. In parallel, SWS providesa refined analysis in a larger box of these dispersive prop-erties of tissues by estimating frequency dependence ofthe shear wave speed.
Statistical methodsThe diagnosis performance of FS and SSI are
compared by using receiver operating characteristic(ROC) curves and box-and-whisker curves on the samecohort. A patient was assessed as positive or negative ac-cording to whether the noninvasive marker value wasgreater than or less than to a given cutoff value, respec-tively. Connected with any cutoff value is the probabilityof a true positive (sensitivity) and the probability of a truenegative (specificity). The ROC curve is a plot ofsensitivity vs. (1-specificity) for all possible cutoff values.The most commonly used index of accuracy is the areaunder the ROC curve (AUROC), with values close to1.0 indicating high diagnosis accuracy. Optimal cutoffvalues for liver stiffness were chosen to maximize thesum of sensitivity and specificity and positive and nega-tive predictive values were computed for these cutoffvalues. By using these cutoff values, the agreementbetween FS and SSI was evaluated. Statistical analyseswere performed with Matlab R2007a software (Math-works, Natick, MA, USA) using the statistical analysistoolbox and Medcalc software (Mariakerke, Belgium).
RESULTS
Liver stiffness mapping using SSIThe Young’s modulus corresponding to the stiffness
of the liver tissues are presented for 4 patients in Figure 4.The elasticity mapping is superimposed with the corre-sponding B-mode images on which the fat and muscleregion are well differentiated from the liver region andthe elasticity is mapped only in the liver region.Figure 4a, b, c and d show the elasticity mapping forpatients who have been classified as predicted fibrosislevels F1, F2, F3 and F4, respectively.
The median elasticity derived from these maps areequal to 4.786 0.83 kPa for the patient with F1, 10.646
Fig. 4. Bidimensional liver elasticity maps assessed using thesupersonic shear imaging (SSI) technique superimposed tothe corresponding B-scan. The Young’s modulus representingthe liver stiffness is represented in color levels. (a): patient59 - F1. E5 4.786 0.83 kPa (b): patient 51 - F2. E5 10.6461.10 kPa (c): patient 39 - F3. E5 14.526 2.20 kPa (d): patient
22 - F4. E 5 27.43 6 2.64 kPa.
1366 Ultrasound in Medicine and Biology Volume 37, Number 9, 2011
Contrary to FS, as vibration induced by the radiationforce creates a short transient excitation, the frequencybandwidth of the generated shear wave is large, typicallyranging from 60 to 600 Hz (Fig. 3). Such wideband‘‘shear wave spectroscopy’’ can give a refined analysisof the complex mechanical behavior of tissue. As shownin Figure 3, the shear wave dispersion law can be assessedfrom displacement movies in the region-of-interest.
Thus, the global elasticity imaged by SSI makes useof higher frequency content and is also influenced by thedispersive properties of the liver tissues because it aver-ages the full mechanical response of the liver tissuesover a large bandwidth. In parallel, SWS providesa refined analysis in a larger box of these dispersive prop-erties of tissues by estimating frequency dependence ofthe shear wave speed.
Statistical methodsThe diagnosis performance of FS and SSI are
compared by using receiver operating characteristic(ROC) curves and box-and-whisker curves on the samecohort. A patient was assessed as positive or negative ac-cording to whether the noninvasive marker value wasgreater than or less than to a given cutoff value, respec-tively. Connected with any cutoff value is the probabilityof a true positive (sensitivity) and the probability of a truenegative (specificity). The ROC curve is a plot ofsensitivity vs. (1-specificity) for all possible cutoff values.The most commonly used index of accuracy is the areaunder the ROC curve (AUROC), with values close to1.0 indicating high diagnosis accuracy. Optimal cutoffvalues for liver stiffness were chosen to maximize thesum of sensitivity and specificity and positive and nega-tive predictive values were computed for these cutoffvalues. By using these cutoff values, the agreementbetween FS and SSI was evaluated. Statistical analyseswere performed with Matlab R2007a software (Math-works, Natick, MA, USA) using the statistical analysistoolbox and Medcalc software (Mariakerke, Belgium).
RESULTS
Liver stiffness mapping using SSIThe Young’s modulus corresponding to the stiffness
of the liver tissues are presented for 4 patients in Figure 4.The elasticity mapping is superimposed with the corre-sponding B-mode images on which the fat and muscleregion are well differentiated from the liver region andthe elasticity is mapped only in the liver region.Figure 4a, b, c and d show the elasticity mapping forpatients who have been classified as predicted fibrosislevels F1, F2, F3 and F4, respectively.
The median elasticity derived from these maps areequal to 4.786 0.83 kPa for the patient with F1, 10.646
Fig. 4. Bidimensional liver elasticity maps assessed using thesupersonic shear imaging (SSI) technique superimposed tothe corresponding B-scan. The Young’s modulus representingthe liver stiffness is represented in color levels. (a): patient59 - F1. E5 4.786 0.83 kPa (b): patient 51 - F2. E5 10.6461.10 kPa (c): patient 39 - F3. E5 14.526 2.20 kPa (d): patient
22 - F4. E 5 27.43 6 2.64 kPa.
1366 Ultrasound in Medicine and Biology Volume 37, Number 9, 2011

Supersonic shear Imaging (Aixplorer®) Comparison with TE and ARFI in CLD
Cassinoto et al. J Hepatol 2014; in press N= 349 patients with CLD
27
Table 3: Areas under the receiver operating characteristic curve (with 95% confidence
interval) for the diagnostic accuracy of SSI, Fibroscan, ARFI, and serum fibrosis
biological markers for the diagnosis of histologic fibrosis stage.
A direct “head-to-head” comparison between the AUROCs of the 3 impulse
elastographic tests and those of the Fibrotest and FIB-4 are presented in supplementary
data 3.
n=349 ≥F1 ≥F2 ≥F3 F4
SSI 0.89 (0.84-0.92)
0.89 (0.84-0.92)
0.92 (0.89-0.95)
0.92 (0.89-0.95)
Fibroscan 0.84 (0.77-0.89)
0.83 (0.78-0.87)
0.86 (0.81-0.89)
0.90 (0.86-0.93)
ARFI 0.81 (0.73-0.87)
0.81 (0.75-0.85)
0.85 (0.80-0.89)
0.84 (0.79-0.88)
Fibrotest 0.79 (0.71-0.85)
0.74 (0.68-0.79)
0.78 (0.73-0.83)
0.81 (0.75-0.85)
FIB-4 0.77 (0.70-0.83)
0.75 (0.70-0.80)
0.77 (0.72-0.82)
0.82 (0.76-0.86)
APRI 0.73 (0.66-0.79)
0.71 (0.65-0.77)
0.72 (0.66-0.77)
0.74 (0.67-0.80)
Forns index 0.71 (0.61-0.78)
0.70 (0.63-0.75)
0.75 (0.69-0.80)
0.78 (0.71-0.83)
AST/ALT 0.58 (0.49-0.65)
0.61 (0.55-0.67)
0.67 (0.60-0.72)
0.74 (0.67-0.79)

Challengers for measuring liver stiffness Advantages & disavantages
• Can be implemented on a regular US machine
• High applicability • Performance close to TE
• Advantages ARFI
• Disadvantages • Further validation needed • Narrow range of values • Quality criteria not defined
• Can be implemented on a regular US machine • High range of value (2-150 kPa) • Performance higher than TE ?
• Advantages SWE
• Disadvantages • Further validation needed • Quality criteria? • Limited data on reproducibility
Berzigotti & Castera. J Hepatol 2013; 59: 180-2