-
Etude des canaux ioniques: intrts pour la physiopathologie et le
traitement des troubles de la motricit
Cours international: mdecine gnomique, du diagnostic la thrapie
17-21 octobre 2016-Institut Pasteur de Tunis
Arnaud Monteil
[email protected]
-
Ion channels
- Ion channels are gated pores that permit the passive flow of
ions down their electrochemical gradients.
- More than 400 genes are known that encode ion channel
subunits. - Alternative splicing and heteromeric assembly of
different subunits increase the diversity of ion
channels. - Such many channels are needed to accomplish very
complex cellular functions. - Dysfunction of ion channels are key
events in many pathological processes. - Ion channels are target of
importance in a pathological context.
-
Ion channel classes
Ashcroft, 2006
-
Some examples of currents
Piezo2 (mechano-gated) Nav1.3 (voltage-gated)
nAChR (Ligand-gated, direct) NALCN (Ligand-gated through
GPCRs)
-
3D models depicting VGNCs in 3 different states
Kim, 2014
-
Introduction
-
Introduction
-
Skeletal muscle channelopathies
1- Mutations in AchR subunits causes myasthenia (muscle
weakness) by preventing binding of acetylcholine. 2- Loss of
presynaptic K+-channel function (KV1.1, KCNA1) leads to increased
transmitter release and enhanced muscle contraction. 3-
Downregulation of presynaptic Ca2+ channels causes myasthenia by
preventing neurotransmitter release. 4- Gain-of-function mutations
in the muscle Na+ channel (Nav1.4, SCN4A) cause hyperexcitability
and myotonia. 5- Loss-of-function mutations in ClC channels cause
hyperexcitability and myotonia. 6- Loss-of- function mutations in
Kir1.1 cause hyperexcitability and myotonia. 7- Mutations in muscle
CaV channels (Cav1.1, CACNA1S) impair Ca
2+ release from intracellular stores, producing malignant
hyperthermia or paralysis. 8- RYR channels impair Ca2+ release from
intracellular stores, producing malignant hyperthermia or
paralysis.
Ashcroft, 2006
-
Skeletal muscle channelopathies
-
Kim, 2014
Skeletal muscle channelopathies
Cannon, 2015
-
Recurrent episodes of weakness, lasting minutes to hours, with
spontaneous full recovery.
Provocation of attacks by environmental stresses: - Rest after a
period of vigorous exercise.
- Carbohydrate-rich meals.
- Shifts of serum potassium (high or low).
- Exposure to cold.
- Emotional stress.
- Pregnancy.
Over times, some patients develop a slowly permanent
weakness.
Periodic Paralysis
-
The transient loss of muscle excitability during an attack of
weakness is caused by depolarization of the resting membrane
potential.
Three different mechanisms have been identified. - A persistent
Na+ caused by a defect of inactivation (1-2% remains open), other
defects in
gain-of-function mutants (gating, inactivation, hyperpolarized
shift of activation).
- Loss-of-function changes for inward rectifier potassium
channels (Kir2.1, Kir2.6, Kir3.4).
- Gating pore current.
Periodic Paralysis
Rudel et al, 1984
-
Hypokalemic Periodic Paralysis (CACNA1S, SCN4A)
-
Hyperkalemic Periodic Paralysis (SCN4A)
-
Hyperkalemic Periodic Paralysis (SCN4A)
-
Hyperkalemic Periodic Paralysis (SCN4A)
-
Therapeutic management of periodic paralysis
Acetazolamide is beneficial for about 50% of HypoPP patients
with Cav1.1 but not Nav1.4 mutations.
K+-supplements (HypoPP).
Avoidance of large carbohydrate-rich meals (HypoPP).
KATP openers (cromakalin; HypoPP).
Na+-K+-Cl- co-transporter (NKCC) inhibitor (bumetanide;
HypoPP).
Avoidance of K+-rich food (Nav1.4 - HyperPP).
Carbohydrate snack to truncate an episode (Nav1.4 -
HyperPP).
Promote kaliuresis with diuretics (Nav1.4 - HyperPP).
Carbonic anhydrase inhibitors (acetazolamide, dichlorphenamide;
Nav1.4 - HyperPP).
-
Inability of muscle to relax after voluntary effort.
The after-contractions may persist for many seconds.
With repeated movements, the intensity of myotonia diminishes
over seconds to minutes and may even become asymptomatic.
Conversely, some affected individuals have paradoxical worsening
of myotonic stiffness with repeated effort (paramyotonia). This
process is aggravated by muscle cooling.
Additional triggers have been associated with worsering
myotonia: - Potassium administration.
- Emotional stress.
- Pregnancy.
- Hypothyroidism.
- Depolarizing general anesthetics.
- Cold exposure.
Myotonia
-
Myotonia
Two different mechanisms have been identified: - Reduction of
the resting chloride conductance.
- Gain-of-function changes to the voltage-dependent gating of
Nav1.4 sodium channels.
-
Myotonia congenita (CLCN-1)
- Divided into dominant (Thomsen disease) and recessive (Becker
disease) forms. - Over 200 mutations in the CLCN1 gene have been
reported.
some cases can be total, a direct treatment tar-geted to the
CLC-1 protein is practically impos-sible. T heoretically, direct
treatment could bepossible if the function is only partially
reducedas in the case of dominant myotonia or in thecase of
mutations that have residual function as,e.g., the M485V mutation
that reduces thesingle-channel conductance [Wollnik et al.,1997]. A
drug that increases the open probabil-ity could then increase the
Cl conductance ofthe skeletal muscle and abolish the
hyperexcit-ability. T he pharmacological agents that inter-fere
most strongly with CLC-1 are 9-anthracenecarboxylic acid (9AC) and
the S() enantiomerof p-chloro-phenoxy-propionic acid (CPP), bothof
which inhibit the muscle Cl conductance andCLC-1with an apparent
affinity in the 10-50 mMrange [Palade and Barchi, 1977; De Luca et
al.,1992; Steinmeyer et al., 1991b; Aromataris etal., 1999; Pusch
et al., 2000]. CPP and also 9ACare most likely open channel
blockers that, inaddition, reduce the open probability by
imped-
ing channel opening of closed, drug-bound chan-nels [Pusch et
al., 2001; Accardi and Pusch, un-published observations]. These
substances aretherefore not suited to increase CLC-1
mutantactivity.
A pharmacological treatment could also beaimed at increasing
non-specifically the Cl con-ductance of muscle. No useful drug with
thatproperty is, however, known so far.
In practice, many patients manage the situa-tion without any
medication. If treatment is nec-essary, in general the muscle
fibers are renderedless excitable by partially inhibiting the
voltage-gated Na+ channel with local anesthetics suchas mexiletine
or related drugs [Lehmann-Hornand Jurkat-Rott, 1999].
Dominant and recessive myotonia are causedby mutations of the
same gene coding for themuscle Cl channel, CLC-1. T he
mechanismbehind the different modes of inheritance of
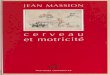
FIGURE 2. Localization of missense mutations. The approximate
position of recessive (blue squares), dominant (redcircles),
semi-dominant (red-blue hexagons), and sporadic (green squares)
mutations is shown in a topology model of theprimary protein
sequence. The length of the various segments is approximately to
scale. The topology was chosen ac-cording to Schmidt-Rose and
Jentsch [1997].
Pusch, 2002
-
Popponen et al, 2008
Myotonia congenita (recessive mutations of CLCN-1)
Kubisch et al, 1998
-
Myotonia congenita (dominant mutations of CLCN-1)
Kubisch et al, 1998
-
Myotonia congenita (SCN4A)
-
Paramyotonia congenita (SCN4A)
-
Avoidance of cold environments.
Voltage-gated sodium channels blockers (tocainimide, mexitetine,
flecainimide).
Acetazolamide (carbonic anhydrase inhibitor)?
Therapeutic management of Myotonia congenita
-
Disease ChannelProtein Gene
Cognitive impairment with orwithoutcerebellarataxia
Nav1.6: sodium channel, voltage-gated, type VIII, subunit
SCN8A
Episodicataxiatype1
Kv1.1:potassiumchannel,voltage-gated,shaker-relatedsubfamily,member1
KCNA1
Episodicataxiatype2
Cav2.1:calciumchannel,voltage-gated,P/Qtype,1Asubunit
CACNA1A
Episodicataxiatype5 Cav4:calciumchannel,voltage-gated,4subunit
CACNB4
Spinocerebellarataxiatype6
Cav2.1:calciumchannel,voltage-gated,P/Qtype,1Asubunit
CACNA1A
Spinocerebellarataxiatype13
Kv3.3: potassium channel, voltage-gated,
Shaw-relatedsubfamily,member3
KCNC3
Autosomal-Dominant CerebellarAtaxia
Cav3.1: calcium channel, voltage-gated, T type, 1Gsubunit
CACNA1G
CLIFAHDDsyndrome(dominant) NALCN:sodiumchannel,leak,subunit
NALCN
Infantile hypotonia withpsychomotor retardation and
characteristic facies (IHPRF,recessive)
NALCN:sodiumchannel,leak,subunit NALCN
Channelopathies-related ataxia
-
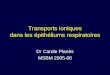
Snutch & Monteil, Neuron. 2007 May 24;54(4):505-7.
Cladogram of Subunits for the 4-Domain Ion Channel Family
- Central Nervous System - Heart - Adrenal Gland - Thyroid Gland
- Salivary Gland - Mammary Gland - Islets of Langerhans
-
Dominant-Negative Effects of Misfolded Mutants of VGCC
Mezghrani et al, 2008
-
NALCN regulates the neuronal resting membrane potential
Hippocampal neurons M. musculus
(Lu et al, 2007, Cell)
RPeD1 neurons L. stagnalis
(Lu et al, 2011, Plos ONE)
Premotor interneurons C. elegans
(Xie et al, 2013, Neuron)
Retrotrapezoid nucleus neurons M. musculus
(Shi et al, 2016, J. Neurosci.)
C4 nerve root recordings from brain stem spinal cord M.
musculus
(Lu et al, 2007, Cell)
-
Congenital contractures of limbs and face, hypotonia and
developmental delay (Chong et al, 2015, Am J Hum Genet; Aoyagi et
al, 2015, Hum Mutat; Wang et al, 2016, Clin Genet; Fukai et al,
2016, J Hum Genet; Karakaya et al, 2016, Neuropediatrics; Sivaraman
et al, 2016, J Clin Neurosci; Bend et al, 2016, Neurology)
Infantile neuroaxonal dystrophy (Kroglu et al, 2013, J Med
Genet)
Infantile hypotonia with psychomotor retardation and
characteristic facies (Al-Sayed et al, 2013, Am J Hum Genet ; Gal
et al, 2016, Eur J Med Genet)
NALCN in human diseases
-
Dominant-negative effect of NALCN mutations (CLIFFAHDD)
Chong et al, 2015
-
Aoyagi et al, 2015
An animal model for the CLIFFAHDD syndrome
-
Correction of NALCN deficiency by acting on other channels
Kasap et al, 2016
-
Correction of NALCN deficiency by acting on other channels
(4-AP: inhibitor of voltage-gated K+ channels)
-
Correction of NALCN deficiency by acting on other channels
(Quinine: inhibitor of voltage-gated K+ channels)
-
Correction of NALCN deficiency by acting on other channels
-
Correction of NALCN deficiency by acting on other channels
(FPL-64176: activator of voltage-gated Ca2+ channels)
-
Correction of NALCN deficiency by acting on other channels
(CBNX: activator of Gap Junctions)
-
Correction of NALCN deficiency by acting on other channels
(MFQ: activator of Gap Junctions)
-
Akinsie: L'akinsie est une lenteur d'initiation des mouvements
avec une tendance l'immobilit (mouvements volontaires, mouvements
associs, mouvements d'ajustement postural, mouvements d'expression
gestuelle et motionnelle), et ce, en l'absence de paralysie. Cela
est d un problme d'activation de zones du cerveau (atteinte de la
voie nigro-strie entranant un dficit en dopamine).
Dyskinsie: la dyskinsie activit motrice involontaire, lente et
strotype affectant prfrentiellement la face (langue, lvres,
mchoire) stendant au tronc et aux membres.
Dysplasie: Une dysplasie est une malformation ou dformation
rsultant d'une anomalie du dveloppement d'un tissu ou d'un organe,
qui survient au cours de la priode embryonnaire ou aprs la
naissance.
Myotonie: une myotonie se caractrise par une dcontraction lente
et difficile d'un muscle la suite d'une contraction volontaire.
Paralysie priodique: Les paralysies priodiques sont un groupe de
maladies gntiques rares qui conduisent une faiblesse musculaire ou
une paralysie (rarement la mort) partir de facteurs dclenchant
courants tels que le froid, la chaleur, des repas riches en
glucides, le jene, le stress, l'excitation et l'activit physique de
toute nature.
Ataxie: l'ataxie est une pathologie neuromusculaire qui consiste
en un manque de coordination fine des mouvements volontaires. Elle
n'est pas lie une dficience physique des muscles mais plutt une
atteinte du systme nerveux. Le trouble de la coordination est
partiellement corrig par le contrle visuel.
Dfinitions