Embed Size (px)
Citation preview

16 janv. 2009
LiverCenter
VHC
Traitement des cas simples
Traitement des cas compliqués
Thierry Poynard
Vlad Ratziu, Yves Benhamou
16 janv. 2009
LiverCenter
Treatment of Acute Hepatitis C:
A la carte from 0 to 1 year
16 janv. 2009
The Definition of Acute Hepatitis C
• Exposure to HCV
• Within 4 months
• Anti-HCV seroconversion
• Raised ALTs
• HCVRNA positivity
3
16 janv. 2009
Rationale for Treating Acute HCV
• High risk of chronicity
• Risk of spreading the virus
• Chances for better cure (no fibrosis, recovery of immune response)
4
16 janv. 2009
Anti-Viral Treatment of Acute HCV
• Randomized controlled trials
• Meta-analysis
• Uncontrolled trials
5
16 janv. 2009
RCTs of IFN! in Acute HCV
• VILLADOMIU n=28 ! ! Hepatology ! 1992 ! !
• LI n=32 ! ! ! China J Int Med 1993! !
• LAMPERTICO n=48 ! Hepatology ! 1994 !!
• HWANG n=23 ! ! J Hepatol ! 1994 !!
4 trials; n=141
All patients transfused
Age 51yrs, 62% males
All IFN !-2b alone
12 weeks of treatment
9-15 months fw-up
6
16 janv. 2009
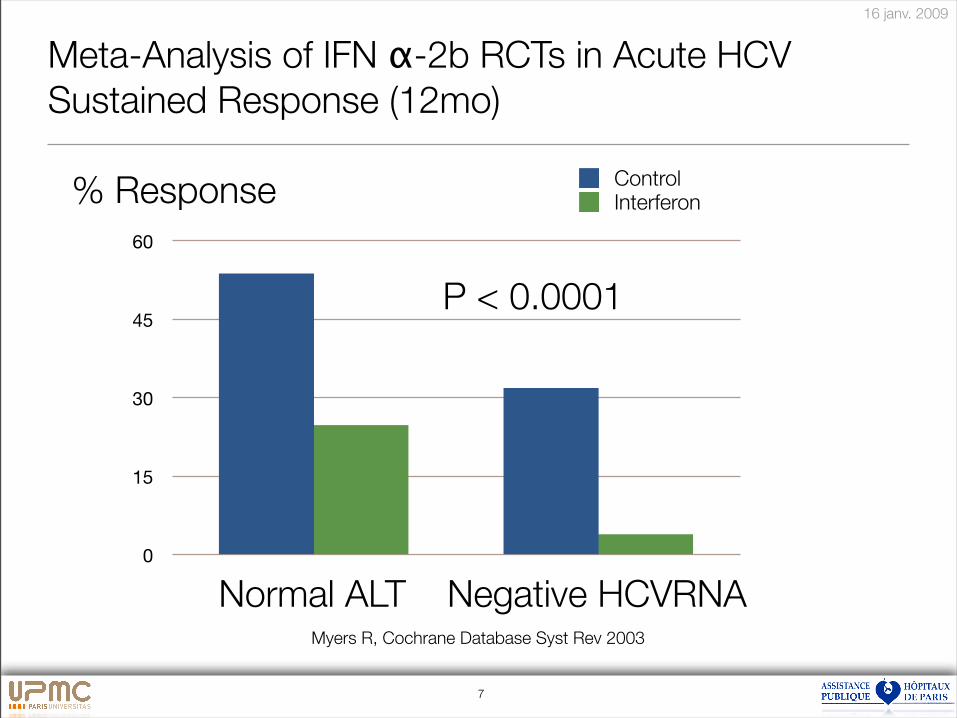
Meta-Analysis of IFN !-2b RCTs in Acute HCV
Sustained Response (12mo)
0
15
30
45
60
P < 0.0001
Myers R, Cochrane Database Syst Rev 2003
Normal ALT Negative HCVRNA
% Response ControlInterferon
7
16 janv. 2009
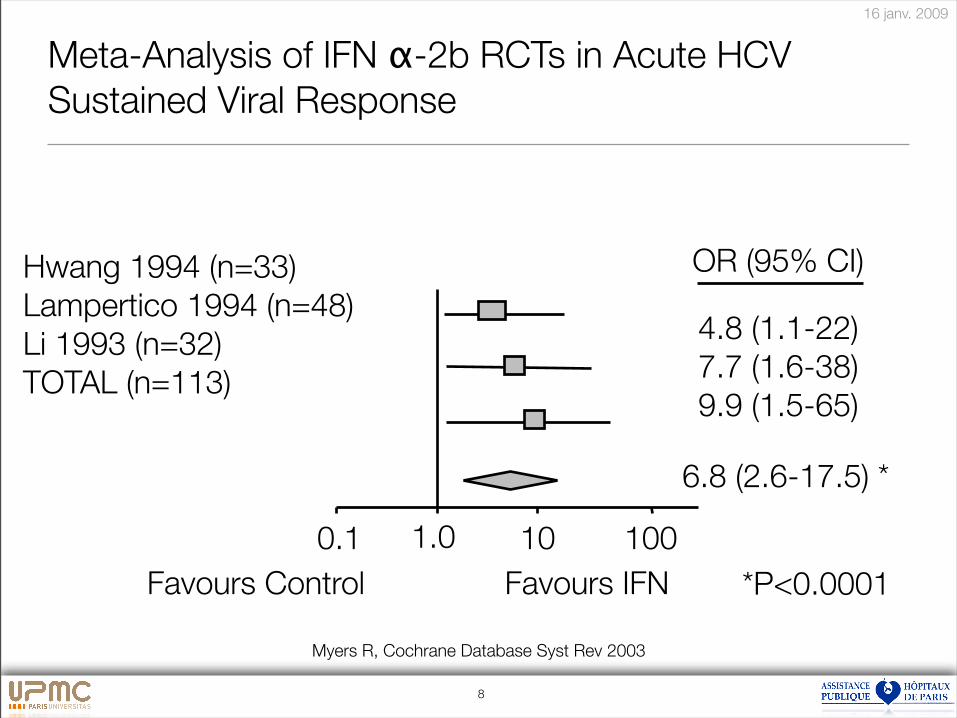
Meta-Analysis of IFN !-2b RCTs in Acute HCV
Sustained Viral Response
Myers R, Cochrane Database Syst Rev 2003
*P<0.0001
Hwang 1994 (n=33)
Lampertico 1994 (n=48)
Li 1993 (n=32)
TOTAL (n=113)
1.0 100100.1
4.8 (1.1-22)
7.7 (1.6-38)
9.9 (1.5-65)
6.8 (2.6-17.5) *
Favours IFNFavours Control
OR (95% CI)
8
16 janv. 2009
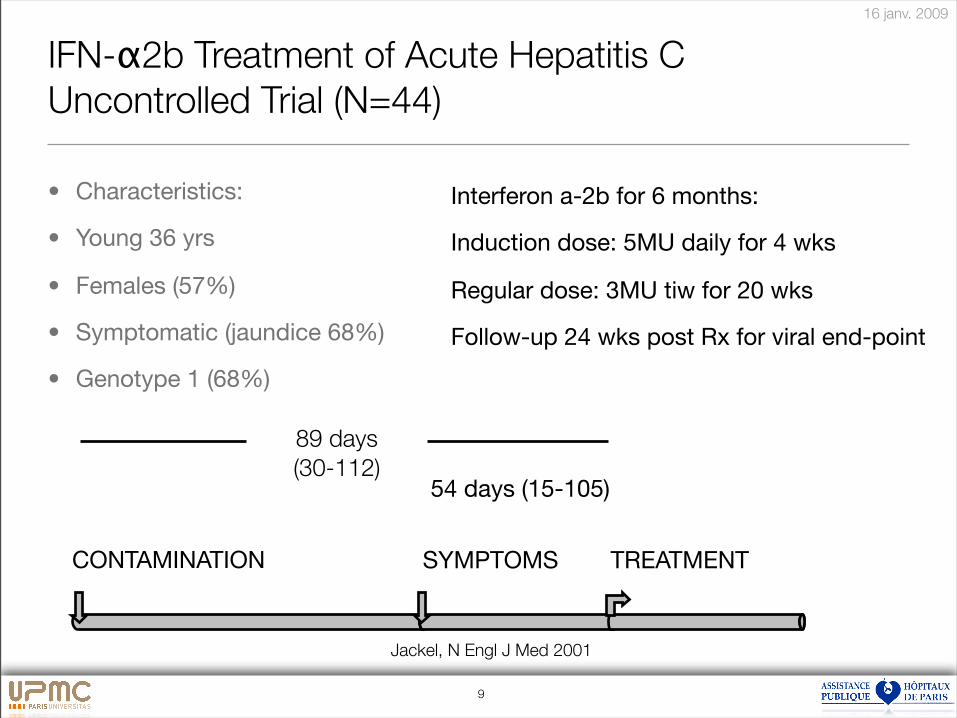
IFN-!2b Treatment of Acute Hepatitis C
Uncontrolled Trial (N=44)
• Characteristics:
• Young 36 yrs
• Females (57%)
• Symptomatic (jaundice 68%)
• Genotype 1 (68%)
Interferon a-2b for 6 months:
Induction dose: 5MU daily for 4 wks
Regular dose: 3MU tiw for 20 wks
Follow-up 24 wks post Rx for viral end-point
CONTAMINATION SYMPTOMS TREATMENT
54 days (15-105)
89 days
(30-112)
Jackel, N Engl J Med 2001
9
16 janv. 2009
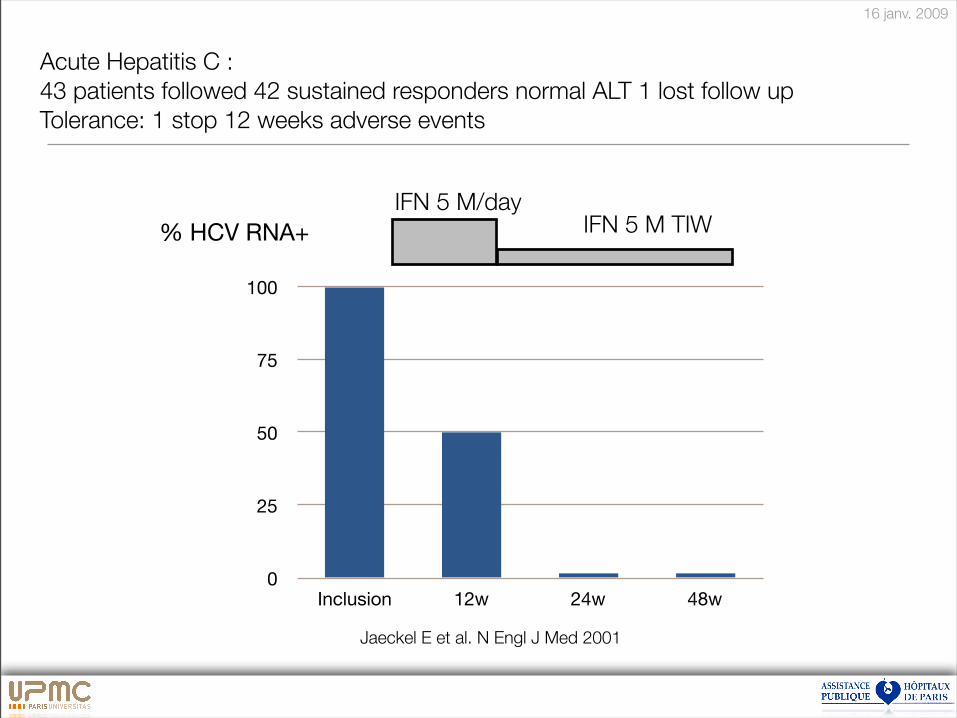
0
25
50
75
100
Inclusion 12w 24w 48w
Acute Hepatitis C :
43 patients followed 42 sustained responders normal ALT 1 lost follow up
Tolerance: 1 stop 12 weeks adverse events
IFN 5 M TIWIFN 5 M/day
Jaeckel E et al. N Engl J Med 2001
% HCV RNA+
16 janv. 2009
Anti-Viral Treatment of Acute HCV
STRATEGIES
11
16 janv. 2009
Hypothesis:
Early control of viral replication prevents chronicity
• Treat all patients ?
• Treat early ?
• Doses of IFN ?
• Ribavirin ?
• Duration of treatment ?
12
16 janv. 2009
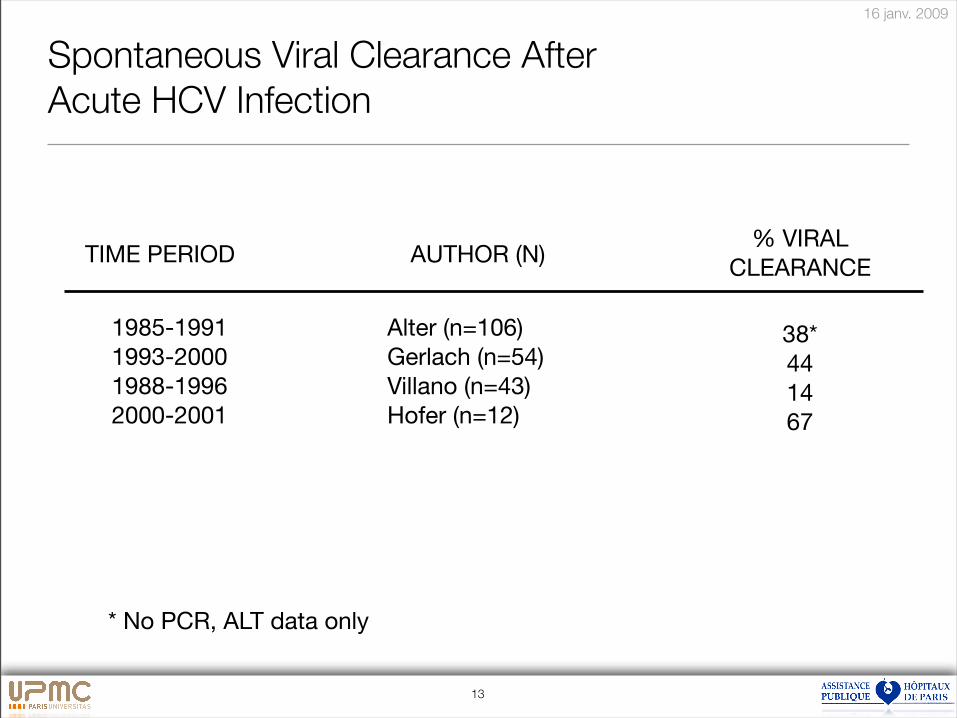
Spontaneous Viral Clearance After
Acute HCV Infection
38*
44
14
67
1985-1991 Alter (n=106)
1993-2000 Gerlach (n=54)
1988-1996 Villano (n=43)
2000-2001 Hofer (n=12)
AUTHOR (N)TIME PERIOD% VIRAL
CLEARANCE
* No PCR, ALT data only
13
16 janv. 2009
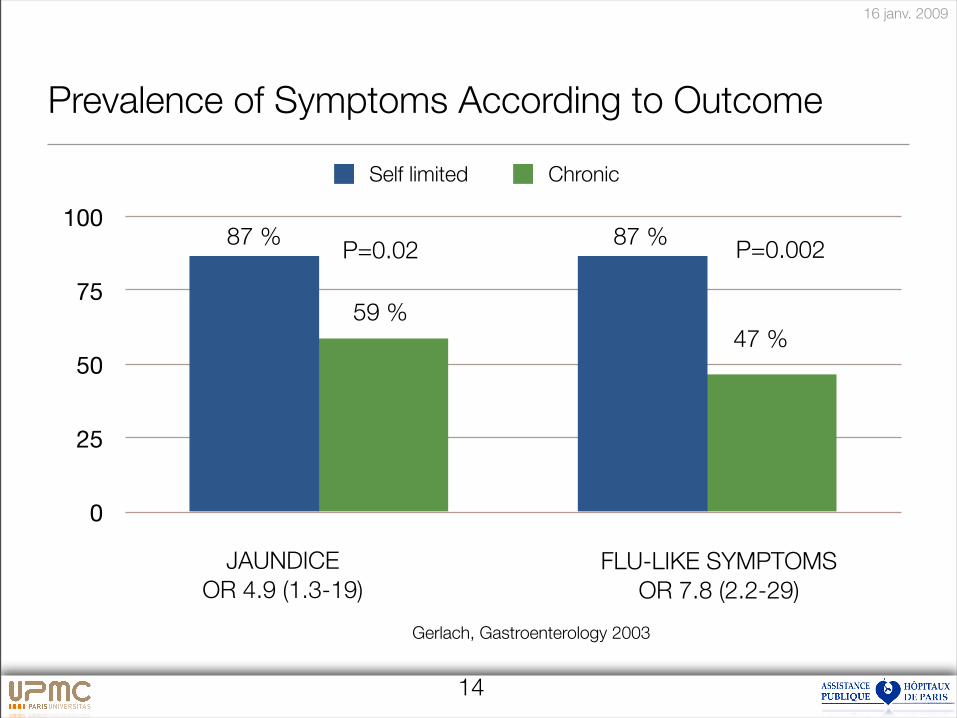
Prevalence of Symptoms According to Outcome
0
25
50
75
100
JAUNDICE
OR 4.9 (1.3-19)
FLU-LIKE SYMPTOMS
OR 7.8 (2.2-29)
87 %
59 %
87 %
47 %
P=0.02 P=0.002
Gerlach, Gastroenterology 2003
14
Self limited Chronic
16 janv. 2009
Predictors of Spontaneous Viral Clearance ...
• Younger age (?)
• Females (?)
• White vs. Blacks (?)
• Rare Quasispecies
• Genotype non-1
• ALT useless
• Can normalize despite viral persistence (50%)
15
16 janv. 2009
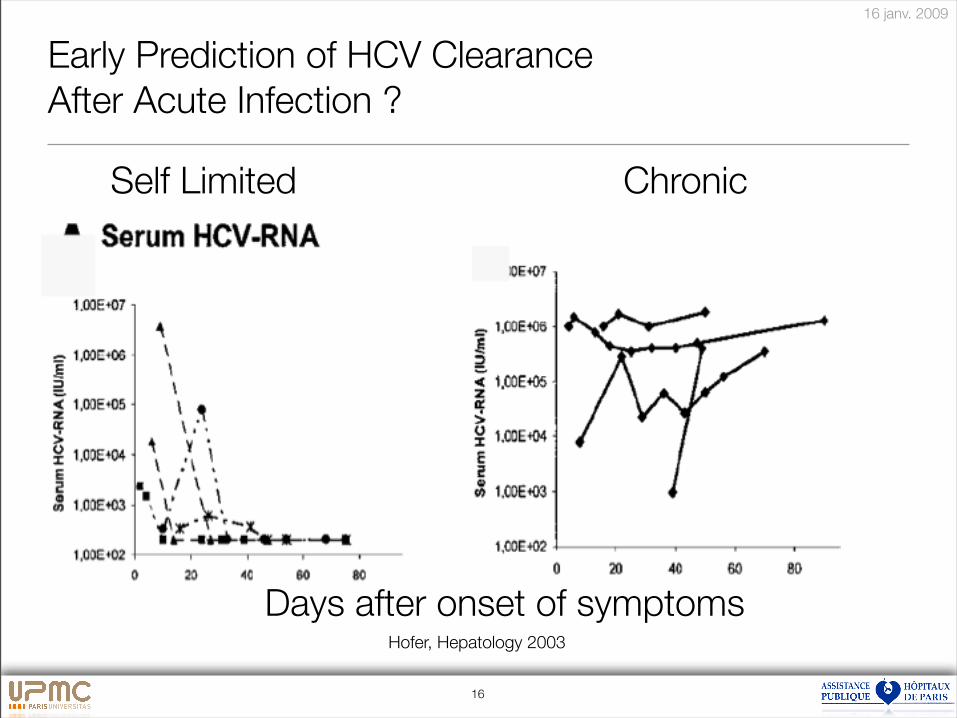
Early Prediction of HCV Clearance
After Acute Infection ?
Days after onset of symptoms
Self Limited Chronic
Hofer, Hepatology 2003
16
16 janv. 2009
Proposal: Treatment Restricted to Patients
that Fail to Clear the Virus
• Asymptomatic or
• HCVRNA still detectable 3-4 months after onset of
symptoms
• PEG IFN (± ribavirin) treatment, at least 24 weeks ??
17
16 janv. 2009
LiverCenter
Treatment of Chronic Hepatitis C:
A la carte from 0 to 5 years
16 janv. 2009
Prise en charge de l’Hépatite C en 2008
• Améliorer le dépistage
• Simplifier le bilan
• Améliorer le traitement
• A la carte
• Ne pas baisser les bras
19
16 janv. 2009
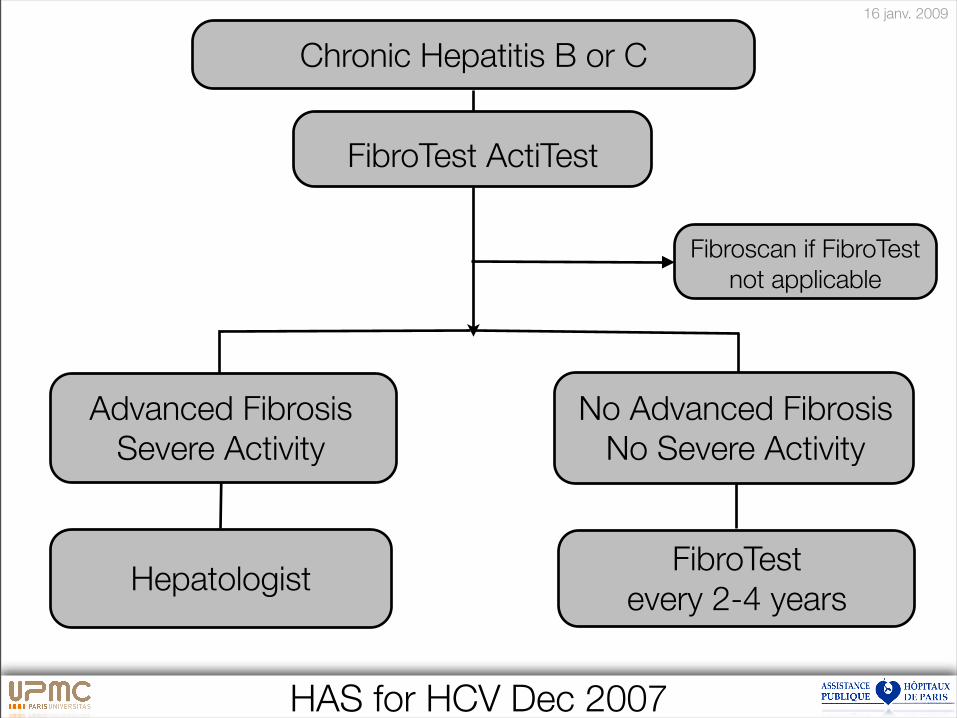
Chronic Hepatitis B or C
FibroTest ActiTest
Advanced Fibrosis
Severe Activity
Hepatologist
Fibroscan if FibroTest
not applicable
No Advanced Fibrosis
No Severe Activity
FibroTest
every 2-4 years
HAS for HCV Dec 2007
16 janv. 2009
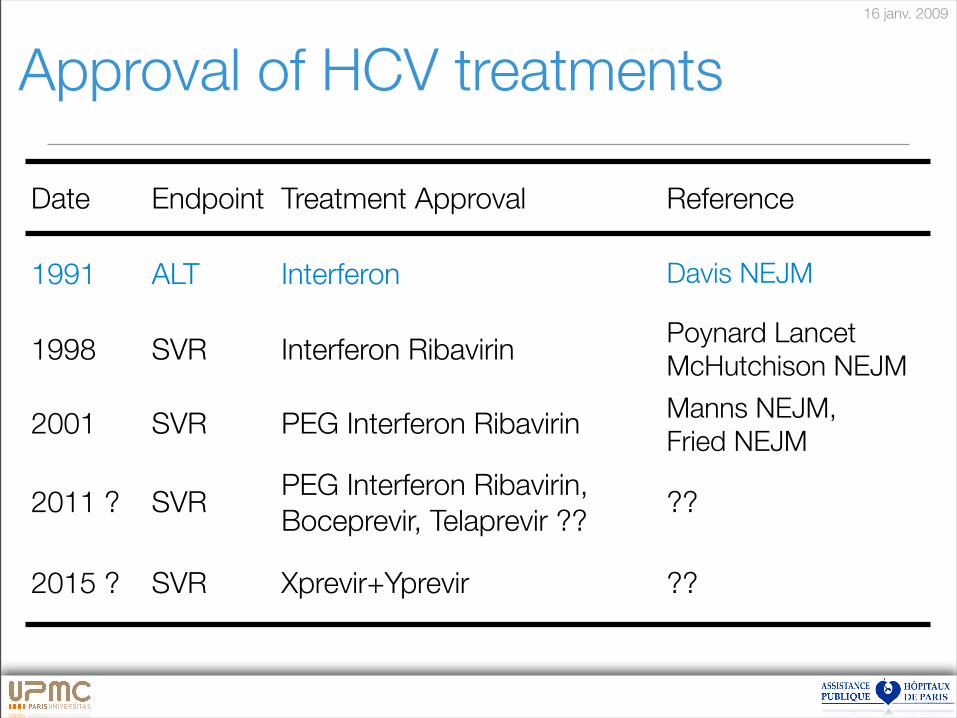
Date Endpoint Treatment Approval Reference
1991 ALT Interferon Davis NEJM
1998 SVR Interferon RibavirinPoynard Lancet
McHutchison NEJM
2001 SVR PEG Interferon RibavirinManns NEJM,
Fried NEJM
2011 ? SVRPEG Interferon Ribavirin,
Boceprevir, Telaprevir ????
2015 ? SVR Xprevir+Yprevir ??
Approval of HCV treatments
16 janv. 2009
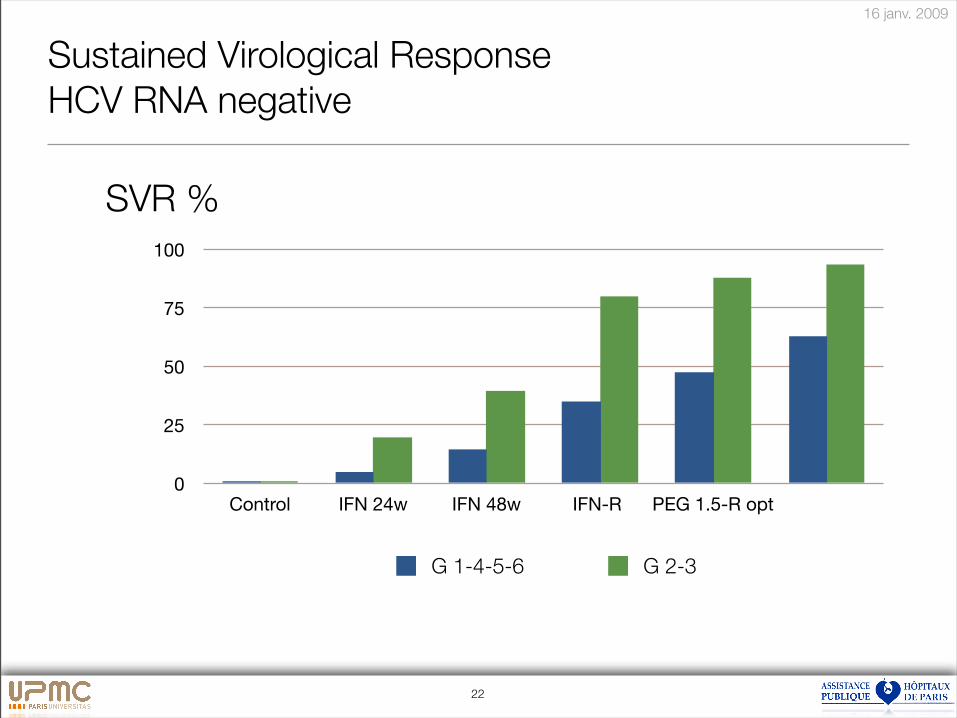
Sustained Virological Response
HCV RNA negative
0
25
50
75
100
Control IFN 24w IFN 48w IFN-R PEG 1.5-R opt
G 1-4-5-6 G 2-3
22
SVR %
16 janv. 2009
Factors associated with SVR in HCV
Sure
• Genotype
• Viral load
• Fibrosis stage
• Age (Duration)
• HIV
• Male
• BMI,Steatosis,Diabetes
Poynard et al Lancet 2003
23
16 janv. 2009
24
Traitement à la carte avec PEG-Riba?
• Attention aux faux amis
• G2 et G3
! mais
• F2F3F4
• Attention au gras et au sucre
Poynard et al Hepatology 2000, Lancet 2003, Hepatology 2003
16 janv. 2009
25
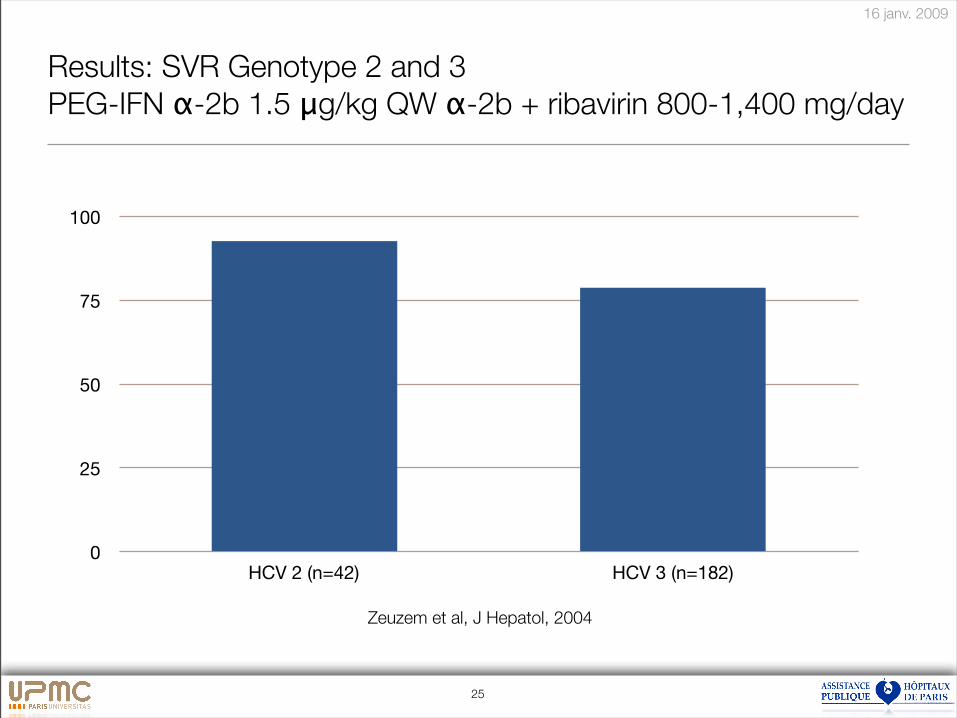
Results: SVR Genotype 2 and 3
PEG-IFN !-2b 1.5 "g/kg QW !-2b + ribavirin 800-1,400 mg/day
0
25
50
75
100
HCV 2 (n=42) HCV 3 (n=182)
Zeuzem et al, J Hepatol, 2004
16 janv. 2009
26
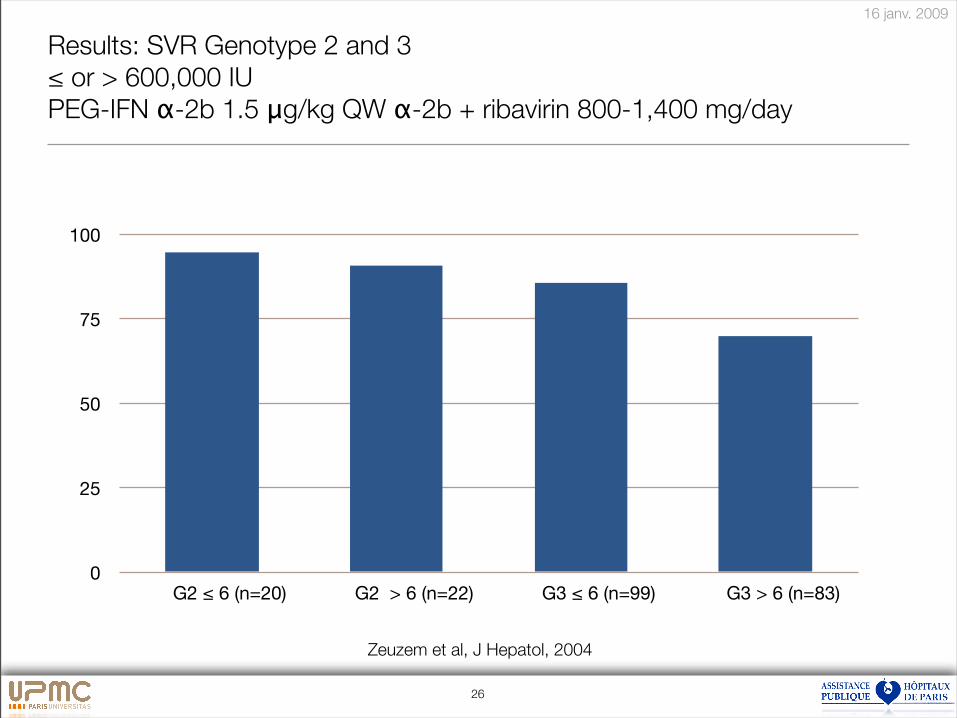
Results: SVR Genotype 2 and 3
! or > 600,000 IU
PEG-IFN !-2b 1.5 "g/kg QW !-2b + ribavirin 800-1,400 mg/day
0
25
50
75
100
G2 " 6 (n=20) G2 > 6 (n=22) G3 " 6 (n=99) G3 > 6 (n=83)
Zeuzem et al, J Hepatol, 2004
16 janv. 2009
27
A la carte regimen with PEG-Riba?
• Longer duration for Genotype 2 and 3 if
• Advanced fibrosis F2F3F4
• Steatosis in genotype 2
• HIV
Poynard et al Hepatology 2000, Lancet 2003, Hepatology 2003
16 janv. 2009
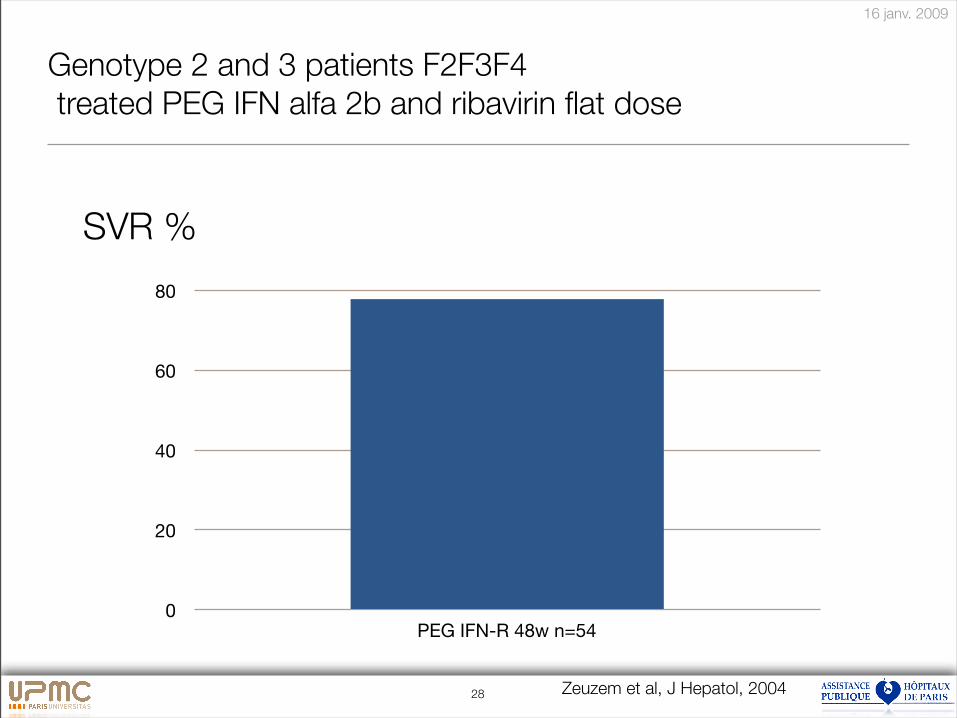
Genotype 2 and 3 patients F2F3F4
treated PEG IFN alfa 2b and ribavirin flat dose
0
20
40
60
80
PEG IFN-R 48w n=54
Zeuzem et al, J Hepatol, 200428
SVR %
16 janv. 2009
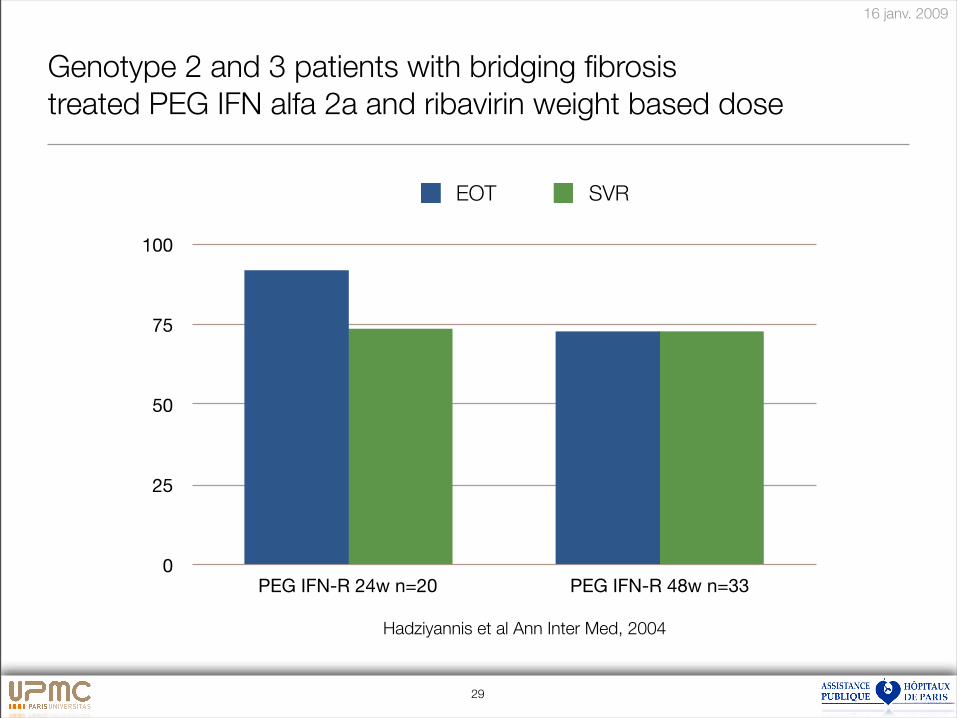
Genotype 2 and 3 patients with bridging fibrosis
treated PEG IFN alfa 2a and ribavirin weight based dose
0
25
50
75
100
PEG IFN-R 24w n=20 PEG IFN-R 48w n=33
EOT SVR
Hadziyannis et al Ann Inter Med, 2004
29
16 janv. 2009
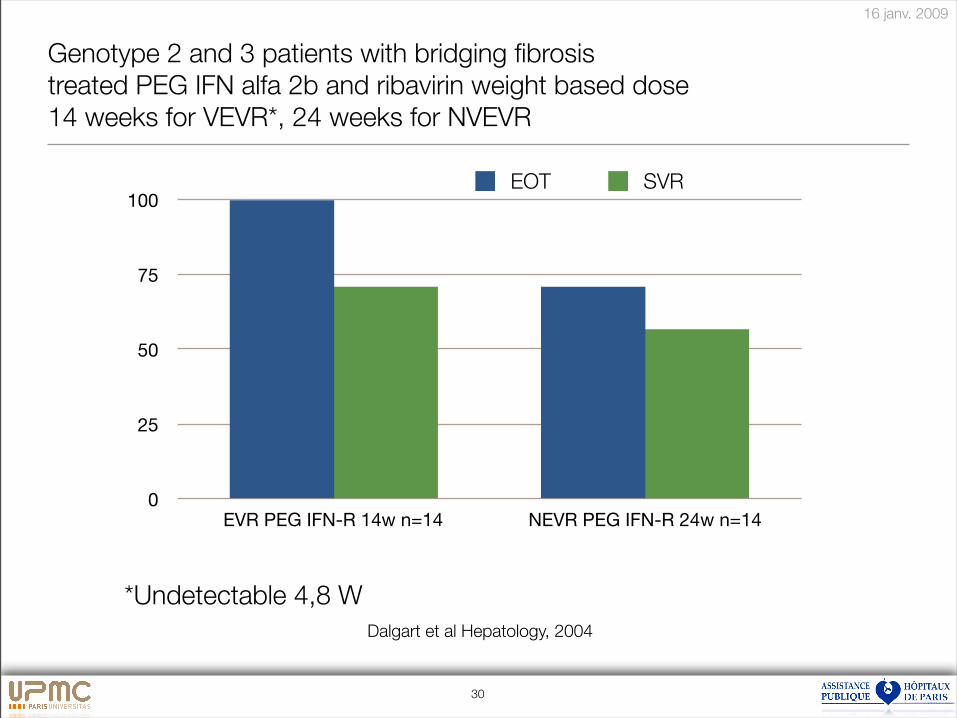
Genotype 2 and 3 patients with bridging fibrosis
treated PEG IFN alfa 2b and ribavirin weight based dose
14 weeks for VEVR*, 24 weeks for NVEVR
0
25
50
75
100
EVR PEG IFN-R 14w n=14 NEVR PEG IFN-R 24w n=14
EOT SVR
Dalgart et al Hepatology, 2004
*Undetectable 4,8 W
30
16 janv. 2009
31
A la carte regimen with PEG-Riba?
• Shorter duration (2-4 months)
• For Genotype 2 and 3, if no relapse factors
Poynard et al Hepatology 2000, Lancet 2003, Hepatology 2003
16 janv. 2009
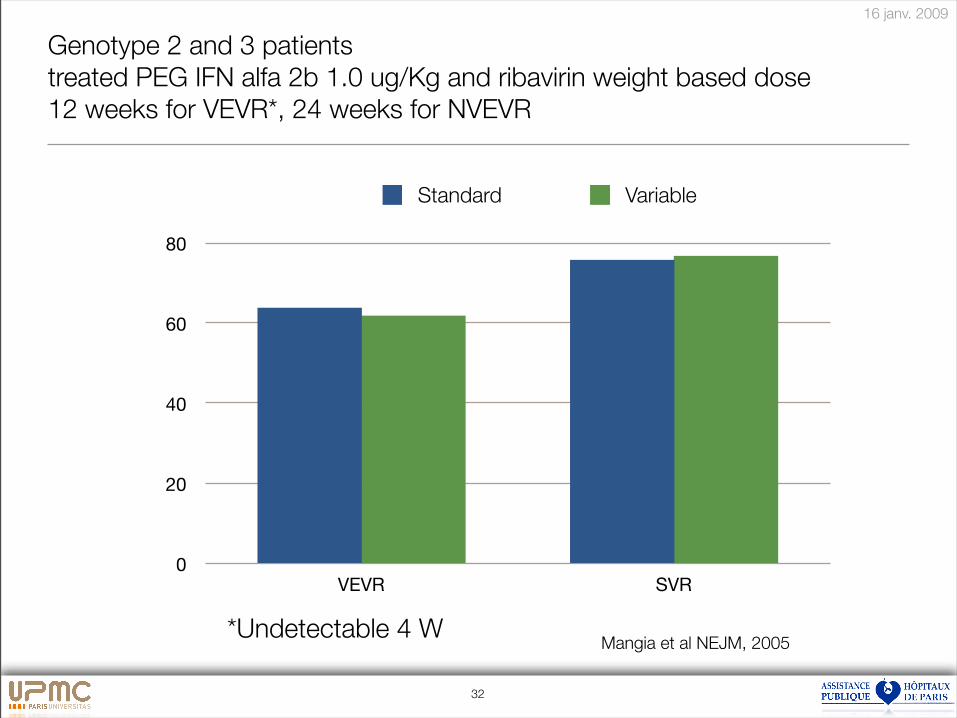
32
Genotype 2 and 3 patients
treated PEG IFN alfa 2b 1.0 ug/Kg and ribavirin weight based dose
12 weeks for VEVR*, 24 weeks for NVEVR
0
20
40
60
80
VEVR SVR
Standard Variable
Mangia et al NEJM, 2005*Undetectable 4 W
16 janv. 2009
33
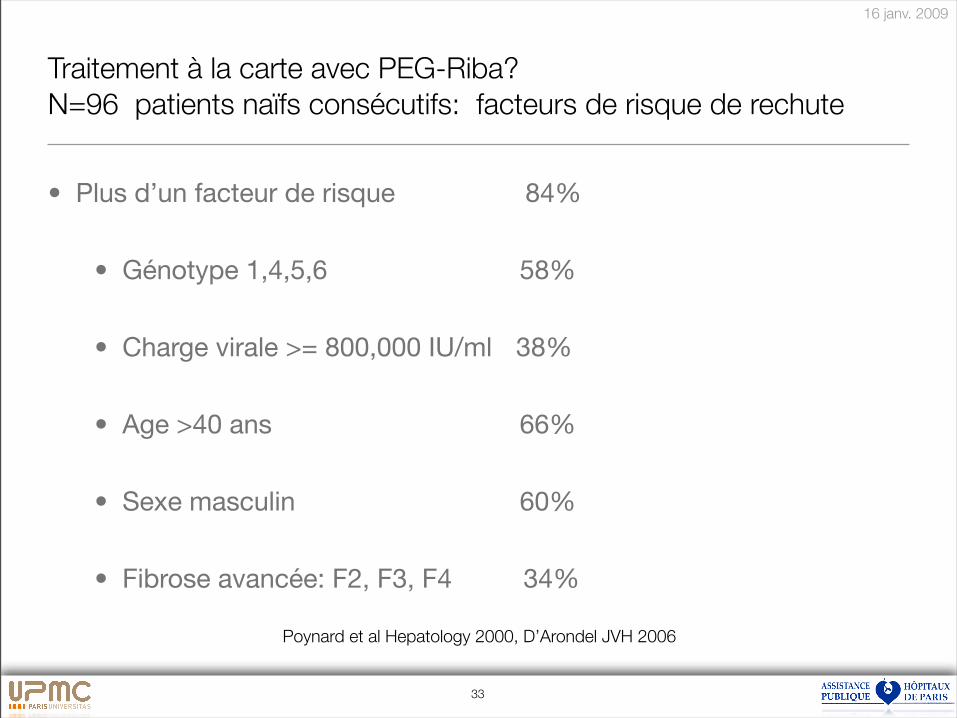
Traitement à la carte avec PEG-Riba?
N=96 patients naïfs consécutifs: facteurs de risque de rechute
• Plus d’un facteur de risque# # 84%
• Génotype 1,4,5,6 ## # 58%
• Charge virale >= 800,000 IU/ml ! 38%
• Age >40 ans ! ! ! ! 66%
• Sexe masculin !! ! ! 60%
• Fibrose avancée: F2, F3, F4 # # 34%
Poynard et al Hepatology 2000, D’Arondel JVH 2006
16 janv. 2009
34
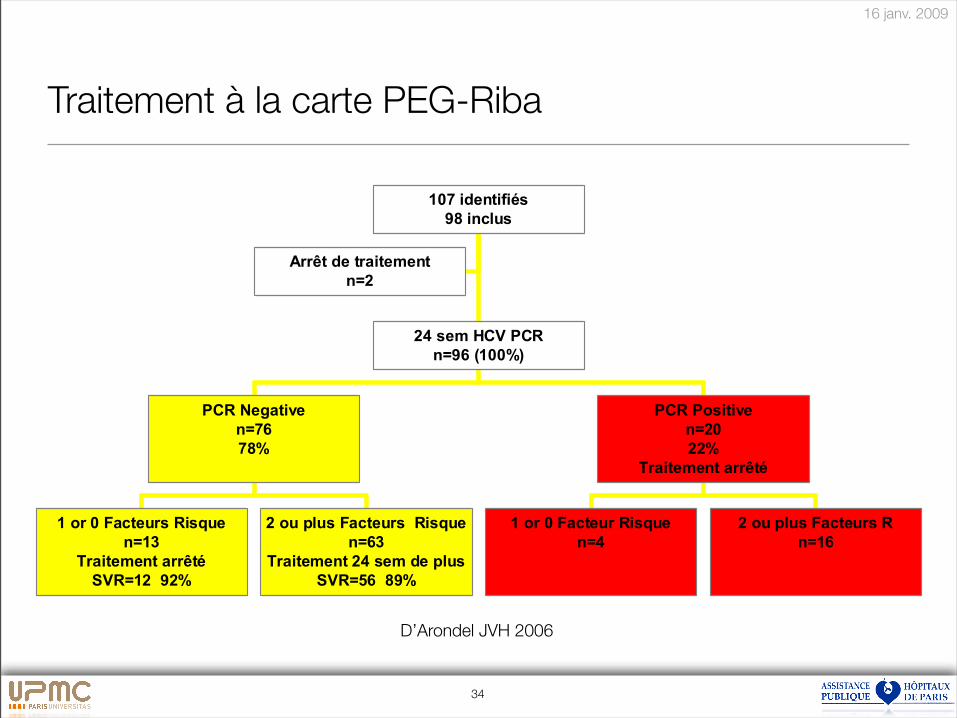
Traitement à la carte PEG-Riba
D’Arondel JVH 2006
35
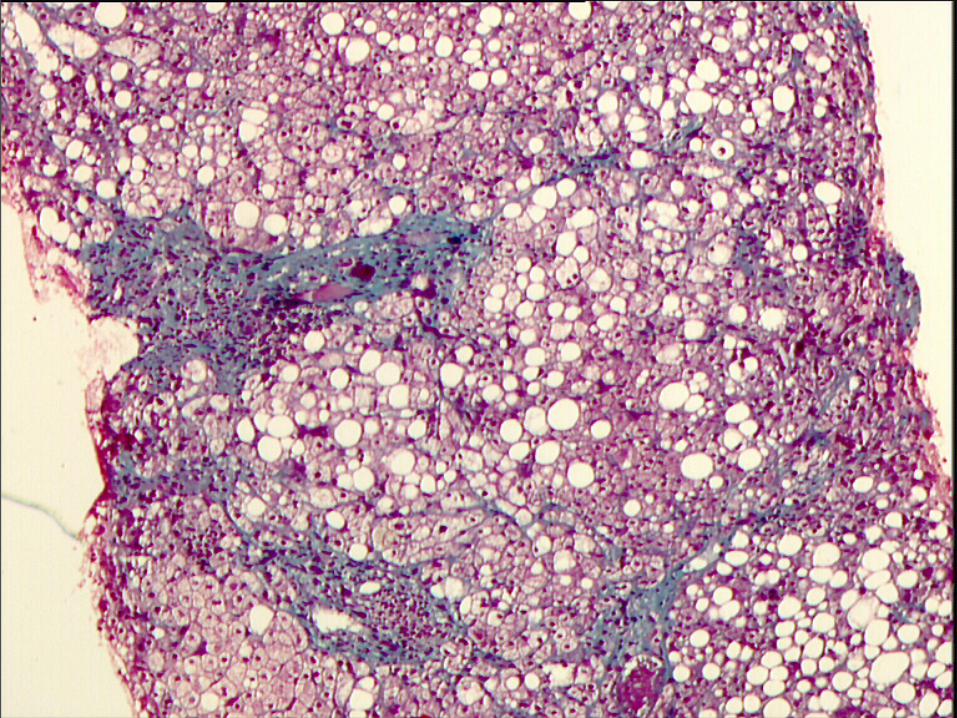
Background
16 janv. 2009
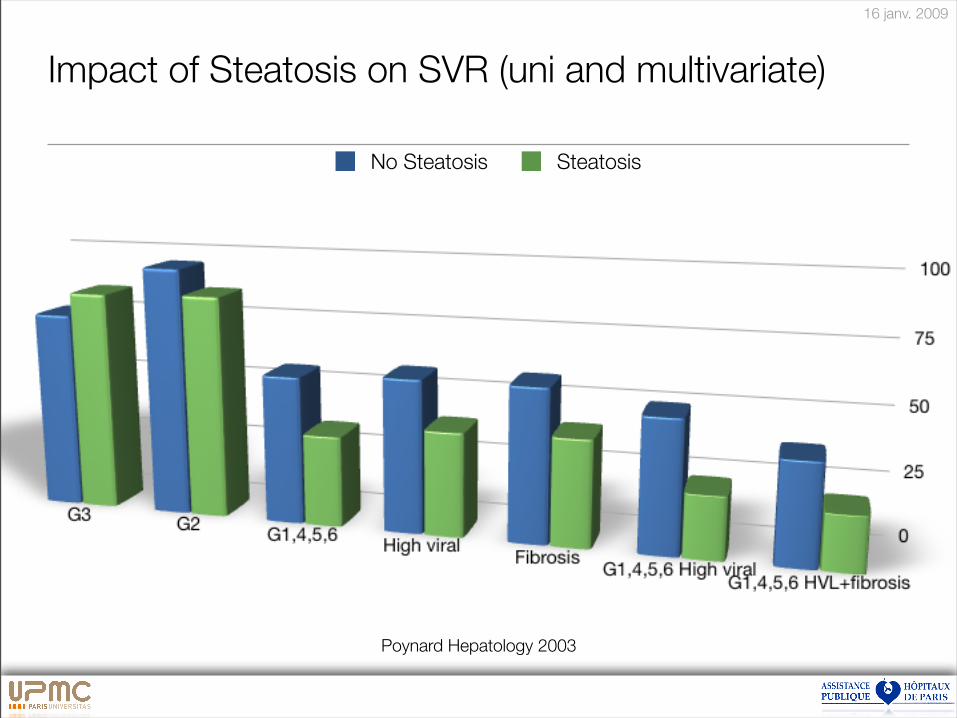
Impact of Steatosis on SVR (uni and multivariate)
No Steatosis Steatosis
Poynard Hepatology 2003
16 janv. 2009
A la carte suisse, ou à l’américaine ?
37
16 janv. 2009
38
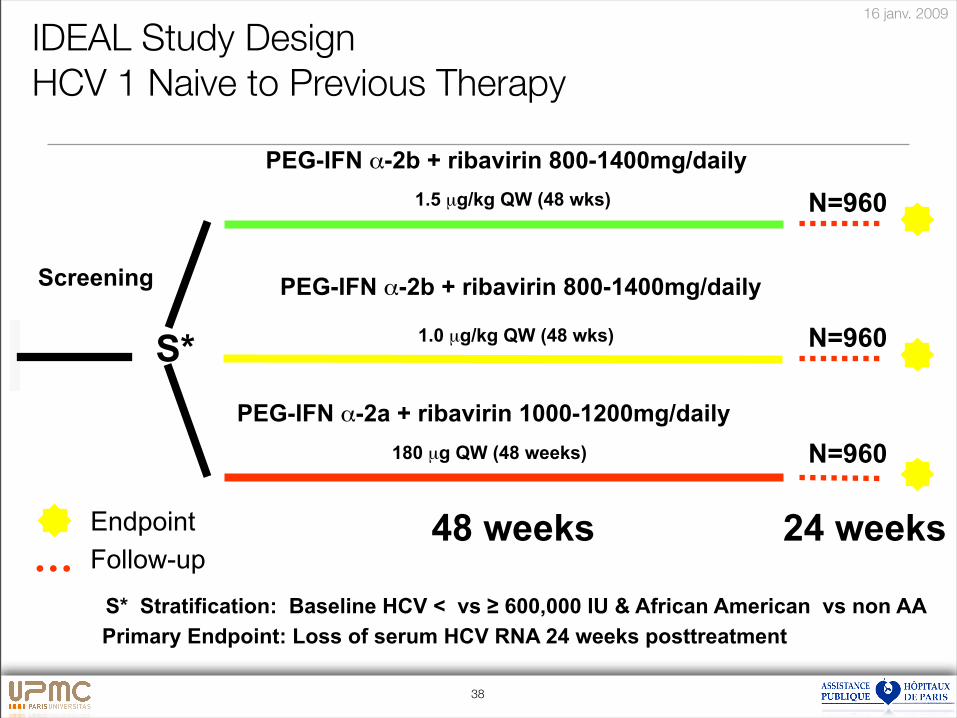
IDEAL Study Design
HCV 1 Naive to Previous Therapy
PEG-IFN !-2b + ribavirin 800-1400mg/daily
1.0 µg/kg QW (48 wks) N=960
PEG-IFN !-2a + ribavirin 1000-1200mg/daily
N=960180 µg QW (48 weeks)
Screening
PEG-IFN !-2b + ribavirin 800-1400mg/daily
N=9601.5 µg/kg QW (48 wks)
Endpoint
Follow-up48 weeks 24 weeks
Primary Endpoint: Loss of serum HCV RNA 24 weeks posttreatment
S* Stratification: Baseline HCV < vs ! 600,000 IU & African American vs non AA
S*
16 janv. 2009
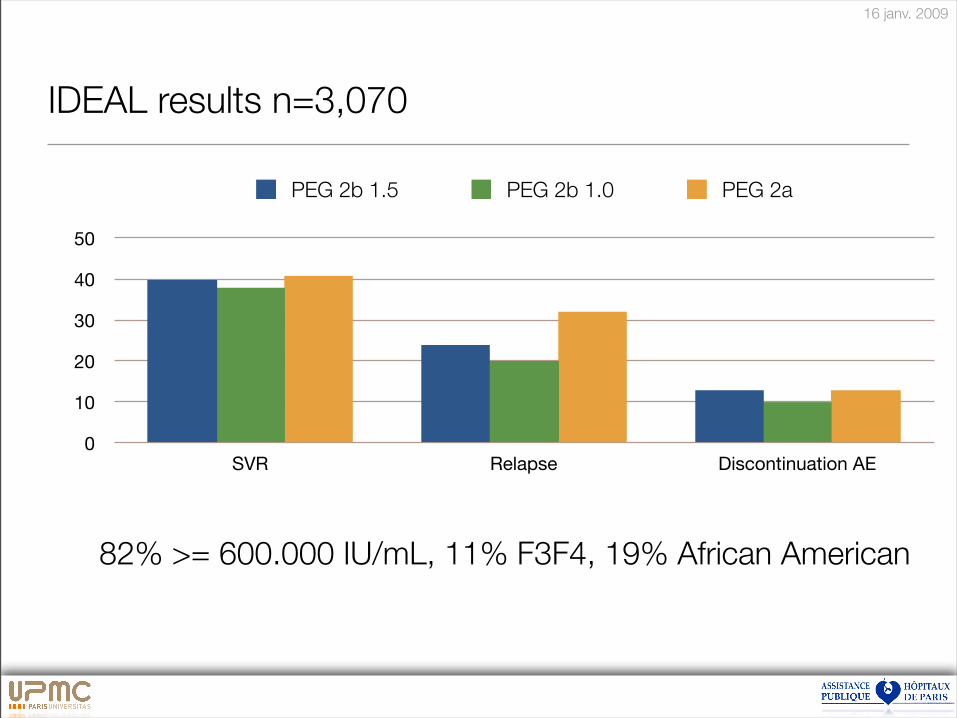
IDEAL results n=3,070
0
10
20
30
40
50
SVR Relapse Discontinuation AE
PEG 2b 1.5 PEG 2b 1.0 PEG 2a
82% >= 600.000 IU/mL, 11% F3F4, 19% African American
16 janv. 2009
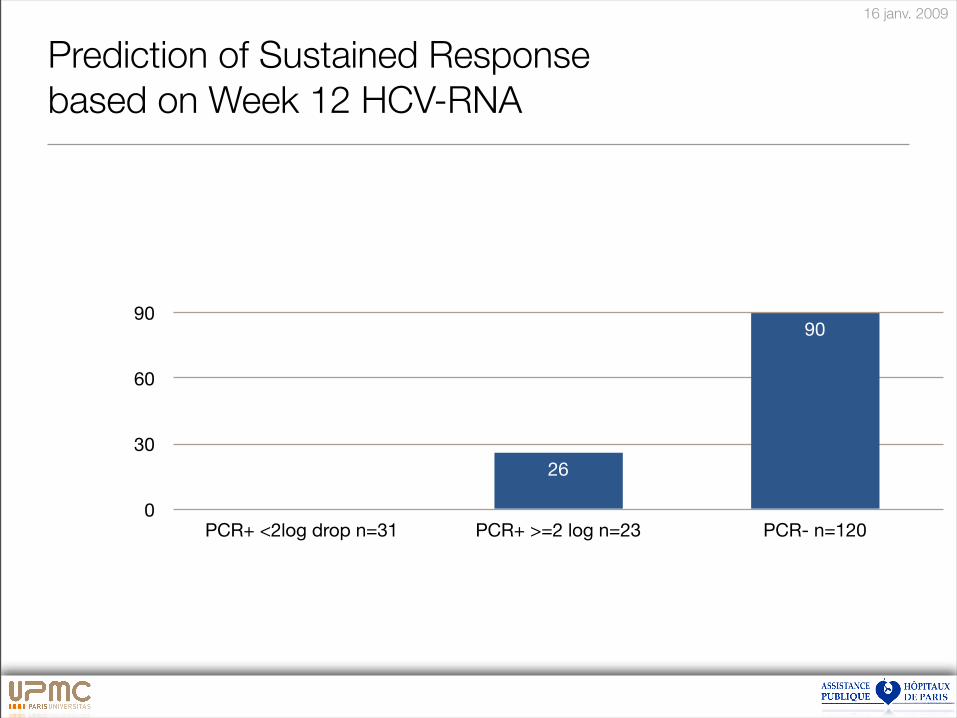
Prediction of Sustained Response
based on Week 12 HCV-RNA
0
30
60
90
PCR+ <2log drop n=31 PCR+ >=2 log n=23 PCR- n=120
90
26
16 janv. 2009
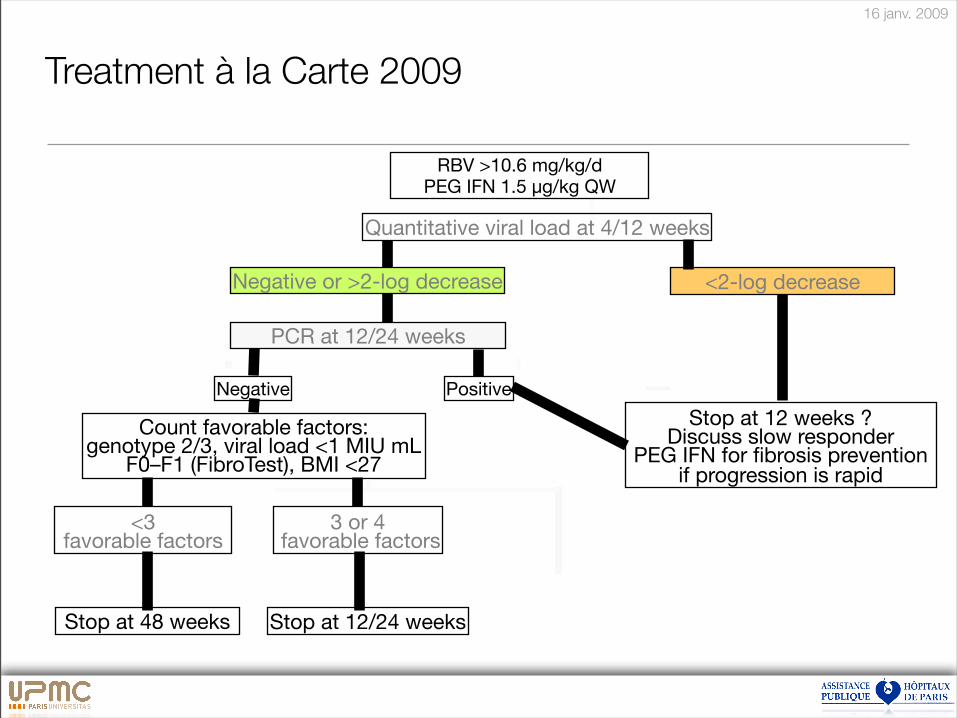
Count favorable factors:genotype 2/3, viral load <1 MIU mL
F0–F1 (FibroTest), BMI <27
Treatment à la Carte 2009
Stop at 48 weeks
Positive
PCR at 12/24 weeks
Negative or >2-log decrease <2-log decrease
RBV >10.6 mg/kg/dPEG IFN 1.5 µg/kg QW
<3 favorable factors
Stop at 12/24 weeks
3 or 4 favorable factors
Stop at 12 weeks ? Discuss slow responder
PEG IFN for fibrosis prevention if progression is rapid
Quantitative viral load at 4/12 weeks
Negative

16 janv. 2009
LiverCenter
VHC
Traitement des cas simples
Traitement des cas compliqués
Thierry Poynard
Vlad Ratziu, Yves Benhamou
16 janv. 2009
Prise en charge de l’Hépatite C en 2008
• Améliorer le dépistage
• Simplifier le bilan
• Améliorer le traitement
• A la carte
• Ne pas baisser les bras
43
16 janv. 2009
44
Traitement à la carte avec PEG-Riba?
• Ne pas baisser les bras
• Traitement anti-fibrosant
• Sujet de plus de 65 ans
Poynard et al, Lancet 2003, Thabut et al AJG 2006
16 janv. 2009
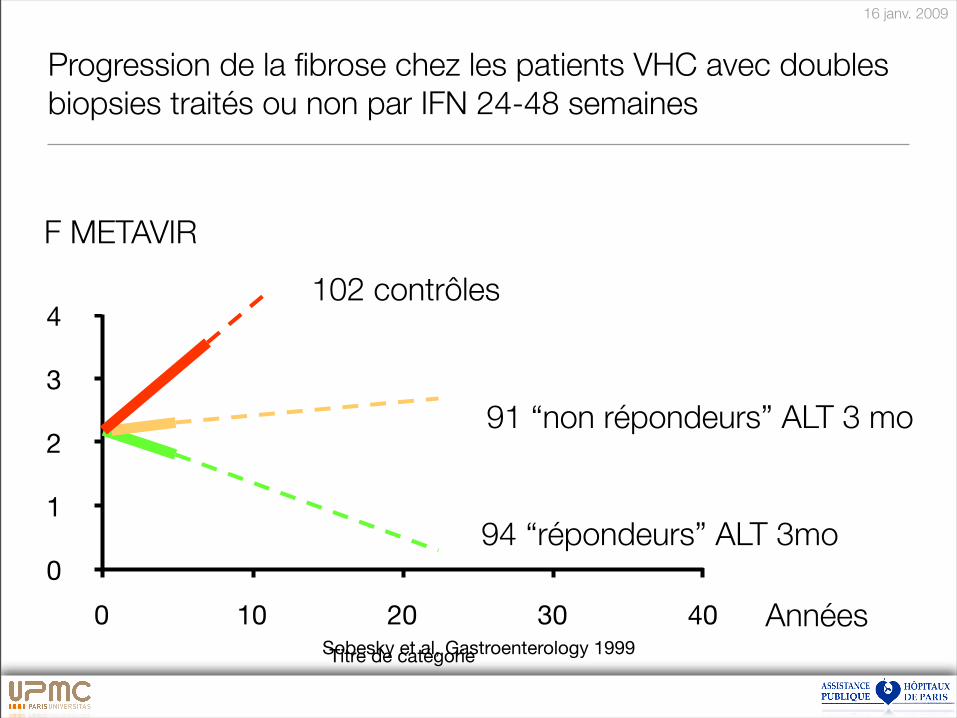
Progression de la fibrose chez les patients VHC avec doubles
biopsies traités ou non par IFN 24-48 semaines
0
1
2
3
4
0 10 20 30 40
Titre de catégorieSobesky et al, Gastroenterology 1999
Années
102 contrôles
91 “non répondeurs” ALT 3 mo
94 “répondeurs” ALT 3mo
F METAVIR
16 janv. 2009
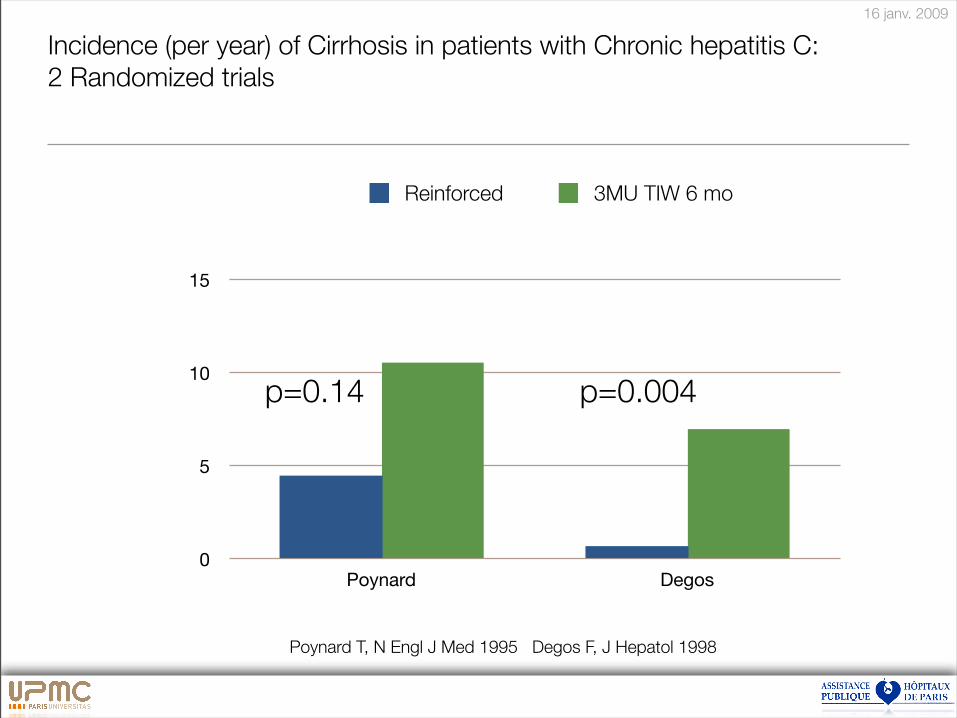
Incidence (per year) of Cirrhosis in patients with Chronic hepatitis C:
2 Randomized trials
"
0
5
10
15
Poynard Degos
Reinforced 3MU TIW 6 mo
p=0.004p=0.14
Poynard T, N Engl J Med 1995 Degos F, J Hepatol 1998
16 janv. 2009
Histologic Improvement of Fibrosis in Patients with Hepatitis C
Who Have Sustained Response to Interferon Therapy
• 593 patients 2 biopsies
• 106 Untreated patients 4.8 years
• 304 IFN virologic non-responders 3.2 years
• 183 IFN virologic responders 3.2 years
47
Y Shiratori, Ann Int Med 2000
16 janv. 2009
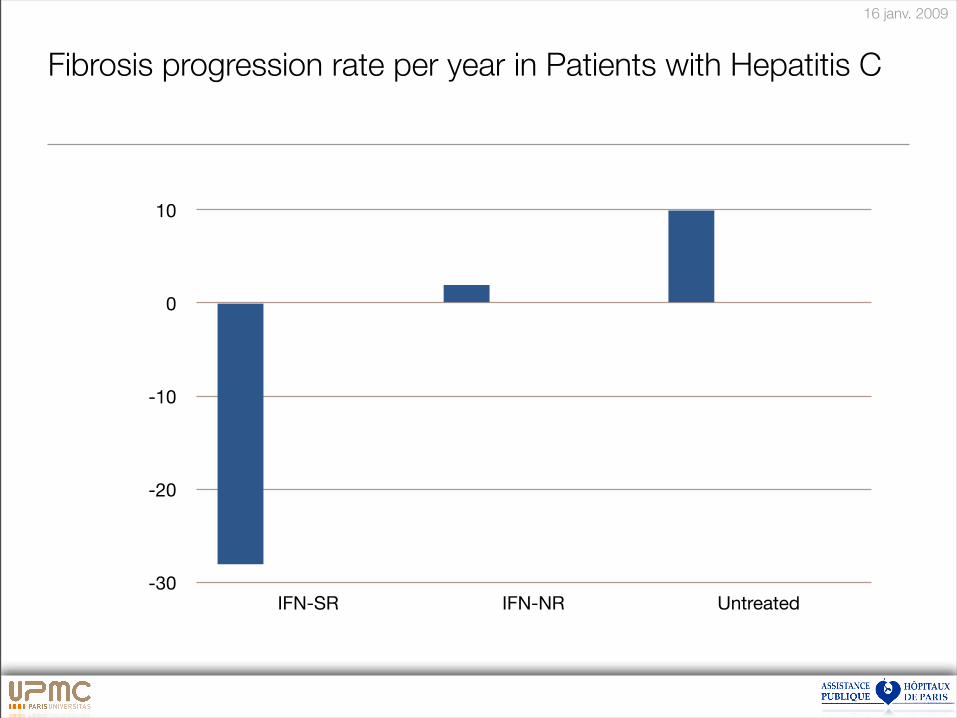
Fibrosis progression rate per year in Patients with Hepatitis C
-30
-20
-10
0
10
IFN-SR IFN-NR Untreated
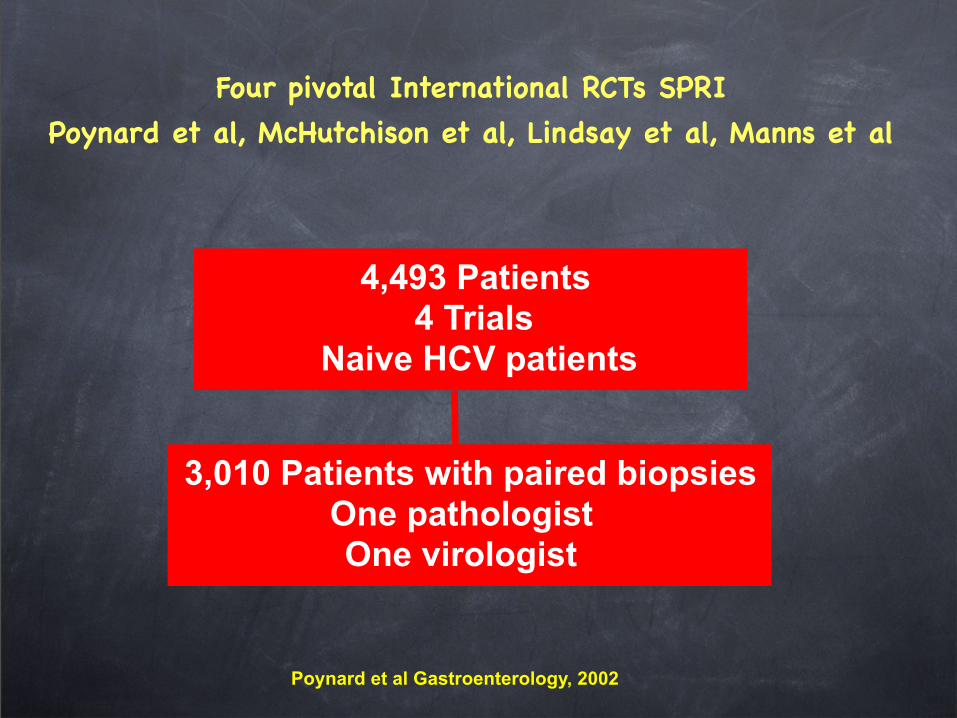
Four pivotal International RCTs SPRI
Poynard et al, McHutchison et al, Lindsay et al, Manns et al
3,010 Patients with paired biopsies
One pathologistOne virologist
4,493 Patients4 Trials
Naive HCV patients
Poynard et al Gastroenterology, 2002
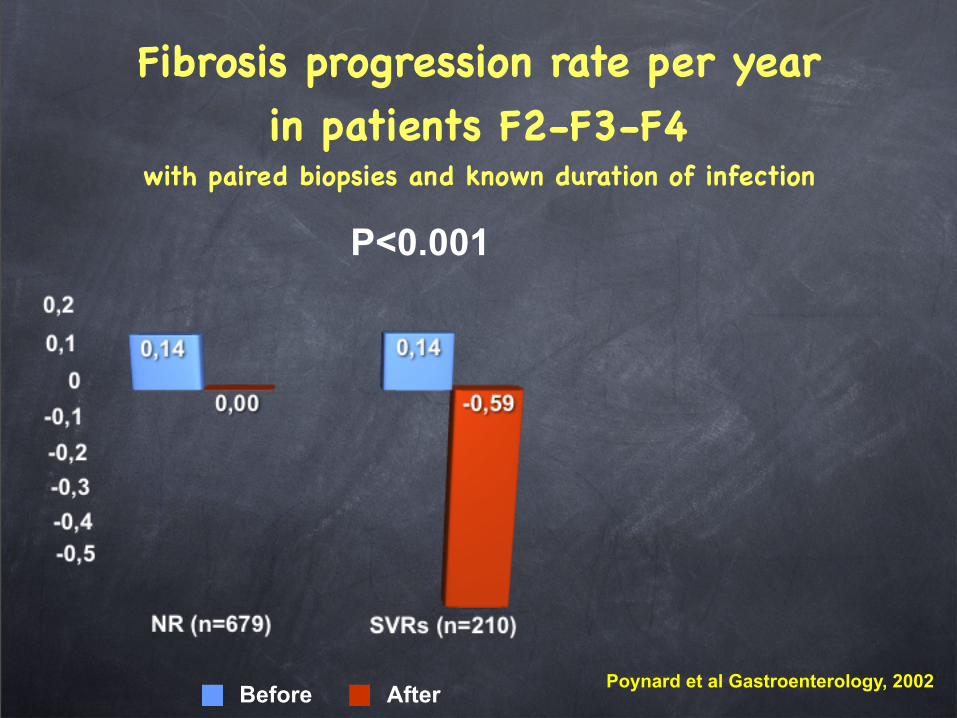
Fibrosis progression rate per year in patients F2-F3-F4
with paired biopsies and known duration of infection
Before After
P<0.001
Poynard et al Gastroenterology, 2002
51
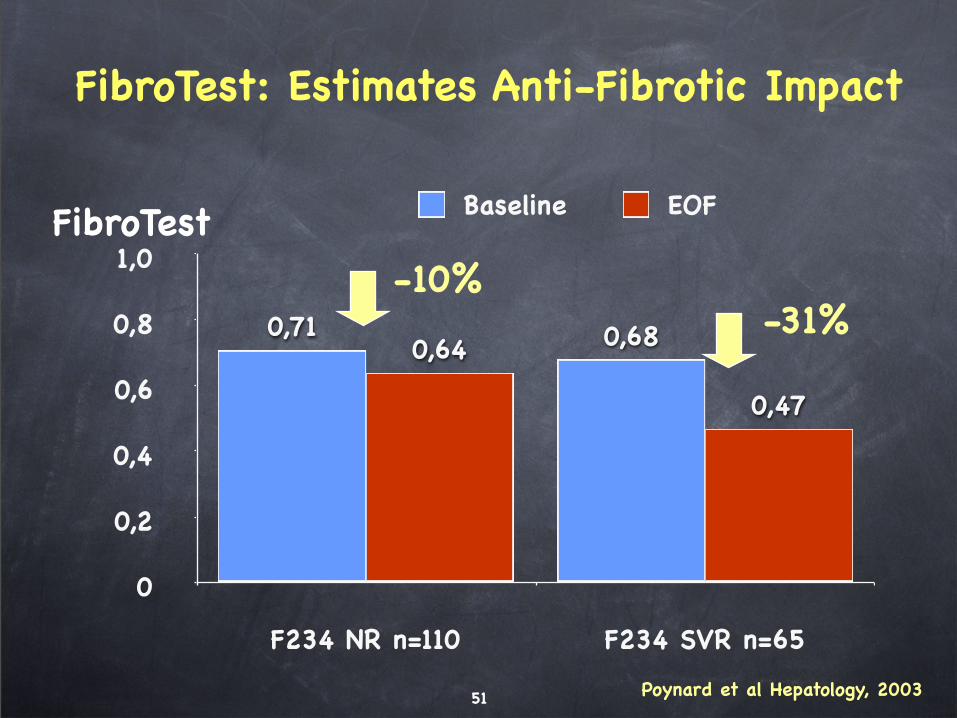
FibroTest: Estimates Anti-Fibrotic Impact
0
0,2
0,4
0,6
0,8
1,0
F234 NR n=110 F234 SVR n=65
0,47
0,64 0,680,71
Baseline EOF
-10%-31%
Poynard et al Hepatology, 2003
FibroTest
52
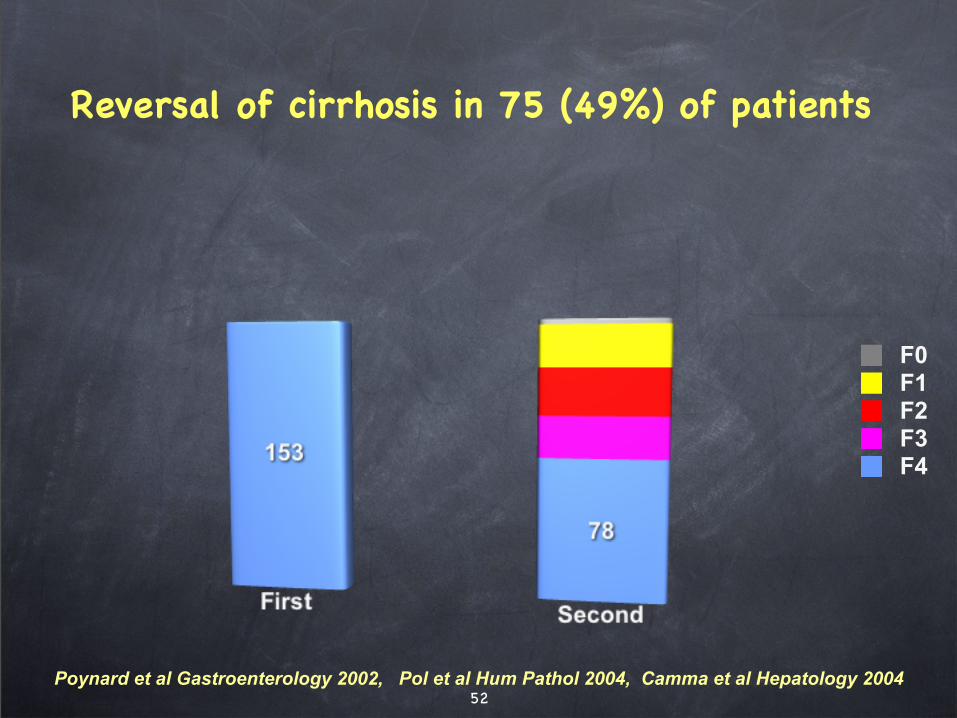
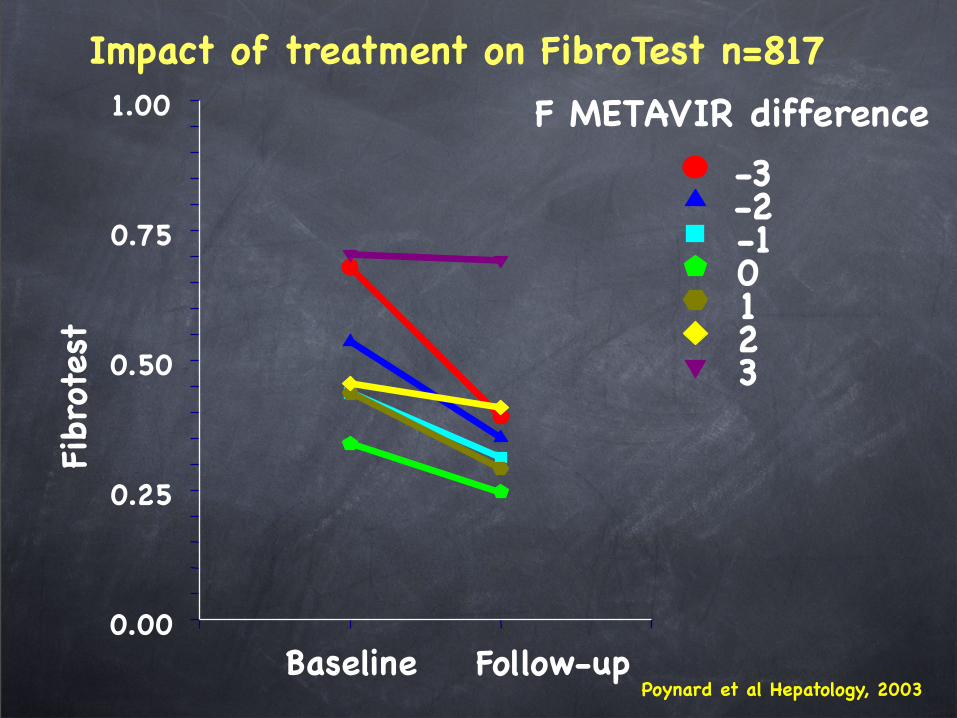
Reversal of cirrhosis in 75 (49%) of patients
F4F3F2F1F0
Poynard et al Gastroenterology 2002, Pol et al Hum Pathol 2004, Camma et al Hepatology 2004
0.00
0.25
0.50
0.75
1.00
Impact of treatment on FibroTest n=817
Baseline
Fibr
otes
tF METAVIR difference
-3-2-10123
Follow-upPoynard et al Hepatology, 2003
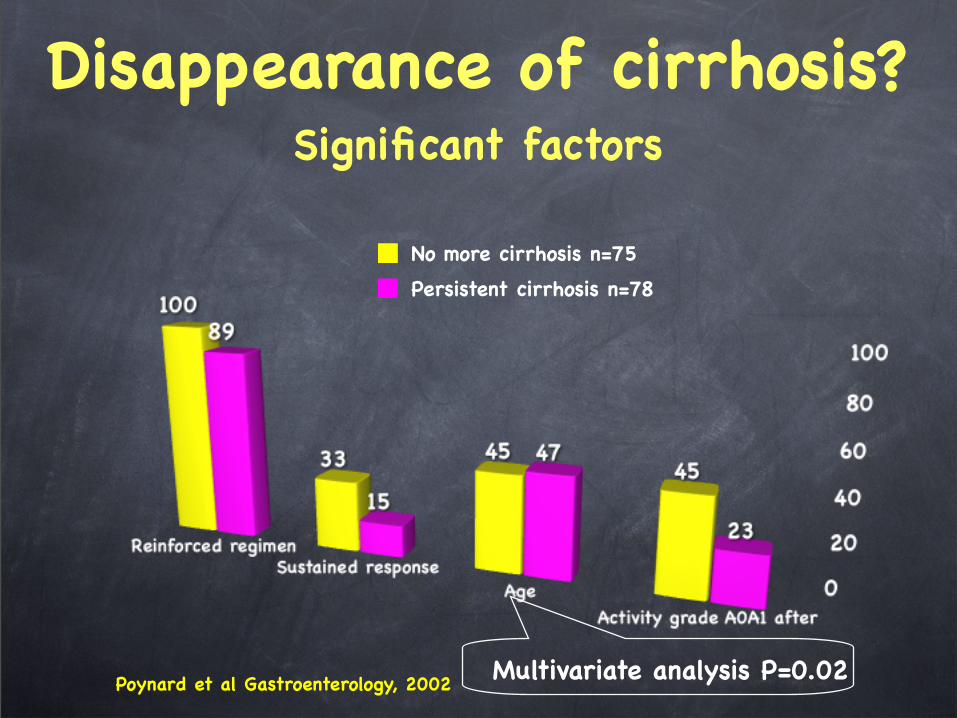
Disappearance of cirrhosis? Significant factors
No more cirrhosis n=75
Persistent cirrhosis n=78
Multivariate analysis P=0.02Poynard et al Gastroenterology, 2002
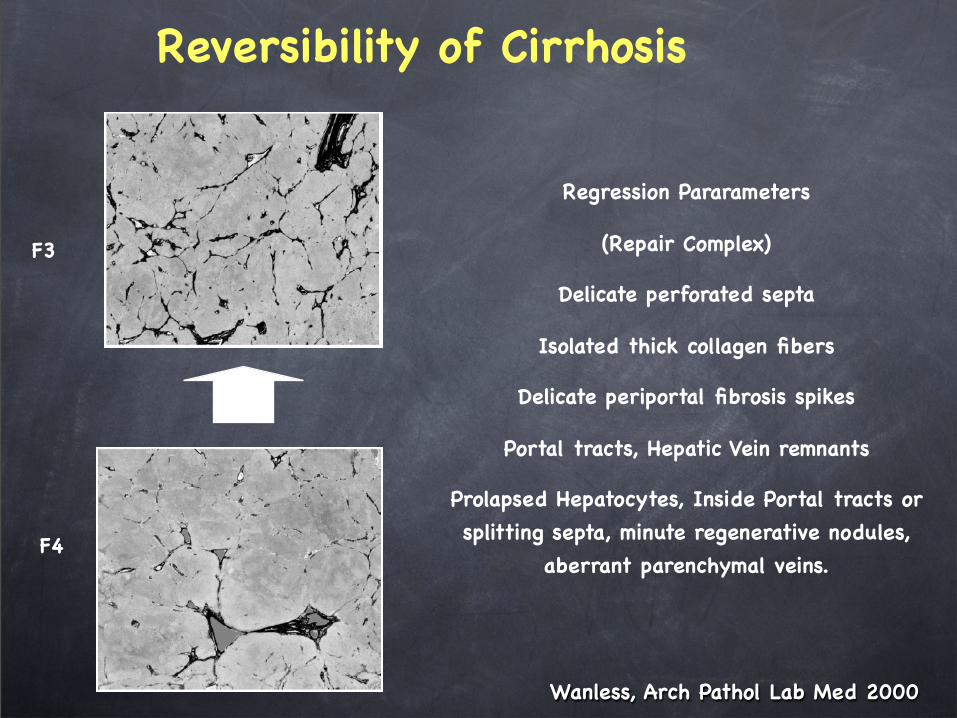
Reversibility of Cirrhosis
Wanless, Arch Pathol Lab Med 2000
F4
F3
Regression Pararameters
(Repair Complex)
Delicate perforated septa
Isolated thick collagen fibers
Delicate periportal fibrosis spikes
Portal tracts, Hepatic Vein remnants
Prolapsed Hepatocytes, Inside Portal tracts or
splitting septa, minute regenerative nodules,
aberrant parenchymal veins.
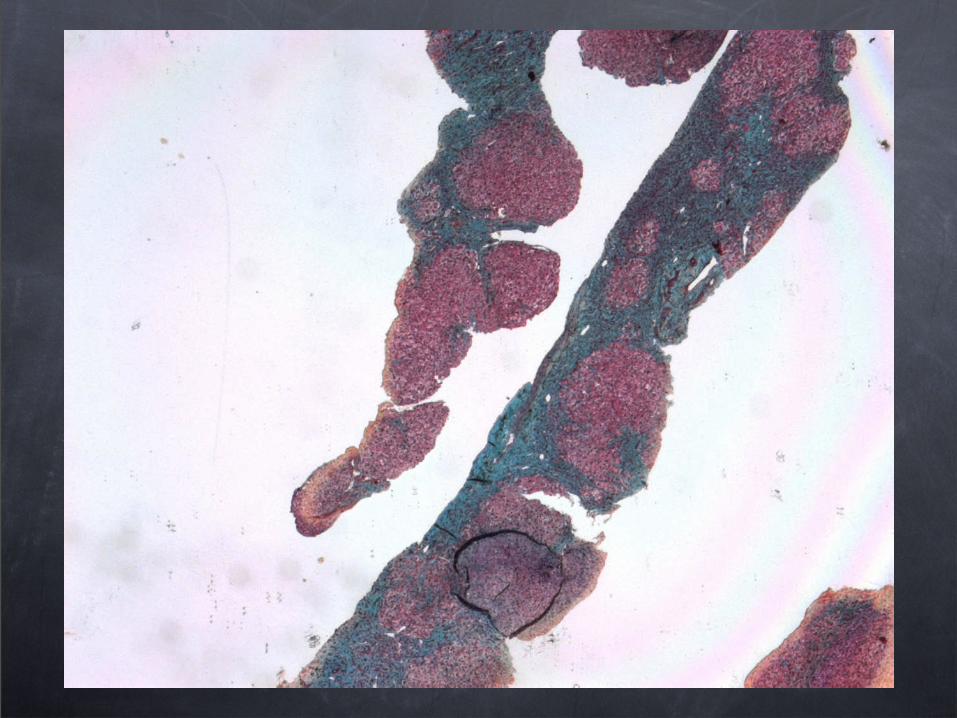
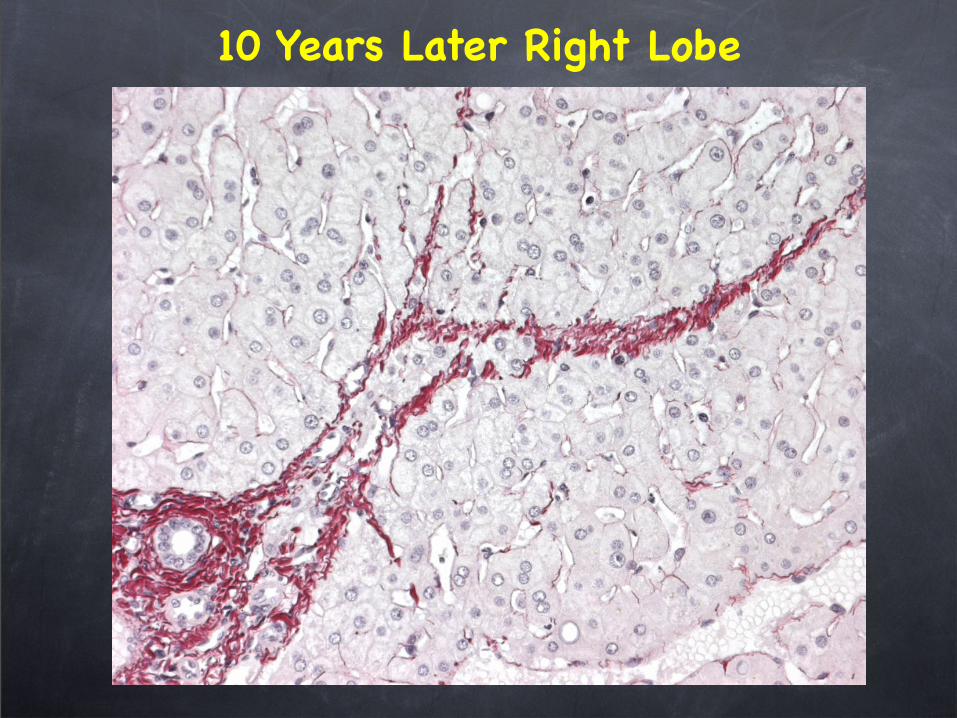
10 Years Later Right Lobe
Impact in SVR
Less cirrhosis
Less complications
Less deaths
Beware of HepatoCellular Carcinoma in Sustained Virological responders
previously F3 or F4
60
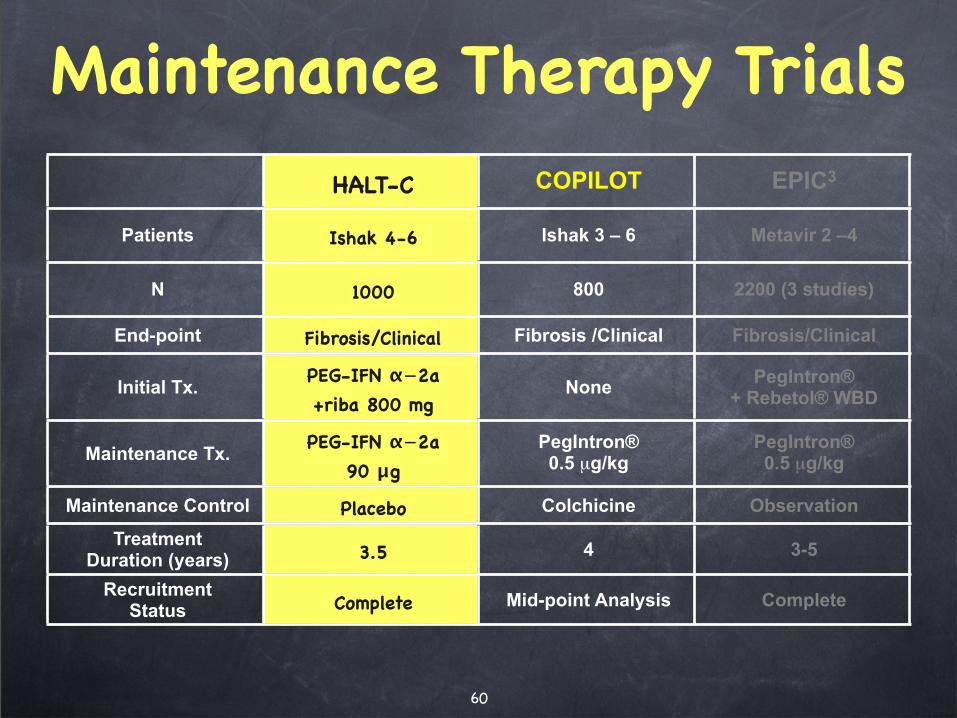
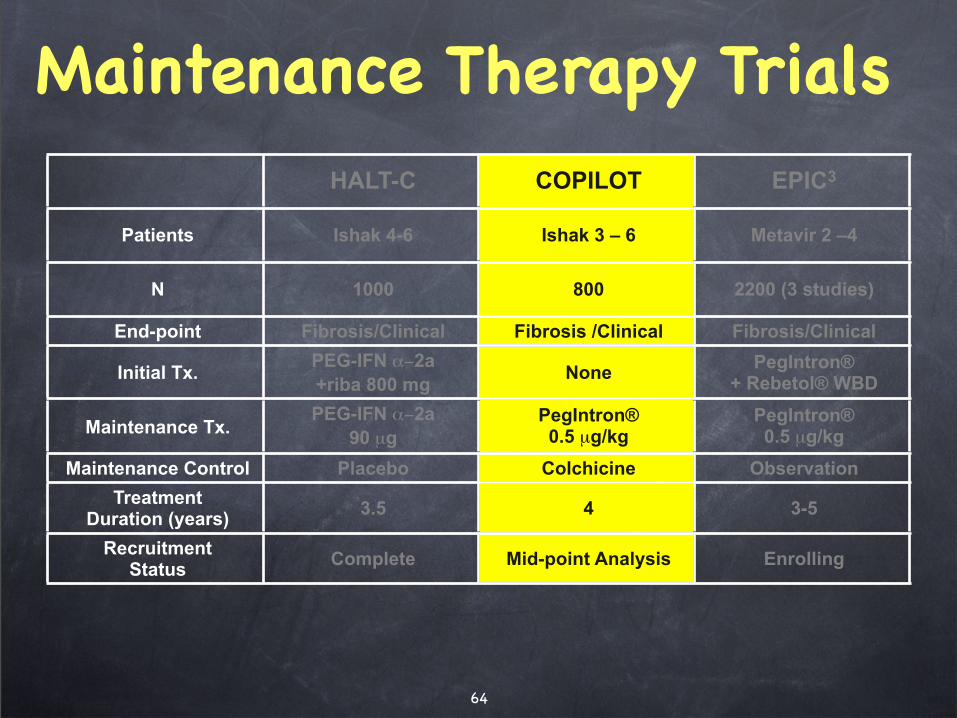
Maintenance Therapy Trials
HALT-C COPILOT EPIC3
Patients Ishak 4-6 Ishak 3 – 6 Metavir 2 –4
N 1000 800 2200 (3 studies)
End-point Fibrosis/Clinical Fibrosis /Clinical Fibrosis/Clinical
Initial Tx.PEG-IFN !"2a
+riba 800 mgNone
PegIntron®+ Rebetol® WBD
Maintenance Tx. PEG-IFN !"2a
90 #g
PegIntron®0.5 µg/kg
PegIntron®0.5 µg/kg
Maintenance Control Placebo Colchicine Observation
TreatmentDuration (years) 3.5 4 3-5
RecruitmentStatus Complete Mid-point Analysis Complete
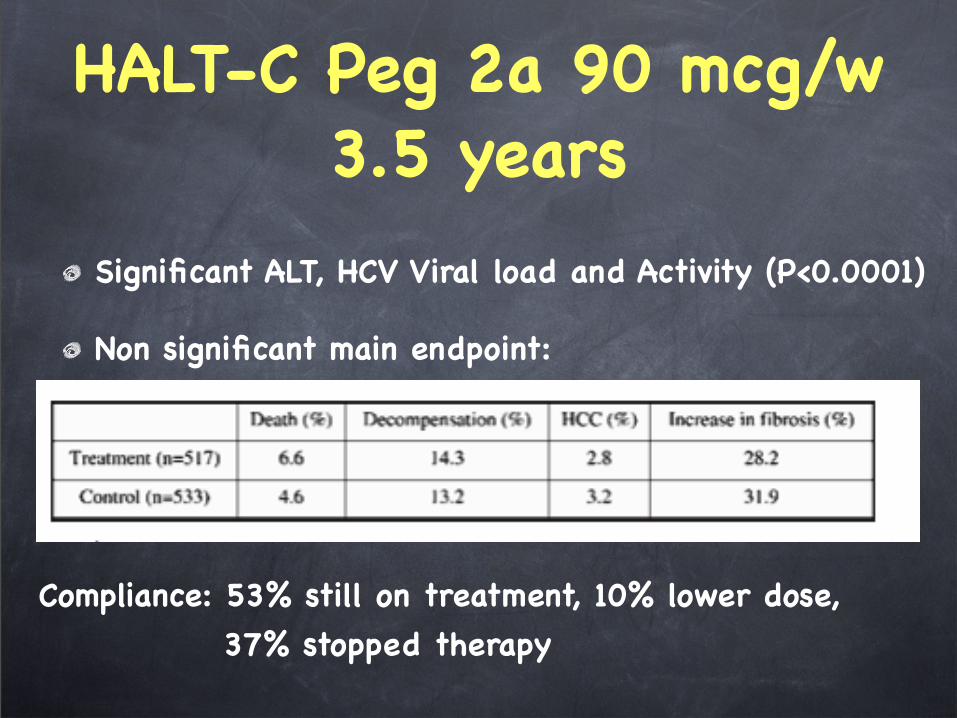
HALT-C Peg 2a 90 mcg/w3.5 years
Significant ALT, HCV Viral load and Activity (P<0.0001)
Non significant main endpoint:
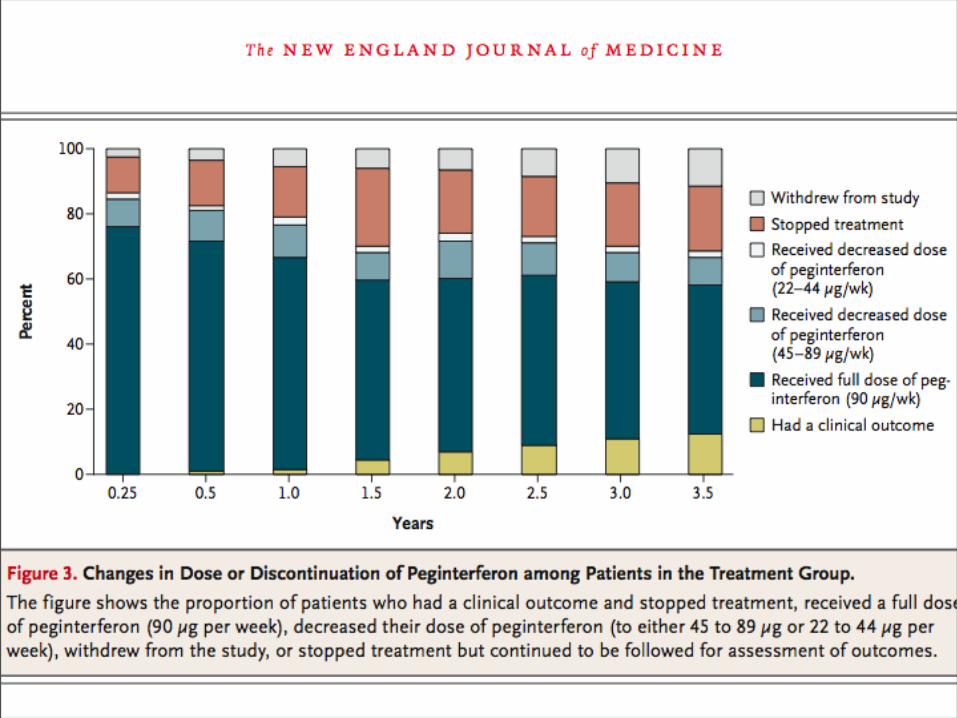
Compliance: 53% still on treatment, 10% lower dose,
37% stopped therapy
64
Maintenance Therapy TrialsHALT-C COPILOT EPIC3
Patients Ishak 4-6 Ishak 3 – 6 Metavir 2 –4
N 1000 800 2200 (3 studies)
End-point Fibrosis/Clinical Fibrosis /Clinical Fibrosis/Clinical
Initial Tx.PEG-IFN !"2a
+riba 800 mgNone
PegIntron®+ Rebetol® WBD
Maintenance Tx. PEG-IFN !"2a
90 µg
PegIntron®0.5 µg/kg
PegIntron®0.5 µg/kg
Maintenance Control Placebo Colchicine Observation
TreatmentDuration (years)
3.5 4 3-5
RecruitmentStatus
Complete Mid-point Analysis Enrolling
65
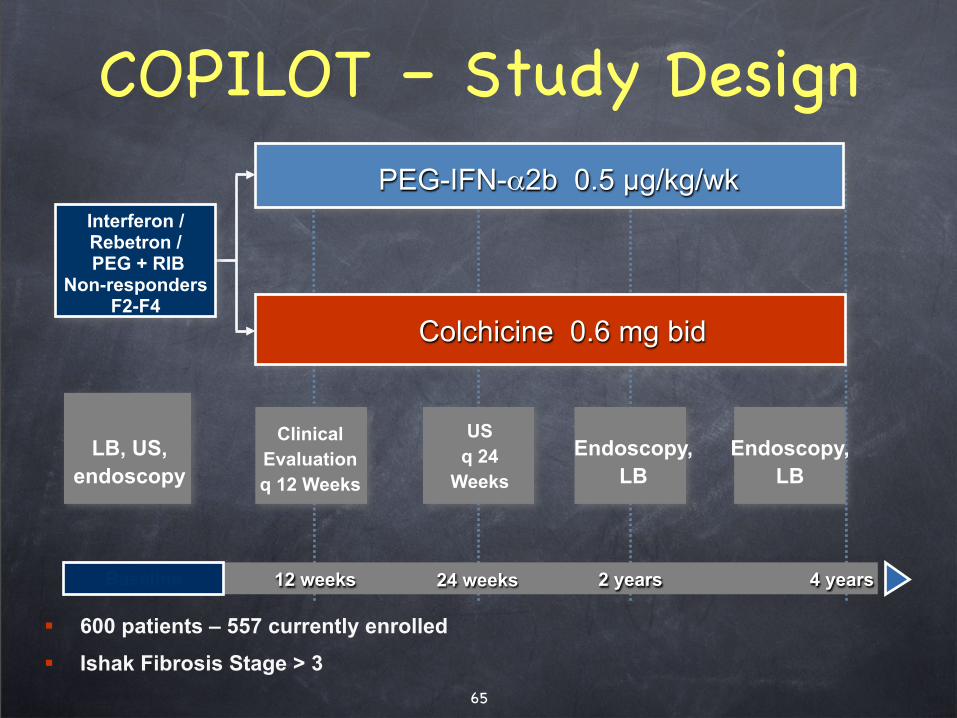
Colchicine 0.6 mg bid
LB, US,
endoscopy
PEG-IFN-!2b 0.5 !g/kg/wk
Clinical
Evaluation
q 12 Weeks
US
q 24
Weeks
Endoscopy,
LB
Endoscopy,
LB
Interferon /Rebetron / PEG + RIB
Non-respondersF2-F4
5 JahreBaseline 12 weeks 24 weeks 2 years 4 years
COPILOT – Study Design
! 600 patients – 557 currently enrolled
! Ishak Fibrosis Stage > 3
66
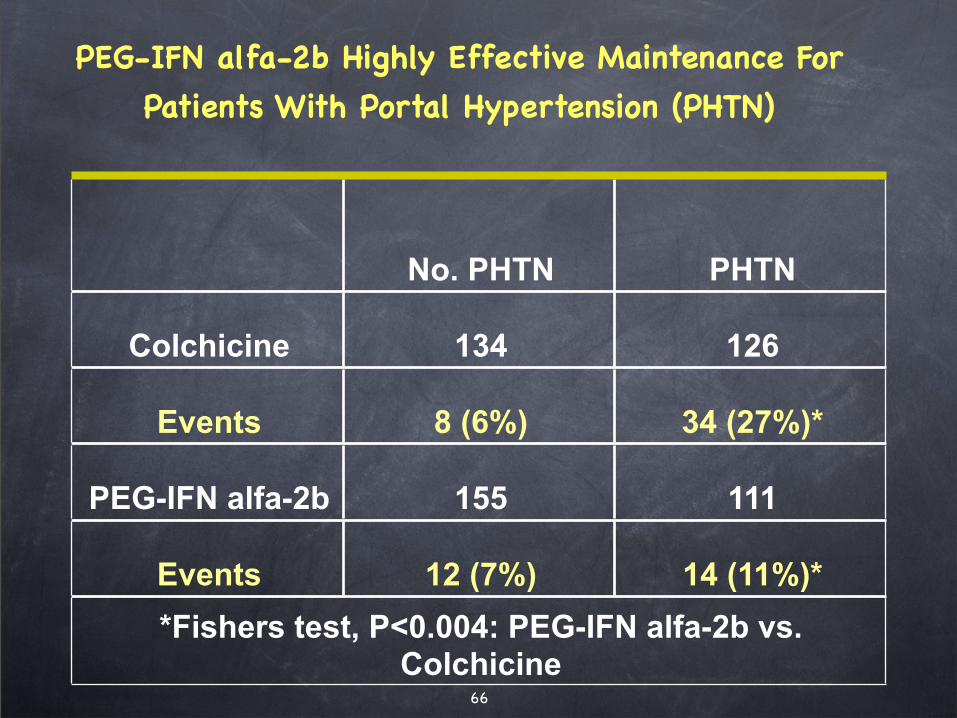
PEG-IFN alfa-2b Highly Effective Maintenance For
Patients With Portal Hypertension (PHTN)
No. PHTN PHTN
Colchicine 134 126
Events 8 (6%) 34 (27%)*
PEG-IFN alfa-2b 155 111
Events 12 (7%) 14 (11%)*
*Fishers test, P<0.004: PEG-IFN alfa-2b vs. Colchicine
67
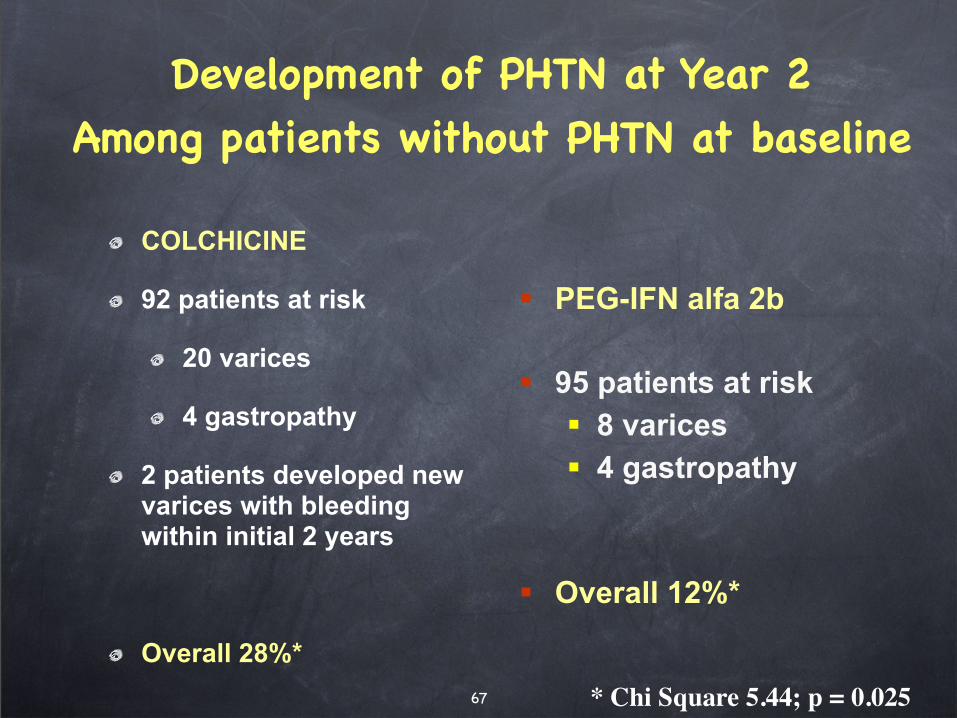
Development of PHTN at Year 2Among patients without PHTN at baseline
COLCHICINE
92 patients at risk
20 varices
4 gastropathy
2 patients developed new varices with bleeding within initial 2 years
Overall 28%*
! PEG-IFN alfa 2b
! 95 patients at risk
! 8 varices
! 4 gastropathy
! Overall 12%*
* Chi Square 5.44; p = 0.025
68
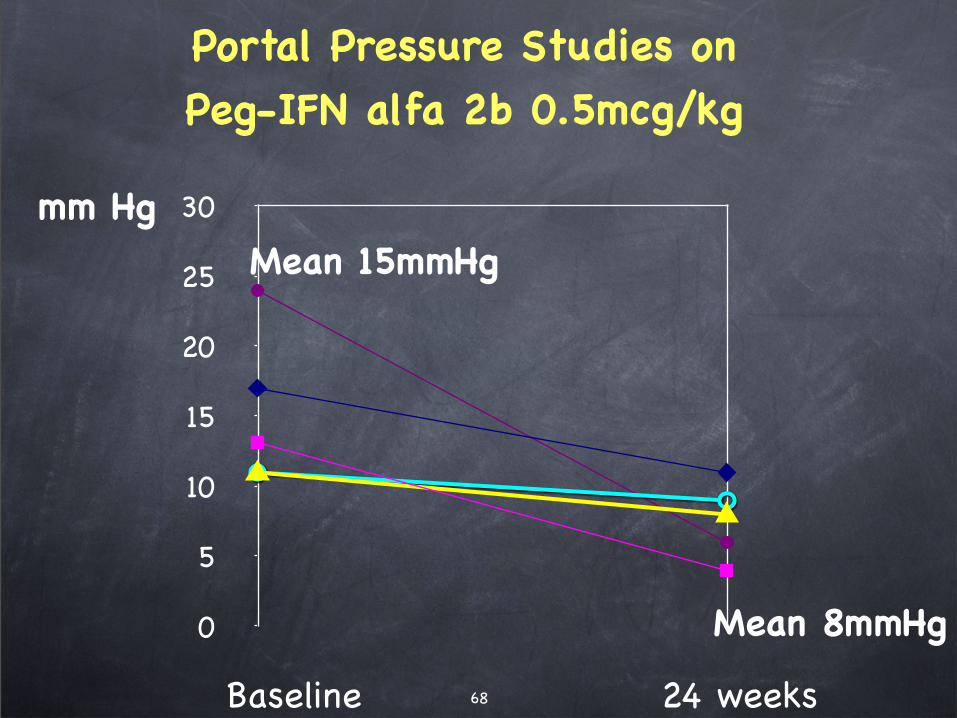
Portal Pressure Studies on Peg-IFN alfa 2b 0.5mcg/kg
0
5
10
15
20
25
30mm Hg
Baseline 24 weeks
Mean 15mmHg
Mean 8mmHg
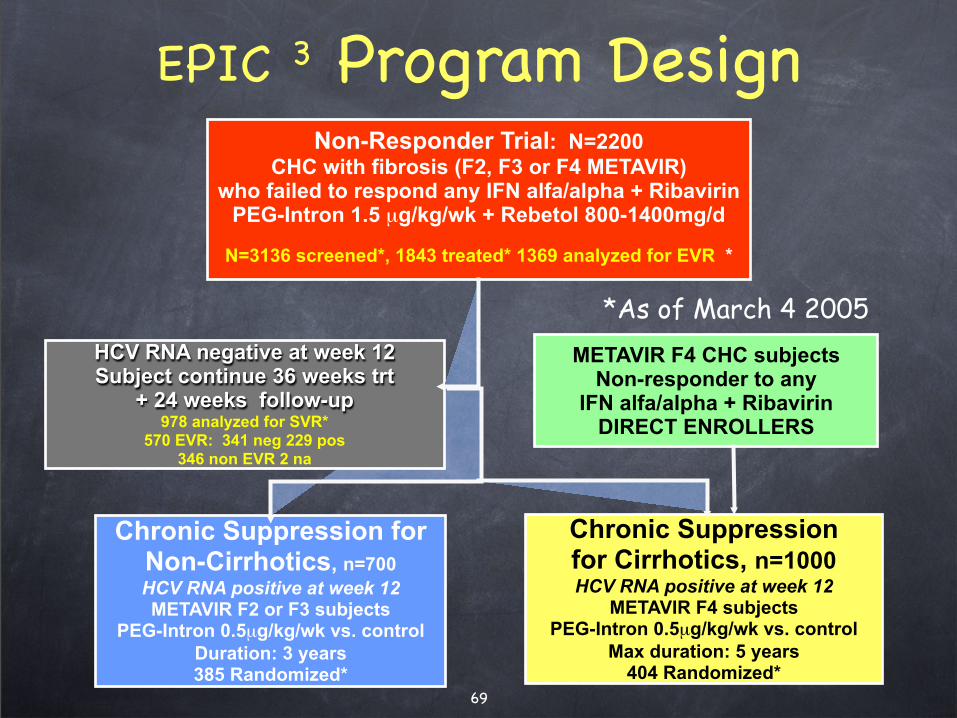
Chronic Suppression for Non-Cirrhotics, n=700
HCV RNA positive at week 12METAVIR F2 or F3 subjects
PEG-Intron 0.5µg/kg/wk vs. control
Duration: 3 years385 Randomized*
69
EPIC 3 Program DesignNon-Responder Trial: N=2200
CHC with fibrosis (F2, F3 or F4 METAVIR) who failed to respond any IFN alfa/alpha + Ribavirin
PEG-Intron 1.5 µg/kg/wk + Rebetol 800-1400mg/d
N=3136 screened*, 1843 treated* 1369 analyzed for EVR *
HCV RNA negative at week 12Subject continue 36 weeks trt
+ 24 weeks follow-up978 analyzed for SVR*
570 EVR: 341 neg 229 pos346 non EVR 2 na
Chronic Suppression for Cirrhotics, n=1000HCV RNA positive at week 12
METAVIR F4 subjects PEG-Intron 0.5µg/kg/wk vs. control
Max duration: 5 years404 Randomized*
METAVIR F4 CHC subjects Non-responder to any
IFN alfa/alpha + Ribavirin DIRECT ENROLLERS
*As of March 4 2005
16 janv. 2009
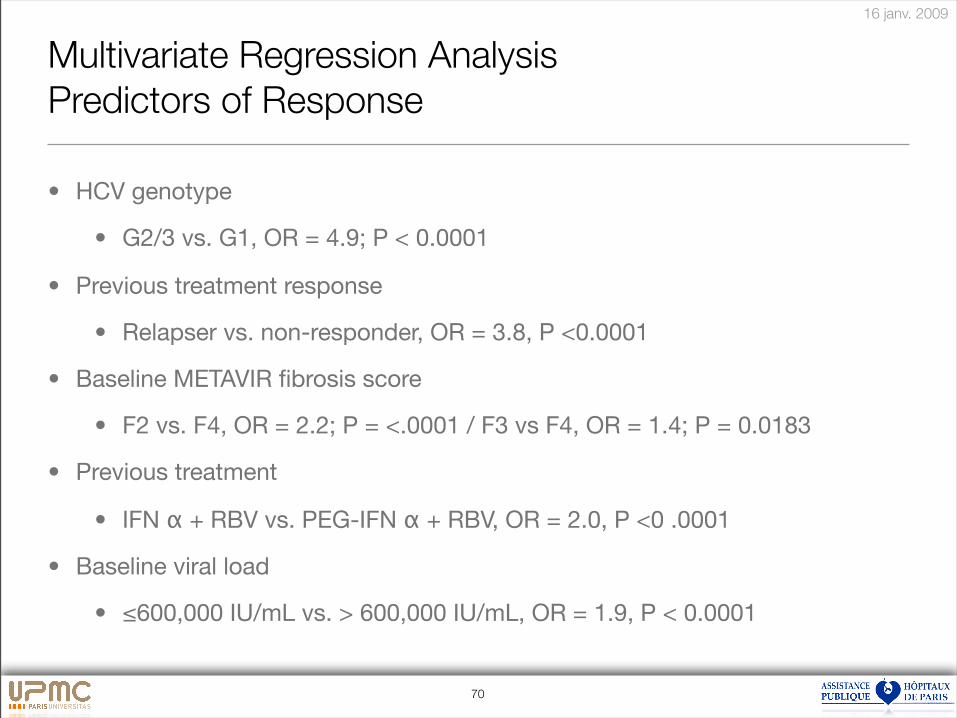
70
Multivariate Regression Analysis
Predictors of Response
• HCV genotype
• G2/3 vs. G1, OR = 4.9; P < 0.0001
• Previous treatment response
• Relapser vs. non-responder, OR = 3.8, P <0.0001
• Baseline METAVIR fibrosis score
• F2 vs. F4, OR = 2.2; P = <.0001 / F3 vs F4, OR = 1.4; P = 0.0183
• Previous treatment
• IFN ! + RBV vs. PEG-IFN ! + RBV, OR = 2.0, P <0 .0001
• Baseline viral load
• "600,000 IU/mL vs. > 600,000 IU/mL, OR = 1.9, P < 0.0001
16 janv. 2009
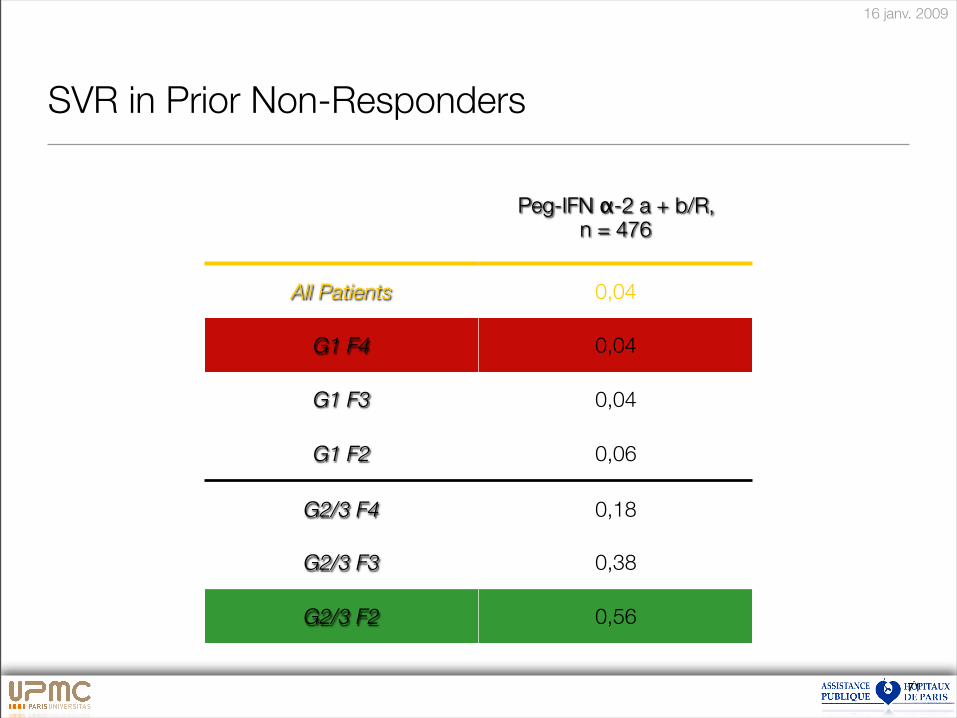
71
SVR in Prior Non-Responders
Peg-IFN !-2 a + b/R,n = 476
All Patients 0,04
G1 F4 0,04
G1 F3 0,04
G1 F2 0,06
G2/3 F4 0,18
G2/3 F3 0,38
G2/3 F2 0,56
16 janv. 2009
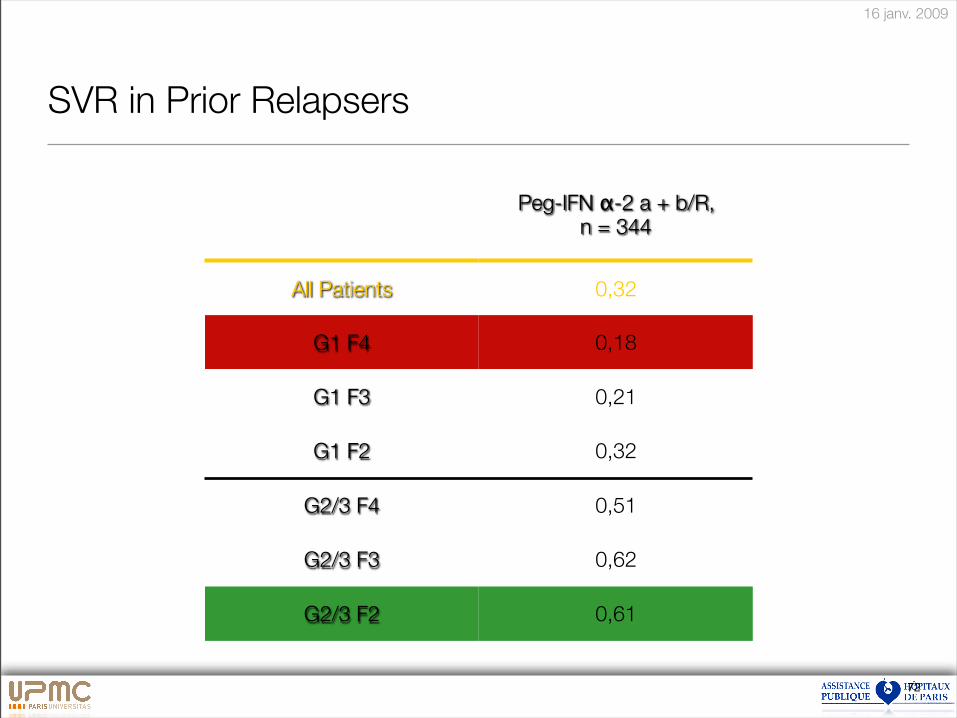
72
SVR in Prior Relapsers
Peg-IFN !-2 a + b/R,n = 344
All Patients 0,32
G1 F4 0,18
G1 F3 0,21
G1 F2 0,32
G2/3 F4 0,51
G2/3 F3 0,62
G2/3 F2 0,61
16 janv. 2009
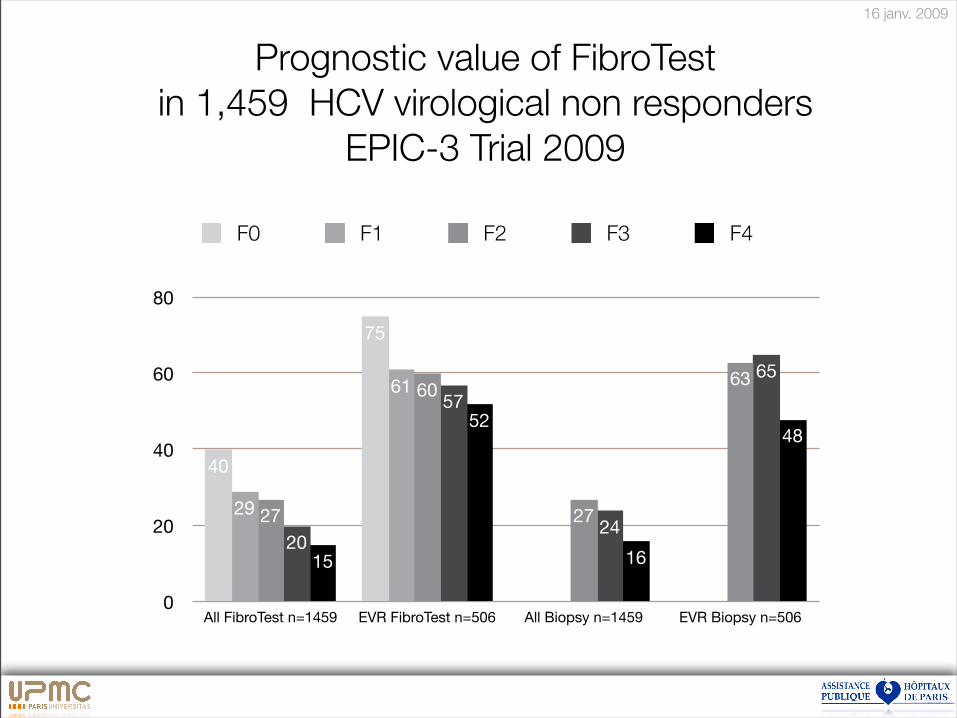
0
20
40
60
80
All FibroTest n=1459 EVR FibroTest n=506 All Biopsy n=1459 EVR Biopsy n=506
48
16
52
15
65
24
57
20
63
27
60
27
61
29
75
40
F0 F1 F2 F3 F4
Prognostic value of FibroTest
in 1,459 HCV virological non responders
EPIC-3 Trial 2009
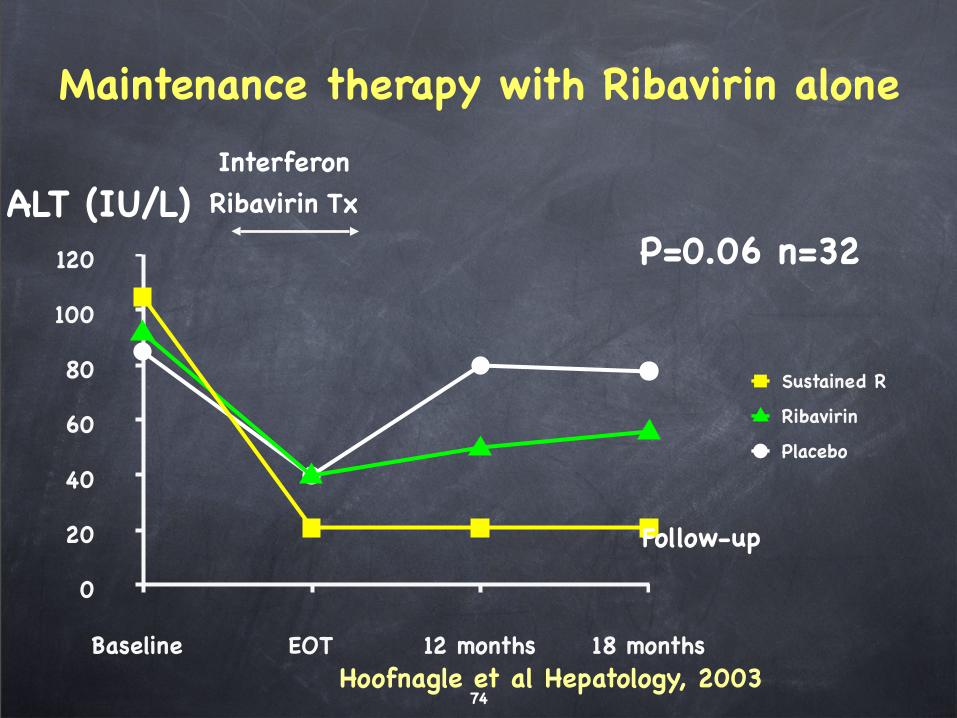
74
Maintenance therapy with Ribavirin alone
0
20
40
60
80
100
120
Baseline EOT 12 months 18 months
Sustained R
Ribavirin
Placebo
Hoofnagle et al Hepatology, 2003
Interferon
Ribavirin Tx
Follow-up
P=0.06 n=32ALT (IU/L)
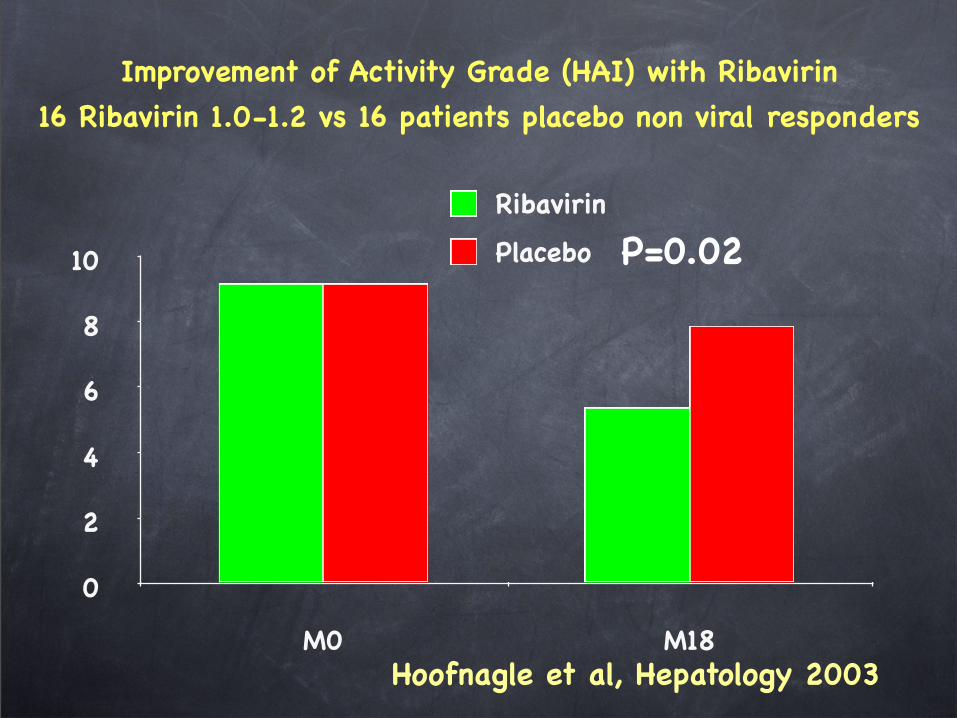
Improvement of Activity Grade (HAI) with Ribavirin
16 Ribavirin 1.0-1.2 vs 16 patients placebo non viral responders
0
2
4
6
8
10
M0 M18
Ribavirin
Placebo
Hoofnagle et al, Hepatology 2003
P=0.02
16 janv. 2009
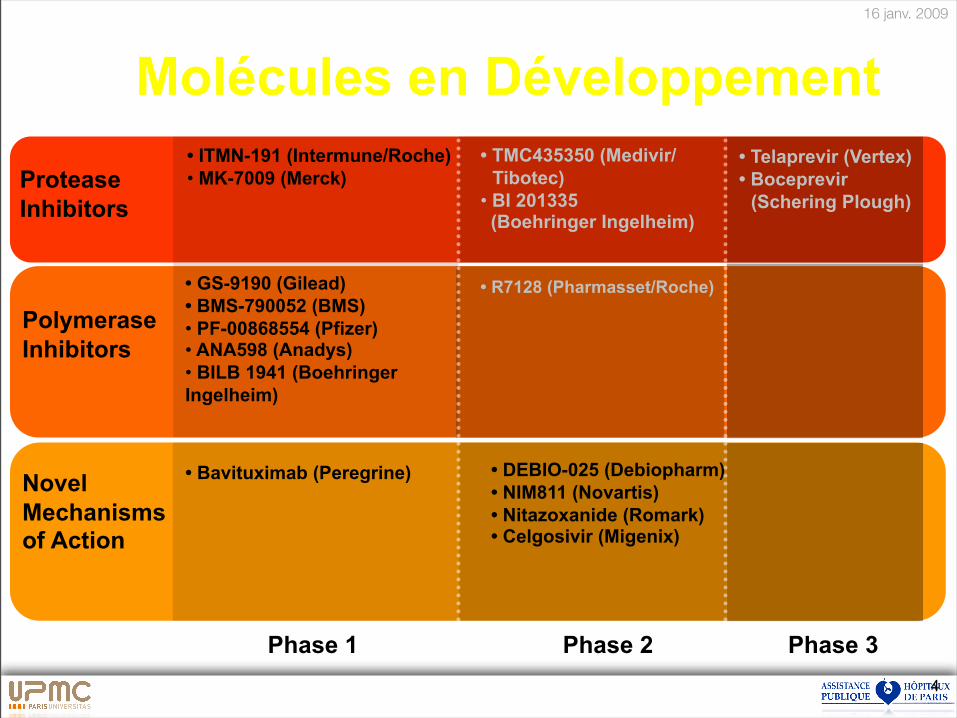
4
Molécules en Développement
Phase 1 Phase 3 Phase 2
Protease
Inhibitors
Polymerase
Inhibitors
• Telaprevir (Vertex)
• Boceprevir
(Schering Plough)
Novel
Mechanisms of Action
• ITMN-191 (Intermune/Roche)
•!MK-7009 (Merck)
• GS-9190 (Gilead)
• BMS-790052 (BMS)
•! PF-00868554 (Pfizer) •! ANA598 (Anadys)
•! BILB 1941 (Boehringer
Ingelheim)
• Bavituximab (Peregrine)
• TMC435350 (Medivir/
Tibotec)
•!BI 201335 (Boehringer Ingelheim)
• R7128 (Pharmasset/Roche)
• DEBIO-025 (Debiopharm)
• NIM811 (Novartis)
• Nitazoxanide (Romark) • Celgosivir (Migenix)
16 janv. 2009
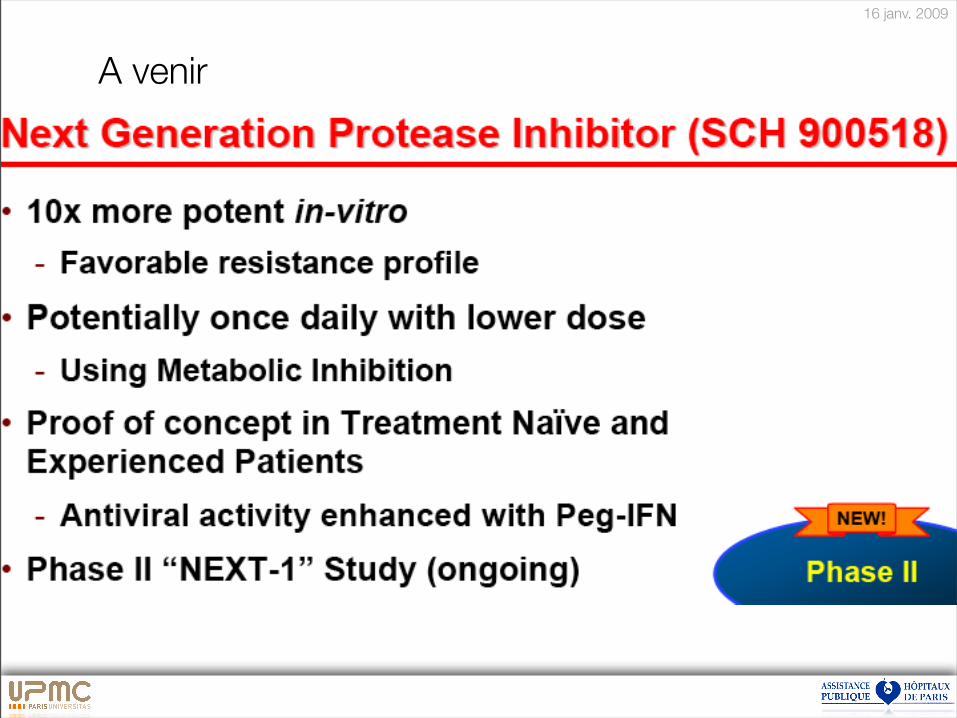
A venir
16 janv. 2009
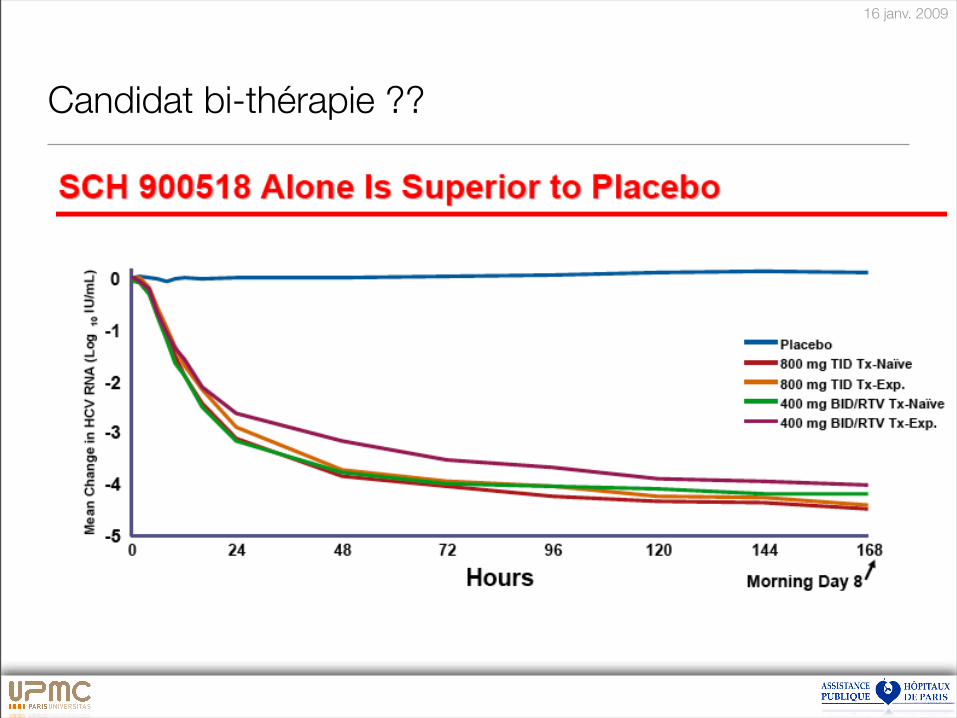
Candidat bi-thérapie ??
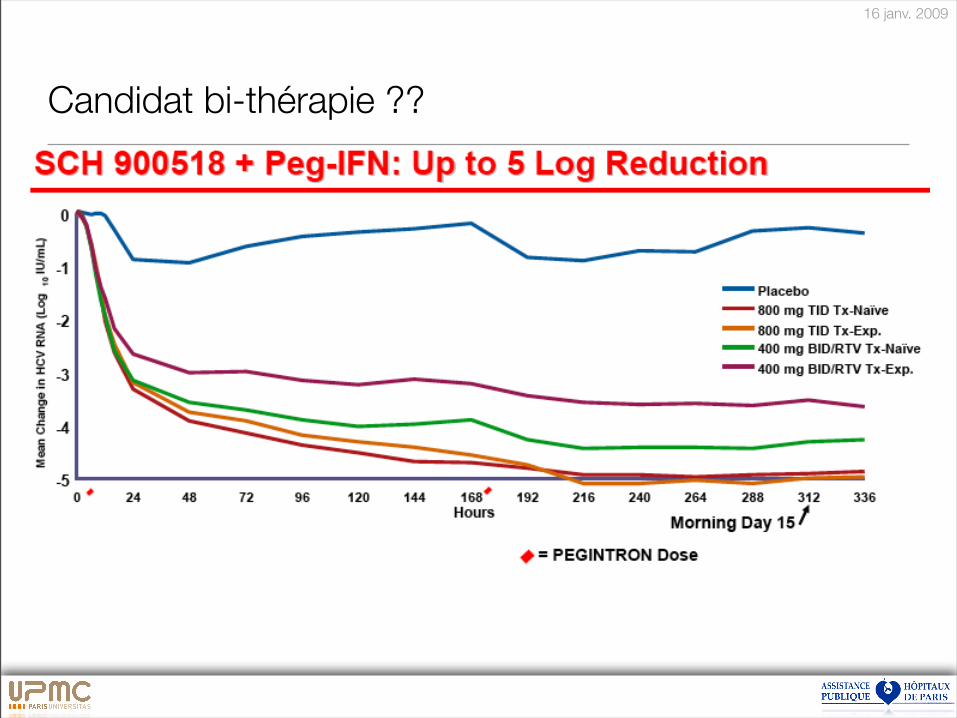
16 janv. 2009
Candidat bi-thérapie ??
80
Traitement hépatite C 2009
Intensifier dépistage
Simplifier bilan initial et suivi
Traiter «!à la carte!»:
• Fibrose, Poids, Stéatose, Age
Tolérance
Efficacité non virologique:
• Freiner la progression de la Fibrose
81
Difficult to treat patientsAdverse events
Coinfected HIV
Cirrhotic
Aged patients
Uremic
Hemophiliac
Thalassemic
Anemic
Neutopenic
Thrombopenic
IV drug user
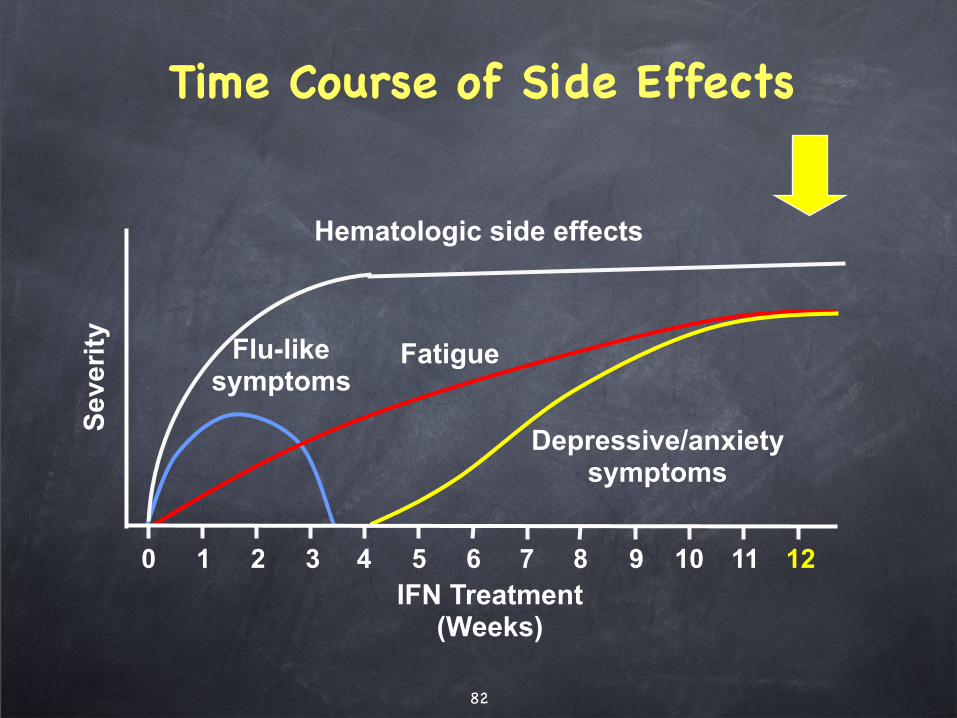
82
0 4 5 11 12
IFN Treatment (Weeks)
Severi
tyTime Course of Side Effects
6 7 8 9 101 2 3
FatigueFlu-likesymptoms
Depressive/anxietysymptoms
Hematologic side effects
83
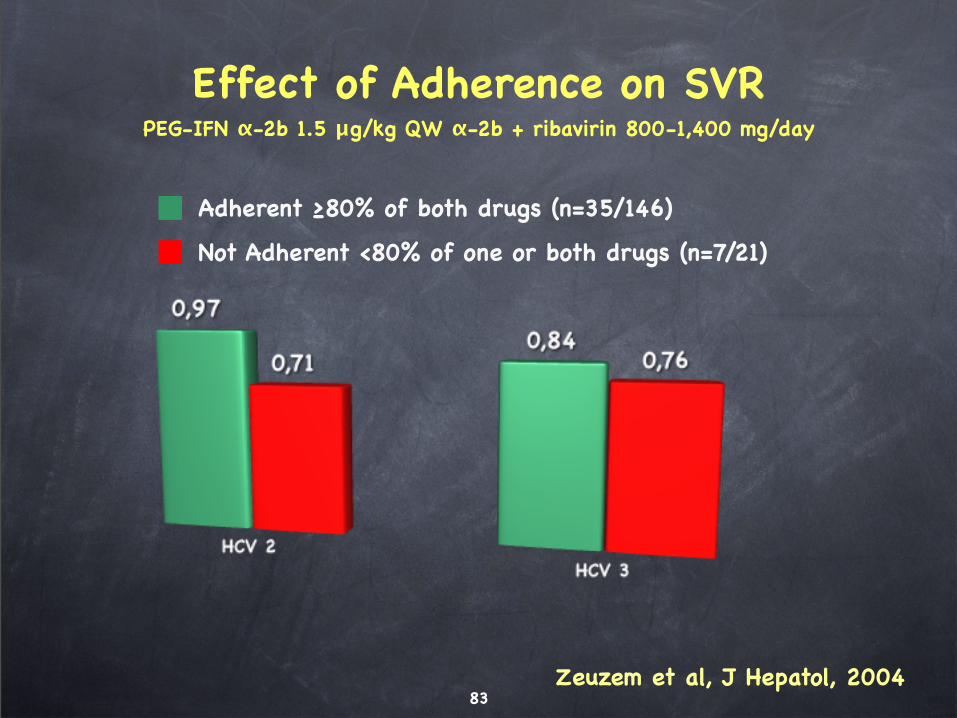
Adherent "80% of both drugs (n=35/146)
Not Adherent <80% of one or both drugs (n=7/21)
Effect of Adherence on SVRPEG-IFN !-2b 1.5 #g/kg QW !-2b + ribavirin 800-1,400 mg/day
Zeuzem et al, J Hepatol, 2004
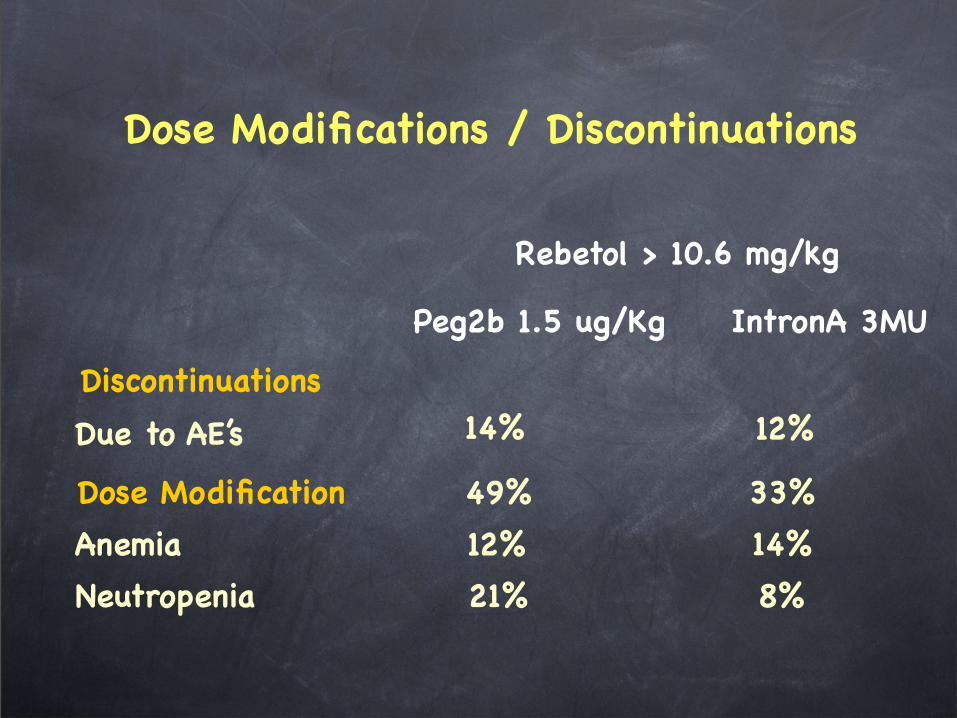
Dose Modifications / Discontinuations
Rebetol > 10.6 mg/kg
Peg2b 1.5 ug/Kg IntronA 3MU
Discontinuations
Dose Modification
14% 12%
49% 33%
Anemia
Neutropenia
12% 14%
21% 8%
Due to AE’s
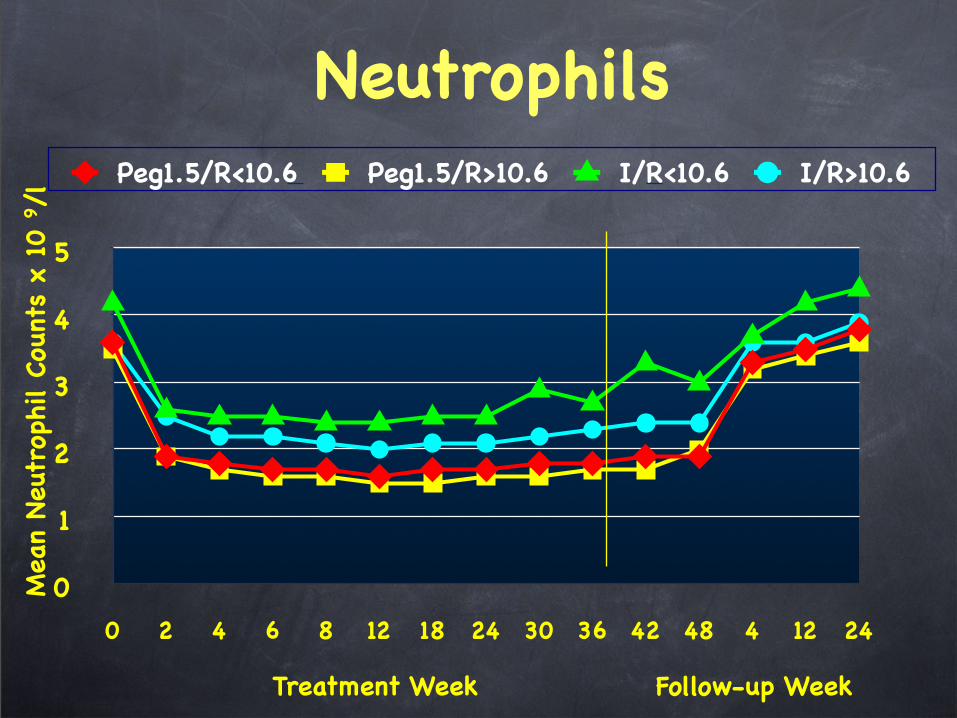
Neutrophils
0
1
2
3
4
5
0 2 4 6 8 12 18 24 30 36 42 48 4 12 24
Peg1.5/R<10.6 Peg1.5/R>10.6 I/R<10.6 I/R>10.6
Treatment Week Follow-up Week
Mea
n Neu
trop
hil Cou
nts
x 10
9/l
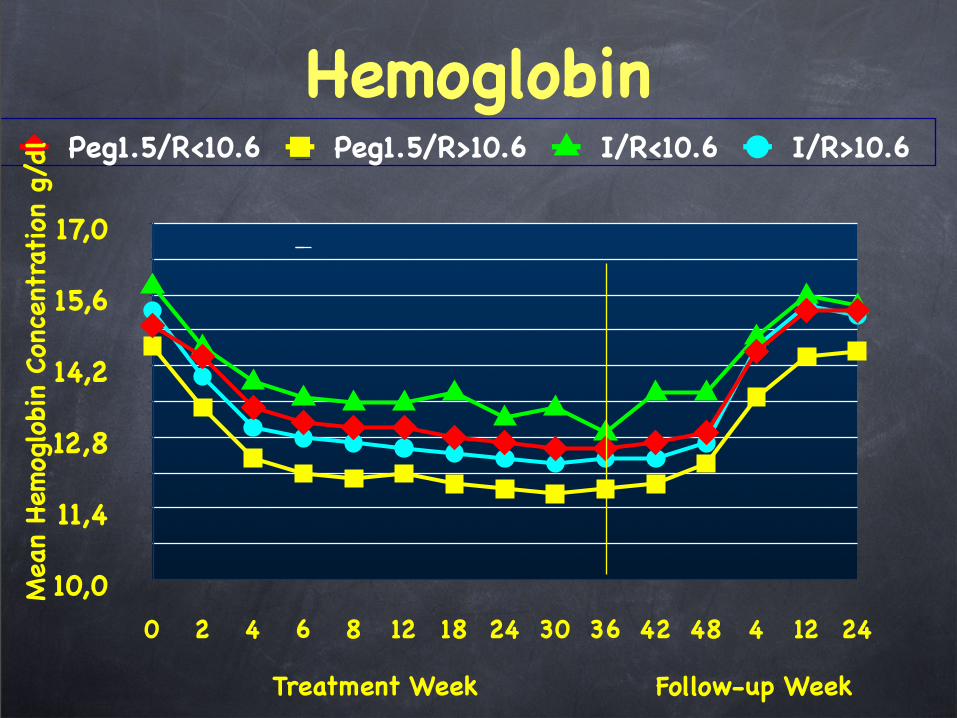
Hemoglobin
10,0
11,4
12,8
14,2
15,6
17,0
0 2 4 6 8 12 18 24 30 36 42 48 4 12 24
Peg1.5/R<10.6 Peg1.5/R>10.6 I/R<10.6 I/R>10.6
Treatment Week Follow-up Week
Mea
n Hem
oglobi
n Con
cent
ration
g/d
l
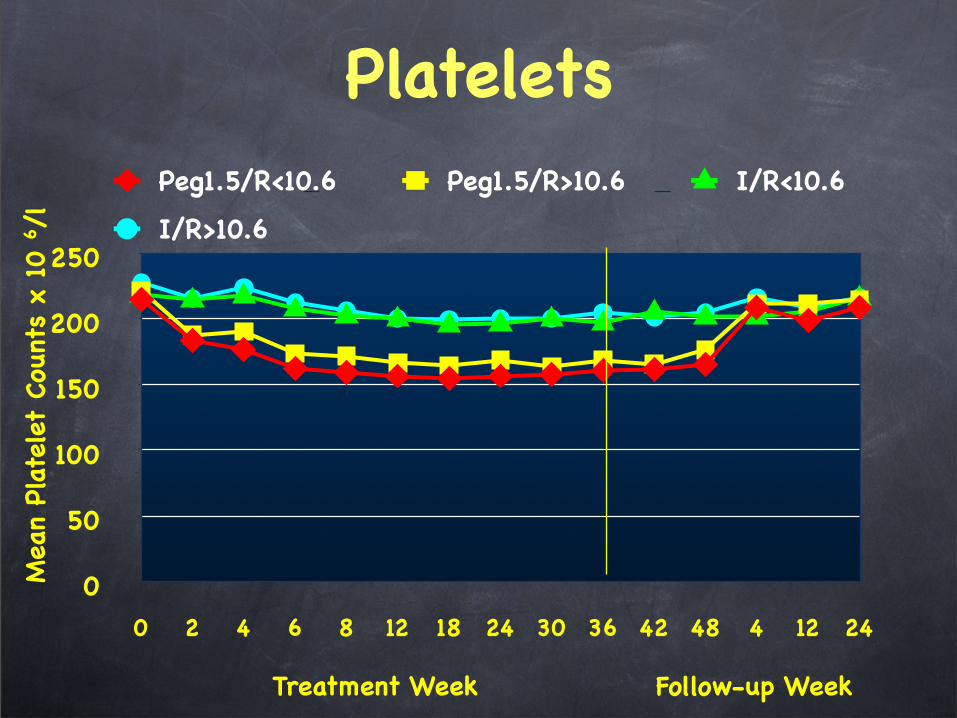
Platelets
0
50
100
150
200
250
0 2 4 6 8 12 18 24 30 36 42 48 4 12 24
Peg1.5/R<10.6 Peg1.5/R>10.6 I/R<10.6
I/R>10.6
Treatment Week Follow-up Week
Mea
n Pl
atelet
Cou
nts
x 10
6/l
88
Hepatitis C Virus-Infected Patients ReportCommunication Problems With Physicians
Susan Zickmund, Stephen L. Hillis, Mitchell J.
Barnett, Laura Ippolito, and Douglas R. LaBrecque
Hepatology 2004;39:999 –1007
89
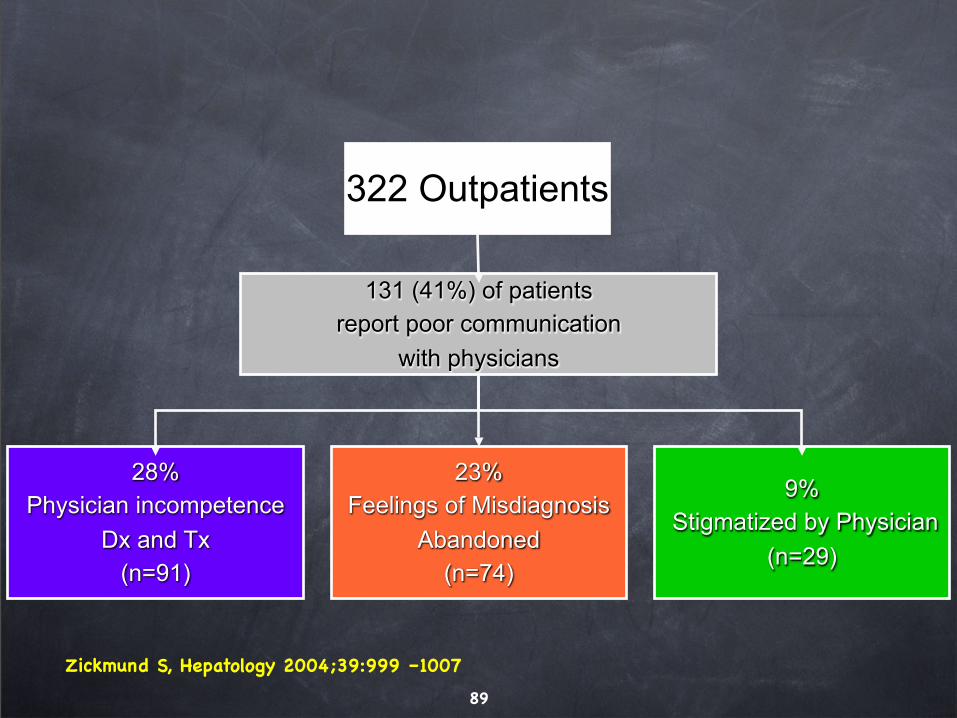
322 Outpatients
131 (41%) of patients
report poor communication
with physicians
28%
Physician incompetence
Dx and Tx
(n=91)
23%
Feelings of Misdiagnosis
Abandoned
(n=74)
9%
Stigmatized by Physician
(n=29)
Zickmund S, Hepatology 2004;39:999 –1007
90
Difficult to treat patientsAdverse events
Coinfected HIV
Cirrhotic
Aged patients
Uremic
Hemophiliac
Thalassemic
Anemic
Neutopenic
Thrombopenic
IV drug user
91
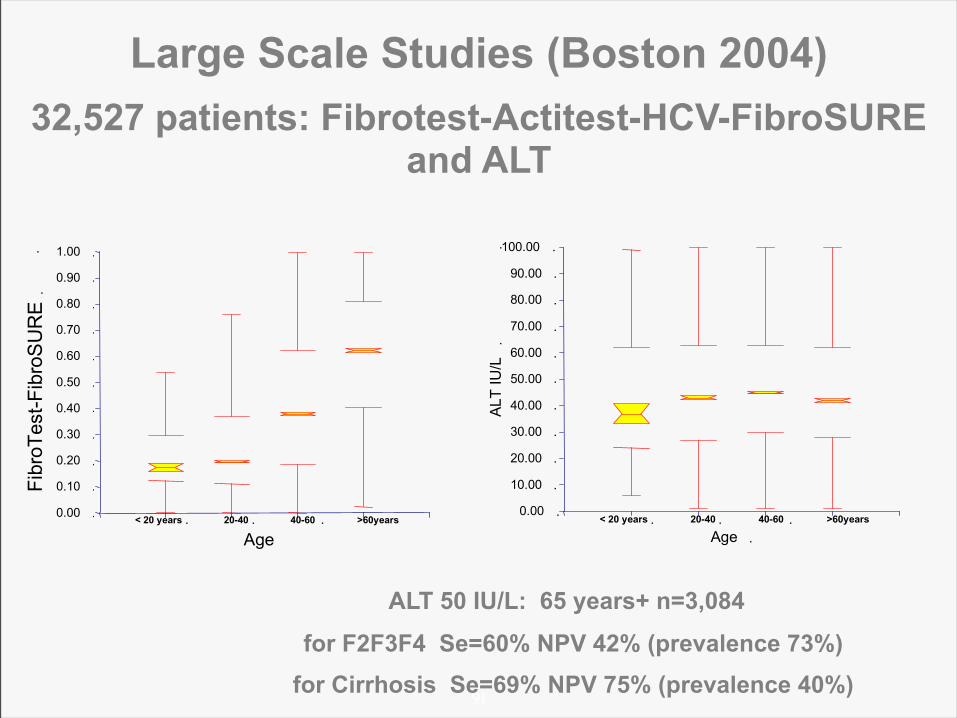
Large Scale Studies (Boston 2004)
32,527 patients: Fibrotest-Actitest-HCV-FibroSURE and ALT
ALT 50 IU/L: 65 years+ n=3,084
for F2F3F4 Se=60% NPV 42% (prevalence 73%)
for Cirrhosis Se=69% NPV 75% (prevalence 40%)
92
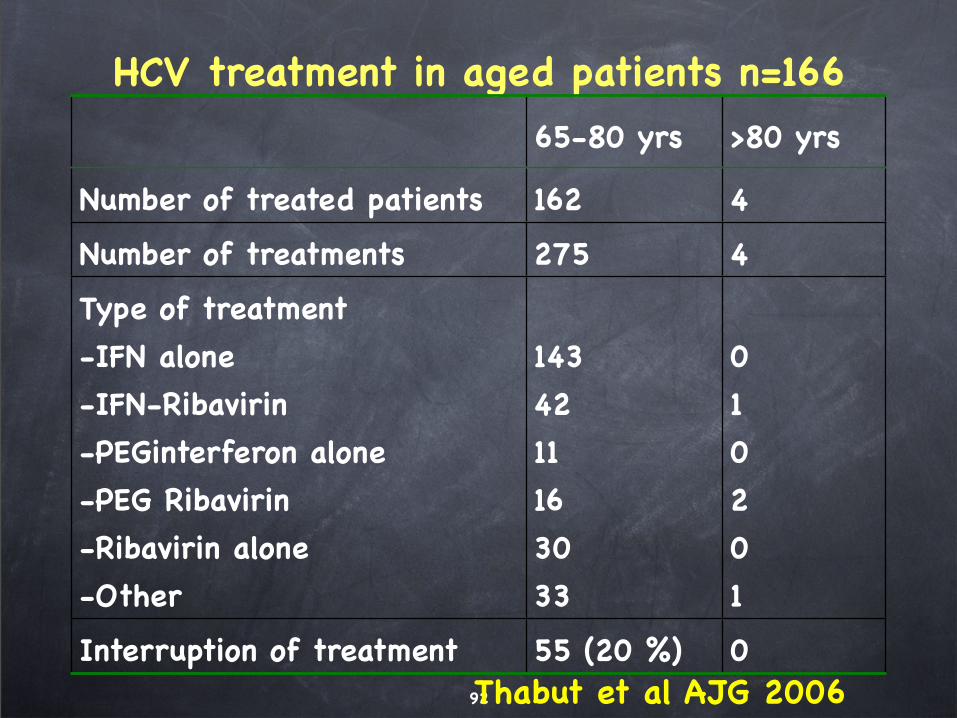
HCV treatment in aged patients n=166
65-80 yrs >80 yrs
Number of treated patients 162 4
Number of treatments 275 4
Type of treatment
-IFN alone
-IFN-Ribavirin
-PEGinterferon alone
-PEG Ribavirin
-Ribavirin alone
-Other
143
42
11
16
30
33
0
1
0
2
0
1
Interruption of treatment 55 (20 %) 0Thabut et al AJG 2006
93
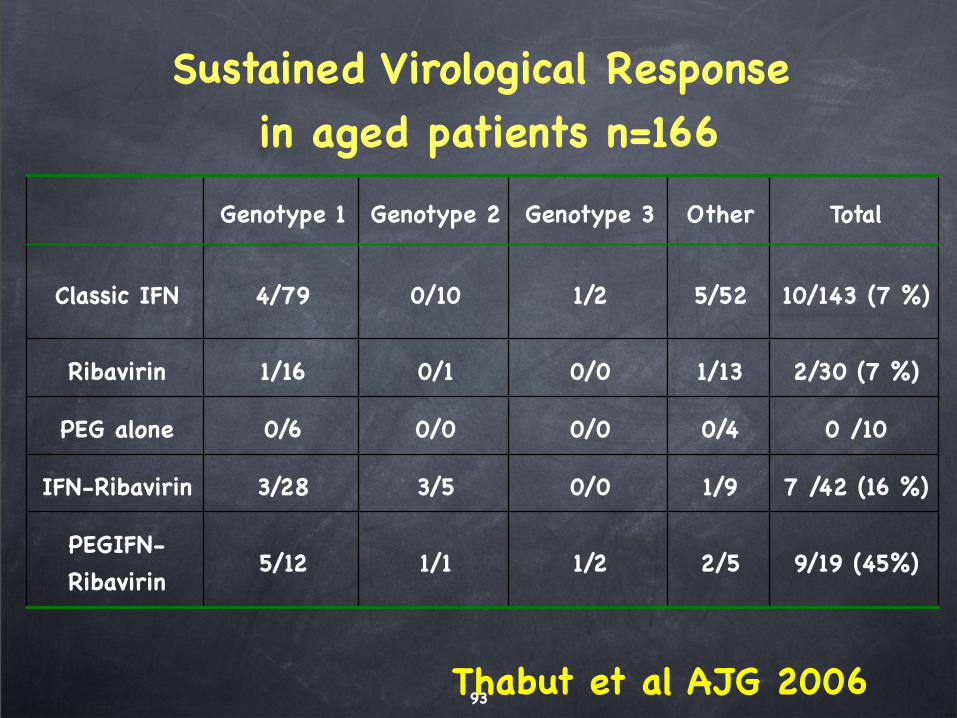
Genotype 1 Genotype 2 Genotype 3 Other Total
Classic IFN 4/79 0/10 1/2 5/52 10/143 (7 %)
Ribavirin 1/16 0/1 0/0 1/13 2/30 (7 %)
PEG alone 0/6 0/0 0/0 0/4 0 /10
IFN-Ribavirin 3/28 3/5 0/0 1/9 7 /42 (16 %)
PEGIFN-
Ribavirin5/12 1/1 1/2 2/5 9/19 (45%)
Sustained Virological Response in aged patients n=166
Thabut et al AJG 2006
94
Difficult to treat patientsAdverse events
Coinfected HIV
Cirrhotic
Aged patients
Uremic
Hemophiliac
Thalassemic
Anemic
Neutopenic
Thrombopenic
IV drug user
95
Difficult to treat patientsAdverse events
Coinfected HIV
Cirrhotic
Aged patients
Uremic
Hemophiliac
Thalassemic
Anemic
Neutopenic
Thrombopenic
IV drug user
96
Renal Diseases
Renal insufficiency
Hemodialysis
Renal transplantation
97
Renal insufficiency
IFN, PEG-IFN:
Same dose or slightly reduced
Ribavirin:
Adjusted plasma concentration ?,
• 10-15 micromol/L ?
Start 200mg per week
• Range 170-300 mg/day
EPO: 20,000-30,000 UI/week
98
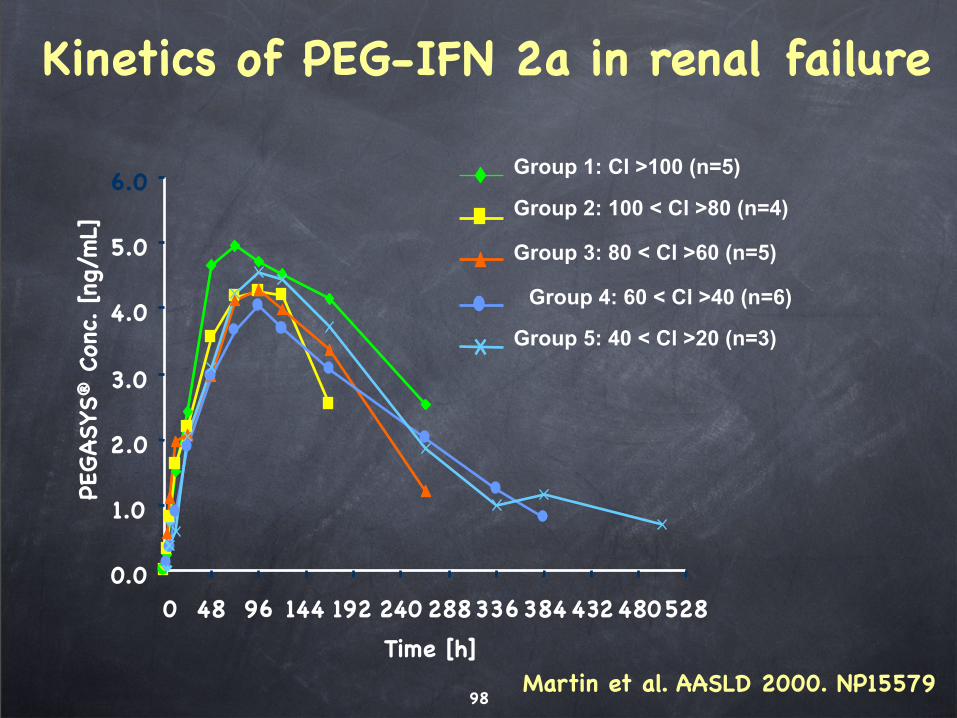
0.0
1.0
2.0
3.0
4.0
5.0
6.0
0 48 96 144 192 240 288336384432480528
Time [h]
PEGASYS
® C
onc. [ng
/mL]
Group 1: Cl >100 (n=5)
Group 2: 100 < Cl >80 (n=4)
Group 3: 80 < Cl >60 (n=5)
Group 4: 60 < Cl >40 (n=6)
Group 5: 40 < Cl >20 (n=3)
Martin et al. AASLD 2000. NP15579
Kinetics of PEG-IFN 2a in renal failure
99
Renal insufficiencyIFN, PEG-IFN:
Same dose or slightly reduced
Ribavirin:
Adjusted plasma concentration ?,
• 10-15 micromol/L ?
Start 200mg per week
• Range 170-300 mg/day
EPO: 20,000-30,000 UI/week
100
Renal Diseases
Renal insufficiency
Hemodialysis
Renal transplantation
101
Interferon alfa for HCV infection in hemodialyzed
INF alfa is feasable in dialysis patients
Poorly tolerated
• discontinuation: 20-40%;
• reduction: 60%
Efficient: at least as efficient than in the general population (pharmacokinetic of INF)
Frequent histological improvement
102
Ribavirin in Hemodialyzed
Warning Hemolysis +++
increased risk despite the absence of variation of the level of serum ribavirin
long duration of the risk; accumulation of metabolites in erythrocytes
Particularly with aziathioprine
Low doses of ribavirin
200 mg after each dialysis
200 daily
Increased doses of EPOThervet et al. Transplantation 1994
Thevenot et al. JVH 1997
103
Interferon and Ribavirin in Hemodialyzed
Associated (synergistic effect?) with IFN or PEG-IFN
Low doses of ribavirin
200 mg after each dialysis
200 daily
Increased doses of EPO
# Tang et al. J Hepatol 2003
Park J et al. DDW 2005
Personal experience 25 cases 40% SVR
104
Renal Diseases
Renal insufficiency
Hemodialysis
Renal transplantation
105
Summary
Treatment options in HCV patients with Renal disorders
No Transplantation Scheduled:
As in non uremic:
• F0F1: Follow-up FibroTest /12mo or biopsy /3y
• F1-F2: FibroTest /6mo or biopsy /y
• F2F3F4: Treatment A la Carte
Transplantion Scheduled:
• Treatment A la Carte as soon as possible
• Double transplantation in F4 non-responders
Transplanted:
• F0F1: Follow-up FibroTest /12mo or biopsy /3y
• F1-F2: FibroTest /6mo or biopsy /y
• F2F3F4:
– Ribavirin
– Liver Transplantation in F4 non-responders
106
Conclusions
Prevention of hepatitis in renal diseases
Treatment “A la Carte” feasible and effective before transplantation
Treatment limited after transplantation
107
Difficult to treat patientsAdverse events
Coinfected HIV
Cirrhotic
Aged patients
Uremic
Hemophiliac
Thalassemic
Anemic
Neutropenic
Thrombopenic
IV drug user
Hemophiliac Patients
Massively contaminated,
Coinfection HIV,
Same natural history,
Biopsy worse cost-benefit rate
Same treatments, including transplantation
Same results than in non-hemophiliacs
Thalassemic PatientsMassively contaminated,
Progression of fibrosis
• Iron overload
• Insulin-resistance
Same treatments, including bone marrow transplantation
Blood transfusion sometimes needed
Anemic PatientsRibavirin dose dependent reversible hemolytic anemia
Erythropoietin (epoetin alfa)
• 40,000 U/week vs standard
• Hemoglobin drop: 0.3 g vs 2.9 g/dL
• 900 vs 700 mg/day ribavirin
• When to start ?
–Anemic at baseline <11g Hb?
–During treatment if <11g Hb ?
Neutropenic PatientsGranulocyte colony-stimulating factor (G-CSF)
• Potentiates effect of EPO
• 300 microG SC 1-3 / week
• Maintain Neutrophils >750/mm3
• Adverse events
– Skin rash
– Vasculatis
– Bone pain, myalgia
– Thrombocytopenia, splenomegaly
– Leukemoid reaction
– Exacerbation of psoriasis
Thrombopenic Patients
Problematic in cirrhotic patients
Severe thrombopenia exceptional in non cirrhotic
Thrombopoietin
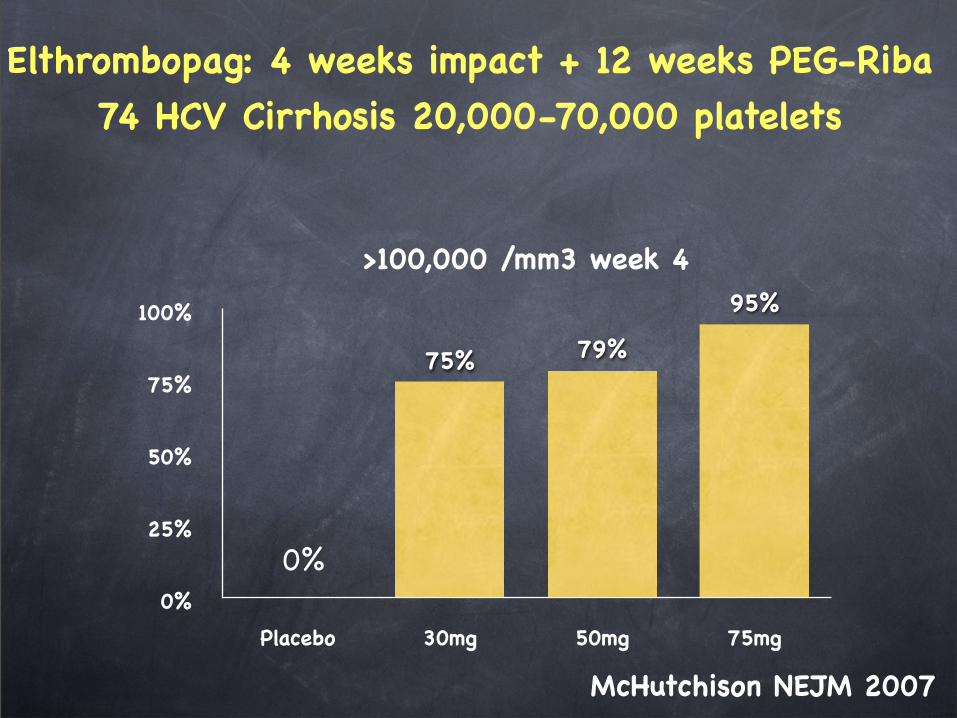
0%
25%
50%
75%
100%
Placebo 30mg 50mg 75mg
95%
79%75%
>100,000 /mm3 week 4
McHutchison NEJM 2007
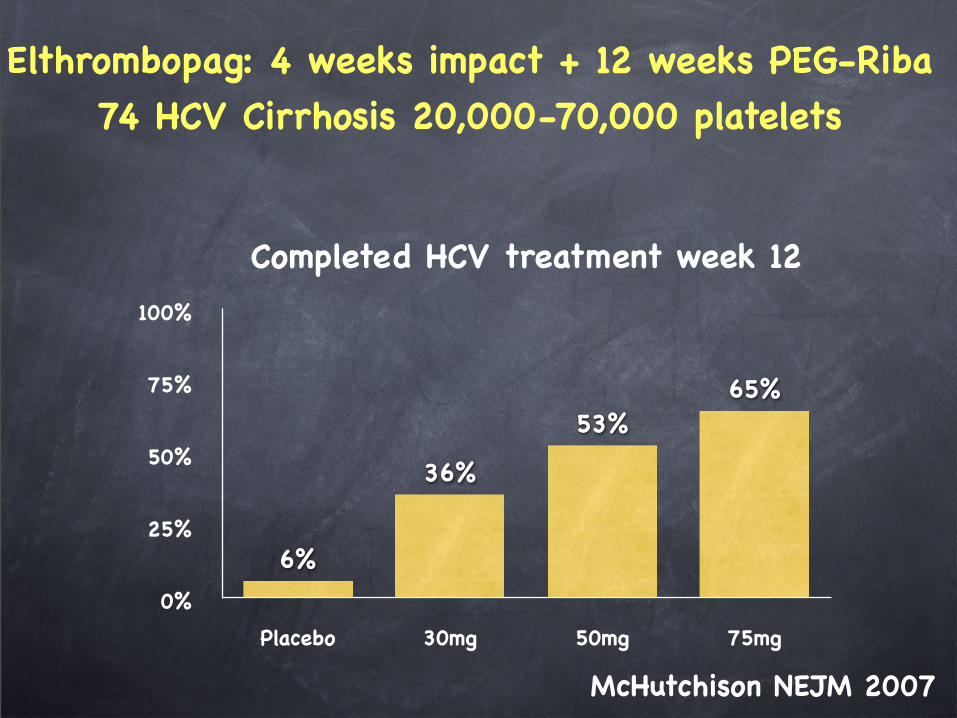
Elthrombopag: 4 weeks impact + 12 weeks PEG-Riba74 HCV Cirrhosis 20,000-70,000 platelets
0%
0%
25%
50%
75%
100%
Placebo 30mg 50mg 75mg
65%53%
36%
6%
Completed HCV treatment week 12
McHutchison NEJM 2007
Elthrombopag: 4 weeks impact + 12 weeks PEG-Riba74 HCV Cirrhosis 20,000-70,000 platelets
Elthrombopag: Adverse events
Headache
Thrombosis
116
Traitement hépatite C 2008
Intensifier dépistage
Simplifier bilan initial et suivi
Traiter « à la carte »:
• Fibrose, Poids, Stéatose, Age
Tolérance
Efficacité non virologique:
• Freiner la progression de la Fibrose