Embed Size (px)
Citation preview

� � ����������Vol. 34, pp. 93�99, 2006
������������� ����������������� �������� !�
��
���
���
��
��� :�� 18� 5� 25��
� ����������������������� !"#$%&'()*+,-� �.� !"#/0+*$�1-2& 34 5)(/67,���. ��� !89:�;<= >?@A BCD=E FG$����� 89��155H� ������ 48�>? 40�� �IJKLMKN�OI CT 8P�= DICOM server Q��.�R6%S�.�������TU �.�VWX2Y8;<= Z� !89:=E �.R$Q��[�A\/��@��]/^_= ������@�$Q����]`$2abE��6%S�.����TU\ ��@�$+c)\>?@%d�]/�T=*+E-������@/0+*$����.Q���]`-2abE 5�5A$�����$�]/$ef2+ ����.Q�� !"#-���$�]/ef,5A8]�=*+, gE �.�VWX$ ��@�$h[�/ ������@�$i[�/jk-�lm,Vk-nbE �op�qra( ������$������T Q��.� !#-ef�m& ��Qst��$������.Q�/F=* $u��n,5A-vabE wx y&�zm,%{/2bEi|}[���� ����i���~�/6+* 5)(����$����A=*���!8CDm,5A-��A��,
����lacrimal fossa, nasolacrimal canal, CT, postoperative status
��������� ����������������$Qst���# ����T ����[��l2Y����� !#-ef,A�v)*6d1��3� �?���\5)(/$� /��m, �.$��i[����[�/�gd Qst���iH8jk= [��/�& ��6%S������/%,Qst� !"#/!+�.�#\��U),- ���"�A=*�
���#�/0+*���$��(),\��4�5��;A=*�$�$%�-C =E¡d��()2+¢� £Ri|}�&¤/!+ ���� �������������~�$i|}[/¥v),5A-¦&2d §�A ¨~�©ª$«=&u¬=E6� =a= i|}�$�.���i�'���$()- ®���8¯,5A-�°c���CD±*A=*��²³´µ+A�l¶·¸���-��A2, �op�$ �IJKLMKN�OI CT Digital Imaging and Communica-tions in Medicine �DICOM� server /%, Multi�������� ,¹º�»¼
93
35

Planar Reconstruction �MPR� ����� �������� ����������������� ������ �������������
�����
�������� � ! 16� 5"�#$ ! 18� 3"�%&�'()���*� CT +,�-.��/��01� ��*23/� 89���466 �� �4 23 �; Caldwell-Luc 52 92 4� 6752#$�89�: ; 32.0 �� �<=��528 4� 23 ; 23.3 �� �<>���52 43 4�23 ; 9.3 �� Caldwell-Luc 52��<=��52 24� 23 ; 20.0�� Caldwell-Luc 52��<>=��52 10 4� 23 ; 29.0 �����59 �� ?� 30 �� �� 28�85 @� ; 60.1 @�ABC� ��*52�DE�����*F 48���� 32 �� ?� 16 �� �� 23�77 @� ; 52.9@�� ��*F�G�HI�CT�-.��� JKLMN�/� 40 ���� 18 �� ?� 22 �� �� 13�83@� ; 44.7@��O�� MNP� CT-.������ �QR� IS� T�EU�O�� ������ABCV�W !X#$�Y�Z�[�"�\]�^I��� ��*52&_`�� mucocele/�&a�b�� #+$���c���d�ef�ghijklj�16jklj�mnoh
CT Aquilion �Toshiba, Japan�� pq��� 22 cm�� %r 120kv� �%& 300mA� 500msec�17'�sntuvwx 0.5mm, yuz{|i 0�7 mm �mnoh{|i 11� �}~�� �� 14 cm� bone al-gorithm ���!��� }~(������ }~�Reid ��(& .&.��������u�pqg�n|�j 512�512 pixel )������ DICOM server&'��� ��x����h 300� ��x��* 1500 �� +��y�u�u Exavision �Ziosoft. Inc. � L�� MPR �����,�#$��-�.�.�ED$-.��� �
�/�����L/ABC=/�0�� ���������� ���L/�=/��*4������O�� ��$���1�&��D.���� ���&a�b�������/�&B���+$���Fig. 1�� �$& ¡c�2¢=3�£¤4&�������I4¥�¦§¨��5�� ��������©ª/�I�%«6�/��23/�&a�b��423/��¬c&����� ��$��5£�MNPc23P� MNPc����*FPc�7®�� T-test � t0.05 �8¯°O�c�b+5��� ±�� L²9�:³��<´�& grade 0;µ¶E�� grade 1; ·;µ¶� grade 2; <$#Eµ¶� grade 3; =��µ¶��¸�9c�b>5�³E�� � 4a� grade &?@���
� �
��*23�1554�� ����*F�964�� MN�804���P����L/0�� ���=/0������������ ���L/�=/��*4���� ;AABCB�C°� Table 1 &��cA
Table 1. Mean Diameter of NLC, Wall Thickness of LF and NLC in Postoperative group �only on PostoperativeSides�, Chronic Sinusitis Group and Normal Subjects
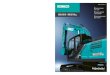
Fig. 1. Thin and uniform bony wall of LF in a 37-
year-old woman with chronic sinusitis.
¹º»¼94
36

����� ������ ��� ��� 5.6mm, �� 6.0 mm ��������� �������� 4.7 mm, 4.9 mm, ������� 4.4mm�� �� !�"#$%� ���������&'%�()*+"#�� ����������������()*�������� �� �,&-()*�"#./���t�0.13�� ��0�12�34�� � 0.63 mm, ������ 0.40 mm,�� 0.37 mm�� �����56()�73�-&��� �������,&-� t�0.49�()*�./��� �����������812�34�9%:%� 0.64�0.78mm, ������ 0.45�0.59 mm, �� 0.44�0.50 mm �� ����������56()�73�-&�� �Fig. 2�� �������,&-� t�0.49�����()*�.;� ����<().73+"#�� ���� � ��0�2
3� ����23�=6-�� ����>?����56()� � @A1273��������������������0�12�34� ������B CDE12�34�C&-()*�"#$%./��� �����FG��=�HIJ�� K8LMN�HI+�� O8HI+P�JQ���RS� � 0.92 Q� �������4.3 Q� �� �2.9 Q�� ������K�LN�TM� ��������O�LN�TM�HM����� ���56��� ���()*�"#$%��� UVW*�X�@Y; over-lap=�Z[�/.�\]=����012�34�^_`�,&-�� ���� 53�155�34.2��� ������ 11�96�11.5��� �� 14�80�17.5����>?�abQ�������0273�c�de���0fL 78� fL/$Fg� 78� Fg� 38� Fg�/$L 48� L 328����� h�� �����02�ij73 28� kl�.���� 18�����12��dmn�-&��� 38�oh%-&�� p1q�rs���0O8�tu��>?��� 2 8� ������� 1 8"#$%��vL� w8����� �������������xy�K2gz{�|_X�9%:%�39.4� 32.9� 32.1 cm ���� w8�������(). @+}���� ��������()*�./�� �Table 2���~q�@Y4�,&-� Table 3 ��C�����q�����& grade 34 � 63�9� +�#����� �Fig. 3�� ���������'/� 1��� grade 0� grade 1 ��� 84.4�� 14.6�\]���
Table 2. Mean Distance between Outer Wall of Lower NLC in Postopera-
tive Group �Cases with Bilateral Operation�, Chronic SinusitisGroup and Normal Subjects
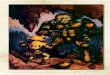
Fig. 2. A thickened bony wall of left LF �arrow� in a85-year-old man after operation.
����������D�������� 95
37

� �
�������� Unger1� ��� ����� � ��������� Caldwell-Luc ������������ ����� !� "#$�%&� '�(�)*+,� ����-./012�3�� 45� 67���8 ��������� !9:7�� "#$�%&/012�3�1��3�� ;21 <���=�>?� @3�����A�B�C����D��� EF7GH ����=IJ�KL4�/M12����� ��=�NO�P>?��QRS�T�5��UV�WX�5YZ[�51P3� '�C\� 0.2�0.4mm�'���]��^���� ���_*/"#�_`ab� �*/�� �Z>cd2�3��
"#����e�_�����*�������e������_*��>cd2�����fgd 5�17 mm�KLd2�3�7�� hij���������!d� ��k 0.63 mm ���k/�l !��3�/� ;2 Caldwell-Luc ���mn ��$op�/qr2�D�/stuvw�;�/Fx�N@�yz12�� ��$op�� CT
"� ��{|����}~�����d2� ;2 ������"���=�����\������/��d2����=��S"#���e/� C�"�S���� C�)�S)���/>c��3�8�� �7��=�d 17�20 mm�7�� ����"��1)� ��� @2� C\ 3��5����/�Z��* 5 ��30 ����S�@��r29�� ���W�����k�C\ 2.9 ���������3�� hW����D����/�l �)* +,��35/� ;2������"#$�%&/��� ����C\�/�* ��w����� ��=��,��+,� ��=)��\� ¡�¢f/��5�yz12�� ���"#$�fgd�£¤�� ¥1� %&��tm¦§¨P4� %&�5��/��k� 6©Sªz5� «��67���8k�%&/¬12P3�� �®��r¯�P%&/°�±²�� ¥1�P%&S�wD� 1��M��Z� 67���8����C\���*+, ³1P3´¨7/yz12�� ��k���=�\� ¡/�l ¢f��35� «�� 67���8k�)���=�µ�¢¶�l��®5���� ��=�\� ¡ �����l·/Pt� ��¸��)*��+,��S¬P�®5� ;21�;��1�"�´¨7/��d2��¹_�Zqr2�35 Caldwell-Luc � «��
Table 3. Size of Maxillary Antrum in Postoperative Group �only on Postoperative Sides�, ChronicSinusitis Group and Normal Subjects
Fig. 3. A 58-year-old woman with bilateral postopera-
tive sinuses. Contraction of the maxillary antrum
and thickened wall are noted on the right side.
Right NLC shows dilatation and thickened wall.
Left side shows neither antral contraction nor
dilated NLC.
ºF»¼96
38

������������� ��������� ������ �FESS; functional endoscopicsinus surgery�� Caldwell-Luc����� ��������10�� ����� Caldwell-Luc � �!"�#�$�% !"�&&��'()��*�� � +� FESS �,-�./�0&���Caldwell-Luc � �0&�,-�%1�234�� +56��� ��56�!"�7�8�9��'()���:;���<������ =>����?����� �@�A�����B�� C� 10D���E�FG� ������HI�JK�L� #HM��N�L�OP4B�6�� ����4����� ���� �@�A���4� ���Q������=R��S��T��11�� Russell)5��� ?U ���VWX�J�<#��RY�CT 4�Z[� #��RY�S� CT� ��\]��^���_`�����a[<��� �� �4����b/� ��\]��^RY�S� c��T4B��4� ���K)��S�d!#�e��fg��"#��� h�� �������J�<ij$4B��?�Qk�������lm� �� ������ 1980�nK)%o[<m�� ����i#�e�Q&pA�q_'��rstu�e��([������ /)v�[<���Vwxyz�G�<�� {8|*��-�+}~�,�-��i��G�<�WX%!.���&� �,i�T4B����a�B�12�� [K[� ���� v/�0�#�4��Vwxyz�!"�b/��� �����V�� 1��B��-�� w����<��������HK2K�23A�"#�B�� ��3�#$����� v/4%!A���������4�A������ �4�������� =>�Q�����4���4B�� 58����v/4i��V��4�����#����$�B��-� ��VWX������b/���6�#e��77���� �� ����� =>����V����mv/48��9���6��:234�K������V��������;A�� v/4��� ��;��T4B�� [K[�)� #�$��-����� K)�<����44m�� #��=>�id!��A7�8�!"�� I���W�4B�������� =>
��56�=�G���13�� ��3�#$�I��7�>�kpG��?�L4B�� :���56�����!L�� �¡¢A��-�e������ �4�������J�<#e���T��S4m� CT�� 2£�[<¤�@4� � �CT �¥�A��4� $�RY��44m� �HKG¦§����¨©4m��ª(�� [K[� ��3K)��V� CT2£�«¬�AB�C(�i�4B�� ���� �����3���V�1=� #$®�¯°±�i�v/�¥�A����D²[��'(��
� �
���� v/Q58����v/4���3���V�=Y1��³¡�´µ[�� ¶�+� c[� ��)�v/4�=Y1�����!�����E)K��� ����3���V�=Y1��x·��a��<J)�� %1�4���¸���� $� ¹��Fr�4�A����� º&G»A������� ����� =>�Q�� ���������� ¢��[<iHIG�'()���
� �
1� Unger JM. The paranasal sinuses. In: Paul LWand Juhl JH �eds�, Paul and Juhl’s Essentials ofRoentgen Interpretation, 5th ed, J. B. Lippin-
cott Company, Philadelphia, 1987: 1051�1065.2� Mancuso AA and Hanafee WN. Computedtomography and magnetic resonance imaging
of the head and neck, 2nd ed, Williams &
Wilkins, Baltimore, 1985: 20�41.3� Som PM. CT of the paranasal sinuses. Neuro-ladiology 1985; 27: 189�201.
4� Massoud TF Whittet HB and Anslow P. CT-dacryocystography for nasolacrimal duct ob-
struction following paranasal sinus surgery. Br
J Radiol. 1993; 66: 223�227.5� Russell EJ Czervionke L Huckman M DanielsD and McLachlan D. CT of the inferomedial
orbit and the lacrimal drainage apparatus:
Normal and pathologic anatomy. AJR 1985;
145: 1147�1154.
���� ���������¼�=Y1� 97
39

6� ������ DCR ��������� ��� 2004; 17: 206�207�
7� ����� II� ������ ����� � !�� "#$%� &'(� &)*+��Practical ophthalmology. ,-.� /0� 2003:12�17.
8� 12345� 678��9� :;.� /0�1979�
9� Zinreich SJ Kennedy DW Rosenbaum AE
Gayler BW Kumar AJ and Stammberger H.
Paranasal sineuses: CT imaging requirements
for endoscopic surgery. Radiology 1987; 163:
769�775.
10� <=>?@� �ABC� �� D�E� ��FG 2004; 20: 652�664.
11� ������ DCR �����H��� ��� 2004; 17: 378�380.
12� Hunink MGM de Vries-Knoppert WAEJ
Balm AJM and Luth WJ. Dacryocystography
after paranasal sinus surgery. Br J Radiol.
1988; 61: 362�365�13� Wormald PJ Kew J and Hasselt A. Intranasal
anatomy of the nasolacrimal sac in endoscopic
dacryocystorhinostomy. Otolaryngology�Head and neck surgery 2000; 123: 307�310.
IJK298
40

Abstract
Deformation of Lacrimal Fossa and Nasolacrimal Canal after
Paranasal Sinus Operation and in Chronic Sinusitis.
Yoshiko Kurihara
Objective: As have been already described in the literature, the bony wall of maxillary antrum is
thickened and sclerotic, and antral contraction may occur in chronic sinusitis and after paranasal sinus
operation. However, bony nasolacrimal canal �NLC� is also deformed, but no quantitative data have beenpublished on bony NLC in patients with postoperative status and chronic sinusitis. In the present study, I
have measured the diameter and the wall thickness of lacrimal fossa �LF� and NLC.Materials and methods: Eighty-nine post-operative cases of paranasal sinuses �bilateral 66 cases,
unilateral 23 cases, mean 60.1 years; male�female�59�30�, 48 cases with chronic paranasal sinusitis �mean52.9 years; male�female�32�16,� and 40 normal subjects �mean 44.7 years, male�female�18�22� weremeasured. The diameter of NLC �upper and lower portions�, medial wall thickness of LF and NLC weremeasured. The outer distance between distal end of bilateral NLC and angle of inclination of NLC were also
measured. CT examination was performed with multidetector CT with 0.5 mm collimation and measure-
ment was performed on Exavision �Ziosoft�, with reconstruction.Results: The mean diameter of NLC in the post- operative group �upper; 5.6 mm, lower; 6.0 mm� was
statistically enlarged as compared with that of normal subjects �4.4 mm both�. The chronic sinusitis group�4.7 mm, 4.9 mm, respectively� showed no statistical deference from the normal group in upper diameter ofNLC. The wall thickness of LF and upper NLC in post-operative groups were statistically thick �post-operative; 0.63, 0.64, normal; 0.37, 0.44 mm, respectively�, however, those in chronic sinusitis group were not�chronic sinusitis; 0.40, 0.45 mm, respectively�. The angle of the inclination of NLC showed outer deviationin the postoperative group and inner deviation in the chronic sinusitis group.
Conclusion: After the operation of paranasal sinuses, dilatation of NLC and thickening of bony wall of
LF and NLC occurred definitely, and these phenomena were confirmed statistically. It is said that both
postoperative sinus and chronic sinusitis have sclerotic and thickened bony wall of maxillary antrum,
however, consequence of statistical deformation of LF and upper NLC occurs only in the former. Currently,
dacryocystorhinostomy and sinus surgery have been performed endoscopically. This technique can reduce
surgical invasion dramatically, but there is no information on bony structure. The structural change of
lacrimal drainage apparatus should be considered and ensured before these operations. Evaluation of
postoperative NLC and LF with CT scan is an adequate technique which will avoid technical trouble during
the operation and complications.
Department of Radiology, St. Marianna University of Medicine
�������������� ��� 99
41